studies cerebrospinalfluidcirculation in tuberculous …
TRANSCRIPT

STUDIES OF THE CEREBROSPINAL FLUID CIRCULATIONIN TUBERCULOUS MENINGITS IN CHILDREN
PART HI. A REVIEW OF 100 PNEUMOENCEPHALOGRAMSBY
JOHN LORBERFrom the Department of Child Health, University of Sheffield
(RECEIVED FOR PUBLICATION OCTOBER 27, 1950)
Since the introduction by Dandy of the techniqueof ventriculography (1918) and encephalography(1919) their use has become an indispensable partof neurological investigations. No mention wasmade of their use in tuberculous meningitis until1927 when Eckstein reported on the examination of20 children suffering from this disease. He foundvarying degrees of hydrocephalus and presumed thatthis was inevitable in tuberculous meningitis. Hisview accorded with the usual necropsy findings andthereafter little further work was carried out untilthe advent of streptomycin. Since then manyreferences have been made to air studies in thisdisease. Hydrocephalus was frequently found andits causes were analysed by Cairns (1949). In spiteof the extensive work on various aspects of tuber-culous meningitis treated with streptomycin, onlytwo detailed reports were found on encephalographyin presumably unselected groups of cases (Murano,1948: Schonenberg, 1950).
Present InvestigationMaterial. This investigation began in September,
1948. At first air studies were only carried out forspecial reasons. The investigation was soonextended when increasing experience suggested thatthe procedures were safe and that more could belearnt by systematic and repeated examinations.Between January, 1949, and August, 1950, at leastone pneumoencephalogram* has been performed onall but two patients treated for tuberculous menin-gitis. The two patients excluded were moribundon admission and died within a few days. Noexaminations were carried out in four other patientsadmitted in the latter half of 1948. Three of thesedied, and one recovered without any complications.With the exception of these six cases, the presentseries is consecutive and unselected. Five children
* This term swill be used for both encephalograms and ventriculo-grams, unless others-ise stated.
28
treated at the same hospital but not under our owncare were also investigated.
This study reports the results of the first 100examinationst on 58 children aged between 5 monthsand 12 years. Tuberculous meningitis was bacterio-logically confirmed in 57. The exception was aone-year-old tuberculin positive child of tuberculousparents, who showed the radiological appearancesof a primary tuberculous lung complex. Thecerebrospinal fluid was characteristic and after22 months was still slightly abnormal, the childhaving recovered apart from a residual hemiparesis.
Objects of the Investigation. The long termobjects of this investigation were: (I) a morecomplete understanding of the circulation of thecerebrospinal fluid in tuberculous meningitis;(2) the determination of the incidence and the sitesof obstruction within the ventricular system and thesubarachnoid cisterns; (3) the determination of theincidence, degree, permanency, and causes ofhydrocephalus; (4) the establishment of criteria ofprognosis on the basis of encephalographic findings;(5) the correlation of encephalographic patternswith subsequent physical and mental development;and (6) possibly the finding of definite criteria forthe selection of suitable cases for treatment, andconversely, for the abandonment of treatment onhumanitarian grounds.
Methods. All encephalograms were performedunder rectal thiopentone anaesthesia (Lorber, 1950a).Air was injected by the lumbar route in all cases,except where spinal block necessitated the cisternalroute. Approximately two-thirds to three-quartersof the fluid removed was replaced by air, 20 to 80 ml.being injected while the child was in the sittingposition. An attempt was made to introduce airinto the ventricles as well as the subarachnoid spacesby appropriate positioning of the head (Brain. 1947).
+ 89 encephalograms and 11 ventriculograms.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

FIG. I a.
Much information may be obtained by the injectionof as little as 5 to 10 ml. of air, if the films are takenin the erect position. This method was employedby Flesch and Gefferth (1949) on a large number ofcases. This volume of air can be injected after a
routine therapeutic puncture without any prepara-
tion. This method was used only as an intermediatestep in the present investigation. Figs. I and laillustrate the result of one such examination.Encephalography was preferred to ventriculo-
graphy because the former will usually, at the same
time, outline the ventricular system as well as thesubarachnoid space, and it is easier to detect blocksin any situation by that technique (Davidoff andDyke, 1946a). Ventriculography was done if theventricles failed to fill due to obstruction of thepathways, or if encephalography was contra-indicated by papilloedema.The whole procedure was carried out in the x-ray
department. Pilot films were taken during theinjection of air to guide the positioning of the headand the assessmnt of the volume of air to beinjected. The final radiographs of the skull weretaken in four standard positions: antero-posteriorand lateral with the patient horizontal and erect
respectively. Additional views were taken if thefilms suggested special features requiring elucidation.The radiographs were interpreted by the standards
of Caffey (1945) and Davidoff and Dyke (1946).An encephalogram was judged to be normal if theventricular system filled well, showed no signs ofdilatation, and if air was obviously present in thesubarachnoid spaces (Figs. 2, 2a, and 3, 3a).Dilatation of the ventricles was diagnosed if the sizeof the ventricles exceeded the limits given byDavidoff and Dyke.
After-effects. These procedures were found tobe safe. With one exception no serious after-effectswere noted. One infant had been unconscious forthree and a half months before ventriculographywhich disclosed extreme hydrocephalus (Fig. 4, 4a).He died within 24 hours of the examination. Hisdeath may have been accelerated.Pneumoencephalography was well tolerated by
most childeren, especialy if they spent three hoursin an oxygen tent following the examination. Thisprocedure has been shown to hasten the absorptionof the injected air (Fine, Frehling, and Starr, 1935;Kornreich, 1948; Schwab, Fine, and Mixter, 1937).The children had often no memory of the examina-tion and were found sitting up and playing six orseven hours after it. Moderate headache and somevomiting for 24 hours was, however, fairly frequent.Air must be removed if symptoms of excessivepressure should supervene. The after-effects wereproportionately milder when the volume of injectedair was less. This was also noted by Davidoff andDyke (1946b).
It has been suggested that pneumoencephalo-graphy may precipitate a relapse of the menigitis(MacCarthy and Mann, 1950). The probablefallacy of this statement was pointed out elsewhere(Lorber, 1950b). In none of the present series wasthere clinical or other evidence of relapse withintwo months of the examination. It is as well toremember, however, that the introduction of air mayprovoke a considerable cellular reaction even inpatients whose cerebrospinal fluid was normal atthe beginning of the injection. This pleocytosismay occasionally reach several thousand cells butwill usually subside within eight days (Cestan andRiser, 1924; Eley and Vogt, 1932; Hermann, 1922;Kryspin-Exner, 1932; Merritt and Fremont-Smith,1937; Schwab and von Storch, 1937; Thurzo andNagy, 1923; and Tschugunoff, 1929). The increasein the cell count starts immeitely after the injectionof air. In one of the present series of cases separateexamination of each 5 ml. specimen of fluid duringthe course of an encephalogram showed a tenfoldincrease in the cell count. A mere rise in cell countfollowing pneumoencephalography should not be
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

FIG. }.
FiGs. 2 and Za.-Normal enceph-alogram from acase of tuber-culous meningitis32 sweeks afterthe beginning oftreatment show-ing normal sizedlateral ventricles(1), air in the sub-arachnoid space(6). and the sella
(13).
FIG. 2a.
FIG. 4a.
FIG. 4.Fs. 4 and 4a.-Ventriculor showing extrenc dilatation of thelateral vntricles (1), gss widening ofthe sutus (I1), and air trappodin the basal cistern (7) behind the seila (13), and in the posteriorfosa (9). The chd ded wihi 24 hourns of the Cxamiati_
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

Fms 6 and 6-Lateral view of Figs. 12 and 12a, showing dilatationof all parts ofthe venrsicular system; the laeral ventricles (1), foranof Momo (2), third ventricls (3), Sylvian aqueduct (4), and fourthventricle (5). The sutue ar widened (11) and therc is no sub-arachnoid air. Air distends the cistei maxna (9), but there is nobubbJe of air behind the sells (13), indicating obstrution in the basa
csterns.
uasai us I) oen;m tu seuTs(13). No subarachnoid air.
FIG. 6ak
F}G. 7 and 7a.-Encephalogram (AP)-oin probable
block at the tentorialopeniag- The lateralventricls (1) aregrosy dilated, thesutire lmes (I1) arewidened. Subduralair is seen under thetentorium (8) andalong the fatx (10).No subarachnoid air.
Fc;. 7a.
FIG. 5a.
-cephalograthe tentorialal ventriclesc is air in theand a large
the distended
_
F}G. 7.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from
taken therefore as an indication of relapse in theabsence of other evidence.
Re-Ids. The results of the present investigationare ied in two groups according to theradiological findings. In the first group are thosechildren in whom the examination disclosed normalconditions, and in the second those in whom theappearances wer abnormal. As six ofa consecutiveseries of 64 cases were not investigated, the propor-tion of normal to abnormal findings is probablyslightly distorted, because in five of the six omittedcases, the appearances would probably have beenabnormal.
Group I: Cien wi Norma Radiolgical
Twenty-eight, or nearly half the children belongedto Group I. In 11 of them only one examinationwas carried out, and in eight of these was performedeither late in the course of treatment or aftertreatment had been concluded, at an average of33 weeks after the first steptomycin injection. Allthese children were in good clinical condition atthat time.The examinations were repeated two to four times
in 17 of the 28 children whose initial encephalogramwas normal. In 15 of these 17 the initial examina-tion was carried out at an average of 2 -3 weeks afterthe start of treatment when streptomycin had alreadyhad an opportunity to effect some improvement.The subsequent examinations were carried out
either for clinical reasons (unfavourable progress,convulsions, relapse) or to assess the condition
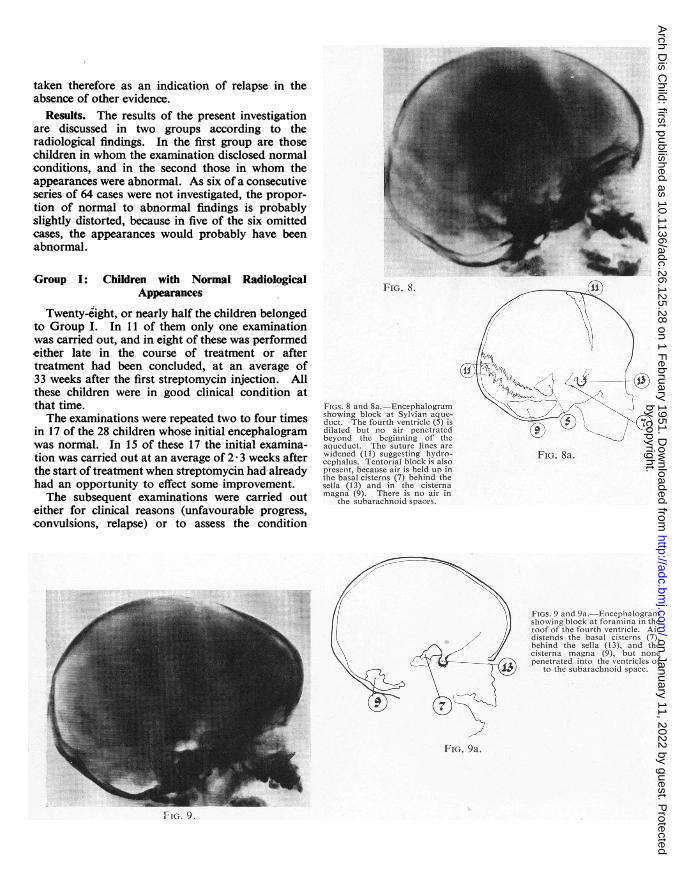
FIGs. 8 and 8ashowing blociduct. The foidilated but inbeyond theaaueduct. The sutur lines arewidened (I1) suggesting hydro-cephalus. Tentorial block is alsopresent, because air is held up inthe basal cisterns (7) behind thesella (13) and in the cisternamagna (9). There is no air in
the subarachnoid spaces.
FIG. 8a.
FK;. 9 and 9a.-Encephalogimshowmg block at foramma inroof of the fourth vanticie rdistends the basal cisterns (7).behind the sella (13), and theciterna maga (9) but n&epenetraed into the ventricks or
to the subarachnoid space.
FIG. 9a.
116. ~~~~~~~~~~~~~~~. 4~~~~~~~r1G. V.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

CEREBROSPINVAL FLUID CIRCULATION IN MENINGITIS: HI
towards the end of the proposed course of treat-ment. In 11 children the appearances remainednormal after an average interval of 18 weeksbetween the first and last examinations. In six otherchildren pathological changes appeared at thesecond or a later examination. This leaves altogether22 children with normal encephalographic appear-ances. in 18 of whom they were found between fourand 14 months after the beginning of treatment.Hydrocephalus is thus by no means an essentialpathological feature of tuberculous meningitis.
Group II: Children with Abnormal RadiologicalAppearances
There were 36 children in Group 11, including thesix in whom the first examination was normal, butin whom abnormalities were detected later. Threemain abnormalities were seen: (1) the presence ofone or more blocks in the cerebrospinal pathways;(2) absence of air in the subarachnoid space; and(3) hydrocephalus of various degrees. As the lasttwo features are usually the result of the first, allthree were often found together. In addition, someless common features (cyst formation, subdural air)were also noted.
Blocks. Blocks other than those within thespinal theca were seen in 30 of the 36 children andin two others their presence was not definitelyexcluded by ventriculography. In five childrenblocks were demonstrated at two sites, but in everyone of the 30 cases with blocks one of these wassituated either at the tentorial opening or in thebasal cisterns. A block at the tentorial openingcan be recognized in the lateral film by the collectionof air in the distended cisterns behind the sellatogether with the absence of subarachnoid air(Smith, Vollum, and Cairns, 1948) and often by thecollection of air under the tentorium (Figs. 5 and 5a).The encephalogram is similar when the blockoccludes the basal cisterns, except that the air isheld further back, in the cisterna magna (Figs. 6and 6a). In the anteroposterior film the normalfilling of the lateral ventricles, with the absence ofsubarachnoid air and often the presence of a largecollection of subdural air under the tentorium, isstrong indirect evidence of a block at these sites,especially if the ventricles are already dilated (Figs.7 and 7a.) The presence of air in the sulci over thehemispheres excludes the possibility of a block atthe tentorial opening, irrespective of other suggestivefeatures.
In two children the block occluded the Sylvianaqueduct. This is a rare condition in tuberculousmeningitis. It was demonstrated by the failure ofthe ascending air to outline the ventricular systemabove the level of the distal end of the Sylvian
aqueduct (Figs. 8 and 8a). At necropsy these blockswere verified by the finding of a small tuberculomacompletely obstructing the aqueduct in each case.In three other cases the foramina in the roof of thefourth ventricle were obliterated, as shown by airdistending the basal cisterns, but failing to enterthe ventricles (Figs. 9 and 9a) having been injectedby the lumbar route. These blocks were alsoverified at necropsy.
It is of great practical interest to know the timeof onset of these blocks. Although it was foundthat they may occur at any stage of the disease andduring treatment, it seems likely that in the largemajority they were already present before treatmenthad started. As no encephalograms were performedin any of these children before treatment, this cannotbe stated with certainty. In 17 of the 30 patientswith blocks, however, the examination was carriedout within a fortnight, and in 22 within five weeksof the beginning of the treatment, and the blockswere already present. In only six children was theappearance of blocks observed during the courseof the treatment after a previously normal encephalo-gram. These were demonstrated between six and53 weeks after intrathecal treatment had started andactive infection was still present in all. When sucha block appears it can often be recognized by therapid deterioration in the child's condition.
CASE 1. A girl of 4j years had been treated fortuberculous meningitis and her clinical condition hadbeen favourable for eight months although the cerebro-spinal fluid remained grossly abnormal and tuberclebacilli were found from time to time. Her progress wasfollowed at intervals by repeated encephalograms, andthree of these all showed normal appearances. She wasbright, active, and interested during this time, playinglike a normal child. In the thirty-sixth week she startedvomiting, complained of headache, became drowsy, andwithin a week became unconscious. An air encephalo-gram now showed a block at the basal foramina, andpenicillin assay (Lorber and Stewart, 1950) confirmedthis finding. In spite of ventricular punctures she diedwithin a fornight. Necropsy confirmed the diagnosis.
Absence of Air in the Subarachnoid Space. Absenceof air in the subarachnoid space was the second mainabnormality noted. This may occasionally occurin normal persons without an obvious reason, butin this series good filling of the subarachnoid spacewas seen with remarkable regularity in children withotherwise normal encephalograms and its absencewas regularly connected with or followed by otherabnormalities. In three children the absence ofsubarachnoid air was the first abnormality notedand preceded the development of hydrocephalus.There were only four children in whom hydro-cephalus was demonstrated in spite of the presence
4
33
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
of some subarachnoid air, and in one of them thehydrocephalus was unilateral.
Occasionally air may find its way into the sub-dural space after lumbar injection. Subdural airis not necessarily pathological, and its importancelies in the possibility of confusing it with air in thesubarachnoid space. If mistaken for the latter,cortical atrophy or the absence of tentorial blockmay be incorrectly inferred. Subdural air does notoccupy the sulci but occupies the whole surface ofthe brain and it is mobile, as shown when films are
taken in various positions of the head (Figs. 10 and
lOa, 11 and la). In anteroposterior projectionstaken in the upright position it may outline thelongitudinal sinus (Figs. 11 and Ila) and oftenoccupies the space along the falx and the undersurface of the tentorium (Figs. 7 and 7a). Moredetailed observations regarding subdural air maybe found in a study by Smith and Crothers (1950).
Hydrocephasb Hydrocephalus is the thirdcommon abnormality (Figs. 6 and 6a, 12 and 12a).Its presence was demonstrated in 34 of the 36childreninthissecondgroup. In the othertwoventri-cular fiDing was not obtained by encephalograms
TABLE 1CLNICAL AND ENCEPHALOGRAPHiC FEATuiEs IN SIX CHILDREN WITH HYDROCEPHALUS
Age on PAdmis- Condition at (weeks after Condition Legth of
Casc sion of beginning at Trie of Result of Folow-up Condition*No. (Years) Sex Treatmen treatment) E l y Examiation (months) on 30.9.50.
First: 7 Coma Considerable Physically welLhydrocephahu 26 C.S.F. normaL
2 1* M. Comans Retre (I.Q.=S3).Second: 22 Recovered No changeFirst: 2 Coma Moderate Very well.
hydrocephalus C.S.F. normal.(Fig. 13) Optic atrophy.
Vision (6112:6124).Increased Fields resticted.hydrocepbalus (I.Q.=101.)
3 5 F. Coma Second: 7 Coma, spinal Cyst nghtblock frontal lobe
(Fig. 14.)
17
Fully consciousThird: 17 Doing well,
spinal blockrsolved
Same(Fig. 15.)
First: S Drowsy, irritable, Slight WelL C.S.F. normaLwasting hydrocephalus Hemiplegic, deaf, and
4 1 M. Drowsy, Second: 21 Much brighter, Gross hydro- 17 grossly retarded.apathetic recovering cephalus. Cyst (I.Q.=below 30).
right frontallobe
First: i Coma, hemiplegia Slightly dilated Very well
S 3j F. Coma,heiipkegia
Second: 5 Drowsy, irritabk,hemip)egia
Third: 7 Same
ventriclesNo block
Iereasedhydrocephadtstentorial block
Considerablehydrocephalus
C.S.F. normal.
Residual hemip
(T.Q.=77.)
12
Fourth: 17 Very well, Samehemipkegia
First: I Extremely ill, Moderate Very well.
bulbar palsy hydrocephatis C.S.F. slightlyAcutely ill, abnormal.
6 5 F. fully Second: Recovering, Much increased 8 Still treated.conscious satisfactory hydrocephalus (I.Q.= 100i.)
pxogress
First: i Coma Moderate Well. C.S.F. normal.hydrocephalus Rapid menal
improvement
Gross continuin.hydrocephalus, (I.Q.=61.)
7 2X M. Coma Second: 9 Conscious but eplaly ofblind posterior
horns
at
T}hird: 27 Recovered, and Regression ofhas good vision hydrocepbalus
to original siz
Al children alive on 20.1.51. Minimum follow-up 12 months.
34
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

FTIGS. 10 andI Oa.-L at e ra I
c-,iew taken withbrow up, show-ing lateral
-Ventricks (1).the sella (13),and a pocket of,-ubdural air (10)covering the
"-ontal cortex
-4
FiG. IOa. FI. 10
Flbt 11 and 1 a-Antero-posterior view, showing the lateralventricles (1), air in the subdural space (10) outlining the superiorloudina sin (12). The shaded area is the surface of the brain.
There is no air in the subarachno,d space.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

Fi;. 13 and 13a.-First encephalogram (Case 3) two weeks afterbeginning of treatment showing moderate dilatation of the lateralentricles (1) but not of the fourth ventricle (5). Air is held up under
the tentorium (8) and there is none in the subarachaoid spaces. Thesella is shown (13).
FIG. 13.
FIG. 14.
Fios. 14 and 14a.-Ventriculogr a m(Case 3) seven weeksafter beginning oftreatment, sbowinggross increase in thesize of the lateralventricles (I) sincethe previousexamination. Air isstill held up underthe tentorium (8)and also in the basalcistrns (7) behindthe sella 13). Thereis a large cy-st (14)in the tight frontallobe.communicatingwith the ventricle.
FIG. 14a.
I Fws. 15 and 15a.-i-a __ncpnaio-rM enpaogram (recumbentposition) 17 weeksafter admission ofCase 3 showing atleast as great dilata-tion of the lateralventricles (1) as be-fore. The foramenof Monro (2) andthe third ventricle(3) are also demon-strated Air is stillpresent under thetentorium (8) and inthe basal csterns (7)behind the sclla (I 3).The right frontallobe cyst (14) is stillpresent. There isno air in thesubarachnoid space.
FIC. 13a.
FIG. 15.FIG. 15a.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

FIGs. 16 and 16a.-Encephalo-gram of Case 7, at the time ofblindness showg gross diata-ion of the lateral ventricles (1)but cialy that of theposterior horns. Air is collect-ing unler the tentorium (8) andin the ciaterna manna, but nonebehind the sella (13). There isno air in the subarachnoid space.
Hemiplegia was presenside. There is subdu
tentornum (8).
FIG. 16a.
'aumatic cystar puncturerable dilatationnd air collectshere is no air iid space.
and 18a.-A!and traumaticIre following viit lateral vent
FIG. 17a. FIG. IS7A.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
due to blocking of the foramina in the roof ofthe fourth ventricle. Ventriculography was notperformed, but at necropsy ventricular dilatationwas found in both cases and the site of the blockwas confirmd.The hydrocephalus was symmetrical in all but
three cases although slight differences in size betweenthe two lateral ventricles were frequently seen. Aslight tilt or rotation of the head was enough tocause such apparent asymmetry. In three children,however, one lateral ventricle was definitely largerthan the other (Fig. 18 and 18a): all had hemiplegiaon the opposite side of the body.
T'he degree of hydrocephalus varied from slight(Figs. 11 and lla) to extreme (Figs. 4 and 4a),according to the timing of the examination. Theexamination was not repeated in nine children whoseclinical progress was poor and in whom considerablehydrocephalus was demonstrated on the firstoccasion. It is likely that hydrocephalus increasedfurther in size up to the time of their death. Thisbelief is based on the observation of 13 otherchildren who are either dead or whose conditionmakes recovery extremely unlikely and in whomrepeated examinations showed a progressive increasein the degree of hydrocephalus.
It is of particular importance to observe theprogress of hydrocephalus in those children whomade an apparent recovery or are making such goodprogress that their recovery is likely. There are
six such children in this series whose progress waswatched by repeated air studies. Details are
presented in Table 1, but some addition is necessary
in two cases.
CASE 3. The spontaneous formation of a cerebralcyst in the right frontal lobe communicating with thelateral ventricle was demonstrated at the secondexamination, when the first ventricular puncturewas performed. The cyst was in front of theneedle's track (Fig. 14 and 14a). Soon after thisexamination the child's sensorium began to clear andsome four weeks later she was fully conscious. Sincethen her progress has been excellent and she was verywell when the last encephalogram was performed.Further examinations were not justifiable and thereforethe present size of her ventricles is not known withcertainty, but it seems that in spite of considerablehydrocephalus she is a bright, intelligent girl. Her I.Q.is 101, and she has a good memory for past and recentevents, except for a period of amnesia during her illness.She has a normal personality and excellent physique.Unfortunately she has bilateral optic atrophy andrestricted visual fields, although her vision is good. Herpupils are dilated and fail to react to light.CAsE 7. This boy was found to be totally blind when
he regained consciousness, and he remained blind fortwo months. His slight papilloedema did not appear tobe the cause of the blindness. The second encephalogram
taken during this time, however, showed considerableincrease of the hydrocephalus which especially affectedthe posterior horns of the lateral ventricles (Figs. 16 and16a). It was thought that the blindness was probablydue either to the destruction or compression of thefibres of the optic radiation. His vision slowly returnedand at present it appears to be normal. The child madea remarkable recovery and his mental developmentrapidly approached normal. Just before treatment wasconcluded a third encephalogram was performed. Theappearances were strikingly better, the size of theventricles being much less, similar to that shown onFig. 14. The posterior horns of the lateral ventriclesshowed the greatest regression in size. This is the onlycase in which regression of the hydrocephalus wasobserved.
In addition to the hydrocephalus the spontaneousformation of a cyst was demonstrated within thesubstance of the frontal lobes in two cases (Nos. 3and 4). The formation of a cyst in a parietal lobewas demonstrated in a 5-months-old infant twoweeks after a ventricular puncture. This cyst wasexactly at the site of the track of the needle (Figs. 17.17a, and 18, 18a).
Correhtion of Encephalographic Findings withClinal Progress
After this survey of the cardinal findings it isinteresting to compare the fate of the children inthe two groups. For this purpose only those44 patients will be considered who on September 30.1950, have been observed for more than sevenmonths from the beginning of treatment. Twenty-four (540 ) of those 44 survived (Table 2).
TABLE 2FOLLOw-UP PERIOD OF SURVIVORS ON 30.9.50*
Months Number
7-9 4 )
9-12 3
12-15 4,
15-18 5 -13
18-24 4 1
24-31 4 4
7-31 24
* All survisors were alive on 20.1.51, a minimum of 11 monthsafter the beginning of treatment.
Of the 18 children in whom the findings wereconsistently normal only two died, and only one ofthem from meningitis (Table 3). This boy was ina severely anergic phase and had practically normal
38
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

CEREBROSPINAL FLUID CIRCULATION IN MENINGITIS: IITE 3
CoNDmoN* oF CHmuREn wrrH NoRMAL AND ABNORMAL PNEUMoENCEPHALOGRAMS
Pneumoencephalogram
Condition on September 30, 1950 Normal Abnormal
No neurological disability 13Mentally normal Optic atrophy 1
Hemiplegia 1Recovered
No neurological disability 2Deafness -
Alive Retarded Hemiplegia - 2Hemiplegia and deafness -
Still under treatment 2 1
Total alive 16 8
Dead 2 18
Total 18 26
* Minimum follow-up of seven months. All alve on 20.1.51.
cerebrospinal fluid throughout his illness except thata heavy growth of tubercle bacilli was obtainedfrom almost all specimens of fluid examined. Atnecropsy there was but slight exudate and theventricles were little larger than normal. Thisenlargement took place after the encephalogramwas performed.The second child was being treated for miliary
tuberculosis at the time when meningitis developed.She responded well to treatment, and was dischargedwith a normal cerebrospinal fluid and radio-graphically and clinically normal lungs. Twomonths later she returned with fulminating phthisisand there was no response to further streptomycintreatment. At necropsy the meninges and theventricular system were normal, but there wereseveral small encapsulated subcortical tuberculo-mata.
Excluding two children still on treatment, 13 ofthe 16 survivors in the first group are physically andmentally normal. One acquired deafness duringtreatment before she could speak and consequentlyshe is dumb as well. These handicaps obviouslyretarded her mental development, although there isreason to believe that she is retarded even beyondthat.Of the 26 patients with abnormal enecphalograms
18 (69%) died, all of them of meningitis. Excludingone child (Case 6) who is still on treatment, thereare seven survivors in this second group. All ofthem have hydrocephalus. There is not one amongthem without some residual neurological or mentallesion. Only one child in this group has so farescaped death or major disability (Case 3). Three
other children will probably be able to lead a useful,if restricted, life, in spite of their disabilities. Theremaining three are so severely retarded that theyare never likely to be able to fend for themselves.
This apparent close correlation between theencephalographic findings and the fate of thechildren must be assessed with regard to the severityof their disease at the beginning of the treatment.All cases were classified on admission into one ofthree groups, according to the criteria of theMedical Research Council (1948). This classifica-tion was used in the assessment of the results(Table 4).Of the 44 children who have been followed for a
miniimum of seven months, 11 were classified as'early,' 18 as ' intermediate,' and 15 as ' advanced 'cases. It is well established that most early caseswill recover if adequately treated, but only a fewin the advanced state will be saved. The prognosisis very doubtful in cases of intermediate severity.
In this series the initial encephalogram was withinnormal limits in all children in the early stage of thedisease, but subsequently it became abnormal inone of them. This child and another died (ofphthisis), but the remaining nine survived. Thusencephalography confirmed the good prognosis ofthis group.Of the 15 advanced cases 13 had initially and
permanently abnormal encephalograms. In onlytwo was the first encephalogram normal and in oneof these it became abnormal later. This last childand four others survived with the various dis-abilities which have been described, and ten died.Thus encephalography strssed the poor prognosis
39
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

40
PROGNOSIS OF CHILDREN
ARCHIVES OF DISEASE IN CHILDHOODTABIE 4
wITH TuBERcuious MENorGrs CORRELATED wrrH STAGE OF DIASE AT BEGINNING OFTREATmwr AND ENCEPHALOGRAPHJC FINDINGs
Clinical Stage Encephalograms Number of Cases Survivors (Oo)Initial Final
Normal Normal 10 9(82)
Early Normal Abnormal
Abnormal Abnormal
Normal Normal 7 7> (78)
Intermediate Normal Abnormal 2
Abnormal Abnormal 9 3 (33)
Normal Normal I
Advanced Normal Abnormal 1 1
Abnormal Abnormal 13 4 (30)
Normal Normal 1886> (77)
Total Normal Abnormal 4
Abnormal Abnormal 22 7 (31)
of this group, both as regards chances of survivaland the likelihood of residual defects.The group between these two extemes is the most
important because it is the largest and because ofthe uncertainty of the prognosis as judged byexisting clinical criteria. At the best about half ofthem may recover but it is not possible to say whichhalf. Of the 18 children in this group nine hadinitially normal encephalograms: seven recovered(78%) and the encephalograms became abnormallater in the two fatal cases. Of the nine withinitially abnormal encephalograms only three arealive (33%) and one of them is an idiot. With thehelp of encephalography this group could bedivided into two halves, one with a good and onewith a bad prognosis (Table 4).The last feature investigated was the prognosis of
nine relapsed* cases of meningitis in relation to thepneumoencephalographic findings. The examina-tions were performed soon after the relapse. Infive of them the appearances were normal and theysurvived. In the other four the appearances wereabnormal. These are all dead.
DiscussioxCertain objects of this investigation were set out* I Relapse ' is used in a broad sense to denote the conditior of
chidren who were clinically well and whose cerberospinal fluid waseither normal (two cases) or approaching normal (seven cases), butwere not necessariy off intramuscular treatment at the time.
at the beginning of this study and these will beexamined in the light of the results presented.
(1) Over 100 reports on the treatment of tuber-culous meningitis commented on the frequency ofhydrocephalus. Many of them illustrated this bypneumoencephalograms or pathological specimens.Very few reports, however, mention that hydro-cephalus is not an invariable finding. The reasonfor this is that pneumoencephalograms were usuallyperformed in selected cases, either because someabnormality was expected or because the patient'sclinical condition was unsatisfactory and surgicalintervention was contemplated. This led to thebelief that at least some degree of hydrocephalus isinevitable in all cases and this view was supportedby Cairns (1949). Janbon, Bertrand, Salvaing, andVernhet (1949), however, report that only 63qo oftheir 55 patients had hydrocephalus, but no furtherdetails were given. Only two encephalographicstudies reported the result in small series ofunselected cases. Murano (1948) found normalventricles in two out of 19 cases. Unfortunately thereproductions of his radiographs do not allow theircritical assessment, but Schonenberg (1950) repro-duced two encephalograms which appear to be-normal and there were other similar cases in hisseries of 26.
It is because of this background, that the most
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

CEREBROSPINAL FLUID CIRCULATION IN MENINGITIS: HIunexpected outcome of the planned investigation ofthis virtually unselected group of children was thefrequency with which perfectly normal conditionswere discovered. Yet there is no theoretical reasonwhy ventricular dilatation should occur in the earlystages of tuberculous meningitis before obstructionof the pathways has had time to develop. Nor doessuch an obstruction necessarily develop if treatmentis promptly instituted. This was conclusivelydemonstrated in the early and some of the inter-mediate cases of meningitis of this series, whererepeated examinations were performed. In approxi-mately 4000 of all cases no abnormal findings werepresent at any time.The necropsy findings of streptomycin-treated
cases of tuberculous meningitis are only of limitedvalue as these cannot represent the conditions in thesurvivors. The findings in untreated cases arenearer to the conditions obtained in the living.Although most textbooks consider hydrocephalusas one of the characteristic features of the disease,some support for the observations of the presentinvestigation may be found in the monograph onthe pathology of hydrocephalus by Russell (1949a).She found only slight degrees of hydrocephalus insome cases of tuberculous meningitis, and in othersthere was none.
Lincoln (1947) was struck by the infrequency ofhydrocephalus in cases where the duration of illnessto death was less than three weeks (nine out of40 cases, 22.50o). In cases of longer duration theincidence rose to 63.60o (14 out of 22). Perry(1950) reports a 310O incidence of hydrocephalus inhis 80 cases. It is therefore reasonable to expectthat these proportions need not be exceeded ifeffective treatment is given early in the disease.
(2) Obstructions were observed in more than halfof the cases, either within the ventricular system,or, much more frequently, at the tentorial openingand in the subarachnoid cisterns. In this respectthe present investigation fully confirms theencephalographic findings of Cairns (1949), Feld(1949), Janbon et al. (1949), and Smith et al. (1948).In pyogenic meningitis blockage of the Sylvianaqueduct or the foramina of Magendie and Luschkamay occur, due to deposition of inspissatedpus (Cairns, 1949), but obstruction at these siteswas rarely found in this series, because of the clearnature of the fluid in tuberculous meningitis.
Great importance is attached to the absence ofsubarachnoid air as a sign of blockage at thetentorial opening. Feld (1949) also drew attentionto this sign which he considered an indication forsurgical intervention before hydrocephalus has timeto develop. In the three cases of the present serieswhere subarachnoid air was absent but with initially
normal-sized ventricles, hydrocephalus developed inall. Whether any operative procedures would havebeen of value is unlikely in view of the publishedevidence (Feld, 1949).
(3) The incidence of hydrocephalus was almostthe same as the incidence of obstructive lesions, andoccurred in the same patients. This observation isin full accord with that of Russell (1949b) that anobstructive lesion can be found in at least 99°0 ofcases of internal hydrocephalus. Nevertheless infour cases a moderate degree of hydrocephalus wasobserved in the presence of subarachnoid air andthe absence of demonstrable obstruction, and sucha case has also been illustrated by Feld (1949).This hydrocephalus is probably of the passive typeand the ventricles merely enlarge to occupy the spaceleft by the shrunken brain substance, due possiblyto loss of nerve tissue as a direct result of coincidentencephalitis or infarction. It is possible that thislatter mechanism does play some part in the othermuch larger group of cases of hydrocephalus with aknown obstructive element. Support for thissuggestion may be found in the observation thatappreciable enlargement of the head was rare evenwhen the ventricles were of extreme size. There isno doubt, however, that obstruction is the dominantelement in the production of hydrocephalus.
In only six cases of the present series did hydro-cephalus develop in the course of treatment whennormal encephalograms had been previouslyobtained, showing that early diagnosis may avertthis frequent complication. Conversely, hydro-cephalus, or the obstruction leading to it, wasprobably already present before treatment was begunin the large majority of the more advanced cases.This latter observation was more definitely estab-lished by Sch6nenberg (1950) who performedencephalograms on 26 patients before therapy.These facts strengthen the belief that intrathecalstreptomycin plays no part in the causation ofhydrocephalus, but merely renders it more obviousby prolonging the patient's survival (De, 1949).One of the most important problems is the
permanency of hydrocephalus in surviving patients.It is well established that even a considerable degreeof hydrocephalus may regress if the obstructiongiving rise to it is removed in time. Instances of thishave been recorded by Fincher, Strewler. andSwanson (1948), Swanson and Perrett (1950).Torkildsen (1948), and Walker and Hopple (1949)in cases of cerebral tumour or stenosis of theSylvian aqueduct, but regression of the hydro-cephalus in tuberculous meningitis has not beenpreviously described in the available literature. Ofthe six surviving cases of hydrocephalus repeatedencephalograms showed no decrease in its degree
41by copyright.
on January 11, 2022 by guest. Protected
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.26.125.28 on 1 February 1951. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
in two, and a substantial increase in three, in spiteof considerable clinical improvement or indeedrecovery of physical and mental health when thelast encephalogram was performed. Cairns andTaylor (1949) had a similar experience with an adultpatient. In one child in this series definiteregression of the hydrocephalus was noted (Case 7),and consequently this may have occurred in othersafter the last encephalogram was performed. Thisproblem is the subject of further investigations.The aetiology of the spontaneous formation of a
cyst in the brain substance in two cases is not quitecertain. They may represent porencephalic cavitiesdue to arteritis and infarction. Arteritis is afrequent pathological feature of tuberculous menin-gitis (Daniel, 1949; Doniach, 1949; Hektoen, 1896;Rigdon and Lefeber, 1950; Smith and Daniel, 1947;Winter, 1950), but there has been no description ofarteritis leading to the formation of large cerebralcysts. Torkildsen's (1948) explanation is morelikely. He reported on the spontaneous rupture ofthe ventricular ependyma in five cases of hydro-cephalus due to cerebral tumour. This rupture wasthought to have been caused by the differencebetween the high intraventricular and the lowsubarachnoid pressure and was followed by cystformation. Cerebral cyst formations have beendescribed in hydrocephalus of various aetiologies(Childe and McNaughton, 1942; de Lange, 1929;Penfield, 1929; Pennybacker and Russell, 1943; andSweet, 1940) including one in an untreated case oftuberculous meningitis (Russell, 1949c). Torkildsen(1948) writes:
Occasionally hydrocephalic patients give a historyof sudden subsidence of the signs of increasedintracranial tension which conceivably may be dueto ventricular rupture with formation of a shortcircuit giving the cerebrospinal fluid direct access tothe subarachnoid space.
It may be more than coincidence that the appearanceof the cysts in the patients of the present series moreor less coincided with a striking clinical improvementalthough actual communication with the subarach-noid space was not demonstrated.Another case in this series supports the second
theory. This infant had gross hydrocephalus, andat necropsy several ruptures were found in theependyma of both lateral ventricles (Fig. 19), verysimilar to those of the case of Pennybacker andRussell (1943). It is assumed that there had beenno time for cysts to develop.
(4) The correlation between the encephalographicfindings, the stage of the disease, and the prognosishave already been analysed in detail (Tables 3 and 4).It is beyond the scope of this paper to correlate theencephalographic findings with all other factors
which are generally thought to be of prognosticsignificance, e.g., age, coexisting miliary and otherforms of tuberculosis, and the length of delay beforetreatment is instituted (Lorber, 1950c). In thisseries, however, encephalography was a very reliablesingle prognostic criterion. If taken together withall the other known factors, a correct prognosismay be given in almost all cases.
(5) Amatruda (1942) and Casamajor, Laidlaw.and Kozinn (1949) have pointed out that there isno definite correlation between encephalographicappearances and various degrees of mental develop-ment and that encephalography does not picture thefunctional capacity of the cerebrum. Amatrudanoted that children with even gross communicatinghydrocephalus may do particularly well from thestandpoint of development. The observations ofthese authors apply to a large extent to the survivorsof tuberculous meningitis in this series, but withcertain reservations. Using the methods describedelsewhere (Lorber, 1949) no apparent deteriorationwas detected in the intellectual capacity of 15 ofthe 16 survivors with normal encephalograms, butthree of the eight survivors with variable degreesof hydrocephalus are severely retarded. It isinteresting, however, that two children with con-siderable hydrocephalus have I.Q.s above 100.Although the numbers in this hydrocephalic groupare small, it seems that mental deterioration is morefrequent when ventricular dilatation is present.
(6) The most difficult problem is whether selectionof cases for treatment and the abandonment oftreatment on humanitarian grounds is justifiable ornot. Many children live a vegetative existence formonths, and streptomycin may not only unneces-sarily prolong their suffering, but, worse still, may
FiG. I9.-Spontaneous rupture of the ventricular ependyma in a caseof tuberculous meningitis with gross hydrocephalus.
42by copyright.
on January 11, 2022 by guest. Protected
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.26.125.28 on 1 February 1951. D
ownloaded from

CEREBROSPINAL FLUID CIRCULATION IN MENINGITIS: 1I 43
cure them of their infection and thus create serioussocial and moral problems. It would be of greatpractical advantage if one could recognize thesecases early. Criteria are needed to define certaincases as untreatable, just as there are criteria forjudging certain cancers inoperable. The observa-tions in the present series suggest that encephalo-graphy may substantially contribute to the fulfilmentof this need, but much more experience is necessarybefore any firm rules may be formulated. It is,however, probably advisable to interrupt treatmentearly where really gross hydrocephalus (Fig. 4)exists.
SwxmOne hundred pneumoencephalograms were per-
formed on 58 children suffering from tuberculousmeningitis. With the possible exception of one case,no serious after-effects were noted. No relapse ofthe meningitis followed within two months of anyexamination.
In 18 children normal conditions existed four to14 months after beginning the treatment.
Abnormalities were found in 36 children. In sixof these a previous pneumoencephalogram had beennormal. Three main abnormalities were detected.
(I) One or more blocks other than spinal oneswere found in 30 cases. In all of these there wasa block at the tentorial opening or in the basalcisterns. In two cases there was an additionalblock at the Sylvian aqueduct, and in three othersin the foramina of the fourth ventricle. Theseblocks were usually present at or soon after thebeginning of treatment.
(2) In no case of tentorial or basal cisternalblock was there subarachnoid air. This signpreceded the hydrocephalus in three cases. Inonly four children was any degree of hydro-cephalus seen when subarachnoid air was present.Subarachnoid air must be distinguished fromsubdural air which may occur in any enscephalo-gram.
(3) Hydrocephalus of varying degrees wasfound in 34 cases. Clinical recovery was almostcomplete in eight of these children. Repeatedpneumoencephalograms in six of them showed anincrease in the degree of the hydrocephalus inthree, no change in two, and a decrease in one.In three hydrocephalic children cerebral cysts
developed; in two cases spontaneously and in theother following a ventricular puncture. Theaetiology of the cysts is discussed.A close correlation was found betw-een encephalo-
graphic appearances and prognosis. After aminium follow-up period of eleven months 16 of18 children with normal encephalograms were aliveand only one of the survivors was left with serious
neurological sequelae. One of the deaths was notdue to meningitis.Of 26 children with abnormal encephalograms
only eight were alive after the same period ofobservation. They all have neurological or mentalresidual lesions, and these are serious in five.Of nine cases of meningitis which relapsed, five
had normal encephalograms and survived. Thefour others died.No absolute dividing line was found regarding
mental development following recovery fromtuberculous meningitis in children with normal andabnormal encephalograms, but only one child outof 16 became retarded where the final encephalo-gram was normal, and three of eight children whosurvived with hydrocephalus are grossly retarded.In two cases considerable hydrocephalus wascompatible with good intelligence.
It is suggested that further experience may wellshow that encephalography supplies criteria for theselection of cases for treatment and for the abandon-ment of treatment.
I wish to thank Professor R. S. Lllingworth and Dr.T. Colver for permission to investigate their cases;Professor Illingworth, Dr. Honor V. Smith, Dr. S. A.Doxiadis, and Dr. D. G. H. Stone for their criticism;Dr. J. L. Emery for the pathological data; Dr. T. Lodgeand Sister Mallinder for the radiographs; Mr. A. F.Taylor for the photographs and Mr. A. S. Foster for theline drawings.
REFERENCESAmatruda, C. S. (1942). J. Pediat., 21, 147.Brain, W. R. (1947). 'Diseases of the Nervous System,'
3rd ed., p. 251. London.Caffey J. (1945). 'Pediatric X-ray Diagnosis,' pp. 136-
151. Chicago.Cairns, H. (1949). Brit. med. J., 1, 969.
and Taylor, M. (1949). Proc. ro.y. Soc. M4fed.,42, 155.
Casamajor. L.. Laidlaw. R. W., and Kozinn, P. J. (1949).J. Amer. med. Ass.. 140, 1329.
Cestan and Riser (1924). Bull. Soc. med. H6p. Paris,48, 953.
Childe, A. E.. and McNaughton, F. L. (1942). Arch.NVeurol. Psvchiat., Chicago, 47, 768.
Dandy, W. E. (1918). Ann. Surg., 68, 5.(1919). Ibid., 70, 397.
Daniel, P. M. (1949). Proc. roy. Soc. Mfed., 42, 169.Davidoff, L. M., and Dyke, C. G. (1946a). 'The Normal
Encephalogram,, p. 15, 2nd ed. (1946b), p. 38.London.
De, S. N. (1949). Brit. med. J., 2, 214.Doniach, 1. (1949). J. Path. Bact., 61, 253.Eckstein, A. (1927). Ergebn. inn. Med., Kinderheilk.,
32, 548.Eley, R. C., and Vogt. E. C. (1932). Amer. J. Roentgenol.
27, 686.Feld, M. (1949). Senz. H6p. Paris, 25, 3512.Fincher, E. F., Strewler. G. J., and Swanson, H. S. (1948).
J. Neurosurg.. 5, 213.Fine. J., Frehling, S., and Starr. A. (1935). J. Thorac.
Surg., 4, 635.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from

44 ARCHIVES OF DISEASE IN CHILDHOODFlesch, I., and Gefferth, C. (1949). Paed. danub., 5, 158.
(English summary, p. 166.)Hektoen, L. (1896). J. exp. Med., 1, 112.Herrmann, G. (1922). Med. Klinik., 18, 1146.Janbon, M., Bertrand, L.. Salvaing, J., and Vernhet, J.
(1949). Sem. Hop. Paris, 25, 3478.Kornreich, C. J. (1948). Arch. Neurol. Psychiat.,
Chicago, 60, 512.Kryspin-Exner, W. (1932). PsYchiat.-neurol. Wschr., 34,
509.Lange, C. de (1929). Proc. Acad. Sci. Amst., 32, 78.Lincoln, E. M. (1947). Amer. Rev. Tuberc., 56, 75.Lorber, J. (1949). Archives of Disease ini Childhood,
24, 289.(1950a). Brit. med. J., 2 1.(1950b). Lancet, 1, 467.(1950c). Proc. roy. Soc. Med., In the press.and Stewart, S. M. (1950). Archives of Diseasein Childood, 25, 404.
MacCarthy, D., and Mann, T. P. (1950). Lancet, 1, 341.Medical Research Council, Streptomycin in Tuberculosis
Trials Committee (1948). Ibid., 1, 582.Merritt, H. H., and Fremont-Smith, F. (1937). 'The
Cerebrospinal Fluid,' p. 223. Philadelphia.Murano, G. (1948). Pediatria, 56, 657.Penfield, W. (1929). Arch. Neurol. Psychiat., Chicago,
22, 358.Pennybacker, J., and Russell, D. S. (1943). J. .Aeurol.
Psychiat., 6, 38.
Perry, T. L. (1950). Pediatrics, 5, 988.Rigdon. R. H., and Lefeber, E. J. (1950). Amer. Rev.
Tubere., 61, 247.Russell, D. S. (1949). Observations on the Pathology
of Hydrocephalus.' Spec. Rep. Ser. med. Res.Cowi.,Lond.,No. 265. a, p. 82, b, p. 8, c, p. 124.
Schonenberg, H. (1950). Arztl. Wschr., 5, 106.Schwab, R. S., Fine, J., and Mixter, W. J. (1937). Arch.
Neurol. Psychiat., Chicago, 37, 1271.and von Storch, T. J. C. (1937). New Engl. J.Med.. 217, 21.
Smith, H. V., and Crothers, B. (1950). Pediatrics, 5,375.and Daniel, P. M. (1947). Tubercle, Lond., 28, 64.and Vollum, R. L., and Cairns, H. (1948). Lancet,1, 627.
Sweet, W. H. (1940). Arch. Neurol. Pschiat., Chicago.44, 532.
Swanson, H. S., and Perret, G. (1950). J. Neurosurg.,7, 115.
Thurz6, E. von, and Nagy, M. (1923). Dtsch.Nerventheilk., 79, 374.
Torkildsen, A. (1948). J. Neurosurg., 5, 327.Tschugunoff, S. A. (1929). Z. ges. Neurol. Psychiat.,
122, 452.Walker, A. E., and Hopple, T. L. (1949). J. Pediat.,
35, 671.Winter, W. J. (1950). Amer. Rev. Tuberc., 61, 171.
by copyright. on January 11, 2022 by guest. P
rotectedhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.26.125.28 on 1 F
ebruary 1951. Dow
nloaded from