subarachnoid hemorrhage diagnosis-what to do j. stephen huff, md fourth-year student elective...
DESCRIPTION
Objectives Rule out SAH without performing an LP every time!TRANSCRIPT

Subarachnoid hemorrhage
diagnosis-what to do
J. Stephen Huff, MD
Fourth-Year student elective director
Professor of Emergency Medicine and Neurology
University of Virginia
Virginia College of Emergency PhysiciansHot Springs, Virginia 2016
Corey Heitz, MDDirector, Undergraduate
Medical Education
Assistant Professor of Emergency MedicineVirginia Tech Carilion

Disclosures
none

Objectives
Rule out SAH without performing an LP every time!

What are we looking for?
Aneursymal SAH
or
Non-aneurysmal SAH

Aneurysmal SAH
High morbidity and mortality
Possibility of “sentinel bleeding”

Non-aneurysmal SAH
Aka perimesencephalic SAH
Usually venous
Minimal long term effects

Point #1:
We aren’t just looking for blood, we are looking for aneurysmal bleeding

Testing algorithm
POSITIVE: NO LP
NEGATIVE, LP POSITIVE
NEGATIVE, LP NEGATIVE
CT
CT
CT
angio
angio
done
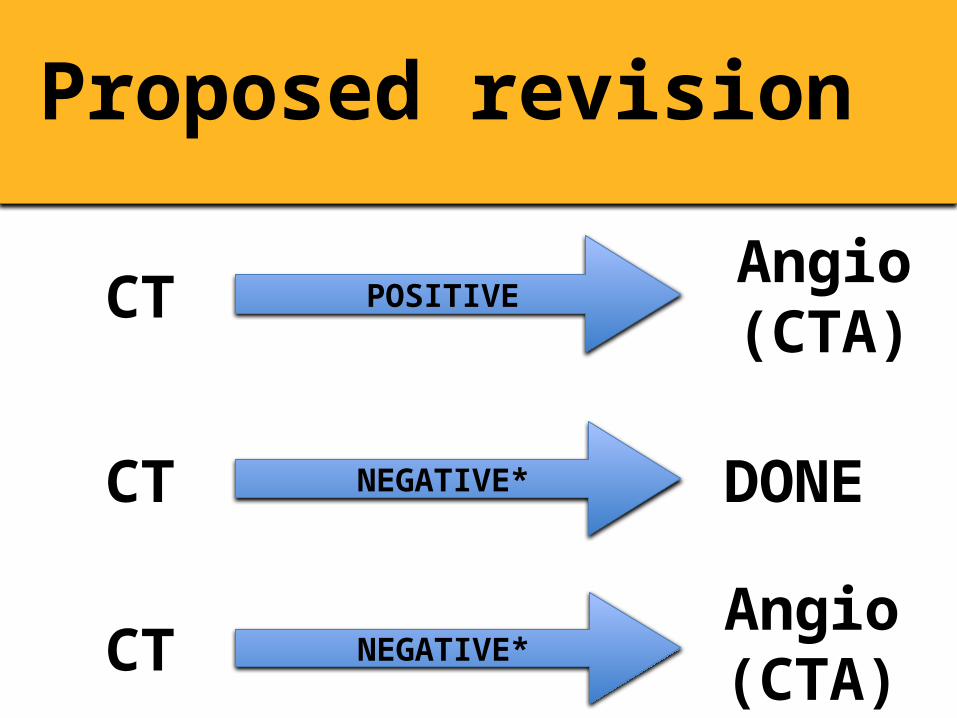
Proposed revision
POSITIVE
NEGATIVE*
NEGATIVE*
CT
CT
CT
Angio (CTA)
DONE
Angio (CTA)

Let’s talk about LP
Invasive
Sometimes painful
Complications
Doesn’t diagnose aneurysm!
But if it’s a good test…
2 true positives in 302 patients
~1 in 200 after negative head CT

Risk/Benefit
NND: 150-200
NNH: 10-20

Point #2:
LPs are low yield, high adverse effects
But is CT good enough?
Perry et al 2011:953 patients CTed within 6 hours:
all SAHs diagnosed
Backes et al 2012: validated sens/spec of 100%

But is CT good enough?
Dubosh 20168907 patients13 missed SAH on CT1.46 per 1000 CTs
LR- for CT: 0.010 (0.003-0.034)
NND for LP: 700

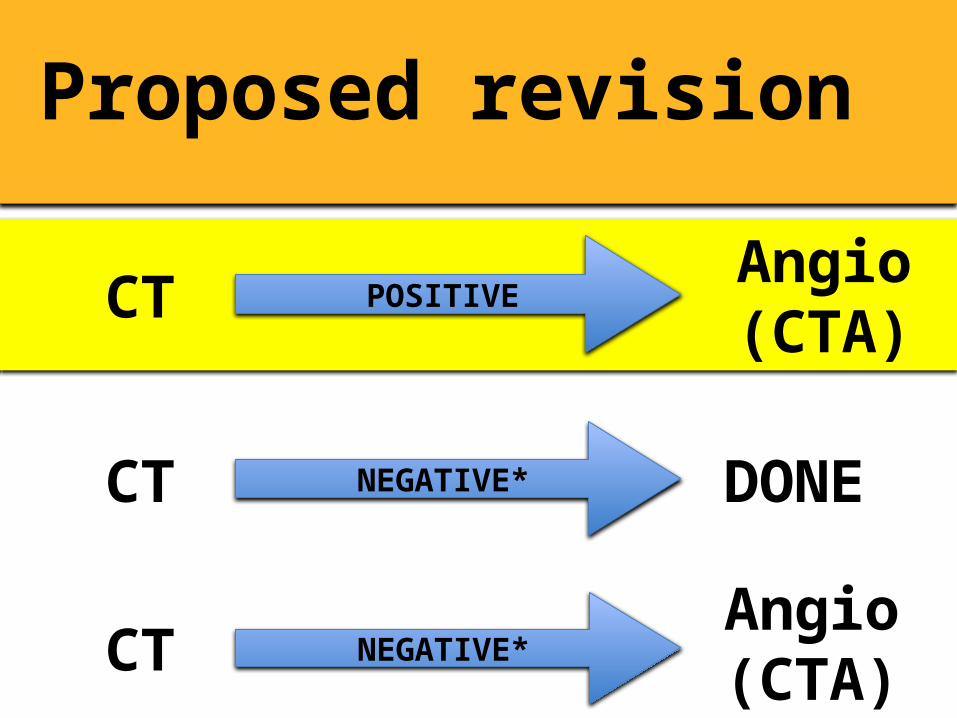
Proposed revision
POSITIVE
NEGATIVE*
NEGATIVE*
CT
CT
CT
Angio (CTA)
DONE
Angio (CTA)
Proposed revision
POSITIVE
NEGATIVE*
NEGATIVE*
CT
CT
CT
Angio (CTA)
DONE
Angio (CTA)

Proposed revision
POSITIVE
NEGATIVE*
NEGATIVE*
CT
CT
CT
Angio (CTA)
DONE
Angio (CTA)

Proposed revision
POSITIVE
NEGATIVE*
NEGATIVE*
CT
CT
CT
Angio (CTA)
DONE
Angio (CTA)

Summary
LPs are low yield and fair # of complications
CT within 6 hours is excellent
Positives go to angio anyway
700 LPs to diagnose 1 missed bleed? Insane