supplement to care m a n a g e d · supplement to advances in treatment and management of early...
TRANSCRIPT

S U P P L E M E N T T O
Advances in Treatment And Management Of Early Breast Cancer
HIGHLIGHTS
• Breast Cancer: An Overview of the Disease
• Advances in Systemic Treatment ofEarly Breast Cancer in Postmenopausal Women
• Managing Treatment of Early BreastCancer in Postmenopausal Patients:A Nurse Practitioner’s View
• A Medical Director’s Perspective On Early Breast Cancer
Volume 14, No. 12December 2005
SEPTEMBER 2005
M A N A G E D
CareCare
Sponsored by AstraZeneca Pharmaceuticals, LP

MANAGED CARE (ISSN 1062-3388) is published monthly by MediMedia USA Inc., 780 Township Line Road, Yardley, PA 19067.This is Vol. 14, No. 12. Periodicals postage paid at Morrisville, Pa., and at additional mailing offices. POSTMASTER: Send addresschanges to MANAGED CARE, 780 Township Line Road, Yardley, PA 19067. Price: $10 per copy, $93 per year in the United States;$120 per year elsewhere. E-mail: [email protected]. Phone: (267) 685-2788; fax (267) 685-2966; circulation inquiries (267) 685-2789. Copyright ©2005 MediMedia USA Inc.
EditorJOHN A. MARCILLE
Managing EditorFRANK DIAMOND
Senior Science EditorPAULA SIROIS
Associate EditorTONY BERBERABE
Senior Contributing EditorPATRICK MULLEN
Contributing editors to this supplementLINDA HULL FELCONE
JACK MCCAIN
LYDIA WITMAN
Design DirectorPHILIP DENLINGER
Editor, Custom Publications MediMedia Managed Markets PublishingMICHAEL D. DALZELL
Senior Editor, Custom PublicationsKATHERINE T. ADAMS
Group PublisherTIMOTHY P. SEARCH, RPH
Director of New ProductDevelopmentTIMOTHY J. STEZZI
Eastern Sales ManagerSCOTT MACDONALD
Midwest Sales ManagerTERRY HICKS
Director of Production ServicesWANETA PEART
Circulation ManagerJACQUELYN OTT

December 2005
Advances in Treatment and Management Of Early Breast Cancer
Opinions are those of the authors and do not necessarily reflect those of the institutions that em-ploy them, nor of MediMedia USA, or the publisher, editor, or editorial board.
Clinical judgment must guide each clinician in weighing the benefits of treatment against therisk of toxicity. Dosages, indications, and methods of use for products referred to in this supple-ment may reflect the clinical experience of the authors or may reflect the professional literature or other clinical sources and may not be the same as indicated on the approved package insert.Please consult the complete prescribing information on any products mentioned in this publica-tion. MediMedia USA assumes no liability for the information published herein.
Introduction ..........................................................................................................................3HARLAN A. LEVINE, MDChief Clinical Officer, UnitedHealth Group, Specialized Care ServicesGolden Valley, Minn.
Breast Cancer: An Overview of the Disease ..............................................................4JOHN E. PIPPEN JR., MDChairman, Breast Tumor Site Committee, Baylor-Sammons Cancer Center, DallasTexas Oncology, Dallas
Advances in Systemic Treatment Of Early Breast Cancer in Postmenopausal Women ...........................................10GENEROSA GRANA, MDDirector, Cancer Institute of New Jersey, Cooper Hospital, Camden, N.J.Associate Professor of Medicine, Division of Hematology and Oncology,
Robert Wood Johnson Medical School, Cooper Hospital/University Medical CenterAdjunct Assistant Professor, Coriell Institute for Medical Research, Camden, N.J.
Managing Treatment of Early Breast Cancer In Postmenopausal Patients: a Nurse Practitioner’s View................................16JUDITH K. MUCH, CRNP, AOCNP, APRN.BCOncology Nurse Practitioner, Integrated Oncology Care, Lehigh Valley HospitalAllentown, Pa.
A Medical Director’s Perspective on Early Breast Cancer.................................22HARLAN A. LEVINE, MDChief Clinical Officer, UnitedHealth Group, Specialized Care ServicesGolden Valley, Minn.
S U P P L E M E N T T O
M A N A G E D
CareCare

Breast cancer imposes a substantial burden on managed care or-ganizations and their individual members. As the US popula-tion ages, this burden is likely to increase. In this supplement,
two oncologists (Generosa Grana, MD, and John E. Pippen Jr., MD),an oncology nurse (Judith K. Much, CRNP, AOCNP, APRN.BC), andI (a medical director) share insights about the nature of the disease andstrategies to improve outcomes in patients with early-stage breastcancer.
It is incumbent on health plans to adopt a patient-centered approachto early breast cancer, focusing on those issues that are important tothe individual. Emphasis should be placed on early diagnosis, sensi-tivity to the wide range of emotions that patients experience on beingdiagnosed with breast cancer, appropriate treatment that conformswith the patient’s preferences, and efforts to reduce the risk of recur-rence.
Tamoxifen has been the mainstay of adjuvant drug treatment aimedat reducing the risk of recurrence, which is associated with increasedmorbidity, mortality, and cost. Yet, in light of the emergence of newinformation about the utility of aromatase inhibitors as adjuvanttherapy, such as that provided by the Arimidex, Tamoxifen, Alone orin Combination (ATAC) study (Howell 2005), oncologists may havemore options in the future. Early indications are that, in comparisonwith tamoxifen, aromatase inhibitors increase disease-free survival forpostmenopausal women with hormone receptor-positive early-stagebreast cancer, which represents the majority of cases. Oncologists andpatients should be heartened to know that their options for address-ing breast cancer recurrence are expanding.
It should be remembered, however, that drug therapy is just onecomponent among many in a comprehensive approach to breast can-cer management and treatment — and, as the article by Much makesclear, that the team of health care providers entrusted with deliveringcomprehensive care is headed by the patient.
ReferenceHowell A, Cuzick J, Baum M, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in
Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer.Lancet. 2005;365:60–62.
EARLY BREAST CANCER / MANAGED CARE 3
INTRODUCTIONHARLAN A. LEVINE, MD
Chief Clinical Officer, UnitedHealth Group, Specialized Care Services

Breast cancer is a malignant tumor that has devel-oped from cells in the breast and that can spreadto other areas of the body, such as the liver, skin,
bones, brain, or lungs. Survival, defined as alive and dis-ease-free at greater than 5 years from diagnosis, has im-proved in the past several decades (Jemal 2005) via bet-ter screening, earlier detection, and improved treatmentand monitoring (Elmore 2005). Nevertheless, instancesof some types of cancer, such as ductal carcinoma in situ(DCIS), have risen, most likely because increased routinescreening has led to increased detection of early-stagecancers (Huston 2005).
Among women, breast cancer is the second leadingcause of cancer deaths, after lung cancer. Breast cancer isalso the most common cancer in women after non-melanoma skin cancer. In the United States in 2005, anestimated 211,240 new cases of breast cancer will be di-agnosed in women, and an estimated 40,410 women willdie from the disease. Lifetime risk for a woman is 1 in 7(ACS 2005). The disease is most prevalent in NorthAmerica, closely followed by other developed countries;as countries develop, risk rises. Most notably, risk riseswith age; 80 percent of breast cancers occur in post-menopausal women. Inheritance of a faulty gene is thecause of only 5 percent to 10 percentof breast cancers (BCC 2005).
Men can also develop the disease,and account for 1 percent of all breastcancer diagnoses. In the United Statesin 2005, an estimated 460 men willdie from breast cancer (ACS 2005),and men with breast cancer have agreater chance of developing prostatecancer.
RISK FACTORSEach woman has a unique combi-
nation of risk factors for developingbreast cancer, and it is hard to predictwho will develop the disease. Risk fac-tors include sociodemographic, here-ditary, and physical conditions. Manywomen with hereditary potential (ie,strong family history of breast can-cer) do not develop the disease, andvice versa. Women who previously
have had breast cancer, particularly if they were diag-nosed at an early age, are at a greater risk of developingbreast and other cancers, specifically ovarian cancer.Studies suggest that early menarche, delayed or absentparity (childbearing), lack of breastfeeding, and delayedmenopause contribute to heightened estrogen levels,consequently increasing the risk of breast cancer. Thesehormonal conditions are common in women in devel-oped countries.
Age is the most significant risk factor, possibly be-cause of lifetime exposure to factors that increase dam-age to genetic material in the breast cell. Moderate riskfactors are shown in Table 1 and slight risk factors areshown in Table 2.
GENETICS OF BREAST CANCERWomen with a family history of breast cancer repre-
sent only 5 to 10 percent of all women with breast can-cer. While it is possible to inherit altered genes that in-crease the risk of cancer, all breast cancer is genetic in thesense that it arises from mutations of genetic material incell DNA (Blachford 2002). These mutations are causedby conditions internal and external to the body. For ex-ample, current and recent users of hormone replacement
4 MANAGED CARE / SUPPLEMENT
Breast Cancer: An Overview of the DiseaseJOHN E. PIPPEN JR., MDChairman, Breast Tumor Site Committee, Baylor-Sammons Cancer Center, DallasTexas Oncology, Dallas
TABLE 1 Moderate risk factors for developing breast cancer
• Increased age. About 77 percent of women diagnosed with breastcancer each year are over age 50, and almost half are age 65 andolder; increased risk with age is possibly from lifetime exposure tohormones.
• Direct family history. A first-degree relative (eg, mother or sister)with breast cancer, especially if the relative was diagnosed at a young age.
• Genetics. Carriers of mutations in one or both of the breast genesBRCA1 and BRCA2 account for 10 percent of breast cancer diagnoses;mutations in other genes (such as p53) also increase risk.
• Personal history of benign or cancerous breast disease. Benignbreast disorders, such as atypical hyperplasia and lobular carcinomain situ, increase the risk of developing breast cancer (Hartmann 2005),as does having had breast cancer previously.
• Postmenopausal breast density. High breast density after meno-pause increases risk.
SOURCE: ADAPTED FROM ACS 2003, 2005
EARLY BREAST CANCER / MANAGED CARE 5
therapy (HRT) are at increased risk for developing breastcancer, though the risk seems to return to that of thegeneral population within 5 years of stopping HRT (ACS2005). Table 3 lists known genetic mutations that conferan increased likelihood of developing breast cancer.
Oncogenes, or genes that promotecell division, encourage cancer when“turned on” by mutation, leading torapid cell replication in the host tissue.Tumor-suppressor genes, such as genesp53, BRCA1, and BRCA2, slow downcell division; mutations that “turn off”tumor-suppressor genes can be inher-ited or caused by external factors suchas viruses that have tumor suppressor-inactivating genes in their DNA.
Several genes that affect breast andovarian cancer risk are autosomal re-cessive, which means a woman will notdevelop breast cancer if she has inher-ited a normal version of the gene fromat least one parent. Nonetheless, evennormal genes can be damaged by envi-ronmental causes, ie, carcinogens, in-cluding:
• Tobacco products (eg, cigarettesand cigars)
• Pollutants: chemicals (eg, pesti-cides that act like estrogens)
• High-dose radiation
TYPES OF BREAST CANCERBreast cancer is classified by a woman’s menopausal
status, whether the cancer has spread, the size and loca-tion of the tumor, genetics, hormone receptor status ofthe tumor, and the nature of cell nuclei.
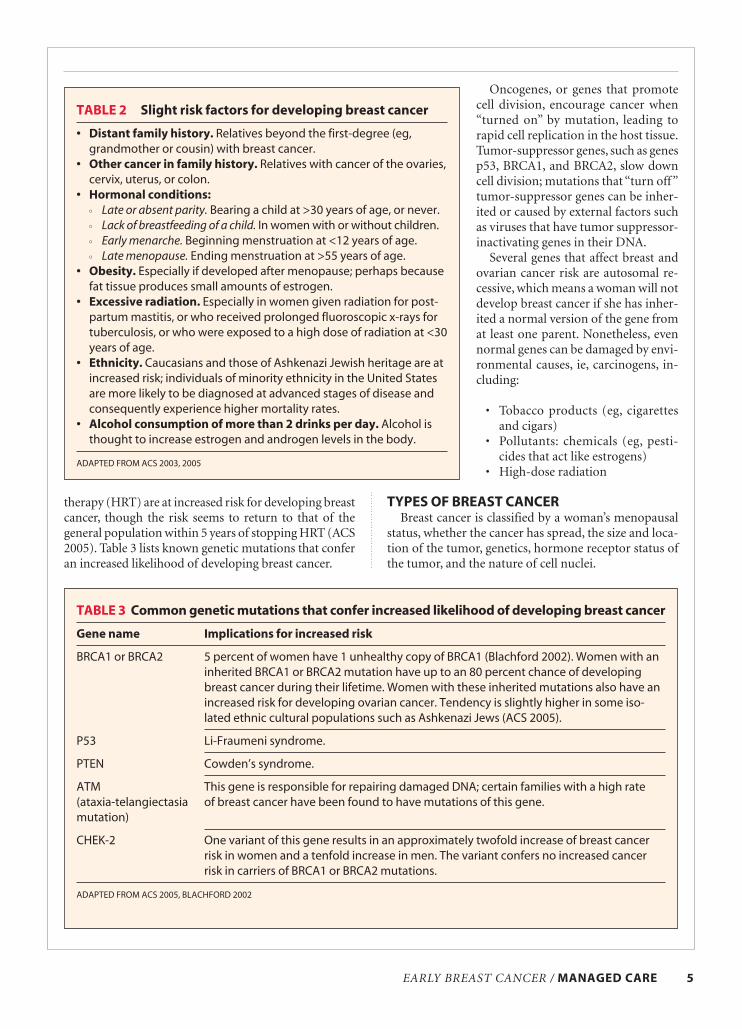
TABLE 2 Slight risk factors for developing breast cancer
• Distant family history. Relatives beyond the first-degree (eg,grandmother or cousin) with breast cancer.
• Other cancer in family history. Relatives with cancer of the ovaries,cervix, uterus, or colon.
• Hormonal conditions:
•• Late or absent parity. Bearing a child at >30 years of age, or never. •• Lack of breastfeeding of a child. In women with or without children.•• Early menarche. Beginning menstruation at <12 years of age.•• Late menopause. Ending menstruation at >55 years of age.
• Obesity. Especially if developed after menopause; perhaps becausefat tissue produces small amounts of estrogen.
• Excessive radiation. Especially in women given radiation for post-partum mastitis, or who received prolonged fluoroscopic x-rays for tuberculosis, or who were exposed to a high dose of radiation at <30years of age.
• Ethnicity. Caucasians and those of Ashkenazi Jewish heritage are atincreased risk; individuals of minority ethnicity in the United Statesare more likely to be diagnosed at advanced stages of disease andconsequently experience higher mortality rates.
• Alcohol consumption of more than 2 drinks per day. Alcohol isthought to increase estrogen and androgen levels in the body.
ADAPTED FROM ACS 2003, 2005
TABLE 3 Common genetic mutations that confer increased likelihood of developing breast cancer
Gene name Implications for increased risk
BRCA1 or BRCA2 5 percent of women have 1 unhealthy copy of BRCA1 (Blachford 2002). Women with aninherited BRCA1 or BRCA2 mutation have up to an 80 percent chance of developingbreast cancer during their lifetime. Women with these inherited mutations also have anincreased risk for developing ovarian cancer. Tendency is slightly higher in some iso-lated ethnic cultural populations such as Ashkenazi Jews (ACS 2005).
P53 Li-Fraumeni syndrome.
PTEN Cowden’s syndrome.
ATM This gene is responsible for repairing damaged DNA; certain families with a high rate (ataxia-telangiectasia of breast cancer have been found to have mutations of this gene.mutation)
CHEK-2 One variant of this gene results in an approximately twofold increase of breast cancerrisk in women and a tenfold increase in men. The variant confers no increased cancerrisk in carriers of BRCA1 or BRCA2 mutations.
ADAPTED FROM ACS 2005, BLACHFORD 2002

6 MANAGED CARE / SUPPLEMENT
Two noninvasive breast lesions include ductal carci-noma in situ (DCIS) — in ducts, and lobular carcinomain situ (LCIS) — in lobules (milk-producing glands).Table 4 describes the characteristics of DCIS and LCIS.Figures 1 and 2 show breast tissue and the common lo-cations of breast cancer.
The most common type of breast cancer is infiltrat-ing (invasive) ductal carcinoma (IDC), which originatesin a milk duct. A less common type of invasive canceroriginates in a breast lobule. Table 5 lists comparisons ofthese two types of invasive breast cancer.
Rare types of breast cancer, comprising less than 5percent of all breast cancers, include medullary carci-noma, Paget’s disease, inflammatory breast cancer, phyl-lodes tumor (rarely malignant), and tubular carcinoma.Table 6 lists tests used to diagnose the presence and typeof breast cancer.
DIAGNOSTIC METHODS AND PROGNOSTIC INDICATORS
Factors that affect prognosis are tumor size, location,stage, and molecular characteristics (eg, estrogen recep-tor, progesterone receptor, HER2/neu), histological char-acteristics, and patient characteristics (ie, age, meno-pausal status, and family genetic history).
Grading of an invasive cancer helps achieve a moreaccurate prognosis. Histologic tumor grade is based onthe arrangement of cancer cells in relation to each other,and how many of the cancer cells are in the process of di-viding (mitotic count).
Grade 1 (well-differentiated) cancers have relativelynormal-looking cells that do not appear to be grow-ing rapidly and are arranged in small tubules.
Grade 2 (moderately differentiated) cancers have fea-tures between grades 1 and 3.
Grade 3 (poorly differentiated) cancers, the highestgrade, lack normal features and tend to grow andspread more aggressively.
TABLE 4 Common breast adenocarcinomas (cancers in situ)
Name Characteristics
Ductal carcinoma in situ • Early form of noninvasive breast cancer.(DCIS) • Sometimes called intraductal or noninvasive.
• Localized inside milk ducts. • Cancer cells do not spread elsewhere in or beyond breast.• Diagnosed frequently by micro calcifications, usually by mammogram. • Has three grades (high, intermediate, low) based on microscopic exam of tissue.• Increase in grade value corresponds to likelihood of progression to invasive disease.
Lobular carcinoma in situ • Sometimes classified as a precancerous lesion, but more accurately, as a marker (LCIS) for increased risk for subsequent development of invasive cancer.(also called lobular • Originates in the lobule (milk-producing gland) and does not penetrate through neoplasia) the wall of the lobule.
• Women with this condition have a higher risk of developing an invasive breast cancer in the same breast or the other breast.
ADAPTED FROM ACS 2005
FIGURE 1 Cross-section of healthy breast tissue,depicting location of lobes, ducts, andaxillary nodes
SOURCE: NCI 2005
Lymph nodes
Lobules
Ducts
Nipple
Areola
Fat
Lobe
EARLY BREAST CANCER / MANAGED CARE 7
DCIS (noninvasive) cancer is sometimes given a “nu-clear grade”based on how abnormal the cancer cells are,and any presence of necrosis (dead or degenerating can-cer cells) also is noted (ACS 2005).
PREDICTIVE FACTORSMolecular characteristics of breast cancer serve as
both prognostic and predictive factors.
Estrogen and progesterone sensitivity are indicatedby the presence of receptors for these hormones. Tu-mors are referred to as ER positive (estrogen sensitive)or PR positive (progesterone sensitive), or simply hor-mone positive. Patients with hormone-positive tumorstend to have a better prognosis and are much more likelyto respond to hormone therapy (predictive for response)than women whose tumors lack these receptors.
Approximately one third of breast cancers have toomuch of a cell-growth-promoting protein called HER2/neu. HER2/neu-positive tumors have too many (morethan two) copies of the gene that instructs cells to pro-duce HER2/neu protein expressed on the surface of thecell. HER2/neu-positive tumors tend to grow and spreadmore aggressively than other breast cancers. HER2/neu-positive tumors respond better to anthracycline chemo-
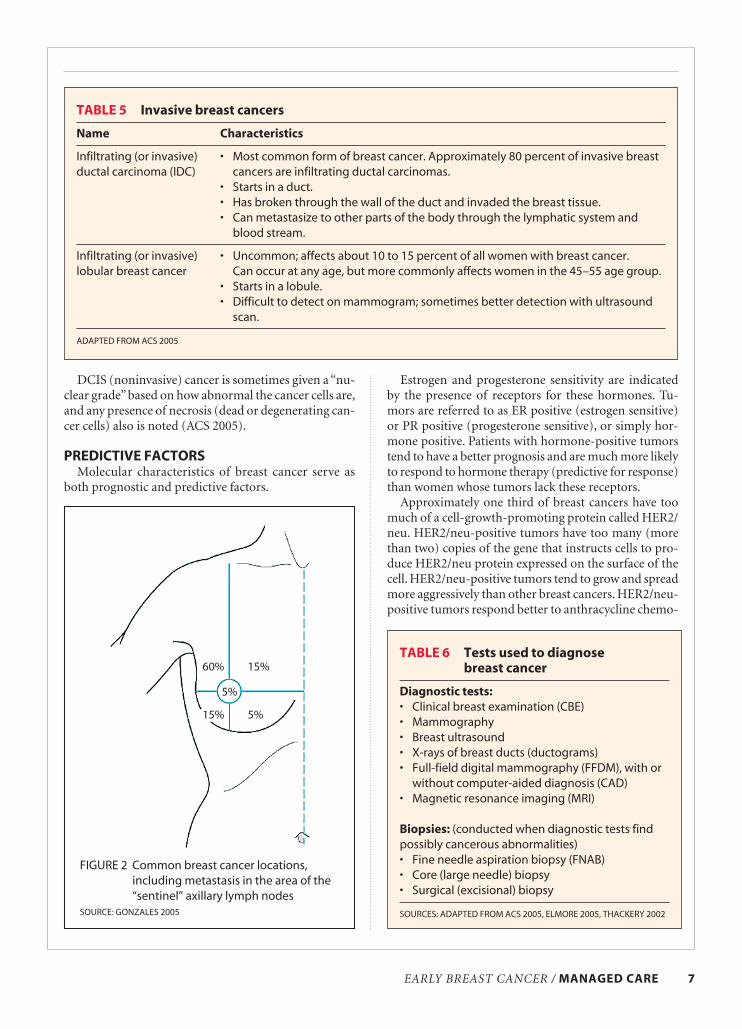
TABLE 6 Tests used to diagnose breast cancer
Diagnostic tests:
• Clinical breast examination (CBE)• Mammography• Breast ultrasound• X-rays of breast ducts (ductograms)• Full-field digital mammography (FFDM), with or
without computer-aided diagnosis (CAD)• Magnetic resonance imaging (MRI)
Biopsies: (conducted when diagnostic tests findpossibly cancerous abnormalities)• Fine needle aspiration biopsy (FNAB)• Core (large needle) biopsy• Surgical (excisional) biopsy
SOURCES: ADAPTED FROM ACS 2005, ELMORE 2005, THACKERY 2002
TABLE 5 Invasive breast cancers
Name Characteristics
Infiltrating (or invasive) • Most common form of breast cancer. Approximately 80 percent of invasive breast ductal carcinoma (IDC) cancers are infiltrating ductal carcinomas.
• Starts in a duct.• Has broken through the wall of the duct and invaded the breast tissue.• Can metastasize to other parts of the body through the lymphatic system and
blood stream.
Infiltrating (or invasive) • Uncommon; affects about 10 to 15 percent of all women with breast cancer.lobular breast cancer Can occur at any age, but more commonly affects women in the 45–55 age group.
• Starts in a lobule.• Difficult to detect on mammogram; sometimes better detection with ultrasound
scan.
ADAPTED FROM ACS 2005
FIGURE 2 Common breast cancer locations,including metastasis in the area of the“sentinel” axillary lymph nodes
SOURCE: GONZALES 2005
60% 15%
15% 5%
5%

8 MANAGED CARE / SUPPLEMENT
therapy drugs than HER2/neu-negative tumors,and also can be treated with trastuzumab — anantibody to the HER2 receptor that prevents theprotein from stimulating cell growth (JohnsHopkins 1998).
Other predictive tests evaluate the p53 tumor-suppressor gene, epidermal growth factor recep-tor, microvessel density (the number of smallblood vessels that supply oxygen and nutrition tothe cancer), genes that stimulate microvesselgrowth, and ploidy (number of sets of chromo-somes in a cell).
Combining prognostic and predictive infor-mation of the breast cancer informs treatmentchoices pertaining to adjuvant chemotherapy.Assessing the HER2/neu, ER/PR status, and pro-liferation rate helps classify the aggressiveness ofthe cancer and potential for metastasis.
STAGINGTypes of metastasis include regional (cancer
has spread into lymph nodes) and systemic (can-cer has spread to other parts of the body such aslungs, bones, liver, skin, and soft tissue). Breastcancer often progresses to become systemic earlyin the course of disease (Thackery 2002). Thepresence of cancer in lymph nodes, the numberof nodes affected, and tumor size are the best in-dicators of metastasis. Figures 1 and 2 show breasttissue and the common locations of cancer.
By the time it is noticed, a tumor is usually 1centimeter in size, has been growing for 1 to 5years, contains a billion cells, and may alreadyhave spread. Micrometastases are minute cancerdeposits in other organs and are hard to detect.The tests in Table 7 are used to detect metastasis.The extent of metastasis determines the stage ofcancer.
Staging is done after node status has been es-tablished by surgery and before administeringtreatment. Table 8 shows the five stages and theircharacteristics.
Assessment of a patient’s unique clinical situ-ation determines which adjuvant therapy is mostlikely to decrease the risk of recurrence, and includes con-sideration of age, general physical condition, and tumorcharacteristics.
LIVING WITH BREAST CANCERDuring treatment for breast cancer, patients experi-
ence a range of physical and emotional effects depend-ing on the treatment method. Most patients also expe-rience some degree of “posttreatment syndrome,”struggling with feelings of depression and confusion, asense of loss, fear of recurrence, and a desire to reengage
in their lives, living a healthier lifestyle physically andemotionally (Shockney 2002). The risk of recurrence isreduced by pharmaceutical and surgical treatments. Forindividuals at a high risk of developing breast cancer,either for the first time or a new primary, the risk/bene-fit of different preventive strategies is weighed. Preven-tive strategies include changes in diet, taking a medica-tion such as tamoxifen to prevent cancer development,an exercise program, prophylactic surgery (eg, mastec-tomy), and chemoprevention.
Breast cancer is a diverse disease among those who
TABLE 8 Pathologic stages of breast cancer
Stage Characteristics
0 Stage 0 is carcinoma in situ.I Stage l tumor is no larger than 2 centimeters (about 1
inch) and has not spread outside the breast.II Stage ll cancer meets 1 of the following 3 conditions:
tumor is no larger than 2 centimeters and has spread tosome lymph nodes in the armpit (axillary lymph nodes);tumor is between 2 and 5 centimeters (from 1 to 2inches) and may have spread to axillary lymph nodes;tumor is larger than 5 centimeters (2 inches) and has notgrown onto chest wall or spread to axillary lymph nodes.
III Stage lll is divided into stages lllA, lllB, and lllC. In lllA,the tumor is smaller than 5 centimeters (2 inches) andhas spread to internal mammary or axillary lymphnodes, or is larger than 5 centimeters (2 inches) and hasspread to internal mammary or axillary lymph nodes. InlllB, the tumor has grown onto structures near the breast(including skin, ribs, and muscles in the chest wall), andmay or may not appear in nodes. In lllC, the tumor is anysize and has spread to axillary nodes or to 1 or morelymph nodes near the collarbone, or to internal mam-mary lymph nodes that are enlarged because of the can-cer. The cancer has not spread to distant sites.
IV Stage lV cancer has tumors of any size and has spreadto distant sites in the body such as bones, lungs, liver,brain, or lymph nodes far from the breast.
SOURCES: ADAPTED FROM ACS 2005, BCO 2005, THACKERY 2002
TABLE 7 Imaging tests used to evaluate breastcancer stage (extent of metastasis)
• Chest x-ray• Bone scan• Computed tomography (CT)• Magnetic resonance imaging (MRI)• Positron emission tomography (PET)
SOURCE: ADAPTED FROM ACS 2005

develop it. Fortunately, survival rates have been improvedby increased awareness and education about the disease,including increased routine screenings. Our ability tocharacterize the clinical nature of tumor tissue and toclassify the type of disease also has extended disease-freeyears of life and has reduced mortality (Harvard Women’sHealth Watch 2004). Now, more than 90 percent of stageI patients and over 80 percent of stage II patients survive.Those with stage III cancer survive in about 50 percentof cases, and those with stage IV in 20 percent of cases(ACS 2005). Treatment advances are tending toward apreventive model, and improvements in general allowmore individualized diagnosis, prognosis, and treatment.
ReferencesACS (American Cancer Society). 2005. Detailed Guide. Breast
Cancer. American Cancer Society. Available at:«http://www.cancer.org/docroot/CRI/content/CRI_2_4_1X_What_is_breast_cancer_5.asp». AccessedSept. 6, 2005
ACS. Breast Cancer Facts & Figures 2003–2004. American CancerSociety. Atlanta: American Cancer Society. 2003.
BCC (Breast Cancer Care). Available at: «http://www.breastcancercare.org.uk/». Accessed Sept. 6, 2005.
BCO (Breast Cancer Organization). Available at:«http://www.breastcancer.org». Accessed Aug. 26, 2005.
Blachford SL, ed. Gale Encyclopedia of Genetic Disorders. BreastCancer. Farmington Hills, Mich: Gale Group. 2002:173–178.
Elmore JG, Armstrong K, Lehman CD, Fletcher SW. Screeningfor breast cancer. JAMA. 2005:293:1245–1256.
Gonzales R, Zeiger RF, Tierney LM Jr, et al, online eds. CurrentMedical Diagnosis and Treatment 2005. 44th ed. Availableat: «http://www.accessmedicine.com». McGraw Hill. 2005.Accessed Sept. 5, 2005.
Hartmann L, Sellers TA, Frost MH, et al. Benign breast diseaseand the risk of breast cancer. N Engl J Med. 2005;353:229–237.
Harvard Women’s Health Watch. Advances in early-stage breastcancer treatment. 12(2):1–3, 2004.
Huston TL, Simmons RM. Ablative therapies for the treatmentof malignant diseases of the breast. Am J Surg. 2005;189(6):694–701.
Jemal A, Murray T, Ward W. Cancer statistics, 2005. CA: A Can-cer Journal for Clinicians. 2005;55:10.
Johns Hopkins. Been Hearing About Herceptin? Here are theFacts. In Artemis: The Johns Hopkins Avon FoundationBreast Center Monthly Journal. October 1998. Available at:«http://www.hopkinsmedicine.org/breastcenter/artemis/199810/feature.html». Accessed Sept. 6, 2005.
NCI (National Cancer Institute). Available at: «http://www.cancer.gov/cancertopics/understanding-breast-changes».Accessed Sept. 6, 2005.
Shockney L. Preparing breast cancer patients for life after treat-ment — survivor retreats. In Artemis: the Johns HopkinsAvon Foundation Breast Center Monthly Journal. March2002. Available at: «http://www.hopkinsmedicine.org/breastcenter/artemis/200203/feature0.html». Accessed Sept.6, 2005.
Thackery E, ed. Gale Encyclopedia of Cancer. A Guide to Cancerand Its Treatment. Breast Cancer. Detroit: Gale Group.2002:142–151.
EARLY BREAST CANCER / MANAGED CARE 9

Early breast cancer is defined as cancer that can beremoved surgically and is confined to the breastand local and regional lymph nodes. Breast can-
cer is a particularly invasive cancer, and the cancer canbe bilateral and/or travel through the lymph or blood todistant sites; this risk is particularly prominent in thefirst decade after diagnosis, but it remains during the second decade (EBCTCG 2005). Mortality from breastcancer has fallen since the 1990s and continues to de-cline, largely because of earlier detection and treatmentadvances, including hormonal therapy, which came intogeneral use in the 1990s (ACS 2005). The mortality ratefrom breast cancer for middle-aged patients in theUnited States and the United Kingdom dropped by 25to 30 percent in the 1990s, despite rising incidence rates(EBCTCG 2005). For stage I and II breast cancer, chemo-therapy and hormonal therapy have been proven tolower the risk of recurrence and death. The challenge inoncology is tailoring the specific treatment to the patientas well as her disease characteristics and her overallhealth.
The Early Breast Cancer Trialists’ Collaborative Group(EBCTCG) was established in 1984 to pool data from allrandomized trials of early breast cancer. In its most recent analysis (results from the year 2000), it assessed cumulative 15-year recurrence and mortality rates fromtheir three earlier metaanalyses of nearly 150,000 pa-tients in 200 randomized trials of systemic adjunctivetherapy. Many of the trials had long-term follow-up pe-riods (EBCTCG 2005). When the authors analyzed the15-year survival benefits of chemotherapy and hormonaltherapy combinations, they found that the 15-year deathrate was cut in half among women with hormone re-ceptor (HR)-positive tumors treated with 6 months ofanthracycline-containing chemotherapy and 5 years oftamoxifen compared to patients treated with neither ofthe two, with survival gains increasing over the 15-yearanalysis span.
Specifically, anthracycline-based polychemotherapywith FAC or FEC regimens reduced the annual risk ofdeath by approximately 20 percent in women 50 to 69
years of age. For patients with HR-positive tumors, 5years of adjuvant tamoxifen reduced the annual breastcancer death rate by 31 percent in all age groups. The reductions were additive, so that in HR-positive women50 to 69 years of age who had been on an anthracycline-based chemotherapy regimen followed by 5 years oftamoxifen, the total risk reduction was 45 percent. Tras-tuzumab, too, has been shown to reduce recurrence riskby 52 percent after 3 years in HER2/neu-positive cancerswhen added to chemotherapy. This dramatic reductionled to a much improved survival rate at 4 years and a sig-nificant overall survival benefit (ASCO 2005).
All the major classes of adjuvant therapy — chemo-therapy, biologic therapy, and hormonal therapy — haveresulted in significant risk reductions for recurrence andmortality when used in appropriate patients. The chal-lenge for the clinician is to determine which patientsshould receive these agents as initial adjuvant therapy andwhether these agents should be used alone or in combi-nation — concurrently or sequentially.
PROGNOSIS OF BREAST CANCERThe first step in treating a breast cancer patient is to
determine the prognosis of the disease and, subsequently,to assess the specific effects of therapies. Many variablesaffect treatment decisions about whether to use chemo-therapy, hormonal treatments, or biologic treatment.Factors that specifically affect prognosis are tumor size,nodal status (whether and how many nodes are involved[captured in the staging of the cancer]), and histologicgrade (focusing on microscopic tumor characteristicsrelating to the organization of cells in the tumor tissuecompared with that of the local normal tissue). Other fac-tors that determine prognosis — and thus, treatmentchoice and chronology — are estrogen and progesteronereceptor status, HER-2/neu amplification, and the age ofthe patient.
A useful resource for adjuvant therapy decision mak-ing is a Web site housing an algorithm to predict re-currence risk: «www.adjuvantonline.com». This alsohelps clinicians to assess a patient’s prognosis and treat-
10 MANAGED CARE / SUPPLEMENT
Advances in Systemic Treatment of Early Breast Cancer in Postmenopausal WomenGENEROSA GRANA, MDDirector, Cancer Institute of New Jersey, Cooper Hospital, Camden, N.J.Associate Professor of Medicine, Division of Hematology and Oncology,
Robert Wood Johnson Medical School, Cooper Hospital/University Medical CenterAdjunct Assistant Professor at the Coriell Institute for Medical Research, Camden, N.J.

ment effectiveness in the context of available clinicaltrial data.
Other decision-making toolsGene expression-profiling tools are available commer-
cially, which may help the oncologist formulate a prog-nosis and support a treatment plan. Although these testsare not yet — and may never be — a sole indicator ofwhich categories of drugs to use, they are valuable whena physician is debating between two treatment courses.Tissue microarray profiling allows multigene screeningof the specific tumor to predict risk of metastasis and re-currence using a “recurrence score” (Paik 2004). Thistest can be performed on a small piece of paraffin-embedded tissue obtained from the initial diagnosticprocedure. Costing approximately $3,500, this test hasdemonstrated value in a select patient group — lymph-node negative, stage I or II, and hormone receptor-positive. Studies in broader subgroups of patients are on-going. In a case, for example, in which a woman has anode-negative, estrogen receptor-positive tumor under4 centimeters in size, genotyping can clarify prognosisand help with the decision of whether to use chemother-apy, hormone therapy, or both. Both the Oncotype DX21-gene array profile (Genomic Health) and the “Ams-terdam” technique, developed by the Netherlands Can-cer Institute, await broader testing (Bast 2004).
GUIDELINES FOR TREATMENTWithout guidelines and treatment algorithms, deci-
sion-making for adjuvant therapy would be difficult,and explaining options to a patient would be nearly im-possible. Up-to-date guidelines are available from the National Comprehensive Cancer Network; these guide-lines have reached a broad audience and have beenadopted by many clinicians (Bennett 2003). Future stud-ies will reveal whether the guidelines have resulted in improvements in the quality of medical care.
The goal of systemic therapy for early breast cancer is toeliminate microscopic disease known as micrometastases.Currently approved systemic therapy options include:
• Chemotherapy to kill rapidly dividing cancer cells • Hormonal therapy using a third-generation non-
steroidal aromatase inhibitor such as anastrozole orletrozole or the steroidal aromatase inhibitor exem-estane to block estrogen production, or using ta-moxifen to block the stimulatory effects of estrogenvia the estrogen receptor
ChemotherapyThe goal of chemotherapy is to prevent recurrences
and relapse with the fewest number of side effects, thegreatest degree of cost-effectiveness, and the highestquality of life. Typically, 4 to 6 cycles of chemotherapy are
given at 2- to 3-week intervals. Chemotherapy consistsprimarily of cytotoxins that kill the rapidly dividing cells;polychemotherapy has been demonstrated to substan-tially improve long-term relapse-free and overall survival,respectively, in premenopausal and postmenopausalwomen, up to age 70, who have node-positive and node-negative disease (EBCTCG 2005). Chemotherapeuticagents are administered along with various supportivetherapies such as antiemetics or growth factors.
In the EBCTCG’s recent metaanalysis (2005), a re-duced risk of recurrence and death was seen with the useof CMF (cyclophosphamide, methotrexate, fluorouracil)versus nil; use of an anthracycline-containing regimen in-creased the level of benefit. The taxanes (docetaxel andpaclitaxel) further add to the survival benefit. Generally,in women age 50 to 59, anthracycline-based chemother-apy reduced mortality by 20 percent. Unfortunately,there were not enough women over 70 years old includedto analyze the optimal chemotherapy regimen in thisage group.
Although the best combinations of adjuvant agents arebecoming clearer, thanks to large clinical studies andmetaanalyses, a breast cancer physician still needs to de-cide in whom to use chemotherapy and which specificagents to select for a given patient.
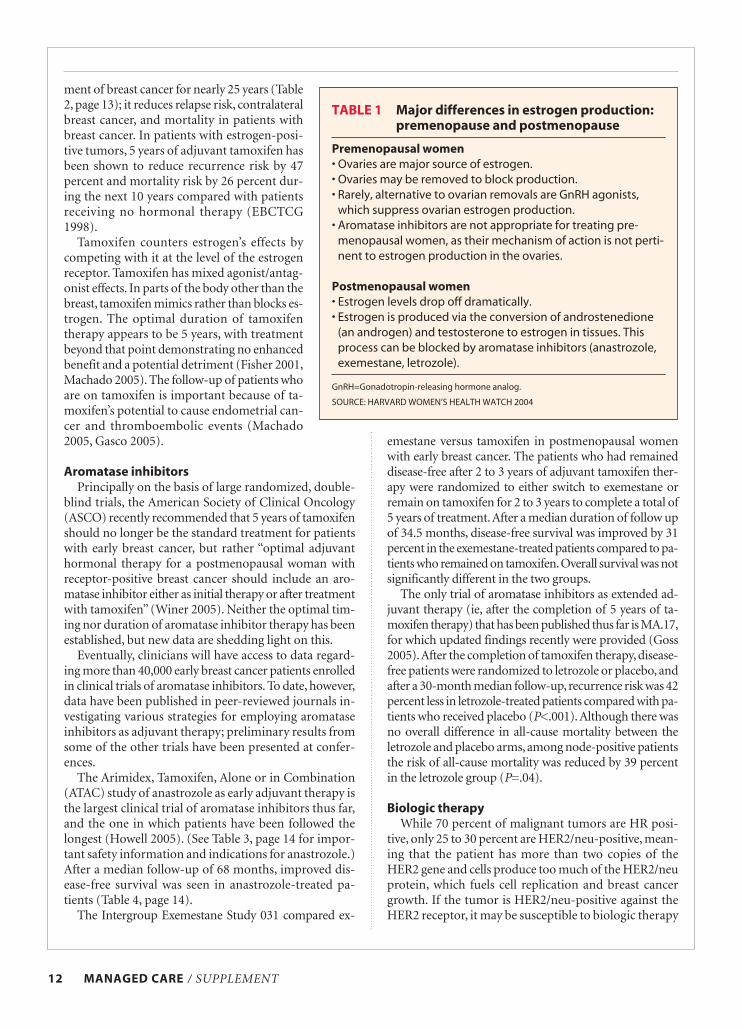
Hormonal therapyThe rationale for hormonal therapy is to deprive the
breast tumor of estrogen, which is implicated in tumorprogression. In premenopausal women, drugs such asluteinizing hormone-releasing hormone (LHRH) ago-nists or surgical removal of ovaries switch off the pro-duction of ovarian estrogens. Aromatase inhibitors,which block peripheral production of estrogen, are in-dicated only for postmenopausal women because of themechanism of action (Table 1, page 12). Tamoxifen, whichblocks binding of estrogen to the estrogen receptor, is ef-fective in premenopausal and postmenopausal women.
HORMONAL THERAPY: RECURRENCE ANDBREAST CANCER MORTALITY OUTCOMES
The use of chemoendocrine therapy has cut the annualdeath rate from estrogen-receptor positive breast cancerin half (EBCTCG 2005), even though many of these reg-imens included chemotherapy and hormonal regimensthat now are considered less than optimal. Nevertheless,one third of node-positive patients died of breast cancerduring the first, second, and third decade after diagno-sis (EBCTCG 2005). Research continues to determine thebest treatment sequence as well as the optimal hormonalagents to reduce this number further.
TamoxifenTamoxifen, a selective estrogen receptor modulator
(SERM), has been used as an adjuvant hormonal treat-
EARLY BREAST CANCER / MANAGED CARE 11
ment of breast cancer for nearly 25 years (Table2, page 13); it reduces relapse risk, contralateralbreast cancer, and mortality in patients withbreast cancer. In patients with estrogen-posi-tive tumors, 5 years of adjuvant tamoxifen hasbeen shown to reduce recurrence risk by 47percent and mortality risk by 26 percent dur-ing the next 10 years compared with patientsreceiving no hormonal therapy (EBCTCG1998).
Tamoxifen counters estrogen’s effects bycompeting with it at the level of the estrogenreceptor. Tamoxifen has mixed agonist/antag-onist effects. In parts of the body other than thebreast, tamoxifen mimics rather than blocks es-trogen. The optimal duration of tamoxifentherapy appears to be 5 years, with treatmentbeyond that point demonstrating no enhancedbenefit and a potential detriment (Fisher 2001,Machado 2005). The follow-up of patients whoare on tamoxifen is important because of ta-moxifen’s potential to cause endometrial can-cer and thromboembolic events (Machado2005, Gasco 2005).
Aromatase inhibitorsPrincipally on the basis of large randomized, double-
blind trials, the American Society of Clinical Oncology(ASCO) recently recommended that 5 years of tamoxifenshould no longer be the standard treatment for patientswith early breast cancer, but rather “optimal adjuvanthormonal therapy for a postmenopausal woman with receptor-positive breast cancer should include an aro-matase inhibitor either as initial therapy or after treatmentwith tamoxifen” (Winer 2005). Neither the optimal tim-ing nor duration of aromatase inhibitor therapy has beenestablished, but new data are shedding light on this.
Eventually, clinicians will have access to data regard-ing more than 40,000 early breast cancer patients enrolledin clinical trials of aromatase inhibitors. To date, however,data have been published in peer-reviewed journals in-vestigating various strategies for employing aromatase inhibitors as adjuvant therapy; preliminary results fromsome of the other trials have been presented at confer-ences.
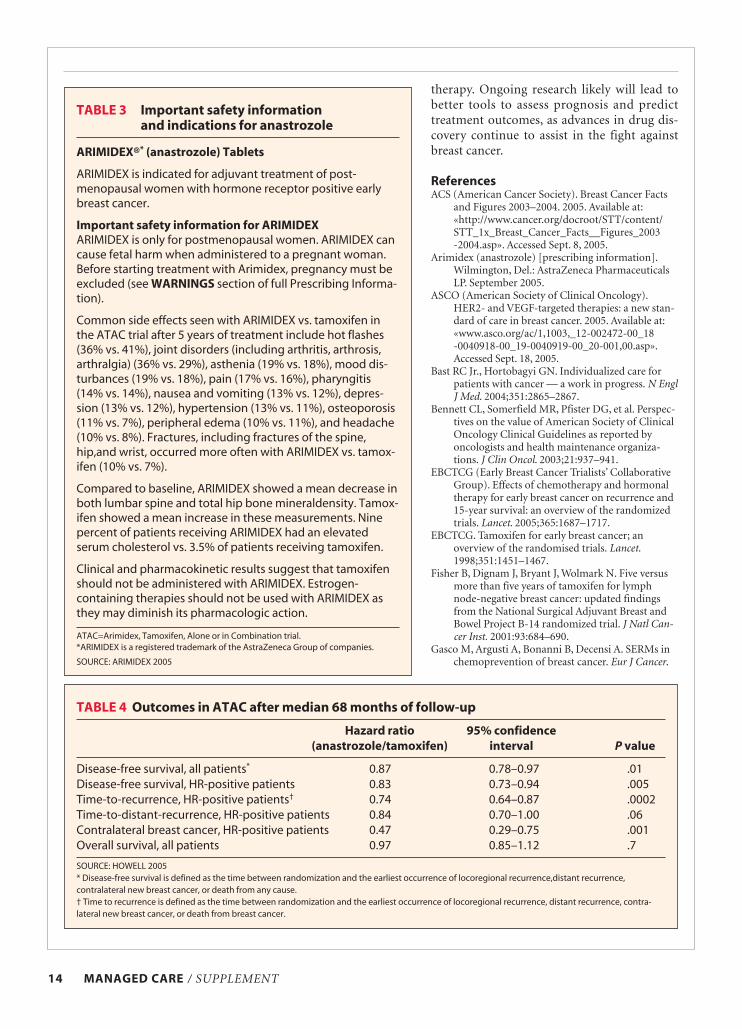
The Arimidex, Tamoxifen, Alone or in Combination(ATAC) study of anastrozole as early adjuvant therapy isthe largest clinical trial of aromatase inhibitors thus far,and the one in which patients have been followed thelongest (Howell 2005). (See Table 3, page 14 for impor-tant safety information and indications for anastrozole.)After a median follow-up of 68 months, improved dis-ease-free survival was seen in anastrozole-treated pa-tients (Table 4, page 14).
The Intergroup Exemestane Study 031 compared ex-
emestane versus tamoxifen in postmenopausal womenwith early breast cancer. The patients who had remaineddisease-free after 2 to 3 years of adjuvant tamoxifen ther-apy were randomized to either switch to exemestane or remain on tamoxifen for 2 to 3 years to complete a total of5 years of treatment.After a median duration of follow upof 34.5 months, disease-free survival was improved by 31percent in the exemestane-treated patients compared to pa-tients who remained on tamoxifen.Overall survival was notsignificantly different in the two groups.
The only trial of aromatase inhibitors as extended ad-juvant therapy (ie, after the completion of 5 years of ta-moxifen therapy) that has been published thus far is MA.17,for which updated findings recently were provided (Goss2005).After the completion of tamoxifen therapy,disease-free patients were randomized to letrozole or placebo, andafter a 30-month median follow-up,recurrence risk was 42percent less in letrozole-treated patients compared with pa-tients who received placebo (P<.001). Although there wasno overall difference in all-cause mortality between theletrozole and placebo arms, among node-positive patientsthe risk of all-cause mortality was reduced by 39 percentin the letrozole group (P=.04).
Biologic therapyWhile 70 percent of malignant tumors are HR posi-
tive, only 25 to 30 percent are HER2/neu-positive, mean-ing that the patient has more than two copies of theHER2 gene and cells produce too much of the HER2/neuprotein, which fuels cell replication and breast cancergrowth. If the tumor is HER2/neu-positive against theHER2 receptor, it may be susceptible to biologic therapy
12 MANAGED CARE / SUPPLEMENT
TABLE 1 Major differences in estrogen production:premenopause and postmenopause
Premenopausal women
• Ovaries are major source of estrogen.• Ovaries may be removed to block production. • Rarely, alternative to ovarian removals are GnRH agonists,
which suppress ovarian estrogen production. • Aromatase inhibitors are not appropriate for treating pre-
menopausal women, as their mechanism of action is not perti-nent to estrogen production in the ovaries.
Postmenopausal women
• Estrogen levels drop off dramatically.• Estrogen is produced via the conversion of androstenedione
(an androgen) and testosterone to estrogen in tissues. Thisprocess can be blocked by aromatase inhibitors (anastrozole,exemestane, letrozole).
GnRH=Gonadotropin-releasing hormone analog.
SOURCE: HARVARD WOMEN’S HEALTH WATCH 2004

that keeps HER2/neu from transmitting growth signalsto breast cancer cells.
There are encouraging early data from three adjuvanttrials among high-risk lymph node-negative patients andlymph node-positive patients, including a combinedanalysis of the North Central Cancer Treatment Group(NCCTG) N9831 and NSABP B-31.
CONCLUSIONAdvances in hormonal therapy, chemotherapy, and
ongoing research in biologic therapy have allowed clini-cians to evaluate a multipronged approach to loweringrisk of recurrence, greatly increasing disease-free survivalrates. Large clinical trials such as ATAC are helping to es-tablish the role of aromatase inhibitors in hormonal
EARLY BREAST CANCER / MANAGED CARE 13
TABLE 2 Tamoxifen “box” warning and indications
NOLVADEX®* (tamoxifen citrate) Tablets
Metastatic Breast Cancer: NOLVADEX is effective in the treatment of metastatic breast cancer in women andmen. In premenopausal women with metastatic breast cancer, NOLVADEX is an alternative to oophorectomy orovarian irradiation. Available evidence indicated that patients whose tumors are estrogen receptor positive aremore likely to benefit from NOLVADEX therapy.
Adjuvant Treatment of Breast Cancer: NOLVADEX is indicated for the treatment of node-positive breastcancer in postmenopausal women following total mastectomy or segmental mastectomy, axillary dissection,and breast irradiation.
NOLVADEX is indicated for the treatment of axillary node-negative breast cancer in women following totalmastectomy or segmental mastectomy, axillary dissection, and breast irradiation.
NOLVADEX reduces the occurrence of contralateral breast cancer in patients receiving adjuvant therapy withNOLVADEX for breast cancer.
Ductal Carcinoma in Situ (DCIS): In women with DCIS, following breast surgery and radiation, NOLVADEX is indicated to reduce the risk of invasive breast cancer. (See BOXED WARNING at the beginning of full PrescribingInformation.)
Reduction in Breast Cancer Incidence in High Risk Women: NOLVADEX is indicated to reduce the incidenceof breast cancer in women at high risk for breast cancer. NOLVADEX is indicated only for high-risk women. “Highrisk” is defined as women at least 35 years of age with a 5-year predicted risk of breast cancer ≥1.67%, as calcu-lated by the Gail Model. (See BOXED WARNING at the beginning of full Prescribing Information.)
Important Safety Information about NOLVADEX
WARNING - For Women with Ductal Carcinoma in Situ (DCIS) and Women at High Risk for Breast Cancer:
Serious and life-threatening events associated with NOLVADEX in the risk reduction setting (women at high riskfor cancer and women with DCIS) include uterine malignancies, stroke, and pulmonary embolism. Incidencerates for these events were estimated from the NSABP P-1 trial (see CLINICAL PHARMACOLOGY-Clinical Stud-
ies-Reduction in Breast Cancer Incidence in High-Risk Women). Uterine malignancies consist of both endo-metrial adenocarcinoma (incidence rate per 1,000 women-years of 2.20 for NOLVADEX vs. 0.71 for placebo) anduterine sarcoma (incidence rate per 1,000 women-years of 0.17 for NOLVADEX vs. 0.0 for placebo†). For stroke,the incidence rate per 1,000 women-years was 1.43 for NOLVADEX vs. 1.00 for placebo.‡ For pulmonary em-bolism, the incidence rate per 1,000 women-years was 0.75 for NOLVADEX vs. 0.25 for placebo.‡ Some of thestrokes, pulmonary emboli, and uterine malignancies were fatal. Health care providers should discuss the poten-tial benefits versus the potential risks of these serious events with women at high risk of breast cancer andwomen with DCIS considering NOLVADEX to reduce their risk of developing breast cancer. The benefits ofNOLVADEX outweigh its risks in women already diagnosed with breast cancer. Women who are pregnant or planto become pregnant should not take NOLVADEX.
When used to reduce the incidence of breast cancer in high-risk women or in women with DCIS, NOLVADEX iscontraindicated in women who require anticoagulant therapy or have a history of deep vein thrombosis or pul-monary emboli.
Cataracts and cataract surgery also occurred more frequently in clinical trials with NOLVADEX than placebo.The most frequently reported adverse reactions with NOLVADEX were hot flashes and vaginal discharge.
SOURCE: NOLVADEX 2005
*NOLVADEX is a registered trademark of the AstraZeneca Group of companies.
†Updated long-term follow-up data (median length of follow-up is 6.9 years) from NSABP P-1 study. See WARNINGS: Effects on the Uterus-
Endometrial Cancer and Uterine Sarcoma in NOLVADEX Prescribing Information.
‡See Table 3 under CLINICAL PHARMACOLOGY- Clinical Studies in NOLVADEX Prescribing Information.
therapy. Ongoing research likely will lead tobetter tools to assess prognosis and predicttreatment outcomes, as advances in drug dis-covery continue to assist in the fight againstbreast cancer.
ReferencesACS (American Cancer Society). Breast Cancer Facts
and Figures 2003–2004. 2005. Available at:«http://www.cancer.org/docroot/STT/content/STT_1x_Breast_Cancer_Facts__Figures_2003-2004.asp». Accessed Sept. 8, 2005.
Arimidex (anastrozole) [prescribing information].Wilmington, Del.: AstraZeneca PharmaceuticalsLP. September 2005.
ASCO (American Society of Clinical Oncology).HER2- and VEGF-targeted therapies: a new stan-dard of care in breast cancer. 2005. Available at:«www.asco.org/ac/1,1003,_12-002472-00_18-0040918-00_19-0040919-00_20-001,00.asp».Accessed Sept. 18, 2005.
Bast RC Jr., Hortobagyi GN. Individualized care forpatients with cancer — a work in progress. N EnglJ Med. 2004;351:2865–2867.
Bennett CL, Somerfield MR, Pfister DG, et al. Perspec-tives on the value of American Society of ClinicalOncology Clinical Guidelines as reported byoncologists and health maintenance organiza-tions. J Clin Oncol. 2003;21:937–941.
EBCTCG (Early Breast Cancer Trialists’ CollaborativeGroup). Effects of chemotherapy and hormonaltherapy for early breast cancer on recurrence and15-year survival: an overview of the randomizedtrials. Lancet. 2005;365:1687–1717.
EBCTCG. Tamoxifen for early breast cancer; anoverview of the randomised trials. Lancet.1998;351:1451–1467.
Fisher B, Dignam J, Bryant J, Wolmark N. Five versusmore than five years of tamoxifen for lymphnode-negative breast cancer: updated findingsfrom the National Surgical Adjuvant Breast andBowel Project B-14 randomized trial. J Natl Can-cer Inst. 2001:93:684–690.
Gasco M, Argusti A, Bonanni B, Decensi A. SERMs inchemoprevention of breast cancer. Eur J Cancer.
14 MANAGED CARE / SUPPLEMENT
TABLE 3 Important safety information and indications for anastrozole
ARIMIDEX®* (anastrozole) Tablets
ARIMIDEX is indicated for adjuvant treatment of post-menopausal women with hormone receptor positive earlybreast cancer.
Important safety information for ARIMIDEXARIMIDEX is only for postmenopausal women. ARIMIDEX cancause fetal harm when administered to a pregnant woman.Before starting treatment with Arimidex, pregnancy must beexcluded (see WARNINGS section of full Prescribing Informa-tion).
Common side effects seen with ARIMIDEX vs. tamoxifen inthe ATAC trial after 5 years of treatment include hot flashes(36% vs. 41%), joint disorders (including arthritis, arthrosis,arthralgia) (36% vs. 29%), asthenia (19% vs. 18%), mood dis-turbances (19% vs. 18%), pain (17% vs. 16%), pharyngitis(14% vs. 14%), nausea and vomiting (13% vs. 12%), depres-sion (13% vs. 12%), hypertension (13% vs. 11%), osteoporosis(11% vs. 7%), peripheral edema (10% vs. 11%), and headache(10% vs. 8%). Fractures, including fractures of the spine,hip,and wrist, occurred more often with ARIMIDEX vs. tamox-ifen (10% vs. 7%).
Compared to baseline, ARIMIDEX showed a mean decrease inboth lumbar spine and total hip bone mineraldensity. Tamox-ifen showed a mean increase in these measurements. Ninepercent of patients receiving ARIMIDEX had an elevatedserum cholesterol vs. 3.5% of patients receiving tamoxifen.
Clinical and pharmacokinetic results suggest that tamoxifenshould not be administered with ARIMIDEX. Estrogen-containing therapies should not be used with ARIMIDEX asthey may diminish its pharmacologic action.
ATAC=Arimidex, Tamoxifen, Alone or in Combination trial.*ARIMIDEX is a registered trademark of the AstraZeneca Group of companies.
SOURCE: ARIMIDEX 2005
TABLE 4 Outcomes in ATAC after median 68 months of follow-up
Hazard ratio 95% confidence
(anastrozole/tamoxifen) interval P value
Disease-free survival, all patients* 0.87 0.78–0.97 .01Disease-free survival, HR-positive patients 0.83 0.73–0.94 .005Time-to-recurrence, HR-positive patients† 0.74 0.64–0.87 .0002Time-to-distant-recurrence, HR-positive patients 0.84 0.70–1.00 .06Contralateral breast cancer, HR-positive patients 0.47 0.29–0.75 .001Overall survival, all patients 0.97 0.85–1.12 .7
SOURCE: HOWELL 2005* Disease-free survival is defined as the time between randomization and the earliest occurrence of locoregional recurrence,distant recurrence,contralateral new breast cancer, or death from any cause.† Time to recurrence is defined as the time between randomization and the earliest occurrence of locoregional recurrence, distant recurrence, contra-lateral new breast cancer, or death from breast cancer.
2005 Jun 15 [Epub ahead of print].Goss P, Ingle JN, Martino S, et al. Randomized trial of letrozole
following tamoxifen as extended adjuvant therapy in recep-tor-positive breast cancer: updated findings from NCICCTG MA.17. J Natl Can Inst. 2005;97:1262–1271.
Harvard Women’s Health Watch. Advances in early-stage breastcancer treatment. 2004;12:1–3.
Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arim-idex, Tamoxifen, Alone or in Combination) trial after com-pletion of 5 years’ adjuvant treatment for breast cancer.Lancet. 2005;365:60–62.
Machado F, Rodriguez JR, Leon JP, et al. Tamoxifen and en-
dometrial cancer. Is screening necessary? A review of the lit-erature. Eur J Gynaecol Oncol. 2005;26:257–265.
Nolvadex (tamoxifen) [prescribing information]. Wilmington,Del.: AstraZeneca Pharmaceuticals LP. March 2005.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recur-rence of tamoxifen-treated, node-negative breast cancer. NEngl J Med. 2004;351:2817–2826.
Winer EP, Hudis C, Burnstein HJ, et al. American Society ofClinical Oncology Technology Assessment on the use of ad-juvant therapy for postmenopausal women with hormone-receptor-positive breast cancer: Status Report, 2004. J ClinOncol. 2005;23:619–629.
EARLY BREAST CANCER / MANAGED CARE 15

16 MANAGED CARE / SUPPLEMENT
Breast cancer is a heterogeneous disease, necessi-tating individualized care. Most patients with early(operable) breast cancer, regardless of age or
menopausal status, are presented with a menu of optionsfor treatment, including surgery, radiation therapy,chemotherapy, and hormonal agents. The range ofchoices is overwhelming for most patients, and evenwith clear guidance, they continue to seek informationfrom the popular press, the Internet, family, and friends.Unless they happen to pick accurate sources, they can be-come confused about their prognosis and appropriatecare. Care of a breast cancer patient can be accomplishedoptimally through coordinated case management, coun-seling, and emotional and informational support. Thehealth care team provides its most valuable service by as-sisting patients in facing these difficult decisions, learn-ing to live with a cancer diagnosis, and by providingcomfort and support throughout diagnosis, treatment,and surveillance.
THE ONCOLOGY NURSE’S ROLEThe cancer care team comprises the primary care
physician, medical oncologist, radiation oncologist, sur-geon or surgical oncologist, pathologist, social worker,case manager, and the oncology nurse, with the lattersometimes spending the most time with the patient. Theoncology nurse thus is ideally positioned to provide aconsistent message over time by individualizing and co-ordinating care services.Yet, at the heart of nursing is theunderstanding that the patient and her family are thehead of this team.
The nurse’s duties depend on educational level andscope of practice. These duties can range from handlingcrises to routine care to telephone triage expeditingsymptom management. Maintaining the patient’s emo-tional well-being involves coaching her through anxietyand fear while making long-term plans to reduce heroverall health risk and minimize the disease’s psycho-social effects.
Nurses often can improve outcomes by informing de-cisions and reintegrating patients into the communityduring surveillance. Although the majority of relapses
occur within the first 5 posttreatment years, elevated re-currence risk persists for 20 years (Rosen 1993). Unfor-tunately, the recurrence risks and importance of propermedical surveillance must be made clear to the patientwhen she is trying to put the experience behind her. Pa-tients should be connected with educational resources re-garding recurrence risk and preventive measures, andthey may need to be reminded to continue medicationthroughout years of surveillance and monitoring. Oftenpatients believe “a pill” is not as strong or important asother medications used for cancer.
CONNECTING THE PATIENT WITH RESOURCES
An important role for the nurse is connecting patientswith resources. For example, if the patient cannot pay fora medication, a nonprofit organization such as theAmerican Cancer Society may be able to help. In addi-tion, each pharmaceutical company has its own patientassistance program (Table 1).
The office business staff or social worker usually man-ages reimbursement, but the nurse often must cope withclinical conflicts that arise from a patient’s inability to ob-tain a medication because it is not on formulary.A healthcare plan may cover a less-effective antinausea medica-tion but not a newer, more effective one. Similarly, theplan may pay for an Infusoport but not for maintenancesyringes or flushing units, meaning extra inconveniencefor patients who must return to the practitioner’s officeto flush the unit.
Payors sometimes follow Medicaid or Medicare for-mularies without researching the effect on patient care.Patients’ needs are highly individualized, while formu-laries are designed to standardize treatment. Oncologynurses often provide documentation to managed careformularies to provide “medical necessity” for off-formulary dispensing.
Emotional and spiritual support for patients who areliving with cancer can be achieved through family, sup-port groups, individual counseling, and religious orga-nizations. In the book The Anatomy of Hope, Groopmanilluminates ways to tell the truth without incurring de-
Managing Treatment of Early Breast Cancer In Postmenopausal Patients:A Nurse Practitioner’s ViewJUDITH K. MUCH, CRNP, AOCNP, APRN.BCOncology Nurse Practitioner, Integrated Oncology Care, Lehigh Valley Hospital, Allentown, Pa.

EARLY BREAST CANCER / MANAGED CARE 17
spair and to provide hope without misleading patients,arguing that hope has a biological healing effect.
With shorter postsurgery hospital stays, an increasedamount of early care after surgery falls on the patient’sfamily. Often, the caregiver needs emotional support.Books by caregivers and support groups have helpedothers cope when they find themselves to be caregiversovernight. Patient education and counseling are aided byorganizations, publications, and Web sites (Table 1).
During this time of decision-making, much care andsensitivity must be given to the patient. Sending the pa-tient to specific informational Web sites is preferable totheir surfing the Internet and finding disconcerting, con-tradictory, or confusing information that may not be pertinent to the patient’s clinical situation. It is impor-tant to tailor the information to the needs of the patient,depending on the patient’s educational level, culture, per-sonality type, and level of sophistication.Most patients will need additional infor-mation.When patients and their caregiversreceive feedback on their condition while ina state of high anxiety, they forget most ofwhat is said.
CLINICAL MANAGEMENTDiagnosis. Diagnosis of breast cancer is
made by fine needle aspiration, core nee-dle biopsy, stereotactic biopsy, needle, wirelocalization, or incisional or excisionalbiopsy. Management of breast cancer de-pends on the diagnosis: tumor size, lymphnode status, predictive/prognostic mark-ers (most importantly, estrogen receptor[ER] and progesterone receptor [PR] sta-tus and HER2/neu), menopausal status,and performance status.
During this most important time forthe patient, the nurse has a key role in ed-ucating the patient and family regardingthe techniques used for diagnosis: eg, whatto expect, how to prepare, and how tomanage discomfort or symptoms follow-ing diagnostic procedure. Following thediagnosis, the nurse guides the patientthrough interpretation of the operativeand pathologic findings, and helps to co-ordinate the next step in the process. Cer-tainly at this time, as at other key points inthe cancer care trajectory, clear, conciseexplanations are necessary, and the nurse’srole is pivotal in that respect.
Treatment. The role of nurses in man-aging women who are diagnosed withbreast cancer is well demonstrated in thetreatment of the elderly. Controversy per-
sists in the medical community over what constitutes ap-propriate care for the older postmenopausal womanwith breast cancer. While the mortality rate for breastcancer has declined for women under age 70, it has beensteady in women ages 70 to 79, and it has increased inwomen over age 80. This is likely to be related to under-treatment (Bouchardy 2003). Older women are perceivedas having less aggressive breast cancer than youngerwomen. Any comorbidities could make standard treat-ment challenging.
Oncology case management. In treating older womenwith breast cancer, the involvement of nurse case man-agers has resulted in improved management (Goodwin2003). Nurse case managers offer highly individualizedinteraction with the patient, sometimes extending tohome or hospital visits, accompanying her to the physi-cian and to other appointments, and speaking with her
TABLE 1 Patient resources
Web sites
• American Cancer Society «www.cancer.org»
• Dana Farber/Brigham and Women’s Cancer Center«www.brighamandwomens.org/bwhcancer/cancer»
• Look Good… Feel Better «www.lookgoodfeelbetter.org»
• National Cancer Institute «www.nci.nih.gov»
• National Coalition for Cancer Survivorship «www.cansearch.org»
• Susan G. Komen Breast Cancer Foundation «www.komen.org»
• Y-ME National Breast Cancer Organization «www.y-me.org»
Supportive/educational programs and products
• Breast Cancer Patient Education Service — AstraZeneca CancerSupport Network (1-866-99-AZCSN [1-866-992-9276])
• I Can Cope — educational program offered by American Cancer Society, with classes taught by health care professionals andother knowledgeable people about issues facing people withcancer (1-800-ACS-2345)
• Reach to Recovery — American Cancer Society program enlist-ing breast cancer survivors who serve as trained volunteers tosupport and comfort patients before, during, and after breast can-cer treatment, by phone or face to face (1-800-ACS-2345)
Products
• Look Good, Feel Better — a free, nonmedical, brand-neutral, national public service program to help women offset appear-ance-related changes from cancer treatment (1-800-395-LOOK)
• tlc (Tender Loving Care) — American Cancer Society Web siteoffering products for women diagnosed with or recovering frombreast cancer «www.tlccatalog.org/»
Prescription drug assistance programs
• PPA Rx – Partnership for Prescription Assistance — free/discount drug programs available in many states (1-800-ACS-2345)

18 MANAGED CARE / SUPPLEMENT
on the telephone, all with the intention of decreasing ser-vice fragmentation.
Patients who benefit most from a nurse case man-ager’s assistance are those facing multiple barriers to op-timal care, such as advanced age, chronic debilitatingconditions, cognitive impairment, low income, poor so-cial support (unmarried, living alone, or living with a frailspouse), and complex therapy involving multiple pro-viders. The nurse case manager does not recommend onetreatment over another but ensures that the patient isaware of all her options, that other members of the can-cer care team recognize special circumstances affectingtheir patient, and that the treatment chosen by the pa-tient is provided.
Local regional therapyIf the tumor is small, the patient may be offered
breast-conserving therapy (BCT) (lumpectomy plus ra-diation therapy). This is followed by hormonal manip-ulation if the tumor is ER positive. The 20-year follow-up of the National Surgical Adjuvant Breast and BowelProject (NSABP) B-06 randomized trial continues toshow equivalency of breast-conserving therapy andmodified radical mastectomy (Fisher 2002). Breast-conserving therapy, if feasible, is therefore the NationalCancer Institute’s currently recommended standard ofcare.
More conservative surgical evaluation of axillarylymph nodes via sentinel lymph node biopsy (SLNB)has led to less-intensive postoperative care. Many sur-geons have adopted SLNB as the standard of care, basedon preliminary interim analyses from studies showingthat short-term survival and recurrence rates are sim-ilar to those of traditional axillary lymph node dissec-tion (ALND). Long-term survival data are not yet avail-able.
If the tumor is large, a woman may elect to have ei-ther mastectomy or neoadjuvant therapy, in which thechemotherapy or hormonal therapy is given prior tosurgery to shrink the tumor to facilitate breast conser-vation. A lymph node dissection (either sentinel orcomplete) is conducted unless the woman is frail andelderly and the prognostic information gained by thelymph node surgery will not influence the treatmentplan. Tumor size and lymph node status dictate theneed for radiation, even if the woman proceeds to mas-tectomy.
Making a decision about surgery (lumpectomy plusradiation vs. mastectomy), with or without breast re-construction, raises many questions and necessitates co-ordination between the various practitioners, includingthe breast surgeon, plastic surgeon, and often the medi-cal oncologist. Patients with a strong family history ofbreast or ovarian cancer may need genetic counselingprior to surgery to determine the need for bilateral mas-
tectomy and to decrease the high risk of contralateralcancers.
The clinical sequelae of breast cancer surgery can in-clude changes in body image, sexual complications, painand numbness, shoulder dysfunction, and lymphedema.Clinical management of these sequelae includes coun-seling, arm exercises, elevation, and massage.
Radiation therapy New techniques in radiation therapy are aimed at
shortening treatment, thus minimizing toxicity (Keisch2005). Advances in whole-breast irradiation includehypofractionation and intensity-modulated radiationtherapy (IMRT). Hypofractionated doses have beenused once weekly in elderly women, predominantly toreduce local recurrence rates (Maher 1995, Ortholan2005).
Another advance in radiation therapy is acceleratedpartial breast irradiation (APBI), which uses either con-ventional external beam technique or brachytherapy toconcentrate the radiation on the local tumor bed wheremost local recurrences occur. Early results are promising,but data are short-term and confirmatory clinical trialsare continuing. Three-dimensional conformal radiationtherapy (3DCRT) is a less invasive form of APBI that focuses on a limited portion of the breast, causing lessdamage to surrounding tissue.
Radiation therapy can cause lymphedema, skinchanges, and sensory changes. Management of radia-tion damage includes acute and long-term effects.Nurses help by advising on symptom-specific mea-sures. Radiation treatment for breast cancer does notcause nausea or taste changes. If skin irritation devel-ops as a reaction to radiation, advice can be given toavert further trauma.
Systemic therapyFollowing surgery, many patients will be offered
chemotherapy, hormone therapy, or both to reduce therisk of recurrence. The type of adjuvant chemotherapy de-pends on life expectancy, comorbid conditions, molecularcharacteristics of the tumor (ER, PR, HER2/neu status),and the risk/benefit ratio of giving the treatment.
Tamoxifen’s standing as the preeminent hormonetherapy is being challenged (in postmenopausal, ER-positive patients) by the newer, third-generation aro-matase inhibitors (AIs) — anastrozole, exemestane, andletrozole.
ChemotherapyIn the United States, adjuvant chemotherapy is stan-
dard care for node-positive breast cancer. Many combi-nations of agents are used for chemotherapy, and po-tential side effects from each combination vary. Also,each drug affects patients differently, and the same pa-

EARLY BREAST CANCER / MANAGED CARE 19
tient can undergo chemotherapy with variable adverseeffects after each cycle.
Some side effects are universal for cancer chemother-apy. The most common problem is fatigue, which canlead to dizziness and falls. It is important to evaluate theetiology of fatigue, eg, if the fatigue is a result of anemia,then intervention is possible. Neutropenia is the most se-rious adverse effect of cytotoxic chemotherapy becauseit increases the patient’s risk of fever and life-threateninginfections. Prior to the onset of chemotherapy-inducedneutropenia, prophylactic administration of hematopoi-etic growth factors should be considered for elderly pa-tients or when high-risk regimens (eg, TAC) are em-ployed.
Advice on sleep, diet, and exercise can help preventdizziness and falls in the very compromised elderly pa-tient. Although practitioners once advised patients torest whenever fatigued from chemotherapy, we nowknow that exercise helps decrease fatigue and other sideeffects while increasing the patient’s psychological well-being (Mock 2001).
Patients with cancer often have anemia, as a conse-quence of the cancer or chemotherapy, or both (Groop-man 1999). Anemia may cause extreme weakness,dyspnea on exertion, pale skin, headache, loss of con-centration, and difficulty sleeping. Anemia often can bemanaged by weekly subcutaneous injections of erythro-poietin.
Alopecia. Hair loss (alopecia) is an ef-fect of chemotherapy’s attack on rapidlyreplicating cells, such as those in hair fol-licles or bone marrow. This effect, too, ishighly variable: One patient can keep herhair while another can lose it all after thefirst dose of chemotherapy. This gener-ally happens when a patient receives an-thracycline-based chemotherapy; hair lossusually occurs about 14 days after thetreatment and can start slowly and con-tinue to total baldness. Although alopeciais not serious clinically, it is an emotion-ally devastating side effect of chemother-apy. Careful counseling regarding the tim-ing of hair loss can help a patient prepareto buy a wig that is similar to her naturalhair before the hair comes out.
Other chemotherapy side effects. Nau-sea and vomiting are among chemother-apy’s most disturbing side effects.Chemotherapy regimens are classified bytheir emetic potential; based on that clas-sification and taking into account patientrisk factors for nausea/vomiting, an anti-nausea regimen can be tailored. Patientsand families need to be informed as to
which antinausea drugs can be used on an as-neededbasis and which must be given around the clock. Bowelchanges generally can be managed with over-the-counter preparations, but the clinician should instructthe patient on their use. Finally, studies have shown thatcognitive dysfunction associated with chemotherapy,popularly known as “chemo brain,” does exist (Tannock2004). In controlled studies of patients with breast can-cer, rates of cognitive dysfunction ranged from 16 to 50percent.
Hormonal therapiesHormonal therapies, which are aimed at reducing risk
of recurrence of breast cancer in the hope of reducingmorbidity and mortality, have different adverse effectprofiles. The adverse effects associated with hormonetherapies should be managed by weighing individualrisk factors. Oncology nurses should be equipped to dis-cuss with the patient the risks and benefits of each ther-apy when it is being considered and after treatment ini-tiation to improve treatment adherence and to minimizethe consequences of potential adverse effects.
Unlike the antiestrogen tamoxifen, aromatase in-hibitors have no partial agonistic effects on the estrogenreceptor and thus are less likely to be associated withestrogenic side effects but more likely to be associatedwith side effects against which estrogen is thought to be
TABLE 2 Adverse events (%) in Arimidex, Tamoxifen,Alone or in Combination (ATAC) trial
Anastrozole Tamoxifen
(n=3092) (n=3094)
Hot flashes 36 41Joint symptoms, including joint
disorder, arthritis, arthrosis, and arthralgia 36 29
Fatigue/asthenia 19 18Mood disturbances 19 18Nausea and vomiting 13 12Fractures, all 10 7
Spine, hip, or wrist 4 3Wrist/Colles 2 2Hip 1 1Spine 1 1
Vaginal bleeding 5 10Ischemic cardiovascular disease 4 3Vaginal discharge 4 13Ischemic cerebrovascular disease 3 3Venous thromboembolic events 3 5
Deep vein thrombosis 2 2Endometrial cancer 0.2 0.6
SOURCE: ARIMIDEX 2005

20 MANAGED CARE / SUPPLEMENT
protective. Thus, during 68 months of follow-up in a trialcomparing tamoxifen and anastrozole, adverse events(Table 2, page 19) that were more likely to be experiencedby tamoxifen-treated patients were endometrial cancer,ischemic cerebrovascular disease, venous thromboticevents, deep vein thrombosis, hot flashes, vaginal bleed-ing, and vaginal discharge, while adverse events morelikely to be experienced by anastrozole-treated patientsincluded fractures of the hip, wrist, and spine, and jointsymptoms such as arthritis, arthrosis, and arthralgia(Arimidex 2005).
All postmenopausal women should have a bone min-eral density (BMD) scan performed with dual-energy x-ray absorptiometry (DEXA) to determine baselineBMD, as well as follow-up DEXA scans periodically tomonitor bone loss. Women must be advised to immedi-ately report any vaginal bleeding for prompt investiga-tion by the primary practitioner or gynecologist. Routinetransvaginal ultrasounds are not necessary to measureendometrial thickness because, unlike postmenopausalbleeding, it is not a predictor of endometrial cancer andfrequently leads to unnecessary biopsies.
Reports about patients’ compliance with AI treatmentin community settings have not yet been published, buta few studies about adherence to adjuvant tamoxifentherapy are available. Although compliance with ta-moxifen therapy in such settings has been found to bebetter than compliance with other drug treatments forother chronic conditions (Partridge 2003), compliancewith tamoxifen therapy is not optimal. In a community-based study of women newly diagnosed with stage I orstage II breast cancer, 15 percent discontinued tamoxifenafter about 2 years of follow-up (Demissie 2001). In thisstudy, women who reported side effects were more likelyto discontinue tamoxifen, but side effects were morelikely to be reported by women whose emotional healthwas worse at baseline and by patients younger than age75. In addition, this study highlighted the importance ofeffective communication, as patients’ confidence in theirabilities to communicate with their physicians was asso-ciated with increased compliance.
To probe more deeply into the reasons for tamoxifendiscontinuance, patients’ beliefs about the risks andbenefits of tamoxifen therapy were studied (Fink 2004).This study enrolled women with newly diagnosed ER-positive breast cancer. During 2 years of follow-up, theprevalence of discontinuance was 21 percent, with themajority of those who stopped taking tamoxifen doingso during the first year. A patient’s age, the complexityof the medication regimen, and side effects were not as-sociated with discontinuation of tamoxifen therapy.Rather, the predictors of tamoxifen discontinuance werehaving four or more positive lymph nodes (relative risk,2.5 compared with no positive nodes), and holding neu-tral or negative beliefs about the risks and benefits of ta-
moxifen therapy (relative risk, 3.0 compared with pos-itive beliefs).
Taken together, these findings suggest an importantrole for the nurse oncologist in enhancing rates of com-pliance with hormone therapy (by being attentive to thepatient’s emotional state), in educating patients about theimportance of adjuvant therapy and its role in reducingrecurrence risk, and in facilitating effective communica-tion between the patient and other members of the can-cer care team.
Patients should be instructed to call their practitionerif they decide to stop hormonal medication. Further,they need to let their practitioner know if they are to behospitalized, particularly when on tamoxifen. Because ofincreased risk of thromboembolic events, tamoxifenshould be stopped if a person is bedridden.
CONCLUSIONThe oncology nurse is a pivotal member of the breast
cancer care team. Acting as an educator, counselor, me-diator, and advocate, the oncology nurse is well posi-tioned to help a patient cope with the wide-ranging im-plications of a breast cancer diagnosis, the vagaries oftreatment, and the vigilance and long-term interven-tions required thereafter to reduce the risk of recur-rence. By integrating care, linking patients to the manycancer resources, and engaging families in cancer careteams, nurses can improve outcomes for breast cancer.The experience for the patient and the managed care or-ganization can be optimized by keeping care as seam-less as possible and sensitively informing the patient ofthe rationale, risks, and benefits of treatment and moni-toring.
References Arimidex (anastrozole) [prescribing information]. Wilming-
ton, Del.: AstraZeneca Pharmaceuticals LP. September2005.
Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatmentstrongly decreases prognosis of breast cancer in elderlywomen. J Clin Oncol. 2003;21:3580–3587. Epub 2003 Aug 11.
Demissie S, Silliman RA, Lash TL. Adjuvant tamoxifen: predic-tors of use, side effects, and discontinuation in olderwomen. J Clin Oncol. 2001;19:322–388.
Fink AK, Gurwitz J, Rakowski W, et al. Patient beliefs and tamox-ifen discontinuance in older women with estrogen recep-tor-positive breast cancer. J Clin Oncol. 2004;22:3309–3315.
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of arandomized trial comparing total mastectomy, lumpec-tomy, and lumpectomy plus irradiation for the treatmentof invasive breast cancer. N Engl J Med. 2002;347:1233–1241.
Goodwin JS, Satish S, Anderson ET, et al. Effect of nurse casemanagement on the treatment of older women with breastcancer. J Am Geriatr Soc. 2003;51:1252–1259.
Groopman JE, Itri LM. Chemotherapy-induced anemia inadults: incidence and treatment. J Natl Cancer Inst. 1999;91:1616–1634.

EARLY BREAST CANCER / MANAGED CARE 21
Keisch M, Vicini F. Applying innovations in surgical and radia-tion oncology to breast conservation therapy. Breast J.2005;11(suppl 1):S24–S29.
Maher M, Campana F, Mosseri V, et al. Breast cancer in elderlywomen: a retrospective analysis of combined treatmentwith tamoxifen and once-weekly irradiation. Int J RadiatOncol Biol Phys. 1995;31:783–789.
Mock V, Pickett M, Ropka ME, et al. Fatigue and quality of lifeoutcomes of exercise during cancer treatment. CancerPract. 2001;9:119–127.
Ortholan C, Hannoun-Levi JM, Ferrero JM, et al. Long-term re-sults of adjuvant hypofractionated radiotherapy for breast
cancer in elderly patients. Int J Radiat Oncol Biol Phys.2005;61:154–162.
Partridge AH, Wang PS, Winer EP, Avorn J. Nonadherence toadjuvant tamoxifen therapy in women with primary breastcancer. J Clin Oncol. 2003;21:602–606.
Rosen PP, Groshen S, Kinne DW, Norton L. Factors influencingprognosis in node-negative breast carcinoma: analysis of767 T1N0M0/T2N0M0 patients with long-term follow-up.J Clin Oncol. 1993;11:2090–2100.
Tannock IF, Ahles TA, Ganz PA, van Dam FS. Cognitive impair-ment associated with chemotherapy for cancer: report of aworkshop. J Clin Oncol. 2004;22:2233–2239.

22 MANAGED CARE / SUPPLEMENT
The mountains of statistics with which medical di-rectors necessarily concern themselves on a dailybasis tend to conceal the fact that all the abstract
data points ultimately represent real people with veryreal hopes and fears. Fear, more than hope, is foremostin the mind of a woman with newly diagnosed breastcancer. With emotional reactions often dominating log-ical thought, such news tends to be overwhelming. Inthis article, I will address the real-life issues that breastcancer patients face every day, whether they are livingwith this condition or with a history of the condition,and therefore also living with the sobering possibility ofrecurrence.
It is my hope that, armed with knowledge of recent ad-vances in the treatment of breast cancer [Editor’s note:see “Advances in Systemic Treatment of Early Breast Can-cer in Postmenopausal Women,” pp. 10–15], medical di-rectors can promote programs that will be able to raisethe hopes and allay the fears of their members withbreast cancer. Moreover, because medical directors viewbreast cancer from a perspective that encompasses theentire spectrum of the disease, ranging from strategiesthat are aimed at prevention and early detection to thelong-term surveillance of patients who have been treatedpreviously, they are well positioned to advocate a widerange of interventions that could attenuate breast can-cer’s substantial burden within their managed popula-tion (Table 1).
ECONOMIC BURDEN OF BREAST CANCERDirect and indirect medical costs for breast cancer
vary widely, depending on the disease stage. It has beenestimated that in the United States breast cancer ac-counts for about 15 to 20 percent of all cancer costs(Radice 2003), which in 2001 amounted to $157 billion(direct costs, $56 billion; indirect morbidity costs, $16 bil-lion; indirect mortality costs, $85 billion).
In an employed population of women age 50 to 64years, average annual direct and indirect costs for breastcancer patients were higher than those for patients withosteoporosis or cardiovascular disease (Table 2, page 24).Compared with matched control subjects without can-cer, employed breast cancer survivors report losing 4times as many days from work (21.0 vs. 5.7) in the pre-vious 12-month period (Yabroff 2004). The authors note
that this measure underestimates the effects of breastcancer on productivity because it omits working-agepeople without jobs who were unable to work because ofpoor health.
CHANGING DEMOGRAPHICS Today, about 3.5 percent of the US population — 9.8
million people — are cancer survivors, compared with1.5 percent (3 million people) of the US population in1971 (MMWR 2004). The 2.2 million Americans whoever have received a diagnosis of breast cancer accountfor the largest proportion of this group: 22 percent. Nu-merous factors contribute to the increased number ofcancer survivors: increased screening with mammogra-phy leading to earlier diagnosis; improved treatment;prevention of cancer recurrence; prevention of advanceddisease, reduced mortality from other causes (eg, myo-cardial infarction); and an increase in the number ofolder persons, who account for the majority of new can-cer cases in general, and breast cancer in particular.
Regardless of the kind of health plan with which amedical director is associated, demographic changes dic-tate that breast cancer will become a matter of increas-ing concern. Currently, about 178 million Americans areenrolled in MCOs — approximately half of whom are females facing the well-publicized 1-in-8 lifetime risk ofbreast cancer. Those who are not yet old enough for, ordo not have known inherited risk warranting yearlymammography, are candidates for educational programsthat will heighten their awareness of breast cancer.
Because of the aging of the population in the UnitedStates, the number of postmenopausal women willcontinue to increase, along with the subset of post-menopausal women eligible for Medicare because theyhave attained age 65 (Figure, page 24). The populationdepicted in the figure (women age >50) represents the agegroup in which about 78 percent of new cases of invasivebreast cancer and 86 percent of breast cancer deathsoccur (ACS 2003).
In any health plan, it is the responsibility of the medi-cal director to make sure that a system is in place to sup-port breast cancer patients in obtaining the informationto help them understand their treatment options. A sys-tem established in a commercial plan may differ in somerespects from one set up for a Medicare population, but
A Medical Director’s Perspective On Early Breast CancerHARLAN A. LEVINE, MD
Chief Clinical Officer, UnitedHealth Group, Specialized Care Services, Golden Valley, Minn.

EARLY BREAST CANCER / MANAGED CARE 23
all will be aimed at the same goal: helping a woman di-agnosed with breast cancer maximize the likelihood ofa positive outcome and minimize the chance of recur-rence.
HELPING BREAST CANCER PATIENTS At the time of diagnosis, it is essential for the clinician
to explain the differences among the stages of breast can-cer and the levels of aggressiveness of the tumor. The pa-tient with stage I breast cancer may not readily grasp thefact that her cancer has been diagnosed at an early stagewhen it is still confined to the breast (and perhaps locallymph nodes) and surgical treatment is likely to be highlyeffective in removing detectable disease. Patients mayfind comfort in learning that today the 5-year survivalrates for localized and regional breast cancer are 98 per-
cent (compared with 80 percent in the 1950s) and 80 per-cent, respectively (ACS 2005). Telling patients about thesophisticated techniques used to determine staging andaggressiveness, along with the reasons for determiningthe HER2/neu status and the estrogen/progesterone re-ceptor status of their tumors, also may be beneficial inhelping them understand the nature of their disease andits prognosis. It is important to explain that detectingmarkers of aggressiveness (such as HER2/neu status)can help in making the decision for a more aggressivetreatment plan that can increase the chances of long-termsurvival.
In this context of hopefulness, clinicians then can as-sist the patient in drawing a mental map depicting thepath that is most likely to lead to a positive outcome. Thismap would address the multidisciplinary services pro-
TABLE 1 Burden of female breast cancer in the United States
Measure
Cancer survivors
New cases of
invasive breast
cancer, 2005
Deaths, 2005
Person-years of life
lost from cancer,
1997
Average years of
life lost per person
from cancer, 1997
Units
2.2 million (22% of all livingAmericans ever diagnosed
with breast cancer)
211,000* (32% of the 663,000 new
cancer cases among women;15% of the 1.4 million newcases among both sexes)
40,000(15% of the 275,000 cancer
deaths among women;7% of the 570,000 cancer
deaths among both sexes)
809,000
19.3
Breast cancer
rank order
1
1 (women)
2 (both sexes)
2 (women)
3 (both sexes)
2
6
Rank of other cancers in proximity
to breast cancer
2. Prostate (17%)3. Colorectal (11%)4. Gynecological (10%)
WOMEN
2. Lung and bronchus (12%)3. Colorectal (11%)BOTH SEXES
1. Prostate (17%)3. Colorectal (11%)
WOMEN
1. Lung and bronchus (26%)3. Colorectal (10%)BOTH SEXES
1. Lung and other respiratory organs(13%)
2. Colorectal (10%)
1. Lung and bronchus (2.2 million)3. Colorectal (758,000)
1. Childhood (69.3)2. Testis (34.8)3. Hodgkin’s lymphoma (26.0)4. Cervix uteri (25.9)5. Brain and other nervous system (21.9)
*The ACS also predicts 50,000 new cases of ductal carcinoma in situ (DCIS) in 2005, the majority of which, without treatment,will progress to invasive cancer.
SOURCES: ACS 2005, BROWN 2001, MMWR 2004, YABROFF 2004

24 MANAGED CARE / SUPPLEMENT
vided by a comprehensive health careteam, including surgical options, radi-ation therapy, chemotherapy, hormonaltherapy, immunotherapy, long-termsurveillance following the initial ther-apy, and support services. Because somepatients may associate cancer treatmentof any kind with unproven and poten-tially dangerous experimentation, anexplanation that the health plan en-dorses the use of evidence-based guide-lines, such as those that are promul-gated by the National ComprehensiveCancer Network «www.nccn.org», may help the patientto better accept the process. Many benefit coverage planscover clinical trials under certain conditions, and thehealth plan adds value both in its establishing the stan-dards for a national or academic sponsorship of these tri-als and by making members and physicians aware of theopportunity.
Because of the complexities of breast cancer treat-ment and the fact that so many options are available atevery stage and level of aggressiveness, the treatmentmap for breast cancer can be cir-cuitous. The resulting care can befragmented, because it involvesnumerous clinicians. Medical di-rectors should work to ensure thatevery breast cancer patient has theservices of a trustworthy clinician-guide who can reduce fragmenta-tion and help the patient to navi-gate the treatment maze.
At numerous points, the breastcancer patient may be uncertainabout where she should turn forhelp or what she should do next.Medical directors should developprograms that facilitate access toreliable consumer-friendly infor-mation and serve to activate thewoman with breast cancer to takeappropriate action.
Today, variation exists in howphysicians treat disease. Healthplan programs should aim to en-sure that the breast cancer patientis informed of the evidence-basedoptions and the benefits and risksof each, and that her personal pref-erences are taken into account inthe decision-making process.
Furthermore, the clinician-guide can help the patient becomea better consumer of health care
services by teaching her the questions she should askher treating physicians. For example, in addition toknowing that in many cases breast-conserving surgeryand mastectomy have equivalent survival rates, she needsto know that both options are available to her in orderto chose between them in accordance with her personalpreferences. Likewise, a postmenopausal woman needsto know whether she is eligible for hormone therapywith tamoxifen or an aromatase inhibitor (anastrozole,exemestane, or letrozole).
TABLE 2 Economic burden of breast cancer among post-menopausal employees
Direct Indirect
costs costs Total
Breast cancer (n=555) $13,925 $8,236 $22,161Cardiovascular disease (n=1,710) $12,055 $4,990 $17,045Osteoporosis (n=2,314) $6,259 $4,039 $10,298Random sample (n=7,575) $2,951 $2,292 $5,243
SOURCE: SASSER 2005
FIGURE Estimated number of postmenopausal women in United
States, 2005–2015
In thousands
SOURCE: US CENSUS BUREAU 2004
700
600
500
400
300
200
100
02005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Year
Age 65+Age 50–64

EARLY BREAST CANCER / MANAGED CARE 25
In the presentation of information about any aspectof breast cancer, clinicians should be mindful that pa-tients vary tremendously in their desire for information,and in their ability to process it. An inadequate amountof information for one patient may constitute informa-tion overload for another. Moreover, the manner inwhich information is presented may protect patientsagainst the development of depression or anxiety, orboth (Burgess 2005). Simply giving women a choiceamong surgical options does not protect against depres-sion and anxiety, but communicating with them effec-tively does.
Depression and anxiety. Aside from diminishing qual-ity of life, depression interferes with problem-solving,self-care, and compliance with cancer treatment andmay also adversely affect prognosis. (Somerset 2004).About one quarter of breast cancer patients have co-morbid depression, in comparison with a prevalence ofabout 6 percent in the general population (Aapro 1999).In the first year following a diagnosis of early breast can-cer, nearly half the women experience depression, anxi-ety, or both (Burgess 2005). Afterwards, rates of depres-sion and anxiety decline to about 25 percent in years 2through 4, and to 15 percent in year 5. If breast cancerrecurs, however, the prevalence of depression and anxi-ety may actually exceed the prevalence occurring after theinitial diagnosis. Women diagnosed with a recurrence ofbreast cancer report the same feelings of terror, shock,and disbelief as they did after the initial diagnosis (Payne1996).
The identification of breast cancer patients with de-pression is complicated by the fact that many signs andsymptoms of depression — such as weight loss, sleep dif-ficulties, and fatigue — coincide with the effects of can-cer.Women may have negative psychological reactions toradiation therapy or chemotherapy that need to be rec-ognized and addressed. Self-rating scales such as theBeck Depression Inventory or the Carroll DepressionRating Scale are among the tools that are available forscreening for major or minor depression, so that anti-depressant therapy can be initiated (Somerset 2004). In
addition, many support groups are available to helpbreast cancer patients and their families through thechallenges of the illness and its treatment. This supportcan be a significant adjunct to the pharmacologic andcognitive treatment of depression.
REDUCING THE RISK OF RECURRENCENot surprisingly, recurrence of breast cancer is asso-
ciated with an increase in pain, suffering, mortality, andcost. A retrospective analysis of a cohort of 1,616 womenwith early breast cancer (stage I and II) in the Henry FordHealth System (a large, vertically integrated Midwesternhealth care system employing salaried physicians) foundthat over a median follow-up of 44.5 months, patientswith recurrence had a 7.6-fold higher risk of death com-pared with patients without recurrence, with the hazardratio varying by site (distant, 13.6; locoregional, 4.5;contralateral breast, 3.0) (Lamerato 2005). Charges forpatients with recurrence were substantially higher thanthose for patients without evidence of recurrence($157,215 vs. $74,568) (Lamerato 2004). Costs over 6 and12 months were highest for patients with distant recur-rence (Table 3).
Adjuvant hormone therapy is directed at reducing therisk of breast cancer recurrence. Until recently, tamoxifenwas standard treatment for women with ER-positivebreast cancer, with 1, 2, and 5 years of adjuvant treatmenthaving been shown to reduce the risk of recurrence by 18,25, and 42 percent, respectively, and the risk of all-causemortality by 10, 15, and 22 percent in women with earlybreast cancer (EBCTCG 1998). The benefits of tamoxifentherapy occur predominantly in women with ER-posi-tive tumors, with a 50 percent relative reduction in re-currence and a 28 percent relative reduction in all-causemortality being reported after 5 years of adjuvant treat-ment. The benefits of 5 years of adjuvant tamoxifen ther-apy persist for at least 10 years, with relative reductionsin disease recurrence and all-cause mortality being 47percent and 26 percent, respectively, after 10 years offollow-up. In women with operable breast cancer, how-ever, extending the duration of adjuvant tamoxifen treat-
TABLE 3 Mean charges before and after breast cancer recurrence in a Midwestern health system
Before recurrence After recurrence
6 months 12 months 6 months 12 months
Overall $10,715 (n=104) $12,344 (n=62) $45,855 (n=104) $79,253 (n=62)Locoregional recurrence $8,507 (n=35) $11,341 (n=21) $33,174 (n=35) $61,027 (n=21)Contralateral breast $4,788 (n=17) $11,182 (n=12) $35,909 (n=17) $50,131 (n=12)Distant recurrence $14,136 (n=52) $13,580 (n=29) $57,842 (n=52) $104,502 (n=29)
SOURCE: LAMERATO 2004

26 MANAGED CARE / SUPPLEMENT
ment beyond 5 years appears to offer no further advan-tage in patients with ER-positive breast cancer and neg-ative axillary lymph nodes (Fisher 2001).
The third-generation aromatase inhibitors (Table 4),while not yet shown to offer any mortality benefit incomparison with tamoxifen, have been demonstrated toreduce the risk of breast cancer recurrence in women
with ER-positive tumors. The American Society of Clini-cal Oncology has recommended that an aromatase in-hibitor be included as adjuvant therapy for such pa-tients, either as initial therapy or subsequent to tamoxifen(Winer 2005).
The benefit from aromatase inhibitors may be a classeffect, but as of now, anastrozole is the only one with data
TABLE 4 Third-generation aromatase inhibitors
Generic name
Trade name/
manufacturer
Mechanism
of action
Half-life
Initial US
FDA approval
Route/dosing form
(strength)
Price per month,
approximate
Indications
(all indications
are for post-
menopausal
women)
Anastrozole
ARIMIDEX®*/AstraZeneca
Nonsteroidal inhibitor(reversible, type II)
50 hours
1995 (December)
Oral/tablet (1 mg)
$258 ($8.60/tablet × 30)§
$214 ($7.13/tablet × 30)ıı
• Treatment of advancedbreast cancer that has progressed following tamoxifen therapy
• First-line treatment of HR-positive or HR-unknownlocally advanced ormetastatic breast cancer
• Adjuvant treatment of HR-positive early breast cancer
Exemestane
AROMASIN®†/Pfizer
Steroidal inactivator(irreversible, type I)
24 hours
1999 (October)
Oral/tablet (25 mg)
$265 ($8.84/tablet × 30)§
$224 ($7.46/tablet × 30)ıı
• Treatment of advancedbreast cancer that has progressed following treatment with tamox-ifen
• Adjuvant treatment of postmenopausalwomen with estrogen-receptor positive earlybreast cancer who havereceived 2 to 3 years of tamoxifen and areswitched to exemes-tane for completion of atotal of 5 years of adju-vant hormonal therapy
Letrozole
FEMARA®‡/Novartis
Nonsteroidal inhibitor(reversible, type II)
48 hours
1997 (July)
Oral/tablet (2.5 mg)
$276 ($9.18/tablet × 30)§
$217 ($7.23/tablet × 30)ıı
• Treatment of advancedbreast cancer that has progressed following antiestrogen therapy
• First-line treatment of HR-positive or HR-unknown locally advanced ormetastatic breast cancer
• Extended adjuvant treat-ment of early breast cancerafter 5 years of adjuvant tamoxifen therapy
* ARIMIDEX is a registered trademark of the AstraZeneca Group of companies.
† AROMASIN is a registered trademark of Pfizer.
‡ FEMARA is a registered trademark of Novartis Pharmaceuticals.§ All monthly prices have been calculated from the average wholesale price per tablet, based on prices accessed November 2005 at First DataBank.
Comparable monthly price calculated on basis of 30 tablets for tamoxifen 20 mg is $113.77 ($3.79/tablet). ııAll monthly prices have been calculated from the average retail price per tablet, based on prices accessed November 2005 at «www.drugstore.com».
Comparable monthly price calculated on basis of 30 tablets for tamoxifen 20 mg is $37.99 ($1.27/tablet).
SOURCES: MANUFACTURERS’ PRESCRIBING INFORMATION

EARLY BREAST CANCER / MANAGED CARE 27
supporting its use as first-line early adjuvant monother-apy. After a median follow-up of 68 months, HR-positivepatients treated with anastrozole in ATAC had a 17 per-cent reduction in the risk of recurrence compared to thetamoxifen-treated patients (Howell 2005). In the HR-positive patients, the absolute difference in time to re-currence, in favor of anastrozole, was 1.7 and 3.7 percentafter 3 and 6 years, respectively.
The aromatase inhibitors offer adverse-event profilesthat differ from that of tamoxifen. In the ATAC (Arim-idex, Tamoxifen, Alone or in Combination) trial, with 68months of follow-up in comparison with tamoxifen, pa-tients who were receiving anastrozole were less likely toexperience endometrial cancer (odds ratio [OR], 0.20),ischemic cerebrovascular disease (OR, 0.70), venousthrombotic events (OR, 0.61), deep vein thrombosis(OR, 0.64), hot flashes (OR, 0.80), vaginal bleeding (OR,0.50) and vaginal discharge (OR, 0.24) but they weremore likely to experience fractures (OR, 1.49) andarthralgia (OR, 1.32) (Howell 2005).
As they weigh the risks versus benefits of hormonaltherapies from their different perspectives, medical on-cologists and primary care physicians occasionally mayfind themselves in disagreement about which agent orcombination of agents is best for a given patient. In suchinstances, the medical director may be able to mediate aresolution, perhaps by simply reminding the physiciansof the importance of placing the patient’s informed pref-erences in the forefront of their professional recom-mendations.
VARIATIONS IN TREATMENT A distressing trend in medical care in the United States
is the increasing disparity in breast cancer death rates be-tween white and African-American women. As recentlyas 1981, the age-adjusted death rates for both groupswere essentially equal (about 31 per 100,000), but sincethen, a gap has developed and widened, to the extent that,by 2000, the excess deaths among African-Americanswere more than 30 percent greater than those amongwhite women (ACS 2003). This difference, a serious pub-lic health problem, is explained more by socioeconomicfactors than by any biological characteristics; equal treat-ment should lead to equal outcomes (Shavers 2002).Medical directors need to take a close look at the sub-populations served by their health plans to make sure thatthe same level of treatment is extended to every patient,and that screening is used appropriately to diagnosisbreast cancer at an early stage. They may need to considerculturally sensitive and focused communication andmessaging.
Possibly reflecting uncertainty about the value ofmammography owing to conflicting recommendations,rates of mammography have reached a plateau among alltypes of MCOs (NCQA 2004). In commercial and Medi-
care plans, breast cancer screening rates have hoveredaround 75 percent for the past 4 years, while in Medic-aid plans the rate has been no greater than 56 percentduring this period. This HEDIS measure estimates thepercentage of women ages 52 to 69 who had at least 1 mammogram in the previous 2 years. Medical directorscan encourage their health plans to improve their per-formance in this HEDIS measure, and to make suremammography rates are consistent across subgroupswithin the health plan.
CONCLUSIONBy virtue of their leadership positions, medical direc-
tors are capable of substantially lessening the burdenthat is imposed by breast cancer on their health plans andon individual members. It is incumbent on medical di-rectors to adopt a consumer-oriented, culturally sensitiveapproach to early breast cancer, focusing on the issuesthat are important to the patient. As more is learnedabout the way individuals respond to stress, cope withchronic conditions, and approach significant decisionmaking, the health plan can play a central role in shar-ing these insights with their members and their networkphysicians. Emphasis should be placed on early diagno-sis, sensitivity to the patient’s wide range of emotions, ap-propriate treatment that conforms with the patient’spreferences, and efforts to reduce the risk of disease re-currence.
ReferencesAapro M, Cull A. Depression in breast cancer patients: the need
for treatment. Ann Oncol. 1999;10:627–636.American Cancer Society (ACS). Breast Cancer Facts & Figures
2003–2004. Atlanta: American Cancer Society. 2003. Avail-able at: «http://www.cancer.org/downloads/STT/CAFF2003BrFPWSecured.pdf». Accessed Aug. 19, 2005.
American Cancer Society (ACS). Cancer Facts & Figures 2005.Atlanta: American Cancer Society. 2005. Available at:http://www.cancer.org/downloads/STT/CAFF_finalPWSecured.pdf». Accessed Aug. 19, 2005.
Arimidex (anastrozole) [prescribing information]. Wilmington,Del.: AstraZeneca Pharmaceuticals LP. September 2005.
Aromasin (exemestane tablets) [prescribing information]. NewYork: Pharmacia & Upjohn Co., Division of Pfizer Inc.September 2004.
Brown ML, Lipscomb J, Snyder C. The burden of illness of can-cer: economic cost and quality of life. Annu Rev PublicHealth. 2001;22:91–113.
Burgess C, Cornelius V, Love S, et al. Depression and anxiety inwomen with early breast cancer: five year observational co-hort study. BMJ. 2005;330:702. Epub 2005 Feb 4.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG).Tamoxifen for early breast cancer: an overview of the ran-domised trials. Lancet. 1998;351:1451–1467.
Femara (letrozole tablets) [prescribing information]. EastHanover, N.J.: Novartis Pharmaceuticals Corp. November2004.
Fisher B, Dignam J, Bryant J, Wolmark N. Five versus more thanfive years of tamoxifen for lymph node-negative breast can-cer: updated findings from the National Surgical Adjuvant

28 MANAGED CARE / SUPPLEMENT
Breast and Bowel Project B-14 randomized trial. J NatlCancer Inst. 2001;93:684–690.
Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arim-idex, Tamoxifen, Alone or in Combination) trial after com-pletion of 5 years’ adjuvant treatment for breast cancer.Lancet. 2005;365:60–62.
Lamerato L, Havstad S, Gandhi SK, Jones DA. Costs of initial,continuing and terminal care in US patients with recur-rence following early breast cancer. Poster presented atAmerican Society of Clinical Oncology, Orlando, Fla., May15–17, 2005.
Lamerato LE, Havstad S, Gandhi SK, Jones DA. The economicburden of breast cancer recurrence: findings from a retro-spective analysis of health system data. Poster presented at27th Annual San Antonio Breast Cancer Symposium, Dec.8–11, 2004.
Morbidity and Mortality Weekly Report (MMWR). Cancer sur-vivorship — United States, 1971–2001. MMWR. 2004;53:526–528.
NCQA (National Committee for Quality Assurance). The Stateof Health Care Quality 2004. Washington: NCQA. 2004.Available at: «http://www.ncqa.org/communications/SOMC/SOHC2004.pdf». Accessed Aug. 15, 2005.
Payne DK, Sullivan MD, Massie MJ. Women’s psychological re-actions to breast cancer. Semin Oncol. 1996;23(suppl 2):89–97.
Radice D, Redaelli A. Breast cancer management: quality-of-lifeand cost considerations. Pharmacoeconomics. 2003;21:383–396.
Somerset W, Stout SC, Miller AH, Musselman D. Breast cancerand depression. Oncology. 2004;18:1021–1048.
Shavers VL, Brown ML. Racial and ethnic disparities in the re-ceipt of cancer treatment. J Natl Cancer Inst. 2002;94:334–357.
US Census Bureau. 2004. US interim projections by age, sex,race, and Hispanic origin. Available at: «http://www.census.gov/ipc/www/usinterimproj/». Accessed Aug 16,2005.
Winer EP, Hudis C, Burstein HJ, et al. American Society of Clini-cal Oncology technology assessment on the use of aro-matase inhibitors as adjuvant therapy for postmenopausalwomen with hormone receptor-positive breast cancer: sta-tus report 2004. J Clin Oncol. 2005;23:619–629. Epub 2004Nov 15.
Yabroff KR, Lawrence WF, Clauser S, et al. Burden of illness incancer survivors: findings from a population-based na-tional sample. J Natl Cancer Inst. 2004;96:1322–1330.

233074 12/05