surgeon led biopsy of musculoskeletal tumours
DESCRIPTION
Surgeon led biopsy of musculoskeletal tumours. Robert U. Ashford Stanley W. McCarthy S. Fiona BonarRichard A. Scolyer Rooshdiya Z. KarimPaul D. Stalley NSW Bone & Soft Tissue Sarcoma Service. “Poorly performed biopsies compromise limb salvage surgery and patient survival”. - PowerPoint PPT PresentationTRANSCRIPT

Surgeon led biopsy of musculoskeletal tumours
Robert U. Ashford Stanley W. McCarthy
S. Fiona Bonar Richard A. Scolyer
Rooshdiya Z. Karim Paul D. Stalley
NSW Bone & Soft Tissue Sarcoma Service
“Poorly performed biopsies compromise limb salvage
surgery and patient survival”Mankin JBJS 1982
Biopsy of Musculoskeletal Tumours• Tertiary Centre is best & core biopsy preferred
• Fraught with complications– Mankin (1982 & 1986) :– 23% error rate– 17% complication rate– 5% amputation rate because of biopsy
• Our experience– Pollock & Stalley 2004– 38% of biopsies performed elsewhere hindered Rx– 17% amputation rate

Biopsy of Suspicious Lesions
• CT guided biopsy for all ?– 127 Biopsies– 20% non-correlation rate (25 patients)– 10 Non-diagnostic CT Bx (6/10 malignant)– 1 Major error: CT Bx – Schwannoma ; Excision
- synovial sarcoma
Altuntas et al (2004): ANZ J SurgAltuntas et al (2004): ANZ J Surg
Sydney to Venice
16304 km

DistanceSydney to
Albury 560km Bega 420km Bourke 775km Broken Hill 1159km Coffs Harbour 572km Dubbo 407km Grafton 618km Wagga 470km
London to Venice 1139 kmLondon to Geneva 740 kmNew York to Washington 328 kmToronto to New York 831 km

RPAH Protocol
1. MDT Sarcoma Clinic Assessment
2. Completion of imaging
3. Biopsy 1. Surgeon (Consultant / Fellow)
2. GA
3. Core Biopsy (Trucut)
4. Frozen Section with surgeon present
5. Repeat Biopsy Core or open if 4 not representative
Study
• Retrospective review of all biopsies performed at RPAH under the care of the senior author for 2 years (July 2003 – June 2005)
• Comparison of core, core proceed to open and open biopsies
• Analysis of accuracy and non-diagnostic rates
• Comparison with CT core biopsies from literature

Biopsy Technique
Biopsy Method Number Percentage
Trucut Core 93 34.3%
Core proceed to open 11 4.1%
CT Core 24 8.9%
Open (Incisional, Curetting)
76 28.0%
Excisional 58 21.4%
Reamings 9 3.3%
Total 271 100%
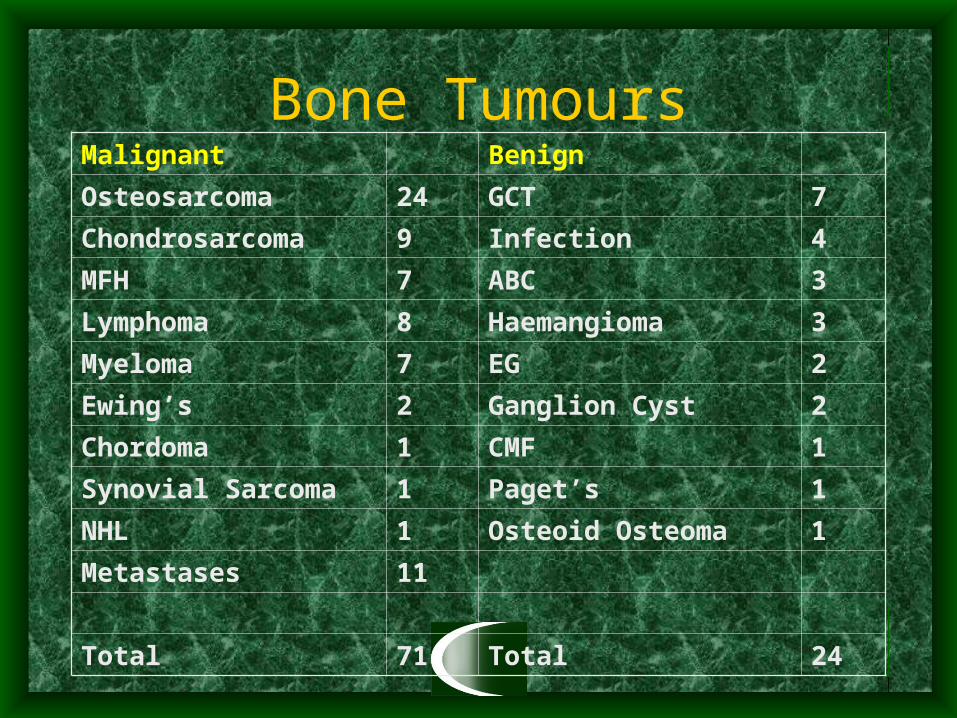
Bone TumoursMalignant Benign
Osteosarcoma 24 GCT 7
Chondrosarcoma 9 Infection 4
MFH 7 ABC 3
Lymphoma 8 Haemangioma 3
Myeloma 7 EG 2
Ewing’s 2 Ganglion Cyst 2
Chordoma 1 CMF 1
Synovial Sarcoma 1 Paget’s 1
NHL 1 Osteoid Osteoma 1
Metastases 11
Total 71 Total 24

Soft Tissue Tumours
Malignant Benign
MFH 8 Desmoid Fibromatosis 3
Leiomyosarcoma 4 Fibroma 3
Synovial Sarcoma 3 Schwannoma 2
Liposarcoma 1 Myxoma 2
Fibromyxoid sarcoma 1 Synovial Chondromatosis
1
Fibrosarcoma 1 Neuroma 1
Myofibrosarcoma 1 Haemangiopericytoma 1
Rhabdomyosarcoma 1
Total 20 Total 13
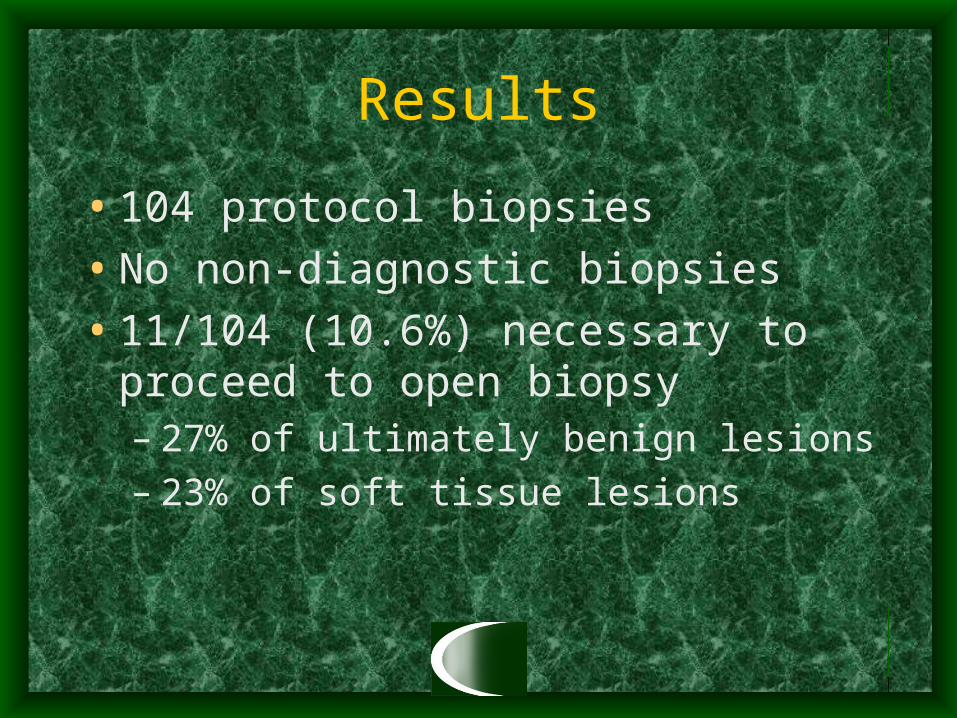
Results
• 104 protocol biopsies
• No non-diagnostic biopsies
• 11/104 (10.6%) necessary to proceed to open biopsy– 27% of ultimately benign lesions– 23% of soft tissue lesions
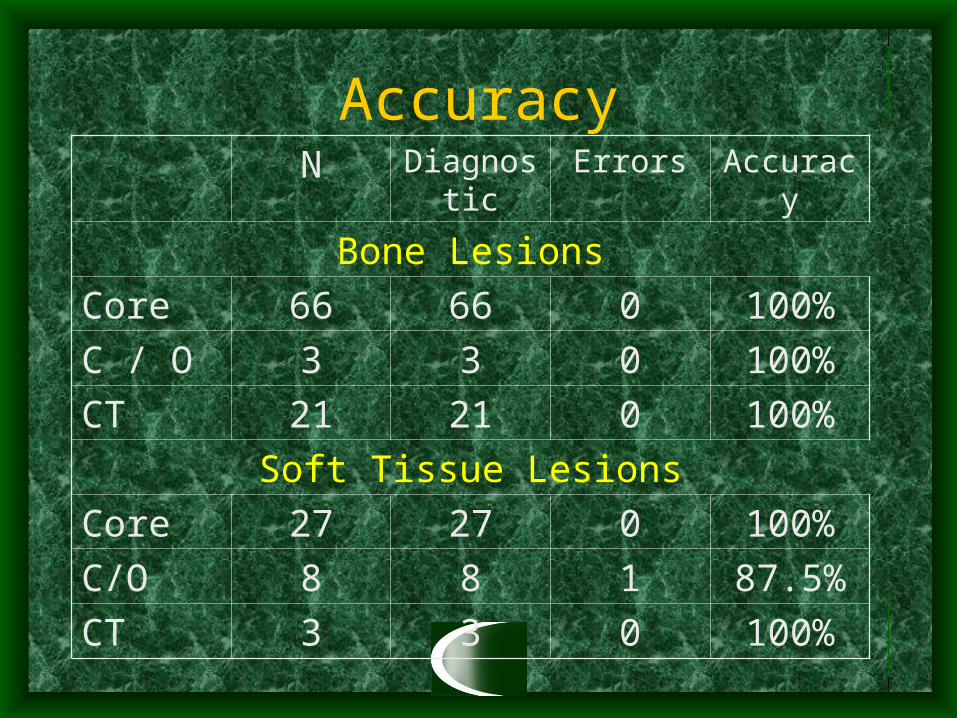
AccuracyN Diagnostic Errors Accuracy
Bone Lesions
Core 66 66 0 100%
C / O 3 3 0 100%
CT 21 21 0 100%
Soft Tissue Lesions
Core 27 27 0 100%
C/O 8 8 1 87.5%
CT 3 3 0 100%

One Error
• 62 Female with thigh mass
• Non-diagnostic imaging
• F/S diagnosis: lymphoid tissue favour Hodgkin’s Disease
• Final diagnosis: B cell lymphoma
• No alteration in surgical management

Discussion
• Tertiary centre is best
• Core biopsy is often appropriate
• Adding frozen section eradicates risk of non-diagnostic biopsy
• Open biopsy if core non-diagnostic
• A good pathologist is obligatory

Before doing a biopsy …….. think