surgical affection of oesophagus
TRANSCRIPT

Surgical Affection of Oesophagus
Dr. Bikash PuriAssist. Professor
Nepal Polytechnic Institute, Chitwan
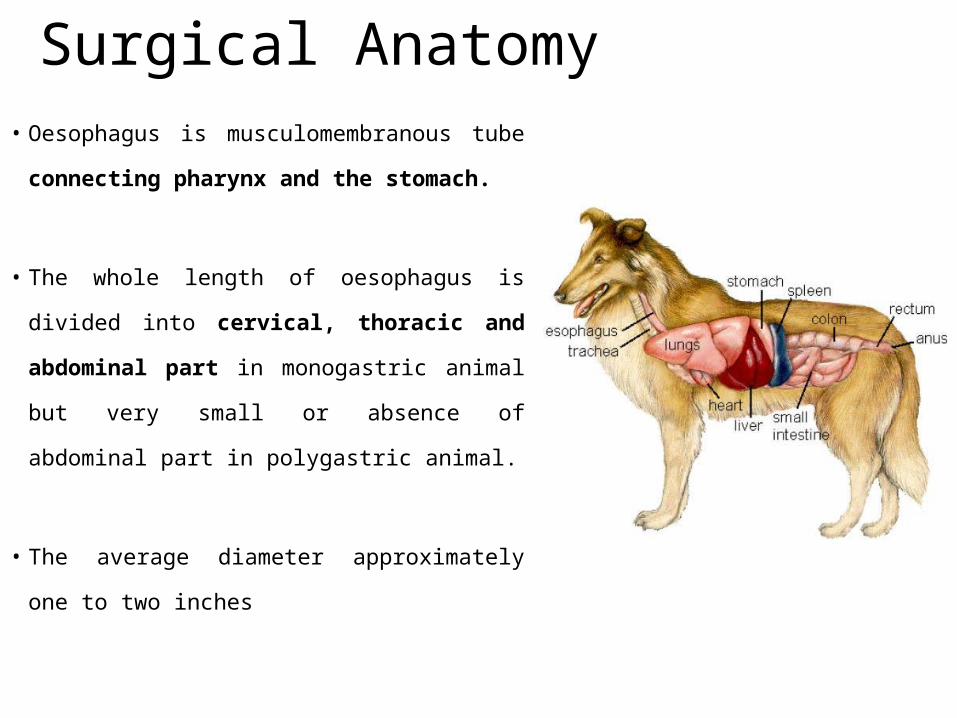
Surgical Anatomy• Oesophagus is musculomembranous tube
connecting pharynx and the stomach.
• The whole length of oesophagus is divided
into cervical, thoracic and abdominal part
in monogastric animal but very small or
absence of abdominal part in polygastric
animal.
• The average diameter approximately one to
two inches
• Begins at the level of the first cervical vertebra.
• Occupies almost dorsal position at origin and passes gradually to
left side of the trachea at the level of about 4th cervical vertebrae.
• Thereafter it occupies the left position of trachea upto 3rd thoracic
vertebrae.
• In the thoracic region it is median in position and enters the
abdominal cavity through hiatus oesophagus and terminates at the
cardia of the stomach.
• As the oesophagus crosses to left side of the trachea it is
accompanied by—
– Dorsally: longus coli and longus capitis muscles
– Laterally: left carotid artery, vagosympathetic trunk, jugular vein and recurrent
laryngeal nerve
• Overlying the oesophagus, following structures are
encountered:
– Skin,
– Cervical fascia
– Cervical paniculus muscle
– Omohyoideus muscle crossing the jugular furrow obliquely form below
upward, forward and inward towards the median line.
Composition of Esophageal wall
Its wall is composed of
• fibrous sheath,
• the tunica adventitia (Outermost layer)
• the muscular coat, (Double layer but in cat single layer)
• the sub-mucous and mucous coat. It is the
strongest layer to place the suture.
• The Blood supply to oesophagus is by branches of
– carotid,
– brachio-oesophageal
– and gastric arteries.
• The nerve supply to oesophagus is by
– vagus,
– glosso-pharyngeal
– and sympathetic nerves.
Blood and nerve supply
Surgical disease of Oesophagus
• Osophageal obstruction
• Oesophageal diverticulum
• Oesophageal stenosis
• Oesophageal wounds and fistula
• Neoplastic growth underneath the oesophagus.
Oesophageal obstruction/ChokeDefination:
– Choke is the intraluminal blockage of oesophagus.
– This condition is frequent in pet animals but infrequent in ruminants.
– Its frequency is higher in cattle but occasionally recorded in buffalo, camels and small
ruminants.
Etiology:
– Intraluminal causes: Example: vegetable (Turnip), fruits (large size lemon and apple), meat ball,
tennis ball, woods, plastic etc.
– Extraluminal causes: Example: large perioesophageal abscess, enlarged mediastinal lymph
nodes and tumors.
– Nutritional deficiencies, Dry feed ,
– Greedy nature of feeding of ruminants
– Oesophageal stenosis.
Symptoms• Swelling in the ventral neck region
• Inability of the animal to swallow feed and water.
• Hyper –salivation
• Animals keeps the neck stretched.
• Severe tympany occurs in complete choke
• The patient remains thirsty and makes attempts to drink water which often
returns back through the nostrils caring food particles with it.
• If obstruction persist for longer duration than it leads to perforation of
oesophagus due to pressure necrosis.
• Regurgitation of swallowed food and water may cause cough and
aspiration pneumonia.
Diagnosis
• Based on history, clinical signs and physical examination
• Obstruction to cervical region can be easily palpated. For obstruction in
thoracic region or doubtful condition, a probang may be passed.
• By measuring the length of the probang inside helps to locate the
obstruction.
Confirmatory diagnosis
• Radiographic examination with contrast media like barium salt past or
• Endoscopic examination in case of perforation
Treatment
• Oesophageal obstruction is usually not life threatening as long
as care is taken to control development of ruminal tympany.
• All extraluminal obstruction needs surgical correction
• The treatment for intraluminal obstruction can be categorized
as conservative and surgical
Conservative Management1. First of all oesophageal spasm should be controlled by applying
neuromuscular blocking agent along with anesthesia or deep sedation.
2. In large animal cervical obstruction should be cleared by placing the thumb or
fingers distal to the foreign body and gradually forcing it upwards until
reaches to pharynx. Then inserting hand obstructing material is removed.
3. Retraction of obstructing materials by Folley Urethral Catheter.
• Here, the folley catheter with a stylet is passed across the foreign obstructing object
and inflating the catheter bulb . Radiograph ascertain the correct position of the
inflatted cuff.
• Gentle retraction of catheter dislodges blunt foreign bodies and pull them out in
4. Push the obstruction material into rumen or stomach using probang
5. Along with this conservative management the animal must be infused with
ringes’s lactate solution
Surgical treatment
• Oesophagotomy is performed.
• It is practical in proximal two-third of cervical
part where the organ is relatively accessible
• Exposure of the caudal cervical oesphagus
form C6 to T2 is more difficult
CONTROL AND ANAESTHESIA
1. The position of animal is right lateral
recumbency after proper sedation.
2. Anaesthesia is by general anaesthesia in small
animals or by local in filtration analgesia at the
site of operation.
SURGICAL TECHNIQUE
1. An incision about twice the length of foreign body should be made
on skin and subcutaneous tissue.
2. The omohyoideus muscle is separated from upper and lower
structure. The areolar tissue is bluntly dissected with the help of
fingers.
3. The trachea is recognized to locate the oesophagus on its lateral
surface.
4. The oesophagus is drawn out and fixed in position by placing
intestinal forceps proximally and distally to foreign body.
5. Operative field is now packed off to avoid any chance of
contamination
6. Make an incision on dorsal wall of oesophagus either anterior or posterior to
obstruction. The incision should be large enough to extract the
obstruction/foreign body.
7. The repair of oesophageal incision can be done in two layers. The mucous
membrane can be sutured with mattress sutures or continuous sutures using
round bodies swaged needle.. The muscularis layer is to be sutured with
continuous lock stitch pattern. The distance between two suture should not
exceed 2-3 mm in small animal and 5mm in large animal.
8. Irrigate the area well with sterile saline mixed with antibiotic solution before
routine skin closure
9. The oesophagus is replaced in its original position.
10. The skin wound is closed in routine manner or it is left as open wound.
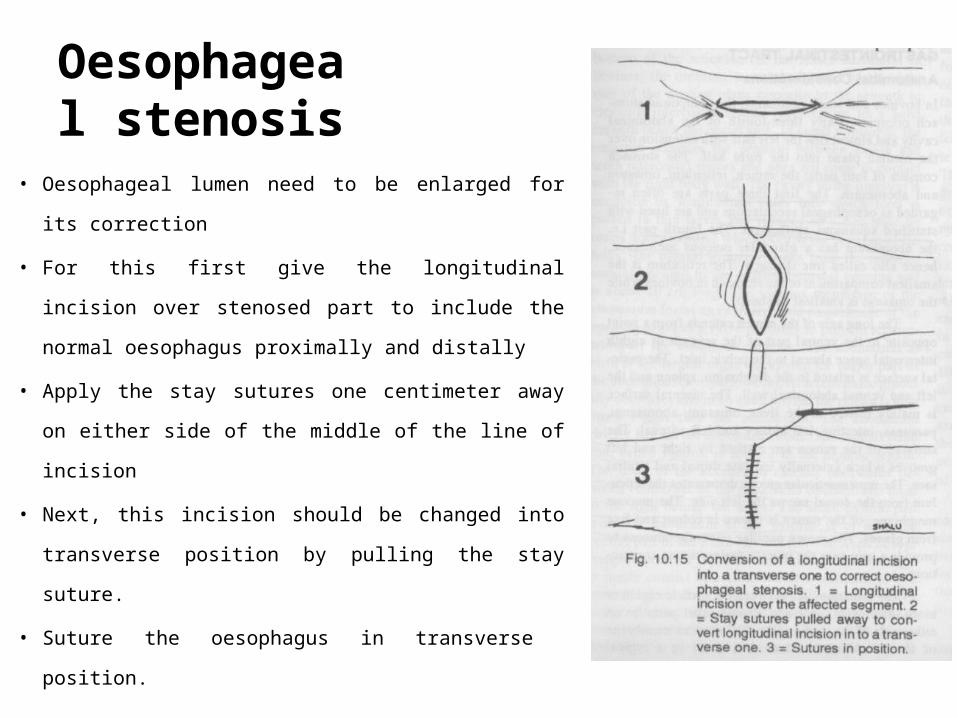
Oesophageal stenosis
• Oesophageal lumen need to be enlarged for its
correction
• For this first give the longitudinal incision over
stenosed part to include the normal oesophagus
proximally and distally
• Apply the stay sutures one centimeter away on
either side of the middle of the line of incision
• Next, this incision should be changed into
transverse position by pulling the stay suture.
• Suture the oesophagus in transverse position.
POST OPERATIVE CARE• Do not allow solid food for few days and intravenous feeding
is done twice daily.
• A course of antibiotics is to be completed (4-5 days)
• Antiseptic dressing of the wound should be carried one till
healing is complete or when sutures are removed after 8-12
days.
IMPORTANT CONSIDERATION/ REMARKS
1. Check hemorrhage during surgery
2. If oesophagus is empty it is recognized by passing a stomach tube.
3. During dissection, prevent damage to recurrent laryngeal nerve.
4. Suturing only oesophagus and leaving the skin wound open is the
procedure of choice because
a) It favours early closure of oesophageal wound
b) It prevents escape of alimentary matter during swallowing.
c) It permits drainage of any material, if present.