students with tbi: who and where are they? what are the effects of tbi? what do they need?
TRANSCRIPT

Students with TBI: Who and Where are They? What are the Effects of TBI? What Do They Need?

The Brain
About 3.5 pounds Consistency of 3 day-old Jello Bony, bumpy case surrounded by less than ¼ cup
of spinal fluid 10 billion neurons
Each neuron connects with others average of 10,000 synapses

Brain Injury
Congenital Brain InjuryPre-birth or during birth
Acquired Brain InjuryAfter birth process
Traumatic Brain Injury(TBI)
Closed Head Injury• Concussion
• Swelling results in further (secondary) injury
• No loss of consciousness • Damage great or greater than
open brain injury
Open Head Injury• Skull is fractured
• Blood & swelling have a place to go

Shearing strainsthroughout thebrain
Subdural veinstorn as brainrotates forward
Swelling ofbrain stem
Damage totemporal lobesfrom roughbones at skull base
Compressionfracture
Types of Damage
in a Closed Head Injury

Coup
Contra-coup

Skull Protrusions
Adapted From: Pang, 1985Skull
Shearing Plane
Brain
Protrusion

Overly Simplified Brain Behavior Relationships
Frontal Lobe
Parietal Lobe
Occipital Lobe
Temporal Lobe
Cerebellum
Brain Stem
Parietal Lobe• Sense of touch• Differentiation: size, shape, color• Spatial perception• Visual perception
Occipital Lobe• Vision
Cerebellum• Balance• Coordination• Skilled motor activity
Frontal Lobe• Initiation• Problem solving• Judgment• Inhibition of behavior• Planning/anticipation• Self-monitoring• Motor planning• Personality/emotions• Awareness of abilities/limitations• Organization• Attention/concentration• Mental flexibility• Speaking (expressive language)
Brain Stem• Breathing• Heart rate• Arousal/consciousness• Sleep/wake functions• Attention/concentration
Temporal Lobe• Memory• Hearing• Understanding language (receptive language)• Organization and sequencing
What’s Different about TBI?
· No two brain injuries are exactly the same.
· Brain injury is complex and varies greatly from person to person.
· Cause, location and severity of injury determine the effects.
· Long-term effects are not always apparent and may present as cognitive and environmental demands increase.
· Attainment of developmental milestones may be effected by a past injury.
· Commonly results in functional deficits that may be identified in another disability category(ies)

Causes of TBI in Children
Motor Vehicle Crashes High Risk Sports ATVs, rodeo, skiing, snow boarding
Motorcycle incidents Pedestrian vehicle incidents Violence Falls Abuse
Shaking

TBI in Children
1.4 million children injured annually Highest risk groups ages 0-4 and 15-19 More likely to survive than adults Less likely to lose consciousness 1/50 kids have had a concussion

Scope of the Problem: Oregon
Approximately 1000 children hospitalized
annually in Oregon
More than 1/3 experience persisting functional
limitations
Expected yield = approx 3,000-4,000 identified
Just over 300 identified for SPED under TBI in
Oregon
Just 50 in NWRESD service area

Why Don’t We Find Them?
• Lack of medical training and referral• Lack of educational training and awareness• Lack of parental recognition• Many “look good” physically• Developmental bias that they will be OK
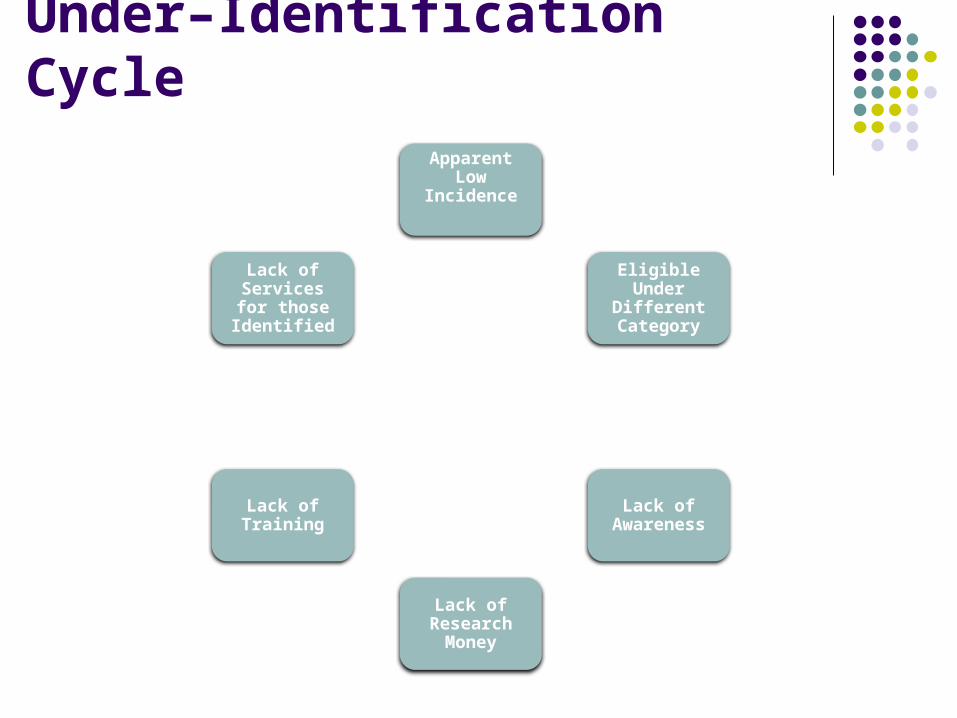
Apparent Low Incidence
Eligible Under Different Category
Lack of Awareness
Lack of Research
Money
Lack of Training
Lack of Services for
those Identified
Under–Identification Cycle

Special Educational Definition of TBI
…an acquired injury to the brain caused by an external physical force, resulting in total or partial functional disability or psychosocial impairment, or both, that adversely affects a child’s educational performance. The term applies to open or closed head injuries resulting in impairments in one or more areas, such as cognition; language; memory; attention; reasoning; abstract thinking; judgment; problem-solving; sensory, perceptual, and motor abilities; psychosocial behavior; physical functions; information processing; and speech. The term does not apply to brain injuries that are congenital or degenerative, or to brain injuries induced by birth trauma.

Sequence of Skill Recovery Motor
Gross motor functioning (1 to 2 months) Sensory
Improves relatively rapidly in children (1 to 2 months) Speech Communication skills
Expressive speech may resolve within a few months, Subtle language problems may persist indefinitely
Measured IQ May be small changes Not as rapid as motor, sensory and speech functions
Memory, Attention, Processing speed May lag for many months or be forever reduced Higher Level Cognition
Information processing Learning under new, complex or difficult situations Ability to adapt to new problems or situations. Children negatively affected by stress more easily than before. May be impacted for years or permanently

2 Years After Injury….
Memory problems (74%) Fatigue (72%) Word-Finding difficulties (67%) Irritability (67%) Impaired Speed of Thinking (64%) Impaired Concentration (62%)
(Ponsford, 1995)
Depressed Mood 40-50% of people with TBI
(Glenn, 2001)

Pet Scans – New Learning
Everything lights up with new learning
Pathways rewire Pathways are created
through repetition Eventually, learning
results in more efficiency
Tend to encode Irrelevant Information

Residual Cognitive Deficits
Disorders of Attention – easily fatigued, impaired shifting, impaired maintenance, impaired selection
Disorders of Memory – poor rote, short term difficulties, storage and retrieval difficulties, prospective memory problems (remembering to remember)
Disorders of Planning – slowed initiation, disinhibition, poor at abstraction, poor sequencing, doesn’t learn from mistakes, doesn’t ask for help, can’t get started

Residual Cognitive Deficits
Disorders of Judgment – misinterprets actions of others, can’t handle multiple bits of information at once, socially unacceptable physical and verbal behaviors, little self awareness of strengths and weaknesses
Disorders of Information Processing Speed – extreme slowness in reaction time, slowed psychomotor activities – writing, talking, etc.
Disorders of Communication – anomia, inefficient word retrieval, hyperverbal, peculiar use of words and phrases, uninhibited word choice
Roberta DePompei, 2009

Observed Behaviors Underlying Problems
Daydreams, pesters peers, fiddles with materials
Blurts out, interrupts, tangential speech
Poor test-taker, inconsistent memory of information
Needs multiple repetitions of directions, acts rude, doodles, bolts
Misunderstands humor, puns, double meanings
Impaired attention, perception, memory
Inflexibility, impulsivity, disorganized thinking
Inefficient storage and/or retrieval of information
Inefficient processing of info: rate, amount, complexity
Difficulty processing abstract information

Observed Behaviors Underlying Problems
Can’t learn new games, decision rules, changes in targeted task
Temper tantrums, sticks with one solution, won’t change mind
Poor social interactions, foul language, hot temper
Lack of awareness, poor task completion, trouble with change
Inflexibility, poor working and short term memory, poor “shifting” (multitask)
Ineffective problem solving and judgment, Limbic dysregulation
Poor judgment, lack of self-awareness, language deficits
Impaired “executive”skills

INTERVENTIONS – What do they need?
0-21

Physical Challenges

EXECUTIVE FUNCTIONS
• Difficulty holding instructions/Information
• New learning is most difficult• Difficulty with multiple cognitive
demands (writing)
• Metacognition• Goal-Directed activity• Problem solving for attainment of
future goal• Inability to form Mental
representations & interpretations
• Difficulty with multi-Step tasks• Engaging in independent tasks• Organizational difficulties
• Inhibition• Rigidity/Inflexibility• Sustained Energy• Poor monitoring and awareness
of behavior• Frequent distractions
Self Regulation
Planning
MemoryStrategic Learning

Memory Interventions Repeat often and summarize Have child paraphrase, doodle, condense for encoding Carry assignment sheet for each class Closed-ended tasks (fill-in vs. essay) Categorize or “chunk” information Use visualization Link new information to prior knowledge Give examples with instruction Discrete task objectives (Vocabulary) Rehearsal (often doesn’t work real well) Visual interventions such “Inspiration” Software Auditory interventions such as tape recorder, books on
tape

Self Regulation Reduce distractions in work area Make tasks shorter Behavior contract Divide work into smaller segments Use cues (words, sounds, tactile) to alert person to pay
attention Build in choice Increase joyfulness, high interest and relationship Ignore dis-inhibited response Incentive Systems Keep tools and materials available Keep it structured Allow for frequent breaks

Slow processing speed

Processing Speed Strategies
The Wright Family Story! Give more time to complete requested tasks Slow pace of Instruction Note taker Condense tasks Music Use Scaffolding and Modeling

Strategic Learning Strategies Prompts and reminders Provide scoring rubric Have child provide a written plan Break down tasks and timelines (note cards) Coaching Structured teaching Re-teach affect and social clues Flexible performance options Visual and written instructions High degree of tactile reinforcers Teach Note Methods SQ3R (Survey, question, read, write, review)

Concrete ThinkingDifficulty with abstraction, synthesis, inference etc.

Planning Interventions Draw maps, use lists, timelines, visual schedules Goal Setting Color-code materials, information (definition vs.
main idea Electronic organizers Preview completed assignment Answer – “How will I know when I am done?” Establish Routines Use paraphrasing, re-teaching, reciprocal
coaching Meet at beginning and end of day Post-activity reflection

Self-Regulation and Behavior
Goal
Obstacle
Plan
Predict
Do
Review

Template PromptsPlan-Do-Review
Goal “What do you need to do?” “What are we here for?” “What will it look like when it’s finished?”
Obstacle “What stands or might stand in the way of accomplishing the goal?”
Plan “What will you do first, second, third, etc?” Student makes prediction about success of plan “Will it
be hard or easy?” Is it scary or not scary?”“Will it take an hour or take 6 hours?” “Is it a choice or not a choice?”
Do “Let me know if you need any help.”
Review “How did that work out?” “What would you do differently?” “Do you think you met your goal?”

Behavioral Interventions(Very Common)
Conduct a FBA Give very clear written and verbal guidelines
Big 5 When to start What to do How much to do What finished looks like What to do next
Coach to assist with misperceptions Implement Positive Behavior Supports

Self
Regulation
Executive
Functioning
Communication Skills
We must teach and support the underlying processes to get to self-regulationR. DePompei 2009

What Can You Do?
Remember that TBI is vastly under identified When you see unexplained behaviors or
learning characteristics….suspect! Ask! “Has your child ever had a blow to the
head or a concussion?” Add the question to medical cards Visit some of the great websites available

NWRESD TBI Educational Consulting Team
Laura Bekken [email protected] 503-614-1683
Cindy Hodges [email protected] 503-614-1670
Kristy Young [email protected] 503-614-1672

Oregon Brain Injury Resources
http://www.tr.wou.edu/tbi Resource librarian (Laura Beck) is available to
find specific information for your particular request regarding TBI
http://www.tbied.org• TBI Educator website from Teaching Research
Institute is very dense with information, resources, forms, training opportunities

Websites of Interest
http://www.bianys.org/learnet/ - LearnNet – excellent resource for educators and parents
http://www.schoolbehavior.com/conditions_edfoverview.htm
http://www.braininjurypartners.com/login/?next=/ especially for parents-Username=wear your Password=helmet
www.cde.state.co.us/cdesped -Enter “TBI manual” in search for excellent educator’s manual on TBI

QUESTIONS/COMMENTS