summary of benefits and coverage: what this plan covers ... · work) 0% coinsurance not covered...
TRANSCRIPT
1 of 6
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 1/1/2020 – 12/31/2020
HMO HDHP Bronze 6900 Coverage for: Individual/Family | Plan Type: HMO
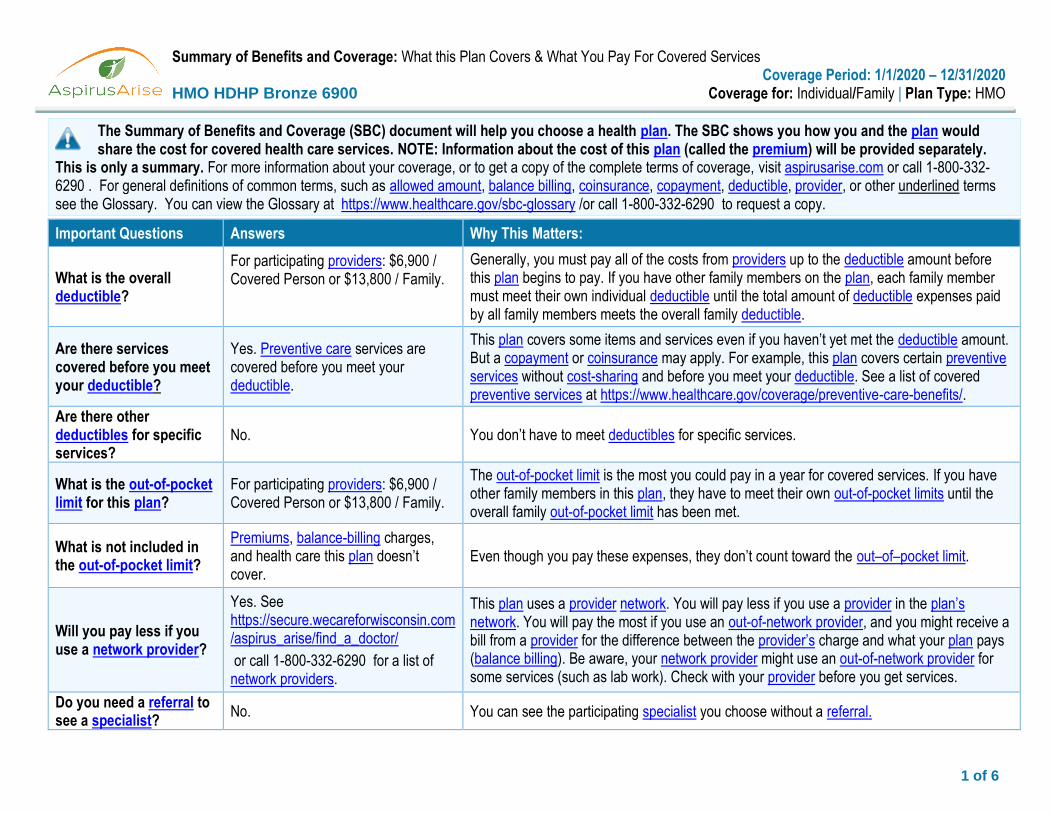
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit aspirusarise.com or call 1-800-332-6290 . For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at https://www.healthcare.gov/sbc-glossary /or call 1-800-332-6290 to request a copy.
Important Questions Answers Why This Matters:
What is the overall deductible?
For participating providers: $6,900 / Covered Person or $13,800 / Family.
Generally, you must pay all of the costs from providers up to the deductible amount before this plan begins to pay. If you have other family members on the plan, each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the overall family deductible.
Are there services covered before you meet your deductible?
Yes. Preventive care services are covered before you meet your deductible.
This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive services without cost-sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
Are there other deductibles for specific services?
No. You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
For participating providers: $6,900 / Covered Person or $13,800 / Family.
The out-of-pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
What is not included in the out-of-pocket limit?
Premiums, balance-billing charges, and health care this plan doesn’t cover.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
Will you pay less if you use a network provider?
Yes. See https://secure.wecareforwisconsin.com/aspirus_arise/find_a_doctor/
or call 1-800-332-6290 for a list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network. You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
Do you need a referral to see a specialist?
No. You can see the participating specialist you choose without a referral.
2 of 6
Common
Medical Event Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information Participating Provider (You will pay the least)
Non-Participating Provider
(You will pay the most)
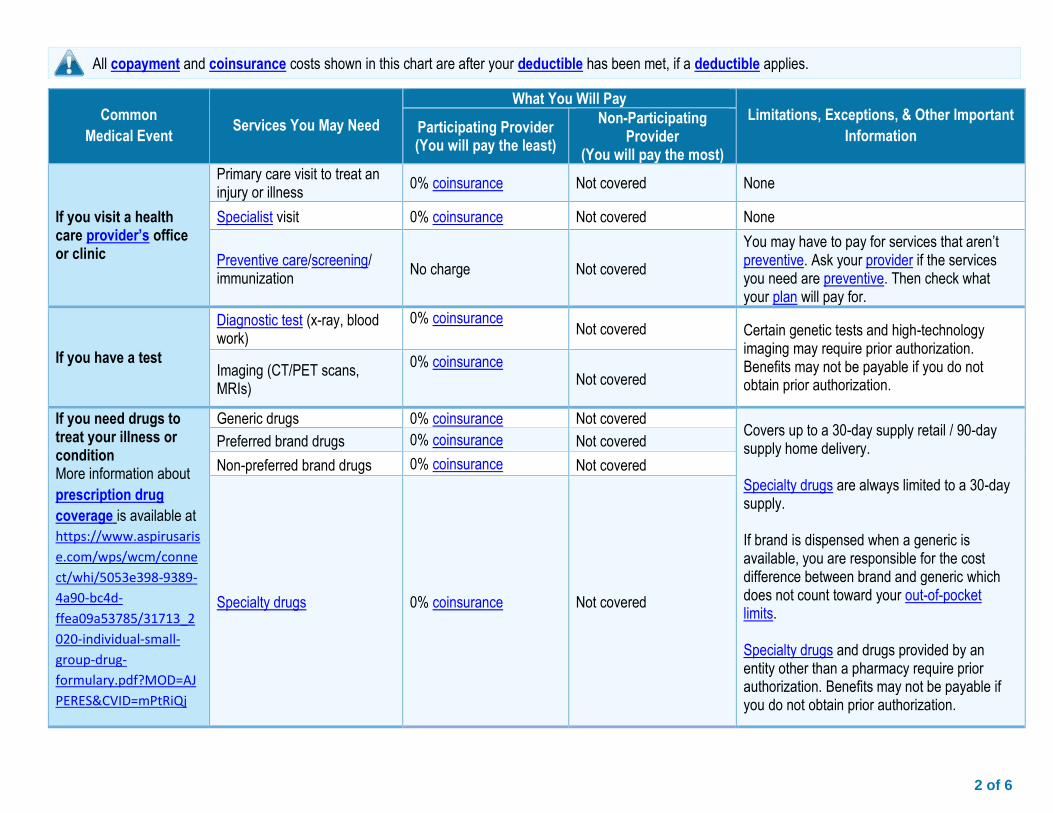
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness
0% coinsurance Not covered None
Specialist visit 0% coinsurance Not covered None
Preventive care/screening/ immunization
No charge Not covered
You may have to pay for services that aren’t preventive. Ask your provider if the services you need are preventive. Then check what your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood work)
0% coinsurance Not covered Certain genetic tests and high-technology
imaging may require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
Imaging (CT/PET scans, MRIs)
0% coinsurance Not covered
If you need drugs to treat your illness or condition More information about
prescription drug
coverage is available at
https://www.aspirusaris
e.com/wps/wcm/conne
ct/whi/5053e398-9389-
4a90-bc4d-
ffea09a53785/31713_2
020-individual-small-
group-drug-
formulary.pdf?MOD=AJ
PERES&CVID=mPtRiQj
Generic drugs 0% coinsurance Not covered Covers up to a 30-day supply retail / 90-day supply home delivery. Specialty drugs are always limited to a 30-day supply. If brand is dispensed when a generic is available, you are responsible for the cost difference between brand and generic which does not count toward your out-of-pocket limits. Specialty drugs and drugs provided by an entity other than a pharmacy require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
Preferred brand drugs 0% coinsurance Not covered
Non-preferred brand drugs 0% coinsurance Not covered
Specialty drugs 0% coinsurance Not covered
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
3 of 6
Common
Medical Event Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information Participating Provider (You will pay the least)
Non-Participating Provider
(You will pay the most)
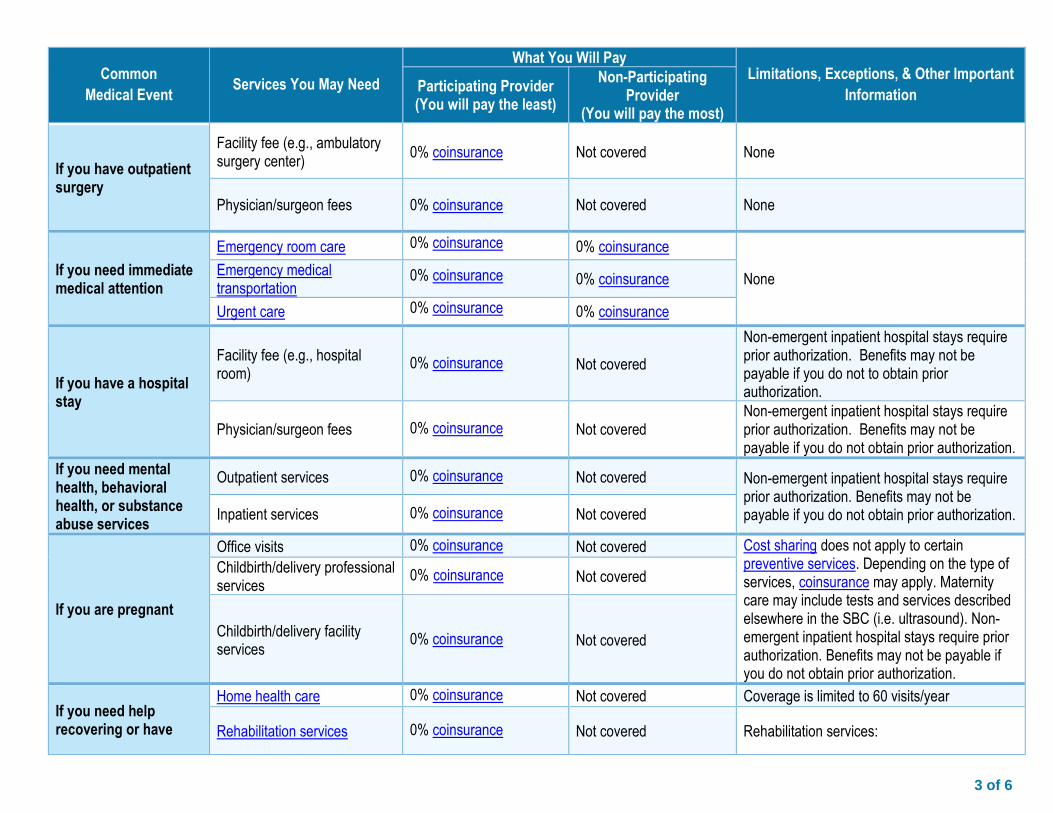
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center)
0% coinsurance Not covered None
Physician/surgeon fees 0% coinsurance Not covered None
If you need immediate medical attention
Emergency room care 0% coinsurance 0% coinsurance
None Emergency medical transportation
0% coinsurance 0% coinsurance
Urgent care 0% coinsurance 0% coinsurance
If you have a hospital stay
Facility fee (e.g., hospital room)
0% coinsurance Not covered
Non-emergent inpatient hospital stays require prior authorization. Benefits may not be payable if you do not to obtain prior authorization.
Physician/surgeon fees 0% coinsurance Not covered Non-emergent inpatient hospital stays require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
If you need mental health, behavioral health, or substance abuse services
Outpatient services 0% coinsurance Not covered Non-emergent inpatient hospital stays require prior authorization. Benefits may not be payable if you do not obtain prior authorization. Inpatient services 0% coinsurance Not covered
If you are pregnant
Office visits 0% coinsurance Not covered Cost sharing does not apply to certain preventive services. Depending on the type of services, coinsurance may apply. Maternity care may include tests and services described elsewhere in the SBC (i.e. ultrasound). Non-emergent inpatient hospital stays require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
Childbirth/delivery professional services
0% coinsurance Not covered
Childbirth/delivery facility services
0% coinsurance Not covered
If you need help recovering or have
Home health care 0% coinsurance Not covered Coverage is limited to 60 visits/year
Rehabilitation services 0% coinsurance Not covered Rehabilitation services:
4 of 6
Common
Medical Event Services You May Need
What You Will Pay Limitations, Exceptions, & Other Important
Information Participating Provider (You will pay the least)
Non-Participating Provider
(You will pay the most)
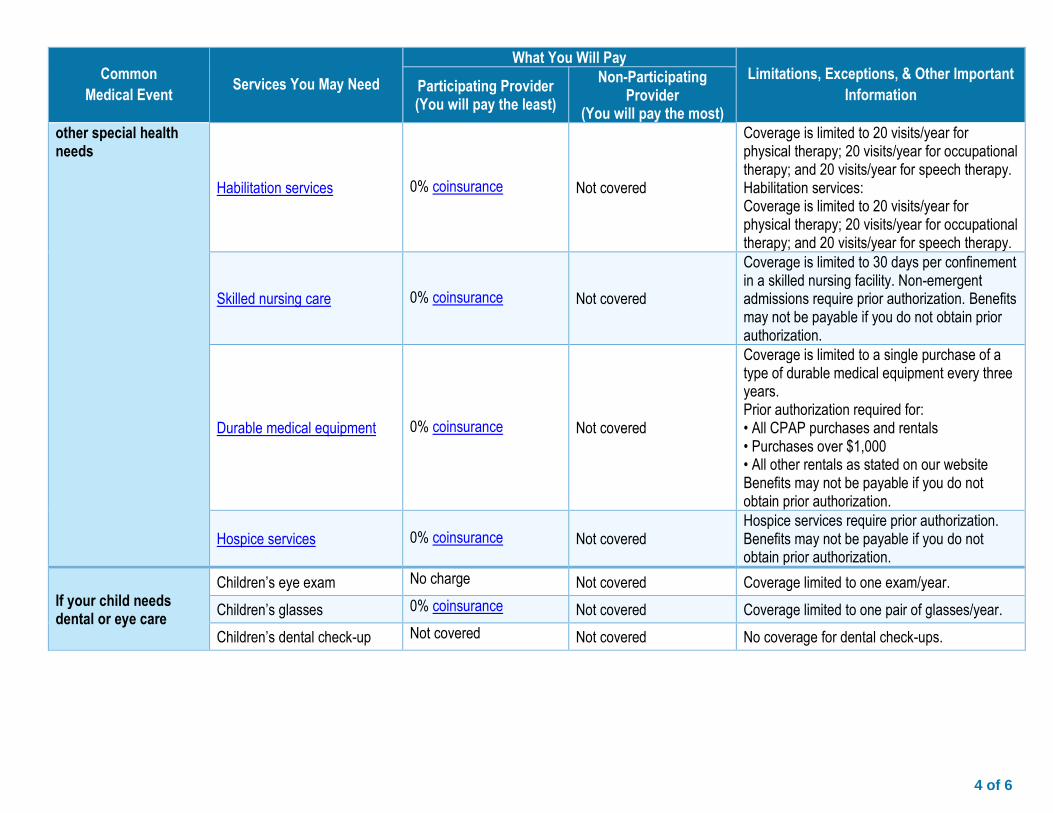
other special health needs
Habilitation services 0% coinsurance Not covered
Coverage is limited to 20 visits/year for physical therapy; 20 visits/year for occupational therapy; and 20 visits/year for speech therapy. Habilitation services: Coverage is limited to 20 visits/year for physical therapy; 20 visits/year for occupational therapy; and 20 visits/year for speech therapy.
Skilled nursing care 0% coinsurance Not covered
Coverage is limited to 30 days per confinement in a skilled nursing facility. Non-emergent admissions require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
Durable medical equipment 0% coinsurance Not covered
Coverage is limited to a single purchase of a type of durable medical equipment every three years. Prior authorization required for: • All CPAP purchases and rentals • Purchases over $1,000 • All other rentals as stated on our website Benefits may not be payable if you do not obtain prior authorization.
Hospice services 0% coinsurance Not covered Hospice services require prior authorization. Benefits may not be payable if you do not obtain prior authorization.
If your child needs dental or eye care
Children’s eye exam No charge Not covered Coverage limited to one exam/year.
Children’s glasses 0% coinsurance Not covered Coverage limited to one pair of glasses/year.
Children’s dental check-up Not covered Not covered No coverage for dental check-ups.
5 of 6
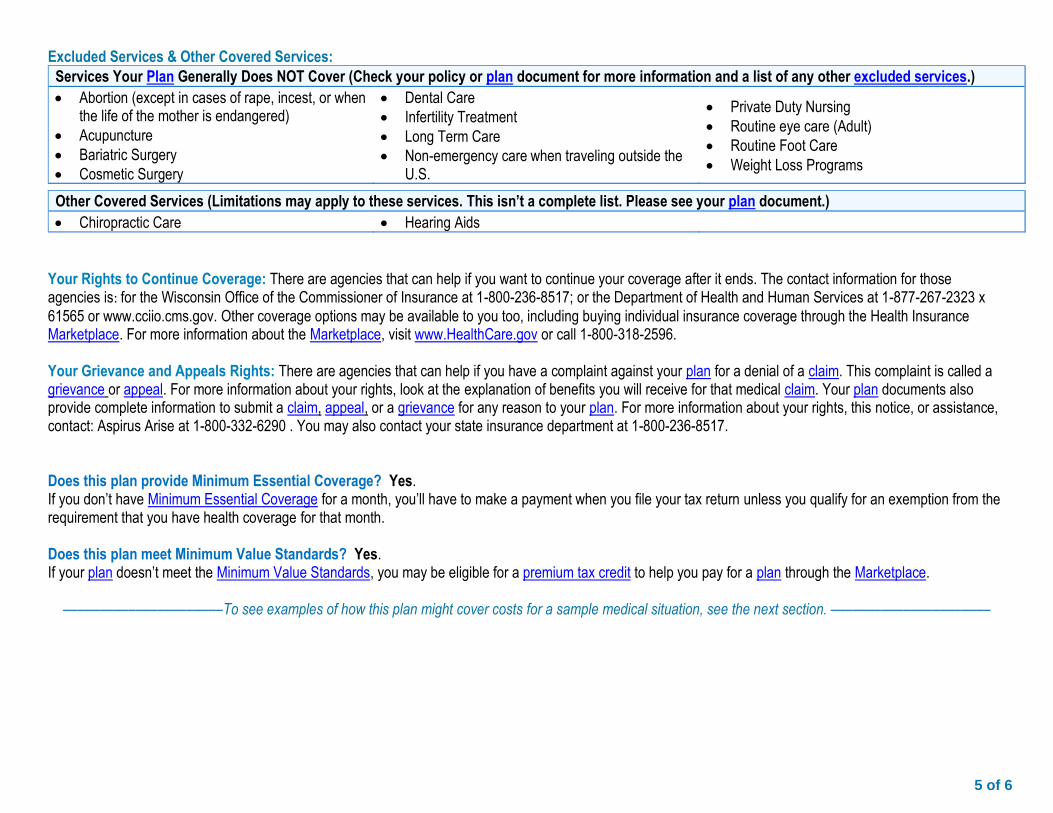
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
• Abortion (except in cases of rape, incest, or when the life of the mother is endangered)
• Acupuncture
• Bariatric Surgery
• Cosmetic Surgery
• Dental Care
• Infertility Treatment
• Long Term Care
• Non-emergency care when traveling outside the U.S.
• Private Duty Nursing
• Routine eye care (Adult)
• Routine Foot Care
• Weight Loss Programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
• Chiropractic Care • Hearing Aids
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: for the Wisconsin Office of the Commissioner of Insurance at 1-800-236-8517; or the Department of Health and Human Services at 1-877-267-2323 x
61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596. Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Aspirus Arise at 1-800-332-6290 . You may also contact your state insurance department at 1-800-236-8517. Does this plan provide Minimum Essential Coverage? Yes. If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month. Does this plan meet Minimum Value Standards? Yes. If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section. ––––––––––––––––––––––
6 of 6
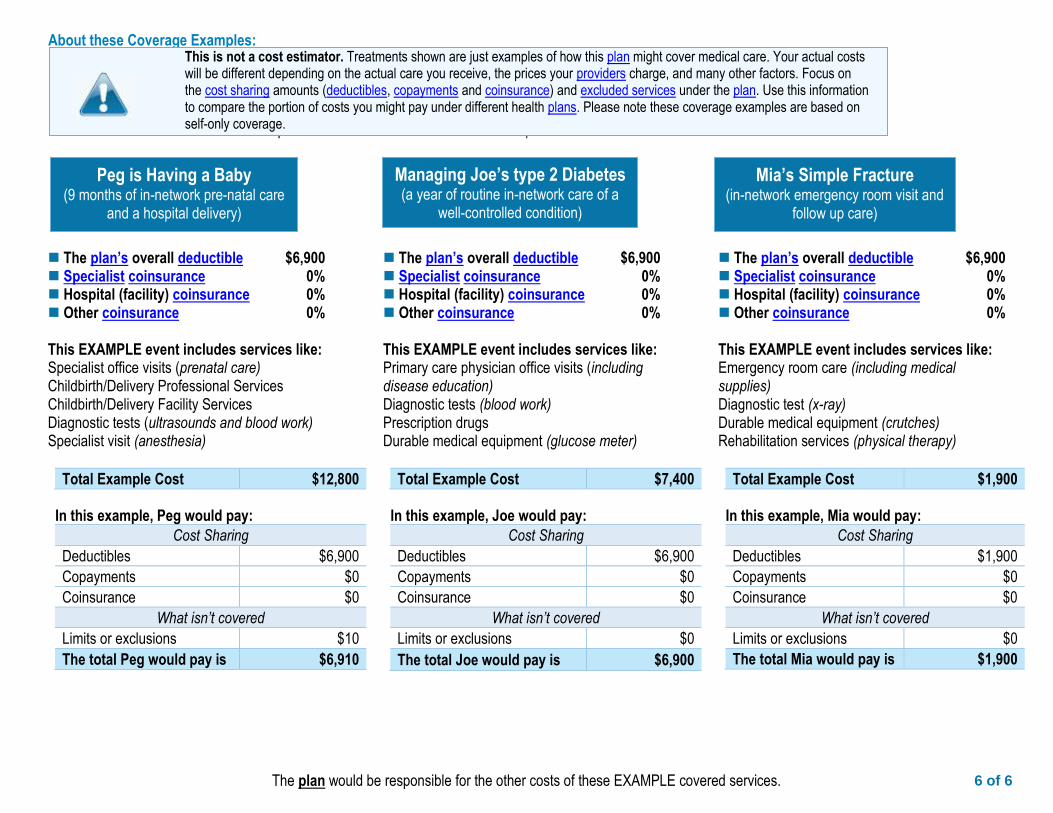
The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a hospital delivery)
Mia’s Simple Fracture
(in-network emergency room visit and follow up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-controlled condition)
◼ The plan’s overall deductible $6,900 ◼ Specialist coinsurance 0% ◼ Hospital (facility) coinsurance 0% ◼ Other coinsurance 0% This EXAMPLE event includes services like: Specialist office visits (prenatal care) Childbirth/Delivery Professional Services Childbirth/Delivery Facility Services Diagnostic tests (ultrasounds and blood work) Specialist visit (anesthesia)
Total Example Cost $12,800
In this example, Peg would pay:
Cost Sharing
Deductibles $6,900
Copayments $0
Coinsurance $0
What isn’t covered
Limits or exclusions $10
The total Peg would pay is $6,910
◼ The plan’s overall deductible $6,900 ◼ Specialist coinsurance 0% ◼ Hospital (facility) coinsurance 0% ◼ Other coinsurance 0% This EXAMPLE event includes services like: Primary care physician office visits (including disease education) Diagnostic tests (blood work) Prescription drugs Durable medical equipment (glucose meter)
Total Example Cost $7,400
In this example, Joe would pay:
Cost Sharing
Deductibles $6,900
Copayments $0
Coinsurance $0
What isn’t covered
Limits or exclusions $0
The total Joe would pay is $6,900
◼ The plan’s overall deductible $6,900 ◼ Specialist coinsurance 0% ◼ Hospital (facility) coinsurance 0% ◼ Other coinsurance 0% This EXAMPLE event includes services like: Emergency room care (including medical supplies) Diagnostic test (x-ray) Durable medical equipment (crutches) Rehabilitation services (physical therapy)
Total Example Cost $1,900
In this example, Mia would pay:
Cost Sharing
Deductibles $1,900
Copayments $0
Coinsurance $0
What isn’t covered
Limits or exclusions $0
The total Mia would pay is $1,900
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
Non-D
iscri
min
ati
on a
nd L
anguage A
ccess
Policy
Asp
irus
Ari
se H
ealt
h P
lan o
f W
isconsi
n,
Inc.
(Asp
irus
Ari
se)
com
plies
wit
h a
pplicable
fe
dera
l civ
il r
ights
law
s and d
oes
not
dis
cri
min
ate
on t
he b
asi
s of
race,
colo
r, n
ati
onal
ori
gin
, age,
dis
abilit
y,
or
sex.
Asp
irus
Ari
se d
oes
not
exclu
de p
eople
or
treat
them
dif
fere
ntl
y b
ecause
of
race,
colo
r, n
ati
onal ori
gin
, age,
dis
abilit
y,
or
sex.
Asp
irus
Ari
se:
Pro
vid
es
free a
ids
and s
erv
ices
to p
eople
wit
h d
isabilit
ies
to c
om
munic
ate
eff
ecti
vely
wit
h u
s, s
uch a
s:
Q
ualifi
ed s
ign language inte
rpre
ters
W
ritt
en info
rmati
on in o
ther
form
ats
(la
rge p
rint,
audio
, access
ible
ele
ctr
onic
form
ats
, oth
er
form
ats
)Pro
vid
es
free language s
erv
ices
to p
eople
whose
pri
mary
language is
not
English
, su
ch a
s:
Q
ualifi
ed inte
rpre
ters
In
form
ati
on w
ritt
en in o
ther
languages
If y
ou n
eed t
hese
serv
ices,
call u
s at
the p
hone n
um
ber
on t
he a
ttached c
orr
esp
ondence,
your
ID c
ard
, or
the n
um
ber
list
ed o
n A
spir
usA
rise
.com
.
If y
ou b
elieve t
hat
Asp
irus
Ari
se h
as
failed t
o p
rovid
e t
hese
serv
ices
or
dis
cri
min
ate
d in
anoth
er
way o
n t
he b
asi
s of
race,
colo
r, n
ati
onal ori
gin
, age,
dis
abilit
y,
or
sex,
you c
an
file
a g
rievance w
ith:
Asp
irus
Ari
se
Nondis
cri
min
ati
on G
rievance C
oord
inato
r P.O
. Box 7
458
Madis
on,
WI 53707
Em
ail:
WPSN
ondis
cri
min
ati
on@
wpsi
c.c
om
You c
an f
ile a
gri
evance in p
ers
on,
by m
ail,
or
by e
mail.
If y
ou n
eed h
elp
filin
g a
gri
evance,
the N
ondis
cri
min
ati
on G
rievance C
oord
inato
r is
available
to h
elp
you.
You c
an a
lso f
ile a
civ
il r
ights
com
pla
int
wit
h t
he U
.S.
Depart
ment
of
Healt
h a
nd H
um
an
Serv
ices,
Off
ice f
or
Civ
il R
ights
ele
ctr
onic
ally t
hro
ugh t
he O
ffic
e f
or
Civ
il R
ights
Com
pla
int
Port
al,
available
at
ocrp
ort
al.
hhs.
gov/ocr/
port
al/
lobby.j
sf;
by m
ail a
t U
.S.
Depart
ment
of
Healt
h a
nd H
um
an Serv
ices,
200 I
ndependence A
venue SW
, Room
509F,
HH
H Buildin
g,
Wash
ingto
n,
DC 2
0201;
or
by p
hone a
t 1–8
00–3
68–1
019,
TTY:
1–8
00–5
37–7
697.
Com
pla
int
form
s are
available
at
hhs.
gov/ocr/
off
ice/fi
le/in
dex.h
tml.
29791-080-1611
Alb
ania
n V
INI R
E: N
ëse
flis
ni s
hq
ip, j
u o
fro
hen
sh
ërb
ime
nd
ihm
e gj
uh
ëso
re f
alas
. Na
tele
fon
on
i në
nu
mri
n e
tel
efo
nit
që
gjen
det
në
korr
esp
on
den
cën
e b
ash
kën
gjit
ur,
në
pje
sën
e p
ërp
arm
e të
kar
tës
suaj
ID
ose
në
nu
mri
n e
ren
dit
ur
në
adre
sën
ww
w.a
spir
usa
rise
.co
m (
TTY:
711
).
Ara
bic
يهنبت
:ًا نجا
مك
لحة
تا م
يةغو
اللة
عدسا
لم ات
ماخد
ن فإ ،
يةرب
لع اغة
اللث
حدتتت
كنا إذ
.ة
جهبال
و أقة
رفلم
الة
ساربال
د جو
مو ال
فاتله
اقم
رى
علا بنل
صات
أك
بصة
خا ال
يةهو
الف
ريتع
ة اقط
لبة
ميما
ألا
ة ليتا ال
يةون
ركت
إلل اعاقمو
بالج
رمد
القم
ر ال
ىعل
و w
ww
.asp
iru
sari
se.c
om
(ي
صالن
ف اتله
ا :
711
.)
Fren
ch À
NO
TER
: Si
vo
us
par
lez
le f
ran
çais
, des
ser
vice
s d
'ass
ista
nce
lin
guis
tiq
ue
grat
uit
s so
nt
à vo
tre
dis
po
siti
on
. A
pp
elez
-no
us
au n
um
éro
de
télé
ph
on
e in
diq
ué
sur
le c
ou
rrie
r jo
int,
au
rec
to d
e vo
tre
cart
e d
'iden
tité
ou
au
nu
mér
o
ind
iqu
é su
r le
sit
e In
tern
et w
ww
.asp
iru
sari
se.c
om
(A
TS :
711)
.
Ger
man
HIN
WEI
S: W
enn
Sie
Deu
tsch
sp
rech
en, s
teh
en f
ür
Sie
kost
enlo
s Sp
rach
assi
sten
zdie
nst
e zu
r V
erfü
gun
g. R
ufe
n
Sie
un
s an
. Sie
fin
den
die
Tel
efo
nn
um
mer
au
f d
em b
eige
fügt
en S
chre
iben
, au
f d
er V
ord
erse
ite
Ihre
r ID
-Kar
te o
der
un
ter
ww
w.a
spir
usa
rise
.co
m (
TTY:
71
1).
Hin
di ध्यान द ें: अग
र आप ह
िन्दी
बोलत
े ि ैं तो
आपके
ललए भ
ाषा स
िायता
सेवाए ँन
निःश ुल्
क उप
लब्ध ि ैं।
िमें संलग्
न पत्र
ाचार पत
ा,आपके
पिचान पत्र
(आईडी क
ाडड) के
सामने के पषृ्ठ पर
हदए ग
ए फोन
नंबर
या w
ww
.asp
iru
sari
se.c
om
पर हदए ग
ए नंबर
पर कॉल
करें (T
TY: 7
11)।
Hm
on
g TS
HW
J X
EEB
: Yo
g h
ais
tias
ko
j hai
s lu
s H
mo
ob
, peb
mu
aj c
ov
kev
pab
cu
am h
ais
ua
koj h
om
lus
pu
b r
au k
oj
yam
tsi
s xa
m t
us
nq
i hlo
li. H
u r
au p
eb
tu
s n
ab n
paw
b x
ov
too
j nyo
b r
au n
taw
m d
aim
nta
wv,
sab
hau
v n
tej n
taw
m k
oj
dai
m id
loss
is n
ab n
paw
b x
ov
too
j nyo
b r
au h
auv
ww
w.a
spir
usa
rise
.co
m (
TTY:
71
1).
Ko
rean
주목
해 주
세요
: 한
국어
를 사
용하
시는
경우
, 언
어 지
원 서
비스
를 무
료로
이용
하실
수 있
습니
다. 첨
부된
서신
, ID
카드
앞면
또는
ww
w.a
spir
usa
rise
.co
m에
나와
있는
전화
번호
로 연
락해
주십
시오
(TTY
: 711
).
Po
lish
UW
AG
A: j
eśli
mó
wis
z p
o p
ols
ku, m
oże
sz s
korz
ysta
ć z
bez
pła
tnej
po
mo
cy ję
zyko
wej
. Zad
zwo
ń p
od
nu
mer
po
dan
y w
zał
ączo
nej
ko
resp
on
de
ncj
i, z
prz
od
u k
arty
iden
tyfi
kacy
jnej
lub
nu
mer
po
dan
y n
a st
ron
ie w
ww
.asp
iru
sari
se.c
om
(TT
Y:
711)
.
Ru
ssia
n В
НИ
МА
НИ
Е! Е
сли
Вы
го
вор
ите
по
-рус
ски
, Вы
мо
жет
е б
есп
лат
но
во
спо
льз
ова
ться
усл
угам
и п
ерев
од
чика
. П
озв
он
ите
по
лю
бо
му
но
мер
у, у
каза
нн
ом
у: в
пр
икр
епл
енн
ом
пи
сьм
е, н
а л
иц
ево
й с
тор
он
е В
ашей
и
ден
тиф
ика
ци
он
но
й к
арты
ил
и н
а са
йта
х w
ww
.asp
iru
sari
se.c
om
(те
лет
айп
: 711
).
Span
ish
ATE
NC
IÓN
: Si h
abla
esp
año
l, lo
s se
rvic
ios
de
asis
ten
cia
de
idio
ma
está
n d
isp
on
ible
s p
ara
ust
ed, s
in n
ingú
n
cost
o p
ara
ust
ed. L
lám
eno
s al
nú
mer
o d
e te
léfo
no
qu
e se
en
cuen
tra
en la
co
rres
po
nd
enci
a ad
jun
ta, e
n la
par
te d
e ad
elan
te d
e su
tar
jeta
de
iden
tifi
caci
ón
o e
n e
l nú
mer
o in
dic
ado
en
ww
w.a
spir
usa
rise
.co
m (
TTY:
711
).
Taga
log
BIG
YAN
G-P
AN
SIN
: Ku
ng
Taga
log
ang
gin
agam
it m
on
g w
ika,
may
mga
ser
bis
yon
g tu
lon
g sa
wik
a n
a m
aku
kuh
a m
o n
ang
wal
ang
bab
ayar
an. T
awag
an k
ami s
a n
um
ero
ng
tele
po
no
na
nas
a n
akal
akip
na
sula
t, n
asa
har
apan
g b
ahag
i ng
iyo
ng
id c
ard
o n
akal
ista
ng
nu
mer
o s
a w
ww
.asp
iru
sari
se.c
om
(TT
Y: 7
11)
.
Trad
itio
nal
Ch
ines
e 注意:如果您使用繁體中文,您可以免费獲得語言援助服務。請撥打隨附之通訊上、
ID 卡
正面或以下網址:
ww
w.a
spir
usa
rise
.co
m 列出的電話號碼與我們聯絡
(TT
Y: 7
11)。
Vie
tnam
ese
CH
Ú Ý
: N
ếu
qu
ý v
ị n
ói tiế
ng
Việ
t, c
hú
ng
tô
i có
cá
c d
ịch
vụ
hỗ
trợ
ng
ôn
ng
ữ m
iễn
ph
í d
àn
h c
ho
qu
ý
vị. H
ãy g
ọi ch
o c
hú
ng
tô
i th
eo
số
điệ
n th
oạ
i có
trê
n th
ư từ
đín
h k
èm
, m
ặt
trư
ớc th
ẻ id
củ
a q
uý v
ị h
oặ
c s
ố đ
iện
th
oạ
i đ
ượ
c n
iêm
yế
t tr
ên
ww
w.a
spir
usa
rise
.co
m (
TTY:
711
).
Pen
nsy
lvan
ia D
utc
h G
EB A
CH
T: W
ann
du
Dei
tsch
sch
wet
zsch
t, d
u k
ann
sch
t Sc
hp
roo
ch S
ervi
ces
grie
ge, m
itau
s K
osc
hd
. R
uf
un
s m
it d
er N
um
mer
uff
die
att
ach
ed c
orr
esp
on
den
ce, d
ie v
on
ne
Seid
e vu
n d
ei ID
Kaa
rde
od
der
die
Nu
mm
er u
ff
ww
w.a
spir
usa
rise
.co
m (
TTY:
71
1).
Lao
ສ ໍາລັບທ່ານທ ່ສົນໃຈ
: ຖ້າທ່ານເວ ົ້າພາສາລາວ
, ມ ບ ໍລ ິການຊ່ວຍເຫ ຼືອດ້ານພາສາໂດຍບ ໍ່ຄ ິດຄ່າໃຊ້ຈ່າຍ
ສ ໍາລັບທ່ານ
. ທ່ານສາມາດໂທ
ຫາພວກເຮ ົາໄດ້ທ ່ໝາຍເລກຢ ່ເທ ິງຈົດໝາຍຕິດຕ່ໍທ ່ຕິດຄັດມາ, ດ້ານໜ້າບັດປະຈ ໍາຕົວຂອງທ່ານ
ຫ ຼື ໝ
າຍເລກທ ່ລະບຸໄວ້ໃນ
ww
w.a
spir
usa
rise
.co
m (
TT
Y: 7
11
).