study guide ok respiratory-semester-vi-tayang-2017
TRANSCRIPT

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
1
STUDY GUIDE “The Respiratory System and Disorders”
Semester VI 20 Feb – 30 March 2017
DEPARTMENT OF MEDICAL EDUCATION FACULTY OF MEDICINE UDAYANA UNIVERSITY
DENPASAR 2017

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
2
TABLE OF CONTENTS
Page
Table of Contens 1
Introduction 2
Curriculum 3
Planner team & Lecturers 4
Facilitators 6
General Time Table 7
Important Informations 8
Meeting of the students’ representative 8
Self Assessment 8
Assessment Method 8
Time Table (Regular Class) 9
Time Table (English Class) 14
Learning Programs 19

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
3
INTRODUCTION
The medical curriculum has become increasingly vertically integrated, with stronger basic concept and support by clinical examples and cases to help in the understanding of the relevance of the underlying basic science. Basic science concepts may help in the understanding of the pathophysiology and treatment of diseases. Respiratory system and disorders block has been written to take account of this trend, and to integrate core aspects of basic science, pathophysiology and treatment into a single, easy to use revision aid. The respiratory system consists of a pair of lungs within the thoracic cage. Its main function is gas exchange, but other roles include speech, filtration of microthrombin arriving from systemic veins and metabolic activities such as conversion of angiotensin I to angiotensin II and removal or deactivation of serotonin, bradykinin, norepinephrine, acetylcholine and drugs such as propranolol and chlorpromazine. So this block will discuss about anatomy, histology, symptom and signs of lung disease and its pathophysiology, major upper respiratory diseases, major lung diseases, major pediatric lung disease, and basic principle concept to education, prevention, treatment and rehabilitation in respiratory system disorder in patient, family and community. The learning process will be carried out for 6 weeks (27 working days) starts from 22nd of February 2016 as shown in the time table. The final examination will be conducted on 4th of April 2016 in the form of MCQ. The learning situation include lecture, individual learning, small group discussion, plenary session, practice, and clinical skill. Most of the learning material should be learned independently and discuss in SGD by the students with the help of facilitator. Lecture is given to emphasize the most important thing of the material. In small group discussion, the students gave learning task to lead their discussion. This simple study guide need more revision in the future, so that the planners kindly invite readers to give any comments and critics for its completion. Thank you. Planners

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
4
CURRICULUM RESPIRATORY SYSTEM AND DISORDER
Aims :
· Comprehend the structure, physiologic, and pathologic of the respiratory system. · Interpret the laboratory and imaging examination of the respiratory system
disorders · Diagnose and treat the patient with common respiratory system disorders · Plan education, prevention, management and rehabilitation of respiratory system
disorders to patient, family and community. Learning outcomes:
· Concern about the size of problem and diversity of respiratory disease in the community
· Able to describe the structure and function of the respiratory system · Able to interpret the result of examination (physical, laboratory, function test,
blood gas analysis and chest imaging) · Able to explore patients with respiratory problem (runny nose, cough, dyspnea,
non cardiac chest pain, hemoptysis) · Able to manage major upper respiratory diseases (tonsillitis, rhinitis, sinusitis) · Able to manage major lung diseases (TBC, asthma, COPD, lung cancer,
pneumonia, occupational lung disease, pleural disease) on patient, family and community
· Able to manage major pediatric lung disease (bronchiolitis, TB, asthma) · Able to implement DOTS program against TB · Able to implement the strategy of smoking cessation, especially in patient with
respiratory disease Curriculum contents:
· Structural and function of the respiratory system · Physiology of lung in related with oxygen consumption and acid base balance · Symptoms and signs of lung disease · Pathophysiology of respiratory system disorders · Basic physical, laboratory and imaging examination · Interpretation of examination results. · Drugs that commonly used in respiratory system disorders (decongestant, anti-
asthma & bronchodilators, antitussive, expectorant · Basic principle concept to education, prevention, treatment and rehabilitation in
respiratory system disorders in patient, family and community.
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
5
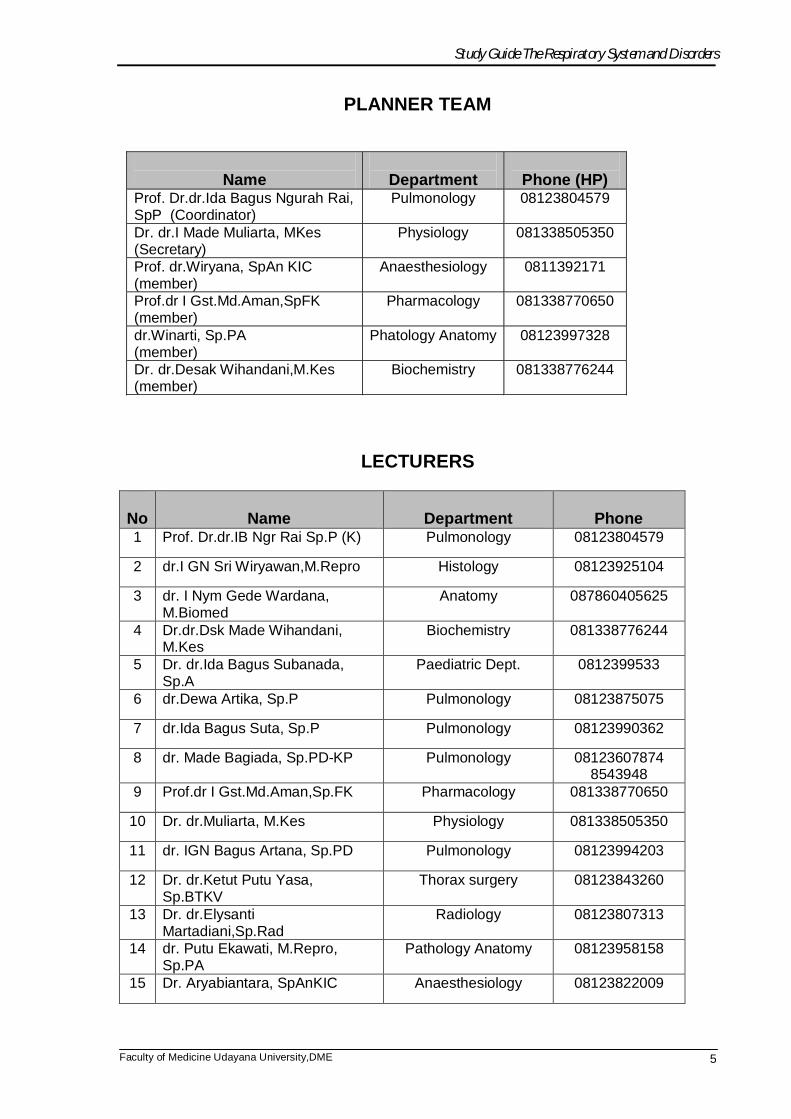
PLANNER TEAM
Name
Department
Phone (HP)
Prof. Dr.dr.Ida Bagus Ngurah Rai, SpP (Coordinator)
Pulmonology 08123804579
Dr. dr.I Made Muliarta, MKes (Secretary)
Physiology 081338505350
Prof. dr.Wiryana, SpAn KIC (member)
Anaesthesiology 0811392171
Prof.dr I Gst.Md.Aman,SpFK (member)
Pharmacology 081338770650
dr.Winarti, Sp.PA (member)
Phatology Anatomy 08123997328
Dr. dr.Desak Wihandani,M.Kes (member)
Biochemistry 081338776244
LECTURERS
No
Name
Department
Phone
1 Prof. Dr.dr.IB Ngr Rai Sp.P (K) Pulmonology 08123804579
2 dr.I GN Sri Wiryawan,M.Repro Histology 08123925104
3 dr. I Nym Gede Wardana, M.Biomed
Anatomy 087860405625
4 Dr.dr.Dsk Made Wihandani, M.Kes
Biochemistry 081338776244
5 Dr. dr.Ida Bagus Subanada, Sp.A
Paediatric Dept. 0812399533
6 dr.Dewa Artika, Sp.P Pulmonology 08123875075
7 dr.Ida Bagus Suta, Sp.P Pulmonology 08123990362
8 dr. Made Bagiada, Sp.PD-KP Pulmonology 08123607874 8543948
9 Prof.dr I Gst.Md.Aman,Sp.FK Pharmacology 081338770650
10 Dr. dr.Muliarta, M.Kes Physiology 081338505350
11 dr. IGN Bagus Artana, Sp.PD Pulmonology 08123994203
12 Dr. dr.Ketut Putu Yasa, Sp.BTKV
Thorax surgery 08123843260
13 Dr. dr.Elysanti Martadiani,Sp.Rad
Radiology 08123807313
14 dr. Putu Ekawati, M.Repro, Sp.PA
Pathology Anatomy 08123958158
15 Dr. Aryabiantara, SpAnKIC Anaesthesiology 08123822009

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
6
16 dr.Putu Siadi Purniti,Sp.A Paediatric 08123812106
17
Dr. Ayu Setyorini, SpA Paediatric 081353286780
18 dr.DGA Eka Putra,Sp.THT Otorhinolaryngology 0813387826317
18 dr. Luh Made Ratnawati, Sp.THT(KL)
Otorhinolaryngology 08123806108
19 dr. Putu Andrika, Sp.PD-KIC Pulmonology 08123989192
20 dr. Gede Ketut Sajinadiyasa, Sp.PD
Pulmonology 085237068670
21 Prof. Suardana, Sp.THT Otorhinolaryngology 0811385299

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
7
~ FACILITATORS ~ Regular Class (Class A)
No Name Group Departement Phone Venue (2&3 rd floor)
1 dr. Gde Somayana, Sp.PD
A1 Interna 081345136913 2nd floor:
R.2.09
2 dr. Ida Bagus Wirakusuma, MOH A2 Public Health 08124696647
2nd floor: R.2.10
3 dr. I Gusti Ngurah Pramesemara , M.Biomed, Repro
A3 Andrology 081338605087 2nd floor:
R.2.11
4 Dr.dr. Tjok G A Senapathi, Sp.An. KAR A4 Anasthesi 081337711220
2nd floor: R.2.12
5 Dr. dr. I Dewa Made Sukrama, MSi, Sp.MK(K) A5 Microbiology 081338291965
2nd floor: R.2.13
6 Dr.dr. Ketut Sudartana, Sp.B-KBD A6 Surgery 0811398996
2nd floor: R.2.14
7 dr. I Kadek Swastika , M Kes
A7 Parasitologi 08124649002 2nd floor:
R.2.15
8 dr. Made Widhi Asih, Sp.Rad (K)
A8 Radiologi 081916442626 2nd floor:
R.2.16
9 dr. Ketut Sudiasa, Sp.B (K) Trauma A9 Surgery 08123811106
2nd floor: R.2.23
10 dr. I Made Oka Negara, FIAS
A10 Andrology 085935054964 3nd floor:
R.3.21
11 dr. Ida Ayu Sri Wijayanti, M.Biomed, Sp.S A11 Neurology 081337667939 3nd floor:
R.3.22
12 dr. I Gusti Ayu Agung Elis Indira , Sp.KK A12 Dermatology 081338718384 3nd floor:
R.3.23 English Class (Class B)
No Name Group Departement Phone Venue (2&3rd floor)
1 Dr. dr. Desak Made Wihandani, M.Kes
B1 Biochemistry 081338776244
2nd floor: R.2.09
2 dr. I Gusti Ayu Sri Darmayani, Sp.OG
B2 DME 081338644411
2nd floor: R.2.10
3 Dr. dr. Made Ratna Saraswati, Sp.PD-KEMD-FINASIM
B3 Interna 08123814688
2nd floor: R.2.11
4 dr. I Gusti Ayu Artini, M.Sc B4
Pharmacology 08123650481 2nd floor:
R.2.12
5 dr. Ni Ketut Sri Diniari, Sp.KJ B5
Psychiatry 081338748051 2nd floor:
R.2.13
6 Dr.dr. I Wayan Sudarsa, Sp.B (K) Onk
B6 Surgery 0811398971
2nd floor: R.2.14

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
8
7 Dr. dr. Anak Agung Wiradewi Lestari , Sp.PK
B7 Clinical Pathology 08155237937
2nd floor: R.2.15
8 Dr.dr. Susy Purnawati, MKK B8
Fisiology 08123989891 2nd floor:
R.2.16
9 Dr.dr. Ni Made Linawati, M.Si B9
Histology 081337222567 2nd floor:
R.2.23
10 Dr.dr. Elysanti Dwi Martadiani, Sp.Rad
B10 Radiology 081805673099
3nd floor: R.3.21
11 dr.Kumara Tini, Sp.S B11
Neurology 081238701081 3nd floor: R.3.22
12 dr. Nyoman Suryawati , M.Kes, Sp.KK
B12 Dermatology 0817447279 3nd floor:
R.3.23
GENERAL TIME TABLE FOR A AND B CLESSES
CLASS A CLASS B
TIME ACTIVITIES TIME ACTIVITIES 08.00-09.00 Lecture 09.00-10.00 Lecture
09.00-10.30 Independent learning 10.00-11.30 Student project
10.30-12.00 SGD 11.30-12.00 Break
12.00-12.30 Break 12.00-13.30 Independent learning
12.30-14.00 Student project 13.30-15.00 SGD
14.00-15.00 Plenary session 15.00-16.00 Plenary session
There are several types of learning activity:
· Lecture
· independent learning based on the lecture’s topic
· Small group discussion to solve the learning task
· Practice
· Student project
· Clinical skill and demonstration
· Self assessment at the end of every topic
· Plenary session
Lecture will be held at room 401, while discussion rooms available at 3rd floor (room A309-A317, A319)

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
9
IMPORTANT INFORMATIONS
Meeting of the students’ representative In the middle of block schedule, a meeting is designed among the student
representatives of every small group discussions, facilitators, and resource persons. The
meeting will discuss the ongoing teaching learning process, quality of lecturers and
facilitators as a feedback to improve the next process. The meeting will be taken based on
schedule from Medical Education Unit.
SELF ASSESSMENT
Self assessment of each lecture will be given after each lecture session, and will be
marked. This mark can determine whether the student pass this block or not. Any final mark
between 62-64 will be reconsidered with self assessment’s mark to see the student’s status.
Any student with self assessment’s mark 70 or more will pass this block. And for the lower
one will have to attend the remedial examination. It is important to do this self assessment
cautiously, because this activity may be your ticket to pass this block just at First
examination.
ASSESSMENT METHOD Assessment in this theme consists of: SGD : 5%
Final Exam : 80%
Student Project : 15%
Final mark 65 or more considered to pass this block. Certain conditions applied for those
with final mark between 62 – 64. These students will be analyzed using their self
assessment’s mark. Students with final mark 62 – 64 and self assessment’s mark equal or
more than 65 will also considered pass this block. The value of marking:
A ≥ 80
B+ >70-79
B 65-70

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
10
TIME TABLE REGULAR CLASS
DAY/DATE TIME ACTIVITY VENUE PIC
1 Monday Feb 20,
2017
08.00-08.15 Introduction Class room Prof.I.B. Rai 08.15-09.00 Lecture 1
Anatomy of Respiratory System
Class room dr.Wardana
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr.Wardana
2 Tuesday Feb 21,
2017
08.00-09.00 Lecture2 Histology of Respiratory System
Class room dr. Sri Wiryawan
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Sri Wiryawan
3 Wednesday
Feb 22, 2017
08.00-09.00 Lecture 3 Physiology of Respiratory System: Ventilation
Class room dr. Muliarta
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Muliarta
4 Thursday Feb 23,
2017
08.00-09.00 Lecture 4 Physiology of Respiratory System: Gas Exchange, diving, altitude
Class room dr. Muliarta
09.00-15.00
Independent learning
Practice : Anatomy, Histology
Anatomy: 1st floor
dr. Wardana
Histology: 4th floor
dr. Sri Wiryawan
5 Friday Feb 24,
2017
08.00-09.00 Lecture 5 Carriage of oxygen and Carbon dioxide
Class room dr. Desak Wihandani
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Desak
Wihandani
RE
GU
LA
R C
LA
SS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
11
6
Monday Feb 27, 2017
08.00-09.00 Lecture 6 Control of acid base balance, Arterial Gas Analysis (AGA)
Class room dr. Desak Wihandani
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Desak
Wihandani
7 Tuesday
Feb 28, 2017
08.00-09.00 Lecture 7 Control of Respiratory Function and Blood Gas Analyzes
Class room dr. Arya Biantara
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room Prof. Wiryana
8 Wednesday
March 1, 2017
08.00-09.00 Lecture 8 Pathology of Respiratory Tract
Class room dr. Ekawati
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room dr. Ekawati
9 Thursday March 2,
2017
08.00-09.00 Lecture 9 Lung Defense Mechanism
Class room dr. Ekawati
09.00-15.00
Independent learning
Practice : Physiology, Pathology Anatomy (PA)
Physiology: 2nd floor
dr. Muliarta
PA: Joint Lab (4th floor)
dr. Ekawati
10 Friday
March 3, 2017
08.00-09.00 Lecture 10 Pharmacological and non pharmacological interventions
Class room Prof. Aman
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room Prof. Aman
11 08.00-09.00 Lecture 11 Class room Prof. Aman
RE
GU
LA
R C
LA
SS
RE
GU
LA
R C
LA
SS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
12
Monday March 6,
2017
Pharmacological and non pharmacological interventions
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room Prof. Aman
12 Tuesday March 7,
2017
08.00-09.00 Lecture 12 Respiratory Imaging
Class room dr. Elysanti
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Elysanti
13 Wednesday
March 8, 2017
08.00-09.00 09.00-10.00
Lecture 13 Bronchiolitis, asthma in children, Pneumonia, Bronkopneumonia,
Class room dr. IB Subanada dr. Ayu Setyorini
10.00-11.30 Independent learning 11.30-13.00 SGD Disc room Facilitator 13.00-13.30 Break 13.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room dr. IB Subanada
14 Thursday March 9,
2017
08.00-09.00 09.00-10.00
Lecture 14 Aspiration Pneumonia ,Pertusis TB in children, Difteri
Class room
dr. Ayu Setyorini dr. Siadi Purniti
10.00-11.30 Independent learning 11.30-13.00 SGD Disc room Facilitator 13.00-13.30 Break 13.30-14.00 Student project 14.00-15.00 Plenary session Class room dr. Siadi Purniti
15 Friday
March 10, 2017
08.00-09.00 09.00-10.00
Lecture 15 Pulmonary TB and Extrapulmonary TB, TB in the Immunocompromised Host, Abses TB
Class room dr. Sutha, dr. Bagiada
10.00-11.30 Independent learning 11.30-13.00 SGD Disc room Facilitator 13.00-13.30 Break 13.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room dr. Sutha,
dr. Bagiada
16 Monday
08.00-09.00 Lecture 16 Asthma, COPD
Class room Prof. IB Rai, dr. Artana
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator
RE
GU
LA
R C
LA
SS
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
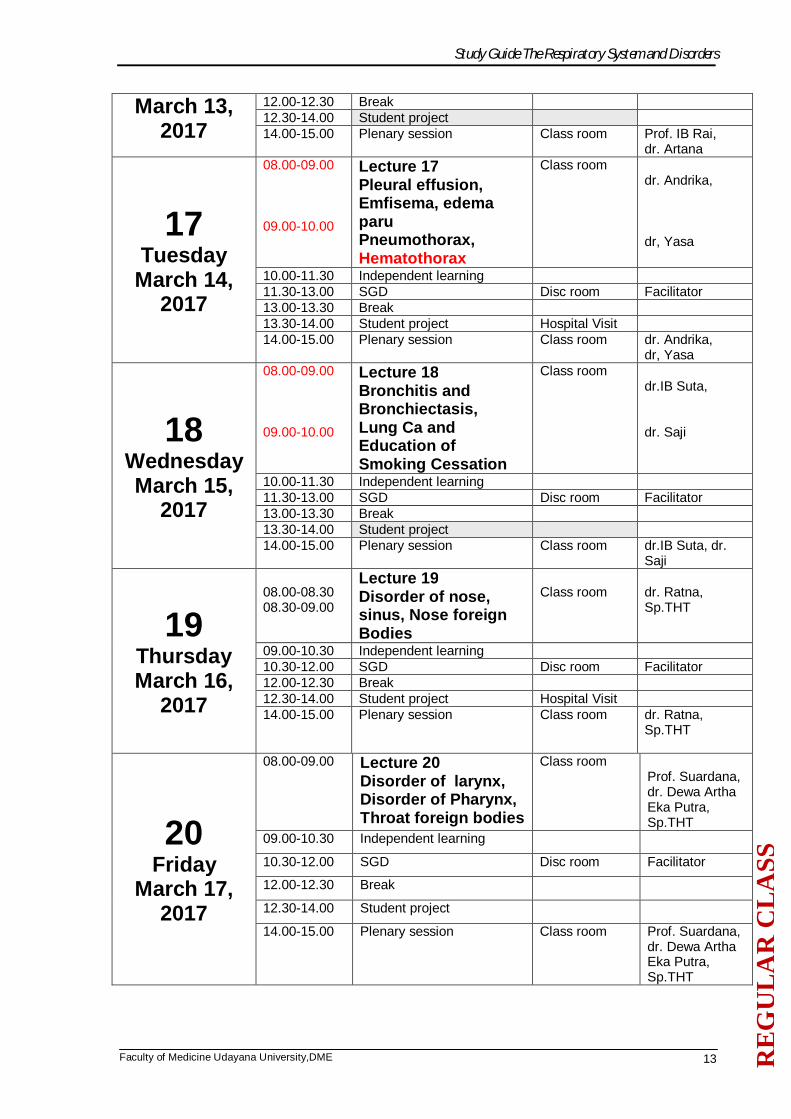
13
March 13, 2017
12.00-12.30 Break 12.30-14.00 Student project 14.00-15.00 Plenary session Class room Prof. IB Rai,
dr. Artana
17 Tuesday
March 14, 2017
08.00-09.00 09.00-10.00
Lecture 17 Pleural effusion, Emfisema, edema paru Pneumothorax, Hematothorax
Class room dr. Andrika, dr, Yasa
10.00-11.30 Independent learning 11.30-13.00 SGD Disc room Facilitator 13.00-13.30 Break 13.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room dr. Andrika,
dr, Yasa
18 Wednesday March 15,
2017
08.00-09.00 09.00-10.00
Lecture 18 Bronchitis and Bronchiectasis, Lung Ca and Education of Smoking Cessation
Class room dr.IB Suta, dr. Saji
10.00-11.30 Independent learning 11.30-13.00 SGD Disc room Facilitator 13.00-13.30 Break 13.30-14.00 Student project 14.00-15.00 Plenary session Class room dr.IB Suta, dr.
Saji
19 Thursday March 16,
2017
08.00-08.30 08.30-09.00
Lecture 19 Disorder of nose, sinus, Nose foreign Bodies
Class room
dr. Ratna, Sp.THT
09.00-10.30 Independent learning 10.30-12.00 SGD Disc room Facilitator 12.00-12.30 Break 12.30-14.00 Student project Hospital Visit 14.00-15.00 Plenary session Class room dr. Ratna,
Sp.THT
20 Friday
March 17, 2017
08.00-09.00 Lecture 20 Disorder of larynx, Disorder of Pharynx, Throat foreign bodies
Class room Prof. Suardana, dr. Dewa Artha Eka Putra, Sp.THT
09.00-10.30 Independent learning
10.30-12.00 SGD Disc room Facilitator
12.00-12.30 Break
12.30-14.00 Student project
14.00-15.00 Plenary session Class room Prof. Suardana, dr. Dewa Artha Eka Putra, Sp.THT
RE
GU
LA
R C
LA
SS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
14
21 Monday
March 20, 2017
08.00-15.00
BCS: Physical Diagnostic of Thorax Dewasa BCS: Radio Imaging BCS: Pemasangan dan Perawatan WSD (Pre-test, lecture, demo Practice, discussion)
Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
Dr. Saji dr. Elysanti dr. yasa
22 Tuesday
March 21, 2017
08.00-15.00
BCS: Spirometri BCS: Pengambilan cairan Pleura, Punksi, Decompresi jarum BCS: Nebulisasi dan terapi oksigen (Pre-test, Lecture, practice, demo)
Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Muliarta dr. Yasa dr. Arya Biantara
23 Wednesday March 22,
2017
08.00-15.00
BCS: Radio imaging BCS: Physical Diagnostic of Thorax Bayi Anak BCS: Physical Diagnostic of Thorax Dewasa (Pre-test, lecture, practice, demo)
Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Elysanti dr. Ayu Setyorini dr. Saji
24 Thursday March 23,
2017
08.00-15.00
BCS: Bronchoscopy, Provocation test, Radio Imaging BCS: CPEP pada Bayi BCS: Physical Diagnostic of Thorax Dewasa (Pre-test, lecture, demo)
Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr Artana dr. Elysanti dr. Arya Biantara dr. Saji
25 Friday
March 24, 2017
08.00-15.00
BCS: Physical Diagnostic of Thorax Bayi Anak BCS: Perawatan WSD, Decompresi Jarum BCS: Rhinoskopi Posterior (Practice, post-test)
Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Ayu Setyorini dr. Yasa THT

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
15
26 Thursday March 30,
2017 Examination

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
16
TIME TABLE ENGLISH CLASS
DAY/DATE TIME
VENUE PIC
1 Monday Feb 22,
2016
09.00-09.15 Introduction Class room Prof.I.B. Rai 09.15-10.00 Lecture 1
Anatomy of Respiratory System
Class room dr.Wardana
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr.Wardana
2 Tuesday Feb 23,
2016
09.00-10.00 Lecture2 Histology of Respiratory System
Class room dr. Sri Wiryawan
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Sri Wiryawan
3 Wednesday
Feb 24, 2016
09.00-10.00 Lecture 3 Physiology of Respiratory System: Ventilation
Class room dr. Muliarta
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Muliarta
4 Thursday Feb 25,
2016
09.00-10.00 Lecture 4 Physiology of Respiratory System: Gas Exchange, diving, altitude
Class room dr. Muliarta
10.00-16.00
Independent learning
Practice : Anatomy, Histology
Anatomy: 1st floor
dr. Wardana
Histology: 4th floor
dr. Sri Wiryawan
5 Friday Feb 26,
2016
09.00-10.00 Lecture 5 Carriage of oxygen and Carbon dioxide
Class room dr. Desak Wihandani
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Desak
Wihandani
EN
GL
ISH
CL
ASS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
17
6
Monday Feb 29, 2016
09.00-10.00 Lecture 6 Control of acid base balance, Arterial Gas Analysis (AGA)
Class room dr. Desak Wihandani
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Desak
Wihandani
7 Tuesday March 1,
2016
09.00-10.00 Lecture 7 Control of Respiratory Function and Blood Gas Analyzes
Class room Prof. Wiryana
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room Prof. Wiryana
8 Wednesday
March 2, 2016
09.00-10.00 Lecture 8 Pathology of Respiratory Tract
Class room dr. Winarti
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room dr. Winarti
9
Thursday March 3,
2016
09.00-10.00 Lecture 9 Lung Defense Mechanism
Class room dr. Winarti
10.00-16.00 Independent learning Practice : Physiology,
Pathology Anatomy (PA) Physiology: 2nd floor
dr. Muliarta
PA: Joint Lab (4th floor)
dr. Winarti
10 Friday
March 4, 2016
BKFK
11 Monday March 7,
2016
09.00-10.00 Lecture 10 Pharmacological and non pharmacological interventions
Class room Prof. Aman
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project
EN
GL
ISH
CL
ASS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
18
15.00-16.00 Plenary session Class room Prof. Aman
12 Friday
March 11, 2016
09.00-10.00 Lecture 11 Pharmacological and non pharmacological interventions
Class room Prof. Aman
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room Prof. Aman
13 Monday
March 14, 2016
09.00-10.00 Lecture 12 Respiratory Imaging
Class room dr. Elysanti
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Elysanti
14 Tuesday
March 15, 2016
09.00-10.00 Lecture 13 Bronchiolitis, asthma in children, Pneumonia
Class room dr. IB Subanada
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room dr. IB Subanada
15 Wednesday March 16,
2016
09.00-10.00 Lecture 14 TB in children, Difteri, Pertusis
Class room dr. Siadi Purniti
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr. Siadi Purniti
16 Thursday March 17,
2016
09.00-10.00 Lecture 15 Pulmonary TB and Extrapulmonary TB, TB in the Immunocompromised Host, Abses TB
Class room dr. Sutha,
dr. Bagiada
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room dr. Sutha,
dr. Bagiada
09.00-10.00 Lecture 16 Asthma, COPD
Class room Prof. IB Rai, dr. Artana
EN
GL
ISH
CL
ASS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
19
17 Friday
March 18, 2016
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room Prof. IB Rai,
dr. Artana
18 Monday
March 21, 2016
09.00-09.00 Lecture 17 Pleural effusion, Pneumothorax, Hematothorax
Class room dr. Andrika, dr, Yasa
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room dr. Andrika,
dr, Yasa
19 Tuesday
March 22, 2016
08.00-09.00 Lecture 18 Bronchitis and Bronchiectasis, Lung Ca and Smoking Cessation
Class room dr.Dewa Artika, dr. Saji
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project 15.00-16.00 Plenary session Class room dr.Dewa Artika,
dr. Saji
20 Wednesday March 23,
2016
09.00-09.30 09.30-10.00
Lecture 19 Disorder of nose, sinus
Class room
dr. Ratna, Sp.THT
12.00-13.30 Independent learning 13.30-15.00 SGD Disc room Facilitator 11.30-12.00 Break 10.00-11.30 Student project Hospital Visit 15.00-16.00 Plenary session Class room dr. Ratna,
Sp.THT
22 Monday
March 28, 2016
08.00-15.00
BCS: Spirometry BCS: WSD, Radio Imaging (Pre-test, lecture, demo Practice, discussion)
Class Room Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Muliarta dr. Yasa dr. Elysanti
23 Tuesday
March 29, 2016
08.00-15.00
BCS: Physical Diagnostic of Thorax BCS: Bronchoscopy BCS: THT (Pre-test, Lecture, practice, demo)
Class Room Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Saji dr. Sutha dr. Lely
EN
GL
ISH
CL
ASS

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
20
24 Wednesday March 30,
2016
08.00-15.00
BCS: Spirometry BCS: Physical Diagnostic of Thorax (Pre-test, lecture, practice, demo)
Class Room Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Muliarta dr. Saji
25 Monday
March 31, 2016
08.00-15.00
BCS: Physical Diagnostic of Thorax BCS: Provocation test BCS: THT (Pre-test, lecture, demo)
Class Room Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Saji dr Artana dr. Lely
26 Friday April 1, 2016
08.00-15.00
BCS: Physical Diagnostic of Thorax, Provocation test, Spirometry, WSD, Bronchoscopy, Radio Imaging, THT (Practice, post-test)
Class Room Physiology Dept. (2nd floor Joint Lab (4th Floor) Anatomy (1st floor)
dr. Saji dr Artana dr. Sutha dr. Muliarta dr. Yasa dr. Elysanti dr. Lely
27 Monday April 5,
2016 Examination

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
21
LEARNING PROGRAMS
LECTURE 1 ANATOMY OF RESPIRATORY TRACT
Abstract dr. I Nyoman Gede Wardana, M.Biomed
The respiratory system consists of conducting zone and respiratory zone. Conducting zone, whose walls are too thick to permit exchange of gases between the air in the tube and the blood stream. The nostrils (nares), nasal cavity, pharynx, larynx, trachea, bronchi, and terminal bronchioles are included in this zone. Respiratory zone, whose walls are thin enough to permit exchange of gases between tube and blood capillaries surrounding them. Air travels to the lungs through that zone. The right lung divided into three lobes: superior, middle, and inferior. The left lung divided into two lobes: superior and inferior. Each lung cover by a membrane that called pleura. Both lungs are inside the thoracic cage. The thoracic cage is formed by the vertebral column behind, the ribs, and intercostal spaces on other side and the sternum and costal cartilages in front. Below it separated from the abdominal cavity by diaphragm Learning Task Vignette 1: Kesawa, 32 years old, was seen in the clinic ten days ago, was diagnosed with rhinitis and sent home with instructions for increased fluids, decongestants, and rest. Kesawa presents today with worsened symptoms of malaise, low-grade temperature, nasal discharge, night time coughing, mouth breathing, early morning pain over sinuses, and congestion. The doctor diagnose he is suffering sinusitis.
1. Describe the boundaries of the nasal cavity and its blood supply 2. Describe the paranasal sinuses and its opening at nasal cavity
Vignette 2: Gotawa, a singer-18 years old came to clinic with complain a hoarse voice for 3 days. She also suffers sore throat, nose block, and fever. She was diagnosed laryngitis
1. Describe the structure of larynx and location of vocal cord 2. Describe the intrinsic and extrinsic muscle of larynx
Vignette 3: Mande, 30 years old male came to clinic with chief complaint difficulty to breath start from this morning. He also suffers cough, runny nose and fever. He has history bronchial asthma when he was 2 years old. The doctor diagnose he is suffering bronchial asthma.
1. Describe the structure of trachea 2. Describe the different between right and left main bronchus 3. Describe the principal different between trachea, bronchi, and bronchioles
Vignette 4: A 57-year-old male is admitted to the hospital with a chief complaint of shortness of breath for 2 weeks. The radiology examination shows a large left-side pleural effusion.
1. Describe the different between right lung and left lung 2. Describe the structure of pleura 3. Describe the structure of thoracic wall

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
22
LECTURE 2 HISTOLOGY OF RESPIRATORY TRACT
dr. Sri Wiryawan, MRepro Abstract The lower respiratory tract consists of : the lower part of the trachea, the two main bronchi, lobar, segmental, and smaller bronchi, bronchioles and terminal bronchioles, and last but not least is the end respiratory unit. These structure make up the tracheobronchial tree. As for the structure distal to the main bronchi along with a tissue known as the lung parenchyma. There are several structure we should also understand, when talking about lower respiratory tract. Several structures such as thorax, mediastinum, pleurae and pleural cavity, and lung. Thorax especially thoracic cavity and thoracic wall protect our lung and mediastinum and also play an important role in respiratory process. The mediastinum, which has a role in protecting our heart , located between the two lungs, and contains the heart and great vessels, trachea and esophagus, phrenic and vagus nerves, and lymph nodes. The pleurae covers the external surface of the lung, and is then reflected to cover the inner surface of thoracic cavity. Pleurae divided into the visceral (lines the surface of the lung) and parietal (lines the thoracic wall and diaphragm) one. The space between these two pleurae called as pleural cavity which contains a thin film fluid to allow the pleurae to slip over each other during breathing. The lungs are placed within the thoracic cavity. The lungs contain airways structure, vessels, lymphatic and lymph nodes, nerves, and supportive connective tissue. The trachea divides and form the left and right primary bronchi, which in turn divide to form lobar bronchi. Each lobar bronchi divide again to give segmental bronchi to supply air to bronchopulmonary segments. The tracheobronchial tree can also be classified into two functional zones: the conducting zone (proximal to the respiratory bronchioles) which involved in air movement, and the respiratory zone (distal to the terminal bronchioles) which involved in gaseous exchange. The other term to show functional structure of the lower respiratory tract is the acinus. The acinus defined as the part of the airway that is involved in gaseous exchange. The acinus consist of respiratory bronchioles, alveolar ducts, and alveoli as the smallest functional structure of the lung. The areas of lung containing groups of between three to five acini surrounded by parenchimal tissue are called lung lobules. The alveolus is an blind-ending terminal sac of respiratory tract. Most gaseous exchange occurs in the alveoli. The alveoli are lined with type I (structural) and type II (produce surfactant) of pneumocytes cell. The understanding about histological pattern of these functional structures of the lung is important in pathophysiology of lung problems. Learning Tasks
I. Structure of The Upper Respiratory tract Krishna, a man, 25 years old came to doctor Arjuna clinic with fever, sore throat, sneezing, runny nose and sometimes blocked nose. He also cannot smell well. The doctor diagnoses Krishna with acut Rhinopharingitis. 1. Describe the histological structure of the upper respiratory tracts
are involved ? 2. Describe the histological structure and function of epiglottis !
3. Compare the histological structure and function between vestibular fold and vocal fold !
II. Structure of The Lower Respiratory tract
Radha, a 17 years old beautiful girl, came to doctor Laksmi clinic with shortness of breath, wheezing and cough with phlegm. The doctor diagnoses Radha with Asthma.
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
23
1.Describe the histological structure of the lower respiratory tracts are involved ?
2.Compare the histological structure and function between terminal bronchioles and respiratory bronchioles !
3.Describe the histological structure of the interalveolar septum ! 4.Describe the histological structure of blood-air barrier ? 5.Describe about the pulmonary surfactant ?
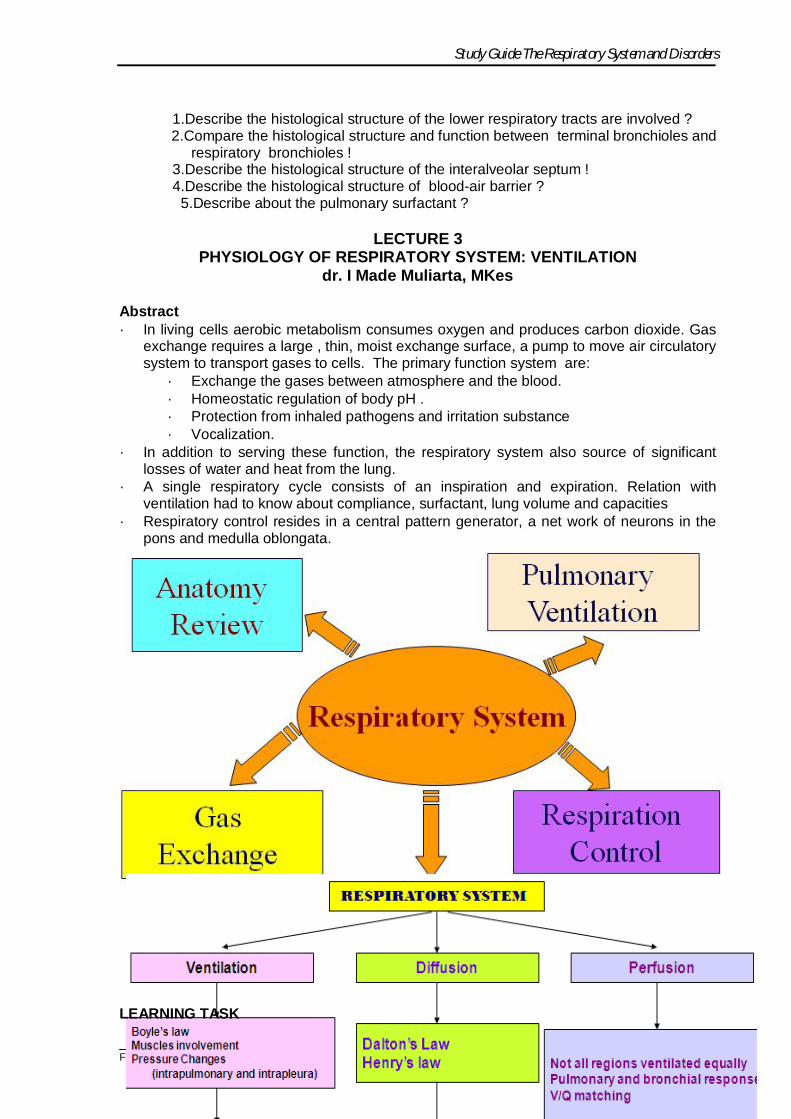
LECTURE 3
PHYSIOLOGY OF RESPIRATORY SYSTEM: VENTILATION dr. I Made Muliarta, MKes
Abstract · In living cells aerobic metabolism consumes oxygen and produces carbon dioxide. Gas
exchange requires a large , thin, moist exchange surface, a pump to move air circulatory system to transport gases to cells. The primary function system are:
· Exchange the gases between atmosphere and the blood. · Homeostatic regulation of body pH . · Protection from inhaled pathogens and irritation substance · Vocalization.
· In addition to serving these function, the respiratory system also source of significant losses of water and heat from the lung.
· A single respiratory cycle consists of an inspiration and expiration. Relation with ventilation had to know about compliance, surfactant, lung volume and capacities
· Respiratory control resides in a central pattern generator, a net work of neurons in the pons and medulla oblongata.
LEARNING TASK
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
24
dr. Muliarta, MKes 1. What is the sequence of event during quiet inspiration (muscle involvement, pressure
changes (intrapulmonary and intrapleura), volume changes) 2. What is pulmonary ventilation and alveolar ventilation means? 3. Andi, male, 30 years old, has a puncture wound due to car accident in his right chest
and penetrate his pleural cavity. The patient has complained shortness of breathing and doctor determine that his lung is collapsed. a. What is this condition called? b. Describe the mechanism of the lung collapse! c. What kind respiratory system compensation to anticipate this condition (lung
collapse) d. How can he still be alive in this condition?
4. Describe the Boyle’s Law!
LECTURE 4 PHYSIOLOGY OF RESPIRATORY SYSTEM: GAS EXCHANGE, DIVING,
ALTITUDE dr. I Made Muliarta, MKes
Abstract Gas exchange during external respiration occurs in respiratory membrane. Several factors may influence gas exchange. Dalton’s law and Henry’s law may apply during gas exchange. Some physiologic responses on respiratory system at high altitude and during diving. Some illnesses/injuries related pressure change may occurs at high altitude and during diving. LEARNING TASK dr. Muliarta, MKes 1. Describe the Dalton’s Law! 2. Describe the factors that influence oxygen diffusion from alveoli into the blood! 3. Predict the response of the pulmonary arterioles and bronchioles when PO2 increase
and PCO2 decrease! 4. Describe some illnesses/injuries due to high altitude 5. Describe some illnesses/injuries due to diving
LECTURE 5 CARRIAGE OF OXYGEN AND CARBON DIOXIDE
dr. Desak Wihandani
Abstract Gas Transport The supply of oxygen to the tissues is our most immediate physical need. We take in about 250 ml of oxygen gas per minute and this is our most pressing physical need. If our oxygen supply is interrupted for more than a few minutes, irreversible damage is done to some tissues, notably the brain. Oxygen is abundantly available in the air around us but cannot diffuse into our tissues at sufficient rate to meet our needs. It must be transported from the lung, the specialized organ for gas exchange, by the blood to all the other tissue. While oxygen has to be transported from lungs to tissues, carbon dioxide must be transported from the tissues for excretion by the lungs. Carbon dioxide has physicochemical properties that make its transport less difficult then transport of oxygen. Carbon dioxide can

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
25
be transported in the blood in three ways: in simple solution, by reversible conversion to bicarbonate and by reversible combination with haemoglobin to form carbamino haemoglobin. LEARNING TASK:
1. Describe the structure and function of hemoglobin 2. Describe the mechanism of oxygen binding to hemoglobin 3. Describe the differences between hemoglobin and myoglobin 4. Describe the mechanism of oxygen binding to myoglobin 5. Describe conformational differences between deoxygenated and oxygenated Hb! 6. Summarize the processes by which carbondioxide is transported from peripheral
tissues to the lungs
LECTURE 6 CONTROL OF ACID BASE BALANCE, ARTERIAL GAS ANALYSIS (AGA)
dr. Desak Wihandani Abstract Acid-Base Balance There is large daily flux of oxygen, carbon dioxide and hydrogen ion through the human body. Carbon dioxide generated in tissues dissolves in H2O to form carbonic acid, which in turn dissociates releasing hydrogen ion. The blood concentration of hydrogen ion is constant, it remains between 36 and 46 nmol/L (pH 7,36-7,46). Changes in pH will affect the activity of many enzyme and tissue oxygenation. Problems with gas exchange and acid-base balance underlie many diseases of respiratory system. Blood Gases Blood gas measurement is an important first-line investigation performed whenever there is a suspicion of respiratory failure or acid-base disorders. In respiratory failure, the results of such measurements are also an essential guide to oxygen therapy and assisted ventilation. The key clinically used parameters are pH, pCO2 and pO2, the bicarbonate concentration is calculated from pH and pCO2 values. Learning Task:
1. Describe organs in our body involved in acid-base balance, and how they work 2. Describe acid-base balance disorders! What is mean by : a. Respiratory
alkalosis, b. metabolic alkalosis, c.respiratory acidosis, and d. metabolic acidosis
3. In which condition respiratory acidosis and respiratory alkalosis occurs ? 4. What is the importance of blood gas measurement. To perform measurement
where are the blood sample taken from? What kind of measurement are done?
LECTURE 7
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
26
CONTROL OF RESPIRATORY FUNCTION Prof. Dr. dr. Wiryana, SpAn
Abstract
When considering contol of breathing, the main control variable is PaCO2 (we try to control this value near to 40 mmHg). This can be carried out by adjusting the respiratory rate, the tidal volume, or both. By controlling PaCO2 we are effectively controlling alveolar ventilation (see Ch.3) and thus PACO2. Although PaCO2 is the main control variable, PaO2 is also controlled, but normally to a much lesser extent than PaCO2. However, the PaO2 control system can take over and become the main controlling system when the PaO2 drops below 50 mmHg. Control can seem to be brought about by :
1. Metabolic demands of the body (metabolic control)-tissue oxygen demand and acid-base balance.
2. Behavioural demands of the body (behavioral control) – singing, coughing, laughing (i.e.control is voluntary). These are essentially feedback and feed-forward control systems, respectively. The
behavioural control of breathing overalys the metabolic control. Its control is derived from higher centres of the brain. The axons of neurons whose cell bodies are situated in the cerebral cortex bypass the respiratory centres in the brainstem and synapse directly with lower motor neurons that control respiratory muscles. This system will not be dealt with in this next;we shall deal only with the the metabolic control of respiration. Learning Tasks
1. Discuss the central control of breathing with reference to the pontine respiratory group and the dorsal-ventral respiratory groups of medulla spinalis
2. List the different types of receptors involved in controlling the respiratory system 3. Describe factors that stimulate central and peripheral chemoreceptor 4. outline the response of the respiratory system to change in carbon dioxide
concentration, oxygen concentration and pH. 5. discuss the mechanism thought to influence the control of ventilation in exercise 6. discuss the changes that occur in response to high altitude
LECTURE 8 PATHOLOGY OF UPPER AND LOWER URINARY TRACT
dr. Ni Wayan Winarti, SpPA
ABSTRACT
The term upper airways is used here to include the nose, pharynx, and larynx and their related parts. Disorders of these structures are among the most common afflictions of humans, but fortunately the overwhelming majority are more nuisances than threats. Inflammatory diseases are the most common disorders of the upper respiratory tract, i.e. rhinitis, sinusitis, pharyngitis, tonsillitis and laryngitis. It may occur as the sole manifestation of allergic, viral, bacterial or chemical insult. Although most infections are self-limited, they may at times be serious, especially laryngitis in infancy or childhood, when mucosal congestion, exudation, or edema may cause laryngeal obstruction. Tumors in these locations are infrequent but include the entire category of mesenchymal and epithelial neoplasms. Some distinctive types are nasopharyngeal angiofibroma, Sinonasal (Schneiderian) Papilloma, Olfactory Neuroblastoma and Nasopharyngeal Carcinoma.
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
27
Classification of lower respiratory tract (lung) diseases can be made based on the result of lung function test, although some authors prefer etiology and pathogenesis background. Some important diseases are obstructive lung disease (asthma, COPD, bronchiectasis) and restrictive lung disease (ARDS), and also infections, diseases of vascular origin and tumors. Pleura as protective structure of the lungs, are sometimes involved as secondary complication of some underlying disease, but in rare case, can be primary. Because of the complexity of respiratory disease, it is important to understand their pathogenesis, supported by recognizing their morphologic changes. LEARNING TASK Case 1 A male patient, 16 year old, came to a doctor with chief complaint difficulties in breathing. It has occurred since 1 month ago. This patient suffers from rhinitis alergica since he was 3 year old. On physical examination, a pedunculated nodule in right nasal cavity was found. It was whitish in color, 1.5 cm in diameter occluding the nasal cavity.
1. Based on clinical finding, what is the most possible diagnosis? 2. What are the DDs? 3. Describe the morphological appearance (macroscopy and microscopy) that
supposed to be found to confirm your diagnosis! 4. Explain the pathogenesis of this diasease!
Case 2 A male patient, 65 year old, has suffered from dyspnea and productive cough since 1 year ago. Lung function test showed increased of FEV1 with normal FVC (confirm an obstructive lung disease). He is a heavy smoker since he was 25 year old. No history of atopy. No evidence of cardiac disorders.
A. Mention 4 diseases including in the spectrum of obstructive lung disease! B. Explain their pathogenesis! C. Distinguish their morphology!
Case 3 A female patient, 50 year old, has suffered from tumor of right lung with pleural effusion. As the first step to confirm the diagnosis, doctor asked the patient to do cytology test.
A. Mention some cytology test can be choose for this patient! B. Among the test mention above (A), which one is the most simple and non-invasive?
And, discuss how to collect the specimen
LECTURE 9 LUNG DEFENCE MECHANISM
dr. Ni Wayan Winarti, SpPA
Abstract Respiratory tract is an organ that constantly exposed by contaminated air. It is there
fore a small miracle that the normal lung parenchyma remains sterile. Fortunately, a plethora of immune and non immune defense mechanisms exist in the respiratory system, extending from the nasopharynx all the way into alveolar airspaces.
The major categories of defense mechanisms to be discussed include : (1)physical or anatomic factors related to deposition and clearance of inhaled materials, (2)antimicrobial peptides, (3) phagocytic and inflammatory cells that interact with inhaled materials, (4)adaptive immune response, which depends on prior exposure to recognize the foreign
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
28
materials. Each components appears to have a distinct role, but a tremendous degree of redundancy and interaction exists among different components. Any condition breaks down the lung defense mechanism may result in lung injury and respiratory tract infections Learning Tasks
1. Defense mechanism of the lung and respiratory tract ca be divided into four major categories. Mention them, their components and explain how each of them acts against foreign materials.
2. Explain about diseases or conditions that break the lung defense mechanism down which result in increase susceptibility to respiratory tract infections
LECTURE 10 PHARMACOLOGICAL AND NON PHARMACOLOGICAL INTERVENSION I
Prof. dr. GM Aman
Abstract Drugs for cough, rhinitis, asthma bronchiale
Cough is a protective reflex mechanism that removes foreign material and secretions from the bronchi and bronchioles. It can be inappropriately stimulated by inflammation in the respiratory system or by neoplasia. In these cases, antitussive (cough suppressant) drugs are sometimes used. It should be understood that these drugs merely suppress the symptom without influencing the underlying condition. In cough associated with bronchiectasis or chronic bronchitis, antitussive drugs can cause harmful sputum thickening and retention. They should not be for the cough associated with asthma.
Most drugs used in rhinitis are effectively relief the symptom of rhinitis, not affect the underlying disease. No drug can relief symptom completely. Drugs are more effective for allergic rhinitis than non allergic rhinitis, and acute form of allergy respond more favorable than chronic form of allergy. The most common drugs used for rhinitis are antihistamine, nasal disodium cromoglycate, nasal decongestant, anticholinergic, intranasal corticosteroid.
Bronchial Asthma is a disease characterized by airway inflammation, edema and reversible bronchospasm. Bronchodilator and anti-inflammatory are the most useful drugs used in asthma. B2 selective agonists, muscarinic antagonists, aminophylline and leucotriene receptor blockers are the most effective bronchodilator. Anti-inflamatory drugs such as corticosteroid, mast cell stabilizers, leucotriene antagonists, and an anti IgE antibody are widely used. Short acting B2 agonist are the most widely used for acute asthma attack, by relaxing airway smooth muscle. Theophylline, aminophylline and antimuscarinic agent are also used for acute asthma attack. Long term control can be achieved with an anti-inflammatory agent such as corticosteroid (systemic or inhaled), with leucotriene antagonist, mast cell stabilizers (cromolyn or nedocromil). Long acting B2 agonists such as Salmeterol and Formeterol, are effectively in improving asthma control, when taken regularly. Learning Tasks Day 10 The patient complained about a sore throat and a nasty cough. It started two weeks ago with a cold. The cold was over within a week, but he continued coughing, especially at night. He is a heavy smoker. After physical examination you diagnosed a dry, tickling cough.

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
29
Task 1 1. Differentiate between Antitussive, Expectorant, Mucolytic 2. Differentiate the effects of Codeine, Dextromethorphan and Diphenhydramine 3. List the side effects of Codeine 4. In this patient, what kind of anti cough you give best. Task 2 If the patient also has sneezing, rhinorrhea and congested nose and then you diagnosed as rhinitis. 1. List the group of drugs used for Rhinitis 2. List the drugs used as oral nasal decongestant, and describe the important side effects. 3. List the side effects of intranasal decongestant 4. what is the drug of choice for patient suffer from Rhinitis Medicamentosa
LECTURE 11 PHARMACOLOGICAL AND NON PHARMACOLOGICAL INTERVENSION II
Prof. dr. GM Aman Task Day 11 If the patient come with cough, breathless, and in your examination, you found wheezing. After physical examination you diagnosed Acute attack of bronchial asthma. 1. Chose the drug of first choice for this patient 2. List the side effects of this drug 3. Compare the effect of this drug with Salmeterol 4. Theophyllin is a bronchodilator, but has a narrow safety margin. List the side effects &
toxic effect of Theophyllin. 5. Ipratropium not as effective as Salbutamol in treating bronchial asthma. What is the
main use of Ipratropium 6. Cromolyn and Nedocromil are often used for Asthma bronchial. Describe the
mechanism of action of Cromolyn (Disodium Cromoglycate) 7. To decrease the side effet of Corticosteroid in asthma patient, Corticosteroid often use
as inhaled Corticosteroid. What are the side effect of inhaled Corticosteroid 1. List the anticough that are contraindicated in acute asthma attack. 2. If you need anticough, what drug you give best
LECTURE 12 RESPIRATORY IMAGING
dr. Elysanti, Sp.Rad Abstract The imaging investigations of the chest may be considered under the following heading:
1. Simple X- Ray.(conventional X-ray) 2. Chest screening. 3. Tomography. 4. Bronchography. 5. Pulmonary angiography. 6. Isotope scanning. 7. Computed tomography(CT-scan) 8. MRI. 9. Needle biopsy.

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
30
The conventional Chest X Ray has to diagnose the anatomical disorders of the chest for example:
1. Lungs disease-----pneumonia, mass, atelectasis etc. 2. Pleural disease----pleural effuse, pneumothorax etc 3. Cardiac disease----cardiomegali 4. Bone disorders ----fracture 5. Soft tissue disease—emphysema cutis.
Sometimes conventional X-ray diagnostic can not enough for diagnostic of the chest disorders, for this the CT scan, MRI, bronchography and arteriography can be help. Learning Tasks A male patient, 68 years old, with chronic cough and hemoptoe. · What is the imaging choice for establish the diagnosis ? · What kind of diagnosis you will consider if the imaging revealed some consolidation at
the apex of the right lung accompanied by rib destruction? A 1- month old female patient is suffered from fever and dyspneu · What kind of abnormality you hope to see on the chect X ray film? · What do you thing about the diagnosis of the disease?
LECTURE 13 BRONCHIOLITIS AND
ASTHMA IN CHILD Dr. IB Subanada, SpA
Abstract Bronchiolitis is an acute inflammatory disease of the lower respiratory tract
(bronchioles) caused predominantly by respiratory syncytial virus (RSV). The inflammation response characterized by bronchiolar epithelial necrosis, bronchiolar occlusion, and peribronchiolar collection of lymphocytes. Bronchiolus become edematous and obstructed with mucus and celluler debris, which may lead to partial or complete collapse of the bronchioles. By the age 2 years nearly all children have been infected, with severe disease more common among infants aged 1-3 months. The clinical manifestation, initially upper respiratory signs and symptoms and followed by obstructed bronchioles signs and symptoms. The white blood cell and differential counts are usually normal. Chest x-ray reveals hyperinflation, peribronchial cuffing, and atelectasis. The mainstay of therapy is supplemented oxygen with close monitoring and supportive care. There are higher incidence of wheezing and asthma in children with history of bronchiolitis. Pooled hyperimmune RSV intravenous immunoglobulin (RSV-IVIG) and palivizumab intramuscular are effective to preventing severe RSV disease in high risk infants. The case fatality rate is less than 1%. Learning Tasks
A 6-months old male infant came to Outpatient Clinic, Department of Child Health, Medical School, Udayana University, Sanglah Hospital, Denpasar with the chief complaint of difficult to breath since yesterday. According to his mother, three days before, he suffered from coryza, cough, and low grade fever. On physical examination, fast breathing, wheezing and a prolonged expiratory phase were found. Please discuss his mother the disease of the infant!

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
31
Learning Tasks 1. explain the pathological concept of asthma in child 2. explain the clinical manifestations of asthma in child 3. explain the diagnosis principles of asthma in child 4. determine the severity of asthma and the degree of asthma attack in child 5. construct management plans for asthma attack in child (reliever) and determine the
need for controller management 6. abl to identify the need for referral
LECTURE 14 TB IN CHILD
dr. Ni Putu Siadi Purniti, SpA Abstract
Tuberculosis (TB) is systemic infection cause by Mycobacterium tuberculosis complex : M tuberculosis, M. Bovis, M. africanum, M. microti, and M. canetti. Tuberculosis infection occurs after inhalation of infective droplet nuclei containing M. tuberculosis. A reactive tuberculin skin test and the absence of clinical and radiographic manifestations are the hallmark of this stage. Tuberculosis disease occurs when sign and symptoms or radiographic changes becaome apparent. In the year 2001 prevalens rate of TB is 5,6/100.000 population, of these, 931 (6 % ) cases occurred in children < 15 year of age (rate 1,5/100.000 population). Transmission of M tuberculosis is person to person, usually by airborne mucus droplet nuclei, particles 1-5 µm in diameter that contain M tuberculosis. In the United States, most children are infected with M. tuberculosis in their home by adult patient tuberculosis close to them. The tubercle bacilli multiply initially within alveoli and alveolar duct. Most of bacilli are killed, but some survive within nonactivated macrophages, which carry them through lymphatic vessels to the regional lymph nodes. When the primary infection is the lung, the hilar lymph nodes ussualy are involved. The primary complex of tuberculosis includes local infection at the portal of entry ( primary focus) and the regional lymph nodes that drain the area. During the development of the primary complex, tubercle bacilli are carried to most tissues of the the body through the blood and lymphatic vessels.Pulmonary tuberculosis that occurs more than a year4 after the primary infection is usually caused by endogenous regrowth of bacilli persisting in partially encapsulated lesions. The majority of children with tuberculosis infection develop no signs or symptoms at any time. Occasionally, infection is marked by low grade fever and mild cough, and rarely by high fever, cough, malaise, and flu like symptoms. Several drugs are used to effect a relatively rapid cure and prevent the emergence of secondary drug resistance during therapy. The standard therapy of intrathoracic tuberculosis (pulmonary disease and/or hilar lymphadenopathy) in children, recommended by the CDC and AAP, is 6 month regiment of isoniazid (INH), rifampin (RIF) supplemented in the first 2 month of treatment by pyrazinamide (PZA). Learning Tasks In Outpatient Clinic Department of Pediatric, the baby 10 month of age carried by the mother with the chief complaint is loss of weight since 3 month, suffered low grade fever, chronic cough, malaise and flu like symptoms. The grandfather whom was diagnosed pulmonary tuberculosis and she has been in recent closed contact. In physical examination found that there were enlargement of neck lymph nodes. Learning Resources Nelson Textbook of Pediatrics Ed. 17 th 2004: pp 958-972

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
32
LECTURE 15 PULMONARY TB AND EXTRAPULMONARY TB
TB IN THE IMMUNOCOMPROMISED HOST dr. IB Sutha, SpP and dr. Bagiada, SpPD
PULMONARY TB AND EXTRAPULMONARY TB dr. IB Sutha, SpP Abstract
WHO estimates that about 9.27 million new cases in 2007 compared with 2.24 million cases in 2006, with 44% or 4.1 million cases of the infectious cases (sputum smear new cases with positive). TB problem in Indonesia is a national problem, the case is increasing and increasingly concerned with the increasing HIV infection and AIDS are rapidly growing emergence of multi-drug resistance TB problem.
Tuberculosis is an infectious disease directly caused by the bacteria Mycobacterium tuberculosis that primarily attacks the lungs. TB bacteria are rod-shaped, aerobic with a complex cell wall structure, it was mainly composed of fatty acids that are acid resistant and can survive in a dormant form.
TB germs enter through inhalation of the bacteria will reach the alveoli and catched by alveolar macrophages, the bacteria will die. If the germs stay alive it will proliferate to form primary apex (Primer Apex) and will limphogen or hematogenous spread. Primary apex surround by limphogen spreading form the "primary complex of Ghon" and formed specific cellular immunity is characterized by a positive tuberculin test. If the immunity is low, complex primary complications, the patient became ill and the symptoms and clinical signs of disease. M. tuberculosis may attack any organ of the body and most importantly the lungs.
Clinical symptoms involve respiratory symptoms and prodromal symptoms, whereas clinical signs obtained at once with the examination depends on the type and extent of lesions in the lungs and surrounding organs. Radiological examination of the thorax will get the infiltrates, fibrosis and kaverna. Bacteriological examination by smear and culture of sputum smear examination.
TB treatment follow national treatment program. Tuberculosis control which refers to the eradication of TB WHO guideline.
Objectives 1. Knowing the microbiology, epidemiology and pathogenesis of tuberculosis 2. Knowing the clinical symptoms, clinical and radiological signs of pulmonary TB and extra-pulmonary TB 3. Able to clasify Tuberculosis 4. able to explain treatment program of tuberculosis and side effect 5. Able to describe the prevention of tuberculosis and MDR TB
Triger A male patient aged 25 years came to a health center with complaints of bloody cough every time since one month ago. That was not originally phlegm but since two weeks ago a yellowish productive cough. The coughing did not disappear with anti-cough medicine. Shortness of breath and chest pain is absent. Patients feel the slightly fever and night sweating and also weakness, no appetite. Patients had never been sick before, enough food, smoking and family sometimes there is no similar illness. Physical examination has been found: look thin, alert state, blood pressure 110/70 mmHg; pulse rate 108 x/mnt; Respiration rate 24 breaths/mnt, T.aksila 370C. Lymph nodes enlargement on the right

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
33
neck. On chest examination: symmetrical right-left chest, normal heart, vesicular breath sounds in the chest and rhales on the third upright. Learning Tasks: 1. What should you do to ensure the diagnosis of this patient? 2. What should you do for this patient with enlargement of gland in the neck? 3. If the sputum smear examination results - / +2 / -, what is diagnosis? 4. Explain the treatment program appropriate to this patient! 5. Explain about patient monitoring and Communication-Information-and Education for this patient and his family? TB IN THE IMMUNOCOMPROMISED HOST dr. Made Bagiada, SpPD-KP Sebagai seorang dokter yang bekerja di tingkat pelayanan primer, pemahaman tentang diagnosis dan penatalaksanaan TB pada imunokompromais sangatlah penting. Kejadian TB lebih tinggi pada imunokompromais dibanding dengan non-imunokompromais. Penyakit infeksi kronik ini bila tidak ditangani dengan baik menyebabkan morbiditas dan mortalitas yang tinggi. Di Indonesia dengan beban TB tinggi (nomor 5 di dunia) akan lebih tinggi lagi dengan meningkatnya prevalensi penderita HIV/AIDS. TB adalah penyakit infeksi kronis yang disebabkan oleh M.tuberculosis. Tempat masuk dan target organ terbanyak adalah paru. Orang yang terinfeksi M.tuberculosis hanya sebagian kecil yang menjadi sakit TB dan sebagian besar tidak menjadi sakit (latensi). Orang yang tidak sakit (latensi) akan menjadi sakit (reaktivasi) atau TB aktif bila terjadi penurunan daya tahan tubuh atau imunitas (imunokompromais). Secara umum klinis TB ditandai dengan batuk-batuk produktif lebih dari 2 – 3 minggu disertai dengan gejala-gejala respiratorik lainnya dan gejala non-respiratorik. Namun, manifestasi klinis dari TB pada individu imunokompromais terletak pada derajat beratnya penurunan imunitas. Sering tanda dan gejala TB atipikal, sering terjadi kesalahan diagnosis, sehingga prognosis menjadi lebih buruk. Imunokompromais adalah suatu kondisi dimana sistem kekebalan tubuh seseorang melemah atau tidak ada. Individu yang imunokompromais kurang mampu melawan atau memerangi infeksi karena respon imun yang berfungsi tidak benar. Contoh orang imunokompromais adalah mereka yang terinfeksi HIV atau AIDS, wanita hamil, atau sedang menjalani kemoterapi atau terapi radiasi untuk kanker. Kondisi lain dengan imunokompromais, seperti kanker tertentu dan kelainan genetik, diabetes mellitus, dan penderita yang mendapatkan terapi TNF-α. Individu immunocompromised kadang-kadang lebih rentan terhadap infeksi serius dan /atau komplikasi dibanding orang sehat. Mereka juga lebih rentan untuk mendapatkan infeksi oportunistik, yaitu infeksi yang biasanya tidak mengenai orang yang sehat. Dalam keadaan penderita dengan imunokompromais, seorang dokter harus dapat mengenali penyakit TB aktif. Diagnosis TB pada imunokompromais adalah dengan menemukan kuman BTA pada sputum baik dengan pemeriksaan langsung BTA maupun kultur. Pengobatan TB penderita imunokompromais sama dengan pada non-imunokompromais dan pengobatan TB-nya diutamakan. Dokter harus mampu mengidentifikasi penderita TB pada imunokompromais yang tidak respon (resisten) dengan obat TB, sehingga dapat melakukan tindakan lebih dini untuk menurunkan perburukan prognosis (kematian).

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
34
Objektif
1. Mampu menjelaskan penegakan diagnosis TB pada imunokompromais 2. Mampu menyusun program pengobatan jangka panjang penderita TB pada
imunokompromais 3. Mampu mengidentifikasi kemungkinan gagal respon pengobatan (resisten) penderita
TB pada imunokompromais 4. Mampu menyusun pengobatan utama pada penderita TB dengan imunokompromais 5. Mampu mengidentifikasi penderita TB dengan imunokompromais yang perlu rujukan
lebih lanjut. Trigger Anda sebagai seorang dokter yang bekerja di sebuah Puskemas, datang seorang pasien laki-laki, usia 28 tahun. Dia mengeluhkan panas badan sejak lebih kurang 2 minggu. Demam tidak begitu tinggi dan tidak sampai menggigil. Disamping demam juga ada batuk-batuk ringan tanpa disertai dahak yang dialami lebih dari 1 minggu. Penderita sudah minum obat penurun panas dan obat batuk yang dibeli di warung tapi tidak ada kesembuhan. Berat badan penderita dirasakan menurun drastis belakangan ini. Napsu makan berkurang sehingga badan penderita dirasakan semakin kurus. Penderita adalah seorang sopir pengangkut barang jawa – bali, sudah menikah dan mempunyai anak wanita usia 4 tahun. Sesekali penderita minum bir. Penderita mempunyai tattoo di badannya yang dibuat sewaktu penderita klas 1 SMA. Tugas Diskusikan!
1. Jelaskan bagaimana Sdr memastikan bahwa pasien tersebut memang menderita TB dan imunokompromais!
2. Mengapa TB laten menjadi reaktivasi (TB aktif)? 3. Bagaimana Sdr mengenali pasien TB imunokompromais mengalami Immune
Reconstitution Inflammatory Syndrome (IRIS)? 4. Jika ternyata pasien tersebut menderita TB dengan imunokompromais bagaimana
cara menyusun pengobatan penderita? 5. Bagaimana cara menilai respon pengobatan TB pada pasien dengan
imunokompromais? 6. Jelaskan kriteria TB pada imunokompromais!
LECTURE 16
ASTHMA Prof. IB Rai
Abstract Airway hyper responsiveness is known as the denominator underlying all form of asthma. The basis of this abnormal bronchial response is not fully understood. Most current evidence suggests that bronchial inflammation is the substrate for this hyper responsiveness, manifested by the presence of inflammatory cells and by damage of bronchial epithelium. In extrinsic (allergic) asthma, bronchial inflammation is caused by type I hypersensitivity reactions, but in intrinsic asthma, the cause is less clear. Incriminated in such cases are viral infections of the respiratory tract and inhaled air pollutant such as sulfur dioxide, ozone and nitrogen dioxide.

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
35
Objektif: 1. Mampu menjelaskan penegakan diagnosis asma 2. Mampu menyusun program pengobatan jangka panjang asma 3. Mampu mengidentifikasi pasien dengan serangan asma akut. 4. Mampu memberikan pengobatan awal pasien dengan serangan asma akut. 5. Mampu mengidentifikasi pasien asma akut yang perlu perawatan inap di rumah
sakit, dan merujuknya Triger: Anda sebagai seorang dokter yang bekerja di sebuah Puskesmas kota, datang seorang pasien wanita, usia 36 tahun. Dia menyampaikan bahwa telah menderita asma sejak usia remaja. Dalam 3 bulan terakhir ini, dia mengalami serangan asma hampir setiap 3 hari , termasuk serangan di malam hari. Untungnya, kata pasien, serangan asmanya dapat diatasi dengan obat semprot yang dia miliki. Pasien menginginkan agar terbebas dari penyakitnya ini. Tugas: Diskusikan!
1. Jelaskan bagaimana Sdr. memastikan bahwa pasien tersebut memang menderita asma!
2. Apakah asma pasien tersebut dalam keadaan terkontrol? Jelaskan! 3. Apakah inhaler yang dipergunakan oleh pasien tersebut termasuk ke dalam
kelompok pelega (reliever)? Jelaskan perbedaan fungsi antara reliever dan controller, dan sebutkan obat-obat dari kedua kelompok tersebut!
4. Susun rencana penatalaksanaan jangka panjang pasien tersebut! 5. Apabila suatu saat pasien tersebut mengalami suatu serangan asma akut, terapi
apa yang akan Sdr. berikan? 6. Jelaskan kreteria serangan asma akut berat!
LECTURE 16 CHRONIC OBSTRUCTIVE PULMONARY DISEASE
dr. IGN Bagus Artana, SpPD Chronic Obstructive Pulmonary Disease (COPD) is a disease state characterized by airflow limitation that is not fully reversible. COPD is the fourth leading cause of death in the world and the number of patients is projected to increase worldwide in the future. Tobacco accounts for an estimate of 90% to the risk of developing COPD. Patient with COPD first complaining chronic cough with sputum and followed by dyspnea. This condition worsening progressively until the patient unable to do his daily activities. Treatment aim for COPD is to decrease symptom, without stopping the progression of this disease. Prevention is more important in this condition, such as by smoking cessation program. Objektif:
1. Mampu menjelaskan penegakan diagnosis PPOK serta penilaian kombinasi pasien 2. Mampu menyusun rencana pengobatan pada kasus PPOK stabil 3. Mampu menangani factor risiko pasien PPOK 4. Mampu menentukan eksaserbasi akut dari PPOK 5. Mampu menjelaskan manajemen gawat darurat pasien dengan PPOK
eksaserbasiakut Kasus: Seorang pasien laki-laki usia 70 tahun datang bersama anaknya kepoliklinik paru Rumah Sakit Daerah tempat anda bertugas dengan mengeluh sesak nafas. Sesak nafas dirasakan

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
36
sangat berat, berpakaian pun pasien mengaku sesak. Sebelumnya pasien memang merokok sejak usia 20 tahun sebanyak 2 pak sehari. Pasien juga mengatakan sering opname di rumah sakit karena serangan sesak nafas yang sangat berat. Pasien dan keluarganya ingin mengetahui dengan pasti mengenai penyakitnya serta tindak lanjut penanganannya. Tugas: Diskusikanlah mengenai:
1. Jelaskan bagaimana penegakan diagnosis pasien tersebut 2. Bagaimanakan kombinasi penilaian pasien ini? Data apa saja yang saudara
perlukan untuk melengkapi kombinasi penilaian tersebut 3. Sebutkan dan jelaskan obat-obat yang dapat digunakan untuk menangani kasus
PPOK stabil 4. Bagaimana anda menyusun rencana penatalaksanaan pasien ini secara
komprehensif? 5. Bagaimana penatalaksanaan pasien ini apabila mengalaami PPOK eksaserbasi akut
?
LECTURE 17 PLEURAL EFFUSION
dr. Putu Andrika, SpPD-KIC PNEUMOTHORAX dr. Yasa, SpBTKV
PLEURAL EFFUSION dr. Putu Andrika, SpPD-KIC
Membran tipis pleura terdiri dari dua lapisan yaitu pleura visceralis dan pleura parietalis. Penumpukan cairan melebihi jumlah fisiologis 10-20 ml disebut efusi pleura, akibat dari peningkatan produksi yaang melebihi kemampuan absorpsi. Penting untuk menegakkan diagnosis berdasarkan anamnesis yang baik dan pemeriksaan fisik yang teliti, pemeriksaan radiologi torak serta melakukan pungsi pleura. Analisis cairan pleura akan sangat berguna untuk menuntun kearah penyebab efusi pleura. Dibedakan cairan efusi yang transudat dan eksudat. Volume efusi pleura yang banyak akan menimbulkan gangguan fungsi respirasi yang memerlukan pengeluaran cairan efusi melalui aspirasi cairan pleura (torako sentesis) atau melalui pemasangan chest cube (Water Seal Drainage). Dalam mengelola pasien dengan efusi selain menangani keluhan akibat menumpuknya cairan efusi juga harus menangani penyebab terjadinya efusi tersebut. Objektif:
1. Mampu menjelaskan penegakan diagnosis efusi pleura 2. Mampu menilai analisis cairan pleura 3. Mampu merencanakan pemeriksaan penunjang untuk mendapatkan penyebab
terjadinya efusi pleura. 4. Mampu mengidentifikasi kasus yang memerlukan penanganan segara dan
kasus yang harus dirujuk ke rumah sakit. Triger: Seorang wanita muda datang dengan keluhan sesak nafas yang semakin memberat sejak seminggu. Pada pemeriksaan fisik didapatkan frekwensi nafas 24x/mnt, suhu tubuh 37,5 o C, pemeriksaan torak asimetris, kanan tertinggal, perkusi redup dan suara nafas melemah di bagian kanan bawah. Penderita juga mengeluh batuk batuk sejak 3 bulan yang lalu dan pernah batuk berisi darah segar sedikit, juga nampak semakin kurus.

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
37
Tugas: Diskusikan
1. Apakah kemungkinan penyebab keluhan pasien tersebut? 2. Pemeriksaan penunjang apa yang diperlukan? 3. Perlukah melakukan parasentesis? (jelaskan) 4. Perlukah pemasangan WSD, apa alasannya?
PNEUMOTORAKS dr. Yasa, SpBTKV Pneumotoraks merupakan salah satu kegawatdaruratan di bidang paru yang berarti terisinya rongga pleura oleh udara. Pneumotoraks ini perlu mendapatkan perhatian serius, karena dengan penanganan yang cepat dan tepat akan sangat mengurangi angka kematiannya. Sebagai seorang dokter yang ada di fasilitas kesehatan primer, sangat diperlukan pengetahuan mengenai keadaan ini. Diagnosis pneumotoraks dapat ditegakkan dari anamnesis, pemeriksaan fisik dan foto polos dada. Pneumotoraks dapat dibagi berdasarkan berbagai kriteria, tetapi yang paling sering adalah dibagi menurut terjadinya (pneumotoraks artifisial, traumatic, serta spontan) serta berdasarkan jenis fistelnya (pneumotoraks terbuka, tertutup, dan ventil). Beberapa kondisi pneumotoraks akan sangat mengancam nyawa, sehingga memerlukan penanganan yang tepat dan segera. Penatalaksanaan pneumotoraks pada prinsipnya adalah mengeluarkan udara yang ada di rongga pleura tersebut, terapi penyebabnya, serta edukasi untuk mencegah berulangnya pneumotoraks pada pasien yang memiliki risiko. Objektif:
1. Mampu menjelaskan penegakan diagnosis pneumotoraks 2. Mampu menyebutkan beberapa penyebab pneumotoraks yang sering dijumpai 3. Mampu menjelaskan beberapa pembagian jenis pneumotoraks 4. Mampu menyusun rencana penatalaksanaan pasien dengan pneumotoraks
Kasus: Seorang pasien laki-laki usia 30 tahun datang kePuskesmas tempat anda bertugas dengan mengeluh sesak nafas tiba-tiba dan sangat berat. Pasien sebelumnya dengan riwayat menderita penyakit TB paru dan sudah berobat dengan lengkap. Sebelumnya pasien sempat terbatuk-batuk, kemudian tiba-tiba sesak nafas. Pasien ini tampak sesak dan sianosis. Tugas: Diskusikan mengenai
1. Jelaskan temuan fisik dan foto polos dada yang kemungkinan ditemukan pada pasien pneumotoraks tersebut
2. Sebutkan beberapa penyebab pneumotoraks yang anda ketahui 3. Bagaimana penatalaksanaan kasus dengan pneumotoraks tersebut ?
LECTURE 18 BRONCHITIS AND BRONCHIECTASIS
dr.Dewa Artika, SpP
LUNG CA AND SMOKING CESSATION dr. Gede Ketut Sajinadiyasa, SpPD
BRONKITIS dan BRONKIEKTASIS dr. Dewa Made Artika, SpP Untuk menentukan suatu Bronkitis dan Bronkiektasis tidaklah terlalu sulit, tapi diperlukan suatu pemahaman untuk mendiagnosis dan penatalaksanaan Bronkitis dan Bronkiektasis
Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
38
dengan baik dan benar. Disamping prevalensinya cukup tinggi, penyakit ini bila tidak ditangani dengan baik, akan berlanjut menjadi lebih parah. Bronkitis adalah inflamasi saluran napas sentral yang mengenai mukosa ditandai oleh batuk dengan dahak, sering disertai dengan panas dan sesak.Bronkiektasis adalah kelainan pada dinding bronkus besar dan sedang berupa kelemahan otot sehingga terjadi pelebaran lumen, karena proses infeksi transmural dan pelepasan mediator. Diagnosis Bronkitis berdasarkan pada anamnesa, pemeriksaan fisik dan foto toraks, sedang bronkiektasis ditegakkan dengan anamnesa, pemeriksaan fisik, foto toraks, CT Scan, dan kultur sputum. Prinsip penatalaksanaan Bronkitis dan Bronkiektasis adalah dengan menghilangkan batuk dan produksi dahak. Bila disertai tanda infeksi dapat ditambahkan antibiotika. Pada Bronkiektasis perlu dilakukan Chest Fisioterapi atau bronkoskopi untuk mempermudah pengeluaran sputum. Pada keadaan eksaserbasi sering disebabkan oleh infeksi apakah viral atau bakteri. Obyektif
1. Mampu menjelaskan penegakan diagnosis bronkitis dan bronkiektasis 2. Mampu menyususn program pengobatan jangka panjang 3. Mampu mengidentifikasi pasien dengan keadaan eksaserbasi 4. Mampu memberikan pengobatan awal pasien dengan serangan akut 5. Mampu mengidentifikasi pasien eksaserbasi yang perlu rawat inap dan merujuknya.
Kasus Seorang penderita laki umur 35 th datang dengan keluhan : batuk berdahak sejak 3 bulan dan memberat sejak 5 hari yang lalu dan disertai dengan panas badan. Bila diperhatikan dahaknya ada 3 lapis yaitu dari atas sampai bawah mulai dari yang bening sampai keruh dan batuknya terutama pagi hari. Dikatakan pula setahun lalu pernah menderita sakit seperti ini dan kadang disertai sesak napas, bila dahaknya sulit dikeluarkan. Tugas Diskusikan
1. Jelaskan bagaimana sdr. Memastikan bahwa pasien tsb. menderita bronkitis 2. Bagaimana sdr membedakan dengan bronkiektasis. 3. Apakah penderita tsb dalam keadaan eksaserbasi, jelaskan 4. Jelaskan prinsip pengobatan pasien dg bronkitis dan bronkiektasis 5. Obat-obat apa saja yang diperlukan pada pasien tsb diatas 6. Apa yang dikerjakan bila sputum pasien tsb diatas sulit dikeluarkan
KANKER PARU (LUNG CANCER) dr. Gede Ketut Sajinadiyasa, SpPD Kanker Paru merupakan penyebab kematian tersering diantara kematian oleh karena kanker di seluruh dunia baik pada laki-laki ataupun perempuan. Insiden kanker paru di dunia diperkirakan 1,3 juta kasus per tahunnya. Kanker paru terjadi sebagai akibat proses yang komplek antara paparan karsinogen dan kerentanan genetik. Faktor kebiasaan dan lingkungan berhubungan dengan terjadinya kanker paru dan merokok merupakan faktor risiko utama. Jenis histologi kanker paru sebagian besar adalah Small Cell Lung Cancer (SCLC) dan Non Small Cell Lung Cancer(NSCLC) . NSCLC terdiri atas squamus cell carcinoma, adeno carcinoma dan large cell carcinoma. Manifestasi klinis dari kanker paru dapat asimtomatik pada stadium awal dan baru bergejal pada stadium lanjut. Pasien biasanya datang dengan keluhan batuk, batuk darah, sesak, nyeri dada dan suar serak. Sering juga dijumpai tanda-tanda syndrome paraneoplastik dan gejala umum seperti anoreksia, asthenia dan berat badan yang menurun. Diagnosis kanker paru dapat ditegaknya dengan anamnesis, pemeriksaan fisik dan pemeriksaan penunjang. Pemeriksaan penunjang yang umum dikerjakan seperti sitologi sputum, rontgen dada, ct scan toraks, Biopsi(FNAB/TTB), bronkoskopi, PET scan dan lainnya. Setelah diagnosis ditegakkan dan sebelum memulai pengobatan ditentukan stadium penyakit dan status performan. Dengan diketahuinya jenis histology dan stadium

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
39
penyakit kemudian ditentukan modalitas terapi. Modalitas terapi pada pasien kanker paru diantaranya adalah pembedahan, kemoterapi, radiasi dan target terapi Objektif
1. Mengetahui pathogenesis , faktor risiko dan usaha preventif kanker paru 2. Dapat mengetahui klasifikasi kanker paru 3. Mengetahui proses penegakan diagnosis dan stadium kanker paru 4. Mengetahui modalitas penunjang dalam penegakan diagnosis 5. Mengetahui modalitas terapi kanker paru dan merujuk
Triger Seorang pasien laki-laki umur 65 tahun datang ketempat pratek saudara sendirian dengan keluhan batuk berdarah. Satu minggu yang lalu pasien sempat menjalani cek up didapatkan pada foto rontgen dada, tumor dengan ukuran diameter 2,5 cm pada hilus kiri menempel di pinggang jantung kiri. Pada pemeriksaan USG abdomen didapatkan tumor multiple ukuran diameter sekitar 1-1,5 cm pada hati, sedang pemeriksaan yang lain dalam batas normal. Pasien memiliki kebiasaan merokok sejak umur 20 tahun dengan jumlah 1-2 bungkus per harinya. Tugas
1. Apa yang saudara lakukan untuk memastikan diagnosis pasien ini? 2. Kalau diperlukan tindakan invasive, prioritas tindakan yang saudara usulkan?
Jelaskan alasannya! 3. Bila ini kanker paru, apa kemungkinan klasifikasi histologinya? 4. Tentukan stadium pasien ini dan status performannya serta alasannya! 5. Tentukan modalitas terapinya!
LECTURE 19
DISORDERS OF NOSE AND SINUS dr. Ratna, SpTHT
Abstract Nasal foreign bodies are commonly encountered in emergency departments.
Although more frequently seen in the pediatric, they can also occur in adult. Children’s interests in exploring their bodies make them more prone to lodging foreign bodies in their nasal cavities.
References
1. Textbook Diseases of the Ear, Nose and Throat edited by Martin Burton CHURCHILL LIVINGSTQNE 15TH ED 2000: Section 5 The Larynx, Pharynx and Oesophagus. Pp 165-206
LECTURE 20 DISORDERS OF PHARYNX AND LARYNX
Prof. Suardana, SpTHT, dr. Dewa Artha Eka Putra, SpTHT
Abstract

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
40
The Adenoids (pharyngeal tonsils) are a triangular mass of lymphoid tissue located
on the posterior aspect of the boxlike nasopharynx. The nasopharynx serves as a conduit for Inspired air and Sinonasal Sections that drain from the nasal cavity into the oropharynx. a resonance box for for speech and a drainage area for the Eustachian tube — middle ear mastoid complex. Adenoid have three types of Surface epithelium ciliated pseudostratified squamous, and transitional.
The Adenoids and tonsils, like all lymphoid tissue, enlarge when infected. Although lymphoid tissue does act to fight infection. Some time bacteria and viruses can lodge within it and survive. Group A B—hemolytic streptococcus (GABHS) is classically described as the only bacterium implicated frequently in acute Adenoiditis or tonsilitis.
Chronic infection, either viral or bacterial, can keep the pad of adenoids enlarged for years, even into adulthood. Some viruses, Such as the Epstein Barr virus, can cause dramatic enlargement of lymphoid tissue.
Clinical classification of the adenoid : Acute adenoiditis, recurrent Acute Adenoiditis, chronic adenoiditis and obstructive Adenoid Hyperplasia. Clinical classification of the tonsils: acute tonsillitis, recurrent acute tonsillitis, chronic tonsillitis, and obstructive tonsilar hyperplasia.
The main symptoms of adenoid diseases is Rhinorhea, chronic nasal obstruction (associated with Snoring and obligate mouth breathing), malodorous, cough, post nasal drip, sinusitis, otitis media and a hyponasal voice. The main symptomsof tonsils diseases are: sore throat, dysphagia, fever, halithosis, muffled voices, snoring, and other symptomsof sleep disturbance and tender cervical adenopathy.
Adenoiditis is best diagnosed by clinical history, physical examination. nasopharyngoscopy and Radiography. The physical examination should include both anterior and posterior rhinoscopy. A lateral neck Radiograph and Sinus Radiography taken to show soft tissue density, can show the adenoids and sinus. Tonsilitis is diagnosed by clinical history, physical examination, throat culture, and flexible laryngoscope.
Management of diseases of the adenoids and tonsils: antimicrobial, intranasal steroids and adenoidectomy. Indications for tonsillectomy and adenoidectomy are obstruction, infection and Neoplasia.
The anatomy of the larynx consist of cart.Haginous framework bound together by ligaments and covered with muscle and mucous membrane. The most important cartilage is the arytenoid cartilages which is can rotate and slide on the cricoid cartilage and thus play an important role in the movement of the vocal cords. The epiglottis is a leaf-shape cartilage of the larynx which is attached to the base of the tongue by the glossoepiglottic ligament and inner part of thyroid cartilage. The thyroid cartilage is that which makes the prominence upon the front of the neck known as ‘Adam’s apple, particularly visible in man. Interior of the larynx can looking down by laryngoscopy indirect or direct. The function of the larynx includes protection of lower respiratory tract and phonation. The protection of respiratory tract acting by the epiglottis, sensory nerve supply which is produce cough and vocal cords. Voices or phonation is produce by vocal cords function consist adduction and abduction movement and vibration of the vocal cords.
Patient with a foreign body in his/her pharynx, or oesophagus, usually knows what has happened and is usually right. It can stick in his tonsils, his vallecula, his pyriform fossa, or in his postcricoid region. Most fish bones stick in accessible regions, usually the back of the tongue or tonsils. Foreign bodies seldom stick in the larynx itself, except when an affluent, elderly, and often intoxicated diner gets a piece of steak caught in his larynx, as a result of which he gasps and collapses. Treat him immediately.

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
41
Throat
Normal Vocal cord and disorders The symptoms of laryngeal disorders are hoarseness, dysphonia and stridor.
Hoarseness is caused by an abnormal flow of air past the vocal cords. The voice is harsh when turbulence is created by the irregularity of the vocal cords. The irregularity of the vocal cord caused by vocal nodule, edema of the vocal cord and laryngitis. Dysphonia is weakness of the voice caused by paresis or paralysis of the vocal cords. And aphonia is loss of voice. Stridor is a high pitch sound, is produce by lesion that narrowing the airway. If narrowing of the airway upper the vocal cord produce inspiratory stidor, and if narrowing the airway below the vocal cord will produce inspiratory and expiratory stridor.
Some lesion will be discussed are vocal cord nodule, vocal cord paralysis, laryngeal palillomas and gastrolaryngopharyngeal reflux disease. Vocal nodule or Singer’s nodes is benign lesion in the vocal cord particularly at the site of the junction of the anterior third and posterior two-thirds of the cord (halfway along the membranous cord). This condition is caused by misuse of the voice or overuse as well as singers, teachers, priest, actors who have not undergone formal voice training. Misuse of the voice also happen in the schoolchildren, sometime call by screamer’s node.
Vocal cord paralysis causes of dysphonia symptom, define as weakness or even though temporary loss of the voice (aphonia). A vocal cord may paralysed by mechanical fixation of the arytenoids or vocalis muscle or by nerve paralysis. Paralysis may be unilateral or bilateral and the cords paralysed in abduction or adduction. Abduction paralysis causes loss of the voice because the cord can not move to the midline position and adduction paralysis, the cords can not move to the lateral position and cause severe stridor.
Laryngeal papilloma is a benign lesion single or multiple, non keratinizing papilloma in characteristic is due by infection of human papilloma virus type 6 and 11. Papillomatosis present more frequently in children than in adult, the peak incidence occurring between 2

Study Guide The Respiratory System and Disorders
Faculty of Medicine Udayana University,DME
42
and 5 years of age, and very common of high recurrent. Relaps or recurrent may be precipitated by trauma or immunosuppressive condition.
Gastrolaryngeal reflux is very common condition to causes hoarseness. The pathology of gastro-esophageal-laryngeal reflux disease may be a result of direct effect of gastric acid, bile salts or enzymes on mucosa of the larynx. Learning Tasks 1. Describe and discuss of specific symptoms of the larynx disease & disorders. 2. Describe and discuss etiology and patophysiology of hoarseness, dysphonia and stridor
with its clinical implication 3. Manage and provide initial management or refer patient with certain larynx disease and
disordes
Learning Tasks 1. Describe and discuss of etiology of adenoid diseases. 2. Explain pathogenesis of adenoid diseases. 3. Describe and discuss of clinical classification of diseases in the adenoids 4. Describe clinical evaluation to support diagnosis of the adenoid diseases. 5. Manage and provide initial management or refer patient with certain adenoid
diseases. 6. Explain indications for adenoidectomy. 7. Describe complications of adenoid diseases and adenoidectomv.
Learning Resources
1. Textbook Diseases of the Ear, Nose and Throat edited by Martin Burton CHURCHILL LIVINGSTQNE 15TH ED 2000: Section 5 The Larynx, Pharynx and Oesophagus. Pp 165-206
2. Textbook Current Medical Diagnosis & Treatment Edited by Lawrence M.Tierney,Jr. Stephen J.Mc Phee, Maxine A.Papadakis 45 Ed 2006: Diseases of the Larynx p209-213
3. Linda Brodsky. Christhopher Poje. Tonsilitis, Tonsillectomy and Adenoidectomy. In BaiIe BJ Editor. Head and Neck Surgery-Otolaryngologv 3 ed. Philadelphia Lippincort Williams and Willkins; 2001 p 979— 991.