suicide in australia – key facts - squarespace · immigration detention at risk groups of young...
TRANSCRIPT
Suicide in Australia – Key Facts 1. Suicide data is poor, limited and often unavailable. The official number of
suicide deaths reported is generally some 20-30% below the actual number.
2. One-quarter of the Australian population are poorly informed about suicide
3. Between 2004 and 2014, there has been a 22% increase in the number of suicide deaths in Australia
4. Suicide is the leading cause of death for both adult males and females aged 15-44 years and a major cause for males 45-54 years and over 75 years.
5. Between 8 and 10 Australians die by suicide everyday and there is an estimated 180 people who attempt suicide, with nearly half hospitalised.
6. In 2014, suicide accounted for 97,066 years of potential life lost – this is the highest of all causes of death and nearly 3.3 times the number of years of potential life lost to breast cancer.
7. Long term unemployment increases the risk of suicide, and poor precarious employment can contribute to poorer psychological health than no employment at all
8. HIV/AIDS received $2.9 billion in federal funding in 2013, and the death rate between 2003 and 2013 from AIDS fell 53.2 percent; the equivalent numbers for heart disease are $1.2 billion and 29.1 percent; for prostate cancer, the figures are $266 million and 13.7 percent. Suicide prevention received $37 million in 2013, and the death rate rose by 20.4 percent in the decade to 2013.
9. Intentional self-harm is the leading cause of death for those aged 10-24.
© ConNetica
May 2016
Suicide in Australia – Key Facts
CONNETICA May 2016 2 of 12
1. Suicide in Australia This document provides a brief overview of suicide and suicide prevention in Australia. Suicide is now a major public health issue with more years of potential life lost to suicide than any other cause of death. Yet the Australian public is poorly informed about suicide. We are one of the few developed countries not to ever have had a public suicide prevention education campaign.
A significant segment of the community is unable to talk about suicide or suicidality and cannot read-the-signs of someone who is suicidal and trying to communicate their sense of hopelessness. This is unlike the publics’ awareness of almost every other major cause of premature death.
What is suicide and suicidal behaviour?
• Suicide is defined as the intentional taking of one’s own life.
• Suicidal behaviour is a broader term and includes self-inflicted and potentially injurious behaviours, and includes: suicidal ideation (serious thoughts about taking one’s life), suicide plans, suicide attempts and completed suicide.
• People who experience suicidal ideation and make suicide plans are at increased risk of suicide attempts, and people who experience all forms of suicidal thoughts and behaviours are at greater risk of completed suicide.
How many Australians are affected by suicide?
• Officially, the statistics record approximately 2,400-2,800 suicide deaths per annum over the past five years, with nearly 80 percent being males.
• Between 2004-14, there has been a 22% increase in the number of suicide deaths in Australia.
• Suicide is the leading cause of death for both adult males and females aged under the age of 44 years and is a notable cause of death in males over 75 years. Between eight-ten Australians die by suicide EVERYDAY and there is an estimated 180 people who attempt suicide EVERYDAY, half of whom require hospitalisation as a result.
• Deaths due to suicide significantly exceed fatalities from motor vehicle accidents (by 250%).
• Suicide is implicated in many poisonings, falls and motor vehicle accidents. It is generally accepted that the actual number of deaths is 20-30% higher than the official numbers. If this is applied to 2014, it equates to 3,437-3,723 deaths at an average age of just 44 years.
• Suicide deaths have profound effects on families, friends, workplaces and whole communities. It is estimated that for every suicide, 6 people are deeply affected and thirty more affected. Over a 10-year period, nearly a million Australians will be impacted.
• Suicide or an attempt can cause not only immense distress to individuals, but also vicarious trauma among the wider community (e.g. individuals in workplaces often witness/experience the impact of a suicide and are typically left at a loss, asking themselves how to help, why they didn’t see the warning signs, what they could have done/said to prevent the tragedy. Those close to the person who has died will often blame themselves for the decision of the individual to take their own life. The combination of grief, guilt and remorse often remains for years.
• The impact of a suicide or suicide attempt on first responders, such as police, ambulance and fire brigade, should also not be underestimated. The responses to suicide are further complicated by community stigma and perceptions of the act of suicide as a failure on the part of either the deceased (to cope) or the family (for not having intervened or prevented the suicide).

Suicide in Australia – Key Facts
CONNETICA May 2016 3 of 12
Why do people suicide?
• The causes of suicide are complex and vary among individuals and across age, cultural, racial and ethnic groups.
• Suicide risk is influenced by an array of factors – sociological, psychological, environmental, cultural and biological. Nonetheless, this complexity masks the reality that almost all people who attempt or complete suicide had one or more warnings signs before their death.
What about suicide among Aboriginal and Torres Strait Islanders?
• The rate of suicide among Aboriginal and Torres Strait Islanders Australians is double that of non-indigenous Australians. In some remote areas it is many times higher. Suicide caused nearly one in three deaths (29 per cent) of Indigenous Australians aged between 15 and 34 and was the leading cause of death in this age group between 2008 and 2012. In 2014, suicide accounted for 5.2% of all indigenous deaths compared to 1.8% for non-indigenous people. Aboriginal and Torres Strait Islander people are almost twice as likely to die by suicide than non-indigenous people.
• In rural and remote Indigenous areas, suicide deaths often spark clusters of suicides. Suicide deaths, particularly by hanging, are frequently witnessed by many members of an Indigenous community.
• These situations can often lead to the mounting problem of intergenerational transmissions of trauma and grief, and may result in the overuse of drugs and alcohol, incarceration, self-harm, seemingly reckless self-destructive behaviours and, in some cases, suicide.
• Over the past 30 years Indigenous suicide has increased, with young Indigenous males being the most at risk. Young Aboriginal Torres Strait Islander males (15-19 years) are 4.4 times more likely to die by suicide than are other young Australian males. Similarly, young Aboriginal Torres
65,000-70,000
Suicide in Australia – Key Facts
CONNETICA May 2016 4 of 12
Strait Islander females (15-19 years) are 5.9 times more likely to die by suicide than are other young females.
• Despite the years of rhetoric, there has been little data collected on suicide prevention efforts for Indigenous Australians with most programs too small and too short to have any chance of affecting change.
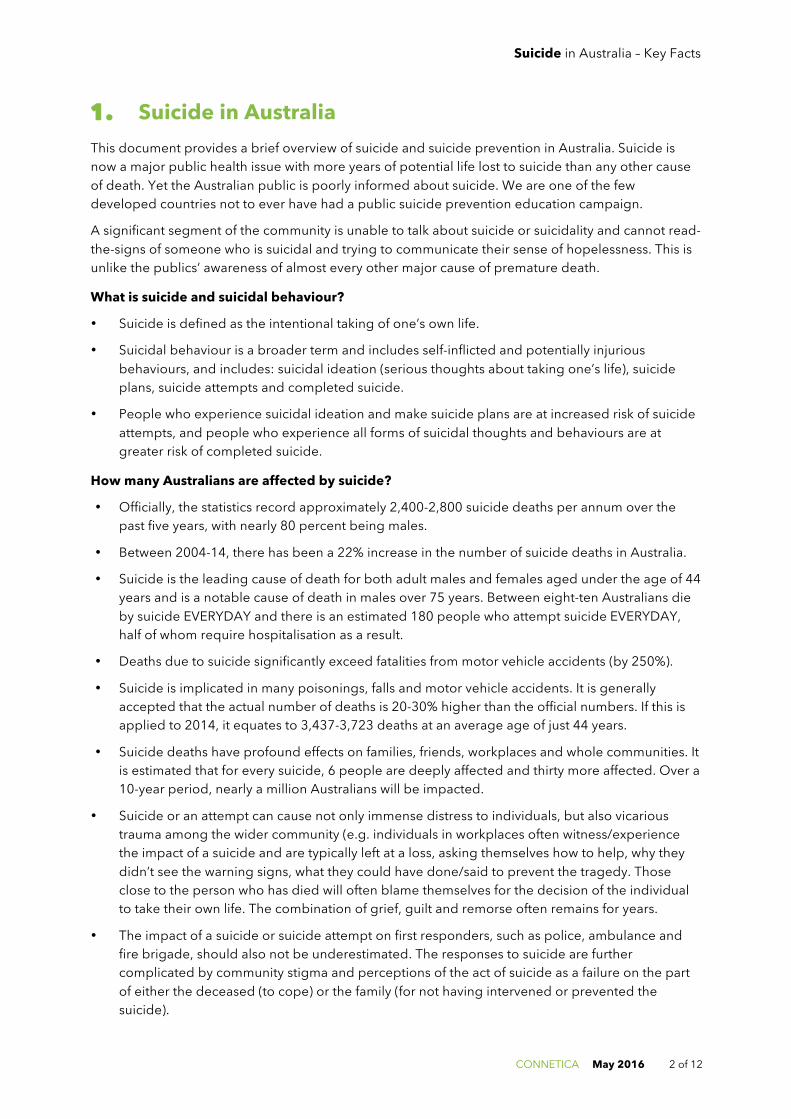
In the above graph, note the very significant increases in falls and poisonings in the past decade and that trajectory following that of deaths due to intentional self-harm (suicides).
What is the economic and personal impact?
• Suicide and suicidal behaviour both bear substantial human, social and economic costs. Presently there are no detailed studies on the cost of suicide and self-harm to the Australian community.
• One estimate of the financial cost to Australia as a result of suicide and suicidal behaviour has been calculated at $17.5B (in 2009). This is approximately 1.5% of Gross Domestic Product (GDP), or $795 per person, per year.
• On the other hand, our investment in suicide prevention through the Federal Government is less than $3.50 per person per year.

Suicide in Australia – Key Facts
CONNETICA May 2016 5 of 12
2. Young People, Suicide and Self-Harm • Suicide and self-harm is a predominant issue among young people.
• Deliberate self-harm can be defined as ‘an act with a non-fatal outcome in which an individual deliberately did one or more of the following: initiated behaviour (for example, self cutting, jumping from a height), which they intended to cause self harm; ingested a substance in excess of the prescribed or generally recognised therapeutic dose; ingested a recreational or illicit drug that was an act that the person regarded as self harm; or ingested a non-ingestible substance or object’.
• ABS data shows that intentional self harm is the leading cause of death for young people aged 15-24 (see below figure).
0
200
400
600
800
NSW VIC QLD SA WA TAS NT ACT
Sucides location 2008-‐2012
15-‐24 25-‐34 35-‐44 45-‐54 55-‐64 65-‐74 75-‐84 85+
Suicide in Australia – Key Facts
CONNETICA May 2016 6 of 12
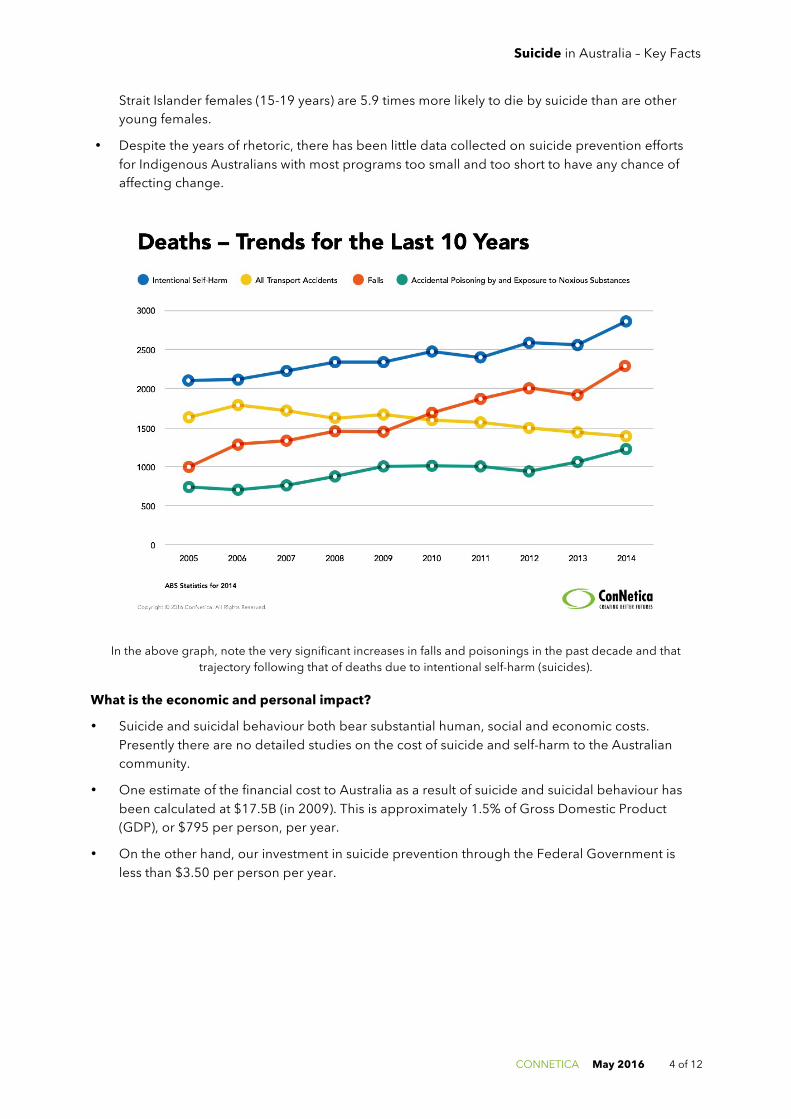
• There are numerous different ways a person can self-harm, more common of which include cutting or burning skin, hair plucking/pulling, skin picking, punching or hitting, using drugs and alcohol, and deliberate starvation.
• There are a range of causal factors associated with self-harm, most commonly self-harming behaviour is experienced by those who’ve experienced trauma (particularly childhood trauma), individuals who encounter social problems (including isolation, bullying or those coming to terms with sexuality and gender diversity) or experience low self-esteem, and people experiencing psychological distress (such as anxiety, personality disorders or psychosis).
• The reasons why someone self-harms is deeply personal, however research indicates that people who self-harm seek relief from distress and experience relief from distress following injurious behaviour, are seeking to punish themselves or to anti-dissociate (feel alive) and sensation-seeking (relief from feeling numb). The Australian National Epidemiological Study of Self-Injury (ANESSI) in 2010 found that the most common motivation for self-injury was to manage emotions (57.2%), followed by self-punishment (24.7%).
Copyright © 2016 ConNetica. All Rights Reserved.
In 2013-14 over 9000 young people were hospitalised due to self harm
9,000
1 in 10 young people have
engaged in self harming behaviour
Self Harm Amongst Australia’s Youth Orygen, The National Centre of Excellence in Youth Mental Health 2016
Hospitalisation rates for Women are Nearly
higher than Men
Aboriginal & Torres Strait
Islander PeopleLGBTIQ Women Rural & Remote Juvenile Justice
FacilitiesMental Illness Immigration Detention
At risk groups of young people
INDIGENOUS AUSTRALIANS aged 15-24 are 5 TIMES MORE likely to be hospitalised

Suicide in Australia – Key Facts
CONNETICA May 2016 7 of 12
3. The Journey Toward Suicide A number of submissions were made to the Senate Inquiry into Suicide in Australia in 2010. The majority of these stories were from people who had experienced the suicide of someone close to them – often within their families – and included those bereaved by suicide, survivors of suicide and those who experience suicidal ideation. While reflecting the intense pain, guilt, soul searching and aloneness associated with suicide loss, these stories also provide unique, poignant insights into the painful inner turmoil of the loved ones who suicide.
We believe 9 Key Themes require attention
1. Suicide can be prevented
A resounding theme in many stories from the bereaved was that they felt the suicide of a loved one could have been prevented. A haunting revelation made by some suicide attempters in their story was the common feeling that when they made a suicide attempt, they never really wanted to end their life, but rather take away the emotional pain that they were experiencing in that moment.
Imagine if every person who was going through such emotional turmoil had someone with whom they could talk about their options for working through their problems and decide together what could be done to ease their emotional pain, without having to end their life.
WE NEED TO BUILD THE CAPACITY AND CONFIDENCE OF AUSTRALIANS TO BE ABLE TO RECOGNISE AND RESPOND TO THIS VERY COMMON HUMAN NEED.
2. Shortage or deficiency of professional care for suicidal behaviour
Other stories from the bereaved expressed that a number of health agencies let them down. All too frequently, these stories recalled how their loved one was turned away from care, not provided with appropriate care or follow-up care, or that they were not informed or involved in the care planning of the suicidal loved one.
WE NEED TO ENSURE THAT EVERY PERSON WHO SEEKS HELP WHEN FACING A PERSONAL CRISIS RECEIVES NON-JUDGMENTAL, EVIDENCE INFORMED CARE AND CONTINUITY OF CARE TO ENABLE THEM TO RETURN TO GOOD
HEALTH. SURVEILLANCE SYSTEMS, THAT ASSIST MAINTAIN CONTINUITY OF CARE SHOULD BE TRIALED.
3. Rural and remote challenges
People who wrote about their experience with suicide and living in rural and remote areas expressed that often help is not available in the local town, forcing people to either travel to major centres, or wait for a scheduled time when relevant professionals travel to a town from a major centre. In some cases, this time may devastatingly be too late. Frustration was also expressed about long waiting lists, and often having no alternatives for the suicidal person’s care.
WE NEED TO ENSURE THAT NO MATTER WHERE YOU LIVE, YOU ARE ABLE TO ACCESS CARE. DIGITAL, TELEPHONE BASED AND FACE-TO-FACE SERVICES MUST BE NETWORK.
4. Misunderstanding and stigma associated with suicide
Experience of a fear of the unknown around suicide was reflected in many stories, and a resounding recommendation from those with suicide experience was that suicide awareness campaigns, and education around suicide needs to be provided to the Australian community; starting with our youth. Stories reflected that we have a duty of care to make it easier for future generations to discuss and address suicide, providing them with the tools to recognise, acknowledge, and prevent suicide.
WE NEED TO START TO TALK ABOUT SUICIDE. TALKING ABOUT SUICIDE DOES NOT CAUSE SUICIDE. WE CAN ALL CONTRIBUTE TO BREAKING DOWN THE STIGMA.

Suicide in Australia – Key Facts
CONNETICA May 2016 8 of 12
5. Mental illness and suicide
Many of the personal stories also discussed a link with diagnosed mental illness. In many other cases, it was clear that disabling mental health conditions were present but were unrecognised at the time. This was often recognised in retrospect by the bereaved. There was unmistakable evidence in these stories that mental health literacy in the community needs to be significantly improved to ensure people receive appropriate treatment but also to improve opportunities for saving lives. This improvement needs to be accompanied by improved access to mental health services.
Although mental illness is not always associated with suicidal ideation, the experiences of many individuals who were and are living with such illnesses was clearly apparent in many stories.
WE NEED TO CONTINUE TO EDUCATE THE AUSTRALIAN COMMUNITY ON MENTAL ILLNESSES AND WHAT THEY CAN DO EVERYDAY TO BE MORE MENTALLY HEALTHY
6. Major Life Events matter
Losing one’s job, being unemployment over extended periods, job insecurity, financial stress, intimate partner problems, death of close friends or family members, bullying or harassment, violence and abusive relationships, natural disasters – all of these ‘life events’ or circumstances can act as triggers for suicidal behavior.
This was particularly evident in the stories where the person’s own coping mechanisms and resources were becoming overwhelmed. Problem drinking and/or gambling – often over an extended period - were clearly associated with many of the suicide deaths. It featured as a contributing factor in a downward spiral of deteriorating relationships, employment difficulties and general despair, which exacerbated loneliness and alienated key supports.
What is remarkable is the resilience and sustained support offered by many significant others seeking to support people whose lives were affected by alcohol misuse. What is tragic is how little support many of these people received from services.
WE NEED TO BUILD THE RESILIENCE OF INDIVIDUALS AND COMMUNITIES FACING HARDSHIP OR MAJOR ECONOMIC CHANGES. WE NEED TO ENSURE OUR CHILDREN ARE EQUIPPED WITH THE COPING SKILLS FOR THE
UNCERTAINTIES OF THE 21ST CENTURY.
7. Lives changed forever - Family interventions after a suicide
It was evident from the stories told by the bereaved that having to rebuild their lives again was an overwhelming prospect; to carry on and regain some sense of normalcy without the loved one who has died by suicide. The reality is, that for many of these people, they will be haunted by losing a loved one to suicide every day for the rest of their lives, and all story writers’ were unified when they expressed that losing a loved one in this way should never happen.
A striking feature of these stories was how often those left behind had to cope with minimal informal or professional support. In some cases, where multiple suicides occurred in a family. We know that bereavement support works – it saves lives after the first suicide.
EVERY FAMILY, EVERY WORKPLACE, EVERY COMMUNITY AFFECTED BY SUICIDE MUST GET THE SUPPORT NEEDED TO BEST COPE WITH THE LOSS.
8. Responding to Suicide Risk
Constantly it was reported that hospital Emergency Department’s are ill-equipped and inappropriate environments to undertake suicide risk assessment. Despite years of efforts to improve this situation, the risks of being treated with disregard, disrespect and trivialised on presentation to a hospital ED remains high. Alternative settings for people experiencing a personal crisis and at risk of suicide are now commonplace in many developed countries. Australia, has almost no alternative setting to ED.

Suicide in Australia – Key Facts
CONNETICA May 2016 9 of 12
The reasons for the failure of clinicians in busy ED units or in under-resourced mental health wards are more to do with the context – the time available and the nature of the relationship between the persons involved.
However, the needs of communities as divisive as Broome or Balmain, require regionally relevant approaches. One sizes fits nobody.
WE NEED TO BUILD REGIONALLY RELEVANT AND INTEGRATED ALTERNATIVES TO ED FOR ASSESSMENT AND EARLY SUPPORT AND CARE FOR PEOPLE IN CRISIS OR AT RISK OF SUICIDE.
9. The Need for Answers and Action
Many of the stories spoke to the frustration with the lack of focus on mental health and suicide prevention, the lack of available effective therapies and services overwhelmed. Too often our suicide prevention efforts have been too small in scale, too short in duration and too poorly resourced to make any difference. Such examples clearly demonstrate the need for suicide prevention strategies to address risk at both the community and population levels, rather than just that of the individual.
WE NEED TO MOVE AWAY FROM A SCATTER-GUN APPROACH TO THE RECOMMENDATIONS OF THE NATIONAL MENTAL HEALTH COMMISSION AND ESTABLISH 12 LARGE REGIONAL TRIALS TO BUILD KNOWLEDGE AND
CAPACITY TO TURN THE TIDE ON SUICIDE AND SELF-HARM.
FOR MORE INFORMATION AND STATISTICS ABOUT SUICIDE IN AUSTRALIA, VISIT
http://www.mindframe-media.info/for-media/reporting-suicide/facts-and-stats

Suicide in Australia – Key Facts
CONNETICA May 2016 10 of 12
References/Sources Aguirre, R. T. P., McCoy, M. K., & Roan, M. 2013. Development Guidelines from a Study of Suicide Prevention Mobile Applications (Apps). Journal of Technology in Human Services, 31(3): 269–293. http://doi.org/10.1080/15228835.2013.814750.
Ahlfors, R. 2010. Many Sources, One Theme: Analysis of Cyberbullying Prevention and Intervention Websites. Journal of Social Sciences, 6(4): 515–522. http://doi.org/10.3844/jssp.2010.515.522
Australian Bureau of Statistics (2013). Causes of Death, Australia, 2011. Catalogue No. 3303.0. Belconnen, ACT: Commonwealth of Australia.
Australian Bureau of Statistics. (2016). Causes of Death, Australia, 2014. Catalogue No. 3303.0. Belconnen, ACT: Commonwealth of Australia.
Australian Institute of Health and Welfare, 2015. Australia's hospitals 2013–14: at a glance. Health services series no. 61. Cat. no. HSE 157, Australian Government, Canberra.
Behar, 1986. What are Wraparound Services? Butte County Network of Care for Behavioural Health.
Bradford, S., & Rickwood, D. 2012. Psychosocial assessments for young people: a systematic review examining acceptability, disclosure and engagement, and predictive utility. Adolescent Health, Medicine and Therapeutics, 3: 111–125. http://doi.org/10.2147/AHMT.S38442
Campbell, D. 2015. A&E staff attitudes to patients in mental health crisis ‘often shocking’. The Guardian, Friday 15 June 2015. http://www.theguardian.com/society/2015/jun/12/ae-staff-attitudes-to-patients-in-mental-health-crisis-often-shocking Chan, J. K., Farrer, L. M., Gulliver, A., Bennett, K., & Griffiths, K. M. 2016. University Students’ Views on the Perceived Benefits and Drawbacks of Seeking Help for Mental Health Problems on the Internet: A Qualitative Study. JMIR Human Factors, 3(1), e3. http://doi.org/10.2196/humanfactors.4765
Chapman R, Martin C, 2014. Perceptions of Australian emergency staff toward patients presenting with deliberate self-poisoning: a qualitative perspective. Int Emer Nurs 22, 140-145.
Coia D and Glassborow R, 2009. Mental health quality and outcome measurement and improvement in Scotland. Curr Opin Psychiatry, 22(6): 643-7.
Covington D. 2014. The Value of a Life: Zero Suicide in Healthcare. http://www.zerosuicide.org
Davis, Nicola, 2005. Integrated Pathways – A guide to good practice. National Leadership and Innovation Agency for Healthcare, Wales.
Gallan A and Shattell M, 2015. Patient Experience Measurement Ignores Mental Health: Suggestions for Healthcare Organisations. Issues in Mental Health Nursing, 36: 311-314.
Griffiths K, Mendoza J, Carron-Arthur B, 2015. Whereto mental health reform in Australia: is anyone listening to our independent auditors? MJA 202 (4) · 2 March 2015
Goldstein Grumet J and Hogan M. 2014. The emerging Zero Suicide Paradigm: reducing suicide for those in care. Presentation National Action Alliance for Suicide Prevention, 28 August 2014.
Ghoncheh, R., Gould, M. S., Twisk, J. W., Kerkhof, A. J., & Koot, H. M. 2016. Efficacy of Adolescent Suicide Prevention E-Learning Modules for Gatekeepers: A Randomized Controlled Trial. JMIR Mental Health, 3(1). http://doi.org/10.2196/mental.4614
Hawton, K., Rodham, K., Evans, E., & Weatherall, R. 2002. Deliberate self harm in adolescents: self report survey in schools in England. BMJ, 325(7374):1207–1211. http://doi.org/10.1136/bmj.325.7374.1207
Johnson, S. 2013. Alternatives to acute admission: what do we know?. Mental health Science Unit, University College London.
Klonsky, E. D. 2007. Non-suicidal self-injury: An introduction. Journal of Clinical Psychology, 63(11): 1039–1043. http://doi.org/10.1002/jclp.20411
Knesper, D. J., American Association of Suicidology, & Suicide Prevention Resource Center. 2010. Continuity of care for suicide prevention and research: Suicide attempts and suicide deaths subsequent to discharge from the emergency department or psychiatry inpatient unit. Newton, MA: Education Development Center, Inc.
Large MM and Ryan CJ, 2014. Suicide risk catergorisation of psychiatric inpatients: what it might mean and why it is of no use. Australian Psychiatry, May.
Lee G, Endacott R, Flett K et al., 2006. Characteristics of patients who did not wait for treatment in the emergency department: a follow up survey. Accident & Emergency Nursing 14; 56-62.
Lockett P, Mendoza J and Davenport T. 2015. Mid-term Review of the Northern Adelaide Local Health Network, Community Walk-in Service. Prepared for SA Health by Seaview Consulting & ConNetica Consulting (Unpublished).
Luxton, D. D., June, J. D., & Chalker, S. A. 2015. Mobile Health Technologies for Suicide Prevention: Feature Review and Recommendations for Use in Clinical Care. Current Treatment Options in Psychiatry, 2(4): 349–362. http://doi.org/10.1007/s40501-015-0057-2
Luxton D, June JD & Comtois KA, 2012 Can Postdischarge follow-up contacts prevent suicide and suicidal behaviour? A review of the literature. Crisis 34(1): 32-41.
Suicide in Australia – Key Facts
CONNETICA May 2016 11 of 12
Macarthur Foundation Network on Mental Health Policy Research, 2007. Development and process for the New Mexico Behavioural Health Local Collaboratives: Improvements, impediments and opportunities. http://www.bhc.state.nm.us/pdf/lc_final_report_oct_2007.pdf McPhedran, S and De Leo, D. 2013. Miseries suffered, unvoiced, unknown? Communication of suicideal intent by men in “rural” Queensland, Australia. Suicide & Life-Threatening Beh.
Madsen T and Nordentoft M 2012. Risk factors for inpatient suicide do not translate into meaningful risk categories. J Clin Psychiatry 73: 1034-35.
Martin, G., Swannell, S., Harrison, J., & Taylor, A. 2010. The Australian National Epidemiological Study of Self-Injury (ANESSI). Brisbane, Australia: Centre for Suicide Prevention Studies.
Mendoza J, Harvey S & Wands M, 2015. One System, One Team: Hospital Transitions Pathways Project – Final Report. Prepared for the Brisbane North Primary Health Network, Partners in Recovery Program. Caloundra, Qld. ConNetica
O’Connor, R. 2015. Presentation, Suicide Prevention Australia Conference, Hobart.
Philibert I and Barach P, 2012. The European HANDOVER Project: a multi-nation program to improve transitions at primary-care-inpatient interface. BMJ Quality & Safety 21: 1-6.
Rickwood, D. J., Mazzer, K. R., Telford, N. R., Parker, A. G., Tanti, C. J., & McGorry, P. D. 2015. Changes in psychological distress and psychosocial functioning in young people visiting headspace centres for mental health problems. Medical Journal of Australia, 202(10). Retrieved from https://www.mja.com.au/journal/2015/202/10/changes-psychological-distress-and-psychosocial-functioning-young-people
Robinson, J and Pirkis J. 2014. "Research priorities in suicide prevention: An examination of Australian-based research." Australian Health Review 38(1): 18-24
Ryan CJ and Large MM. 2013. Suicide risk assessment: where are we now? Med J of Aust; 198(9) 462-463.SANE Australia, 2014. Lessons for Life: New research finds Australians who have attempted suicide find it difficult to access the professional help they need to recover. https://www.sane.org/images/Media_Release_2014/10_December_2014_lessons_for_life2.pdf
Schiff LB, Holland KM, et al. 2015. Acute and chronic risk preceding suicidal crises among middle-aged men without known mental health and/or substance abuse problems. Crisis; 36(5): 304-15.
Shafiei T, Gaynor N and Farrell G, 2011. The characteristics, management and outcomes of people identified with mental health issues in an emergency department, Melbourne, Australia. J Psychiatric & Mental Health Nursing, 18(1); 9-16.
Shattell MM, et al., 2014. A recovery-oriented alternative to hospital emergency departments for persons in emotional distress: "the living room". Issues Ment Health Nurs.; 35(1):4-12
Shea SC. 2009. Suicide Assessment. Part 2: uncovering suicidal intent using the Chronological Assessment of Suicide Events (Case Approach). Psychiatric Times; 26(12) Dec 3, 2009
Shepperd S, Lannin NA, Clemson LM, et al, 2013. Discharge planning form hospital to home. Cochrane Database Systematic Review ; 1.
Sjølie H1, Karlsson B, Kim HS, 2010. Crisis resolution and home treatment: structure, process, and outcome - a literature review. J Psychiatr Ment Health Nurs.;17(10):881-92.
Skovgaard Larsen, J. L., Frandsen, H., & Erlangsen, A. 2016. MYPLAN – A Mobile Phone Application for Supporting People at Risk of Suicide. Crisis, 1–5. http://doi.org/10.1027/0227-5910/a000371
Spears, B. A., Kofoed, J., Bartolo, M. G., Palermiti, A., & Costabile, A. 2012. Positive uses of social networking sites: Youth voice perspectives. In A. Costabile & B. A. Spears (Eds.), The Impact of Technology on Relationships in Educational Settings. London: Routledge.
Stanley, B., & Brown, G. K. 2012. Safety planning intervention: a brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice, 19(2): 256–264.
Substance Abuse and Mental health Services Administration. 2014. Crisis services: effectiveness, cost-effectiveness and funding strategies. HHS Publication No. 14-4848. Rockville, MD.
Suicide Prevention Australia. 2010. Position Statement: Crisis Response and the Role of the Emergency Services and First Responders to Suicide and Suicide Attempts. Suicide Prevention Australia, Sydney.
Suicide Prevention Resource Center. 2013. Continuity of care for suicide prevention: The role of emergency departments. Waltham, MA: Education Development Center, Inc.
Suicide Prevention Resource Center. 2015. Caring for Adult Patients with Suicide Risk: A Consensus Guide for Emergency Departments. Waltham, MA: Education Development Center, Inc.
Tabol, C., Drebing, C. & Rosenheck, R, 2010. Studies of 'supported' and 'supportive' housing: a comprehensive review of model descriptions and measurement. Evaluation and Program Planning, 33, 446–456.
Van Veen M, et al., 2014. Structured assessment of suicide risk in a psychiatric emergency service: Psychometric evaluation of the Nurses’ Global Assessment of Suicide Risk scale (NGASR). Int J Soc Psych. 1-10.
Waring J, Marshall F and Bishop S, 2015. Understanding the occupational and organisational boundaries to safe hospital discharge. J of Health Services Research & Policy, Vol 20(sup 1); 35-44.

Suicide in Australia – Key Facts
CONNETICA May 2016 12 of 12
Willging et al., 2007. “We never used to do things this way”: Behavioral health care reform in New Mexico, Psychiatric Services,
58(12), 1529-1531.
While D, Bickley H, Roscoe A, Windfuhr K, Rahman S, Shaw J, Appleby L, Kapur N, 2012. Implementation of mental health service recommendations in England and Wales and suicide rats, 1997-2006: a cross-sectional and before and after observational study. Lancet; 379: 1005-1012.