stump the professor: challenges in … · ct head negative. 3 days later blood cultures revealed...
TRANSCRIPT

STUMP THE PROFESSOR:
CHALLENGES IN ENDOCARDITIS
Brittany Weber MD, PhD

Outside Hospital Course
History of Present Illness:
52 year old male with history of bicuspid AV and bioprosthetic AVR presented with fevers, malaise
Labs notable for WBCs 9K, Platelets 11K, Lactate 3.7, Troponin-I 3.7, NT pro-BNP 34,000, Cr 1.8
Admitted to MICU and treated with broad-spectrum abx.
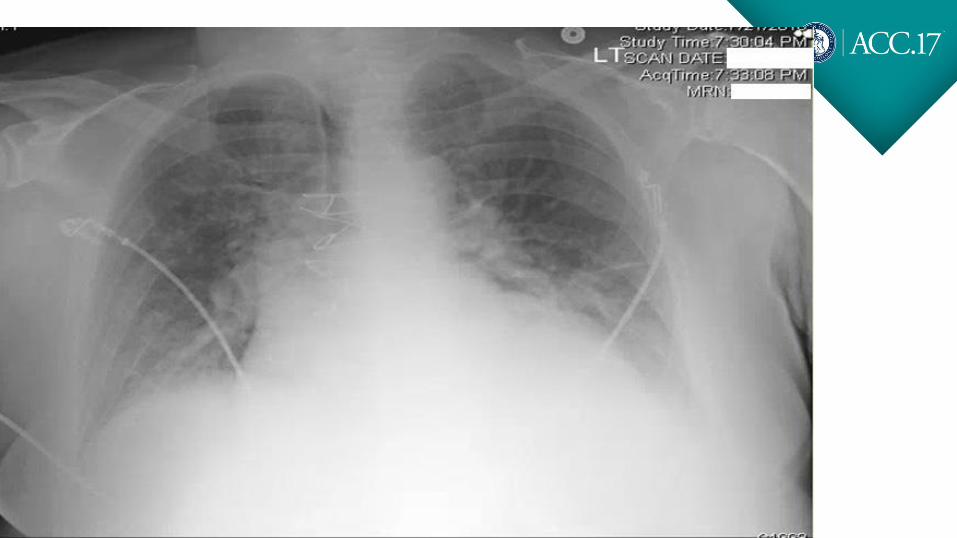
CXR negative. CT abdomen with duodenal fat stranding and lymphadenopathy. CT head negative.
3 days later blood cultures revealed MSSA. Antibiotics were switched to oxacillin, rifampin,
gentamicin and he was transferred to the BWH for further care.
Past Medical History
Past Medical History• Bicuspid Aortic Valve
• Streptococcus endocarditis in July 2004 after
deep dental scaling, treated with 6 weeks of IV
antibiotics.
• Developed worsening DOE over next year,
found to have severe aortic regurgitation and
underwent 27 Carpentier Edwards
bioprosthetic AVR in May 2005
Social History• Single, designer for sheet metal and
plastics
• 4-5 beers per week. Occasional
cigarettes. No IVDU
Home MedicationsASA 81mg
Multivitamin

Physical Exam
Vitals: T 38.2 °C (100.7 °F) | P 102 | BP 130/58 mmHg | RR 20 | 94% RA
• General: Ill-appearing, no acute distress
• HEENT: palatal petechiae, epistaxis, no LAD
• CV: JVP 12 cm H20, tachycardic, regular rate. Normal S1 and S2. 3/6 mid-
peaking systolic murmur at RUSB, 2/6 diastolic decrescendo murmur at RUSB.
No S3 or S4. Laterally displaced and diffuse PMI
• Pulm: Bibasilar crackles up to mid lung fields
• Abd: soft, mildly distended, mild TTP, normoactive BS, no
hepatosplenomegaly,
• Ext: splinter hemorrhages on fingernails, petechiae diffusely over extremities,
back, and abdomen.
• Neuro: A&Ox3, CN II-XII intact. Sensation and strength intact

Admission ECG

Old ECG
V1
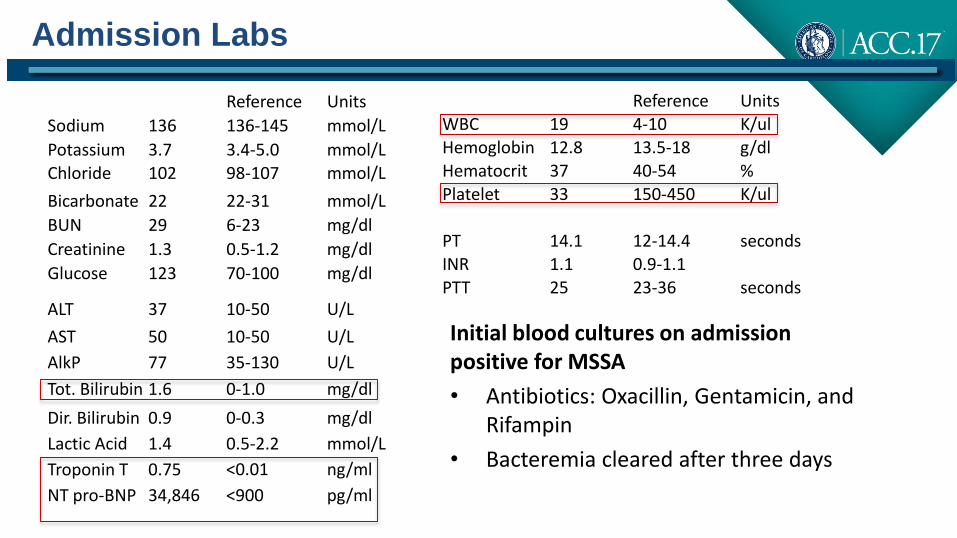
Admission Labs
Reference Units
Sodium 136 136-145 mmol/L
Potassium 3.7 3.4-5.0 mmol/L
Chloride 102 98-107 mmol/L
Bicarbonate 22 22-31 mmol/L
BUN 29 6-23 mg/dl
Creatinine 1.3 0.5-1.2 mg/dl
Glucose 123 70-100 mg/dl
ALT 37 10-50 U/L
AST 50 10-50 U/L
AlkP 77 35-130 U/L
Tot. Bilirubin 1.6 0-1.0 mg/dl
Dir. Bilirubin 0.9 0-0.3 mg/dl
Lactic Acid 1.4 0.5-2.2 mmol/L
Troponin T 0.75 <0.01 ng/ml
NT pro-BNP 34,846 <900 pg/ml
Reference Units
WBC 19 4-10 K/ulHemoglobin 12.8 13.5-18 g/dl
Hematocrit 37 40-54 %
Platelet 33 150-450 K/ul
PT 14.1 12-14.4 secondsINR 1.1 0.9-1.1PTT 25 23-36 seconds
Initial blood cultures on admission positive for MSSA
• Antibiotics: Oxacillin, Gentamicin, and Rifampin
• Bacteremia cleared after three days

How is endocarditis diagnosed in 2017?

Modified Duke Criteria for Endocarditis
Definite IE:
2 Major Criteria
1 Major and 3 Minor
Criteria
5 Minor
Possible IE:
1 Major and 1 Minor Criteria
3 Minor Criteria
Echo (+) for IE as Major Criteria:
Vegetation
Abscess
New partial dehiscence of prosthetic valve

Updated Diagnostic Approach by ESC IE Guidelines
Eur Heart J (2015) 36 (44): 3075-3128

Transthoracic Echo
• LVEDD: 58 mm
• Wall thickness: 15 mm
• Diffusely hypokinetic with EF 46% (Simpsons)
• Mild MR. PASP 37
• Aortic valve prosthesis: Stable, severe AI, High gradients

Hospital Course
• TEE planned
• Cardiac Surgery consulted for AVR
• Recommended optimization of volume status prior to surgery
• ID consulted for antibiotic management
• Developed acute kidney injury felt to be secondary to Gentamicin
• Antibiotics switched to Oxacillin, Rifampin, and Levofloxacin

Progressive PR prolongation
PR 216ms 224ms

EGFR
Progressive anuric renal failure
0
10
20
30
40
50
60
Day 1 Day 2 Day 3 Day 4 Day 5
•Hemodialysis planned

TEE
Short Axis Aortic Valve Long Axis Aortic Valve

Post-op TEE comparison
2005 2016

Surgical Risk
Untreated endocarditis Treated endocarditis
Source: Risk Model and Variables - STS Adult Cardiac Surgery Database Version 2.81
Risk of mortality 14.30%
Morbidity or Mortality 59.40%
Permanent Stroke 2.50%
Prolonged Ventilation 60%
Renal Failure N/A
Reoperation 20%
STS Risk Score Procedure: AV Replacement
Risk of mortality 7.80%
Morbidity or Mortality 42.60%
Permanent Stroke 1.30%
Prolonged Ventilation 41%
Renal Failure N/A
Reoperation 14%
STS Risk Score Procedure: AV Replacement

Thomas J. Cahill et al. JACC 2017;69:325-344
Indications for early surgery
1. Heart Failure
2. Uncontrolled
Infection
3. Prevention of
embolism

Hospital Course
• Urgent surgery was considered.
• Valve was stable. Tolerating severe AI. Blood cultures were negative. Likely
abscess.
• Renal shutdown
• Hemodialysis was started for volume removal
• Cardiac 18F-FDG PET was obtained

Preparation for 18F-FDG Cardiac PET
WHAT TO EAT AND DRINK THE NIGHT BEFORE YOUR EXAM
The night before your scan at your regular dinnertime, start a high fat, high protein no carbohydrate diet and avoid sugars (glucose, fructose, sucrose, etc). You should also eat breakfast 3 hours before your appointment time.
Your choice of dinner and breakfast- should include:
Fatty unsweetened foods (fried in butter or olive oil, broiled, but notgrilled):
Chicken, turkey, fish, meats, meat only sausages, fried eggs, bacon, scrambled eggs prepared without milk, omelet prepared without milk or vegetables, fried eggs and sausages, fried eggs and bacon, hotdogs (plain -without the bun), hamburgers (plain - without the bun or vegetables) A lot of patients will have fried chicken for supper (just a suggestion).
You should not eat any food containing carbohydrates and sugars including:
Milk, cheese, bread, bagels, cereal, cookies, toast, pasta, crackers, muffins, peanut butter, peanuts, fruit juice, potatoes, candy, fruit, rice, chewing gum, mints, cough drops, vegetables, beans, alcohol, Anything with Splenda.
You should drink clear liquids without milk or sugars
INSULIN DEPENDENT DIABETICS - Do not alter your insulin pump settings.
AVOID STRENUOUS EXERCISEat least one day prior to scan.
Zero carbohydrate
High fat

Cardiac 18F-FDG PET/CT
Axial Coronal

Periannular Extension
• 10-40% of native valve
• 56-100% of prosthetic valves
Complications: 1. Abscess2. Pseudoaneurysm3. Aorto-cavitary fistulas
Ann Thorac Cardiovasc Surg 2009

Wang et al. JAMA. 2007; 297:1354-1361
Abscess Higher in Hospital Mortality

Postop Hospital Course
Operative Findings:
•Large abscess at right and left coronary cusps
•Large annular defects from debridement
•Regent Mechanical AVR (21 mm)

Aortic valve bioprosthesis severely deteriorated and right coronary leaflet was destroyed
Hospital Course
•Post-op course was complicated by shock and vasoplegia
•Worsening neurological status and imaging evidence of new posterior MCA stroke
•Blood cultures became positive for Candida Tropicalis
•Two weeks post-op he continued to have poor recovery and the family decided to
transition to comfort care measures. Autopsy was declined.

Conclusions
•Prosthetic valve endocarditis has high mortality
•Management of prosthetic valve endocarditis is challenging
•Multi-disciplinary heart team approach is critical
•Timing of surgery can be challenging
•Echocardiography is the initial imaging modality
•Advanced imaging modalities such as 18F-FDG PET/CT can help guide teams
in clinical decision making

William Osler in 1885 Gulstonian Lectures:
“Few Diseases present greater difficulties in the
way of diagnosis than malignant endocarditis,
difficulties which in many cases are
insurmountable.”

Acknowledgements
BWH Cardiovascular Division
•Sharmila Dorbala, M.D.,M.P.H
•Matthew Steinhauser, M.D.
•Patrycja Galazka, M.D.
•Donna Polk, M.D., M.P.H
•Jose Rivero, M.D.
•BWH Cardiovascular Co-fellows
ACC FIT Committee
•Akhil Narang, M.D.
•Shashank Sinha, M.D.
•Kristin West


FDG PET/CT Increases Sensitivity of Modified Duke Criteria in Diagnosis of PVE
Saby et al. JACC. 2013
P=0.008NPV100%

Proposed Approach to Diagnosis of PVE
Saby et al. JACC. 2013

18 FDG-PET/CT Improves the Diagnostic Accuracy of the
Modified DC in Patients with suspected IE,
Prosthetic Valves, and Cardiac Devices
Pizzi et al.
Circulation
2015

PET Reclassified 90% of Patients with Possible IE
Pizzi et al. Circulation 2015

1.PET/CT detected 14 (15%) cases of peripheral embolism
2. PET/CT provided alternative diagnosis in 54% of IE negative cases
3. PET/CT detected 6 unsuspected neoplastic lesions
Additional Benefits of Whole Body FDG/PET CT
Pizzi et al. Circulation 2015

What Do We Look for on Imaging?
Feature Tips Best Modality
Vegetation Independent Motion from the valve
Sensitivity:TTE: ~75%TEE: >90%CTA: ~85-90%
Perivalvular Abscess More Common in AorticProsthetic Valves; Small Anterior Abscess May be Better Seen with TTE
TTE: ~50%TEE: ~90%PET CTA in Prosthetic Valves
Pseudoaneurysm/Fistula
Cavity/Communicates with CV Lumen
CTA>TEE>TEE
Valve Dehiscence in Prosthetic Valves
Perivalvular Regurgitation/ +/-Rocking Motion of the Valve
TEE>TTE>CTA

Differences between 2014 AHA/ACC Guidelines
and AHA Scientific Statement
2014 AHA/ACC ValvularGuidelines-IE Portion
• Led by Cardiologists
• In addition to TTE/TEE recommends CT as a Class IIarecommendation…when anatomy cannot be clearly delinated by echocardiography
• Led by Infectious Disease
Physicians
• Mostly mentions echo as a
diagnostic modality
AHA Scientific Statement

Diagnostic Imaging Approach
AHA/ACC 2014 Valvular Guidelines

Diagnostic Imaging Approach
AHA Scientific Statement
Larry M. Baddour et al. Circulation. 2015;132:1435-1486
“The use of multimodality imaging in IE may increase in the
future as the risks and benefits of each diagnostic tool is defined”

ESC Infective Endocarditis Guidelines Boost Role of
Imaging in Diagnosis of IE

ESC: Imaging Major Criteria for
Diagnosing Endocarditis
Echocardiogram- Positive for IE
18 FDG PET/CT-Abnormal activity around the site of
prosthetic valve implantation detected by (only if
prosthesis was implanted >3 months) or radiolabeled
leukocytes SPECT/CT
Cardiac CT -Definite paravalvular lesion