stroke in children
TRANSCRIPT



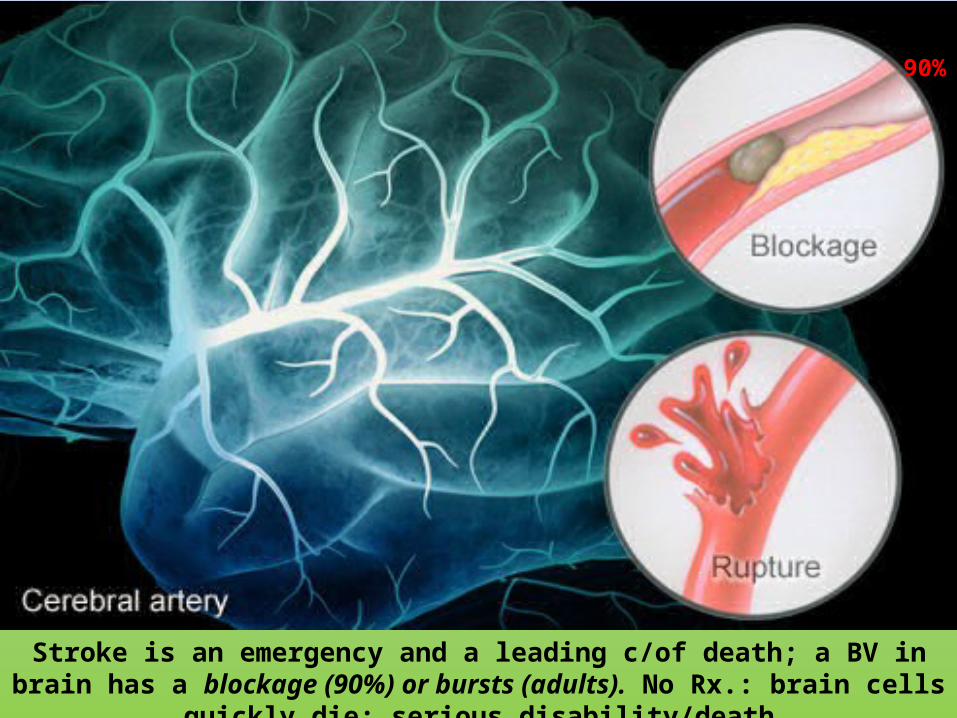
Stroke is an emergency and a leading c/of death; a BV in brain has a blockage (90%) or bursts (adults). No Rx.: brain cells quickly die: serious disability/death
90%
Stroke is sudden onset of focal neuro-deficit due to occlusion of blood supply or hemorrhage in the brain causing SS lasting >24h
SS: symptoms and signs. BE: both eyes
Definition

Bangladesh Scenario
• Stroke is the 3rd leading c/of death• WHO: Bangladesh at mortality from stroke ranks 84• Prevalence: 0.3%. HTN is the main cause of IS and HS• Disability-Adjusted Life-Years from stroke: 485/10k• GoB needs to emphasize healthcare development to cope
with stroke
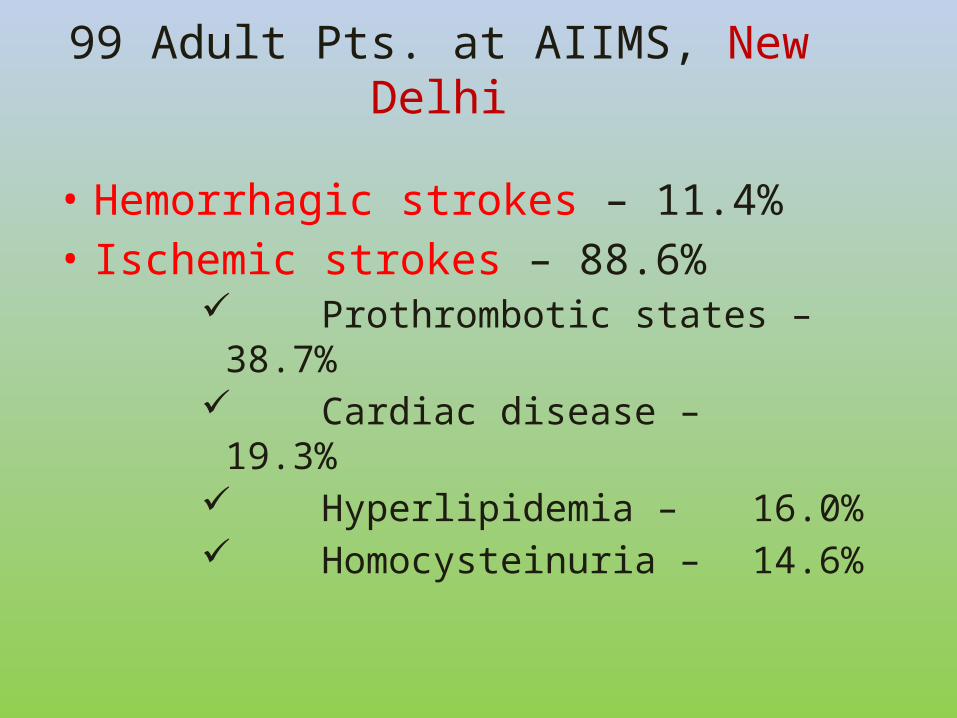
• Hemorrhagic strokes – 11.4%• Ischemic strokes – 88.6%
Prothrombotic states – 38.7% Cardiac disease – 19.3% Hyperlipidemia – 16.0% Homocysteinuria – 14.6%
99 Adult Pts. at AIIMS, New Delhi
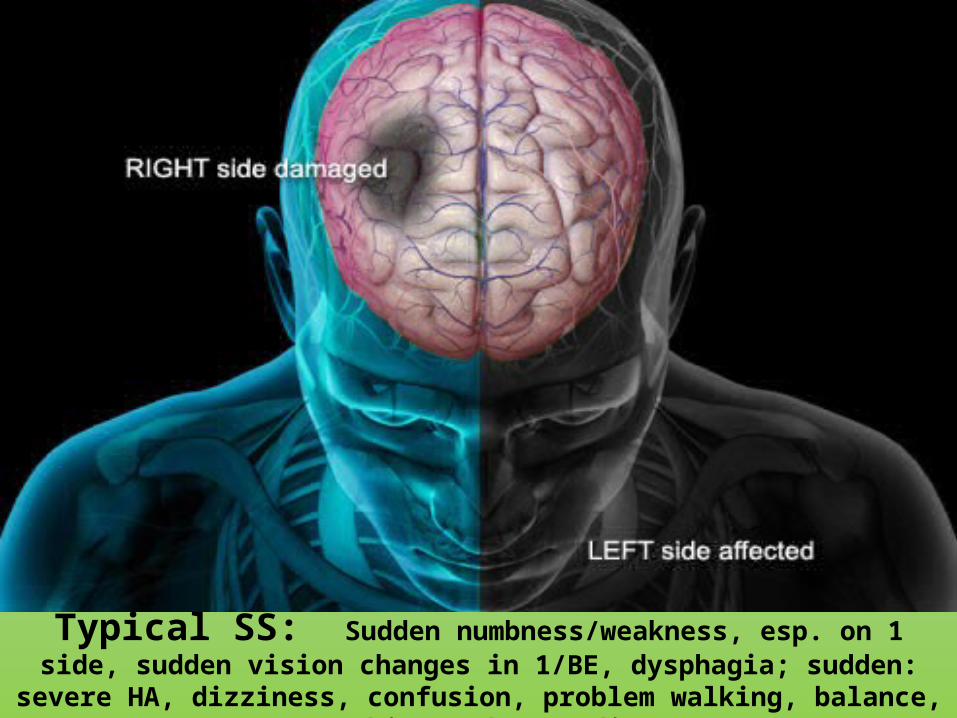
Typical SS: Sudden numbness/weakness, esp. on 1 side, sudden vision changes in 1/BE, dysphagia; sudden: severe HA, dizziness, confusion, problem walking,
balance, speaking/understanding

Test: F.A.S.T.: Face: smile: 1 side droops? Raise Arms: does 1 side drift down? Speech. Can s/he repeat a simple sentence? Trouble talking, slur words? Time

STROKEIN CHILDREN

• Not exactly known; 3-13/100k/y• In INDIA: 13-33/100k/y • USA: 2.52/100k/y –14y– 1.89– hemorrhagic– 0.65- ischemic
• Children & Young adults: <5% of all strokes• Occurs in all age groups (NB-teenagers)• It may even occur before birth• 1/2,300 – 5k/NB have a stroke
NB: newborn. LB: live born
Incidence in Children
• Stroke is the 6th c/of death in children while in adult it is 3rd, ranking behind HD & cancer
• As common as brain tumors
• Impacts of strokes– Mortality 6-40% (hemorrhagic: x2)– Morbidity• Neurological d – 60%• Seizures – 15%• HA

Risk Factors Childhood Stroke (USA)• Cardiac D 19%• Coagulation D 14%• Dehydration 11%• Vasculitis 7%• Infection 6%• Dissection 5%• Neoplasm 4%• Metabolic D 3%• Moyamoya, SCD, Perinatal
Complication, andOthers: each 2%
Multiple risk factors are often present& predict worse outcome

Congenital
Aortic Stenosis, MS VSD, PDA Cyanotic CHD involving R-L shunt Inherited con. tissue d: Marfan, Ehlers-Danlos syn
Acquired Endocarditis, cardiomyopathy Arrthymia, Rh F Psoriatic HD
Cardiac Causes
Diagonal earlobe crease

• Disorder of RBC: SCD, Polycythemia• D. of WBC: Leukemia, lymphoma• D. of Platelets: Thrombocytosis, -penia
• D. of clotting: Protein C, S deficiency Factor V, antithrombin III deficiency Paroxysmal noc. Hb.nuria IBD, lupus anticoagulants Neonatal & childhood CSVT
Hematological Causes

SCD– 25 % develop stroke by 45y. Recurrent in 67%– IS predominantly in childhood– Hemorrhagic with steroid and HTN– Sinovenous thrombosis, posterior leukoencephalopathy,
watershed ischemia– Silent infarcts; more in the frontal lobe (17% under14)– HS (ICH/SAH) in adults– High WBC in inf. and anemia can precipitate
IS: ischaemic stroke. HS: hemorrhagic stroke

Moya –Moya AV malformations Aneurysm Sturge Weber syn Fibromuscular dysplasia
VASCULAR DISEASE
Normal lateral projection angiogram with injection of IC artery
Suzuki grades I to II with narrowing of IC artery before dev. of extensive collateral vessels


• Infection Meningitis HIV encephalopathy Local head & neck inf.
• Autoimmune d. SLE, Takayasu arteritis, PA nodosa Sarcoidosis Mixed CT D
INFLAMMATORY DISORDERS

METABOLIC DISORDERS
• Homocystinuria• Pseudoxanthoma elasticum• Fabry disease• Mitochondrial encephalopathies:
MELAS Leigh syn
Drug induced Amphetamines, cocaine

• Trauma• Child abuses• Placental embolism• ECMO therapy• Post varicella
Misc. Causes



Thrombosis occludes anterior, middle, posterior basilar, vertebral & internal carotid arteries. Arterial thrombosis more
common at atheromatous plaques or stenosis of arteries
Thrombi embolise to distal region
Causing intracranial ischemia & infarction
Intracranial Thrombosis

Emboli arise mainly from atheromata
within great vessel or from heart
Intracranial Embolism

Pathophysiology of Hemorrhage
20 % strokes are from rupture of IC aneurysmChacot – Bouchard aneurysms are usually due to chr. HTN
They usually involve small penetrating (0.8-1.0 mm) lenticulostriate br. of MCA in the basal ganglia, brainstem and midbrain. Cause IC hge.




Arterial ischemic stroke (AIS) Cerebral SinoVenous thrombosis (CSVT) IC hemorrhage
Types of Stroke Syn.

SIGNS &
SYMPTOMS

Seizures
Extreme sleepiness
A tendency to use only 1 side of body
Newborns and Infants
CN: cranial nerve. HA: headache. V: vomiting
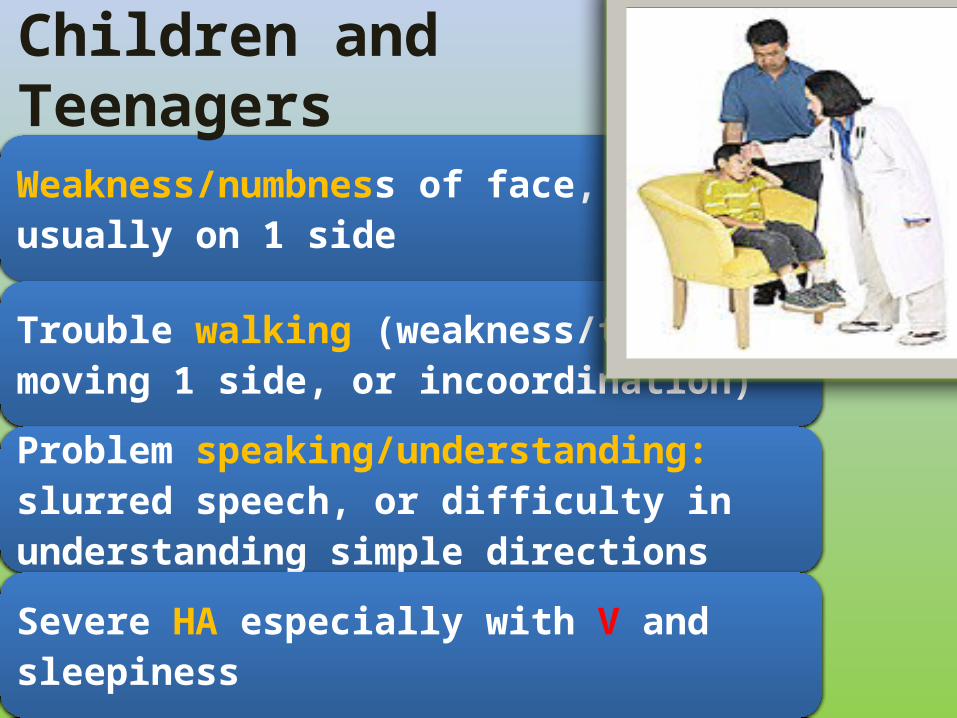
Weakness/numbness of face, arm/leg,usually on 1 side
Trouble walking (weakness/trouble moving 1 side, or incoordination)
Problem speaking/understanding: slurred speech, or difficulty in understanding simple directions
Severe HA especially with V and sleepiness
Children and Teenagers

Trouble seeing clearly in 1 or both eyes
Severe dizziness/incoordination: losing balance/falling
New seizures, especially if affecting 1 side of body and followed by paralysis on the side of the seizure activity
Progressively worsening non-stop HA with drowsiness and repetitive V, lasting days without relief
Complaint of acute onset of the "worst HA of my life"
Contd….

Lesion can be divided in 2 groups based of CN palsy as :
CN palsy on same side as that of hemiplegia
CN palsy on opposite to that of hemiplegia
Localization of Lesion in Hemiplegia

• Lesion above the level of brain stem (Ipsilateral hemiplegia); at the level of either
Cortex Sub cortical region Internal capsule
CN Palsy on Same Side as that of H..
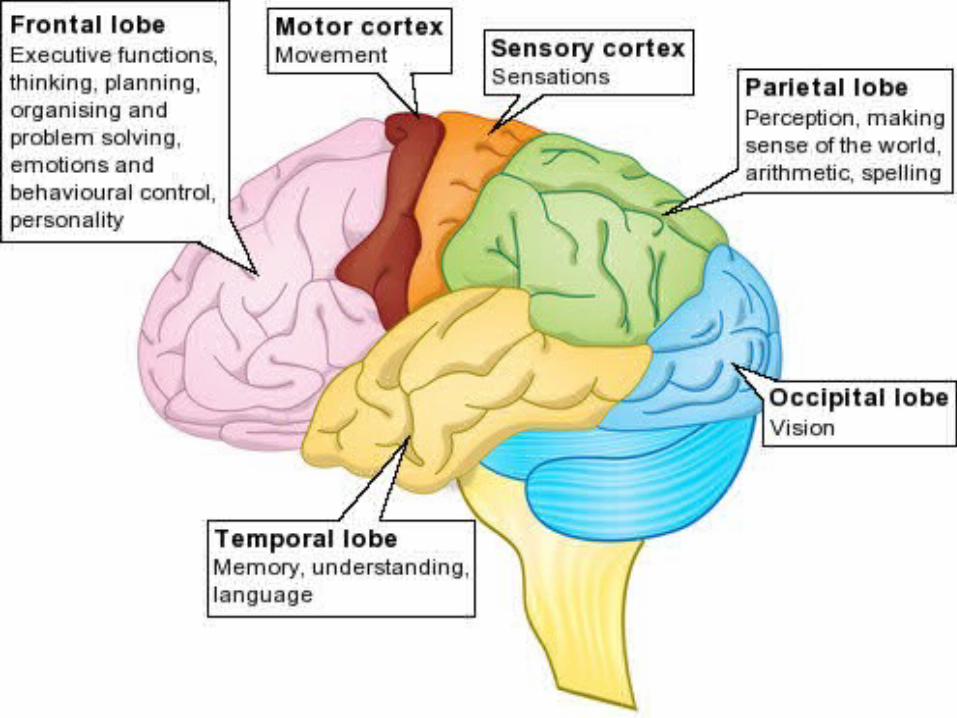

Lobes of the Cerebrum
Parietal Lobe
Temporal Lobe
Frontal Lobe
Limbic Lobe
Occipital Lobe


• Hemiparesis or Monoparesis• Involvement: Upper limb > LL or vice versa• Altered sensorium, convulsion
• Cortical sensory loss: asteriognosis, agraphesthesia • Aphasia (If dominant cortex)
Cortical Lesion

Frontal Lobe
is responsible for higher cognitive functions:
• Problem solving• Spontaneity• Memory• Language• Motivation• Judgment• Impulse control• Social/sexual behavior

• Altered behavior• Upper limb> LL• Motor aphasia• Convulsions• Bladder & bowel involvement• Persistent neonatal reflexes on opposite side
Frontal Lobe Involvement

Parietal Lobea role in our sensations of touch, smell, taste. It also processes sensory and spatial awareness,
and is a key component in eye-hand
co-ordination and arm movement
It also contains a specialized area
called Wernicke area that is responsible
for matching written words with the sound of
spoken speech

–Cortical sensory loss–Astereognosis
Parietal Lobe Involvement

Temporal Lobe
plays a role in emotions, and is also responsible for smelling, tasting, perception, memory, music, aggressiveness, sexual behavior
It also contains the language area

• TL epilepsy• Sensory aphasia• Memory loss
Temporal Lobe Involvement
Occipital Lobe
controls vision and recognition

OCCIPITAL LOBE INVOLVEMENT
Homonymous hemianopia

INTERNAL CAPSULE LESION
Dense hemiplegiaHemianaesthesiaHomonymous hemianopiaDysarthria
SUB CORTICAL LESION
Similar to cortical lesion except loss of cortical sensation & convulsions

• Lesion at/below the level of brain stem (Contra lateral hemiplegia). Lesion can be either of
Midbrain Pons Medulla Spinal cord ( b/w C 1 – C4 )
CN Palsy on Opposite Side to that of …

• Weber Syn.: CN3 palsy + contra lateral hemiplegia• Benedict Syn.: CN3 palsy + contra lateral H + red nucleus
affection( tremor, rigidity & ataxia on opposite side)
H: hemiplegia
Mid brain lesion
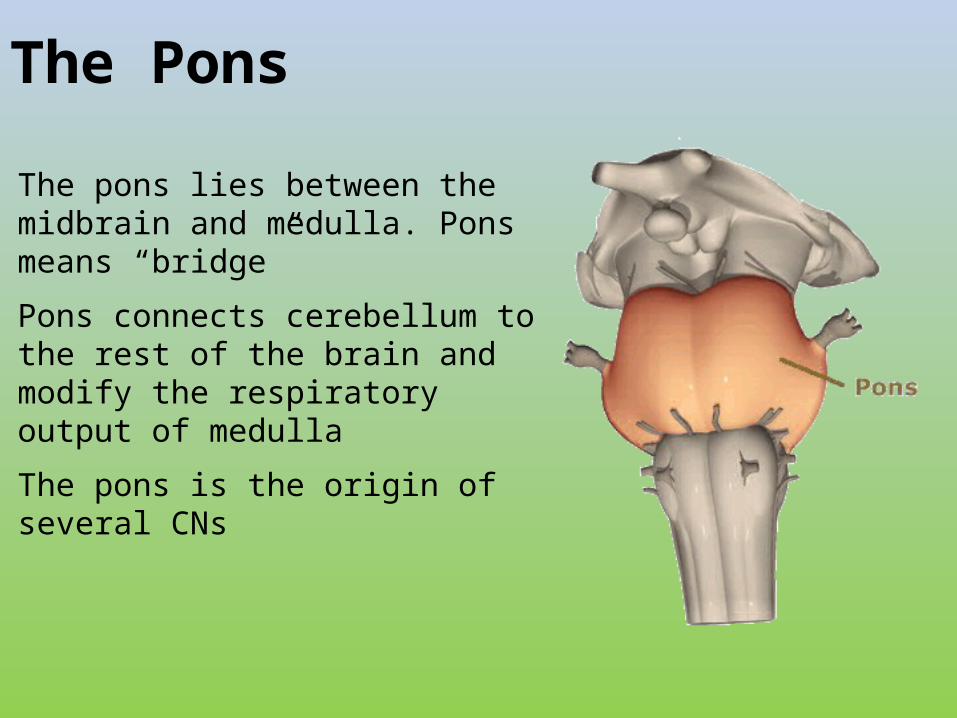
The Pons
The pons lies between the midbrain and medulla. Pons means “bridge”
Pons connects cerebellum to the rest of the brain and modify the respiratory output of medulla
The pons is the origin of several CNs

• Millard Gubbler Syn.: CN7 palsy + contra lateral H• Foville Syn.: CN6&7 palsy+ contra lateral hemiplegia
Pons lesion

• Jackson Syn.: CN12 palsy + contra lateral hemiplegia
Medullary lesion
• Brown Sequard Syn.: Hemiplegia + CN palsy + differential sensory loss (loss of vibration & joint sense on same side & pain ,touch & temp. on opposite
Spinal Cord Lesion
Focal cerebral ischemia IC hemorrhage Cerebral abscess, encephalitis (HSV) Brain tumor Alternating hemiplegia of infancy MS Malingering/conversion disorder Epilepsy: Todd's paralysis or a focal inhibitory seizure Complicated migraine
Differential Diagnosis
Seizures
Raised IC tension
Hypertension
Aphasia
Skeletal deformities
Complications
• FIRST LINE: Performed within 48h of admission • SECOND LINE: Performed within first week • THRID LINE: Performed as per need
Diagnostic Evaluation

CBC FilmBlood sugar, BUN, S electrolytes ( Na, K, Ca, Mg, Phos.) AST, ALT, S. lipid profile CXR, CT brain, MRI brain & MR angiography Ultrasonography ANA ECG
FIRST LINE


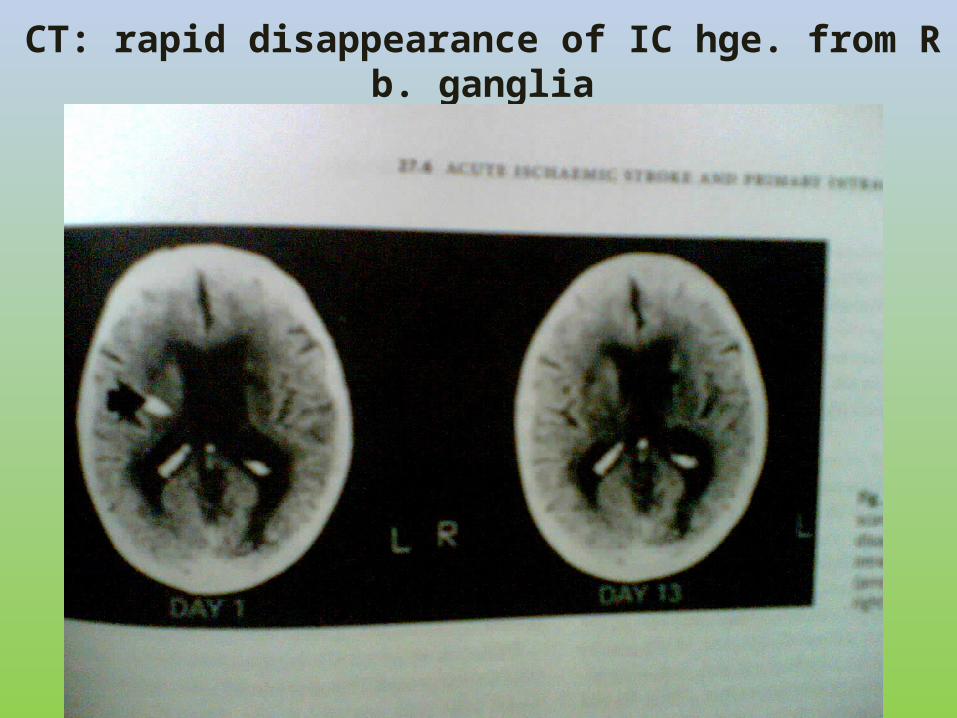
CT: rapid disappearance of IC hge. from R b. ganglia

Echo- (transthoracic) with saline contrast Transcranial and/or carotid dopplers MR angiogram, EEG Rh. Factor, S. amino a., urine for organic a. Blood culture. Hb. electrophoresis Complement profile, VDRL Lactate/pyruvate, ammonia CSF: cell count, protein, glucose, lactate
SECOND LINE

Antithrombin III Protein C (activity and antigen) Factor V Leiden mutation Antiphospholipid antibody; Lupus-anticoagulant Anticardiolipin
Hypercoagulable Evaluation

HIV Lyme, Mycoplasma, Cat-scratch titers Cardiac MRI Echocardiogram (transesophageal) Muscle Biopsy DNA testing for MELAS Cerebral angiogram (transfemoral) Leptomeningeal biopsy Serum homocysteine after methionine load
THIRD LINE

MANAGEMENT

Time = Brain Damage: every second counts. Hypoxia kills brain cells within mins. Clot-busting drugs can curb damage, if used in 3h of attack. Stroke is a top c/of long-term
disability

• 1st step is to DD ischemic & HS• Anticoagulant Rx is contraindicated in HS• Hyperglycemia & HTN worsen the stroke• Multidisciplinary approach
General Consideration before Rx

Rx primarily is directed towards stabilizing systemic factors & management of the underlying causes
Arterial Ischemic Stroke (AIS)

Intracranial tension:1. Fluid restriction2. Mannitol3. Steroids
4. Shunt surgery ( In special case)
Hypertension: by appropriate antihypertensive
Supportive Care

Fluid balance Hyperglycemia Hyperthermia Seizures with AED ABT to prevent secondary inf.
AED: antiepileptic drugs, ABT: antibiotic
Contd…..

HEPARIN: -
•28U/kg/h in infants,
•20U/kg/h in >1y
•18U/kg/h in older children for 5-10d
•LMW Heparin: 0.5-1U/ml
Loading dose 75- 100 /kg iv over 10 min followed by
maintenance dose :
Antithrombotic Rx

Antiplatelet: -Aspirin 3-5mg/kg/d Clopidrogel
Oral anticoagulants: Wafarin for secondary prevention of stroke if aspirin Fails. Congenital or acquired HD, severe coagulable states, arterial dissection & recurrent AIS or TIA while on aspirin
Thrombolytic agents: streptokinase & urokinase to dissolve the existing thrombus
Contd….

Physiotherapy
Occupational therapy
Psychological therapy
Rehabilitation Therapy

Surgical repair of Fallot T
Regular phlebotomy for thrombosis in Polycythemia
BT to prevent future episodes of stroke in SCD
Surgery for AVM & aneurysm
Steroids & immunosuppressants in autoimmune d.
Specific Rx

Variable. Mostly dependent upon underlying cause80% survived 10y after an IS, most with residual
hemiparesisPoor prognosis with seizures during infancy, and with an
angiographic pattern of Moyamoya disease
HS have higher mortality than IS Pts. with HS & coma have higher mortality
Prognosis

Persistence of hemi paresis one month after the stroke
cortical location
Moyamoya pattern on angiography
Risk Factors for Poor Outcome

Early Dx and intervention for children with stroke in order to improve their recovery rate and prevent recurrence
Early Dx and close monitoring of children at high risk for stroke
Education and support for families of children with strokes
Education about childhood stroke for HCP
Education for the general public about childhood strokes
Ongoing research into the causes of childhood stroke and effective Rx and prevention strategies
GOAL

Amiakum falls, Bandarban!

THANKYOU