study on tobacco and women - amazon s3s3.amazonaws.com/zanran_storage/ · table 2.3 age-sex...
TRANSCRIPT
Regional Situation Analysis of Women and Tobacco in South-East Asia
Conducted for World Health Organization – Regional Office for South-East Asia
By: Dr. Nyo Nyo Kyaing

Contents
ACKNOWLEDGEMENTS i CONDUCTING THE STUDY ii EXECUTIVE SUMMARY iv
INTRODUCTION 1 PART ONE: BASIC INFORMATION Demography 5 Health Status Indicators 7 Development Indicators 9 Literacy and Education 12 PART TWO: PREVALENCE OF TOBACCO USE AMONG FEMALES IN SOUTH-EAST ASIA REGION
14
Types of tobacco products used in South-East Asia Region 14 (A) Main commercial smoking products 14 (B) Main smokeless tobacco products 15 Bangladesh 16 Prevalence of tobacco use among females in Bangladesh 16 Types of tobacco products used in Bangladesh 19 Trends of annual consumption of cigarettes in Bangladesh 20 Expenditure for tobacco by Bangladeshi women 21 Bhutan 23 Prevalence of tobacco use among females in Bhutan 23 Types of tobacco products used in Bhutan 23 Democratic People’s Republic of Korea 24 Consumption of manufactured cigarettes 24 India 25 Prevalence of tobacco use among females in India 25 Types of tobacco products used in India 27 Prevalence of tobacco use among female youth in India 27 Trend of annual consumption of manufactured tobacco products in India
28
Indonesia 29 Prevalence of tobacco use among females in Indonesia 29 Prevalence of tobacco use among female youth in Indonesia 32 Types of tobacco products used in Indonesia 32 Trend of tobacco products consumption in Indonesia
33
Maldives 34 Prevalence of tobacco use among females in Maldives 34 Types of tobacco products used in Maldives 34 Annual consumption of tobacco products in Maldives 36 Myanmar 37 Prevalence of tobacco use among females in Myanmar 37 Prevalence of smoking among female youth in Myanmar 40 Types of tobacco products used in Myanmar 40 Annual consumption of tobacco products in Myanmar 43 Nepal 44 Prevalence of tobacco use among females in Nepal 44 Prevalence of smoking among female youth in Nepal 46 Types of tobacco products used in Nepal 46 Annual consumption of tobacco products in Nepal 47 Sri Lanka 48 Prevalence of tobacco use among females in Sri Lanka 48 Prevalence of tobacco use among female youth in Sri Lanka 50 Types of tobacco products used in Sri Lanka 50 Annual consumption of tobacco products in Sri Lanka 51 Thailand 52 Prevalence of tobacco use among females in Thailand 52 Prevalence of smoking among Thai Youth 54 Types of tobacco products used in Thailand 54 Annual consumption of manufactured cigarettes in Thailand 55 PART THREE: HEALTH CONSEQUENCES OF TOBACCO USE 58 Health risks for women who smoke 58 Cancers Cardio-vascular diseases 59 Reproductive Health 59 Others 60 Health Consequences for women who are exposed to ETS 60 Health risks for women who use smokeless tobacco 60 Burden of diseases attributable to smoking 61 Burden of diseases attributable to smoking in South-East Asia Region 62 BANGLADESH 67 Morbidity from Tobacco Use in Bangladesh 67 Morbidity due to Second-hand Smoking in Bangladesh 67 Mortality from Tobacco Use in Bangladesh 68 BHUTAN 69 Morbidity and Mortality from Tobacco Use in Bhutan 69 Democratic People’s Republic of Korea 70 Morbidity and Mortality from Tobacco Use in DPR Korea 70

INDIA 71 Morbidity due to smokeless tobacco use in India 71 Morbidity due to smoking in India 71 Morbidity due to exposure to ETS in India 72 Mortality from tobacco use in India 73 INDONESIA 76 Morbidity from tobacco use in Indonesia 76 Morbidity from exposure to ETS in Indonesia 80 Mortality from tobacco use in Indonesia 82 Maldives 84 Morbidity from tobacco use in Maldives 84 Mortality due to tobacco use in Maldives 85 Myanmar 86 Morbidity due to tobacco use in Myanmar 86 Studies on health consequences of tobacco in Myanmar. 90 Morbidity due to ETS in Myanmar 91 Mortality due to tobacco use in Myanmar 91 NepaL 93 Morbidity due to tobacco use in Nepal 93 Morbidity due to Exposure to Environmental Tobacco Smoke in Nepal 93 Mortality due to tobacco use in Nepal 93 Sri Lanka 96 Morbidity due to tobacco use in Sri-Lanka 96 Morbidity due to exposure to ETS in Sri-Lanka 96 Mortality due to tobacco use 96 Thailand 98 Mortality from tobacco use in Thailand 98 PART FOUR: WOMEN IN THE TOBACCO EMPLOYMENT 105 Women in the tobacco employment 105 Occupational hazards of tobacco employment in South-East Asia Region. 106 PART FIVE: CAMPAIGNING AGAINST TOBACCO 109 PART SIX : CONCLUSIONS AND RECOMMENDATIONS 114 ANNEX: 120
TABLES
Table 1.1 Demographic Indicators of South-East Asia Region……………………... 6
Table 1. 2 Female adult population 15 years and above (millions)………………….. 7
Table 1. 3 Health Status Indicators in South-East Asia Region……………………… 8
Table 1.4 Infant, Maternal and Under Five Mortality Rates in South-East Asia
Region……………………………………………………………………. 9
Table 1.5 Components and calculation of Human Development Indicators of
South-East Asia Region, 1999………………………………………….... 10
Table 1.6 Percentage or population living in poverty in selected countries of the
South-East Asia Region…………………………………………………... 11
Table 1.7 Human Poverty Index (HPI-1) in selected countries of South-East Asia
Region, 2000……………………………………………………………… 11
Table 1.8 Gross primary and secondary enrolment ratios in selected countries of the
South-East Asia Region, 1990- 1996……………………………………... 12
Table 2.1 Prevalence of tobacco use among females in Bangladesh………… …….. 16
Table2.2 Estimated female population by age and smoking rates, Bangladesh,
1996 ……………………………………………………............................ 17
Table 2.3 Age-sex specific female prevalence of smoking (%) by age group and
region (Current smokers), Bangladesh, 2001. .......................................... 17
Table 2.4 Female prevalence of smoking (%) by education group and region
(Current smokers), Bangladesh, 2001………………………………….... 19
Table 2.5 Prevalence of tobacco use (%) among females for different types of
tobacco products by region (Current users), Bangladesh, 2001…………... 19
Table 2.6 Trend of Annual Consumption of Cigarettes and Bidis, Bangladesh,
(1975-1999)……………………………………………………………….. 21Table 2.7 Average Daily Expenditure on Tobacco by females, Bangladesh,1995….. 22
Table 2.8 Average Daily Expenditure for Tobacco by females, Bangladesh, 1997… 22
Table 2.10 Prevalence of tobacco use among females, India (1987-88 to 1998-99)…. 25
Table 2.11 Prevalence of tobacco use among females (from different sources)
India, (1987-88 to 2001)………………………………………………….. 27
Table 2.12 Tobacco use among female school-going children aged 13-15 years,
India………………………………………………………………………. 28
Table 2.13 Trend of Annual Consumption of Cigarettes and Bidis, India
(1970-1999)………………………………………………………………. 28
Table 2.14 Prevalence of female smoking by age group, Indonesia (1993-2001)……. 30
Table 2.15 Tobacco use prevalence (smoking and smokeless) among females by
age group, Indonesia (1993 to 1998)…………………………………….. 31
Table 2.16 Selected Prevalence Surveys on smoking in Indonesia…………………... 31
Table 2.17 Youth female Smoking in Indonesia, (1985 -2000)………………………. 32
Table 2.18 Prevalence of tobacco use for population 15 years and above, by sex and
tobacco product, Indonesia, 1998 ………………………………………... 33
Table 2.19 The average number of cigarettes consumed by female smokers,
(in pieces annually), Indonesia, 1995…………………………………….. 33
Table 2.20 Annual Consumption of manufactured cigarettes, Indonesia (1970-2000). 34
Table 2.21 Prevalence of female smoking by age group, Maldives (1997, 2001)…… 34
Table 2.22 Prevalence of female smoking by age group, Maldives ( 2001)…………. 35
Table 2.23 Annual Consumption of manufactured cigarettes………………………… 36
Table 2.24 Prevalence of tobacco use among females > 15 years, Myanmar, 2001…. 37
Table 2.25 Prevalence rates of smoking among females from specific studies
conducted in Myanmar…………………………………………………… 38
Table 2.26 Prevalence rates of smoking among females for specific groups
from studies conducted in Myanmar…………………………………. 38
Table 2.27 Age-sex specific prevalence of current smoking among females in
Myanmar, 2001…………………………………………………………… 39
Table 2. 28 Types of tobacco used in Myanmar, 2001……………………………….. 40
Table 2. 29 Percentage distribution of types of tobacco used within sex groups,
Myanmar, 2001………………………………………………………….. 42
Table 2.30 Annual Consumption of manufactured cigarettes……………………….. 43
Table 2.31 Female smoking prevalence in Nepal (1980 to 2001)……………………. 44
Table 2.32 Smoking prevalence rate for female population 10 years of age and over
by ecological region and literacy, Nepal, 2000…………………………… 45
Table 2.33 Number of cigarettes/bidi smoked during most recent pregnancy by
literacy, Nepal, 1997……………………………………………………… 46
Table 2.34 Youth female smoking in Nepal, (1987-2001)…………………………… 46
Table 2.35 Cigarette and bidi smoking rates (%) for population 15 years of age and
over and estimates of per capita consumption of cigarettes and bidi,
Nepal, 2000………………………………………………………………. 47
Table 2.36 Trend of Annual Consumption of Cigarettes and Bidis in Nepal………... 47
Table 2.37 Prevalence of tobacco use among females in Sri Lanka …………………. 49
Table 2.38 Youth female smoking, Sri Lanka, 1999…………………………………. 50
Table 2.39 Trend of Annual Consumption of manufactured cigarettes in Sri Lanka… 51
Table 2.40 Female Smoking prevalence in Thailand, 1976 to 2001…………………. 52
Table 2.41 Estimated smoking prevalence trends by sex and population aged 15 or
more and males’ intensity of smoking compared to females in
Thailand,1986-1999……………………………………………………… 53
Table 2.42 Smoking prevalence by urban/rural division, sex and smoking habit,
Thailand, 1999 ………………………………………………………….. 53
Table 2.43 Smoking prevalence among Thai women by Region, 1996……………… 53
Table 2.44 Prevalence of Youth smoking, 1999……………………………………… 54
Table 2.45 Types of tobacco products used in Thailand by Region, 1996…………… 55
Table 2.46 Types of tobacco products used in Thailand by Urban and Rural, 1996… 55
Table 2.47 Trend of annual consumption of manufactured cigarettes in Thailand….. 55Table 3.1 Mortality Attributable to Smoking, by Region 62
Table 3.2 Female Mortality from Cancer in 2000 for SEAR countries, World age-
standardized mortality rate per 100,000 population, all ages……………... 64
Table 3.3 Female Mortality from cancer in 2000 World age-standardized mortality
rate per 100,000 population, >45 ……………………………………….. 65
Table 3.4 Age-standardized incidence rate of cancer per 100,000 population for
females in countries of South-East Asia Region, 2000………………….. 66
Table 3.5 Mortality from Cancer, 2000, World Age-Standardized Mortality Rate
per 100,000 population for Bangladesh, all ages………………………… 68Table 3.6 Percentage distribution of cause of death for all age groups, Bhutan,
2000………………………………………………………………………. 69
Table 3.7 Mortality from Cancer, 2000 World Age-Standardized Mortality Rate per
100,000 population for DPR Korea, all ages…………………………...... 70Table 3.8 Tobacco-related Cancers , India…………………………………………. 72
Table 3.9 Tobacco-related Diseases, 1996, India……………………………………. 73Table 3.10 Ten Leading Causes of Mortality for Five Years 1996 to 1997, India……… 74
Table 3.11 Mortality rates and age-adjusted relative risks, by type of smokeless tobacco habit,
among cohort study women, Mombai………………………. 74Table 3.12 Mortality rates and age-adjusted relative risks, by daily frequency of smokeless tobacco
habit, among cohort study women, Mombai………….. 75
Table 3.13 Mortality from Cancer, 2000 World Age-Standardized Mortality Rate per
100,000 population for India, all ages……………………………………… 75
Table 3.14 List of Disease, ICD-X International Statistical Classification of Disease
and Related Health Problems, Tenth Revision Code and Estimated
Proportion of Disease Attributable to Tobacco Indonesia
2001……………………………………………………………………….. 77
Table 3.15 Number of Cases of Diseases attributable to tobacco by Gender, Indonesia,
2001……………………………………………………………………….. 79
Table 3.16 Proportion of people exposed to environmental tobacco smoke inside the
house, by age group and gender, Indonesia, 2001…………………………. 81
Table 3.17 Number of Mortality Cases Attributable to Tobacco Use by Disease and
Sex, Indonesia, 2001………………………………………………………. 82
Table 3.18 Mortality from cancer in 2000, Indonesia World age-standardized mortality
rate per 100,000 population for Indonesia, all ages………………………… 83Table 3.19 Tobacco-related diseases: Impatient by primary diagnosis IGM Hospital, Maldives, 2001
and 2002………………………………………………….. 84
Table 3.20 Ten leading causes of Mortality for five years……………………………… 85
Table 3.21 Government Hospital admissions due to tobacco related diseases 1995-
1999…………………………………………………………………………. 86
Table 3.22 Outpatients due to tobacco related diseases 1996-1999……………………. 87
Table 3.33 Cancer cases admitted to Yangon General Hospital, 1991–1999…………... 88
Table 3.34 Total number of cancer cases treated at outpatient departments of Yangon
General Hospital, 1991–1999………………………………………………. 89
Table 3.35 Mortality from cancer in 2000, MyanmarWorld age-standardized mortality
rate per 100,000 population , all ages………………………………………. 92
Table 3.36 Ten leading causes of Mortality related to tobacco for five years, Nepal…... 94
Table 3.37 Causes of death in Nepal……………………………………………………. 94
Table 2.38 Mortality from cancer in 2000 World age-standardized mortality rate per
100,000 population for Nepal, all ages…………………………………… 95
Table 2.39 Mortality from cancer in 2000 World age-standardized mortality rate per
100,000 population in Sri-Lanka, all ages……………………………….. 97
Table3.40 Number of Deaths and Deaths Rates per 100,000 Population, by
Smoking-Related Diseases in Thailand (1996-2000)…………………….
99
Table3.41 Mortality from cancer in 2000, World age-standardized mortality rate per
100,000 population for Thailand, all ages………………………………….. 100
F I G U R E S
Figure 2.1 Age specific prevalence of smoking among females by age group and
region, Bangladesh, 2001……………………………………………… 17
Figure 2.2 Trend of female smoking by age group Bangladesh (1996 to 2001)…….. 18
Figure 2.3 Types of tobacco products used in Bangladesh, 2001……………………. 20
Figure 2.4 Different types of tobacco products used among Females by Region,
Bangladesh 2001…………………………………………………………. 20
Figure 2.5 Trend of annual per capita consumption of manufactured tobacco,
Bangladesh 1970 to 1992……………………………………………….. 21
Figure 2.6 Percent distribution of types of tobacco products used in Maldives, 1997.. 35
Figure 2.7 Percent distribution of types of tobacco use by sex group, Maldives ,2001 36
Figure 2.8 Age pattern of smoking among Myanmar women, 2001…………………. 39
Figure 2.9 Percent distribution of types of tobacco used in Myanmar, MSTE 2001… 41
Figure 2.10 Percent Distribution of Types of Tobacco Used…………………………. 41
Figure 2.11 Percent Distribution of Types of Tobacco Use Within Sex Groups,
Myanmar…………………………………………………………………. 43
Figure 2.12 Female smoking by region, Nepal 2000………………………………….. 45
Figure 3.1 Female Age-standardized mortality rate per 100,000 population from
cancer, all ages…………………………………………………………… 65
Figure 3.2 Female Age-standardized mortality rate per 100,000 for >45…………… 66
i
Acknowledgements
I would like to express my gratitude to the Ministry of Health of Myanmar for allowing me to conduct the survey. My heartfelt thanks go to Dr. Wan Maung, Director General of the Department of Health, Dr. Hla Pe and Dr. Soe Aung, Deputy Directors General of Department of Health, Dr. Sawat Ramaboot and Dr. Khalil Rahman of WHO Regional office for South-East Asia, for their kind help and guidance for the study and to WHO country office of Myanmar for helping me with the process.
I owe my gratitude to Dr. Narintr Timor of WHO Thailand and Dr. Sarah Barber of
WHO Indonesia for arranging my meetings with tobacco focal persons and NGOs. I am very thankful to all the people who had answered the questionnaires and to those who had provided me information through e-mail and internet. I am indebted to all the participants of the WHO/WB Technical Regional Consultation on Effective Collaboration between the Health and Financial Sectors for Tobacco Control held in Jakarta, Indonesia from 3rd to 4th December 2003 who had provided invaluable information for the study.
My sincere thanks go to my Director of Public Health, Dr. San Shway Wynn for his
understanding and support throughout the study. I also owe my immense gratitude to my family and friends who had helped through the study.

ii
CONDUCTING THE STUDY
This study was conducted with the technical and financial support of the Tobacco Free Initiative Unit of WHO Regional Office for South-East Asia. Dr. Sawat Ramaboot, Coordinator of Health Promotion Unit, and Dr. Khalil Rahman, Regional Tobacco Focal Point of SEARO provided inputs for conducting the study. The study started in June 2003.
Most of the information for the study was obtained from reviewing of existing
documents such as country reports, country profiles, WHO and other UN publications, articles published in international journals and from several websites. The tobacco control/global link website have provided invaluable information for the study. A lot of personal communications via email had been conducted with tobacco activists of the Region who had been very kind and helpful to share any information they have on the subject.
A questionnaire on the situation analysis of women and tobacco in the SEAR was
developed by the author and sent to the WHO Regional Office for South-East Asia. Dr. Sawat Ramaboot and Dr. Khalil Rahman reviewed the questionnaire and gave comments and suggestions. In August 2003, after a few modifications to adjust country situations, questionnaires were sent to all WHO country offices through WHO Regional Office. Nine out of eleven countries filled in the questionnaires and returned back to the author through SEARO.
The author visited Thailand and Indonesia in December 2003. In Thailand, meetings
were arranged between the author and Tobacco focal point from WHO country office of Thailand Dr. Narintr Tima, Dr. Prakit Vattesatokit chairman of Action on Smoking and Health, Ms. Bung-on Rotthipakdee from Thai Health Foundation and other ASH staff , and Miss Ramida Russel (ex- Miss Thailand and ex-ASH staff, an active anti-tobacco campaigner).
In Indonesia, the author met with chairpersons and members of Central Committee
for Tobacco Control, Indonesia Heart Foundation, Indonesia Cancer Foundation, and Indonesian Women against Tobacco. They willingly provided information on their ongoing activities and their views on the situation of tobacco control in Indonesia.
During a workshop held in Jakarta from 3rd to 4th December, 2003, WHO/World
Bank Technical Regional Consultation Effective Collaboration between the Health and Financial Sectors for Tobacco Control, the author had the opportunity to meet many focal persons from member countries. Not only did the participants of the workshop generously provided additional invaluable information for the study but they also gave very good suggestions for the report.
During 2001 and 2002, WHO SEAR had helped countries to conduct very important surveys regarding to tobacco; sentinel prevalence surveys were conducted in Bangladesh, India, Indonesia, Myanmar, Nepal and Sri Lanka; economics studies were conducted in Bangladesh, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka and Thailand. A lot of

iii
information in this study was based on these country reports. Additional information was also obtained from country presentations at various Regional Consultation Meetings. The study was in fact, a systematic review of all the information obtained from existing documents and reports. Answers from the country focal points and organizations to the questionnaire had been very informative and meeting with focal persons from countries at Indonesia and Thailand provided much needed information for the study.
iv
EXECUTIVE SUMMARY
South-East Asia Region comprises of eleven countries: Bangladesh, Bhutan, Democratic Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor- Leste. The population in the South-Eat Asia Region is estimated to be a little over 1.6 billion in the year 2003, estimates of adult female population in the Region was about 460 million in the year 2000 which is expected to increase to 700 million by the year 2030.
The current tobacco consumption rates in the Region ranges from 25.7% and 59.6% for men. Although female smoking prevalence in the South East Asia Region was considered to be low (except in Nepal, Bangladesh, Myanmar and Maldives) compared to global figures of around 12% for women, the number of women using tobacco in the Region was considerable, due to the huge size of female population in the Region. In 2000, it is estimated from the available data that there were more than 120 million women using at least one form of tobacco (smoking or smokeless) in the Region. In Bangladesh alone, estimates for 2001 showed that there were 8.5 million women smokers, most of them smoking bidis. In India, it was reported that one third of women used at least one form of tobacco, this came to around 100 million women above 15 years of age.
Prevalence rates of tobacco use and pattern of types of tobacco use differ greatly in the Region. High prevalent rates of smoking and smokeless tobacco users were found in Bangladesh, Maldives, Nepal and Myanmar. Although low smoking rates were reported from India and Sri Lanka, prevalence of smokeless tobacco use was very high among Indian women and also high among the rural women of Sri Lanka. Smoking rates were low among Bhutanese, Thai, Korean, Sri Lankan and Indonesian women. Female smoking rates were increasing in India and Bangladesh; it has increased rapidly in Bangladesh mainly among the poor; in India female smoking has nearly doubled in the urban areas and increased by 60% in the rural areas. Declining trends of female smoking rate were found in Thailand and Maldives.
The pattern of smoking among women was quite different in the Region compared to developed countries. Despite fears of western influence and less social stigma against women smoking, it has yet to become a fashionable and modern habit among educated and urban women in most countries of the Region. Smoking is still a “men” thing; it has been accepted as a norm for adult men for centuries and is still a male behaviour in most countries of South-East Asia.
The majority of women smokers belong to the poor and uneducated and rural areas have higher prevalence than the urban areas. In Bangladesh, not only prevalence of smoking is higher among the poor, consumption is also increasing sharply. Cigarette consumption, which is used mainly by the relatively well off and the educated was declining whereas consumption of bidis among the poor has sharply increased over the years. General trend

v
also shows increasing expenditure on tobacco by poor women; during 1995 to 1997, the potential in calories of rice for the average tobacco user nearly doubled for Bangladeshi women.
In Maldives where smoking is very much part of Maldivian culture, prevalence of female smoking (29.4% in 1997 and 15.6% in 2001) is among the highest in the Region. Tobacco use is also widely practiced among rural women in Nepal (29%) and Myanmar (21.9%) where it has been culturally and socially accepted since ancient times. Smoking of cheroots and hand-rolled cheroots is commonly practiced among Myanmar rural women and mostly in the older age groups. Smoking rates among women greatly differ between regions in Nepal; it is highest in the mountains, followed by the mid-hills and the Tarain. The majority of smokers in Nepal smoke cigarettes, a few smoke bidis and hukkah. Nepalese women smoke much cheaper products such as bidis than males. Among smoking products, kretek (clove cigarette) is unique of Indonesia and is reported to be more harmful than white cigarettes.
Literacy also greatly affects smoking rates. In Nepal, female literate population is four times less likely to smoke than the illiterates.
Exceptions are found in Thailand, where relatively higher rates of female smoking were found among certain professionals such as business women, air hostess, women working in beauty saloons and women educated in other countries; and in Bhutan where smoking was higher among the educated and in urban areas.
In countries like India and Bangladesh, where smokeless tobacco use was very common among females, women started tobacco use with smokeless products unlike men. India was unique in having many varieties of smokeless tobacco products; although only a few women smoke (2.5% in 1998-99) a large percentage (12.4%) of women use smokeless tobacco products. A 1997 survey in Mumbai reported 57.5% of tobacco use among women, consuming exclusively of smokeless tobacco products. A very high percentage of Bangladeshi women (47%) also used betel quid and chewed dried tobacco leaf (26%).
Around 20% of tobacco users in Nepal and 2.9% of tobacco users in Myanmar consumed smokeless tobacco. In Sri Lanka, smokeless tobacco use was practiced only among the females in rural areas, and is considered as “village behaviour”. In the villages, a high percentage of women were found to chew betel quid and also chewing of raw tobacco.
Many studies have reported the negative health consequences of tobacco use among women. It has been estimated that women smokers who die of a smoking related disease lose on average 14 years of potential life. Use of tobacco, including smokeless tobacco, is estimated to have caused more than 100,000 female deaths in developing countries in 1995. It is also estimated that women will account for an increasing proportion of all smoking-
vi
attributable deaths in coming years. The gender gap between men and women closes as smoking prevalence in women approximates that of men.
Worldwide, it is estimated that tobacco causes about 8.8% of deaths (4.9 million) and 4.1% of DALYs (59.1 million). As smoking is more common among males than females worldwide, attributable mortality is greater in males (13.3%) than females (3.8%). Approximately 16% of the global attributable burden occurred in the South-East Asia Region.
World Health Organization estimates that approximately 500,000 tobacco-related deaths occurred in the South-East Asia Region. This estimate is much lower than estimates done by countries, the estimate for tobacco attributable mortality was between 630,000 to 800,000 for India and more than 570,000 for Indonesia and 14,000 for Nepal. In India 4% of all deaths among women was estimated as related to tobacco. In Indonesia over 200,000 female deaths are attributable to tobacco each year. In Thailand, 42,000 deaths were attributed to tobacco in 1993.
Worldwide in 1990, approximately 10% of female cancer deaths resulted from smoking. Tobacco-related cancers account for about half of all cancers among men and one-fourth among women. Oral cancers account for one-third of the total cancers, with 90% of the patients being tobacco chewers. India had one of the highest oral cancers in the world. The highest reported incidence rate in the world for cancer of the mouth is among women in Bangalore, India, where women have considerably higher rates than men; this pattern is also found in Madras again in India. A much higher incidence of oral sub-mucous fibrosis was seen among women in India. Tobacco-related cancers account for one-fourth of all cancers among females in India.
Estimates from 2001 data in Indonesia demonstrate that tobacco contributes to 193,666 cases of cancer (all types) of which the majority are lung cancer cases (96,163); in addition, tobacco accounts for 31,847 deaths annually due to lung cancer.
Cancer mortality in Myanmar is apparently affecting not only males, as in all SEA countries, but also females. This is explained by female mortality rates that are higher than in most other countries of the Region. Oral cavity, oesophagus and lung cancers are the major killers among both males and females in Myanmar.
According to GLOBOCAN, age-specific female lung cancer death rates are highest in Myanmar followed by Thailand. Oral cavity cancer deaths are highest in Bangladesh followed by Sri Lanka, Nepal and India.
In Sri Lanka, figures for 1985-1986 showed that about 10% of all cancers in the total population were related to tobacco use. The incidence of cancer in women that could be related to tobacco use increased from 1 per 100,000 population in 1985 to 1.57 per 100,000 in 1990.

vii
The incidence of lung cancer among Northern Thai women is one of the highest in Asia and among the highest in the world, with an annual age-adjusted incidence rate of 37.4 per 100,000.
In all countries of the Region, except in Thailand and Bhutan, smoking prevalence rates among men are very high, usually above global figures. As the majority of smokers smoke at home and public places, there is an ever-increasing incidence of lung cancer among women and non-smokers exposed to environmental tobacco smoke.
In Bangladesh, Nepal and other countries, high incidence of ARI cases were reported among children exposed to ETS. Indoor air pollution due to use of fuel and exposure to tobacco smoke and other fumes contributed to high incidences of ARI cases among children in the Region. Perinatal deaths, abortions and low-birth weight babies are also reported due to maternal smoking and passive smoking. Stillbirths, low-birth weight babies and prenatal mortality have been reported among female tobacco chewers as well. In Bangladesh, women who were passive smokers of bidis during pregnancy had twice the number of perinatal deaths than those women from similar characteristics but who were married to companions with no tobacco habit.
Smoking has also been identified as one of the major risk factors for hypertension in India. Indonesian data demonstrates that more than 3 million cases of tobacco attributable to cardiovascular diseases annually, in addition to more than 190,000 deaths. Various retrospective studies in Indonesia, relates smoking behaviour with higher incidence of cardiovascular diseases (including stroke), and respiratory tract infection and cancer.
India estimates that there were 4.21 million females suffering from COPD each year. Overall, more than ½ million Indonesian suffer from respiratory diseases annually due to tobacco use, and more than 90,000 die from these conditions.
In India alone, there was an estimate of 10 million workers employed in the tobacco industry, approximately 60% of them are women and 12% to 15% of them are children, mainly young girls. Although there is no data on women employed in tobacco business for the Region, it is estimated that 10 to 12 million females are engaged in a wide range of tobacco industry from planting, weeding, picking, binding and tying of tobacco leaves to rolling of bidis and cheroots. These workers have to suffer from various health and social consequences arising from long hours of monotonous work in unhealthy, crowded conditions. Common disorders include rheumatic joint pains, stomach troubles, back-aches, impaired vision, piles, chronic cough, tuberculosis, stunted growth etc. and women and young girls are also deprived of labour rights in many bidi industries. Green tobacco sickness is also reported from Indonesia.
Each country in the Region has its own tobacco control policy and government and state institutions are working hand in hand with UN and international agencies, local and

viii
international NGOs towards tobacco control. Countries have also different stages of tobacco legislation; Thailand has success stories in the area of tobacco legislation, India has recently enacted a comprehensive tobacco control law, Myanmar and Nepal are in the process of coming up with tobacco control laws. Many countries have set rules and regulations, mainly to protect nonsmokers’ health from being exposed to Environmental Tobacco Smoke. Quite a few NGOs in the Region such as Action on Smoking or Health of Thailand had taken innovative actions and motivated and pushed governments to come up with tobacco control policies and legislation.
Thailand has its own programme known as “Thai women do not smoke”. This project and many other activities had been proved to be successful to counteract the tobacco industry’s techniques to lure women into the habit of smoking cigarettes. Country programmes should set such targets to prevent young girls from experimenting tobacco. In the mean time, as most of the tobacco users in the Region belong to the poor and the uneducated, programmes should aim at educating the poor and promoting their health. Female education plays a very important role. Community awareness campaigns should be aimed to reach the grassroots level. Community-based cessation of tobacco use programmes should be expanded to the rural areas, where women of older age group spend their time and their hard-earned scarce resources on tobacco.

1
INTRODUCTION
It is well known that smoking of tobacco products began as a habit of men in developed countries and has been adopted by women in those countries at a later stage. Men in developing countries followed the habit of smoking and only recently have women in developing countries begun to smoke, although the use of smokeless tobacco has been taking place among them much earlier. The epidemic of tobacco-related diseases had expanded from developed to developing countries and tobacco use is increasingly becoming a major health issue for women as well as men. 1 WHO estimates that there are currently 4.9 million deaths a year related to tobacco, a figure expected to rise to more than 10 million by the year 2030 with 70% of them in the developing countries. By 2030, tobacco will account for more deaths than the total deaths from malaria, maternal conditions, and injuries combined.
According to WHO estimates in 1995, there are about 1.1 billion smokers in the world, representing about one-third of the global population aged 15 years and over. The vast majority of the smokers are in developing countries (800 million) and most of these are men (700 million). Overall consumption has fallen among males in most high-income countries but it is on the increase among males in low- and middle-income countries and among females worldwide. About one-third of regular smokers in developed countries are women, compared with only about one in eight in developing countries. 2
Global estimates in 1995 indicate that about 12% of women smoke compared to about 47% of men. It was estimated that about 236 million women in the world were daily smokers in 1995. About 22% of women in developed countries and 10% of women above 15 years of age in developing countries smoke tobacco.3 Unless new, innovative and sustainable initiatives were implemented, it is predicted that prevalence of female smoking in both developed and developing countries will be around 20% by 2025 with the number of women smokers in the world rising to 532 million. The tobacco industry is targeting women with alluring campaigns and with women’s increasing spending power making cigarettes more affordable for them, the prevalence of smoking among women in developing countries is predicted to increase. The female population in developing countries will rise from the present 2.5 billion to 3.5 billion by 2025, so even if the prevalence remains low, the absolute number of women smokers will increase. 4
This huge increase in the number of women smokers around the world will have enormous consequences on health, the economy, the family and the environment. In addition to smoking; women also chew tobacco and use other forms of smokeless tobacco. In countries like India, prevalence of smokeless tobacco use was five times higher than smoking rates among women. Scientific evidences show that smokeless tobacco use is highly related to oral cancers.

2
Tobacco use and tobacco related illness is a serious health problem in the South-East Asia Region even at present. The current consumption rates ranges from 25.7% to 59.6% of men and although female smoking prevalence in the South East Asia Region was considered to be low (1.7% to 6.7%) except in Nepal (29%), Bangladesh (21% ), Myanmar (21% ) and Maldives (15%); recent prevalence reports from countries like India and Bangladesh show increasing prevalence among females.
Indonesia is ranked as having the fifth largest number of smokers in the world, while in India and Thailand it has been estimated that there are approximately 240 million and 11 million tobacco users. In Bangladesh there are estimated 20 million smokers, 5 million of them women in 1996 , in the year 2001 it was estimated that there were 8.5 million women smokers. 5 Smokeless tobacco use remains high in India, Bangladesh, Myanmar and Nepal although it is very low in Thailand and Sri-Lanka except in certain regions.
South-East Asia Region has become a lucrative market for tobacco industry. Tobacco consumption in the Region is increasing rapidly, especially among the youth and the poor.
India accounted for 65% of the Region’s total tobacco leaf production in 1990-91 which increased to 71% in 1998-1999. 6 Indonesia continues to be the largest producer of cigarettes in the Region, followed by India, Thailand and Bangladesh. Indonesia, Thailand and India were among the world’s largest cigarette consumers in 1994 accounting for 5.7% of the world’s total. Although India ranked only 14th for manufactured cigarette consumption, if the estimated amount of bidis consumed is added to the amount of cigarettes consumed, India ranks second globally in total cigarettes/bidis consumption. 6 Even though females consume much less proportion than men, the effects of environmental tobacco smoke on women and children should be seriously taken. The effects of passive smoking are more pronounced in the South-East Asia Region where the high level of nicotine and tar levels in cigarettes, bidis and kreteks, the poor implementation of laws banning smoking at public places and high incidence of indoor smoking put non-smokers as well as women and children at a high risk of tobacco-related diseases.
WHO estimates that there are approximately 500,000 tobacco-related deaths in the Region 6. India has one of the highest incidences of oral cancers in the world. Tobacco related cancers account for about half of all cancers among men and one-fourth among women. Tobacco-related illnesses such as cancer, cardiovascular and respiratory diseases are already major problems in most countries in the Region. Approximately half of all cancers in men in India are tobacco related, while over 60% of those suffering from heart disease below the age of 40 are smokers. There is an estimated 12 million cases of preventable tobacco related illnesses each year in India. In Sri Lanka, it is estimated that over 43% reported of cancers are tobacco related. Oral carcinoma is the most prevalent

3
form of cancer in Sri Lanka and cardiovascular diseases is the leading cause of death. Thailand reports 10,000 cases of tobacco related lung cancer each year. In India, tobacco attributable mortality has been estimated to be 80,000 per year while in Indonesia; in 2001, (21%) of all deaths were attributable to tobacco, and is expected to rise dramatically within the next few decades. According to a report by the Ministry of Health of Republic of Indonesia, the estimated number of mortality cases attributable to tobacco use in the year 2001 was 412,964; 211,271 males and 201,693 females. 7
Women constitute 60% of the work force of many bidi and cheroot making industries in the Region and suffer tobacco-related occupational hazards such as backaches, stiff joint pains, chronic asthma, tuberculosis, fatigue and weakness, mental trauma, stunted growth etc. In Indonesia, a study found that the incidence of Green Tobacco Sickness is 63.7% among tobacco farmers. Common complaints of green tobacco sickness include dizziness, headache and fatigue. 7
It is estimated that in India about 6 million roll bids and 4 million collect leaves. Since it involves working at home it includes children especially girls. In all steps of bidi workers 65% happen to be women and there are 15% children mostly girls. Women are paid less than men and children the least of all for the same work. As a huge percentage of women and children are illiterate, the employers can take advantage of them and they cannot fight back as a group for their rights. 8
Many research studies had been conducted on the issue of women and tobacco. These studies reported issues specific to women regarding to initiation, maintenance and cessation of tobacco use. It was often stated that women are less likely to plan to quit smoking than are men and are harder to quit also. Other studies reported that although women quit smoking at the same rate as men, they are less able to maintain cessation long-term. Men started to smoke for reasons such as peer pressure, parental smoking, rebellious behaviour etc. whereas women are more likely to smoke for tension reduction, depression, family violence, and fear of weight gain.
This study tries to analyze the situation of women and tobacco in South-East Asia Region. There is very limited data available; most of the data available are from surveys with different designs which could not be compared scientifically. There is also very limited data on women employed in tobacco industry, the extent of women exposed to ETS, and the tobacco-related morbidity and mortality. However, all available information has been compiled and recorded with the hope to be served as a baseline for further studies and for planning and monitoring of tobacco control programmes in the Region.
4
References
1. Virginia L. Ernester. Impact of Tobacco Use on Women’s Health. In WHO: Women and the Tobacco Epidemic, Challenges for the 21st Century. WHO in collaboration with the Institute for Tobacco Control, Johns Hopkins School of Public Health . Canada, 2001.
2. World Health Organization. Tobacco or Health: A Global Status Report. Geneva, World Health Organization , 1997.
3. Ranson K, Jha P, Chaloupka F, Yurekle A. Effectiveness and cost-effectiveness of price increases and other tobacco control policy interventions. In Jha Prrabhat, Frank Chaloukpka . (Eds). Tobacco Control Policies in Developing Countries. New York: Oxford University Press, 2000.
4. Dr. Judith Mackey. Preface in Women and the Tobacco Epidemic, Challenges for the 21st Century. WHO in collaboration with the Institute for Tobacco Control, Johns Hopkins School of Public Health. Canada, 2001.
5. Bangladesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in Bangladesh . Dhaka..June 2001
6. World Health Organization, Regional Office for South-East Asia Region: Health Situation in the South-East Asia Region 1999-2000. World Health Organization, Regional Office for South-East Asia Region New Delhi, 2001.
7. Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco Control Strategy. English Summary, December 3, 2003.
8. Mira B. Aghi. Women, Children and Tobacco. Paper presented at the WHO International Conference on Global Tobacco Control Law, New Delhi, India, January 2000.
9. World Health Organization, Regional Office for South-East Asia Region: Women of South-East Asia: A Health Profile. World Health Organization, Regional Office for South-East Asia Region New Delhi, 2001

5
PART ONE: BASIC INFORMATION
The WHO South-East Asia Region comprises eleven countries and is characterized by diversity in geographical, meteorological, economical, social and cultural aspects. It comprises of Bangladesh, Bhutan, Democratic Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor Leste. Countries in the Region range in size from Maldives with an area of around 300 square kilometers to India with a land area of over 3 million square kilometers. There is great variety in physical features as well, including an island nation (Sri Lanka), the world’s largest (Indonesia) and among the smallest (Maldives) archipelago countries, the predominantly flat alluvial plains of Bangladesh, and the world’s tallest mountain ranges in India and Nepal.
Demography
The population in the South-East Asia Region is estimated to be a little over 1.6 billion in 2003 and is projected to increase to over 1.75 billion in the year 2010. Although the population in the South East Asia Region as a percentage of the world’s population has declined from 26.11% to 25% over the last decade, the UN’s medium variant projections indicate that this share will increase to 26.03% by 2030. Countries of the Region vary widely in terms of population size. Maldives has a population of a few hundred thousands; Bangladesh and Indonesia have more than a hundred million each, while India reached a landmark in 2000 when its population exceeded one billion. Bangladesh, India and Indonesia are among the most populous countries in the world, and account for 88.2% of the world’s population. 1 The Region is the most densely populated region in the world; in 2000, at 222 persons per sq km, was almost five times the global figure. Bangladesh and Maldives were the most densely populated countries, while Bhutan and Myanmar were the least Table 1.1.
Estimate of adult female population in the Region in 2000 was about 460 million which will increase to 700 million by the year 2030. Except Myanmar and Thailand, population of males exceeds that of females in all countries. In some countries (Bangladesh and India) the relatively higher proportion of males in the population is at least in part due to the higher female than male mortality during childhood and in the reproductive age group. In DPR Korea, the sex ratio males per 100 females is projected to change in favour of females by 2010. 2
Countries in the Region have undertaken substantial efforts to reduce the growth of their populations. The average annual population growth rate for the Region as a whole has steadily declined from 2.14% in 1980-85 to 1.66% in 2002.
The age distribution of the population is rapidly changing in SEAR countries as in many developing countries. Adults in the working age group 15-64 years have become an increasing proportion of the general population, while the proportion of the population aged 65 and above has also increased. In 2000, 33.2% of the population belongs to 0-14 age group, 62% belongs to 15 to 64 age group and 4.8% belongs to over 65 years age group. 2

6
Table (1.1) Demographic Indicators of South-East Asia Region
Country Mid-2003 population (millions)
Sex Ratio (Males per 100 females) for 2000
Annual Growth Rate% 2002
% Urban 2003
Population density (per sqkm) 2000
Bangladesh 135.7 106.4 1.9 23 954 Bhutan 2.3 102.1 2.9 8 14 DPR Korea 22.6 100.8 0.5 61 185 India 1068.5 106.5 1.7 28 307 Indonesia 219.8 100.6 1.3 44 111 Maldives 0.28 105.4 2.0 29 977 Myanmar 52.1 98.8 2.0 29 71 Nepal 24.2 105.2 2.2 14 157 Sri Lanka 19.1 105.6 0.8 24 288 Thailand 62.8 98.0 0.7 31 122 Timor-Leste 0.75 107.24 1.8 7.8 --
SEAR 1608.13 101.6 1.66 29.8 222
Sources:
1: UNITED NATIONS, World Population Prospects, The 2002 Revision (New York, 2003)
2. ESCAP: Estimates based on available data
3. Bangladesh Bureau of Statistics, Population Census 2001, Preliminary Report, 2001
4. Ministry of Planning and National Development, Maldives: Statistical Year Book, Maldives 2002 2002)
5: Nepal, Population Census 2001; National report(Kathmandu Central Bureau of Statistics, 2002) and Nepal Demographic and Health Survey 2001(Alverton, Maryland, USA)
6: Thailand; Estimates Provided by the Institute for Population and Social Research Nakhon Pathom, Mahidol University 2003
9. WHOSEARO: Women of South East Asia: A Health Profile , WHOSEARO, 2000.
10. WHO SEARO : Health Situation in the South-East Asia Region,1999-2000. WHOSEARO, 2001.
11. Statistical Year Book 2002.
7
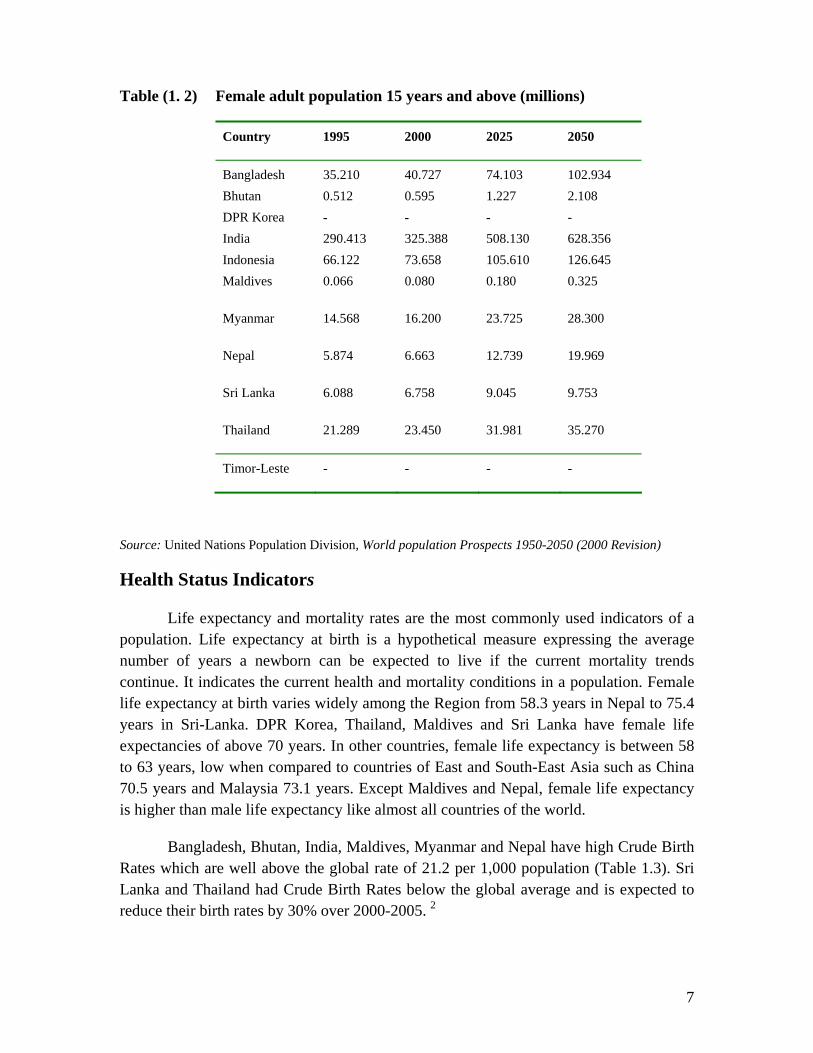
Table (1. 2) Female adult population 15 years and above (millions)
Country 1995 2000 2025 2050
Bangladesh 35.210 40.727 74.103 102.934 Bhutan 0.512 0.595 1.227 2.108 DPR Korea - - - - India 290.413 325.388 508.130 628.356 Indonesia 66.122 73.658 105.610 126.645 Maldives 0.066 0.080 0.180 0.325
Myanmar 14.568 16.200 23.725 28.300
Nepal 5.874 6.663 12.739 19.969
Sri Lanka 6.088 6.758 9.045 9.753
Thailand 21.289 23.450 31.981 35.270
Timor-Leste - - - -
Source: United Nations Population Division, World population Prospects 1950-2050 (2000 Revision)
Health Status Indicators
Life expectancy and mortality rates are the most commonly used indicators of a population. Life expectancy at birth is a hypothetical measure expressing the average number of years a newborn can be expected to live if the current mortality trends continue. It indicates the current health and mortality conditions in a population. Female life expectancy at birth varies widely among the Region from 58.3 years in Nepal to 75.4 years in Sri-Lanka. DPR Korea, Thailand, Maldives and Sri Lanka have female life expectancies of above 70 years. In other countries, female life expectancy is between 58 to 63 years, low when compared to countries of East and South-East Asia such as China 70.5 years and Malaysia 73.1 years. Except Maldives and Nepal, female life expectancy is higher than male life expectancy like almost all countries of the world.
Bangladesh, Bhutan, India, Maldives, Myanmar and Nepal have high Crude Birth Rates which are well above the global rate of 21.2 per 1,000 population (Table 1.3). Sri Lanka and Thailand had Crude Birth Rates below the global average and is expected to reduce their birth rates by 30% over 2000-2005. 2

8
A considerable decline in mortality has been recorded in South-East Region over the years. Between the period 1980-85 and 2000-2005, the crude death rates are projected to decline in all countries except DPR Korea.
Table (1. 3) Health Status Indicators in South-East Asia Region
Life expectancy at birth (years)Reported (1996-2001)
Country Crude Birth Rate (per 1,000
population)2002
Crude Death Rate
(per1,000 population)
2002
Male Female
Bangladesh 28.1 8.6 60.7 60.5
Bhutan 34.4 8.5 60.8 63.2
DPRKorea 16.2 11.0 63.04 70.94
India 28.1 8.6 62.4 63.4
Indonesia 20.6 7.3 61.9 65.7
Maldives 35.7 6.0 70.7 72.2
Myanmar 24.2 6.3 61.0 63.9
Nepal 32.6 9.6 58.8 58.3
Sri Lanka 16.3 6.6 70.7 75.4
Thailand 13.0 6.0 69.9 74.9
Timor Leste 31.7 15.1 46.7 48.4
SEAR 23.6 8.2
World 21.2 8.9 62.9 67.1
Source: United Nations Population Division, World population Prospects 1950-2050 (2000 Revision)
Rates for infant mortality and under five mortality per 1,000 live births and maternal mortality ratio per 100,000 live births are shown in Table 1.4. These data are different from country reports but are taken from the same source to have a consistent view. Bangladesh and Nepal have very high maternal mortality ratio, Myanmar, Nepal, Bangladesh and India have high infant and under five mortality rates. Sri-Lanka and Thailand have low mortality rates compared to other countries in the Region.
When infant and child mortality rates were differentiated by sex in countries where information is available, it was found that all countries of the Region had a higher male infant mortality although female post-neonatal mortality rates exceeded that for

9
males in Bangladesh and India. 1 Female child mortality rates 1-4 years exceeded male child mortality rates in all countries of the Region except Sri Lanka and Thailand. 1
Table (1.4) Infant, Maternal and Under Five Mortality Rates in South-East Asia Region
Country Infant Mortality Rate (per 1,000 live
births) Estimates for
2003
Under five mortality (per1,000 live
births)
Estimates for 2003
Maternal Mortality Ratio
1995
Bangladesh 63 86 600 Bhutan 53 79 500 DPRKorea 45 58 35 India 64 83 440 Indonesia 41 51 470 Maldives 38 48 390 Myanmar 83 127 170 Nepal 70 97 830 Sri Lanka 20 23 60 Thailand 20 26 44 Timor Leste 135 (2000) na na
Source: IMR and U5 MR: United Nations Population Division, World population Prospects 1950-2050 (2000 Revision) MMR- WHO/UNICEF/UNFPA, Maternal Mortality in 1995, Abouzahr and Wardlaw, 2001
Infectious and parasitic diseases featured prominently as a cause of death in females across the different countries. Alongside communicable and parasitic diseases, chronic diseases and degenerative conditions were also among the leading causes of female mortality. These included diseases of the circulatory system such as cardiovascular disease and hypertension, diseases of the respiratory system such as bronchitis and asthma, and neoplasm. For example, cardiovascular problems were among the top three causes of female deaths in India, Indonesia, Sri Lanka and Thailand. 1
Development Indicators
According to the definition by United Nations Development Programme (UNDP), human development index is a composite of achievements in basic human capabilities in three fundamental dimensions- a long and healthy life, attaining knowledge, and a descent standard of living. The values for these three valuables and the computed HDI for the three countries are shown in Table 1.5.
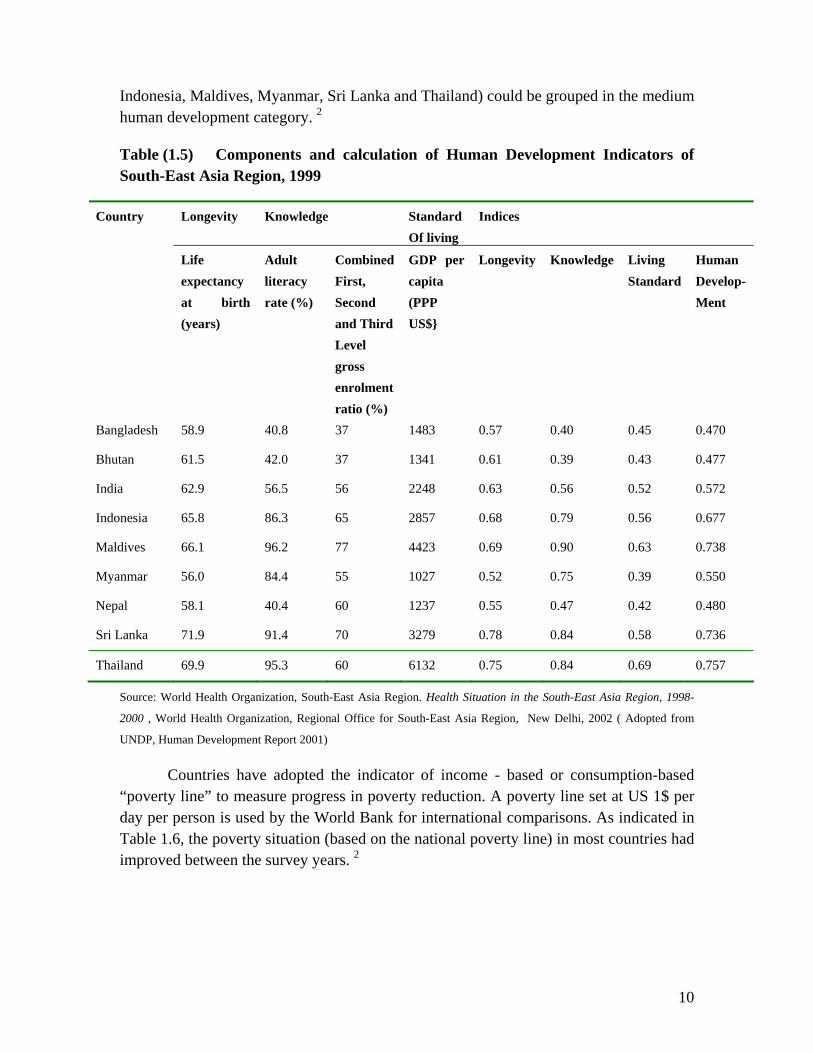
The countries were grouped into three categories (high, medium and low human development), depending on their respective HDI values. In 1999, no country in the Region was in the high human development category. Only six countries (India,
10
Indonesia, Maldives, Myanmar, Sri Lanka and Thailand) could be grouped in the medium human development category. 2
Table (1.5) Components and calculation of Human Development Indicators of South-East Asia Region, 1999
Longevity Knowledge Standard Of living
Indices Country
Life expectancy at birth (years)
Adult literacy rate (%)
CombinedFirst, Second and Third Level gross enrolment ratio (%)
GDP per capita (PPP US$}
Longevity Knowledge Living Standard
Human Develop- Ment
Bangladesh 58.9 40.8 37 1483 0.57 0.40 0.45 0.470
Bhutan 61.5 42.0 37 1341 0.61 0.39 0.43 0.477
India 62.9 56.5 56 2248 0.63 0.56 0.52 0.572
Indonesia 65.8 86.3 65 2857 0.68 0.79 0.56 0.677
Maldives 66.1 96.2 77 4423 0.69 0.90 0.63 0.738
Myanmar 56.0 84.4 55 1027 0.52 0.75 0.39 0.550
Nepal 58.1 40.4 60 1237 0.55 0.47 0.42 0.480
Sri Lanka 71.9 91.4 70 3279 0.78 0.84 0.58 0.736
Thailand 69.9 95.3 60 6132 0.75 0.84 0.69 0.757
Source: World Health Organization, South-East Asia Region. Health Situation in the South-East Asia Region, 1998-
2000 , World Health Organization, Regional Office for South-East Asia Region, New Delhi, 2002 ( Adopted from
UNDP, Human Development Report 2001)
Countries have adopted the indicator of income - based or consumption-based “poverty line” to measure progress in poverty reduction. A poverty line set at US 1$ per day per person is used by the World Bank for international comparisons. As indicated in Table 1.6, the poverty situation (based on the national poverty line) in most countries had improved between the survey years. 2

11
Table (1.6) Percentage or population living in poverty in selected countries of the South-East Asia Region.
Country Population (%) below the National poverty line Population below the International poverty line (below $1 a day)
Survey year Rural Urban National Survey year Population (%)
Bangladesh 1991-92 46.0 23.3 42.7 1995-96 39.8 14.3 35.6 1996 29.1 India 1992 43.5 33.7 40.9 1994 36.7 36.7 35.0 1997 44.2 1992-2000* 27.1 27.1 26.1 Indonesia 1996 12.3 12.3 11.3 1998 22.0 22.0 20.3 1999 15.2 Nepal 1995-96 44.0 44.0 42.0 1995 37.7 Sri Lanka 1995-96 45.5 45.5 40.6 1990-91 38.1 38.1 35.3 1995 6.6 Thailand 1990 … … 18.0
1992 15.5 10.2 13.1 1998 <2
Source: World Health Organization, South-East Asia Region. Health Situation in the South-East Asia Region, 1998-
2000 , World Health Organization, Regional Office for South-East Asia Region, New Delhi, 2002 (From World Bank,
The World Development 2000/2001
UNDP developed a new index called the “Human Poverty Index (HPI)” in order to measure the multi-dimensional aspects of poverty. HPI is derived from the same social development dimensions used for calculating HDI (longevity, knowledge and decent standard of living) but use different measures. It focuses on the deprivations in the three dimensions: longevity as measured by the probability of not surviving to age 40, knowledge as measured by the adult literacy rate; and overall economic provisioning, public and private as measured by the percentage of people not using improved water sources and the percentage of children who are underweight. HPT for countries whose data are available are shown in Table 1.7. 2
Table (1.7) Human Poverty Index (HPI-1) in selected countries of South-East Asia Region, 2000
Country HPI (%) Rank
Thailand 14.0 21
Maldives 15.8 25
Sri Lanka 18.0 31
Indonesia 21.3 38
Myanmar 28.0 43
India 34.3 55
Bangladesh 43.3 73
Nepal 44.2 77
Source: World Health Organization, South-East Asia Region. Health Situation in the South-East Asia Region, 1998-2000 , World Health Organization, Regional Office for South-East Asia Region, New Delhi, 2002 ( Adopted from UNDP, Human Development Report 2001)

12
Literacy and Education
In almost all countries of the Region, primary education is compulsory; the compulsory period ranging from 5 to 9 years. The gross enrollment ratio for primary education is almost 100% in all countries. Adult literacy rates vary among the countries. While Maldives, Sri Lanka and Thailand have achieved literacy rates over 90%, Bangladesh, Bhutan and Nepal are still lagging behind. It was estimated that in 2000, India has the largest population of illiterate adults. 2
In Bangladesh, Bhutan, India and Nepal, the illiteracy rates among women are well over 50%. Nepal (76.2%) and Bangladesh (70.5%) have the highest female illiteracy rates among the Region. The gap between male and female illiteracy is widest in Nepal while in Maldives the rates are nearly equal and are also the lowest in the Region (3.6% and 3.7% respectively).
Table (1.8) Gross primary and secondary enrolment ratios in selected countries of the South-East Asia Region, 1990- 1996.
Country Duration in years SEX Primary School enrolment ratio (%)
Secondary School enrolment ratio (%)
Compulsory Education
Primary Education
1990 1996 1990 1996
Bangladesh 5 5 Total 72 … 19 … Male 77 … 25 … Female 66 … 13 … India 8 5 Total 97 100 44 49 Male 110 109 55 59 Female 84 90 33 39 Indonesia 9 6 Total 115 113 44 51 Male 117 115 48 55 Female 114 110 40 48 Maldives … 5 Total … 128 … 59 Male … 130 … 59 Female … 127 … 60 Myanmar 5 5 Total 106 121 23 30 Male 108 … 23 29 Female 105 … 23 30 Nepal 5 5 Total 108 113 33 42 Male 132 129 46 51 Female 81 96 20 33 Sri Lanka 9 5 Total 106 109 74 75 Male 107 110 71 72 Female 105 108 77 78 Thailand 6 6 Total 99 87 30 56 Male 100 … 31 … Female 98 … 30 …
Source: World Health Organization, South-East Asia Region. Health Situation in the South-East Asia Region, 1998-2000 , World Health Organization, Regional Office for South-East Asia Region, New Delhi, 2002 (From UNESCO, World Education Report 2000)

13
References
1. World Health Organization, Regional Office for South-East Asia Region. Women of South-East Asia Region, A Health Profile, New Delhi, 2000.
2. World Health Organization, Regional office for South-East Asia Region. Health Situation in the South-East Asia Region, 1998-2000 , New Delhi, 2002
3. World Health Organization. World Health Report 2002, Geneva, 2002.
4. United Nations Development Programme: Human Development Report 2002, New York, USA, 2001

14
PART TWO: PREVALENCE OF TOBACCO USE AMONG FEMALES IN SOUTH-EAST ASIA REGION
It was estimated that about 250 million women in the world are daily smokers.
About 22% of women in developed countries and 10% of women in developing countries smoke tobacco. In addition, many women in the South East Asia Region use smokeless tobacco. Although female smoking prevalence in the South East Asia Region was considered to be low (1.7% to 6.7%) except in Nepal (29%) Bangladesh (24%) and Myanmar (21%); recent prevalence reports show increasing prevalence among females.
Types of tobacco products used in South-East Asia Region
Regarding tobacco consumption, SEAR has some unique problems. People in the Region use both smoking and smokeless forms of tobacco. Various forms of smoking and smokeless tobacco products used in the Region are described below;
(A) Main commercial smoking products include:-- 1) bidis –popular form in India, Nepal, Sri Lanka , Maldives and Bangladesh, made
up of locally grown tobacco. Bidi or biri is made of about 0. 2 to 0.5 gram of raw tobacco flakes (naturally cured) rolled by hand in tendu leaf (Diosyrus mebunoxylon or Diospyrus ebenum) or white paper. Tendu itself is responsible for 60% of its weight. Filter less and smaller- sized 50-60 mm bidi is available in Bangladesh. In India, sun dried and flaked tobacco is rolled in dried tendu leaves and secured in a thread. Indian bidis are sold in bundles of 8 to 24 but can be also purchased loose. Bidis in India may be longer-length (80 mm), bidi with filter (80 mm), herbal filter bidi (70 mm) made by various types of herbal leaves instead of sun-cured tobacco and bidi wrapped by paramit tree’s leaf called dhumti and banana leaf. In Bangladesh, bidis are sold in packets of 25. Bidis contain tar levels of 40 to 50 mg and 1.74 to 2.05 mg of nicotine.
2) kreteks ( indigenous cheroots containing tobacco, cloves and cocoa) mainly used in Indonesia. They contain a wide range of exotic flavorings and eugenol which has an anaesthetizing effect, allowing for deeper smoke inhalation. Kreteks contain 41 to 71 mg tar level whereas nicotine level ranges between 0.9 to 3.2 mg. Kreteks are smoked by 80% of current smokers in Indonesia. Despite their small size, their tar and carbon dioxide deliveries can be higher than manufactured cigarettes because of the need to puff harder to keep them lit.
3) cheroots (shreds of tobacco and/or stem of tobacco wrapped with thenatphet leaves) mainly used in Myanmar. Cheroots are smoked by 75% of current smokers in Myanmar.
4) chuttas (cheroots made from rolled tobacco leaves) are smoked extensively by women in some rural areas of India who practice reverse smoking by placing the lighted end of chutta inside the mouth.
5) cigarettes: most cigarettes manufactured in the Region have tar levels ranging from 18 to 30 mg and 1.55 to 1.92 mg nicotine. India, Indonesia and Thailand were among the world’s 25 leading cigarette consumers in 1994 accounting for the world’s 5.7% of the world’s consumption.

15
6) klobots/self-rolled cigarettes , used in Indonesia
7) cigars are made of air-cured and fermented tobacco with a tobacco wrapper, and come in many shapes and sizes, from cigarette-sized cigarellos, double coronas, cheroots, stumpen, chutta and dumptis. In reverse chitta and dhumpti smoking, the ignited end of the cigar is placed inside the mouth.
8) hand-rolled cheroots are smoked in all countries but only by a selected few.
9) dhumtis (conical cheroots) used in India
10) kakkad/chilm/sulfa ( smoking of tobacco in clay pipe)
11) hukka (hubble bubble) or watery tobacco or water pipe
12) pipes (wooden, clay , metal etc.)
(B) Main smokeless tobacco products include:
1) khaini :a mixture of tobacco and lime prepared in the palm, formed into a ball and places in the moth, usually in the groove between the cheek and gums.
2) masheri: roasted or half-burnt tobacco prepared by baking on a hot metal plate, powdered and used primarily for cleaning teeth, sometimes placed in the mouth as an alternative for chewing tobacco. Also known as mishiri / misheri .
3) pan masala: betel quid with tobacco, areca nuts and staked lime wrapped in a betel leaf. They can also contain other sweetening and flavoring agents. Pan is usually prepared by applying slaked lime and catechu to a betel leaf, to which small pieces of areca nut are added. Condiments and sweetening agents may be added. Tobacco is the most important ingredient of pan for regular users. The ingredients are folded in betel leaf and chewed. Varieties of pan include kaddipudi, hogesoppu, gundi, kadapam, zarda, pattiwala, kiwam, mishiri and pills.
4) gutcha: industrially manufactured chewing tobacco product.
5) oral use of snuff is also practiced in some specific areas. Moist snuff is taken orally. A small amount of ground tobacco is held in the mouth between the cheek and gum. Dry snuff is powdered tobacco that is inhaled through the nose or taken by mouth. Once widespread, its use is now in decline.
Smokeless tobacco in various forms is very common in India and to a small extent
in Bangladesh, Nepal, Bhutan, Bangladesh and Sri Lanka. They are consumed in Myanmar but mostly in the form of betel quid with tobacco. Chewing of raw tobacco is also practiced in the Region but not so extensively as other smokeless products. In India, women especially take to using smokeless tobacco use as it is more socially acceptable than smoking.
Whether it is inhaled, sniffed, sucked or chewed, or whether it is mixed with other ingredients, there is no safe way of using tobacco.
Sources: 1. Dr. Judith Mackey and Dr. Michael Erikson. The Tobacco Atlas. WHO. Geneva, 2002.

16
2. Shoba John and Shailesh Vaite. Tobacco and Poverty: Observations from India and Bangladesh. PATH Canada. October, 2002.
3. Rahman M and Fukui T: Bidi smoking and Health: Journal of Public Health(2000) 114, 123-127. www.nature.com/ph
BANGLADESH
Bangladesh is one of the countries consuming more tobacco than it produces as it
is a net tobacco importer. Bangladesh has a population about 130 million; it is one of the least developed countries with half of the population still living below abject poverty. A thriving tobacco industry coexists with this devastating poverty.3
Prevalence of tobacco use among females in Bangladesh
The WHO publication “ Tobacco or Health: A Global Status Report” 1997 stated that since 1980, smoking prevalence among males in Bangladesh has decreased from 67% to 60% but smoking rates for females have increased rapidly, from 1% to 15%; among female workers in 1980 the smoking rate was already 20%. The WHO SEARO publication “Country Profiles on Tobacco or Health” stated that the overall prevalence of tobacco use in Bangladesh has increased from 37% to 39%. Bidi consumption is rising; over 80% of smokers frequently smoked bidis in addition to other forms of tobacco; bidis were especially popular among the poor and those living in rural areas. The report also stated that in 1996, there were 20 million smokers in Bangladesh of which 5 million were women.
Table 2.1 shows prevalence of tobacco use among females from 1990 to 2001. Not being National surveys, it is difficult to interpret trends of female smoking in Bangladesh. Although comparatively, tobacco use prevalence was less among females than males, prevalence in terms of proportions and numbers clearly indicate that currently more women use tobacco than in 1990. Tobacco use prevalence among females was reported highest in 2001. Table (2.1) Prevalence of tobacco use among females in Bangladesh
Year Female % Estimated female smokers above 15 years (millions)
19901 15 4.8 19952 4.6 1.6 19963 3.6 1.3 1997 4 4.0 1.4 20015 20.9 8.5
1. WHO. Tobacco or Health: A Global Status Report. Geneva, 1997. 2 Bangladesh Bureau of Statistics. Prevalence of Smoking in Bangladesh, Dhaka , November, 1995 3. Efforymson D. and Saifuddin A. Hungry for Tobacco: An analysis of the economic impact of tobacco on the
poor in Bangladesh. PATH Canada. July 2000.. 4. Bangladesh Bureau of Statistics, Report of Survey on Prevalence of Morbidity, Treatment Expenditures,
Fertility,Immunization and Smoking, July 1997. 5. Bangladesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in
Bangladesh, Dhaka.. June 2001

17
Figure (2.1) Age specific prevalence of smoking among females by age group and region, Bangladesh, 2001
0 10 20 30 40 50 60 70
10_14 15-19 20-34 35-49 50 andaboveAge group
Prev
alen
ce o
f sm
okin
g Rural
Urban
In a 1996 study, smoking rates of females was estimated for age groups above 15
years (Table 2.2). It shows that smoking rates increases with age and reaches a maximum of 6.6% among 35 to 49 years age group. The study estimated the number of female smokers in 1996 as more than 1.3 million, out of which 0.6 million belong to the poor. Table (2.2 ) Estimated female population by age and smoking rates, Bangladesh, 1996
Age Population Smoking rates (%)
Number of smokers
Number of poor smokers
15-19 5,826,000 0.9 52,434 -- 20-34 14,161,000 3.3 467,313 -- 35-49 8,853,000 6.6 584,298 -- 50+ 7,079,000 2.8 198,212 --
Total 15+ 35,919,000 3.6 1,302,257 612,060 Source: Efforymson D. and Saifuddin A. Hungry for Tobacco: An analysis of the economic impact of tobacco on the poor in Bangladesh. PATH Canada. July 2000..
The study conducted by Bangladesh Bureau of Statistics in 1995, “Prevalence of
Smoking in Bangladesh” reported similar patterns among age groups. It reported female prevalence rates as 0.7%, 3.0%, 8.4% and 9.1% for 15-19, 20-34, 35-49 and 50+ age groups respectively. Table (2.3) Age-sex specific female prevalence of smoking (%) by age group and
region (Current smokers), Bangladesh, 2001. Age group ural Urban Total 10-14 0.8 - 0.5 15-19 1.8 0.2 1.3 20-34 19.9 9.8 15.9 35-49 42.9 28.9 37.1 50 and above 64.5 46.3 58.6 All 24.8 14.9 20.9
Source: . Bangledesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in Bangladesh . Dhaka..June 2001

18
Figure 2.2 shows the increase in prevalence of female smoking over the years. The 2001 study reported much higher prevalence rate than in 1996 and 1997. All studies reported highest prevalence rates among older women of 50 and above. Regarding to regional variation, while two-thirds of the female respondents were found to use tobacco products at 50 years and above, less than 50% of the urban female respondents were found to do so at similar ages.
In 2001, Bangladesh Institute of Development Studies (BIDS) conducted a sentinel prevalence and reported as “Craving for Nicotine: A Study on Tobacco Prevalence in Bangladesh”. It reported a high prevalence rate of 20.9% among females. This study was conducted in two sites, Chittagong and Rangpur.
According to this study, comparatively, tobacco use prevalence among females
was less in urban areas than in rural areas; 14.9% versus 24.8%. Prevalence was systematically lower among the urban females across all age groups. Tobacco use was very low for female respondents at their teenage years. It became higher above 35 years and became highest above 50 years. Use of tobacco among females’ 10-14 age groups was only 0.5%. (Table 2.3)
There were wide differentials in prevalence of smoking between greater zilas and urban-rural residential status. The 1995 study reported that female smoking rate was lowest in Pabna (0.9%) and highest in Chittagong Hill Tracts (27.3%).5
The BIDS study reported tobacco prevalence to be highest among female
widowers (63%) followed by married and separated/divorced categories.
Literacy and education were found to be inversely correlated with tobacco use. Among illiterate males, nearly 77% were tobacco users, while among females the corresponding rate was 41%. Prevalence of tobacco use among females with up to five
Figure (2.2) Trend of female smoking by age group Bangladesh (1996 to 2001)
0 0.9 3.3 6.62.80.3 1.2 3.1
6.9 9.3
0.5 1.3
15.9
37.1
58.6
0 10 20 30 40 50 60 70
10_14 15-19 20-34 35-49 50 andabove
Age group
Prev
alen
ce ra
te
1996 1997 2001

19
years of schooling was half the rate of males and only 8% among women with high school education and above. 5 Table (2.4) Female prevalence of smoking (%) by education group and region
(Current smokers), Bangladesh, 2001.
Education group ural Urban Total Illiterate 43 34 41
Primary School/read and
write
27 23 26
Secondary Education 13 12 13
Graduate and post graduate 7 9 8
Total 24.8 14.9 20.9
Source: Bangledesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in Bangladesh . Dhaka..June 2001
Types of tobacco products used in Bangladesh
Various types of tobacco are used in Bangladesh. A very high percentage of females 47.1% used betel quid and 25.8% chewed dried tobacco leaf. 5
According to surveys in 1979 and 1981, over 80% smokers frequently smoked
bidis in addition to other forms of tobacco. Bidis are especially popular among the poor and those living in rural areas. Consumption of bidis continues to increase, while cigarette sales are declining.
Table (2.5) Prevalence of tobacco use (%) among females for different types of tobacco products by region (Current users), Bangladesh, 2001
Type of tobacco product
Rural females % Urban females % Total %
Cicigarette 1.08 1.56 1.2 Bidi 5.16 7.68 4.08 Gul 2.76 0.36 2.28 Betel quid with tobacco 2.04 3.84 15.48 Chewing tobacco 11.4 0.24 9.6 Gutcha 12.72 0.12 2.88 Total 24.8 14.9 20.9
Source: Bangladesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in Bangladesh. Dhaka.. June 2001
The BIDS survey, 2001 reported that there was a definitive pattern in the use of tobacco between the male and female respondents. While males used smoked tobacco such as cigarettes and bidis in the beginning, females reported to have started with various types

20
of smokeless tobacco products such as betel nut with quid and dried tobacco leaf with or without lime. Only 10% of females started tobacco use with smoked products. The incidence of gul and khaini was also noticeable among the female respondents. Use of cheap smokeless tobacco product viz. betel nut with quid was also found to be high among the urban females.
Trends of annual consumption of cigarettes in Bangladesh
It was found that although per capita cigarette consumption has decreased in Bangladesh, per capita consumption of bidis has increased substantially. Between 1975 and 1999, bidi consumption increased by nearly 2.5 times. (Table 2.5)
Figure (2.4) Different types of tobacco products used among Females by Region, Bangladesh 2001
0 5 10 15
Cigarette
Bidi
Gul
Betel quid with tobacco
Chewing tobacco
Gutcha
Urban females % Rural females %
Figure (2.3)Types of tobacco products used in Bangladesh, 2001
Cigarette3%
Bidi7%
Hookah
1%
Betel quid47%Khaini
8%
Dried tobacco leaf26%
Gul8%
Figure (2.3)Types of tobacco products used in Bangladesh, 2001
Cigarette3%
Bidi7%
Hookah
1%
Betel quid47%Khaini
8%
Dried tobacco leaf26%
Gul8%
21
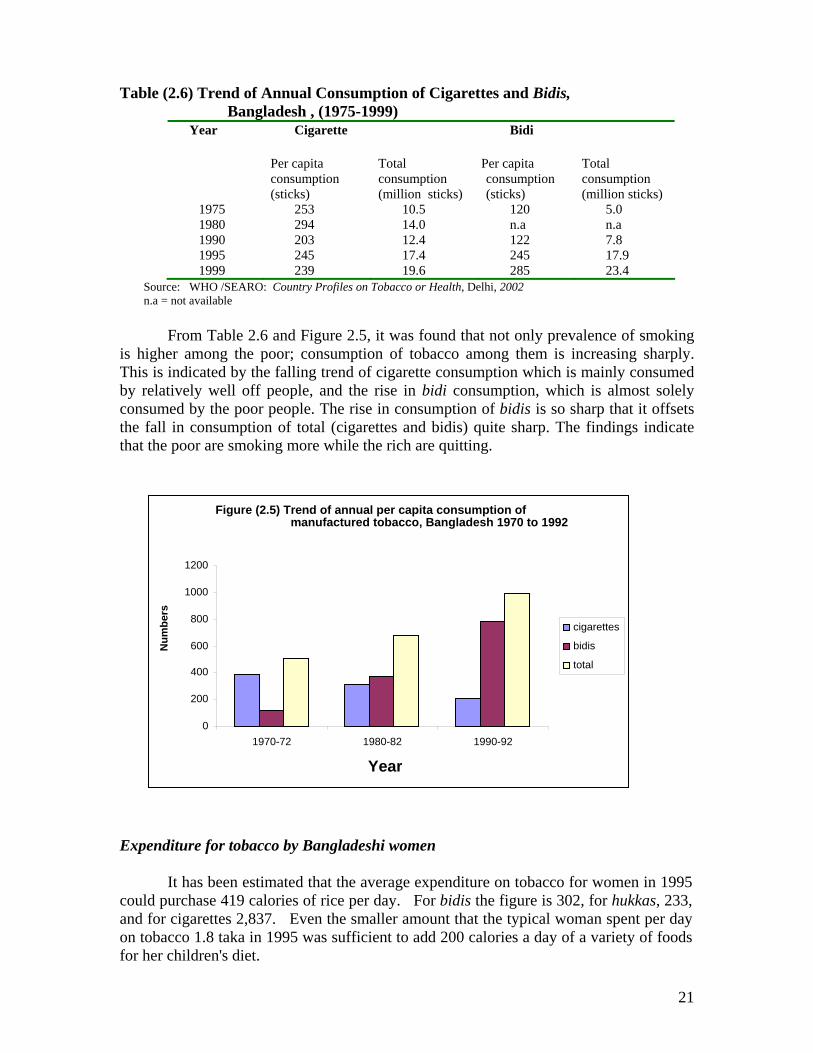
Table (2.6) Trend of Annual Consumption of Cigarettes and Bidis, Bangladesh , (1975-1999)
Year Cigarette Bidi
Per capita consumption (sticks)
Total consumption (million sticks)
Per capita consumption (sticks)
Total consumption (million sticks)
1975 253 10.5 120 5.0 1980 294 14.0 n.a n.a 1990 203 12.4 122 7.8 1995 245 17.4 245 17.9 1999 239 19.6 285 23.4
Source: WHO /SEARO: Country Profiles on Tobacco or Health, Delhi, 2002 n.a = not available
From Table 2.6 and Figure 2.5, it was found that not only prevalence of smoking
is higher among the poor; consumption of tobacco among them is increasing sharply. This is indicated by the falling trend of cigarette consumption which is mainly consumed by relatively well off people, and the rise in bidi consumption, which is almost solely consumed by the poor people. The rise in consumption of bidis is so sharp that it offsets the fall in consumption of total (cigarettes and bidis) quite sharp. The findings indicate that the poor are smoking more while the rich are quitting.
Expenditure for tobacco by Bangladeshi women
It has been estimated that the average expenditure on tobacco for women in 1995 could purchase 419 calories of rice per day. For bidis the figure is 302, for hukkas, 233, and for cigarettes 2,837. Even the smaller amount that the typical woman spent per day on tobacco 1.8 taka in 1995 was sufficient to add 200 calories a day of a variety of foods for her children's diet.
Figure (2.5) Trend of annual per capita consumption of manufactured tobacco, Bangladesh 1970 to 1992
0
200
400 600
800
1000
1200
1970-72 1980-82 1990-92
Year
Num
bers
cigarettes bidis total
22
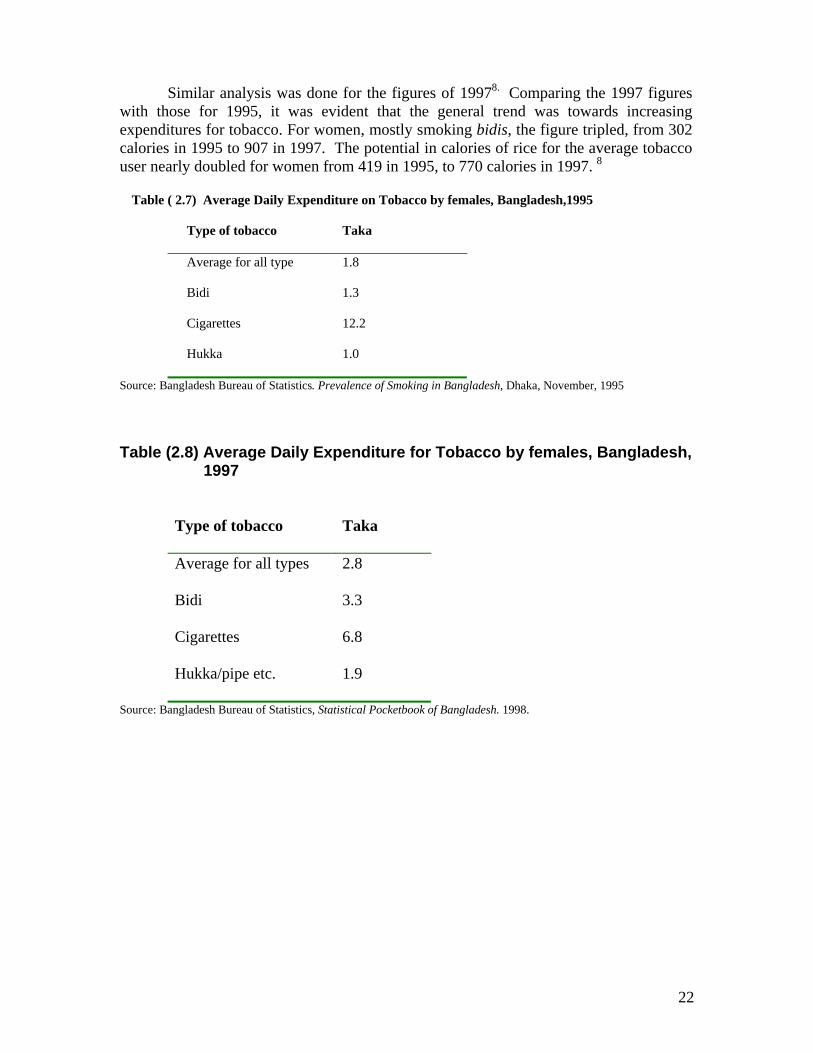
Similar analysis was done for the figures of 19978. Comparing the 1997 figures with those for 1995, it was evident that the general trend was towards increasing expenditures for tobacco. For women, mostly smoking bidis, the figure tripled, from 302 calories in 1995 to 907 in 1997. The potential in calories of rice for the average tobacco user nearly doubled for women from 419 in 1995, to 770 calories in 1997. 8
Table ( 2.7) Average Daily Expenditure on Tobacco by females, Bangladesh,1995
Type of tobacco Taka
Average for all type 1.8
Bidi 1.3
Cigarettes 12.2
Hukka 1.0
Source: Bangladesh Bureau of Statistics. Prevalence of Smoking in Bangladesh, Dhaka, November, 1995
Table (2.8) Average Daily Expenditure for Tobacco by females, Bangladesh, 1997
Type of tobacco Taka
Average for all types 2.8
Bidi 3.3
Cigarettes 6.8
Hukka/pipe etc. 1.9
Source: Bangladesh Bureau of Statistics, Statistical Pocketbook of Bangladesh. 1998.
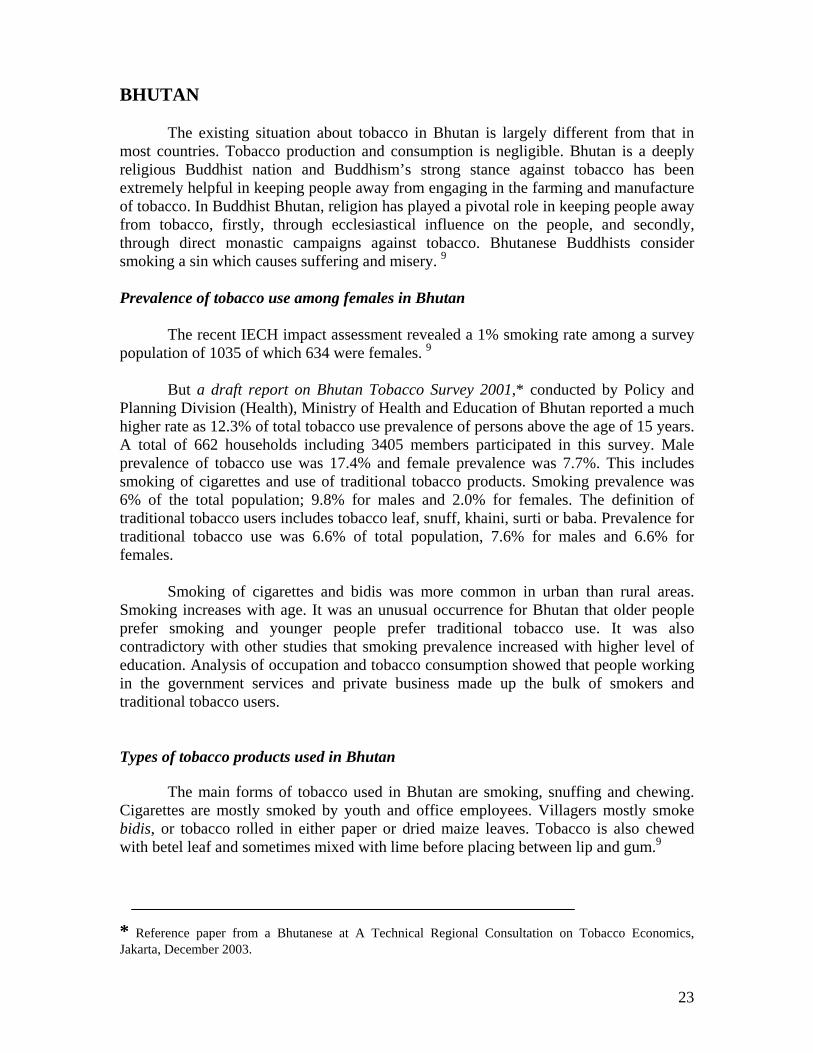
23
BHUTAN
The existing situation about tobacco in Bhutan is largely different from that in most countries. Tobacco production and consumption is negligible. Bhutan is a deeply religious Buddhist nation and Buddhism’s strong stance against tobacco has been extremely helpful in keeping people away from engaging in the farming and manufacture of tobacco. In Buddhist Bhutan, religion has played a pivotal role in keeping people away from tobacco, firstly, through ecclesiastical influence on the people, and secondly, through direct monastic campaigns against tobacco. Bhutanese Buddhists consider smoking a sin which causes suffering and misery. 9 Prevalence of tobacco use among females in Bhutan
The recent IECH impact assessment revealed a 1% smoking rate among a survey population of 1035 of which 634 were females. 9
But a draft report on Bhutan Tobacco Survey 2001,* conducted by Policy and Planning Division (Health), Ministry of Health and Education of Bhutan reported a much higher rate as 12.3% of total tobacco use prevalence of persons above the age of 15 years. A total of 662 households including 3405 members participated in this survey. Male prevalence of tobacco use was 17.4% and female prevalence was 7.7%. This includes smoking of cigarettes and use of traditional tobacco products. Smoking prevalence was 6% of the total population; 9.8% for males and 2.0% for females. The definition of traditional tobacco users includes tobacco leaf, snuff, khaini, surti or baba. Prevalence for traditional tobacco use was 6.6% of total population, 7.6% for males and 6.6% for females.
Smoking of cigarettes and bidis was more common in urban than rural areas. Smoking increases with age. It was an unusual occurrence for Bhutan that older people prefer smoking and younger people prefer traditional tobacco use. It was also contradictory with other studies that smoking prevalence increased with higher level of education. Analysis of occupation and tobacco consumption showed that people working in the government services and private business made up the bulk of smokers and traditional tobacco users. Types of tobacco products used in Bhutan
The main forms of tobacco used in Bhutan are smoking, snuffing and chewing. Cigarettes are mostly smoked by youth and office employees. Villagers mostly smoke bidis, or tobacco rolled in either paper or dried maize leaves. Tobacco is also chewed with betel leaf and sometimes mixed with lime before placing between lip and gum.9
* Reference paper from a Bhutanese at A Technical Regional Consultation on Tobacco Economics, Jakarta, December 2003.

24
DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
DPR Korea has very few women smokers. In 1985, it was reported that approximately 42% of the adult population smoked, albeit very few women. It was reported that 31.8% of 20-29 year-olds were ex-smokers, implying that they had succeeded in quitting smoking rather early in life.9
Consumption of manufactured cigarettes Tobacco (2.9) Annual consumption of manufactured cigarettes per adult, DPR Korea, (1970-72 to 199-92)
Year Annual average per adult (15+)
1970-72 1050 1980-82 1210 1990-92 960
Source: WHO. Tobacco or Health, A Global Status Report. Geneva, 1997.

25
INDIA
India ranks second among the 25 major tobacco producers in the world. It produces about 600 million kg of tobacco per year of which about 1/3 is flu - cured organic tobacco. This accounts for a good 10% of the total world production of tobacco. More and more tobacco companies (cigarettes, bidis, and chewing tobacco) are entering the market each day and the number of small manufactures controlling much localized market is on the rise.
It has been estimated that in 1992, 6.1% of the world’s un-manufactured tobacco and 1.5% of the total manufactured cigarettes were consumed in India. It was also estimated that about one third of women in India used at least one form of tobacco; that means more than 200 million females above 15 years of age in India were using one form of tobacco or another. Prevalence of tobacco use among females in India
National data on tobacco use prevalence among Indians have been recorded by the National Sample Survey Organization (NSSO). According to the 47th round 1987/88 and the 50th round 1993/94 of the National Sample Survey, tobacco use prevalence data are available for rural and urban sections of the population. The National Family Health Survey (NFHS-2) 1998-99 has collected data on tobacco use and smoking, and prevalence of tobacco use among females has been presented in Table 2.10. Table (2.10) Prevalence of tobacco use among females, India (1987-88 to 1998-99)
Year Rural % Urban % Total % 1987-88 11.1 5.9 9.7 1993-94 8.8 4.0 7.5 1998-99 13.8 8.8 12.4
Source: WHO/SEARO. Country Profiles on Tobacco or Health, New Delhi, 2002.
There is a decline in tobacco consumption for total population (32.8% in 1987-88
to 28.3% in 1998-99) for all people regardless of residence and sex. However the NHS-2 shows a higher overall tobacco use prevalence 20.5% compared to 1993-94 when it was 19.5%. Unfortunately, the growth in the number of tobacco users has taken place among the females as their prevalence has more than doubled in the urban areas. In the rural areas it has risen by nearly 60%. 9
Consumption of smokeless tobacco products is apparently more common among
women than among men. For the total population also, the overall tobacco use prevalence 20.5% was higher than the overall smoking prevalence 16.2%. NFHS-2, the second National Survey reported 2.5% of women who smoked and 12.4% of women who chewed panmasala or tobacco. According to this survey, smokeless tobacco use is five times greater than smoking among women.
Differences in tobacco use also vary among communities. Sikhs do not use any tobacco at all and Parsis use very little. However, tobacco use is permissible among

26
Hindus, Muslims and Christians. The prevalence rates for women differed widely, depending on areas surveyed. Varying from 0% to 67%, it was an average of 15% in Bhavnagar and 67% in Andhrra Pradesh. 10
A 1997 survey in Mumbai of adults, aged 35 years and above showed a high prevalence 57.5% of tobacco use among women, consuming exclusively smokeless tobacco products. The most common smokeless tobacco practice among women was mishri use 44.5% of smokeless users 11
Tobacco use among school personnel in Bihar in 2001 reported identical
prevalence of tobacco use among men 77.0% and women 77.0%: there was little difference in smokeless tobacco use among men 58.7% and women 53.4%. Although smoking among women in India is generally proscribed, prevalence of smoking among women in this sample was quite high 31% and most of it was cigarette smoking 26.9%. 12
A study in one Indian district of 10,000 individuals found that 46% practiced reverse smoking, and of these 62% were women. 13 Another study from Mizoram, India (1999) found tobacco consumption rate among women to be 45.7% with the majority using smokeless forms of tobacco. 14
The Study on Prevalence of Tobacco Use in Karnataka and Uttar Pradesh of India in 2001 reported current tobacco use of 14.9% among females of Karnataka and 9.1% among females of Uttar Pradesh. Prevalence increases with age reaching the peak level in the 70+ years among females. Prevalence of tobacco use was higher in rural areas as compared to urban areas in most age groups, except among teenagers where prevalence was comparable or higher than rural areas. 15
This study also reported that prevalence of current smoking was less than prevalence of current smokeless tobacco use: most of the current tobacco users are smokeless tobacco users. According to this study, only 0.6% of females in Karnataka and 0.6% of females in Utar Pradesh smoked compared to 14.4% and 6.6% accordingly. In Karnataka prevalence of smokeless tobacco users among females was even higher than males. Prevalence of smokeless tobacco use increased with age for both sexes. It was lower among educated women although clear-cut reducing prevalence trends with increasing education were not observed in all age-groups among men. Prevalence of smokeless tobacco use was comparatively lower in both the States among women with family income above Rs 5000 per month.
Prevalence of smoking among men was higher in rural than in urban areas but the prevalence was comparable in the two areas among females. Higher family income and higher education levels were associated with lower chance of smoking.
Tobacco use among dental students of Patna Dental College reported that among 26 females, 38.% reported current use and 11.5% past use; all the current users were smokeless tobacco users. 16
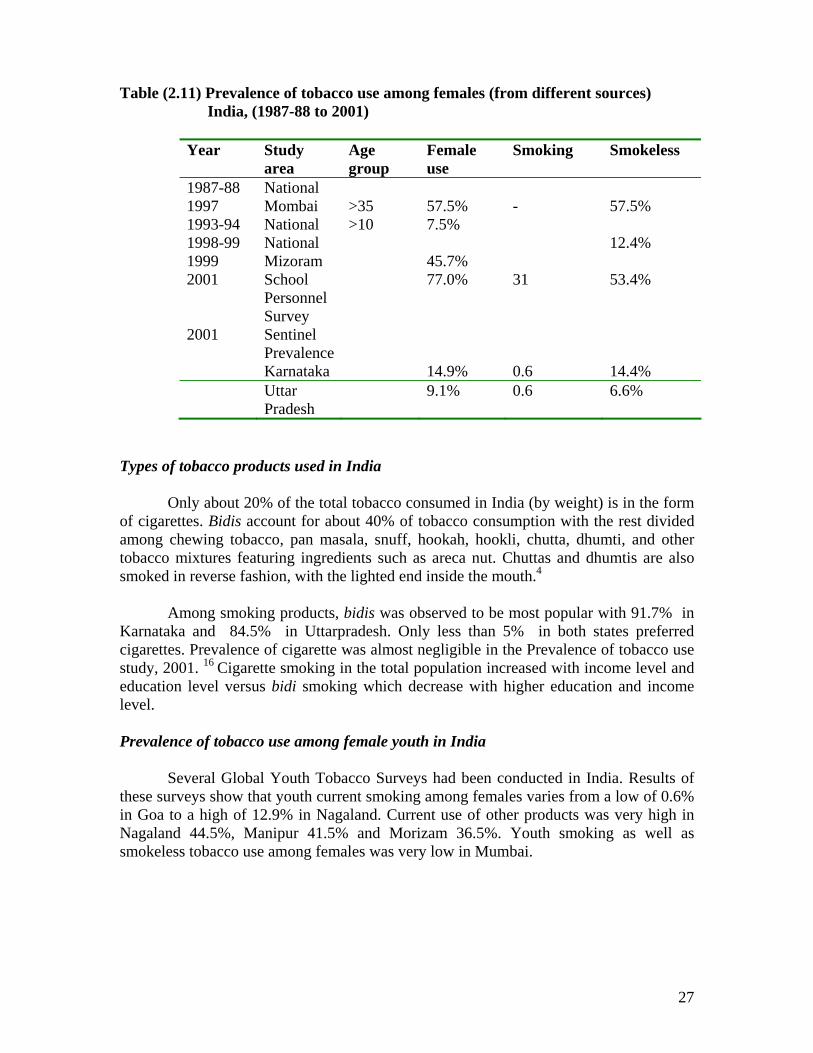
27
Table (2.11) Prevalence of tobacco use among females (from different sources) India, (1987-88 to 2001)
Year Study area
Age group
Female use
Smoking Smokeless
1987-88 National 1997 Mombai >35 57.5% - 57.5% 1993-94 National >10 7.5% 1998-99 National 12.4% 1999 Mizoram 45.7% 2001 School
Personnel Survey
77.0% 31 53.4%
2001 Sentinel Prevalence
Karnataka 14.9% 0.6 14.4% Uttar
Pradesh 9.1% 0.6 6.6%
Types of tobacco products used in India
Only about 20% of the total tobacco consumed in India (by weight) is in the form of cigarettes. Bidis account for about 40% of tobacco consumption with the rest divided among chewing tobacco, pan masala, snuff, hookah, hookli, chutta, dhumti, and other tobacco mixtures featuring ingredients such as areca nut. Chuttas and dhumtis are also smoked in reverse fashion, with the lighted end inside the mouth.4
Among smoking products, bidis was observed to be most popular with 91.7% in Karnataka and 84.5% in Uttarpradesh. Only less than 5% in both states preferred cigarettes. Prevalence of cigarette was almost negligible in the Prevalence of tobacco use study, 2001. 16 Cigarette smoking in the total population increased with income level and education level versus bidi smoking which decrease with higher education and income level. Prevalence of tobacco use among female youth in India
Several Global Youth Tobacco Surveys had been conducted in India. Results of these surveys show that youth current smoking among females varies from a low of 0.6% in Goa to a high of 12.9% in Nagaland. Current use of other products was very high in Nagaland 44.5%, Manipur 41.5% and Morizam 36.5%. Youth smoking as well as smokeless tobacco use among females was very low in Mumbai.

28
Table (2.12) Tobacco use among female school-going children aged 13-15 years, India
State Current
Smoking cigarettes %
Current use other products%
Current user%
Manipur 5.6 41.9 47.2 Meghalay 6.5 26.4 32.0 Rajasthan 1.8 8.9 10.3 Tripura 6.6 30.8 36.9 Sikkim 10.5 28.6 38.3 Nagaland 12.9 44.5 56.4 Maharastra 4.2 7.7 11.1 Goa 0.6 2.7 3.2 Mozoram 13.4 36.5 48.7 Mumbai 0.2 1.4 1.6
Source: Global Youth Tobacco Survey Fact Sheets
Trend of annual consumption of manufactured tobacco products in India In 1992, 6.1% of world total unmanufactured tobacco and 1.5% of world total manufactured cigarettes were consumed in India. Only about 20% of the total tobacco consumed in India (by weight) is in the form of cigarettes. Bidis account for about 55% of tobacco consumption about 675000 million bidis with the rest divided among various forms of smokeless tobacco. According to Table 2.13, although per capita consumption of manufactured tobacco products appears to have fallen: the absolute number of cigarette sticks consumed in 1999 has increased by nearly one-third compared to 1970 figures. Bidi consumption however has steadily increased over the years. Table (2.13) Trend of Annual Consumption of Cigarettes and Bidis,India (1970-1999)
Year Cigarette Bidi Per capita
consumption (sticks)
Total consumption (million sticks)
Per capita consumption (sticks)
Total consumption (million sticks)
1970 190 62908 840 284971 1980 178 75197 1130 446113 1990 101 54867 1220 601911 1999 147 95975 1297 850000
Source: WHOSEARO: Country Profiles on Tobacco or Health , New Delhi, 2002

29
INDONESIA
Indonesia is the fourth most populous nation in the world with a long historical tradition of tobacco growing and tradition. Tobacco is a familiar commodity to all Indonesians and has been known for a long time. The product is freely traded and may be bought by all levels of the community and all age groups, from children to adults. Tobacco products, especially cigarettes are available from almost every retailer, shop and street vendor. Cigarettes are easily available to all, in urban areas and even in isolated areas. Indonesia is famous for its aromatic kretek cigarettes, which are made from a mixture of tobacco and cengkih (cloves).
Given its large population and smoking prevalence, Indonesia ranks fifth among countries with the highest tobacco consumption countries globally. Consumption has increased steadily since the 1960s. The Tobacco Source Book of the Ministry of Health reported an increasing smoking prevalence from 26.9% in 1995 to 31.5% in 2001. 33
In Indonesia, smoking among men is regarded as culturally appropriate whereas the culture was less accepting of the smoking behaviour of women and that it could be said that promotion attempts aimed at women by the cigarette industry had yet not succeeded in overcoming the cultural resistance. The cultural values in Indonesia stigmatize smoking among women as morally flawed. 17 The WHO Tobacco or Health, Global Status Report 1997 stated that nationally prevalence of smoking was 60% for men and 5% for women. In 2001, male smoking prevalence was reported as 62.2% and female prevalence as 1.3%. 33 It could be stated that smoking prevalence among men was among the highest in the Region. Prevalence of tobacco use among females in Indonesia
Data on the prevalence of smoking by women in Indonesia was obtained from small-scale surveys conducted by health promotion organizations and academic investigators, and the large-scale official national surveys. Official Indonesian statistical publications often cite data on female smoking from aged 10 years, a practice which yields a lower rate than would the use of an age group of 20 years or older. 17
In the report published by Chapman and Wong in 1990, estimates of female adult smoking ranged from 3.6% to 10%. 17 In a study conducted in a rural area of West Java, Thomas Ganiwijaya et. al reported a very high prevalence of smoking among males 84% versus female prevalence of 5%. 18
In reviewing rates of smoking in Indonesia, Pol and Brand cited a study of some 4,000 adults in three cities conducted in 1986 and 1990 by Survey Research Indonesia, which reported an increase in the female smoking rate between these years from 5% to 7% in Jakarta and from 4% to 8% in Bandung, whereas the rate in Surabaya remained static at 1%. 17
The national household health survey, conducted in 1986, estimated a rate of 3.6% for regular and occasional female smokers 10 years of age and over. Suhardi’s monograph on smoking prevalence in Indonesia estimated that national prevalence of smoking (daily and occasional) for Indonesian females aged 10 years and older was 2%

30
and for women 20 years and older was 2.6% compared to 61.35 and 68.8% for respective ages among males. 17 The same study reported differences in estimates of female smoking among different provinces. The results defy attempts to predict female smoking rates by reference to religion or ethnicity. The province of Jamb, which is 96% Muslim, has a female smoking rate more than seven times that of West Nusa Tenggara which has the same ratio of Muslims in its population. Predominantly Christian Iranian Jaya has a rate of female smoking more than four times that of predominantly Christian East Timor. Bali, which is 93% Hindu and Aceh, which is 98% Muslim, share comparatively low rates of female smoking. 17
During 1997–98, the smoking prevalence among females increased, both in urban and rural areas. The rise of smoking prevalence among females in 1998 was probably due to the lifestyle change among females in the urban areas: in the past females were too shy to smoke in public, but in urban areas this is changing. According to Barraclough (1999), the increase of the smoking prevalence is probably caused by a weakening of stigma and Western cultural influences. 19
The smoking prevalence in rural areas was higher compared with urban areas. The higher level of smoking prevalence in rural areas was probably due to the low level of knowledge of the health risks of smoking, in addition to the lower formal education level compared to those living in urban areas. Access to information about smoking hazards was also less available. The following tables are prepared from “An economic analysis of tobacco control in Indonesia”, a study by Demographic Institute, Faculty of Economics, University of Indonesia; WHO/SEARO Report, 2001. The researchers had processed data from Longitudinal Indonesian Family Life Surveys, 1993, 1997 and 1998. 19 Table (2.14) Prevalence of female smoking by age group, Indonesia (1993-2001)
Year Age group Urban females
Rural females
Total Females
1993* >15 4.4 5.0 4.7 1995 # >15 1.2 2.0 1.7 1997* >15 2.2 3.2 2.7 1998* >15 3.7 3.7 3.7 2001# >15 1.1 1.5 1.3
Source: * Demographic Institute Faculty of Economics , University of Indonesia, An economic analysis of tobacco control in Indonesia, 2001, WHO/SEARO Report, 2001. (Calculated from Longitudinal Indonesian Family Life Surveys)
# . Ministryof Health Republic of Indonesia. The Tobacco Source Book: Data to Support a National Tobacco Control Strategy. English Summary, Jakarta, December 3, 2003. (Processed from National Socio-economic Survey 1995 and 2001)
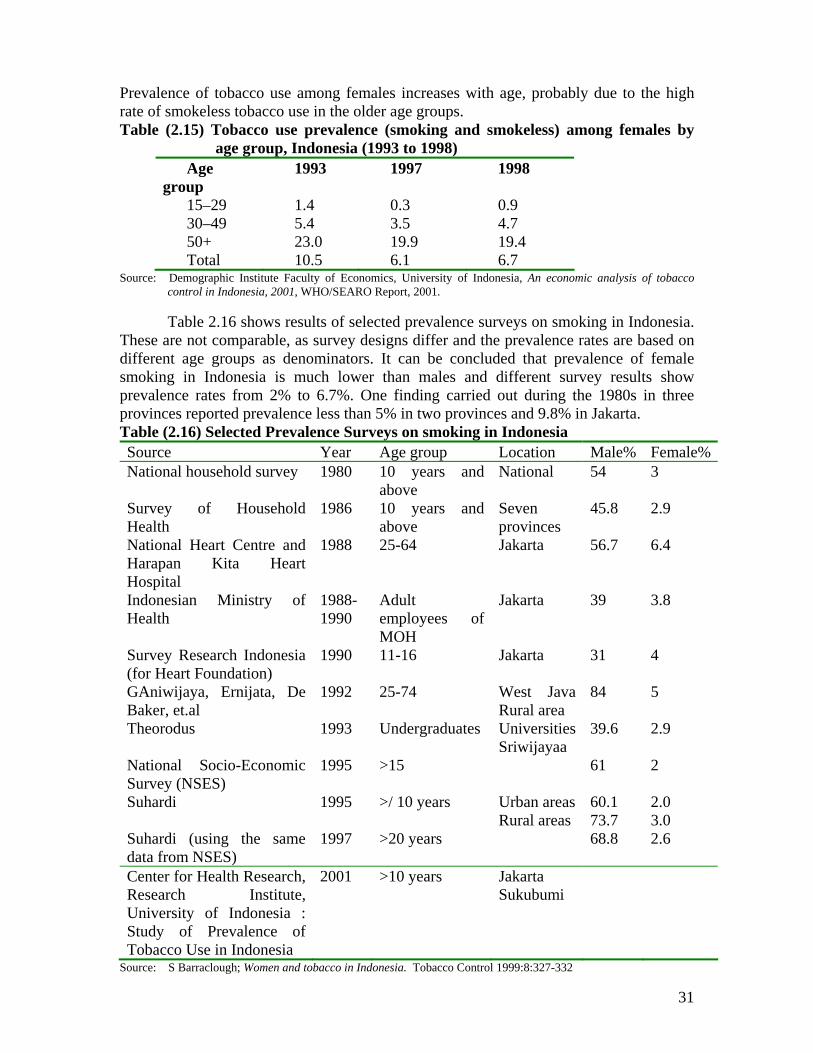
31
Prevalence of tobacco use among females increases with age, probably due to the high rate of smokeless tobacco use in the older age groups. Table (2.15) Tobacco use prevalence (smoking and smokeless) among females by
age group, Indonesia (1993 to 1998) Age
group 1993 1997 1998
15–29 1.4 0.3 0.9 30–49 5.4 3.5 4.7 50+ 23.0 19.9 19.4 Total 10.5 6.1 6.7
Source: Demographic Institute Faculty of Economics, University of Indonesia, An economic analysis of tobacco control in Indonesia, 2001, WHO/SEARO Report, 2001.
Table 2.16 shows results of selected prevalence surveys on smoking in Indonesia.
These are not comparable, as survey designs differ and the prevalence rates are based on different age groups as denominators. It can be concluded that prevalence of female smoking in Indonesia is much lower than males and different survey results show prevalence rates from 2% to 6.7%. One finding carried out during the 1980s in three provinces reported prevalence less than 5% in two provinces and 9.8% in Jakarta. Table (2.16) Selected Prevalence Surveys on smoking in Indonesia Source Year Age group Location Male% Female%National household survey 1980 10 years and
above National 54 3
Survey of Household Health
1986 10 years and above
Seven provinces
45.8 2.9
National Heart Centre and Harapan Kita Heart Hospital
1988 25-64 Jakarta 56.7 6.4
Indonesian Ministry of Health
1988-1990
Adult employees of MOH
Jakarta 39 3.8
Survey Research Indonesia (for Heart Foundation)
1990 11-16 Jakarta 31 4
GAniwijaya, Ernijata, De Baker, et.al
1992 25-74 West Java Rural area
84 5
Theorodus 1993 Undergraduates Universities Sriwijayaa
39.6 2.9
National Socio-Economic Survey (NSES)
1995 >15 61 2
Suhardi 1995 >/ 10 years Urban areas 60.1 2.0 Rural areas 73.7 3.0 Suhardi (using the same data from NSES)
1997 >20 years 68.8 2.6
Center for Health Research, Research Institute, University of Indonesia : Study of Prevalence of Tobacco Use in Indonesia
2001 >10 years Jakarta Sukubumi
Source: S Barraclough; Women and tobacco in Indonesia. Tobacco Control 1999:8:327-332

32
Demographic Institute Faculty of Economics, University of Indonesia. An economic analysis of tobacco control in Indonesia, 2001, WHO/SEARO Report, 2001. WHO. Tobacco or Health, A Global Status Report. Geneva, 1997
A 1985 survey of primary schoolchildren in Jakarta found that 49% of boys and 9% of girls aged 10 to 14 were daily smokers. 4 However, a study in Jakarta in 1990 reported that only 1% of 11-14 year olds and 6% of 16 year olds were daily smokers, although the figures for occasional smokers were 15%, 22% and 44% respectively. The study also revealed that the vast majority of youth smokers 95% smoked kreteks and 72% reported that their parents did not know that they smoked. Prevalence of tobacco use among female youth in Indonesia
Smoking habits started during childhood, and age at uptake is decreasing rapidly. The vast majority of smokers (68.8%) started their habit before they turned 19 years old. The Global Youth Tobacco Survey conducted in 2000 reported female prevalence (13-15) years as (5%).
The GYTS survey reported a very high exposure to tobacco smoke : (67.4%) live in homes where others smoke, (81.6%) are around others who smoke in places outside their home, (65.9%) have one or more parents who smoke, (18.5% ) have most or all friends who smoke. Table (2.17) Youth female Smoking in Indonesia, (1985 -2000)
Year Age
group Female
prevalence% 1985 10-14 9 1990 11-14 ? 2000 13-15 5
Source: WHO: Tobacco or Health, A Global Status Report Global Youth Tobacco Survey 1999-2001, Fact sheet Types of tobacco products used in Indonesia.
Most tobacco consumed in Indonesia is in the form of cigarettes. Most cigarettes in Indonesia are different from other cigarettes as they have cloves added to the tobacco. These are known as kreteks. Kreteks are known to contain a relatively high portion of harmful substances, particularly with unfiltered clove cigarettes. According to Suhardi 1997, a filtered kretek is about 75% tobacco and 25% clove. Compounds have been found in kretek smoke comparable to those found in white cigarettes, as well as certain compounds which derive from the clove additive and give kretek its unique taste. Kreteks contain more tar and nicotine than white cigarettes, which make them more hazardous to health. The filtered kretek is the smoke of choice in Indonesia. Between 85% and 90% of all cigarettes smoked in Indonesia are kreteks. In 1999, out of 34 663 household samples spending money on cigarettes, 64% of them bought filtered kretek and 31% of them unfiltered kretek (Adioetomo et al., 2001).19
Smoking tobacco products used in Indonesia include kreteks or clove /tobacco mix cigarettes; white cigarettes ; kelembak/ siong cigarettes which are almost the same as an ordinary clove cigarette, but use additional ingredients such as kemenyan (a tree

33
resin) and kelembak (Chinese rhubarb); klobot which are cigarettes with dried corn husk wrappers; pipe tobacco and self-rolled cigarettes.
Smokeless tobacco use are in the form of dried tobacco leaves rolled to the size of a thumb and inserted into the mouth between lips and teeth and betel quid with tobacco. The study of prevalence of tobacco use in Indonesia (2001) carried in two urban Jakarta and rural Sukabumi reported that almost half of respondent smokers 49% reported of smoking cigarette products daily and about 40% of smoking kretek daily. Only about 2% reported use of cigar/klibot/self—wrapping daily. In that study only about 1% as ever used betel quid and less than 1/2 % of experiencing the use of chewing tobacco. For females, using betel quid and chewing was found only among > 60 years age group.
Table (2.18) Prevalence of tobacco use for population 15 years and above, by sex and
tobacco product, Indonesia, 1998 Tobacco use prevalence Male % Female % Total% Cigarette 55.8 3.4 28.4 Self-rolled 8.5 0.5 4.3 Pipe 0.1 0.0 0.1 Chewing 0.2 3.0 1.7 Any type of tobacco use 59.7 6.7 31.9
Source: Demographic Institute Faculty of Economics , University of Indonesia. An economic analysis of tobacco control in Indonesia, 2001, Jakarta, 2001.
Trend of tobacco products consumption in Indonesia. According to Table 2.20, an Indonesian women consumed an average of 2481 piece annually in 1995. The average number of cigarettes consumed is highest among the 15-29 age group. Table (2.19) The average number of cigarettes consumed by female smokers, (in
pieces annually), Indonesia, 1995 Age group Urban Rural Total 15–29 2593 2685 2652 30–49 2527 2441 2465 50+ 2201 2482 2415 Total 2434 2499 2481
Source: Demographic Institute Faculty of Economics, University of Indonesia. An economic analysis of tobacco control in Indonesia, 2001, Jakarta, 2001. From Table 2.20, it was found that annual per capita consumption of
manufactured cigarettes had increased drastically over the years, in 2000, it has become nearly five times than that of 1970.
Table (2.20) Annual Consumption of manufactured cigarettes, Indonesia (1970-2000)
Year Per capita consumption (sticks)
Total consumption (million sticks)
1970 469 32581 1980 906 80672 1990 1137 133740

34
1995 1183 156666
1998 1405 198526
Source: WHOSEARO: Country Profiles on Tobacco or Health 2002 MALDIVES Maldives is one of the few countries in the world where tobacco is not cultivated although tobacco consumption is very common in the country. Smoking is very much part of Maldivian tradition and till very recently, a social visit was not completed without a few puffs of hookah, guduguda, cigar or pipe. 9 Prevalence of tobacco use among females in Maldives Two national surveys had been conducted in 1997 and 2001 by the Department of Public Health. The 1997 survey involved 4510 households and 13125 respondents over 16 years of age and the 2001 survey included 2168 households and 7261 respondents over 16 years of age. Prevalence of smoking among females was quite high compared to other countries in the Region (except Myanmar). Table (2.21) Prevalence of female smoking by age group, Maldives (1997, 2001)
Year Age
group Urban
females% Rural
females%
Total females %
1997 * >16 years 13 31 29.4 2001** >16 years 15.6
Source: Department of Public Health, Maldives.
In the 1997 national survey, 59% of respondents >16 years were found to be smokers: 57.4% were males and 29.4% females. Cigarette smoking is common among all ages. Other types of usage: the hubble- bubble and tobacco chewing are highest among older age groups. While 44% of tobacco users smoke cigarettes, 33% are chewers. Cigarette smoking is the most common means of tobacco consumption in the country. Of male smokers, 65% smoke cigarettes while 15% of female smokers consume cigarettes.
Among women, 47% chew tobacco, 35% use guduguda and 14% smoke cigarettes. About 40% tobacco users are 45 years old and above. While a quarter of the users are in the 25-34 age group, 10% are below 25 years of age.
The 2001 national survey reported that while 51.1% are cigarette smokers, 14.8% used the hubble-bubble and 32.9% chewed tobacco.
There are more tobacco users in the island communities than in the capital. In the outer atolls 42% population are smokers while only 24% of the urban population smokes.
Types of tobacco products used in Maldives Smoking forms used in Maldives include bidis, cigars, cigarettes, hubble-bubble (hookah), guduguda and pipes. Bidis and cigarettes are the major forms of cigarettes
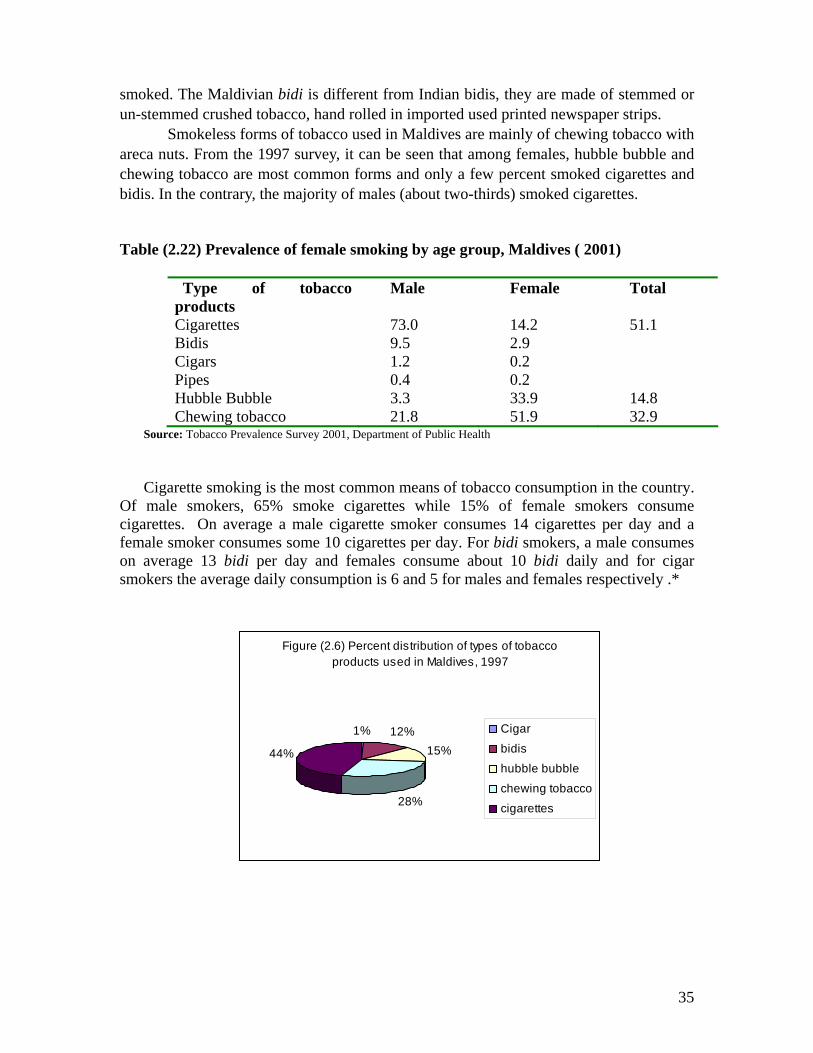
35
smoked. The Maldivian bidi is different from Indian bidis, they are made of stemmed or un-stemmed crushed tobacco, hand rolled in imported used printed newspaper strips.
Smokeless forms of tobacco used in Maldives are mainly of chewing tobacco with areca nuts. From the 1997 survey, it can be seen that among females, hubble bubble and chewing tobacco are most common forms and only a few percent smoked cigarettes and bidis. In the contrary, the majority of males (about two-thirds) smoked cigarettes.
Table (2.22) Prevalence of female smoking by age group, Maldives ( 2001)
Type of tobacco products
Male Female Total
Cigarettes 73.0 14.2 51.1 Bidis 9.5 2.9 Cigars 1.2 0.2 Pipes 0.4 0.2 Hubble Bubble 3.3 33.9 14.8 Chewing tobacco 21.8 51.9 32.9
Source: Tobacco Prevalence Survey 2001, Department of Public Health Cigarette smoking is the most common means of tobacco consumption in the country.
Of male smokers, 65% smoke cigarettes while 15% of female smokers consume cigarettes. On average a male cigarette smoker consumes 14 cigarettes per day and a female smoker consumes some 10 cigarettes per day. For bidi smokers, a male consumes on average 13 bidi per day and females consume about 10 bidi daily and for cigar smokers the average daily consumption is 6 and 5 for males and females respectively .*
Figure (2.6) Percent distribution of types of tobacco products used in Maldives, 1997
1% 12%15%
28%
44%
Cigar
bidishubble bubble
chewing tobacco
cigarettes
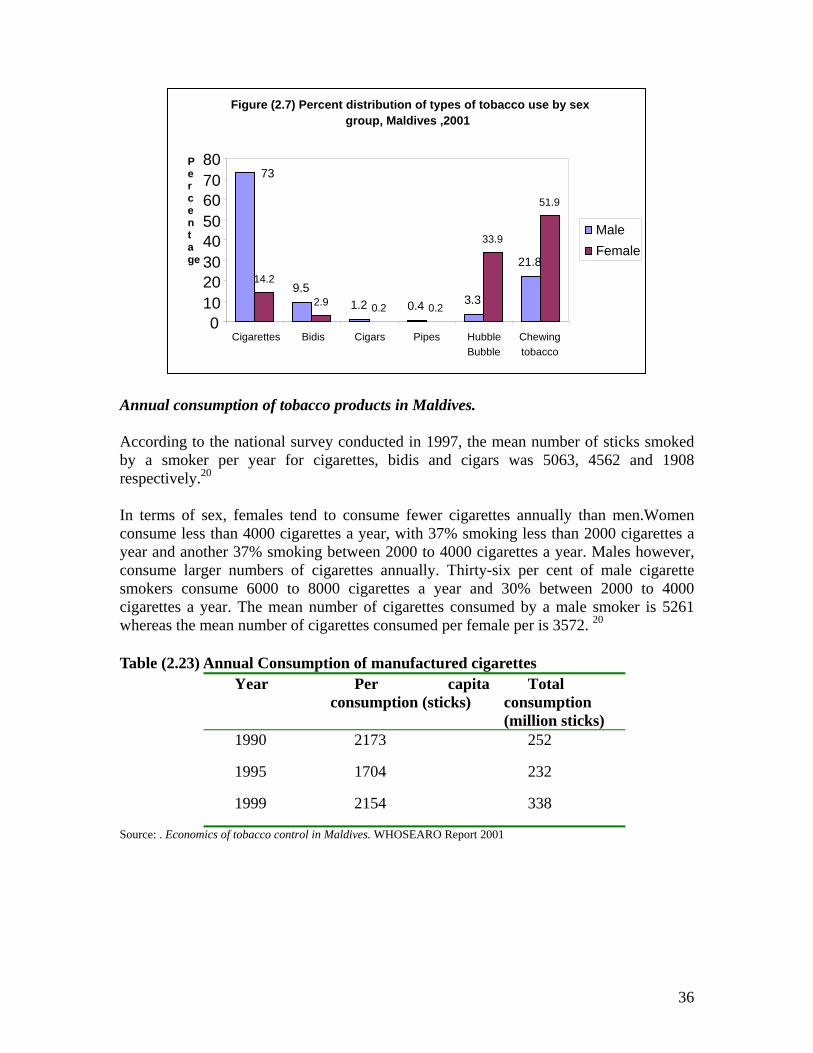
36
Annual consumption of tobacco products in Maldives. According to the national survey conducted in 1997, the mean number of sticks smoked by a smoker per year for cigarettes, bidis and cigars was 5063, 4562 and 1908 respectively.20 In terms of sex, females tend to consume fewer cigarettes annually than men.Women consume less than 4000 cigarettes a year, with 37% smoking less than 2000 cigarettes a year and another 37% smoking between 2000 to 4000 cigarettes a year. Males however, consume larger numbers of cigarettes annually. Thirty-six per cent of male cigarette smokers consume 6000 to 8000 cigarettes a year and 30% between 2000 to 4000 cigarettes a year. The mean number of cigarettes consumed by a male smoker is 5261 whereas the mean number of cigarettes consumed per female per is 3572. 20
Table (2.23) Annual Consumption of manufactured cigarettes
Year Per capita consumption (sticks)
Total consumption (million sticks)
1990 2173 252
1995 1704 232
1999 2154 338
Source: . Economics of tobacco control in Maldives. WHOSEARO Report 2001
Figure (2.7) Percent distribution of types of tobacco use by sex group, Maldives ,2001
73
9.5 1.2 0.4 3.3
21.8 14.2
2.9 0.2 0.2
33.9
51.9
0 10 20 30 40 50 60 70 80
Cigarettes Bidis Cigars Pipes HubbleBubble
Chewingtobacco
Male Female
P e r c e n t a ge

37
MYANMAR Tobacco use is widely practiced in Myanmar where it is culturally and socially accepted since ancient times. Prevalence of female smoking is among the highest in the South East Asia Region. Although only a few percent of urban females smoke, about one fifth of the adult females in the rural area smoke some form of tobacco products, mostly in the form of cheroots or hand-rolled cheroots. Smokeless tobacco in the form of betel quid with tobacco is also quite commonly used among Myanmar women, mostly in the rural areas. Prevalence of tobacco use among females in Myanmar The Myanmar sentinel tobacco use prevalence study conducted in 2001 reported prevalence of female current smokers as 21.9% and current smokeless tobacco users as 8.0% .(Table 2.25) Table (2.24) Prevalence of tobacco use among females > 15 years, Myanmar, 2001
Type of User Female %
Current tobacco user 27.0 Current smoker 21.9 Current smokeless 8.0
Source: Nyo Nyo Kyaing :Myanmar Sentinel tobacco use prevalence study 2001, WHOSEARO report, 2001.
A few studies had been conducted to find the prevalence rates of smoking,
smokeless tobacco use and tobacco use among the general population and sub-groups. Different studies used different survey designs and the rates had been calculated on different age groups. None of the surveys could be taken as national survey. However, from Table 2.26 which shows the findings from these surveys, it can be stated that prevalence of smoking among Myanmar females was around 20%, it was higher in rural areas than in urban areas.
Table 2.26 shows prevalence of smoking among specific sub-population groups. It was found that smoking was low among health personnel compared to general population. Youth smoking rates (6%) and adolescent rates (1.4%) was low among females.

38
Table (2.25) Prevalence rates of smoking among females from specific studies conducted in Myanmar Percentage of smokers
Source Year Region Age Residence Female% 1.Cardio-vascular disease survey
1989/90
Yangon Division 18+ Urban 46
2.Smoking prevalence survey
1999 29 townships of Bago, Magwe and Mandalay Division
All ages Urban and rural 9
3.Smoking prevalence survey
2000 29 townships of Bago, Magwe and Mandalay Division
All ages Urban and rural 28.8
4. Research on socio-econmic determinants of tobacco use
2000 Insein, Madaya and Hinthada
15+ Peri-urban and rural 20.1
5.Study on Tobacco economics Household survey
2000 Magwe, Ayethayar Maulamyine Bago, Monywa
10+ Urban Rural Total
6.3 7.3 7.1
6.Myanmar sentinel tobaccouse prevalence study
2001 Pakkuku Hinthada
15+ Urban Rural Total
15.4 24.4 21.9
7.Study of tobacco use among women in Bago Division
2003 Daik-U Nyaung Lay Bin Taung-U Ye Tar She’
12+ Urban Rural Total
17.62 21.55 20.73
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003.
Table (2.26) Prevalence rates of smoking among females for specific groups from studies conducted in Myanmar.
Percentage of smokers Source Year Region Age Residence Female%
1. A study of smoking habits among middle and high school children
1991 North Okkalapa Yangon division
10-18 Peri-urban 2.9
2. Smoking habits of Myanmar health personnel
Rapid survey of women
3. Rapid survey of women 4. Study on prevalence trend of youth smoking
5.Adolescent reproductive health survey
1994 1996 1999 2000
25 townships of Yangon Division
Thanlyin
29 townships of Bago, Magwe and Mandalay Division Yangon Division
18+ 18+ 15-24 15-24
Urban and rural
Urban Rural Urban and rural Urban and rural
2.8
8.2 24.8
6
1.4
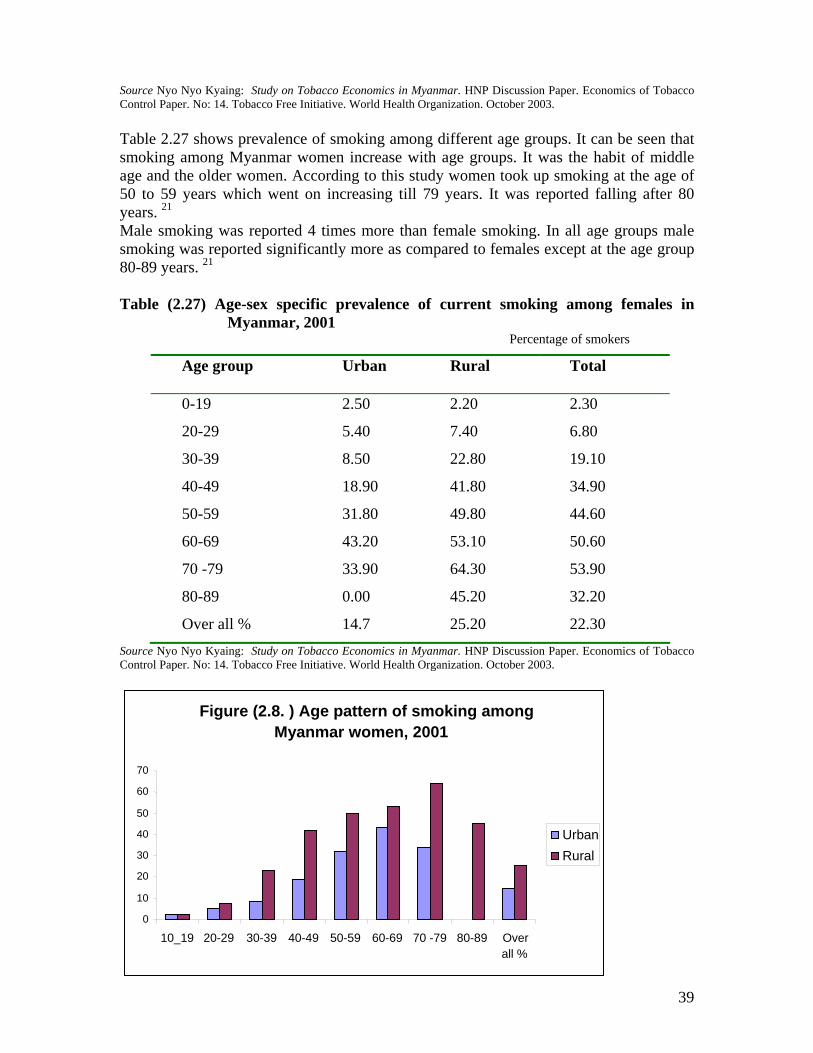
39
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003. Table 2.27 shows prevalence of smoking among different age groups. It can be seen that smoking among Myanmar women increase with age groups. It was the habit of middle age and the older women. According to this study women took up smoking at the age of 50 to 59 years which went on increasing till 79 years. It was reported falling after 80 years. 21 Male smoking was reported 4 times more than female smoking. In all age groups male smoking was reported significantly more as compared to females except at the age group 80-89 years. 21
Table (2.27) Age-sex specific prevalence of current smoking among females in Myanmar, 2001
Percentage of smokers
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003.
Age group Urban Rural Total
0-19 2.50 2.20 2.30
20-29 5.40 7.40 6.80
30-39 8.50 22.80 19.10
40-49 18.90 41.80 34.90
50-59 31.80 49.80 44.60
60-69 43.20 53.10 50.60
70 -79 33.90 64.30 53.90
80-89 0.00 45.20 32.20
Over all % 14.7 25.20 22.30
Figure (2.8. ) Age pattern of smoking among Myanmar women, 2001
0 10 20 30 40 50 60 70
10_19 20-29 30-39 40-49 50-59 60-69 70 -79 80-89 Overall %
Urban Rural

40
Source: Nyo Nyo Kyaing et al, Tobacco Free Initiative Project, Department of Health, Myanmar Sentinel Tobacco Use Prevalence Study 2001, WHO SEARO Report 2001. Prevalence of smoking among female youth in Myanmar
The GYTS was conducted in Myanmar in 2001; among the sampled population of 4721, 37.3% of males and 4.7% of females were reported as current users. About 3.8% were current smokers and 6.6% were current smokeless tobacco users. About 21.3% of students were currently smoking at the time of survey. More than 20% were using smokeless tobacco. The majority (two-thirds) of current smokers who bought any form of smoking tobacco in a store were not refused purchase because of their age. 22
In 1999, a study on smoking prevalence trends among youth found that over half of those aged 15-24 years were smokers. Prevalence among female youth was a little below 6%23. Cheroot was the most favored tobacco, followed by cigarettes. The proportion of tobacco users among out-of-school youth was higher than those in school. Types of tobacco products used in Myanmar
From all studies ever conducted on tobacco in Myanmar, it was found that the most common form of tobacco used in Myanmar was in the form of cheroots, either produced by cottage industries or by domestic companies. Survey findings show that cheroots were most commonly used in both urban and rural areas, followed by home rolled tobacco.
Cheroots are thin and long and are wrapped with a specific form of leaf called "thatnatphet" . Myanmar tobacco leaves are sun-tanned and grounded, their stems are baked and chopped and these are mixed with tamarind and wrapped with " thanatphet" leaves to roll into cheroots. All the cheroots are hand-rolled. In this report cheroots refer to those made at the cottage industries and " hand-rolled cheroots" refer to those rolled by the users themselves at home. "Home - rolled tobacco" may be wrapped with corn-tusk, thanatphet leaves or paper. Tobacco wrapped with corn-tusk was also called "Pyaung-Phu-Phet" and tobacco wrapped with thanatphet leaf is called "phet-kyan" where as tobacco wrapped in a piece of paper or with sheaths from betel-nut trees are called "put-chun". In this chapter, all these forms are collectively shown as "Hand rolled tobacco". Chewing of tobacco includes chewing of betel quid with tobacco mixed with lime and chewing of raw tobacco. Both categories had been classified as chewing tobacco in this report. Table (2. 28) Types of tobacco used in Myanmar, 2001
Sr. No: Type of tobacco Urban % Rural % Total%
1 Cheroots 49.4 72.8 66.7
2 Hand -rolled Cheroots 24.1 17.9 19.5
3 Cigarettes 14.4 6.5 8.5
4 Cigars 0.4 0.8 0.7
5 Chewing of tobacco 12.0 2.1 4.6
Total 100 100 100

41
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003. Cheroots were more widely used in rural areas and smoking of cigarettes was more common in urban areas. Because all types of hand -rolled cheroots were collectively shown in one category, it was higher in urban than in rural areas, although tobacco wrapped with corn-tusk and paper are more widely used in the rural areas. (Figure 2.6)
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003.
Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003.
Figure (2.9) Percent distribution of types of tobacco used in Myanmar, MSTE 2001
49.4
24.114.4
0.412
72.8
17.96.5 0.8 2.1
020406080
Cheroots Hand -rolledCheroots
Cigarettes Cigars Chewing of tobacco
Types of tobacco used
Per
cent
age Urban
Rural
F i g u r e ( 2 . 1 0 ) P e r c e n t D i s t r i b u t i o n o f T y p e s o f T o b a c c o U s e d
C h e r o o t s6 6 %
H a n d r o l l e d T o b a c c o
1 9 %
C ig a r e t t e s9 %
C ig a r s1 %
C h e w in g o f t o b a c c o
5 %
C h e r o o t sH a n d r o l l e d T o b a c c oC i g a r e t t e sC i g a r sC h e w i n g o f t o b a c c o
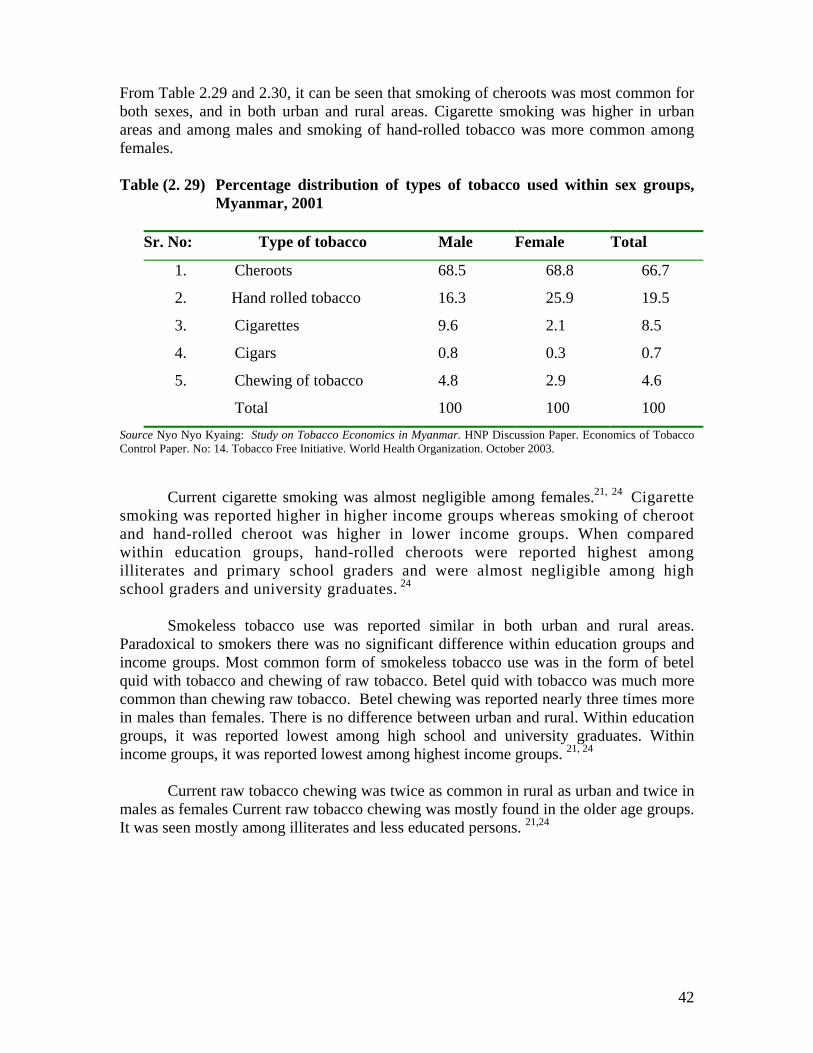
42
From Table 2.29 and 2.30, it can be seen that smoking of cheroots was most common for both sexes, and in both urban and rural areas. Cigarette smoking was higher in urban areas and among males and smoking of hand-rolled tobacco was more common among females. Table (2. 29) Percentage distribution of types of tobacco used within sex groups,
Myanmar, 2001
Sr. No: Type of tobacco Male Female Total
1. Cheroots 68.5 68.8 66.7
2. Hand rolled tobacco 16.3 25.9 19.5
3. Cigarettes 9.6 2.1 8.5
4. Cigars 0.8 0.3 0.7
5. Chewing of tobacco 4.8 2.9 4.6
Total 100 100 100 Source Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiative. World Health Organization. October 2003.
Current cigarette smoking was almost negligible among females.21, 24 Cigarette
smoking was reported higher in higher income groups whereas smoking of cheroot and hand-rolled cheroot was higher in lower income groups. When compared within education groups, hand-rolled cheroots were reported highest among illiterates and primary school graders and were almost negligible among high school graders and university graduates. 24
Smokeless tobacco use was reported similar in both urban and rural areas. Paradoxical to smokers there was no significant difference within education groups and income groups. Most common form of smokeless tobacco use was in the form of betel quid with tobacco and chewing of raw tobacco. Betel quid with tobacco was much more common than chewing raw tobacco. Betel chewing was reported nearly three times more in males than females. There is no difference between urban and rural. Within education groups, it was reported lowest among high school and university graduates. Within income groups, it was reported lowest among highest income groups. 21, 24
Current raw tobacco chewing was twice as common in rural as urban and twice in males as females Current raw tobacco chewing was mostly found in the older age groups. It was seen mostly among illiterates and less educated persons. 21,24

43
Source: Nyo Nyo Kyaing et al, Tobacco Free Initiative Project, Department of Health, Household Survey, Myanmar Study on Tobacco Economics, 2001, WHOSEARO Report, 2001.
Figure 2.8 shows the higher prevalence of smoking of cigarettes, cigars and
chewing of tobacco among males, and the higher prevalence of smoking of hand-rolled tobacco among females. Rate of smoking of cheroots was the same in both sexes.
Annual consumption of tobacco products in Myanmar. On an average, a smoker consumes 3-4 smoking tobacco products a day. During 1970-72, the annual adult per capita consumption of manufactured cigarettes was 90. By 1990-92, it increased to 150 and by 1999-2000, it increased to 495. 25 Table (2.30) Annual Consumption of manufactured cigarettes
Year Per capita consumption (sticks)
Total consumption (million sticks)
1970-72 90 1463
1980-82 140 2878
1990-92 150 3920
1999-00 495 15811
Source: WHOSEARO . Country Profiles on Tobacco or Health. New Dehli, 2002.
68 .5 68.8
16.3
25 .9
9 .6
2.1 0.8 0 .3
4.82.9
0
10
20
30
40
50
60
70
C heroo ts H a nd ro lled tobacco C igare ttes C igars C hew ing o f to baccoT ypes o f T obacco
F igure (2 .11) P ercent D is tribution o f T ypes o f T obacco U se W ith in S ex G rou ps, M yanm ar
M aleFem a le

44
NEPAL
Smoking is a common practice in Nepal regardless of age or sex. Prevalence of smoking among Nepalese women is among the highest in the Region along with Myanmar and Maldives. Prevalence of tobacco use among females in Nepal
Several studies had been carried out on prevalence of tobacco use. A few studies were carried out in 1979 and early part of 1980s (Pandey et al., 1988). They are not representative of the whole country, as the sample surveys are purposive. 26. In the early 1980s, 64.2% of the population aged 20 and above were found to be smokers, and the corresponding figures for males and females were 75.5% and 53.6% (Table 2.32). 27 The study on tobacco economics in Nepal shows a smoking prevalence rate of 45% among the population 20 years of age and over, 56.2% for males and 34.1% for females. 24.
Smoking prevalence among the population aged 20 and over was relatively low in the urban areas compared to the rural areas in the 1980s and this pattern remained the same in the 2000 economics study. Smoking rates among females in rural areas was four times greater than in urban areas. It could be stated that female smoking prevalence rates in Nepal were among the highest in the Region. Prevalence rates of female smoking in the rural areas were nearly two to three times higher than the urban areas.
In all regions and at all times, males smoked more than females. Male smoking rates were also among the highest in the Region. The difference between the males and females smoking prevalence rates is smaller among the mountain population than people from other regions. 27
In Table 2.32, prevalence rates of female smoking from various studies were
shown. As the survey designs were different representing different population sub-groups, the findings could not be drawn into a trend line. Table (2.31) Female smoking prevalence in Nepal (1980 to 2001)
Year Age group Smoking female prevalence% Urban Rural Total 1980s a >20 14.2 59.6 53.6 1983 b ? 62.4 2000 c >20 20.7 35.7 34.1 2000 d >15 28.7 2000 c >10 14.8 24.9 23.8 2001e >15 19.9 32.9 44.7
Source: a: Pandey MR, Basnyat, Neupane RP. Chronic bronchitis and cor-pulmonale in Nepal: a scientific epidemiological study.Kathmandu, Mrigendra Medical Trust, 1988.
b. WHO. Tobacco or Health, A Global Status Report, 1997. c. Nepal Health Economics Association, Study on tobacco economics in Nepal, WHOSEARO report 2001. d. WHOSEARO. Country profiles on Tobacco or Health, New Delhi, 2002 e. Karki, YB. High tobacco use in the high hills of Nepal,2002.

45
Smoking prevalence rates differ from 77.7% in Uccha Phadi Pradesh to 37.0% in urban Kathmandu. While 71.7% of females in Uccha Phadi Pradesh smoked, only 14.2% of women in Kathmandu smoked. 27 Smoking prevalence rates by geographical region among Nepalese women for the population 15 years of age and over are shown in Figure 2.9. It was found that smoking prevalence is the highest in the high mountain region, followed by the mid-hills and the Tarain. 26
Adult literacy rate in Nepal is low. The overall literacy rate increased from 27% in 1992 to 39% by 1999. The female literacy rate however remains much lower than the male literacy rate. In 1999, female literacy rate was 23% versus male literacy rate of 58%.
Literacy seems to affect smoking habits. The female literate population is more than four times less likely to smoke (7.5%) than the illiterate population (38.6%). Literacy seems to affect smoking among females much more than among males 31.9% versus 59.9%. 26 In another study in 2002, smoking rates among illiterate females was also reported nearly four times than the literates 44.3% versus 12.6%. 28
Table (2.32) Smoking prevalence rate for female population 10 years of age and
over by ecological region and literacy, Nepal, 2000 Residence Literate % Illiterate % Mountain 14.5 56.1 Hill 9.8 43.9 Tarai 5.8 32.3 Total 7.5 38.6
Source: Nepal Health Economics Association. Study on tobacco economics in Nepal, 2001. WHOSEARO Report,
2001.
Figure (2.12) Female smoking by region, Nepal 2000
54.9
30.323.6
0
10
20
30
40
50
60
Mountain Hill Tarai
Female 15+ %

46
During the mid 1990s a survey was carried out among married women of reproductive age, who were asked (in addition to many other questions), about smoking habits. That survey also reported low smoking prevalence among women who were literate. Much higher percentage of illiterate women (27.6%) was found smoking in their last pregnancy than the literate women (7.4%). (Table 2.34).
Table(2.33) Number of cigarettes/bidi smoked during most recent pregnancy by
literacy, Nepal, 1997 Number Literate (%) Illiterate (%) None 92.6 72.4 0–9 5.3 19.5 10–19 1.4 6.1 20+ 0.7 1.9 Total % 100.0 99.9 Total (n) 1923 1609
Source: NPC, CBS, June 1998. Further analysis report on antenatal, delivery, postnatal services, literacy and polio coverage. Nepal multiple indicator surveillance, fifth cycle (March–May 1997). In collaboration with UNICEF/Nepal.
It was reported that although fewer women smoke compared to male counterparts,
they begin to smoke earlier 15.8 years than their male counterparts 17.0 years which is true in all regions of the country. 26
Prevalence of smoking among female youth in Nepal
Pandey et al., 1987 and Jhan et al., 1999 had collected smoking behaviour data among the young population which were limited to specific areas. According to the survey carried out by Pandey et al 1987 in 1983–84 in a rural hill area, the prevalence of smoking among youths aged 8 to 19 years, was about 12.6%.26
Among young people, smoking was found to be much more common in males (17.3%) than females (6.7%). The Study on Tobacco Economics in Nepal conducted in 2000 showed that smoking prevalence increased with age; among the 16–19 year olds it was about 30%while among the younger ones it was only about 2%. It also reported a 3.8% prevalence rate for 10–19 year olds in the rural population, with more young males smoking (6.1%) than young females (1.4%). Apparently smoking has drastically declined among the young age populations in the rural areas of Nepal in the past 15 years.26 Table (2.34) Youth female smoking in Nepal, (1987-2001)
Year Age group Region Female prevalence %
1987 a 8-19 Rural hill 6.7 2000 b 10-19 Rural 1.4 2001c 13-15 National 6.4
Source: a. Pandey et al
b: Epidemiological study of tobacco smoking behaviour among young people in a rural community of the hill region of Nepal with special reference to attitude and beliefs. Community medicine, 9(2):110–20.
c . GYTS fact sheet

47
Types of tobacco products used in Nepal
Tobacco products in Nepal comprise of manufactured cigarettes of different types
and brands, bidi (dry tobacco wrapped in dry leaves), kakkad/sulfa (tobacco smoked in a clay pipe), hukka (hubble-bubble or water pipe) and various kinds of chewing tobacco.
Among all respondents aged 10 and over, 31.6% were currently smokers and of
them, 79% were cigarette smokers, 8.8%, used bidi, 9.8% used kakkad/sulfa and 2.4% used hukka and 9.4% consume khaini. Data on the quantity of cigarette/bidi sticks showed that females smoked slightly more sticks 2230.7 sticks than males 2138.5 sticks. 26
The bidi smoked in the hills and mountains is not manufactured like a regular
manufactured bidi in the Tarai. In the uplands, the smokers buy loose tobacco and wrap it in dry tree leaves to smoke. This process is much cheaper than buying even the cheapest cigarettes. Also the males smoke more expensive cigarettes than the females. No wonder, as shown above, women, on average consume more cigarette/bidi sticks a year than men but spend less. 26
Traditional forms of smoking such as kakkad/sulfa and hukka are eroding fast in Nepal. 26
Annual consumption of tobacco products in Nepal According to Study on Tobacco Economics, a smoking Nepalese woman smokes about 400 cigarettes and 97 bidis per year. (Table 2.36) Table (2.35) Cigarette and bidi smoking rates (%) for population 15 years of
age and over and estimates of per capita consumption of cigarettes and bidi, Nepal, 2000
Age 15+ Cigarette smoking prevalence rate (%)
Bidi smoking prevalence rate (%)
Cigarettes consumed per capita annually
Bidi consumed per capita annually
Male 40.5 3.27 828 106 Female 20.4 3.51 429 97 Both sexes
30.3 3.40 626 102
Source: Nepal Health Economics Association. Study on tobacco economics in Nepal, 2001.. WHOSEARO Report, 2001.
There is an increase in per capita consumption of tobacco products annually over the years (Table 2.36).

48
Table (2.36) Trend of Annual Consumption of Cigarettes and Bidis in Nepal
Year Cigarette Bidi
Per capita consumption (sticks)
Total consumption (million sticks)
Per capita consumption (sticks)
Total consumption (million sticks)
1970 172 1135 na na 1980 224 1851 na na 1989 626 6695 na na 2000 626 8538 102 1391.8
Source: WHOSEARO: Country Profiles on Tobacco or Health, New Delhi, 2002.
SRI LANKA
Although smoking among men in Sri Lanka was very high, prevalence of smoking among women was relatively low, around 4% to 6% of adults above 15 years. Youth female smoking was also low. Smokeless tobacco use was practiced only among the females in the rural areas and is considered as “village behaviour”. Prevalence of tobacco use among females in Sri Lanka
The first major study conducted on tobacco use in Sri Lanka was in the year 1989 by Randeniya Bernard and Weerasooriya W.A.J of National Cancer Control Programme, “ Smoking Patterns of Sri Lanka” .30 Prior to that, a few epidemiological studies and adhoc surveys have been conducted. Out of these, one of the first available studies was that carried out in Kandy in 1971.31
This study reported that 15.9% of females aged 15 years and above were smokers.
The 1989 study was conducted in four administrative districts with a sample size of 10,000 subjects. It reported female smoking prevalence as only 0.8% which is among the lowest in the Region. The study did not report the prevalence of smokeless tobacco use.
The other two major studies referred in this report are “Consumption, Production and Distribution Patterns of Tobacco, Alcohol and Other Drugs Among the Sri Lankan Population 1992, conducted by Alcohol and Drug Information Center and referred to as TAD 1992 which collected 1991 data and “Sri Lanka Integrated Survey 1999-2000” known as SLIS 2000, which collected 2000 data by World Bank.
The TAD survey obtained information on three districts only: Colombo which is urbanized and developed and Hambantota, and Polonnaruwa, both of which are rural farming districts. However, it collected detailed information on the smoking behavior of individuals. The SLIS (2000) survey, on the other hand, was an island-wide survey weighted to obtain a nationally representative sample. However, it provided information only on the current tobacco use of individuals, where tobacco use include tobacco for smoking as well as tobacco for chewing.

49
Due to differences in coverage, and sample designs, a straightforward comparison of the results of these surveys is difficult, but approximate comparisons of smoking and tobacco use patterns are provided in Table 2.38.
In 1988 , the overall prevalence of cigarette smoking among adults 15 years of age and above was 28.6%, extremely high at 54% for males compared to 0.8% among females. It was found that smoking among men remarkably come down to 25.7% in 2000/2001 although female smoking prevalence has gone up from 0.8%to 1.7%. The Sentinel Tobacco Use Prevalence Study conducted in two districts of Colombo and Matara in 2001, reported the smoking prevalence rate of 8.2% among females although it was lower than males 33.7%. The overall prevalence according to this survey was 20.8%.
Although the vast majority of women in Sri Lanka do not smoke, a number of them chew betel quid. A survey conducted in a village showed that 64% of betel quid chewing females, and 46% of males use tobacco in their betel quid. It also reported also 11% of females chewing tobacco. The highest prevalence of smokeless tobacco use was among those with no schooling and the lowest among high secondary. There was a steady decrease in use as the socio-economic level improved. 30
In both the rural and urban sectors there were more males than females among current smokers. The ratio of male to female current smokers was 1:16 in the rural sector and 1:15 in the urban sector. Studies reported that tobacco use was more common in the rural area than in the urban area. In the case of females it was four times more in rural than urban 13.3 versus 3.2. 30
The Sentinel Prevalence Study also reported a steep decline in the use of tobacco among both sexes with higher education. There was a steep decline up to secondary education and the lowest prevalence was among those with higher secondary education after which there was a slight increase among university graduates and professionals.
Along with an increase in income there was a decline in the current use of tobacco. Table (2.37) Prevalence of tobacco use among females in Sri Lanka
S/N Study Year Study Area Age Group
Female Smoking Prevalence%
Female tobacco use prevalence%
Female Smoke-less Tobacco Use Prevalence %
1. Tobacco Smoking in Sri Lanka a
1971 Kandi 15 and above
15.9
2. Smoking Patterns of Sri Lanka b
1989 Matara Matela Badulla Anuradhapura
12 years and above
0.84
3. Consumption, Production and Distribution Patterns of Tobacco, Alcohol and Other Drugs Among the Sri Lankan
1992 lombo mbantota lonnaruwa
1.0 1.0 1.0

50
Population c 4. Sri Lanka Integrated
Survey d 2000 lombo
mbantota lonnaruwa Lanka
3.0 8.0 4.0 6.0
5. Sentinel Tobacco Use Prevalence Study 2001 e
2001 Colombo (urban) Matara (Rural)
15 + 1.9 1.5 1.7
3.2 13.3 8.2
12 2
6. Epidemiological survey f 2002 Rural 1.0 22 Betel quid with tobacco 64% Chewing tobacco 11%
Source: a: Uragoda C. G and Senewiratna B. “Tobacco Smoking in Sri Lanka”. , Journal of Tropical Medicine and Hygiene, 1971 pp 145-147.
b: Randeniya Bernard and Weerasooriya W.A.J. “ Smoking Patterns of Sri Lanka”, National Cancer Contro Programme, Sri Lanka, 1989.
c: Alcohol and drug information center: Consumption, Production and Distribution Patterns of Tobacco, Alcohol and Other Drugs Among the Sri Lankan Population 1992, known as TAD 1992, Sri Lanka 1992.
d: World Bank. Sri Lanka Integrated Survey 1999-2000, known as SLIS 2000,. e: Olcott Gunasekara. Sentinel tobacco Use Prevalence Study 2001, WHOSEARO Report 2001. f: NCD Unit, MOH: Epidemiological survey , 2002.
Prevalence of Tobacco Use among the female youth in Sri Lanka
The Global Youth Tobacco Survey conducted in 1999 reported prevalence of
female tobacco use prevalence as 6.1%, cigarette smoking prevalence as 1.7% and non-cigarette tobacco use as 5.3%. Cigarette smoking prevalence was higher among males than females, but the gap between boys and girls narrows when it comes to non-cigarette tobacco use. Table (2.38)Youth female smoking, Sri Lanka, 1999
Year Age group
Female cigarette smoking
prevalence %
Non-cigarette tobacco
prevalence among
females%
Female tobacco use prevalence
%
1999 a 13-15 1.7 5.3 6.1 Source: GYTS Fact Sheet
Types of tobacco products used in Sri Lanka
Currently in Sri Lanka, tobacco is consumed in two forms: for smoking and for chewing. Chewing tobacco is used mainly as a complement to betel. Smoking is mainly done in the form of cigarettes, bidis, and cigars. Tobacco is also smoked in pipes, but in

51
very small quantities. According to the Kandi study in 1971, 90.5% of smokers used cigarettes.
Cigarettes constitute the most popular form of tobacco used; however bidis are used by at least 50% of all smokers; among male smokes, about 74% smoked cigarettes, 50% smoked bidis, 15% smoked cigars, 11% chewed tobacco and 0.3% smoked pipes. Among female smokers, about 58%smoked cigarettes, 52% bidis and 21% cigars. 4
The Epidemiological study conducted by NCD Department of Ministry of Health also reported that 21% of female smokers smoked cigars. Hence, in Sri Lanka, a considerable percentage of females smoked cigars which are unusual for women.
According to sentinel prevalence survey, among both sexes, current cigarette smoking was higher than bidi smoking. For females the ratio was for every bidi smoker there were nearly seven cigarette smokers. Prevalence of cigarette smoking among males and females was 1 female smoker to 17 male smokers. For bidi smoking it was 1 female smoker to 22 male bidi smokers.
The difference between urban and rural was not so marked for cigarette smoking. In the case of bidi smoking the prevalence in the rural sector was 14 times more than in the urban sector.
There were more current users of pan quid in the rural sector when compared with the urban sector. It was seven times more for both males and females. Current use of pan quid decreased with education. Annual Consumption of manufactured cigarettes
Annual per capita consumption of manufactured cigarettes is declining in Sri
Lanka. Table (2.39) Trend of Annual Consumption of manufactured cigarettes in Sri Lanka
Year Per capita consumption (sticks)
Total consumption (million sticks)
1970 417 3035 1980 545 5229 1990 464 5329 1995 407 5137 1997 374 4907 1998 367 4848 1999 366 5049
Source: WHOSEARO: Country Profiles on Tobacco or Health 2002

52
THAILAND
Smoking has never been a prevalent past time amongst Thai women. At its height,
around 5% of all Thai women smoked and this has now been reduced to 2.5%. This decline has been in absolute numbers as well, despite population increases. However certain groups of women smoke at a much higher rate. One such group is women in the northern region where 8.2% smoke. Tobacco is grown in this region and smoking amongst women has a longer history than other areas. Lung cancer is the most common form of cancer amongst northern Thai women reflecting their higher rate of smoking. This area has also experienced the greatest decline in the rate of women smoking, which has remained static elsewhere in Thailand. 32
Those with higher level of education are less likely to smoke than those with little education. Smokers living in rural areas are switching from hand-rolled to manufactured cigarettes, and smokers of non-filter cigarettes are in turn switching to filtered cigarettes. The groups most inclined to smoke imported cigarettes are medium to high income earners, youths, and women. 4
Prevalence of smoking among females in Thailand
In Thailand, males smoke much more than females. In 1986, the percentage of male smokers was 57.6% compared to 4.8% of females. Both male and female smoking has declined over the years and by 1999, the proportion of male smokers was 44.1% compared to 2.6% of females. But the gap between males and females has widened in the last 13 years. Male intensity compared to females increased from 12 fold in 1986 to 17.0 in 1999. 9 (Table 2.41) Table (2.40) Female Smoking prevalence in Thailand, 1976 to 2001.
Year Female prevalence % 1976 a 6 1986b 4.8 1991b 4.4 1995 a 4 1996b 2.7 1999b 2.6 1999 c 2.4 2001d 2.2
Source: a : WHO: Tobacco or Health: A Global Status Report, 1997. b: National Statistical Office, Office of the Prime Minister, National Surveys in 1986,1996 and 1999. c: National Statistical Office, Thailand: Report of Health and Welfare Survey. d :National Statistical Office(2001): The survey of cigarette smoking

53
Table (2.41) Estimated smoking prevalence trends by sex and population aged 15 or more and males’ intensity of smoking compared to females in Thailand 1986-1999
Year Both sexes Smoking
population Males Females Males
intensity compared to females
1986 30.9 10.4 57.6 4.8 12.0 1991 29.8 29.8 56.0 4.4 12.7 1996 25.5 25.5 49.2 2.7 18.2 1999 22.9 22.9 44.1 2.6 17.0
Source: National Statistical Office, Office of the Prime Minister, National Surveys in 1986,1996 and 1999.
In relative terms, smoking participation rate tends to be higher in rural areas than in urban areas. Around 22% of rural Thais who were not less than 11 years old smoked while only 16% of urban Thais in the same age-category smoked. It should be added that the difference was mainly caused by the rate of male heavy smokers, which was approximately 41% in rural areas, but over 29% in urban areas. (Table 2.42) Smoking rates were much higher among males than females, irrespective of area. If there are no effective preventive measures, female smoking could be a very attractive target for cigarette companies.
Table (2.42) Smoking prevalence by urban/rural division, sex and smoking habit,
Thailand, 1999
Smoking habit Total % Urban % Rural % Regular smoker
20.50 15.24 21.98
Male Regular smoker
38.86 29.73 41.34
Female Regular smoker 2.36 1.65 2.56 Note: In this survey, urban means areas covered by Bangkok metropolis and municipal areas. Source: National Statistical Office, Thailand. : Report of Health and Welfare Survey The study in 1996 reported 2.3% of urban females compared to 3.5% of rural
females. It was highest in the North (8. 2% )(Table 2.44).
Table (2.43) Smoking prevalence among Thai women by Region, 1996 Residence Women smokers % Former Smokers
(women)% Thailand 3.2 0.9 Urban 2.3 0.6 Rural 3.5 1.0 Bangkok 2.5 0.7 Central 2.6 0.5 North 8.2 3.4 North-East 1.3 0.2
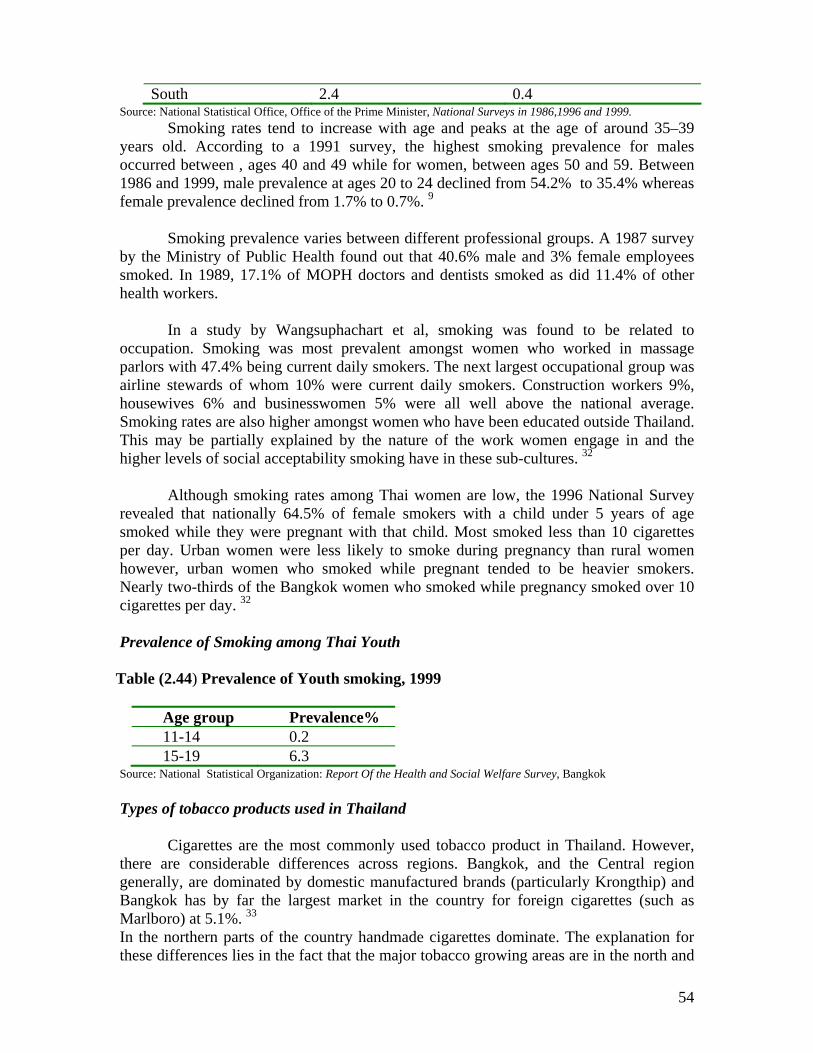
54
South 2.4 0.4 Source: National Statistical Office, Office of the Prime Minister, National Surveys in 1986,1996 and 1999.
Smoking rates tend to increase with age and peaks at the age of around 35–39 years old. According to a 1991 survey, the highest smoking prevalence for males occurred between , ages 40 and 49 while for women, between ages 50 and 59. Between 1986 and 1999, male prevalence at ages 20 to 24 declined from 54.2% to 35.4% whereas female prevalence declined from 1.7% to 0.7%. 9
Smoking prevalence varies between different professional groups. A 1987 survey
by the Ministry of Public Health found out that 40.6% male and 3% female employees smoked. In 1989, 17.1% of MOPH doctors and dentists smoked as did 11.4% of other health workers.
In a study by Wangsuphachart et al, smoking was found to be related to occupation. Smoking was most prevalent amongst women who worked in massage parlors with 47.4% being current daily smokers. The next largest occupational group was airline stewards of whom 10% were current daily smokers. Construction workers 9%, housewives 6% and businesswomen 5% were all well above the national average. Smoking rates are also higher amongst women who have been educated outside Thailand. This may be partially explained by the nature of the work women engage in and the higher levels of social acceptability smoking have in these sub-cultures. 32
Although smoking rates among Thai women are low, the 1996 National Survey revealed that nationally 64.5% of female smokers with a child under 5 years of age smoked while they were pregnant with that child. Most smoked less than 10 cigarettes per day. Urban women were less likely to smoke during pregnancy than rural women however, urban women who smoked while pregnant tended to be heavier smokers. Nearly two-thirds of the Bangkok women who smoked while pregnancy smoked over 10 cigarettes per day. 32 Prevalence of Smoking among Thai Youth
Table (2.44) Prevalence of Youth smoking, 1999
Age group Prevalence% 11-14 0.2 15-19 6.3
Source: National Statistical Organization: Report Of the Health and Social Welfare Survey, Bangkok
Types of tobacco products used in Thailand
Cigarettes are the most commonly used tobacco product in Thailand. However, there are considerable differences across regions. Bangkok, and the Central region generally, are dominated by domestic manufactured brands (particularly Krongthip) and Bangkok has by far the largest market in the country for foreign cigarettes (such as Marlboro) at 5.1%. 33 In the northern parts of the country handmade cigarettes dominate. The explanation for these differences lies in the fact that the major tobacco growing areas are in the north and
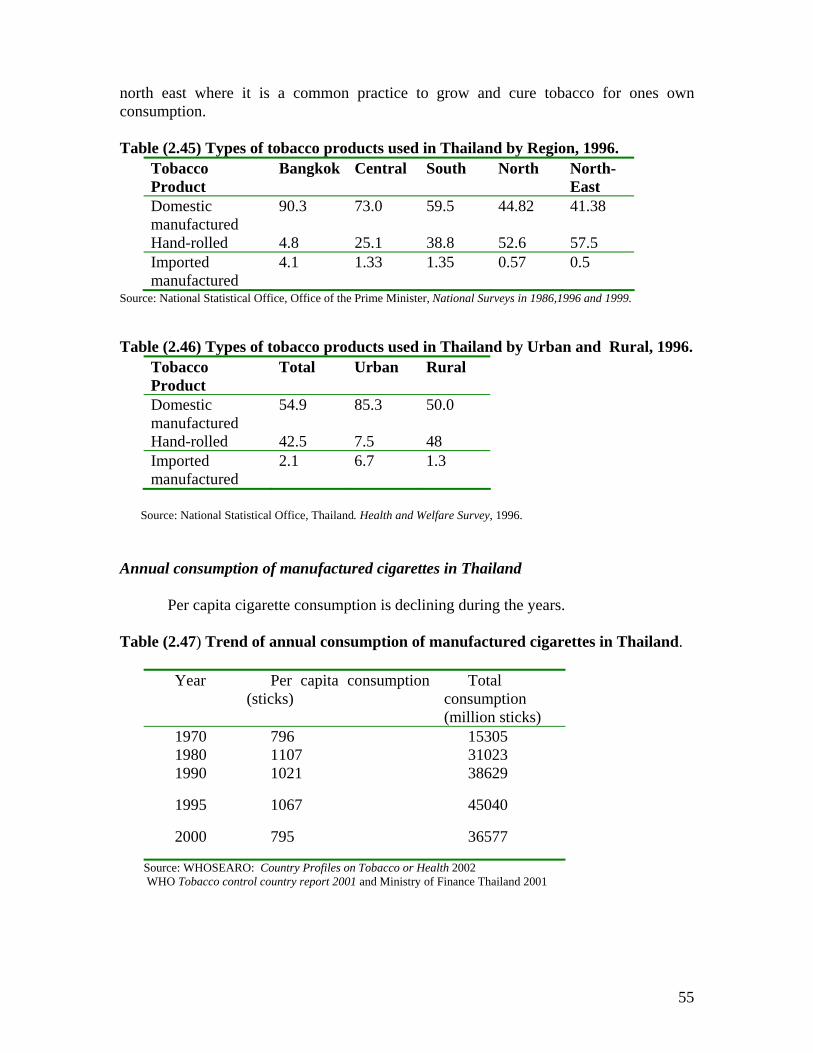
55
north east where it is a common practice to grow and cure tobacco for ones own consumption. Table (2.45) Types of tobacco products used in Thailand by Region, 1996.
Tobacco Product
Bangkok Central South North North-East
Domestic manufactured
90.3 73.0 59.5 44.82 41.38
Hand-rolled 4.8 25.1 38.8 52.6 57.5 Imported manufactured
4.1 1.33 1.35 0.57 0.5
Source: National Statistical Office, Office of the Prime Minister, National Surveys in 1986,1996 and 1999.
Table (2.46) Types of tobacco products used in Thailand by Urban and Rural, 1996. Tobacco Product
Total Urban Rural
Domestic manufactured
54.9 85.3 50.0
Hand-rolled 42.5 7.5 48 Imported manufactured
2.1 6.7 1.3
Source: National Statistical Office, Thailand. Health and Welfare Survey, 1996.
Annual consumption of manufactured cigarettes in Thailand
Per capita cigarette consumption is declining during the years. Table (2.47) Trend of annual consumption of manufactured cigarettes in Thailand.
Year Per capita consumption (sticks)
Total consumption (million sticks)
1970 796 15305 1980 1107 31023 1990 1021 38629
1995 1067 45040
2000 795 36577
Source: WHOSEARO: Country Profiles on Tobacco or Health 2002 WHO Tobacco control country report 2001 and Ministry of Finance Thailand 2001

56
References
1. Dr. Judith Mackey and Dr. Michael Erikson. The Tobacco Atlas. WHO. 2002.
2. Shoba John and Shailesh Vaite. Tobacco and Poverty: Observations from India and Bangladesh. PATH Canada. October, 2002.
3. Bangladesh Institute of Development Studies. Craving for Nicotine: A study on Tobacco Prevalence in Bangladesh . Dhaka..June 2001
4. World Health Organization. Tobacco or Health: A Global Status Report. World Health Organization, Geneva, 1997.
5. Bangladesh Bureau of Statistics. Prevalence of Smoking in Bangladesh, Dhaka , November, 1995
6. Efforymson D. and Saifuddin A. Hungry for Tobacco: An analysis of the economic impact of tobacco on the poor in Bangladesh. PATH Canada. July 2000.
7. Bangladesh Bureau of Statistics, Report of Survey on Prevalence of Morbidity, Treatment Expenditures, Fertility, Immunization and Smoking, July 1997.
8. Zulfiqar Ali , Atiur Rahman and Taifur.“ A Study on Tobacco Economics” . HNP Discussion paper. Economics of Toabcco Control paper No. 16. Tobacco Free Initiative World Health Organization. November 2003.
9. World Health Organization, Regional Office for South-East Asia Region. Country Profiles on Tobacco or Health, World Health Organization, Regional Office for South-East Asia Region New Delhi, 2002
10. WR-India . Tobacco or Health Country Profile India 2001, unpublished
11. PC Gupta. Survey of socio- demographic characteristics of tobacco use among 99,598 individuals in Bombay, India using handheld computers . Tobacco Control, vol 5,114-120. BMJ publishing group.
12. Sinha D N, Gupta PC, Pednekar MS, Jones JT and Warren CW. Tobacco use among school personnel in Bihar, India, Tobacco Control 2002:11:82-83.
13. Gopalan S, Shiva M, editors. National profile on women, health and development: India. New Dehli: Voluntary Health Association of India; 1999
14. Chaturvedi HK, et.al. Tobacco use in Mizoram, India: socioeconomic differences in pattern. Southeast Asian j Tropical Medicine Public Health 1998.
15. Indian Council of Medical Research. Prevalence of Tobacco Use in Karnataka and Uttar Pradesh, 2001. WHO/SEARO Report, 2002.
16. Sinha D. N and Gupta, P.. Tobacco use among students of Patna Dental College, Bihar, LIFELINE, WHO,SEARO.v 7:11-12, January 2002.
17. Barraclough S. Women and tobacco in Indonesia. Tobacco Control 1999; 8;327-332.
18. Thomas Ganiwijaya et.al. Prevalence of smoking in a rural area of West java, Indonesia. Tobacco Control 1995, 4:335-337.
57
19. Demographic Institute Faculty of Economics , University of Indonesia, An economic analysis of tobacco control in Indonesia, 2001, WHO/SEARO Report, 2001.
20. Ahmed Afaal and I. Riaz Shareef. Economics of tobacco control –The Maldives. HNP Discussion Paper.Economics of Tobacco Control Paper No. 17. Tobacco Free Initiative World Health Organization. November 2003.
21. Nyo Nyo Kyaing :Myanmar sentinel tobacco use prevalence study 2001, WHOSEARO Report, 2001.
22. Nyo Nyo Kyaing et al, Myanmar GYTS Report, 2001.
23. Myo Oo, Tracy Sein et al., Department of Preventive and Social Medicine, Institute of Medicine 1. Prevalence trend of youth smoking in 29 townships of Bago, Magwe and Mandalay divisions, September 1999.
24. Nyo Nyo Kyaing et al, Tobacco Free Initiative Project, Department of Health, Household Survey, Myanmar Study on Tobacco Economics, 2001. WHO SEARO Report .
25. Fric, Anton. Fact sheet on Tobacco Situation in Myanmar. WHOSEARO. Draft Report, 2001.
26. Yagya B. Karki. Kiran Dev Pant and Badri Raj Pande. Study on tobacco economics in Nepal. HNP Discussion Paper. Economics of Tobacco Control paper No.13..
27. Pandey MR, Basnyat, Neupane RP, Chronic bronchitis and cor-pulmonale in Nepal: a scientific epidemiological study.Kathmandu, Mrigendra Medical Trust, 1988.
28. Karki, YB. High tobacco use in the high hills of Nepal, 2002.
29. Nisha Arunatilake and Maduwanthi Opatha: The Economics of Tobacco in Sri Lanka. HNP Discussion paper. Economics of Tobacco Control Paper No. 12. Tobacco Free Initiative. World Health Organization . October 2003.
30. Olcott Gunasekara. Sentinel tobacco Use Prevalence Study 2001, WHOSEARO Report 2001.
31. Uragoda C. G and Senewiratna B. “Tobacco Smoking in Sri Lanka”. , Journal of Tropical Medicine and Hygiene, 1971 pp 145-147.
32. ASH Thailand: Thai Women and Tobacco: Internet. www.tobaccofreeasia.com
33. National Statistics Office. 'Report of the Health and Welfare Survey',1996,
34. Ministry of Health Republic of Indonesia. The Tobacco Source Book: Data to Support a National Tobacco Control Strategy. English Summary, Jakarta, December 3, 2003.
35. Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiaitve. World Health Organization. October 2003.

58
PART THREE: HEALTH CONSEQUENCES OF TOBACCO USE
Health risks for women who smoke
Many studies have reported the negative health consequences of tobacco use among women. It has been estimated that women smokers who die of a smoking related disease lose on average 14 years of potential life. 1 Use of tobacco, including smokeless tobacco, is estimated to have caused more than 100,000 female deaths in developing countries in 1995. It is also estimated that women will account for an increasing proportion of all smoking- attributable deaths in coming years. The gender gap between men and women closes as smoking prevalence in women approximates that of men. 2
Health consequences of smoking among women is summarized in the following :
Cancers
Dozens of epidemiologic studies had demonstrated that smoking is strongly associated with an increased risk of lung cancer in women, and that risk increases with duration and amount of smoking and decreases with time since smoking cessation. Among women in developed countries as a whole, lung cancer ranks third among all cancers in both number of new cases and deaths, after cancers of the breast and colon. Among women in developing countries as a whole, lung cancer ranks fifth among cancers in numbers of new cases and deaths, after cancers of the colon, rectum, cervix, breast and stomach. 2
In 1995, an estimated one-third of all cancer deaths in developed countries 47% of male cancer deaths and 14% of female cancer deaths were attributable to smoking. Worldwide in 1990, approximately 10% of female cancer deaths resulted from smoking. Cigarette smoking is the major cause of lung cancer among women. Age-adjusted lung cancer mortality rates among US women have increased nearly 600% since 1950. In countries where smoking among women became common relatively early in the 20th century, the vast majority of lung cancer deaths are due to smoking. In the United States, about 90% of all lung cancer deaths are attributable to smoking. Lung cancer rates are intermediate or remain low in populations of women in whom smoking was adopted later or is still relatively uncommon. 2
Smoking is also the major cause of cancer of the oropharynx and bladder among women. Evidence is also strong that women who smoke have increased risk for cancer of the pancreas and kidney. For cancer of the larynx and oesophagus, evidence that smoking increases the risk among women is more limited but consistent with large increases in risk. 1
Women who smoke may have a higher risk for liver cancer and colorectal cancer than women who do not smoke. Smoking is consistently associated with an increased risk

59
for cervical cancer. The extent to which this association is independent of human papilloma virus infection is uncertain.1
Cardio-vascular diseases 1,2
Smoking is a major cause of coronary heart disease among women. Risk increases with the number of cigarettes smoked and the duration of smoking.
Women who smoke have an increase risk for --
• coronary heart disease
• ischaemic stroke
• sub-arachnoid haemorrhage
• peripheral vascular arthrosclerosis
Reproductive Health 1,2
Women smokers experience unique risks related to menstrual and reproductive function. Women who smoke have:
• Increased risk for primary and secondary fertility
• Increased risk for conception delay
• Increase in risks for ectopic pregnancy and spontaneous abortion
• Increased risk for adverse pregnancy outcomes:
premature rupture of membranes
abruptio placentae placenta separation from the uterus
placenta praevia abnormal location of the placenta
preterm delivery
giving birth to low-birth-weight infant babies and small for gestational age babies which is associated with perinatal, neonatal, and infant morbidity and mortality, the longer the mother smokes during pregnancy, the greater the effect on the infant’s birth weight.
giving birth to stillborn child death of infant in peri-natal period and the risk for sudden infant death
syndrome
60
• Women who smoke are less likely to breast-feed their infants than are women who do not.
Women who quit smoking before or during pregnancy reduce the risk for adverse reproductive outcomes, including difficulties in becoming pregnant, infertility, and premature rupture of membranes, preterm delivery and low-birth weight. 1
Some studies suggest that cigarette smoking may alter menstrual function by increasing the risks for painful menstruation, secondary ammenorrhoea and menstrual irregularity. Women smokers have natural menopause at a younger age than do nonsmokers, and they may experience more severe menopausal symptoms.1
Others
Smoking is the primary cause of chronic obstructive pulmonary diseases, including bronchitis and emphysema in women, and the risk increases with the amount and duration of smoking. Mortality rates for Chronic Obstructive Airway Disease have increased among women for the past 20 to 30 years.
Women who smoke have an increased risk of hip fracture. They also have a moderately elevated risk for rheumatoid arthritis, cataract and age-related macular degeneration.
Prevalence of smoking is generally higher for women with anxiety disorders, bulimia, depression, attention deficit disorder and alcoholism; it is particularly high among patients with diagnosed schizophrenia. 1
Health Consequences for women who are exposed to ETS
Exposure to ETS is a cause of lung cancer among women nonsmokers. Studies also support a causal relationship between exposures to ETS and coronary heart disease among women nonsmokers.
Infants born to women who are exposed to ETS during pregnancy may have a small decrement in birth weight and a slightly increased risk for intrauterine growth retardation. 1
Health risks for women who use smokeless tobacco
Chewing of tobacco and chewing of betel quid with tobacco is highly associated with many cancers such as cancer of the mouth, lips, tongue etc. The highest reported incidence rate for cancer of the mouth is among women in Bangalore, India where women have considerably higher rates than men; this pattern is also found in Madras in India. 5

61
Women who chew tobacco gave birth to babies weighing anywhere from 100 to 400 gram less than delivered by women with no habit. The crude still birth rate per 1,000 births was 50 in women who chewed tobacco as compared to a rate of 17.1in women who did not use tobacco. 5
Burden of diseases attributable to smoking
Smoking habits started in the industrialized and spread to developing countries. Among industrialized countries where the habit of smoking has been common for decades, previously among men and followed by women, smoking is estimated to cause over 90% of lung cancer in women. Lung cancer is overtaking breast cancer as the commonest malignancy of women in the parts of the world where smoking is increasing like in countries of central and Eastern Europe and also in Western Europe wherever women have not refrained from smoking.
Lung cancer is only one of innumerable adverse health consequences of smoking for women. In 1985, lung cancer accounted for approximately 21% of all smoking-attributable deaths among women in developed countries, in other words, about 79% of tobacco’s toll was due to diseases other than lung cancer. Smoking is one of the major causes of coronary heart disease in women. Relative risks of coronary heart disease associated with smoking are greater for younger women than for older women. The relative risk of chronic obstructive airway disease was 12.8 in current smokers compared with nonsmokers. Approximately 90% of chronic obstructive pulmonary disease in CPSII was attributable to smoking.1
In the industrialized countries, the attributable fractions are 56-80% for chronic respiratory disease and 22% for cardiovascular disease. Worldwide, it is estimated that tobacco causes about 8.8% of deaths (4.9 million) and 4.1% of DALYs (59.1 million). As smoking is more common among males than females worldwide, attributable mortality is greater in males (13.3% ) than females (3.8%) .2 In 1995, an estimated one-third of all cancer deaths in developed countries 47% of male cancer deaths and 14% of female cancer deaths were attributable to smoking. Risks for many cancers are increased among women who smoke, including cancers of the lung, mouth, pharynx, esophagus, larynx, bladder, pancreas, kidney and cervix. Worldwide in 1990, approximately 10% of female cancer deaths resulted from smoking. 1
Worldwide, the attributable fractions for tobacco were about 12% for vascular disease, 66% for trachea bronchus and lung cancers and 38% for chronic respiratory disease, although the pattern varies by sub region. Approximately 16% of the global attributable burden occurred in the South-East Asia Region. Attributable mortality of tobacco in high mortality developing countries in South-East Asia Region is 7% of total

62
for males and 1.5% of total for females. For low mortality developing countries SEAR the figures are 12.2% of total for males, and 2.9% of total for females. 3
Table 3.1 Mortality Attributable to Smoking, by Region
WHO Region Cigarette consumption per capita1 in pieces
Number of mortality in thousands
Africa 480 125 The Americas 1,530 772 Eastern Mediterranean 890 182 Europe 2,080 1,273 South East Asia 415 580 Western Pacific 1,945 1, 093 World Total 1,325 4 ,023
Source: WHO. The World Health Report: Archives 1995-2000. WHO 1995, page 67
Burden of diseases attributable to smoking in South-East Asia Region
Tobacco use and tobacco related illness is a serious health problem in the region. WHO estimates that approximately 500,000 tobacco-related deaths occurred in the South-East Asia Region. Evidence shows that the health consequences of tobacco are indeed more serious in women. It is coming out that women smokers develop lung cancer earlier than men despite starting smoking at a later age and smoking fewer cigarettes or bidis than men.4
Tobacco-related illnesses such as cancer, cardiovascular and respiratory diseases are already major problems in most countries in the Region. Approximately half of all cancers in men in India are tobacco related, while over 60% of those suffering from heart disease below the age of 40 are smokers. There is an estimated 12 million cases of preventable tobacco related illnesses each year in India. In Sri Lanka, it is estimated that over 43% reported of cancers are tobacco related. Oral carcinoma is the most prevalent form of cancer in Sri Lanka and cardiovascular diseases is the leading cause of death.4
Thailand reports 10,000 cases of tobacco related lung cancer each year. In India, tobacco attributable mortality has been estimated to be 80,000 per year while in Indonesia, the Ministry of Health estimated that in the year 2001, there were 5.3 million persons, 2.6 million males and 2.8 million females who were sick with tobacco-

63
attributable illnesses. The estimated number of deaths attributable to tobacco in the same year was 412,964 persons, 211,271 males and 201,639 females.
India had one of the highest oral cancers in the world. The highest reported incidence rate in the world for cancer of the mouth is among women in Bangalore, India where women have considerably higher rates than men; this pattern is also found in Madras again in India. 4
The infants of mothers who smoke during pregnancy have birth weights approximately 200 to 250 g lower, on average, than infants born to nonsmoking women and they are more likely to be small for gestational age. Research in India has confirmed that babies born to women who smoke bidis during pregnancy are on average 200 g lower in body weight. Also in India women exposed to passive smoking has been reported to deliver low birth weight babies with a proportion of 1.8 to 1 who are not exposed.5
Risks of stillbirth, neonatal death and sudden infant death syndrome are also greater among the offspring of women who smoke.
For the countries in most of Asia, which have very high smoking rates among men and low prevalence among women, the prevalence data for men imply that the majority of women are exposed to tobacco smoke. Environmental Tobacco Smoke (ETS) is a major women’s issue in SEAR, where rates of smoking for women has been traditionally low compared with men. For women, pregnancies represent a period of particular vulnerability, during which exposure to tobacco smoke may adversely affect the developing fetus.
Exposure of women with asthma to ETS is also concern as a factor that might exacerbate the disease. Involuntary smoking in adults increases the risk of lung cancer in non-smoking women married to smoking men, studies conducted in the USA showed the RR of 1:19 for passive smoking. In Bangladesh, women who were passive smokers of bidis during pregnancy had twice the number of perinatal deaths than those women from similar characteristics but who were married to companions with no tobacco habit.6
Hazards of tobacco also include occupational hazards of workers employed at the tobacco industry. In India and Bangladesh, it is estimated that only about 10% of bidis are made at the factory. The rest are rolled at home. Women constitute 50% of the work force of many cigarette and bidi making industries in the Region and suffer similar tobacco-related occupational hazards as their male counterparts.
Many Muslim women who would not work at all, work in the bidi industry because it allows them to work at home. 5

64
Estimates of tobacco workers in India are 6 million for rolling bids and 4 million for collecting leaves. Since it involves working at home it includes children especially girls. In all steps of bidi workers 65% happen to be women and there are 15% children mostly girls. Women are paid less than men and children the least of all for the same work.
Health hazards of bidi industry include the following: 7,8
• accidents such as falling from trees, snake bites and insect bites during tendu collection
• long hours of continuous sitting cross legged in unhealthy atmosphere doing a monotonous job; lack of exercise---- backaches, muscle pain, joint pain--- rheumatic syndromes stunted growth in girl children
• chronic asthma, allergies • piles • stomach troubles • prone to TB due to inhalation of tobacco dust in crowded areas. • impaired vision • Abuse and harsh treatment by the supervisors and employers
In the study conducted by Dr. M Rahman and T Fukui in 2000, it was stated that concentrations of nicotine, tar and other toxic agents in the smoke are higher for bidi than for other cigarettes. It also stated that bidi smoking is considered to cause about 2-3 times greater nicotine and tar inhalation than do conventional cigarettes, due to the poor combustibility of the bidi wrapper and greater puff frequency needed to keep the bidi light. Overall toxicity is higher in bidi smoke compared to cigarettes. Since bidi is hand-rolled, workers employed in bidi factories are at risk of developing cancerous conditions due to exposure to tobacco-dust and flakes. 13 A study by Suriani in 1996 80 tobacco farmers in Temanngung , Central Java found that the rate of Green Tobacco Sickness incidence is 63.7%. Common complaints are dizziness, headache and fatigue.
Table (3.2) Female Mortality from Cancer in 2000 for SEAR countries, World age-standardized mortality rate per 100,000 population, all ages
Female ASR Cancer
Bangladesh DPK India Indonesia Myanmar Nepal Sri Lanka
Thailand
Oral cavity 9.78 0.33 4.43 0.54 2.05 5.03 7.05 2.40 Nasopharynx 0.35 0.06 0.18 1.25 1.34 0.24 0.05 0.81 Other 3.54 0.11 1.32 0.19 1.37 1.45 1.82 0.45
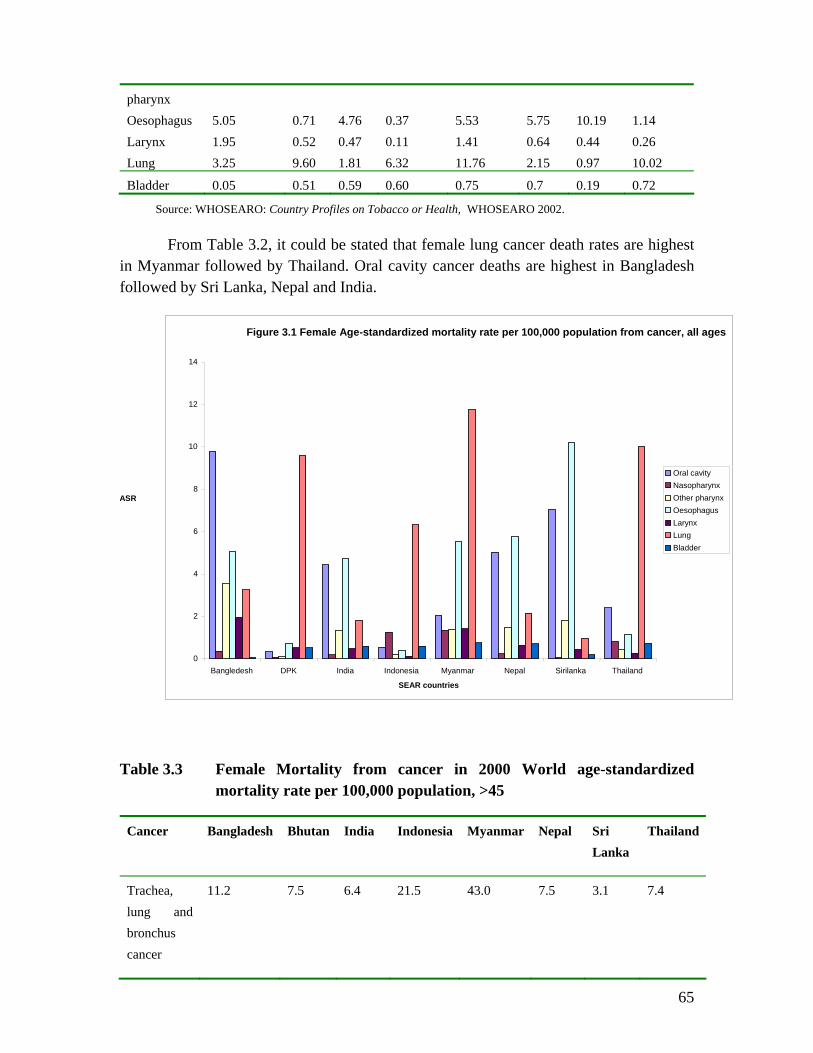
65
pharynx Oesophagus 5.05 0.71 4.76 0.37 5.53 5.75 10.19 1.14 Larynx 1.95 0.52 0.47 0.11 1.41 0.64 0.44 0.26 Lung 3.25 9.60 1.81 6.32 11.76 2.15 0.97 10.02
Bladder 0.05 0.51 0.59 0.60 0.75 0.7 0.19 0.72
Source: WHOSEARO: Country Profiles on Tobacco or Health, WHOSEARO 2002.
From Table 3.2, it could be stated that female lung cancer death rates are highest in Myanmar followed by Thailand. Oral cavity cancer deaths are highest in Bangladesh followed by Sri Lanka, Nepal and India.
Table 3.3 Female Mortality from cancer in 2000 World age-standardized mortality rate per 100,000 population, >45
Cancer Bangladesh Bhutan India Indonesia Myanmar Nepal Sri Lanka
Thailand
Trachea, lung and bronchus cancer
11.2 7.5 6.4 21.5 43.0 7.5 3.1 7.4
Figure 3.1 Female Age-standardized mortality rate per 100,000 population from cancer, all ages
0
2
4
6
8
10
12
14
Bangledesh DPK India Indonesia Myanmar Nepal Sirilanka Thailand SEAR countries
ASR Oral cavityNasopharynxOther pharynxOesophagusLarynxLungBladder
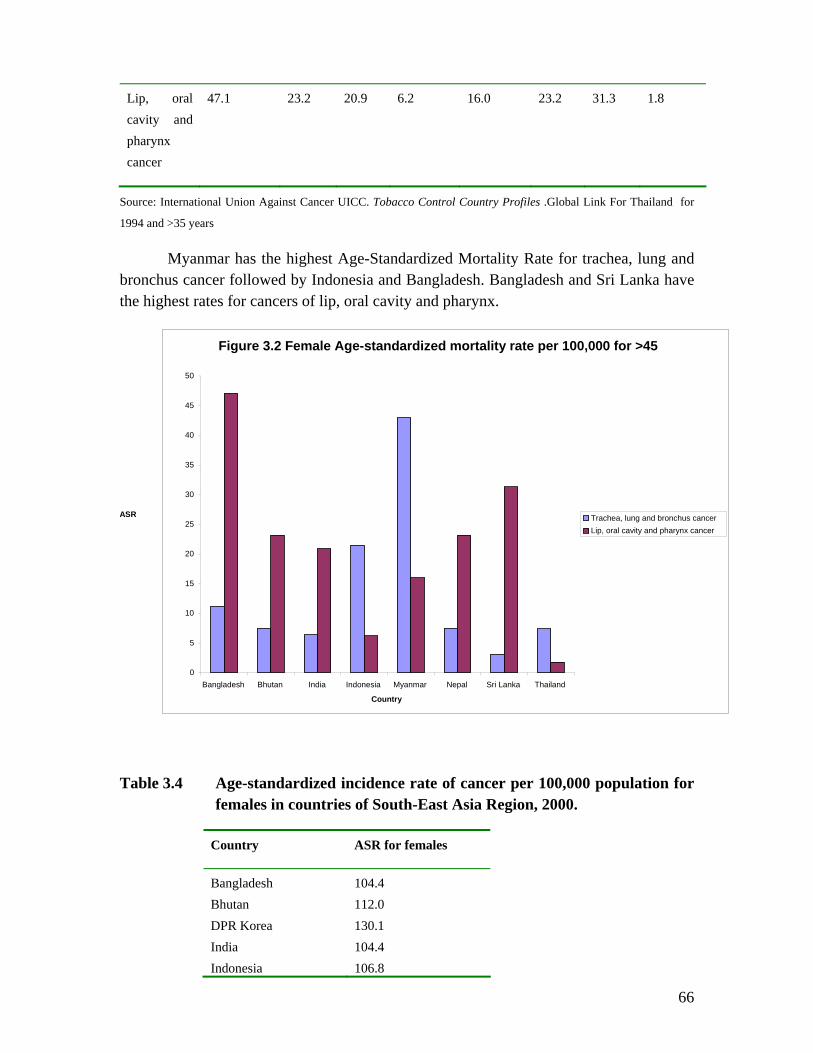
66
Lip, oral cavity and pharynx cancer
47.1 23.2 20.9 6.2 16.0 23.2 31.3 1.8
Source: International Union Against Cancer UICC. Tobacco Control Country Profiles .Global Link For Thailand for
1994 and >35 years
Myanmar has the highest Age-Standardized Mortality Rate for trachea, lung and bronchus cancer followed by Indonesia and Bangladesh. Bangladesh and Sri Lanka have the highest rates for cancers of lip, oral cavity and pharynx.
Table 3.4 Age-standardized incidence rate of cancer per 100,000 population for females in countries of South-East Asia Region, 2000.
Country ASR for females
Bangladesh 104.4 Bhutan 112.0 DPR Korea 130.1 India 104.4 Indonesia 106.8
0
5
10
15
20
25
30
35
40
45
50
Bangladesh Bhutan India Indonesia Myanmar Nepal Sri Lanka Thailand
Country
ASR Trachea, lung and bronchus cancerLip, oral cavity and pharynx cancer
Figure 3.2 Female Age-standardized mortality rate per 100,000 for >45

67
Maldives NR Myanmar 117.8 Nepal 112.0 Sri Lanka 104.4
Thailand 117.9
Source; GLOBOCAN 2000-International Agency for Research on Cancer, WHO
BANGLADESH
Morbidity from Tobacco Use in Bangladesh
The Bangladesh Cancer Society estimates that a significant proportion of all cancers in the country are related to tobacco use. Cancers of the oral cavity, pharynx and larynx account for 30% of all cancers in Bangladesh. 9 Of all cancers in Bangladesh, 62.4% affected males and 37.6% affected females. The common cancers among males were that of bronchus/lung 28%, larynx 7.5% and oesophagus 6%. Among females 19% of cancers were due to cancer cervix while 17% were due to breast cancers. Almost 13% of cancers in women were related to bronchus/lung. 17
A hospital-based study found oral cancer as one of the common cancers in Bangladesh. It was observed that oral cancers were common in older age groups, and the proportion was higher in males compared to females. Both smoking and chewing were associated with oral cancers among males while among females, chewing of tobacco with betel quid appeared to play a dominant role. 9
A hospital-based case-control study conducted in Rajshahi in 1999 , Bangladesh suggested that bidi smoking may well play a more important role in causing thromboangitis obliterans (Buerger’s disease) in Bangladesh. It leads to the speculation that unprocessed and low-grade tobacco used for producing bidi might play a more potent role to initiate the disease than cigarettes. 15 Buerger’s disease mainly affects young male smokers, although very few cases have been reported in ex-smokers and smokeless tobacco users, in those over 50 years old and among women.
Morbidity due to Second-hand Smoking in Bangladesh
A study on prevalence of acute respiratory tract infection and its risk factors in under five children was conducted in 1997 to determine the prevalence and risk factors of the disease among under five children in a rural community in Bangladesh. The prevalence of ARI was 58.7% and mean number of episodes of ARI was 1.75 per child per year. Among studied risk factors parental smoking 61% vs. 39% was found in significantly higher proportions in ARI victims compared to those without ARI. 12
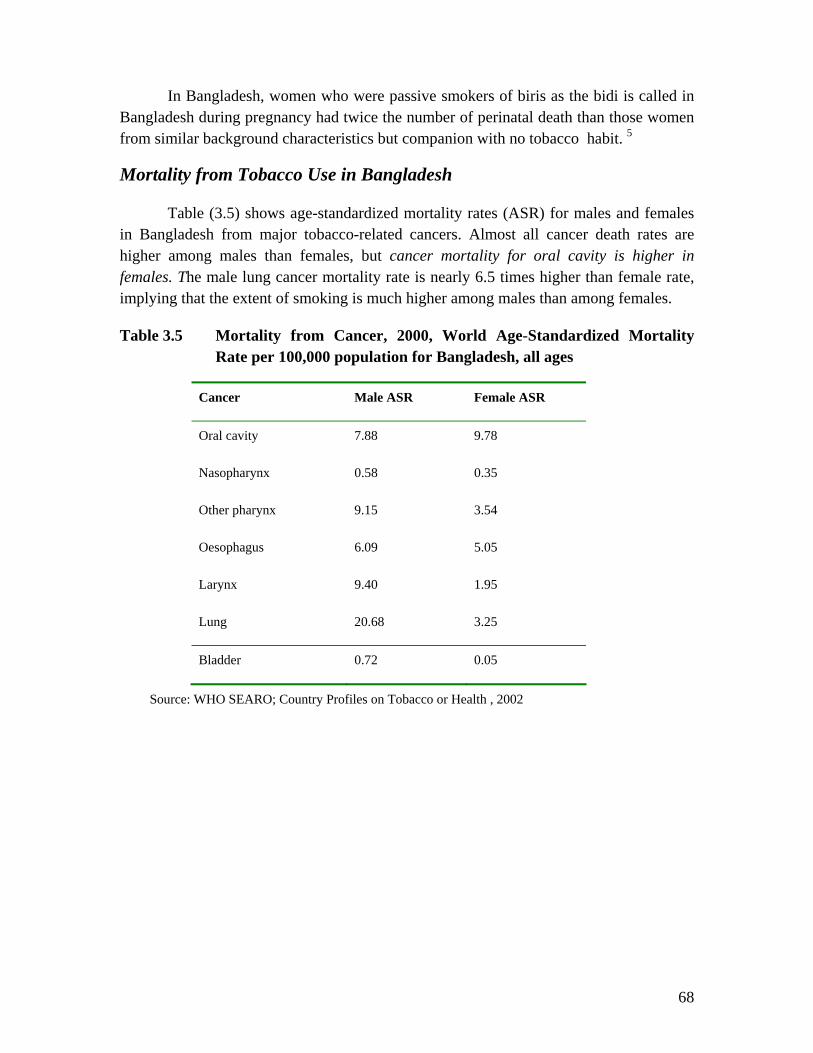
68
In Bangladesh, women who were passive smokers of biris as the bidi is called in Bangladesh during pregnancy had twice the number of perinatal death than those women from similar background characteristics but companion with no tobacco habit. 5
Mortality from Tobacco Use in Bangladesh
Table (3.5) shows age-standardized mortality rates (ASR) for males and females in Bangladesh from major tobacco-related cancers. Almost all cancer death rates are higher among males than females, but cancer mortality for oral cavity is higher in females. The male lung cancer mortality rate is nearly 6.5 times higher than female rate, implying that the extent of smoking is much higher among males than among females.
Table 3.5 Mortality from Cancer, 2000, World Age-Standardized Mortality Rate per 100,000 population for Bangladesh, all ages
Cancer Male ASR Female ASR
Oral cavity 7.88 9.78
Nasopharynx 0.58 0.35
Other pharynx 9.15 3.54
Oesophagus 6.09 5.05
Larynx 9.40 1.95
Lung 20.68 3.25
Bladder 0.72 0.05
Source: WHO SEARO; Country Profiles on Tobacco or Health , 2002
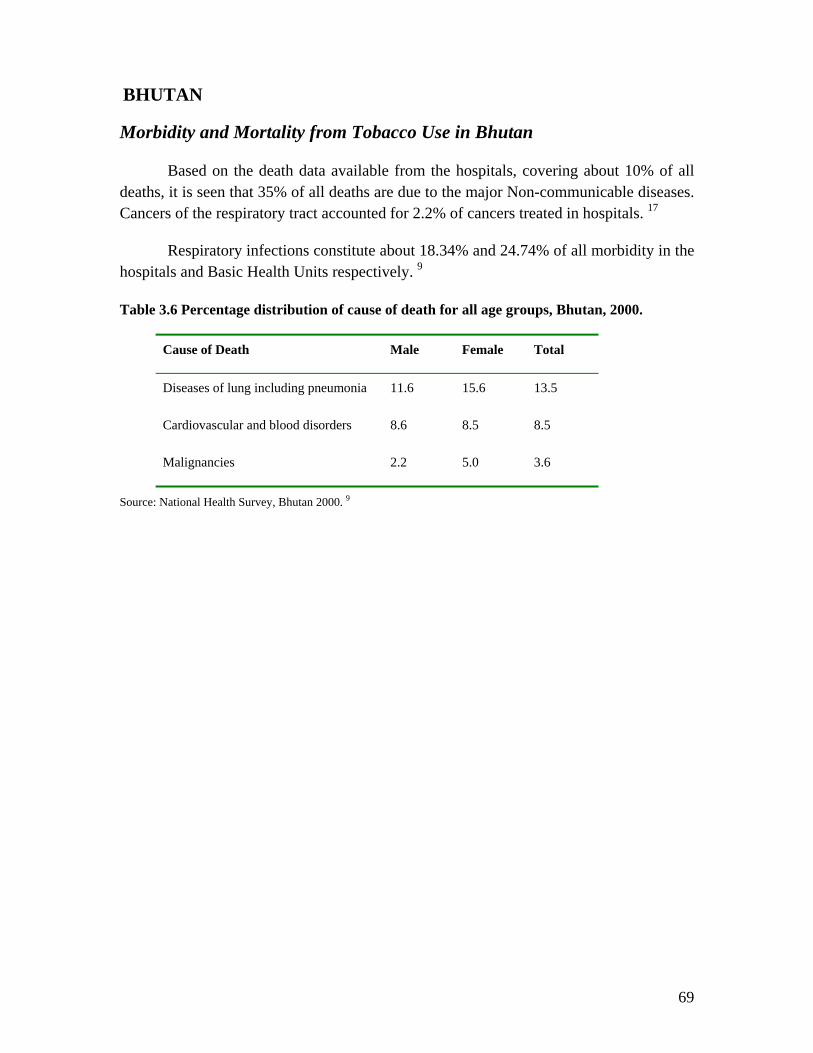
69
BHUTAN
Morbidity and Mortality from Tobacco Use in Bhutan
Based on the death data available from the hospitals, covering about 10% of all deaths, it is seen that 35% of all deaths are due to the major Non-communicable diseases. Cancers of the respiratory tract accounted for 2.2% of cancers treated in hospitals. 17
Respiratory infections constitute about 18.34% and 24.74% of all morbidity in the hospitals and Basic Health Units respectively. 9
Table 3.6 Percentage distribution of cause of death for all age groups, Bhutan, 2000.
Cause of Death Male Female Total
Diseases of lung including pneumonia 11.6 15.6 13.5
Cardiovascular and blood disorders 8.6 8.5 8.5
Malignancies 2.2 5.0 3.6
Source: National Health Survey, Bhutan 2000. 9

70
DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
Morbidity and Mortality from Tobacco Use in DPR Korea
For the year 2000, the International Agency for Research on Cancer estimated the smoking-related disease impact by estimating cancer deaths for males and females. Lung cancer death rates for both males and females are very high. Among males, it is the highest in the Region (40.17%).9
Table (3.7) Mortality from Cancer, 2000 World Age-Standardized Mortality Rate per 100,000 population for DPR Korea, all ages
Cancer Male ASR Female ASR
Oral cavity 1.36 0.33
Nasopharynx 0.23 0.06
Other pharynx 0.66 0.11
Oesophagus 7.49 0.71
Larynx 4.16 0.52
Lung 40.17 9.60
Bladder 2.65 0.51
Source: WHO SEARO; Country Profiles on Tobacco or Health , 2002

71
INDIA
Morbidity due to smokeless tobacco use in India
India has one of the highest rates of oral cancer in the world, oral cancer has been traditionally described as a major form of cancer in India and it continues to rise. Tobacco-related cancers account for about half of all cancers among men and one-fourth among women. Oral cancers account for one-third of the total cancers, with 90% of the patients being tobacco chewers. 9
In addition to mouth cancer, gutka, an industrially manufactured food item, causes another serious disease: oral sub-mucous fibrosis which has a very high potential for cancer development; the relative risk is almost 400 times that of a non-user. An increasing prevalence of oral sub-mucous fibrosis has been observed, especially in younger individuals. A comparison of the age-distribution of recently reported oral sub-mucous fibrosis cases and incident cases reported in the past clearly establishes that the disease is now occurring at much younger ages. 20
A study calculating incidence of oral sub-mucous fibrosis reported the annual incidence of oral sub-mucous fibrosis as 8.0 per 100,000 among men and 29.0 per 100,000 for women in an intervention area with a strong component of health education on tobacco and areca nut chewing. An earlier 10-year follow-up study, with no intervention component, served as control, reported the annual incidence for oral sub-mucous fibrosis as 21.3 per 100,000 for men and 45.7 for women controls. 21 A much higher incidence of oral sub-mucous fibrosis was seen among women.
Morbidity due to smoking in India
A few studies had been conducted in India regarding to health consequences of bidi and cigarette smoking. According to the cohort study of all-cause mortality among tobacco users in Mumbai, India, by Dr. PC Gupta, the relative risk was 1.39 for cigarette smokers and 1.78 for bidi smokers, with an apparent dose-response relationship for frequency of smoking. 19
At present lung cancer ranks among the top three killers in men in almost every metropolis in India. The highest incidence rate has been recorded in Bombay 14.6/ 100,000 and the lowest in Barshi 2.0/100,000. How much of these can be attributed to smoking cannot be commented on as no case-control or cohort studies have ever been undertaken in India. The situation is more alarming in other developing countries, where there is no authentic data on tobacco use or lung cancer incidences. The situation is alarming, with ever-increasing incidence among women and non-smokers exposed to smoke passive smokers. 22
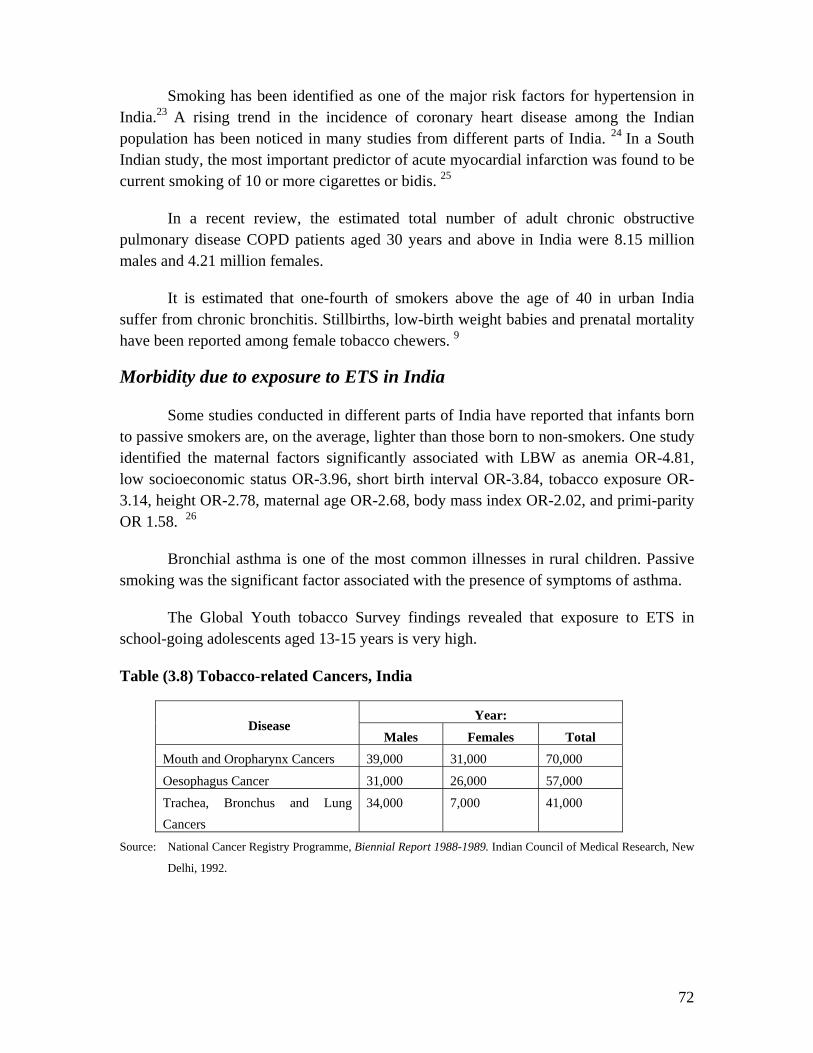
72
Smoking has been identified as one of the major risk factors for hypertension in India.23 A rising trend in the incidence of coronary heart disease among the Indian population has been noticed in many studies from different parts of India. 24 In a South Indian study, the most important predictor of acute myocardial infarction was found to be current smoking of 10 or more cigarettes or bidis. 25
In a recent review, the estimated total number of adult chronic obstructive pulmonary disease COPD patients aged 30 years and above in India were 8.15 million males and 4.21 million females.
It is estimated that one-fourth of smokers above the age of 40 in urban India suffer from chronic bronchitis. Stillbirths, low-birth weight babies and prenatal mortality have been reported among female tobacco chewers. 9
Morbidity due to exposure to ETS in India
Some studies conducted in different parts of India have reported that infants born to passive smokers are, on the average, lighter than those born to non-smokers. One study identified the maternal factors significantly associated with LBW as anemia OR-4.81, low socioeconomic status OR-3.96, short birth interval OR-3.84, tobacco exposure OR-3.14, height OR-2.78, maternal age OR-2.68, body mass index OR-2.02, and primi-parity OR 1.58. 26
Bronchial asthma is one of the most common illnesses in rural children. Passive smoking was the significant factor associated with the presence of symptoms of asthma.
The Global Youth tobacco Survey findings revealed that exposure to ETS in school-going adolescents aged 13-15 years is very high.
Table (3.8) Tobacco-related Cancers, India
Year: Disease
Males Females Total Mouth and Oropharynx Cancers 39,000 31,000 70,000
Oesophagus Cancer 31,000 26,000 57,000
Trachea, Bronchus and Lung Cancers
34,000 7,000 41,000
Source: National Cancer Registry Programme, Biennial Report 1988-1989. Indian Council of Medical Research, New
Delhi, 1992.

73
Table (3.9) Tobacco-related Diseases, 1996, India
Year: Disease
Males Females Total
Ischaemic Heart Disease 7.6 million 8.1 million 15.7 million
Chronic Obstructive Pulmonary Disease
8.9 million 5.2 million 14.0 million
Source: Department of Health, Ministry of Health and Family Welfare, Report of the Expert Committee on The
Economics of Tobacco Use . Government of India, New Delhi, February 2001.
Mortality from tobacco use in India
Estimates of tobacco-attributable mortality in India based on the results of cohort studies in rural areas of Ernakulam District, Kerala and in Srikakulam District, Andhra Pradesh, reported tobacco related mortality in the country as 630,000 deaths per year. Other studies estimate 800,000 tobacco-related deaths per annum in India. It is estimated that 40% deaths among men and 4% deaths among women are tobacco related. Cardiovascular disease, cancer and chronic obstructive pulmonary disease have been identified as the major causes of these deaths. 9
A cohort study of all cause mortality among tobacco users in Mumbai, India reported a relative risk of 1.39 for cigarette smokers and 1.78 for bidi smokers, with an apparent dose-response relationship for frequency of smoking. It reported that women were basically smokeless tobacco users, with the relative risk among such users being 1.35 and a suggestion of dose-response relationship.
The findings established bidi smoking as no less hazardous as smoking cigarettes and indicate that smokeless tobacco use may also cause higher mortality. This study also reported all-cause mortality and the relative risks for various types of tobacco use. Among women, annual mortality rate per 1,000 was reported as 7.6 among no tobacco users and 13.7 among smokeless tobacco users and 12.7 among smokers. Age adjusted relative risk for smokeless tobacco users among women was 1.35 and among female smokers was 1.28. 19

74
Table (3.10) Ten Leading Causes of Mortality for Five Years 1996 to 1997, India
Rank No Disease
1 Respiratory System
2 Circulatory System
3 Infectious and parasitic diseases
4 Conditions originating in the perinatal period
5 Venomous animal conatact
6 Inflammatory diseases of nervous system
7 Viral infections
8 Neoplasms
9 Diseases of blood and blood forming agents
10 External causes of mortality
Source: Survey of causes of death 1996*97. Registrar Central of India. In: Health Information of India 1999,
Central Bureau of Health Intelligence, Directorate General of Health Services, Ministry of Health and Family
welfare, Government of India, New Delhi.
Table (3.11) Mortality rates and age-adjusted relative risks, by type of smokeless tobacco habit, among cohort study women, Mombai
Type of tobacco product Mortality rate Age-adjusted mortality rate
Age-adjusted
relative risk
Mishri 8.6 12.3 1.24
Mishri and others 20.1 14.8 1.49
Betel quid 14.3 11.8 1.19
Other tobacco 20.9 16.0 1.62
Areca nut 15.8 12.6 1.27
No-tobacco use 7.6 9.9 1.00
Source: Prakesh C. Gupta & Hemali C. Mehta: Cohort study of all-cause mortality among tobacco users in
Mumbai, India; Bulletin of WHO, 2000,
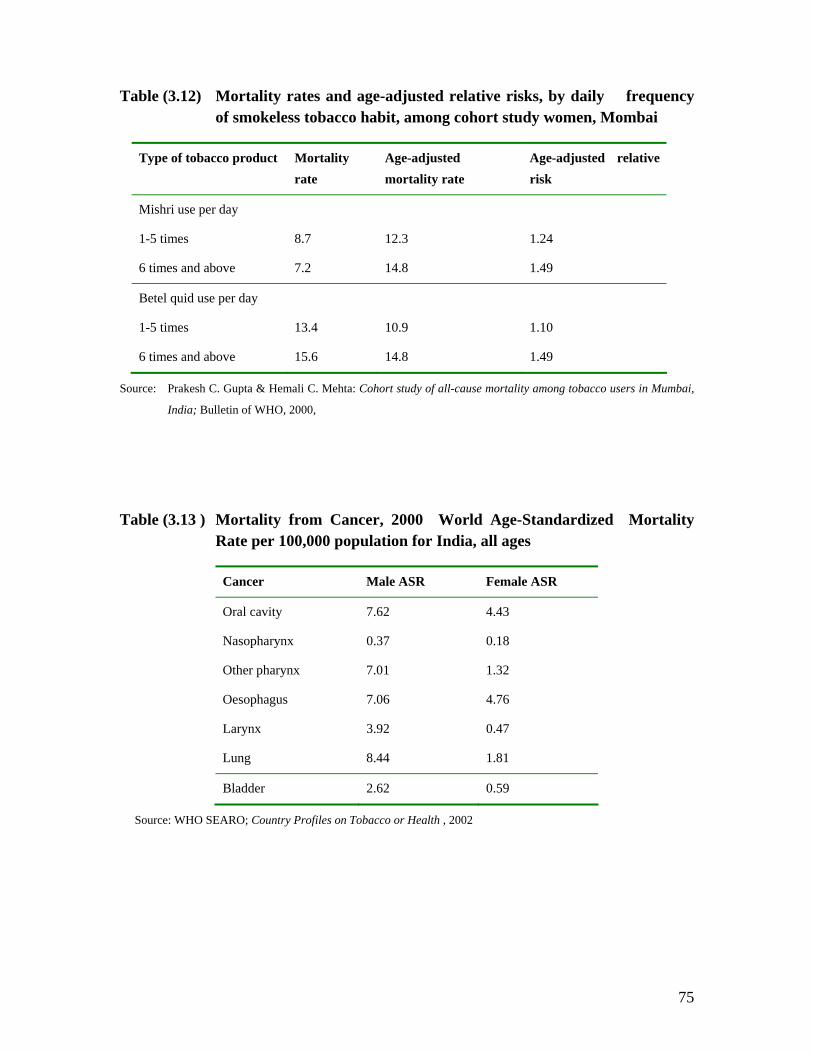
75
Table (3.12) Mortality rates and age-adjusted relative risks, by daily frequency of smokeless tobacco habit, among cohort study women, Mombai
Type of tobacco product Mortality rate
Age-adjusted mortality rate
Age-adjusted relative risk
Mishri use per day
1-5 times
6 times and above
8.7
7.2
12.3
14.8
1.24
1.49
Betel quid use per day
1-5 times
6 times and above
13.4
15.6
10.9
14.8
1.10
1.49
Source: Prakesh C. Gupta & Hemali C. Mehta: Cohort study of all-cause mortality among tobacco users in Mumbai,
India; Bulletin of WHO, 2000,
Table (3.13 ) Mortality from Cancer, 2000 World Age-Standardized Mortality Rate per 100,000 population for India, all ages
Cancer Male ASR Female ASR
Oral cavity 7.62 4.43
Nasopharynx 0.37 0.18
Other pharynx 7.01 1.32
Oesophagus 7.06 4.76
Larynx 3.92 0.47
Lung 8.44 1.81
Bladder 2.62 0.59
Source: WHO SEARO; Country Profiles on Tobacco or Health , 2002
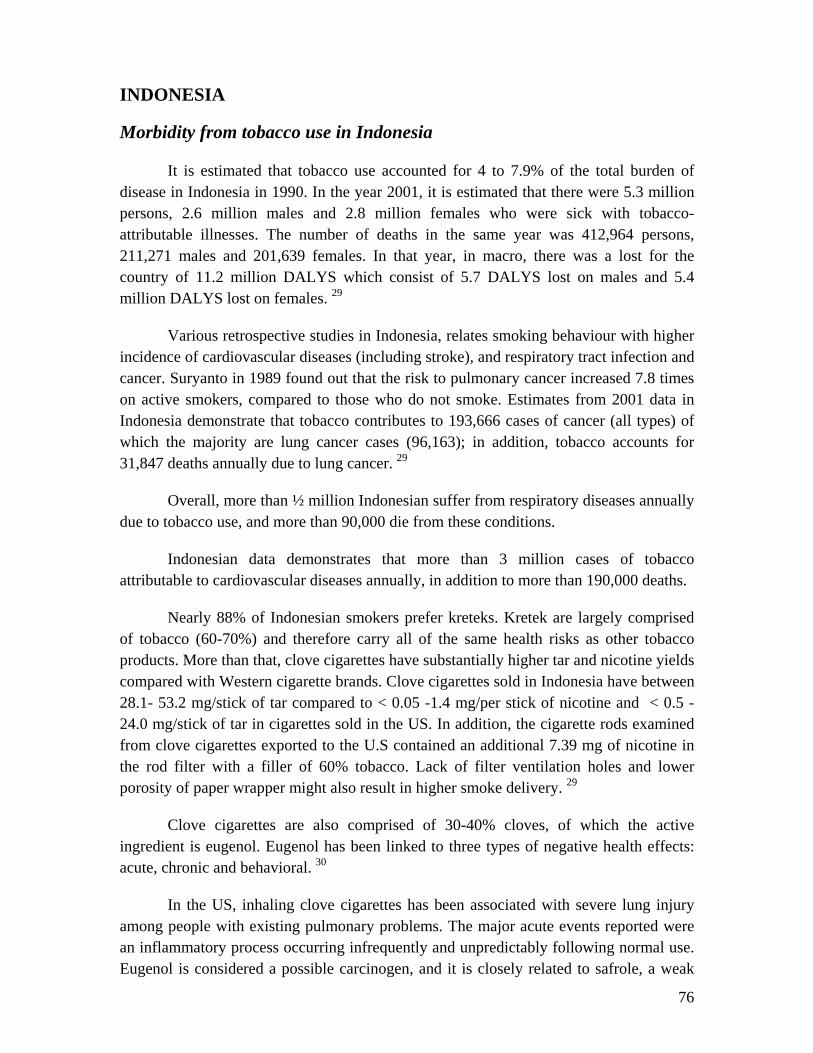
76
INDONESIA
Morbidity from tobacco use in Indonesia
It is estimated that tobacco use accounted for 4 to 7.9% of the total burden of disease in Indonesia in 1990. In the year 2001, it is estimated that there were 5.3 million persons, 2.6 million males and 2.8 million females who were sick with tobacco-attributable illnesses. The number of deaths in the same year was 412,964 persons, 211,271 males and 201,639 females. In that year, in macro, there was a lost for the country of 11.2 million DALYS which consist of 5.7 DALYS lost on males and 5.4 million DALYS lost on females. 29
Various retrospective studies in Indonesia, relates smoking behaviour with higher incidence of cardiovascular diseases (including stroke), and respiratory tract infection and cancer. Suryanto in 1989 found out that the risk to pulmonary cancer increased 7.8 times on active smokers, compared to those who do not smoke. Estimates from 2001 data in Indonesia demonstrate that tobacco contributes to 193,666 cases of cancer (all types) of which the majority are lung cancer cases (96,163); in addition, tobacco accounts for 31,847 deaths annually due to lung cancer. 29
Overall, more than ½ million Indonesian suffer from respiratory diseases annually due to tobacco use, and more than 90,000 die from these conditions.
Indonesian data demonstrates that more than 3 million cases of tobacco attributable to cardiovascular diseases annually, in addition to more than 190,000 deaths.
Nearly 88% of Indonesian smokers prefer kreteks. Kretek are largely comprised of tobacco (60-70%) and therefore carry all of the same health risks as other tobacco products. More than that, clove cigarettes have substantially higher tar and nicotine yields compared with Western cigarette brands. Clove cigarettes sold in Indonesia have between 28.1- 53.2 mg/stick of tar compared to < 0.05 -1.4 mg/per stick of nicotine and < 0.5 -24.0 mg/stick of tar in cigarettes sold in the US. In addition, the cigarette rods examined from clove cigarettes exported to the U.S contained an additional 7.39 mg of nicotine in the rod filter with a filler of 60% tobacco. Lack of filter ventilation holes and lower porosity of paper wrapper might also result in higher smoke delivery. 29
Clove cigarettes are also comprised of 30-40% cloves, of which the active ingredient is eugenol. Eugenol has been linked to three types of negative health effects: acute, chronic and behavioral. 30
In the US, inhaling clove cigarettes has been associated with severe lung injury among people with existing pulmonary problems. The major acute events reported were an inflammatory process occurring infrequently and unpredictably following normal use. Eugenol is considered a possible carcinogen, and it is closely related to safrole, a weak

77
hepatic carcinogen. Some people perceive kretek to be less harmful to health. In fact eugenol numbs the throat and allows for deeper inhalation. Deep inhalation increases exposure to carbon monoxide, which greatly increases the risk of heart attack. Behaviour associated with smoking kreteks includes slower smoking and more puffs because the rods of the clove are firmly packed. Selective additives also include ammonia which may increase nicotine absorption, flavorings to enhance taste, menthol, cocoa to dilute airways. 29,30
An investigative study of the risk factors for early deaths among patients with ischaemic stroke and intracerebral haemorrhage in Indonesia, found ex-smokers status as one of the risk factors for early death. Another study predicted that in the future cardiovascular disease would emerge as a major public health problem. 9
It is estimated that in the year 2001, there were 5.3 million persons, 2.6 million males and 2.8 million females who were sick with tobacco-attributable illnesses. The number of deaths in the same year was 412,964 persons, 211,271 males and 201,639 females. In that year, in macro, there was a lost for the country of 11.2 million DALYS which consist of 5.7 DALYS lost on males and 5.4 million DALYS lost on females. 29
Suriani’s survey 1996 on 80 tobacco farmers in Temanngung , Central Java found that the rate of Green Tobacco Sickness incidence is 63.7%.Common complaints are dizziness, headache and fatigue. 29
Table (3.14 ) List of Disease, ICD-X International Statistical Classification of Disease and Related Health Problems, Tenth Revision Code and Estimated Proportion of Disease Attributable to Tobacco Indonesia 2001.
Disease ICD-X
Code
PAR
A. Neoplasms
1. Mouth and oropharynx cancers
C 00-14 0.70
2. Oesophagus cancer C15 0.30
3. Stomach cancer C16 0.25
4. Kidney cancer C64 0.08
5. Liver cancer C22 0.10
6. Pancreas cancer C25 0.20
7. Trachea, bronchus and lung cancers
C33-34 0.90

78
8. Larynx cancer C32 0.15
9. Cervix uteri cancer C53 0.30
10. Ovary cancer C56 0.10
11. Bladder cancer C67 0.10
12. Myeloid & Monocytic Leukaemia
C92-93 0.15
B. Cardiovascular Diseases
1. Ischaemic Heart Diseases I 20-25 0.35
2. Hypertension I 10 0.20
3. Stroke I 60-69 0.40
4. Atherosclerosis I 70 0.12
5. Aortic Aneurysm I 71 0.05
6. Other arterial disease I 73-78 0.15
C. Respiratory Diseases
1. COPD J 44-47 0.70
2. Pneumonia J 12-18 0.10
3. Bronchitis, Emphysema J 40-43 0.70
D. Others
1. Burns T 20-32 0.05
2. Cataract H 25-28 0.04
3. Infertility Disorder N 97 0.08
4. Menstrual Disorder N 91-92 0.08
5. Azoospermia N 46 0.04
6. Dental caries and diseases of pulp
K 02-04 0.30
7. Periodontal disease K 05 0.15
8. Respiratory Distress Syndrome
P 22 0.10
9. Low birth weight P 07 0.30
10. Birth Asphyxia P 21 0.14
11. SIDS P 95 0.20
E. Passive Smokers
1. Lung cancer C 34 0.40
2. Ischaemic Heart Disease I 20-25 0.20
Source: Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco
Control Strategy.English Summary, December 3, 2003
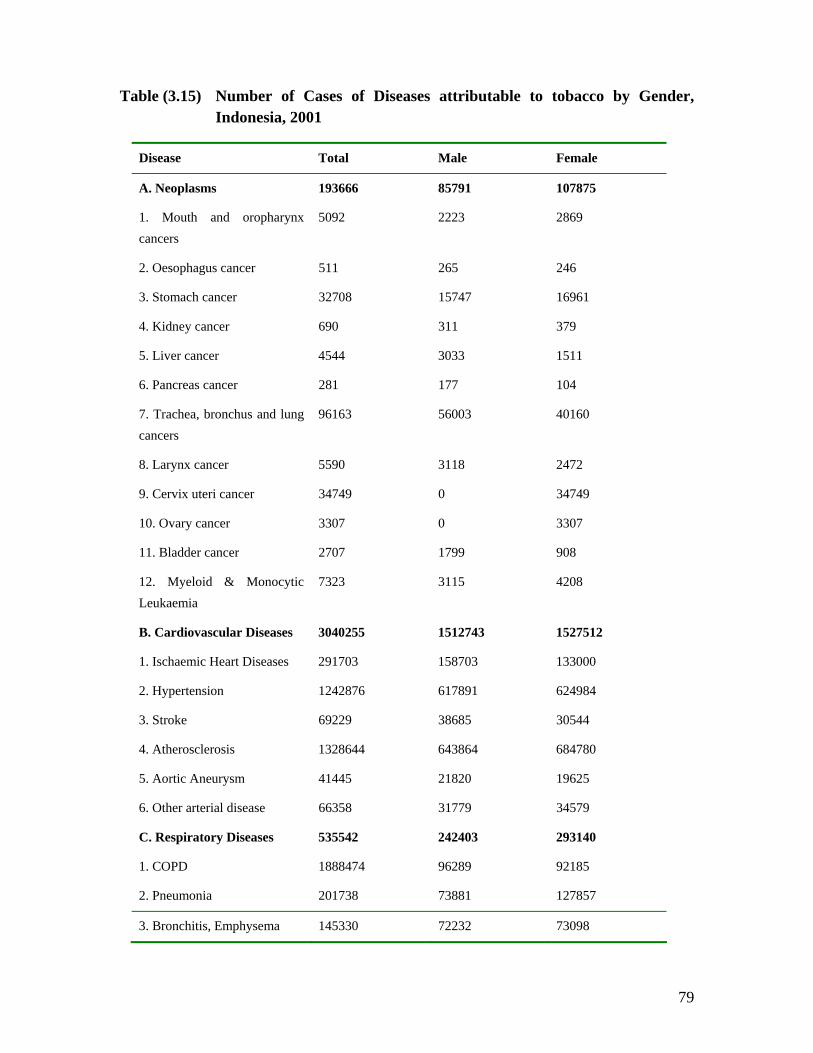
79
Table (3.15) Number of Cases of Diseases attributable to tobacco by Gender, Indonesia, 2001
Disease Total Male Female
A. Neoplasms 193666 85791 107875
1. Mouth and oropharynx cancers
5092 2223 2869
2. Oesophagus cancer 511 265 246
3. Stomach cancer 32708 15747 16961
4. Kidney cancer 690 311 379
5. Liver cancer 4544 3033 1511
6. Pancreas cancer 281 177 104
7. Trachea, bronchus and lung cancers
96163 56003 40160
8. Larynx cancer 5590 3118 2472
9. Cervix uteri cancer 34749 0 34749
10. Ovary cancer 3307 0 3307
11. Bladder cancer 2707 1799 908
12. Myeloid & Monocytic Leukaemia
7323 3115 4208
B. Cardiovascular Diseases 3040255 1512743 1527512
1. Ischaemic Heart Diseases 291703 158703 133000
2. Hypertension 1242876 617891 624984
3. Stroke 69229 38685 30544
4. Atherosclerosis 1328644 643864 684780
5. Aortic Aneurysm 41445 21820 19625
6. Other arterial disease 66358 31779 34579
C. Respiratory Diseases 535542 242403 293140
1. COPD 1888474 96289 92185
2. Pneumonia 201738 73881 127857
3. Bronchitis, Emphysema 145330 72232 73098

80
Disease Total Male Female
D. Others 1359471 633630 725841
1. Burns 47218 24490 22728
2. Cataract 264331 131654 132677
3. Infertility Disorder 10310 4990 5319
4. Menstrual Disorder 10413 0 10413
5. Azoospermia 2623 2623 0
6. Dental caries and diseases of pulp 595871 264382 331489
7. Periodontal disease 244361 112007 132354
8.Respiratory Distress Syndrome 33296 16885 16411
9. Low birth weight 133996 67952 66044
10. Birth Asphyxia 17054 8648 8406
11. SIDS 24769 12561 12208
E. Passive Smokers 268481 135952 132529
1. Lung cancer 52169 25964 26205
2. Ischaemic Heart Disease 216312 109988 106324
Total patients 539417 2610519 2786898
Source: Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco
Control Strategy.English Summary, December 3, 2003
Research studies have also established a positive relationship between habitual smoking of clove cigarettes and dental decay. The prevalence of clove dental caries was related to the years of smoking and the number of cigarettes smoked per day. 9
Morbidity from exposure to ETS in Indonesia
In Indonesia, men smoke even in the most enclosed places and even in the presence of children. The family home is a popular place for smoking by men and women. Almost all 91.8% smokers aged more than 10 years stated that they smoked at home in the presence of family members. Data from the national socioeconomics survey indicated that 92.8% of male daily smokers and 93.8% of female smokers smoked inside the home.
It is estimated that the number of people regularly exposed to environmental tobacco smoke in their homes exceeds 97 million, or 48.9% of the population. The
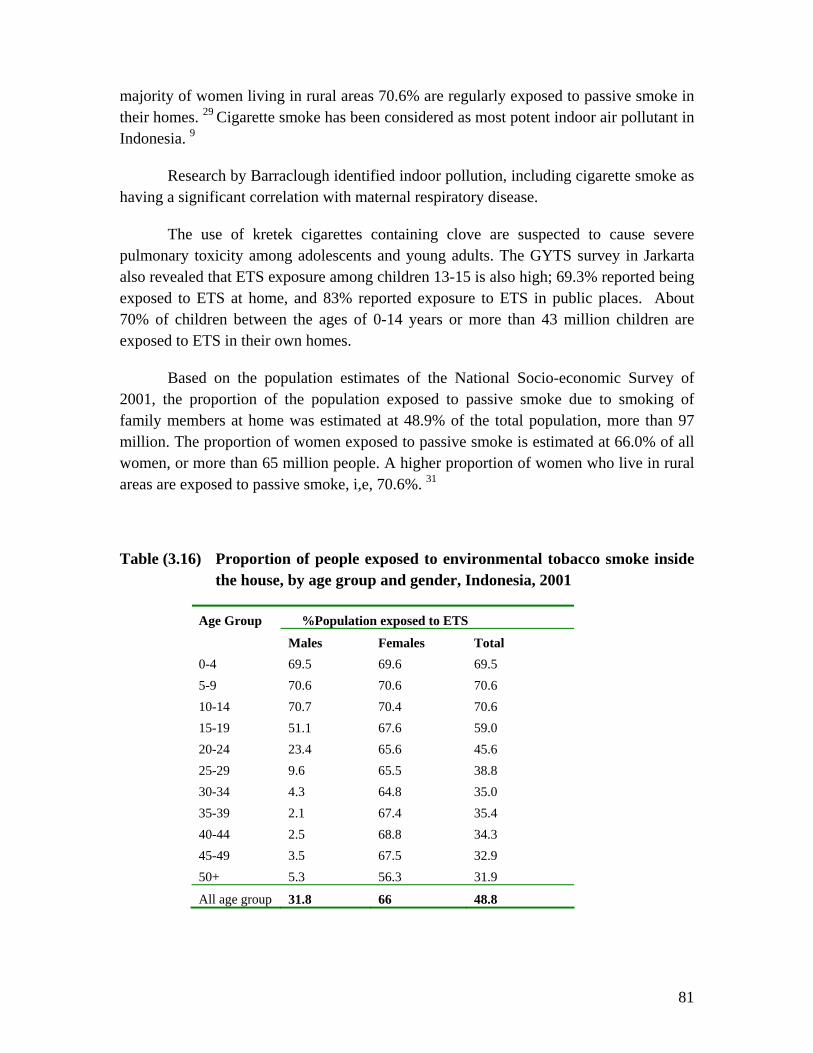
81
majority of women living in rural areas 70.6% are regularly exposed to passive smoke in their homes. 29 Cigarette smoke has been considered as most potent indoor air pollutant in Indonesia. 9
Research by Barraclough identified indoor pollution, including cigarette smoke as having a significant correlation with maternal respiratory disease.
The use of kretek cigarettes containing clove are suspected to cause severe pulmonary toxicity among adolescents and young adults. The GYTS survey in Jarkarta also revealed that ETS exposure among children 13-15 is also high; 69.3% reported being exposed to ETS at home, and 83% reported exposure to ETS in public places. About 70% of children between the ages of 0-14 years or more than 43 million children are exposed to ETS in their own homes.
Based on the population estimates of the National Socio-economic Survey of 2001, the proportion of the population exposed to passive smoke due to smoking of family members at home was estimated at 48.9% of the total population, more than 97 million. The proportion of women exposed to passive smoke is estimated at 66.0% of all women, or more than 65 million people. A higher proportion of women who live in rural areas are exposed to passive smoke, i,e, 70.6%. 31
Table (3.16) Proportion of people exposed to environmental tobacco smoke inside the house, by age group and gender, Indonesia, 2001
%Population exposed to ETS Age Group
Males Females Total 0-4 69.5 69.6 69.5 5-9 70.6 70.6 70.6 10-14 70.7 70.4 70.6 15-19 51.1 67.6 59.0 20-24 23.4 65.6 45.6 25-29 9.6 65.5 38.8 30-34 4.3 64.8 35.0 35-39 2.1 67.4 35.4 40-44 2.5 68.8 34.3 45-49 3.5 67.5 32.9 50+ 5.3 56.3 31.9
All age group 31.8 66 48.8
82
Source: Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco
Control Strategy.English Summary, December 3, 2003
Mortality from tobacco use in Indonesia
Indonesia's Health Ministry estimates that 57,000 Indonesians die of smoking-related diseases every year. Comparable data point to an increase in major chronic diseases associated with smoking. In the eighties, emphysema was high, 20 per 1,000 in men and 2 per 1,000 in women. Estimates suggest that tobacco-attributable mortality rose from 2% to 3% of all deaths in 1980 to 3% to 4% in 1986. In 2001, 21% of all deaths were attributable to tobacco, and is expected to rise dramatically within the next few decades. 9 According to Table (3.16) estimated number of mortality cases attributable to tobacco use in the year 2001 was 412,964; 211,271 males and 201,693 females. 29
Table (3.17) Number of Mortality Cases Attributable to Tobacco Use by Disease and Sex, Indonesia, 2001.
Disease Total Male Female
A. Neoplasms 61512 29326 32186
1. Mouth and oropharynx cancers 2727 1183 1544
2. Oesophagus cancer 389 201 188
3. Stomach cancer 10522 5046 5476
4. Kidney cancer 356 166 190
5. Liver cancer 3171 2033 1138
6. Pancreas cancer 258 161 97
7. Trachea, bronchus and lung cancers 31847 18368 13479
8. Larynx cancer 1651 905 746
9. Cervix uteri cancer 5880 0 5880
10. Ovary cancer 1829 0 1829
11. Bladder cancer 261 0 261
12. Myeloid & Monocytic Leukaemia 2621 1264 1357
B. Cardiovascular Diseases 190990 101406 89584
1. Ischaemic Heart Diseases 39668 24649 15019
2. Hypertension 92154 45741 46413
3. Stroke 26443 15169 11274
4. Atherosclerosis 27398 13245 14153
5. Aortic Aneurysm 1388 725 663
6. Other arterial disease 3938 1876 2062
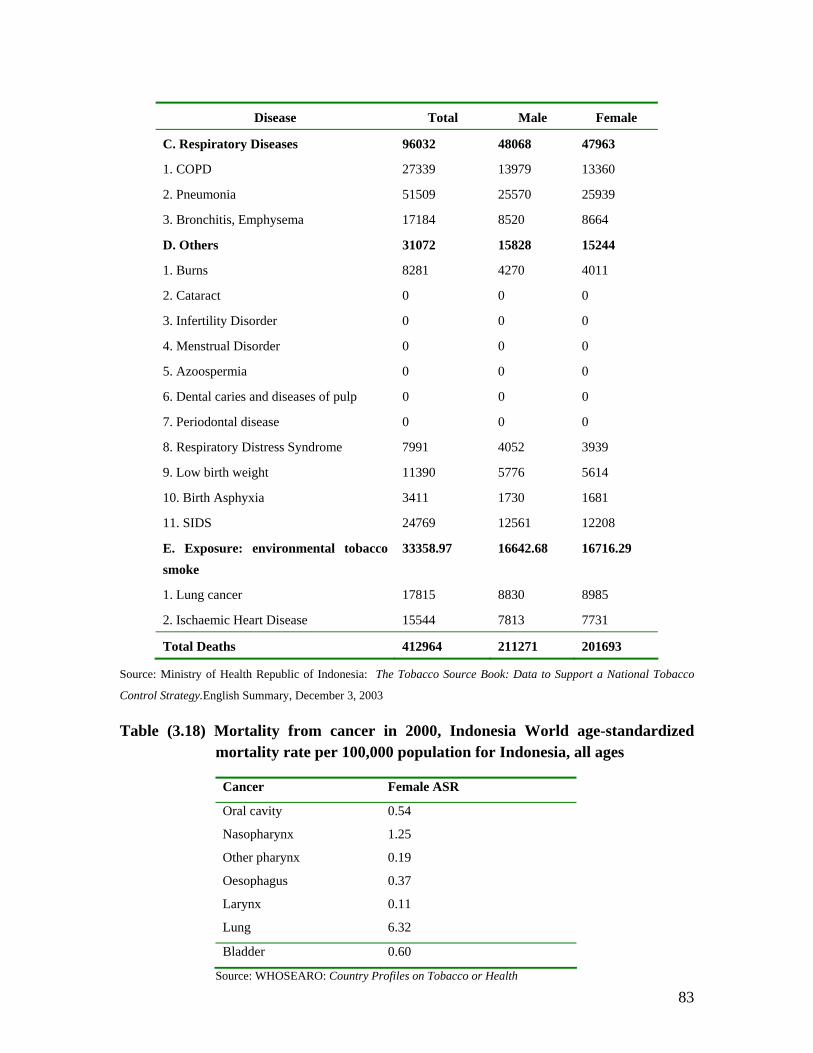
83
Disease Total Male Female
C. Respiratory Diseases 96032 48068 47963
1. COPD 27339 13979 13360
2. Pneumonia 51509 25570 25939
3. Bronchitis, Emphysema 17184 8520 8664
D. Others 31072 15828 15244
1. Burns 8281 4270 4011
2. Cataract 0 0 0
3. Infertility Disorder 0 0 0
4. Menstrual Disorder 0 0 0
5. Azoospermia 0 0 0
6. Dental caries and diseases of pulp 0 0 0
7. Periodontal disease 0 0 0
8. Respiratory Distress Syndrome 7991 4052 3939
9. Low birth weight 11390 5776 5614
10. Birth Asphyxia 3411 1730 1681
11. SIDS 24769 12561 12208
E. Exposure: environmental tobacco smoke
33358.97 16642.68 16716.29
1. Lung cancer 17815 8830 8985
2. Ischaemic Heart Disease 15544 7813 7731
Total Deaths 412964 211271 201693
Source: Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco
Control Strategy.English Summary, December 3, 2003
Table (3.18) Mortality from cancer in 2000, Indonesia World age-standardized mortality rate per 100,000 population for Indonesia, all ages
Cancer Female ASR
Oral cavity 0.54
Nasopharynx 1.25
Other pharynx 0.19
Oesophagus 0.37
Larynx 0.11
Lung 6.32
Bladder 0.60
Source: WHOSEARO: Country Profiles on Tobacco or Health
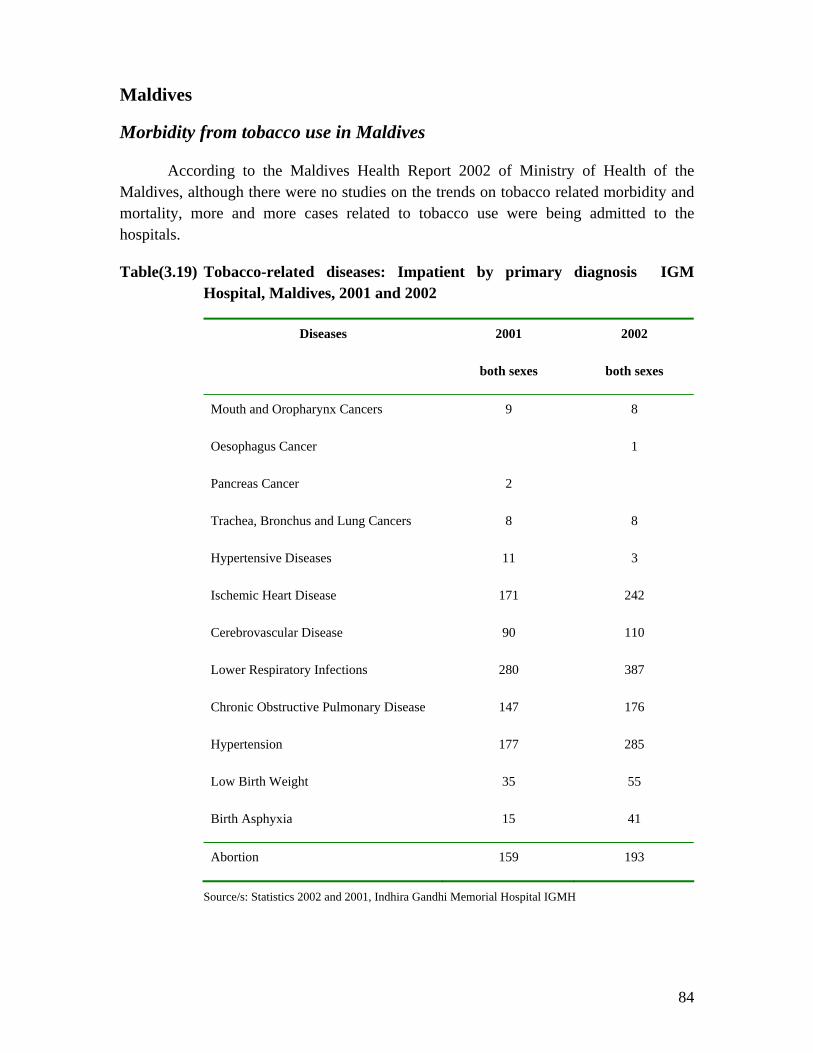
84
Maldives
Morbidity from tobacco use in Maldives
According to the Maldives Health Report 2002 of Ministry of Health of the Maldives, although there were no studies on the trends on tobacco related morbidity and mortality, more and more cases related to tobacco use were being admitted to the hospitals.
Table(3.19) Tobacco-related diseases: Impatient by primary diagnosis IGM Hospital, Maldives, 2001 and 2002
Diseases 2001
both sexes
2002
both sexes
Mouth and Oropharynx Cancers 9 8
Oesophagus Cancer 1
Pancreas Cancer 2
Trachea, Bronchus and Lung Cancers 8 8
Hypertensive Diseases 11 3
Ischemic Heart Disease 171 242
Cerebrovascular Disease 90 110
Lower Respiratory Infections 280 387
Chronic Obstructive Pulmonary Disease 147 176
Hypertension 177 285
Low Birth Weight 35 55
Birth Asphyxia 15 41
Abortion 159 193
Source/s: Statistics 2002 and 2001, Indhira Gandhi Memorial Hospital IGMH
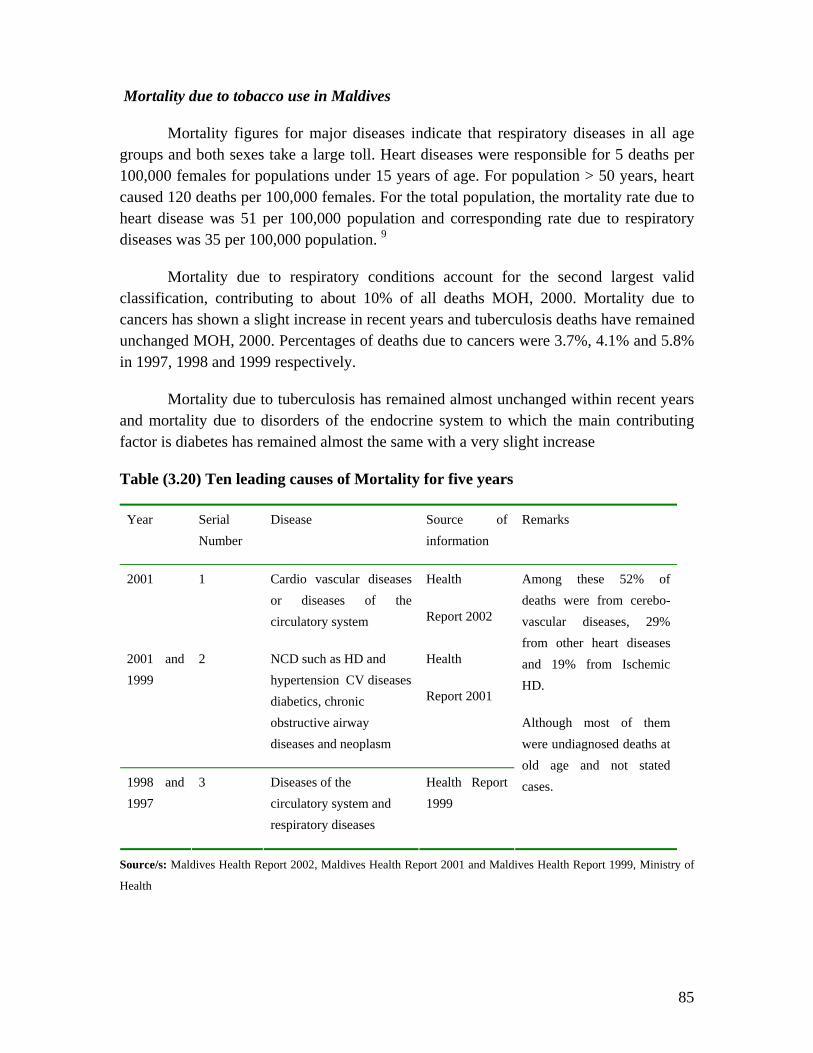
85
Mortality due to tobacco use in Maldives
Mortality figures for major diseases indicate that respiratory diseases in all age groups and both sexes take a large toll. Heart diseases were responsible for 5 deaths per 100,000 females for populations under 15 years of age. For population > 50 years, heart caused 120 deaths per 100,000 females. For the total population, the mortality rate due to heart disease was 51 per 100,000 population and corresponding rate due to respiratory diseases was 35 per 100,000 population. 9
Mortality due to respiratory conditions account for the second largest valid classification, contributing to about 10% of all deaths MOH, 2000. Mortality due to cancers has shown a slight increase in recent years and tuberculosis deaths have remained unchanged MOH, 2000. Percentages of deaths due to cancers were 3.7%, 4.1% and 5.8% in 1997, 1998 and 1999 respectively.
Mortality due to tuberculosis has remained almost unchanged within recent years and mortality due to disorders of the endocrine system to which the main contributing factor is diabetes has remained almost the same with a very slight increase
Table (3.20) Ten leading causes of Mortality for five years
Year Serial Number
Disease Source of information
Remarks
2001 1 Cardio vascular diseases or diseases of the circulatory system
Health
Report 2002
2001 and 1999
2 NCD such as HD and hypertension CV diseases diabetics, chronic obstructive airway diseases and neoplasm
Health
Report 2001
1998 and 1997
3 Diseases of the circulatory system and respiratory diseases
Health Report 1999
Among these 52% of deaths were from cerebo-vascular diseases, 29% from other heart diseases and 19% from Ischemic HD.
Although most of them were undiagnosed deaths at old age and not stated cases.
Source/s: Maldives Health Report 2002, Maldives Health Report 2001 and Maldives Health Report 1999, Ministry of
Health

86
MYANMAR
Morbidity due to tobacco use in Myanmar
In Myanmar there is an increasing trend of non-communicable diseases over the years. Table 3.21 shows the number of admissions to government hospitals, of selected tobacco-related diseases: cancer of the lips, tongue, oesophagus, stomach, liver, larynx, lungs, cervix and bladder; tuberculosis of the respiratory system; chronic bronchitis; emphysema; chronic obstructive airway disease; hypertension; ischaemic heart disease; and stroke. There has been an increase in admissions of cancers of the oesophagus, stomach, lungs and larynx and also an increase in admissions due to tuberculosis of the respiratory system and stroke.
Several studies being carried out have revealed that there is also an increase in oral cancer cases among patients with history of smoking and chewing habits. A study on some 6000 rural people aged 15 and above examined the prevalence of oral precancerous lesions and its link with smoking and chewing. The study showed the prevalence of preleukoplakia as 0.3%, leukoplakia as 1.7%, lichen planus as 0.4%, luekokeratosis nicotina palate as 2.3%, erythoplakia as 0.1%, sub-mucous fibrosis as 0.1%, and cancer as 0.03%. A positive correlation was found between smoking habits and lesions. 9 The results of a cross-sectional survey conducted in three urban townships of Yangon City and one rural township of Hmawbi, showed that the risk of obesity and smoking in the occurrence of cardiovascular CVD was high in both urban and rural communities. Smoking was found as a major risk factor for CHD and Hypertension.
Table(3.21) Government Hospital admissions due to tobacco related diseases 1995-1999
Tobacco- related disease 1995 1996 1997 1998 1999
Lip cancer 0 13 0 0 13
Tongue cancer 81 53 77 110 116
Oesophageal cancer 297 318 386 425 528
Stomach cancer 987 995 1210 1084 1158
Liver cancer 757 663 669 535 553
Larynx cancer 406 889 232 343 257

87
Lung cancer 743 902 1 004 1 797 1 544
Cervical cancer 960 1 154 1 390 1 921 2 084
Bladder cancer 108 80 129 96 180
Respiratory tuberculosis 18 47
7 16 544 17 207 19 001 23 135
Chronic bronchitis 879 517 502 508 656
Emphysema 54 93 51 82 142
COAD 635 650 656 1 098 965
Hypertension 7 813 5 678 6 847 7 738 7 025
Ischaemic heart disease 1 978 2 043 2 613 3 114 2 265
Stroke 3 717 3 648 3 822 4 253 4 156
Total admissions 803 5
05 888 965 842 234 884 902 869 153
Source: Ministry of Health, Department of Health, Health Management Information System. In Nyo Nyo Kyaing , A study on Tobacco Economics in Myanmar. HNP Discussion Paper series. Economics of Tobacco Control Paper. TFI WHO. October 2003. Table 3.22 shows data on outpatients for respiratory tuberculosis, chronic bronchitis and hypertension from 1996 to 1999. There is an increase in number of cases of respiratory tuberculosis over the years, and the number of chronic bronchitis cases was highest in 1999. Table (3.22) Outpatients due to tobacco related diseases 1996-1999
Tobacco-related disease 1996 1997 1998 1999
Respiratory tuberculosis 31 460 29 847 32 267 34 687
Chronic bronchitis 6 453 5 647 4 840 7 260
Hypertension 43 560 46 787 47 593 41 947
Total outpatients 2 190 100 2 173 160 2 025 540 1 929 547
Source: Ministry of Health, Department of Health, Health Management Information System. In Nyo Nyo Kyaing , A study on
Tobacco Economics in Myanmar. HNP Discussion Paper series. Economics of Tobacco Control Paper. TFI WHO.
October 2003.
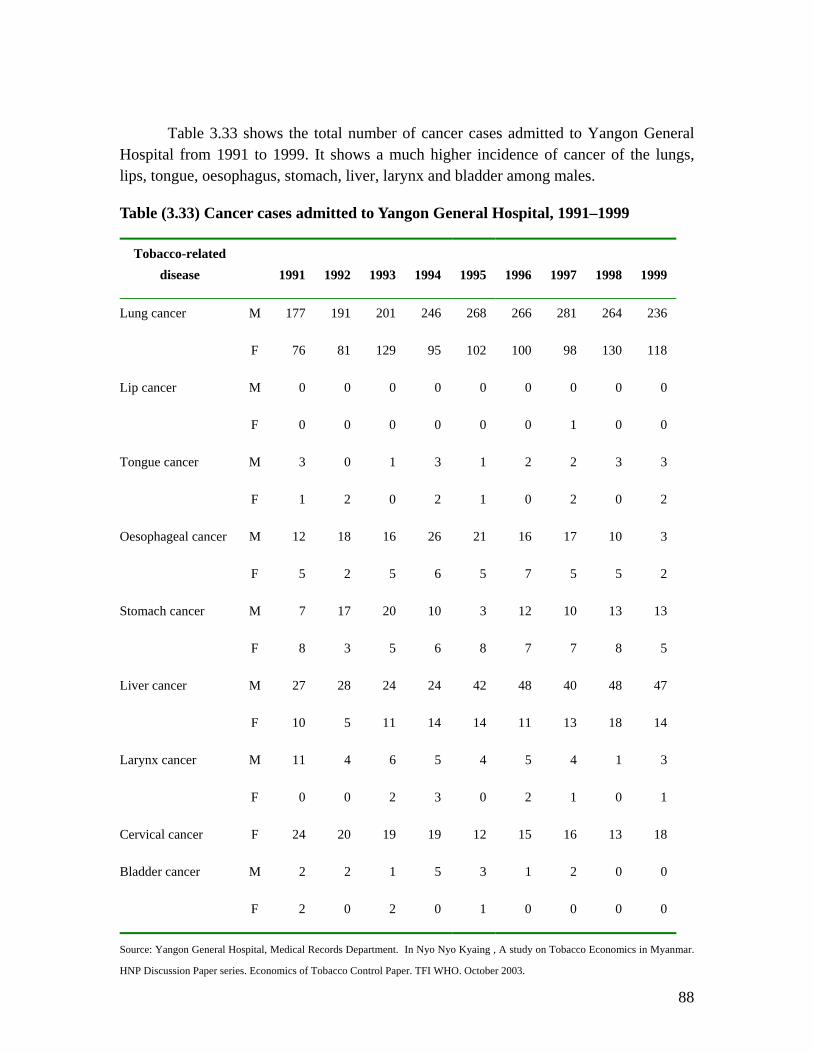
88
Table 3.33 shows the total number of cancer cases admitted to Yangon General Hospital from 1991 to 1999. It shows a much higher incidence of cancer of the lungs, lips, tongue, oesophagus, stomach, liver, larynx and bladder among males.
Table (3.33) Cancer cases admitted to Yangon General Hospital, 1991–1999
Tobacco-related disease 1991 1992 1993 1994 1995 1996 1997 1998 1999
Lung cancer M 177 191 201 246 268 266 281 264 236
F 76 81 129 95 102 100 98 130 118
Lip cancer M 0 0 0 0 0 0 0 0 0
F 0 0 0 0 0 0 1 0 0
Tongue cancer M 3 0 1 3 1 2 2 3 3
F 1 2 0 2 1 0 2 0 2
Oesophageal cancer M 12 18 16 26 21 16 17 10 3
F 5 2 5 6 5 7 5 5 2
Stomach cancer M 7 17 20 10 3 12 10 13 13
F 8 3 5 6 8 7 7 8 5
Liver cancer M 27 28 24 24 42 48 40 48 47
F 10 5 11 14 14 11 13 18 14
Larynx cancer M 11 4 6 5 4 5 4 1 3
F 0 0 2 3 0 2 1 0 1
Cervical cancer F 24 20 19 19 12 15 16 13 18
Bladder cancer M 2 2 1 5 3 1 2 0 0
F 2 0 2 0 1 0 0 0 0
Source: Yangon General Hospital, Medical Records Department. In Nyo Nyo Kyaing , A study on Tobacco Economics in Myanmar.
HNP Discussion Paper series. Economics of Tobacco Control Paper. TFI WHO. October 2003.
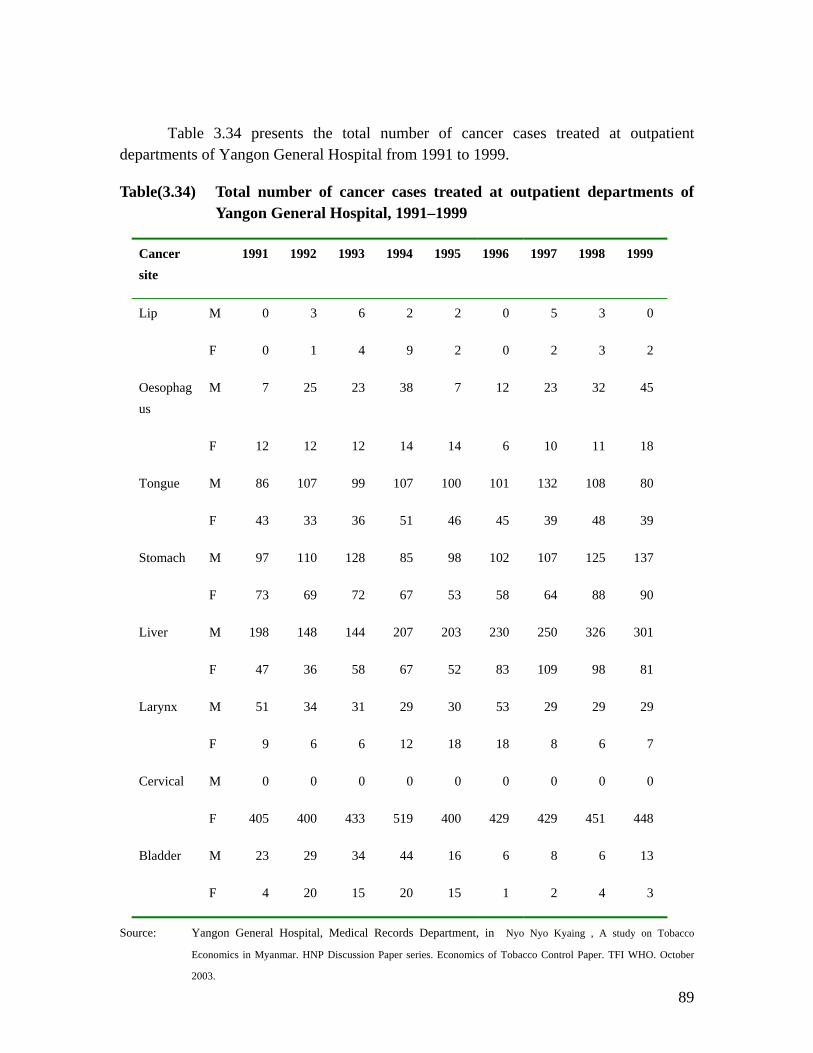
89
Table 3.34 presents the total number of cancer cases treated at outpatient departments of Yangon General Hospital from 1991 to 1999.
Table(3.34) Total number of cancer cases treated at outpatient departments of Yangon General Hospital, 1991–1999
Cancer site
1991 1992 1993 1994 1995 1996 1997 1998 1999
Lip M 0 3 6 2 2 0 5 3 0
F 0 1 4 9 2 0 2 3 2
Oesophagus
M 7 25 23 38 7 12 23 32 45
F 12 12 12 14 14 6 10 11 18
Tongue M 86 107 99 107 100 101 132 108 80
F 43 33 36 51 46 45 39 48 39
Stomach M 97 110 128 85 98 102 107 125 137
F 73 69 72 67 53 58 64 88 90
Liver M 198 148 144 207 203 230 250 326 301
F 47 36 58 67 52 83 109 98 81
Larynx M 51 34 31 29 30 53 29 29 29
F 9 6 6 12 18 18 8 6 7
Cervical M 0 0 0 0 0 0 0 0 0
F 405 400 433 519 400 429 429 451 448
Bladder M 23 29 34 44 16 6 8 6 13
F 4 20 15 20 15 1 2 4 3
Source: Yangon General Hospital, Medical Records Department, in Nyo Nyo Kyaing , A study on Tobacco
Economics in Myanmar. HNP Discussion Paper series. Economics of Tobacco Control Paper. TFI WHO. October
2003.
90
Studies on health consequences of tobacco in Myanmar.
In 1988 the respiratory effects of occupational exposure to tobacco dust was carried out on 476 workers from Cigarette Factory No: 1, Yangon . High prevalence of cough, tightness of chest and breathlessness in females and chronic phlegm in males were found. Chronic respiratory effects of occupational exposure to tobacco dust was observed in females. 34
In 1989, a retrospective analysis of clinical profiles and risk factors of 70 patients, with acute myocardial infarction admitted into the Yangon General hospital and New Yangon General Hospital during the year 1988 were made. Subgroup analysis revealed that 43 patients were smokers, 26 smoked cheroot, 6 cigarettes and only 1 smoke cigar. 35
In 1990, a retrospective analysis of clinical profiles of 360 patients with acute myocardial infarction admitted into the Yangon General Hospital and New General Hospital from January 1987 to October 1990 were made. Subgroup analysis showed that 26 patients were under the age of 45 and among these patients the majority 77% smoked. Among the smokers 65% smoked cheroots , 20% cigarettes, 10% cigar and the rest pipe. 36
In 1987, the survey of chronic respiratory disease in urban and rural communities was conducted. Out of 8476 persons interviewed 34.05% appeared to be smokers and the proportion of male to female smoking was 2:1. The lowest income groups, farmers and the least educated groups smoked the most. Higher incidence of chronic respiratory disease was found among the smokers in all categories.39
In 1990, a preliminary study on effect of cheroot smoking on ventilatory functions was conducted with the aim of determining whether cheroot smoking has similar effect. A study of ventilatory functions was carried out on 36 Myanmar male pure cheroot smokers and the results compared with those found in 39 Myanmar male nonsmokers. Significant trend towards decrease in FVC1 and FEV1, values according to increasing smoking indices were found among the cheroot smokers. 38
In 1990, the effect of cigarette smoking on nasal mucociliary activity was conducted. Nasal mucociliary transport rates of healthy twenty male non smokers and twenty cigarette smokers were measured using Saccharin Crystal Technique by Proctor1973. Significant decrease in nasal mucociliary transport rates was observed in cigarette smokers. 39

91
In the year 1996, a study of the effects of tobacco smoking on lipid profile of apparently healthy Myanmar adults was conducted. The nicotine content of imported cigarette (Lucky Strike) and locally manufactured cheroot ( Joe Thein) were determined by using High Performance Liquid Chromatography HPLC. The results showed that although net tobacco weight per cheroot was significantly greater than cigarette, the mean nicotine content per cigarette was significantly greater than that of cheroot. Significant rise of serum FFA in acute state of smoking was seen in both cheroot smoking and cigarette smoking. 40
In 1997, a study of lung functions in cigarette smokers and cheroot smokers was conducted in 75 apparently healthy men, consisting of 30 nonsmokers, 25 cigarette smokers and 20 cheroot smokers, 22 to 68 years old. It is concluded that both cigarette smoking and cheroot smoking are associated with a decrease in pulmonary functions. Effect of cheroot smoking is more marked than that of cigarette smoking. 41
National health Plan data reveals the prevalence rates for hypertension as 42/1000 population for urban, 57/1000 population for rural; prevalence rate for Ischaemic Heart Disease as 13/1000 population for urban and 8/1000 population for rural. Recent surveys conducted by the Department of Medical Research revealed a prevalence rate of hypertension ranging from 20% to 25% of the population. Evaluation of risk factors among patients presenting with acute myocardial infarction yielded smoking (67%), hypertension (41%), hypercholesterolaemia (30%) and diabetes mellitus (23%).
Morbidity due to ETS in Myanmar
A study by MC Gready et al shows that babies born to cheroot smoking mothers weighed 1159 gram less than babies of non-smoking mothers. The same study revealed that carbon monoxide in inhaled cheroot smoke was six times greater than that produced from UK cigarettes. Smoking in pregnancy results in reduced intervillous placental blood flow a nicotine effect and increased concentration of carbon monoxide, in blood reducing the amount of oxygen available to the foetus. 9
As most adult smokers smoked at home and in public places, the Myanmar GYTS 2001 revealed that nearly 4 in ten never smokers and more than 6 in ten current smokers were exposed to smoke from others in their home in the past 7 days; more then 4 in ten never smokers and more than 7 in ten current smokers were exposed to smoke from others.41
Mortality due to tobacco use in Myanmar
Table (3.35) shows age-standardized mortality rates for males and females in Myanmar from major tobacco-related cancers. Cancer mortality in Myanmar is

92
apparently affecting not only males, as in all SEA countries, but also females. This is explained by female mortality rates that are higher than in most other countries of the Region.
Oral cavity, oesophagus and lung cancers are the major killers among both males and females in Myanmar. 9
Table (3.35) Mortality from cancer in 2000, Myanmar World age-standardized mortality rate per 100,000 population, all ages
Cancer Female ASR
Oral cavity 2.05
Nasopharynx 1.34
Other pharynx 1.37
Oesophagus 5.53
Larynx 1.41
Lung 11.76
Bladder 0.75
Source: WHOSEARO: Country Profiles on Tobacco or Health

93
NEPAL
Morbidity due to tobacco use in Nepal
A study by Pandey et al (1988) showed high prevalence of chronic bronchitis; 33.9% among men and 28.3% among women and chronic obstructive lung disease. Prevalence of tobacco use combined with the use of unventilated indoor fires for cooking and heating caused high rates of lung diseases in Nepal. A report in 1998 mentioned that there were 60,000 cancer patients admitted to six hospitals in Nepal in 1997 (Kathmandu Post, January 29, 1998). It is reported that the “consumption of cigarettes and tobacco coupled with the ever growing environmental pollution has its share in the alarming growth of cancer cases”. Another most recent study reports Gutkha chewing becoming increasingly popular in the Tarai of Nepal. ( Kathmandu Post, February 13, 2001). 42
Morbidity due to Exposure to Environmental Tobacco Smoke in Nepal
The infants of mothers who smoke during pregnancy have lower average birth weight than infants born to non-smoking women. The survey of 1997 shows that proportionately more smoking mothers gave birth to small (20.6%) and very small (3.3%) infants compared to non-smoking mothers (15.2% and 2.2% respectively). Studies show high risk of stillbirth neonatal death and sudden infant death syndrome greater among the offspring of women who smoke. Study shows proportionately more smoking mothers experiencing stillbirth and birth of dead infants (2.7%) than their non-smoking counterparts (2.1%) similarly fewer smoking mothers (95.4%) had their infants surviving well than the mothers who did not smoke during pregnancy (96.2%). (Source: The Department of Health Services. Katmandu, Nepal)
Mortality due to tobacco use in Nepal
Smoking related annual deaths are estimated at nearly 14,000 for the population aged over 35. On the basis of per capita spending on health estimated by the World Bank, and considering the population at relative risk of smoking, the health costs attributable to smoking were estimated at Rs 3.1 billion in 2000. Death and morbidity due to smoking-related causes for the under 35 population would make the health costs even higher. 9

94
Table (3.36) Ten leading causes of Mortality related to tobacco for five years, Nepal
Serial Number
Disease
1 Lung Cancer
2 Cancer of the mouth, oesophagus, larynx and pharynx
3 Ischaemic heart disease
4 Cerebrovascular disease
5 Chronic Obstructive Pulmonary Diseases COPD
6 Digestive tract cancers
7 Hypertension
8 Low birth weight
Source/s National Anti-Tobacco IEC strategy for Nepal 2004-2008
Table (3.37) Causes of death in Nepal
Cause of death Male % Female % Total %
Group 1
Infectious, maternal, perinatal and nutritional problems
pneumonia, bacterial diseases, intestinal infections, bronchitis, asthma, abortion complications, tuberculosis, etc.
48.1 51.3 49.7
Group 2
Non-communicable and congenital problems
digestive disorders, cardiovascular diseases, diseases of the nervous system, etc.
44.0 40.2 42.1
Group 3
Injuries and accidents 6.8 7.0 6.9
Unclassified 1.0 1.5 1.0
Total % 100.0 100.0 100.0
Total number 120 539 125 839 246 432
Source: World Bank, June 2000

95
Table(2.38) Mortality from cancer in 2000 World age-standardized mortality rate per 100,000 population for Nepal, all ages
Cancer Female ASR
Oral cavity 5.03
Nasopharynx 0.24
Other pharynx 1.45
Oesophagus 5.75
Larynx 0.64
Lung 2.15
Bladder 0.75
Source: WHOSEARO: Country Profiles on Tobacco or Health , New Delhi, 2002

96
SRI LANKA
Morbidity due to tobacco use in Sri-Lanka
In Sri Lanka, figures for 1985-1986 showed that about 10% of all cancers in the total population were related to tobacco use. The incidence of cancer in women that could be related to tobacco use increased from 1 per 100,000 population in 1985 to 1.57 per 100,000 in 1990. 18
Heart disease ranks as the number one cause of mortality in Sri Lanka, with tobacco contributing significantly. Stroke mortality and prevalence of hypertension have increased rapidly. In rural populations, the prevalence is two to three times lower than in urban subjects. Hypertension and stroke occur at a relatively younger age in Sri Lanka. Smoking has been proved to be one of the risk factors for hypertension in most countries of Asia.
Oral cancer is the most common form of cancer in the country, with over 90% attributable to prolonged tobacco chewing and smoking. In 1985, it was estimated that 43.1% of all cancers were tobacco related. The cancer Control Programme estimated that around 60% of cancers among males were attributable to tobacco. Oral cancer accounted for 22% of all cancers, both in males and females. 9
Morbidity due to exposure to ETS in Sri-Lanka
The GYTS 1999 revealed a high exposure to ETS. About 55.8% live in homes where at least one member of the family smokes.
A case-control study, carried out among a group of children in Sri Lanka admitted with symptoms of asthma, and age-matched controls, revealed the passive smoking was a risk factor for asthma. 9
Mortality due to tobacco use
Heart disease ranks as the number one cause of mortality in Sri-Lanka with tobacco contributing significantly.
Age-standardized mortality rate for Oral cavity cancer is the highest among males in Sri Lanka compared to all other countries. The oral cavity cancer mortality rate among females is the second highest (7.05) in Sri-Lanka with women in Bangladesh having the highest oral cavity cancer (9.78) rate in the Region. 9
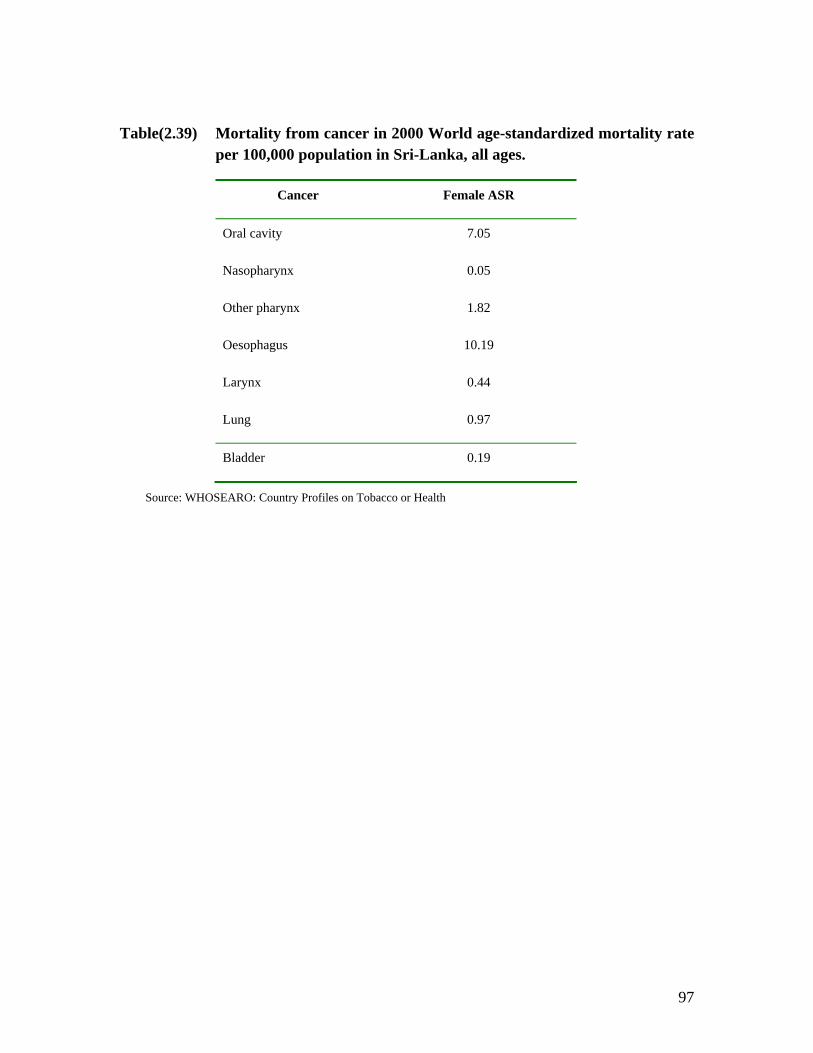
97
Table(2.39) Mortality from cancer in 2000 World age-standardized mortality rate per 100,000 population in Sri-Lanka, all ages.
Cancer Female ASR
Oral cavity 7.05
Nasopharynx 0.05
Other pharynx 1.82
Oesophagus 10.19
Larynx 0.44
Lung 0.97
Bladder 0.19
Source: WHOSEARO: Country Profiles on Tobacco or Health

98
Thailand
Mortality from tobacco use in Thailand
Many studies carried out in Thailand pointed to a relationship between cigarette smoking and disease. Theera 1994 based on the statistics of lung cancer patients who received treatments between 1967 and 1993, concluded that there was a significant relationship between smoking and lung cancer. Around 78% of his lung cancer patients were smokers, most of them heavy smokers. The results of studies conducted by Sirikunya et.al. 2000 point to similar conditions. Cigarette smoking is also highly related to laryngeal cancer. Around 85% of laryngeal cancer patients were smokers. Table 3.22 provides numbers of deaths and death rates for some of the main smoking –related diseases in Thailand , from 1996 to 2000. 31
Lung cancer is the leading malignancy among men and a common malignancy among women in Thailand. Popularly used Thai cigarettes contain high levels of tar and tobacco-specific N-nitrosamines TSNA carcinogens. Carbon monoxide CO levels in the smoke of popular Thai cigars KHIO and cigars from Myanmar sold in Thailand are high.9
The incidence of lung cancer among Northern Thai women is one of the highest in Asia and among the highest in the world, with an annual age-adjusted incidence rate of 37.4 per 100,000. The incidence rate differs significantly among geographical districts. A comparative study of women living in the Sarapee area showed the highest crude incidence rate 40.9% while the Chom Tong area in Chiang Mai Province, showed on of the lowest rate 8.5%. This difference was detected despite the geographical and cultural closeness of the two areas. Lung cancer was more prevalent among those with a history of both benign respiratory diseases and tobacco smoking. The results suggested that tobacco Khio smoking, along with fungi infestation, might explain the high incidence of female lung cancer in Northern Thailand. 32
Mitacl et al have indicated that cancers of the lung and of the upper aero-digestive tract have increased in the last decade. They also noted an increase in primary cancer of the liver, especially of cholangiocarcinoma, in the north-eastern provinces of Thailand. The analytical data were in line with the rate of lung cancer in Thailand. It suggested that volatile and tobacco-specific nitrosamines are associated with increased risk of primary liver cancer among those Thais who smoke cigarettes and also carry liver fluke infestation.
One study suggested that smoking and the use of charcoal stoves increased indoor particulate matter levels. Another study found that there was a significant association between the low birth weight of infants and maternal smoking habit RR+ 2.9, p>0.05 and father’s smoking habit RR+1.5, p>0.05. 9

99
Table(3.40) Number of Deaths and Deaths Rates per 100,000 Population, by Smoking-Related Diseases in Thailand (1996-2000)
1996 1997 1998 1999 2000 Disease
Number Rate Number Rate Number Rate Number Rate Number Rate
1. Malignant neoplasm of trachea,
bronchus and lung 2913 4.9 2,936 4.9 3,500 5.7 4,220 6.9 5,486 8.9
2. Malignant neoplasm of lip, oral cavity
and pharynx 651 1.1 404 0.7 574 0.9 675 1.1 762 1.2
3. Malignant neoplasm of cervix uteri 380 0.6 318 0.5 408 0.7 672 1.1 871 1.4
4. Malignant neoplasm of stomach 388 0.6 245 0.4 365 0.6 458 0.7 648 1
5. Malignant neoplasm of bladder 105 0.2 74 0.1 84 0.1 146 0.2 202 0.3
6. Malignant neoplasm of larynx 98 0.2 62 0.1 59 0.1 125 0.2 171 0.3
7. Malignant neoplasm of pancreas 148 0.2 89 0.1 202 0.3 523 0.8 479 0.8
8. Other heart diseases 42,962 71.9 40,556 67.1 36,355 59.4 25,695 41.7 13,406 21.7
9. Cerebrovascular disease 6,297 10.5 5,962 9.9 4,283 7 6,631 10.8 8,260 13.4
10. Hypertensive disease 3,053 5.1 2,054 3.4 2,029 3.3 2,987 4.9 3,403 5.5
11. Acute rheumatic fever and chronic
rheumatic heart disease 554 0.9 561 0.9 267 0.4 165 0.3 51 0.1
12. Ischaemic heart diseases 2,784 4.7 1,870 3.1 2,199 3.6 4,849 7.9 6,251 10.1
13. Pneumonia 6,859 11.5 5,532 9.1 5,522 9 8,645 14 8,334 13.5
14.Respiratory tuberculosis 3,445 5.8 2,443 4 3,150 5.2 4,701 7.6 5,941 9.6
Source: Health Statistic Department, Ministry of Public Health, year 2000 31

100
Table(3.41) Mortality from cancer in 2000, World age-standardized mortality rate per 100,000 population for Thailand, all ages
Cancer Female ASR
Oral cavity 2.40
Nasopharynx 0.81
Other pharynx 0.45
Oesophagus 1.14
Larynx 0.26
Lung 10.02
Bladder 0.72
Source: WHOSEARO: Country Profiles on Tobacco or Health, New Delhi, 2002
101
References
1. Women and Smoking : A Report of the Surgeon General-2001. CDC; Women and Smoking Fact Sheet
2. Virginia L. Ernester. Impact of Tobacco Use on Women’s Health. In WHO: Women and the Tobacco Epidemic, Challenges for the 21st Century. WHO in collaboration with the Institute for Tobacco Control, Johns Hopkins School of Public Health . Canada, 2001.
3. World Health Organization. World Health Report 2002. Geneva, 2002.
4. World Health Organization, Regional Office for South-East Asia Region Health Situation in the South-East Asia Region, 1998-2000. New Delhi, 2002.
5. Mira B. Aghi. Women, Children and Tobacco. Paper presented at the WHO International Conference on Global Tobacco Control Law, New Delhi, India, January 2000.
6. Jonathan M. Samet and Gonhuan Yang. Passive Smoking, Women and Children. In WHO: Women and the Tobacco Epidemic, Challenges for the 21st Century.WHO in collaboration with the Institute for Tobacco Control, Johns Hopkins School of Public Health . Canada, 2001.
7. Shoba John and Shailesh Vaite. Tobacco and Poverty: Observations from India and Bangladesh. PATH Canada. October, 2002.
8. Efforymson D. and Saifuddin A. Hungry for Tobacco: An analysis of the economic impact of tobacco on the poor in Bangladesh. PATH Canada. July 2000.
9. World Health Organization, South-East Asia Regional Office: Country Profiles on Tobacco or Health. New Delhi, 2002
10. World Health Organization. The World Health Report Archives 1995-2000.page 67. 1995
11. International Union Against Cancer (UICC). Tobacco Control Country Profiles .Global Link. www.globalink.org
12. Rahman MM, Rahman AM. Department of Community Medicine, Rangpur Medical College.: Prevalence of acute respiratory tract infection and its risk factors in under five children. Bangladesh Medical Research Council Bulletin. 1997 Aug;23(2):47-50.
102
13. Rahman M and Fukui T: Bidi smoking and Health: Journal of Public Health(2000) 114, 123-127. www.nature.com/ph
14. Bangladesh Bureau of Statistics. Prevalence of Smoking in Bangladesh, Dhaka , November, 1995
15. Rahman M, Samad Abdus, Chowdry, Fukui Tsuguya, Hira Kenji and Shimbo Takuro. “ Association of thromboangitis obliterans with cigarette and bidi smoking in Bangladesh: a case-control study”. International Jounel of Epidemiology 2000; 29;266-270.
16. Zulfiqar Ali , Atiur Rahman and Taifur.“ A Study on Tobacco Economics” . HNP Discussion paper. Economics of Toabcco Control paper No. 16. Tobacco Free Initiative World Health Organization. November 2003.
17. World Health Organization, Regional Office for South-East Asia Region; “ Noncommunicable Diseases in South-East Asia Region: A Profile”. New Delhi, 2002.
18. World Health Organization, Regional Office for South-East Asia Region. Women of South-East Asia Region, A Health Profile, World Health Organization, Regional Office for South-East Asia Region, New Delhi, 2000.
19. Prakesh C. Gupta & Hemali C. Mehta: Cohort study of all-cause mortality among tobacco users in Mumbai, India; Bulletin of WHO, 2000, 78(7) 877-883).
20. P C Gupta. Mouth cancer in India: a new epidemic? Journal of Indian Med Association: 1999 Sept; 97(9):370-3)
21. Murti PR, Gupta PC, Bhonsle RB, Daftary DK, Mehta FS, Pindborg JJ: Effect on the incidence of oral submucous fibrosis of intervention in the areca nut chewing habit. Journel of Oral Pathological Medicine. 1990 February: 19(2) :99-100.
22. Pandey M, Mathew A, Nair MK. Global perspective of tobacco habits and lung cancer: a lesson for third world countries. : Eur J Cancer Prev. 1999 Aug; 8(4):271-9.
23. Singh R. B et al, Hypertension and stroke in Asia: prevalence , control and strategies in developing countries for prevention. J Hum Hypertension: 14(10-11):749-763.October 2000.
24. Gupta R. Prevention of Coronary Heart Disease among Indians: focus on primary prevention. Journal of Indian Medical Association. 98(11):703-704. November 2000.
103
25. Pais P et al. Risk factors for acute myocardial infarction in Indians: a case control study. Lancet. 10: 348(9024): Risk Factors for acute myocardial infarctions in Indians: a case control study. Lancet. 10:348 (9024)”358-363. August 1996.
26. Deshmukh JS, Motghare DD, Zodpey SP, Wadhva SK. Low birth weight and associated maternal factors in an urban area. Indian Pediatr. 1998 Jan;35(1):33-6.
27. Rajesh P Dikshit and Shiela Kanhere. Tobacco habits and risk of lung, oropharyngeal and oral cavity cancer: a population-based case-control study in Bhopal, India. International Journal of Epidemiology 2000: 29:609-614.
28. Study on Tobacco Economics in Indonesia. Report to World Health Organization South-East Asia Regional Office, 2001.
29. Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco Control Strategy. English Summary, December 3, 2003
30. Guidotti, TL Critique of available studies on the toxicology of kretek smoke and its constituents by routes of entry involving the respiratory tract. Arch.Toxicol 1989; 63:7-12.
31. Isra Sarntisart: An economic Analysis of Tobacco Control in Thailand. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 15. Tobacco Free Initiative. World Health Organization, October 2003.
32. ASH Thailand: Thai Women and Tobacco: www.tobaccofreeasia.com.
33. Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiaitve. World Health Organization. October 2003.
34. Phyu Phyu Aung et al, Department of Physiology, Institute of Medicine1, Department of Medical Science and Physiology Research Division, Department of Medical Research Chronic respiratory effects of occupational exposure to tobacco dust, (1988)
35. Aung et al, CVD Project, Department of Health Profiles of patients with myocardial infarction admitted to coronary care units of Yangon General Hospital and New Yangon General Hospitals,( 1989)

104
36. Aung, Aung Chein, Kyi Kyi san Amung, Khin Mar Yi, Kywe Kywe Thein, Khin Thida Thwin, A clinical profile of acute myocardial infarction patients under the age of 45 years, 1990
37. Professor Kyaw Tint, Thein Ngwe, Department of Preventive and Social Medicine, Institute of Medicine 1 and CVD Project , Chronic Respiratory disease in urban and rural communities, (1990) Phyu Phyu Aung et al, Occupational Health Unit, Department of Health and Nutrition Research Division, Department of Medical Research ,A preliminary study on effect of cheroot smoking on ventilatory functions, (1990)
38. Maung Maung Cho, Phyu Phyu Aung and Tin Tun, The Effect of Cigarette Smoking on Nasal Mucociliary Activity (1990)
39. Kyaw Nyunt thein, Myo Win, Thin Thin Hlaing & Nyunt Tin, A study of the effects of tobacco smoking on lipid profile of apparently healthy Myanmar adults, 1996
40. Phyu Phyu Khin, Maung Maung & San Yi, Institute of Medicine, Mandalay, The study of lung functions in cigarette smokers and cheroot smokers, 1997.
41. Myanmar GYTS Fact Sheet.
42. Yagaya B. Yarki. A Study on the Economics of Tobacco in Nepal. Tobacco Free Initiative, World Health Organization, October 2003.
105
CHAPTER FOUR: WOMEN IN THE TOBACCO EMPLOYMENT
Women in the tobacco employment
In most countries of the Region, reporting and recording of employment data for persons engaged in tobacco industry is not complete. Most of the reports were based on whatever information was available. For those countries where the principle tobacco product used is in the form of cigarettes, the majority of employed persons are males; but in countries such as India, Bangladesh and Myanmar where products other than cigarettes are mainly used, the majority of people engaged in the tobacco industry are women and young girls.
In India- the majority of people engaged in tobacco employment are women. Women are involved in a whole range of jobs associated with tobacco like planting, weeding, making and maintaining beds, picking tobacco leaves, tying leaves, and removing leaves after drying, grading of tobacco and rolling of bidis.1
Bidi industry in India is the largest employer after agriculture and construction sector, at times the biggest and occasionally the only employer in the area. Bidi industry is a cottage industry no matter whether it is in rural or urban area. An estimate of bidi industry is around 10 million (6million rolling bidi, 4 million collecting leaves). 2
Bidi workers in India and Bangladesh consist mainly of women and children, with men considering the work too low or otherwise beneath them. Women comprise 65% of workforce in the bidi industry and children around 1 to 25%. 2 Most of the children are girls since it involves working at home. The majority of the workers are very poor and illiterate.
According to the Annual Survey of Industries (ASI) in 1993-94, about o.5 525 million workers found employment in the production of various tobacco products. Lately, bidi manufacturing seems to have been moving to the factory sector. Its employment has increased from 1,465 in 1971 to over 440,000 in 1993-94. This does not cover all bidi workers. According to the Labor Ministry, the figure is 4.4 million for the bidi sector. Another source of data is the National Sample Survey Organization (NSSO) 50th round data (1993-94) according to which, taking all stages of tobacco related activities, total employment in 1993-94 was 359,342 persons of whom 1,350,963 were males and 2,208,361 were females. 3
In Bangladesh, currently about 180,000 people are employed in tobacco leaf processing and tobacco manufacturing, wholesaling and retailing occupations. 4
Men consider sitting work unmanly and combined with low-pay; refuse to do the work, forcing their wives and children into it instead. Among bidi-making families, there
106
is a high rate of polygamy. Women and children engaged in bidi work can support themselves, allowing men to marry more wives. 2
In Nepal, by 96/97 there were 38 establishments producing tobacco products and the number of total employees was 3,213. Multipurpose household budget survey (1988) and household budget survey (1999) collected information on the economically active population 10 years of age and over who were engaged in bidi and cigarette processing. According to those survey reports, in Nepal 0.2% were engaged in tobacco industry; more males (0.4%) than females (0.1%). There was more tobacco production in urban than in rural areas. Female employment represented only a small portion of total manufacturing tobacco employment. Tobacco farming is on the decline in Nepal. 5
In Myanmar, official documents from the Department of Labour in 1997 recorded the number of female employees in cheroot industries as 2,303. It is estimated that there is at least four or five times of this number. Apart from the possibility that the cheroot industries did not register all those who were employed on a daily wage or salary, most factories hired women who took the material to their homes to roll. It is estimated that these women made up 60% of the tobacco industry. 6
In Indonesia, data for tobacco employment in the year 2003 was 245,626, 82.3% of them being women. 7
Occupational hazards of tobacco employment in South-East Asia Region.
Many women engaged in tobacco industry suffered from conditions arising from long hours of continuous sitting cross-legged in an unhealthy atmosphere doing a monotonous job. Among the many problems faced by those in bidi work are fatigue and weakness due to the repetitive and boring nature and long duration of work, stiff joints, back-aches, pain in the arm and different body parts, loss of appetite, dizziness, heartburn, stomach upset, fever, headache. There are also other complaints such as piles and stunted growth due to long hours of work without exercise or play. Vision also became impaired after many years of rolling bidis and cheroots.
Most of the working conditions in bidi and cheroot industries are poor, the places are poorly ventilated, crowded with tobacco dust and smell bad. Inhalation of tobacco dust for prolonged periods induces chronic asthma among the workers. Tuberculosis is also a common finding among the bidi workers in India and Bangladesh. Lack of space and crowded working conditions led to easy spread of infection among the workers.
In the bidi industry of India and Bangladesh, women are paid less and children the least. Discrimination was found in any way. As most of the female workers are poor and uneducated, they are timid and shy; they are also afraid that they might loose whatever

107
small amount of money they earn from the job; they do not know their rights and are least likely to ask for improvements in working conditions. They have to bear abuse and harsh treatment from their supervisors and bosses for fear of loosing the job.
Women continue to be cheated by all the tiers of this industry and but worse they end up sacrificing the lives of their children to the unhealthy dreariness of bidi industry for hours on end that stunts their future growth and aspirations. 2
Suriani’s survey 1996 on 80 tobacco farmers in Temanngung , Central Java found that the rate of Green Tobacco Sickness incidence is 63.7%. Common complaints are dizziness, headache and fatigue. The risk factors influencing GTS are work experience, location of leaves to be plucked, and utilization of safety equipment. 9
108
References
1. Shoba John and Shailesh Vaite. Tobacco and Poverty: Observations from India and Bangladesh. PATH Canada. October, 2002.
2. Mira B. Aghi: Women, children and tobacco ; paper prepared for WHO International Conference on Global Tobacco Control Law, 7 to 9 January, New Delhi, India.
3. World Health Organization, Regional Office for South-East Asia. Country Profiles on Tobacco or Health, New Delhi, 2002.
4. Statement by Dr. Selina Ashan : Current situation in Bangladesh in terms of tobacco control and the estent of enforcement of existing policies. A Technical Regional Consultation on the Economics of Tobacco Control, Jakarta, Indonesia.
5. Yagaya B. Yarki. A Study on the Economics of Tobacco in Nepal. HNP Discussion Paper. Economics of Tobacco Control paper No: 13, Tobacco Free Initiative, World Health Organization, October 2003
6. Nyo Nyo Kyaing: Study on Tobacco Economics in Myanmar. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 14. Tobacco Free Initiaitve. World Health Organization. October 2003.
7. Indonesian Heart Foundation , Jakarta.
8. Zulfiqar Ali , Atiur Rahman and Taifur.“ Appetite for Nicotine: An economic analysis of Tobacco Economics” . HNP Discussion paper. Economics of Toabcco Control paper No. 16. Tobacco Free Initiative World Health Organization. November 2003.
9. Ministry of Health Republic of Indonesia: The Tobacco Source Book: Data to Support a National Tobacco Control Strategy. English Summary, December 3, 2003
10. Isra Sarntisart: An economic Analysis of Tobacco Control in Thailand. HNP Discussion Paper. Economics of Tobacco Control Paper. No: 15. Tobacco Free Initiative. World Health Organization, October 2003.
11. Efforymson D. and Saifuddin A. Hungry for Tobacco: An analysis of the economic impact of tobacco on the poor in Bangladesh. PATH Canada. July 2000.
109
PART FIVE: CAMPAIGNING AGAINST TOBACCO
Governments of all countries in the Region are fighting against the tobacco epidemic in collaboration and coordination with International Agencies and local as well as International NGOs. Up to date, 9 out of 11 countries had signed the Framework Convention on Tobacco Control. Sri Lanka was among the first five countries to ratify the FCTC and the other countries are in the process of ratifying it.
In Bangladesh through an executive order issued in 1988, restriction has been imposed on advertising of tobacco in the government mass media including Radio and Television. Through the same executive order, issued in 1988, the government prohibited smoking at the Presidential House, the hospital premises and all domestic flights of the national airliner. Bangladesh has also drafted a Bill on “Smoking and Use of Tobacco Product Control Act” which has been vetted by relevant Ministries of the government and is awaiting final approval by the National Legislative Body.
Bangladesh Anti-Tobacco Alliance (BATA) was formed in October 1999. BATA consists of fifteen member organizations active in tobacco control. BATA' s purpose is to contribute to the health and well-being of all Bangladeshis by educating the public and policymakers about the dangers of tobacco, and by helping to strengthen the nation's tobacco control legislation. BATA member Work for a Better Bangladesh, with PATH Canada, has conducted several studies on tobacco, including Children's Exposure to Cigarette Ads and Hungry for Tobacco: An analysis of the economic impact of tobacco on the poor in Bangladesh and British American Tobacco's Youth Smoking Prevention Campaign: What are its actual objectives?.
In Bhutan, there is a complete ban on tobacco advertisement, promotion and sponsorship.
There is also a complete ban on tobacco advertising, promotion and sponsorship in DPRK.
In India , the Cigarettes and Other Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003 was enacted in the year 2003. The Act, inter-alia provides for ban on smoking in public places, ban on direct and indirect advertising and sponsorship of tobacco products, ban on sale of tobacco products to minors and regulating the packaging and labeling of tobacco products and restriction of sale of tobacco products to minors.
Organizations working in the area of tobacco control include Autonomous Academic Institutions, Association of Professionals, Institutes involved in Tobacco cessation program, Religious Bodies and associations and Pharmaceutical companies.
In Indonesia, government regulation No 81/1999 had regulations on nicotine and tar
content, disclaimer / warning on health problems, registration to MOH, limitation of sales through vending machines, restriction of advertisement, designation of smoke free areas, community participation to help control policy implementation and diversification of tobacco plant. Violations are subject to penalty.

110
Unfortunately due to pressure from the tobacco manufacturers, current policies and regulations are much weaker. Amendment No 38/2000 was made with provisions to adjust production according to regulations (large producers from 5 years to 7 years). Smoking scenes are prohibited from tobacco advertisements but advertisements are permitted in electronic media after 20:00 hours. In practice, advertisement continues to air beyond the regulations. Smoke free areas are limited not as stated in regulations, there is lack of community involvement, no sanctions were imposed and regulations and policy are not promoted properly. There were no regulations specifically to control clove cigarette (eugenol); only tar and nicotine; High clove leads to high tar and addiction. Article on diversification plant is in-effective in reducing nicotine level and there was no law enforcement at all.
Rights of non smokers to have protection of involuntary exposure to tobacco smokes, is not promoted properly. There is no regulation to prohibit person under 15 to purchase, possess, use or sell tobacco products.
National Committee for Tobacco Control was established with 23 member organizations including the Indonesian Heart Foundation. Most of the member organizations have other areas of work apart from tobacco control. The Committee coordinates among the member organizations towards tobacco control. The Indonesian Smoking Control Foundation, Indonesian Cancer Foundation, Consumer’s Groups etc. also work actively in the tobacco campaign. Indonesian Women against Tobacco is also an active NGO, campaigning against tobacco. Most of the NGOs focus on health education, school-based anti-tobacco campaigns, child to child and youth to youth communications, advocacy through all forms of media and lobbying against tobacco industry. They monitor tobacco advertisements and report to the government about breaking in the regulations. They even went into a lawsuit against one tobacco giant but lost the case unfortunately. They wrote to the President and to the parliament demanding for stronger regulations. Like in the case of ASH and Thailand, NGOs in Indonesia lobbied the government and the Ministry of Health for stronger regulations and to sign the FCTC. They receive little technical guidance from the MOH or UN agencies on their campaigning.
In Maldives, in most of the islands, Women’s Development Committees of the islands play an important role regarding tobacco use and control. With their effort and hard work, in 7 islands all women has stopped tobacco use and the islands are known as women’s tobacco free islands. Their work was recognized by the government authorities hence the Ministry of Health has awarded them a special certificate. More islands are taking the same path and working on tobacco control in the island level.
Tobacco control regulations of the Maldives include: regulation on tobacco advertising (1984), regulation on sale of tobacco products to minors (1991) and regulation on smoking in public places and government buildings (1993, 94, 97).A high-level anti-tobacco committee was formed in 1996. In 2000, households not using tobacco were awarded a special certificate by the Ministry of Health. Import duty on tobacco products increased 3 fold. Ministry of Health received WHO anti-tobacco award in 1997 and Minister of Education received WHO anti-tobacco award in 2002.
In the 1940’s, importation of tobacco was banned and smoking in public was also banned by law. Later in the 1940’s a new law came into effect that controlled the amount of

111
tobacco importation and also introduce a licensing mechanism for tobacco importers. In 1951 a new law banned all forms of tobacco in the country; however, these initiatives were later dissolved after a popular public revolt in the late 1950’s. No Law on tobacco control existed since then.
Myanmar officially launched the National Tobacco Control Programme in the
year 2000. Strong political commitment became more evident when the Office of the State Peace and Development Council officially formed the National Tobacco Control Committee in March 2002 which is headed by the Minister for Health and includes heads of departments and local NGOs as members. This Committee set guidelines for the tobacco control measures to be implemented in the country. The Ministry of Information had prohibited advertisement of tobacco on television ,radio and all electronic media since 1997. Following the guidelines set by the National Health Committee and National Tobacco Control Committee, tobacco advertising billboards had been banned from the vicinity of schools, hospitals, health facilities, sports stadiums and maternity homes since May 2002 and after the completion of contracts between the tobacco industry and the city development committees, all tobacco advertisements were banned from all over the country in April 2003. According to the instructions issued by the General Administration Department of the Ministry of Home, tobacco advertisement were been banned from the newspapers, journals and magazines in early 2003.
The Ministry of Health is in the process of endorsing the Control of Smoking Law which is mainly concerned with protection of non-smokers’ health from exposure to tobacco smoke, prohibition of sales to minors and comprehensive ban on tobacco advertisement.
Many national NGOs are involved in anti-tobacco campaigning. The Maternal and Child Welfare Association, chaired by the wife of the Prime Minister, has members in all the townships and villages in the country, is the largest NGO that has formed partnership with the Ministry of Health in many health programmes including advocacy and community awareness campaigns for tobacco control. Other NGOs include Myanmar Medical Association, Myanmar Nurses Association, Myanmar Anti-Narcotics Association, Myanmar Health Assistant’s Association, Myanmar Music Association, Myanmar Film Association etc.
In Nepal, The National Health Education Information and Communication Centre, Ministry of Health, has drafted the smoking (Prohibition and control) Act, 2058. This draft covers many areas of FCTC; prohibition of smoking and spitting at Institutions and public places, restriction of sale to minors etc.
B.P. Koirala memorial Cancer Hospital, Bharatpur provides health education including education on harmful effects of tobacco products to outpatients and attendants, two times a day at outpatient waiting hall. Mrigendra-Samjhana Medical Trust provides health education and services to rural people of Nepal and one of the main activities is to educate people about the harmful effects of tobacco consumption. Nepal Cancer Relief Society is involved in preventive and treating cancer patients. Its prevention activities also provide anti tobacco education to its clients and their friends and relatives. The priority area of Janak Memorial Service Centre are health education on the harmful effects of tobacco, alcohol and drug use mainly school based programme. National Front Against Tobacco advocates against tobacco using high level influential individuals from different sections of

112
the society, the activities of this organization are limited to holding conferences and seminars annually.
In Sri Lanka, although there is no direct programme to prevent tobacco use exclusively among women, the “No tobacco Programme” launched by the Ministry of Health educate young women to deglamourize smoking and to make young males understand that smoking makes them non-attractive and socially unacceptable. Tobacco legislation in Sri Lanka include: Consumer Protection Act No: 1 of 1979 which includes compulsory government warning on cigarette packs, Railway Services Act No; 20 of 1971 which prohibited smoking and chewing of betel in and around the trains and also on the premises, Transport Law No 19 of 1978, which prohibited smoking in buses, Children and Young Persons Ordinance which prohibited sale of tobacco/cigarettes to persons under 16 years, Public administrative Circular No 08/99 which prohibit smoking in State Institutions and Air Lanka smoking ban.
Thailand’s comprehensive tobacco control measures are recognized internationally as one of the success stories in Asia. As early as 1967, health warnings on tobacco products had been requested by Medical Association of Thailand and the warnings appeared on cigarette packages in 1974. In 1985, cigarette advertising was banned on electronic media and smoking was banned in the House of Representatives. In the year 1986, Action on Smoking and Health (ASH) started as “Thai Anti-smoking Campaign Project”. In 1988, Thailand Tobacco Monopoly was ordered to refrain from advertising. National Committee for the Control of Tobacco Use was established in 1989. In 1992, two laws were enacted: Non-smokers’ Health Protection Act and Tobacco Products Control Act. Under these laws, public places were designated as non-smoking areas and these are expanded in 2002. Tobacco taxes are increased gradually from 55% in 1994 to 75% in 2001; 2% of cigarette and tobacco tax are levied for Health Promotion Fund. The success of Thai tobacco control measures reflected in the decline of smoking rates among both sexes.
ASH is the successor of TASCP (Thai Anti-smoking Campaign Project) which was formed in 1986. In 2000, the Rockefeller Foundation funded ASH as the center for the South-East Asia Tobacco Control Alliance. The activities of ASH/TASCP represent the core of NGO actions in Thailand.
Thailand has long felt that preventing women from smoking is a neglected area in tobacco control programmes and research worldwide. Faced with the import of cigarettes targeted at women, the TASCP in 1994 set up the “Thai women Do Not Smoke Project” with the objective of preserving the nonsmoking norm among Thai women. The project was supported by Miss Thailand and a number of young movie and television stars, who acted as presenters for the program. In 1996, when the Thai Tobacco Monopoly (TTM) announced that it would begin marketing a brand of cigarette to women to compete with Virginia Slims, ASH mobilized influential Thai women to oppose this move. Women members of Parliament, celebrities and writers all joined the campaign. All these efforts resulted in TTM’s dropping its plans to introduce “women’s” cigarettes. Although research studies in 1999, had predicted that smoking by women could rise to 15% in Thailand over the next 25 years, while smoking among men could drop to about 25%, it is hoped that active movements by the civil society in Thailand, in collaboration with the Ministry of Health could prevent this trend. The Thai women Do Not Smoke project is being funded by the new Thai Health Promotion Foundation.

113
References
1. Country responses to questionnaire for the study.
2. Country presentations at Regional Consultation on Development of Multisectoral
mechanisms for Comprehensive Tobacco Control Strategy, Yangon, December, 2002
3. Country presentations at A Technical Regional Consultation on the Economics of
Tobacco Control, Jakarta, December 2003.
4. Statement by Dr. Selina Ashan : Current situation in Bangladesh in terms of
tobacco control and the extent of enforcement of existing policies. A Technical
Regional Consultation on the Economics of Tobacco Control, Jakarta, Indonesia.
5. BATA website
6. Dr. Prakit Vateesatokit: Tailing Tobacco Control Efforts to the Country. In
Tobacco Control Policy: in Strategies Successes and Setbacks. World Bank and
Research for International Tobacco Control (RITC).
7. Meetings with ASH, National Committee (Indonesia) for Tobacco Control
Indonesian Heart Foundation, Indonesian Women against Tobacco.
114
PART SIX: CONCLUSIONS AND RECOMMENDATIONS Conclusions
It could be stated that the situation of women and tobacco in South-East Asia Region is somewhat different from other Regions in many areas.
A huge percentage of women tobacco users chew some form of smokeless tobacco in various forms; many countries including Indonesia, India, Sri Lanka and Thailand do not accept smoking as suitable behaviour for girls and women. There is still a form of social stigma against women smoking. The majority of women tobacco users in India started use of tobacco by chewing. Although smokeless tobacco use is low in Thailand and Sri Lanka, it is very high in India, Bangladesh, and Nepal and to a certain extent in Myanmar. Burden of disease arising from smokeless tobacco use in the Region has not been estimated, smokeless tobacco use is still taken as a lesser problem than smoking. Anti-tobacco campaigns usually aim towards prevention and control of smoking and fail to include smokeless tobacco use as part of their campaign activities.
Higher prevalence of smoking was seen among women residing in rural areas, among the uneducated and the poor. Unlike developed countries where the majority of young, educated and socialized women smoke under the influence of factors such as socialization, peer pressure, experimentation, liberation, stress, anxiety, depression etc; the majority of women smokers in South-East Asia Region smoke at an older age and the determinants of smoking were quite different from the developed countries. Smoking was more of a social habit of spending time with guests, killing boredom arising from monotonous nature of household chores and smoking something handy and cheap as it could be rolled by one’s own hands. It was a habit of decades or even centuries. In Thailand, the majority of women smokers reside in the North; where tobacco is grown, whereas smokers of metropolitan areas belong to some groups influenced by western culture.
Tobacco Industry’s luring for women by introducing women’s brands has yet to gain
momentum in the Region. Women still stick to older traditional forms of tobacco products made locally. Very cheap tobacco products are easily available for women of the Region in various forms, many of them not being licensed and not following any tobacco product regulations. A huge portion of women smokers smoke hand-rolled tobacco products, cheap bidis and cheroots etc. They could not spend as much money as their male counterparts on tobacco. Still, tobacco money was depriving many families of tobacco users from food, clothing, education and health expenditures.
Among the women smokers of the Region that belong to the poor and the uneducated, weight gain is not a big issue. Women smokers who could not quit are mainly because of addiction, there were very few persons that do not quit for fear of weight gain. It was mainly that tobacco use has become part of their daily routine. Most of them has not received adequate information on dangers of tobacco use, how tobacco use could effect on the health, social and economic aspects of their lives, how quitting could bring great benefit to them, where to seek for counseling and support even if they want to quit etc. There are no studies conducted in the Region specifically on the difference between men
115
and women on cessation of tobacco use although many studies conducted globally reported the controversial finding that women faced more difficulty to quit smoking than men.
Due to the high prevalence of tobacco use among women of the South-East Asia
Region, burden of disease attributable to smoking and smokeless tobacco use among women is huge. Lung cancer rates and oral cancer rates are very high among the women; other diseases attributable to tobacco such as Chronic Obstructive Airway Disease, hypertension and coronary heart diseases are also high.
In countries like Indonesia, Nepal, Bangladesh etc. prevalence of smoking among males was more than 50%. In general, men are heads of households and took the advantage of smoking freely inside their homes. They also smoke in public places. Although there are legislations against smoking at public places in most countries, enforcement of these legislations in most countries is quite low. Hence, the danger of women and children exposed to ETS is considerably high. Women and children suffer from many diseases related to inhalation of ETS.
Huge number of women being employed in the bidi and other tobacco industry are being deprived of human rights; labour rights, child rights and the rights of women. They suffer from many health hazards and receive very little money for their hard work. Many women in Bangladesh and India started working in various jobs related to tobacco since they were young and were deprived of their childhood. Little action had been taken by governments regarding to tobacco employment and working conditions at bidi and other cottage industries. Recommendations
What should be done for the women of South-East Asia Region to reduce their tobacco use and to prevent them from becoming prey to the Tobacco Industry’s various techniques? Recommendations for World Health Organization, member countries and NGOs are specified below under different areas of action that should be taken.
• Information support for tobacco control • Promotion of community awareness • Legislation and political commitment • Cessation • Research
Information support for tobacco control The World Health Organization could play a leading role in providing information support for tobacco control to all its member countries. Technical assistance should be provided by experts to form national policies and plan of actions, to formulate strategic plans for tobacco control where gender issues should be specifically highlighted.
116
Evidence-based information regarding to tobacco use in women, the hazards of tobacco use, their effect on the foetus and the pregnant mother, hazards of tobacco handling and inhaling of tobacco dust among tobacco workers etc should be shared among member countries and widely disseminated. Success achieved as well as challenges faced by the countries should also be reported to WHO to be able to share within countries. Tactics of tobacco industries particularly their activities aiming to recruit women and youth smokers in developing countries should be carefully monitored and subsequently informed to member countries. Networking among countries on tobacco control among SEAR countries should be established, a specific website should be developed if possible. Technical expertise for networking should be provided by TFI unit of WHO Headquarters. Tobacco-control networking is also vital for all WHO member countries. A database on tobacco-related information should be established with regular reporting and monitoring systems. Countries should be provided with updated information of what other countries are doing as well as recent findings of evidence-based best practice; they should also receive feedback on areas needed to be strengthened. Activities of member countries should also be recognized by WHO TFI, these should be recorded and disseminated.
It is learnt that in a meeting organized by WHO and CDC in Copenhagen, it was decided that each region within WHO will develop an on-line tobacco information system of country-specific data which will be linked to a global portal at HQ. This would give information on all aspects of tobacco – prevalence, economics and industry behavior, legislation, FCTC and general policy of tobacco control. This decision is highly appreciated by member countries and is hoped to be implemented in the near future.
At the Regional Workshop for Surveillance held in Delhi in October 2003, Member
countries had also recommended for the development of a Regional Surveillance system for tobacco use among population sub-groups. (Partnering Global Information System for Tobacco Control: GISTOC). It has been highly recommended to integrate and operationalize surveillance activities in country work-plans and develop a Regional on-line database.
WHO and other agencies should allocate funds for National sentinel surveys of
tobacco use, monitoring system of tobacco production, consumption, expenditure and tobacco-related diseases.
Partnership within Ministries, UN and international agencies and NGOs is vital for
the sharing of information necessary for the planning, implementing and evaluating of Regional and national comprehensive tobacco control programmes.
Countries should build their own database and gather information related to tobacco consumption, production, tobacco employment and the proportion of women engaged in the employment, incidence of tobacco related diseases, price and tax measures etc. To facilitate this process, establishment of Tobacco Control Committees at the National

117
Level is required. The Committees should include representatives from all related departments as well as representatives of National and International NGOs. This Committee should be responsible for collecting and sharing of information within different sectors. NGOs could collect data and disseminate information. Many NGOs had played important roles in providing crucial information for country delegates at FCTC negotiating sessions. NGOs should also focus on the situation of women and tobacco in the Region and provide information to policy makers and programme planners. Promotion of community awareness World Health Organization should allocate adequate funds to tobacco control programmes of member countries for awareness campaigns; community awareness programmes need technical as well as financial assistance from WHO. Tobacco control programmes in all countries of the Region should emphasize on educating the public on the negative impact of tobacco use on all aspects: health, social and economic effects. Resources should be mobilized from any possible source, such as the Health budget, ear-marked tax, donations, grants etc. Messages should be given through all forms of media, electronic, print, folk media etc. in every possible way.
As the majority of women smokers in the South-East Region belong to the poor and
the uneducated, it is very important that measures should be sought for to make the health education messages reach the rural poor, to women residing in the urban slums, to the illiterate women and to women who have to stay at home and are unable to reach by existing education programmes. This could be done by Multisectoral collaboration and coordination; Ministry of Health alone would not be able to reach to all the target groups.
It is also a crucial issue to impart information on dangers of ETS to the majority of
adult men who had taken for granted that smoking inside homes and public places was their inborn right. The majority of men were ignorant of the fact or indifferent to the fact that their smoking hurt the people near them including their children and their spouses.
It is estimated that expenditure on tobacco ranges from 5% to more than 20% of
household expenditures. Among low income groups, it could be even higher. The tobacco money is depriving the children and women from nutritious food and other basic necessities. This fact and the burden of tobacco-related diseases on the household economy could be made known to the public through various measures.
NGOs play an important role in promoting community awareness. They could work
in certain areas such as school health, empowerment of women groups, involvement of men in family decision etc. Encouragement and support by governments for NGO movements towards tobacco control is essential.
Legislation
118
The World Health Organization has led member countries towards the historical endorsement of Framework Convention on Tobacco Control. Up to this day, nine countries of SEAR had signed the Convention and 2 member countries, Sri Lanka and India had ratified it. It is learnt that other member countries are in the process of ratifying the convention. It is learnt that to make the treaty a reality at country level, WHO is committed to providing assistance in the following forms:
• Information material documentation (e.g. toolkits) • Development of Model national legislation or elements to be included in a
national legal framework;
• Training courses, awareness raising workshops at the regional and/or subregional level.
• Country-specific assistance, e.g. building of institutional capacities. • Provision of infrastructural support to developing countries.
Almost all countries in the Region have some form of legislation / regulation on tobacco control. However, the existing laws, rules and regulations of certain countries have areas to be strengthened. It is urgently required to enforce legislation which includes comprehensive ban of tobacco advertisement, prohibition of smoking and spitting at public places, prohibition of sale to minors, designation of public places as smoke-free and health warning on cigarette packages in local language. Legislation should include measures for special protection of women and children against the dangers of tobacco use. Inclusion of dangers of tobacco in the school curriculum starting from the primary level is a very effective measure to prevent the youth from experimenting tobacco. As women share a substantial portion of tobacco employment, it is also required to enforce labour rules and regulations for women and children employed in the tobacco employment. Many female workers are minors and they have been mistreated by their employers who took advantage of their age and ignorance. Most of the cheroot and bidi industries are cottage industries, women and girls took the materials and roll them at home and they are not covered by labour regulations and social security services.
NGOs could focus on income generation for women, women empowerment and community education for women. Dangers of tobacco should be included in self-care at home manuals and other manuals and booklets aiming to educate the women on self-help basis. Cessation
World Health Organization and other UN agencies and donors should provide technical and financial support to member countries for Cessation of tobacco use including Nicotine replacement therapy (NRT), counseling and physician support. Many developing countries in the Region are not able to afford for NRT.
119
Countries have many constraints to establish cessation clinics based on drugs and
equipments. Community-based cessation programmes have proved to be successful in project areas of the Region. These should be expanded to all countries and cover rural and remote areas. These community-based cessation programmes could also be conducted jointly with NGOs.
Research We are still lacking of evidences to advocate the decision makers and to plan,
implement and monitor programmes. A much wider area of research necessary to prevent and control tobacco deaths in the Region.
The following research areas are identified for women and tobacco in the Region: • Research studies for burden of disease due to tobacco in the Region including
passive smoking. • Research on prevalence of low-birth weight, abortion and other complications
arising from tobacco use among pregnant women. • Knowledge, Attitude and Prevalence studies among adolescent girls and women
regarding to tobacco use and its effects. • Monitoring of tobacco industry activities towards women and girls. • More specific studies on women engaged in tobacco employment emphasizing on
their mental, social and health effects.
120
120
Annex
Questionnaire for Regional Analysis of Women and Tobacco in
South East Asia Region.
This questionnaire is designed to collect information related to the general socio-
economic and health status of women, situation of tobacco use among women, impact of
tobacco use and tobacco labour on women’s health and economy and situation of tobacco
control policies and legislations in WHO South East Asia Region. This questionnaire
comprises of four parts as follows:
Part 1: Prevalence of tobacco use
Part 2: Health consequences of tobacco
Part 3. Tobacco control activities related to women
Part4: Laws, Acts and Regulations related to tobacco and women
In each part of the questionnaire, the data can be derived from reports, records or surveys
either national level or sub-national level. Please identify the source or sources of data
wherever possible.
If there are other information related to women and tobacco in your country which is not
included in this questionnaire, please add that information into the profile.
Thank-you four your cooperation and commitment towards tobacco control in South East
Asia Region.
121
121
Questionnaire for Regional Analysis of Women and Tobacco in
South East Asia Region.
Name of country ------------------------------------------------------------------------
Completed by:
Name: --------------------------------------------------------------------------------------------
Designation--------------------------------------------------------------------------------------
Department/Institute/Organization -----------------------------------------------------------
------------------------------------------------------------------------------------------------------
-----------------------------------------------------------------------------------------------------
Address ------------------------------------------------------------------------------------------
-----------------------------------------------------------------------------------------------------
-----------------------------------------------------------------------------------------------------
-----------------------------------------------------------------------------------------------------
e-mail address -----------------------------------------------------------------------------------
Fax:------------------------------------------------------------------------------------------------
Telephone ---------------------------------------------------------------------------------------
PART 1: TOBACCO USE PREVALENCE
122
122
1.1. Smoking prevalence (%) by gender and region (Current smokers)
Urban Rural Total Year Male Female Total Male Female Total Male Female Total
Source/s -------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
1.2 Age-sex specific prevalence of smoking (%) by education group and region (Current smokers) Year:
Urban Rural Total Education Male Female Total Male Female Total Male Female Total Illiterate Primary school /read and write
Secondary Education
Graduate Post Graduat
Total Source/s --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
1.3 Prevalence of tobacco use (%) for different types of tobacco products by gender and
region (Current users) Year:
Urban Rural Total

123
123
tobacco products
Male Female Total Male Female Total Male Female Total
Cigarettes Bidis Cheroots Cigars Pipes Watery tobacco
Betel quid with tobacco
Chewing tobacco
Gutcha Pan masala
Total Source/s -------------------------------------------------------------------------------------------------
1.4 Trend of Annual Per capita Consumption of Cigarettes
Year Male Female Total Total
Source/s -------------------------------------------------------------------------------------------------
1.5 Trend of Annual Per capita Consumption of Other Tobacco Products
Year Male Female Total

124
124
Total
Source/s -------------------------------------------------------------------------------------------------
1.6 Attitude and perception of the community towards tobacco use ( If any survey done on KAP of the community including smokers as well as
nonsmokers ) Year of study:
Urban Rural Total Attitude Male Female Total Male Female Total Male Female Total Positive attitude towards tobacco use
Negative attitude towards tobacco use
No opinion
Total Source/s ------------------------------------------------------------------------------------------------- 1.7. Are there any data on percentage of women exposed to Environmental Tobacco Smoke ? If yes, please describe briefly ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ PART 2: HEALTH CONSEQUENCES OF TOBACCO 2.1 Ten leading causes of Mortality for five years
125
125
Year Serial Number
Disease Source of information
Remarks
Source/s ------------------------------------------------------------------------------------------------- 2.2 Tobacco related diseases.
2001 2002 Disease
Males Females Total Males Females Total
Mouth and Oropharynx Cancers
Oesophagus Cancer
Pancreas Cancer
Trachea, Bronchus and Lung Cancers
Hypertensive Diseases
Ischemic Heart Disease
Cerebrovascular Disease
Lower Respiratory Infections
Chronic Obstructive Pulmonary Disease
Hypertension
Low Birth Weight
Birth Asphyxia
126
126
Premature labour
Abortion
Total Cases
Source/s ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ Part 3. Tobacco control activities related to women
3.1 .Are there any women’s organizations or any NGOs working to prevent and
control of tobacco use among women ? If yes, please describe briefly ---------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
3.2 Are there any health education programmes in your country aiming at
prevention and control of tobacco use among women? If yes, please describe
briefly.-------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
Part 4: LAWS, ACTS AND REGULATIONS RELATED TO TOBACCO
4.1 Are there any tobacco control laws enacted in your country? If yes, please state the
name of the law, year being enacted and a brief account of the contents of the law. If
available, please attach the related documents-----------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
4.2. Are there any regulations related to tobacco control? If yes, please state a brief
account of the regulations and the year they were issued. If available, please attach the
127
127
rules, regulations or standing orders related to tobacco control..--------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
4.3 Are there any laws, rules and regulations related to tobacco control that have special
provisions to protect women from the tobacco epidemic? If yes, please state them and
briefly explain them. If available, please attach the document. ---------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------