suicide and the teenage brain: which prevention ... · pdf filewhy a mental health academic...
TRANSCRIPT

Matt Byerly, M.D.Director, Center for Mental Health Research and RecoveryProfessor, Department of Cell Biology and Neuroscience
Montana State University
Suicide and the Teenage Brain: Which Prevention Interventions are Most Promising?

Why a Mental Health Academic Center in Montana
• 3rd highest suicide rate in the country
– Highest in recent prior years and top 4 for 30 years
• Limited number of mental health clinicians, especially in frontier settings
• Populations with especially high mental health risks
– Multiple Native American Nations
– 2nd highest per-capita Veteran population in U.S.
2

Center MissionSaving Lives and Helping Families
Through Science
• Conduct research to identify what works (or works better) for mental health prevention, diagnosis, and treatment in Montana and similar rural settings
• Support implementation of advances as they are identified

Vision of the Center
“…partnering with the world’s preeminent mental health scientists to advance
innovation and discovery related to mental health prevention, diagnosis, and
treatment.”

Collaborating with World Leaders
• Suicide Prevention (Danuta Wasserman, M.D.)– Director, WHO Collaborating Centre for Research, Methods
Development and Training in Suicide Prevention
• Computerized diagnosis/treatment (John Greist, M.D.)*– “Father” of computerized mental health diagnosis/treatment – Professor Emeritus, Univ. of Wisconsin School of Medicine
• Alzheimer's (Soo Borson, M.D.)*– National leader in Alzheimer’s clinical research– Professor Emerita, University of W School of Medicine
• Biomarker’s (Madhukar Trivedi, M.D.)– National leader mental health biomarker research
*New Affiliate Faculty Members of MSU CMHRR/Dept CBN5

CMHRR MembersFaculty Members• Sandra Bailey, Ph.D., MSU Extension
• Matt Byerly, M.D., Director, CMHRR, MSU Cell Biology and Neuroscience
• Frances Lefcort, Ph.D., MSU Cell Biology and Neuroscience
• Janet Lindow, Ph.D., MSU Cell Biology and Neuroscience
• Mark Schure, Ph.D., MSU Health & Human Development
Key Collaborators and Associates• Bill Bryan, Ph.D., founder and Executive Director of One Montana
• Jason DeShaw, B.A., musician and mental health advocate
• Paul Gatzemeier, B.E., Executive Director of Horses Spirits Healing, Inc
• Matt Kuntz, J.D., Executive Director of National Alliance on Mental Illness
• Gary Popiel, B.S., President of the National Alliance for Mental Illness-MT
• John Rush, M.D., Professor Emeritus, Duke-National University of Singapore
• Emily Matt Salois, MSW, ACSW, MSU INBRE Community Engagement Core
• Western Montana Mental Health Center, mental health services provider in MT
• Sara Young, M.Ed., MT INBRE Director of Tribal Health and Tribal College Programs

CMHRR Administrative Team
• Elizabeth Bannister, B.A., Managing Director
• Theresa Marchwick, B.S., Business Manager
• Kiara Baker, Admin Assistant

Areas of Focus and Related Initial Efforts
• Resiliency
– Testing the two most promising resiliency interventions
• Youth Aware of Mental Health or “YAM”
• Good Behavior Game in Native American youth
• Precision Diagnosis and Treatment
– “Biomarker” research to make diagnosing more objective and treatment more precise
• Access to Proven Treatments
– Online therapy for depression in rural communities
– Supporting development of a mental health workforce
• Mental health specialty focus within MSU Extension8

Computerized Cognitive Behavior Therapy for Depression/Wellness:
CMHRR Efforts in Montana

Web-Based Cognitive Behavioral Therapy Intervention for the
Prevention of Suicidal Ideation in Medical Interns: A Randomized
Clinical Trial
10
Guille et al. JAMA Psychiatry. 2015

Suicidal Thoughts over 12 Months
12
21
0
5
10
15
20
25
30
35
40
cCBT Control
Cas
es
P<0.03*
11Guille et al. JAMA Psychiatry. 2015

Computerized CBT programs(Mark Schure, Ph.D.)
• Computerized versions of CBT first developed in the 1980s
• The Thrive program is one of the most sophisticated versions to date, using:
– Personal assessments
– Videos to educate/engage users
– Personalized feedback on progress
• Uncontrolled trials among 297 patients found average reduction of 39% in depression severity scores
• Large RCT underway in Kaiser system
Next Steps for Thrive in Montana
• Cultural adaptation for rural America nearly completed in Montana
• Randomized controlled trial in Montana starting in the fall

Thrive Clips

Additional Current Projects
• Collaborating with Billings Clinic on 2 Alzheimer’s projects in Glendive and Lewistown
• Addressing mental health stigma in youth
• Improving medication adherence in schizophrenia
• Testing equine assisted horse therapy in veterans
• Collaborating with SiteOne Therapeutics to develop a non-opioid pain medication
• Identifying biomarkers of response to specific antidepressant medications

Building Mental Health Resilience
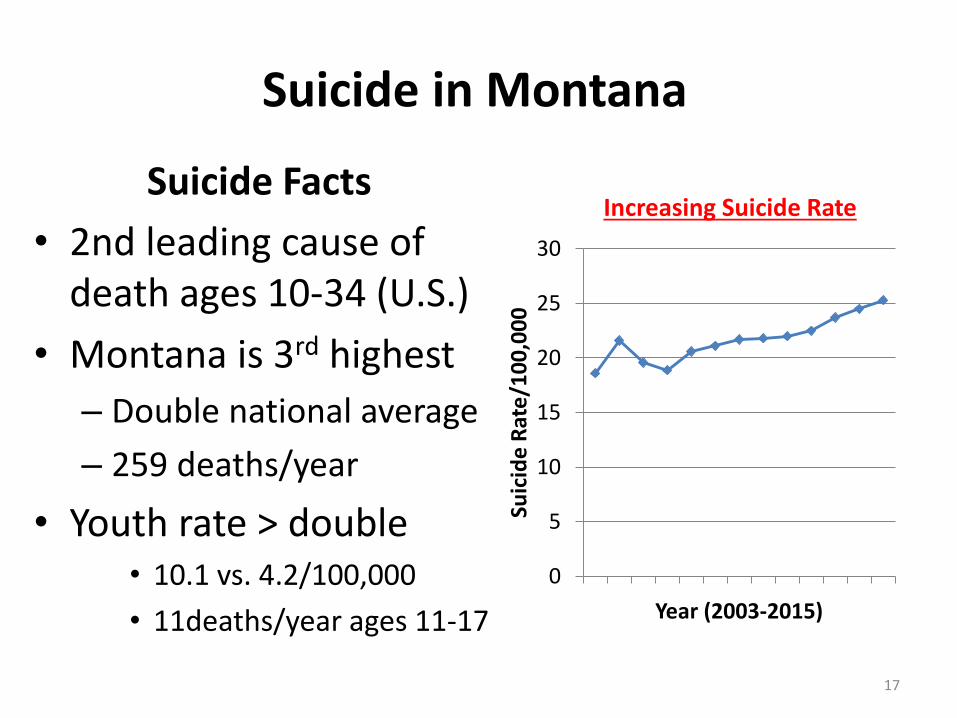
Suicide in Montana
Suicide Facts
• 2nd leading cause of death ages 10-34 (U.S.)
• Montana is 3rd highest
– Double national average
– 259 deaths/year
• Youth rate > double• 10.1 vs. 4.2/100,000
• 11deaths/year ages 11-17
Increasing Suicide Rate
0
5
10
15
20
25
30
Suic
ide
Rat
e/1
00
,00
0
Year (2003-2015)
17

Reducing Suicide: Challenges
• Screening: U.S. Preventive Services Task Force states “insufficient evidence” for screening
• Prevention: No mental health resilience/ suicide prevention interventions meet “gold standard” evidence for effectiveness
• Treatment: There ARE proven treatments for depression and suicidality (once they occur), but Montana has limited mental health workforce to provide these

Getting Off Track When Implementing Practices that are
NOT Based on Evidence from RCT’s

Gabapentin in the acute treatment of refractory bipolar disorder
• Open-label study of 28 participants
• CONCLUSIONS:– “Gabapentin appears to have acute anti-manic
and anti-depressant properties as an adjunctive agent for refractory bipolar illness. Prospective double-blind studies are needed to further delineate its acute efficacy when used as monotherapy and its prophylactic efficacy as monotherapy or in conjuction with other mood stabilizers.”
Altshuler. Bipolar Disord, 1999.

Randomized Controlled Trial of Gabapentin in Bipolar Mania
• Results: Both treatment groups had a decrease in total YMRS from baseline to endpoint, but this decrease was significantly greater in the placebo group (−9) than the gabapentin group (−6) (p<0.05)
Pande. Bipolar Disorders, 2000

RCT’s of Suicide Prevention Interventions that Evaluated Suicide Attempts and/or Suicidal Thoughts
Intervention Reductions in Suicide Attempts/Thoughts (vs. Control) in Gold-Standard RCT Studies
Notes
YAM 54% / 45%• YAM may have broader effects (e.g., for
depression)
• Delivered to 9th graders• 36 hours of facilitator
training/5 hrs with students• Published in The Lancet
SOS (3 studies) 33%, 33%, 64% / 0%, 0%, 0% • Delivered to mostly 9th
graders • 4-10 hours teacher
train/prep/1-3 hrs with students
GBG 50% / 40% • Lifetime risk assessed at young adulthood• Broader impact on mental health service use,
alc/drug misuse, antisocial PD
• Delivered to 1st and 2nd
graders• 40 hours teacher training +
considerable follow-up• Daily, class environment
Professional Screening (within schools)
41% / 26% (NS) • Delivered to 9th graders • Mental health
diagnosticians/ treaters needed

Intervention Reductions in Suicide Attempts/Thoughts (vs. Control) in Gold-Standard RCT Studies
Notes
Online CBT ?/ 43% • Delivered to Medical Interns• 4 hours of participation• Published in JAMA Psychiatry
Sources of Strength
?/ 15% (NS)• NIMH and Australian RCT’s ongoing
• High school peer leaders• Adult mentoring • Designed to increase positive
coping norms and practices, help-seeking and increase youth-adult connections.
Selective Identify-Refer (“Gatekeeper”) Interventions (4 Negative Studies)QPR (2 studies)
23% / 6% (NS)
2nd RCT of QPR found no difference in staff querying of students about suicide
• Delivered to 8th & 10th graders • 1 hr gatekeeper training
MHFA • No impact in single study evaluating suicidality outcomes (in adults)
• Uncontrolled trial in 15-17 year-old students had positive impact on several outcomes, but “too few” helping events to see difference vs. control
• Single negative RCT in adults• No evidence yet of reducing
suicidality in teen version• 8 hours of gatekeeper training
RCT’s of Suicide Prevention Interventions that Evaluated Suicide Attempts and/or Suicidal Thoughts

Why?
Universal interventions (YAM, GBG) appear to have greater impact than selective/gatekeeper
interventions (QPR, MHFA)

Challenges of Selective Identify-Refer (“Gatekeeper”) Interventions
• 80% of youth with a recent suicide attempt said they would not talk to a counselor or other adultif they needed help1
– Most thought there was not an adult at school who could help them
• Less than 25% of youth referred to care make it to care2
• This means an estimated 5% of suicidal youth may make it to care with gatekeeper interventions
25
1Wyman et al., J Consult Clin Psychol. 2008; 2Personal communication, D. Wasserman, 2015.

Universal Interventions: Deliver to All Youth

27
• Culturally sensitive universal intervention program that is driven by youth
www.y-a-m.org

YAM Elements• Delivered by “outside” facilitators• 28-page booklet for students
– Awareness of Mental Health and Health Risk Behaviors – Self-Help Advice– Stress and Crisis– Depression and Suicidal Thoughts– Helping a Troubled Friend– Getting Advice – Who to Contact
• Six educational posters displayed in the classroom• Two, 1-hour interactive discussion sessions• 3 hours of role-play
– Dilemmas/Choices– Crises/Stress– Depression/Suicidal thoughts Wasserman et al, Lancet 2015
28

Role Play• Dilemmas Examples:
– “For a while now, you have been checking out someone you think is hot….Just when you approach the person to say “hi”, one of their friends starts laughing hysterically pointing at your zipper that is open.” This is how you feel. This is what you’d do.
– “….It’s getting late and you are going home. You realize that your friend’s sister who is driving you is drunk.” This is how you feel. This is what you’d do.
• Role play examples:
– Bullying, social media problems, how to help a troubled friend, depression and suicidal thoughts

Fewer Suicide Attempts over 1 Year
14
2022
34
0
5
10
15
20
25
30
35
40
YAM ProfScreen QPR Control
Cas
es
P<0.229
Wasserman et al, Lancet 2015
P<0.014*
Approx. 2,200 per group
P<0.158
30
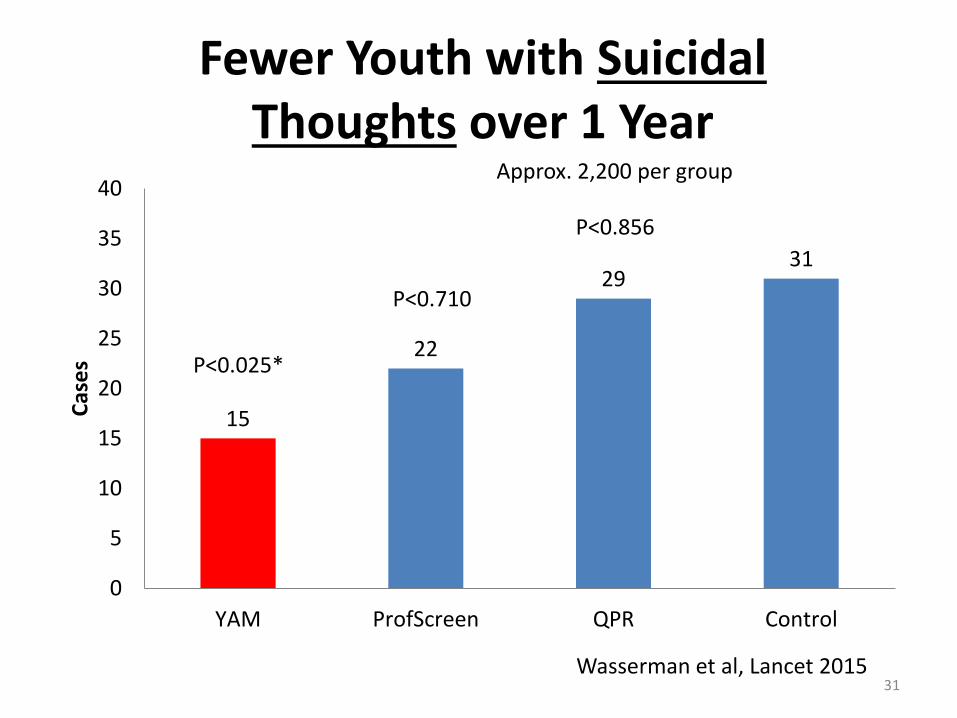
Fewer Youth with Suicidal Thoughts over 1 Year
15
22
2931
0
5
10
15
20
25
30
35
40
YAM ProfScreen QPR Control
Cas
es
P<0.856
Wasserman et al, Lancet 2015
P<0.025*
Approx. 2,200 per group
P<0.710
31

Additional Positive YAM Outcomes
• 30% reduction in new cases of depression
• YAM had the greatest cost-effectiveness of the 3 interventions (lowest cost per quality of adjusted life year gained)
Wasserman, Psychiatr Pol, 2016

Montana YAM Efforts
• First collaborative group in the US to test YAM (Montana-Texas)
• Cultural adaptations led by Montana group
• NIMH Grant in preparation for gold standard test (RCT) of YAM in Montana and Texas
• Plan to adapt and test a young adult version
Montana Schools in Pilot Study of YAM
• Browning
• Gardiner, Helena
• Capital HS
• Helena HS
• Lodge Grass
• Miles City
• Pryor
• Terry

Preliminary Results of Montana-Texas Pilot YAM Study (All Montana)
• Significant improvement in 2 of 4 help seeking actual behaviors:
– talking with teacher/school staff about
• a) what to do when one is depressed, and
• b) what to do when someone has suicidal thoughts.
– Strong trend (p=0.07 [p≤0.05 considered significant]) towards improvement on a third of the 4 individual help seeking actual behaviors:
• talking with your friends about depression.
• Significant improvement in mental health literacy

Preliminary Results of Montana-Texas Pilot YAM Study
(General and Native American Populations)
General Population (N=approx. 350)• Significant improvement in 3 of 4 help seeking actual behaviors• Significant (and greater) improvement in mental health literacy• Significant improvement in knowledge/perception of resources:
– I believe I know where to turn, should I ever experience mental health problems
– I know the name of the staff member at school who is the person to first seek help from for a student with a mental health problem
– There is an adult at school I could talk to if I had a personal problem
• Trend (p=0.09) towards improved coping skillsNative American Population (N=84)• Trend (p=0.07) towards reduced anxiety symptoms (effect size 0.22)

Preliminary Results of Montana-Texas Pilot YAM Study (Texas)
• Significant reduction in depression and anxiety symptoms at a clinically relevant magnitude (effect size 0.32 and 0.3, respectively)
• Awaiting results on other outcomes

Differences in Texas & Montana Models
Texas Model
• Centralized group with “expert” leader & 3 facilitators
• Delivery of many classes/facilitator (36)
• Enhanced fidelity approaches
Montana Model
• Decentralized structure, with 10 facilitators
• Few classes/facilitator (7)
• Limited fidelity approaches

Collaborative YAM Grants between Extension Service and CMHRR:
• Sandra Bailey, Ph.D. leading Extension
• Bill Bryan, Ph.D. of One Montana is key collaborator
• $362,000 grant from USDA
• $92,000 from the Montana Mental Health Trust
• Training of 17 Extension faculty and evaluation of YAM delivery in 17 counties

YAM Extension Faculty/Counties

What Will It Cost to Reduce Suicide in Montana/the US?
• Sufficient spending on effective programs
• Note, no public health programs with gold-standard evidence of effectiveness to date
• YAM
– $57-137 per student
– $628k-1.5 million/year for 1 (11,000 student) grade
• $12,500/year per US public school student1
• $7,300/year per Montana public student2
1National Center for Education Statistics2Montana OPI