“stud y on delirium- etiol ogy, clinical profil e and …
TRANSCRIPT

“STUD
TH
M
TH
DY ON
PR
Su
HE TAMI
GOVER
MD (PSY
HE TAMI
A
DELIR
ROFILE
ubmitted fo
ILNADU D
CHE
RNMENT K
C
CHIATR
B
ILNADU D
CHEN
A Disserta
RIUM-
E AND
or M.D. D
Dr. M.G.R
NNAI, TA
KILPAUK
CHENNAI
RIC MEDI
BRANCH
Dr. M.G.R
NNAI, TA
May 202
ation on
ETIOL
OUTC
Degree exam
R. MEDICA
AMILNAD
K MEDICA
I-600010
ICINE) E
– XVIII
R. MEDICA
AMILNAD
20
LOGY,
COME”
minations
AL UNIV
DU
AL COLL
EXAMINA
AL UNIV
DU.
CLINIC
”
VERSITY,
LEGE,
ATION
VERSITY,
CAL

BONAFIDE CERTIFICATE
This to certify that the Dissertation entitled “STUDY ON
DELIRIUM- ETIOLOGY, CLINICAL PROFILE AND
OUTCOME” is a bonafide record of work done by
Dr.C.J.DHIINESH in the department of Psychiatry, Government
Kilpauk Medical College, Chennai, during his Post Graduate Course from
2017 to 2020. This is submitted as partial fulfilment for the requirement
of M.D. Degree examinations – Branch – XVIII (Psychiatry) to be held
in May 2020.
Prof. Dr. P. Vasanthamani, Prof. Dr. M. Malaiappan, MD,
MD, DGO, MNAMS, MBA., Professor and Head,
The Dean, Department of Psychiatry,
Govt. Kilpauk Medical College, Govt. Kilpauk Medical College,
Chennai. Chennai

CERTIFICATE
This is to certify that “STUDY ON DELIRIUM- ETIOLOGY,
CLINICAL PROFILE AND OUTCOME” is a bonafide work of
Dr.C.J.DHIINESH in partial fulfilment of the requirements for the M.D
Psychiatric Medicine examination (Branch-XVIII ) of the Tamilnadu
Dr. M.G.R Medical University, Chennai, to be held in May, 2020.
GUIDE & HEAD OF THE DEPARTMENT Dr. MALAIAPPAN MD,
Professor& HOD
Department of Psychiatric Medicine,
Kilpauk Medical College,
Chennai.
DECLARATION
I, Dr. C.J.DHIINESH, solemnly declare that the dissertation titled
“STUDY ON DELIRIUM- ETIOLOGY, CLINICAL PROFILE
AND OUTCOME” is a bonafide work done by me in Government
Kilpauk Medical College, Chennai, during March 2018 – September -
2019 under the guidance and supervision of
Prof. Dr M. MALAIAPPAN, MD (Psychiatry).
This dissertation is submitted to “The Tamilnadu Dr M.G.R.
Medical University, Chennai”, Tamilnadu as a partial fulfillment for the
requirement of M.D. Degree examinations – Branch – XVIII (Psychiatry)
to be held in May 2020.
Place: Chennai
Date: (Dr. C.J.DHIINESH)
Urkund Analysis Result Analysed Document: Study on Delirium- etiology, clinical profile and outcome 2.docx
(D58076191)Submitted: 11/1/2019 4:35:00 PM Submitted By: [email protected] Significance: 23 %
Sources included in the report:
7fe579f8-58b6-4862-ae17-926437b89d25 80cdabda-2bf3-47e4-be64-fd8842f80282 6b4acd7b-cac8-4271-ae54-69b23eb38977 92c2b4eb-bae4-4d5b-9b16-7be0bbed9559 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5028550/
Instances where selected sources appear:
32
U R K N DU

CERTIFICATE – II
This is to certify that this dissertation work titled “STUDY ON
DELIRIUM- ETIOLOGY, CLINICAL PROFILE AND
OUTCOME” of the candidate Dr. C.J.DHIINESH with Registration
Number: 201728351 for the award of M.D in the branch of
PSYCHIATRIC MEDICINE. I personally verified the urkund.com
website for the purpose of plagiarism check. I found that the uploaded
thesis file contains from introduction to conclusion pages and result
shows 23% percentage of plagiarism in the dissertation.
GUIDE & SUPERVISOR SIGN
WITH SEAL
Place: Chennai
Date:
ACKNOWLEDGEMENTS
I am very grateful to My Guide Dr. M. MALAIAPPAN, without
whose patience and constant motivation, this work would not be possible.
My Professor Dr JAYAKRISHNAVENI, for her invaluable help in
completing this thesis.
My Assistant Professors Dr. Sharon Joe Daniel, Dr. Bakyaraj and
Dr. Vamsi Sreenivas for their valuable opinion and constructive
suggestions during the planning and analysis of this research work.
My Assistant Professor Dr.A.P. Mythili for her guidance and
suggestions.
All the patients and their family members who co-operated for the
study.
All my colleagues and my family for their support and
encouragement.

TABLE OF CONTENTS
S.NO TOPIC PAGE NO
1 INTRODUCTION 1
2 AIMS AND OBJECTIVES 2
3 REVIEW OF LITERATURE 3
4 METHODOLOGY 34
5 STATISTICAL ANALYSIS 41
6 RESULTS 43
7 DISCUSSION 74
8 CONCLUSION 80
9 LIMITATIONS 82
10 BIBLIOGRAPHY
11 ANNEXURE
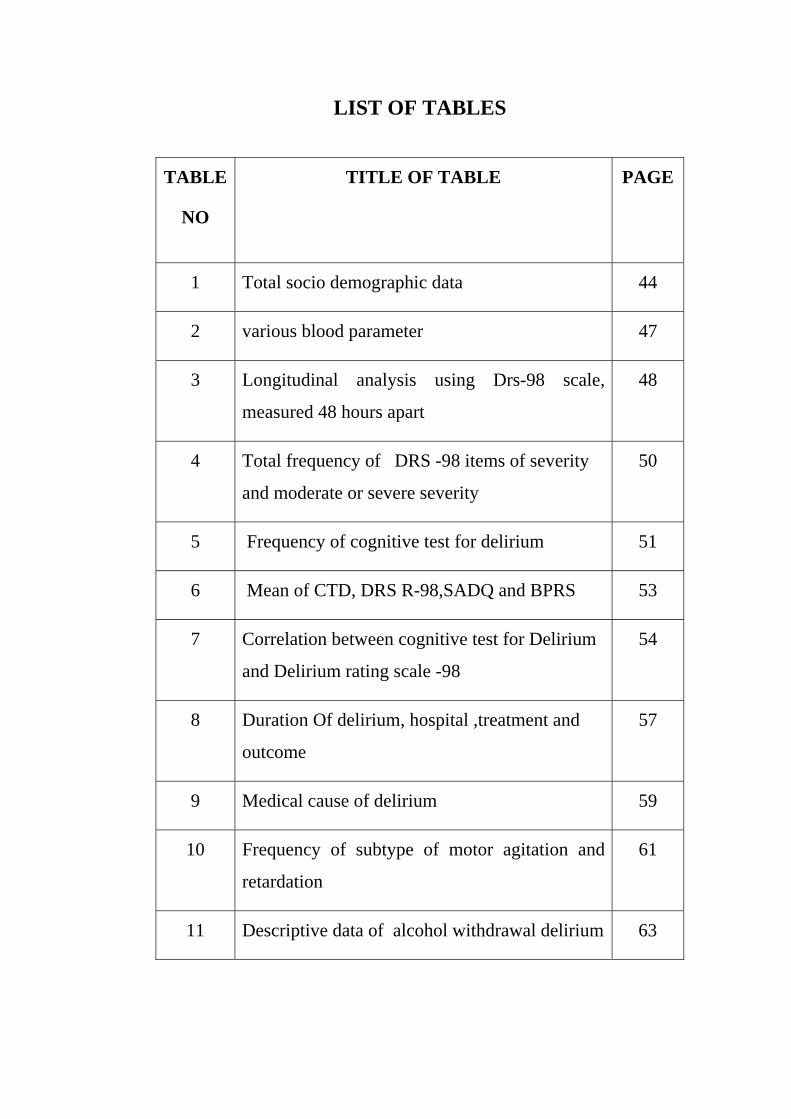
LIST OF TABLES
TABLE
NO
TITLE OF TABLE PAGE
1 Total socio demographic data 44
2 various blood parameter 47
3 Longitudinal analysis using Drs-98 scale,
measured 48 hours apart
48
4 Total frequency of DRS -98 items of severity
and moderate or severe severity
50
5 Frequency of cognitive test for delirium 51
6 Mean of CTD, DRS R-98,SADQ and BPRS 53
7 Correlation between cognitive test for Delirium
and Delirium rating scale -98
54
8 Duration Of delirium, hospital ,treatment and
outcome
57
9 Medical cause of delirium 59
10 Frequency of subtype of motor agitation and
retardation
61
11 Descriptive data of alcohol withdrawal delirium 63

12 Compare the medical and alcohol withdrawal
delirium, Age and Delirium Cause.
64
13 Comparison of demographic details between
alcohol withdrawal and medical illness delirium
66
14 Comparison of frequency of symptom profile
and severity between groups
68
15 Duration of delirium comparison between both
groups
70
16 Independent Samples Test between Delirium
Cause and Total duration of delirium
71
17 Treatment and outcome of delirium between
two groups
72
18 Independent Samples Test between Delirium
Cause and Total duration of Hospital
73

LIST OF FIGURES
Figure
No
TITLE OF FIGURE Page No
1 Frequency of subject obtained 43
2 Frequency of socio demographic score 46
3 SURFACE Diagram frequency of DRS -98 49
4 Bar chart showing frequency of cognitive test for
delirium
52
5 Pie chart showing outcome of the delirium 58
6 Bar chart showing distribution Medical cause of
delirium
60
7 Bar chart Compare the Age of medical and alcohol
withdrawal delirium
65
8 Surface diagram depicting mean difference between
alcohol withdrawal Delirium and other cause of
medical delirium
67

1
“STUDY ON DELIRIUM- ETIOLOGY, CLINICAL
PROFILE AND OUTCOME”
INTRODUCTION
Delirium is an acute confusional state. The onset is rapid and has
fluctuating course. It presents with alterations in consciousness and
disturbance in sleep wake cycle, thinking and memory, disordered
attention, hallucinations and delusions, and physical agitation or hypo
activity. The cause of it may be neurological or psychological and the
presentation also varies between them according to Daniel et al., This
study was conducted over period of one year for detailed evaluation
delirium related phenomenology and its outcome .The aim of the study is
to strengthen our knowledge of this highly prevalent yet poorly studied
condition by assessing the phenomenology (psychological and physical
event) both cross -sectionally and longitudinally during course of an
episode
2
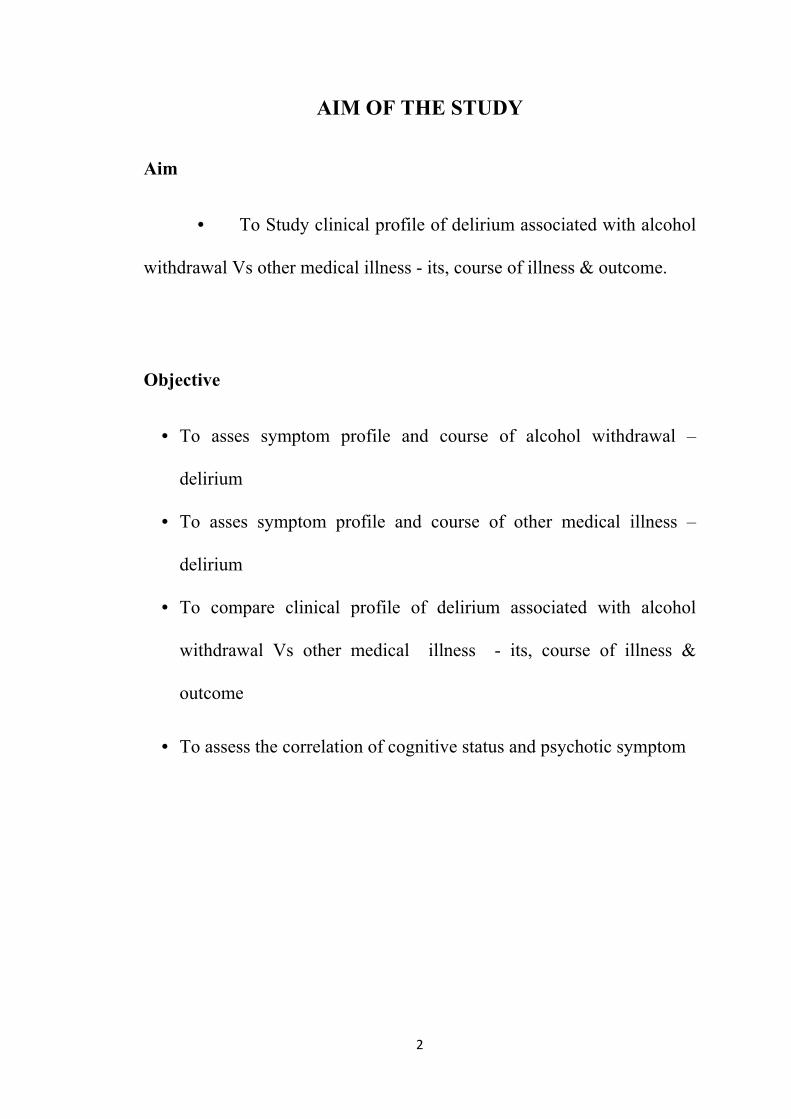
AIM OF THE STUDY
Aim
• To Study clinical profile of delirium associated with alcohol
withdrawal Vs other medical illness - its, course of illness & outcome.
Objective
• To asses symptom profile and course of alcohol withdrawal –
delirium
• To asses symptom profile and course of other medical illness –
delirium
• To compare clinical profile of delirium associated with alcohol
withdrawal Vs other medical illness - its, course of illness &
outcome
• To assess the correlation of cognitive status and psychotic symptom
3
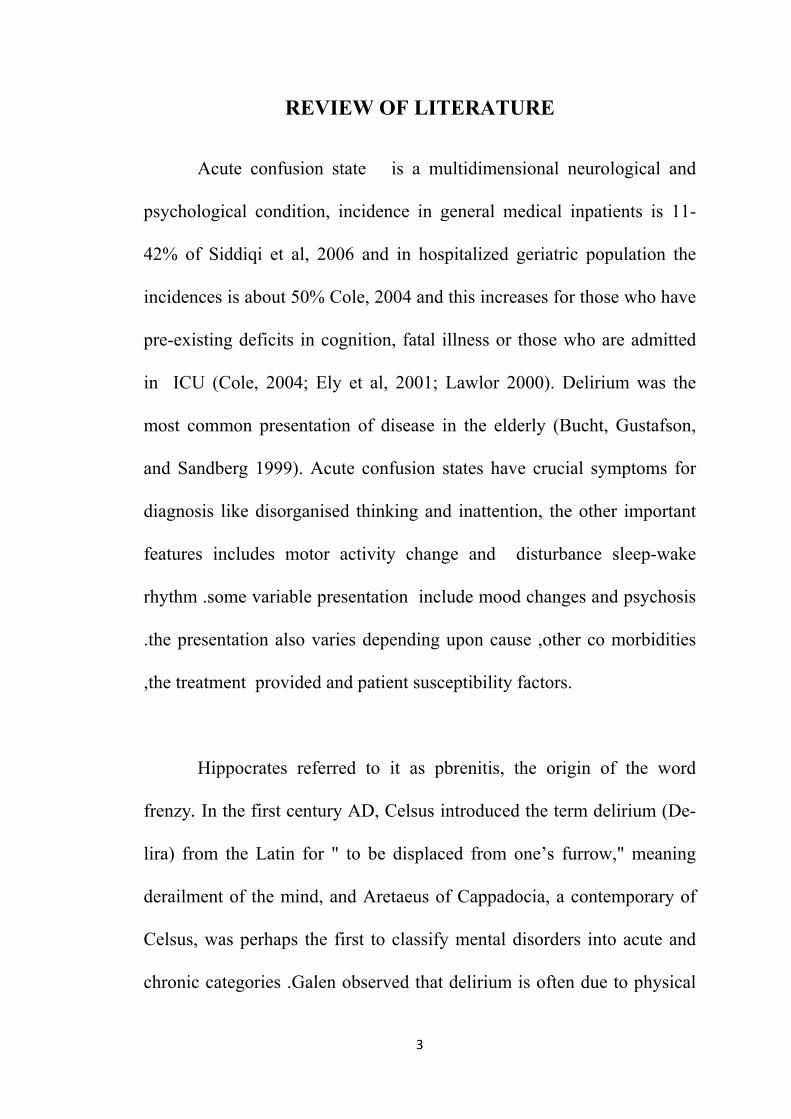
REVIEW OF LITERATURE
Acute confusion state is a multidimensional neurological and
psychological condition, incidence in general medical inpatients is 11-
42% of Siddiqi et al, 2006 and in hospitalized geriatric population the
incidences is about 50% Cole, 2004 and this increases for those who have
pre-existing deficits in cognition, fatal illness or those who are admitted
in ICU (Cole, 2004; Ely et al, 2001; Lawlor 2000). Delirium was the
most common presentation of disease in the elderly (Bucht, Gustafson,
and Sandberg 1999). Acute confusion states have crucial symptoms for
diagnosis like disorganised thinking and inattention, the other important
features includes motor activity change and disturbance sleep-wake
rhythm .some variable presentation include mood changes and psychosis
.the presentation also varies depending upon cause ,other co morbidities
,the treatment provided and patient susceptibility factors.
Hippocrates referred to it as pbrenitis, the origin of the word
frenzy. In the first century AD, Celsus introduced the term delirium (De-
lira) from the Latin for " to be displaced from one’s furrow," meaning
derailment of the mind, and Aretaeus of Cappadocia, a contemporary of
Celsus, was perhaps the first to classify mental disorders into acute and
chronic categories .Galen observed that delirium is often due to physical

4
diseases that affects the mind "sympathetically." In the nineteenth
century, Gower’s found that these patients could he either lethargic (hypo
active) or hyperactive. Barrough proposed that delirium constituted a
impairment of three main internal senses: including memory, cognition
and imagination. Thomas Willis in his book 1672 treatise De Anima
Brutorum stated delirium is a specific set of symptoms and not a disease.
John Hunter defined delirium as “a cessation of consciousness” of one’s
own existence. Bonheoffer, in his classification of organic behavioral
disorders, established that delirium is associated with clouding of
consciousness. Finally, Kngel and Romano described alpha slowing and
delta and theta intrusions on electroencephalograms (LLCs) and
correlated these change with clinical severity. They also noted that
treating the medical cause resulted in reversal of both the clinical feature
and the EEG changes of delirium.
Glossary of term
Many terms used to describe this disorder:
Acute brain failure,
Acute brain syndrome,
Acute cerebral insufficiency,
Acute confusional state,
Acute organic syndrome,
5
Delirium,
Encephalitis,
Encephalopathy,
Intensive care unit psychosis,
Toxic metabolic state,
Central nervous system toxicity,
Para neoplastic limbic encephalitis,
Sun downing,
Cerebral insufficiency,
Organic brain syndrome,
Exogenous psychosis,
Metabolic encephalopathy,
Organic psychosis,
Toxic encephalopathy,
Toxic psychosis,
Major Problems in recognizing delirium is defining the disorder.
Delirium mostly reflects a global failure of brain metabolism from a large
variety of medical etiologies, yet it is difficult to judge the impact of
medical conditions on the brain.
6
Delirium may lead to
Delay in postoperative mobilization,
Prevention of early rehabilitation,
Increased rate of nursing home placement,
Increased need for home care services,
Increased distress to caregivers
Risk Factors for Delirium
Risk factors for delirium is categoried into two , predisposing and
precipitating factors
Predisposing
Demographics
Age more than 65,
Male sex.
Pervious Cognitive status
Dementia,
Cognitive impairment,
History of delirium.
7
Functional status
Functional dependence,
Immobility,
History of falls,
Low level of activity.
Sensory impairment
Hearing,
Vision.
Decreased oral intake
Dehydration,
Malnutrition.
Drugs
Treatment with psychotropic drugs,
Treatment with drugs with anticholinergic properties,
Alcohol abuse.
Coexisting medical conditions
Severe medical diseases,
Chronic renal or hepatic disease,
8
Stroke,
Neurological disease,
Metabolic abnormalities,
Infection with HIV,
Fractures or trauma.
Precipitating Factors for Delirium
Drug induced as like with
Sedative hypnotics,
Narcotics,
Anticholinergic drugs,
Polypharmacy,
Alcohol or drug withdrawal.
Primary neurologic diseases like
Stroke,
Nondominant hemispheric Intracranial bleeding,
Meningitis or Encephalitis.
Intercurrent illnesses like
Infections,
Iatrogenic complications,
Severe acute illness,
Hypoxia,
9
Hyponatremia,
Shock,
Anemia,
Fever or hypothermia,
Dehydration,
Poor nutritional status,
Low serum albumin levels,
Metabolic derangements.
Surgical procedures like
Orthopedic surgery,
Cardiac surgery,
Prolonged cardiopulmonary bypass,
Non cardiac surgery.
Environmental factors like
Admission to intensive care unit,
Use of physical restraints,
Use of bladder catheter,
Use of multiple procedures,
Pain,
Emotional stress,
Prolonged sleep deprivation.

10
Protective Factors
Good pre morbid functioning before delirium predicts better
outcomes. Educational programs that target clinicians, consultants,
clinical staffs and primary care providers giving training and creating
awareness regarding the disorder among them demonstrated benefit.
Placement of liaison psychiatrists on others specialty orthopedic units
improved coordination of care. Other interventions such as a focus on
nutrition, increased rehabilitation, and attention to visual and hearing
impairment
PATHOPHYSIOLOGY
Their exist heterogeneity in etiologies and the presentations of
delirium. There may not be one mechanism that encompasses the entire
syndrome. Disturbance in brain oxygen supply versus demand has been
one of the theories proposed for delirium. Impaired oxidative metabolism
appears to be a predisposing factor for later development of delirium.
EEG studies have demonstrated diffuse slowing of cortical background
activity, which does not correlate with underlying causes.
11
Neuropsychologic and Neuroimaging studies revealed, in the non
dominant brain generalized disruption in higher cortical function, with
dysfunction in the prefrontal cortex, subcortical structures, thalamus,
basal ganglia, frontal and temporoparietal cortex, fusiform cortex and
lingual gyri
There was two hypotheses to understanding into the complex
pathophysiology of delirium.
1. Neurochemical imbalances
2. Inflammation
Acetylcholine
Cholinergic deficiency is found to be associated with delirium as it
is involved in rapid eye movement (REM) sleep, attention, arousal, and
memory. Administration of anticholinergic drugs can induce delirium in
humans and animals, and serum anticholinergic activity is increased in
patients with delirium. Physostigmine a cholinergic agent reverses
delirium associated with anticholinergic drugs and also in delirium from
alcohol withdrawal, ketamine in anesthesia, H2 receptor antagonist
delirium, and γ -hydroxybutyric acid withdrawal.

12
Dopamine
Dopaminergic drugs and bupropion are recognized precipitants of
delirium, and dopamine antagonists (e.g., antipsychotic agents)
effectively treat delirium symptoms. Dopaminergic excess also appears to
contribute to delirium, possibly owing to its regulatory influence on the
release of acetylcholine
Glutamate.
Wernicke encephalopathy presenting with delirium showed
glutamate abnormalities. Excitatory neurotoxic effects(mediated via the
N-methyl-D-aspartate [NMDA] receptor), may cause neuronal death and
can be associated with delirium
γ-Aminobutyric Acid
Delirium secondary to benzodiazepine and alcohol withdrawal
associated with abnormalities in GABA
Hepatic encephalopathy is caused by many factors and associated
with increased GABA and serum ammonia levels.
Ammonia and metabolites are known to induce and aggravate
astrocyte swelling that initiate a cascade of events leading to delirium. In
elevated ammonia levels can contribute to increased glutamate and
glutamine levels, which are precursors to GABA.
13
Inflammation
CNS response to systemic inflammation during a state of blood–
brain barrier compromise
Cytokines
Interleukin-1 (IL-1), IL-2, IL-6, tumor necrosis factor-α (TNF-α),
and interferon which alter the permeability of the blood–brain barrier and
neurotransmission after trauma, primary hyperparathyroidism, delirium
tremens and post cardiac surgery
Chronic Stress.
Chronic stress activates the sympathetic nervous system and
hypothalamic–pituitary– adrenocortical axis which results in increased
cytokine levels and chronic hypercortisolism. Chronic hypercortisolism
has deleterious effects on hippocampal serotonin 5-HT1A receptors.
ETIOLOGIES
Major causes of delirium
Metabolic Hepatic encephalopathy, uremia, hypoglycemia,
disorders hypoxia, hyponatremia, hypocalcemia/ hypercalcemia,
Hypomagnesemia/ hypermagnesemia, other electrolyte disturbances,
acidosis, hyperosmolar coma, endocrinopathies (thyroid, parathyroid,

14
pituitary), porphyria, vitamin deficiencies (thiamine, vitamin
R|2,nicotinic acid, folic acid), toxic and industrial exposures (carbon
monoxide, organic solvent, lead, manganese, mercury, carbon disulfide,
heavy metals)
Drug related Withdrawal syndromes (alcohol, benzodiazepines,
barbiturates, other), amphetamines, cocaine, coffee, phencyclidine,
hallucinogens, inhalants, meperidine and other narcotics,
antiparkinsonism drugs, sedative hypnotics, corticosteroids,
anticholinergic andantihistaminic drugs, cardiovascular agents
(betablockers, clonidinc, digoxin), psychotropics (phenothiazines,
clozapine, lithium, tricyclicantidepressants, trazodone), 5-fluorouracil
andcytotoxic antineoplastics, anticonvulsants(phenobarbital, phenytoin,
valproate), cimetidine, disulfirarn, ergot alkaloids, salicylates,
methyldopa, and selected antiinfectiousagents (acyclovir, amphotericin
B,cephalexin, chloroquine, isoniazid, rifampin)
Infections Meningitis, encephalitis, brain abscess, neurosyphilis,
Lyme neuroborreliosis, cerebritis, systemic infections with septicemia.
Neurological Strokes, epilepsy, head injury, hypertensive
encephalopathy, brain tumors, migraine, otherneurovascular disorders.
15
Perioperative Specific surgeries (cardiac, orthopedic,
ophthalmologics!), anesthetic and drug effects, hypoxia and anemia,
hyperventilation, fluid and electrolyte disturbances, hypotension,
embolism,infection or sepsis, pain, fragmented sleep, sensory deprivation
or overload.
Miscellaneous Cerebral vasculitidcs, paraneoplastic and
limbicencephalitis, hyperviscosity syndromes, trauma,cardiovascular,
dehydration, sensory deprivation
DIAGNOSIS
Approaches to Diagnosis
The underlying cause of delirium might present as occult or
atypical presentations of many diseases in the elderly, including
myocardial infarction, infection, and respiratory failure as delirium is
often the sole manifestation of serious underlying disease. Initial step
preadmission and current medications should be reviewed for indication
and risk: benefit such as long-standing medications can contribute to
delirium and should be reevaluated. Detail medical history and substance
abuse (occult alcohol or benzodiazepine use), which can contribute to
delirium be elevated.

16
ICD-10
F05 Delirium, not induced by alcohol and other psychoactive
substances
An etiologically nonspecific syndrome characterized by concurrent
disturbances of consciousness and attention, perception, thinking,
memory, psychomotor behaviour, emotion, and the sleep-wake cycle. It
may occur at any age but is most common after the age of 60 years. The
delirious state is transient and of fluctuating intensity; most cases
recover within 4 weeks or less. However, delirium lasting, with
fluctuations, for up to 6 months is not uncommon. Especially when
arising in the course of chronic liver disease, carcinoma, or sub acute
bacterial endocarditis. The distinction that is sometimes made between
acute and sub acute delirium is of little clinical relevance; the condition
should be seen as a unitary syndrome of variable duration and severity
ranging from mild to very severe. A delirious state may be superimposed
on, or progress into, dementia. This category should not be used for states
of delirium associated with the use of psychoactive drugs specified in
F10-F19. Delirious states due to prescribed medication (such as acute
confusional states in elderly patients due to antidepressants) should be
coded here. In such cases, the medication concerned should also be
recorded by means of an additional T code from ICD-10.
17
Diagnostic guidelines For a definite diagnosis, symptoms, mild or
severe, should be present in each one of the following areas:
(a) Impairment of consciousness and attention (on a continuum from
clouding to coma; reduced ability to direct, focus, sustain, and shift
attention);
(b) Global disturbance of cognition (perceptual distortions, illusions and
hallucinations
- most often visual; impairment of abstract thinking and comprehension,
with or without transient delusions, but typically with some degree of
incoherence;
impairment of immediate recall and of recent memory but with
relatively intact remote memory; disorientation for time as well as, in
more severe cases, for place and person);
(c) Psychomotor disturbances (hypo- or hyperactivity and unpredictable
shifts from one to the other; increased reaction time; increased or
decreased flow of speech; enhanced startle reaction);

18
(d) Disturbance of the sleep-wake cycle (insomnia or, in severe cases,
total sleep loss or reversal of the sleep-wake cycle; daytime drowsiness;
(e)emotional disturbances, e.g. depression, anxiety or fear, irritability,
euphoria, apathy,or wondering perplexity.
The onset is usually rapid, the course diurnally fluctuating, and the
total duration of the condition less than 6 months. The above clinical
picture is so characteristic that a fairly confident diagnosis of delirium
can be made even if the underlying cause is not clearly established. In
addition to a history of an underlying physical or brain disease,
evidence of cerebral dysfunction (e.g. an abnormal
electroencephalogram, usually but not invariably showing a slowing of
the background activity) may be required if the diagnosis is in doubt.
Includes: acute brain syndrome
acute confusional state (nonalcoholic)
acute infective psychosis
acute organic reaction
acute psycho-organic syndrome
19
Differential diagnosis. Delirium should be distinguished from other
organic syndromes, especially dementia (F00-F03), from acute and
transient psychotic disorders (F23.-), and from acute states in
schizophrenia (F20.-) or mood [affective] disorders (F30-F39) in which
confusional features may be present. Delirium, induced by alcohol and
other psychoactive substances, should be coded in the appropriate
section (F1x. 4).
F05.0 Delirium, not superimposed on dementia, so described
This code should be used for delirium that is not superimposed upon
pre-existing dementia.
F05.1 Delirium, superimposed on dementia
This code should be used for conditions meeting the above criteria but
developing in the course of a dementia (F00-F03).
F05.8 Other delirium
Includes: delirium of mixed origin sub acute confusional state or delirium
20
F05.9 Delirium, unspecified
1x.4 Withdrawal state with delirium
A condition in which the withdrawal state (see F1x.3) is
complicated by delirium
Alcohol-induced delirium tremens should be coded here.
Delirium tremens is ashort- lived, but occasionally life-threatening, toxic-
confusional state with accompanying somatic disturbances. It is usually a
consequence of absolute or relative withdrawal of alcohol in severely
dependent users with a long history of use. Onset usually occurs after
withdrawal of alcohol. In some cases the disorder appears during an
episode of heavy drinking, in which case it should be coded here.
Prodromal symptoms typically include insomnia, tremulousness, and fear.
Onset may also be preceded by withdrawal convulsions. The classical
triad of symptoms includes clouding of consciousness and confusion,
vivid hallucinations and illusions affecting any sensory modality, and
marked tremor. Delusions, agitation, insomnia or sleep-cycle reversal,
and autonomic over activity are usually also present.
21
Excludes: delirium, not induced by drugs and alcohol (F05.-)
The diagnosis of withdrawal state with delirium F1x.40 Without
convulsions F1x.41 With convulsions
CLINICAL FEATURES
Attention
Attention is the ability to focus on specific stimuli to the exclusion
of others. the aspect of consciousness that relates to the amount of effort
exerted in focusing on certain aspects of an experience, activity, or task.
Arousal, a basic prerequisite for attention, indicates
responsiveness or excitability into action.
Coma, stupor, wakefulness, and alertness arc states of arousal
Awareness and alertness are maintained by the ascending reticular
activating system in the brainstem which projects to the thalamus and
cortex; a bilateral frontal and parietal cortical network enables selective
attention to particular events and types of stimuli, and divided attention to
multiple events and stimuli. This cortical control system modulates
activity in sensory cortices as well as the motor areas involved in
response preparation. The distributed brain networks that regulate
22
attention are vulnerable to many different disease processes. Deficits of
attention are a cardinal feature of delirium Acute Onset with Fluctuating
Course
Delirium onset rapidly over hours or days but rarely over more
than a week and fluctuations in the course occur throughout the day.
There are lucid intervals interspersed with the daily fluctuations. Gross
swings in attention, arousal, or both occur unpredictably and irregularly
and become worse at night.
Attention is the most common and cardinal symptom of delirium.
Clinical feature of are distractible, and stimuli may gain attention
indiscriminately, trivial ones often getting more attention than important
ones. All components of attention ate disturbed, including selectivity,
sustainability, processing capacity, case of mobilization, monitoring of
the environment, and the ability to shift attention when necessary.
Disorganized Thinking
In delirium stream of thought is disturbed, there are multiple
intrusions of competing thoughts and sensations, and patients are unable

23
to order symbols, carry out sequenced activity, and organize goal-directed
behavior .Confusion defined as inability to maintain the stream of thought
with accustomed clarity, coherence, and speed. Decreased relevance of
the speech content and decreased reading comprehension is characteristic
of delirium. Confused speech is further characterized by an abnormal
rate, frequent dysarthria, and nonaphasic misnaming, particularly of
words related to stress or illness, such as those referable to
hospitalization. Speech reflects this jumbled thinking. Speech shifts from
subject to subject and is rambling, tangential, and circumstantial, with
hesitations, repetitions, and perseverations.
Altered Level of Consciousness
Consciousness or clarity of awareness Most patients have lethargy
and decreased arousal. In hyper alert patients, the extreme arousal does
not preclude in attention deficits because patients are indiscriminate in
their alertness, are easily distracted by irrelevant stimuli, and cannot
sustain attention. The two extremes of consciousness may overlap or
alternate in the same patient or may occur from the same causative factor

24
Delirium in Patients with Dementia
Dementia is the leading risk factor for delirium, and fully two-
thirds of cases of delirium occur in patients with dementia. Underlying
vulnerability of the brain in patients with dementia may predispose them
to the development of delirium as a result of insults related to acute
medical illnesses, medications, or environmental perturbations. Delirium
and dementia are both associated with decreased cerebral metabolism,
cholinergic deficiency, and inflammation, reflecting their overlapping
clinical, metabolic, and cellular mechanisms. The prevalence of delirium
increased according to the severity of the patient’s prior cognitive
impairment. Except for disorganized thinking, all symptoms of delirium
were similar among patients with mild, moderate, and severe prior
cognitive impairment. training nurses to recognize subtle changes in
mental status among those patients who were older with prior cognitive
impairment may prevent the under detection of delirium.
Jackson et al treating the underlying reversible cause of delirium
brings the patient’s functional and cognitive status back to premorbid
levels.

25
First, epidemiologic studies have documented long-term cognitive
decline in patients with delirium, after controlling for relevant covariates.
Second, several causes of delirium may not be completely reversible,
particularly those resulting in neuronal injury and permanent cognitive
sequelae, such as prolonged hypoxia or hypoglycemia. Third,
Neuroimaging studies demonstrate regions of hypo perfusion in patients
with delirium. Thus, delirium may herald the onset of dementia in many
instances. Fourth, dementia with Lewy bodies, which includes fluctuating
cognition and visual hallucinations as core signs, illustrates the overlap of
delirium and dementia.( Voyer P, Cole MG, McCusker J, Belzile E.et
al. 2006;15(1):
Delirium can worsen the course of an underlying dementia, with
dramatic decline cognitive, result in more rapid progression of functional
losses and worse long-term outcomes.
Delirium might serve as an important model for research by
offering unique approach to advance the general understanding of
cognitive disorders and dementias.

26
Studying of delirium provides an important opportunity to clarify
the link between brain pathophysiology and behavioral manifestations,
which might hold broader implications for other cognitive and psychiatric
disorders. Newer strategies to increase acetylcholine activity in the brain
through the use of procholinergic agents and avoidance of highly
anticholinergic drugs and use of drugs to enhance cerebrovascular flow
(e.g., anti-inflammatory or antiplatelet agents),use of selective dopamine
antagonists that affect D1, D2, D3, and D4 receptors differently targeted
new therapeutic approaches in delirium may offer opportunities for early
intervention, preservation of cognitive-reserve capacity, and prevention
of permanent cognitive damage by which may potentially delay or abate
the ultimate development of dementia.
Physical Examination
Examination should elicit any signs of systemic illness, focal
neurological abnormalities, meningism, increased intracranial pressure,
extracranial cerebrovascular disease, or head trauma. In delirium, less
specific findings include an action or postural tremor of high frequency
(8-10 Hz), asterixis or brief lapses in tonic posture, especially at the wrist;
multifocal myoclonus or shocklikc jerks from diverse sites; choreiform
movements; dysarthria; and gait instability. agitation or psychomotor
retardation, apathy, waxy flexibility,catatonia, or carphologia ("lint-

27
picking" behavior). The presence of hyperactivity of the autonomic
nervous system may be life threatening because of possible dehydration,
electrolyte disturbances, or tachyarrhythmia’s
Laboratory Tests
Complete blood cell count; measurements of glucose, electrolytes,
blood urea nitrogen, creatinine, transaminase, and ammonia levels;
thyroid function tests; arterial blood gas studies; chest x-ray films;
electrocardiogram; urinalysis; and urine drug screening. computed
tomographic or magnetic resonance imaging scan of the brain, especially
if there are focal neurological findings or suspicions of increased
intracranial pressure, a space-occupying lesion, or head trauma. when the
cause is uncertain the lumbar puncture should be done
EEG changes Disorganization of the usual cerebral rhythms and
generalized slowing are the most common changes.
Both hypoactive and hyperactive subtypes of delirium have
similar EEG slowing, low-voltage fast activity is also present on
withdrawal from sedative drugs or alcohol EEG patterns from intracranial
causes of delirium include focal slowing, asymmetric delta activity, and
paroxysmal discharges (spikes, sharp waves, and spike-wave complexes).

28
Periodic complexes, such as triphasic waves, and periodic lateralizing
epileptiform discharges may help in the differential diagnosis.
Clinical
feature
Delirium Dementias Stroke with
Wernicke's
aphasia
Schizophren
ia
Course
Acute onset; hours,
days, or more
Insidious onset
Sudden onset;
chronic, stable
Insidious
more
Attention
Markedly impaired
attention
and arousal
months
or years;
progressive
Normal
Normal
Fluctuation
Prominent in
attention
arousal; disturbed
day-night
cycle
Normal early;
impairment
later
Absent
Absent
Perception
Misperceptions;
hallucinations,
usually visual,
fleeting; paramnes
Prominent
fluctuations
absent; lesser
disturbances in
day-night cycle
Normal
Hallucinatio
n
with present
Speech and
language
Abnormal clarity,
speed, and
coherence;
disjointed and
dysarthric;
misnaming;
Perceptual
abnormalities
much less
prominent*; Early
anomia; empty
speech;
Prominent
paraphasias and
neologisms;
empty speech;
abnormal
comprehension
Disorgantion

29
characteristic
dysgraphia
abnormal
comprehension
paramnesia
Other
cognition
Disorientation to
time, place;
recent memory and
visuospatial
abnormalities
Disorientation to
time, place;
multiple other
higher
cognitive deficits
No other
necessary
deficits
Behavior
Lethargy or
delirium;
nonsystematized
delusions;
emotional lability
Disinterested;
disengaged;
disinhibitcd;
delusions and
other psychiatric
symptoms
Paranoia
possibly
ensuing
Electroence
phalogy
Diffuse slowing;
low-voltage
fast activity; specific
pattern
Normal early; mild
slowing
later
Normal

30
TREATMENT
Nonpharmacologic Management
Nonpharmacologic interventions was the first line in the
management of a patient with suspected delirium.
Modifying the patient’s surroundings to maximize the safety and
calmness of the environment to provide reassurance and decrease fear and
agitation associated with delirium. Paper and pencil should be provided to
improve communication when the patient cannot respond verbally
because of intubation, adequate control of pain. Physical activity should
be initiated as soon as possible in order to minimize the adverse effects of
immobility (e.g., pressure sores), avoid deconditioning and enhance
orientation. Normal sleep–wake cycles can be promoted by the use of
daytime activity and environmental cues (such as windows and clocks)
family members can reassure the patient, provide reorientation, and
reduce anxiety and agitation
Pharmacologic Management
Benzodiazepines can increase both the risk and duration of
delirium, particularly in the elderly; the use of benzodiazepines should be
reserved for the management of agitation associated with sedative–
hypnotic withdrawal
31
Electroconvulsive Therapy
As a last resort for delirious patients with severe agitation who are
not responsive to pharmacotherapy given en bloc or daily for several
days,sometimes with multiple treatments per day ECT use in delirium
should be monitored closely as ECT can cause delirium on its own.
Treatment of Specific Etiologies of Delirium
Anticholinergic Intoxication
Anticholinergic poisoning almost always results in delirium and is
often present with physical agitation and visual hallucinations. Physical
signs of antimuscarinic action include widely dilated, poorly reactive
pupils; warm, dry skin; dry mouth; fever; tachycardia; elevated blood
pressure; constipation; and urinary retention and cardiac monitoring. Use
of cholinesterase inhibitors Physostigmine was effective
Wernicke Encephalopathy
Clinical feature manifest as nystagmus and ophthalmoplegia,
mental status changes, and unsteadiness of stance and gait, although this
triad is 16 percent of patients Wernicke encephalopathy is a medical
emergency, Thiamine should be initiate immediately, either
intravenously or intramuscularly, to ensure adequate absorption
32
Substance Intoxication
First step in treating substance abuse–related delirium is the
cessation of that substance. For benzodiazepine ingestions, treatment is
benzodiazepine receptor antagonist flumazenil. In ingestions of multiple
substance such as benzodiazepines and tricyclic antidepressants or
carbamazepine flumazenil may precipitate cardiac dysrhythmias or
seizures. Opiate intoxication can be treated with Reversal with naloxone
or naltrexone may be considered with adequate support and monitoring of
the cardiovascular and respiratory status. Naloxone acts through
competitive binding at opioid receptors, can reverse all the receptor-
mediated actions of opioids, and is indicated for patients who have
significant CNS or respiratory depression.
Substance Withdrawal
An evidence-based guideline from the American Society of
Addiction Medicine recommends benzodiazepines as a first-line agent for
the treatment of alcohol withdrawal
33
Treatment in Special Population
Antiparkinsonian agents are frequently implicated in causing a
delirium. Decreasing the dosage of the antiparkinsonian agent has to be
weighed against a worsening of motor symptoms clozapine is
recommended as it is the best studied of the second-generation
antipsychotic medications.
34
METHODOLOGY AND MATERIAL
This is a longitudinal follow up study, conducted at kilpauk
medical hospital Consecutive subjects who were diagnosed with delirium
were taken into the study. The standardized protocol treatment was
provided by the treating physician .Need for the study was explained and
informed consent was obtained in writing from the care givers.
Information was collected from care givers, staff nurse and from medical
records .Rating Scale was administered during the initial session .Follow
up was done using Delirium rating scale revised – 98 and Delirium
etiology check list was administered once in 2 days up to period of 1
month till the subject recovered, absconded or expired. The sample
consisted of 152 subjects (76 alcohol withdrawal vs 76 other medical
cause). The duration of the study was from march 2018 to September
2019 (18 month).
Inclusion
Meets DSM 5 criteria for delirium
Age >18years
consecutive delirium patients admitted in medical ward

35
All delirium subject admitted alcohol withdrawal was
considered to be a definite contributory etiological factor (with or
without other etiological factor)
Ethical approval
Ethical approval for the study was obtained from the Ethics
committee, Government Kilpauk Medical College, Chennai.
Tools used
• Semi structured socio demographic proforma (Name, age,
hospital no., gender, type of family)
• Kuppuswamy socioeconomic scale
Delirium rating scale revised – 98
Delirium etiology check list
Cognitive Test for Delirium [CTD]
Brief Psychiatric Rating Scale (BPRS)
Severity Of Alcohol Dependence Questionnaire (SADQ)

36
Kuppuswamy socioeconomic status scale
The modified Kuppuswamy scale is used to measure the
socioeconomic class. The instrument was structured by Kuppuswamy in
1976. it comprises several scores such as income per month of the
family, occupation of the family head along with , education which
gives a score between 3 -29. According to instrument the study
population is classified into five socioeconomic classes which includes
1. Upper.
2. Upper middle.
3. Lower middle.
4. Upper lower.
5. Lower.
The score for education is between 1 to 7, occupation between 1 to
10 and monthly income between 1 to 12. The scale was repeatedly
modified because of the price index changes as it that affects the validity
of the monthly income subset in the instrument (Patro BK et al. 2012.,
Sharma et al .2014., Kumar BR et al. 2012,, Saleem Sheikh e
37
Cognitive Test for Delirium
It is a neuropsychological function test that relay on visual
abilities and can be administered to individuals including those who are
cannot speak or intubated. It is initially structured for ICU patients who
are severely ill. The instrument uses non verbal responses such as raising
hand, nodding head, pointing by the patients. It measures the 5
neuropsychological domains
1. Orientation.
2. Attention.
3. Memory.
4. Comprehension.
5. Vigilance
It is scored between 0-30, the higher scores represents better
cognitive function. A cut off of <19 is used to differentiate delirium from
other disorders, it is also used as a unidimensional and continuous
measure of cognition in acute confusional state. It can distinguish reliably
between depression, schizophrenia and dementia (Hart et al, 1996).
38
Revised Delirium Rating Scale (DRS-R-98)
This scale is most widely used instrument for measure the severity
of symptom in acute confusional state; it can be used both as an
assessment and a diagnostic tool. It consists of3 diagnostic items
(physical disorder, fluctuation of symptoms, temporal onset of symptoms)
and 13 severity items and it covers most of the symptoms. The individual
items severity is scored between 0 to 3 points. The total DRS-R98
severity scores between from 0-39 with severe delirious state indicating
higher scores. Diagnosis of delirium is made with a cut-off score >15.
The whole scale is used initially for indentifying different differential
diagnosis by capturing specific features of acute confusional state like
acute onset of symptom severity and fluctuating nature. The scale is used
to score symptoms from variable periods and can be used as a follow up
instrument. Inter-rater reliability is high, specificity ,validity and
sensitivity form differentiating acute confusional state from other
neuropsychiatric disorders such as schizophrenia, depression, and
dementia is high(Trzepacz et al, 2001).
39
Etiological assessment
The Delirium Aetiology Rating Checklist (DEC), assesses the
different aetiologies of acute confusional state by scoring 12 contributing
causes. Each causal category is scored between a five-point scales
ranging from
0. Ruled out
1, present but apparently not contributory
2. Present and possibly contributory
3. Likely cause
4. Definite cause
It allows for two or more concomitant causes for Acute
confusional state. (Meagher and Trzepacz, 2009)
Severity of alcohol dependence questionnaire (SADQ)
The SADQ is a scale for measuring alcohol dependence severity.
It was categories as the level of dependency to alcohol in based on score
of 30+ as severe dependency and between scores of 16-30 as moderate
dependency and of less than 16 taken as mild dependency. Questions
cover following Onset of withdrawal symptoms, Frequency of alcohol

40
consumption, Affective withdrawal symptoms, Physical withdrawal
symptoms, Relief drinking
Brief Psychiatric Rating Scale
The Brief Psychiatric Rating Scale assesses psychopathology
(Hafkenscheid, 1991).an 18 items scale is used since 1967 as the standard
version. The five factor scores including, tension-excitement, withdrawal-
retardation, thinking disturbance, hostile suspiciousness, and anxious
depression, other than psychotic phenomology can also be scored. Due to
its flexibility and easy adaptability it is used widely in research and
clinical settings. (Van der Does (1993).Overall, J.E., & Hafkenscheid, A.
(1991) Gorham, D.R. (1962)

41
STATISTICAL ANALYSIS
Descriptive data.
• Frequency,
• Percentage,
• Mean,
• Standard deviation calculated.
Comparison between the groups was done by using- SPSS-14
• 2‐tailed Student’s t,
• chi‐square,
• Fisher’s exact tests.
Sample size-76 vs 76
• Confident index -95%
• Power-75%

42
• Sample size calculated using previous study Sandeep Grover
et el Delusion Prevalence,–general medical condition (27.8%) & Alcohol
withdrawal delirium (48.2%)[p=.001]
Calculated and derived value a sample size of =76 general medical
condition vs 76 Alcohol withdrawal delirium

43
RESULT
A total of 152 subjects were taken for this study in which 76
subjects were diagnosed to have alcohol withdrawal delirium and 76
subjects were diagnosed having other medical cause of delirium
The subjects were enrolled from Psychiatric Ward 35.5% (54),
Medicine Ward 31.6% (48), Intensive care unit 19.1% (29), Surgery
Ward 8.6%(13), Orthopedic Ward 2.6%(4), obstetrics and gynecology
1.3%(2), and causality 1.3%(2).
Diagram 1 frequency of subject obtained
.
Percentage
Psychiatric Ward 35.5%
Medicine Ward 31.6%
Intensive care unit 19.1%
Surgery Ward 8.6%
Orthopedic Ward 2.6%
obstetrics and gynecology1.3%
causality1.3%

44
Table : Total socio demographic data
Age 16-30 years (23) 15.1%
31-45 years (34) 22.4%
46-60 years (56) 36.8%
Above 60 years (39) 25.7%
Gender Male (131) 86.2%
Female (21) 13.8%
Socio-Economic Status Upper (2)
Upper Middle (7)
Lower Middle (72)
Upper Lower (57)
Lower (14)
Type of Family Nuclear (104)
68.4%
Joint (45) 29.6%
Extended (3) 2.0%
H/o of Concurrent
Substance Use
SLT (32)
21.1%
Cannabis (6)
3.9%
Nicotine (57)

45
37.5%
Previous h/o of Seizures (26)
17.1%
Previous h/o of Head
Injury
(1)
.7%
Previous h/o Delirium
Tremens
(20)
13.2%
Family h/o Psychiatric
Illness
(8)
5.3%
Family h/o Alcohol Use
Disorder
(30)
19.7%
The mean age of participants was 49.The male to female ratio
was86:14. The most of the subjects are from lower middle socioeconomic
state (47.4%) according to Kuppuswamy socio demographic score,
followed by Upper Lower socioeconomic states 37.5%, Lower
socioeconomic states 9.2% Upper Middle socioeconomic states 4.6%
Upper socioeconomic states 1.3%.Type of Family of subjects were
nuclear 68.4%, Joint29.6% and Extended2.0%.
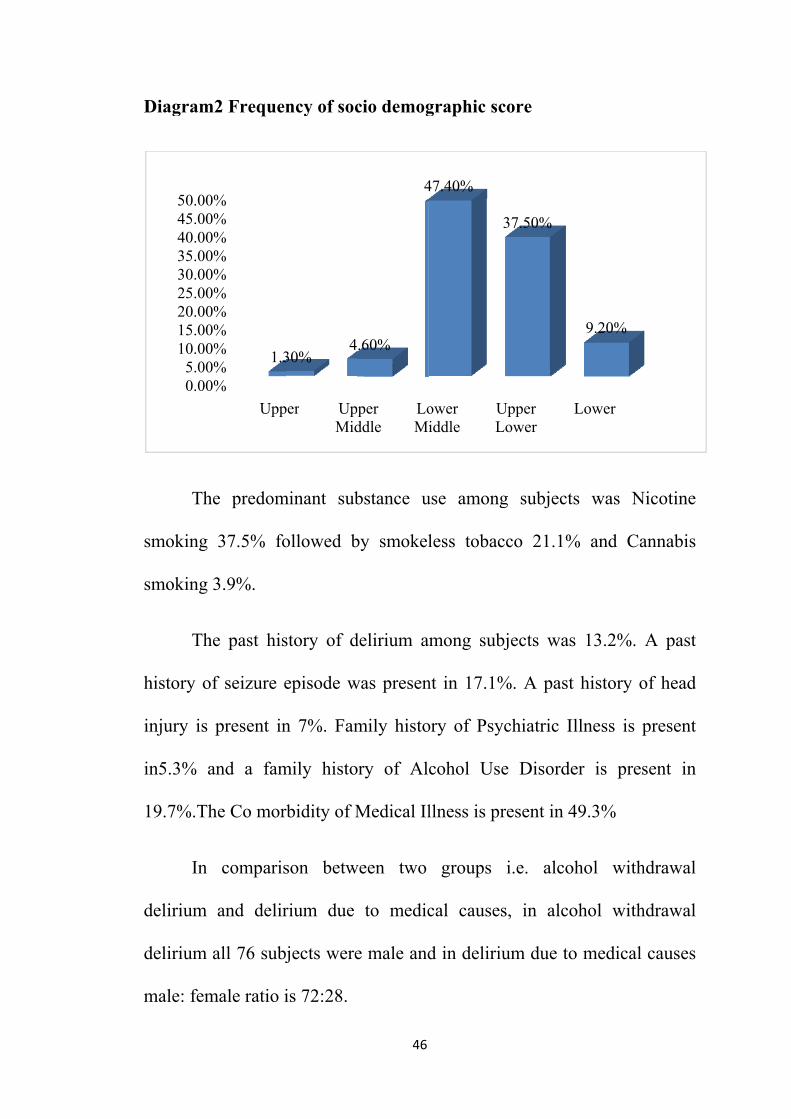
Diagram2
The
smoking
smoking 3
The
history of
injury is
in5.3% a
19.7%.Th
In
delirium
delirium a
male: fem
0.00%5.00%
10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%50.00%
2 Frequen
e predom
37.5% fo
3.9%.
e past his
f seizure e
present in
and a fam
he Co mor
comparis
and delir
all 76 subj
male ratio i
%%%%%%%%%%%
Upp
1.3
ncy of soc
minant sub
ollowed b
story of d
episode w
n 7%. Fam
mily histo
rbidity of M
son betw
rium due
jects were
is 72:28.
per UpMid
30%4
46
cio demog
bstance u
by smokel
delirium a
was presen
mily histo
ory of Al
Medical Il
ween two
to medic
e male and
per ddle
LoMi
.60%
4
graphic sc
use among
less tobac
mong sub
nt in 17.1%
ory of Psy
cohol Us
llness is pr
groups
cal cause
d in deliri
ower iddle
UL
47.40%
core
g subject
cco 21.1%
bjects was
%. A past
ychiatric I
e Disorde
resent in 4
i.e. alco
s, in alco
ium due to
Upper Lower
37.50%
ts was N
% and Ca
s 13.2%.
t history o
Illness is p
er is pres
49.3%
ohol with
ohol with
o medical
Lower
9.20%
Nicotine
annabis
A past
of head
present
sent in
hdrawal
hdrawal
causes
47
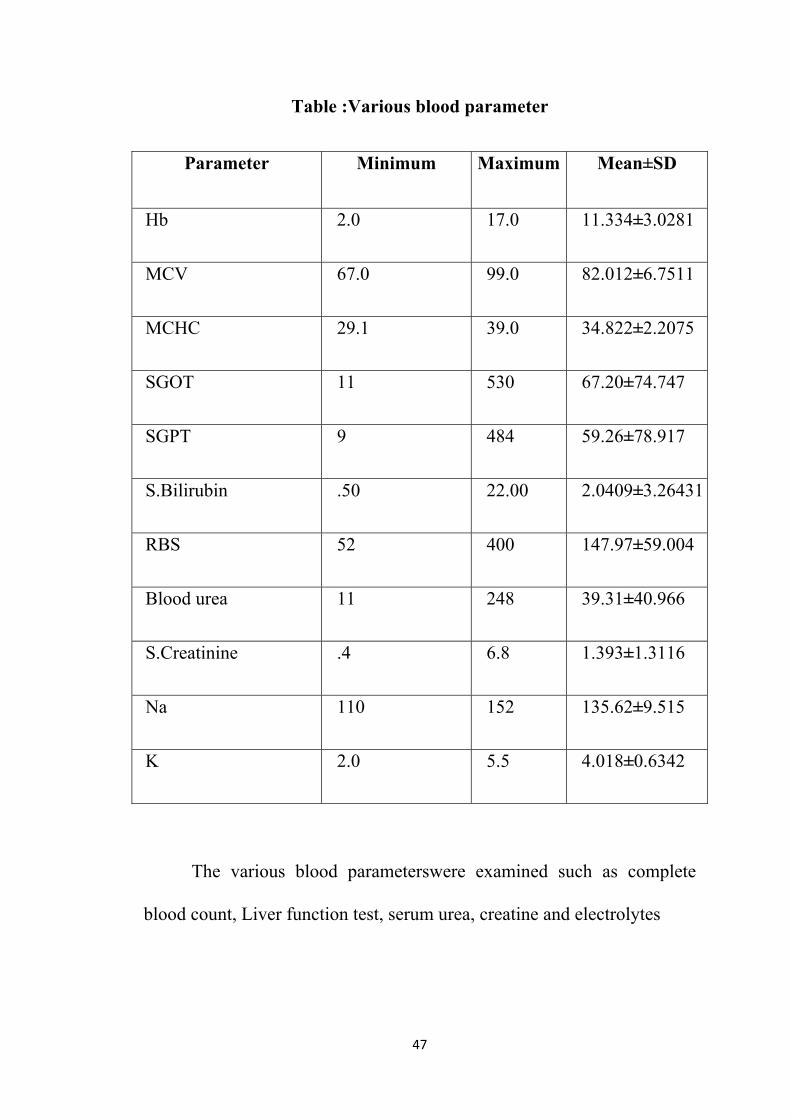
Table :Various blood parameter
Parameter Minimum Maximum Mean±SD
Hb 2.0 17.0 11.334±3.0281
MCV 67.0 99.0 82.012±6.7511
MCHC 29.1 39.0 34.822±2.2075
SGOT 11 530 67.20±74.747
SGPT 9 484 59.26±78.917
S.Bilirubin .50 22.00 2.0409±3.26431
RBS 52 400 147.97±59.004
Blood urea 11 248 39.31±40.966
S.Creatinine .4 6.8 1.393±1.3116
Na 110 152 135.62±9.515
K 2.0 5.5 4.018±0.6342
The various blood parameterswere examined such as complete
blood count, Liver function test, serum urea, creatine and electrolytes

48
Table: Longitudinal analysis using Drs-98 scale, measured 48 hours
apart
Parameters DRS-1 DRS-2 DRS-3
Mean±SD Mean±SD Mean±SD
Sleep wake cycle
disturbance
2.75±0.434 1.26±0.750 0.46±0.562
Perceptual Disturbance 1.19±1.270 0.23±0.521 0.06±0.238
Delusions .51±1.042 0.18±0.624 0.09±0.445
Liability of affect 2.05±0.961 0.75±0.721 0.21±0.440
Language 1.36±1.216 0.40±0.721 0.05±0.240
Thought process
abnormalities
0.61±0.971 0.22±0.542 0.09±0.333
Motor agitation 1.76±1.223 0.66±0.745 0.14±0.383
Motor retardation 0.89±1.213 0.32±0.637 0.09±0.421
Orientation 2.13±0.995 0.70±0.789 0.13±0.376
Attention 2.03±1.023 0.51±0.651 0.08±0.316
Short-term memory 1.52±1.104 0.46±0.650 0.07±0.274
Long-term memory 0.99±1.058 0.30±0.562 0.05±0.300
Visuospatial ability 1.45±1.167 0.39±0.710 0.07±0.307

49
SURFACE Diagram frequency of DRS -98
00.5
11.5
22.5
3
Sleep-wake cycle disturbance Perceptual
DisturbanceDelusions
Lability of affect
Language
Thought process abnormalities
Motor agitationMotor retardation
OrientationAttention
Short-term memory
Long-term memory
Visuospatial ability
Temporal onset of symptoms
Fluctuation of symptom severity
Physical disorder
DRS-1
DRS-2
DRS-3
50
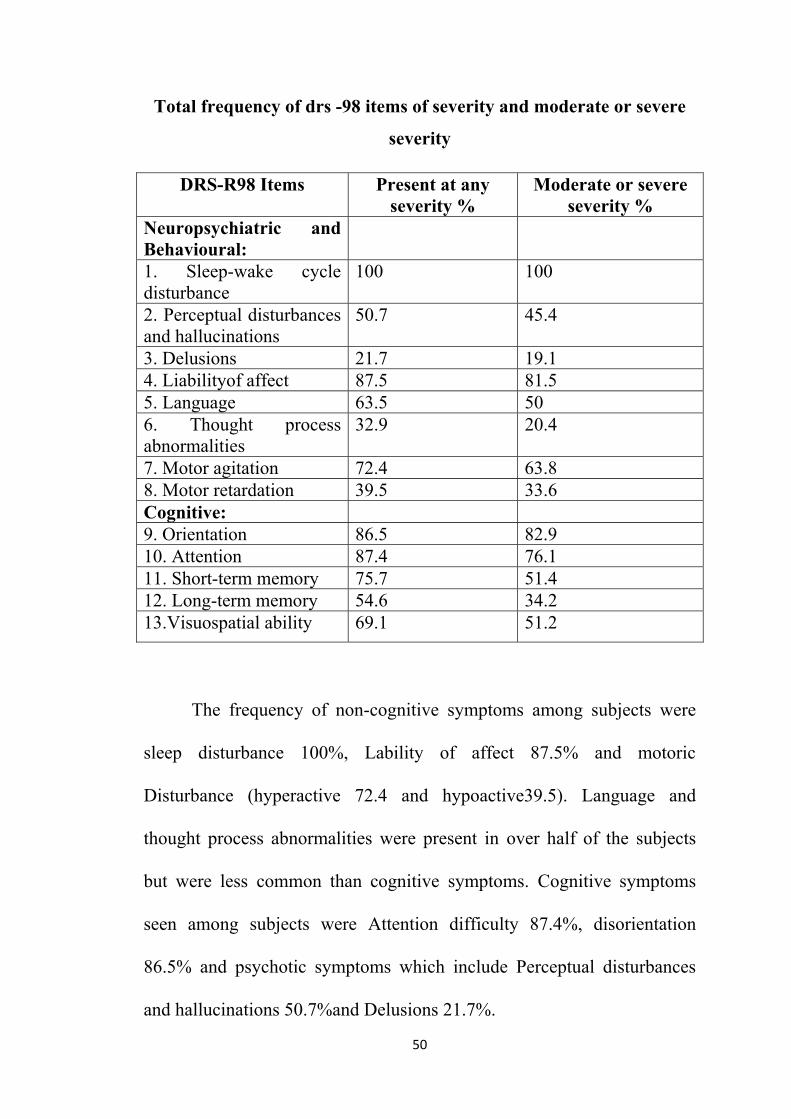
Total frequency of drs -98 items of severity and moderate or severe
severity
DRS-R98 Items Present at any severity %
Moderate or severe severity %
Neuropsychiatric and Behavioural:
1. Sleep-wake cycle disturbance
100 100
2. Perceptual disturbances and hallucinations
50.7 45.4
3. Delusions 21.7 19.1 4. Liabilityof affect 87.5 81.5 5. Language 63.5 50 6. Thought process abnormalities
32.9 20.4
7. Motor agitation 72.4 63.8 8. Motor retardation 39.5 33.6 Cognitive: 9. Orientation 86.5 82.9 10. Attention 87.4 76.1 11. Short-term memory 75.7 51.4 12. Long-term memory 54.6 34.2 13.Visuospatial ability 69.1 51.2
The frequency of non-cognitive symptoms among subjects were
sleep disturbance 100%, Lability of affect 87.5% and motoric.
Disturbance (hyperactive 72.4 and hypoactive39.5). Language and
thought process abnormalities were present in .over half of the subjects
but were less. common than cognitive .symptoms.. Cognitive symptoms
seen among subjects were Attention difficulty 87.4%, disorientation
86.5% and psychotic symptoms which include Perceptual disturbances
and hallucinations 50.7%and Delusions 21.7%.
51
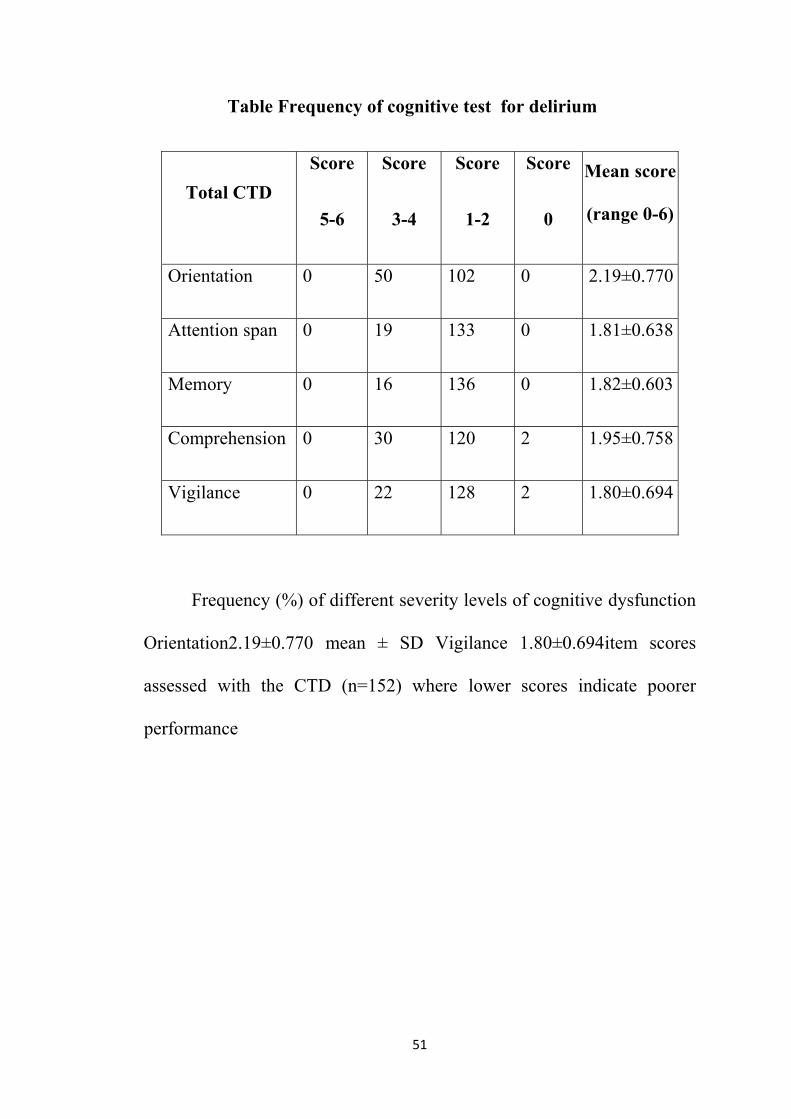
Table Frequency of cognitive test for delirium
Total CTD Score
.5-6
Score.
3-4
Score.
1-2
Score
0
Mean .score
(range 0-6)
Orientation. 0 50 102 0 2.19±0.770
Attention .span 0 19 133 0 1.81±0.638
Memory 0 16 136 0 1.82±0.603
Comprehension. 0 30 120 2 1.95±0.758
Vigilance. 0 22 128 2 1.80±0.694
Frequency (%) of different .severity levels of cognitive. dysfunction
Orientation2.19±0.770 .mean ± SD Vigilance 1.80±0.694.item scores
assessed .with the CTD (n=152) where .lower scores indicate poorer
.performance

0
50
0
0
102
0
Sco
0
19
133
0
ore 5-6
52
0
16
136
Score 3-4
0
3
6
0
Score 1-
0
120
2
2 Score
0
22
128
2
e 0
53
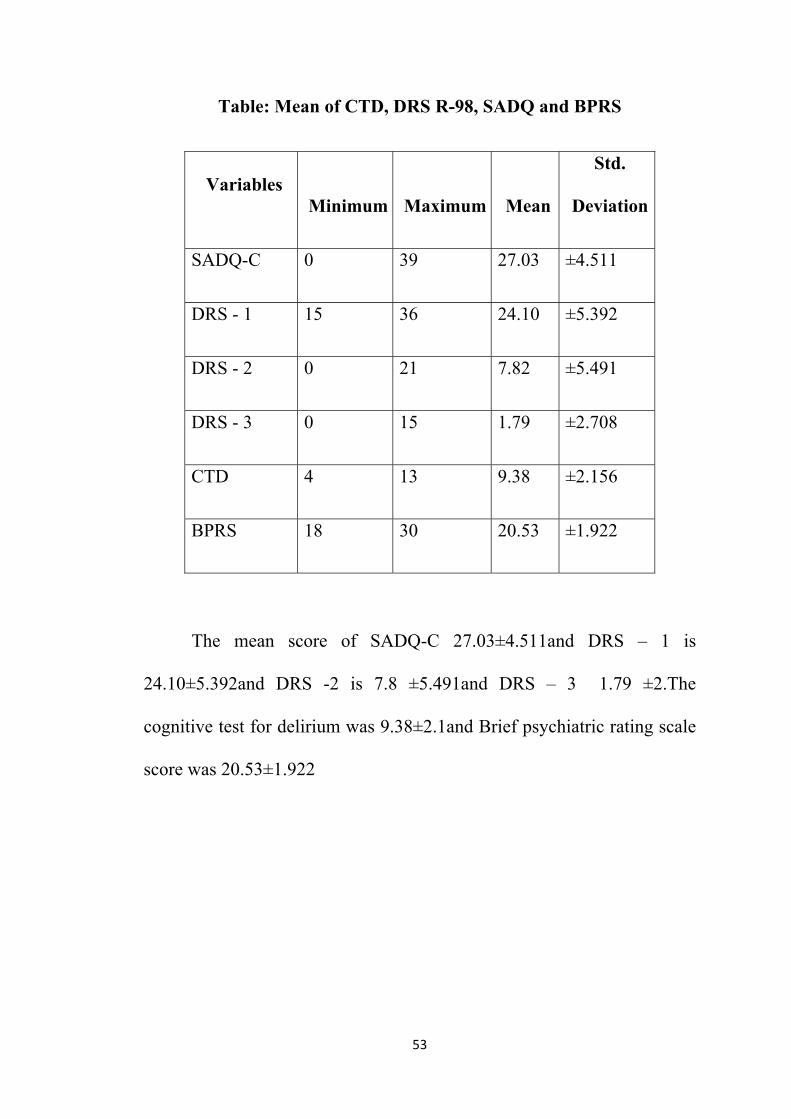
Table: Mean of CTD, DRS R-98, SADQ and BPRS
Variables Minimum Maximum Mean
Std.
Deviation
SADQ-C 0 39 27.03 ±4.511
DRS - 1 15 36 24.10 ±5.392
DRS - 2 0 21 7.82 ±5.491
DRS - 3 0 15 1.79 ±2.708
CTD 4 13 9.38 ±2.156
BPRS 18 30 20.53 ±1.922
The mean score of SADQ-C 27.03±4.511and DRS – 1 is
24.10±5.392and DRS -2 is 7.8 ±5.491and DRS – 3 1.79 ±2.The
cognitive test for delirium was 9.38±2.1and Brief psychiatric rating scale
score was 20.53±1.922
54
Table Correlation between cognitive test for Delirium and Delirium
rating scale -98
DRS
CTD Orientation.
Attention
.span Memory Comprehension. Vigilance
Sleep-wake. cycle
disturbance
-0.015
(0.856)
-0.006
(0.942)
0.076
(0.353
-0.096
(0.242)
0.027
(0.737)
Perceptual .
Disturbance
0.145
(0.074)
0.086
(0.292)
0.193*
(0.017
0.023
(0.779)
0.180*
(0.027)
Delusions. 0.348**
(0.000)
-0.071
(0.385)
0.120
(0.141
0.374**
(0.000)
0.127
(0.118)
Lability of . affect -0.112
(0.169)
0.189*
(0.020)
0.097
(0.235
-0.069
(0.396)
-0.063
(0.439)
Language. -0.067
(0.411)
-0.167*
(0.040)
-0.162*
(0.047
-0.082
(0.313)
-0.336**
(0.000)
Thought .process
abnormalities
0.057
(0.484)
0.027
(0.739)
0.113
(0.167
0.092
(0.259)
-0.002
(0.977)
Motor .agitation 0.092
(0.260)
0.076
(0.353)
0.047
(0.569
009
(0.910)
0.050
(0.538)
Motor .retardation -0.227**
(0.005)
-0.077
(0.343)
-0.181*
(0.026
-0.113
(0.164)
-0.222**
(0.006)
55
Orientation -0.293**
(0.000)
0.196*
(0.015)
-0.059
(0.472
-0.124
(0.129)
-0.230**
(0.004)
Attention. 0.078
(0.341)
-0.002
(0.977)
-0.046
(0.575
-0.016
(0.849)
-0.030
(0.716)
Short-term
.memory
-0.032
(0.698)
0.057
(0.485)
-0.174*
(0.032
-0.050
(0.538)
-0.034
(0.681)
Long-term
memory.
-.0291**
(0.000)
-0.002
(0.982)
-0.158
(0.052
0.041
(0.617)
-0.119
(0.144)
Visuospatial
.ability
-0.022
(0.789)
-0.027
(0.742)
-0.023
(0.776
-0.096
(0.237)
-0.238**
(0.003)
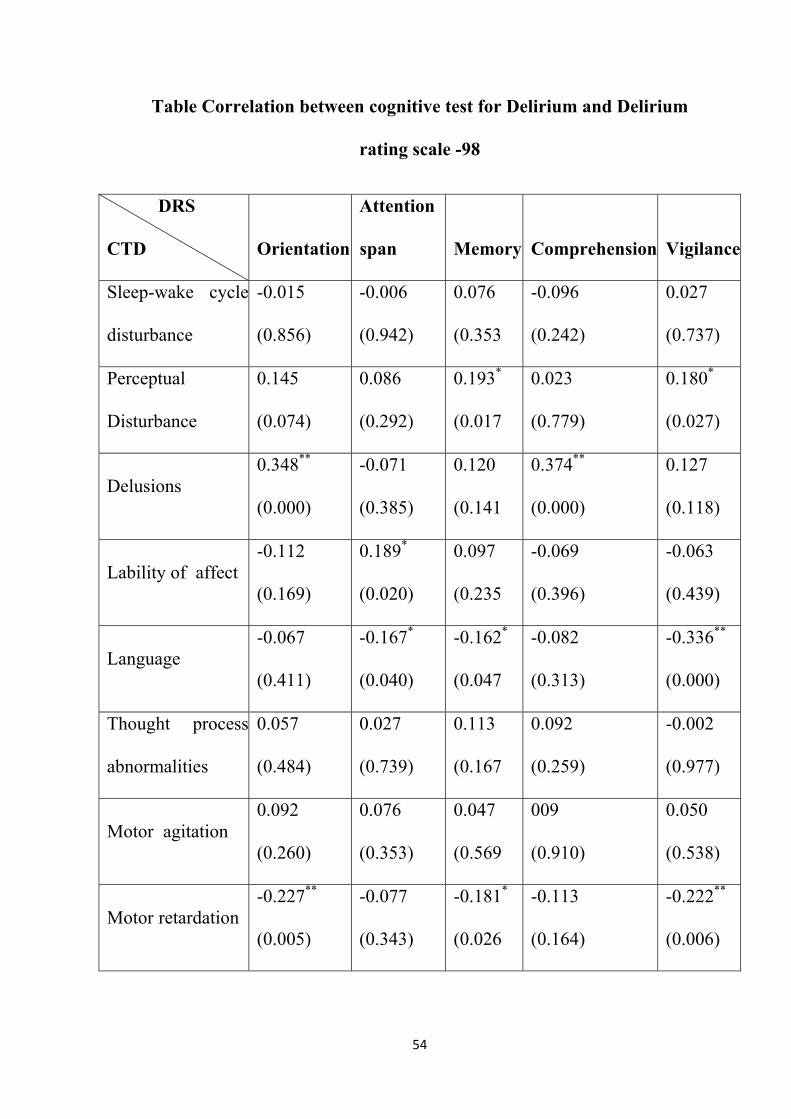
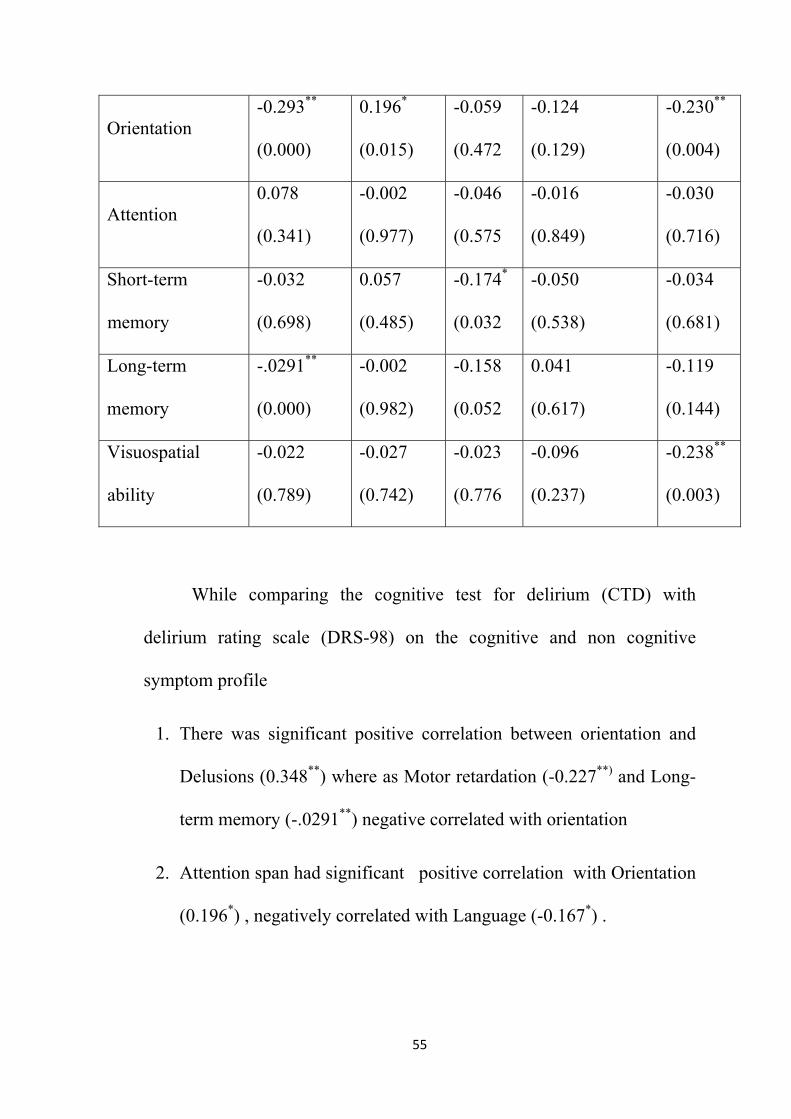
While comparing the cognitive test for delirium (CTD) with
delirium rating scale (DRS-98) on the cognitive and non cognitive
symptom profile
1. There was significant positive correlation between orientation and
Delusions (0.348**) where as Motor retardation (-0.227**) and Long-
term memory (-.0291**) negative correlated with orientation
2. Attention span had significant positive correlation with Orientation
(0.196*) , negatively correlated with Language (-0.167*) .

56
3. Positive correlation between Memory and perceptual Disturbance
(0.193*) was present. Short-term memory (-0.174*) and Motor
retardation ( 0.181*) negatively correlated.
4. Comprehension had significant positive correlated Delusions
(0.374**)
5. Vigilance had significant positive correlation with Perceptual
Disturbance (0.180*) and negatively correlated with Language(-
0.336** ) Visuospatial ability (-0.238**), Orientation (-0.230**) and
Motor retardation(-0.222**).

57
Table duration of delirium, hospital ,treatment and outcome
DAYS TOTAL
SUBJECT
Total duration of delirium 1 25
2 58
3 34
4 19
>5 16
Total duration of Hospital <5 77
6-10 43
11-45 32
TRATMENT GIVEN Benzodiazepam Usage (82 ) 56.5%
Antipsychotic Usage (22) 14.4%
Outcome Recovered 137 90.2%
Death 11 7.2%
Absconded 4 2.6%
The duration of hospital stay hospital stay is 8 days and in half of
the subjects the delirium resolved within 2 days (83). Treatment given is
benzodiazepines 56.5%, antipsychotic 14.4%.

58
The outcome of the delirium in subjects is Recovered 90.2%
Death7.2% Absconded2.6%.
outcome of the delirium
Recovered 90.2%
Death7.2%
Absconded2.6%

59
Table: Medical cause of delirium
Causes Possible Probable
Drug. intoxication 0 0
Drug. withdrawal (5)6.5% 0
Metabolic/.endocrine (19)25% 41 (53.9%)
Traumatic .brain injury 0 0
Seizures (4)5.2% (8) 10.5%
Infection. intracranial (8)19.8% (2) 2.6%
Infection. (systemic) 6 (9 )11.8%
Neoplasm. intracranial 0 (1) 1.3%
Neoplasm systemic (1) 1.3% 0
Cerebrovascular. (19)25% (3) 3.9%
Organ .insufficiency (6)7.8% 0
Other central .nervous system 0 (2 )2.6%
Others. (2)2.6% 0
According to delirium check list, cause of medical delirium (76)
with most definite and likely cause (>3) were Metabolic/endocrine (41)
53.9%, Infection (systemic) 11.8%, Seizures10.5%, Cerebrovascular
3.9%, Infection intracranial and Other central nervous system is2.6%. In
possible contributory and present and not contributory cause (<2),

Metabolic
insufficien
causes2.6
Subtypes
The
who score
those who
and those
is subtype
0
5
10
15
20
25
30
35
40
45
c/endocrin
ncy 7.8%
6% and sys
s of medic
e motor a
e positive
o score po
e who are
ed as mixe
ne cause i
%, Drug
stemic Ne
cal cause o
actives has
on motor
ositive on
scored po
ed type
60
is 25%, In
withdraw
eoplasm 1.
of deliriu
s been sub
r agitation
n motor re
ositive in b
nfection i
wal 6.5%
.3%,
m
btyped by
issubtype
etardation
both moto
intracrania
%, Seizur
y using drs
ed as hype
is subtye
r agitation
al 19.8%,
res5.2%,
s-98 scale
eractive ty
ed as hypo
n and retar
P
P
Organ
Others
e, those
ype and
oactive
rdation
Possible
Probable

61
Table Frequency of subtype of motor agitation or retardation
Causes.
Subtypes
Hypoactive Mixed Hyperactive
Percent Percent Percent
Drug. withdrawal (6) 7.9% (1) 1.3% (4) 5.3%
Metabolic/.Endocrine (3) 3.9% (13) 17.1% (37) 48.7%
Seizures. 0 (2) 2.6% (4) 5.3%
Infection
.(Intracranial) (3) 3.9% (8) 10.5% (2) 2.6%
Infection .(Systemic) (2) 2.6% (6) 7.9% (9) 11.8%
Neoplasm
.(Intracranial) 0 0 (1) 1.3%
Neoplasm.
(systemic) 0 (1) 1.3% 0
Cerebrovascular. 0 (17) 22.4% (3) 3.9%
Organ. Insufficiency (10) 13.2% (6) 7.9% 0
Other (Central
.Nervous System) 0 0 (2) 2.6%
Other 0 2 2.6% 0

62
The hyper active delirium is seen more in delirium due to
Metabolic/Endocrine causes(48.7%) and mixed type is seen in delirium
due to Cerebrovascular causes (22.4%) and hypoactive delirium is seen in
delirium due to Organ Insufficiency (13.2%)
63
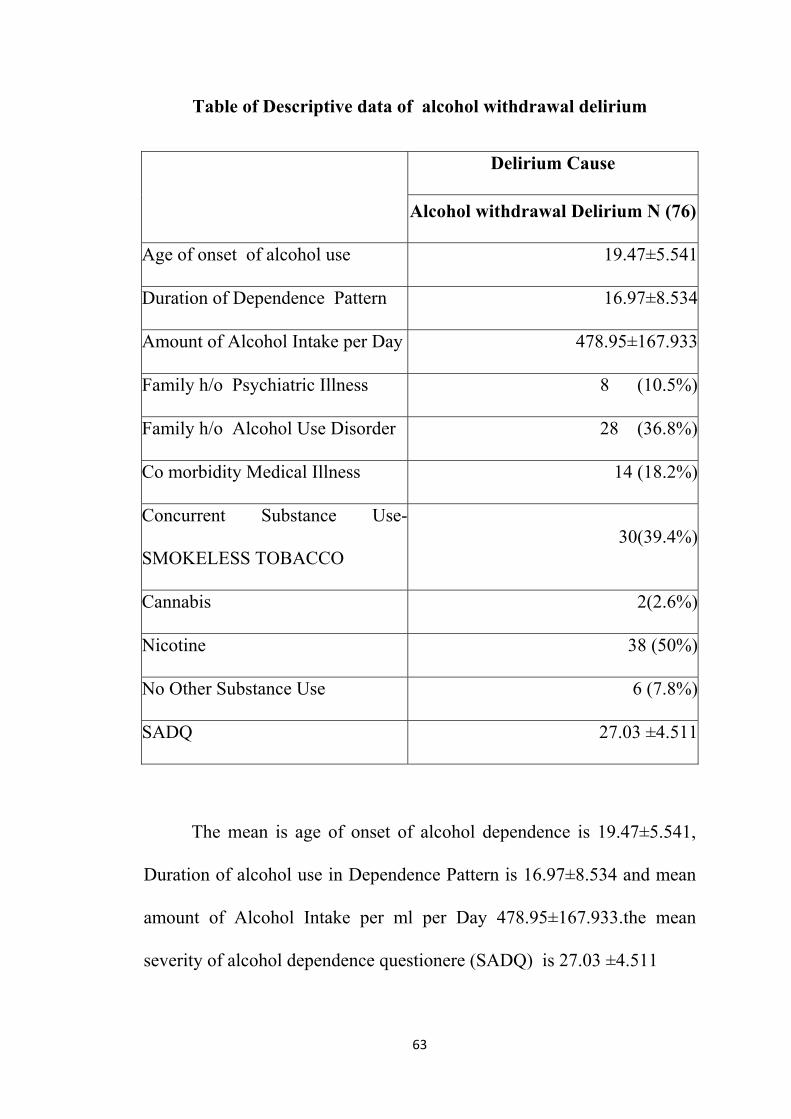
Table of Descriptive data of alcohol withdrawal delirium
Delirium Cause
Alcohol withdrawal Delirium N (76)
Age of onset of alcohol use 19.47±5.541
Duration of Dependence Pattern 16.97±8.534
Amount of Alcohol Intake per Day 478.95±167.933
Family h/o Psychiatric Illness 8 (10.5%)
Family h/o Alcohol Use Disorder 28 (36.8%)
Co morbidity Medical Illness 14 (18.2%)
Concurrent Substance Use-
SMOKELESS TOBACCO 30(39.4%)
Cannabis 2(2.6%)
Nicotine 38 (50%)
No Other Substance Use 6 (7.8%)
SADQ 27.03 ±4.511
The mean is age of onset of alcohol dependence is 19.47±5.541,
Duration of alcohol use in Dependence Pattern is 16.97±8.534 and mean
amount of Alcohol Intake per ml per Day 478.95±167.933.the mean
severity of alcohol dependence questionere (SADQ) is 27.03 ±4.511

64
Table of Compare the medical and alcohol withdrawal delirium
Age and Delirium Cause
Age
Delirium Cause
Chi-
Square
Value
P-ValueAlcohol withdrawal
Delirium
N 76
Medical
Illness
Delirium
N 76
16-30 years 14 9
16.108 <0.001*31-45 years 24 10
46-60 years 28 28
Above 60 years 10 29
On comparing the age between medical illness delirium and
alcohol with drawal Delirium, most subjects having medical illness
delirium are more than 60 years of age. This have been shown statistical
significance when compared to the alcohol withdrawal delirium (p value
0.01)

65
0
5
10
15
20
25
30
35
16-30 years 31-45 years 46-60 years Above 60 years
Alcohol withdrawal Delirium
Medical Illness Delirium

66
Table : Comparison of demographic details between alcohol
withdrawal and medical illness delirium
Variable
Compare
Chi-Square
Value P-Value
Alcohol
withdrawal
Delirium
N 76
Medical
Illness
Delirium
N 76
Previous h/o
Seizures
22
28.9%
4
5.2% 15.033a ns
Previous h/o Head
Injury
0 1 1.007 0.316(ns)
Previous h/o
Delirium
18
23.6%
2
2.6% 14.739 0.001**
Family h/o
Alcohol Use
Disorder
28
36.8%
2
2.6% 28.074 0.001**
Family h/o
Psychiatric Illness
8
10.5%
0 8.444 0.006**
Comorbidity
Medical Illness
14
61 58.142 0.001**

67
On comparing the past history of seizure, there were no significant
differences between alcohol withdrawal delirium and medical illness
delirium. The Family history of Psychiatric Illness in Alcohol withdrawal
Delirium (10.5%)is statistically significant withChi-Square Value 8.444 p
value is < 0.006**. In Medical illness delirium Comorbid Medical
Illness(such as hypertension, diabetes etc.) were statically significant with
Chi-Square value of58.142 and p value of 0.001**.
Surface diagram depicting mean difference between alcohol
withdrawal Delirium and other cause of medical delirium
On Comparing the clinical profile differences among groups,
it was found that subjects with alcohol withdrawal Delirium had more
psychotic symptomatic such Perceptual Disturbance 1.45, Delusions
.89and motor disturbances - Motor agitation 2.22
.00
.501.001.502.002.503.00
Sleep-…Perceptual …
Delusions
Lability of …
Language
Thought …
Motor …Motor …
OrientationAttention
Short-…
Long-term …
Visuospati…
Temporal …
Fluctuatio…Physical …
DRS-1 Medical Illness DeliriumDRS-3 Alcohol withdrawal Delirium DRS-2Medical Illness DeliriumDRS-3 Alcohol withdrawal Delirium

68
Table: comparison of frequency of symptom profile and severity
between groups
Delirium rating scale
R 98
Present at any .severity
%
Moderate .or severe
severity %
Alcohol
withdrawal.
Delirium
N 76
Medical
Illness
.Delirium
N 76
Alcohol
withdrawal
.Delirium
N 76
Medical
Illness
Delirium
N 76
Neuropsychiatric. and
Behavioural:
1. Sleep-wake. cycle
disturbance
100 100 100 100
2. Perceptual.
disturbances and
hallucinations
63.2 38.2 55.2 35.6
3. Delusions 36.3 5.3 33.7 4
4. Lability .of affect 84.2 90.8 78.9 84.2
5. Language 50 76.3 36.2 63.1
6. Thought .process
abnormalities
36.2 28.9 23.4 17.1
69
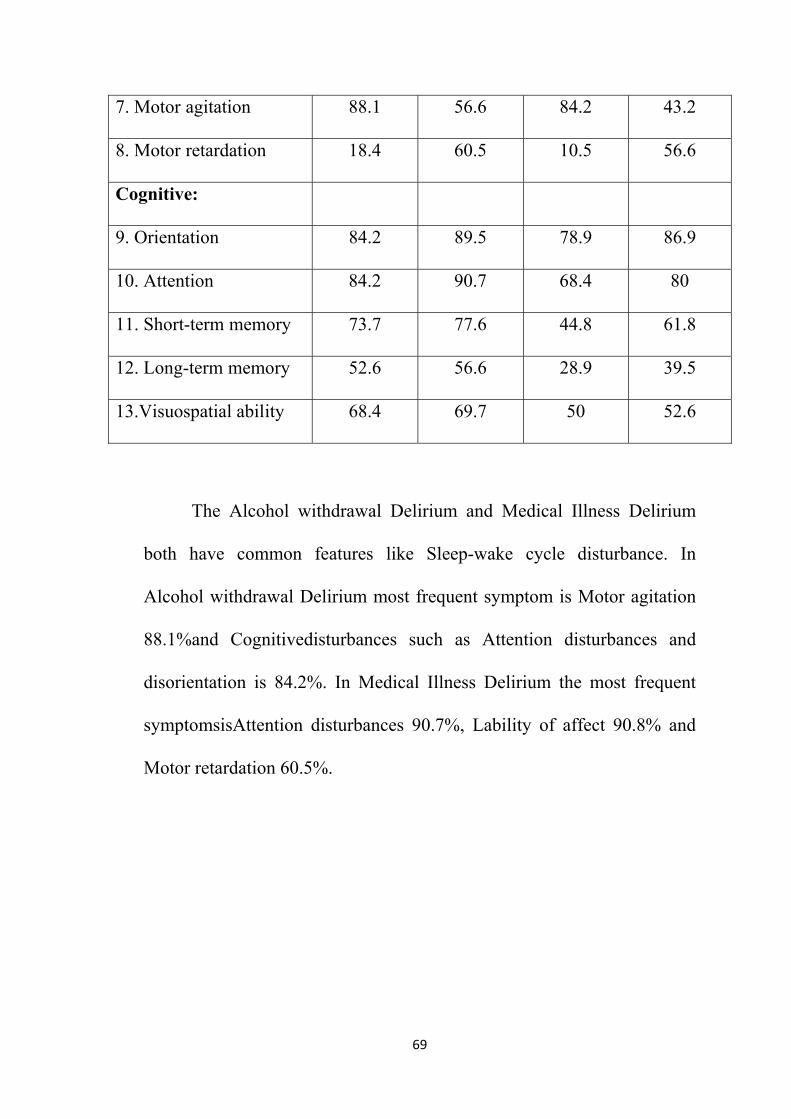
7. Motor. agitation 88.1 56.6 84.2 43.2
8. Motor. retardation 18.4 60.5 10.5 56.6
Cognitive:
9. Orientation. 84.2 89.5 78.9 86.9
10. Attention 84.2 90.7 68.4 80
11. Short-term .memory 73.7 77.6 44.8 61.8
12. Long-term. memory 52.6 56.6 28.9 39.5
13.Visuospatial abil.ity 68.4 69.7 50 52.6
The Alcohol withdrawal Delirium and Medical Illness Delirium
both have common features like Sleep-wake cycle disturbance. In
Alcohol withdrawal Delirium most frequent symptom is Motor agitation
88.1%and Cognitivedisturbances such as Attention disturbances and
disorientation is 84.2%. In Medical Illness Delirium the most frequent
symptomsisAttention disturbances 90.7%, Lability of affect 90.8% and
Motor retardation 60.5%.
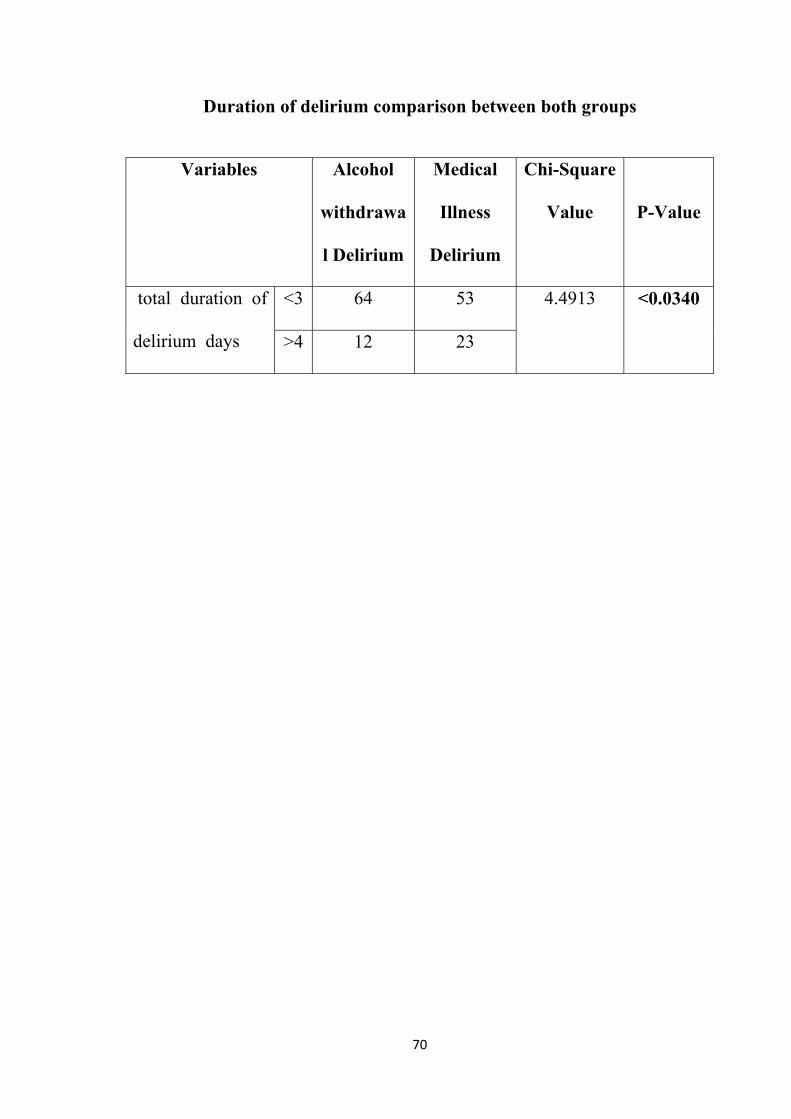
70
Duration of delirium comparison between both groups
Variables Alcohol
withdrawa
l Delirium
Medical
Illness
Delirium
Chi-Square
Value
P-Value
total duration of
delirium days
<3 64 53 4.4913
<0.0340
>4 12 23

71
Independent Samples Test between Delirium Cause and Total duration of delirium
Total
duration
of delirium
Delirium Cause
t-value P-ValueAlcohol withdrawal
Delirium
Medical
Illness
Delirium
2.45±1.171 3.22±3.408 1.878 .062
This table compares between the total duration of delirium
between Alcohol withdrawal and Medical Illness groups. In Alcohol
Withdrawal Delirium (84.2%) and Medical Illness Delirium (69%)
recovery is seen in 3 days. Delirium persisting for more than 3days in
Alcohol withdrawal group is about 15.8%and Medical Illness group is
about 30.3%, there no statistical significance among two groups
regarding the duration of delirium.
72
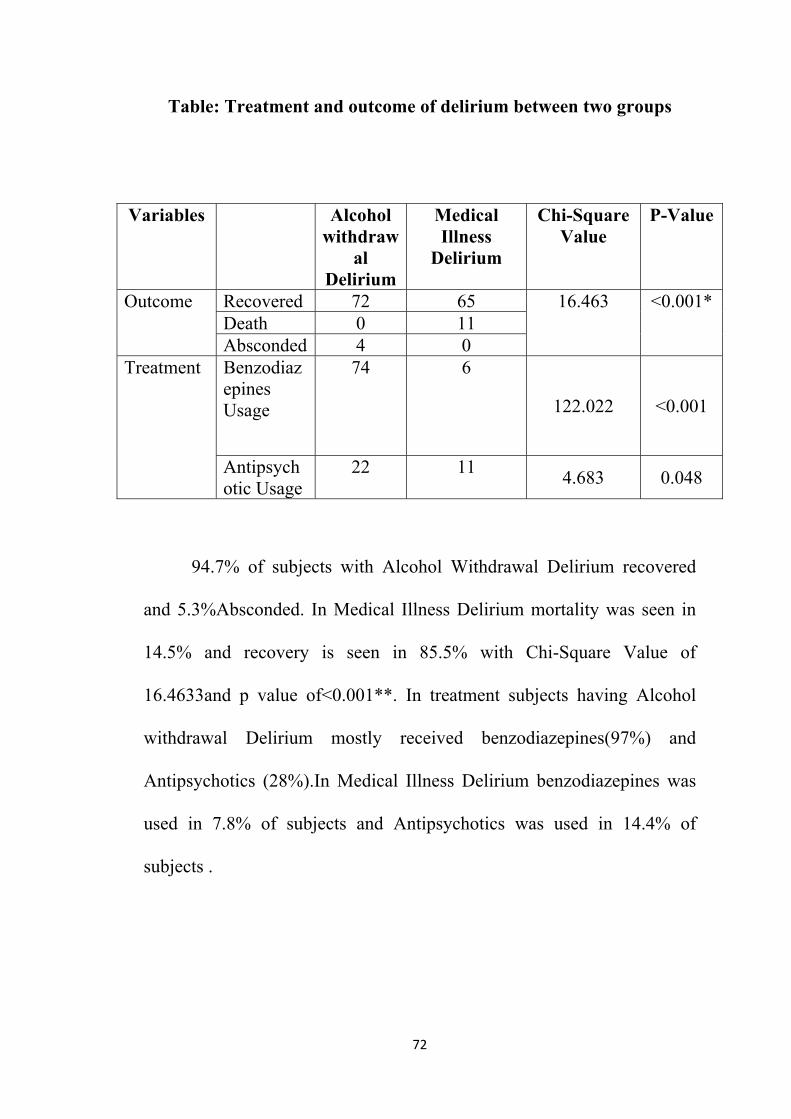
Table: Treatment and outcome of delirium between two groups
94.7% of subjects with Alcohol Withdrawal Delirium recovered
and 5.3%Absconded. In Medical Illness Delirium mortality was seen in
14.5% and recovery is seen in 85.5% with Chi-Square Value of
16.4633and p value of<0.001**. In treatment subjects having Alcohol
withdrawal Delirium mostly received benzodiazepines(97%) and
Antipsychotics (28%).In Medical Illness Delirium benzodiazepines was
used in 7.8% of subjects and Antipsychotics was used in 14.4% of
subjects .
Variables Alcohol withdraw
al Delirium
Medical Illness
Delirium
Chi-Square Value
P-Value
Outcome Recovered 72 65 16.463 <0.001* Death 0 11 Absconded 4 0
Treatment Benzodiazepines Usage
74 6
122.022 <0.001
Antipsychotic Usage
22 11 4.683 0.048

73
Independent Samples Test between Delirium Cause and Total
duration of Hospital
Total
duration of
Hospital
Delirium Cause
t-value P-ValueAlcohol withdrawal
Delirium
Medical
Illness
Delirium
5.50±2.517 11.37±8.230 5.945 <0.001**
Comparing the total duration of mean hospital stay between the
two groups using t –test, hospital stay in medical illness delirium is
11.37±8.230 days and Alcohol withdrawal Delirium is 5.50±2.517 days ,
longer hospital stay is seen with statistical significance (p value
<0.001**) in medical illness delirium.

74
DISCUSSION
The delirium is considered as a neuropsychiatric syndrome that
results from an underlying medical condition or substance
intoxication/withdrawal. This study was one of the few attempts at
examining various descriptive data of delirium and phenomenology of
delirium with both cross sectional and Longitudinal scales such as drs-
98. DRS-98 examine subjects 48 hours apart for three consecutive times
and measure the cognitive defect. With cognitive delirium rating scale
cognitive deficit is measured and compared with DRS-98for
phenomenological differences. Another interesting thing is that very few
studies have looked into the relation between orcompared Alcohol
Withdrawal Delirium and other Medical Illness Delirium as groups.
The mean age of participant in this study is 49, 25.7% of subjects
in this study are above 60, in similar studies (done by Sandeep Grover et
al 2013) the mean age is 44.5(SD: 13.05; range 22–85 years) and subjects
who are above 60years of age is 8%.Subjects who are above 60 years are
found to have episodes of delirium due to medical illness which is
significantly greater than those who have alcohol withdrawal delirium ,
this may be attributed to increased age which is a risk factor as increased
age increases cognitive deficit which predisposes elderly population to

75
develop delirium, this finding is also in line with an another study
Maclullich et al, 2009. Most subjects who have Alcohol withdrawal
Delirium belongs to an younger age group population as substance use is
greater among the younger population.
The male to female ratio is 86: 14. This large difference is noted
as all of the subjects from alcohol withdrawal Delirium (76) are male.
This study is conducted in urban population at a tertiary care center and
majority of subjects belonged to lower middle socioeconomic states
47.4%
The various risk factors were assessed such as history of delirium,
co morbidity illness, seizure, concurrent substance use, family history of
alcohol and psychiatric illness. In subjects who have Alcohol Withdrawal
Delirium, past history of delirium has shown significant differences when
compared to medical illness delirium. Past history of delirium was
considered as a risk factor to develop delirium as delirium cause
cognitive defects which predisposes further multiple episodes in future (
grover et al 2013). The co morbid medical illnesses(such as hypertension,
Diabetes etc) are high and showedsignificantly high correlation to
Medical Illness delirium,which is considered as a predisposer to
Delirium.AFamily history of psychiatric illness in Alcohol withdrawal
76
Delirium was significant and similar finding is seen in Thiercelin N,
Rabiahevallier Z Rusch E ,Et Al 2012.
A comparison of frequency of various symptoms between Alcohol
withdrawal Delirium and Medical Illness delirium was assessed byDRS –
r 98.Alcohol withdrawal Delirium had high prevalence of Perceptual
disturbances and hallucinations, Delusions and Thought process
abnormalities and low prevalence of Motor retardation , Language
disturbances. This finding was similar to Grover et al. However,
frequency of core symptom such as Attention and Orientation was no
different in the both groups of delirium. Hence the core symptoms of
delirium are seen in subject with delirium due to any cause, underlying
etiology may contribute to subtle differences in the symptomatology.
In the delirium etiological check list, the most common factors
apart from alcohol withdrawal are metabolic /endocrine abnormalities
53.9%, followed by Cerebrovascular25%, infection systemic11.8%,
similar finding is seen in previous studies Grover et al. In medical illness
delirium the frequency of pattern motor subtype has been assessed. The
hyperactive type was 48% and hypoactive type was 13.7% and mixed
type was 22.4% which show no statistical significance, to earlier studies
done. The morality rate in this study is 7.2% when compared to gover et
77
al 2012 this value is low, this may be because no mortality was noted in
alcohol withdrawal delirium in our study.
The delirium rating score -98 was used in 3 consecutive session
every two days and the finding suggests early delirium usually presents as
psychomotor disturbances and sleep-wake cycle disturbances, a similar
finding was seen in Fann et al, 2005. Sleep disturbances, emotional
labiality, and orientation difficulties are most persistent symptoms and
these findings were similar with that of Levkoff et al, 1994; McCusker et
al, 2003.When compared between groups the medical illness delirium had
statically significant difference in language symptoms.
Delirium symptoms are categorized into ‘core’ features which
includes disturbances of orientation, memory, attention, sleep-wake
cycle, thought processes, language) and ‘associated’ features that varies
in presentation includes different motoric profiles ,affective disturbances,
psychotic symptoms) (APA, 1999; Trzepacz, 1999). The evaluation of
equivalent cognitive items on the CTD and DRS-R98 have high
correlations (inversely as expected) in spite of one being a cognitive test
measuring current status and the other being a symptom rating scale
assessing behavioral and cognitive symptoms in a 48-hour period.There
was significant positive correlation between cognitive domain (such as
78
orientation, Memory, Comprehension and Vigilance )with that of
psychotic symptoms ( such as Perceptual Disturbance, Delusions) ,it may
be because cognitiveimpairmentcauses misperceptions or
misunderstanding of the external environment or individual’s
susceptibility to psychotic symptoms or as a part of mood disturbances
Francis, 1992.Various studies comparing psychotic symptoms of Acute
confusional state with that of schizophrenia found that in acute
confusional state hallucinations are visual more than auditory and formal
thought disorders which are frequently found are illogicality and poverty
of thinking and thought content disturbances involve themes of
immediate surroundings and circumstances (Cutting, 1987). The
visuospatial ability scores were correlated with disorientation, this may be
reflecting the role that is shared by representative posterior parietal cortex
in both orientation and visuospatial functions (Trzepacz 1999).
Themean morality rate in this study is12.7%, whereas comparing
the mortality rate of Alcohol Withdrawal Delirium and Medical Illness
delirium, the mortality rate in medical illness delirium was 14.4%,this
finding was similar to gover et al 2013. Hypoactive delirium is reported
to have a Poorer Prognosis Lam et al, 2003; Kelly et al, 2001; Olofsson et
al, 1996.The mean duration of delirium was 2 days similar finding was
found in earlier studies gover et al 2013.Alcohol withdrawal group had a
79
mean duration of delirium of2.45±1.171and most of them recovered in
2days as similar to earlier study conducted in India gover et al 2013. On
comparing the both groups there were no significance in total duration of
delirium. The mean total duration of hospital stay is 8 days. There was
significant difference in mean total duration of hospital stay in Medical
Illness group (11.37±8.230) than the Alcohol withdrawal Delirium group
(5.50±2.517) similar finding seen in and reluizmoschetta et al
80
CONCLUSION
In this study, the proportion of medical cause of delirium was
more in the elderly population. No significant differences were found
between the two groups in terms of type of family, socioeconomic status
and gender.
Medical illness delirium was higher than alcohol withdrawal
delirium with increasing age. Statistical significance was found for
subjects with previous history of delirium in alcohol withdrawal delirium
group than in medical illness delirium group. No significant difference
was found not in regards to past history of head injury and past history of
seizures. Alcohol withdrawal delirium group had significant higher
proportion of family history of psychiatric illness compared to the control
group.
In medical illness delirium group the delirium etiology check list
showed metabolic / endocrine abnormalities as the most common cause
and the motor subtype of most of them were hyperactive. When delirium
symptoms severity was compared between the two groups with the DRS
R-98 high prevalence of psychotic symptoms was seen in alcohol
withdrawal delirium and there was no difference in core feature of
delirium. In the longitudinal follow up of every two between two groups
81
with DRS R-98, initial 48 hours is characterized by behavior symptoms
(psychomotor disturbances and disrupted sleep wake cycle) and core
symptoms (attention impairment, orientation difficulties, emotional
labiality). On comparison of cognitive test of delirium and delirium rating
scale, there was positive correlation with cognitive domain and psychotic
domain. The mean duration of delirium was 3 days. The medical illness
delirium group had significant higher mortality rate compared to alcohol
withdrawal delirium. The total duration of hospital stay was found to be
more for medical illness delirium. The medical illness subjects belonged
to a older age group and had poorer prognosis when compared to alcohol
withdrawal group which had a younger population with better recovery.

82
LIMITATION
• Since the study was a hospital based inpatient study, the study
population may not represent less severe cases. Hence less severe
cases could be missed out.
• The investigator was not blinded with diagnosis of the patient and
hence the chance of observer error has to be considered.
• The DRS R98 scale was used in the study population only for a
limited period

BIBLIOGRAPHY
1. A study of symptom profile and clinical subtypes of delirium, David
Meagher MD, DPM, MRCPsych, MSc (Neuroscience), MHSc
(Clinical Teaching) University of Limerick Medical School and
Limerick Mental Health Services
2. Management of Alcohol Withdrawal Delirium ichael F. Mayo-Smith,
MD, MPH; Lee H. Beecher, MD; Timothy L. Fischer, DO; David A.
Gorelick, MD, PhD; Jeanette L. Guillaume, MA; Arnold Hill, MD;
Gail Jara, BA; Chris Kasser, MD; John Melbourne,MD;
3. Symptom Profile and Outcome of Delirium Associated with Alcohol
Withdrawal Syndrome: A Study from India Sandeep Grover, MD,
Akhilesh Sharma, MD, Natasha Kate, MD, Surendra K. Mattoo, MD,
Debasish Basu, MD, Subho Chakrabarti, MD, Savita Malhotra, MD,
Ajit Avasthi, MD
4. The delirium subtypes: A review of prevalence, phenomenology,
pathophysiology, and treatment response DANIELE STAGNO,
M.D.,1 CHRISTOPHER GIBSON, PH.D.,2 AND WILLIAM
BREITBART, M.D.2 1Service de Psychiatrie de Liaison, CHUV-CH-
1011 Lausanne, Switzerland 2Department of Psychiatry and

Behavioral Sciences, Memorial Sloan-Kettering Cancer Center,New
York, New York
5. Delirium: Phenomenologic and Etiologic Subtypes stopher A. Ross,
M.D., Ph.D., Carol E. Peyser, M.D.,ra Shapiro, M.D., and Marshal E
Folstein, M.D. Department of Psychiatry The Johns Hopkins
University School of Medicine Baltimore, Maryland, U.S.A.
6. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the
management of pain, agitation, and delirium in adult patients in the
intensive care unit. Crit Care Med. 2013;41
7. Bellelli G, Frisoni GB, Turco R, Lucchi E, Magnifico F. Delirium
superimposed on dementia predicts 12-month survival in elderly
patients discharged from a postacute rehabilitation facility. J Gerontol
A Biol Sci Med Sci. 2007;62
8. Brown TM. Basic mechanisms in the pathogenesis of delirium. In:
Stoudemire A, Fogel BS, Greenberg DB, eds. The Psychiatric Care of
the Medical Patient. 2nd ed. New York: Oxford University Press;
2000.

9. Camus V, Gonthier R, Dubos G, Schwed P, Simeone I. Etiologic and
outcome profiles in hypoactive and hyperactive subtypes of delirium.
J Geriatr Psychiatry Neurol. 2000;13 Cole M, McCusker J,
Dendukuri N, Han L. The prognostic significance of subsyndromal
delirium in elderly medical inpatients. J Am Geriatr Soc.
2003;51:754–760.
10. Collinsworth AW, Priest EL, Campbell CR, Vasilevskis EE, Masica
AL. A review of multifaceted care approaches for the prevention and
mitigation of delirium in intensive care units. J
Intensive Care Med. 2016;31(2):127–141.11
11. Fang CK, Chen HW, Liu SI, Lin CJ, Tsai LY. Prevalence, detection
and treatment of delirium in terminal cancer inpatients: a prospective
survey. Jpn J Clin Oncol. 2008;
12. Fick D, Foreman M. Consequences of not recognizing delirium
superimposed on dementia in hospitalized elderly individuals. J
Gerontol Nurs. 2000;26:30–40.
13. Gagnon P, Allard P, Mâsse B, DeSerres M. Delirium in terminal
cancer: a prospective study using daily screening, early diagnosis, and
continuous monitoring. J Pain Symptom Manage.2000;19(6):

14. Häussinger D, Schliess F, Kircheis G. Pathogenesis of hepatic
encephalopathy. J Gastroenterol Hepatol. 2002;17 (Suppl 3):
15. Inouye, SK, RDG Westendorp, Saczynski JS. Delirium in elderly
people. Lancet. 2014;383
16. Jackson JC, Gordon SM, Hart RP, Hopkins RO, Ely EW. The
association between delirium and cognitive decline: a review of the
empirical literature. Neuropsychol Rev. 2004;
17. Kalisvaart KJ, de Jonghe JF, Bogaards MJ, Vreeswijk R, Egberts TC.
Haloperidol prophylaxis for elderly hip-surgery patients at risk for
delirium: a randomized placebo-controlled study. J Am Geriatr Soc.
2005;53:.
18. Lawlor PG, Gagnon B, Mancini IL, Pereira JL, Hanson J. Occurrence,
causes, and outcome of delirium in patients with advanced cancer: a
prospective study. Arch Intern Med. 2000;160(6):
19. Levkoff SE, Marcantonio ER. Delirium: a major diagnostic and
therapeutic challenge for clinicians caring for the elderly. Compr Ther.
1994;20:

20. Liptzin B, Levkoff SE. An empirical study of delirium subtypes. Br J
Psychiatry. 1992;161: Marcantonio ER, Flacker JM, Michaels M,
Resnick NM. Delirium is independently associated with poor
functional recovery after hip fracture. J Am Geriatr Soc. 2000;
21. McCusker J, Cole M, Dendukuri N, Belzile E, Primeau F. Delirium in
older medical inpatients and subsequent cognitive and functional
status: a prospective study. Can Med Assoc J. 2001;165:
22. McCusker J, Cole M, Dendukuri N, Han L, Belzile E. The course of
delirium in older medical inpatients: a prospective study. J Gen Intern
Med. 2003;18:.
23. Naughton BJ, Saltzman S, Ramadan F, Chadha N, Priore R. A
multifactorial intervention to reduce prevalence of delirium and
shorten hospital length of stay. J Am Geriatr Soc. 2005;53(1):18–23.
24. Peterson JF, Pun BT, Dittus RS, Thomason JW, Jackson JC. Delirium
and its motoric subtypes: a study of 614 critically ill patients. J Am
Geriatr Soc. 2006;54(3):
25. Ritchie J, Steiner W, Abrahamowicz M. Incidence of and risk factors
for delirium among psychiatric inpatients. Psychiatr Serv.1996;47(7):.

26. Rockwood K. The occurrence and duration of symptoms in elderly
patients with delirium. J Gerontol Med Sci. 1993;48:M162–M166.
27. Rockwood K, Cosway S, Carver D, Jarrett P, Stadnyk K. The risk of
dementia and death after delirium. Age Ageing. 1999;28:.
28. Rockwood K, Cosway S, Stolee P, Kydd D, Carver D. Increasing the
recognition of delirium in elderly patients. J Am Geriatr Soc. 1994;
29. Rudolph JL, Ramlawi B, Kuchel GA, McElhaney JE, Xie D.
Chemokines are associated with delirium after cardiac surgery. J
Gerontol A Biol Sci Med Sci. 2008;
30. Rummans TA, Evans JM, Krahn LE, Fleming KC. Delirium in
elderly patients: evaluation and management. Mayo Clin Proc.
1995;70:989–998.
31. Santana Santos F, Wahlund LO, Varli F, Tadeu Velasco I, Eriksdotter
Jonhagen M. Incidence, clinical features and subtypes of delirium in
elderly patients treated for hip fractures. Dement
Geriatr Cogn Disord. 2005;20(4)

32. Seaman JS, Schillerstrom J, Carroll D, Brown TM. Impaired
oxidative metabolism precipitates delirium: a study of 101 ICU
patients. Psychosomatics. 2006;47:56–61.
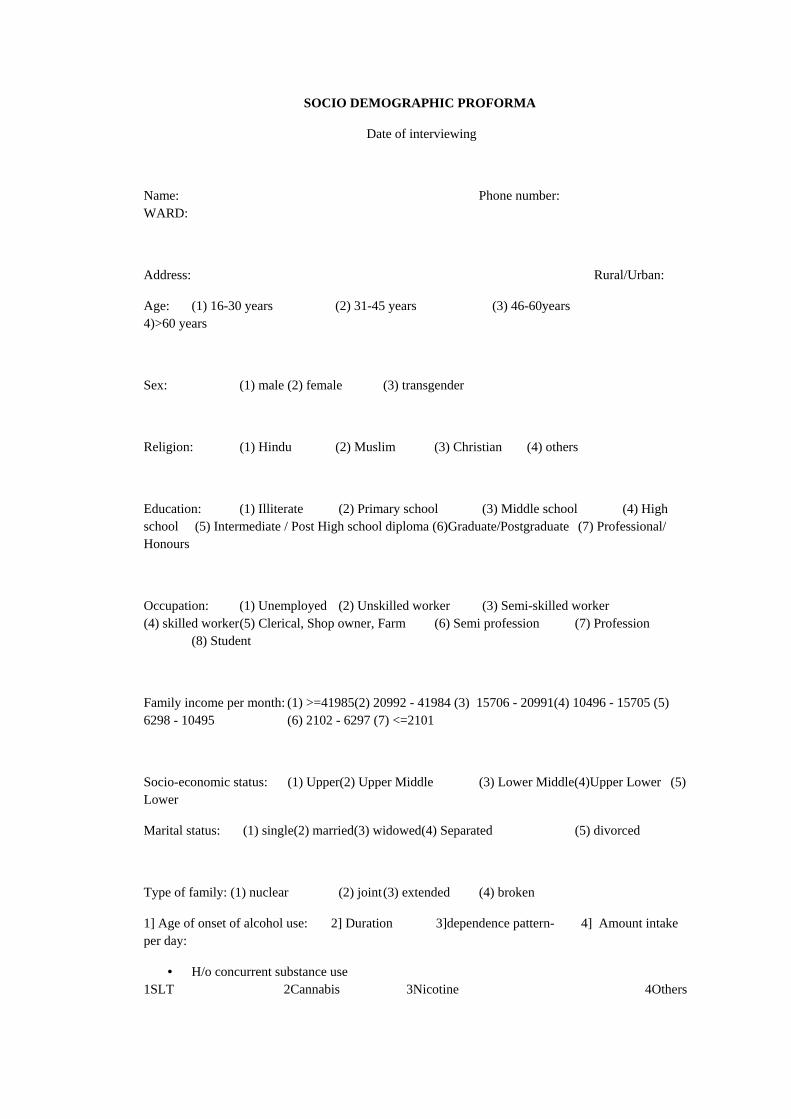
SOCIO DEMOGRAPHIC PROFORMA
Date of interviewing
Name: Phone number: WARD:
Address: Rural/Urban:
Age: (1) 16-30 years (2) 31-45 years (3) 46-60years 4)>60 years
Sex: (1) male (2) female (3) transgender
Religion: (1) Hindu (2) Muslim (3) Christian (4) others
Education: (1) Illiterate (2) Primary school (3) Middle school (4) High school (5) Intermediate / Post High school diploma (6)Graduate/Postgraduate (7) Professional/ Honours
Occupation: (1) Unemployed (2) Unskilled worker (3) Semi-skilled worker (4) skilled worker (5) Clerical, Shop owner, Farm (6) Semi profession (7) Profession (8) Student
Family income per month: (1) >=41985(2) 20992 - 41984 (3) 15706 - 20991(4) 10496 - 15705 (5) 6298 - 10495 (6) 2102 - 6297 (7) <=2101
Socio-economic status: (1) Upper(2) Upper Middle (3) Lower Middle(4)Upper Lower (5) Lower
Marital status: (1) single(2) married(3) widowed(4) Separated (5) divorced
Type of family: (1) nuclear (2) joint (3) extended (4) broken
1] Age of onset of alcohol use: 2] Duration 3]dependence pattern- 4] Amount intake per day:
• H/o concurrent substance use 1SLT 2Cannabis 3Nicotine 4Others

Last use of concurrent substance use:
Previous h/o seizures: Yes/No previous h/o co morbidity medical illness-
Previous h/o head injury: Yes/No duration-
Previous h/o delirium tremens: Yes/No on treatment-
Family h/o Alcohol use disorder: Yes/No
Family h/o psychiatric illness: Yes/No
DAY 1 3 5 7 9 11 13 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
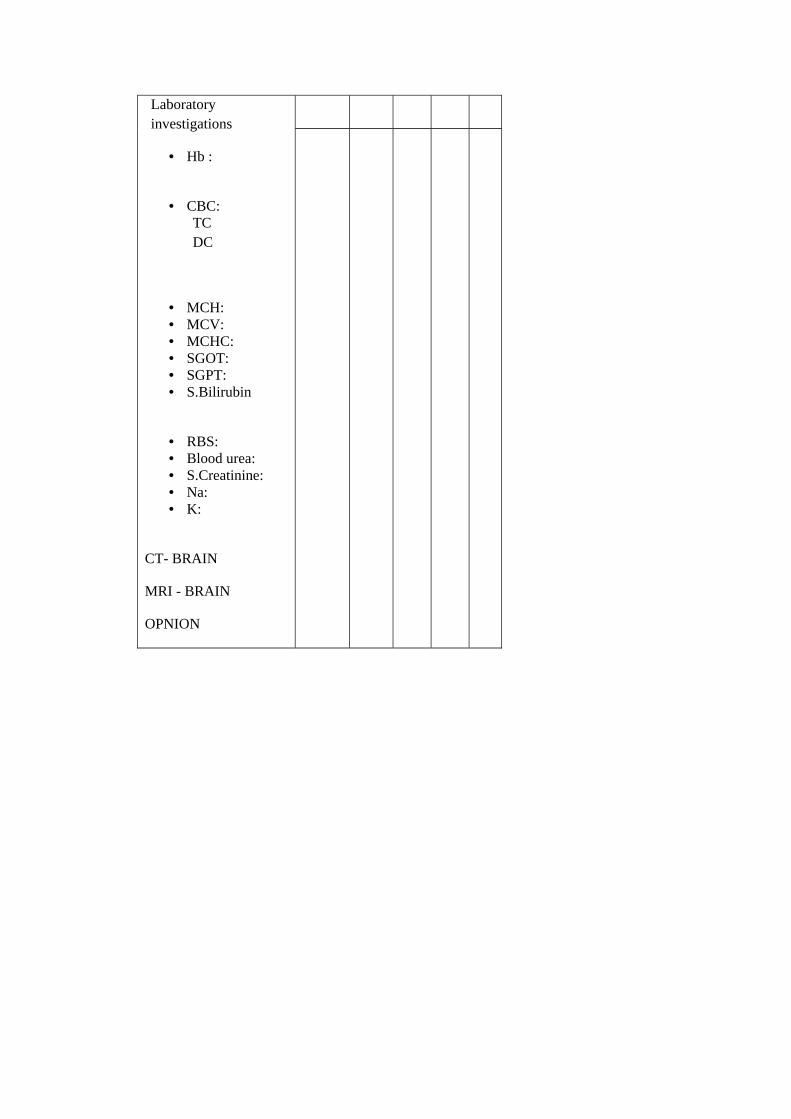
Laboratory investigations
• Hb :
• CBC: TC DC
• MCH: • MCV: • MCHC: • SGOT: • SGPT: • S.Bilirubin
• RBS: • Blood urea: • S.Creatinine: • Na: • K:
CT- BRAIN
MRI - BRAIN
OPNION

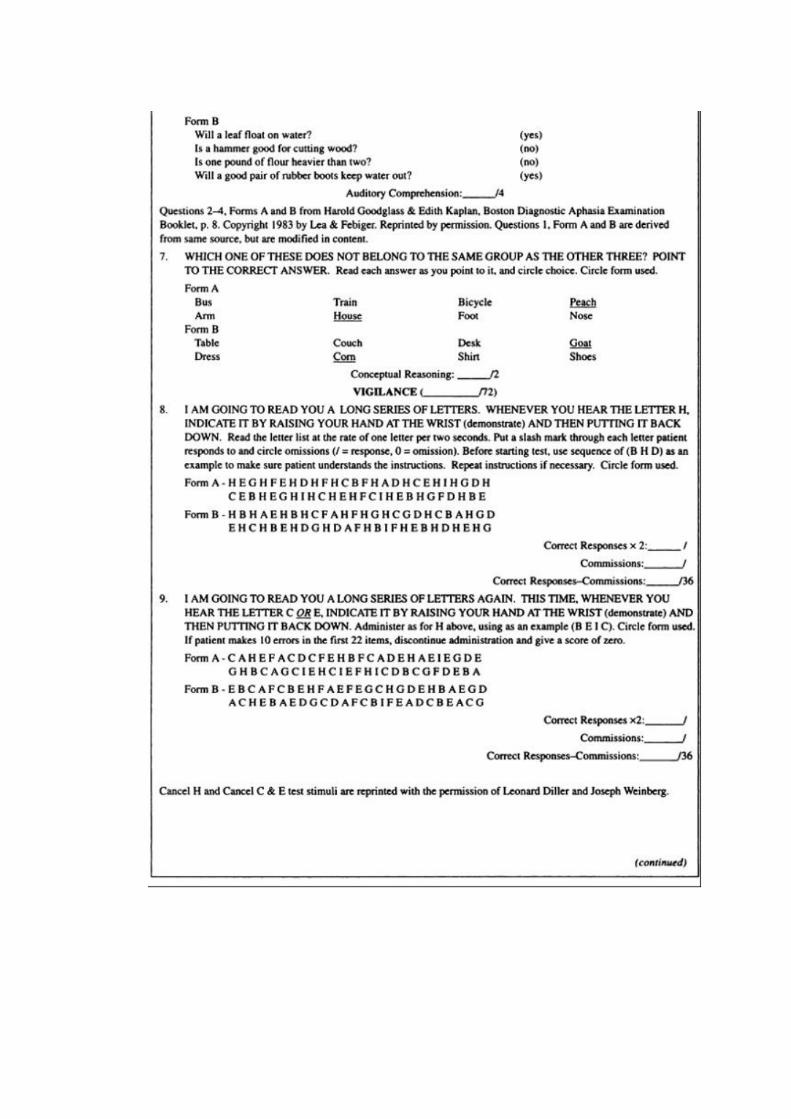
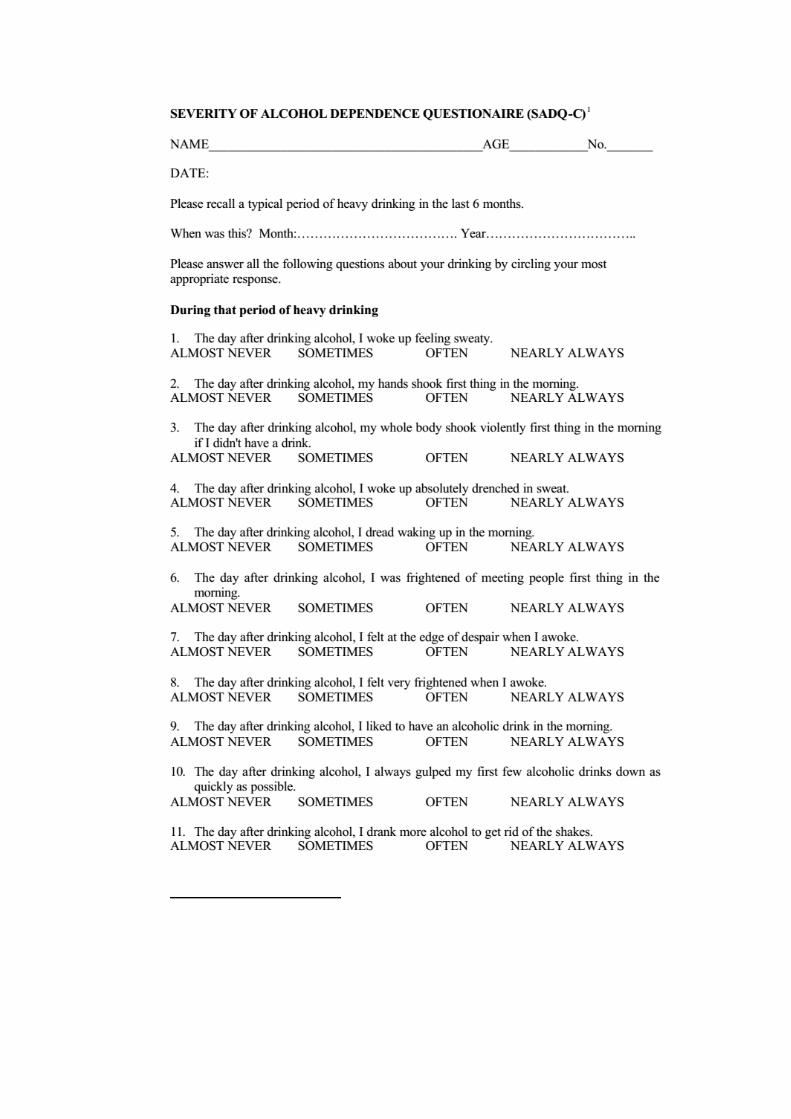

Total duration of delirium- Outcome – recovered/ death /discharge/absconded

Definite cause
4
Likelycause
3
Present and possible
contributor
2
Present but apparently
not contributing
1
Ruled out/not present/not relevant
0
Drug intoxication
Drug withdrawal
Metabolic/endocrine
Traumatic brain injury
Seizures
Infection (intracranial
Infection (systemic)
Neoplasm (intracranial)
Neoplasm (systemic)
Cerebrovascular Organ insufficiency
Other (central nervous system)
Others


INFORMED CONSENT FORM
STUDY: Study on Delirium etiology, clinical profile and outcome”.
STUDY CENTRE: Govt. Kilpauk Medical College Hospital, Chennai.
PATIENT’S NAME :
PATIENT’S AGE :
I.P NO. :
Patient may check ( ) these boxes
I confirm that I understood the purpose of the procedure for the above study.
( )
I had the opportunity to ask question and all my questions and doubts have
been answered to my complete satisfaction. ( )
I understand that my participation in the study is voluntary and that I am free to
withdraw at any time without giving reason, without my legal rights being
affected. ( )
I understand that the ethical committee members and the regulatory authorities
will not need my permission to look at my health records, both in respect of the
current study and any further research that may be conducted in relation to it,
even if I withdraw from the study I agree to this access.
( )
However, I understand that my identity will not be revealed in any information
released to third parties or published, unless as required under the law.
( )
I agree not to restrict the use of any data or results that arise from the study.
( )
I agree to take part in the above study and to comply with the instructions given
during the study and faithfully co-operate with the study team and to
immediately inform the study staff if I suffer from any deterioration in my
health or well being or any unexpected or unusual symptoms. ( )
I hereby consent to participate in this study. ( )
I hereby give permission to undergo complete clinical examination and
diagnostic tests including haematological, biochemical, radiological tests.
( )
Signature / thumb impression
Patient’s name and address:
Place:
Date:
Signature of the investigator:
Study investigator’s name:
Place:
PARTICIPANTS' INFORMATION SHEET
Investigator : Dr. C.J. Dhiinesh,
Name of the participant :
Study title: “Study on delirium etiology, clinical profile and outcome”.
You are invited to take part in this research study. We have got approval
from the IEC. You are asked to participate because you satisfy the eligibility
criteria.
What is the purpose of this research?
In this study, we aim to assess symptom profile and course of alcohol
withdrawal – delirium and other medical illness – delirium. To
compare clinical profile of delirium associated with alcohol withdrawal
Vs other medical illness - its, course of illness & outcome. To assess
the correlation of cognitive status and psychotic symptom
Benefits:
This study will benefit all people who are undergoing treatment for –
delirium and help improve the success rate of treatment, and also improves
their quality of life.
Discomforts and risks:
No interventional procedure is done in this study.

Confidentiality:
Patients who participate in the study and their details will be maintained
confidentially and at any cost, those details will not be let out.
Right to withdraw:
Patients will not be forced to complete the study. At any cost, in such
circumstances the treatment will not be compromised.
Signature/Thumb impression of the participant:
Signature of the investigator:
Date :
Place:

சுய ஒப்புதல் படிவம்
ஆய்வு ெசய்யப்படும் தைலப்பு:
"டிலிrயம் எேயாலாலஜி, மருத்துவ சுயவிவரம் மற்றும் விைளவு
பற்றிய ஆய்வு".
ஆராய்ச்சி நிைலயம்: கீழ்ப்பாக்கம் மருத்துவக்கல்லூr அரசு
மருத்துவமைன, ெசன்ைன.
பங்கு ெபறுபவrன் ெபய :
உறவு முைற:
பங்கு ெபறுபவrன் எண்:
பங்கு ெபறுபவ இதைன ( ) குறிக்கவும்
ேமேல குறிப்பிட்டுள்ள மருத்துவ ஆய்வின் விவரங்கள் எனக்கு
விளக்கப்பட்டது. என்னுைடய சந்ேதகங்கைளக் ேகட்கவும்,
அதற்கான தகுந்த விளக்கங்கைளப் ெபறவும் வாய்ப்பளிக்கப்பட்டது.
( )
நான் இவ்வாய்வில் தன்னிச்ைசயாகத்தான் பங்ேகற்கிேறன். எந்தக்
காரணத்தினாேலா எந்தக் கட்டத்திலும் எந்த சட்ட சிக்கலுக்கும்
உட்படாமல் நான் இவ்வாய்வில் இருந்து விலகிக் ெகாள்ளலாம்
என்றும் அறிந்து ெகாண்ேடன். ( )
இந்த ஆய்வு சம்மந்தமாகவும், ேமலும் இது சா ந்த ஆய்வு
ேமற்ெகாள்ளும்ேபாதும், இந்த ஆய்வில் பங்குெபறும் மருத்துவ
என்னுைடய மருத்துவ அறிக்ைககைளப் பா ப்பதற்கு என் அனுமதி
ேதைவயில்ைல என அறிந்துெகாள்கிேறன். நான் ஆய்வில் இருந்து
விலகிக் ெகாண்டாலும் இது ெபாருந்தும் என அறிகிேறன். ( )
இந்த ஆய்வின் மூலம் கிைடக்கும் தகவல்கைளயும், பrேசாதைன
முடிவுகைளயும் மற்றும் சிகிச்ைச ெதாட பான தகவல்கைளயும்

மருத்துவ ேமற்ெகாள்ளும் ஆய்வில் பயன்படுத்திக் ெகாள்ளவும்,
அைதப் பிரசுrக்கவும் என் முழு மனதுடன் சம்மதிக்கிேறன். ( )
இந்த ஆய்வில் பங்கு ெகாள்ள ஒப்புக்ெகாள்கிேறன். எனக்குக்
ெகாடுக்கப்பட்ட அறிவுைரகளின் படி நடந்துெகாள்வதுடன், இந்த
ஆய்ைவ ேமற்ெகாள்ளும் மருத்துவ அணிக்கு உண்ைமயுடன்
இருப்ேபன் என்றும் உறுதியளிக்கிேறன். என் உடல் நலம்
பாதிக்கப்பட்டாேலா அல்லது எதி பாராத வழக்கத்திற்கு மாறாக
ேநாய்க்குறி ெதன்பட்டாேலா உடேன அைத மருத்துவ அணியிடம்
ெதrவிப்ேபன் என உறுதி அளிக்கிேறன். ( )
இந்த ஆய்வில் எனக்கு மருத்துவப் பrேசாதைன ெசய்து ெகாள்ள
மற்றும் ஆய்வில் பங்ேகற்க நான் முழு மனதுடன் சம்மதிக்கிேறன்.
( )
பங்ேகற்பவrன் ைகெயாப்பம் / கட்ைடவிரல் ேரைக:
இடம்: ____________________________
ேததி: _____________________________
பங்ேகற்பவrன் ெபய மற்றும் விலாசம்::
ஆய்வாளrன் ைகெயாப்பம் _________________________
இடம் _________________________
ேததி __________________________
ஆய்வாளrன் ெபய ____________________________
ஆராய்ச்சி தகவல் தாள்
கீழ்பாக்கம் அரசு ெபாது மருத்துவமைனயில் டிலிrயம்
எேயாலாலஜி, மருத்துவ சுயவிவரம் மற்றும் விைளவு பற்றிய
ஆய்வு
பங்ேகற்க நாங்கள் விரும்புகிேறாம். இந்த ஆராய்ச்சியில்
பங்ேகற்பதால் தங்களது ேநாயின் ஆய்வறிக்ைகேயா அல்லது
சிகிச்ைசேயா பாதிக்கப்படாது என்பைதயும் ெதrவித்துக்
ெகாள்கிேறாம்.
இந்த ஆராய்ச்சியின் முடிவுகைள அல்லது கருத்துகைள
ெவளியிடும் ேபாேதா அல்லது ஆராய்ச்சியின் ேபாேதா தங்களது
ெபயைரேயா அல்லது அைடயாளங்கைளேயா ெவளியிடமாட்ேடாம்
என்பைதயும் ெதrவித்துக் ெகாள்கிேறாம்.
இந்த ஆராய்ச்சியில் பங்ேகற்பது தங்களுைடய விருப்பத்தின்
ேபrல் தான் இருக்கிறது. ேமலும் நங்கள் எந்ேநரமும் இந்த
ஆராய்ச்சியில் இருந்து பின்வாங்கலாம் என்பைதயும்
ெதrவித்துக்ெகாள்கிேறாம்.
இந்த சிறப்புப் பrேசாதைனகளின் முடிவுகைள ஆராய்ச்சியின்
ேபாேதா அல்லது ஆராய்ச்சியின் முடிவின் ேபாேதா தங்களுக்கு
அறிவிப்ேபாம் என்பைதயும் ெதrவித்துக்ேகாள்கிேறாம்.
ஆராய்ச்சியாள ைகெயாப்பம் பங்ேகற்பாள ைகெயாப்பம்
ேததி: