stuart tobin, m.d. chief of the nano-divison of dermatology ullin leavell professor of dermatology...
TRANSCRIPT

Stuart Tobin, M.D.Chief of the Nano-Divison of Dermatology
Ullin Leavell Professor of DermatologyAssociate Professor of Dermatology

What is the pathogenesis of acne?
Acne development is polygenic and multifactorial.
Main pathogenetic factors contribute to the disease:
•Sebaceous gland hyperplasia and excess sebum production. •Sebaceous follicle size and number of lobules per gland are increased in patients with acne. Androgens stimulate sebaceous glands to enlarge and produce more sebum, which is most prevalent during puberty. •Abnormal follicular differentiation. In normal follicles, keratinocytes are shed as single cells into the lumen and then excreted. In acne, keratinocytes are retained and accumulate due to their increased cohesiveness.

• Propionibacterium acnes colonization. • These gram-positive, non-motile rods are found
deep in follicles and stimulate the production of pro-inflammatory mediators and lipases. While there may be increased numbers of P acnes in acne, bacterial counts often do not correlate with acne severity.
• Inflammation and immune response. Inflammatory cells and mediators flow into the disrupted follicle, leading to the development of papules, pustules, nodules and cysts.
Open Comedones Closed Comedones Papules Pustules Cysts (Inflamed and Non-inflamed)

Open Comedones

Closed Comedones

Acne Papules

Pustules

Inflamed Cyst
Non-inflamed Cyst

Skin Cleansing with a mild astringent soap Purpose Soap
Acne Mechanica Oil Free Makeup, water based and non-
comedogenic Defining Goals and distinguishing between
active disease and discoloration and scarring

Step 1 Therapy- Topicals
Antibiotics (Clindamycin, Erythromycin) Tretinoins Adapalene (3% and 5%) Azelaic acid Benzoyl peroxide (2.5% to 10%) Saliclyic acid Sulfur

Step 2 Therapy- Systemic Medications Oral Antibiotics Minocycline (50 to 100mg/bid) Doxycycline (75 to 150mg daily) Erythromycin & Azithromycin Bactrim (80/400) 160 po bid Spironolactone 50-200mg q.d. OCP (high estrogen/low progesterone ratio) Yaz Intralesional Steroid injections

Step 3 Therapy Isotretinoin ( Accutane) 1mg/kg/day 30 to40 mg bid) Adverse Reactions. Xerosis,
musculoskeletal pain, depression, IBD, Monthly monitoring of CBC, Pregnancy
Tests, LFT’s, Triglycerides, BMP

Eczema in Greek means to weep translates as vesicle/blister formation
Sub Types 1. Contact Dermatitis 2. Atopic Dermatitis 3. Nummular Dermatitis 4. Xerotic Dermatitis 5. Dyshidrotic Eczema 6. Seborrheic Dermatitis

Poison Ivy

Contact Dermatitis – Poison Ivy

1. If it’s wet, dry it. Translated- Compressing dries out lesions
Compresses: A. Saline B. Aluminum Acetate ( Dome Boro, Blu Boro) C. Milk Compresses 2. Topical Steroids 3. Systemic Steroids
P.S Stay away from Poison Ivy

Atopic Dermatitis

Atopic Dermatitis

Support Measures: 1. Decrease soap and water exposure 2. Avoid rough fabrics to the skin ( wool etc) 3. Moisturizing lotions daily to the skin 4. With infrequent bathing using a moisturizing
soap like Dove 5. Bleach Baths to reduce skin flora causing
infection ( 1/4 to 1/2 cup per full bath) 6. Diet ? 7. Antibiotic ointment to nares to reduce
bacterial exposure

1. Topical Therapies: ◦ A. Pediatric Topical Steroids ( Hydrocortisone 1-2.5%
cream, Triamcinolone 0.025% cream, Desonide 0.05% cream, Dermatop 0.1% cream)
◦ B. Topical Tacrolimus ( Elidel, Protopic ) ◦ C. Mupirocin Ointment applied to nares
2. Oral Medications: A. Hydroxyzine 10mg/5cc ( pediatric dosage)
B. Systemic Steroids- Prednisone Taper C. Systemic Antibiotics ( Cephalexin, Amoxicillin)

Nummular (coin shaped) Dermatitis

Topical Steroids ( Pediatric or Adult Strength)
Topical Tacrolimus Systemic Steroids tapered over 2 weeks Systemic Antibiotics

Xerotic Eczema or Dermatitis Craquele

1. If its dry, you want to wet it. Translates- Moisturizing the skin with lotions, emollients, Vaseline, Aquaphor, Crisco (pediatrics)
2. Decreasing soap and water exposure
3. Topical Steroid Ointments NOT Creams which have a tendency to dry the skin
4. Prescription Moisturizer ( 12% Lactic Acid Lotions)

Dyshidrotic Eczema ( Hand or Foot Eczema)
Weeping Stage
Dry Stage

WET WEEPING STAGE 1. Dry it with soaks/compresses 2. Topical Steroid Creams 3. Topical Tacrolimus 4. Systemic Steroids
DRY CRACKING STAGE 1. Lubricate and Emollient with moisturizing
lotions and ointments 2. Topical Steroid Ointments 3. Topical Tacrolimus Ointments- Protopic

Seborrheic Dermatitis

1. Mild, low potency Topical Steroids- Hydrocortisone 1-2.5%, Desonide 0.05% etc.
2. Topical Ketoconazole
3. Shampoos for hair bearing areas (scalp and beard) – Ketoconazole Shampoo, Tar Shampoos, Selenium Sulfide Shampoos, Zinc Pyrithione Shampoo
4. Topical Steroids Solutions and Sprays for hair bearing areas

Psoriasis

1. Scale Removers – 3% Salicyclic Acid in Mineral Oil, T-Sal Shampoo
2. Tar Shampoos- T-gel Shampoo, Zetar Shampoo
3. Cortisone Shampoos- Clobex Shampoo 4. Topical Steroids 5. Topical Tars 6. Vitamin D Derivatives (Dovonex &
Vectical) 7. Ultraviolet Light ( Natural or Artificial)

8. Anthralin Ointments 9. Intralesional Injections – Kenalog
10mg/ml diluted. This is NOT intramuscular injections which should be avoided in Psoriasis
10. Hydroxyzine 25-50mg P.O.

1. PUVA Therapy 2. Narrow Band Ultraviolet Light ( Light Box
Therapy)

1. Chemotherapy Agents- Methotrexate 15-25 mg weekly ( most cost effective, and most insurance companies require a trial of MTX)
2. TNF ( Tumor Necrosis Factor) inhibitors First Choice- Adalimumab (Humira)
Entanercept ( Enbrel)
3. IL inhibitors – Stelara

Tinea Coporis
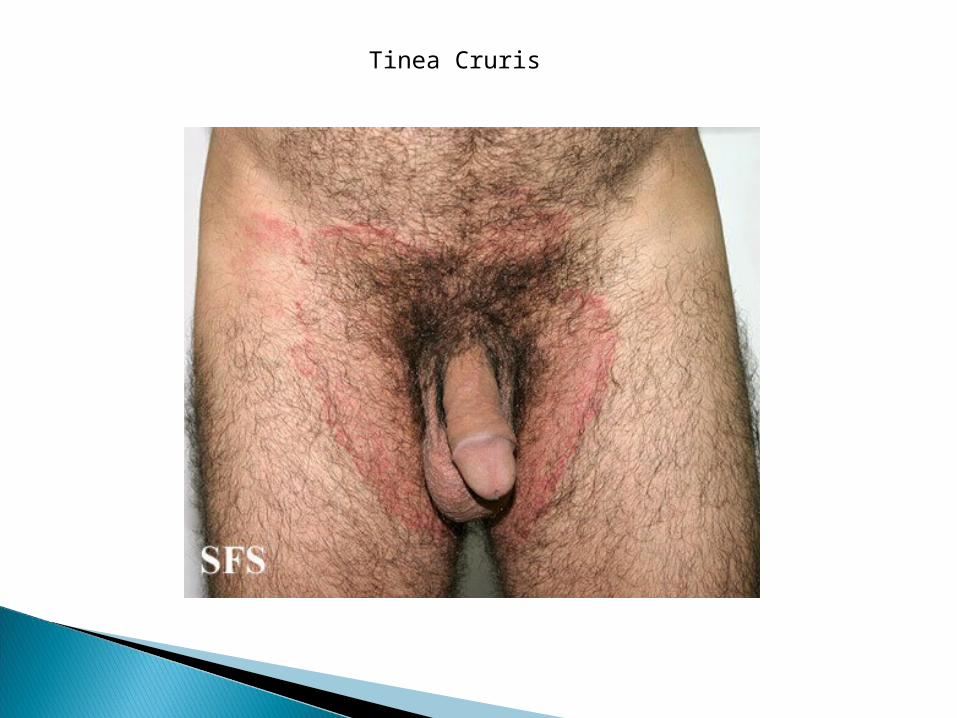
Tinea Cruris

Tinea Pedis

OPnychomycoses

Tinea Capitis

KOH Prep

Fungus Culture
Topical Antifungals: Ketoconazole, clortrimazole BID for 4 weeks
Systemic Antifungals: 1. Terbenifine (Lamisil) 250mg 2. Griseseofulvin for tinea capitis 3. Diflucan not as affective for trichophyton
infections.

Remember this lecture is all I ask and yet If Memory proves too great a task
Forget
Paraphrase Quote from Percy French