structured clinical management supporting generalist mental health practitioners to work effectively...
TRANSCRIPT

Structured Clinical Management
Supporting generalist mental health practitioners to work effectively with people with borderline personality disorder.

Presenters
Emma Hickey and Rachael Line
Clinical Psychologists
Five Boroughs Partnership NHS Foundation Trust
Email:
[email protected] - Trust PD & SCM lead

Aims
To give you a basic understanding of SCM. Share how we have applied it. Prompt you to consider how it could look in your service.

Background to Structured Clinical Management
Organised Case Management specific to borderline personality disorder

What is SCM?
Developed by Anthony Bateman, Peter Fonagy, Rory Bolton and Eric Karas at the Halliwick Unit, London.
Evidenced based. Generalist mental health. Supportive approach with case management and
advocacy support.

Structured Clinical Management
Involves helping the person to:
oProblem solveoManage a crisisoDevelop skills to manage emotions/impulses/interpersonal
interactionoUse medication and services appropriately
NOTE: primary aim of SCM is to reduce unnecessary hospital admissions

Specialist/Generalist treatments: the evidence base
Mentalization based treatment (MBT) ‘v’ structured clinical management (SCM (Bateman & Fonagy, 2009b)
Other generalist treatments, comparable to SCM also shown to be effective (McMain, Guimond, Cardish, Streiner, & Links, 2012)

Borderline Personality Disorder:An evidence-based guide for generalist mental health professionals
Anthony W. Bateman, Consultant Psychiatrist and
Psychotherapist, UK and Roy Krawitz, Consultant
Psychiatrist and DBT therapist, Waikato District Health Board,
New Zealand

Implementing SCM within Five Boroughs Partnership NHS Foundation Trust
Halton, Knowsley, Warrington, St Helens, Wigan and Leigh


An opportunity
Pre-Recovery Teams:
Personality Disorder Hub Co-delivered training (EBEs and EBOs) with focus on awareness
and attitudes. Development of specialist psychological treatments.
Recovery Teams:
Training and implementation of generic treatment (SCM pilot). Increasing range of evidence based treatments.

borderline personality disorder identified
SCM
DBT or MBT
SCM
5BP Personality Disorder Care Pathway
COMPLEXITY
Specialisttreatment
Engagement focus
Generic treatment

SCM pilot
2 day SCM training by Anthony Bateman for:
SCM supervisors/champions. Mental Health workers (3 per Recovery Team). Psychiatrists. EBE and carer consultant.

Piloting SCM within 5BP
Each SCM practitioner to see 3 people over 18 months. Inclusion and exclusion criteria. Frame of SCM – weekly 1:1 session and skills group. Weekly supervision. Measures (see appendix). POD.
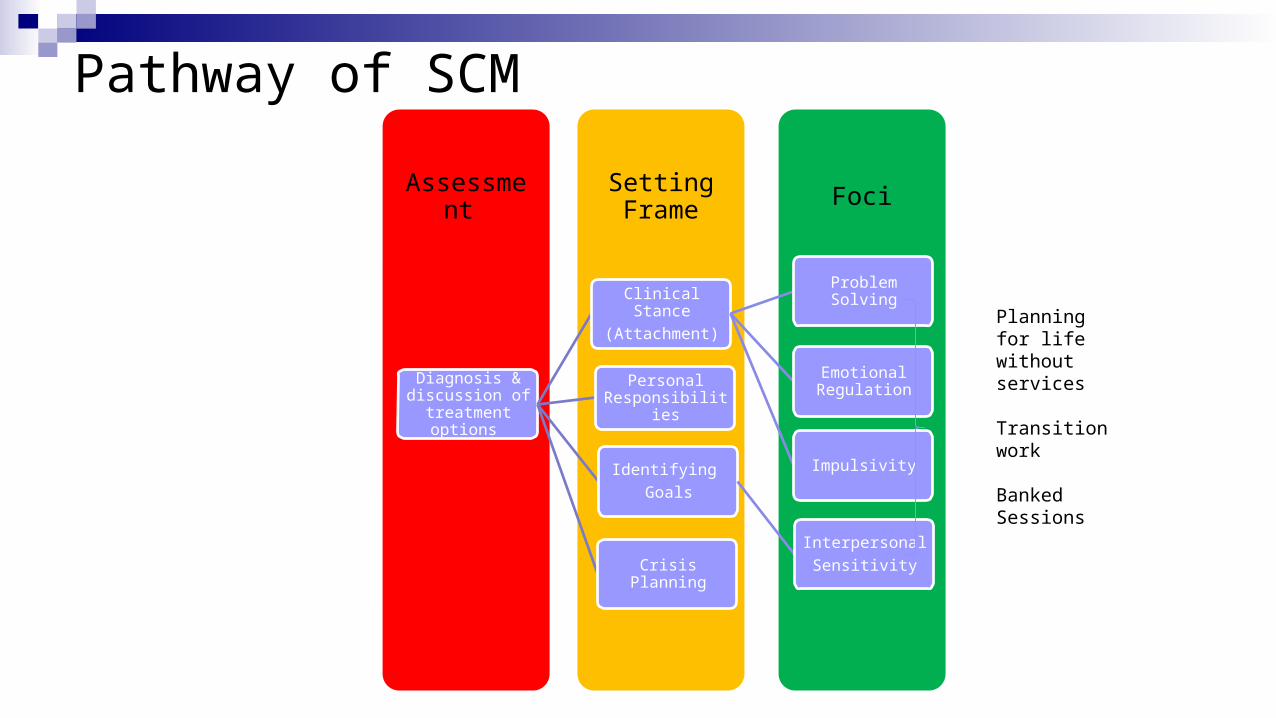
Pathway of SCM
FociSetting FrameAssessment
Diagnosis & discussion of
treatment options
Clinical Stance
(Attachment)
Problem Solving
Emotional Regulation
Impulsivity
Crisis Planning
Personal Responsibilities
Identifying
Goals
Interpersonal
Sensitivity
Planning for life without services Transition work
Banked Sessions

Assessment
Up to 6 outpatient sessions (40 minutes). Assessment and diagnosis. Explanation of treatment approach. Building therapeutic alliance.
Clinical stance within SCM
Reliable and consistent. Active, responsive and curious. Realistic expectations. Team work and communication. Hope and optimism.
Expect patients to be active in controlling their life.
Change is expected.


Setting Frame
Socialisation to SCM (up to 3 months) Weekly 1:1 sessions (40 minutes). Development of motivation and establishment of therapeutic
alliance. Focus on:
Clinical stance (attachment). Personal responsibility. Setting goals. Crisis planning.
Setting Frame
Collaborative development of:
• Clinician and patient responsibilities.• Comprehensive formulation and goals.• Hierarchy of therapeutic areas.• Crisis planning – risk assessment and management.• Stabilisation of drug misuse and alcohol abuse.• Involvement of families, relatives, partners and other

Crisis Plans
One of the most important things you can do. Key pointers to an effective crisis plan:
• Not adequate to have to attend A & E. • Collaboratively developed plan.• Use previous examples (three) that led to self destructive.
behaviour/or contact to services. • What can you, friends & family, professionals do and not do.

A quick word about admissions and medication
Admission
Define purpose. Agree aims of admission. Monitor progress. Integrate SCM. BEWARE of setting unattainable
targets.
Prescribing
Consider long term plan Try to avoid crisis prescribing Follow NICE guidance Co-occurring conditions
Foci
Weekly 1:1 (40 minutes). Weekly group sessions (90 minutes). Working on hierarchy of therapeutic areas. Problem Solving underpins.

SCM: Non-specific interventions
Non specifics remain key:
Attitude. Empathy. Validation. Positive regard. Advocacy.

SCM: Specific interventions
Problem Solving underpins core treatment strategies:
• Emotion management.• Mood regulation.• Impulse control.• Interpersonal sensitivity.• Interpersonal problems.• Suicidality and self-harm and management of risk.

Content of Group
Psycho-education and problem solving.Incorporating mentalization principles about self and others.Involves:
•Problem Solving/Mindfulness Module •Tolerance of Emotions and Mood Management Module•Impulsivity Module•Enhancing Relationship Skills Module
All sessions to include a skills component and time spent problem solving a relevant issue of the group members choice.

Where are we up to?
Individual SCM. Weekly supervision. Group work – coming soon. POD – coming soon. SCM awareness/skills training for remaining recovery team
staff, inpatient staff, home treatment staff.

Lessons learnt so far….
Competing demands for SCM practitioners. Whole system approach. Highlighting competencies. Positive attitudes towards personality disorder & recovery. Whole system approach. Validation is key!

What are service users saying about SCM?
“ I think that the Agreement is really good idea because it is between both of us and helps me to have some structure and responsibility in my life”
“Learning more about my diagnosis, symptoms and what medication is prescribed and why, helps to give me more insight into my diagnosis and how the diagnosis and symptoms effect my daily life and the risks that come was some of the symptoms”

What are service users saying about SCM?
“The crisis plans helps me to come to an agreement that between us is for my own benefit and to assist me when in Crisis but I feel it needs to have more in it to prevent any more admissions because this is a big anxious issue for me”
The Goals are good because it gives me things to aim for both in the short and long term”

What SCM practitioners are saying
Hope...but realistic Really like the structure Need flexibility so can tailor it to the individual Hadn’t realised how little they understood of their care plan Good to start SCM with someone you already know Seeing the benefits for service users But am I really doing SCM?

References Bateman A, Fonagy P. Randomized controlled trial of out-patient mentalization based
treatment versus structured clinical management for borderline personality disorder. American Journal of Psychiatry. 2009;1666:1355-64.
Bateman,A., & Fonagy,P. (2013). Impact of clinical severity on outcomes of mentalisation-based treatment for borderline personality disorder. British Journal of Psychiatry, 203, 163-164.
McMain, S., Guimond, T., Cardish, R., Streiner, D., & Links, P. (2012). Clinical outcomes and functioning post-treatment: a tow-year follow-up of dialectical behaviour therapy versus general psychiatric management for borderline personality disorder. American Journal of Psychiatry, 169, 650-661.
McMain, S., Links, P., Gnam, W., Guimond, T., Cardish, R., Korman, L., et al. (2009). A randomised controlled trial of dialectical behaviour therapy versus general psychiatric management for borderline personality disorder. American Journal of Psychiatry, 166, 1365-1374.

Measures used within 5BP for SCM
Weekly:• PHQ-9: Patient Health Questionnaire.• WEMWBS: Warwick-Edinburgh Mental Well Being Scale.• WSAS: Work and Social Adjustment Scale.• Service usage over the past week.
Start, 6 months, 12 months and end point:• SAPAS: Standardized Assessment of Personality Abbreviated Scale.• EQ-5D-5L: EuroQol (quality of life).• PTEQ: Perceived Threat from Emotions Questionnaire.
• PEQ: Patient Experience Questionnaire (not used at start).
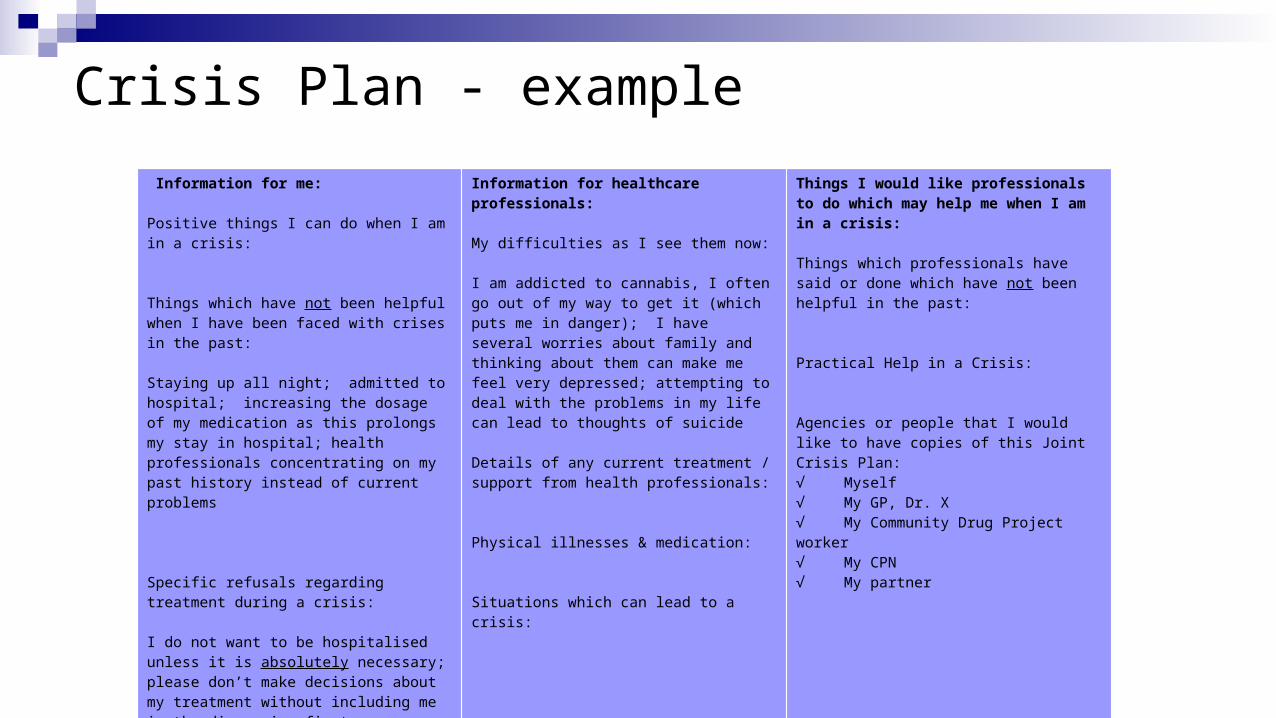
Crisis Plan - example
Information for me: Positive things I can do when I am in a crisis: Things which have not been helpful when I have been faced with crises in the past:
Staying up all night; admitted to hospital; increasing the dosage of my medication as this prolongs my stay in hospital; health professionals concentrating on my past history instead of current problems
Specific refusals regarding treatment during a crisis: I do not want to be hospitalised unless it is absolutely necessary; please don’t make decisions about my treatment without including me in the discussion first
Information for healthcare professionals: My difficulties as I see them now:
I am addicted to cannabis, I often go out of my way to get it (which puts me in danger); I have several worries about family and thinking about them can make me feel very depressed; attempting to deal with the problems in my life can lead to thoughts of suicide Details of any current treatment / support from health professionals:
Physical illnesses & medication:
Situations which can lead to a crisis:
Things I would like professionals to do which may help me when I am in a crisis: Things which professionals have said or done which have not been helpful in the past:
Practical Help in a Crisis: Agencies or people that I would like to have copies of this Joint Crisis Plan: √ Myself√ My GP, Dr. X√ My Community Drug Project worker√ My CPN√ My partner