supervisory board advisory board - mophp-ye. · pdf filesupervisory board advisory board ......
TRANSCRIPT
YHMRJ August/2004
Advisory Board Supervisory Board
- Prof. Kaled Batarge - Prof. Mohammed Y. Al-Noame - Prof. Ahmed Al-Hadrani - Prof. Thabet M. Nasher - Dr. Yaseen A. Al-Qubati - Prof. Abdullah A. Gonaeed - Prof. Ahmed M. Al-Haddad - Dr. Arwa M. Al-Rabeea - Dr. Yehya A. Raja a - Dr. Abdullkarim A. Shaiban - Prof. Ahmed Abdrabo - Dr. Nageeb A. Al-Galeel - Dr. Ali Kaid K. Al-Sharabe - Dr. Abdullkarim Rasea - Dr. Salem Ba-Nagah - Dr. Yahya Al-Babelee - Prof. Saleh Al-Sallame - Dr. Talal Hyder - Dr. Mahfood Ba-Mashmoos
Co-Editor Editor-in-chief M. Tarek S. Asa'ad Prof. AbdulMageed S. Al-Kolide
Secretary of Editor Managing Editor Dr. Taha A. Al-Sorori Dr. Ahmed A. M. Al-Qubati
Address:
Republic of Yemen, Sana a, Ministry of Public Health & Population, Research Center, TelFax: 00967-1-252192, P.O.Box: 3797, Email: [email protected]

YHMRJ August/2004
Definetion of Research Center:
The health research Center established in the Ministry of Health at the year 1997, It s considered to be specialized in quality tasks and Goals. It s a main supporter of Health policies, programs and reformes. It s depend on national caders for it s programs and Goals.
General Objective:
1- The Determination of the policies, strategies and priorities of Health research.
2- To strength the ability of Health & medical research and to develop the skills of the professional researchers in preparing and bringing out health researches and studies to gain from it s results.
3- Formation of the national health and medical research committee and it s roll especially in ethical review.
4- Establishment of the health research brunches in the main cities: Aden, Al-Hodeidah, Hearamout, and Taiz.
5- Establishment of specialized referenced library with update technical methods.
6- Coordination and cooperation with health programs, academic institutions, governmental and International organizations to develop and speed up the activities of health research.

YHMRJ August/2004
Final report for the project entitled
Knowledge attitude and practice of university students toward substance abuse in Sana'a, Republic of Yemen (1.D RPC O2/191)
Submitted to: DR. Mohamad abdulrab RA /RPC .EMRO .WHO
Submitted by: principal investigators: Mr.Abdulrakib Ahmad AlHanani(1)
CO-investigators: Dr Yahia Ahmad Raja a(2)
Mr. Adel Mahyoob Al Samia(3) Mr. Hisham Mohmad al Mahbashi(4) Date of submission : / / 2004
Knowledge, attitude and practice of university students toward substance abuse in Sana a, Republic of Yemen
Introduction: Psychoactive substance use is a worldwide problem. It poses a significant threat to
the health, social and economic fabric of families, communities and nations. The extent of worldwide psychoactive substance use is estimated at 2 billion alcohol users, 1.3 billion smokers and 185 million drug users(1). Substance abuse continued to be a major health and socioeconomic problem in the region. Although alcohol use has not reached an alarming level owing to strict Islamic prohibition, there is evidence that it exists (2). The countries most affected by narcotics are Afghanistan, Iran and Pakistan. Available information indicates that the flow of narcotics to countries of Gulf Cooperation Council are on rise. Egypt, Libya - to lesser extent-, Morocco, Sudan, Syria and Tunisia are in danger of reaching such situation. Consumption of psychotropic substances is reported in many parts of the region .(3)
Khat use is a part of life style in Yemen, Djibouti, Somalia, and Ethiopia(4). It is chewed also in southern parts of Saudi Arabia (5). Khat appeared also in United States and several European countries(6).
1- Academic educator, Nursing division, Faculty of Medicine and Health sciences ,Sana a University. 2- Associate professor, Community Medicine Department Faculty of Medicine and Health sciences, Sana a
University. 3- Researcher, Health Research Center MoPH&P. 4- Academic educator, Nursing division Faculty of Medicine, and Health sciences Sana a University.
YHMRJ August/2004
Tobacco continues to be the substance causing the maximum health damage globally. World Health Organization (WHO) estimates that tobacco causes about 8.8% of deaths (4.9 million) and 4.1% of disability-adjusted life-years (DALYs) (59.1 million).
Tobacco is cultivated in many regions around the world including Yemen and can be legally purchased in all countries. The dried leaf of the plant Nicotiana tabacum is used for smoking, chewing or snuff. Smoking causes substantially increased risk of mortality from lung cancer, upper aerodigestive cancer, several other cancers, heart disease, stroke, chronic respiratory disease and a range of other medical causes. Smoking also harms others (passive smoking). Smoking during pregnancy adversely affects fetal development. While cigarette smoking causes the majority of the adverse health effects of tobacco, smoking cigars or Shisha are also hazardous (1). In a study in Lebanon the prevalence of smoking among university students was 40%, 21% only narghile, 7.6% only cigarettes and 11.3% smoking both cigarette and narghile. The prevalence of cigarette smoking among males and females was 36.8%, 14.8% respectively (7). Another study in North West Ethiopia revealed the lifetime prevalence of smoking among college students was 13.1 %. Majority of students 87.1 % knew that cigarette smoking is a risk factor for lung diseases including lung cancer (8). In south Western Saudi Arabia, the prevalence of regular tobacco smoking among university students was 17.5% in Education College and 13.6% in Medical College. Daily smokers constituted 88.5% and 72.4% respectively. Cigarette smoking ranked first for both groups of students (84.3% and 70.4%), followed by Shisha (traditional Arabic smoking pipe) 39.6% and 51% while cigar ranked last 3.9% and 3.7%. Previous attempts to stop smoking were reported by 75% of college of education smokers and 55.6% of the medical college smokers. Future intention to stop smoking was 81.3% of education college smokers as compared to 63% of medical college smokers. Most students of both groups showed either positive or strongly positive attitudes toward public action against smoking. However, smokers showed less positive attitude than did non-smokers (9). The prevalence of smoking among university students in Jordan was 26.6%. Prevalence of smoking was 50.2% among males and 6.5% among females. Also, prevalence of smoking increased significantly according to year of study: first year, 9.6%; second year, 25.0%; third year, 28.9%; and fourth year, 56.7%. Two- thirds of the smokers intended to quit smoking in the future (10).
Khat is a plant known as Catha edulis forsk. Its fresh leaves are used, by chewing, for its psychostimulant effect (11). This effect can be accounted for by the mechanism of cathinone which is a liable substance structurally related to amphetamine (12). Khat chewing might be exacerbate symptoms in-patients with pre-existing psychiatric
YHMRJ August/2004
disease(13). Khat chewing is significantly associated with duodenal ulcer (14), increased incidence of acute myocardial infarction (15) and haemorridal disease (16). The lifetime prevalence of Khat chewing among colleges students of Northwest Ethiopia was 26.7%. Many students believe that Khat chewing have health risks 81,1% such as addiction and gastrointestinal tract problems. Rate of Khat chewing habit increases with age and year of study (7). Substance abuse is the use of a drug or other substance for a non-medical use, with the aim of producing some type of 'mind-altering' effect in the user. This includes both the use of illegally produced substances, and the abuse of legal drugs, in a use for which the substance was not intended. Often this involves use of the substance in excessive quantities. Many different types of drugs can be abused: not only illegal drugs such as heroin, cannabis, cocaine or ecstasy, but also prescription drugs such as tranquillizers, analgesics (painkillers) and sleeping pills. Even medicines that can be bought of the supermarket shelf can be abused (such as cough mixtures or herbal remedies). Some of the risks associated with drug abuse include: risk to personal safety (danger of death or injury by overdose, accident or aggression), damage to health (including brain damage, liver failure, mental problems etc.), legal consequences (risk of imprisonment, fines and criminal record) and destructive behavior (harm to self, family and friends (17). The estimated prevalence of illicit drug use over the world was 185 million drug users. An estimate from the United Nations Drug Control Programme of the prevalence of opioid use in the year 2001 among people over the age of 15 years was 0.4- 0.6% in the Eastern Mediterranean region(1). Cocaine use varies to a similar extent, but the prevalence of amphetamine use is estimated to be 0.1 - 0.3% in most regions. Globally, 0.4% of deaths (0.2 million) and 0.8% of (DALYs) (11.2 million) are attributed to overall illicit drug use. Illicit drug use account for the highest proportion of disease burden among low mortality, industrialized countries in the Americas, Eastern Mediterranean and European regions. In these areas illicit drug use accounts for 2- 4% of all disease burden among men (1). The diazepam use rates among Nigerian males was found more than female students(18). The lifetime prevalence of diazepam derivatives use (benzodiazepines) among medical students in Zagreb University was 33% ( 9 ). The prevalence of substance abuse among Shiraz University students was 21% for opium and 12% for cannabis. There was only one report of heroin use (0.5%)(20). The prevalence of illicit drug use in a sample of Turkish medical students was 4% (cannabis, ecstasy, and cocaine) at least once in their lifetime. The mean ages of first use of illicit drugs were earlier for junior medical students than seniors (21)
The marijuana and hashish prevalence among medical students in Barcelona was 9.6%(22), while the lifetime prevalence of marijuana use among medical students in Zagreb University was 35%. Repeated marijuana use was reported by 3.9% students (23).

YHMRJ August/2004
Global alcohol consumption has increased in recent decades, with most or all of this increase occurring in developing countries. It has health and social consequences via intoxication, dependence and other biochemical effect. In addition to chronic diseases that may affect drinkers after many years of heavy use. Alcohol contributes to traumatic outcomes that kill or disable at a relatively young age, resulting in the loss of many years of life to death or disability. Overall there is a causal relationship between alcohol consumption and more than 60 types of disease and injury. Alcohol is estimated to cause 20
30 % worldwide of esophageal cancer, liver cancer, cirrhosis of the liver, homicide, epilepsy and motor vehicle accidents. Worldwide, alcohol causes 3.2% of deaths (1.8 million) and 4.0% of DALYs (58.3 million)(1). The prevalence of alcohol ever use among Shiraz University students in Iran was 25% and 13% who use in 6 months prior to survey (19). The overall prevalence of lifetime alcohol use among Turkish medical students was 46%. Senior students are more likely to use alcohol than junior students (n = 83, 58% vs. n = 123, 40.5%). There was no gender difference in drinking alcohol in either group(20). Khat chewing, Tobacco smoking are noticed among university students in Yemen, the magnitude of the habits together with the possibility of other habits (e.g. drugs ) are obscure ,the objectives of this study are : - Generally, to explore knowledge, attitudes and practices of university students toward substance use in Sana'a city Republic of Yemen. Specifically, - To estimate the prevalence of Khat, tobacco, and drug use among students of Sana a
University. In addition to ascertain knowledge and attitude among students to substance use.
- To correlate substance use with gender and level of education.
Methodology:
Study setting and population : Sana a University which represent the biggest public university in Yemen and the student who pursue their education reflect the socio economic diversity students in the cuontery . Total University students are 50,000.All attendant students; males and females were 36517. Males were 22555(61.8%)and females were 13962 (38.2%). Self-administered Arabic questionnaire was prepared and internally validated by 4 experienced researchers from Community Medicine Dept and Health Research Centre for reviewing and refining. Then pre-tested on 50 students (males and females) for final revision. Field visit: visits to university administration and colleges for consent and to find out numbers of attendant students in each level to help in adopting sampling. Study design: Cross sectional Sample size: A total of 3263 male and female students responded to the questionnaire Out of 3420 targeted student.

YHMRJ August/2004
Response rate: The total response rate is 95.4%. The response rates for the core variables are presented in table 1.
Table 1. Response rate for individual core variables. Response rate Missing Categories
No. % No. % Khat 3155 96.7 108 3.3
Tobacco 3103 95.1 160 4.9
Mental substance 2977 91.2 286 8.8
Alcohol 2873 88.2 390 11.9 Sex 3217 98.6 46 1.4
Level 3174 97.3 89 2.7
Sampling technique: The sample was stratified according to sex for each level of university education. The sample size of each stratum was estimated to be 384 students. We divided total number of students in each level into clusters ( around 384 each ) and selected one randomly from the random list of the Epi 6 computer program (table 2). Table 2. Number of student clusters according to level and sex.
Clusters Level Males Females
1 12 8
2 11 7 3 8 7
4 and more 9 8 Total 40 30
Data collectors were selected from the graduates of Sana a university then they were trained about data collection procedure, targeted cluster, time of distribution and collection of questionnaire. Questionnaire forms were distributed either pre- lecture (15 minutes before entrance of lecturer) or 15 minutes before the end of the lecture during the period from 16/8/2003- 20/12/2003. Data entry and analysis : Data were entered and processed in a P.C using SPSS programme version 11.5. Constraints: Data collection stopped during the holy month of Ramadan due to high absenteeism.

YHMRJ August/2004

YHMRJ August/2004
Results:
Table 1. Distribution of students according to sex and level
Personal characteristic
%
male
1612 50.1
Female 1605 49.9 Sex
Missing 46
L 1 837 26.4
L 2 727 22.9
L 3 845 26.6 Level
L 4 and more 765 24.1
Missing 89
Mean age Male 21.7
2.4 years Female 21.2
2.4 years
Mean age for both 21.47
2.4 years
Table 2. Prevalence of Khat, tobacco, substance and alcohol use in relation to sex Khat Tobacco Substance Alcohol Sex
%
%
%
%
Male 1276 81.6 433 26.9 54 3.7 50 3.5
Female 403 25.9 123 7.7 25 1.7 9 0.6
Chi- square 970.6 207.3 11 29
P 0. 0001
0.0001 0.001
0.0001
OR 12.6 3.5 2.2 5.7
YHMRJ August/2004
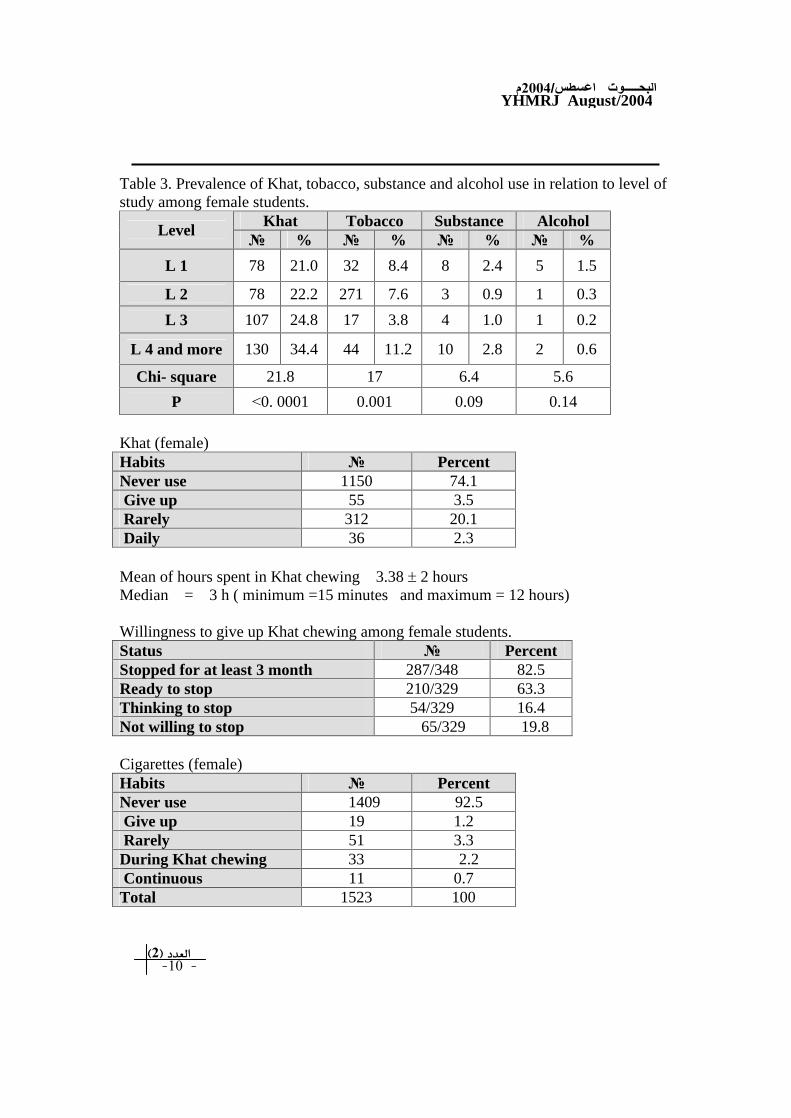
Table 3. Prevalence of Khat, tobacco, substance and alcohol use in relation to level of study among female students.
Khat Tobacco Substance Alcohol Level
%
%
%
%
L 1 78 21.0 32 8.4 8 2.4 5 1.5
L 2 78 22.2 271 7.6 3 0.9 1 0.3
L 3 107 24.8 17 3.8 4 1.0 1 0.2
L 4 and more 130 34.4 44 11.2 10 2.8 2 0.6
Chi- square 21.8 17 6.4 5.6
P 0. 0001 0.001 0.09 0.14
Khat (female) Habits
Percent Never use 1150 74.1 Give up 55 3.5 Rarely 312 20.1 Daily 36 2.3
Mean of hours spent in Khat chewing 3.38
2 hours Median = 3 h ( minimum =15 minutes and maximum = 12 hours)
Willingness to give up Khat chewing among female students. Status
Percent Stopped for at least 3 month 287/348 82.5 Ready to stop 210/329 63.3 Thinking to stop 54/329 16.4 Not willing to stop 65/329 19.8
Cigarettes (female) Habits
Percent Never use 1409 92.5 Give up 19 1.2 Rarely 51 3.3 During Khat chewing 33 2.2 Continuous 11 0.7 Total 1523 100

YHMRJ August/2004
Cigarette smoking Median 4 cigarrettes Minimum 1 Maximum 20
Willingness to quit cigarette smoking among female students. Status
Percent Not willing to stop 58/85 68.2 Stopped for at least 1 month 28/41 68.3 Ready to quit 11/85 12.9 Thinking to stop within the next 6 months 16/85 18.8
Number of girls (ever used ) who tried to stop smoking (no = 36) 94.74% Mean of trials 3.2 Median 3 Minimum 0 Maximum 20
Reasons for quitting from cigarette smoking among female students Reason Number Percent
Health reasons 6 35.3 Economic reasons 3 17.6 Social reasons 4 23.5 Other reasons 3 17.6 Health , economic and social reasons 1 5.9
Shisha (females) Habits
% Never use 1449 95.8 Give up 0 0.0 Rarely 59 3.9 Daily 4 0.3 Total 1512 100
Substance (female) Habits
% Never use 1448 98.3 Give up 5 0.34 Rarely 16 1.09 Daily 4 0.27 Total 1473 100

YHMRJ August/2004
Type of substance according to ever use (females)
Type
%
Diazepam 10 25.6 Hashish 3 7.7 Cocaine 3 7.7 Heroin 1 2.6 Other 1 2.6 All types 1 2.6 Type not determined 20 51.3
Total 39 100
Stop substance (female) Status
% Stopped for at least 1 month 13/19 68.4 Not willing to stop within 6 months 3/16 18.8 Ready to stop 7/16 43.8 Thinking to stop 6/16 37.5
Total
Alcohol (female) Habits
% Never use 1408 99.4 Give up 3 0.21 Rarely 6 0.42
Table 3. Prevalence of Khat, tobacco, substance and alcohol use in relation to level in males
Khat Tobacco Substance Alcohol Shesha Level
%
%
%
%
% L 1 343 78 92 20.2 17 4.2 8 2 26 6.4 L 2 274 75.5 78 21 11 3.2 10 3.1 16 4.9 L 3 321 84.9 117 29.8 9 2.5 9 2.6 15 4.4 L 4 and more 314 87.5 139 37.9 17 5.1 22 6.7 46 14.8 Chi- square 23.6 41.1 3.6 13.5 33.1 P
0.0001
0.0001 0.31 0.004
0.0001
YHMRJ August/2004
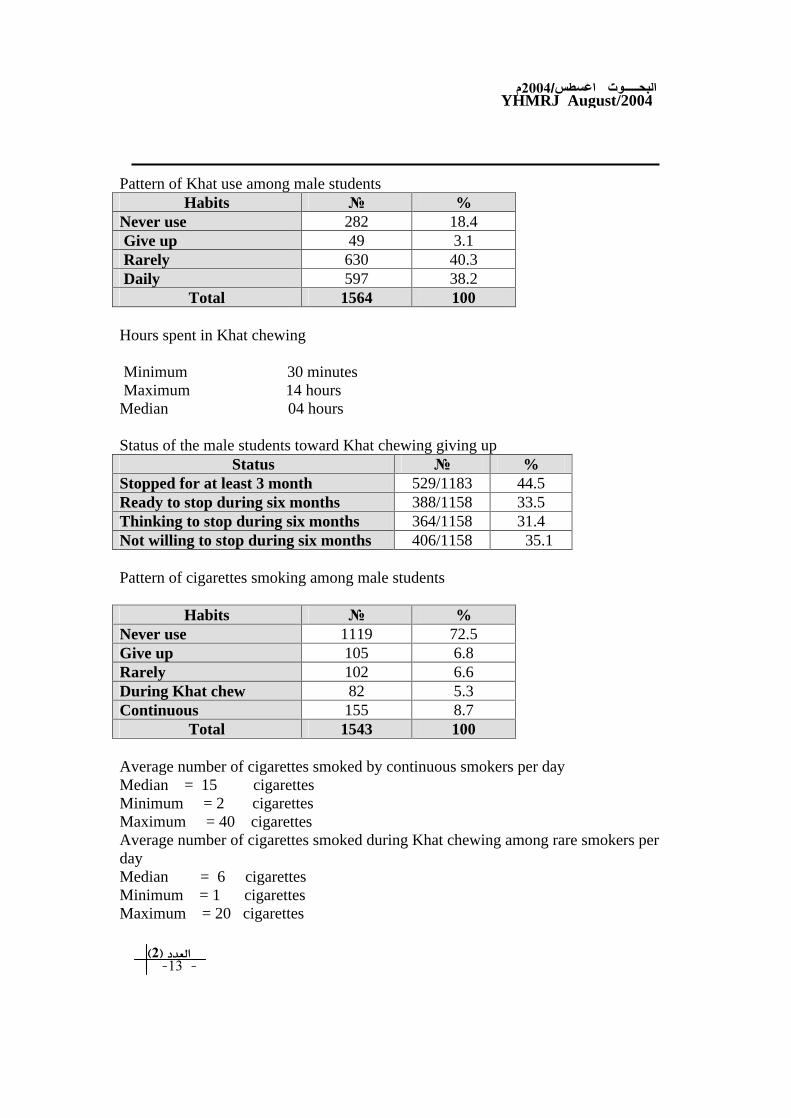
Pattern of Khat use among male students
Habits
%
Never use 282 18.4 Give up 49 3.1 Rarely 630 40.3 Daily 597 38.2
Total 1564 100
Hours spent in Khat chewing
Minimum 30 minutes Maximum 14 hours Median 04 hours
Status of the male students toward Khat chewing giving up Status
% Stopped for at least 3 month 529/1183 44.5 Ready to stop during six months 388/1158 33.5 Thinking to stop during six months 364/1158 31.4 Not willing to stop during six months 406/1158 35.1
Pattern of cigarettes smoking among male students
Habits
% Never use 1119 72.5 Give up 105 6.8 Rarely 102 6.6 During Khat chew 82 5.3 Continuous 155 8.7
Total 1543 100
Average number of cigarettes smoked by continuous smokers per day Median = 15 cigarettes Minimum = 2 cigarettes Maximum = 40 cigarettes Average number of cigarettes smoked during Khat chewing among rare smokers per day Median = 6 cigarettes Minimum = 1 cigarettes Maximum = 20 cigarettes
YHMRJ August/2004
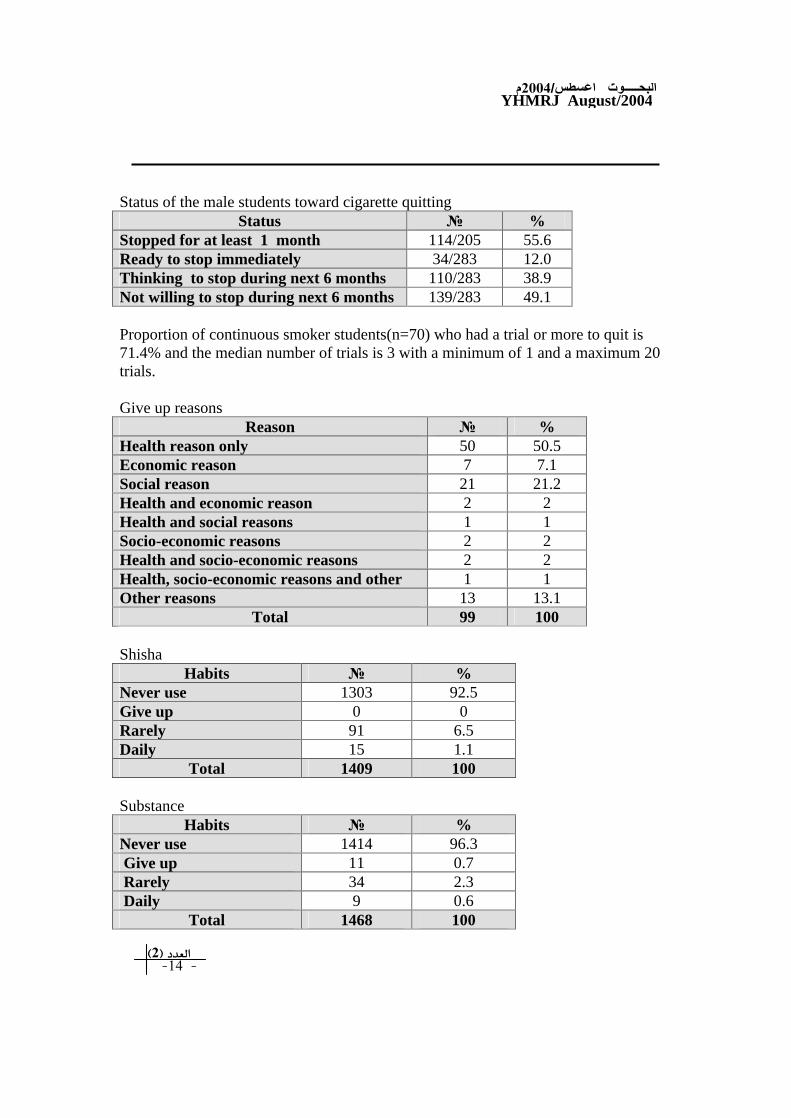
Status of the male students toward cigarette quitting
Status
%
Stopped for at least 1 month 114/205 55.6 Ready to stop immediately 34/283 12.0 Thinking to stop during next 6 months 110/283 38.9 Not willing to stop during next 6 months 139/283 49.1
Proportion of continuous smoker students(n=70) who had a trial or more to quit is 71.4% and the median number of trials is 3 with a minimum of 1 and a maximum 20 trials. Give up reasons
Reason
% Health reason only 50 50.5 Economic reason 7 7.1 Social reason 21 21.2 Health and economic reason 2 2 Health and social reasons 1 1 Socio-economic reasons 2 2 Health and socio-economic reasons 2 2 Health, socio-economic reasons and other 1 1 Other reasons 13 13.1
Total 99 100
Shisha Habits
% Never use 1303 92.5 Give up 0 0 Rarely 91 6.5 Daily 15 1.1
Total 1409 100
Substance Habits
% Never use 1414 96.3 Give up 11 0.7 Rarely 34 2.3 Daily 9 0.6
Total 1468 100

YHMRJ August/2004
Type of substances used among male students who admitted use
Type of substance
%
Diazepam 21 15.8 Hashish 18 13.5 Cocaine 4 3.0 Heroin 1 0.8 Other 1 0.8 Hashish and cocaine 1 0.8 Type not determined 87 65.4
Total 133 100
Stop substance Status /total
% Stopped for at least 1 month 29/42 69 Ready to stopped 21/44 47.7 Thinking to stopped 13/44 29.5 Not willing to stop 10/44 22.7
Alcohol Habits
% Never use 1370 96.5 Give up 12 0.8 Rarely 22 1.5 After Khat chewing 7 0.5 Daily 9 0.6
Total 1420 100
Alcohol status in males Status
% Ready to stop 0.0 0. Thinking to stop 11 25.6 Not willing to stop within 6 months 32 74.4
Total 43 100
YHMRJ August/2004
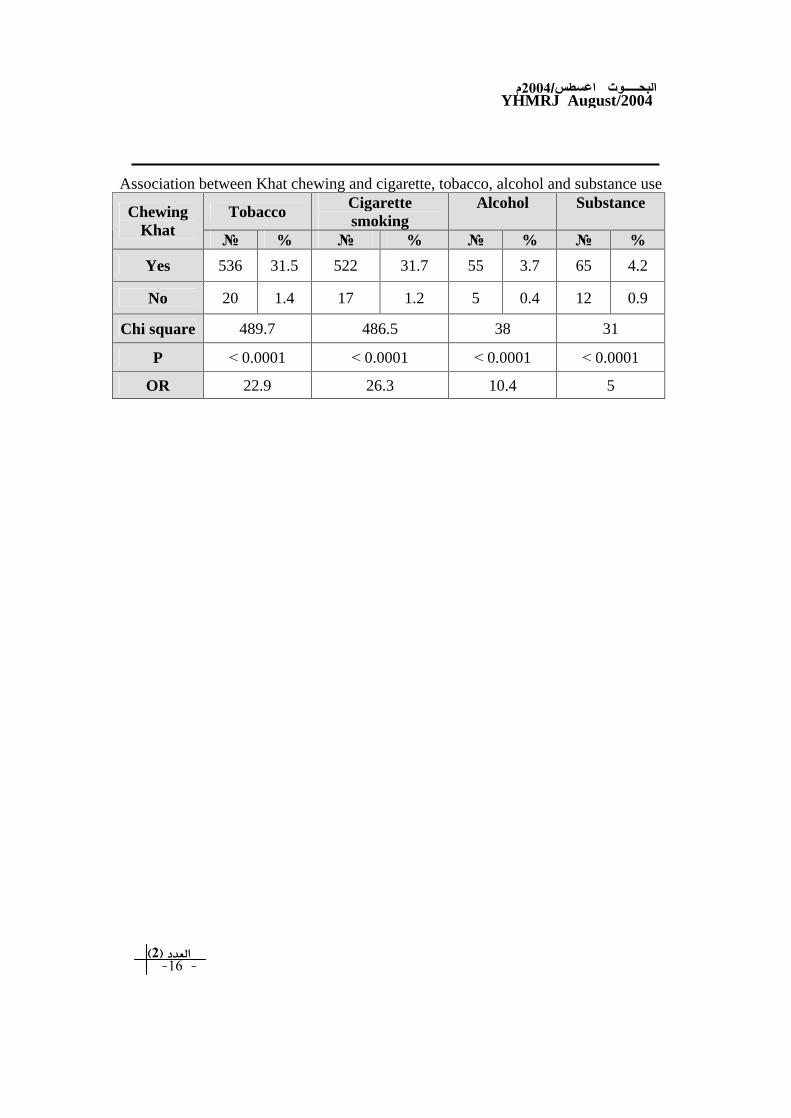
Association between Khat chewing and cigarette, tobacco, alcohol and substance use
Tobacco Cigarette smoking
Alcohol Substance Chewing Khat
%
%
%
%
Yes 536 31.5 522 31.7 55 3.7 65 4.2
No 20 1.4 17 1.2 5 0.4 12 0.9
Chi square
489.7 486.5 38 31
P
0.0001
0.0001
0.0001
0.0001
OR 22.9 26.3 10.4 5
YHMRJ August/2004
Thyroid cancer in Yemen.
Abdulmughni YA, Al-Hureibi MA, Al-Hureibi KA, Ghafoor MA, Al-Wadan AH, Al-Hureibi YA. Assistant Professor, Department of Surgery, Faculty of Medicine, Sana'a University, PO Box 2481, Sana'a, Yemen. Tel. +967 73761714. Fax. +9671 440-777. E-mail: [email protected]
OBJECTIVE: To evaluate the characteristics of thyroid cancer (TC) patients in regard to demographic distribution, histological variants, mode of presentation and modalities of diagnosis and treatment.
METHODS: We retrospectively audited the records of 97 consecutive cases with histologically proved thyroid cancer between 1997 and 2001 presenting to the Kuwait University Hospital, Sana'a, Yemen.
RESULTS: Patients with TC in this study comprise 17.7% of goiter patients who were admitted at the same period. Females constituted 89.7% (n=87), and males 10.3% (n=10). The average age of diagnosis was 38.4 years. More than two thirds were at the age of <40. Among patients with goiter, the percentage of carcinoma was higher in the following groups, males (37.9% versus 16.6%, p=0.028), patients aged >47 (25.8% versus 12.6%, p=0.001), patients with enlarged lymph nodes (9.3% versus 3.8%, p=0.020), and patients with recurrent disease after being operated for a presumably benign disease (8.2% versus 2.9%, p=0.012). The average period since patients noticed the swelling until seeking medical help was 4 years. Most patients (90%) came from highland areas. Multinodular swelling was the most common clinical finding (43.3%), and hoarseness was the most common symptom (17.5%). In histopathological examination, papillary carcinoma accounted for 93.8% of the cases and papillary microcarcinoma was found in 10 cases (10.3%). The papillary/follicular carcinoma ratio was 22:1. Hormone assay and ultrasonic imaging were the most commonly used investigations. Sub total thyroidectomy was the most common procedure used in treatment (39%). CONCLUSION: Not all histological variants of TC are represented in this study. Papillary carcinoma formed the bulk of TC cases. Salt iodization program might have an effect on the incidence of thyroid malignancy, and on the papillary/follicular carcinoma ratio. Better level of expertise is needed in the field of fine needle aspiration and ultrasonography. A consensus has to be reached, which is based on our environment and capabilities, where TC has to be managed aggressively by experienced surgeons. Yemen is in real need of a national cancer registry to assess the problem on a national level.
PMID: 14758381 [PubMed - in process]

YHMRJ August/2004
Diagnostic and therapeutic management of acute abdomen in
Hajah, Yemen] [Article in German]
Al-Gamrah A. Republikkrankenhaus Sanaa, Lehrkrankenhaus der Universitat Sanaa, Republik Jemen.
We report on the results of surgical treatment in 236 patients admitted with clinical signs of acute abdomen between the 1st of January 2000 and the 31st of December 2003 at the District Hospital of Hajah in northwest Yemen. Hajah, a city 2500 m above sea level, has 60,000 inhabitants and serves an area with 800,000 inhabitants. The hospital was funded by the Saudi Arabian government and built in 1997. Data on patients with acute abdominal pain were prospectively collected and analysed according to diagnosis, age, sex, and duration of symptoms. The most frequent cause was acute appendicitis, followed by incarcerated inguinal hernia. Complicated ulcer diseases of the upper gastrointestinal tract and gynaecological disorders were also frequently diagnosed. Gunshot wounds were the most frequent trauma. Despite the limited diagnostic equipment at the Hajah District Hospital and the short duration of hospital stay, there was no fatal event during the 1-year period analysed. The management of patients with acute abdominal pain and the ability to arrive at exact diagnosis is dependent on the availability of diagnostic means such as abdominal ultrasound and CT scan. However, especially in rural countries with only rudimentary technology, far more depends on the professional training and qualification of the surgeons responsible.
PMID: 15007526 [PubMed - as supplied by publisher]

YHMRJ August/2004
Trace metals in the brown mussel Perna perna from the coastal
waters off Yemen (Gulf of Aden): how concentrations are affected by weight, sex, and seasonal cycle.
Sokolowski A, Bawazir AS, Wolowicz M. Laboratory of Estuarine Ecology, Institute of Oceanography, University of Gdansk, Al. M. Pilsudskiego 46, 81-378 Gdynia, Poland. [email protected]
The effects of seasonal cycle, sex of individuals, and changes of soft tissues weight on accumulated trace metal concentrations (Cd, Cu, Fe, Mn, Pb, Zn) were examined in the brown mussel Perna perna collected monthly from a natural rocky habitat in the coastal waters off Yemen, the Gulf of Aden, for a period of ten months. Basic hydrological parameters were recorded simultaneously. All metals analyzed displayed seasonal fluctuations with different temporal patterns and variable amplitudes. Similar seasonal cycles were observed for Cu, Mn, and Pb with an increase in accumulated concentration during the rainy period (NE monsoon), and a decrease thereafter. The concentrations of Cu, Mn, and partially Pb appeared to be related to environmental changes, the concentration of Pb possibly also being related to changes in body weight. Accumulated concentrations of Cu and Mn thus seem to reflect actual metal bioavailability in the ecosystem quite efficiently. The tissue levels of Fe and Cd changed inversely to fluctuations in body weight with additional variation due to monsoon-related environmental changes. The behaviors of Fe and Cd are therefore driven by seasonally changing body weight with a considerable contribution of external factors including fluctuations in hydrological conditions and metal exposure. The Zn concentrations tended to increase gradually throughout most of the year regardless of its concentration in the environment. Zinc is considered to be mainly regulated by physiological mechanisms in the mussel, making its accumulated metal concentration independent to some degree of environmental levels. Significant differences in trace metal concentrations between sexes (in favour of females) might have resulted from more intense formation of reproductive tissues and metal accumulation in sexual products of females during the prespawning and spawning periods.
PMID: 15025166 [PubMed - indexed for MEDLINE]
YHMRJ August/2004
Validity of the self-report version of the strengths and difficulties
questionnaire in Yemen.
Almaqrami MH, Shuwail AY. Assistant Professor of Psychiatry, Faculty of Medicine, University of Dhmar, PO Box 20908, Republic of Yemen. Tel. +967 (1) 240368. Fax. +967 (1) 262426.
OBJECTIVE: The main objective of the study was to determine the validity of the Arabic version of the Strengths and Difficulties Questionnaire (SDQ) Self-Report version in Yemen.
METHODS: Following translation and back translation of the scale into the Arabic language by a panel of experts, psychometric properties were assessed using 600 students from schools (low risk group) and 57 patients attending the Mental Health Hospital in Sana'a, Republic of Yemen (high risk group) from January through to April 2002. The age range of the 2 groups was from 12-17-years-old. Discriminative validity, concurrent validity and factorial validity were studied.
RESULTS: The difference between the means of the "total difficulties"scores in both groups was highly significant (p<0.001); the area under the curve (AUC) of the total scores and subscales scores were ranged from 0.77-0.89. The chance corrected agreements between the clinical diagnosis and SRQ subscales' prediction were significant. The sensitivity and specificity were 72% and 55%. Factor analysis yielded 5 dimensions of emotional symptoms, conduct disorders, hyperactivity, peer problems, and pro-social items.
CONCLUSION: Results of this validation study suggest that the Arabic version of the SRQ of SDQ is valid in Yemen; and it can be a useful tool for investigating childhood behavioral and emotional disorders at clinical settings.
PMID: 15138526 [PubMed - in process]

YHMRJ August/2004
African links and hepatitis B virus genotypes in the Republic of
Yemen Talal A. Sallam(1), C.Y. William Tong(2,*)
1-Department of Microbiology, Faculty of Medicine and Health Sciences, Sana'a University, Sana'a, Republic of Yemen.
2-Department of Infectious Disease, GKT School of Medicine, King's College London and Department of Infection, Guy's and St. Thomas' Hospital Trust, London, United Kingdom, e-mail: C.Y. William Tong ([email protected])
*Correspondence to C.Y. William Tong, Department of Infection, 5th Floor North Wing, St. Thomas' Hospital, Lambeth Palace Road, London SE1 7EH, United Kingdom.
Funded by: Wellcome Trust Research Development Award in Tropical Medicine (to Dr. T.A. Sallam); Grant Number: 055648
Keywords
genotype A and D displacement human migration
Abstract:
Hepatitis B virus (HBV) genotypes in three different communities in the Republic of Yemen with and without significant African links were studied. The subjects included indigenous Yemeni blood donors (n = 987), Africans who had settled down in Yemen for several generations (n = 97) and Soqotrans living on an island in the Indian Ocean close to the African coast (n = 99). Phylogenetic analysis of HBV surface region sequences showed the presence of two major genotypes; A and D: sequences from the blood donors were all genotype D (17/17); those from Africans residing in Yemen were predominantly genotype D (7/8) although one sequence was genotype A; whereas a mixture of genotype A and D was found among the Soqotrans (5/8 and 3/8 respectively). Genotype A sequences were associated with higher viral load, but the difference was not statistically significant. Human migration and international travel, may lead to an interaction between HBV genotypes. The Republic of Yemen is at a location where genotypes A and D meet. The results from this study suggest that genotype A is found only in communities with continuing African links and that genotype D remains the dominant genotype in settled populations. More studies are needed to examine possible long-term changes in HBV genotypes in this region. J. Med. Virol. 73:23-28, 2004. © 2004 Wiley-Liss, Inc.
YHMRJ August/2004
Prevalence and elimination of cataract in a rural setting in Yemen
Volume 3, Issue 3, 1997, Page 408-414 H.R.H. Prince Abdul Aziz Bin Ahmed Bin Abdul Aziz Al-Saud, Mohamad N. Alamuddin and Adel A. Rushood
ABSTRACT A pilot observational study was conducted from 17 to 30 March 1996 in three locations in Yemen, namely Shabwa, Mukalla and Mahweet. The study population included 5341 people who came voluntarily to selected government hospitals for eye care. To determine the prevalence of the different eye diseases, especially cataract, among the study population, the team applied a case study form to collect the necessary data. The team examined patients and performed any surgery required. The findings are analysed, the limitations of the study discussed and recommendations formulated. Pr lence et mination de la cataracte en milieu rural au Y n Resume Une de d'observation pilote a r is au Y n du 17 au 30 mars 1996 dans trois localit
avoir Shabwa, Mukala et Mahweet. La population di comprenait 5341 personnes qui se sont pr nt
volontairement dans les h aux gouvernementaux s ctionn pour recevoir des soins ophtalmologiques. Afin de d rminer la pr lence des diff ntes affections oculaires et en particulier des cataractes dans la population di
l' ipe a utilis n formulaire d' de de cas pour recueillir les donn
n ssaires. Les membres de l' ipe ont examin es patients et ont pratiqu es interventions chirurgicales requises. Les r ltats ont
analys
les limites de cette de ont discut et des recommandations ont formul . Introduction
In collaboration with the Ministry of Health in Yemen, IMPACT/EMR launched a national programme for the prevention of blindness due to cataract in 1995. The elimination of the backlog of cataract in Yemen started in three locations, namely the cities of Shabwa, Mukalla and Mahweet. The objectives of the programme are:
To eliminate the backlog of cataract and at the same time address new cases.
To increase the number of ophthalmologists in Yemen by training local Yemeni doctors. For this purpose, a 12-month diploma course in ophthalmology has been initiated in collaboration with the World Health Organization (WHO). Fifteen doctors were enrolled in the 1996_1997 course and priority in selection was given to those from rural areas.
To bring ophthalmology care to remote areas by stipulating that Yemeni ophthalmologists trained through the programme serve a minimum of two years in remote villages where access to care is limited.
Methodology
A pilot observational study was launched in March 1996 in coordination with Al-Noor Caravan of Al-Basar International Foundation, which was established to

YHMRJ August/2004
develop, encourage and fund projects and programmes aimed at diagnosing, preventing and treating diseases of the visual system and reducing avoidable blindness. The Foundation arranged to send a team of ophthalmologists and other doctors to Yemen from 17 to 30 March 1996 in order to visit the three selected locations, examine the patients and perform the needed operations in the government hospitals in those areas. Objectives of the study
To determine the prevalence of the different eye diseases, especially cataract, among the study population.
To document the progress of the project in order to help in its evaluation and cost_effectiveness.
To help identify shortfalls/problems faced by the team so that they can be avoided in future endeavours.
Recruitment of patients
This was coordinated with the Director of Health, the Governor, the hospital manager and the representative of the charitable Ihsan Society in each of the targeted cities. The arrival of the team was announced in these cities and all persons with eye problems and/or those who suspected any eye problem were invited to attend the government hospital for diagnosis and treatment as needed. The duration of recruitment in each city did not exceed two days. Materials
The IMPACT/EMR project coordinator accompanied the team and, with the help of interviewers recruited from the local community of each city, arranged for the completion of a case study form for each patient seen by the team. The case study form collected the following information: 1) demographic information 2) general health record 3) basic eye examination 4) previous eye surgery 5) recommended action 6) surgery information Due to the large number of patients seen by the physicians, the interviewers were divided into three groups in order to complete the case study forms. The first group was responsible for collecting the demographic and general information about the patients before they were examined by the doctors. The second group, who accompanied the doctors during their examination of the patients, collected the medical information as advised by the doctors. The third group collected the surgery information from the doctors' medical cards. Study population
In all, 5341 people came voluntarily to the selected government hospitals for eye diagnosis and treatment during the stay of the Al-Noor Caravan of Al-Basar International Foundation in the three cities.

YHMRJ August/2004
Limitations of the study
The people seen by the team were those who were health aware and/or those suffering from eye problems. All of the patients came forward voluntarily and wanted to be diagnosed and if necessary treated by the ophthalmologists, especially as the service was provided free of charge. There was no way of telling if most of those who had eye problems in the targeted areas were informed of the service. For future action, it is imperative to document the procedure used to inform the population of the services of the team.
There was a lack of adequate communication between the team and the responsible persons in the selected locations, which resulted in insufficient preparation, such as recruitment of interviewers. In Mukalla, for example, the interviewers were recruited on the same day as the patients came to hospital, which did not allow for proper briefing. Furthermore, it was difficult to find a sufficient number of local interviewers with a good knowledge of English, which was essential for communication with the doctors. Therefore, the number of interviewers (9_11 interviewers in each location) was relatively small compared with the large number of patients seen by the doctors (about 100 patients per doctor per day, on average). This fact did not allow for proper completion of the case study forms, which later affected the quantity of data.
The case study form used did not match that used by the ophthalmologists and therefore could not be used by the interviewers as a substitute. Furthermore, when completing the examination cards the ophthalmologists used abbreviated medical terms not understood by the interviewers.
There were a few logistical problems that hampered the work of the team, such as frequent electricity failures which delayed the photocopying of the case study forms.
Results
Demographic characteristics of the patients The patients came from three locations: Shabwa 2131 (39.9%), Mukalla 1965 (36.8%) and Mahweet 1216 (22.8%); this information was missing for 29 patients. Most of the patients were 60 years and above and predominantly men (73.2%). The majority (67.6%) were married. There was a higher proportion of singles among males than females (24.6% versus 19.6%) and a higher proportion of "others" (divorced, widowed or separated) among females (14.3% versus 4.1%) (Table 1). With regard to educational status, 42.5% were found to be illiterate and only 6.1% held a university degree or higher (Table 2). However, the level of education differed substantially with sex. A higher percentage of males had had secondary and higher education than females (23.1% versus 6.3%) and a much lower percentage were illiterate (32.9%) compared with females (68.8%). Results showed that 95.5% of all employed patients in the study were males (compared to 73.2% in the total study group) (Table 3). Furthermore, 28.4% of all patients were employed, while 69.8% were not working. It is important to note that

YHMRJ August/2004
these "not working" cannot be classified as unemployed, since the technical term "unemployed" has certain characteristics such as age, for example, where the person has to be at least 15 years, and must be actively seeking employment. History of associated clinical conditions The most prevalent associated clinical condition reported was hypertension among the age group of 36_59 years (5.5%), followed by diabetes (3.4%) and heart problems (2.5%). It is important to bear in mind while interpreting these figures that the history of associated clinical conditions was identified through direct interviewing and not through clinical confirmation. Eye conditions and recommended action The distribution of eye diseases among the study population for each eye according to age is shown in Table 4.
The general prevalence of the different eye diseases among the study population was 15.3% in the right eye and 13.9% in the left eye. The most frequent eye disease in both eyes was lens opacity or cataract. Only 0.4% (n = 20) of the eye patients reported having previous eye surgery. Of these, only one case reported having previous lid surgery, while 17 cases reported having previous cataract surgery, the majority of whom were 60 years or more. There were two cases who had had glaucoma surgery; one in the under five years age group and one in the 60+ years age group. It was found that 40.7% of the patients needed some sort of intervention; 20.6% (n = 1101) of all cases in the study needed medical and/or surgical intervention for the right eye, while 20.1% (n = 1076) required similar interventions to alleviate visual problems in the left eye (Table 5). In total, 2177 different interventions (in both eyes) were recommended by the ophthalmologists for the survey sample. A total of 645 persons (12.1% of the total seen by the team) underwent eye surgery. The highest percentage needing operations was in Mahweet government hospital, where 15.3% of the patients seen by the team underwent eye surgery. Table 6
illustrates the distribution of patients who underwent eye surgery in each of the three hospitals according to age and location. The percentage of females who underwent surgery was much higher than males; 24% of female patients needed eye surgery compared with 7.6% of males.Table 7
shows the distribution of patients and surgeries performed by location. The majority of the patients (67.9%) who underwent surgery were in the 60+ years age group. Recommendations
The general prevalence of eye diseases among the study population was 15.3% in the right eye and 13.9% in the left eye. Lens opacity or cataract was found to be the most frequent eye disease in both eyes, representing 57.9% of the abnormalities detected in the left eye and 58.8% in the right eye. The majority (98.9%) of those who were found to be in need of surgical intervention were operated on by the eye team (652 recommended surgical interventions in comparison to 645 surgical operations performed).

YHMRJ August/2004
The limitations of this pilot observational study have to be taken into consideration while planning a programme at the national level. In particular, there is a need for accurate documentation of the following:
patient recruitment procedure
measurement and reporting of visual acuity
follow-up of patients after surgery to study the failure and success rate. For this purpose, it is imperative to:
Modify the case study form and include a part on visual acuity and another on follow-up procedures.
Unify and standardize the case study forms used by both the ophthalmologists and interviewers. The case study form can be completed in duplicate and a copy can be retained by the hospital for follow-up and a copy kept with the IMPACT/EMR coordinator in Yemen.
Train a sufficient number of interviewers, preferably health workers, before the commencement of a study.
YHMRJ August/2004
YHMRJ August/2004
YHMRJ August/2004

YHMRJ August/2004
Neglected Giant Basal cell Carcinoma in the FACE
CASE REPORT AND REVIEW OF LITERATURE
ABDUL RAHIM AL-SAMIE*
YASIN AL-QUBATI,*
Background:
There is an increased presentation (prevalence) of focally infiltrative giant basal cell carcinoma in the face. Objective:
This study and review of literature aimed to highlight on the consequences of neglected Basal Cell Carcinoma. Method:
Study of a case from Yemen with histopathologically had proven presenting an eleven-giant Basal cell carcinoma from the United States. Result: Socio-economic status of the patient and his family played important role in negligence of tiny asymptomatic basal cell carcinoma. Conclusion:
Health education to the public about a symptomatic basal cell carcinoma will raise the awareness and prevent the negligence and infiltration of basal cell carcinoma. Basal cell carcinoma (BCC) is a malignant tumor, which rarely metastasizes, composed of cells similar to those in the basal area of the epidermis and its appendages (1). Giant basal cell carcinomas are rare and preferentially located on the trunk (2). Giant BCC is usually defined as a tumor 10 cm or larger in diameter (3). This large tumor is a rare variant of the usually small, indolent, non-aggressive common BCC (2). These tumors represent 65% to 75% of all cutaneous neoplasms and are the most common cancer in whites (4) but there are considerable evidence that the incidence of BCC is underestimated and under reported (5). BCC is the commonest malignant tumor of the skin in white races (1) and the most common human malignancy (6). The cause of BCC is unknown, but exposure to ultra-violet energy is the most likely cause, because of this, about 75% of basal cells are found on the head and neck, with only about 10% found on the non-sun-exposed trunk (7). Most of these tumors are small easily treated skin lesions, which occur in sun-exposed skin, but early detection and treatment can reduce morbidity and offer substantial cure rate (8). 90% of all basal cell carcinomas are located on the face and forehead, but giant BCCs are rare and if it is presented, they are preferentially located on the trunk.
* Skin and Venereal Diseases Hospital, P.O.Box.No.55722, Taiz, Republic of Yemen

YHMRJ August/2004
CASE REPORT:-
A 45 years old fair skin man had a 10 x 12 cm ill-defined fungating giant ulcer destroying the upper lip, nose, both zygomas, right lower eye lid and extended to both right and left sides of lower lip and forehead with destruction of medial aspect of both right and left eyebrows (Fig 1). On admission, the mouth opening, nose and both eyelids were disappeared and replaced by a big hole outlined by the subcutaneous fat. Speech of the patient became unclear and very difficult. Feeding by mouth becomes not possible and feeding was only possible by a tube through the big hole of the cancer.
The patient had one-year history of bleeding before admission from the whole surface of the lesion aggravated by episodes of sneezing. The oro-pharyngeal veins are engorged and varicose. The liver was tender enlarged and iron deficiency
anaemia was associated. The history revealed long time of traditional healing trials, which include magic, herbal medicines, and mud all lead to infection and more complications. Strong offensive odor was recognized from distance. Consultation of a surgeon was obtained. The result of this consultation was that surgery is not possible and contraindicated due to difficulty related to the lesion and chemotherapy is also contraindicated due to liver problems. After 3 months of conservative treatment in the hospital, the family decided to discharge him. Four months after discharge the patient was passed away.
PATHOLOGICAL FINDINGS:
The patient presented with a history of 15 years duration during which two biopsies were taken. 1st biopsy was taken in Feb 1993 where an incision biopsy of 0.4 x 0.2 x 0.1 cm in size showed cancerous cells under the squamous epithelium, spindle in shape and well-differentiated. The 2nd biopsy was taken in May 1997 after the patient admitted into the Skin and Venereol disease hospital
Taiz. The biopsy sample was sent to the Dermatopathology of Armed Forces Institute of Pathology, Washington, it disclosed basal cell carcinoma, nodular and focally infiltrative type with positive margins.
DISCUSSION:
Low socio-economic status and low health awareness among the public resulted in complicated giant BCC. The people with giant lesion have no concern about their health and whenever the lesion starts to be giant, the patient start to feel shame to report to the medical care and seek treatment. The patient believe that since the traditional treatment trial didn t improve his condition, when the lesion is small, then nothing else would cure when it become big.
YHMRJ August/2004
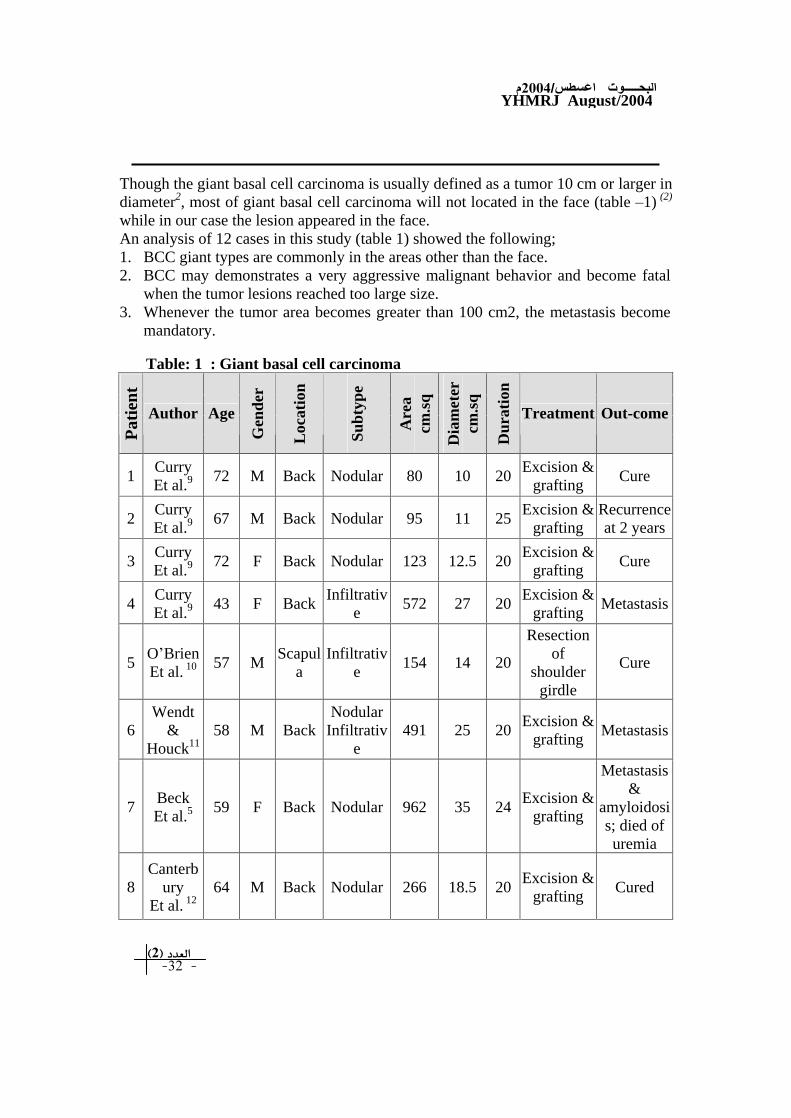
Though the giant basal cell carcinoma is usually defined as a tumor 10 cm or larger in diameter2, most of giant basal cell carcinoma will not located in the face (table 1) (2)
while in our case the lesion appeared in the face. An analysis of 12 cases in this study (table 1) showed the following; 1. BCC giant types are commonly in the areas other than the face. 2. BCC may demonstrates a very aggressive malignant behavior and become fatal
when the tumor lesions reached too large size. 3. Whenever the tumor area becomes greater than 100 cm2, the metastasis become
mandatory.
Table: 1 : Giant basal cell carcinoma
Pat
ient
Author
Age
Gen
der
Loc
atio
n
Subt
ype
Are
a cm
.sq
Dia
met
er
cm.s
q
Dur
atio
n
Treatment
Out-come
1
Curry Et al.9 72 M Back
Nodular
80 10 20 Excision &
grafting Cure
2
Curry Et al.9 67 M Back
Nodular
95 11 25 Excision &
grafting Recurrence at 2 years
3
Curry Et al.9 72 F Back
Nodular
123 12.5 20 Excision &
grafting Cure
4
Curry Et al.9 43 F Back
Infiltrative
572 27 20 Excision &
grafting Metastasis
5
O Brien
Et al. 10
57 M Scapul
a Infiltrativ
e 154 14 20
Resection of
shoulder girdle
Cure
6
Wendt &
Houck11
58 M Back
Nodular Infiltrativ
e 491 25 20
Excision & grafting
Metastasis
7
Beck Et al.5 59 F Back
Nodular
962 35 24 Excision &
grafting
Metastasis &
amyloidosis; died of uremia
8
Canterbury
Et al. 12
64 M Back
Nodular
266 18.5 20 Excision &
grafting Cured

YHMRJ August/2004
9
Mohs
Et al. 13
42 M
Abdomen
Infiltrative
82 10.5 20 Mohs
Micrographic surgery
Abdominal invasion &
death
10
William J.Et.al2
75 M Abdomen
Infiltrative
176 15 20 Radiation
Rupture of abdomen and death
11
William J.Et.al2
61 M Scapul
a
Nodular infiltrativ
e 80 10 30
Mohs Micrographic surgery
& flap
Cure
12
Current study
45 M Face
Nodular infiltrativ
e 120 15
Conservative
Metastasis and death
As the lesion in our patient is not well circumscribed as we calculated the involvement area using the formula h x w = cm2.
REFERENCES:
1. RONA M.MacKIE, Epidermal Skin Tumors, Text book of Dermatology vol.2, Six Ed.(1-3) Pg-1679.
2. William J.Sahl, Jr.MDa, Stephen N.Snw, MDb, and Normal S.Levine, MDc, Giant Basal Cell Carcinoma, Journal of the American Academy of Dermatology, 30 No.5 ; Part 2; 1994; Pg.856-859.
3. Braun-Falco O, Plewig G, Wolff HH, et al., eds. In Dermatology, New York: Springer-Verlag, 1991;1022.
4. Beck H, Anderson JA, Birkler NE, et al. Giant basal cell Carcinoma with metastasis and secondary amyloidosis: report of a case. Acta Derm Venereal (stockh) 1983;63;564
5. Pauer K, Poyzer, Barry N, et,al., the incidence of basal cell carcinoma and their metastasis in Australia and New Zealand. Australas J Dermatol. 1973;14;53-5.
6. Miller SJ. Biology of basal cell carcinoma (part I) JAM ACAD Dermatol. 1991;24:1-13. 7. Karjalainen S, Salo H, Tepp L.Basal Cell and Squamous cell carcinoma of the skin in
finland int. J Dermatol.1989; 28:445-50. 8. June K.Robinson, MD; Jeffrey S.Altman, MD; Alfred W. Rademaker, Phd.,
Socioeconomic status and Attitudes of 51 patients with giant basal and squamous cell carcinoma and paired controls, Arch Dermatol. 1995;131;428-431.
9. Curry MC, Montgomery H, Winklemann RK. Giant basal cell carcinoma. Arch Dermatol 1977;113:316.
10. O Brien CJ, Harvey KM, Harris JP, et al. Shoulder girdle resection for giant basal cell carcinoma. Br J Plast Surg 1984;37:566-8.
11. Wendt JR, Houck JP. A giant basal cell carcinoma with lymph node metastasis: a case report and review of the literature. Contemp Surg 1988;32:33-8.
12. Canterbury TDW, Wheeler WE, Madan E.Giant basal cell carcinoma of the back. W.V Med J 1990;86:291-3.
13. Mohs FE, Jones DL, Koranda FC. Microscopically controlled surgery for carcinomas in patients with nevoid basal cell carcinoma syndrome. Arch Dermatol 1980;116:777-88.