supervised by: dr- al traifi dr- al traifi saad hamdan faisal aldahash meshal alsadhan
TRANSCRIPT
Lower Urinary Tract Symptoms
(LUTS)
Supervised by:
Dr- Al Traifi
Saad hamdanFaisal aldahash
Meshal alsadhan

Objectives:
Why LUTS?Common causes?What are the symptoms?
Patient work upDetails of the Common etiology BPH

INTRODUCTION
LUTS is the commonest presentation in urology.
It’s a group of symptoms not a diseasesIt is due to many diseases

Lower Urinary Tract Symptoms (LUTS)
Causes Benign prostatic hyperplasia (BPH) with
obstruction Detrusor muscle weakness and/or instability Urinary Tract Infection (UTI) Chronic prostatitis Urinary stone Malignancy: prostate or bladder Neurological disease, e.g. multiple sclerosis,
spinal cord injury, cauda equina syndrome
In males:
Outflow obstructionBPHMeatal stenosisImpaired detrusor functionNM dysfunctionDetrusor instabilityImpaired detrusor contractilityPsychogenic voiding dysfunctionInfectionCystitis, prostatitis, prostatic abcess and urethral diverticulum.neoplastic Prostatic cancer, bladder cancerOthers: Bladder diverticulum, stone and interstitial cystitis.

In females :Mostly storage symptomsUTIPregnancyAnxietyOveractive bladderInterstitial cystitis Postmenopausal urogenital atrophyBladder tumor or stoneGenital prolapses or pelvic massMostly voiding symptoms Age related detrusor muscle weaknessObstruction (urethral stricture, urethral wall divertivulum,
periurethral fibrosis) Urethritis Drugs ( diuretics, alcohol, lithium, anticholinergics)

Lower Urinary Tract Symptoms (LUTS)
Voiding (Obstructive)
Hesitancy: delay in starting micturation Poor stream. Straining for voiding Interruption of the urinary stream Terminal dribbling.

Storage (Irritaive)
Frequency. Nocturia. Urgency: sudden desire for urination that
is difficult to postponed. Urge incontinence. dysuria

Post void Symptoms
Post void Dribbling
Sense of incomplete emptying the bladder

History of
DM
Urological intervention
CNS problems and symptoms
Hematuria
Previous urinary retention
Burning Micturation and Febrile UTI
Drugs intake
Constipation

International Prostate Symptoms Score (IPSS) & Q of LNot at All
Less Than1 Time in 5
Less Than Halfthe Time
About Halfthe Time
More Than Halfthe Time
AlmostAlways
1. Over the past month, how often have you hada sensation of not emptying your bladdercompletely after you finished urinating?
0 1 2 3 4 5
2. Over the past month, how often have you hadto urinate again less than 2 hours after youfinished urinating?
0 1 2 3 4 5
3. Over the past month, how often have youfound you stopped and started again severaltimes when you urinated?
0 1 2 3 4 5
4. Over the past month, how often have youfound it difficult to postpone urination? 0 1 2 3 4 5
5-Over the past month, how often have you hada weak urinary stream? 0 1 2 3 4 5
6. Over the past month, how often have you had to push or strain to begin urination? 0 1 2 3 4 5
7. Over the past month, how many times did youmost typically get up to urinate from the timeyou went to bed at night until the time yougot up in the morning?
None
0 1 time 2 times 3 times 4 times 5 times
If you were to spend the rest of your life withyour urinary condition just the way it is now,how would you think/believe about that?
Delighted
0
Pleased
1
Mostly satisfied
2
Mixed equally
3
Unhappy
4
Terrible
5

Clinical Examination
Abdominal examination
Bladder palpation
Kidney palpation
PR examination.

Per- rectal Examination

Investigations
MSU (Mid-stream urine )& Urine culture
Urine Cytology (for presence of cancerous cells under
microscope)
U&E
LFT
PSA (Prostate-specific antigen)

US



Ascending Urethrogram

Urodynamics
Voiding Diary
Uroflometry
Cystometry
Pressure/Flow
Study
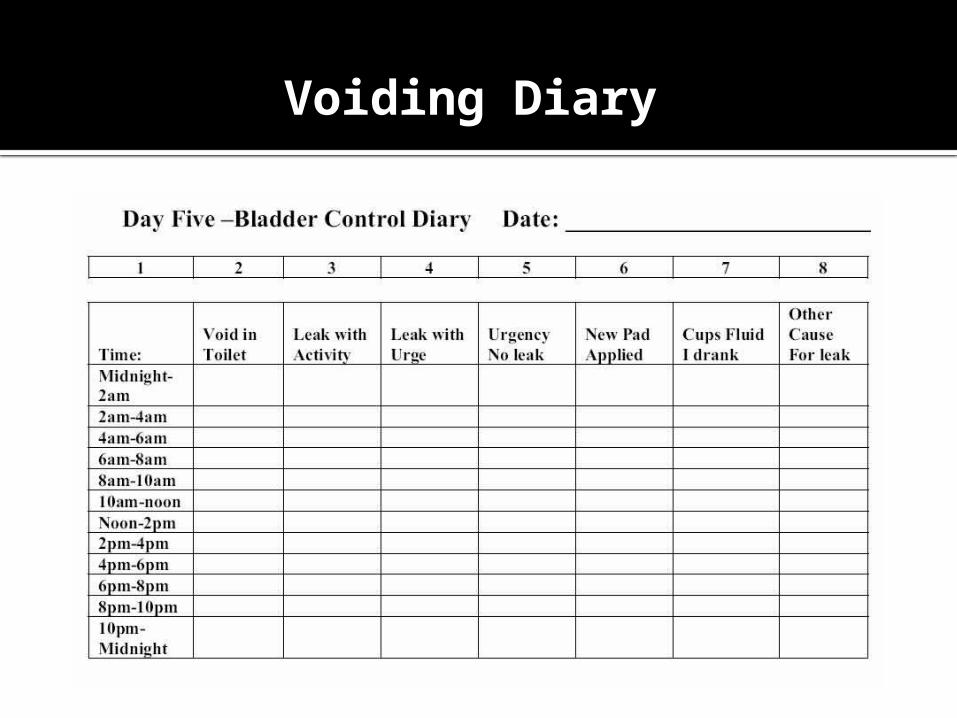
Voiding Diary
Uroflometry

Uroflometry
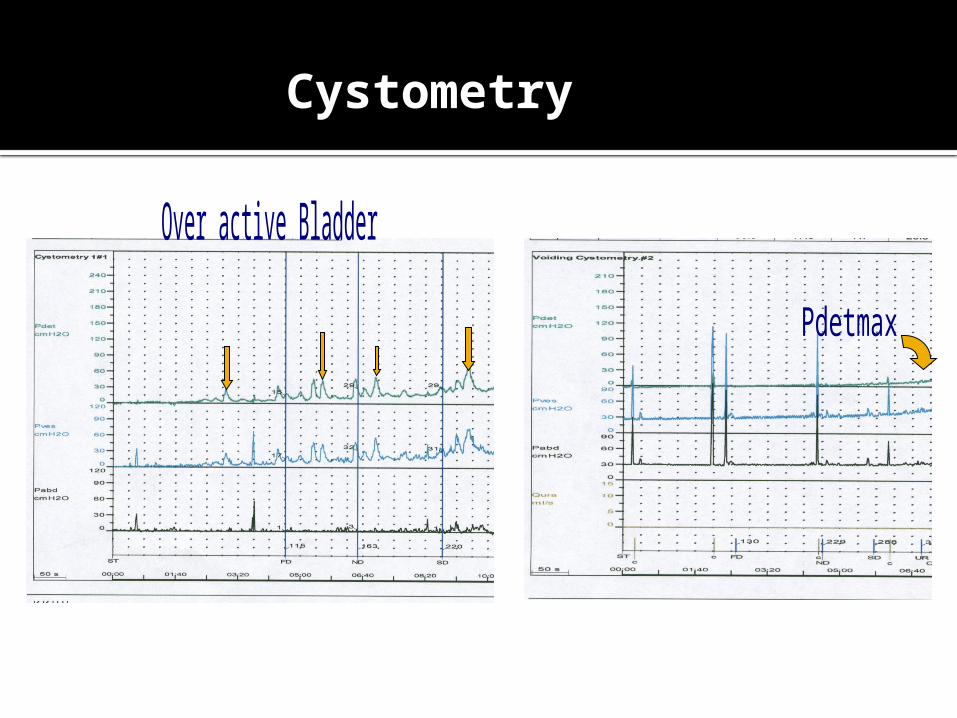
Cystometry
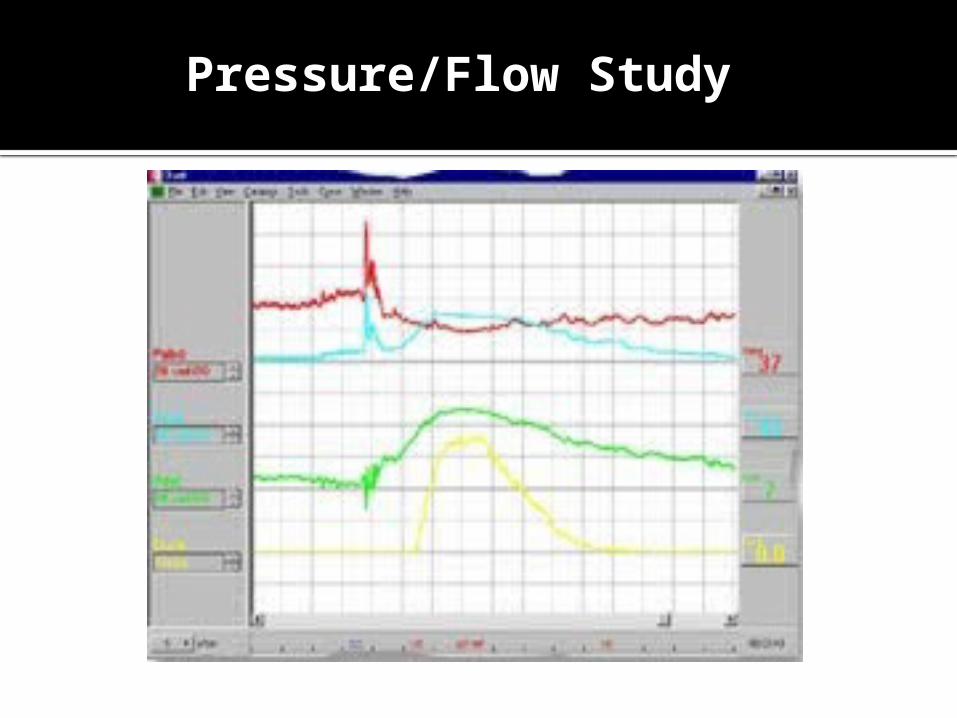
Pressure/Flow Study

Pressure/Flow Study
Management
Watchful Waiting
Alpha Blockers: e.g. Prazosin
Alpha Reductase Inhibitors :e.g.
Finasteride

Benign Prostatic Hyperplasia BPH
• It is the comments etiology of LUTS
Disease of elderly men.
• It is a histological diagnosis and represents as an increase in the number of epithelial and stromal elements of prostate
Con.
• The increase of the elements of prostate ,will result in the formation of large nodules in the periurethral region of the prostate.
• the nodules compress the urethral canal to cause partial, or sometimes complete obstruction of the urethra,
• which interferes with the normal flow of urine.
Clinical manifestation:
Storage symptoms :
• Frequency • Urgency • nocturia
Voiding symptoms :
• Hesitancy • Poor stream • Double voiding • Post void dribbling • Incomplete emptying
Pain and dysuria are usually not present
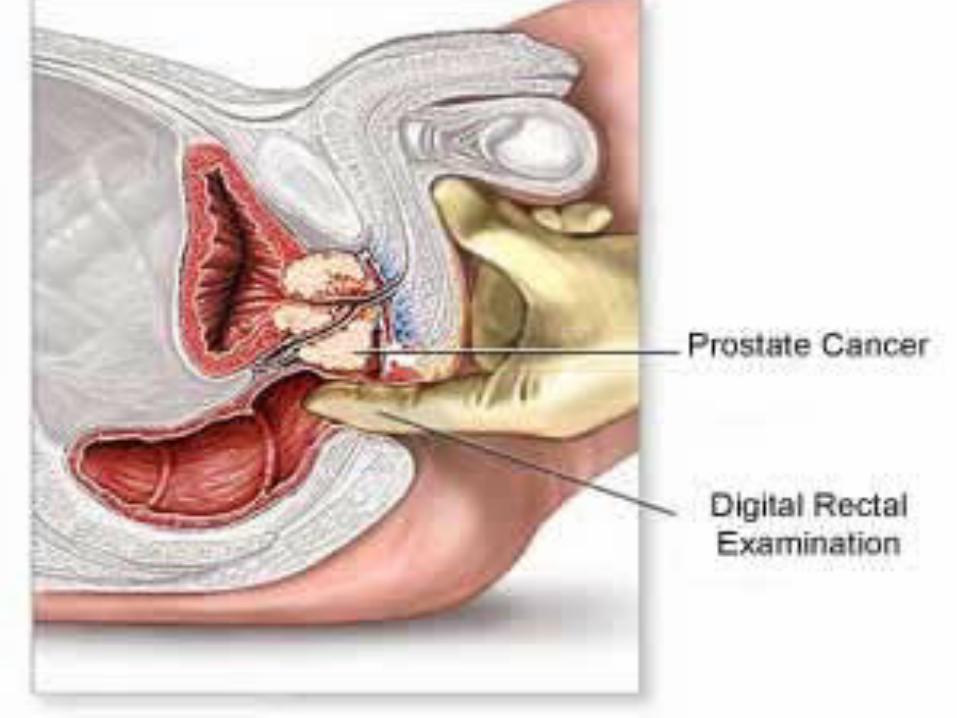
PR examination
Normally, prostate is firm, smooth and with a palpable sulcus.
Signs of BPH: enlarged firm with palpable sulcus.
Sign of malignancy: hard nodular surface with impalpable sulcus.

Investigation
Urinalysis
PSA (prostate specific antigen )
Blood Urea Nitrogen and creatinine
US
Cystoscopy

Treatment
Medical:Tamsulosin:• It blocks adrenergic alpha-1 receptor
of smooth muscle of prostate.
• It decrease bladder neck and urethral resistance.
• It is usually indicated in BPH.
TamsulosinADVERSE EFFECT:1- Headache .2- Arthralgia .3-Rhinitis .4- Decrease libido .5- back pain . Contraindications:1- Liver disease .2- Orthostatic hypotension .3- Hypersensetivity .

Finasteride • It is a 5-alpha reductase inhibitor.
• It is an antiandrogenic drug .
• It is used in case of BPH .
• It is also indicated in case of alopecia in women .
Finasteride
ADVERSE EFFECT:1- Breast enlargement 2- Impotence 3- RashContraindications:1- Hypersensitivity 2- Pregnancy3- Children

BPH Indications for surgery
1. Renal impairment.2. Hydronephrosis.3. Recurrent UTI4. secondary vesical stones5. Recurrent Hematuria 6. Retention of urine7. Significant symptoms not responding
to medication.
Surgery
Transurethral
• Minimal Invasive• Invasive, Transurethral Resection Prostatectomy ( TURP)
Open Prostatectomy
THE END
Notes
BPH is the most common cause of urine obstruction in male .
Terminal voiding dripping: means dripping when the patient still in the bathroom (immediately after voiding).
Post voiding dripping: means dripping ,but when the patient outside the bathroom (after a period of time) .
negative PR test doesn't exclude BPH. Big BPH may lead to increase PSA.

Cont.
> 100 ml is a significant residual volume after void.
The urodynamic is a very accurate diagnostic tool.
CHF patient came with nocturia. In urine retention:
acute : the patient’s complain is pain chronic: the patient complaining of
overflow incontinence. Tamsulosin can cause retrograde
ejaculation in males.

Cont.
Pus >>> culture RBCs >>> cytology
When there is hypertrophy of the wall of bladder (>4cm ) >>urethral constriction.
Middle lobe enlargement doesn't respond to radiotherapy.
Urine flowmetry:Voiding volume must be more than 150-200 ml. in young male adult normal peak flow is 25ml /sec.elderly is more than 15 ml /sec.Female flow is stronger.

Cystometry:- Dertrouser pressure (normal is < 15 ml of water ??)
Pressure flow studyIncreased pressure and decreased flow >>prostateDecreased pressure and decreased flow >>Dertrouser