stroke mimic 2019 few pics - worh.org
TRANSCRIPT

• To Join: • Text KERRYAHRENS516 to 37607 • For all future texts, you text your choice A-E
polleverywhere.com

Kerry Ahrens MD, MSBayCare Clinic Emergency Physician Associate Professor EM UW School of Medicine Medflight Physician Medical Director Oshkosh Fire Dept Co-Chair Wisconsin Stroke Coalition

Disclosures:
• On speakers bureau Genentech

Stroke Mimics
OBJECTIVES
!5
• Discuss & learn the pathologies behind various stroke mimics
• Distinguish stroke mimic vs ‘chameleon’ • Objective & subjective methods to
distinguish a mimic from a stroke • Discuss medical & financial ramifications
of mimics

Stroke is an Emergency!
!6
• 795,000/year

You wake up in the morning, look in the mirror…
!7
•

!8

= Rapid Stroke Activation
!9

Target Stroke Best Practices
!10
Initial Patient Evaluation →10 min Stroke Team Available →15 min CT Scan & Lab initiated →25 min CT Scan & Lab eval →45 min Evaluate t-PA inclusion/exclusion criteria Administer t-PA → DTN goal 60 min *Target Stroke Elite DTN <45 min Pt transferred to inpatient setting → <3 hrs

!11

Case
!12
• 37 yo F pmh obesity, anxiety & depression here with numbness to her R hand/arm, with inability to move hand in addition to difficulty getting her words out. All symptoms began suddenly around 7:30am. Symptoms lasted 10 minutes then are now resolving - after numbness improved, her speech slowly returned. She also had some visual symptoms. Denies fevers, chills. no h/o cardiac issues. Denies abdominal pain, nausea, vomiting or diarrhea. No recent head injuries.

Stroke Mimics - a lot to consider…
!13
• Rate ranges from 9-31% of CVAs • 60% of TIAs
• Approx 8-17% admissions Hyper-Acute Stroke Unit • Several Mimics • difficult to distinguish during Code Stroke!
• $$Cost$$ • unnecessary use of healthcare $$, resources, practitioners
• OMG! I tPA’d that migraine!!!
Allder et al 1999, Dawson 2016

SEIZURE ~20-40%
!14
• One of most common stroke mimic in ED pts • tend to present in POST-ICTAL phase
• + symptoms • motor changes • paresthesias
• neg symptoms ~40% occurrence • postictal aphasia • paresis
• Tend to occur MORE after PARTIAL SEIZURESβ• HOWEVER: seizures HAVE occurred in
CVA⍺• 40% after ischemic stroke, 57% after ICHβGallmetzer et al. 2004, ⍺Bladin et al 2000

Conversion Disorder 0-47%
!15
• ‘They know not what they do…’ • Often have documented psychiatric Hx • depression • fibromyalgia
Lewandowski et al 2015

Glycemic Abnormalities
!16
• Hypoglycemic ~ 32mg/dL • seizure • hemiplegia ~2% ( R>>L…don’t know why)
• Hyperglycemia - DKA, HHS • theory: caused by cellular hyperosmolarity • homonymous hemianopsia • hemiplegia • hemisensory deficits • aphasia • hemichorea-hemiballismus
• Corrects w Glucose correction

Toxic Ingestions
!17
• Can cause: • sedation • altered behaviors
• 1 reason ECG is key in CVA work up • Alcohol intoxication known to cause
lateralizing sx • Salicylate OD (chronic) • → confusion

!18
• Hyper, Hyponatremia • Hepatic encephalopathy • hemiparesis, hemiplegia • seen in ~ 17.4% liver patients
Cadranel et al 2001
Combined Toxic + Metabolic ~ 38.0%
Other Metabolic Abnormalities

Sepsis ~6-20%
!19
• Causes • Encephalopathy • delirium→coma
• Anamnestic reaction • person w prior stroke history weakened by
infection

Migraine ~10-19.6%
!20
• ~25% patients have focal neuro deficits • Theory: due to cortical spreading depression
• aka: excitation of neurons leads to inhibition • Hemiplegic migraine • aura accompanied by motor weakness
• Other Sx • dysarthria, focal weakness, vertigo, ataxia, AMS
• a small # pts have permanent neuro changes 😵 • BUT: 30% stroke patients may have headache at
CVA onset!! 🤬
Goldstein et al 2005
Syncopal Episode ~ 13% mimics
!21
• Can be 1st sign of subarachnoid hemorrhage
• Often confused with vestibulobasilar artery strokes • →AMS

Neoplasm ~2.8%
!22
• 12% diagnosed CVA’s @ presentation→tumors
• Most Common Presenting Sx • vision changes • aphasia • pure motor hemiparesis
• Tend to be Gliomas • also NS lymphoma • Anaplastic astrocytoma

Degenerative Neurologic Disorders
!23
• Multiple Sclerosis • brief paroxysmal sx • dysarthria • ataxia • diplopia, optic neuritis • VF deficit
• sensory deficits • Leukoencephalopathy ($5 word) due to viruses • ADEM (acute demyelination encephalomyelitis) • post-viral, immune-mediated process • shorter onset sx than MS • pediatric population

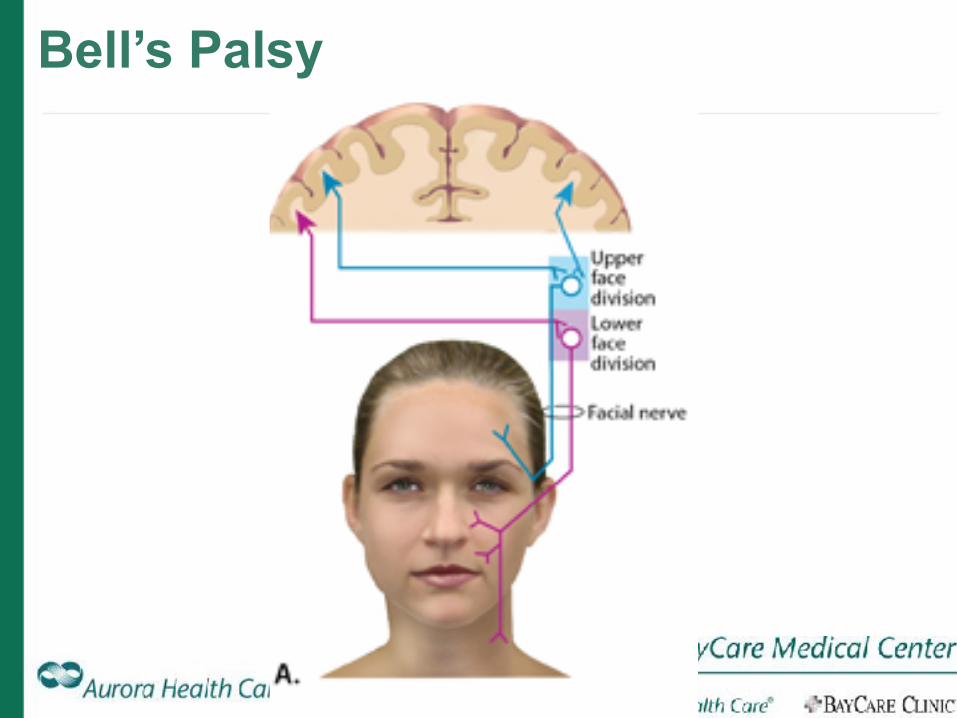
Bell’s Palsy
!24
• A peripheral neurologic issue - NOT Central • est 20/100,000 annually • Symptoms: • unilateral facial weakness: • ptosis • facial droop • slurred speech
• Exact cause unknown • infectious causes • HSV-1 reactivation
Bell’s Palsy
!25Janjua 2011

Bell’s Palsy
!26
• Tends to occur > age 40 • but…
• So, if there’s no frontal sparing = woot! Bell’s?!
…not necessarily • Some Brain stem strokes
have isolated eye w facial weakness • Rapidity of onset • Age/Risk factors From: Janjua HS, Ayoob R, Spencer JD
Janjua 2011

Degenerative Neurologic Disorders
!27
• Myelopathy • affects spinal cord • → motor/sensory loss • causes: • inflammation • infections • trauma • vascular lesions • compressive lesions

Degenerative Neurologic Disorders
!28
• Myelopathy • affects spinal cord • → motor/sensory loss • causes: inflammation, infections,
trauma, vascular lesions, compressive lesions
• Vasculitis • rare • often CAUSES CVA
Stroke Chameleon?
!29
• A CVA that presents as a different condition… • Acute Hemiballismus?
https://www.youtube.com/watch?v=fCL7RWaC3RA • = subthalamic nucleus CVA
• Confusion, agitation, & delirium? • temporal lobe, limbic cortex
lesions • How to tell the difference? • if ACUTE in onset - work it up!
Fernandes et al 2013

Predictors Stroke vs Mimic
!30

Stroke Predictors
!31
1.Strongest predictor: lateralizing weakness • PPV 90% • NPV 43% 😡
2.Atrial Fib History 3.Hypertension 4.Focal Deficits 5.Age > 50
Ali et al 2018

!32
1.Younger, female 2.↓NIHSS • median 5, range 1-15
3.Epilepsy Hx 4.Migraine Hx 5.Paresthesias 6. Sx INCONSISTENT w vascular territory 7.NO Vascular risk factors - HTN, hyperlipidemia, etc 8.Decreased Mental status @ presentation
Mimic Predictors
Hand 2006, Chang 2012

In-hospital Risk Factors
!33
• A fib • in-patients ↑likelihood A Fib-related CVA vs
outpatient • 31% of CVA pts SUBTHERAPEUTIC on anticoag • 6.9% had anti-thrombotics d/c’d for surg
procedures • Make sure to restart ⍺-coags early
• Stroke Alerts for AMS = MIMIC >>> CVA • ~ metabolic vs infectious cause
Vera et al 2011

Imaging to help w diagnosis?
!34
• CT head • LEAST sensitive test • ~12-52%
• CTA? • can visualize vascular
obstructions • increases Sn 70%, Sp~88%
• MRI? of course • BUT Sn >80%, Sp 95% • ~1/3 non-disabling CVA had
neg DWI 4 days post event • 4-29% miss rate of CVA
Nguyen 2015, Makin 2015

What IF we tPA a Mimic?!?!?
!35
• ~1-20% mimics treated with IV tPA • Harm? • hemorrhagic conversion rate: ~1.8 - 5% • 5% study - n=2, 1 was 8d post cath w femoral bleed • most studies report none
• Typically seizure or tumor • per Lewandowski et al.
• Chernyshev, Chen recommend tPA w ANY patient suspected of Acute CVA w/in 3 hours of onset • …regardless if later we determine it was a mimic…
Lewandowski 2015, Zinkstok 2013, Tsivgoulis 2011 Chernyshev et al 2010. Chen 2011

Co💲t of Mimics
!36
• 74 pts diagnosed w Mimics 2009-2013 • Median cost per admission: $5401 • CT head, basic labs • tPA • ICU observation stay >24hrs
• Median LOS: 1 day • Direct Hospital Cost $288,277
(=meds, food, consults, tx, devices, supplies) • Indirect Hospital Cost: $257,975 (utilities, facilities, labor) • Extrapolate to USA: $15,000,000/year
Goyal et al 2015

So…how do we tell?
!37
1.TIMING!! ➡ If acute onset - consider
stroke until proven otherwise 2.Risk Factors
• some suggest mimic • some suggest CVA
3.Neuroanatomy - more likely stroke if it occurs in
particular vascular distribution - Work to understand it

There is NO
!38
• 15% stroke patients had NO LATERALIZING SYMPTOMS
• 6% Sx NOT in Vascular territory • NIHSS? • NIH>10 occurred in 19% mimics
Hand et al 2006

Now Back to Our Case…
!39
• 37 yo F pmh depression, anxiety here with 10 minutes of numbness to her R hand/arm, with inability to move hand in addition to difficulty getting her words out. Visual symptoms described as a ‘flashing zig zag’ when looking to the right. Shortly after resolution of hand numbness, a headache began. Does have hx of rare migraines.
What symptoms push away from CVA and towards a mimic?

Now Back to Our Case…
!40
37 yo F with pmh depression, anxiety here with 10 min of numbness to her R hand/arm, with inability to move hand in addition to difficulty getting her words out. Visual symptoms described as a ‘flashing zig zag’ when looking to the right. Shortly after resolution of hand numbness, a headache began. Does have hx of rare migraines.
• DDX? Complex migraine, IC hemorrhage, IC Mass, CVA • Seen by neurology in house • Negative CT head/CTA • Likely migraine → NOT tPA candidate • D/c home

Recap:
!41
Mimics are a reality we can’t escape
• Look at the entire clinical context • Risk factors ?a fib?? • age • prior dx • epilepsy/psych hx
• It does cost the system ~$5400/mimic • BUT if real CVA benefit outweighs cost
• When in doubt, tPA if you are in the window • 23 yo (Dr. Cady)


References
!43
• Ali et al. Validating the TeleStroke Mimic Score: A prediction rule for identifying stroke mimics evaluated over telestroke networks. Stroke 2018;49:688-692.
• Allder et al. Limitations of clinical diagnosis in acute stroke. The Lancet 1999;354(9189):1523.
• Bladin et al. Seizures after stroke: a prospective multi center study. Arch Neurol 2000;57:1617-22.
• Cadranel et al. Focal neurological signs in hepatic encephalopathy in cirrhotic patients: an underestimated entity? Am J Gastroenterol 2001;96(2):515-8.
• Dawson et al. Stroke mimic diagnoses presenting to a hyperacute stroke unit. Clin Med 2016; 16:423-426.
• Loomis & Mullen. Differentiating Facial Weakness Caused by Bell’s Palsy vs Acute Stroke. Journal of Emergency Medical Services. May 2014. https://www.jems.com/articles/print/volume-39/issue-5/features/differentiating-facial-weakness-caused-b.html. Accessed March 29, 2019.
• Janjua et al. Hypertension in a boy with Bell palsy. Consultant for Pediatricians. 2011; 10(6): 203-206.
• Chang et al. A model to prevent fibrinolysis in patients with stroke mimics. J Stroke Cerebrovasc Dis. 2012 Nov;21(8):839-43

References
!44
• Chernyshev et al. Safety of tPA in stroke mimics and neuroimaging-negative cerebral ischemia. Neurology 2010;74:1340-1345.
• Fernandes et al. Strokes: Mimics and chameleons. Pract Neurol 2013; 13:2108. • Gallmetzer et al. Postictal paresis in focal epilepsies - incidence, duration, and causes:
a video-EEG monitoring study. Neurology 2004; 62:2160-4. • Goldstein et al. Is this patient having a stroke? JAMA 2005;293(19):2391-402. • Goyal et al. Cost Burden of Stroke Mimics and Transient Ischemic Attack after
Intravenous Tissue Plasminogen Activator Treatment. J of Stroke & Cerebrovasc Dis 2015; 24: 828-833
• Hand et al. Distinguishing Between Stroke and Mimic at the Bedside. Stroke 2006;37:769-775.
• Chen et al. Intravenous thrombolytic therapy in patients with stroke mimics: baseline characteristics and safety profile. Eur. J Neurol 2011; 18(10): 1246-50
• Lewandowski et al. Safety and Outcomes in Stroke Mimics after Intravenous Tissue Plasminogen Activator Administration: A Single-center Experience. J of Stroke and Cerebrovasc Dis 2015;24: 48-52.

References
!45
• Makin et al. Clinically confirmed stroke with negative diffusion-weighted imaging magnetic resonance imaging longitudinal study of clinical outcomes, stroke recurrence and systematic review. Stroke 2015;46:3142-3148.
• Nguyen and Chang. Stroke mimics and acute stroke evaluation: clinical differentiation and complications after intravenous tissue plasminogen activator. J of Emerg Med 2015;49(2):244-252.
• Tsivgoulis et al. Safety and outcomes of intravenous thrombolysis in stroke mimics: a 6-year, single-care center study and a pooled analysis of reported series. Stroke 2011:42:1771-4
• Vera et al. In-hospital ischemic strokes in patients admitted to cardiology and cardiac surgery departments. Multi-centre registry. Medicina Clinica 2011; 137(11):479-483.
• Zinkstok et al. Safety of thrombolysis in stroke mimics: results from a multi center cohort study: stroke 2-13;44:1080-1084.