surgical endoscopy 6
DESCRIPTION
June 1997TRANSCRIPT

Laparoscopic partial fundoplication vs laparoscopicNissen-Rosetti fundoplication
Short-term results of 231 cases
D. D. Coster, W. H. Bower, V. T. Wilson, R. T. Brebrick, G. L. Richardson
Grinnell Regional Medical Center, 200 Fourth Avenue, Grinnell, IA 50112, USA, and The Grinnell Institute for Minimally Invasive Surgery, 122Fourth Avenue, Grinnell, IA 50112, USA
Received: 12 December 1995/Accepted: 12 August 1996
AbstractBackground:Since 1992, all patients at our institution whohave met standard accepted criteria for surgical interventionfor complicated gastroesophageal reflux disease have beenentered into a prospective sequential clinical study to evalu-ate outcomes of the laparoscopic approach to the Nissen-Rosetti procedure and a modified Toupet procedure.Methods: A standardized workup with upper GI series,esophagography, and endoscopy was used in all patients.Manometry, pH testing, and other special tests were usedselectively. A measuring technique was used to determinewrap size without the use of dilators. The short gastric ves-sels were left intact in all patients. A cosurgeon approachwas used, with technical factors described herein.Results:Some 226 of 231 cases were completed laparo-scopically (98%)—125 patients in the Nissen-Rosetti groupand 101 in the partial fundoplication group. There were noclinical failures in either group. The partial fundoplicationgroup performed better than the Nissen-Rosetti group in allcategories of comparison. Return to normal eating habitswas much earlier in the partial wrap group (p < 0.0001).Postop distal esophageal sphincter pressures in the twogroups were equal at 15 mmHg. Eight patients sufferedsignificant dysphagia requiring endoscopy and dilatation,all in the Nissen-Rosetti group (p < 0.01). Minor compli-cations occurred in 12% of the total group. There was a totalsurgical revision rate of 3%. There were no gastric or esoph-ageal perforations. Average operative time was 30 min. Av-erage hospital stay was 1.4 days. Hospital charges for thelaparoscopic approach averaged $6,000 dollars compared to$12,000 for the open approach.Conclusion:Laparoscopic partial fundoplication is as effec-tive as laparoscopic Nissen-Rosetti fundoplication, with ahigher satisfaction rate and fewer side effects. Measuring
for wrap and hiatus size eliminates the need for and risk ofusing stiff dilators. By utilizing cosurgeons and currentlyavailable technology, cost, operative time, hospital time,and complications can be reduced to a finite minimum.
Key words: Partial fundoplication — Nissen-Rosetti fun-doplication — Toupet procedure
Over the past 4 years laparoscopic techniques have beennewly applied to the treatment of complicated gastroesopha-geal reflux disease (GERD) in the United States. A varietyof procedures including the Nissen fundoplication, the Ro-setti modification of the Nissen fundoplication, the Toupetpartial fundoplication, the Hill procedure, and the BelseyMark 4 fundoplication have all been successfully performedvia videoscopic technology with good results [1–2, 6, 7, 9,20, 21]. The vast majority of the procedures have beenperformed for type I sliding hiatal hernia with one or moreof the following surgical indications: chronic symptomaticreflux with objective evidence of esophagitis refractory tomaximal medical management, grade 4 esophagitis withstricture, Barrett’s metaplasia, esophageal ulceration withhemorrhage, and chronic aspiration with resultant pneumo-nia, asthma, or acute airway obstruction.
We have previously reported on the outcomes and costanalysis of our first 52 Nissen-Rosetti fundoplications doneor attempted laparoscopically [2]. Emphasis on technicalfactors that enhance the ease of the procedure was made andthe safety and cost-effectiveness of the procedure was con-firmed. Following is an update and results analysis of 125laparoscopic Nissen-Rosetti fundoplications as well as thedescription and results analysis of a modified laparoscopicToupet partial fundoplication technique used in 101 cases.
Materials and methods
In October 1992 we embarked on a prospective sequential clinical study toevaluate the outcome and effectiveness of the laparoscopic approach to
Correspondence to:D. D. Coster, Surgical Associates, 122 Fourth Avenue,Grinnell, IA 50112, USA
Surg Endosc (1997) 11: 625–631
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

antireflux surgery. All patients who have been considered to be surgicalcandidates based on the standard accepted criteria for surgical interventionfor complicated gastroesophageal reflux disease and who have been medi-cally competent to withstand surgery have been entered into the study. Allof the fundoplication procedures have been done by the same five surgeonswith a standardized cosurgeon approach.
The medical/diagnostic workup of patients entering the study consistedof a history and physical examination, chest X-ray, EKG, complete labo-ratory profile, upper GI series, fluoroesophagography, upper abdominalultrasound, and esophagogastroduodenoscopy with or without biopsy.Esophageal manometry and 24-h pH testing were reserved for cases withan atypical presentation, lack of esophagitis on endoscopy, or symptoms orfindings suggestive of esophageal motility disturbances based on history oron any one of the evaluative tests.
During the 3 years of the study, the referral pattern has changed so thatgastroenterologists, internists, and surgeons have referred patients as wellas family physicians. Those patients with thorough evaluations done else-where were not retested unless symptoms had changed significantly. The
majority of diagnostic upper endoscopies, esophageal dilatations, and otherendoscopic therapeutic procedures were done by the surgeons involved inthe study.
The technical aspects of our approach to laparoscopic antireflux sur-gery are as follows. A cosurgeon approach is used in all cases, reducingoperative time and improving safety. Each experienced surgeon operatesfrom his side of the table or assists the opposite surgeon, depending on whocan best do each part of the procedure from their position at the table. Asix-trocar technique allows for placement of a right lateral port for a fixed-position liver retractor, a right upper quadrant port for the cosurgeon’s use,an upper midline port and a left upper quadrant port for the surgeon’s use,and a left lateral port for a Babcock retractor for manipulation of thestomach and gastroesophageal junction. A 45° lens is a necessity so that adownward view of the operative field can be obtained through the supra-umbilical port. A nasogastric tube is placed for gastric decompression,though occasionally placement must wait until the hiatal hernia has beenreduced in order to get the tube to traverse the gastroesophageal junction.Complete dissection of the hiatus with nothing in the esophagus is perfectly
Figs. 1 and 2.Sharp dissection of the peritoneum just above the fundusfrom the left crus all the way over to the first short gastric vessel,followed by excessiveblunt dissection behind the fundus.
Fig. 3. The size of the hiatal opening is then measured using the end ofthe USSC roticulating bowel grasper.
Fig. 4. A sling maneuver is then performed, passing the fundus backand forth to be certain it has no twists.
Figs. 5 and 6.The first stitch incorporates the esophagus at the rightgastroesophageal junction, the fundus, and the pre-aortic fascia andmuscle below the junction of the crural leaves with the first stitch. Theesophagus, fundus, and right crus at the level of the cruralreapproximation are incorporated with the second, thus fixing in place atleast a 2-cm intraabdominal length of esophagus.
Fig. 7. A third suture incorporates the right anterior esophagus and themidportion of the wrap, bringing the right side of the partialfundoplication into its final position.
626

acceptable. Starting the dissection by opening the lesser sac near the cau-date lobe of the liver immediately exposes the right crus as a landmark,facilitating the rest of the dissection. The space between the right crus andesophagus is then opened, followed by the complete dissection of the rightcrus posteriorly until it is seen joining the left crus, actually dissecting themajority of the left crus and creating as much of the posterior esophagealwindow as possible from the right side of the esophagus. Once the anterioresophageal peritoneal covering is opened, and the fundus and angle of Hisis taken down, the window behind the esophagus is already completelyopen and little further dissection is required.
The most important technical point of the entire operation is tocom-pletelytake down the fundus off of the left hemidiaphragm, as the fundusis what makes up the wrap, not the body. This requires sharp dissection ofthe peritoneum just above the fundus from the left crus all the way over tothe first short gastric vessel, followed byextensiveblunt dissection behindthe fundus until it is laying there floppy (Figs. 1 and 2). The windowbehind the esophagus will then be huge, and any remaining attachmentscan easily be removed using a blunt dissector applied from the patient’sright side. It is not necessary to take down any short gastric vessels as long
as this technique is used. There is always ample fundus to use for the wrapusing this dissection approach.
The crura arealways approximated behind the esophagus, taking alarge bite of muscleand peritoneum. One stitch is usually all that isnecessary, and the strength of that stitch is in the peritoneal lining. Thesize of the hiatal opening is then measured using the end of the USSCroticulating bowel grasper. It should be 3 to 3.5 cm from front to back,large enough to accommodate a 60 Fr. bougie, but eliminating the actual needto use one (Fig. 3). Once the size of the opening is confirmed, the roticu-lating grasper can then be passed behing the esophagus to grasp the fundus5 cm lateral to the gastroesophageal junction as it is passed by the othersurgeon.
A ‘‘sling’’ maneuver is then performed, passing the fundus back andforth to be certain it is slack and has no twists. The sling is measured to 6cm in length for a partial fundoplication, and to 8 to 9 cm for a completefundoplication. This measurement is based on the formula {3.14 × diam-eter} for determining the circumference of a circle, in this case, an imagi-nary esophagus with an imaginary 60 Fr. bougie in it that has a totaldiameter of 2.5 to 3 cm (Fig. 4). Measuring eliminates the actual need for
627
bougie placement and the potential for tissue trauma or esophageal orgastric perforation.
Suture placement for the Nissen or Nissen-Rosetti is well known, twostitches commonly being used to fasten the right and left sides of the fundalsling to the anterior esophagus at the gastroesophageal junction and 2 cmabove it, being careful to avoid the anterior vagus nerve. The Endostitch(USSC) instrument is used to do all of the sewing, as it can significantlyreduce operative time.
Many different suture placements for the partial fundoplication havebeen described. We use a five-stitch technique. The first stitch incorporatesthe esophagus at the right gastroesophageal junction, the fundus, and thepre-aortic fascia and muscle below the junction of the crural leaves with thefirst stitch. The esophagus, fundus, and right crus at the level of the cruralreapproximation are incorporated with the second, thus fixing in place atleast a 2-cm intraabdominal length of esophagus (Figs. 5 and 6).
The final two sutures fasten the anterior superior fundus on the left tothe left anterior gastroesophaeal junction and to the esophagus 2 cm abovethat point (Fig. 7). The completed partial wrap should leave at least a 1-cmarea of the anterior esophagus bare. This will allow proper relaxation of thewrap and esophagus with swallowing and always create an adequate high-pressure zone. A third suture incorporates the right anterior esophagus andthe midportion of the wrap, bringing the right side of the partial fundopli-cation into its final position (Fig. 7).
Upon completion of the procedure, the skin is closed with clips, theport sites are injected with Marcaine, and the NG tube is pulled. OralToradol and PCA Demerol are used if the patient has any significant pain.A single dose of IV Zofran and Ancef is given preoperatively for controlof postop nausea and infection prophylaxis, respectively. Diet is advancedfrom full liquids to regular as quickly as the patient can tolerate it, gener-ally within a few hours of surgery. The patient is usually discharged within24 h; up to 10% may go home the day of surgery. Skin clips are replacedwith benzoin and Steristrips at discharge. No carbonated beverages areallowed for at least a few days. Very cold drinks are discouraged, as theycause esophageal spasm in the immediate postop period.
Patient data
Patient data for the total group is summarized in Table 1. The patients werereferred by 19 family physicians, four internists, six surgeons, and twogastroenterologists. A total of 37 communities and five states are repre-sented by the group.
All patients were seen at 1 and 6 weeks postoperatively, at least. Fur-ther follow-up was done by a standardized questionnaire that was sent outto all participants in the study in late 1995, 1 month to 3 years after initialsurgery.
Data analysis was done using the Mann-Whitney test and the chi-
square test for determining probability values for certain comparative datasets within the two subgroups of patients.
Results
The overall group results are summarized in Table 2. Majorreductions in operative time and length of hospital stay werenoted during the course of the study. Laparoscopic costswere dramatically less than open costs. Complication ratesand revision rates were low. There were no gastric or esoph-ageal perforations.
All but five cases (2%) were completed laparoscopi-cally. Reasons for conversion to an open procedure includedextensive adhesions from previous surgery in two, fragiletissues unable to tolerate the trauma of the laparoscopicinstruments in one, a bowel injury while placing a trocarusing an open technique in one with multiple previous sur-geries and dense adhesions, and bleeding from an aberrantleft hepatic artery in one.
Major operations done concurrently with the antirefluxprocedure included cholecystectomy in 19, umbilical or in-guinal hernia repair in four, highly selective vagotomy inone, epiphrenic diverticulectomy in one, and cricopharyn-geal myotomy in one for a symptomatic Zenker’s diverticu-lum.
A total of 11 (5%) postop endoscopies were done forprolonged dysphagia after the laparoscopic Nissen-Rosettifundoplication or for follow-up of Barrett’s metaplasia,with none demonstrating any visual evidence of esophagitis.Those with Barrett’s metaplasia all had a decrease in theamount and severity of inflammation and no progression ofdisease, but there was no regression of the abnormal epi-thelium.
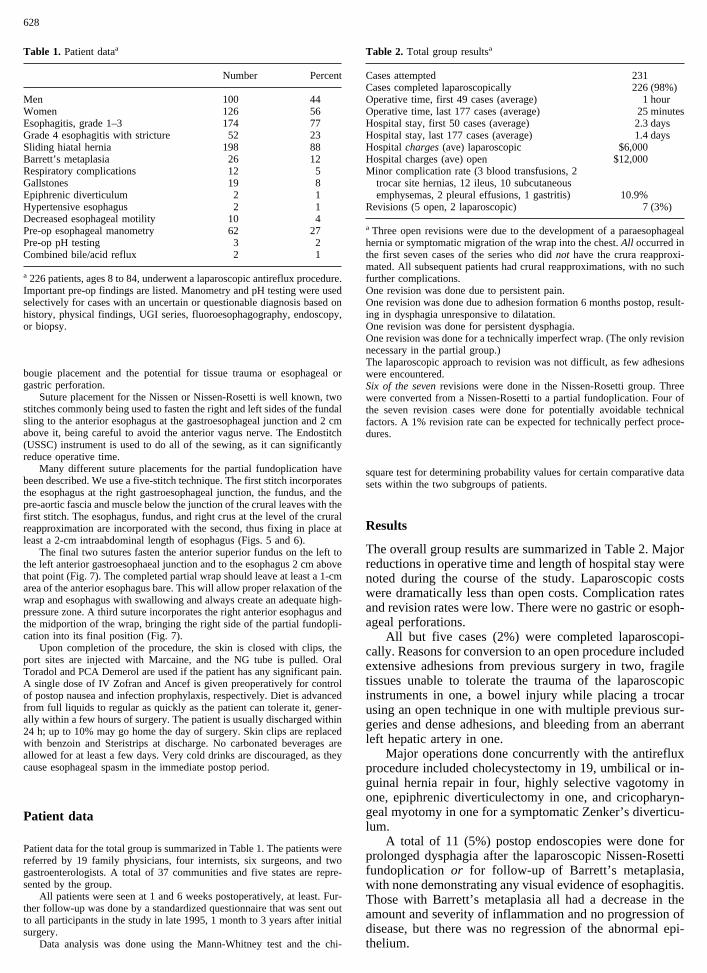
Table 1. Patient dataa
Number Percent
Men 100 44Women 126 56Esophagitis, grade 1–3 174 77Grade 4 esophagitis with stricture 52 23Sliding hiatal hernia 198 88Barrett’s metaplasia 26 12Respiratory complications 12 5Gallstones 19 8Epiphrenic diverticulum 2 1Hypertensive esophagus 2 1Decreased esophageal motility 10 4Pre-op esophageal manometry 62 27Pre-op pH testing 3 2Combined bile/acid reflux 2 1
a 226 patients, ages 8 to 84, underwent a laparoscopic antireflux procedure.Important pre-op findings are listed. Manometry and pH testing were usedselectively for cases with an uncertain or questionable diagnosis based onhistory, physical findings, UGI series, fluoroesophagography, endoscopy,or biopsy.
Table 2. Total group resultsa
Cases attempted 231Cases completed laparoscopically 226 (98%)Operative time, first 49 cases (average) 1 hourOperative time, last 177 cases (average) 25 minutesHospital stay, first 50 cases (average) 2.3 daysHospital stay, last 177 cases (average) 1.4 daysHospitalcharges(ave) laparoscopic $6,000Hospital charges (ave) open $12,000Minor complication rate (3 blood transfusions, 2
trocar site hernias, 12 ileus, 10 subcutaneousemphysemas, 2 pleural effusions, 1 gastritis) 10.9%
Revisions (5 open, 2 laparoscopic) 7 (3%)
a Three open revisions were due to the development of a paraesophagealhernia or symptomatic migration of the wrap into the chest.All occurred inthe first seven cases of the series who didnot have the crura reapproxi-mated. All subsequent patients had crural reapproximations, with no suchfurther complications.One revision was done due to persistent pain.One revision was done due to adhesion formation 6 months postop, result-ing in dysphagia unresponsive to dilatation.One revision was done for persistent dysphagia.One revision was done for a technically imperfect wrap. (The only revisionnecessary in the partial group.)The laparoscopic approach to revision was not difficult, as few adhesionswere encountered.Six of the sevenrevisions were done in the Nissen-Rosetti group. Threewere converted from a Nissen-Rosetti to a partial fundoplication. Four ofthe seven revision cases were done for potentially avoidable technicalfactors. A 1% revision rate can be expected for technically perfect proce-dures.
628

All patients with respiratory symptoms thought to berelated to esophageal reflux had either complete resolutionof all symptoms or a dramatic improvement with decreasedbronchodilator requirements. Two who were on prednisonefor refractory ‘‘asthma’’ were taken off of that drug within2 months of surgery. All reported decreased shortness ofbreath and improved exercise tolerance.
Measurable objective comparisons between the Nissen-Rosetti group and the partial fundoplication group are sum-marized in Table 3.
Subjective comparisons between the two groups basedon the responses to the standardized questionnaire are sum-marized in Table 4.
Discussion
Laparoscopic antireflux surgery has rapidly evolved as thetreatment of choice for complicated gastroesophageal refluxdisease in patients who can withstand a general anesthetic.All of the standard procedures have been applied laparo-scopically with excellent results and minimal complicationrates. It would appear that antireflux surgery is a nearlyperfect type of operation for the laparoscope, as it is a matterof only dissection and repositioning of organs into theirproper locations, with minor modifications. The exposurewith modern equipment is superb, and advancing technol-ogy has made dissecting and suturing an easier task.
Unfortunately, it has been our experience that manypatients are not referred when it first becomes evident thatmedical management is not working, resulting in a consid-erable delay (sometimes years) before definitive surgicaltreatment can be undertaken. The usual explanation forthe delay is that the patient’s condition is not yet ‘‘badenough,’’ or the expected side effects of the surgery areworse than the disease itself (a clear misconception basedon the long, tight wrap of old). This untimeliness of inter-vention can result in permanent esophageal fibrosis, injury,and dysfunction that surgery cannot alleviate, emphasizingthe importance of recognizing early on those patients thatrequire surgical treatment [16]. Patients withcombinedacid/bile reflux do not respond well to treatment with H2blockers or proton-pump antagonists, so prolonged treat-ment with those agents in the face of this problem is con-
traindicated [8]. Those patients with respiratory complica-tions of GERD should be operated upon early, as no amountof acid-reducing or propulsive medication is going to solvetheir respiratory problems. Severe lung damage can occurover the years, some of which may not be reversible.
Progression to dysphagia and stricture in spite of maxi-mal medical therapy is a clear indication for surgery. Re-peated stricture dilatation in this situation is treating a com-plication of a disease process rather than treating the diseaseitself and is inappropriate.
Persistent symptoms in spite of maximal medical man-agement, continued objective evidence of esophagitis inspite of maximal medical management, esophageal ulcerformation, hemorrhage, and Barrett’s epithelium are all in-dications for surgery.
A ‘‘shortened’’ esophagus isnot a contraindication to alaparoscopic approach to surgical repair. On the contrary,visualization is superb in the lower mediastinum with a 45°lens, and dissection and lengthening of the retracted esopha-gus is relatively straightforward. The main fibers holdingthe retracted esophagus in the mediastinum are the denseposterior phrenoesophageal ligaments, which must be tran-sected posterior to the esophagus, thus releasing the organ toits usual length. The anterior and lateral esophageal attach-ments, though important to release in the lower mediasti-num, are not the main retractile elements holding theesophagus in an abnormal location. We have yet to see atrue ‘‘shortened’’ esophagus, although we have operated onmany with that preoperative diagnosis. We question theexistence of such an entity; ‘‘retracted’’ esophagus betterdescribes the condition and reflects the fact that the esopha-gus is in fact of normal length, not shortened.
Barrett’s metaplasia is presumed to be the end result ofinadequately treated GERD and significantly increases therisk of adenocarcinoma of the esophagus. This risk appearsto be highest in patients with combined acid and bile reflux.The number of cases of Barrett’s metaplasia in our series isdiscouraging and indicates a failure of adequate medicaltreatment or delay in referral in every case. These patientsare not only exposed to an increased risk of cancer, but alsomust undergo semiannual endoscopy with biopsy for sur-veillance, an expensive and anxiety-provoking situation forthe patient. A number of these people will go on to developcarcinoma and will require esophagectomy. Clearly there
Table 3. Objective comparative group resultsa
Nissen-RosettiPartialfundoplication
1. Number of patients 125 1012. Median follow-up 30 months 12 months3. Dysphagia requiring dilatation 8 (6%) 0 (0%)
(p < 0.01)
4. Preop LES pressure (62 patients)2.7 mmHg (average
both groups)5. Postop LES pressure 15 mmHg (average) 15 mmHg (average)
(15 patients) (10 patients)6. Measured length of LES pressure zone 2.0–3.0 cm 2.0–3.0 cm (both groups)7. Recurrent postop stricture requiring dilatation
(both within 3 weeks of surgery) 2 (1.6%) 0
a Most patients refused repeat postop studies, as they felt clinically well; 25 agreed to postop esophagealmanometry.
629

are ample reasons to promote a curative surgical approachbefore the development of such complications.
Is there any advantage to performing a 360° (Nissen)wrap? The side effects of the Nissen wrap include flatu-lence, early satiety, mild weight loss, nausea, odynophagia,dysphagia, bloating, and difficulty belching and vomiting.The majority of these side effects soften with time, aretolerable to the patient, and are a reasonable trade-off fortheir usual symptoms of GERD. However, the surgeon mustbe prepared to help the patient deal with these side effects,which may be long term for many [17]. Cure rates for partialfundoplication procedures are identical to the Nissen pro-cedure, objective findings of postoperative pH testing andesophageal manometry are virtually identical, and the sideeffects are definitely fewer [10–12, 18]. Our findings clearlysupport the findings of others who have documented equalcure rates and objective measurements of wrap function aswell as increased patient satisfaction due to decreased sideeffects for the partial fundoplication compared to the Nissenfundoplication. The ability of those undergoing the partialwrap to resume intake of regular food immediately aftersurgery is impressive in our experience. It virtually elimi-nates the risk of significant dysphagia and the need forprolonged diet modification.
A partial fundoplication can be done on any patient withcomplicated GERD and is the preferred wrap for those withscleroderma or a hypomotile esophagus. We fully expect tosee the partial fundoplication become the procedure ofchoice for the surgical treatment of complicated GERD dueto its ease of application, well-documented curative out-come, and few side effects. There is no circumstance whena complete wrap would be superior to a partial one, exceptin the case of an intraoperative distal esophageal perfora-tion, where a complete wrap may be necessary to reinforcethe repair of the perforation, something that should be anextremely rare event using a measuring technique to prop-erly fashion the fundoplication.
In general, patients that present with a classic history forGERD and endoscopic and radiographic findings that con-firm the problem always have an incompetent lower esoph-ageal sphincter mechanism on manometry and have abnor-mal 24-h pH testing [19]. Therefore, thesestraightforwardcases do not require manometry and 24-h pH testing for
diagnostic workup (63% of patients in this series) [5]. Thosecases with an atypical presentation suggestive of esophagealmotility problems, gastric emptying abnormalities, medica-tion-induced disease, or primary duodenogastric bile refluxmust all have esophageal manometry and may need a com-bination of tests including 24-h pH testing, gastric emptyingstudies, and biliary scans. Respiratory complaints are themost difficult to evaluate, so a high index of suspicion isnecessary for those presenting with a combination of asthmaand GERD.
The patient with complicated GERD is extremelypleased with the outcome of laparoscopic antireflux surgery[2, 13, 20]. Reduced pain, very short hospitalization, lowercost, and quick return to normal activities and work makethis approach very attractive, although patient satisfactionappears to be more closely related to relief of symptomsthan to the technical approach to the procedure [13]. Inaddition, the ability to eliminate all reflux-related medica-tions is a big plus from a convenience and cost standpoint.The cost savings over 10 years for a surgical approach tocomplicated GERD has been estimated to be $1,500, andover 20 years to be $10,000, taking into consideration costvariations across the country as well as surgical and medicalcomplications and reoperation [4].
In summary, surgery has been conclusively demon-strated to be significantly more effective than medical man-agement of complicated gastroesophageal reflux disease asfar as symptom improvement and objective signs of esoph-agitis are concerned, with excellent long-term results [14,15]. It is also the only method of reestablishing the normalreflux barrier of the lower esophageal sphincter mechanism,allowing the return of normal esophageal and gastric physi-ology. Restoration of functionrequires the restoration ofnormal anatomy, meaning elimination of the hiatal hernia ifpresent and creation of a fixed intraabdominal esophagealcomponent. Alaparoscopicapproach to curative treatmentof complicated GERD has the added benefits of signifi-cantly reducing cost, recovery time, morbidity, and time lostfrom work. A partial fundoplication has equally good re-sults compared to the Nissen fundoplication, with fewer sideeffects and better patient satisfaction. Patients should bereferred for curative treatment before they have developedirreversible esophageal damage. By utilizing two surgeons
Table 4. Subjective comparative surveya
Nissen-RosettiPartialfundoplication
1. Number of respondents 82 (66%) 62 (62%)2. Symptomatic control (14 no improvement,
10 4 cured)9.2 (average)
(90% 8, 9, or 10)9.8 (average)
(98% 8, 9, or 10)3. Return to completely normal eating habits 83 days (p < 0.0001) 13 days4. Side effects of gassiness, spasm, or bloating
(temporary)86% 62%
5. Inability to burp 12 (15%)(p < 0.001)
0
6. Need for prescription meds for esophagealsymptoms
2 (Propulsid)(1.6%)
0
7. Return to work 17 days(p 4 0.22)
10 days
8. Return to daily routine 11 days 9 days
a Results of a standardized questionnaire sent to all patients are listed. The overall satisfaction rate andgeneral performance of those in the partial fundoplication group were superior.
630

and currently available technology, operative time, hospitaltime, and complications can be reduced to a finite mini-mum. The economic benefits to the patient and employersas well as third-party payers are significant as far as totalcost savings and minimizing lost work hours go. Laparo-scopic antireflux surgery for complicated GERD may wellprove to be one of the most important developments in thefield of laparoscopic general surgery because of the numberof patients who can benefit from it and the overall expectedlong-term improvement in their health as well as the posi-tive overall impact on economic costs.
Acknowledgment.Special thanks to Tom Moore, Ph.D., for statisticalanalysis work. Special thanks to Carlos Ferguson for supporting art work.
References
1. Aye RW, Hill LA, Kraemer JM, Snopkowski P (1994) Early resultswith the laparoscopic hill repair. Am J Surg 167: 542–546
2. Coster DD, Bower WH, Wilson VT, Butler DA, Locker SC, BrebrickRT (1995) Laproscopic Nissen fundoplication—a curative, safe, andcost-effective procedure for complicated gastroesophageal reflux dis-ease. Surg Laparosc Endosc 5(2): 111–117
3. Cuschieri A (1993) Laparoscopic antireflux surgery and repair of hia-tal hernia. World J Surg 17(1): 40–45
4. Deloitte & Touche Management Consulting (1995) Economic impactof laparoscopic Nissen fundoplication, executive summary
5. De Meester TR, Wang CI, Wernly JA, Pellegrini CA, Little AG,Klementschitsch P, Bermudez G, Johnson LF, Skinner DB (1980)Technique, indications, and clinical use of 24 hour esophageal pHmonitoring. J Thorac Cardiovasc Surg 79: 656–670
6. Hill LD, Kraemer SJM, Aye RW, Kozarek RA, et al (1994) Lapro-scopic hill repair. Contemp Surg 44(1): 13–20
7. Hinder RA, Filipi CJ, Wetscher G, Neary P, et al (1994) LaparoscopicNissen fundoplication is an effective treatment for gastroesophagealreflux disease. Ann Surg 220(4): 472–483
8. Hinder RA, Filipi CJ (1995) The laparoscopic management of gastro-esophageal reflux disease. Adv Surg 28: 41–58
9. Kraemer SJM, Aye R, Kozarek RA, Hill LD (1994) Laparoscopic hillrepair. Gastrointest Endosc 40(2, Part 1): 155–159
10. Lundell L, Abrahamsson H, Ruth M, Snadberg N, Olbe LC (1991)Lower esophageal sphincter characteristics and esophageal acid expo-sure following partial or 360 degree fundoplication: results of a pro-spective, randomized, clinical study. World J Surg 15: 115–121
11. McKernan JB (1994) Laparoscopic repair of gastroesophageal refluxdisease/Toupet partial fundoplication versus Nissen fundoplication.Surg Endosc 8: 851–856
12. Mosnier H, Leport J, Aubert A, Kianmanesh R, et al (1995) A 270degree laparoscopic posterior fundoplasty in the treatment of gastro-esophageal reflux. J Am Coll Surg 181: 220–224
13. Rattner DW, Brooks DC (1995) Patient satisfaction following laparo-scopic and open antireflux surgery. Arch Surg 130: 289–294
14. Shirazi SS, Schulze K, Soper RT (1987) Long-term follow-up fortreatment of complicated chronic reflux esophagitis. Arch Surg 122:548–551
15. Spechler SJ (1992) Comparison of medical and surgical therapy forcomplicated gastroesophageal reflux disease in veterans. New Engl JMed 326(12): 786–792
16. Stein HJ, Eypasch EP, De Meester TR, Smyrk TC, Attwood SE (1990)Circadian esophageal motor function in patients with gastroesophagealreflux disease. Surgery 108: 769–777
17. Swanstrom L, Wayne R (1994) Spectrum of gastrointestinal symptomsafter laparoscopic fundoplication. Am J Surg 167: 538–541
18. Thor KBA, Silander T (1989) A long-term randomized prospectivetrial of the Nissen procedure versus a modified Toupet technique. AnnSurg 719–724
19. Waring JP, Hunter JG, Oddsdottir M, Wo J, Katz E (1995) The pre-operative evaluation of patients considered for laparoscopic antirefluxsurgery. Am J Gastroenterol 90(1): 35–38
20. Weerts JM, Dallemagne B, Hamoir E, Demarche M, et al (1993)Laparoscopic Nissen fundoplication: detailed analysis of 132 patients.Surg Laparosc Endosc 3(5): 359–364
21. Yang HK, Del Guercio LRM, Steichen FM (1995) ThoracoscopicBelsey-Mark IV fundoplication. Surg Rounds 277–291
631

Case reports
Laparoscopic repair of a diaphragmatic hernia through the foramenof Morgagni
M. Orita, 1 M. Okino,1 K. Yamashita,1 N. Morita, 2 K. Esato2
1 Department of Surgery, Onoda City Hospital, 1863-1 Higashitakadomari, Onoda, Yamaguchi, 756 Japan2 First Department of Surgery, Yamaguchi University School of Medicine, 1144 Kogushi, Ube, Yamaguchi, 756 Japan
Received: 3 April 1996/Accepted: 3 May 1996
Abstract. A 78-year-old woman is described who pre-sented with a diaphragmatic hernia through the foramen ofMorgagni. A definitive diagnosis was confirmed by a sag-ittal view on magnetic resonance imaging prior to surgery.The hernia was repaired laparoscopically under an abdomi-nal wall lifting technique without pneumoperitoneum, andher symptoms completely resolved postoperatively with noevidence of recurrence. The laparoscopic repair was con-sidered a suitable and safe procedure for the treatment of aMorgagni hernia.
Key words: Morgagni hernia — Abdominal wall liftingtechnique without pneumoperitoneum — Laparoscopy —Omentum
Diaphragmatic hernias through the foramen of Morgagniare rare, and often the preoperative diagnosis is difficult.The standard surgical procedure has required a laparotomyor a thoracotomy for symptomatic patients. We report a caseof a Morgagni hernia which was diagnosed prior to surgeryand repaired laparoscopically, and our patient was the firstcase repaired under an abdominal wall lifting techniquewithout pneumoperitoneum.
Case report
A 78-year-old woman, complaining of epigastral discomfort and tender-ness, presented in our clinic in February 1995. She was 139 cm in heightand weighed 56 kg. She had a history of progressive weight gain of 19 kgover the previous year secondary to poor control of her hypothyroidism.Findings from all routine laboratory studies were normal; however, pul-monary function tests showed a restrictive pattern.
PA chest radiographs demonstrated an abnormal shadow with a clearborder present at the right cardiophrenic angle; the lateral projection de-termined an anterior location of the shadow. Chest computed tomography
(CT) exhibited a homogeneous, solid mass (6 × 11 cm) with smoothmargins and a region of fat density in the right anterior mediastinum (Fig.1A). A mediastinal lipoma was the suspected diagnosis at this time. Thesagittal view of a magnetic resonance imaging (MRI), however, showedcontinuous fatty tissue anterior to the liver through an anteromedial portionof diaphragm directly behind the xiphoid (Fig. 1B). Thus, an omentalherniation through the foramen of Morgagni was considered to be thediagnosis.
Laparoscopic repair was performed on February 27, 1995. Under gen-eral anesthesia, an abdominal wall lifting technique was employed withoutpneumoperitoneum [4, 6]. Two Kirschner wires (1.2 mm in diameter) weretunneled subcutaneously, one transversely just above the umbilicus, andanother transversely just below the xiphoid process. Both wires were at-tached to lifting handles, which were raised upright, and then the abdomi-nal wall was lifted. A laparoscope was introduced through the umbilicus.There appeared to be an oval-shaped defect (2 × 3.5 cm) in the anterioraspect of the diaphragm, containing most of the omentum (Fig. 2A). Theomentum slid synchronously with her respirations. Two additional ports(15 mm in diameter) then were placed on both sides of the costal margins,through which the hernia contents were gently pulled down into the peri-toneal cavity with grasping forceps (Fig. 2B). There were no adhesionsbetween the omentum and the hernial sac. The hernial space could beapproached and visualized more easily with laparoscopy than by laparot-omy or thoracotomy (Fig. 2C).
The hernia defect was closed with five 2-0 silk interrupted sutures,using an intra-abdominal suturing technique (Figs. 2D, 3A,B). The sac wasnot removed. A thin piece of Prolene mesh (3.5 × 5 cm, Ethicon, Inc.Somerville, NJ, U.S.A.) was placed on the closed hernia ring and fixed tothe diaphragm with hernia stapler (Auto Suture, ENDO UNIVERSAL 65,United States Surgical Corporation, Norwalk, CT, U.S.A.) in order toreinforce the repaired site (Fig. 3C,D). A Penrose drain was placed in thesubphrenic space to decompress the air. The patient recovered nicely andhas had no further symptoms or evidence of recurrence following surgery.
Discussion
Hernias which occur in the retroxiphoid region are calledhernias of the foramen of Morgagni. These patients arefrequently obese adults. Our particular patient had rapidweight gain due to the poor control of her hypothyroidism.The differential diagnosis included a pleuropericardial cyst,pleural mesothelioma, pericardial fat pad, mediastinal li-poma, tumor or cyst of the diaphragm, thymoma, and ante-Correspondence to:M. Orita
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 668–670

Fig. 1. A Chest computed tomographydemonstrating a large, retrosternal, homogeneousmass with smooth margins and a fat density.B Asagittal view on magnetic resonance imagingshowing continuous fatty tissue anterior to theliver through an anteromedial portion of thediaphragm directly behind the xiphoid.
Fig. 2. A A laparoscopic view of the Morgagnihernia containing omentum extending from thetransverse colon.B The omentum was pulled backdown into the peritoneal cavity easily withgrasping forceps.C An oval-shaped defect (2 ×3.5 cm) in the anterior aspect of the diaphragm.DThe hernia defect was closed with anintra-abdominal suturing technique; the sac itselfwas not removed.
Fig. 3. A,B The threads were ligatedintra-abdominally.C,D A small piece of Prolenemesh was placed on the closed hernia ring andfixed to the diaphragm with hernia stapler in orderto reinforce the repaired site.
669

rior chest wall tumor [2]. Often the diagnosis is a difficultone to make preoperatively, especially when the sac con-tains only omentum. In our case the sagittal view of an MRIscan was very useful for making this distinction [11]. Op-erative repair is recommended in symptomatic cases or forsuspected strangulation [3]. Since this hernia occurs morefrequently in obese or elderly patients [9], the laparoscopicapproach seems more suitable than the abdominal or trans-thoracic approach, especially if the preoperative diagnosiscan be established.
There were six case reports of Morgagni herniasrepaired laparoscopically before our case [5, 7, 8, 10] (Ta-ble 1). They completed the repair under a pneumoperito-neum without intraoperative complications. Pneumoperito-neum with Morgagni hernias, however, may lead to respi-ratory or circulatory complications [1]. Furthermore, theintraperitoneal suturing technique is facilitated by employ-ing an abdominal wall lifting technique without pneumo-peritoneum.
We, therefore, conclude that the laparoscopic repair of aMorgagni hernia using an abdominal wall lifting techniqueinstead of pneumoperitoneum is technically easy, safe, anda less invasive approach to surgical treatment.
References
1. Chin EF, Duchesne ER (1955) The parasternal defect. Thorax 10:214–219
2. Comer TP, Clagett OT (1966) Surgical treatment of hernia of theforamen of Morgagni. J Thorac Cardiovasc Surg 52: 461–468
3. Fisher L, O’Donnell CJ (1990) A complication of a Morgagni hernia.Australas Radiol 34: 86–88
4. Hashimoto D, Nayeem SA, Kajiwara S, Hoshino T (1993) Laparo-scopic cholecystectomy: an approach without pneumoperitoneum.Surg Endosc 7: 54–56
5. Kuster GGR, Kline LE, Garzo G (1992) Diaphragmatic hernia throughthe foramen of Morgagni: laparoscopic repair case report. J Laparo-endosc Surg 2: 93–100
6. Nagai H, Kondo Y, Yasuda T, Kasahara K, Kanazawa K (1993) Anabdominal wall-lift method of laparoscopic cholecystectomy withoutperitoneal insufflation. Surg Laparosc Endosc 3: 175–179
7. Newman L, Eubanks S, Bridges WM, Lucas G (1995) Laparoscopic diag-nosis and treatment of Morgagni hernia. Surg Laparosc Endosc 5: 27–31
8. Rau HG, Schardey HM, Lange V (1994) Laparoscopic repair of aMorgagni hernia. Surg Endosc 8: 1439–1442
9. Saha SP, Mayo P, Long GA (1982) Surgical treatment of anteriordiaphragmatic hernia. South Med J 75: 280–281
10. Smith J, Ghani A (1995) Morgagni hernia: incidental repair duringlaparoscopic cholecystectomy. J Laparoendosc Surg 5: 123–125
11. Yeager BA, Guglielmi GE, Schiebler ML, Gefter WB, Kressel HY(1987) Magnetic resonance imaging of Morgagni hernia. GastrointestRadiol 12: 296–298
Table 1. Laparoscopic repair in cases of Morgagni hernias
Author Age Gender DiagnosisSide ofthe lesion
Size ofthe defect Contents
Removal ofthe sac Mesh placement
Kuster et al.1992 [5] 67 Female Laparoscopic Right ? Omentum, colon Not removed Not placed
Rau et al.1994 [8] 42 Male Preoperative Right 6 cm Omentum Removed Placed
Newman et al. 57 Female Laparoscopic Right ? Omentum, colon Removed Placed1995 [7] 22 Female Incidental Right ? Liver Removed ? Not placed
70 Female Incidental Right 10 × 15 cm ? Removed ? Not placedSmith and Ghani
1995 [10] 60 Female Incidental Right ? 2 × 3.5 cm Omentum, colon Not removed Not placedOrita et al. 1996 78 Female Preoperative Right 2 × 3.5 cm Omentum Not removed Placed
670

Letters to the editor
The totally extraperitoneal laparoscopic hernia repair
We read with interest the paper by Vanclooster and col-leagues [11] and commend their contribution to this proce-dure. However, we would offer three comments:
First, totally extraperitoneal laparoscopic hernia repairwas developed by Dulucq [1–3] in 1989/90 and by Mc-Kernan [7] not a great deal later. While it seems legitimatefor others to publish their own technical variations, devel-opments, and outcomes, we strongly support recent remind-ers [6] that journal editors and their peer referees owe thereader a duty of diligence: they should insist that authorsexercise proper scholarship by giving credit where it is due.Otherwise the uninformed reader may assume originalityand the informed may infer plagiarism, where the authorintended neither.
Second, the mesh configuration suggested by Van-clooster et al. was presented by one of us several years ago[4, 10]. However, the concept of amputating the inferior andlateral corner ‘‘so the mesh fits better on the iliac vesselsand the psoas muscle’’ is flawed, since it has subsequentlybeen reported [12] that recurrences may occur dorsal/inferior to this inferolateral corner. The most extensive pos-sible coverage of the psoas muscle belly is therefore appro-priate.
Third, the need for mesh fixation remains debatable.However, to fix the cranial border to ‘‘prevent early migra-tion or slipping’’ is illogical: In our joint experience of over1,000 cases and, to our knowledge in all reports in the worldliterature, recurrences pass uniformly caudal to the inferiorborder of the prosthesis. Fixation of the inferior medial partof the mesh to Astley Cooper’s ligament alone [5] may notoffend against the original tension-free notion of Stoppa [8,9] nor interfere with the mechanics of prosthesis retention.To fix the superior border to points that move relative to oneanother within a musculofascial structure contravenes bothprinciples.
Finally, on a minor point, if the structure annotated as‘‘D’’ in Fig. 1 is the testicular vascular bundle, where is thevas deferens?
Despite these comments we congratulate the authors ontheir low complication rate.
References
1. Dulucq J-L (1991) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneale en retrope´ritoneoscopie. CahChir 79: 15–16
2. Dulucq J-L (1992) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneal en pre´-peritoneoscopie. Chirur-gie 118(1–2): 83–85
3. Dulucq J-L (1992) The treatment of inguinal hernias by implantationof mesh through retroperitoneoscopy. Postgrad Gen Surg 4: 173–174
4. Fiennes AGTW, Taylor RS (1994) Learning laparoscopic hernia re-pair. In: Inguinal hernia, advances or controversies? Arregui M, NaganR (eds) Radcliffe, Oxford, pp 475–482
5. Fiennes AGTW, Himpens J, Dulucq J-L (1994) Preperitoneoscopicgroin hernioplasty, current synthesis. Surg Endosc 8(8): 989
6. Horton R, Smith R (1996) Time to redefine authorship (editorial). BrMed J 312: 723
7. McKernan JB (1993) Laparoscopic extraperitoneal repair of inguino-femoral herniation. Endosc Surg Allied Tech 1(4): 198–203
8. Stoppa R, Petit J, Abourachid H (1973) Proce´deoriginal de plastie deshernies de l’aine. L’interposition sans fixation d’une prothe`se en tullede Dacron par voie me´diane pre´peritoneale. Chirurgie 99: 119
9. Stoppa RE, Rives JL, Warlaumont CR (1984) The use of Dacron in therepair of hernias of the groin. Surg Clin North Am 64: 269–285
10. Taylor RS, Fiennes AGTW (1992) A tension free modification of theDulucq preperitoneal laparoscopic hernioplasty. Min Inv Ther 1(Suppl1): 101
11. Vanclooster P, Meersmann AL, de Gheldere CA, Van de Ven CK(1996) The totally extraperitoneal laparoscopic hernia repair. SurgEndosc 10: 332–335
12. Vivekanadan S, Fiennes AGTW (1995) Totally extraperitoneal groinhernioplasty: mechanism of delayed indirect recurrence. Min Inv Ther4(Suppl 1): 55
A. Fiennes
Department of SurgerySt George’s Hospital Medical SchoolCranmer TerraceLondon, SW17 ORE, United Kingdom
J. Himpens
Department of Digestive SurgeryUniversity Hospital Ste PierreRue Haute 201B-1000 Brussels, Belgium
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 696

The author replies
We thank you for the opportunity to answer the letter of Mr.Fiennes. First of all, we certainly do acknowledge that Mr.Dulucq and Mr. Mc Kernan were the pioneers of the extra-peritoneal laparoscopic hernia repair. Honor to whom honoris due. We did not intend to pretend to be the pioneers ofthis technique. We wished only to describe the technique theway we perform it, to describe our own findings, and to givea fair report of our preliminary results.
The reason for cutting the inferolateral corner is not justthat we think it fits better on the iliopsoas but also becausewe are afraid to cause damage to the nerves running on it bydissecting unnecessarily high on the muscle. Since the meshmeasures 15 × 15 cm, we do not think we compromise thestrength of the repair by merely removing a small piece ofits inferolateral corner. We think that dissecting very highon the muscle just to position the whole inferolateral cornerof the mesh flat on the muscle is unnecessary and danger-ous.
We do agree totally that fixation of the mesh is unnec-
essary provided the mesh is large enough, which is obvi-ously the case when using a 15 × 15 cm mesh. In fact, wehave not fixed the mesh since January 1996.
We also agree that the vas deferens is not clearly seen onFig. 1. We chose this shot because of the clearly visiblelarge direct defect.
C. de Gheldere
Heilig Hart ZiekenhuisKolveniersvest 20B-2500 LIERBelgium
P. Vanclooster
Bouwelsesteenweg 62560 NijlenBelgium
Surg Endosc (1997) 11: 697
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The influence of pneumoperitoneum on the peritoneal implantation offree intraperitoneal cancer cells
Recently Hubens et al. published an interesting article en-titled ‘‘The influence of a pneumoperitoneum on the peri-toneal implantation of free intraperitoneal colon cancercells’’ [2]. They reported on the possible implantation ofcancer cells at trocar wounds at the moment of deflation ascells are forced through these wounds by the pressure gra-dient created by the pneumoperitoneum during laparoscopicsurgery for malignant disease. We would like to point outthat this ‘‘chimney effect,’’ as originally described by us,can occur during the entire laparoscopic procedure and notonly at the moment of deflation, as leakage of CO2 along-side trocars during surgery is impossible to prevent with theexisting trocars [3]. Consequently, deflation of the pneumo-peritoneum by letting CO2 escape through one of the trocarsbefore pulling these trocars out of the abdomen will notprevent the occurrence of entrapment of cancer cells in thetrocar wounds.
We fully agree with the authors on the possible advantageof gasless laparoscopy as this could prevent the ‘‘chimneyeffect.’’ In our experimental work we found significantly lesstumor growth at the port sites following gasless laparoscopicsurgery for colon cancer in the rat as compared to laparoscopicsurgery using a CO2 pneumoperitoneum. This techniqueseems promising to treat malignant disease laparoscopically.
References
1. Bouvy ND, Marquet RL, Jeekel J, Bonjer HJ (1996) Impact of gas (less)laparoscopy and laparotomy on peritoneal tumor growth and abdominalwall metastases. Surg Endosc 10: 551
2. Hubens G, Pauwels M, Hubens A, Vermeulen P, Van Marck E, EyskensE (1996) The influence of a pneumoperitoneum on the peritoneal im-plantation of free intraperitoneal colon cancer cells. Surg Endosc 10:809–812
3. Kazemier G, Bonjer HJ, Berends FJ, Lange JF (1995) Port site metas-tases after laparoscopic colorectal surgery for cure of malignancy. Br JSurg 82: 1141–1142
G. Kazemier1
F. J. Berends1
N. D. Bouvy1
J. F. Lange2
H. J. Bonjer1
1 Department of SurgeryUniversity Hospital Rotterdam-DijkzigtDr Molewaterplein 403015 GD, RotterdamThe Netherlands2 Department of SurgerySt. Clara HospitalRotterdamThe NetherlandsCorrespondence to:G. Kazemier
Surg Endosc (1997) 11: 698
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The author replies
We thank Dr. Kazemier et al. for their kind remarks and fullyagree with them that gas leakage can occur during the entireprocedure with subsequent implantation of tumor cells at thetrocar sites. At the moment we are conducting further experi-mental studies on the possible effects of gas leakage on tumorcell implantation and the ‘‘chimney effect,’’ as they havecalled it. Results will be ready for publication soon.
G. Hubens
Department of SurgeryUniversity HospitalUniversity of AntwerpWilrijkstraat 102650 EdegemBelgium
Surg Endosc (1997) 11: 699
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

Laparoscopic cholecystectomy using abdominal wall retraction
Hemodynamics and gas exchange, a comparison with conventional pneumoperitoneum
D. W. Meijer, 1,2 B. P. M. Rademaker,3 S. Schlooz,3 W. A. Bemelman,4,5 L. T. de Wit, 4 J. J. G. Bannenberg,6
T. Stijnen,2 D. F. Gouma4
1 Working Group Development Surgical Technology, Surgical Division, Academic Medical Centre, IWO-gebouw 1 etage k151, University ofAmsterdam, Amsterdam, The Netherlands2 Department of Epidemiology and Biostatistics NIHES, Erasmus University Rotterdam, Rotterdam, The Netherlands3 Department of Anesthesiology, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands4 Department of Surgery, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands5 Department of Surgery, Academic Hospital Leiden, University of Leiden, Leiden, The Netherlands6 Department of Experimental Surgery, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Received: 28 May 1996/Accepted: 14 October 1996
AbstractBackground:Disadvantages related to CO2 pneumoperito-neum have led to development of the abdominal wall re-tractor (AWR), a device designed to facilitate laparoscopicsurgery without conventional pneumoperitoneum (15mmHg CO2). We investigated the effects of the AWR onhemodynamics and gas exchange in humans. We also in-vestigated whether the use of an AWR imposed extra tech-nical difficulties for the surgeon. A pilot study revealed thatcholecystectomy without low-pressure pneumoperitoneumwas technically impossible.Methods: A prospective randomized controlled trial:Twenty patients undergoing laparoscopic cholecystectomywere randomly allocated into group 1: AWR with low-pressure pneumoperitoneum (5 mmHg), or group 2: con-ventional pneumoperitoneum (15 mmHg).Results:Surgery using the AWR lasted longer, 72 ± 16 min(mean ± SD) vs 50 ± 18 min compared with standard lap-aroscopic cholecystectomy. There were no differences be-tween the groups with respect to hemodynamic parameters,although a small reduction of the cardiac output was ob-served using conventional pneumoperitoneum (from 3.9 ±0.7 to 3.2 ± 1.1 l/min) and an increase during AWR (from4.2 ± 0.9 to 5.2 ± 1.5 l/min). Peak inspiratory pressures weresignificantly higher during conventional pneumoperitoneumcompared to AWR. A slight decrease in pH accompanied byan increase in CO2 developed during pneumoperitoneumand during the use of the AWR. In both groups arterial PO2decreased.
Conclusions:The results indicate that the view was im-paired during use of the AWR and therefore its use wasdifficult and time-consuming. Possible advantages of thisdevices’ effects on hemodynamics and ventilatory param-eters could not be confirmed in this study.
Key words: Abdominal wall retraction — Abdominal wallretractor — Pneumoperitoneum
Carbon dioxide (CO2) pneumoperitoneum of 15 mmHg in-traabdominal pressure is generally used for laparoscopicsurgery. Side effects of a pneumoperitoneum such as car-diovascular depression and respiratory acidosis have beendescribed and may be potentially dangerous in patients withunderlying diseases [12]. In addition, CO2 embolism is afeared, although rare, complication of laparoscopic surgerywith pneumoperitoneum, with potentially fatal outcome [7].These disadvantages have led to development of alternativestrategies.
The abdominal wall retractor (AWR) is a new devicedesigned to create a good view during laparoscopic surgerywithout the use of a pneumoperitoneum [1, 3, 5, 6, 10, 14,16]. Recently the feasibility of using the AWR for laparo-scopic surgery in pigs has been analyzed [11]. The use ofthe abdominal wall retractor was associated with fewer he-modynamic side effects and disturbances of gas exchange.However, the effectiveness in humans has not been ana-lyzed.
Although laparoscopic cholecystectomy has generallybeen performed by experienced surgeons, in our institutiona pilot human study with the AWR showed that laparoscop-ic cholecystectomy without pneumoperitoneum was ex-tremely difficult. It was not always possible to achieve ad-
Correspondence to:D. W. Meijer, Department of Surgical Research, IWOgebouw I-151, Academic Medical Centre, Meibergdreef g, 1105AZ Am-sterdam, The Netherlands
Surg Endosc (1997) 11: 645–649
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

equate exposure of the triangle of Calot, which is essentialfor safe dissection of Calot’s triangle. However, the additionof a low-pressure pneumoperitoneum enabled the surgeonto perform the procedure. Therefore, it was decided to add5 mmHg pneumoperitoneum while using the AWR.
The purpose of this study was to assess the safety andefficacy of the AWR in a prospective, randomized con-trolled clinical trial, comparing the use of AWR combinedwith low-pressure pneumoperitoneum with the CO2 pneu-moperitoneum, with particular interest in hemodynamicsand gas exchange during laparoscopic cholecystectomy. Wewere also interested in whether the use of an AWR posedextra technical difficulties for the surgeon.
Patients and methods
Twenty patients with ASA classification 1 or 2 undergoing elective lapa-roscopic cholecystectomy for uncomplicated symptomatic gallstone dis-ease gave informed consent to participate in the study. The patients wererandomly allocated into one of the two groups.
Patients in group 1 underwent laparoscopic cholecystectomy by ab-dominal wall retraction with a low-pressure pneumoperitoneum of 5mmHg. Patients in group 2 underwent standard laparoscopic cholecystec-tomy with CO2 pneumoperitoneum of 15 mmHg.
The study protocol was approved by the Hospital Ethical Committee.
Anesthesia
Premedication consisted of lorazepam 1 mg given orally approximately 1h before induction of anesthesia. A peripheral intravenous infusion of NaCl0.9% was administered at a rate of 6 mlz kg−1 z h−1. Electrocardiogram andpulse oximetry were continuously monitored during the procedure. Anes-thesia was induced with thiopental 3–5 mg/kg−1, followed by atracurium0.5 mg/kg to facilitate endotracheal intubation and fentanyl 5-mkg/kg. An-esthesia was maintained with isoflurane 1.15% (end-tidal concentration).Additional doses of atracurium were given to maintain one or two re-sponses to train-of-four stimulation. During the operation additional dosesof fentanyl were given when signs of insufficient analgesia were present,as indicated by a rise in pulse rate or a blood pressure greater than 20% ofpreinduction values.
After endotracheal intubation the lungs were ventilated with a mixtureof oxygen in air (FiO2 4 0.5). Total minute ventilation was adjusted untilan end-tidal CO2 value between 30 and 40 mmHg was achieved (Dra¨ger,Cicero, Germany). After induction of anesthesia a 20-gauge catheter wasinserted in the left radial artery for blood pressure measurements, cardiacoutput measurements, and blood gas sampling.
Surgical technique
Laparoscopic cholecystectomy with AWR.For retraction of the abdominalwall an AWR with 10-cm wings was used as described by Smith et al. [14](Laparolift TM, Origin Med Systems, Inc. Menlo Park, CA). Low-pressurepneumoperitoneum (5 mmHg) was added to the lifting procedure in allpatients. The position of the surgeon is between the legs of the patient. Firsta 10/11-mm trocar is inserted through the umbilicus using an open tech-nique. Second, the fan is introduced through a right subcostal split incisionunder direct laparoscopic vision to prevent slipping omental fat betweenthe legs of the fan and the abdominal wall. The fan is lifted with theabdominal wall retractor (AWR) up to a pressure of 10–12 on the indicatorof the fan. Two additional trocars are inserted, a 5-mm and a 10/11-mmtrocar in the right lower and left abdomen, respectively. A 5-mmHg pneu-moperitoneum is applied to achieve adequate exposure of Calot’s triangle.
Laparoscopic cholecystectomy with pneumoperitoneum.Abdominal insuf-flation with CO2 was obtained with a pressure-controlled insufflator (Elec-
tronic Laparoflator 26012, Storz, Tuttlingen, Germany). Intraabdominalpressure was controlled from the manometer on the insufflator. Pneumo-peritoneum was achieved by inserting a Veress needle subumbilically. Twoadditional 10/11-mm and one 5-mm trocars are inserted after establishmentof the pneumoperitoneum. The trocars are placed similar to the trocars usedwith the AWR.
Measurements
Measurements were performed at 1, 5, 10, 15, 30, 45 and 60 min afterstarting the pneumoperitoneum or introducing the abdominal wall retrac-tion. Control measurements were made 5 min after ceasing the pneumo-peritoneum or the abdominal wall retraction. In the final analysis, mea-surements at 45 and 60 min were not included because in seven patientsusing conventional pneumoperitoneum the procedure was finished within45 min. The following hemodynamic variables were measured: heart rate,blood pressure, and cardiac output; arterial blood pressure was recordedusing disposable transducers (Baxter, TX). Cardiac output was computedcontinuously from the radial artery pressure, as described by Wesseling etal. [15]. The following ventilatory parameters were measured; end-tidalCO2 (EtCO2), arterial pH, arterial PCO2, arterial PO2, and peak inspiratorypressure. End-tidal CO2 was measured with an infrared mainstreamtransducer (Hewlett Packard, Saronno, Italy). Blood-gas samples were ana-lyzed by a routine method (ABL 4, Radiometer A/S, Copenhagen, Den-mark).
Statistical analysis
Results are expressed as mean ± SD. Data were analyzed with two-wayANOVA for repeated measures between and in between the groups. Whenindicated, differences between means within the groups were analyzedusing pairedt-test means and unpairedt-tests for differences betweenmeans between the groups. Patient characteristics and operation time wereanalyzed with the Mann-Whitney U test.p values of <0.05 were consideredstatistically significant.
Results
Patient characteristics are presented in Table 1. There wereno significant differences between the study groups. Opera-tions performed using the AWR with supplemental low-
Table 1. Patient characteristics
Pneumoperitoneum(15 mmHg)
Abdominal wallretraction +low-pressurepneumoperitoneum(5 mmHg)
Sex F/M 7/2 8/1 nsAge (years) 30–52 22–50 nsWeight (kg) 65 ± 11 68 ± 14 nsHeight 168 ± 7 163 ± 9 ns
Table 2. Operation data and complications
Pneumoperitoneum(15 mmHg)
Abdominal wallretraction +low-pressurepneumoperitoneum(5 mmHg)
Conversion to open surgery 1 1Duration operation (min) 50 ± 18 72 ± 16*Postoperative complication 0 0
* p < 0.05 compared with conventional pneumoperitoneum.
646

pressure pneumoperitoneum lasted significantly longercompared to conventional surgery (Table 2). In two patients(one in each group) the operation could not be completeddue to technical difficulties for which the operation wasconverted (Table 2).
Hemodynamic and ventilatory data are presented inFigs. 1 and 2. There were no significant differences betweenthe groups with respect to baseline and changes in heart rateand systolic blood pressure. Transient increases in diastolicblood pressure during abdominal wall retraction did notresult in significant differences with pressures measuredduring conventional pneumoperitoneum. Cardiac output re-mained unchanged during conventional pneumoperitoneumand showed a significant increase during abdominal wallretraction with low-pressure pneumoperitoneum, whereas atthe start of insufflation a significant reduction of the cardiacoutput was observed with conventional pneumoperitoneum.
Peak inspiratory pressures increased significantly duringlaparoscopy using conventional pneumoperitoneum. In con-trast, peak inspiratory pressures remained unchanged duringabdominal wall retraction with supplemental low-pressurepneumoperitoneum. Differences between both groups weresignificant in this respect. A decrease in arterial pH accom-panied by an increase in CO2 occurred during both conven-tional and low-pressure pneumoperitoneum with abdominalwall retraction although these changes appeared earlier dur-ing conventional pneumoperitoneum. During both tech-niques blood gas analysis showed a decrease in partial ar-terial oxygen pressure, although values at which hemoglo-bin oxygen saturation may become impaired were notreached.
Discussion
The pilot study indicated that laparoscopic cholecystectomyusing the AWR without pneumoperitoneum was technicallydifficult. The major problem during laparoscopy withoutpneumoperitoneum was a view obscured by bowel move-ment in front of the camera. Clear exposure of Calot’s tri-
angle, essential for safe dissection of the cystic duct, wasimpossible. Adding a positive intraabdominal CO2 pressureof 5 mmHg was enough to solve this problem.
Although this technique was feasible as shown in thepresent study, the operation lasted longer when comparedwith the procedure using conventional pneumoperitoneum.The results also indicate that the use of the AWR combinedwith low-pressure pneumoperitoneum leads to similar he-modynamic and gas-exchange changes as compared withconventional pneumoperitoneum. These results are in con-trast with other studies, which suggest that laparoscopiccholecystectomy can be performed with AWR withoutpneumoperitoneum [3, 6, 14]. This contradiction may beexplained by differences in abdominal wall retraction meth-ods, such as wiring of the subcutaneous tissues [6]. Thismay result in a better view as compared with the view usingthe abdominal wall retractor. However, these techniquesinvolve difficult and lengthy assembly and require extrastab wounds, which makes them unpopular with most sur-geons. On the other hand, some authors used the same ab-dominal wall retractor as in this study [3, 14]. Smith usedthe device without pneumoperitoneum successfully in 81%of the laparoscopic cholecystectomies. The results may bedue to extensive training.
The results of this study also contrast with our previousstudy in which the hemodynamic effects of abdominal wallretraction were assessed in pigs [11]. The V-shaped chest ofa pig as compared to the more flat human chest may haveenabled a clear vision in this particular experimental model.
The mean duration of laparoscopic cholecystectomy us-ing the AWR was longer as compared with conventionalpneumoperitoneum. Smith et al. did not report the averageoperation duration [14]. It is unlikely that lack of experiencenegatively influenced our results. The patients were oper-ated upon by two surgeons with extensive experience inlaparoscopic surgery. Furthermore, there was no differencein operation time between the first and last procedure whileusing the abdominal wall retractor; there was also no dif-ference in operation time between the two surgeons.
Fig. 1. Hemodynamic parameters.Data are mean ± SD. *p < 0.05:(h) pneumoperitoneum, (d)abdominal wall retractor comparedwith baseline.
647

Hemodynamic data indicate that blood pressure andheart rate are affected similarly by both methods (ANOVA).Although cardiac output increased during abdominal wallretraction compared with a small decrease during conven-tional pneumoperitoneum, differences in cardiac output be-tween the two techniques were not significant. These find-ings are not in accordance with a previous study in pigswhich indicated that laparoscopy using abdominal wall re-traction results in less cardiovascular depression comparedto conventional pneumoperitoneum [11]. Others alsoshowed that in pigs, positive and expiratory pressure(PEEP) affected hemodynamics less during AWR than dur-ing conventional pneumoperitoneum [16]. The finding thatadding 5 mmHg of pneumoperitoneum results in hemody-namic changes similar to those of higher intraabdominalpressures may indicate that these changes are not caused byincreased intraabdominal pressure. It has been suggestedthat the hemodynamic changes during laparoscopy are atleast partly due to the pharmacological effects of the ab-sorbed CO2. Our findings support this contention.
One may say that cardiac output was measured by a newnoninvasive method, as described before [15]. Using thisdevice, the cardiac output measurements were computedcontinuously from the radial artery pressure. The cardiacoutput changes observed during conventional pneumoperi-toneum are similar to those reported in the literature usingestablished cardiac output measurement techniques. It ispossible that the computer model does not measure the ab-solute values of cardiac output; however, it reliably tracksrelative changes of cardiac output, which is sufficient forthis study.
Respiratory acidosis develops using conventional pneu-moperitoneum as shown by the increase of the arterial PCO2and pH. The use of AWR was also associated with thegradual development of respiratory acidosis. This finding isin agreement with those of others who showed that theincrease of PCO2 during laparoscopy is not linearly relatedto the intraabdominal pressure of CO2 pneumoperitoneum[8]. It is suggested that recruitment of peritoneal absorptionarea is an important factor to determine the rate of CO2absorption from the peritoneal cavity [8, 9]. It is conceiv-able that recruitment of more gas-exchange area during ab-dominal wall retraction may result in an increase of PCO2similar to the increase observed at higher intraabdominalpressures. Alveolar dead space ventilation is also an impor-tant contributor to respiratory acidosis during laparoscopy[8]. The alveolar dead space was not measured in this study.However, it seems possible that alveolar dead space venti-lation increases to the same extent during both methods.
The decrease in pH during conventional pneumoperito-neum seems larger, compared with the use of the abdominalwall retractor, although statistical significance was notreached. It is possible that with a longer operation time thisdifference might reach statistical significance. However, themajority of the laparoscopic cholecystectomies using con-ventional pneumoperitoneum lasted on average 50 min.Consequently we were unable to complete a full set of he-modynamic and gas-exchange values after 30 min in allcases. It seems reasonable to assume that the abdominalwall retractor might be of value with respect to acid–baseequilibrium during operations of longer duration, such asbowel surgery.
Fig. 2. Ventilatory and gas exchange parameters: (d) abdominal wallretractor; (h) pneumoperitoneum. Data are mean ± SD. *p < 0.05 and ¶p< 0.001 compared with baseline.[p < 0.05 compared with pneumoperi-toneum.
648

Arterial oxygenation shows a gradual reduction of thearterial PO2 during the laparoscopic procedures, withoutsignificant differences between both methods. Increased in-trapulmonary shunt or decreased ventilation perfusion ratioas a result of atelectases secondary to the cranial movementof the diaphragm, may be the underlying mechanism of thisphenomenon. There is only one case report that describessevere hypoxemia in a patient with sickle cell anaemia un-dergoing laparoscopic cholecystectomy [4]. Because arte-rial PO2 values remained much higher than values at whichhemoglobin oxygen desaturation occurs, it remains doubtfulwhether the decrease in arterial PO2 is of any clinical rel-evance.
During laparoscopy, using conventional pneumoperito-neum the cranial shift of the diaphragm is associated withdiminished intrathoracic volume. When mechanical venti-lation with fixed tidal volumes is applied, increased airwaypressures will be generated. Indeed, in our study peak air-way pressures increased during laparoscopy using conven-tional pneumoperitoneum. This finding is in agreement withthose of others who reported increased peak and plateauairway pressures secondary to reduced compliance duringlaparoscopy [2]. In contrast, during abdominal wall retrac-tion peak airway pressures did not increase. High airwaypressures may have damaging effects on lungs with bullousemphysema that are prone to the development of baro-trauma [13]. In theory, the use of the abdominal wall re-tractor might be advantageous in these patients because it’suse is not associated with increased airway pressures.
Conclusion
In conclusion, the results of this study are disappointingwith respect to the use of the abdominal wall retractor. Inthe first place, the use of this device is difficult and does notpermit laparoscopic cholecystectomy entirely without pneu-moperitoneum. This takes away some of the suggested ad-vantages of using the abdominal wall retractor, such as lowcosts [6], and the possibility of using conventional instru-ments [14]. Second, the beneficial effects suggested by sev-eral experimental studies with respect to hemodynamics andgas exchange could not be confirmed in this human study.
Considering the results, AWR should not be used duringlaparoscopic cholecystectomy. AWR might be valuable forlower abdominal surgery, although this has to be evaluatedby further study.
References
1. Banting S, Shimi S, Vander VG, Cuschieri A (1993) Abdominal walllift. Low-pressure pneumoperitoneum laparoscopic surgery. Surg En-dosc 7: 57–59
2. Bardoczky GI, Engelman E, Levarlet M, Simon P (1993) Ventilatoryeffects of pneumoperitoneum monitored with continuous spirometry.Anaesthesia 48: 309–311
3. Chin AK, Eaton J, Tsoi EK, Smith RS, Fry WR, Henderson VJ,McColl MB, Moll FH, Organ CJ (1994) Gasless laparoscopy using aplanar lifting technique. J Am Coll Surg 178: 401–403
4. Cunningham AJ, Schlanger M (1992) Intraoperative hypoxemia com-plicating laparoscopic cholecystectomy in a patient with sickle hemo-globinopathy. Anesth Analg 75: 838–843
5. Edelman DS (1994) Alternative laparoscopic technique for cholecys-tectomy during pregnancy. Surg Endosc 8: 794–796
6. Hashimoto D, Nayeem SA, Kajiwara S, Hoshino T (1993) Abdominalwall lifting with subcutaneous wiring: an experience of 50 cases oflaparoscopic cholecystectomy without pneumoperitoneum. Surg To-day 23: 786–790
7. Lantz PE, Smith JD (1994) Fatal carbon dioxide embolism complicat-ing attempted laparoscopic cholecystectomy—case report and litera-ture review [review]. J Forensic Sci 39: 1468–1480
8. Lister DR, Rudston-Brown B, Wariner B, Mc Ewen J, Chan M,Walley KR (1994) Carbon dioxide absorption is not linearly related tointraperitoneal carbon dioxide insufflation pressure in pigs. Anesthe-siology 80: 129–136
9. Mullet CE, Viale JP, Sagnard PE, Miellet CC, Ruynat LG, CouniouxHC, Motin JP, Boulez JP (1993) Pulmonary CO2 elimination duringurgical procedures using intra- or extraperitoneal CO2 insufflation.Anesth Analg 76: 622–626
10. Newman LL, 3d, Luke JP, Ruben DM, Eubanks S (1993) Laparoscop-ic herniorrhaphy without pneumoperitoneum. Surg Laparosc Endosc3: 213–215
11. Rademaker BMP, Meyer DW, Bannenberg JJG, Klopper PJ, KalkmanCJ (1995) Laparoscopy without pneumoperitoneum. Effects of ab-dominal wall retraction versus carbon dioxide insufflation on hemo-dynamics and gas exchange in pigs. Surg Endosc 1995;9:197–201
12. Safran DB, Orlando R (1994) Physiologic effects of pneumoperito-neum [review]. Am J Surg 167: 281–286
13. Slutsky AS (1993) Mechanical ventilation. Chest 104: 1833–1859
14. Smith RS, Fry WR, Tsoi EK, Henderson VJ, Hirvela ER, Koehler RH,Brams DM, Morabito DJ, Peskin GW (1993) Gasless laparoscopy andconventional instruments. The next phase of minimally invasive sur-gery. Arch Surg 128: 1102–1107
15. Wesseling KH, Jansen JRC, Settels JJ, Schreuder J (1993) Computa-tion of aortic flow from pressure in humans using a nonlinear, threeelement model. J Appl Physiol 74: 2566–2573
16. Woolley DS, Puglisi RN, Bilgrami S, Quinn JV, Slotman GJ (1995)Comparison of the hemodynamic effects of gasless abdominal disten-tion and CO2 pneumoperitoneum during incremental positive end-expiratory pressure. J Surg Res 58: 75–80
649

Editorial
Complete and partial laparoscopic fundoplication for gastroesophagealreflux disease
Fundoplication for gastroesophageal reflux disease(GERD), first reported in 1990, represents a significant leapforward in the development of effective therapy in this com-mon condition. The paper by Dr. Coster and colleagues inthis edition ofSurgical Endoscopymakes a strong case forlaparoscopic antireflux surgery early in the course ofGERD, and the authors support their thesis by reporting theshort-term results of 231 patients following complete orpartial fundoplication. Their paper demonstrates that expe-rienced laparoscopic surgeons in a private practice settingusing two co-surgeons can perform fundoplication rapidly,safely, economically, and with good short-term outcome.Several features of the report are likely to give rise to con-troversy, and it is worthwhile to assess their policy andresults against the background of other workers in the samespecialty. These may conveniently be grouped under threeheadings: patient selection, operative strategy, and outcomeassessment.
There is no argument that reduction of unnecessary pre-operative investigations is desirable to limit both costs andpatient discomfort. These authors noted a change in thereferral pattern as the reputation of the operation spread, andthus they were referred patients from different sources withdifferent degrees of workup. This phenomenon is likely tobecome more widespread and it should encourage surgeonsto become experts in understanding the disease process andto be able to take charge of the preoperative workup. Sur-geons who do their own endoscopy, as Dr. Coster and hiscolleagues do, have a different perspective than internists,since the endoscopic view is automatically related to theanatomy the surgeon sees every day in the operating room.The anatomic location and reducibility of the gastroesopha-geal junction and the function and position of the crura allimpact the surgical decision-making process.
What about the necessity of physiologic investigation ofthe esophagus—manometry and 24-h pH monitoring? Arethese uncomfortable tests really necessary for patient care,or are they simply icing on the cake, niceties devised byacademic surgeons to confirm in numeric form what every-one knows anyway? The development of 24-h esophagealpH monitoring has certainly advanced our understanding ofthe pathophysiology of GERD, but is it necessary to confirmexcessive esophageal acid exposure in every patient before
recommending surgery? Dr. Coster and colleagues seem tosuggest that the presence of endoscopic esophagitis is suf-ficient. We disagree. Nonreflux causes of esophagitis, es-pecially pill-induced, may be present in up to 10% of pa-tients, and the visual and histologic characteristics do notdistinguish these causes. However, when the patient has acombination of a significant hiatal hernia typical symptoms,and endoscopic esophagitis, the proportion of patients withnegative 24-h pH monitoring is very small, and the test mayarguably be omitted in this circumstance. The problem isthat a rising indication for the procedure is drug dependencyin patients reported to have had esophagitis in the past, butwho are now healed. In such patients we believe that con-firmation of the diagnosis prior to surgical intervention with24-h pH monitoring is a necessity.
Preoperative appreciation of esophageal contractility isan important factor in deciding on the operative approach.Dr. Coster’s group believes that preoperative motility testsmay be limited to patients with suggestive symptoms,though there is abundant evidence that this is not so [1].Although it is unlikely to be subjected to a randomizedcontrolled trial, the detection of motility abnormalities onpreoperative manometry is widely regarded as important inchoosing a partial fundoplication rather than a total one toavoid the problem with postoperative dysphagia. The basisfor this choice comes from the disastrous results which fol-low fundoplication in unrecognized achalasia and other hy-poperistaltic disorders. Further, an unpublished study car-ried out by one of us (T.R.D.) demonstrated in an in vitromodel using the excised dog esophagus that a total fundo-plication could support a column of water of 15–20 cm buta partial fundoplication exerted virtually no outflow resis-tance. The authors of the present study bypass the problemby advocating partial fundoplication as a routine. The keyissue in the complete vs partial fundoplication controversyis durability. Neither this present paper nor any other fromthe laparoscopic era can yet answer the question because thenecessary follow-up is not available. But years of carefulfollow-up of the most carefully studied partial fundoplica-tion, the Belsey Mark IV operation, indicates steady dete-rioration with time, in contrast to the Nissen procedure,where accumulated experience confirms long-term durabil-ity. We would counsel caution in adopting partial fundopli-cation as the primary surgical treatment for reflux disease. Ifthese authors wish to make a further valuable contribution,they will carefully follow up their patients over the next 10Correspondence to:T. R. DeMeester
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 613–614

years. This is painstaking and labor-intensive work, butsuch an important lesson can be obtained in no other way.Until then, their confident assertion that ‘‘there is no cir-cumstance where a complete wrap would be superior to apartial one except in the case of an intraoperative distalperforation’’ is premature. This same caveat should also beapplied to the authors’ concept of esophageal shortening.Positive-pressure insufflation leads to diaphragmatic eleva-tion and makes it possible to bring below the diaphragm anesophagus which at open surgery would remain retracted inthe mediastinum. If true shortening is present, the fundopli-cation will be constructed under tension and there will atendency for future migration into the chest and/or break-down. Once again, careful long-term follow-up of such pa-tients will be needed to demonstrate the durability of thefundoplication constructed under those circumstances.
Many of the feared complications of the Nissen proce-dure stem from older studies in which a long or tight fun-doplication was performed, and they have largely ceased tobe a significant problem in contemporary practice [5]. Inaddition, careful symptomatic review has shown that evenwith medical treatment patients frequently experiencesymptoms such as flatulence and bloating [3].
Several operative details will be of immediate interest tosurgeons tackling laparoscopic antireflux operations. Theauthors are correct to emphasize the importance of the retrofundic dissection in mobilizing the fundus and cardia fromthe left crus of the diaphragm. This step is much moredeliberate than was common in open fundoplication, and theuse of the 45° lens adds significantly to the ease and safetyof the periesophageal dissection. The use of the USSC au-tomatic suture placement device is certainly time saving,but it may not allow the precision by which experiencedsurgeons feel the depth of the bites taken of crura, esopha-gus, or stomach. Does this paper add to the controversyabout the necessity to take down the short gastric arteriesprior to constructing the fundoplication? Two important re-cent studies given conflicting messages in this connection.The Adelaide group recently reported the results of a smallrandomized trial comparing patients with short gastric di-vision vs those without. No different in symptomatic out-come occurred [4]. On the other hand, Hunter et al. recentlypublished a comparative study in which the incidence ofpostoperative dysphagia was higher in the Nissen-Rosettipatients than in either those with Nissen procedures wherethe short gastrics were divided, or in those with Toupetprocedures [2]. Further, Hunter et al. also demonstrated thetorsion effect produced by the Nissen-Rosetti procedure.
The current study seems rather to support Hunter, in thattheir Nissen-Rosetti patients had a higher incidence of dys-phagia and a longer time to resumption of an unrestricteddiet than the Toupet patients. Rather than resort to an op-eration of uncertain durability such as the Toupet, why notcompare the Nissen-Rosetti with the true Nissen as cur-rently performed, where the fundus is mobilized and thefundus is plicated without torsion around the lower esopha-gus? A properly done laparoscopic Nissen fundoplicationgives good symptomatic results with a low incidence ofdysphagia and other unpleasant side effects, and since itanatomically corresponds to the open Nissen, we can havethe same confidence in its long-term outcome. In conclu-sion, although the authors have given us a good descriptionof two antireflux procedures which they can perform safelyand with extraordinary rapidity, we continue to believe thata correctly constructed, nontwisted, 360° Nissen fundopli-cation in correctly selected patients is the best long-termsolution for most patients with GERD. We now accept thatGERD requires life-long medical therapy, and if the patientopts for surgical therapy, it, too, must last a lifetime!
References
1. Costantini M, Crookes PF, Bremner RB, Hoeft SF, Ehsan A, Peters JH,Bremner CG, DeMeester TR (1993) The value of physiological assess-ment of foregut symptoms in a surgical practice. Surgery 114: 780–787
2. Hunter JG, Swanstrom L, Waring JP (1996) Dysphagia after laparo-scopic antireflux surgery: the impact of operative technique. Ann Surg224: 51–57
3. Spechler SJ, the VA Gastroesophageal Reflux Study Group (1992) Aprospective trial of medical and surgical therapies for gastroesophagealreflux disease. N Engl J Med 326: 786–792
4. Watson DI, Pike GK, Mathew K, Bairgie RJ, Devitt PG, Britten JonesR, Jamieson GG (1996) Prospective double blind randomized trial oflaparoscopic Nissen fundoplication with division and without divisionof the short gastric vessels. In: Peracchia A (ed) Recent advance indiseases of the esophagus. Monduzzi, Milan
5. Woodward ER, Thomas HF, McAlhany JC (1971) Comparison of cruralrepair and Nissen fundoplication in the treatment of esophageal hiatushernia with peptic esophagitis. Ann Surg 173: 782–792
P. F. CrookesT. R. DeMeester
University of Southern California School of MedicineDepartment of Surgery1510 San Pablo StreetSuite 514Los Angeles, CA 90033-4612USA
614

Complications of pediatric laparoscopic surgery
C. Esposito, G. Ascione, V. Garipoli, G. De Bernardo, G. Esposito
Department of Pediatrics, Division of Pediatric Surgery, ‘‘Federico II’’ University of Naples, Via Pansini 5, 80131 Napoli, Italy
Received: 5 July 1996/Accepted: 19 November 1996
AbstractBackground:Surgical complications of laparoscopy mostoften occur during Veress needle or primary trocar place-ment. Veress needle punctures are insignificant and requireno further treatment, whereas trocar-induced vascular inju-ries can be catastrophic. The frequency of vascular andviscus injuries is difficult to calculate because several com-plications are not reported in the literature.Methods:During a 10-year-period (1984–1995), at the Di-vision of Pediatric Surgery at ‘‘Federico II’’ University ofNaples, 430 laparoscopic procedures were performed in 395children with a mean age of 5 years. The incidence of com-plications related to laparoscopy was 1.8% with eight com-plications, one of which was rather severe. The complica-tions included one abdominal wall hematoma, two perfora-tions of abdominal viscus (stomach, ovary), one umbilicalscar complication, one postoperative hydrocele, one subcu-taneous emphysema, and one pneumothorax during a Nis-sen procedure. The only severe complication occurred in ayoung girl with neurologic problems and a kyphoscoliosisoperated on via laparoscopy for a gastroesophageal reflux.She suffered injuries of both right common iliac vessels andseveral intestinal perforations due to blind introduction ofthe first umbilical trocar.Results:In this case rapid conversion, complex vascularreconstruction, and multiple intestinal sutures were per-formed. The Nissen fundoplication with pyloroplasty wasperformed traditionally and the patient left the hospital freeof symptoms after 20 days. The other seven complicationswere resolved without any problem intra- or postopera-tively.Conclusions:The authors believe that the open approachwith a blunt trocar is most important in helping to avoidcomplications in pediatric laparoscopy.
Key words: Laparoscopy — Complications — Open ap-proach
The study of laparoscopic complications raises the problemof how to evaluate this new surgical technique, which hasbeen developing in pediatric surgery only in the last 5–6years. Although there are reports in the literature on therisks related to diagnostic laparoscopy that date back to1950, and although important studies have been publishedon both incidence and severity of complications derivingfrom the use of laparoscopy in adults for digestive or gy-necological surgery, the data on pediatric ages are scanty [3,5, 9]. Peters in his case series of 5,400 laparoscopic inter-ventions reports a complication rate of 5.38%, with a Veressneedle complication rate of 2.6% compared to the opencomplication rate of 1.2% [15]. The aim of this study is toexamine, on the basis of the experiences of these authors,the real incidence of laparoscopic complications in childrenand how to prevent them.
Patients and methods
At the Division of Pediatric Surgery of the Federico II University of Naples430 laparoscopic investigations were performed over a period of 10 yearsextending from November 1984 to June 1995.
The patients’ ages ranged from 8 days to 16 years, with a mean age of5 years. There was a 1.8% complication rate, equal to eight complications,one of which was rather severe (Table 1). In five cases, the complicationsoccurred intraoperatively, whereas three were postoperative complications.
The complications were: two cases of endoabdominal organ perforationwith the Veress needle (a large ovarian cyst and a case of extremely dilatedstomach), a wound infection involving the umbilical scar, a small hema-toma in the abdominal wall, a moderate-degree subcutaneous emphysemathat was resolved intraoperatively, a left hydrocele that manifested itself afew months after surgery for varicocele, and a pneumothorax during aNissen’s procedure that was resolved with a simple puncture at the end ofintervention. Also the left hydrocele, consequent to varicocelectomy, wastreated successfully by simple puncture. The gastric perforation was treatedconservatively according to Taylor’s technique, with a nasogastric intuba-tion for 4 postoperative days.
The only severe complication occurred in a 5-year-old girl sufferingfrom gastroesophageal reflux who was also affected by a severe neuro-logical disorder and kyphoscoliosis. The patient underwent laparoscopy forantireflux fundoplication according to Nissen. After inducing a pneumo-peritoneum with the Veress needle and introducing a 10-mm disposabletrocar in the umbilical scar, a severe hemoretroperitoneum appeared evi-dent through the optics of the laparoscope. An immediate conversion re-vealed lesions of the right common iliac artery, lesions of the homologousvein, and the presence of multiple intestinal perforations. After reimplant-Correspondence to:C. Esposito
Surg Endosc (1997) 11: 655–657
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

ing the iliac artery on the aorta and suturing the lesion on the homologousvein and intestinal perforations, the antireflux gastroplasty, according toNissen’s technique, was completed using conventional surgery. The childwas released from hospital 20 days later without any gastroesophagealreflux or consequences related to the laparoscopic intervention.
Since this episode, we have begun to utilize the open laparoscopy inevery case, to avoid complications related to the closed introduction of thefirst trocar.
Discussion
Surgical complications due to laparoscopy can be classifiedaccording to cause or in relation to the moment when theyoccur [4, 6]. Based on the cause, we can either speak ofnonspecific or specific complications: the former are relatedto procedures that are common to all laparoscopies inde-pendently of the indication, such as the creation of a pneu-moperitoneum; the latter, instead, depend on specific inter-ventions done by the surgeon. Moreover, complications caneither be intrasurgical or postsurgical, depending on wheth-er they occur during or after the intervention.
While we know that the incidence of complications inadult laparoscopy is about 4%, with a 0.03% mortality rate,in pediatric laparoscopy no such data are available in theliterature [11, 12].
Surgical complications are generally related to the in-troduction of either the Veress needle or the first trocar.Veress needle punctures are generally safe and require nofurther treatment, whereas lesions caused by a trocar canhave catastrophic consequences [1, 4, 10]. Bleeding causedby lesions of the abdominal wall vessels generally clotspontaneously; a ligation may be necessary only if the le-sion involves the epigastric vessels. Lesions of the endoab-dominal organs are generally eventless if they are promptlyidentified and treated, whereas endo- and retroperitonealvessel lesions generally require immediate conversion. Theendoabdominal vessels most frequently involved are theaorta, the inferior vena cava, and the iliac vessels, due to thefact that they are located right below the umbilicus, only2–3 cm away [13, 14, 16]. In case of a vessel lesion, thelaparoscopic surgeon must be able to perform an emergencyconversion, doing a temporary hemostasis first and a defi-nite hemostasis after having a global balance of the lesion.
The solution to vessel complications can be more or lesssimple; in more severe cases it is possible to use of venousgrafts or prosthesis.
Vessel lesions treated immediately have a good progno-sis; a delay in treatment can entail severe complications [7].
There are also complications related to insufflation:Even if performed correctly, a pneumoperitoneum can lateron expand itself beyond the endoabdominal cavity. The sub-cutaneous or scrotal diffusion is trivial and uneventful,whereas thoracic involvement, causing either a pneumotho-
rax or a pneumomediastinum, like our case of pneumotho-rax, occurred in the case of Nissen’s fundoplication. Gen-erally a simple puncture is sufficient to treat the pneumo-thorax, which does not occur again after deflation of theabdominal cavity [3].
The so-called ‘‘specific complications’’ are related tothe type of intervention to be performed: They can be due todissection or coagulation maneuvers, to the extraction oforgans or structures that have been dissected, or to neoplas-tic or infectious contamination [12]. No such complicationsoccurred in our series, mainly due to our use of bipolarcoagulation to induce hemostasis, which seems safer andless dangerous compared to monopolar coagulation [6, 8].
As to the removal of dissected organs, the main problemremains related to the size of the organ, as it might benecessary to enlarge the trocar opening or to createminilaparotomies to extract the organ. In the case of a sple-nectomy, it is important to remember that an intraperitonealspleen rupture can cause splenosis [8].
Postsurgical complications are theoretically reduced inlaparoscopy; however, the most common ones are infec-tions, small hematomas, epiploic evisceration or, even rarer,occlusions due to adhesions.
In our series we have two examples of this kind ofcomplication, an umbilical scar infection and a small hema-toma in the abdominal wall, but they were resolved withoutany problem in the first postoperative days, respectively, byadministration of antibiotics for 3 days in the first case anda local compressive medication in the second one.
Another complication that we noticed in the postopera-tive period was a hydrocele in a patient operated on with anIvanissevich procedure for a left varicocele. This problemdepends, as in traditional surgery, on clipping together thespermatic veins and the small lymphatic vessels also presentin the spermatic cord. This complication could be resolved,as in our case, with a simple puncture of the hydrocele. It isimportant to take into account all contraindications to lap-aroscopic surgery. There are, basically, clotting problems,hypovolemic shock, large tumors, and advanced intestinalocclusion; moreover, on the basis of our experience, allvertebral abnormalities in which there is reduced space be-tween the abdominal wall and the retroperitoneal vesselsalso constitute a contraindication.
As several authors have reported, the incidence of com-plications due to the introduction of either the Veress needleor the first trocar does not seem to be related to the sur-geon’s expertise but rather to the number of proceduresperformed. This type of problem has been recently resolvedby the open laparoscopy technique, where the introductionor the first trocar is eye-guided [2, 9]. The other complica-tions can be certainly avoided by the surgeon’s and theteam’s aptness, together with a proper compliance to theindications for surgery.
We believe that in pediatric laparoscopy as in all theother fields of surgery, proper knowledge and careful atten-tion to all the details are the most important factors in avoid-ing complications.
References
1. Apelgren KN, Scheeres DE (1994) Aorta injury, a catastrophic com-plication of laparoscopic cholecystectomy. Surg Endosc 8: 689–691
Table 1. Laparoscopic complications in our experience 1.8% (8 cases)
2 Endoabdominal organ perforations1 Hydrocele1 Pneumothorax1 Subcutaneous emphysema1 Small hematoma of the abdominal wall1 Vascular injury1 Umbilical scar infection
656

2. Begin FG (1993) Cre´ation du pneumope´ritoine sous controˆle visuel. JCoeliochir 5: 18–20
3. Berci G (1994) Complications of laparoscopic surgery. Surg Endosc 8:165–168
4. Bloom DA, Erhlich RM (1993) Omental evisceration through smalllaparoscopy port sites. J Endourol 7: 31–32
5. Capelouto CC, Kavoussi LR (1993) Complications of laparoscopicsurgery. Urology 42: 2–12
6. Delarue A, Guys JM, LouisBorrione C, Simeoni J, Esposito C (1994)Pediatric endoscopic surgery: pride and prejudice. Eur J Pediatr Surg4: 323–326
7. Duckett JW (1994) Editorial: pediatric laparoscopy: prudence please.J Urol 151: 742–743
8. El Ghoneimi A, Valla JS, Limonne B, Montupet P, Chavrier Y, GrindaA (1994) Laparoscopic appendectomy in children: report of 1379cases. J Pediatr Surg 29: 786–789
9. Hasson H (1971) Modified instrument and method for laparoscopy.Am J Obstet Gynecol 110: 886–887
10. Juricic M, Bossavy JP, Izard I, Cuq P, Vaysse P, Juskiewensky S(1994) Laparoscopy appendectomy: case report of vascular injury intwo children. Eur J Pediatr Surg 4: 327–328
11. Niebuhl H, Nahrestedt U, Ruckert K, Hollmann S (1993) Laparoscopicsurgery: mistakes and risks when the method is introduced. Surg En-dosc 7: 412–415
12. Nord HJ (1992) Complications of laparoscopy. Endoscopy 24: 693–700
13. Oshinsky G, Smith AD (1992) Laparoscopic needle and trocar: anoverview of design and complications. J Laparoendosc Surg 2: 117–125
14. Oza KN, O’Donnell N, Fisher JB (1992) Aortic laceration: a rarecomplication of laparoscopy. J Laparoendosc Surg 2: 235–237
15. Peters CA (1995) Complications in pediatric urological laparoscopy:results of a survey. J Urol 155: 1070–1073
16. Waldschmidt J, Schier F (1991) Laparoscopical surgery in neonatesand infants. Eur J Pediatr Surg 1: 145–150
657

Long-term effects of repeated injection sclerotherapy on esophagealmotility and mucosa
B. Isaksson, F. Johnsson, B. Jeppsson
Department of Surgery, Lund University Hospital, S-221 85 Lund, Sweden
Received: 22 April 1996/Accepted: 20 August 1996
AbstractBackground:Endoscopic sclerotherapy (ST), widely usedas treatment of bleeding esophageal varices, might causemotility disturbances of the esophagus as well as mucosaldamage. We performed this study to evaluate the long-termeffects of repeated sclerotherapy on esophageal motility andmucosa.Methods: Ten patients with liver cirrhosis and bleedingesophageal varices treated with repeated ST were evaluatedafter the last ST, median 52 months, by esophageal manom-etry and gastroscopy where forceps biopsies were taken.Results:We found a significant difference in the distalesophageal sphincter intraabdominal length. The distalesophageal sphincter pressure was somewhat lower in theST group although the difference did not reach statisticalsignificance. There was infiltration of neutrophil leukocytesin biopsies from four patients and normal findings in therest.Conclusions:Long-term follow-up evaluation showed sta-tistically longer distal esophageal intraabdominal length inthe ST group. No mucosal alterations were found at thehistopathological investigation.
Key words: Sclerotherapy — Esophageal manometry —Histopathological evaluation
Endoscopic injection sclerotherapy (ST) is a well-established method in the treatment of bleeding esophagealvarices. It has proven to be effective in the treatment of bothacute bleeding episodes as well as electively for eradicationof varices [1, 6, 15, 16]. The most common complaints afterinjection sclerotherapy are fever, retrosternal discomfort,and transient dysphagia; they resolve within 24–48 h.Esophageal ulcerations are common and usually asymptom-atic. They are more likely to occur after large volume andfrequent injections of sclerosants. Esophageal strictures
may require dilatation. Besides this, there may also be mo-tility disturbances of the esophagus [4, 7, 10, 14]. The in-cidence and severity of these disturbances vary in differentreports. We therefore designed this study in order to evalu-ate the long-term effects of repeated sclerotherapy onesophageal motility and relate them to the number of sclero-therapy sessions and volume of injected sclerosants. Wealso tried to evaluate any histological alterations in the mu-cosa and submucosa in the same group of patients.
Materials and methods
Patients
Ten patients, seven men and three women, from 50 to 77 years of age,median age 611⁄2 years, who had been treated with repeated endoscopicsclerotherapy of esophageal varices were compared to a control group often healthy persons 38 to 78 years old with a median age of 42 years. In thecontrol group there were six men and four women.
Initially the patients in the ST group all had bleeding esophageal vari-ces. The varices were due to portal hypertension secondary to liver cirrho-sis, in most cases induced by alcohol abuse. Two patients representedChild’s class A and the other eight Child’s class B.
Methods
Sclerotherapy.The sclerotherapy treatment was administered by a flexiblestandard gastroscope, Olympus GIF-K, with an injection needle catheterthrough which 10 mg/ml polidocanol (Aethoxysclerol) (Chemische FabrikKreussler & Co, GmbH, D-6200, Wiesbaden-Briebrick, Germany) wasgiven in bolus injections of 0.5–1 ml submucosally and paravariceally. Theinjections were given at the gastroesophageal junction and 5–7 cm proxi-mally. The maximal amount given at each treatment session was 30 mlpolidocanol. The first sclerotherapy session was performed acutely due tobleeding esophageal varices and the following were elective in order toeradicate the varices.
Esophageal manometry.This investigation was performed using a station-ary pull-through technique. A three-lumen polyvinyl catheter, with theCorrespondence to:B. Isaksson
Surg Endosc (1997) 11: 663–667
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997
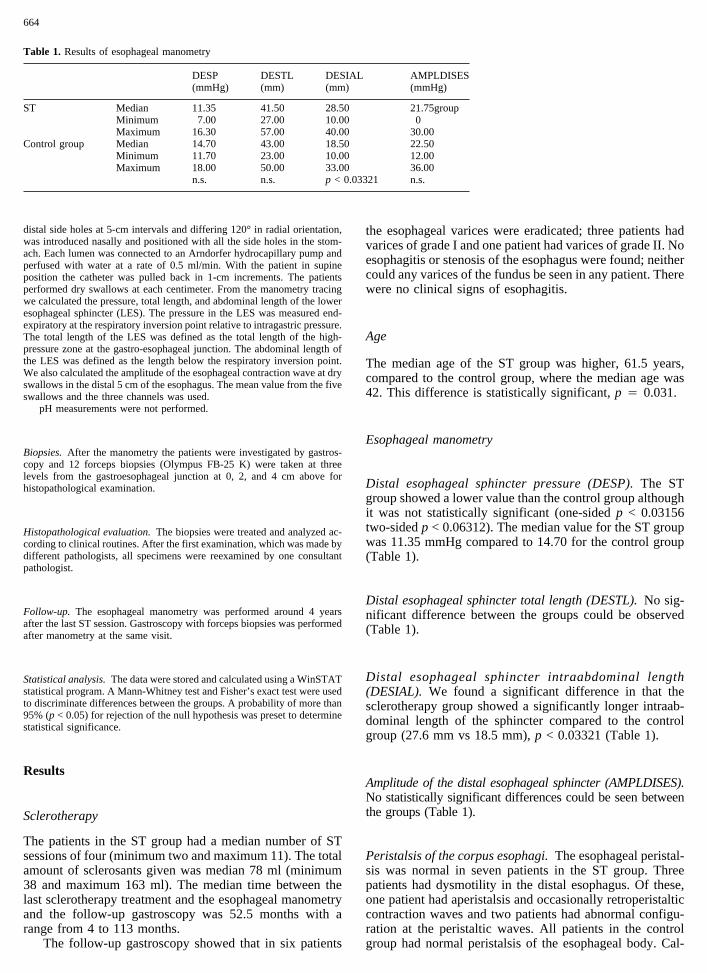
distal side holes at 5-cm intervals and differing 120° in radial orientation,was introduced nasally and positioned with all the side holes in the stom-ach. Each lumen was connected to an Arndorfer hydrocapillary pump andperfused with water at a rate of 0.5 ml/min. With the patient in supineposition the catheter was pulled back in 1-cm increments. The patientsperformed dry swallows at each centimeter. From the manometry tracingwe calculated the pressure, total length, and abdominal length of the loweresophageal sphincter (LES). The pressure in the LES was measured end-expiratory at the respiratory inversion point relative to intragastric pressure.The total length of the LES was defined as the total length of the high-pressure zone at the gastro-esophageal junction. The abdominal length ofthe LES was defined as the length below the respiratory inversion point.We also calculated the amplitude of the esophageal contraction wave at dryswallows in the distal 5 cm of the esophagus. The mean value from the fiveswallows and the three channels was used.
pH measurements were not performed.
Biopsies.After the manometry the patients were investigated by gastros-copy and 12 forceps biopsies (Olympus FB-25 K) were taken at threelevels from the gastroesophageal junction at 0, 2, and 4 cm above forhistopathological examination.
Histopathological evaluation.The biopsies were treated and analyzed ac-cording to clinical routines. After the first examination, which was made bydifferent pathologists, all specimens were reexamined by one consultantpathologist.
Follow-up. The esophageal manometry was performed around 4 yearsafter the last ST session. Gastroscopy with forceps biopsies was performedafter manometry at the same visit.
Statistical analysis.The data were stored and calculated using a WinSTATstatistical program. A Mann-Whitney test and Fisher’s exact test were usedto discriminate differences between the groups. A probability of more than95% (p < 0.05) for rejection of the null hypothesis was preset to determinestatistical significance.
Results
Sclerotherapy
The patients in the ST group had a median number of STsessions of four (minimum two and maximum 11). The totalamount of sclerosants given was median 78 ml (minimum38 and maximum 163 ml). The median time between thelast sclerotherapy treatment and the esophageal manometryand the follow-up gastroscopy was 52.5 months with arange from 4 to 113 months.
The follow-up gastroscopy showed that in six patients
the esophageal varices were eradicated; three patients hadvarices of grade I and one patient had varices of grade II. Noesophagitis or stenosis of the esophagus were found; neithercould any varices of the fundus be seen in any patient. Therewere no clinical signs of esophagitis.
Age
The median age of the ST group was higher, 61.5 years,compared to the control group, where the median age was42. This difference is statistically significant,p 4 0.031.
Esophageal manometry
Distal esophageal sphincter pressure (DESP).The STgroup showed a lower value than the control group althoughit was not statistically significant (one-sidedp < 0.03156two-sidedp < 0.06312). The median value for the ST groupwas 11.35 mmHg compared to 14.70 for the control group(Table 1).
Distal esophageal sphincter total length (DESTL).No sig-nificant difference between the groups could be observed(Table 1).
Distal esophageal sphincter intraabdominal length(DESIAL). We found a significant difference in that thesclerotherapy group showed a significantly longer intraab-dominal length of the sphincter compared to the controlgroup (27.6 mm vs 18.5 mm),p < 0.03321 (Table 1).
Amplitude of the distal esophageal sphincter (AMPLDISES).No statistically significant differences could be seen betweenthe groups (Table 1).
Peristalsis of the corpus esophagi.The esophageal peristal-sis was normal in seven patients in the ST group. Threepatients had dysmotility in the distal esophagus. Of these,one patient had aperistalsis and occasionally retroperistalticcontraction waves and two patients had abnormal configu-ration at the peristaltic waves. All patients in the controlgroup had normal peristalsis of the esophageal body. Cal-
Table 1. Results of esophageal manometry
DESP(mmHg)
DESTL(mm)
DESIAL(mm)
AMPLDISES(mmHg)
ST Median 11.35 41.50 28.50 21.75groupMinimum 7.00 27.00 10.00 0Maximum 16.30 57.00 40.00 30.00
Control group Median 14.70 43.00 18.50 22.50Minimum 11.70 23.00 10.00 12.00Maximum 18.00 50.00 33.00 36.00
n.s. n.s. p < 0.03321 n.s.
664

culated by Fisher’s exact test no significant difference couldbe noted between the groups.
Histopathological findings
Signs of inflammation with infiltration of neutrophil leuko-cytes as in esophagitis were seen in the biopsies from fourpatients; the other six patients had all-normal squamousepithelium. In no specimen were the biopsies deep enoughto show any material from the muscle layer. This made itimpossible to judge whether there was any fibrous reactionin the stroma (Figs. 1–3).
Discussion
Although first reported in 1939 by Crafoord and Freckner[2], who used a rigid endoscope for injection treatment ofbleeding esophageal varices, endoscopic injection sclero-therapy of esophageal varices did not gain popularity untilthe sixties when the flexible endoscopes became more com-monly available.
There are two ways to administer the sclerosing agent.In Europe, except in Great Britain, paravariceal injectionsclerotherapy is the most widely used technique. The mostcommon technique in the US and in the UK is the intra-variceal. The aim of the paravariceal or the submucosal
technique is to thicken the overlying mucosa; the intravari-ceal approach is aimed to induce variceal thrombosis [13].
In our study we used the paravariceal submucosal tech-nique of injecting the sclerosing agent, 1% polidocanol, inbolus injections of 0.5–1 ml at a maximum of 30 ml at everytreatment session. The median total amount of sclerosingagent was 78 ml, the median number of treatment sessionswas four.
No patient in our study had any clinical signs of esoph-agitis. This is in agreement with Sauerbruch and colleagues[9] who used 1% polidocanol in their treatment group. Theydid not record the administration rank but the mean numberof ST sessions was ten and the mean amount of sclerosantagent was 133 ml. The length from ST to study was a meanof 21 months. Compared to their control group, consistingof cirrhotic patients with untreated varices, they found nostatistically significant differences in esophageal pH andmean of reflux episodes.
The long-term complications of sclerotherapy treatmentmay include disturbances of normal function of the esopha-gus. Both decreased distal esophageal sphincter pressureand abnormal peristaltic waves in the esophagus have beenreported [4, 8, 10, 11].
We found in our study a lowered distal esophagealsphincter pressure in the ST group compared to our controlgroup although the difference did not reach a statisticallysignificant level. The median value for the treatment groupwas 11.35 mmHg compared to 14.70 mmHg for the controlgroup. Other investigators report significant reduction of the
Fig. 1. Sclerotherapy group. Slight chronic inflammation with lympho-cytes in the lamina propria. Hematoxylin—eosin (×400).
Fig. 2. Sclerotherapy group. Junctional zone cardia—esophagus. Heavylymphocytic infiltration. Hematoxylin—eosin (×250).
665

lower esophageal sphincter pressure after sclerotherapy.Ogle et al. [7] found that their sclerotherapy group had amaximum sphincter pressure of 12.7 mmHg. The value fortheir cirrhotic patients untreated varices was 17.6 mmHgand 20.9 mmHg for their patients with cirrhosis withoutvarices. In this study the patients were treated with intra-variceal injections of ethyl amine. They were all studiedmuch earlier after ST than our patients.
Uribarrena and colleagues [14] report (in their studywhere they treated the varices by intravariceal injections of5% ethanolamine oleate) a LESP (DESP) of 17.52 mmHgfor the sclerotherapy group, 20.26 mmHg for their group ofcirrhotic patients with untreated varices and 22.86 mmHgfor their control group of healthy persons. Their patientswere studied on the average 12.3 months after ST.
Sauerbruch et al. [8] also report lower tonus of the LESin their sclerotherapy group, 10.7 mmHg vs 13.4 mmHg fortheir healthy volunteers. In this study both intravariceal andparavariceal injections of polidocanol 1% were given.Monometry was performed mean 9.6 months after bleeding.
Other investigators do not find any significantly loweredpressures of the distal esophageal sphincter. So¨derlund andThor [12] used the intravariceal technique and injected 1%polidocanol and studied the patients five months after ST.The same conclusions about the unaltered LES pressurewere drawn by Grande and colleagues [4] and by Larson etal. [5]. The group of Grande used ethyl amine injected intothe varices and the group headed by Larson used 5% sodium
morrhuate injected intravariceally. These studies were per-formed after 1 month and 6 months, respectively, but thetotal volume of sclerosant agent and number of ST sessionswere not recorded.
The lowered distal esophagus sphincter pressure couldbe a result of the known fibrous reaction [3, 10] after sclero-therapy.
In our study we found that the intraabdominal length ofthe distal sphincter was significantly longer in the ST groupcompared to the control group. However, there was no sig-nificant difference in the total length of the distal esopha-geal sphincter, which in our study had a median length forthe sclerotherapy group of 41.7 mm and 43.0 for the controlgroup.
Ogle et al. [7] report an increased LES length. Theyfound that the length of the LES in cirrhotic patients withvarices treated by sclerotherapy was 47.2 mm; in patientswith cirrhosis and untreated varices the length was 42.8mm; and in the patient group with cirrhosis without varicesthe LES length was 33.5 mm.
It is not likely that the length can be prolonged aftersclerotherapy. This finding might represent an artefact inthat the actual length is not altered but seems so measuredby manometry due to the known fibrous reaction, whichmight create a stiffness of the esophageal wall [3, 10].
All these studies were performed within the first monthsafter sclerotherapy. According to our findings, these alter-ations remain permanent.
Regarding the peristalsis of the corpus esophagi, wefound three patients with dysmotility in the distal esopha-gus. The patient with aperistalsis and occasionally retroperi-staltic contractive waves was treated at five ST sessions anda total of 97 ml polidocanol, which is normal for the STgroup. Manometry was performed 76 months after the lastST session. Of the two patients with abnormal configurationof the peristaltic waves one was treated at seven ST sessionsand with a total of 161 ml sclerosant agent. This is morethan the median for the group but not the largest amount ofpolidocanol in the group, 163 ml, which was given at fiveST sessions to a patient who did not show any disturbancesof the peristalsis of the corpus esophagi. Manometry wasperformed 12 months after the last ST session in this secondpatient with dysmotility. The third patient with abnormalconfiguration at the peristaltic waves only got 38 ml poli-docanol at two ST sessions. In this case manometry wasperformed 81 months after the last ST treatment. We couldnot find any connection between the amount of injectedsclerosing agent and the disturbances of peristalsis of theesophagi.
There are two histopathological and morphologicalstudies by Evans et al. [3] and by Soehendra et al. [10]where the alterations of the esophagus wall after sclero-therapy are investigated. In the study of Evans the intravari-ceal technique was used; in the Soehendra work a combinedpara- and intravariceal method was used.
The 1st week after the initial injection an acute reactionwith intramural inflammation and ulceration occurs. This islater replaced by formation of fibrosis at the site of theinjection. The mucosa is first invaded by fibrous tissue; thereaction goes further transmurally and in some cases themuscular layer of the esophagus wall is reached. After thesecond sclerosing session, often after about a week, more
Fig. 3. Sclerotherapy group. Junctional zone. Neutrophil leucocytes in theepithelium and some lymphocytes and plasma cells in the lamina propria.Hematoxylin—eosin (×225).
666

intensive necrosis takes place. Inflammation reaching sub-mucosa and the connective tissue of the adventitia occursand these layers are markedly more affected than the tunicamuscularis. If the fibrous reaction involves the muscularlayer stricture formation may take place. When the necrosishas healed, after about a month after the last injection, iso-lated scars of the esophageal inner wall can be identified.When the cicatrization is marked, the esophageal wall oftenappears rigid and manifests reduced motility. Over timemild strictures often normalize. The histological findingsare extensive fibrotic tissue in the submucosa; in some casesthe muscle layer is involved. In areas where depressed scarsare noticed, the structure of the esophageal wall is not de-stroyed despite considerable fibrosis.
To our knowledge no other investigators have reportedhistopathological findings from a clinical study in combi-nation with manometry investigation. In our study we useda standard technique to take forceps biopsies from the loweresophagus. We did not manage to show any fibrous reactionin any of our specimens, since they all consisted of thesquamous layer of the esophageal wall.
However, in both the above-mentioned studies the his-tologic examinations were performed within 1 or 2 monthsafter sclerotherapy, and no information is available on thelong-term effect in the mucosa-submucosa after submucosalparavariceal injections. The results of this study show thatthis injection technique does not seem to cause any histo-logic alterations even after a long time.
Acknowledgment.Inga Hagerstrand M.D., Ph.D., Department of ClinicalPathology, Lund University Hospital, Lund, Sweden performed the histo-pathological examinations.
References
1. Burnett DA, Rikkers LF (1990) Nonoperative emergency treatment ofvariceal hemorrhage. Surg Clin North Am 70(2): 291–306
2. Crafoord C, Freckner P (1939) New surgical treatment of varicousveins in the oesophagus. Acta Otolaryngol 27: 422–429
3. Evans DMD, Jones DB, Clearly BK, Smith PM (1982) Oesophagealvarices treated by sclerotherapy: a histopathological study. Gut 23:615–620
4. Grande L, Planas R, Lacima G, Boix J, Ros E, Esteve M, Morillas R,Gasull MA (1991) Sequential esophageal motility studies after endo-scopic injection sclerotherapy: a prospective investigation. Am J Gas-troenterol 86(1): 36–40
5. Larson GM, Vandertoll DJ, Netcher DT, Polk HC (1984) Esophagealmotility: effects of injection sclerotherapy. Surgery 96: 703–710
6. O’Connor KW, Lehman G, Yune H, Brunelle R, Christiansen P, HastJ, Compton M, McHenry R, Klatte E, Cockerill E, Holden R, BeckerG, Kopecky K, Hawes R, Pound D, Rex D, Lui A, Snodgrass P,Weddle R, Crabb D, Lumeng L (1989) Comparison of three nonsur-gical treatments for bleeding esophageal varices. Gastroenterology 96:899–906
7. Ogle SJ, Kirk CJC, Bailey RJ, Johnson AG, Williams R, Murray-LyonIM (1978) Oesophageal function in cirrhotic patients undergoing in-jection sclerotherapy for oesophageal varices. Digestion 18: 178–185
8. Sauerbruch T, Wirsching R, Leisner B, Weinzierl M, Phahler M,Paumgartner G (1982) Esophageal function after sclerotherapy forbleeding varices. Scand J Gastroenterol 17: 745–751
9. Sauerbruch T, Wirsching R, Holl J, Grobl J, Weinzierl M (1986)Effects of repeated injection sclerotherapy on acid gastroesophagealreflux. Gastrointest Endosc 32: 81–83
10. Soehendra N, de Heer K, Kempeneers I, Frommelt L (1983) Morpho-logical alterations of the esophagus after endoscopic sclerotherapy ofvarices. Endoscopy 15: 291–296
11. Spence RA, Smith JA, Isacs S, Terblance J (1990) Disturbed oesoph-ageal motility after eradication of varices by chronic sclerotherapy.South Afr Med J 77: 138–140
12. Soderlund C, Thor K (1985) Oesophageal function after sclerotherapyfor bleeding varices. Acta Chir Scand Preprint 524: 1–5
13. Terblanche J, Burroughs AK, Hobbs KEF (1987) Controversies in themanagement of bleeding esophageal varices. N Engl J Med 320: 1393–1398, 1469–1475
14. Uribarrena R, Jimenez J, Fortun MT, Jiminez C, Guerra A, Borda F(1990) Esophageal motility disorders in cirrhotics treated by sclerosingthe varices. Rev Esp Enferm Dig 78(1): 1–5
15. Vestaby D, Hayes PC, Gimson AES, Polson RJ, Williams R (1989)Controlled clinical trial of injection sclerotherapy for active varicealbleeding. Hepatology 9: 274–277
16. Warren WD, Millikan WJ Jr (1990) The relative role of sclerotherapyvs. surgical procedures in portal hypertension. Adv Surg 23: 1–19
667

A murine model of laparoscopic-assisted intervention
J. D. F. Allendorf, M. Bessler, R. L. Whelan
Department of Surgery, Atchley Pavilion 522, Columbia University, 161 Fort Washington Avenue, New York, NY 10032, USA
Received: 19 June 1996/Accepted: 2 November 1996
AbstractBackground:In order to better investigate the effects oflaparoscopic surgery, it is necessary to establish reliable,reproducible, and economical animal models of laparoscop-ic intervention. Here we describe a mouse model of lapa-roscopic-assisted colon resection.Methods: After successful induction of anesthesia themouse is placed in Trendelenburg position and the perito-neal cavity is insufflated with carbon dioxide gas through anangiocatheter placed in the right upper quadrant. A 4-mmrigid scope with camera attachment is then inserted througha midline port created just caudal to the xiphoid. A secondport is then created in the right lower quadrant to allowintroduction of laparoscopic forceps into the peritoneal cav-ity. The cecum, which extends 1.5 cm beyond the ileocecalvalve, is grasped with forceps and exteriorized through theoperative port. Extracorporeally, the cecum is ligated andresected before the cecal stump is returned to the peritonealcavity. The abdominal wall defects are then stapled closed.Results:This simple model can be mastered by individualswith very limited surgical experience. This laparoscopicmodel has been used successfully in our laboratory in anumber of experiments with an intraoperative complicationrate of 3.2% (3/94), which was similar to the open surgerygroup rate of 2.1% (2/95,p 4 0.99 by chi square). Weobserved no postoperative leaks in either group. The onlypostoperative death occurred in the open resection groupdue to dehiscence of the laparotomy wound.Conclusions:We propose that this model may be useful forcomparing the effects of open to laparoscopic surgery.
Key words: Mouse — Murine — Model — Small animal— Laparoscopy — Laparoscopic surgery — Bowel resec-tion cecectomy
In a remarkably brief period of time laparoscopic techniqueshave been introduced for a number of general surgery pro-
cedures including cholecystectomy, gastric fundoplication,splenectomy, and bowel resection. The purported and oftencited advantages of laparoscopic methods include less pain,earlier return of bowel function, and shorter hospitalizations[7]. The rapid clinical introduction of these minimal accessmethods precluded basic science studies to determine theprecise physiologic differences between open and laparo-scopic procedures. Recently, investigators have begun tostudy the effects of laparoscopic surgery vis-a`-vis open sur-gery in a more rigorous manner.
Utilizing animal models, our laboratory has been inves-tigating the physiologic and immunologic consequences oflaparoscopic-assisted bowel resection for the past 4 years.Initially, we used a porcine model of laparoscopic segmen-tal sigmoid resection to evaluate several hemodynamic andphysiologic parameters [5, 6]. While large-animal modelsare advantageous because the surgery more closely approxi-mates that done in humans and because normal-sized in-struments can be used, such models suffer from severalshortcomings. These models are very expensive, especiallyfor survival experiments; therefore the size of the studymust be limited to a small number of animals. Furthermore,physiologic, immunologic, and oncologic assays often re-quire species-specific reagents. Unfortunately, there arelimited assays and reagents available for large-animal mod-els. Finally, few cultured tumor cell lines have been devel-oped for large animals, which makes it difficult to study invivo tumor behavior. It was for these reasons that our labo-ratory endeavored to develop a mouse model for our lapa-roscopic studies.
While the comparison of sham laparotomy to pneumo-peritoneum is quite feasible in mice [1], the main drawbackof the mouse model is that the small size makes it difficultto devise reasonable laparoscopic procedures that can beperformed quickly and safely. Performing an actual bowelresection or other intervention poses a number of problems.It would be technically very challenging to perform bowelanastomoses in mice. The model of laparoscopic-assistedresection presented here permits a bowel resection yet doesnot require an anastomosis.
As the effects of laparoscopic surgery continue to beinvestigated, it is necessary to establish reliable, reproduc-Correspondence to:R. L. Whelan
Surg Endosc (1997) 11: 622–624
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

ible, and economical animal models of laparoscopic inter-vention. For this reason we established and report on amouse model of laparoscopic bowel resection.
Materials and methods
Animals
Five- to 6-week-old female C3H/He mice (Charles River Laboratories,Wilmington, MA) weighing approximately 30–35 g were acclimated to alight cycle and temperature-controlled environment for no less than 48 hprior to surgery. Mice were housed five to a cage in the Columbia Uni-versity Institute of Comparative Medicine and were offered standard rodentchow and water ad libitum. All studies were performed under protocolsapproved by the Columbia University Institutional Animal Care and UseCommittee.
Equipment
This model requires a laparoscopic cart including a monitor, camera at-tachment, light source, insufflator with compressed CO2, and 4-mm-diameter 0° rigid scope. Instruments required include two pairs of finedissecting forceps, dissecting scissors, 2-mm-diameter laparoscopic for-ceps, a small angiocatheter, and a large-bore needle.
Laparoscopic cecectomy
The normal mouse anatomy of the ileocecal region is shown in Fig. 1. Themouse cecum is proportionally much longer than in humans. The ileuminserts high into the right colon, creating a 1.5-cm blind-ended cecum. Theprocedure described below involves the amputation of this structure, whichconstitutes a bowel resection, and yet does not require that an anastomosisbe performed.
After successful induction of anesthesia with ketamine (50 mg/kg) andxylazine (5 mg/kg), the abdomen of a 5–6-week-old mouse is painted withBetadine and alcohol. The animal is placed in Trendelenburg position andthe peritoneal cavity is insufflated with carbon dioxide gas at a pressure of3–5 mmHg through a 25-gauge angiocatheter inserted into the right upperquadrant. An 18-gauge needle is then used to create a midline defect in theabdominal wall just caudal to the xiphoid. This defect is spread to adiameter of 4 mm using forceps. The 4-mm rigid scope with cameraattachment is then inserted through this wound. No trocar is used. Theelasticity of the abdominal wall fascia and musculature provides an airtightseal around the scope. A second port is then created in the right lower
quadrant to allow introduction of the laparoscopic forceps into the perito-neal cavity. As above, an 18-gauge needle is used to create a defect whichis spread with forceps to a diameter of 2 mm. Again, no trocar is needed(Fig. 2).
With the pneumoperitoneum established the abdomen is laparoscopi-cally explored for the terminal ileum and cecum, which are usually foundin the left lower quadrant. The cecum is grasped at its end with the forceps(Fig. 3) and carefully exteriorized through the 2-mm wound in the rightlower quadrant. There is no mesentery, nor are there ligamentous attach-ments tethering the cecum; however, an artery and vein course longitudi-nally along the cecum to its end. Extracorporeally, the cecum and itsvascular supply are ligated together with a single 4-0 silk ligature (Fig. 4).The cecum is then resected and irrigated with normal saline before thestump is gently returned to the peritoneal cavity. The abdominal walldefects are then stapled closed and the animal is allowed to recover fromanesthesia.
Results
To date our laboratory has done 94 laparoscopic-assistedcecal resections using this model which have been pairedwith 95 open cecal resections. Early in our experience, threemice (3.2%) undergoing laparoscopic-assisted cecal resec-tion were sacrificed intraoperatively after inadvertent injuryto bowel or a vascular structure. This was similar to theintraoperative complication rate in the open resection group(2.1%,p 4 0.99 by chi square). There were no postopera-tive leaks from the cecal stump noted in any of the animals.Furthermore, there were no deaths due to peritonitis noted ineither group. The only postoperative death was in the openresection group secondary to evisceration due to dehiscenceof the laparotomy wound.
Fig. 1. Normal anatomy of the mouse colon, ileum, and cecum, demon-strating how the cecum can be amputated without disrupting bowel conti-nuity.
Fig. 2. The mouse instrumented for laparoscopic surgery.
623

Discussion
The mouse model of laparoscopic cecal resection hasproven to be a reliable, economical, and reproducible modelof laparoscopic bowel resection. As stated previously, thismodel allows a bowel resection to be performed yet doesnot require an anastomosis. A bowel anastomosis in amouse would be technically very challenging to perform.As described, the cecal resection can be carried out quicklywith low morbidity and mortality. Experience with nearly100 mice has resulted in an intraoperative complication rateof 3.2%, no postoperative deaths, and no leaks. This modelhas proven to be easy to master. This simple model can be
mastered by individuals with very limited surgical experi-ence after several procedures. The procedure can be com-pleted in less than 10 min in experienced hands. In ourinvestigations, the length of surgery has been standardizedto 20 min.
Murine models have several advantages over large-animal models for the scientific investigation of laparosco-py. Syngeneic species are genetically equivalent to othermembers of the same strain and are therefore ideal for im-munologic studies. Many immunologic assays are well es-tablished in murine species. Tumor models are also wellestablished in murine species. Genetic manipulation is mostpractical in mice. Finally, the short amount of time requiredto complete the procedure and the low cost per animal willallow investigators to include a larger number of animals intheir studies.
Using this mouse model of cecal resection, our labora-tory has tested differences in tumor growth and establish-ment after open vs laparoscopic intervention [2]. We havealso developed a similar model in rats which we have usedto test for postoperative immunological differences afteropen or laparoscopic-assisted bowel resection [3, 4]. Ourexperience with 40 rats has shown an intraoperative com-plication rate of 2.5%, which was the same as that seen afterthe open resection.
Recently, excellent 2-mm laparoscopes as well as im-proved 2-mm grasping laparoscopic forceps and dissectingscissors have been developed by a number of manufacturersand are commercially available. Such instruments will al-low investigators to further limit the size of incisions nec-essary to perform laparoscopic procedures on small animalsand should, therefore, improve these minimal access mod-els.
Acknowledgment.This research was made possible by generous supportfrom the Ethicon division of Johnson and Johnson Inc. and the Associationof Women Surgeons.
References
1. Allendorf JDF, Bessler M, Kayton ML, Oesterling SD, Treat MR, Now-ygrod R, Whelan RL (1995) Increased tumor establishment and growthafter laparotomy vs laparoscopy in a murine model. Arch Surg 130:649–653
2. Allendorf JDF, Bessler M, Whelan RL, Laird D, Horvath K, KaytonML, Nowygrod R, Treat MR (1996) Tumors grow larger after open vslaparoscopic bowel resection in a murine model. Surg Endosc 10: 182
3. Allendorf JDF, Bessler M, Whelan RL, Trokel M, Laird DA, Terry MB,Treat MR (1996) Postoperative immune function varies inversely withdegree of surgical trauma in a murine model. Surg Endosc 11:427–430
4. Allendorf JDF, Bessler M, Whelan RL, Trokel M, Laird DA, Terry MB,Treat MR (1996) Better preservation of immune function after laparo-scopic-assisted versus open bowel resection in a murine model. DisColon Rectum (submitted)
5. Bessler M, Whelan RL, Halverson A et al. (1994) Is immune functionbetter preserved after laparoscopic versus open colon resection? SurgEndosc 8: 881
6. Bessler M, Whelan RL, Halverson A, Allendorf JDF, Nowygrod R,Treat MR (1996) Controlled trial of laparoscopic-assisted vs open colonresection in a porcine model. Surg Endosc 10:732–736
7. The Southern Surgeons Club (1991) A prospective analysis of 1518laparoscopic cholecystectomies. N Engl J Med 325: 1517–1518
Fig. 3. A laparoscopic view of the pelvis showing the cecum grasped at itsblind end.
Fig. 4. The cecum is ligated and resected extracorporeally.
624

The influence of laparotomy and laparoscopy on tumor growth in arat model
C. A. Jacobi,1 J. Ordemann,1 B. Bohm,1 H. U. Zieren,1 C. Liebenthal,2 H. D. Volk,2 J. M. Mu ller1
1 Department of Surgery, Humboldt-University of Berlin, Charite´, Schumann Strabe 20/21, 10098 Berlin, Germany2 Institute of Medical Immunology, Humboldt-University of Berlin, Charite´, Schumann Strabe 20/21, 10098 Berlin, Germany
Received: 7 November 1996/Accepted: 3 December 1996
AbstractBackground:The effects of laparotomy and laparoscopywith different gases on subcutaneous and intraperitonealtumor growth have not been evaluated yet.Methods:Tumor growth of colon adenocarcinoma DHD/K12/TRb was measured in rats after laparotomy, laparos-copy with CO2 or air, and in control group. Cell kineticswere determined after incubation with carbon dioxide or airin vitro and tumor growth was measured subcutaneouslyand intraperitoneally after surgery in vivo.Results:In vitro, tumor cell growth increased significantlyafter incubation with air and CO2. In vivo, intraperitonealtumor weight was increased after laparotomy (1,203 ± 780mg) and after laparoscopy with air (1,085 ± 891 mg) andwith CO2 (718 ± 690 mg) compared to control group (521± 221 mg) (p < 0.05). Subcutaneous tumor growth waspromoted after laparotomy (71 ± 35 mg) and even moreafter laparoscopy with air (82 ± 45 mg) and CO2 (99 ± 55mg) compared to control group (36 ± 33 mg).Conclusions:Insufflation of air and CO2 promote tumorgrowth in vitro. In vivo, intraperitoneal tumor growth seemsto be promoted primarily by intraperitoneal air and subcu-taneous tumor growth by CO2.
Key words: Laparotomy — Laparoscopy — Tumor growth— Air — Carbon dioxide
Laparoscopic techniques are still discussed controversiallyfor treatment of malignancies because port site recurrencesand peritoneal tumor seeding after laparoscopic cholecys-tectomy, colectomy, and gastric resection have been re-ported [3, 4, 6, 7, 11, 12, 15]. Apparently tumor seeding anddevelopment of subcutaneous metastases appear more oftenafter laparoscopic than after open resections of malignant
tumors. The mechanism of this phenomen is still hypotheti-cal [2, 8, 14]. In contrast to these clinical observations,Allendorf et al. have demonstrated that subcutaneous tu-mors were more easily established and grew more aggres-sively after laparotomy than after insufflation with CO2 in amice model [1]. It was suggested that the difference intumor growth is due to postoperative immune advantage inthe laparoscopic group compared to open surgery. Sinceimmunologic changes have not been evaluated in this studythe hypothesis remains theoretical and has not been con-firmed yet. Another important factor in tumor growth,which has not been evaluated until now, may be the influ-ence of the gas used to establish pneumoperitoneum.Whether carbon dioxide, commonly utilized in laparoscopicsurgery, causes subcutaneus port site recurrences has to beevaluated. The influence of air on tumor cell growth hasalso not been investigated.
Therefore, we investigated the influence of differentgases commonly used in laparotomy and laparoscopy ontumor cell growth in vitro, ex vivo, and in vivo.
Methods
In the first experiment the influence of carbon dioxide and air on tumorcells was investigated in vitro in order to evaluate the influence of differentgases on the cell lines without immunological interaction of the host. Airwas chosen to duplicate the situation during laparotomy. The hypothesis ofthe study was that there is a difference in tumor growth between thedifferent gases.
Colonic carcinoma cell line DHD/K12/TRb cells (ECACC) were cul-tured in Dulbecco’s MEM (Biochrom, Germany) and Ham’s F10 medium(Biochrom, Germany) 1:1 supplemented with 10% fetal bovine serum(Gibco BRL, Germany), 2 mmol/l Gluthamin (Biochrom, Germany), andpenicillin-streptomycin (Gibco, Germany) 1,000 IU/ml.
Cells (5 × 106) were suspended in 10 ml of culture medium. They wereincubated either with pure carbon dioxide or air or underwent no furthermanipulation in the control group. The gases were insufflated into theculture flasks (75 cm2/250 ml) through a sterile filter and drawn outthrough a control valve. Pressure during incubation was 0.5 (0–1.0) mmHgin each experiment. Gas analyses of the ‘‘atmosphere’’ in the flasks de-tected absence of oxygen during the incubation with carbon dioxide. Partialpressure of oxygen was 20.8 ± 0.7 kPa after air incubation and 20.5 ± 0.4Correspondence to:C. A. Jacobi
Surg Endosc (1997) 11: 618–621
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

kPa in the control group. Before intervention, oxygen pressure in the me-dium was 24.8 ± 1.7 kPa and carbon dioxide pressure was 2.3 ± 0.3 kPa inall groups. After intervention, oxygen pressure changed to 6.7 ± 0.7 kPa(carbon dioxide), 25.5 ± 1.9 kPa (air), and 23.3 ± 1.8 kPa (control) whereascarbon dioxide pressure was 79.3 ± 3.3 kPa (carbon dioxide), 1.4 ± 0.2 kPa(air), and 2.7 ± 0.6 kPa (control) in the medium.
After 3 h of incubation, cells were washed twice, resuspended, andcultured in 15 wells (1.88 cm2) with a concentration of 104 viable tumorcells/well. Three wells of each group were washed twice with PBS(Charite, Berlin) after 24 h and incubated with 300ml 0.05 trypsin/0.02%EDTA (Biochrom, Germany) for 30 min at 37°C to remove adherent cells.Viable and dead cells were counted after staining with acridine-orange byfluorescence microscopy for 4 days. Experiments were repeated five timesso that 15 wells in each group could be evaluated every 24 h.
In the second experiment, the effect of pneumoperitoneum in rats withcarbon dioxide or air on intraperitoneal tumor cells was evaluated. Tumorcells were injected into the peritoneal cavity of the animals, insufflated for3 h, and removed and cultured ex vivo. These experiments were performedto evaluate the influence of gas insufflation in vivo (pneumoperitoneum)and to minimize the influence of the immunologic response of the tumorhost. The hypothesis of this experiment was that there is a difference intumor growth after in vivo insufflation with air and carbon dioxide.
Fifteen rats were randomized into three groups and all received intra-peritoneal injection of 5 × 106 cancer cells. Pneumoperitoneum with 8mmHg was performed in two groups with insufflation of pure carbondioxide (n 4 5) or air (n 4 5). The other five rats underwent the same3 h of anesthesia and were used as control group. Gas analyses of the‘‘intraabdominal atmosphere’’ detected again absence of oxygen at the endof insufflation with carbon dioxide and a partial oxygen pressure of 20.5 ±0.6 kPa after air insufflation. After 3 h, rats underwent laparotomy andintraperitoneal lavage with 15 ml of medium to harvest the cells. The totalamount of viable tumor cells in the lavage was determined before centrifu-gation of the cell suspension. Cells were again cultured in 15 wells (1.88cm2) with a concentration of 104 cells/well. Kinetics of cell growth weredetermined for 4 days as in the first experiment.
In the animal model, the influence of laparotomy and laparoscopy withcarbon dioxide or air was investigated after intraperitoneal and subcutane-ous application of tumor cells. Tumor growth was measured 5 weeks afterapplication. The hypothesis of this experiment was that tumor growth isincreased after laparotomy compared to laparoscopy and that there is alsoa difference in tumor growth between the different gases used to establishpneumoperitoneum. Intraperitoneal and subcutaneous injection was per-formed to evaluate the effects on different tumor sites.
One hundred male inbred BD IX rats 2 months old (Iffa-Credo,L’Arbresle, France) were acclimated to a climate- and light-cycle-controlled environment for at least 7 days prior to investigations. Theanimals were allowed standard laboratory food and water ad libitum. Allstudies were performed under protocols approved by the local committeesof Animal Use and Care.
Tumor cells 1 × 104 were introduced intraperitoneally and subcutane-ously in all animals. The rats were randomized into four different groups.Laparotomy was accomplished in the first group (n 4 25) and the abdo-men was closed again after 30 min. In the second and third groups, lapa-
roscopy was performed with insufflation of either pure carbon dioxide (n4 25) or air (n 4 25) at a pressure of 8 mmHg over 30 min. Theabdominal wall was incised three times with introduction of 4.5-mm tro-cars to evaluate the development of tumor growth at these incisions. Thecontrol group (n 4 25) underwent tumor cell injection and incisions of theabdominal wall with introduction of 4.5-mm trocars. The animals weresacrificed 5 weeks later, tumors were excised intraperitoneally and subcu-taneously, and the weights were assessed on a balance.
Data are given as mean and standard deviation. Data between groupswere compared using a Kruskal Wallis test for continuous data and theFisher’s exact test for categorical data, if appropriate;p values less than0.05 were considered significant.
Results
First experiment
All tumor cells grew for 4 days (Fig. 1). Insufflation withcarbon dioxide and air led to increased tumor cell growth invitro compared to the control group with significant differ-ence on day 4 (p < 0.05). Tumor growth was promoted evenmore after incubation with air.
Second experiment
Cells were removed from the peritoneal cavity and grownover 4 days (Fig. 2). Tumor growth was stimulated evenmore in this ex vivo experiment and the number of viabletumor cells counted on the 4th day was four times higher inall three groups compared to the results of the first experi-ment. Tumor cell growth in vitro increased after in vivoinsufflation of the cells with carbon dioxide compared to thecontrol group. The number of viable cells was more thanthree times higher in the carbon dioxide group than in thecontrol group (p < 0.05) after 48 and 72 h. Cell kinetics ofthe air group also showed a strong promotion of tumor cellgrowth, reaching significant difference compared to thecontrol group only on day 4 because of an extremely highstandard deviation in this group. After incubation, cellgrowth showed no significant difference between air andcarbon dioxide insufflation.
Fig. 1. In vitro tumor cell growth after insufflation with carbon dioxide (n4 15) and air (n 4 15) in comparison to the control group (n 4 15) (meanand standard deviation, *p < 0.05: carbon dioxide vs control group, §p <0.05: air vs control group).
Fig. 2. In vitro tumor cell growth after insufflation in vivo with carbondioxide (n 4 15) and air (n 4 15) in comparison to the control group (n4 15)(mean and standard deviation, *p < 0.05: carbon dioxide vs controlgroup, §p < 0.05: air vs control group).
619

Third experiment
In vivo, subcutaneous tumor growth was promoted afterlaparotomy (71 ± 35 mg) and even more after laparoscopywith air (82 ± 45 mg) and CO2 (99 ± 55 mg) compared tocontrol group (36 ± 33 mg) (p < 0.05) (Fig. 3). Intraperito-neal tumor weight also differed (p 4 0.007) between thefour groups (Fig. 4). Tumor weights were 1,203 ± 780 mgin the laparotomy group, 1,085 ± 891 mg after laparoscopywith air, 718 ± 690 mg in the CO2 group, and 521 ± 221 mgin the control group.
Frequency of tumor growth was increased (p < 0.001) atthe abdominal trocar sites in carbon dioxide and air groupscompared to the control group (Table 1). These tumors de-veloped most often subcutaneously (95%). After laparoto-my, seven rats developed tumor nodes at the laparotomyincision, ten rats had tumor at the abdominal incisions afterinsufflation with air, 20 rats had tumors after carbon diox-ide, and only two rats developed tumors in the controlgroup. Tumor growth at more than one incision was foundin five rats of the air group, in ten rats of the carbon dioxidegroup, and did not occur at all in the control group.
Discussion
Metastases in the abdominal wall appear more often afterlaparoscopic surgery than after open resection for malignanttumor. Reports of early port site recurrence after laparo-scopic procedures have reduced enthusiasm about laparo-scopic techniques for malignant disease. Currently, an ac-cepted explanation of what may cause these abdominal wallmetastases does not exist [3, 4, 6, 7, 11].
In the first experiment, the direct influence of carbondioxide and air on cultured cells was investigated in vitro.Cell growth of the adenocarcinoma cell line was signifi-cantly stimulated after insufflation with both gases com-pared to control group. The number of viable cells was evenhigher after air incubation than after carbon dioxide. It ishypothesized that the gases act on the cells themselves, butthe mechanisms leading to promotion of the tumor cellgrowth in vitro either by carbon dioxide or air are not clearyet. Therefore, further studies are needed to elucidate thepathophysiological mechanisms of the observations.
In the second experiment, the effect of pneumoperito-neum with carbon dioxide or air on intraperitoneal tumorcells was evaluated in rats. Again tumor cell growth in-creased in the carbon dioxide and air groups compared withthe control group. Additionally, the number of counted cellsafter insufflation in this experiment was higher than in thefirst experiment, which may be caused by peritoneal mac-rophages producing interleukin-1 (IL-1) and lead to promo-tion of cell growth [5].
The animal model used is well established and it isknown that rat colonic carcinoma DHD/K12/TRb growsprogressively when injected subcutaneously [13] or intra-peritoneally [10] in syngeneic animals. In this study, 104
tumor cells were administered subcutaneously and intraper-itoneally because the number of cells is sufficient to estab-lish tumor growth in all animals in preliminary studies.
Intraperitoneal tumor growth differed significantly be-tween the four groups in vivo. Laparotomy markedly in-creased intraperitoneal tumor growth compared to laparos-copy with carbon dioxide and in the control group. Inter-estingly, intraperitoneal tumor weight was similar afterlaparoscopy with air insufflation and laparotomy. Thus, tu-mor growth seems to be promoted by intraperitoneal air andless by an additional trauma in the laparotomy group. Incomparison to laparotomy and laparoscopy with air, lapa-roscopy with carbon dioxide led only to a minor increase ofintraperitoneal tumor growth. This important difference hasnot been seen in the experiments in vitro, which indicatesthat reactions of the tumor host do modify tumor growth invivo.
In contrast to the abdominal site, tumor growth at the
Fig. 3. Weight of tumors taken from the subcutaneous site 5 weeks aftercell application and insufflation (n 4 25 in each group) (mean and stan-dard deviation, as *p < 0.05: carbon dioxide vs control group).
Fig. 4. Weight of intraperitoneal tumors 5 weeks after cell application andinsufflation in the rats (n 4 25 in each group) (mean and standard devia-tion, * p < 0.05: laparotomy and laparoscopy with air vs control group).
Table 1. Incidence (%) of tumor at the abdominal incisions 5 weeks afterthe laparoscopy with carbon dioxide (n 4 25) or air (n 4 25) or withoutpneumoperitoneum (n 4 25)
Tumor growth
Carbondioxide(n 4 25)
Air(n 4 25)
Control(n 4 25)
None 24% 52% 92% p 4 0.0001At 1 incision 24% 24% 8% p 4 0.2At 2 incisions 40% 16% p 4 0.0003At 3 incisions 12% 8% p 4 0.1
620

subcutaneous site was not significantly different betweenthe ‘‘treated’’ groups. Subcutaneous tumor weight wasmostly pronounced in the laparoscopic group with carbondioxide. Carbon dioxide seems to act more on the subcuta-neous site than intraperitoneally, which may be explainedby the high solubility of carbon dioxide in subcutaneoustissue. The results indicate that carbon dioxide actually is animportant factor promoting tumor growth in small trocarincisions. Most of the reported abdominal wall metastasesafter laparoscopic surgery did not occur in the abdominalwall but in subcutaneous tissue close to the trocar incisions[3, 6, 9], which is in accordance with our experiments.Almost all tumor nodes at the abdominal incision were lo-cated in the subcutaneous tissue. If this can be confirmed infuture studies, it may be that early port site recurrences arenot as disastrous as they appear today because local excisionmay be a curative treatment.
In contrast to our results, Allendorf et al. have demon-strated that tumors were more easily established subcutane-ously and grew more aggressively after laparotomy thanafter insufflation with carbon dioxide [1]. In their study amammary carcinoma cell line was used without intraperi-toneal application of the cells. Pneumoperitoneum was per-formed over 30 min with an intraabdominal pressure of only4–6 mmHg, which might have caused lower levels of car-bon dioxide in the subcutaneous tissue. They also found ahigher incidence of tumor in the insufflation group com-pared to the control group. The authors suggested that thereis a postoperative immune advantage in laparoscopy leadingto minor subcutaneous tumor growth compared to laparot-omy. This hypothesis is still unproven. It remains unclearwhether immunologic suppression after laparotomy is re-lated to surgical trauma or other factors like intraperitonealair.
Many questions remain unanswered because the patho-mechanisms of these phenomena are not known yet. If theresults can to be confirmed in other studies they may changean attitude regarding treatment of cancer patients with ques-tionable peritoneal carcinomatosis. They should rather un-dergo laparoscopy in order to evaluate the intraperitonealtumor status than open laparotomy because laparotomy mayharm patients much more than laparoscopy and may reducesurvival time. Furthermore, alternative gases should beevaluated in experimental studies to avoid the effects ofcarbon dioxide on subcutaneous port site metastases.
In conclusion, the results of the study indicate that thedifference in intraperitoneal tumor growth between laparot-omy and laparoscopy is mainly caused by intraabdominal
air and probably not to an additional trauma in the laparot-omy group. However, the hypothesis that air might influ-ence the immune system of the tumor host and increaseimmune suppression after laparotomy more than after lap-aroscopy remains theoretical.
Furthermore, the data suggest that insufflation of carbondioxide may be an important factor which promotes subcu-taneous metastases.
References
1. Allendorf JDF, Bessler M, Kayton ML, Oesterling SD, Treat MR,Nowygrod R, Whelan RL (1995) Increased tumor establishment andgrowth after laparotomy vs laparoscopy in a murine model. Arch Surg130: 649–653
2. Bessler M, Whelan RL, Halverson A, Treat MR, Nowygrod R (1994)Is immune function better preserved after laparoscopic versus opencolon resection? Surg Endosc 8: 881–883
3. Cava A, Roman J, Gonzales Quintela A, Martin F, Aramburo P (1990)Subcutaneous metastasis following laparoscopy in gastric adenocarci-noma. Eur J Surg Oncol 16: 63–67
4. Clair DG, Lautz DB, Brooks DC (1993) Rapid development of um-bilical metastases after laparoscopic cholecystectomy for unsuspectedgallbladder carcinoma. Surgery 113: 355–358
5. Dinarello CA (1994) The biological properties of interleukin-1. EurCytokine Netw 5(6): 517–531
6. Drouard F, Delamarre J, Capron J (1991) Cutaneous seeding of gall-bladder cancer after laparoscopic cholecystectomy. N Engl J Med 325:1316
7. Fusco MA, Paluzi MW (1993) Abdominal wall recurrence after lap-aroscopic-assisted colectomy for adenocarcinoma of the colon. DisColon Rectum 36: 858–861
8. Horgan PG, Fitzpatrick M, Couse NF, Gorey TF, Fitzpatrick JM(1992) Laparoscopy is less immunotraumatic than laparotomy. Mini-mally Invasive Ther 1: 241–244
9. Jacobi CA, Keller H, Mo¨nig S, Said S (1995) Implantation metastasisof unsuspected gallbladder carcinoma after laparoscopy. Surg Endosc9: 351–352
10. Lagadec P, Jeannin JF, Reisser D, Pelletier H, Olsson O (1987) Treat-ment with endotoxins of peritoneal carcinomatosis induced by colontumor cells in rats. Invasion Metastasis 7: 83–95
11. O’Rourke N, Price PM, Kelly S, Sikora K (1993) Tumor inoculationduring laparoscopy. Lancet 342: 368
12. Pezet D, Fondrinier E, Rotman N, Guy L, Lemesle P, Lointier P,Chipponi J (1992) Parietal seeding of carcinoma of the gallbladderafter laparoscopic cholecystectomy. Br J Surg 79: 845
13. Reisser D, Fady C, Lagadec P, Martin F (1991) Influence of theinjection site on the tumorigeniticity of a cloned colon tumor cell linein the rat. Bull Cancer 78: 249–252
14. Torkel MJ, Bessler M, Treat MR, Whelan RL, Nowygrod R (1994)Preservation of immune response after laparoscopy. Surg Endosc 8:1385–1388
15. Wexner SD, Cohen SM (1995) Port site metastases after laparoscopiccolorectal surgery for cure of malignancy. Br J Surg 82: 295–298
621

EndoScope: world literature reviews
Original articles from a wide range of international surgical journals are selected by our editors and presentedhere as a structured summary and critical review.EndoScopeserves as a quick and comprehensive surveyof the expansive endoscopic literature from all the corners of the globe.
Long term results of endoscopic stenting andsurgical drainage for biliary stricture due tochronic pancreatitis
Smits, ME, et alBr J Surg (1996) 83:764–768
A retrospective evaluation of endoscopic stenting in 58 pa-tients with benign biliary stricture due to chronic pancreati-tis is reported with the intention of determining whetherendoscopic therapy alone can replace surgical drainage. Per-sistent jaundice in 46 and cholestasis in 12 patients arenoted (cholestasis being defined as increased alkaline phos-phatase levels thrice the normal value for >1 month). ERCPis performed in all patients with placement of 10-Fr stents.Follow-up is approximately 3–9 months thereafter, withstents being exchanged electively or when patients had re-current symptoms (jaundice, cholangitis, pain). Success isdefined as clinical improvement with stricture regressionand permanent removal of the stent. Median follow-up is 49months.
All patients had relief of jaundice and cholestasis within2 weeks of stent insertion. The overall rate of complicationfollowing ERCP is 9% (two bleedings, one pancreatitis, onecholecystitis and liver abscess, one fever of unknown origin,and zero mortality). Patients had a median of three stentsover a median of 14 months. Stent-related complication rateis 64%, which includes clogging, migration, and erosionnecessitating replacement stents. With 4.1-year median fol-low-up, 28% of the study group show regression of stricturewith permanent removal of stent in about a median of a10-month period; 72% had persistent biliary stricture: 45%requiring continued stenting and 27% undergoing surgery.Indications for surgery are frequent stent-related complica-tions in nine patients, duodenal stenosis in two, and pancre-atic surgery for pain in five with chronic pancreatitis. Pro-cedure type ranges from simple sphincteroplasty to Whippleresection with the majority receiving various biliary by-passes. As such, the resultant postop morbidity of 38%ranged from wound infection to biliary leakage. The authorsconclude that both endoscopic stenting and surgery are ef-fective treatments for biliary stricture in patients withchronic pancreatitis; of particular note is the lower compli-cation rate associated with endoscopy. They do concede,however, that late stent-related complications remain a ma-jor limitation.
Overall, this paper addresses an important issue, themanagement of biliary stricture in the setting of chronic
pancreatitis. As expected, endoscopic management remainsa safe and effective means for treating the early phase ofbiliary obstruction, and the authors emphasize this pointvery well. The patients receiving surgical treatment, on theother hand, remain a distinct group standing apart from theendoscopy responders. The 16 patients requiring surgicaltherapy all underwent previous repeated stenting followedby failure—a major indicator probably reflecting the sever-ity of chronic pancreatitis. Although early stenting is asso-ciated with a lower complication rate, the direct nonstrati-fied comparison to surgical postop morbidity rate remainsequivocal. The authors do identify a distinct role for endo-scopic therapy in biliary stricture due to chronic pancreati-tis.
Endoscopic perforation in unsedated patientsundergoing endoscopy
Hedenbro, JL, Ekelund, MBr J Surg (1996) 83:845–846
The complication rate of esophagogastroduodenoscopy in13,639 cases is presented from data collected since 1990 ina university hospital referral center. Most procedures areperformed without sedation (97.9%) using standard flexibleendoscopes. Only two cases report perforation that requiredoperative repair.
The authors have shown that unsedated endoscopy withthroat analgesia is safe and associated with low perforationrate (0.015%). No significant cardiopulmonary events arenoted and the perforation is well below the usual 0.03–0.05% rate. An additional interesting point is that oxygensaturation monitoring and oxygen supplementation are notroutinely employed although the cost-effectiveness of thisstep is probably negligible.
Relations between oesophageal acid exposureand healing of oesophagitis with omeprazolein patients with severe reflux oesophagitis
Holloway, RH, et alGut (1996) 38:649–654
The effect of omeprazole and severe ulcerative esophagitisdue to acid reflux is examined. Eight-week treatment of
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 679–683

omeprazole at 20 mg per day in 60 patients with grade 3 or4 ulcerative esophagitis is followed by an additional 8-weekcourse of omeprazole at 40 mg daily for those unhealed withinitial therapy. Endoscopy and 24-h esophageal pH moni-toring are performed before treatment and at the end of eachtreatment phase. Only patients with severe erosive pepticesophagitis are entered, and those with reflux diseasemarked by columnar metaplasia or benign stricture withouterosion are excluded.
Of the 60 entered for the study, 55 patients eventuallyunderwent the omeprazole trials. Thirty percent failed toheal in the initial trial, and they all exhibited greater 24-hacid exposure than the group that healed. In the secondphase of the trial, 47% of the unhealed also failed thedoubled dosage trial for additional 8 weeks. Once again, thefailed group exhibited greater acid exposure than the healedsubjects. The authors conclude that patients with severeulcerative esophagitis who are refractory to omeprazolehave greater esophageal acid exposure while receiving treat-ment than responding patients. They attribute this to re-duced responsiveness to acid suppression. An interestingpoint one gathers from this study is the significant numberof patients who may still respond to increased omeprazoledosage after the initial trial failure. Although one-thirdfailed the initial dose, nearly half of the unhealed patientsresponded with increased omeprazole administration. Thenext question is, How about an additional 8-week trial forthe ones who failed to heal?
Eradication of Helicobacter pyloriin patientswith duodenal ulcer lowers basal and peakacid outputs to gastrin releasing peptideand pentagastrin
Harris, AW, et alGut (1996) 38:663–667
The relationship betweenHelicobacter pyloriand gastricacid hypersecretion is explored in patients with duodenalulcer disease. Ten healthy volunteers with normal endos-copy and negativeH. pylori and ten positiveH. pylori pa-tients with documented duodenal ulcer were followed for 6months afterH. pylori eradication with omeprazole andamoxycillin therapy.H. pylori status was determined byhistology, culture, and by the13C-urea breath test. Basalacid output (BAO) and peak acid outputs (PAO) followinggastrin-releasing peptide (GRP) and pentagastrin stimula-tion were recorded before and 6 months afterH. pylorieradication.
Basal and stimulated acid output levels are elevatedmore in theH. pylori group than the negative controls. Sixmonths afterH. pylori eradication, basal and stimulated acidoutputs are all below the initial starting levels. The resultsshowH. pylori involvement in hypersecretion and duodenalulcer disease by revealing lower basal and peak acid outputsto gastrin-releasing peptide and pentagastrin followingH.pylori eradication. Of the ten patients selected initially in the
disease group, only seven completed the study. Perhapsmore numbers in this group will reinforce the data pre-sented. However, these results do point to the role in gastricinflammation ofH. pylori in peptic ulcer disease.
Randomized, prospective, single-blindcomparison of laparoscopic versussmall-incision cholecystectomy
Majeed, AW, et alLancet (1996) 347:989–994
A prospective randomized comparison between electivelaparoscopic and small-incision cholecystectomy in 200 pa-tients involving four surgeons was conducted at Sheffield,UK. All subjects had symptomatic gallstones confirmed byultrasonography and were randomized for elective cholecy-tectomy by either method. The four participating surgeonshad performed a minimum of 40 laparoscopic cholecytec-tomies each as either the principle operator or assistant andno comment was made about their small-incision experi-ence. The small-incision method requires a high transversesubxiphoid incision over the junction of the cystic duct andcommon bile duct. The length of the incision is tailored toindividual cases (median of 7 cm). Standard instruments areused for the ‘‘fundus-last’’ dissection, and finally, as inlaparoscopy, all cases are accompanied by intraoperativecholangiogram.
The authors report a longer time required for laparo-scopic cholecytectomies when compared to the small-incision procedure (median 65 min vs 40 min, respectively,and including cholangiogram time). They found no differ-ence between the groups for hospital stay, time back towork, and time to full activity.
Of the 205 meeting the criteria for elective cholecytec-tomy between 1992 to 1995, only five cases are eliminatedbecause of refusal for randomization, hepatic metastasis, orcirrhosis. Although patient selection was randomized, thefour surgeons participating in the study were still able toaffect the outcome of the study—a design flaw that is al-ways an inherent problem in this type of study. The longertime reported for the laparoscopic procedure may not be asignificant finding as it can certainly be shortened. Finally,the complication reported is notable for one bile duct injuryonly in the laparoscopic group, which was fortunately iden-tified after an intraoperative cholangiogram. An interestingobservation is that the overall conversion rate in the lapa-roscopic group turned out to be 20%, a figure that is a littletoo preferential for the open technique.
Certainly, the authors have shown that for the surgeonswell adapted to the small-incision technique, postoperativerecovery results can be achieved that are similar to thosewith the laparoscopic method. However, it is impossible toremove the bias for or against the procedure of the surgeonsin the study, and therefore true randomization remains ques-tionable.
680

Acute phase is the only significantly reducedcomponent of the injury response afterlaparoscopic cholecystectomy
Targarona, EM, et alWorld J Surg (1996) 20:528–534
This study investigates the response to injury induced bylaparoscopic vs open cholecystectomy by evaluating theneuroendocrine, acute phase, and metabolic responses.Twenty-five patients with noncomplicated gallstones arestudied in prospective but not randomized fashion (12 inlaparoscopic vs 13 in open cholecystectomy groups).
As expected, the requirement for postoperative analge-sia and hospital stay are significantly less in the laparoscop-ic group. Both procedures result in increased levels of serumglucose, lactate, white blood cell count, prolactin, ACTH,cortisol, interleukin-6, C-reactive protein, and arterial PCO2while the levels of total proteins, albumin, prealbumin, freefatty acids, hemoglobin, and arterial pH are decreased. Noappreciable changes in the levels of growth hormone, insu-lin, or glucagon are noted. The notable differences betweenthe two are significantly decreased levels of interleukin-6,C-reactive protein, and prealbumin in the laparoscopicgroup when compared to the open group. The authors con-clude that the less intense acute-phase response may beattributable to the reduced size of the wounds in laparos-copy.
The invited commentary by Haglund and Rastad followsthe article and outlines well some of the problems in thestudy, such as lack of randomized selection groups, toosmall a number of subjects to make an adequate conclusion,and the question of precision of the IL-6 bioassay involved.In addition, while some of the reported parameters in thisstudy substantiate previous reports, others contradict. Per-haps this confusion could be clarified by focusing on therelevance of these biochemical-parameter measurementsin injury response and on the validity of using them togeneralize about acute-phase response in laparoscopy. Thisis an interesting study overall with notable measurements,but perhaps the title and the conclusion could be less gen-eral, as the paper still does not show a direct link betweenwound size and the various inflammatory responses re-ported.
Laparoscopic treatment of gallbladder andcommon bile duct stones: a prospective study
Lezoche, E, et alWorld J Surg (1996) 20:535–542
Single-stage laparoscopic treatment of gallstones and ductalstones in 100 patients is reported. A total of 950 consecutivepatients admitted for elective laparoscopic cholecytectomywere submitted to intraoperative cholangiogram, which
identified the 100 cases. Of these, 26 are included withfailed ERCP retrieval of common bile duct (CBD) stones.The CBD stones are then retrieved laparoscopically using acombination of choledochoscope and an intracorporeal elec-trohydraulic or pulsed-dye laser lithotriptor. The approachis either by trancystic duct CBD (n 4 63) or direct CBD (n4 33) exploration via choledochotomy, with only fourcases converted to open procedure. Biliary drain placementas well as completion cholangiogram is performed for allcases. Retained CBD stones are identified in five patients,of which two are retrieved by ERCP and three by lithotrip-sy. The same surgeon is the principal operator in the entireseries. Finally, the biliary drains are removed 5 weekspostop after obtaining follow-up cholangiogram.
Major morbidity reported includes bile leakage from thecystic stump due to slipped clips (n 4 2) and accidentalremoval of biliary drain (n 4 1), all of which are treatedwith nasobiliary decompression. One mortality involvescardiogenic shock on postop day 3 in an 81-year-old whohad undergone failed ERCP clearance of large CBD stonesand developed cholangitis prior to laparoscopy.
This article clearly demonstrates the relative safety andfeasibility of laparoscopic retrieval of CBD stones as a one-stage procedure in conjunction with laparoscopic cholecys-tectomy. Although there is no control group in the trial, theadvantages of a minimally invasive procedure apply in thisscenario as well. The issue of cost will be the major hurdle;the degree of expertise required for this procedure to gainwide acceptance is also an issue. As in many laparoscopicreports, the data from this series reflect experience of asingle surgeon. It would be interesting to examine pooleddata from multicenter trials to evaluate reasonable successand morbidity rates. What the best treatment of CBD stoneis is a question still unanswered, and further data comparingthe ERCP retrieval vs the laparoscopic method will nodoubt be available in the near future.
Laparoscopic treatment of nonparasitic livercysts: adequate selection of patients andsurgical technique
Gigot, JF, et alWorld J Surg (1996) 20:556–561
Laparoscopic fenestration of nonparasitic liver cysts is per-formed in 26 patients. Seventeen had symptomatic solitaryliver cyst while nine suffered from polycystic liver disease.The major symptom reported is abdominal pain and eight(31%) of these patients had prior treatment failures withconventional methods. Laparoscopic fenestration includeswide cystic wall deroofing of as many cysts as possible withhemostasis achieved by argon-beam coagulation. A perito-neal drain is placed in 23 patients, and all excised cysts areconfirmed by histologic exam. The mean duration of fol-low-up with routine CT scan is 9 months. Recurrence isdefined as reappearance of cysts on CT scan or symptoms.
The feasibility of laparoscopy is 92%, with only twocases requiring laparotomy because of inaccessibility of the
681

cysts. Although the authors claim no major morbidity ormortality, one case of intraoperative cardiac arrest duringinsufflation is noted. The mean postop stay is 4.6 days. Thetwo patients who underwent laparotomy stayed for 8 and 12days, respectively. Clinical recurrence of symptoms is seenin six cases (23%) but only two are attributable to recur-rence of liver cyst. Recurrence documented on CT scan isseen in ten patients (38%) with only one undergoing reop-eration by open fenestration.
The application of laparoscopy in the treatment of livercysts is an appropriate method available and any study thatcontributes to this database is always valuable. Because ofthe rather noticeable recurrences, the authors advocate se-vere restriction of surgical indications and careful selectionof patients. They go so far as to recommend preoperativeultrasound or CT-guided aspiration of these cysts to test forrelief of symptoms, and the laparoscopic approach be re-served only if cyst-related symptoms recur with the cystrecurrence. Although laparoscopy has been shown to befeasible and relatively safe, the follow-up recurrences arediscouraging and certainly do not measure up to conven-tional treatment, which will ultimately decide the future ofany new application. As advocated, perhaps there is a role forlaparoscopy in cases of isolated, easily accessible, liver cysts.
Endoscopic and surgical complications ofwork-up in screening for colorectal cancer
Kewenter, J, Brevinge, HDis Colon Rectum (1996) 39(6):676–680
The purpose of this extensive study is to evaluate the com-plication rate of diagnostic and therapeutic procedures in-volved in massive screening (68,306) and workup for colo-rectal neoplasm. Flexible sigmoidoscopy (FS), up to 60 cm,is performed in 2,108 patients who were Hemoccult positiveon initial screening. Only 39 had to be repeated due to poorbowel prep; 554 polypectomies are performed in 413 (20%)patients with three reported cases (0.5% polypectomies) ofsigmoid colon perforation requiring repair. Only benign ad-enomas are noted on biopsy.
A total of 1,987 patients (94%) of the 2,108, complywith barium enema without complication; 190 (10%) ofthese patients then undergo colonoscopies for abnormalbarium studies. Polyps are removed in 113 patients duringcolonoscopy, of which three (0.03%) sustain complications(one hemorrhage, two perforations).
Laparotomies with appropriate procedures are per-formed on 104 patients (carcinoma 79, adenoma 13, diver-ticular disease four, no tumor five, inflammatory bowel dis-ease two, abdominal aneurysm one). Significant complica-tions developed in 14 (13%) patients, and although theauthors report no deaths, one eventually died 2.5 monthspostop. A total of ten surgeons participated in this trial forexamining and operating the patients involved.
Out of 2,108 patients undergoing sigmoidoscopy, 104(0.05%) eventually undergo laparotomy with 13% morbid-ity and 0.01% mortality; 79 (0.04%) are diagnosed with
carcinoma. There are five false-positive laparotomies in theseries, and these should be included in the morbidity cat-egory. Perhaps laparoscopy should be considered in suchcases. At any rate, the lack of yield for carcinoma by sig-moidoscopy is notable, with the rate of perforation at 0.5%.Barium enema, on the other hand, reveals the 10% from thesame group of patients that required further workup withcolonoscopy with 0% complication. However, despitebarium contrast study and colonoscopy, five patients had toundergo ‘‘negative’’ laparotomies because of equivocalfindings. Overall, this study is a valuable contribution andwill no doubt help us to monitor the current policy involvedin massive screening and workup for the fight against co-lorectal carcinoma.
Cost-effectiveness management of complicatedcholedocholithiasis: laparoscopic transcysticduct exploration or endoscopic sphincterotomy
Liberman, MA, et alJ Am Coll Surg (1996) 182:488–494
This is a valuable study that examines the results and actualcosts of common bile duct stone therapy in the context ofminimally invasive surgery. In a retrospective analysis overa 4-year period, all patients undergoing laparoscopic chole-cystectomy (LC) plus endoscopic sphincterotomy (ES) arecompared to those undergoing LC plus laparoscopic trans-cystic common bile duct exploration (LTCBDE). All pro-cedures were performed at the same institution by differentsurgeons with varying levels of experience. Of the 76 pa-tients with choledocholithiasis, 59 patients underwent LCplus LTCBDE (group 1) and 17 patients underwent LC plusES (group 2). A subset of 21 patients in group 1 who hadurgent LC plus LTCBDE (group 3) because of cholecystitisor cholangitis, with or without pancreatitis, were also ex-amined separately.
In terms of hospital stay, group 1 or even group 3 isassociated with significantly shorter average period (6.1 and6.9 days, respectively) than group 2 (12.4 days,p < 0.001).The average cost in group 1 is $13,151, and $14,732 withprofessional reimbursement, and this includes the sevencomplications (12%) and one death (1.7%) reported. Thecost in group 2 averages about $18,712, or $21,125 withprofessional reimbursement, while there are seven (41%)complications reported, all related to ES, with no deaths,and this is factored into the cost. When group 3 is examined,the urgency of LC plus LTCBDE does not increase theaverage cost ($13,564, or $15,150 with reimbursement) orthe morbidity rate (two complications or 10%). Thus, thepaper concludes that LC plus LTCBDE for CBDS, whetherurgently or electively, has decreased morbidity rates, lengthof hospital stay, and costs when compared to LC plus ES.
The relatively high rate of morbidity reported in group 2probably reflects the degree of illness of these patients atpresentation as well as the small number involved in theretrospective study. As the authors report, the usual reportedES complication rate is 8.2% with 1.3% mortality. Clearly,the 41% morbidity rate reported is too high, and this will no
682

doubt lead to higher costs and hospital stay. The authors doattempt to adjust for this by creating group 3 (21 out of 59patients whose urgent operative indications are similar togroup 2). Interestingly, the cost in group 3 is still less whencompared to group 2; however, the high complication rate ingroup 2 accounts for this difference. Perhaps more numbersin this study and a prospective trial will elucidate the truecomplication rate of ES.
Intravenous infusion cholangiography forinvestigation of the bile duct: a directcomparison with endoscopicretrograde cholangiopancreatography
Bloom, IT, et alBr J Surg (1996) 83:755–757
The newer technique of slow intravenous infusion cholan-giography (IIC) using meglumine iotraxate is assessed using(ERCP) endoscopic retrograde cholangiopancreatogram asa gold standard in patients considered to be at high risk forbile duct stones. A total of 111 consecutive patients withcholelithiasis documented by ultrasound with the followingcriteria are selected: (1) history of jaundice but not on ad-mission, (2) acute pancreatitis, (3) dilated bile ductù6 mmor bile duct stones seen on ultrasound, and (4) abnormalserum bilirubin or alkaline phosphatase at presentation. IIC
is performed in all patients using 2-h IV infusion of meg-lumine iotroxate (Biliscopin; Schering-UK) followed by ab-dominal radiographs and then ERCP within 24 h of thestudy.
Out of 111 consecutive patients, three (2.7%) had in-complete IIC and eight (7.2%) had unsuccessful ERCP,leaving 100 in the study group. No complication is reportedfor IIC while three develop pancreatitis following ERCP; 81patients had normal studies while 16 patients were detectedfor bile duct stones by both procedures. IIC had two false-negatives and one false-positive for bile duct stones whencompared to ERCP (IIC sensitivity4 89%, specificity499%). Ultrasound was neither sensitive nor specific withfive false-negatives and 24 false-positives.
Reactions to contrast media had been the major resistanceto use of IIC for bile duct evaluation. With the use of newercontrast, in this case meglumine iotroxate, an irresistible alter-native to ERCP is available. The reported complication rate forIIC is 1%, while for ERCP an association of 5% or higher canbe expected with global mortality rate of 0.08%. At Stockport,UK, IIC has 0% morbidity, with an ERCP rate of 3%, whilethe cost of ERCP when compared to IIC is tenfold. The au-thors advocate IIC evaluation preoperatively for patients in ahigh-risk category for bile duct stones followed by ERCP ifnecessary, thus reserving ERCP for a therapeutic rather than adiagnostic role. This is a most welcome contribution for evalu-ation of common bile duct stone in the elective setting and nodoubt will help to popularize IIC use in the future.
Reviewers for this issue: F. Chae, J. Sackier
683

A three-trocar technique for limited laparoscopic renal surgery
G. S. Ferzli, J. B. Hurwitz, H. Usal, A. A. Massaad
Department of Laparoendoscopic Surgery, Staten Island University Hospital, 78 Cromwell Avenue, Staten Island, NY 10304, USA
Received: 29 March 1996/Accepted: 1 July 1996
Abstract. Laparoscopic renal surgery usually involves theuse of five or six trocars. This report concerns the authors’technique for performing such surgery through only threetrocars. Semilateral patient positioning, along with addi-tional table rotation, is utilized to facilitate visceral rotationand optimize exposure of the kidney. Four laparoscopicrenal procedures were performed: one renal cyst decortica-tion and three upper pole partial nephrectomies with ureter-ectomies for duplications of the collecting system. Meanoperative time was 148 min with no conversions; there wereno intra- or postoperative complications. All patients toler-ated a liquid diet on postoperative day 1, and the medianhospital stay was 2 days. In selected cases laparoscopicrenal surgery may be approached safety through three tro-cars.
Key words: Laparoscopy — Renal surgery — Nephroure-terectomy
Since 1990 a number of authors have documented the fea-sibility of a laparoscopic approach to the kidney for thetreatment of a wide variety of urological disorders. All thesestudies, however, utilized five or six trocars. This is a re-view of the authors’ experience with four laparoscopic renalprocedures performed with only 3 ports.
Methods
A Foley catheter and a nasogastric tube are inserted in each case followingthe administration of general anesthesia. The patient is placed in a 45°semilateral right decubitus position and pneumoperitoneum is establishedwith a Veress needle. A 30° angled scope is placed through a 10-mmsupraumbilical trocar. Two additional 5-mm trocars are placed under directvision, one subcostally in the midclavicular line, and the other just abovethe iliac crest in the anterior axillary line (Fig. 1). After a routine explor-atory laparoscopy, the dissection is started by incising the lateral attach-
ments of the left colon along the white line of Toldt from the splenicflexure to the iliac vessels. The splenocolic ligament is divided, and theoperating table is then rotated an additional 30° to place the patient in a 75°lateral decubitis position. This significantly aids in mobilizing the leftcolon medially. Adequate exposure of Gerota’s fascia and the ureter is alsoachieved.
Case reports
Four laparoscopic renal resections were performed at this institution by asingle surgeon (G.S.F.) between June and September 1995. None of thesepatients had undergone prior abdominal surgery. The first patient under-went partial excision of the left renal cyst while the other three patients hadleft upper pole nephroureterectomies.
Case 1
A 40-year-old female presented with recurrent flank and back pain. Pre-operative workup with CT of the abdomen, renal and bladder sonography,and urodynamic studies revealed a left renal midpole inhomogeneous cyst,with evidence of intracystic hemorrhage. Aspiration of the cyst was nega-tive for malignancy. Utilizing the technique described above, the cyst wasaccessed by incising Gerota’s fascia and retracting the perirenal fat. Ultra-sonically activated coagulating shears (LCS, Ultracision Inc., Smithfield,RI) were then used to unroof the cyst circumferentially. The contents wereevacuated without spillage, the septae were divided, and multiple biopsieswere taken. These all proved negative for malignancy. Operative time was120 min, with 300 cc estimated blood loss.
Case 2
A 23-year-old female presented with recurrent urinary tract infections.Intravenous pyelography, voiding cystourethrography, cystoscopy with ret-rograde pyelography, renal sonography, and abdominal CT revealed a du-plex system on the left, with a nonfunctioning upper pole and an ectopicureter. Intraoperatively, once the midureter was exposed, the 5-mm lapa-roscope was repositioned from the supraumbilical to the subcostal trocar.The dilated ureter was divided after its origin from the atrophic upper polehad been verified. The distal end was dissected as far down as possible,ligated with an absorbable Endoloop, and removed. During this dissection,care was taken to avoid injury to the normal ureter. The proximal end of theCorrespondence to:G. S. Ferzli
Surg Endosc (1997) 11: 693–695
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

ureter was passed behind the gonadal and renal vessels cephalad. Thelaparoscope was returned to its supraumbilical position, and 30° of Tren-delenburg were added to patient positioning; this permitted the spleen toretract medially, allowing optimum exposure of the renal hilum and supe-rior pole. The upper pole vessels were ligated and divided between clips,after which the parenchyma was excised with the LCS along the line ofdemarcation. Specimens were retrieved in a bag and removed throughslightly enlarged trocar sites, which were closed in two layers. Operativetime was 173 min, with 200 cc estimated blood loss.
Case 3
Case 3 was an 18-month-old baby girl with recurrent urinary tract infec-tions. Renal sonography, voiding cystourethrography, and nuclear renalscan revealed a left duplex system with a nonfunctioning upper pole and anectopic ureter. The approach was similar to case 2, with an operative timeof 180 min and an estimated blood loss of 10 cc.
Case 4
Case 4 was a 24-month-old baby girl with recurrent urinary tract infections.Renal sonography, voiding cystourethrography, cystoscopy with retrogradepyelography, and nuclear renal scan revealed a left duplex system with anonfunctioning upper pole and an ectopic ureter. Operative technique wasonce again similar to case 2. Operative time and blood loss were 120 minand 10 cc, respectively.
Clinical data from the above cases is summarized in Table 1. There wasno morbidity or mortality. No intraabdominal drains were used. Hospitalstays ranged from 1 to 3 days. Postoperative pain was minimal and patientsrequired analgesics only for the first 24 h. All were given meperidineintramuscularly: 75 mg for the adults (five doses for one patient and six forthe other), and 5 mg once for the pediatric patients. All were started onliquid diet on postoperative day 1 and were tolerating regular diet by theday of discharge. On follow-up ranging from 3 to 6 months, all were doingwell and had normal BUN and creatinine levels, as well as negative urinecultures.
Discussion
There have been many applications of laparoscopy to renalsurgery since 1990 [1, 3, 6, 8, 9], but all laparoscopic trans-peritoneal neurectomy techniques reported to date have re-quired five or six trocars [3, 4, 6]. We have been able toachieve adequate exposure using only three trocars by uti-lizing the semilateral decubitus position described above.The rationale behind using fewer ports is not cosmesis, butrather an interest in reducing early and late complications ofunnecessary incisions; these include vascular and bowel in-juries, as well as trocar-site hernias [2, 5, 7]. In this series offour patients, the average operative time (158 min) andhospital stay (3 days) compared quite favorably with studiesin which five or six trocars were used. The operative timesin those series were 240 and 498 min, and the stays were 6and 5 days, respectively [4, 6]. Rotating the operating table30°, in addition to the initial 45° patient position, allowsgravity to retract abdominal viscera, avoiding the need foradditional trocar retractors. Intestinal manipulation withlaparoscopic instruments is also minimized, which mayeliminate the risk of the iatrogenic enterotomies, which havebeen reported as complications of this procedure [6]. Theuse of an angled scope is a necessity, especially for safedissection and manipulation of the hilar structures. The ex-posure is further improved by placing the laparoscopethrough the supraumbilical port during the nephrectomy andswitching it to the subcostal port during the ureterectomy.
Other authors have used a four-trocar technique in aretroperitoneal approach [7]. While this may avoid the ne-cessity of intraperitoneal adhesiolysis, it does not provideexposure of the lower segment of the ureter. Open retroper-itoneal approaches often utilize two incisions. We feel thatthe transperitoneal technique we have adopted offers thebest blend of flexible exposure of the kidney and the fulllength of the ureter, together with minimal morbidity.
Limited laparoscopic renal surgery via three trocars isfeasible, and is safe in selected cases. The use of fewer portsis a simplification of current approaches; whether or not itoffers significant advantages over more conventional tech-niques remains to be determined.
References
1. Clayman RV, Kavoussi LR, Soper NJ, Dierks SM, Meretyk S, DarcyMD, Roomer FD, Pingleton ED, Thomas PG, Long SR (1991) Lapa-roscopic nephrectomy: initial case report. J Urol 146: 278–282
2. Hanney RM, Alle KM, Cregan PC (1995) Major vascular injury andlaparoscopy. Aust N Z J Surg 65: 533–535
3. Jordan GH, Winslow BH (1993) Laparoendoscopic upper pole partialnephrectomy with ureterectomy. J Urol 150: 940–943
4. McDougall EM, Clayman RV, Elashry O (1995) Laparoscopic nephro-
Table 1.
Case Procedure AgeOperativetime (min)
Bloodloss
1 Unroofing of cyst 40 years 120 3002 Upper pole nephroureterectomy 23 years 173 2003 Upper pole nephroureterectomy 18 months 180 104 Upper pole nephroureterectomy 24 months 120 10
Fig. 1. Positioning of three trocars for renal surgery.
694

ureterectomy for upper tract transitional cell cancer: the WashingtonUniversity experience. J Urol 154: 975–979
5. Patterson M, Walters D, Browder W (1993) Postoperative bowel ob-struction following laparoscopic surgery. Am Surg 59: 656–657
6. Rassweiler JJ, Henkel TO, Potempa DM, Coptcoat M, Alken P (1993)The technique of transperitoneal laparoscopic nephrectomy, adrenalec-tomy, nephroureterectomy. Eur Urol 23: 425–430
7. Rassweiler JJ, Henkel TO, Stoch C, Greschner M, Becker P, Preminger
GM, Schulman CC, Frede T, Alken P (1994) Retroperitoneal laparo-scopic nephrectomy and other procedures in the upper retroperitoneumusing a balloon dissection technique. Eur Urol 25: 229–236
8. Stoller ML, Irby PB III, Carrol PR, Osman M (1992) Laparoscopicrenal cyst resection. J Endourol 6: S56
9. Suzuki K, Ihara H, Kurita Y, Kageyama S, Ueda D, Usiyama T,Ohtawara Y, Kawabe K (1993) Laparoscopic nephrectomy for atrophickidney associated with ectopic ureter in a child. Eur Urol 23: 463–465
695

Letters to the editor
The totally extraperitoneal laparoscopic hernia repair
We read with interest the paper by Vanclooster and col-leagues [11] and commend their contribution to this proce-dure. However, we would offer three comments:
First, totally extraperitoneal laparoscopic hernia repairwas developed by Dulucq [1–3] in 1989/90 and by Mc-Kernan [7] not a great deal later. While it seems legitimatefor others to publish their own technical variations, devel-opments, and outcomes, we strongly support recent remind-ers [6] that journal editors and their peer referees owe thereader a duty of diligence: they should insist that authorsexercise proper scholarship by giving credit where it is due.Otherwise the uninformed reader may assume originalityand the informed may infer plagiarism, where the authorintended neither.
Second, the mesh configuration suggested by Van-clooster et al. was presented by one of us several years ago[4, 10]. However, the concept of amputating the inferior andlateral corner ‘‘so the mesh fits better on the iliac vesselsand the psoas muscle’’ is flawed, since it has subsequentlybeen reported [12] that recurrences may occur dorsal/inferior to this inferolateral corner. The most extensive pos-sible coverage of the psoas muscle belly is therefore appro-priate.
Third, the need for mesh fixation remains debatable.However, to fix the cranial border to ‘‘prevent early migra-tion or slipping’’ is illogical: In our joint experience of over1,000 cases and, to our knowledge in all reports in the worldliterature, recurrences pass uniformly caudal to the inferiorborder of the prosthesis. Fixation of the inferior medial partof the mesh to Astley Cooper’s ligament alone [5] may notoffend against the original tension-free notion of Stoppa [8,9] nor interfere with the mechanics of prosthesis retention.To fix the superior border to points that move relative to oneanother within a musculofascial structure contravenes bothprinciples.
Finally, on a minor point, if the structure annotated as‘‘D’’ in Fig. 1 is the testicular vascular bundle, where is thevas deferens?
Despite these comments we congratulate the authors ontheir low complication rate.
References
1. Dulucq J-L (1991) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneale en retrope´ritoneoscopie. CahChir 79: 15–16
2. Dulucq J-L (1992) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneal en pre´-peritoneoscopie. Chirur-gie 118(1–2): 83–85
3. Dulucq J-L (1992) The treatment of inguinal hernias by implantationof mesh through retroperitoneoscopy. Postgrad Gen Surg 4: 173–174
4. Fiennes AGTW, Taylor RS (1994) Learning laparoscopic hernia re-pair. In: Inguinal hernia, advances or controversies? Arregui M, NaganR (eds) Radcliffe, Oxford, pp 475–482
5. Fiennes AGTW, Himpens J, Dulucq J-L (1994) Preperitoneoscopicgroin hernioplasty, current synthesis. Surg Endosc 8(8): 989
6. Horton R, Smith R (1996) Time to redefine authorship (editorial). BrMed J 312: 723
7. McKernan JB (1993) Laparoscopic extraperitoneal repair of inguino-femoral herniation. Endosc Surg Allied Tech 1(4): 198–203
8. Stoppa R, Petit J, Abourachid H (1973) Proce´deoriginal de plastie deshernies de l’aine. L’interposition sans fixation d’une prothe`se en tullede Dacron par voie me´diane pre´peritoneale. Chirurgie 99: 119
9. Stoppa RE, Rives JL, Warlaumont CR (1984) The use of Dacron in therepair of hernias of the groin. Surg Clin North Am 64: 269–285
10. Taylor RS, Fiennes AGTW (1992) A tension free modification of theDulucq preperitoneal laparoscopic hernioplasty. Min Inv Ther 1(Suppl1): 101
11. Vanclooster P, Meersmann AL, de Gheldere CA, Van de Ven CK(1996) The totally extraperitoneal laparoscopic hernia repair. SurgEndosc 10: 332–335
12. Vivekanadan S, Fiennes AGTW (1995) Totally extraperitoneal groinhernioplasty: mechanism of delayed indirect recurrence. Min Inv Ther4(Suppl 1): 55
A. Fiennes
Department of SurgerySt George’s Hospital Medical SchoolCranmer TerraceLondon, SW17 ORE, United Kingdom
J. Himpens
Department of Digestive SurgeryUniversity Hospital Ste PierreRue Haute 201B-1000 Brussels, Belgium
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 696

The author replies
We thank you for the opportunity to answer the letter of Mr.Fiennes. First of all, we certainly do acknowledge that Mr.Dulucq and Mr. Mc Kernan were the pioneers of the extra-peritoneal laparoscopic hernia repair. Honor to whom honoris due. We did not intend to pretend to be the pioneers ofthis technique. We wished only to describe the technique theway we perform it, to describe our own findings, and to givea fair report of our preliminary results.
The reason for cutting the inferolateral corner is not justthat we think it fits better on the iliopsoas but also becausewe are afraid to cause damage to the nerves running on it bydissecting unnecessarily high on the muscle. Since the meshmeasures 15 × 15 cm, we do not think we compromise thestrength of the repair by merely removing a small piece ofits inferolateral corner. We think that dissecting very highon the muscle just to position the whole inferolateral cornerof the mesh flat on the muscle is unnecessary and danger-ous.
We do agree totally that fixation of the mesh is unnec-
essary provided the mesh is large enough, which is obvi-ously the case when using a 15 × 15 cm mesh. In fact, wehave not fixed the mesh since January 1996.
We also agree that the vas deferens is not clearly seen onFig. 1. We chose this shot because of the clearly visiblelarge direct defect.
C. de Gheldere
Heilig Hart ZiekenhuisKolveniersvest 20B-2500 LIERBelgium
P. Vanclooster
Bouwelsesteenweg 62560 NijlenBelgium
Surg Endosc (1997) 11: 697
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The influence of pneumoperitoneum on the peritoneal implantation offree intraperitoneal cancer cells
Recently Hubens et al. published an interesting article en-titled ‘‘The influence of a pneumoperitoneum on the peri-toneal implantation of free intraperitoneal colon cancercells’’ [2]. They reported on the possible implantation ofcancer cells at trocar wounds at the moment of deflation ascells are forced through these wounds by the pressure gra-dient created by the pneumoperitoneum during laparoscopicsurgery for malignant disease. We would like to point outthat this ‘‘chimney effect,’’ as originally described by us,can occur during the entire laparoscopic procedure and notonly at the moment of deflation, as leakage of CO2 along-side trocars during surgery is impossible to prevent with theexisting trocars [3]. Consequently, deflation of the pneumo-peritoneum by letting CO2 escape through one of the trocarsbefore pulling these trocars out of the abdomen will notprevent the occurrence of entrapment of cancer cells in thetrocar wounds.
We fully agree with the authors on the possible advantageof gasless laparoscopy as this could prevent the ‘‘chimneyeffect.’’ In our experimental work we found significantly lesstumor growth at the port sites following gasless laparoscopicsurgery for colon cancer in the rat as compared to laparoscopicsurgery using a CO2 pneumoperitoneum. This techniqueseems promising to treat malignant disease laparoscopically.
References
1. Bouvy ND, Marquet RL, Jeekel J, Bonjer HJ (1996) Impact of gas (less)laparoscopy and laparotomy on peritoneal tumor growth and abdominalwall metastases. Surg Endosc 10: 551
2. Hubens G, Pauwels M, Hubens A, Vermeulen P, Van Marck E, EyskensE (1996) The influence of a pneumoperitoneum on the peritoneal im-plantation of free intraperitoneal colon cancer cells. Surg Endosc 10:809–812
3. Kazemier G, Bonjer HJ, Berends FJ, Lange JF (1995) Port site metas-tases after laparoscopic colorectal surgery for cure of malignancy. Br JSurg 82: 1141–1142
G. Kazemier1
F. J. Berends1
N. D. Bouvy1
J. F. Lange2
H. J. Bonjer1
1 Department of SurgeryUniversity Hospital Rotterdam-DijkzigtDr Molewaterplein 403015 GD, RotterdamThe Netherlands2 Department of SurgerySt. Clara HospitalRotterdamThe NetherlandsCorrespondence to:G. Kazemier
Surg Endosc (1997) 11: 698
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The author replies
We thank Dr. Kazemier et al. for their kind remarks and fullyagree with them that gas leakage can occur during the entireprocedure with subsequent implantation of tumor cells at thetrocar sites. At the moment we are conducting further experi-mental studies on the possible effects of gas leakage on tumorcell implantation and the ‘‘chimney effect,’’ as they havecalled it. Results will be ready for publication soon.
G. Hubens
Department of SurgeryUniversity HospitalUniversity of AntwerpWilrijkstraat 102650 EdegemBelgium
Surg Endosc (1997) 11: 699
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

Technique
Laparoscopic-assisted abdominoperineal resection in the prone position
An alternative technique
K. Koerner, S. Datena, L. Erwin
Emanuel Hospital, 2801 N. Gantenbein Avenue, Portland, OR 97227, USA
Received: 23 October 1995/Accepted: 5 August 1996
Abstract. With the introduction of laparoscopic-assistedabdominoperineal resection (LAPR), the traditional Lloyd-Davies position with the Mayo two-team combined ap-proach is being adapted. The Lloyd-Davies position allowstwo teams of surgeons to work simultaneously, minimizingoperating time. The conditions required for laparoscopy re-strict a simultaneous procedure. Since LAPR is typicallyperformed as a two-stage procedure, we introduce an alter-native position which facilitates the perineal dissection. Wereview the results and technique of LAPR in the proneposition in three patients who were suitable candidates forthis procedure. Three patients underwent LAPR. No opera-tive or postoperative complications were encountered andthe procedures were in keeping with oncologic principles ofresection. Total anesthesia times were less than 3.5 h forthese initial patients. No hemodynamic problems were en-countered due to the choice of patient positioning. Theprone jackknife position greatly increases visualization ofdeep structures, reduces blood loss, enhances dissection,and reduces the technical demands of the laparoscopic por-tion of the procedure.
Key words: Laparoscopic abdominoperineal resection —Prone jackknife position — Alternative technique
Goals of minimally invasive surgery include reducing op-erative time and minimizing the technical demands madeupon the surgeon. In performing traditional abdominoperi-neal resection (APR) with the patient in perineolithotomyposition, the majority of difficult dissection occurs throughthe abdomen for access to the lateral pedicles along therectal wall. Identification of the ureters, especially the left,deep in the pelvis, can also be problematic. Sackier [11]reported a technique for laparoscopic APR (LAPR) in 1992
for a patient with benign disease. LAPR in keeping withoncologic surgical principles was addressed by Descanini etal. [3]. They performed LAPR on a series of 11 fresh ca-davers and subsequently performed autopsies to determinethe extent of the resection. They found that their recom-mended technique of LAPR with proximal ligation of theinferior mesenteric artery, wide clearance of pelvic sidewalls, and complete removal of the mesorectum could beperformed for oncologic procedures. In each of the abovecases, the patients have been positioned in either the peri-neolithotomy position or position was not discussed.
The Lloyd-Davies position was originally recommendedbased on the two-team approach with one team conductingthe abdominal resection while the other carried out the per-ineal dissection. With the introduction of LAPR this ap-proach is being reconsidered. The O.R. conditions requiredfor laparoscopy restrict a simultaneous direct procedure. Inour experience, LAPR is more readily conducted as a two-stage procedure. We therefore suggest an alternative posi-tion for the perineal dissection in order to facilitate dissec-tion. We have found that the prone jackknife positiongreatly increases visualization of deep structures, reducesblood loss, and enhances dissection.
Case reports
Patient 1 is a 40-year-old black male with a 1-year history of increasingrectal bleeding, pain, and decreasing caliber of stool. Digital exam revealeda mass 2.5 cm from the anal verge. Rigid sigmoidoscopy performed to 20cm revealed similar findings with approximately two-thirds obstruction ofthe lumen. Biopsy confirmed moderately differentiated adenocarcinoma.CT of the abdomen and pelvis visualized a mass lesion within the rectumwithout evidence of perirectal invasion, extension, pelvic adenopathy, ormetastases. The patient underwent LAPR with estimated blood loss lessthan 75 cc. O.R. time was 205 min. G.I. continuity returned on the 4thpostoperative day. His recovery has been uneventful.
Patient 2 is a 42-year-old black male who had a mass 1.5 cm above thedentate line. Rigid sigmoidoscopy performed to 20 cm revealed similarfindings. CT revealed no evidence of perirectal invasion, extension, pelvicadenopathy, or metastases. He underwent LAPR with estimated blood lossof 50 cc. The specimen contained 12 nodes none of which were positive.Correspondence to:S. Datena
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 684–686

O.R. time was 195 min. G.I. function returned on postoperative day 3. Hisrecovery has been uneventful.
Patient 3 is a 58-year-old white male who had a fixed mass 2 cm abovethe dentate line. This patient received preoperative irradiation with a re-duction in the size of the mass. LAPR was performed with a total estimatedblood loss of 50 cc. No positive nodes were found in the specimen. Thepatient was discharged home on postoperative day 3. He received postopchemotherapy and irradiation. At 6 months out there was no evidence ofrecurrence.
Technique
The patient is initially placed in the prone position with aslight degree of jackknife and with the head down to opti-mize hemodynamics. The perineum is incised and dissec-tion commences. Using gentle traction the rectum can bemanipulated easily to facilitate dissection. Significant ves-sels are identified and ligated under direct vision. There isless tissue staining with blood as compared to lithotomyposition, which facilitates more careful dissection. Withgentle traction on the rectum, the difficult plane between theprostate and anterior rectum can be carefully dissected.Downward traction facilitates an excellent view of the planeof dissection outside the presacral fascia, thereby avoidingthe presacral venous plexus. The dissection is carried out upto and slightly beyond the peritoneal reflection. With thespecimen freed to this level, it is then placed into a thickspecimen bag and tied with umbilical tape, which is suturedinto place to prevent slipping. The bag and its contents arethen tucked up into the pelvis. A single drain can be placedinto the pelvis and brought out through a separate stab in-cision. The perineum is closed in layers and dressed. Thepatient is then turned to the supine position for the laparo-scopic portion of the procedure.
Since the majority of the difficult dissection has alreadybeen performed, a minimum of access ports will be re-quired. We used gasless laparoscopic technique. Our stan-dard approach for all colon resections is to use a maximumof four ports. A 12-mm port is placed at the umbilicus,followed by a second 12-mm port through the previouslymarked colostomy site. Two 5-mm ports or one 5-mm andone 10-mm port are placed on the right side of the abdomenfor dissection and traction on the colon. This minimumnumber of ports reduces the morbidity for the patient post-operatively. Placing the largest port through the plannedostomy site is also common practice to reduce morbidity.By using two 12-mm ports the operator has the option to usestapling devices through one of two ports should one pro-vide a more advantageous angle of attack over the other. Ifit has not already been done, the peritoneal reflection isincised and the mesentery of the rectosigmoid is takendown. The inferior mesenteric artery is ligated high, leavinga 15–20-mm stump. Although this has not been shown toimprove survival in patients with nodal involvement [11], itdoes aid removal of the rectosigmoid lymphatic drainage forlymph node sampling [3]. The inferior mesenteric vein isalso ligated. The pelvis is reperitonealized using hernia sta-plers. Vicryl mesh screen can also be placed in the pelviswith the hernia stapler if the patient is to receive postopera-tive irradiation.
A pretied Roeder loop is passed around a small corner ofthe distal end of the sigmoid colon. This is brought up to theplanned ostomy site. The umbilical tape attached to the
specimen bag is then brought out through the ostomy siteport. The abdomen is then fully examined for hemostasisbefore preparing the colostomy site. The bagged specimenis then delivered through the ostomy site and sent immedi-ately to pathology to determine whether an adequate mes-enteric specimen has been obtained. The colonic segmentfor the ostomy is brought up with the aid of the pretiedRoeder loop. The abdomen is then reexamined in order toverify the colon has not been torqued in any manner prior tomaturing the colostomy. The colostomy is then matured. Allports are removed and wounds closed.
Discussion
The significantly improved visualization obtained in theprone jackknife position appears to contribute to decreasedblood loss. Total blood loss in each of our cases was 75 ccor less (excluding blood contained within the specimen).This reduction in operative blood loss over conventionaltechnique offers an advantage to patients with rectal cancer.Postoperative infection rates have been shown to be in-creased in colorectal cancer patients who have receivedblood transfusions [4]. Additionally, continued debate oc-curs as to the relationship of blood transfusion to colorectalcancer recurrence [1, 10, 12, 13, 14]. Currently, it appears thata noncausal relationship exists. In any event, most wouldagree that limiting operative blood loss is preferred. Hatadaet al. [7] examined hemodynamics in the prone jackknifeposition in 19 patients and found no significant adverseeffect. In addition, they report an approximate 50% decreasein mean blood loss over lithotomy position based on theirprevious work.
We elected to begin with the perineal portion of theprocedure. Corman recommends that the abdominal portionshould be performed initially [2]. The principles behindinitially performing the abdominal portion center aroundminimizing morbidity and ease of dissection. Of primaryconcern is the need to perform adequate resection. Our pre-operative evaluation in each patient established that the tu-mor was of suitable size, location, and mobility to allow forreverse order. Appropriate workup and clinical judgmentwill determine which patients are suitable for this technique.We believe this sequence permits ease of dissection. Totaloperating time was less than 3.5 h in each case.
The procedure can just as easily be performed, withslight modification, by completing the laparoscopic portioninitially. The laparoscopic portion would then be carried outusing techniques such as that described by Descanini [3].The abdominal specimen is then placed in a specimen bagand buried in the pelvic cavity in the classic Miles method.The patient would then be turned to the prone jackknifeposition for the remainder of the procedure.
Laparoscopic APR can be performed in keeping withoncologic principles [3]. Our specimens had clear marginsand all had negative lymph nodes with adequate sampling.Abdominal wall recurrence at a trocar site has been reported[5, 8]. In one case, the trocar site where the recurrenceoccurred was used only for dissection and did not come incontact with the specimen. In a review by Hughes et al.,tumor recurrence in abdominal wall scar tissue followingopen large-bowel cancer surgery was examined [8]. They
685

suggested that while involvement of the scar tissue wasuncommon, in those cases where it did occur it was morelikely to be a manifestation of incurable systemic malignantdisease as opposed to an isolated occurrence. Regardless ofthe technique, the prognosis appears poor if abdominal scarrecurrence is found [8]. To date, no definitive rate of ab-dominal wall recurrence following laparoscopic large-bowel cancer surgery has been established. Nduka et al. in1994 were able to identify 18 reported cases of cannula-siterecurrence following laparoscopic oncologic procedures[9]. All of these cases involved adenocarcinoma. If uponfurther review the recurrence rate is significantly higherwith laparoscopy, then its use will need to be modified orcurtailed as indicated. With appropriate postoperative fol-low-up these rare recurrences should be identified andtreated.
Geis et al. [6] considered LAPR to be a moderatelydifficult procedure according to their scale, in part becauseof the necessity to mobilize deep in the pelvis. Performingthe majority of the difficult dissection with the patient in theprone position decreases the technical proficiency requiredto complete the laparoscopic portion of the surgery. A sur-geon with moderate experience in advanced laparoscopictechnique should be able to easily perform LAPR with thismethod.
Conclusion
Laparoscopic-assisted abdominoperineal resection is be-coming a common technique in the treatment of benign andmalignant tumors. While LAPR is not appropriate in allcases, preoperative evaluation and clinical judgment willdetermine which procedure should be attempted. Physicalexamination, endoscopy, biopsy, CT, and transrectal ultra-sound can be used in evaluating the patient and planning theappropriate procedure. Our experience has found that blood
loss is considerably decreased and dissection is greatly fa-cilitated by performing the perineal portion of LAPR withthe patient in the prone jackknife position.
References
1. Busch ORC, Hop WCJ, Marquet RL, Jeekel J (1994) Blood transfu-sions and local tumor recurrence in colorectal cancer: evidence of anoncausal relationship. Ann Surg 220: 791–797
2. Corman M (1993) Colon and rectal surgery. 3rd ed. J. B. Lippincott,Philadelphia
3. Descanini WITH, Milsom JW, Bo¨hm B, Fazio VW (1994) Laparo-scopic oncologic abdominoperineal resection. Dis Colon Rectum 37:552–558
4. Ford CD, VanMoorleghem G, Menlove RL (1993) Blood transfusionsand postoperative wound infection. Surgery 113: 603–607
5. Fusco MA, Paluzzi MW (1993) Abdominal wall recurrence after lap-aroscopic-assisted colectomy for adenocarcinoma of the colon: reportof a case. Dis Colon Rectum 36: 858–861
6. Geis WP, Colletta AV, Verdeja JC, Plasencia G, Ojogho O, Jacobs M(1994) Sequential psychomotor skills development in laparoscopic co-lon surgery. Arch Surg 129: 206–212
7. Hatada T, Kusunoki M, Sakiyama T, Sakanoue Y, Yamamura T, Oku-tani R, Kono K, Ishida H, Utsunomiya J (1991) Hemodynamics in theprone jackknife position during surgery. Am J Surg 162: 55–58
8. Hughes ESR, McDermott FT, Polglase AL, Johnson WR (1983) Tu-mor recurrence in the abdominal wall scar tissue after large-bowelcancer surgery. Dis Colon Rectum 26: 571–572
9. Nduka CC, Monson JRT, Menzies-Gow N, Darzi A (1994) Abdominalwall metastases following laparoscopy. Br J Surg 81: 648–652
10. Rehman SU (1993) Laparoscopic abdominoperineal resection of therectum [letter; comment]. Br J Surg 80: 1080
11. Sackier JM, Berci G, Hiatt JR, Hartunian S (1992) Laparoscopic ab-dominoperineal resection of the rectum. Br J Surg 79: 1207–1208
12. Sibbering DM, Locker AP, Hardcastle JD, Chir M, Armitage NC(1994) Blood transfusion and survival in colorectal cancer. Dis ColonRectum 37: 358–363
13. Tang R, Wang JY, Chien CRC, Chen JS, Lin SE, Fan HA (1993) Theassociation between perioperative blood transfusion and survival ofpatients with colorectal cancer. Cancer 72: 341–348
14. Tartter PI (1992) The association of perioperative blood transfusionwith colorectal cancer recurrence. Ann Surg 216: 633–638
686

Laparoscopic cholecystectomy in the elderly
F. M. Tagle,1 J. Lavergne,1 J. S. Barkin,1 S. W. Unger2
1 Division of Gastroenterology, Mt. Sinai Medical Center, University of Miami, School of Medicine, 4300 Alton Road, Miami Beach, FL 33140, USA2 Department of Surgery, Mt. Sinai Medical Center, University of Miami, School of Medicine, 4300 Alton Road, Miami Beach, FL 33140, USA
Received: 17 September 1996/Accepted: 14 October 1996
AbstractBackground:Advanced age with its concomitant comorbidconditions may be associated with increased postoperativelaparoscsopic cholecystectomy (LC) complications andmore frequent conversion to open cholecystectomy (OC).The purpose of this study was to evaluate the outcome ofLC in patients age 65 and older.Methods:Ninety consecutive patients were studied age 65and older, of whom 39 (43%) were males and 51 (57%)were females, mean age 74 years (range 65–98), with 20patients (22%)ù 80. Indications for surgery included bili-ary colic 55 (61%), acute cholecystitis 22 (24%), pancreati-tis 10 (11%), and cholangitis 3 (4%). Seventeen patients(19%) had preoperative ERCP, 12 of which were normal;five had sphincterotomy with stone extraction. Comorbidconditions included hypertension (44%), CAD (17%), car-diac arrhythmias (18), CHF (9%), and COPD (7%).Results:Operative time—mean 1 h 51 min ± SD 43min.Conversion to OC—three patients (3%). Length of stay—mean 5 days (range 1–26). Mortality—two patients (2%)>80 years old, one patient with septicemia and multiorganfailure whose comorbid diseases included CAD, C.F.,COPPED, and elevated BP, one patient with MI postsur-gery, morbid diseases included DM and CAD. Complica-tions—five patients (5%): bile leak from cystic duct stump(one), postsurgery MI (two), incarcerated incisional hernia(one), septicemia (one).Conclusion:Morbidity rates for LC in the elderly popula-tion are not different from that reported for patients less than65 years of age. (5% vs 6%, Fried et al.,Surg Clin North Am1994;74 [2]: 375–387). Our 2% mortality rate is statisticallydifferent from previously reported in a series of patients ofall ages (0.6%, Fried et al.). The 3% rate of conversion toOC in this older population is not significantly differentfrom the patients in Fried et al. series (4%).
Key words: Elderly — Conversion — Comorbid condition
Laparoscopic cholecystectomy (LC) is currently the proce-dure of choice for managing gallstone disease [2, 3]. Over-all, its mortality rate is the same as that for open cholecys-tectomy but its morbidity is less [2, 3, 4, 6]. Advanced agewith its concomitant comorbid conditions has been felt to beassociated with increased postoperative complications [6],as well as more frequent conversion to open cholecystecto-my (OC). With the increasing mean age of our population,it is important to know the morbidity and mortality of pa-tients >65 years of age who undergo LC. Therefore, thepurpose of this study was to evaluate the outcome of LC inpatients age 65 and older.
Patients and methods
We conducted a retrospective study evaluating the medical records of 90consecutive patients age 65 or older who underwent LC from January 1990to June 1994 at Mount Sinai Medical Center, Miami, FL. This represents24% of the total number of patients who had LC during that period. Thefollowing parameters were evaluated: age, sex, indication for surgery, co-morbid disease states, operative time, conversion to OC, complications,performance of ERCP, length of hospital stay, and mortality.
Results
Ninety patients with a mean age of 74.3 ± 7 years (range 65to 98 years) were evaluated. Twenty (22%) patients wereage 80 or older. Thirty-nine (43%) were males and 51 (57%)were females. The indications for surgery included biliarycolic in 55 (61%) patients, acute cholecystitis in 22 (24%),acute pancreatitis in ten (11%), and cholangitis in three(4%).
Comorbid conditions included hypertension in 40 of 90patients (44%), coronary artery disease in 15 of 90 (17%),cardiac arrhythmias in 14 of 90 (18%), congestive heartfailure in eight of 90 (9%), and COPD in six of 90 (7%).Two patients had cirrhosis incidentally discovered intraop-eratively and one patient had a cerebral meningioma (Table1). The mean duration of surgery was 111 min ± 43 min(range 50 to 255 min).
Conversion to OC was required in three of 90 patientsCorrespondence to:J. S. Barkin
Surg Endosc (1997) 11: 636–638
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

(3%) due to their distorted anatomy. Postoperative compli-cations occurred in five patients (Table 2). Two of the fivecomplications were related directly to the surgical proce-dure itself, including one patient with a postoperative cysticduct leak which was treated successfully with an ERCP andsphincterotomy on postoperative day 2. One patient had anincarcerated umbilical hernia at the incision site requiringdecompressive surgery. Medical complications that werenot directly related to the procedure itself included two pa-tients with postoperative myocardial infarction (MI).
The mean postoperative hospital stay was 3 days (range1–26). Mortality occurred in two of 90 patients (2%), bothof whom were older than 80 years (Table 3). One patienthad a postoperative MI complicated by fatal arrhythmias.The second patient with comorbid diseases of congestiveheart failure and COPD was admitted with cholangitis anddied of sepsis and multiorgan failure on postoperative day21.
ERCP was performed preoperatively in 17 patients; 12had normal studies and five had common bile duct stonesthat required sphincterotomy and stone extraction. Threepatients had postoperative ERCP, two of them for suspectedretained common bile duct stones (normal studies) and onefor the treatment of a bile leak from the cystic duct stump.
Discussion
The incidence of complications with OC increases with age[2]. The reported complication rates in patients >65 yearsundergoing open cholecystectomy range between 20% and30% [4, 6]. Currently, LC has replaced open cholecystec-tomy as the preferred approach for the treatment of symp-tomatic cholelithiasis due to its lower morbidity, shorterlength of hospital stay, and lower cost compared to opencholecystectomy [12]. However, the morbidity and mortal-ity of patients >65 years of age who undergo LC have beenonly scantly reported.
The majority of our patients underwent LC for symp-toms of biliary colic (55%). This is similar to that reportedby Fried et al. [2], who also found a higher incidence ofacute cholecystitis and pancreatitis in older patients as anindication for surgery compared to those patients below age65. Patients >65 years would be expected to have an in-creased incidence of comorbidity. We found the expectedhigh incidence, with approximately half of our patients hav-ing CAD, 20% with cardiac arrhythmias and 10% withCHF. The comorbid conditions that were present in ourstudy population are comparable to those reported by otherauthors evaluating LC in the elderly [7, 11, 12] in whichhypertension and CAD are the most commonly encounteredcomorbid disease. We found a 24% incidence of acute cho-lecystitis, and 11% of our patients had acute pancreatitis.This falls between the reported range in patients > age 65who have rates of 8% to 32% of acute cholecystitis inci-dence and is also in accordance with Fried, who had 22%for acute cholecystitis and 11% for acute pancreatitis.
Our mean operative time of 111 min falls within therange reported in a large compilation of series by Godacz ofbetween 54 and 138 min. It is difficult to compare theincidence of postoperative complications between seriesdue to the lack of standardization of reporting as well as theretrospective nature of our study. Nevertheless, our 5%complication rate in patients >65 years is comparable to the5% to 10% published in other series [2, 12]. Other seriesreported an overall complication rate of 24% in patients >65years old undergoing LC [8]. However, 9% were directlyrelated to the surgical procedure itself, including biliarytract injury, wound infection, operative bleeding, and post-procedure cholangitis. We found no wound infections in ourseries. Fried et al. [2] found that wound complications werethe most common problem overall and were found morefrequently in the elderly (1.3%) than in younger patients.
The reported incidence of biliary tract injury rangesfrom 0.3 to 1% [3, 5, 8, 10]. LC is associated with a two- totenfold increase in bile duct injury when compared withconventional cholecystectomy, probably because of inad-equate dissection, inherent limitations to the technique, and/or the learning curve associated with a new technology [1].None of our patients had bile duct or vessel injuries; how-ever, the surgeon was highly experienced. Only one of ourpatients had a postoperative bile leak from the cystic ductstump requiring ERCP with sphincterotomy and stent place-ment.
ERCP was performed prior to surgery in 17 of our pa-tients with clinical and biochemical suspicion of choledo-cholithiasis, only five of whom had CBD stones that wereextracted endoscopically. The issue of ERCP and its timingrelated to LC have been a subject of intense debate in thepast few years. Only 5% of patients considered low risk forcommon bile duct stones actually have stones on intraop-erative cholangiogram [9]. Our data agrees that pre-LC
Table 1. Comorbid diseases
No. patients65–79 years
No. patientsù 80 years
Total no. patients(N 4 90)
Hypertension 31 9 40 (44%)Coronary artery disease 14 1 15 (17%)Cardiac arrhythmias 8 6 14 (18%)Congestive heart failure 3 5 8 (9%)COPD 4 2 6 (7%)Cirrhosis 2 — 2 (2%)Cerebral meningioma 1 — 1 (1%)Diabetes 3 4 7 (8%)
Table 2. Postoperative complications of laparoscopic cholecystectomy
No. patients
Directly related to the surgical procedureBile leak 1Incisional hernias 1
MedicalMyocardial infarction 2Sepsis 1
Table 3. Mortality in patients undergoing LC divided by age groups
65–79years old
ù 80years old
No. patients (%) 70 (78) 20 (22)No. deaths (%) 0 (0) 2 (10)
637

ERCP should be reserved only for patients with signs andsymptoms suggestive of common bile duct pathology.
Conversion to OC was performed in 3% of our patients.This rate is lower than in previously reported series [2, 3,10, 12]. Fried et al. [2] found a global conversion rate of5.4% and, interestingly, reported that the frequency of con-version to OC was significantly higher in the patients olderthan age 65 (10.4% vs 4.1%). They felt that this reflectedthe increased likelihood of complicated gallstone disease,difficulty in resolving the anatomy in older patients, andincreased frequency of adhesions. Our lower rate probablyreflects the experience and technical expertise of our surgi-cal colleagues.
The overall mortality rates after LC regardless of agerange from zero to 0.9% in U.S. series [2, 3] and from 0.1to 0.2% in European series [10]. In Fried series [2], the twodeaths occurred in patients age 65 and older but less thanage 80. Two deaths of our 90 patients occurred in the pa-tients older than age 80, both of whom had severe comorbiddisease. Our overall mortality of 3% is statistically higherthan previously reported, which seems to be due to theinclusion of patients >80 years who had extensive comorbiddisease. Interestingly, though, our subgroup of patients ages65–79 had significant comorbidity as well (Table 2) andtheir mortality was 0%. Conversely, considering only the 20patients age 80 and older, the mortality in that group is 10%(Table 3). Our data suggest that patients >80 years whohave multiple comorbid conditions have a worse prognosisthan those below 80 years.
In conclusion, age up to 80 years, even in patients withextensive comorbid disease, does not seem to be a poor
prognostic factor. These patients should not be excludedfrom surgical intervention. However, >80 years with exten-sive comorbid disease seems to be a negative prognosticfactor in patients undergoing LC.
References
1. Davidoff AM, Pappas TN, Murray EA, Hilleren DJ, Johnson RD,Baker ME, Newman GE, Cotton PB, Meyers WC (1992) Mechanismsof major biliary injury during laparoscopic cholecystectomy. Ann Surg215: 196–202
2. Fried GM, Clas D, Meakins JL (1994) Minimally invasive surgery inthe elderly patient. Surg Clin North Am 74(2): 375–386
3. Gadacz TR (1990) US experience with laparoscopic cholecystectomy.Am J Surg 165: 450–454
4. Ibach JR Jr, Hyme HA, Erb WH (1968) Cholecystectomy in the aged.Surg Gynecol Obstet 126: 523–528
5. Kozarek RA, Gannan R, Baerg R, Wagonfeld J, Ball T (1992) Bileleak after laparoscopic cholecystectomy. Diagnostic and therapeuticapplications of ERCP. Arch Int Med 152: 1040–1042
6. Margiotta SJ, Horvitz JR, Willis IH, Wallack MK (1988) Cholecys-tectomy in the elderly. Am J Surg 156: 509–512
7. Massie MT, Massie LB, Marrangoni AG, D’Amico FJ, Sell HW(1993) Advantages of LC in the elderly and in patients with high ASAclassifications. J Laparoendosc Surg 3(5): 467–475
8. Nennex RP, Impenato PJ, Alcorn CM (1993) Complications of LC ina geriatric population group. NY State J Med 92(12): 518–520
9. Neoptolemos JP, Shaw DS, Carr-Locke DL (1989) A multi variateanalysis of preoperative risk factors in patients with common bile ductstones: implications for treatment. Ann Surg 209: 157–161
10. Perissat K (1993) Laparoscopic cholecystectomy. The European ex-perience. Am J Surg 165: 444–449
11. Saxe A, Lavson J, Phillips E (1993) Laparoscopic cholecystectomy inpatients aged 65 or older. J Laparoendosc Surg 3(3): 215–219
12. The Southern Surgeons Club (1991) A prospective analysis of 1518laparoscopic cholecystectomies. N Engl J Med 324: 1073–1078
638

Palliative gastrojejunostomy
A minimally invasive approach
R. S. Chung,1 P. Li2
1 Department of Surgery, Meridia Huron Hospital, 13951 Terrace Road, Cleveland OH 44112, USA2 Hillcrest Hospital, 6780 Mayfield Road, Mayfield Heights, OH 44124, USA
Received: 28 June 1996/Accepted: 26 July 1996
Abstract. Palliative bypass for neoplastic gastric outlet ob-struction should be minimally invasive. We designed a lapa-roscopically assisted approach that appears to meet theneed. The proximal jejunum is exteriorized by laparoscopyvia an epigastric trocar-site incision. An EEA anvil is in-stalled in the exteriorized jejunum, which is returned to theabdomen. Through this mini-incision, the anterior wall ofthe stomach is opened for insertion of the EEA stapler,which penetrates the posterior gastric wall. When snappedto the anvil and fired, an antecolic gastrojejunostomy iscreated. No mortality or anastomotic leak occurred in twocases. The operation and recovery appeared to be faster thanhistoric controls. This operation is minimally invasive andexpeditious, ideal for patients requiring palliative bypass.
Key words: Minimally invasive — Palliative gastrojejunos-tomy — Gastric outlet obstruction
Palliative bypass for inoperable malignant gastric outlet ob-struction should be expeditious and minimally invasive, inview of limited life expectancy. The following technique,using a mini-incision, was first conceived for a patient whodeveloped gastric outlet obstruction 2 years after a pylorus-sparing Whipple procedure.
Surgical technique
Under general anesthesia, laparoscopy is first performed through a subum-bilical port. A 10-mm port is inserted at the epigastrium and a laparoscopicbowel clamp is used to secure the proximal jejunum loop suitable for theanastomosis. By cutting down on the cannula (Fig. 1), this port site isconverted into a 4-cm incision through which the jejunum is exteriorized.The anvil of a 30-mm EEA stapler (U.S. Surgical) is inserted into thebowel and secured by a pursestring suture (Fig. 2A). A strong suture
(‘‘retrieval loop’’) is threaded into the hole in the shaft of the anvil (Fig.2A), which, together with the jejunum, is returned into the abdomen, leav-ing only the retrieval loop on the exterior (Fig. 2B). This allows a clearexposure of the gastric antrum.
Between stay sutures, the anterior gastric wall is opened with a smallincision for introduction of the EEA stapler (Fig. 3A), the sharp tip ofwhich penetrates the posterior wall. The stomach in this location has beencleared of the omentum and gastroepiploic arcade for a short distance toaccommodate the jejunum. Aided by the retrieval loop, the anvil is hand-guided and snapped to the stapler. The correct approximation of the stom-ach and jejunum is checked visually (Fig. 3B). Firing of the stapler effectsan antecolic, retrogastric gastrojejunostomy. The anastomosis is inspected
Correspondence to:S. Chung
Fig. 1. Locations of the ports used; conversion of the epigastric port siteinto a 4-cm incision. Note that the incision may be horizontal, vertical, oroblique depending on anatomical factors such as adhesions, size of stom-ach, etc.
Surg Endosc (1997) 11: 676–678
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

internally for hemostasis, and the potency of the efferent and afferent limbsis verified by digital exploration. The gastrostomy is then closed withconventional suturing. A final laparoscopic view of the completed opera-tion is obtained by reinflation of the abdomen after wound closure.
Case report
A 62-year-old black female presented with postcibal epigastric fullness,vomiting and weight loss of 1 month duration. Two years prior to presen-
tation, she was treated for a well-differentiated pancreatic carcinoma,staged pathologically T2N1M0, by a pylorus-sparing Whipple operation,followed by chemotherapy and irradiation. She had remained well until theonset of current symptoms. Physical examination showed emaciation,moderate amount of ascites, a palpable liver, and a positive successionsign. CT scan confirmed a large stomach and ascites but showed no livermetastasis. Ascites tap was negative for malignant cells. Endoscopyshowed a patent end-to-side anastomosis of the duodenal cuff to the jeju-num, but marked narrowing just distal to it. The afferent jejunum, whichbears the bile duct and pancreatic anastomoses, was patent. Endoscopicbiopsies of the stenosed areas failed to reveal neoplastic involvement.
Fig. 2. A The proximal jejunum exteriorized via this incision, and the anvil of the EEA stapler secured with a pursestring suture. Note the ‘‘re-trieval loop’’ threaded through the hole at the tip of the anvil.B The jejunum has been returned to the abdomen to facilitate exposure of the stomach, leavingonly the retrieval loop on the exterior.
Fig. 3. A The EEA stapler inserted into the stomach via an anterior gastrostomy.B The gastrojejunostomy staple line is inspected prior to removal of thestapler. The entire circumference can be viewed by moving the retractors.
677

The patient underwent stapled gastrojejunostomy by the above tech-nique. The operation took 35 min and she was discharged on day 4. Symp-tomatic improvement was maintained and weight gain was recorded atfollow-up 1 month after operation.
Discussion
Laparoscopic gastrojejunostomy has been reported for asimilar indication using a totally intracorporeal techniquefor the anastomosis [1, 2]. While our technique does notclaim to be laparoscopic, it also requires no special laparo-scopic expertise, since the main operation is done in theopen wound. The laparoscope facilitates a general exami-nation and identification of the jejunum loop, enabling amini-incision to be used. The operation is also much moreexpeditious than a totally laparoscopic one, which takeslonger and requires four to five ports, probably equivalent tothe mini-incision in length and discomfort.
We have since used this method in another patient, suf-fering from inoperable distal gastric cancer, with equal suc-cess. This simple procedure has little or no learning curveand deserves to be used and confirmed by others.
Acknowledgment.This work was supported by departmental researchfunds.
References
1. Kum CK, Tap CH, Goh PM (1995) Palliation of advanced gastriccancer by laparoscopic gastrojejunostomy. Singapore Med J 36: 228–229
2. Rangraj MS, Mehta M, Zale G, Maffucci L, Herz B (1994) Laparo-scopic gastrojejunostomy: a case presentation. J Laparoendosc Surg 4:81–87
678

Laparoscopic Douglasectomy in the treatment of painfuluterine retroversion
P. von Theobald, P. Barjot, G. Levy
Department of Gynecology, CHRU Caen, Avenue Georges Cle´menceau, 14033 Caen Cedex, France
Received: 22 April 1996/Accepted: 15 July 1996
AbstractBackground:One of the etiologies of pelvic pain in women,often unrecognized, is the Masters-Allen syndrome, whichwas described in 1955 as the ‘‘universal joint cervix’’ syn-drome. It has the following three elements: (1) etiology:obstetrics-related trauma; (2) clinical findings: uterine ret-roversion with hypermobile cervix following elongation ordesinsertion of the uterosacral ligaments; (3) anatomy: vi-sualization of a tearing of the posterior serosa and subperi-toneal fascia of the ligamentum latum.Methods: Forty-one laparoscopic Douglasectomies withuterosacral ligamentopexy were performed in the depart-ment of Gynecology at the University Hospital of Caenduring the period between 1990 and 1995 in patients withpainful retroverted uterus. The patient selection was madethanks to the ‘‘pessary test.’’ The surgical endoscopic pro-cedure, identical to the operation first promoted by Jamainand Letessier in 1976 by laparotomy, is described.Results:Total pain relief was experienced by 31 patients(75%) and partial relief by five patients (5%). Two maincomplications occurred, requiring one laparotomy (bleedingfrom a pelvic varicose vein with a concomitantly occurringbreakdown of the washing-aspiration system) and one sec-ond laparoscopy at day 15 (one case of hematoma below theperitonization revealed by pain). Twenty-three women be-came pregnant again, and had normal deliveries except fortwo cesareans, with no recurrence of pain. Douglasectomyis compared to alternative techniques in the literature. Otherindications for Douglasectomy are discussed.Conclusion:Douglasectomy is the only definitive procedurefor restoring normal anatomy of the pelvic floor in case ofpainful uterine retroversion occurring in a setting of Mas-ters-Allen syndrome. Additionally, it provides for patho-logical analysis of the excised peritoneum. The results ofthis procedure are excellent when the indication is correctlyset, particularly as concerns positive pessary testing.
Key words: Laparoscopic Douglasectomy — Uterine ret-roversion — Pelvic floor
In 1976, Jamain, who had first promoted Douglasectomy,presented his 12-year experience with the surgical techniqueon 265 cases in which the main indication was painful ret-roversion and hypermobility of the uterus [7].
In fact, peritoneal resection of the Douglas pouch, as-sociated with tightening of uterosacral ligaments and peri-tonization to exclude the Douglas pouch, is one of the bestmethods to use to definitively correct retrodeviation andexcessive mobility of the body of uterus and suppress theneurovascular compression responsible for characteristicpelvic pain. The Douglasectomy avoids the occurrence ofperitoneal cysts related to the peritoneal liquid trapped be-low the partitionment of the Douglas pouch created by theuterosacral ligamentopexy.
Treatment of chronic pelvic pain is a much-discussedtopic. Multiple etiologies have been incriminated, namelypsychosomatic causes, and clinical and laboratory tests areoften of little help. Diagnostic laparoscopy has been usefulin diagnosing endometriosis (22% of cases), pelvic adhe-sions (27.4% of cases), pelvic varicose veins (11.4%), ovar-ian cysts (6.5%), ovarian dystrophy (3.2%), and subserousmyoma (2.1%). Typical Masters-Allen syndrome is a find-ing in only 3.8% of cases in this series of 184 laparoscopicexaminations reported by Priou [9] and the pelvis appearsnormal in 28.8% of the female patients.
Masters-Allen syndrome, which was described in 1955as the ‘‘universal joint cervix’’ syndrome, has the followingthree elements [1, 3, 8, 14]:
● Etiology: obstetrics-related trauma● Clinical findings: uterine retroversion with hypermobile
cervix following elongation or desinsertion of the utero-sacral ligamentsCorrespondence to:P. von Theobald
Surg Endosc (1997) 11: 639–642
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

● Anatomy: visualization of a tearing of the posterior serosaand subperitoneal fascia of the ligamentum latum
Materials and methods
All female patients included in these series were multiparous; the averageage was 32 years (27 to 41 years). All suffered from typical pelvic painwhich had been investigated and treated on many occasions. A diagnosis ofMasters-Allen syndrome was made and inclusion in the series was decidedon the basis of the following criteria:
1. Obstetric anamnesis showing a past history of dystocia:large babies,instrumental extraction, breech presentation. Frequently, the uterus wasretrodisplaced prior to pregnancy and the beginning of the disordercould be traced to some obstetrical episode.
2. Typical pelvic pain:It appears and exacerbates during prolonged stand-ing, is aggravated by fatigue, and disappears in the recumbent position.It is invariably associated with dyspareunia. Dysmenorrhea is absentand the pain does not fluctuate during the menstrual cycle.
3. Clinical findings:● An important degree of uterine retroversion/flexion● Pain provoked by mobilization of the uterine fundus: the acute pain
described by the patient can be elicted● Abnormal mobility of the cervix in relation to the uterine body: The
cervix can be mobilized in all directions with the finger, as if it wasarticulated on a ball joint.
4. Pessary test:vaginal insertion of a pessary of the appropriate vagina-adapted size, positioned above the levatores ani muscles, provides forcorrecting the uterine retroversion and hypermobility. When positive, itsuppresses almost immediately the painful symptomatology and con-stitutes a major argument in favor of Masters-Allen syndrome. Whennegative, it will cause no change. The pessary is left in place for about10 days. The pessary is then removed and the pain reappears immedi-ately, unchanged. The relief induced by the pessary is often so marked,when the test is positive, that one female out of two requests that it beleft in place until the operation.
5. Diagnostic laparoscopy:Most of all, this presents the advantage ofexcluding other etiologies of pelvic pain, such as endometriosis, adhe-sions, or salpingitis [9]. However, it should be noted that many patientspresenting Masters-Allen syndrome have undergone multiple laparo-scopic examinations, which have resulted in the wrong diagnosis ofchronic salpingitis or even endometriosis because of the inflammatoryappearance of the pelvic peritoneum. Laparoscopy cannot help visualizetrue ligament disinsertion lesions located at the subperitoneal level [12,14]. It will reveal nonspecific signs, such as minor serous effusion,varicocele, marked retrodeviation of the uterus with a very deep Doug-las pouch reminiscent of enterocele, and typical, sometimes recent, butoften long-standing, fibrous and retractile tears of the ligamentum la-tum. Soutoul’s sign should be tested for to confirm uterine hypermo-bility: 180° rotation of the uterine body around the saggital axis is easilyproduced [13].
Operating procedure
This is identical to the reference procedure by laparotomy. The uterus iscatheterized in order to be able to anteverse the uterine body. Three trocarsare put in place: one umbilical trocar for the optical device, and twosuprapubic trocars of 10- or 12-mm diameter, fitted with 5-mm reducers,allowing for the passage of the needed dissecting instruments (grip forceps,scissors, washing/aspiration material) and suturing instruments (laparo-scopic needle holder, Endostitch, or endoscopic staplers). Sometimes it isnecessary to insert a fourth trocar laterally to the umbilicus on the assistantsurgeon’s side in order to insert a laparoscopic spreader to push the intes-tinal loops back. Dissection of the Douglas peritoneum (Figs. 1 and 2) iscarried out much more conveniently than by laparotomy; it is aided byaquadissection, image magnification, the length of the instruments and ofthe optical device, and by barohemostasis which prevents bleeding fromany source other than pelvic varicose veins, the latter being ideally stoppedby means of titanium clips, if needed. The incision of the peritoneum isperformed just above the uterosacral ligaments after optical localization ofthe ureters. The anterior limit is the torus uteri and the posterior limit is theanterior wall of the rectum. Ligamentopexy of the uterosacral ligaments
(Fig. 3) is carried out using three or four separate stitches with absorbabledecimal 4 suture (Endostitch greatly facilitates the procedure), or by me-chanical endoscopic stapling. Peritonization (Fig. 4) is carried out trans-versely by stapling or by continuous absorbable thread. The mobility of theureters is checked at the end of the procedure.
Results
Forty-one laparoscopic Douglasectomies were performed inthe Department of Gynecology at the University Hospital ofCaen during the period between 1990 and 1995 (Fig. 5). Theaverage duration of the procedure is 75 min (45 to 130) and,out of the 41 operations conducted to date, the only com-plications have been:
● One case of bleeding from a pelvic varicose vein with aconcomitantly occurring breakdown of the washing-aspiration system, forcing the operators to terminate byconventional surgery
● One case of subperitonization hematoma revealed by painat day 8, requiring repeat laparoscopy at day 15
● One case of postoperative endometritis treated with anti-biotics
Surgical results were positive otherwise, although oftenquite painful for the first 48 h; hospital release was on day
Fig. 1. Posterior view of the uterus. Drawing of the peritoneal incision.
Fig. 2. Douglasectomy.
640

4 on average (range 2 to 8). Patients were seen again 2months postoperatively, and then yearly, with an averagefollow-up period of 2.9 years (6 months to 5 years). To date,we have not lost sight of any of the cases. Thirty-one fe-males experienced complete pain relief (75%) and five more(12%) had their symptoms greatly improved. Five patients(12%) experienced no relief after the procedure. None of thesuccessfully operated patients had a recurrence of the pelvicpain and dyspareunia. Twenty-three women became preg-nant again and had a normal delivery (except for two ce-sareans performed for miscellaneous indications), with norecurrence of pain. Four out of the ten who did not improveat all or were only partially improved showed undiagnosedmicroscopic endometriosis of the excised Douglas pouchperitoneum.
Discussion
Chronic pelvic pain in women is difficult to manage anddiagnostic investigations are seldom decisive. Once the
most common etiologies have been excluded, such as in-fection and endometriosis, many practitioners attribute thepain to psychological causes. Two-thirds of the female pa-tients in our series had two or more laparoscopic examina-tions carried out before our intervention, most often by dif-ferent operators. These investigations frequently resulted inthe description of catarrhal salpingitis or soft endometriosis,or even normal pelvic findings. But antibiotic and antiin-flammatory treatments remained consistently without ef-fect. We think that the diagnosis of Masters-Allen syndromeis too often missed. It does not seem to us justified toclassify all these women as hypochondriacs. In fact, ourresults prove us right: When the indication is properly set,87% of the women experience pain relief, which no opera-tion-related ‘‘placebo’’ effect can, in itself, explain. Whensymptoms are present, Masters-Allen syndrome is charac-terized by static disorders of the pelvis, and Douglasectomywith uterosacral ligamentopexy is the only definitive pro-cedure likely to restore normal anatomy. Laparoscopy hasconsiderably facilitated this procedure thanks to image mag-nification and barohemostasis, and has reduced surgical se-quelae for the patients. The parietal complications related toall laparotomies are avoided: hematoma, abscess, eviscera-tion, cosmetic sequelae.
Some laparoscopic techniques exist as an alternative toDouglasectomy:
Ligamentopexy of the round ligaments [4, 5]
This used to be conducted by laparotomy as Doleris’s pro-cedure and was dropped because of the very high rate ofrecurrences within 2 years postoperatively. Manhe`s has re-vived it through the use of laparoscopy. Laparoscopic liga-mentopexy is an easy and rapid procedure consisting in aretightening of the round ligaments by grasping those ex-traperitoneally under laparoscopic control and fixing themby plicature to the aponeurosis of the rectus abdominismuscle. The uterus is thus put back into the intermediate
Fig. 3. Uterosacral ligamentopexy.
Fig. 4. Peritonization.
Fig. 5. Results of the 41 procedures.
641

position, while the degree of anteversion is controlled en-doscopically. In our opinion, this procedure presents severaldisadvantages:
● Recurrences are not less frequent than before. A poorsurgical laparotomic technique is not made good evenwhen touched by the grace of laparoscopy. In fact, theround ligaments are quickly loosened and stretched, andthe treatment of the retroversion is transient.
● Ligamentopexy of the round ligaments tears the uterusforwards and increases the risk of enterocele.
Ventrofixation [10]
This technique, which had long been dropped by all opera-tors, consists of fixing the anterior side of the deperitonizeduterus to the anterior wall of the abdomen. This procedurehas also been revived by laparoscopy. This method seems tous even more worthy of criticism than ligamentopexy of theround ligaments, since it opens the Douglas pouch muchmore yet and hyperanteverses and immobilizes the body ofthe uterus. Enterocele is sure to occur.
Section of the preacral nerve [6]
This procedure was first used by Cotte in 1925, primarily inthe treatment of severe algomenorrhea, and has regainedpopularity among Anglo-Saxon authors with the advent oflaparoscopy. The effect on pain seems quite satisfactory,although no serious study has been published. The disad-vantage here is the lack of repair of the static disorder of thepelvis. Enterocele-type complications have begun to beseen.
Insertion of a pessary
This can only be a temporary cure of the pelvic pain anddyspareunia in these young women, because it often in-volves vaginal infection and restrains one from regular in-tercourse.
Douglasectomy is indicated in pathologies other thanMasters-Allen syndrome [11]:
● Endometriosis of the Douglas pouch: Peritoneal resectionprovides for removal of all lesions and constitutes, in thislocation, an alternative to laser vaporization [15].
● Treatment of prolapse by the abdominal route and, moreparticularly, by laparoscopy: Some authors use Doug-lasectomy as a complementary procedure. It permits oneto obtain a perfect exposure of the posterior side of thecervix and vagina, in the case of posterior prosthesis, andto correct or to prevent the occurrence of enteroceles [2].
● Isolated enterocele, associated or not with genital pro-
lapse, sometimes responsible for digestive obstruction byway of incarceration, and of positional pain [11].
Conclusion
Douglasectomy is the only definitive procedure available torestore normal anatomy of the pelvic floor in the case ofpainful uterine retroversion occurring in a setting of Mas-ters-Allen syndrome. Additionally, it provides for patho-logical analysis of the excised peritoneum. The results ofthis procedure are excellent when the indication is correctlyset, particularly as concerns positive pessary testing. Therelief obtained by pessary insertion is spectacular, so muchso that many female patients request that it be left in placeuntil the surgical procedure. The same relief is regainedafter Douglasectomy and tightening of the uterosacral liga-ments have been carried out.
References
1. Allen WM (1971) Chronic pelvic congestion and pelvic pain. Am JObstet Gynecol 109: 198–202
2. Ameline A, Hughier J (1957) La suspension poste´rieure au disquelombo sacre´. Gynecol Obstet 45: 56–94
3. Atkinson SM Jr (1970) Syndrome de l’universal joint cervix (Allen etMasters). Laceration traumatique des supports ute´rins. Obstet Gynecol36: 510–514
4. Bruhat MA, Dubuisson JB, Pouly JL (1989) Ligamentopexie ante´r-ieure des ronds par voie coelioscopique dans la cure des retroversionsuterines. E.M.C., (Paris, France), Techniques Chirurgicales, UrologieGynecologie, 41515: 32–33
5. Durand A, Abeille JP (1979) La cure de retrode´viation percoeli-oscopique: 6 ans apre`s. Gynecologie 30: 275–278
6. Good MC, Copas PR, Droody MC (1992) Uterine prolapse after lap-aroscopic uterosacral transection. A case report. J Reprod Med 37:995–996
7. Jamain B (1976) La douglassectomie en gyne´cologie. Concours Me´d98: 3687–3691
8. Masters WM, Allen WM (1955) Traumatic laceration of uterine sup-port. Am J Obstet Gynecol 70: 500–513
9. Priou G, Arvis P, Rind A, Fraisse E, Grall JY (1984) Etude de l’apportdiagnostique de la coelioscopie dans le bilan des algies pelvienneschroniques. J Gynecol Obstet Biol Reprod 13: 395–402
10. Querleu D (1994) Cure de prolapsus par ventrofixation: re´edition coe-liochirurgicale d’une mauvaise ope´ration. Rev Fr Gyne´col Obstet 89:164
11. Querleu D, Delahousse G, Decocq J, Parmentier D (1988) La placeactuelle de la douglassectomie. Communication aux 4° Journe´es An-nuelles de la Socie´te Internationale Francophone de Chirurgie Pelvi-enne, Roubaix, 25–26 mars 1988
12. Robert HG, Palmer R, Boury-Heyler C, Cohen J (1974) Les anomaliesde position. In: Pre´cis de gyne´cologie. Masson, Paris, pp 471–477
13. Soutoul JH (1973) Essai de classification des le´sions ligamentairesdans le syndrome de de´sinsertion ute´rine (Masters et Allen) graˆce aune exploration dynamique percoelioscopique et ope´ratoire de la mo-bilite uterine. Gynecologie 24: 339–344
14. Soutoul JH (1974) Syndrome de Masters et Allen avec de´sinsertionuterine. Bilan fonctionnel des le´sions ligamentaires et indications op-eratoires. J Gynecol Obstet Biol Reprod 3: 13–20
15. Wood C, Maher P, Hill D (1993) Laparoscopic removal of endome-triosis in the pouch of Douglas. Aust N Z J Obstet Gynaecol 33:259–299
642
Balloon dissection of the space of Bogros via the femoral canal fortotal extraperitoneal laparoscopic herniorrhaphy
R. C. Read,1,2 R. A. de la Torre,3 J. S. Scott3
1 General Thoracic Surgery, Surgical Service (112 LR), John L. McClellan Memorial Veterans Hospital, 4300 West 7th Street,Little Rock, AR 72205, USA2 University of Arkansas for Medical Sciences, Little Rock, AR, USA3 Suite 214, 600 Medical Drive, Wentzville, MO 63385, USA
Received: 3 April 1996/Accepted: 15 September 1996
Abstract. To obviate the need for general anesthesia ordissection of the rectus sheath, we have transferred laparo-scopic herniorrhaphy back to the groin by first dissectingthe suprainguinal parietoperitoneal space of Bogros via thefemoral canal. Cadaver dissections demonstrated that thepreperitoneal plane could be routinely fingered and dis-tended with a digitally placed balloon introduced through a1-cm incision immediately below the inguinal ligament. A10-mm femoral laparoscopic port was then inserted andpressurized, allowing two standard 5-mm ports to be intro-duced from above, through the lower quadrant, under vi-sion. The procedure was then carried out in the usual way,the mesh being inserted from below. Ten patients (twowomen), 23–73 years old, selected because general anes-thesia was inadvisable, underwent uncomplicated prostheticrepair of unilateral (eight) or bilateral (two) inguinal defects.Half of the peritoneal sacs were pushed up and out of theinguinal canal; 18 months later there were no recurrences(inguinal or femoral). Preliminary experience with this newtechnique is promising. It may prove applicable to retroperi-toneal exposure of the distal aorta and iliac vessels, allowinglaparoscopic bypass for Leriche syndrome.
Key words: Total extraperitoneal inguinal laparoscopicherniorrhaphy — Femoral canal — Space of Bogros
A major limitation of laparoscopic repair is the need forgeneral anesthesia. It has been required, even with the totalextraperitoneal technique, not only to provide relaxation ofthe abdominal musculature but also for periumbilical anes-thesia. This allows the space of Retzius [14] to be ap-proached via the rectus sheath. Distension of the former
inflates the communicating lateral extraperitoneal spaces ofBogros [12] thereby providing a view of the posterior sur-face of the groin(s).
To allow the routine use of spinal, epidermal, regionalblock, or local infiltration anesthesia we have attempted toreturn the entire operation to the groin. Instead of distendingthe suprainguinal parietoperitoneal space of Bogros [12]indirectly by first inflating the midline suprapubic space ofRetzius we have explored the possibility of reversing thesequence. The space of Bogros has been dissected first witha balloon introduced digitally through the femoral canal.Since, in this new approach to a predominantly unilateralaffliction, the rectus sheath does not need to be dissected,laparoscopic herniorrhaphy could potentially be practicablein patients who have a history of previous lower midlineabdominal surgery or in the 10% of individuals whose pos-terior rectus sheath extends anomalously [9] to the pubes,thereby preventing safe trocar insertion into the space ofRetzius.
Anatomy
The space of Bogros
In 1823 the French surgeon Jean Bogros (1786–1825) pre-sented his M.D. thesis to the University of Paris. In it henoted that the peritoneal cavity did not reach all the way tothe groin but left a parietoperitoneal space filled with fattycellular tissue (Fig. 1). Since the distal external iliac arterycoursed posteriorly therein (‘‘The peritoneum extendingfrom the iliac portion of the anterior abdominal wall to theiliac fossa leaves in front a space 13.5–15.5 mm wide wherethe external iliac artery terminates’’), he recommended thatligation of this vessel for aneurysm be performed within thisextraperitoneal space. He approached it by a groin incision,Correspondence to:R. C. Read
Surg Endosc (1997) 11: 687–692
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

transecting the roof and floor of the inguinal canal, 60 yearsbefore Bassini described the same exposure for his classicrepair of inguinal herniation! The advantage of Bogros’soperation over the then-standard approach for proximal ex-traperitoneal ligation, described in 1790 by John Hunter’spupil, Abernethy [1], was that the latter’s incision was lo-cated just medial to the anterior superior iliac spine. It en-tailed a considerable risk of death from peritonitis, if theclosely applied underlying peritoneum was divided (30years before Lister introduced antisepsis!).
Bogros’s original anatomical observations were con-firmed almost a century later by a compatriot, Rouviere[15]:
The peritoneum which lines the deep aspect of the abdomi-nal inguinal wall is reflected from the abdominal wall to-wards the iliac fossa creating a fold of peritoneum in theshape of a gutter concave above and behind. This fold ofperitoneum is such that from the abdominal wall to the iliacfossa the outer layer of the peritoneum is in contact with thesoft tissues of the iliac fossa, some 1–1.5 cm above theinguinal ligament. The peritoneum thus demarcates, with adihedral angle formed by the fascia transversalis and theiliac fossa inferiorly, a triangular prismatic interval filledwith preperitoneal adipose tissue called the space of Bogros.
Later, Testut and Latarget [17] stressed the continuity be-tween the parietoperitoneal spaces of Bogros and Retzius,the kidney, and the spermatic cord.
Bogros also observed that the inferior epigastric vesselsarose in the floor of his space and then coursed inferiorly,overlying their parent external iliac vessels. They turnedanteriorly to supply the rectus muscle within its sheath.Mackay [7] (1889) later pointed out that at the ‘‘bend’’ theepigastric vessels pierce the transversalis fascia to enter theabdominal wall. They, thus, do not course in the extraperi-toneal fat as is classically taught. The vein drains from asuprainguinal plexus recently detailed by Bendavid [3].This vasculature is not located, as he described, within thespace of Bogros but rather between Cooper’s two laminaeof the transversalis fascia [13], the deepest layer of theanterior abdominal wall. The inferior epigastric artery andvein after they enter the parietes lie external to the internalspermatic fascia derived from the transversalis fascial liningof the space of Bogros (posterior lamina) (Fig. 1). Thispreperitoneal funnel passes through one of the two outlets ofthe space of Bogros, the secondary internal abdominal ringof Fowler [13], into the internal abdominal ring in thethicker external lamina of transversalis fascia, thereby form-ing the internal spermatic fascia.
The ureter courses down to the pelvis in the posterio-medial portion of the space of Bogros from which it mayherniate into the inguinal canal. This anatomical relation-ship was repeatedly observed by Henry [4] during an ex-tensive experience with the extraperitoneal approach for theremoval of bilateral ureteric stones in Egyptian patients in-fested with the Bilharzia parasite. Consequently, when ayoung woman presented with bilateral femoral herniation,he rediscovered Cheatle’s midline, extraperitoneal, poste-rior approach to the groin. This operation evolved into thegiant prosthetic reinforcement of the visceral sac (GPRVS)of Stoppa [16], which has formed the basis for laparoscopic,total extraperitoneal prosthetic repair. A unilateral modifi-
cation of the Cheatle-Henry procedure was originally de-scribed by McEvedy in 1950 [8]. Prosthetic repairs throughthis approach include the unilateral GPRVS of Wantz [19].This sequence of events prompted us to investigate whetherthe surgical anatomy was such that, just as the open midlineCheatle-Henry posterior preperitoneal approach gave rise toMcEvedy’s unilateral variant, extraperitoneal balloon dis-section for laparoscopic herniorrhaphy could likewise betransferred from the umbilicus (where it began with trans-peritoneal procedures) to the groin for total extraperitonealrepair.
Femoral canal
The external iliac vessels as they pass into the thigh takewith them a sheath of transversalis and iliac fasciae liningthe extraperitoneal space of Bogros (Fig. 1). Since the me-dial portion of the femoral sheath forms a canal we decidedto use it as a point of entry into the suprainguinal preperi-toneal space which could then be distended to allow lapa-roscopic herniorrhaphy of the groin. The abdominal open-ing of the conical 1.5–3.0-cm-long femoral canal is boundedby an elastic fascial ring enclosed within a rigid aperture.The former is composed anteromedially by Henle’s liga-ment and the iliopubic tract, which separates the overlying
Fig. 1. Sagittal diagram of the femoral canal (F) passing up under theinguinal ligament and canal (I) over the pectineus muscle, ligament ofAstley Cooper (E), and pubic ramus into the space of Bogros (D) beneaththe peritoneum (A). Note posterior lamina transversalis fascia (B), epigas-tric vessels (C), anterior femoral sheath (H), posterior sheath (iliac fascia),and pectineus fascia (G).
688

inguinal canal. Laterally, a septum borders the femoral vein.The rigid component comprises, posteriorly the superiorpubic ramus overlain by Cooper’s ligament, medially Gim-bernat’s ligament, and anteriorly the inguinal ligament. Thefemoral ring (9–27 mm in diameter) is separated from thespace of Bogros and the femoral fossa of the parietal peri-toneum by a flimsy cup-shaped septum, concave superiorly,derived from the posterior lamina transversalis fascia as itinserts into Cooper’s ligament internal to the inferior epi-gastric vessels and their branches. Femoral herniae exit thecanal through an orifice in the fascia lata (foramen ovale)covered by the cribriform plate of Scarpa’s fascia where thesaphenous vein enters the femoral sheath. They becomeincarcerated or strangulated either here or higher up at thefemoral ring.
This textbook description of the anatomy is open toargument. Some consider the femoral canal to be a potentialspace, its presence only becoming manifest with herniation.Measurements taken after death provide information regard-ing what obtains, predominantly, in the elderly, debilitatedor diseased with impaired musculature, aponeuroses, andfasciae. The presence or absence of clot in the external iliacvein, after embalming, also affects data pertaining to thesize of the femoral ring.
Methods
We first studied retrograde intubation of the femoral canal in cadaversobtained from the dissecting room or at autopsy. Initially, entry was at-tempted at the foramen ovale. However this proved to be unsatisfactory fortwo reasons. First, in the absence of femoral herniation, the femoral canaldid not consistently extend this far into the thigh. Secondly, superficialbranches of the saphenous vein interfered and had to be ligated. We there-fore moved proximally to the inguinal skin fold, immediately below theinguinal ligament, just proximal to the inguinal skin sulcus (Holden’s line),the surface landmark separating the abdomen from the thigh. A 1-cmtransverse skin incision was made medial to the palpated femoral artery
and vein. The underlying femoral sheath was cut to unroof the canal (Fig.2). The index finger was then inserted and passed upward beneath theinguinal ligament and the transversalis fascial floor of the inguinal canal toCooper’s ligament overlying the superior pubic ramus. The flimsy trans-versalis fascial femoral septum separating the canal from the space ofBogros offered no resistance, the tip of the finger ‘‘falling into’’ the su-prainguinal extraperitoneal space (Fig. 3). It could be swept around medi-ally behind the rectus abdominis tendon, inferiorly over and behind thepubic ramus toward the obturator foramen, anteriorly to the space ofRetzius, and laterally up behind the secondary internal abdominal ring ofFowler and the inner (preperitoneal) spermatic cord to the anterior abdomi-nal wall (Fig. 1).
The external iliac vein is separated from the femoral canal by a fibrousseptum. It is important that the index finger as it passes upward beneath theinguinal ligament run parallel to it and not wander out of the sheath,making a false passage into the inguinal canal, anteriorly, or Gimbernat’sligament, medially. We distended the space of Bogros with a 750-ml sa-line-filled balloon. It was originally mounted on a standard straight, rigidmandrel designed for infraumbilical insufflation. However, in one instancethe overlying peritoneum was perforated by the blunt tip. We thereforedecided to simply place the balloons digitally. After removing the balloon,a standard 10-mm laparoscopic port was inserted through the femoralincision and pressurized to 8–10 mmHg with CO2. A camera was intro-duced from below and two 5-mm ports were inserted with trocars throughthe distended lower quadrant of the anterior abdominal wall under directvision. Laparoscopic repair was then carried out from above in the usualmanner, the 11 × 15 cm2 polypropylene prosthesis being introduced frombelow through the larger femoral port.
Clinical experience
Early in 1995, eight men and two women, whose ages ranged from 23 to73 years, underwent balloon dissection of the space of Bogros via thefemoral canal by the technique described with uncomplicated laparoscopicrepair of primary and recurrent, unilateral (eight) or bilateral (two) ingui-nal, with indirect (eight) or direct (four) defects. These patients were se-lected out of our main experience with infraumbilical dissection becauseeither their preference or physical condition made general anesthesia in-advisable. Some had a history of previous lower midline abdominal sur-gery. After preoperative assessment and workup had been conducted on anoutpatient basis, patients were scheduled and arrived for 1-day surgeryearly in the morning, having fasted overnight. They received prophylactic
Fig. 2. One-centimeter skin incision deepened over the medial portion ofthe femoral sheath immediately below the inguinal ligament and above theinguinal skin crease (dashed line) and the entry of the saphenous vein(cribriform plate). Fig. 3. Fingering of the space of Bogros through the femoral canal and
ring.
689

antibiotics. They were premedicated and asked to void. They were thenplaced supine on the operating room table and the skin over the groin wasprepared. After infiltration with a local anesthetic—along with intravenoussedation—the femoral skin incision was made and the space of Bogros wasfingered. A 750-ml nonelastomeric balloon (Spacemaker Balloon Dissec-tor, GSI) was inserted and inflated. Repair was accomplished using thetechnique developed in the cadaver.
Results
The femoral canal was patent in all, allowing the space ofBogros to be consistently fingered (Fig. 2). There was nobleeding either before or after insertion and inflation of theballoons, which consistently stretched and everted the bodywall in the groin extending into the midline. The appearanceof the extraperitoneal space was similar to that seen withstandard infraumbilical laparoscopy. However, there wasbetter dissection of the preperitoneal cord structures pos-terolaterally and superiorly. The transversalis fascial liningof the space of Bogros was disrupted only at the femoralring, remaining internal to the rectus muscles and epigastricvessels in the space of Retzius. Despite unilateral inflation,bilateral dissection, and, if necessary, repair, were easilyperformed since the space of Retzius inflated secondarily.Interestingly, reduction of processi vaginales from withinthe inguinal canal was complete in half of those with indi-rect defects. This facilitated dissection and separation of theelements of the spermatic cord from each other and the sacat the internal abdominal ring prior to parietalization. Fol-low-up of at least 6 months has shown no recurrences (in-guinal or femoral). All patients were able to go home afteroutpatient surgery on oral analgesics. The femoral woundshealed well without the late bruising and tenderness oftenseen in the usual periumbilical location. None has devel-oped phlebitis.
Discussion
The presence of a femoral canal, potential or manifest, al-lows the vessels supplying blood to and from the leg toexpand in response to gravity or increased flow; unfortu-nately it can also let bowel escape from the abdominal cav-ity. Nevertheless, this channel continues to serve as a paththrough the abdominal wall, allowing surgeons to relievevisceral entrapment at the femoral ring. As Monroe [10] hasstated, ‘‘The low approach to femoral herniation is almostas old as surgery itself. Before the days of anesthesia op-eration was undertaken only for strangulation or obstructionthe concern of the surgeon being to release the constrictingband without harming the content or causing injury to bloodvessels or bladder.’’ The first elective repair was that ofSocin (1879), ligating and removing the sac from below.Later, to avoid recurrence, a number of surgeons, notablyincluding Bassini (1893), added suturing of Poupart’s liga-ment, Gimbernat’s, the iliopubic tract, or the transversusabdominis muscle and tendon down to either the inguinalligament, the ligament of Astley Cooper, or the pectineusmuscle and fascia. Tension posed a problem and thereforeothers plugged the femoral canal with an agate marble, sa-phenous vein, or prosthetic mesh. Almost all of these pro-cedures are now performed under local anesthesia [6].
In 1989, Bendavid [2] reported a recurrence rate of 6.1%
in 248 patients who had undergone, 5–8 years previously,fascial repair of primary femoral herniation, 91% from be-low. The rate in 211 recurrent cases was 22%. He thereforerecommended that all large or recurrent defects be closedwith his 8-cm polypropylene mesh ‘‘umbrella’’ inserted un-der local anesthesia up to the femoral ring, where it isstitched circumferentially. Munshi and Wantz [11] have re-cently pointed out that this repair would not be suitable forperivascular defects since the prosthesis cannot be stitchedto the external iliac vessels. They report the successful useof the unilateral GPRVS procedure, developed primarily foringuinal herniation, in 69 such difficult primary (15) orrecurrent (54) femoral hernias. Of particular interest to ourstudy is that in six of these patients, who were elderly andtoo debilitated for general anesthesia, an emergency opera-tion was successfully completed from below using localanesthesia.
It could be argued that the presence of a femoral herniaso stretches the fascial confines of the canal, especially itsring and orifice, that it can be more easily entered andworked in. Further, aging and loss of body fat with laxity ofthe abdominal musculature might allow surgical manipula-tions not possible in those with a ‘‘normal’’ femoral canal,possibly including patients presenting with inguinal hernia-tion. Nevertheless, in the most successful fascial repair forthis condition being performed around the world today, theShouldice procedure, the femoral canal is routinely fingeredfrom below to rule out an associated femoral hernia. This isdone through the same 1-cm transverse incision in the fascialata and anterior femoral sheath, immediately below theinguinal ligament, we have used (Fig. 2) except that thesubcutaneous fat in the groin incision is retracted inferiorlyto avoid having to make a separate femoral wound. Ourexperience is similar in that, in our patients with inguinalherniation (or cadavers without) at this level, but not belowat the foramen ovale, the femoral canal was open (Fig. 2)despite the absence of femoral herniation. The intent has notbeen that of Wantz—to perform prosthetic repair throughthe femoral canal—but just to initiate the operation, whichis then carried out laparoscopically from above, using theposterior approach to the groin in the usual manner.
Classical anatomy, using data often obtained before theuse of antibiotics or even antisepsis, teaches that the femoralcanal contains lymph nodes which, presumably, if enlarged,with associated preperitoneal fat, could block passage; how-ever, sepsis is much less common today. Further, failure ofthe transversalis fascia, the most common cause of inguinalherniation in the adult, enlarges the femoral ring by dam-aging its elastic transversalis fascial components, therebyproducing a significant incidence of associated femoral her-niation. Thus, the space of Bogros has two exits (inguinaland femoral canals) through the myopectineal orifice or‘‘hole’’ of Fruchaud, which enlarges in patients with ingui-nal herniation. The use of the umbilicus as the portal forinsufflation derives from the traditional approach to trans-peritoneal laparoscopy. A high periumbilical incision in theabdominal wall (which usually requires general anesthesia),dissection of the rectus sheath, and distension of the spaceof Retzius (the latter only mandated, as unilateral GPRVShas shown, in the more unusual, bilateral herniation) addlittle to unilateral repair itself. Dissection of the lateral su-prainguinal preperitoneal space of Bogros via the femoral
690

canal transfers insufflation for total extraperitoneal laparos-copy from the umbilicus to the groin, thus allowing theroutine use of local epidural or spinal anesthesia. Our pre-liminary experience indicates that this goal can be reached.
The purpose of fingering the transversalis fascia linedfemoral canal is to break through the flimsy femoral septumwhich covers the femoral ring, thereby entering the suprain-guinal parietoperitoneal plane (Fig. 2). It is important torealize that, as Hureau has stressed, this space of Bogros ‘‘isa cleavable space devoid of any real structure but for a scantamount of adipose-cellular tissue. . . . Vessels, nerves andother elements run along the wall’’ [5]. This parietal wall isthe translucent but tough posterior lamina of transversalisfascia originally described in 1807 by Cooper but laterlumped in with the extraperitoneal fatty layer until redis-covered by Read in 1992 [13]. Unfortunately, Bendavid hasrecently described the deep inguinal venous plexus (tribu-taries of the inferior epigastric vein) as arching within thespace of Bogros, thereby raising unnecessary fears of bleed-ing if this plane is entered, as it has to be for adequate repair.‘‘This area is markedly vascular and prone to bleeding andhematomas’’ [3]. Accumulated experience with the unilat-eral or bilateral Stoppa posterior preperitoneal procedureperformed either open or laparoscopically within the spaceof Bogros has shown unequivocally that such veins are notencountered. Our experience with balloon distension of thisextraperitoneal space from below is consonant in that bleed-ing does not occur. Thus the undisturbed parietoperitonealspaces of Bogros and Retzius are essentially avascular andcan therefore serve as fatty shock absorbers protecting thebladder and peritoneal content from stress and strain. Theepigastric vasculature runs external to these parietoperito-neal planes in between the two laminae of transversalisfascia, the deepest layer of the abdominal wall, and is notencountered except with the classical anterior approachfrom the groin or the unilateral posterior preperitoneal in-cision.
Even though the approach of McEvedy has been con-sidered equivalent to the classical Cheatle-Henry midlineincision, anatomically it is not. In the latter the operation isconducted through the extraperitoneal space of Retzius in-ternal to the posterior lamina of the transversalis fascia onwhich the inferior epigastric vasculature, in the parietes liessurrounded by fat. These vessels are retracted anterolater-ally with the rectus muscles. By contrast, McEvedy origi-nally described his incision as being ‘‘within the rectussheath’’ [2]. Thus, initially after transecting the substantialouter lamina of transversalis fascia the surgeon comes downonto the epigastric vessels resting upon the posterior laminaof transversalis fascia. Nyhus, who popularized the McEv-edy incision, initially ligated the inferior epigastric arteryand vein before penetrating the underlying posterior laminatransversalis fascia in order to enter the space of Bogros andrepair the defect. Other surgeons using the posterior pre-peritoneal approach, either open or laparoscopically, havedebated whether the prosthesis should be inserted superfi-cial to or deep to the epigastric vasculature (most settling forthe latter). Gilbert reports [personal communication] thatprosthetic plugs introduced through the internal inguinalring, into the preperitoneal plane, from the classic anteriorapproach can cause bleeding which may extravasate intobizarre locations; presumably Bendavid’s suprainguinal ve-
nous plexus is being torn in the transversalis fascial roof tothe space of Bogros. Thus, laparoscopic exposure of thespace of Bogros, from above or below, has an importantadvantage over the unilateral open preperitoneal approach:Regardless of patient comfort, the epigastric vasculature isnot encountered on the way in; this asset needs to be morewidely appreciated.
It is important to realize that instrumentation developedto mount balloons inserted through the standard transum-bilical approach cannot be automatically applied to this newroute. Here the peritoneum overlies the femoral ring (Fig. 1)and can be easily fingered from the infrainguinal incision(Fig. 3). This compares with a distance of three fingerlengths or more between the umbilicus and the pubes. Ourexperience in the cadaver indicated that mandrels should notbe used from below, and we have therefore made it a rule toinsert the balloons digitally. Just recently, after this initialseries of patients had been operated upon and followed upfor presentation, we contravened this principle in a 75-year-old patient who presented with a history of multiply recur-rent bilateral inguinal herniation and a fresh protrusion inthe left groin. Since he had undergone a suprapubic prosta-tectomy we attempted to obtain a higher posterolateral in-flation of the space of Bogros, hoping thereby to avoid thescarred space of Retzius. After fingering the cavity throughthe femoral canal, a curved rigid mandrel-mounted balloonwas inserted and inflated. Excellent distension, albeit uni-lateral, was obtained. However, when the balloon was with-drawn, bleeding ensued from the incision. We induced gen-eral anesthesia and converted to open repair by incising hismidline scar. The external iliac artery was fibrosed withsurrounding lymph nodes. It had been deviated anterolater-ally, presumably by the blunt tip of the rod. Removal of ahematoma showed a leak distal to a calcified plaque at thetakeoff from the common iliac artery. This was sutured anda GPRVS (unilateral) repair was carried out. Fortunately, hehas done well. Thus, by its breach, the principle of usingonly free-standing, digitally placed everting balloons wasconfirmed. Further, a history of suprapubic prostatectomyremains a contraindication to laparoscopic repair since re-action to it is not restricted to the space of Retzius butextends unpredictably throughout the posterolateral extra-peritoneal space. However, as indicated above, we havebeen able to use this novel approach in other patients withinfraumbilical scarring not extending down to the pubis.
An unexpected advantage of transfemoral inflation isthat the distending force is applied more from below than infront of the peritoneal cavity. Coupled with the Trendelen-burg position, this has resulted in more of Henry’s [4] peri-toneal ‘‘horns of the snail’’ being lifted out of hernial de-fects. This enhanced reduction of hernial sacs has reducedthe amount of preperitoneal fascial funnel dissection re-quired to separate the cord from the peritoneum and toparietalize it before placement of the prosthesis. Hopefully,the incidence of peritoneal tears and damage to the vasdeferens will be reduced. It is interesting that Bogros, whoseoriginal observations are central to this new approach, wasa pioneer vascular surgeon. Exponents [18] of his specialtyin 1972 used the ‘‘normal’’ femoral canal as a new route forthe femorofemoral arterial bypass, demonstrating that, evenin the absence of herniation, inguinal or femoral, there iseasy communication with the space of Bogros, again not
691

from as far down as the foramen ovale. A prosthetic conduitwas introduced via the femoral canal from the ‘‘good’’ leg;it was then passed digitally across the space of Retziusretropubically to the space of Bogros on the ischemic side.By then bringing the graft down the contralateral femoralcanal and anastomosing its two ends to the femoral vesselsa new source of blood flow was provided. In the future,laparoscopic dissection of the space of Bogros via the femo-ral canal may facilitate retroperitoneal exposure of the ter-minal aorta and iliac vessels, thereby preventing iatrogenicherniation through the groin secondary to splitting of theinguinal ligament and abdominal musculature.
Acknowledgment.We appreciate the assistance provided to this study bythe GSI Corporation, Palo Alto, California, and in particular Dr. Thomas J.Fogarty, Dennis Benassi, George Hermann, Ken Mollenauer, and ShellyMonfort. The illustrations were the work of Patricia O’Neal from theUniversity of Arkansas for Medical Sciences Media Department.
References
1. Abernethy J (1811) Surgical observations on the constitutional originand treatment of local diseases and on aneurysms. 2nd ed. Fry andKammerer, Philadelphia
2. Bendavid R (1987) A femoral ‘‘umbrella’’ for femoral hernia repair.Surg Gynecol Obstet 65: 153–156
3. Bendavid R (1992) The space of Bogros and the deep inguinal venouscirculation. Surg Gynecol Obstet 174: 355–358
4. Henry AK (1936) Operation for femoral hernia by a mid-line extra-peritoneal approach: with a preliminary note on the use of this route forreducible inguinal hernia. Lancet 1: 531–533
5. Hureau J (1994) The space of Bogros and the interparieto-peritoneal
spaces. In: Bendavid R (ed) Prostheses and abdominal wall hernias. RG Landes, Austin, TX, pp 74–81
6. Koontz AR (1963) Historical analysis of femoral hernia. Surgery 53:551–555
7. Mackay JY (1889) The relations of the aponeuroses of the transversalisand internal oblique muscles to the deep epigastric artery and to theinguinal canal. In: Cleland J (ed) Memoirs and memoranda inanatomy, vol 1. Williams and Norgate, London, pp 142–145
8. McEvedy PG (1950) Femoral hernia. Ann R Coll Surg Engl 7: 484–496
9. McVay CB, Anson BJ (1940) Composition of the rectus sheath. AnatRec 77: 213–225
10. Monroe A (1964) Femoral hernia: the lower approach. In: Nyhus LM,Harkins HN (eds) Hernia. J B Lippincott, Philadelphia, PA, pp 199–207
11. Munshi IA, Wantz GE (1996) Management of recurrent and perivas-cular femoral hernias by giant prosthetic reinforcement of the visceralsac (GPRVS). J Am Coll Surg 182(5): 417–422
12. Read RC (1995) Surgical comments on the Bogros thesis. PostgradGen Surg 6: 15–17
13. Read RC (1992) Cooper’s posterior lamina of transversalis fascia.Surg Gynecol Obstet 174: 426–434
14. Retzius AA (1858) Some remarks on the proper design of the semi-lunar lines of Douglas. Edinburgh Med J 3: 685–687
15. Rouviere H (1912) Anatomie humaine descriptive, topographique etfonctionelle. Masson, Paris
16. Stoppa RE (1995) The preperitoneal approach and prosthetic repair ofgroin. Hernias. In: Nyhus LM, Condon RE (eds) Hernia. 4th ed. JBLippincott, Philadelphia, PA, pp 188–210
17. Testut L, Latarjet A (1948) Traite d’anatomie humaine—Toure pre-mier. G Dovin, Paris
18. Tyson RR, Reichle FA (1972) Retropubic femorofemoral bypass anew route through the space of Retzius. Surgery 72: 401–403
19. Wantz GE (1993) The technique of giant prosthetic reinforcement ofthe visceral sac performed through an anterior groin incision. SurgGynecol Obstet 176: 497–500
692

Laparoscopic bowel mobilization combined with intraoperativecolonoscopic polypectomy in patients with an inaccessible polyp ofthe colon
K. Smedh,1 S. Skullman,2 A. Kald,2 B. Anderberg,2 P.-O. Nystrom2
1 Department of Surgery, Central Hospital, Central Hospital, S-721 89 Va¨sterås, Sweden2 Department of Surgery, Colorectal Unit, University Hospital, Linko¨ping, Sweden
Received: 5 May 1996/Accepted: 19 September 1996
AbstractBackground:The purpose of this report was to describe asimple technique suitable for polyps where circumstances ofthe bowel anatomy prevent complete access and control ofthe colonoscopic procedure.Methods:By combining laparoscopic mobilization of thebowel with colonoscopic polypectomy, previously inacces-sible polyps could be snared in two patients.Results:Both patients had 3-cm large sessile adenomas inthe sigmoid colon safely removed, and they returned homewithin a day.Conclusions:The described procedure increases the safetyof the otherwise difficult polypectomy and also avoids lap-arotomy with enterotomy or bowel resection as the alterna-tive.
Key words: Laparoscopy — Colonoscopy — Colonicpolyp
In patients with colonic adenomas that are located behind amucosal fold or a sharp bowel bend, it sometimes can beimpossible to get a good endoscopic view to snare the polypsafely. This is most common in the sigmoid colon. It can bedifficult to assess the full extension of the polyp and itspotential malignancy or to get representative biopsies. Insuch cases the polyp is usually resected at laparotomy, or, inrecent years, by laparoscopically assisted techniques [2, 3].A laparoscopic-assisted full-thickness endoscopic polypec-tomy has recently been described for colonic lesions toolarge to be safely removed colonoscopically [1].
In patients with impaired access to colonic polyps a
surgical procedure is described whereby laparoscopic bowelmobilization alone has been combined with colonoscopicpolypectomy in order to reduce the operative procedure.
Technique
The patient is placed in the lithotomy position. After insufflation of gas thecamera port is placed just above or beneath the umbilicus and additionalports are introduced just outside the rectus muscle in each fossa. Thecolonic segment is mobilized from its lateral peritoneal attachments so thatit can be easily moved by atraumatic Babcock forceps. The colonoscope isintroduced through the anus and the polyp is identified. By rotating andstretching the bowel with Babcocks it is now possible to get a good viewto assess the resectability of the polyp and to procede with snare polypec-tomy if justified.
Results
We have performed this combined laparoscopic and endo-scopic technique in two patients, both with 3-cm large sig-moid polyps not possible to remove by simple colonoscopydue to their localization. Both our patients had uneventfulrecovery and histology showed tubulovillous adenomaswith moderate dysplasia.
Discussion
This simple technique of combining laparoscopic mobiliza-tion of the bowel with colonoscopic polypectomy is suitablefor polyps which are resectable with colonoscopy in prin-ciple but where circumstances of the bowel anatomy pre-vent complete access and control of the procedure. After thebowel has been mobilized there is always the possibility toproceed to resection if the polyp appears malignant or largerand more sessile than expected. There is also excellent con-Correspondence to:K. Smedh
Surg Endosc (1997) 11: 643–644
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

trol of potential transmural thermal injury as the externalbowel surface of the polypectomy site is under direct in-spection with the laparoscope. By avoiding a bowel resec-tion the postoperative course is much easier and morestraightforward and the patient can return home within aday.
The described procedure increases the safety of the oth-erwise difficult polypectomy while it also avoids bowel re-section as the alternative. We submit that it will be cost-effective, too, because it avoids uncertainty concerning the
completeness of the polypectomy and hence repetetive en-doscopies are unnecessary.
References
1. Beck DE, Karulf RE (1993) Laparoscopic-assisted full-thickness endo-scopic polypectomy. Dis Colon Rectum 36: 693–695
2. Guillou PJ, Darzi A, Monzon JR (1993) Experience with laparoscopiccolorectal surgery for malignant disease. Surg Oncol 2(Suppl 1): 43–49
3. Monson JRT, Hill ADK, Darzi A (1995) Laparoscopic colonic surgery.Br J Surg 82: 150–157
644

Letters to the editor
The totally extraperitoneal laparoscopic hernia repair
We read with interest the paper by Vanclooster and col-leagues [11] and commend their contribution to this proce-dure. However, we would offer three comments:
First, totally extraperitoneal laparoscopic hernia repairwas developed by Dulucq [1–3] in 1989/90 and by Mc-Kernan [7] not a great deal later. While it seems legitimatefor others to publish their own technical variations, devel-opments, and outcomes, we strongly support recent remind-ers [6] that journal editors and their peer referees owe thereader a duty of diligence: they should insist that authorsexercise proper scholarship by giving credit where it is due.Otherwise the uninformed reader may assume originalityand the informed may infer plagiarism, where the authorintended neither.
Second, the mesh configuration suggested by Van-clooster et al. was presented by one of us several years ago[4, 10]. However, the concept of amputating the inferior andlateral corner ‘‘so the mesh fits better on the iliac vesselsand the psoas muscle’’ is flawed, since it has subsequentlybeen reported [12] that recurrences may occur dorsal/inferior to this inferolateral corner. The most extensive pos-sible coverage of the psoas muscle belly is therefore appro-priate.
Third, the need for mesh fixation remains debatable.However, to fix the cranial border to ‘‘prevent early migra-tion or slipping’’ is illogical: In our joint experience of over1,000 cases and, to our knowledge in all reports in the worldliterature, recurrences pass uniformly caudal to the inferiorborder of the prosthesis. Fixation of the inferior medial partof the mesh to Astley Cooper’s ligament alone [5] may notoffend against the original tension-free notion of Stoppa [8,9] nor interfere with the mechanics of prosthesis retention.To fix the superior border to points that move relative to oneanother within a musculofascial structure contravenes bothprinciples.
Finally, on a minor point, if the structure annotated as‘‘D’’ in Fig. 1 is the testicular vascular bundle, where is thevas deferens?
Despite these comments we congratulate the authors ontheir low complication rate.
References
1. Dulucq J-L (1991) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneale en retrope´ritoneoscopie. CahChir 79: 15–16
2. Dulucq J-L (1992) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneal en pre´-peritoneoscopie. Chirur-gie 118(1–2): 83–85
3. Dulucq J-L (1992) The treatment of inguinal hernias by implantationof mesh through retroperitoneoscopy. Postgrad Gen Surg 4: 173–174
4. Fiennes AGTW, Taylor RS (1994) Learning laparoscopic hernia re-pair. In: Inguinal hernia, advances or controversies? Arregui M, NaganR (eds) Radcliffe, Oxford, pp 475–482
5. Fiennes AGTW, Himpens J, Dulucq J-L (1994) Preperitoneoscopicgroin hernioplasty, current synthesis. Surg Endosc 8(8): 989
6. Horton R, Smith R (1996) Time to redefine authorship (editorial). BrMed J 312: 723
7. McKernan JB (1993) Laparoscopic extraperitoneal repair of inguino-femoral herniation. Endosc Surg Allied Tech 1(4): 198–203
8. Stoppa R, Petit J, Abourachid H (1973) Proce´deoriginal de plastie deshernies de l’aine. L’interposition sans fixation d’une prothe`se en tullede Dacron par voie me´diane pre´peritoneale. Chirurgie 99: 119
9. Stoppa RE, Rives JL, Warlaumont CR (1984) The use of Dacron in therepair of hernias of the groin. Surg Clin North Am 64: 269–285
10. Taylor RS, Fiennes AGTW (1992) A tension free modification of theDulucq preperitoneal laparoscopic hernioplasty. Min Inv Ther 1(Suppl1): 101
11. Vanclooster P, Meersmann AL, de Gheldere CA, Van de Ven CK(1996) The totally extraperitoneal laparoscopic hernia repair. SurgEndosc 10: 332–335
12. Vivekanadan S, Fiennes AGTW (1995) Totally extraperitoneal groinhernioplasty: mechanism of delayed indirect recurrence. Min Inv Ther4(Suppl 1): 55
A. Fiennes
Department of SurgerySt George’s Hospital Medical SchoolCranmer TerraceLondon, SW17 ORE, United Kingdom
J. Himpens
Department of Digestive SurgeryUniversity Hospital Ste PierreRue Haute 201B-1000 Brussels, Belgium
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 696

The author replies
We thank you for the opportunity to answer the letter of Mr.Fiennes. First of all, we certainly do acknowledge that Mr.Dulucq and Mr. Mc Kernan were the pioneers of the extra-peritoneal laparoscopic hernia repair. Honor to whom honoris due. We did not intend to pretend to be the pioneers ofthis technique. We wished only to describe the technique theway we perform it, to describe our own findings, and to givea fair report of our preliminary results.
The reason for cutting the inferolateral corner is not justthat we think it fits better on the iliopsoas but also becausewe are afraid to cause damage to the nerves running on it bydissecting unnecessarily high on the muscle. Since the meshmeasures 15 × 15 cm, we do not think we compromise thestrength of the repair by merely removing a small piece ofits inferolateral corner. We think that dissecting very highon the muscle just to position the whole inferolateral cornerof the mesh flat on the muscle is unnecessary and danger-ous.
We do agree totally that fixation of the mesh is unnec-
essary provided the mesh is large enough, which is obvi-ously the case when using a 15 × 15 cm mesh. In fact, wehave not fixed the mesh since January 1996.
We also agree that the vas deferens is not clearly seen onFig. 1. We chose this shot because of the clearly visiblelarge direct defect.
C. de Gheldere
Heilig Hart ZiekenhuisKolveniersvest 20B-2500 LIERBelgium
P. Vanclooster
Bouwelsesteenweg 62560 NijlenBelgium
Surg Endosc (1997) 11: 697
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The influence of pneumoperitoneum on the peritoneal implantation offree intraperitoneal cancer cells
Recently Hubens et al. published an interesting article en-titled ‘‘The influence of a pneumoperitoneum on the peri-toneal implantation of free intraperitoneal colon cancercells’’ [2]. They reported on the possible implantation ofcancer cells at trocar wounds at the moment of deflation ascells are forced through these wounds by the pressure gra-dient created by the pneumoperitoneum during laparoscopicsurgery for malignant disease. We would like to point outthat this ‘‘chimney effect,’’ as originally described by us,can occur during the entire laparoscopic procedure and notonly at the moment of deflation, as leakage of CO2 along-side trocars during surgery is impossible to prevent with theexisting trocars [3]. Consequently, deflation of the pneumo-peritoneum by letting CO2 escape through one of the trocarsbefore pulling these trocars out of the abdomen will notprevent the occurrence of entrapment of cancer cells in thetrocar wounds.
We fully agree with the authors on the possible advantageof gasless laparoscopy as this could prevent the ‘‘chimneyeffect.’’ In our experimental work we found significantly lesstumor growth at the port sites following gasless laparoscopicsurgery for colon cancer in the rat as compared to laparoscopicsurgery using a CO2 pneumoperitoneum. This techniqueseems promising to treat malignant disease laparoscopically.
References
1. Bouvy ND, Marquet RL, Jeekel J, Bonjer HJ (1996) Impact of gas (less)laparoscopy and laparotomy on peritoneal tumor growth and abdominalwall metastases. Surg Endosc 10: 551
2. Hubens G, Pauwels M, Hubens A, Vermeulen P, Van Marck E, EyskensE (1996) The influence of a pneumoperitoneum on the peritoneal im-plantation of free intraperitoneal colon cancer cells. Surg Endosc 10:809–812
3. Kazemier G, Bonjer HJ, Berends FJ, Lange JF (1995) Port site metas-tases after laparoscopic colorectal surgery for cure of malignancy. Br JSurg 82: 1141–1142
G. Kazemier1
F. J. Berends1
N. D. Bouvy1
J. F. Lange2
H. J. Bonjer1
1 Department of SurgeryUniversity Hospital Rotterdam-DijkzigtDr Molewaterplein 403015 GD, RotterdamThe Netherlands2 Department of SurgerySt. Clara HospitalRotterdamThe NetherlandsCorrespondence to:G. Kazemier
Surg Endosc (1997) 11: 698
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The author replies
We thank Dr. Kazemier et al. for their kind remarks and fullyagree with them that gas leakage can occur during the entireprocedure with subsequent implantation of tumor cells at thetrocar sites. At the moment we are conducting further experi-mental studies on the possible effects of gas leakage on tumorcell implantation and the ‘‘chimney effect,’’ as they havecalled it. Results will be ready for publication soon.
G. Hubens
Department of SurgeryUniversity HospitalUniversity of AntwerpWilrijkstraat 102650 EdegemBelgium
Surg Endosc (1997) 11: 699
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

News and notices
New Address for the European Association forEndoscopic Surgery (E.A.E.S.)
Effective January 1, 1997, the new correspondence, telephone, and faxnumbers of the E.A.E.S. office are:
E.A.E.S. Office, c/o Mrs. Ria Palmen
Luchthavenweg 81Unit 1.425657 EA EindhovenThe Netherlandsor: P.O. Box 3355500 AH VeldhovenThe NetherlandsTel: +31 40 2525288Fax: +31 40 2523102
Volunteer Surgeons NeededNorthwestern Nicaragua LaparoscopicSurgery Teaching Program,Leon, Nicaragua
Volunteer surgeons are needed to tutor laparoscopic cholecystectomy forthis non-profit collaboration between the Nicaraguan Ministry of Health,the National Autonomous University of Nicaragua, and Medical TrainingWorldwide. The program consists of tutoring general surgeons who havealready undergone a basic laparoscopic cholecystectomy course. MedicalTraining Worldwide will provide donated equipment and supplies whenneeded.
For further information, please contact:
Medical Training WorldwideRamon Berguer, MD, ChairmanTel: 707-423-5192Fax: 707-423-7578e-mail: [email protected]
Fellowship in Minimally Invasive SurgeryGeorge Washington Medical CenterWashington, DC USA
A one-year fellowship is being offered at the George Washington Univer-sity Medical Center. Interested candidates will be exposed to a broad rangeof endosurgical Education and Research Center. Active participation inclinical and basic science research projects is also encouraged.
For further information, please contact:
Carole Smith202-994-8425
or, send curriculum vitae to:
Dr. Jonathan M. SackierDirector of Endosurgical Education and ResearchGeorge Washington University Medical CenterDepartment of Surgery2150 Pennsylvania Avenue, N.W.6B-417Washington, DC 20037, USA
Essentials of Laparoscopic SurgerySurgical Skills UnitUniversity of DundeeScotland, UK
Under the direction of Professor A. Cuschieri the Surgical Skills Unit isoffering a three-day practical course designed for surgeons who wish toundertake the procedures such as laparoscopic cholecystectomy. This in-tensely practical program develops the necessary operating skills, empha-sizes safe practice, and highlights the common pitfalls and difficultiesencountered when starting out. Each workshop has a maximum of 18participants who will learn both camera and instrument-manipulation skillsin a purpose-built skills laboratory. During the course there is a live dem-onstration of a laparoscopic cholecystectomy. The unit has a large libraryof operative videos edited by Professor Cuschieri, and the latest books onendoscopic surgery are on display in our Resource area. Course fee in-cluding lunch and course materials is $860.
For further details and a brochure please contact:
Julie Struthers, Unit Co-ordinatorSurgical Skills UnitNinewells Hospital and Medical SchoolDundee DD1 9SYTel: +44 382 645857Fax: +44 382 646042
Advanced Endoscopic SkillsSurgical Skills UnitUniversity of DundeeScotland, UK
Each month Professor Cuschieri Surgical Skills Unit offers a 41⁄2 daycourse in Advanced Endoscopic Skills. The course is intensely practicalwith ‘‘hands on’’ experience on a range of simulated models. The programis designed for experienced endoscopic surgeons and covers advanceddissection techniques, extracorporeal knotting techniques, needle control,suturing, internal tying technique, stapling, and anastomotic technique.Individual workstations and a maximum course number of 10 participantsallows for personal tuition. The unit offers an extensive collection of sur-gical videos and the latest books and publications on endoscopic surgery.In addition, participating surgeons will have the opportunity to see liveadvanced laparoscopic and/or thoracoscopic procedures conducted by Pro-fessor Cuschieri and his team. The course is endorsed by SAGES. Coursefee including lunch and course materials is $1850.
For further details and a brochure please contact:
Julie Struthers, Unit Co-ordinatorSurgical Skills UnitNinewells Hospital and Medical SchoolDundee DD1 9SYTel: +44 382 645857Fax: +44 382 646042
The Practical Aspects of Laparoscopic FundoplicationSurgical Skills UnitUniversity of DundeeScotland, UK
A three-day course, led by Professor Cuschieri, designed for experiencedlaparoscopists wishing to include fundoplication in their practice. The
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 700–702

course covers the technical details of total and partial fundoplication usingsmall group format and personal tuition on detailed simulated models.There will be an opportunity to observe one of these procedures live duringthe course. Maximum course number is six. Course fee including lunch is$1850.
For further details and a brochure please contact:
Julie Struthers, Unit Co-ordinatorSurgical Skills UnitNinewells Hospital and Medical SchoolDundee DD1 9SYTel: +44 382 645857Fax: +44 382 646042
Courses at George Washington University EndosurgicalEducational and Research Center
George Washington University Endosurgical Educational and ResearchCenter is proud to offer a wide range of surgical endoscopy courses. Thesecourses include advanced laparoscopic skills such as Nissen fundoplica-tion, colon resection, common bile duct exploration, suturing, as well assubspecialty courses. Individual surgeons needs can be met with privatetuition. The Washington D.C. area is a marvelous destination to visit forrecreational pursuits which can be arranged by the facility to suit yourpersonal agenda.
For further details please contact:
Carole Smith:Department of Surgery2150 Pennsylvania Avenue NW6BWashington, DC 20037, USATel: (202) 994-8425
Courses at the Royal Adelaide Centre forEndoscopic Surgery
Basic and Advanced Laparoscopic Skills Courses are conducted by theRoyal Adelaide Centre for Endoscopic Surgery on a regular basis. Thecourses are limited to six places to maximize skill development and tuition.Basic courses are conducted over two days for trainees and surgeons seek-ing an introduction to laparoscopic cholecystectomy. Animal viscera insimulators is used to develop practical skills. Advanced courses are con-ducted over four days for surgeons already experienced in laparoscopiccholecystectomy who wish to undertake more advanced procedures. Awide range of procedures are included, although practical sessions can betailored to one or two procedures at the participants request. Practical skillsare developed using training simulators and anaesthetised pigs.
Course fees: $A300 ($US225) for the basic course and $A1,600($US1,200) for the advanced course.
For further details and brochure, please contact:
Dr. D. I. Watson or Professor G. G. JamiesonThe Royal Adelaide Centre for Endoscopic SurgeryDepartment of SurgeryRoyal Adelaide HospitalAdelaide SA 5000 AustraliaTel: +61 8 224 5516Fax: +61 8 232 3471
Advanced Laparoscopic Suturing and SurgicalSkills Courses
MOET InstituteSan Francisco, CA, USA
This intensive hands-on training program is intended to help the surgeondevelop proficiency in the essential laparoscopic surgical techniques.A sequence of progressively challenging exercises has been designed
to enable the surgeon to improve his or her laparoscopic dexterity,efficiency, and creativity. Exact and meticulous technique is emphasized sothat the surgeon can apply these skills with confidence. Personal instructionis provided by Zoltan Szabo, Ph.D., F.I.C.S., Director of the MOETInstitute, and surgeons are allowed to progress their own pace. Each par-ticipant has sole use of a laparoscopic training station equipped withhigh-quality clinical laparoscopic equipment and instrumentation. In-animate, animal tissue, and optional live animal models are utilized. Fea-tures of these program include: fluently choreographed instrumentmovements; economy of movement and ‘‘flawless’’ technique; needle andsuture handling skills (2-0 to 7-0); precision suturing, knotting, ligature,and anastomosis techniques; atraumatic, hemostatic tissue handlingand dissection; optimal angles of approach (coaxial alignment of setupand geometry of port positioning); laparoscopic surgical strategy, tech-nical nuances, and troubleshooting; visual perception problems and solu-tions; magnified eye-hand coordination; and two-handed (ambidextrous)technique.
Courses are offered year-round by individual arrangement. The MOETInstitute is accredited by the Accreditation Council for Continuing MedicalEducation (ACCME) to provide continuing medical education for physi-cians and designates these CME activities for 20–40 credit hours in Cat-egory 1 of the Physician’s Recognition Award of the American MedicalAssociation. These programs are also endorsed by the Society of Gastro-intestinal Endoscopic Surgeons (SAGES).
For further information, please contact:
Wanda Toy, Program AdministratorMicrosurgery & Operative Endoscopy Training (MOET) Institute153 States StreetSan Francisco, CA 94114, USATel: (415) 626-3400Fax: (415) 626-3444
Courses at WISEWashington Institute for Surgical EndoscopyWashington, DC, USA
The Washington Institute of Surgical Endoscopy is pleased to offer thefollowing courses:
Laparoscopic antireflux and hiatal hernia surgery (July 14–15, 1997); Lap-aroscopic management of the common bile duct and difficult cholecystec-tomy (May 15–16, August 11–12, November 10–11, 1997); Laparoscopiccolon and rectal surgery (June 20–21, September 15–16, December 4–5,1997). Also, courses for operating room nurses and technicians will be runon a monthly basis and personal instruction and preceptorship is available.
For further information, please call:
Carole SmithWashington Institute of Surgical Endoscopy2150 Pennsylvania Avenue, N.W.Washington, DC 20037Tel: 202-994-9425
4th International Meeting on Laparoscopic SurgeryMay 1–7, 1997Berne, Switzerland
Main topic: Acute appendicitis: Standard treatment and the role of lapa-roscopic surgery
For further information, please contact:
Mrs. Caroline ZürcherKlinik für Viszerale und TransplantationschirurgieUniversität BernInselspitalCH-3010 Bern, SwitzerlandTel: +41 31 632 97 22Fax: +41 31 632 97 23
701

European Course on Laparoscopic Surgery(French language) May 13–16, 1997(English language) November 18–21, 1997Brussels, Belgium
Course director: G.B. Cadiere
For further information, please contact:
Administrative SecretariatConference Services s.a.Avenue de l’Observatoire, 3 bte 17B-1180 Bruxelles
Tel: (32 2) 375 16 48Fax: (32 2) 375 32 99
Joint Euro Asian Congress of Endoscopic Surgery5th Annual Congress of the European Association forEndoscopic surgery (EAES)3rd Asian-Pacific Congress of Endoscopic SurgeryJune 17–21, 1997Istanbul, Turkey
The Congress will include a joint postgraduate course EAES/SAGES/ELSA on June 17th. For information and registration:
SETUR Congress DepartmentCumhuriyet Cad. No. 10780230 ElmadagIstanbul, TurkeyTel: (90.212) 23003 36Fax: (90.212) 240 82 37
Fellowships in Minimally Invasive SurgeryThe University of Pittsburgh Medical CenterPittsburgh, PA, USA
One year fellowships in advanced minimally invasive surgery in bothgeneral and thoracic surgery are being offered at the University of Pitts-burgh Medical Center beginning on July 1, 1997. Requirements includecompletion of residency training programs in the desired area. The fellow-ships include a competitive salary and travel allowance.
Interested candidates should send a letter of inquiry with curriculum vi-tae to:
Philip R. Schauer, MD (General Surgery) orJames Luketich, MD (Thoracic Surgery)The University of Pittsburgh Medical Center3471 Fifth AvenueSuite 300Pittsburgh, PA 15213-3221
Fellowships in Laparoscopic SurgeryStaten Island University HospitalStaten Island, NY USA
A one year fellowship, to start July 1, 1997, in advanced laparoscopicsurgery is being offered at Staten Island University Hospital. The selectedfellow will be exposed to many advanced general laparoscopic surgeriesincluding: hiatal hernia repair, splenectomy, adrenalectomy, bowel resec-tion, and others. Participation in research projects will be encouraged.
For further information, please contact:
Barbara ColemanCoordinator, Surgical residency programTel: 718-226-9508
9th International MeetingSociety for Minimally Invasive Therapy
July 14–16, 1997Kyoto, Japan
Scientific program to include: Plenary, Parallel, Poster, and Video sessions.Host Chairman: Professor Osamu Yoshida, Department of Urology, KyotoUniversity, 54 Shogoin Kawahara-sho, Sakyo, Kyoto 606, Japan. Phone: +8175 751-3328, Fax: +81 75 751-3740. This meeting coincides with the GionFestival in Kyoto, one of the greatest festivals in Japan.
For further information, please contact:
Secretariat of SMIT 9th Annual International Meetingc/o Academic Conference Planning383 Murakami-choFushimika, Kyoto 612 JapanTel: +81 75 611-2008Fax: +81 75 603-3816
6th World Congress of Endoscopy Surgery ‘‘Roma 98’’6th International Congress of European Associationfor Endoscopic Surgery
June 3–6, 1998Rome, Italy
The program will include: the latest, original high quality research; sym-posia; plenary lectures; abstract presentations (video, oral, and posters);EAES and SAGES postgraduate courses, OMED postgraduate course ontherapeutic endoscopy; working team reports; educational center and learn-ing corner; meeting of the International Society of Nurses and Associates;original and non original scientific reports; and a world expo of newtechnology in surgery.
For further information, please contact:
Congress Secretariat: Studio EGAViale Tiziano, 1900196 Rome, ItalyTel: +39 6 322-1806Fax: +39 6 324-0143
702

First results of laparoscopic gastrostomy
K. Peitgen, M. K. Walz, U. Krause, F. W. Eigler
Department of General Surgery, University of Essen, Hufelandstraße 55, D-45122 Essen, Germany
Received: 5 March 1996/Accepted: 31 July 1996
AbstractBackground:Laparoscopic gastrostomy as an alternative toopen gastrostomy was introduced with various technicalvariants 5 years ago. However, long-term results of thesenew methods are still lacking.Methods:From 4/1993 to 2/1996, laparoscopic gastrosto-mies were performed on 42 patients (50.9 ± 15.6 [24–71]years) with esophageal stenosis in locally advanced hypo-pharyngeal (17 patients) or oropharyngeal (nine patients)carcinoma, incurable esophageal carcinoma (13 patients)and cerebral dyspagia (three patients). Operating time was38 ± 11 min [15–65 min]. Procedure-related mortality was0%. Major complications occurred in 2/42 (4.7%) patients;minor complications were found in 4/42 (9.4%) patients.During a total usage time of 427 months, 14 stoma infec-tions occurred (0.11 infections/100 days).Conclusion:Laparoscopic gastrostomy allows a safe, fast,and cheap reestablishment of enteral nutrition. The proce-dure is minimally invasive and can also be performed underlocal anesthesia. It has become our method of choice inpatients with malignant, nonresectable subtotal stenosis ofthe hypopharynx or esophagus.
Key words: Laparoscopy — Gastrostomy — Enteral nutri-tion
Percutaneous endoscopic gastrostomy (PEG) has become asafe and effective alternative to surgical gastrostomy in pa-tients who require enteral access or gastric decompression[11]. Technical considerations, however, limit the applica-tion of PEG. In patients with subtotal stenosis or a completeobstruction of the hypopharynx or esophagus, e.g., as seenin locally advanced hypopharyngeal or esophageal carci-noma, surgical gastrostomy is indicated [3]. Recently, lap-aroscopic gastrostomy tube implantation has been intro-duced in miscellaneous technical variants as an alternativeto surgical open gastrostomy and to PEG [6, 8, 16, 20, 23,
24]. We introduced laparoscopic gastrostomy as a routineprocedure for patients with total or subtotal esophageal ste-nosis under palliative therapy 30 months ago [23] and here-by present our first long-term results.
Methods
From April 1993 to February 1996, laparoscopic gastrostomies have beenperformed in 42 patients (24 male, 18 female; age 50.9 ± 15.6 [24–71]years). Twenty-eight patients presented with locally advanced hypopha-ryngeal (17 patients) or oropharyngeal (nine patients) carcinoma and 13patients suffered from incurable esophageal carcinoma with subtotal ste-nosis or complete obstruction of the esophagus. Oral nutrition and gastro-scopic pertubation were not possible in all these cases. One patient sufferedfrom a neurologically caused dysphagia after severe head injury; two otherpatients had severe cerebral dysphagia after meningitis (one patient) orremoval of a cerebral tumor (one patient).
Three patients suffered from liver cirrhosis due to alcohol abuse. Onepatient with a hypopharyngeal carcinoma had a previous PEG that wasremoved 3 months prior to laparoscopic gastrostomy. At laparoscopy, onlya thin occluded scar approximately 5 cm long at the former PEG insertionsite was found, and it was left in place. Here, laparoscopic gastrostomycould be performed without problems 2 cm distal to the former PEG in-sertion site.
Thirty-four patients had adjuvant or palliative therapy concerning theirprimary disease (10 patients chemotherapy, 15 patients radiotherapy, ninepatients combined chemo-/radiotherapy) prior to laparoscopic gastrostomy.
Six patients had previous upper abdominal surgery: Three had gastricresections (Billroth I) 8, 11, and 15 years prior to gastrostomy; two otherpatients had an open cholecystectomy 5 and 10 years before gastrostomy.Another patient had an open cholecystectomy with common bile ductexploration 15 years ago. In these six cases, we performed an open lapa-roscopy, choosing a 1.5-cm incision in the umbilical region. After openingthe peritoneum under visual control, we then inserted a trocar-sheath andinsufflated the abdomen under laparoscopic control.
The procedures were performed by eight surgeons. Forty-one patientshad general anesthesia during the procedure; one patient had local anes-thesia with 60 ml of 0.25% bupivacaine and intravenous sedation with 200mg propofole.
Our operative technique for the laparoscopically assisted gastrostomyhas been described in detail recently [23]. As experience progressed, thistechnique has been slightly modified: After creating a pneumoperitoneumof 12 mmHg using a Veress needle under general anesthesia, two 10-mmtrocars and one 5-mm trocar are placed into the abdominal cavity. The first10-mm trocar is inserted below the umbilicus, the second 10-mm trocar isplaced into the left lower quadrant under laparoscopic control. The opticequipment is then adapted to this second trocar. This modification allowsa good exposure of the stomach. A 5-mm trocar is placed into the rightupper quadrant for an atraumatic grasper.Correspondence to:K. Peitgen
Surg Endosc (1997) 11: 658–662
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The anterior wall of the stomach is identified at the region of thecorpus. Using a needle-holder and a grasper, three full-thickness stitches(2-0; e.g., Dexon) are applied, creating a triangle at the level of the stomachwall. In order to fix the corresponding ones at the end of the proceduresubcutaneously, both ends of the sutures are pulled through the abdominalwall by a special awl beneath the left costal margin (Storz, Germany; No.26173 AK).
A 1-cm stab incision of the skin and fascia is then performed in thecenter of the skin-level triangle built by the three sutures. Under laparo-scopic control, the anterior wall of the stomach is punctured percutane-ously, exactly in the center of the two corresponding triangles at the skinlevel and at the stomach level in a strict rectangle to the stomach wall.Through the 18-gauge needle, a guidewire is inserted into the stomach (Fig.1). A 26-French dilator with a peel-away sheath (e.g., C-Pli-26-38; Cook,Monchengladbach, Germany) is pushed over the guidewire into the stom-ach percutaneously. After removing the inner dilator, a 24-French urinarycatheter (e.g., Foley-catheter, Ru¨sch, Kernen, Germany) is placed throughthe maintaining peel-away sheath into the stomach. After inflating theballoon of the catheter, the stomach is then pulled to the abdominal walland the sutures are fixed under traction and progressive reduction of thepneumoperitoneum. At the end of the procedure the correct placement ofthe tube is confirmed radiographically (Figs. 2, 3).
Feeding through the tube commenced 12 to 24 h postoperatively. After2 days of feeding with water, tea, and other liquids, the patients wereinstructed to apply normal, mashed foods into the tube and to maintain theirnutritive habits as close as possible to the time prior to their disease. TheFoley catheter was routinely changed once after 10 to 14 days. Furtherexchanges depended on actual needs. The last 32 of our 42 patients re-ceived a skin-level gastrostomy button device 2 weeks after laparoscopicgastrostomy during outpatient treatment.
Data of all patients have been collected prospectively. All patients wereroutinely seen once a week in the first month. Further follow-ups were keptup by contact with the patients’ family doctors. If possible, data are ex-pressed as mean ± mean standard error (M ± SEM).
Results
The laparoscopic gastrostomies could be performed suc-cessfully in all cases. The mean duration of the procedurewas 38 ± 11 min (15–65 min). In the three patients aftergastric resection, remarkable laparoscopic adhesiolysis wasnecessary in order to identify the corpus region and thegastroduodenal anastomosis. In the three patients after cho-lecystectomy, only moderate adhesiolysis was necessary.Operating time (53 ± 6 [45–75] min; first cut to last su-ture) in the six patients with prior surgery was significantlylonger (p < 0.05, Student’st-test) compared to the 36 pa-tients without prior surgery to the abdomen (34 ± 4 [20–60]min).
None of the patients died related to the procedure. Onepatient with a hypopharyngeal carcinoma died of a myocar-dial infarct 3 days after surgery; another patient with anesophageal carcinoma died 4 days after surgery due to asevere pneumonia based on an esophagopulmonary fistulawhich developed 2 days after surgery.
Fig. 1. The three stay sutures are placed, creating a triangle at the stomach wall for the future three-point gastropexy. The stomach is punctured and theguidewire inserted.
Fig. 2. Radiography of a laparoscopic gastrostomy (patient No. 3, total esophageal stenosis due to hypoharyngeal carcinoma).
Fig. 3. Radiography of a laparoscopic gastrostomy after Billroth I resection (patient No. 26, total esophageal stenosis due to hypoharyngeal carcinoma).
659

In one patient with a complete stenosis of the loweresophagus due to a cardia carcinoma, a gastric perforationwas noticed radiologically 5 h after gastrostomy. This pa-tient suffered from acute abdominal pain. At laparotomy, asmall lesion of the gastric wall was found at a 5-cm distancemedially to the stoma. After suturing of this lesion, thefurther course of this patient was uneventful. The genesis ofthis injury remains unclear, but most likely was caused byunskilled use of the grasping forceps. In another patient, aleakage of contrast fluid was suspected intraoperatively bya falsely interpreted radiography. The suspected perforationof the posterior wall could be excluded by a small midlineincision. No further major postoperative complications re-lated to the procedure were observed.
In four procedures, the transgastric fixation sutures werecut by the stab incision (one case) or torn apart during cath-eter placement (three cases). In three cases, the suturescould be repeated laparoscopically without problems. In onecase, the suture was refixed after moderate enlargementthrough the stoma incision. In one patient with a hypertro-phic left liver lobe due to severe cirrhosis, an additional5-mm trocar had to be inserted in order to hold the lobeaside with a palpation probe.
The mean usage time is now 10.4 ± 1.3 (1–25) months.To date (February 28th, 1996), 12 patients have died of theirprimary disease after 7.8 ± 6.2 (1–15) months with theirgastrostomies; 30 patients are still alive with their gastros-tomies after 9.2 ± 8.1 (1–31) months. During a total usagetime of 12,819 days (427 months), 14 stoma infections oc-curred (0.11 infections in 100 days). One diabetic patientdeveloped a dumping syndrome with attacks of hypoglyce-mia after stoma feeding. These were treated by insuline-dose adaptation and antisecretoric medication. No bleedingevents, episodes of diarrhea, tube displacements, stomaleakages or other complications occurred during long-termfollow-up. One gastrostomy was removed without problemsin the patient with severe head injury after 4 weeks whendysphagia resolved.
Thirty-six of 40 patients (excluding two patients whodied within 3 days after surgery) were able to nourish them-selves mainly on normal sieved foods. Four of the survivingpatients were unable to use mashed foods, mostly due tosocial reasons, and therefore applied pharmaceutically pre-pared liquid food. Bolus feeding and continuous feedingwere both possible in all patients.
Discussion
Placement of feeding tubes is a common procedure for gen-eral surgeons [3, 12, 22]. The introduction of PEG haschanged and improved surgical practice [5, 19]. However,this technique is contraindicated or not feasible under cer-tain conditions. Ascites, previous gastric or other surgery tothe upper abdomen, severe esophageal stenosis due to tu-mors of the oro-/epi-/hypopharynx or the esophagus presentcontraindications to PEG. In these cases, a surgical gastros-tomy is still indicated (Table 1).
We have developed a laparoscopic variant of the classicKader-/Stamm gastrostomy [23] on patients with subtotal ortotal esophageal and used it routinely in the last 34 months.The essential features of our procedure are the transabdom-
inal fixation sutures, the wire-guided dilator (which ensuressafe and tight catheter placement), and the large cathetersizes (which allow easy feeding with normal mashed foods).
Prior surgery to the upper abdomen does not limit thefeasibility of laparoscopic gastrostomy. After only minortechnical modifications (‘‘open’’ laparoscopy, laparoscopicadhesiolysis) we were able to perform laparoscopic gastros-tomies in six patients after previous upper abdominal op-erations. No further trocar accesses were needed. The op-erating time was lengthened significantly, but postoperativecomplications, food intake, and hospital stay were equalcompared to the patients without previous surgery. To ourknowledge, there is no other description of laparoscopicgastrostomy after upper abdominal surgery.
The laparoscopically applied and percutaneously placedsutures are most important for safety reasons. They alloweasy and precise placement of the needle, guidewire, andcatheter. Furthermore, they prevent peritonitis in case of anearly accidental tube loss. Additionally, tube changes arefacilitated. In comparison to other variants of laparoscopicgastrostomies [8, 9], nonabsorbable fixation devices are notneeded. Thus the risk of secondary perforation due to gastricwall necrosis should be reduced. In case of inadvertent in-traoperative rupture of these sutures, laparoscopic reappli-cation is possible. No special catheters are needed as pro-posed by other authors. In our experience, intraoperativeradiography control using a water-soluble contrast liquid ismandatory in order to exclude leakage either due to inad-vertent gastric perforation or insufficient fixation. In thepatient (number 36 in our series) with a gastric wall rupture,this lesion was not detected by laparoscopic control. Rou-tine intraoperative radiography would have detected the le-sion immediately.
Many technical modifications of laparoscopic gastros-tomies have been published since the first description in1991 [24] (Table 2). Most authors used modifications of theconventional Stamm-type gastrostomy first described byRussell [26] using stay sutures [1, 21, 30], T-fasteners oranchors [8, 9], a combination of stay and pursestring sutures[14, 17], fibrin glue [29], and various catheters (Malecot,Foley, suprapubic catheters, Moss tube) in various sizesfrom 12 to 18 French.
The majority of authors [1, 6, 20, 21, 30] used generalanesthesia for their procedures; only two [10, 17] also report
Table 1. Indications for laparoscopic gastrostomy in 42 patients (March1993–February 1996)
Indication PatientsAbdominal pathologyor prior surgery
Oropharyngeal/laryngeal carcinoma
9 1 patient after gastric resection(Billroth I)
Hypopharyngealcarcinoma
17 2 patients after gastric resections(Billroth I)
1 patient after opencholecystectomy
Esophagealcarcinoma
13 3 patients with liver cirrhosis
2 patients after opencholecystectomy
Dysphagia 3 1 polytrauma, 1 patient aftercerebral tumorremoval, 1 patient aftermeningitis
660

on laparoscopic gastrostomies under local anesthesia in in-dividual indications. Gasless laparoscopy as an alternativeapproach to gastrostomy has also been reported [29].
The laparoscopically modified Janeway gastrostomy[13, 18, 20] forms a gastric tube by using a special linearstapling device and thus forms a potentially continent andirrigable stoma. Since a laparoscopic stapler and two maga-zines are required for this technique, this procedure is moredifficult to perform and more expensive than the Stamm-type procedures. Long-term results have not yet been re-ported. Until 1995, only 11 cases in two different modifi-cations had been documented in the literature [13, 18, 20].Furthermore, the potential continence of this variant re-mains debatable [27].
Usually, laparoscopic gastrostomy is a permanent pro-cedure. However, it can be easily undone by simple removalof the catheter, if indicated. Complete restitution is achievedafter three to five days without complications. In our series,one gastrostomy in a patient with cerebral dysphagia afterpolytrauma with severe brain damage was removed after 4weeks without problems. In contrast to our method, removalof Janeway-type gastrostomies requires additional surgery[7, 13, 16, 18]. In comparison to the traditional gastrostomy,postoperative pain is reduced, enteral feeding is possiblewithin 12 h, and hospitalization is short [10]. These facts areof major importance, especially in patients with palliativetreatment. Additionally, palliative therapy (e.g., chemo-therapy, radiation therapy)—if indicated—can be appliedearlier compared to open gastrostomy.
In contrast to the PEG, normal mashed food can prin-cipally be used for nutrition due to the large catheter lumen.This is of psychological and practical importance for thepatients and also reduces costs. Also, endoscopic techniquesdo not uniformly secure the tube to the abdominal wall. The
latter may induce possible complications, including leakage,accidental early tube removal, bowel obstruction, intraper-itoneal catheter migration, intestinal fistulas, and necrosis ofthe stomach or abdominal wall because of excessive trac-tion. There is some information that suggests that the out-come of PEG is experience- and discipline-related [2, 28].
Many references indicate a lower morbidity of PEG inshort-term studies compared to conventional gastrostomies[12, 25, 28] or nasogastric feeding [22]. However, only fewdata exist concerning results of long-term use of PEG andits complications [15, 22]. Our long-term complication rateof 0.11 on 100 usage days reflects the usually overestimatedmorbidity of surgical gastrostomies [12, 28] quite well. Onthe contrary, other series reporting on conventional Stamm-type gastrostomies demonstrated a significantly lower intra-operative morbidity but no significantly different long-termmorbidity compared to PEG [2, 22]. Complications relatedto aspiration [4] should not occur in our patients, as all butthree patients were unable to swallow due to complete orsubtotal esophageal stenosis.
Our results after 42 laparoscopic gastrostomies showthat this technique allows a safe, fast, and cheap reestab-lishment of enteral nutrition in patients with hypopharyn-geal or esophageal stenosis. The procedure has the well-known advantages of minimally invasive surgical tech-niques and can also be performed under local anesthesia. Ithas become our method of choice in patients with malig-nant, nonresectable subtotal stenosis of the hypopharynx oresophagus. Regarding the practical advantages of laparo-scopic gastrostomies and the possibility of using normalmashed foods, further indications for laparoscopic gastros-tomies under local anesthesia should be considered in casesof dysphagic patients requiring long-term gastrostomy feed-ing.
Table 2. Published clinical results of laparoscopic gastrostomy 1992–1996
Reference Year n Catheter type/size Trocars Technical features AnesthesiaTime(minutes) Complications
7 1992 3 18 Fra 3 Anisoperistaltic Janewaygastrostomy, two30-mm endoscopicstaplers
General No data None
21 1992 9 Various/18 Fr 3 2 stay sutures General 35–60 1 gastric bleeding(→ laparotomy)
6 1993 13 Foley 3 No data General No data None8 1993 3 Foley/18 Fr 2 4 T-fasteners General No data None1 1993 3 Moss tube 3 2 stay sutures General 30 No data
10 1994 22 Foley or Malecot/12–14 Fr
2–3 2–4 anchors, dilator-set,peel-away sheath
17 general,5 local
20.5 (10–25) 1 dislocation (→laparotomy)1 death due toperitonitis
30 1994 10 Suprapubic catheter/15 Fr
4 2 stay sutures General No data None
17 1994 9 MIC silicongastrostomy tube
2 2 pursestring sutures + 2stay sutures
6 general,3 local
22 (15–33) 1 dislodgment(→ laparotomy)
18 1995 5 20 Fra 2 Isoperistaltic Janewaygastrostomy, two30-mm endoscopicstaplers
General 30 (25–35) None
This study 1996 42 Foley/24 Fr 3 3 stay sutures, guidewire,dilator set, peel-awaysheath
41 general,1 local
38 (15–65) 1 gastric rupture(→ laparotomy)
a 20-Fr Foley catheter for the first days and at regular intervals for enteral feeding
661

References
1. Albrink MH, Hagan K, Rosemurgy AS (1993) Laparoscopic insertionof the Moss feeding tube. J Laparoendosc Surg 3: 531–534
2. Apelgren KN, Zambos J (1989) Is percutaneous better than open gas-trostomy? A clinical study in one surgical department. Am Surg 55:596–600
3. Au FC (1993) The Stamm gastrostomy: a sound procedure. Am Surg59: 674–675
4. Burtch GD, Shatney CH (1985) Feeding gastrostomy: assistant orassassin? Am Surg 51: 204–207
5. Campos AC, Butters M, Meguid MM (1990) Home enteral nutritionvia gastrostomy in advanced head and neck cancer patients. HeadNeck 12: 137–142
6. Chambon JP, Wurtz A, Saudemont A, Bosse JL, Chevalier D, Quan-dalle P (1993) Celioscopic gastrostomies and jejunostomies. Ann Chir47: 311–315
7. Cossa JP, Marmuse JP, Lecomte P, Le Goff JY, Johanet H, BenhamouG (1992) Tubular gastrostomy using celioscopy. Presse Med 21:1519–1521
8. Duh QY, Way LW (1993) Laparoscopic gastrostomy using t-fastenersas retractors and anchors. Surg Endosc 7: 60–63
9. Edelman DS, Unger SW, Russin DR (1991) Laparoscopic gastros-tomy. Surg Laparosc Endosc 1: 251–253
10. Edelman DS, Arroyo PJ, Unger SW (1994) Laparoscopic gastrostomyversus percutaneous endoscopic gastrostomy: a comparison. Surg En-dosc 8: 47–49
11. Gauderer MW (1992) Gastrostomy techniques and devices. Surg ClinNorth Am 72: 1285–1298
12. Grant JP (1988) Comparison of percutaneous endoscopic gastrostomywith Stamm gastrostomy. Ann Surg 207: 598–603
13. Haggie JA (1992) Laparoscopic tube gastrostomy. Ann R Coll SurgEngl 74: 258–259
14. Horbach T, Reck T, Ko¨ckerling F (1994) Perkutane laparoskopischeGastrostomie (PLG) unter Verwendung einer laparoskopischenTabaksbeutelklemme. Min Inv Chir 3: 179–183
15. Hull MA, Rawlings J, Murray FE, Field J (1993) Audit of outcome of
long-term enteral nutrition by percutaneous endoscopic gastrostomy.Lancet 341: 869–872
16. Lathrop JC, Felix EJ, Lauber D (1991) Laparoscopic Janeway gas-trostomy utilizing an endoscopic stapling device. J Laparoendosc Surg1: 355–359
17. Lee WJ, Chao SH, Chang S, Chen KM (1994) Laparoscopic assistedgastrostomy tube placement. J Laparoendosc Surg 4: 201–204
18. Meyer G, Rau H, Strauss T (1995) Die laparoskopische Gastrostomienach Janeway. Chirurg 66: 719–723
19. Miller RE, Castlemain B, Lacqua FJ, Kotler DP (1989) Percutaneousendoscopic gastrostomy results in 316 patients and review of literature.Surg Endosc 3: 186–190
20. Modesto VL, Harkins B, Calton WC Jr, Martindale RG (1994) Lap-aroscopic gastrostomy using four-point fixation. Am J Surg 167: 273–276
21. Neufang T, Ko¨hler H, Lepsien G, Lu¨dtke FE (1992) Die perkutanelaparoskopische Gastrostomie (PLG). Min Inv Chir 1: 34
22. Pargger H, Kern C (1995) Technische Aspekte der Rehydrierung. ChirPrax 50: 13–22
23. Peitgen K, Walz MK, Krause U, Kruschke A, Eigler FW (1994) Lap-aroscopic Kader fistula. Chirurg 65: 213–216
24. Reiner DS, Leitman IM, Ward RJ (1991) Laparoscopic Stamm gas-trostomy with gastropexy. Surg Laparosc Endosc 1: 189–192
25. Ruge J, Vazquez RM (1986) An analysis of the advantages of Stammand percutaneous endoscopic gastrostomy. Surg Gynecol Obstet 162:13–16
26. Russell TR, Brotman M, Norris F (1984) Percutaneous gastrostomy: anew simplified and cost-effective technique. Am J Surg 184: 132–137
27. Shellito PC, Malt RA (1985) Tube gastrostomy: techniques and com-plications. Ann Surg 201: 180–185
28. Stern JS (1986) Comparison of percutaneous endoscopic gastrostomywith surgical gastrostomy at a community hospital. Am J Gastroen-terol 81: 1171–1173
29. Viani PM, Poggi RV, Pinto A (1995) Gasless laparoscopic gastros-tomy. J Laparoendosc Surg 5: 245–249
30. Wolfram T, Albrecht R, Voigtsberger P (1994) Perkutane laparosko-pische Gastrostomie. Chir Prax 48: 63–68
662

Port site electrosurgical (diathermy) burns during surgical laparoscopy
P. D. Willson,1 J. D. van der Walt,2 D. Moxon,1 J. Rogers1
1 Academic Surgical Unit, Royal London Hospital, London, E1 1BB, United Kingdom2 Department of Histopathology, Royal London Hospital, London, E1 1BB, United Kingdom
Received: 12 August 1996/Accepted 26 November 1996
AbstractBackground:Direct and capacitive coupling of diathermycurrent have been reported as causes of occult injury duringsurgical laparoscopy.Methods:In order to determine the incidence of electrosur-gical injury adjacent to metal and plastic cannulas, skinbiopsies at 19 port sites used for monopolar electrosurgerywere analyzed for coagulative necrosis. Prior to surgery thecannulas were randomized to either metal or plastic.Results:Coagulative necrosis was observed at nine electro-surgery port sites compared to only one control (x2 44.872;df 4 1; 0.05 >p > 0.02). Plastic cannulas affordedno greater protection from skin burns than metal cannulas.Conclusions:Burns may be the result of direct or capacitivecoupling to metal cannulas or capacitive coupling to theskin edge across plastic cannulas. The potential exists forburns to other tissues also in close proximity to a cannulaused for electrosurgery.
Key words: Electrosurgery — Surgical diathermy — Ca-pacitive coupling — Direct coupling — Patient burns
Inadvertent monopolar electrosurgical burns occurring out-side laparoscopic view have been reported following surgi-cal laparoscopy [5, 6]. Although these have been attributedto direct coupling (live contact) or capacitive coupling(electromagnetic induction) the true incidence with whichthese phenomena cause patient injury is unknown. Thisstudy presents definitive evidence of burns caused by elec-trosurgery during surgical laparoscopy.
Methods
Nineteen port sites in 15 consecutive patients undergoing laparoscopiccholecystectomy or fundoplication were randomized to receive either ametal or plastic cannula for electrosurgical instruments.
Following surgery, skin biopsies were taken from the lower edge of thecannula wound. This was fixed in formalin, prepared for histological sec-tioning and stained with hematoxylin and eosin. Control biopsies weretaken in the same patient from the lower edge of a cannula wound not usedfor electrosurgery.
Sections were viewed after staining by the same consultant pathologist(J.D.W.) who was blind to both the cannula type and biopsy site. Coagu-lative necrosis within the epidermis was graded 0–III (Table 1).
Results
Eleven plastic and eight metal cannulae were used for elec-trosurgical instruments. Nine of the 19 electrosurgery portwounds had evidence of coagulative necrosis, nine showedno coagulative necrosis, and one biopsy was equivocal.Thirteen of the 15 control biopsies showed no coagulativenecrosis, one revealed coagulative necrosis, and one wasequivocal (Table 2). Equivocal biopsies were affected bycrush artefact.
The higher incidence of coagulative necrosis in the dia-thermy cannula group is statistically significant both whenall diathermy wounds are included together (x2 4 4.872[Yates corrected];df 4 1; 0.05 > p > 0.02) and whenseparated out by the type of cannula used (x2 4 7.342;df4 2; 0.05 >p > 0.02). Equivocal biopsies were incorpo-rated with the group showing no necrosis.
Discussion
Coagulative necrosis occurs after sudden tissue ischemia,chemical injury, and thermal injury. The only likely causefor the coagulative necrosis seen in these patients is thermalinjury from monopolar diathermy.
Monopolar electrosurgery involves current passing be-tween an active electrode and a return plate across the pa-tient. The cannula represents one of several return paths tothe patient plate. Burns may occur along any part of thereturn path if the power density in the tissue exceeds 7.5W/cm2 [3]. The burns demonstrated in this study show thatinadvertent coupling to the cannula occurs during electro-surgical laparoscopy and is more commonly associated with
Correspondence to:P. D. Willson, Department of Surgery, St Mary’s Hos-pital, Praed Street, London W2 1NY, United Kingdom
Surg Endosc (1997) 11: 653–654
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

those ports where diathermy is used. This may be due todirect contact or arcing to a metal cannula from an activeelectrode (direct coupling) or due to electromagnetic induc-tion to a metal cannula or directly to skin across a plasticcannula (capacitive coupling) [2–4].
The single burn seen in the control group is most likelydue to direct coupling to the control cannula.
Although skin burns of the type identified in this studyare of little clinical consequence to the patient, the studyindicates that monopolar electrosurgical energy can betransmitted across both metal and plastic cannulas and in-jure tissue in close proximity to the cannula. Such proximity
to bowel, however, may lead to more serious injury [5]. Inaddition, the data demonstrate that it is not the characteris-tics of the cannula or insulation materials which are theimportant determinant of skin burns but rather the closeproximity of the wound to the electrosurgical instrument.Plastic cannulas afford no greater protection than metal can-nulas against skin burns although the mechanism with plas-tic cannulas is capacitive coupling whereas with metal can-nulas direct coupling may also be a cause.
Theoretically the only electrosurgical instruments whichcan avoid this potential from both direct and capacitivecoupling are bipolar instruments where the return electrodeis guaranteed to be at the site of application of the surgicalcurrent. Coaxially shielded instruments are an alternativemeans of reducing the risk from capacitive coupling andinsulation breaks but not from direct coupling.
In general, reduction in the probability of electrosurgicalburns may be achieved by using low diathermy generatorsettings (30 W or less) and low-voltage wave forms (blendor cut) [1].
References
1. Department of Health (1994) Diathermy injury during laparoscopic sur-gery. Safety Action Bull SAB(94)38.
2. McAnena OJ, Willson PD (1993) Diathermy in laparoscopic surgery. BrJ Surg 80: 1094–1096
3. Tucker RD, Voyles CR, Silvis SE (1992) Capacitive coupled straycurrents during laparoscopic and endoscopic electrosurgical proce-dures. Biomed Instrum Technol 26: 303–311
4. Voyles CR, Tucker RD (1992) Education and engineering solutions forpotential problems with laparoscopic monopolar electrosurgery. Ameri-can J Surg 164: 57–62
5. Willson PD, McAnena OJ, Peters EE (1994) A fatal complication ofdiathermy in laparoscopic surgery. Minim Invasive Ther 3: 19–20
6. Willson PD, van der Walt JD, Rogers J (1995) Electrosurgical couplingto a metal cannula causing skin burns during laparoscopic surgery.Minim Invasive Ther 4: 163–164
Table 1. Grading of epidermal burns
Grading Definition
0 No coagulative changesI Coagulative changes in the epidermis, all layers intactII Coagulative changes with loss of up to 50% of the
epidermisIII Coagulative changes with loss of over 50% of the
epidermis
Table 2. Epidermal burns by grade and cannula type
Burn grade
Electrosurgicalcannulas Nonelectrosurgical
cannulas(control)Plastic Metal
0 5 4 13I 2 1 0II 2 0 0III 2 2 1Crush artefact:
unable to assess 0 1 1
654

Prospective evaluation of a minimally invasive approach for treatmentof bile-duct calculi in the high-risk patient
M. Trias,1 E. M. Targarona,1 E. Ros,2 J. M. Bordas,3 R. M. Perez Ayuso,2 C. Balague,1 I. Pros,1 J. Teres2
1 Service of General and Digestive Surgery, Hospital Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain2 Gastroenterology Service, Hospital Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain3 Endoscopy Unit, Hospital Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain
Received: 17 May 1996/Accepted: 12 September 1996
AbstractBackground:The best approach to bile duct stones in high-risk patients is controversial. We showed in a randomizedtrial that open surgery had a morbi-mortality similar to thatof endoscopic sphincterotomy alone (ES) and less late bil-iary complications. The aim of this study was to evaluate aminimally invasive approach to duct stones in high-risk pa-tients compared with open surgery or ES alone.Methods:Sixty high-risk patients (mean age 80 years) sus-pected of duct stones were treated by ES + laparoscopiccholecystectomy (LC). High-risk factors were: age > 70years, Goldman cardiac index > 13, chronic pulmonary dis-ease, liver cirrhosis, neurologic deficit, and severe obesity.Results:ERCP success was 87%. Duct stones were found in75%. LC succeeded in 92%. Post-LC stay was 4 days. Over-all morbidity was 19% and mortality was 3%. Recurrentsymptoms (mean follow-up: 9 months) was 3.6%. Whencompared with open surgery or ES alone, ES + LC had asimilar morbi-mortality, but shorter postop stay (p < 0.001).Late symptoms appeared in 20% after ES alone vs 4% afteropen surgery or ES plus LC (p < 0.04).Conclusions:Combined ES + LC is an effective alternativeto open surgery or ES alone for treatment of duct stones inhigh-risk patients.
Key words: Bile duct stones — Laparoscopic cholecystec-tomy — Endoscopic sphincterotomy — High-risk patient— Elderly
It has been classically considered that morbidity and mor-tality following bile duct surgery increase with age andassociated disease [15, 18]. Before the rapid spread of lap-aroscopic surgery, endoscopic sphincterotomy (ES) leaving
the gallbladder ‘‘in situ’’ was proposed as an alternative toopen surgery in high-risk patients with bile duct calculi [19].We recently showed in a prospective and randomized trialthat open surgery and ES leaving the gallbladder ‘‘in situ’’had a similar immediate morbi-mortality in this subset ofpatients and that surgery prevented long-term biliary com-plications derived from the presence of the gallbladder [16].Logically, the next therapeutic approach to evaluate in thesepatients would be the applicability of minimally invasivetherapy. It has been shown that laparoscopic surgery can beapplied safely in elderly or high-risk patients [4, 9]. The bestaccepted policy for treatment of bile-duct stones in the lap-aroscopic era is the combined endoscopic-laparoscopic ap-proach [2, 12], but to our knowledge it has never beencompared with open surgery or endoscopic treatment. How-ever, a randomized trial becomes difficult once a new tech-nique is well accepted. Therefore, we present in this papera series of 60 consecutive patients, suspected of having bileduct stones and defined as high risk, treated with a mini-mally invasive approach. The results of this series have beencompared with those of a previous study by the same sur-gical team [16], with the analogous criteria of high-riskdefinition, in order to discover the potential advantages ofthe laparoscopic approach in this selected subset of patients.
Materials and methods
Between September 1991 and September 1994, we performed a prospec-tive and randomized trial in which we compared the early and late resultsof open surgery vs endoscopic sphincterotomy leaving the gallbladder ‘‘insitu’’ for treatment of bile-duct stones in high-risk patients; the results havebeen published elsewhere [16] and are summarized in Tables 1–3.
From October 94 to December 95, and following the same criteria as inthe previously cited study (outlined below), we tested the efficacy of alaparoscopic approach, associated with preoperative endoscopic sphincter-otomy (ES) if required, in a consecutive series of 60 symptomatic patientswith cholecystolithiasis and a clinical diagnosis of bile-duct stones.
All high-risk gallstone patients presenting with biliary pain, jaundice,Correspondence to:M. Trias
Surg Endosc (1997) 11: 632–635
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997
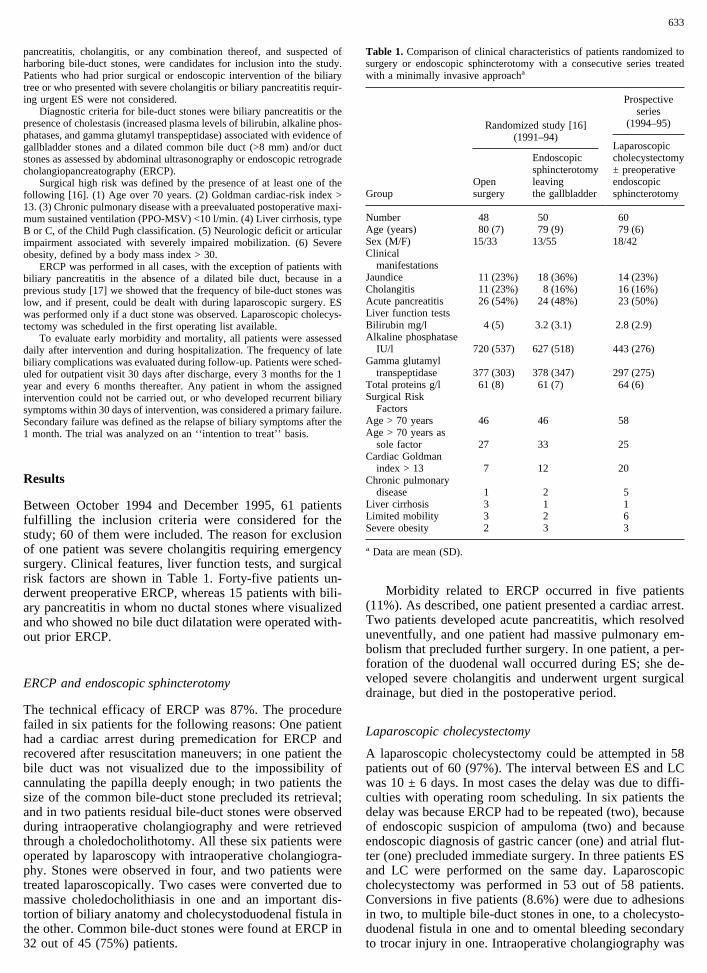
pancreatitis, cholangitis, or any combination thereof, and suspected ofharboring bile-duct stones, were candidates for inclusion into the study.Patients who had prior surgical or endoscopic intervention of the biliarytree or who presented with severe cholangitis or biliary pancreatitis requir-ing urgent ES were not considered.
Diagnostic criteria for bile-duct stones were biliary pancreatitis or thepresence of cholestasis (increased plasma levels of bilirubin, alkaline phos-phatases, and gamma glutamyl transpeptidase) associated with evidence ofgallbladder stones and a dilated common bile duct (>8 mm) and/or ductstones as assessed by abdominal ultrasonography or endoscopic retrogradecholangiopancreatography (ERCP).
Surgical high risk was defined by the presence of at least one of thefollowing [16]. (1) Age over 70 years. (2) Goldman cardiac-risk index >13. (3) Chronic pulmonary disease with a preevaluated postoperative maxi-mum sustained ventilation (PPO-MSV) <10 l/min. (4) Liver cirrhosis, typeB or C, of the Child Pugh classification. (5) Neurologic deficit or articularimpairment associated with severely impaired mobilization. (6) Severeobesity, defined by a body mass index > 30.
ERCP was performed in all cases, with the exception of patients withbiliary pancreatitis in the absence of a dilated bile duct, because in aprevious study [17] we showed that the frequency of bile-duct stones waslow, and if present, could be dealt with during laparoscopic surgery. ESwas performed only if a duct stone was observed. Laparoscopic cholecys-tectomy was scheduled in the first operating list available.
To evaluate early morbidity and mortality, all patients were assesseddaily after intervention and during hospitalization. The frequency of latebiliary complications was evaluated during follow-up. Patients were sched-uled for outpatient visit 30 days after discharge, every 3 months for the 1year and every 6 months thereafter. Any patient in whom the assignedintervention could not be carried out, or who developed recurrent biliarysymptoms within 30 days of intervention, was considered a primary failure.Secondary failure was defined as the relapse of biliary symptoms after the1 month. The trial was analyzed on an ‘‘intention to treat’’ basis.
Results
Between October 1994 and December 1995, 61 patientsfulfilling the inclusion criteria were considered for thestudy; 60 of them were included. The reason for exclusionof one patient was severe cholangitis requiring emergencysurgery. Clinical features, liver function tests, and surgicalrisk factors are shown in Table 1. Forty-five patients un-derwent preoperative ERCP, whereas 15 patients with bili-ary pancreatitis in whom no ductal stones where visualizedand who showed no bile duct dilatation were operated with-out prior ERCP.
ERCP and endoscopic sphincterotomy
The technical efficacy of ERCP was 87%. The procedurefailed in six patients for the following reasons: One patienthad a cardiac arrest during premedication for ERCP andrecovered after resuscitation maneuvers; in one patient thebile duct was not visualized due to the impossibility ofcannulating the papilla deeply enough; in two patients thesize of the common bile-duct stone precluded its retrieval;and in two patients residual bile-duct stones were observedduring intraoperative cholangiography and were retrievedthrough a choledocholithotomy. All these six patients wereoperated by laparoscopy with intraoperative cholangiogra-phy. Stones were observed in four, and two patients weretreated laparoscopically. Two cases were converted due tomassive choledocholithiasis in one and an important dis-tortion of biliary anatomy and cholecystoduodenal fistula inthe other. Common bile-duct stones were found at ERCP in32 out of 45 (75%) patients.
Morbidity related to ERCP occurred in five patients(11%). As described, one patient presented a cardiac arrest.Two patients developed acute pancreatitis, which resolveduneventfully, and one patient had massive pulmonary em-bolism that precluded further surgery. In one patient, a per-foration of the duodenal wall occurred during ES; she de-veloped severe cholangitis and underwent urgent surgicaldrainage, but died in the postoperative period.
Laparoscopic cholecystectomy
A laparoscopic cholecystectomy could be attempted in 58patients out of 60 (97%). The interval between ES and LCwas 10 ± 6 days. In most cases the delay was due to diffi-culties with operating room scheduling. In six patients thedelay was because ERCP had to be repeated (two), becauseof endoscopic suspicion of ampuloma (two) and becauseendoscopic diagnosis of gastric cancer (one) and atrial flut-ter (one) precluded immediate surgery. In three patients ESand LC were performed on the same day. Laparoscopiccholecystectomy was performed in 53 out of 58 patients.Conversions in five patients (8.6%) were due to adhesionsin two, to multiple bile-duct stones in one, to a cholecysto-duodenal fistula in one and to omental bleeding secondaryto trocar injury in one. Intraoperative cholangiography was
Table 1. Comparison of clinical characteristics of patients randomized tosurgery or endoscopic sphincterotomy with a consecutive series treatedwith a minimally invasive approacha
Group
Randomized study [16](1991–94)
Prospectiveseries
(1994–95)
Laparoscopiccholecystectomy± preoperativeendoscopicsphincterotomy
Opensurgery
Endoscopicsphincterotomyleavingthe gallbladder
Number 48 50 60Age (years) 80 (7) 79 (9) 79 (6)Sex (M/F) 15/33 13/55 18/42Clinical
manifestationsJaundice 11 (23%) 18 (36%) 14 (23%)Cholangitis 11 (23%) 8 (16%) 16 (16%)Acute pancreatitis 26 (54%) 24 (48%) 23 (50%)Liver function testsBilirubin mg/l 4 (5) 3.2 (3.1) 2.8 (2.9)Alkaline phosphatase
IU/l 720 (537) 627 (518) 443 (276)Gamma glutamyl
transpeptidase 377 (303) 378 (347) 297 (275)Total proteins g/l 61 (8) 61 (7) 64 (6)Surgical Risk
FactorsAge > 70 years 46 46 58Age > 70 years as
sole factor 27 33 25Cardiac Goldman
index > 13 7 12 20Chronic pulmonary
disease 1 2 5Liver cirrhosis 3 1 1Limited mobility 3 2 6Severe obesity 2 3 3
a Data are mean (SD).
633

performed in 49 patients and it showed bile duct stones insix. Two patients were converted, and in the remaining four,the stones were extracted by choledocholithotomy (threecases) or through the cystic duct (one case). Postoperativemorbidity occurred in six patients (10%). Three patients hadliver bed bleeding and two of them required reoperation.One patient presented a prolonged ileus. One of the patientsconverted to open surgery developed wound sepsis, and inanother, who was converted due to a distorted anatomy andseverely scarred gallbladder, a bile-duct transection oc-curred necessitating a hepaticojejunostomy. The patientdied of intraabdominal sepsis 10 days later. Overall mor-bidity (endoscopic plus laparoscopic) was 19% (11 patients)and overall mortality 3% (two patients).
Follow-up
A follow-up was carried out in 55 out of 58 (95%) patientswho were discharged. Mean follow-up was 9 ± 4 months.Two patients out of 55 (3.6%) developed recurrent symp-toms of biliary origin. In one patient with spilled stonesduring gallbladder retrieval, a stone discharge through theumbilicus was observed and required surgical exploration ofthe umbilical wound. A second patient developed obstruc-tive jaundice due to a pancreatic cancer not identified duringERCP or surgery, and a percutaneous stent was required.
Discussion
The therapeutic approach to bile duct stones has changeddramatically during recent years, especially in the elderlyand in patients with associated medical conditions, a subsetof patients traditionally considered poor surgical candidates.Surgery is a safe treatment for biliary stones, with mortalityrates of less than 0.5% for cholecystectomy and of 1.5% ifthe bile duct is explored [18]. Several series in the early1980s suggested that mortality increases sharply (up to30%) in the elderly or high-risk patient [15, 18], althoughthere was a lack of uniformity in the definition of ‘‘highrisk.’’ Surgical mortality rates have declined, however, inthe last decade. A survey of 12 series of patients older than70 years operated on for bile-duct stones published from1988 to 1992 showed a mortality range between 0 and 9%,and in eight series it was below 4% [3, 6]. With the aim ofreducing this morbidity and mortality, many authors haveproposed that the endoscopic extraction of calculi, leavingthe gallbladder, could be a useful alternative, with a lowerimmediate morbidity and mortality [19]. During recentmonths three prospective, randomized trials have shown thesafety of open surgery compared with ES as the only treat-ment of bile-duct stones in patients with cholecystolithiasis[5, 8, 16]. Two of these studies [5, 16] showed that theincidence of biliary symptoms during follow-up was higherin patients treated with the endoscopic approach in whichthe gallbladder was preserved than in those operated on. Theresults of one of these trials have been used as a reference[16] to evaluate the applicability of mimimally invasivetechniques in a series of elderly or high-risk patients oper-ated by the same team, and using the same criteria to definehigh risk.
In order to take advantage of a less aggressive surgicalapproach, it seems logical to apply laparoscopic techniques
Table 2. Technical efficacy and immediate morbidity and mortality; com-parison of the results of a randomized trial between open surgery and ESwith a consecutive series treated with a minimally invasive approach
Group
Randomized study [16](1991–94)
Prospectiveseries
(1994–95)
Laparoscopiccholecystectomy± preoperativeendoscopicsphincterotomy
Opensurgery
Endoscopicsphincterotomyleavingthe gallbladder
Primary failure 3 (6%) 6 (12%) 7 (11%)Immediate morbidity 11 (23%) 8 (16%) 11 (18%)Severe complications 4 5 5
Intraabdominal sepsis 3 (1a) — —Cholangitis — 4 (2a) 1 (1a)Pneumonia 1 (1a) — —Stroke — 1 (1a) —Cardiac arrest — — 1Bile-duct injury — — 1 (1a)Bleedingb — — 2
Minor complications 7 3 6Wound infection 4 — 1Pancreatitis — 1 2Atelectasis 2 — —Urinary infection 1 — 1Catheter sepsis — 2 —Hemoperitoneum — — 1Ileus — — 1
Immediate mortality 2 (4%) 3 (6%) 2 (3%)Pre treatment stay, days 11 (5) 11 (8) 11 (6)Post treatment stay, days 11 (8) 5 (4) 4.4 (4)*Overall stay, days 21 (9) 16 (10) 19 (8)**
a Died.b Both patients needed to be reoperated on.* p < 0.001 vs open surgery.
** p < 0.001 vs ES alone.
Table 3. Events during follow-up; comparison of the results of a random-ized trial between open surgery and ES with a prospective series treatedwith a minimally invasive approach
Group
Randomized study [16](1991–94)
Prospectiveseries
(1994–95)
Laparoscopiccholecystectomy± preoperativeendoscopicsphincterotomy
Opensurgery
Endoscopicsphincterotomyleavingthe gallbladder
Patients followed 43 46 53Biliary complications
during follow-up 3 (6%)* 10 (21%) 2 (3.6%)*Biliary colic 1 2 —Acute cholecystitis — 3 —Cholangitisa 2 2 —Jaundiceb — 3 1Umbilical stone
discharge — — 1Readmissions for
biliary complications 2 (4%)** 11 (23%) 1 (2%)**Reoperation —** 7 (15%) 1 (2%)**Endoscopy 2 (4%) 1 (2%) 1 (2%)
a All four patients had common bile-duct calculi.b Common bile-duct calculi in two patients.* p < 0.04 vs ES alone.
** < 0.01 vs ES alone.
634

in elderly and high-risk patients. At this moment the pre-ferred approach for bile duct stones is a combined one, withES preceding laparoscopic cholecystectomy (LC) [2, 10,11], although several series have shown the feasibility of apurely laparoscopic approach [12, 13]. When applied in theelderly or high-risk patient, there are specific aspects to bothERCP and LC that need to be considered. Regarding ERCP,it is well known that the frequency of ductal calculi anddilated ducts is higher in older than in younger patients;hence, endoscopic treatment is more challenging in theformer. In this series ERCP was successfully accomplishedin 87% of the patients in whom it was attempted, with amorbidity of 10% and a mortality of 2%. Recently, Deenit-chin et al. [1] related the outcome of ES to age in 1,103patients (921 younger than 80 years and 182 older than 80years) and found a similar success in stone retrieval al-though older patients needed more accessory maneuversthan younger ones (lithotripsy or stenting, 19% vs 9%) andhad higher morbidity (13% vs 7%) and mortality (1% vs0%). Another consideration is that laparoscopic surgerycould be more difficult in the elderly because these patientshave longer and more complicated histories of biliary dis-ease and are more likely to have peritoneal adhesions anddistorted anatomy. Also, there is a high proportion of pa-tients with previous upper abdominal surgery, additionallyincreasing technical difficultly. The conversion rate in thisseries was 8.6%, which compares favorably with the 10%rates[9] in other series of LC in the elderly. Finally, theincreased frequency of associated medical diseases makesthe perioperative control of the patient more difficult due tothe cardiopulmonary changes induced by pneumoperito-neum. In this series, in which 30% of patients had associ-ated cardiac disease, none had to be converted due to im-possibility of maintaining the pneumoperitoneum.
In our patients, most bile-duct stones were retrieved byendoscopic means. In a minority of patients, ductal stoneswere identified and treated during LC but two conversionswere necessary because of massive choledocholithiasis inone patient and a cholecystoduodenal fistula in another. Thedilemma that arises in trying to avoid a negative preopera-tive ERCP and pursuing laparoscopic exploration of the bileduct should be solved in future years.
During the late 1980s, and before the widespread use oflaparoscopic surgery, the general opinion among surgeons,supported by two prospective randomized trials [7, 14], wasthat the combination of ES plus open cholecystectomy wasnot superior to open surgery for patients with bile-duct cal-culi. Although comparative trials are lacking, most surgeonsnow prefer laparoscopic surgery preceded by ES. The use ofrandomized trials to scientifically prove the benefits of newalternative therapies is difficult when new treatment mo-dalities become widely used, as occurred with LC. Keepingthe objection in mind that this was not a randomized trial,the comparison of the results of this prospective series witha previous randomized trial from the same institution andthe same surgical team with analogous inclusion criteriapermits some conclusions to be drawn. The endoscopio-plus-laparoscopic approach had a similar success rate toopen cholecystectomy with bile-duct exploration, with asimilar overall morbidity and mortality. Follow-up data alsoshowed minimal morbidity of biliary origin in these patients.
The postoperative hospital stay was shorter in the pa-
tients treated with ES followed by LC than in those previ-ously submitted to open surgery (Table 2). However, theoverall duration of hospitalization was similar in both cho-lecystectomy groups. An important shortcoming of the en-doscopic-plus-laparoscopic approach in a busy general hos-pital is that cholecystectomy cannot be scheduled soon afterES. Thus, the mean delay was 10 days in our study.
To evaluate the advantages that minimally invasive sur-gery can offer to the elderly or high-risk patient with anintact gallbladder presenting with choledocolithasis, futuretrials should compare preoperative endoscopic therapy fol-lowed by LC with simultaneous LC and bile-duct explora-tion [10–12].
References
1. Deenitchin GP, Konomi H, Kimura H, Ogawa Y, Naritomi G, ChijiwaK, Trias M, Ikeda S (1995) Reappraisal of safety of endoscopic sphinc-terotomy for common bile duct stones in the elderly. Am J Surg 170:51–54
2. Erickson RA, Carlson B (1995) The role of ERCP in patients withlaparoscopic cholecystectomy. Gastroenterology 109: 252–263
3. Escarce JJ, Shea JA, Chen W, Quian Z, Schwartz JS (1995) Outcomesof open cholecystectomy in the elderly: a longitudinal analysis of21,000 cases in the prelaparoscopic era. Surgery 117: 156–164
4. Fried GM, Clas D, Meakins JL (1994) Minimally invasive surgery inthe elderly patient. Surg Clin North Am 74: 375–387
5. Hammarstro¨m LE, Holmin, Stridbeck H, Ihse I (1995) Long termfollow up of a prospective randomized study of endoscopic versussurgical treatment of bile duct calculi in patients with gallbladder insitu. Br J Surg 82: 1516–1521
6. Moreaux J (1995) Traditional surgical management of common bileduct stones: a prospective study during a 20 year experience. Am JSurg 169: 220–226
7. Neoptolemos JP, CarrLocke DL, Fossard DP (1987) Prospective ran-domised study of preoperative endoscopic sphincterotomy versus sur-gery alone for common bile duct stones. BMJ 294: 470–474
8. Panis Y, Suc B, Escat J (1995) Surgery versus endoscopic sphincter-otomy for choledocholithiasis: results of a prospective randomizedstudy. Gastroenterology 109: A431
9. Passone N, Navez B, Cambier E, Baert G, Richir Ch, Guiot P (1995)Cholecystectomie coelioscopique chez le sujet aˆge. Ann Chir 49: 291–295
10. Perissat J (1994) Operative treatment of common bile duct stones:laparoscopic cholecystectomy and endoscopic treatment. Eur J Gas-troenterol Hepatol 6: 857–863
11. Perissat J, Huibregtse K, Keane FGBV, Russell RCG, Neoptolemos JP(1994) Treatment of bile duct stones in the laparoscopic era. Br J Surg81: 799–810
12. Phillips EH (1994) Controversies in the management of common ductcalculi. Surg Clin North Am 74: 931–947
13. Phillips EH, Libermann M, Carroll BJ, Fallas MJ, Rosenthal RJ, HiattJR (1995) Bile duct stones in the laparoscopic era. Is preoperativesphincterotomy necessary? Arch Surg 130: 880–886
14. Stiegman GV, Goff JS, Mansour A, Pearlman N, Reveille RM, NortonL (1992) Precholecystectomy endoscopic cholangiography and stoneretrieval is not superior to cholecystectomy, cholangiography andcommon duct exploration. Am J Surg 163: 227–230
15. Targarona EM, Pros I, Trias M (1992) Tratamiento de la coledocoli-tiasis en el paciente de riesgo elevado. Med Clin (Barc) 98: 69–73
16. Targarona EM, Perez Ayuso RM, Bordas JM, Ros E, Pros I, MartinezJ, Teres S, Trias M (1996) Randomised trial of endoscopic sphincter-otomy with gallbladder left in situ versus open surgery for commonbileduct calculi in high-risk. Lancet 347: 926–929
17. Targarona EM, Balague´ C, Espert JJ, Perez Ayuso RM, Ros E, Na-varro S, Bordas JM, Teres S, Trias M (1995) Laparoscopic treatmentof acute biliary pancreatitis. Int Surg 80: 365–368
18. Tierney S, Lillemoe KD, Pitt HA (1995) The current management ofcommon duct stones. Adv Surg 28: 271–299
19. Winslet MC, Neoptolemos JP (1991) The place of endoscopy in themanagement of gallstones. Baillieres Clin Gastroenterol 5: 99–129
635

Original articles
How safe is ERCP to the endoscopist?
R. V. Cohen, M. A. Aldred, W. S. Paes, A. M. F. Fausto, J. R. Nucci, E. M. Yoshimura, E. Okuno, M. E. Garcia,L. M. Maruta, E. M. C. Tolosa
Division of Surgical Endoscopy, Health Physics, Occupational Medicine and Dosimetry Laboratory, University of Sa˜o Paulo, Sa˜o Paulo, Brazil
Received: 15 July 1996/Accepted: 7 November 1996
AbstractBackground:Interventional techniques in endoscopy suchas endoscopic retrograde cholangiopancreatography(ERCP) have greatly increased since laparoscopic cholecys-tectomy has become widespread; mainly these techniquesdeal with common bile duct stones. Fluoroscopy is usuallyemployed, and chronic exposure to X-ray, in spite of therelative low dose, can lead to potentially unhealthy condi-tions such as malignancies like bone marrow and other solidcancers. A median of 18 years of life is lost per fatal cancer,including the time of latency since exposure. Nor shouldone forget benign condition such as cataracts that can leadto partial or complete blindness and which surely impairlife’s quality.Methods:Simulated examinations were carried at the Uni-versity Hospital (Sa˜o Paulo, Brazil) using an anthropomor-phic phantom in place of the physician. Four sets of dosim-eters were placed in the forehead, neck, torso, and lowerabdomen (with and without a lead apron) and standardERCP fluoroscopic techniques were employed.Results:The dose equivalents were calculated and com-pared to the recommended exposure doses of national andinternational boards of radiation protection.Conclusions:Based on the results found and compared tostandards, working safely means: (1) A lead (0.5 mm thick-ness) apron is fundamental. Without it less than oneERCP\month should be performed. (2) With an apron, 23examinations/month are allowed. (3) No thyroid protectiongrants only 19 exams/month. (4) Performing ERCP withoutlead glasses is hazardous to the eye, allowing only sevenERCPs monthly.
Key words: ERCP — Radiological protection — Radiationexposure protection — Interventional laparoscopy — Com-mon bile duct stones management
The combination of endoscopic retrograde cholangiopan-creatography (ERCP) with endoscopic sphincterotomy andstone extraction has acquired an expanded role in the man-agement of choledocholithiasis in the minimal access sur-gery era [1, 2, 3]. During those procedures, fluoroscopic andradiographic images are taken with paramedical and medi-cal staff near the patients. Even if the level of exposure toX-rays during ERCP is low, it is important to stress that itis a chronic exposure that can lead to potentially unhealthyconditions such as malignancies and benign conditions suchas eye disorders (cataract) [7].
The goal of this paper is to evaluate the dose equivalentthat the medical staff is exposed to during exams (ERCPs)performed at the Division of Surgical Endoscopy, Univer-sity Hospital, University of Sa˜o Paulo, Brazil. The equiva-lent dose resulting from staff exposure was compared torecommended limits issued by international boards of ra-diation protection [8] and to Brazilian national standards[4]; then an ideal maximum number of examinations al-lowed per month and year was established in order to assureto the medical team the best protection against deleteriouseffects of ionizing radiation.
Methods
The endoscopic procedures were simulated by employing a recipient con-taining water as the patient and an anthropomorphic phantom (Aldersonphantom) as the endoscopist who has control of the fluoroscopic equipment(wearing a 0.5-mm-thickness lead apron). The position of the phantom waschosen to achieve the maximum exposure during ERCP, using data cal-culated by a radiation monitor (Radcal Corporation, model 9015; Wash-ington, DC) on radiation exposure. The phantom was set up in an uprightposition at a distance of 55 cm from the examination table. Each doseequivalent was calculated from the measurements of four thermolumines-cent dosimeters (TLD 100) located in different sites of the phantom: theforehead, neck, torso and lower abdomen (under and over the apron). Thedosimeters were calibrated at the Dosimetry Laboratory, Physics Institute,University of Sao Paulo [9, 12].
Measurements were performed for fluoroscopic and radiographic ex-posures, using four sets of TLDs. During fluoroscopy three sets weresubmitted to three different irradiation times (20, 40, and 60 min). Fluo-roscopy was simulated with consecutive displays of 85 kVp and 2.2 mA,breaking each 5 min. The last set of TLDs was submitted to an irradiation
Correspondence to:R. V. Cohen, Rua Wanderley, 1482 ap. 53, 05011-001Sao Paulo SP, Brazil
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 615–617

equivalent to six plain radiographic films. The plain films were obtained at85 kVp and 100 mA.
The quantity ‘‘dose-equivalent’’ (H) is limited to radiation protectionapplications and is calculated as the product of the absorbed dose (D) by aquality factor (Q) that takes into account the type of radiation (a, b, g, orn). Dose equivalent is measured in units of Sievert (Sv), e.g., 1 mSv—onemilliSievert—is equivalent to an energy of 103 Joules per 1 kilogram oftissue mass.
Results
The average dose equivalent, measured during fluoroscopyand performing the six static films, is shown on Table 1.
The estimated time of exposure to ionizing radiationduring the performance of ERCPs at the Division of Surgi-cal Endoscopy, University of Sa˜o Paulo, is 20 min andgenerally four films are taken. Bearing in mind that thepoints of measurement can be analogous to some anatomicparts, respectively the crystalline, thyroid, gonads, andwhole body (torso + abdomen), the total equivalent-dosewas calculated (Table 2).
Limits established by Brazilian standards (NationalCommission of Nuclear Energy, CNEN, Sa˜o Paulo, Brazil)and international boards (International Commission of Ra-diation Protection—ICRP, London, England) are shown onTable 3. Considering the limits of dose equivalents as astandard of working safely, according to CNEN-NE 3.01and ICRP 60, and the total doses obtained per procedure atthe Division of Surgical Endoscopy (Table 2), the maxi-mum number of procedures that the staff can perform safelywas determined (Table 4).
Discussion
The combination of endoscopic retrograde cholangiopan-creatography (ERCP) with endoscopic sphincterotomy (ES)and stone extraction has acquired an expanded role in themanagement of choledocolithiasis. With the rapid growth oflaparoscopic cholecystectomy (LC), the evaluation andtreatment of suspected common bile duct stones have beenlimited, and the main approach combined to LC to commonduct stones has been until now in many centers the combi-nation of ERCP and ES [1, 6, 11]. To perform those pro-cedures, exposure of the medical and paramedical staff toionizing radiation is required. Even though the exposition islow, it is continuous and may lead to hazardous conse-quences.
Information on the risk of cancer following radiationexposure comes from a large number of epidemiologicalstudies and has recently been reviewed by the United Na-tions Scientific Committee on the Effects of Atomic Radia-tion (UNSCEAR) and by the US Committee on the Bio-logical Effects of Ionizing Radiation (BEIR V)[5, 14]. Thepopulations that have been studied include:
1. Over 90,000 survivors of the atomic bombings of Hiro-shima and Nagasaki
2. 14,000 mostly male patients in the UK treated for anky-losing spondylitis with X-rays
3. 83,000 women in eight countries treated for cervical can-cer with X or gamma radiation
Very few studies have followed the entire population untilthe end of life. The temporal pattern of risk was assessed instudies as the Life Span Study [10] of A bomb survivors.Those studies showed that for the main cancer secondary toradiation exposure—leukemia—the peak is about 7 years ofexposure followed by a tailing off in risk. The relative risksdepend on the age at the time of exposure, dose level andrate, and if the individual who was dealing with ionizing
Table 1. Equivalent doses for medical and paramedical staff; fluoroscopyand radiographs
Dosimeters site
Equivalent dosesHT (mSv) for 1 hfluoroscopy
Equivalent dosesHT (mSv)6 films
Forehead 4.35 0.33Neck 5.50 0.31Torso (inside apron) 0.15 0.03Torso (outside apron) 4.79 0.32Lower abdomen (inside
apron) Nonmeasurable NonmeasurableLower abdomen (outside
apron)a 0.20 0.07
a Located below the table. Works as protection from ionizing radiation.
Table 2. Equivalent doses per procedure; calculated from Table 1
Site/organ
Equivalentdoses(fluoroscopy,mSv)
Equivalentdoses(radiographs,mSv)
Equivalentdoses(total)
Crystalline 1.45 0.22 1.67Thyroid 1.84 0.21 2.05Whole body—apron 0.050 0.02 0.07Whole body—no
apron 1.60 0.22 1.82Gonads—apron Nonmeasurable Nonmeasurable NonmeasurableGonads—no aprona 0.067 0.05 0.12
a Located below the table. Works as protection from ionizing radiation.
Table 3. Occupational limits of doses; yearly basis
Organ/site
Occupationallimits CNEN(yearly) mSv
Occupationallimits ICRP-60 (yearly) mSv
Whole body 50 20 (5-year basis)Crystalline 150 150Skin 500 500
Table 4. ERCP’s maximum number (monthly/yearly) where CNEN andICRP-60 limits are respected
Organs
Maximum allowedexams (CNEN, Brazil)
Maximum allowedexams (ICRP-60)
Year Month Year Month
Crystalline 89 7 89 7Thyroid 243 19 — —Whole body
(with apron) 714 57 285 23Whole body
(without apron) 27 2 10 0.8
616

radiation got a specific oncogen in his genoma. No oneshould forget that there are different temporal patterns ofrisk for different cancer types. For leukemia, after adjust-ment for age at exposure, the relative risk appeared to beconstant over time, mainly if the subject is constantly ex-posed as the staff that performs endoscopic procedures un-der fluoroscopy. For solid cancers, such as lung, breast,thyroid, and GI (colon and stomach) cancers, the relativerisk decreases about 10 to 20 years following exposure [13].Following leukemia, solid GI cancers, breast, lung, and thy-roid malignancies are the commonest neoplasias followingradiation exposure.
It is important to stress that those data are only relativeto deaths secondary to ionizing-radiation-induced cancers.Quality of life tends to decrease to important levels, if it’sconsidered the time taken for the diagnosis and treatment ofsecondary cancers. Besides neoplastic affections, in spite ofthe lack of significant statistical data, crystalline injury wasdescribed [14], and this benign condition can lead to afeared situation that may follow chronic exposition to ra-diation—complete blindness.
Keeping in mind all the potential hazards related tochronic exposure to ionizing radiation, and comparing thedose equivalent taken by the phantom to international stan-dards (Table 3), it is concluded that working safely means:
1. Wearing a lead apron (0.5-mm thickness) is fundamen-tal: without it, less than one ERCP should be performedper month; only four examinations should be performedin a period of 5 months.
2. With an apron, 23 exams/month are allowed.3. No thyroid protection grants only 19 exams per month.4. Performing ERCP without lead glasses is hazardous to
the eye, allowing only seven ERCPs per month.
Besides lead aprons, glasses and thyroid shields are impor-tant protective devices and should allow an increased num-ber of safe monthly examinations.
It must always be emphasized that radiation carcino-genic induction is a process with no threshold dose, e.g.,even for small doses the probability of ocurrence is not zero.Specialists set limits as a way to keep the incidence ofmalignancies at acceptably low levels. However, focusing
on benign effects such as cataracts, the limiting doses mightbe adopted as threshold doses.
References
1. Arregui M, Davis CJ, Akrush AM, Nagan R (1992) Laparoscopiccholecystectomy combined with endoscopic sphincterotomy and stoneextraction or laparoscopic choledocoscopy and electrohydraulic litho-tripsy for management of cholelithiasis with choledocolithiasis. SurgEndosc 6: 10–15
2. Cohen RV, Schiavon CA, Moreia L, Tolosa EMC (1994) What isminimally invasive surgery? In: Cohen RV (ed) Metabolic and sys-temic responses following interventional laparoscopy. RG Landes Bio-medical, Austin, TX
3. Cohen RV, Shiavon CA, Schaffa TD (1995) Laparoscopic cholecys-tectomy can be safely performed without intraoperative cholangiogra-phy. Surg Laparosc Endosc 5(2): 165–166
4. Comissa˜o Nacional de Energia Nuclear (1988-NE 3.01.) DiretrizesBasicas de Radioprotec¸ao, Brası´lia, Brasil
5. Committee on the Biological Effects of Ionising Radiation (BEIR V)(1990) Health effects of exposure to low levels of ionising radiation.National Academy of Sciences, National Academy Press, Washington,DC
6. Fink AS (1993) To ERCP or not to ERCP. That is the question. SurgEndosc 7(5): 375–376
7. Gray J, Ragozzino M, Gazzi R (1981) Normalized organ doses forvarious diagnostic radiologic procedures. Am J Radiol 137: 463–470
8. International Commission on Radiation Protection ICRP Publication60 (1990) Recommendations of the International Commission on Ra-diological Protection. Pergamon Press, Oxford
9. Nucci JR, Aldred WS, Paes AM, Okuna E (1995) Sistema de Moni-toracao Individual de Rotina do Laborato´rio de Dosimetria do Institutode Fısica da Universidade de Sa˜o Paulo. Presented at the SegundoCongresso de Seguridad Radiologica e Nuclear, Cusco, Peru, October23–27
10. Shimizu Y, Kato H, Nagai Y (1988) Life span study report 11. Part II:cancer mortality in the years 1950–1985 based on the recently reviseddoses (DS86). Hiroshima, RERF TR5-88
11. Surick B, Washington M, Ghazi A (1993) ERCP in conjunction withlaparoscopic cholecystectomy. Surg Endosc 7: 388–392
12. Tresniak P, Yoshimura EM, Cruz MT, Okuno E (1990) Brazilianfluorite-base dosimetric pellets: history and post-use review. RadiatProt Dosim 24: 167–170
13. Tucker MA, Meadows AT, Boice JD (1984) Cancer risk followingtreatment for childhood cancer. In: Boice JD, Fraumeni (eds) Radia-tion carcinogenesis: epidemiology and biological significance. RavenPress, New York, pp 211–224
14. UNNSCEAR (1988) Sources, Effects and Risks of Ionising Radiation.Report to the General Assembly, United Nations, New York
617

Long-term results after laparoscopic cholecystotomy in a child withsymptomatic gallstone disease
B. M. Ure, E. P. Eypasch, H. Troidl
II. Department of Surgery of the University of Cologne, Ostmerheimerstraße 200, 51109 Cologne, Germany
Received: 10 May 1996/Accepted: 29 May 1996
Abstract. Cholecystotomy has been suggested for symp-tomatic gallstone disease in selected children. This sugges-tion is supported by a potential reduction in the frequency ofthe so-called postcholecystotomy syndrome. To our knowl-edge, laparoscopic cholecystotomy has not been reportedyet. However, gallstone recurrence has been reported up to4 years after conventional cholecystotomy and therefore wewaited to publish our results for that period of time. A12-year-old girl with idiopathic symptomatic gallstone dis-ease and a normal kinetic of the gallbladder underwent lap-aroscopic cholecystotomy. The laparoscopic technique wassimilar to laparoscopic cholecystectomy but the gallbladderwas left in place and multiple gallstones were removed.Intraoperative cholecystoscopy revealed three additionalsmall stones. They were removed by subsequent lavage ofthe gallbladder. Choledocholithiasis was excluded by intra-operative cholangiography and the gallbladder was closedusing an Endo GIA. There were no intraoperative or post-operative events. The patient is free of complaints withoutrecurrent gallstones on ultrasound examination today, 4years after the operation. Laparoscopic cholecystotomy rep-resents a feasible alternative to laparoscopic cholecystec-tomy.
Key words: Cholelithiasis — Cholecystotomy — Laparos-copy — Children
Symptomatic gallstone disease is uncommon in childhood,but in recent years the frequency has been reported to beincreasing [1, 5, 7]. Cholecystectomy is recommended asstandard treatment for symptomatic gallstones in children.However, some reports on cholecystotomy in selected caseshave been published [7, 13]. Since the introduction of lap-
aroscopic cholecystectomy [4, 12, 15] numerous advantagesof this technique have been proven in adult series [15, 16]and it has been reported to be safe and feasible in children[6, 11, 18]. To our knowledge, laparoscopic cholecystotomyin children and the long-term results of the technique havenot been published yet.
Patient and methods
The patient was a 12-year-old girl who had suffered occasional attacks ofsevere upper abdominal pain since 6 months of age. Pain and nausea wereaggravated by food and in particular by fatty meals. There was no historyof jaundice and no family history of hemolytic disease. Ultrasound exami-nation revealed multiple stones in the gallbladder. The diameter of thecommon bile duct was 2.6 mm without evidence of choledocholithiasis.The volume of the gallbladder reduced from 32 ml to 13 ml after a stan-dardized meal. On plain x-ray and laboratory examinations there were nopathological findings.
The operation was performed under general anesthesia with the patientin prone position. The surgeon stood between the legs of the patient; oneassistant stood on the right and a second assistant on the left side [15]. A1-cm incision was made in the infraumbilical fold and the pneumoperito-neum was introduced with a Veress needle. The pressure was kept at 12mmHg maximum. A 10-mm 30° laparoscope was inserted and four addi-tional trocar sites were set in place (Fig. 1). The gallbladder was openedusing unipolar electrocoagulation and the gallstones were removed by agrasping forceps. Subsequent cholecystoscopy revealed three additionalstones which were removed by lavage and a suction device. Additionalstones of the common bile duct were excluded by cholangiography whichwas performed via a catheter through the cystic duct. The gallbladder wasclosed using a 11-mm Endo GIA (Auto Suture). The operation time was140 min; there was no blood loss.
Results
The patient had oral fluids the evening after the operationand regular meals on day 1. No postoperative complicationswere recorded. On discharge at day 3 the patient was free ofcomplaints. Today, 4 years after the operation there are nodiet restrictions, no attacks of abdominal pain, and no otherabdominal symptoms. On ultrasound examination there isno evidence for recurrence of gallstones.Correspondence to:B. M. Ure
Surg Endosc (1997) 11: 671–672
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

Discussion
Childhood cholelithiasis has been associated with severaldisorders, in particular with hemolytic disease [1, 5]. How-ever, in children with idiopathic gallstone disease gallstoneproduction is believed to be caused by a temporary vulner-ability [7]. Thus, removing the gallstones by cholecys-totomy and leaving the gallbladder in place has been sug-gested [7, 13]. This suggestion is supported by a potentialreduction in the frequency of the so-called ‘‘postcholecys-tectomy syndrome,’’ which has been reported in up to 42%of patients after cholecystectomy [2, 17]. In addition, thereis evidence for an association between cholecystectomy andcolorectal cancer [9]. An increased relative risk of up to 3.5times for right-sided colonic cancer in women has beenreported [8].
Robertson et al. [13] reported a series of nine patients onwhom they successfully performed cholecystotomy, five ofwhom were children with hereditary spherocytosis who un-derwent splenectomy in the same session. All nine patientswere asymptomatic 0.3–7.5 years after surgery. However, inone child with spherocytosis an asymptomatic gallstone wasdetected on ultrasound examination after 2 years. Molanderand Bergdahl [7] performed cholecystotomy in one childwith congenital spherocytosis and in six children with id-iopathic symptomatic gallstones. One of the six childrenunderwent cholecystectomy later on because of dyskinesiaof the gallbladder, but there is no follow-up information onthe remaining six children. Out of three other case reports[3, 10, 14] one child was free of complaints and free ofgallstones after 11 years [14]. Another patient was chole-cystectomized after 6 years for persisting symptoms due toa poorly functioning gallbladder [10]. Another patient un-derwent cholecystectomy 4 years later for recurrent gall-stones [3]. Therefore, it was decided to not publish thepresent case report until 4 years after cholecystotomy.
None of these authors had investigated the kinetic of thegallbladder by ultrasound or x-ray examination prior to cho-lecystotomy. In our opinion, this is essential for selecting
candidates for cholecystotomy. The function of the gall-bladder in our patient was normal before and after the op-eration on ultrasound examination.
Numerous advantages of laparoscopic compared to con-ventional cholecystectomy have been reported for adult pa-tients [15, 16]. In small series of children the technique wasperformed safely and effectively with a short hospital stayand recovery period [6, 11, 18]. We suggest that childrenwith idiopathic symptomatic gallstone disease and a normalfunction of the gallbladder may be candidates for laparo-scopic cholecystotomy. They may profit from the advan-tages of the laparoscopic as compared to the conventionaltechnique.
References
1. Bailey PV, Connors RH, Tracy TF, Cirilo S-A (1989) Changing spec-trum of cholelithiasis and cholecystitis in infants and children. Am JSurg 158: 585–588
2. Bates T, Ebbs SR, Harrison M, A’Hern RP (1991) Influence of cho-lecystectomy on symptoms. Br J Surg 78: 964–976
3. Carswell WR, Willis JD (1969) Cholecystitis with gall-stones in in-fancy and childhood. Br J Surg 56: 547–548
4. Dubois F, Ikard PF, Berthelot G, Levard H (1990) Coelioscopic cho-lecystectomy. Preliminary report of 36 cases. Ann Surg 211: 60–62
5. Holcomb GW, Holcomb III GW (1990) Cholelithiasis in infants, chil-dren, and adolescents. Pediatr Rev 11: 268–274
6. Holcomb III GW, Olsen DO, Sharp KW (1991) Laparoscopic chole-cystectomy in the pediatric patient. J Pediatr Surg 10: 1186–1190
7. Molander M-L, Berhdahl S (1992) Gallbladder disease, primary cho-lelithiasis, or gallbladder hydrops: review of 32 children. Pediatr SurgInt 7: 328–331
8. Moorehead RJ, Kernohan RM, Patterson CC, McKelvey STD, ParksTG (1986) Does cholecystectomy predispose for colorectal cancer?Dis Colon Rectum 29: 36–38
9. Moorehead RJ, McKelvey STD (1989) Cholecystectomy and colorec-tal cancer. Br J Surg 76: 250–253
10. Moosa AR (1973) Cholelithiasis in childhood. J R Coll Surg Edinb 18:42–46
11. Newman KD, Marmon LM, Attori R, Evans S (1991) Laparoscopiccholecystectomy in pediatric patients. J Pediatr Surg 10: 1184–1185
12. Perissat J, Collet D, Belliard R (1990) Gallstones: laparoscopic treat-ment—cholecystectomy, cholecystotomy and lithotripsy. Surg Endosc4: 1–5
13. Robertson JFR, Carachi R, Sweet EM, Raine PAM (1988) Cholelithi-asis in childhood: a follow-up study. J Pediatr Surg 23: 246–249
14. Soderlund S, Zetterstro¨m B (1962) Cholecystitis and cholelithiasis inchildren. Arch Dis Child 37: 174–180
15. Troidl H, Spangenberger W, Langen R, Al-Jaziri A, Eypasch E, Neu-gebauer E, Dietrich A (1992) Laparoscopic cholecystectomy: technicalperformance, safety, and patient benefits. Endoscopy 24: 252–261
16. Ure BM, Troidl H, Spangenberger W, Lefering R, Dietrich A, Neu-gebauer E (1994) Pain after laparoscopic cholecystectomy. Surg En-dosc 8: 90–96
17. Ure BM, Troidl H, Spangenberger W, Lefering R, Dietrich A, EypaschE, Neugebauer E (1995) Symptoms more than one year after laparo-scopic cholecystectomy. Br J Surg 82: 267–270
18. Vinograd I, Halevy A, Klin B, Negri M, Bujanover Y (1993) Lapa-roscopic cholecystectomy: treatment of choice for cholelithiasis inchildren. World J Surg 17: 263–266
Fig. 1. Placement of five trocar incision sites in laparoscopic cholecys-totomy.
672

Endoscopic hydrostatic balloon dilation of ulcer-induced pyloricstenosis in rheumatoid arthritis and secondary amyloidosis
K. Hizawa,1 Y. Ohta,1 H. Satou,2 K. Aoyagi,1 K. Eguchi,3 M. Fujishima 1
1 Second Department of Internal Medicine, Faculty of Medicine, Kyushu University, Maidashi 3-1-1, Higashi-Ku, Fukuoka 812-82, Japan2 First Department of Surgery, Faculty of Medicine, Kyushu University, Maidashi 3-1-1, Higashi-Ku, Fukuoka 812-82, Japan3 Second Department of Pathology, Faculty of Medicine, Kyushu University, Maidashi 3-1-1, Higashi-Ku, Fukuoka 812-82, Japan
Received: 11 July 1996/Accepted: 23 July 1996
Abstract. We describe a 50-year-old Japanese woman withrheumatoid arthritis who presented with near-complete gas-tric outlet obstruction. The patient also suffered from sec-ondary gastrointestinal and cardiac amyloidosis. Gastros-copy revealed multiple huge gastric antral ulcers in whichamyloid deposits were identified on histologic examination.The ulcers became scars after treatment with omeprazole,which cause in severe pyloric stenosis. Endoscopic hydro-static balloon dilation under fluoroscopic guidance was per-formed twice for 10 min. The pyloric outlet remained suf-ficiently patent 22 months later.
Key words: Rheumatoid arthritis — gastric outlet obstruc-tion-pyloric stenosis
Patients with rheumatoid arthritis (RA), who require long-term nonsteroidal antiinflammatory drugs (NSAIDs) andcorticosteroids, have a tendency to develop relapsing gastricantral ulcers which infrequently result in pyloric channelstenosis [3, 8, 11, 12, 14]. In addition, secondary gastroin-testinal amyloidosis (SGIA) is a well-known serious com-plication in RA patients [13]. In these patients, surgicalintervention should be carefully approached because of anassociated hemorrhagic diathesis, impaired wound healing,and a high rate of cardiac and renal involvement [10, 15].We describe a patient with RA and SGIA in whom a severegastric outlet obstruction was successfully managed by en-doscopic hydrostatic balloon dilation.
Case report
A 50-year-old Japanese woman was admitted to our hospital in January1994 with a complaint of diarrhea of 2 months’ duration. The patient had
been suffering from RA for 20 years. Her recent medications consisted oforal prednisolone 5 mg and loxoprofen 180 mg per day. According to theAmerican Rheumatism Association, her arthritis was class II and stage IV[1]. There was occult blood in her stool, but no causative agent was de-tected by culture. Laboratory data revealed a thrombocytosis (55 × 104/ml),but no leucocytosis or anemia. C-reactive protein was 0.1 mg/d1 and serumrheumatoid factor was 1169 IU/ml. Serum chemistry indicated a hypopro-teinemia (total protein, 5 g/dl), but no abnormality of liver or renal func-tion. An upper gastrointestinal endoscopy on admission showed extensivegranularity in the gastric and duodenal mucosa. Biopsy of these areasrevealed amyloid deposits (Fig. 1), and the material was confirmed asamyloid A protein by histochemical investigation [13]. We therefore con-sidered her symptoms to be due to secondary gastrointestinal amyloidosisresulting from long-standing RA. The patient also manifested congestiveheart failure, probably due to cardiac amyloidosis as suggested by echo-cardiography.
Total parenteral nutrition therapy (TPN) was administered and the pa-tient’s diarrhea subsequently improved. However, the patient’s RA wors-ened, requiring intermittent administration of diclofenac suppositories andintraarticular injection of triamcinolone acetate. The patient, furthermore,began to experience epigastric pain even with the prophylactic adminis-tration of famotidine 40 mg daily. The endoscopy performed 60 days after
Correspondence to:K. HizawaFig. 1. Biopsy specimen shows marked amyloid deposits in the laminapropria mucosa (H.E, ×66).
Surg Endosc (1997) 11: 673–675
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

admission showed multiple and large ulcers in the gastric antrum. Al-though, 50 days later, the gastric ulcers had healed after the additionaltreatment with omeprazole 20 mg, pyloric scarring with nearly completeobstruction of the gastric outlet channel had developed (Fig. 2A). AlthoughTPN was continued, her obstructive symptoms of nausea and vomitingremained. Endoscopic balloon dilation was therefore attempted alternativeto surgical intervention. Because the pyloric outlet could not be clearlyidentified on endoscopy, we inserted a radifocus wire (Terumo) through thenarrow canal of outlet obstruction into the duodenum under fluoroscopicguidance with torque control. We passed through a small-caliber catheterover the wire and then exchanged the wire for a standard guidewire (Mi-crovasive). Using a 15-mm Rigiflex balloon dilator (Microvasive), hydro-static dilation was performed, maintaining balloon inflation for 10 min with3 atm (Fig. 3). One week later, this procedure was repeated, and thediameter of the gastric outlet widened to more than 10 mm. The patient wassubsequently able to eat a regular diet. Her clinical course after dilation wasuneventful, and she was discharged in August 1994. Since then, the patienthas been maintained on acid-suppressive therapy with per oral famotidineand has been free of any symptoms. Follow-up endoscopy performed inMarch 1996 revealed sufficient patency of the gastric outlet and no recur-rence of ulcer (Fig. 2B).
Discussion
NSAIDs are well known to be causative agents of gastricmucosal injury. A prospective study by Caruso and Bianchi
Porro [3] has indicated that about 10% of subjects devel-oped a gastric ulcer 3 to 12 months after the administrationof NSAIDs. Larkai et al. [8] have reported that a gastriculcer was found on endoscopy in more than 10% of arthriticpatients receiving chronic NSAIDs. They also suggestedthat the ulcers were characterized by a lack of pain and werelocated in the gastric prepyloric region [8]. These ulcersmight thus lead to pyloric scarring and gastric outlet ob-struction as they are recurrent and can be overlooked inasymptomatic patients. In a recent study by Weaveret al.[14], prolonged NSAIDs use was associated with gastricoutlet obstruction. Ulcers in RA patients receiving chronicNSAIDs are more frequent when concomitant corticoste-roids are used [12]. Ohtsuka [11] has speculated that de-creased gastric mucosal blood flow is associated with ulcerformation in RA patients. In addition, RA is occasionallycomplicated by SGIA [13], which manifests as ischemiclesions in the gut due to perivascular amyloid deposits [10].Our patient had all these risk factors for developing severepyloric stenosis.
In patients with SGIA, particularly involving the heartand kidney, surgery should be carefully approached becauseof unfavorable postoperative results [10, 15]. Therefore, we
Fig. 2. Gastroscopy in May 1994, reveals severe pyloric scarring (arrow,A). The gastric outlet channel remains patent 22 months after the dilation(B).
Fig. 3. Rigiflex balloon catheter threaded over the guide wire is positionedprecisely under fluoroscopic guidance (A). The balloon is inflated with aradiopaque solution and remains dilated for 10 min with 3 atm (B).
674

chose endoscopic balloon dilation alternative surgery in thispatient, which was managed successfully and safely. Eventhough the pyloric stenosis was so severe that the outletcanal could not be clearly identified, we were able to passthrough the narrow canal using a radifocus guidewire(Terumo) under fluoroscopic guidance with a torque con-trol. Since a successful report by Benjaminet al. in 1984[2], endoscopic balloon dilation has been applied for benigngastric outlet obstruction, and the efficacy over the shortterm has been established [4, 6].
However, the safety and long-term results are now beingdebated. Kuwada and Alexander [7] have reported that thelong-term success rate was only 16% during a median ob-servation of 45 months. In a recent study by Lauet al. [9],the ulcer complication-free rate at 3 years was 55%, andone-half of the patients required subsequent surgery becauseof recurrent obstruction, perforation, or bleeding. Kozarek[5] has stated that the results seem to depend on patientselection, standardization of the procedures (air or liquidinsufflation, or under fluoroscopy) and patient compliancewith acid-suppressing drugs. Although further follow-up isnecessary, our patient maintained her clinical improvementfor 22 months after the dilation.
References
1. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, CooperNS (1988) The American Rheumatism Association 1987 revised cri-teria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315–324
2. Benjamin SB, Glass RL, Cattau EL, Miller WB (1984) Preliminaryexperience with balloon dilation of the pylorus. Gastrointest Endosc30: 93–95
3. Caruso I, Bianchi Porro G (1980) Gastroscopic evaluation of anti-inflammatory agents. Br Med J 280: 75–78
4. DiSario JA, Fennerty MB, Tietze CC, Hutson WR, Burt RW (1994)Endoscopic balloon dilation for ulcer-induced gastric outlet obstruc-tion. Am J Gastroenterol 89: 868–871
5. Kozarek RA (1996) Endotherapy for gastric outlet obstruction. Gas-trointest Endosc 43: 173–174
6. Kozarek RA, Botoman VA, Patterson DJ (1990) Long-term follow-upin patients who have undergone balloon dilation for gastric outletobstruction. Gastrointest Endosc 36: 558–561
7. Kuwada SK, Alexander GL (1995) Long-term outcome of endoscopicdilation of nonmalignant pyloric stenosis. Gastrointest Endosc 41: 15–17
8. Larkai EN, Smith JL, Lidsky MD, Graham DY (1987) Gastroduodenalmucosa and dyspeptic symptoms in arthritic patients during chronicnonsteroidal anti-inflammatory drug use. Am J Gastroenterol 82:1153–1158
9. Lau JYW, Chung SCS, Sung JJY, Chan ACW, Ng EKW, Suen RCY,Li AKC (1996) Through-the-scope balloon dilation for pyloric steno-sis: long-term results. Gastrointest Endosc 43: 98–101
10. O’Doherty DP, Neoptolemos JP, Wood KF (1987) Place of surgery inthe management of amyloid disease. Br J Surg 74: 83–88
11. Ohtsuka E (1992) Upper gastrointestinal endoscopic findings and gas-tric mucosal blood flow in patients with rheumatoid arthritis. FukuokaActa Med 83: 62–71
12. Piper JM, Ray WA, Daugherty JR, Griffin MR (1991) Corticosteroiduse and peptic ulcer disease: role of nonsteroidal anti-inflammatorydrugs. Ann Intern Med 114: 735–740
13. Tada S, Iida M, Yao T, Kawakubo K, Yao T, Okada M, Fujishima M(1994) Endoscopic features in amyloidosis of the small intestine: clini-cal and morphologic differences between chemical types of amyloidprotein. Gastrointest Endosc 40: 45–50
14. Weaver GA, Harper RL, Storey JA, Jenkins PL, Marrell NB (1995)Nonsteroidal antiinflammatory drugs are associated with gastric outletobstruction. J Clin Gastroenterol 20: 196–198
15. Yood RA, Skinner M, Rubinow A, Talarico L, Cohen AJ (1983)Bleeding manifestations in 100 patients with amyloidosis. JAMA 249:1322–1324
675

Letters to the editor
The totally extraperitoneal laparoscopic hernia repair
We read with interest the paper by Vanclooster and col-leagues [11] and commend their contribution to this proce-dure. However, we would offer three comments:
First, totally extraperitoneal laparoscopic hernia repairwas developed by Dulucq [1–3] in 1989/90 and by Mc-Kernan [7] not a great deal later. While it seems legitimatefor others to publish their own technical variations, devel-opments, and outcomes, we strongly support recent remind-ers [6] that journal editors and their peer referees owe thereader a duty of diligence: they should insist that authorsexercise proper scholarship by giving credit where it is due.Otherwise the uninformed reader may assume originalityand the informed may infer plagiarism, where the authorintended neither.
Second, the mesh configuration suggested by Van-clooster et al. was presented by one of us several years ago[4, 10]. However, the concept of amputating the inferior andlateral corner ‘‘so the mesh fits better on the iliac vesselsand the psoas muscle’’ is flawed, since it has subsequentlybeen reported [12] that recurrences may occur dorsal/inferior to this inferolateral corner. The most extensive pos-sible coverage of the psoas muscle belly is therefore appro-priate.
Third, the need for mesh fixation remains debatable.However, to fix the cranial border to ‘‘prevent early migra-tion or slipping’’ is illogical: In our joint experience of over1,000 cases and, to our knowledge in all reports in the worldliterature, recurrences pass uniformly caudal to the inferiorborder of the prosthesis. Fixation of the inferior medial partof the mesh to Astley Cooper’s ligament alone [5] may notoffend against the original tension-free notion of Stoppa [8,9] nor interfere with the mechanics of prosthesis retention.To fix the superior border to points that move relative to oneanother within a musculofascial structure contravenes bothprinciples.
Finally, on a minor point, if the structure annotated as‘‘D’’ in Fig. 1 is the testicular vascular bundle, where is thevas deferens?
Despite these comments we congratulate the authors ontheir low complication rate.
References
1. Dulucq J-L (1991) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneale en retrope´ritoneoscopie. CahChir 79: 15–16
2. Dulucq J-L (1992) Traitement des hernies de l’aine par mise en placed’un patch prothe´tique sous-pe´ritoneal en pre´-peritoneoscopie. Chirur-gie 118(1–2): 83–85
3. Dulucq J-L (1992) The treatment of inguinal hernias by implantationof mesh through retroperitoneoscopy. Postgrad Gen Surg 4: 173–174
4. Fiennes AGTW, Taylor RS (1994) Learning laparoscopic hernia re-pair. In: Inguinal hernia, advances or controversies? Arregui M, NaganR (eds) Radcliffe, Oxford, pp 475–482
5. Fiennes AGTW, Himpens J, Dulucq J-L (1994) Preperitoneoscopicgroin hernioplasty, current synthesis. Surg Endosc 8(8): 989
6. Horton R, Smith R (1996) Time to redefine authorship (editorial). BrMed J 312: 723
7. McKernan JB (1993) Laparoscopic extraperitoneal repair of inguino-femoral herniation. Endosc Surg Allied Tech 1(4): 198–203
8. Stoppa R, Petit J, Abourachid H (1973) Proce´deoriginal de plastie deshernies de l’aine. L’interposition sans fixation d’une prothe`se en tullede Dacron par voie me´diane pre´peritoneale. Chirurgie 99: 119
9. Stoppa RE, Rives JL, Warlaumont CR (1984) The use of Dacron in therepair of hernias of the groin. Surg Clin North Am 64: 269–285
10. Taylor RS, Fiennes AGTW (1992) A tension free modification of theDulucq preperitoneal laparoscopic hernioplasty. Min Inv Ther 1(Suppl1): 101
11. Vanclooster P, Meersmann AL, de Gheldere CA, Van de Ven CK(1996) The totally extraperitoneal laparoscopic hernia repair. SurgEndosc 10: 332–335
12. Vivekanadan S, Fiennes AGTW (1995) Totally extraperitoneal groinhernioplasty: mechanism of delayed indirect recurrence. Min Inv Ther4(Suppl 1): 55
A. Fiennes
Department of SurgerySt George’s Hospital Medical SchoolCranmer TerraceLondon, SW17 ORE, United Kingdom
J. Himpens
Department of Digestive SurgeryUniversity Hospital Ste PierreRue Haute 201B-1000 Brussels, Belgium
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997Surg Endosc (1997) 11: 696

The author replies
We thank you for the opportunity to answer the letter of Mr.Fiennes. First of all, we certainly do acknowledge that Mr.Dulucq and Mr. Mc Kernan were the pioneers of the extra-peritoneal laparoscopic hernia repair. Honor to whom honoris due. We did not intend to pretend to be the pioneers ofthis technique. We wished only to describe the technique theway we perform it, to describe our own findings, and to givea fair report of our preliminary results.
The reason for cutting the inferolateral corner is not justthat we think it fits better on the iliopsoas but also becausewe are afraid to cause damage to the nerves running on it bydissecting unnecessarily high on the muscle. Since the meshmeasures 15 × 15 cm, we do not think we compromise thestrength of the repair by merely removing a small piece ofits inferolateral corner. We think that dissecting very highon the muscle just to position the whole inferolateral cornerof the mesh flat on the muscle is unnecessary and danger-ous.
We do agree totally that fixation of the mesh is unnec-
essary provided the mesh is large enough, which is obvi-ously the case when using a 15 × 15 cm mesh. In fact, wehave not fixed the mesh since January 1996.
We also agree that the vas deferens is not clearly seen onFig. 1. We chose this shot because of the clearly visiblelarge direct defect.
C. de Gheldere
Heilig Hart ZiekenhuisKolveniersvest 20B-2500 LIERBelgium
P. Vanclooster
Bouwelsesteenweg 62560 NijlenBelgium
Surg Endosc (1997) 11: 697
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The influence of pneumoperitoneum on the peritoneal implantation offree intraperitoneal cancer cells
Recently Hubens et al. published an interesting article en-titled ‘‘The influence of a pneumoperitoneum on the peri-toneal implantation of free intraperitoneal colon cancercells’’ [2]. They reported on the possible implantation ofcancer cells at trocar wounds at the moment of deflation ascells are forced through these wounds by the pressure gra-dient created by the pneumoperitoneum during laparoscopicsurgery for malignant disease. We would like to point outthat this ‘‘chimney effect,’’ as originally described by us,can occur during the entire laparoscopic procedure and notonly at the moment of deflation, as leakage of CO2 along-side trocars during surgery is impossible to prevent with theexisting trocars [3]. Consequently, deflation of the pneumo-peritoneum by letting CO2 escape through one of the trocarsbefore pulling these trocars out of the abdomen will notprevent the occurrence of entrapment of cancer cells in thetrocar wounds.
We fully agree with the authors on the possible advantageof gasless laparoscopy as this could prevent the ‘‘chimneyeffect.’’ In our experimental work we found significantly lesstumor growth at the port sites following gasless laparoscopicsurgery for colon cancer in the rat as compared to laparoscopicsurgery using a CO2 pneumoperitoneum. This techniqueseems promising to treat malignant disease laparoscopically.
References
1. Bouvy ND, Marquet RL, Jeekel J, Bonjer HJ (1996) Impact of gas (less)laparoscopy and laparotomy on peritoneal tumor growth and abdominalwall metastases. Surg Endosc 10: 551
2. Hubens G, Pauwels M, Hubens A, Vermeulen P, Van Marck E, EyskensE (1996) The influence of a pneumoperitoneum on the peritoneal im-plantation of free intraperitoneal colon cancer cells. Surg Endosc 10:809–812
3. Kazemier G, Bonjer HJ, Berends FJ, Lange JF (1995) Port site metas-tases after laparoscopic colorectal surgery for cure of malignancy. Br JSurg 82: 1141–1142
G. Kazemier1
F. J. Berends1
N. D. Bouvy1
J. F. Lange2
H. J. Bonjer1
1 Department of SurgeryUniversity Hospital Rotterdam-DijkzigtDr Molewaterplein 403015 GD, RotterdamThe Netherlands2 Department of SurgerySt. Clara HospitalRotterdamThe NetherlandsCorrespondence to:G. Kazemier
Surg Endosc (1997) 11: 698
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

The author replies
We thank Dr. Kazemier et al. for their kind remarks and fullyagree with them that gas leakage can occur during the entireprocedure with subsequent implantation of tumor cells at thetrocar sites. At the moment we are conducting further experi-mental studies on the possible effects of gas leakage on tumorcell implantation and the ‘‘chimney effect,’’ as they havecalled it. Results will be ready for publication soon.
G. Hubens
Department of SurgeryUniversity HospitalUniversity of AntwerpWilrijkstraat 102650 EdegemBelgium
Surg Endosc (1997) 11: 699
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

Early international results of laparoscopic gastrectomies
P. M. Y. Goh, A. Alponat, K. Mak, C. K. Kum
Department of Surgery, National University Hospital, 5 Lower Kent Ridge Road, 119074 Singapore
Received: 7 August 1996/Accepted: 28 October 1996
AbstractBackground:The first totally laparoscopic Billroth II gas-trectomy was performed in 1992. To date, laparoscopic gas-trectomy has been performed by a small number of surgeonsaround the world and the laparoscopic approach has beenextended to Billroth I and total gastrectomy. The aim of thisstudy is to review the state of laparoscopically performedgastrectomies in the international scene.Methods:Questionnaires were prepared and sent to everysurgeon in the world known by the authors or their contactsto have performed a laparoscopic gastrectomy. A question-naire survey was started in July 1994 and completed byNovember 1994. Data collected included age, sex, type ofgastric resection, technique of reconstruction after resection,average duration of surgery, time to liquid and solid intake,postoperative hospital stay, complications, and opinions ofthe surgeons.Results:Sixteen surgeons contributed to this study. A totalnumber of 118 cases of laparoscopic gastrectomies, com-prising Billroth I (11), Billroth II (87), vagotomy and an-trectomy (10), and total gastrectomy (10) had been per-formed. The indications were gastric and/or duodenal ulcersand benign and malignant gastric tumors.Conclusions:Laparoscopic gastrectomy was found to besuperior to the open technique by 10 of 16 surgeons becauseof faster recovery, less pain, and better cosmesis. The pro-cedure was an expensive and long operation according tofour. Two surgeons were uncertain of any benefit because oflimited experience.
Key words: Laparoscopic gastrectomy — International re-sults — Questionnaire survey
After the first successful totally laparoscopic Billroth II gas-trectomy was performed in the Singapore National Univer-
sity Hospital, laparoscopic gastrectomy began being per-formed by a number of surgeons around the world. Somemodifications to the original procedure have been described[4, 6]. The laparoscopic approach has also been extended toother related operations such as wedge resection, Billroth Igastrectomy, and total gastrectomy. The indications havealso been expanded to early gastric cancer and palliativeresections for advanced gastric cancer.
The aim of this study is to evaluate the early interna-tional gastrectomy results. As the data is diverse, uncon-trolled, and incomplete, we feel that this study has morevalue as a historical record of the development of a newprocedure than as a scientific testimony to its efficacy at thismoment. It would, for instance, be extremely nice to havethe data of the initial experience of open gastrectomyaround the world during the year 1885, 4 years after itsinitial development by Theodore Billroth.
Materials and methods
In order to evaluate the state of laparoscopic gastrectomy today, we pre-pared a questionnaire and sent it to every surgeon in the world known bythe authors or their contacts to have performed a laparoscopic gastrectomy.As the procedure had just been described, we assumed that the numberwould be small and that not many would be left out. The study was startedin July 1994 and all questionnaires were returned by 30 November 1994.Several surgeons who stated that they only performed endoscopic mucosalresections or wedge resections were excluded. Our own series of 18 caseswith Billroth II gastrectomy were included.
Data collected included age, sex, indication for operation, type of gas-tric resection, technique of reconstruction after resection, numbers of en-dostaplers (Endo-GIA) used, average duration of surgery, average time tomobilize the patient, time to liquid and solid intake, mean hospital stay,time to return to work, postoperative complications, and surgeon’s opinionon laparoscopic gastrectomy.
Results
The questionnaire was answered by all of those surgeonswho received it. According to the data collected from thesesurgeons and our own experience (16 surgeons from 16Correspondence to:P. M. Y. Goh
Surg Endosc (1997) 11: 650–652
SurgicalEndoscopy
© Springer-Verlag New York Inc. 1997

different centers in 12 countries), the numbers of laparo-scopic gastrectomies were 118, comprising 11 Billroth Igastrectomy, 87 Billroth II gastrectomy, 10 vagotomy, andantrectomy and 10 total gastrectomy. The range in numberof cases reported by contributors was one to 22. Eighty-four(71%) of the cases were men and 34 (29%) were women;mean age was 49 years ranging from 24 to 91 years. Thedata provided by contributors represents a consecutive ex-perience.
The most common indication for operation was gastriccancer (in 46–38% of the cases). The stage of these tumorsand lymph node status were not stated in the questionnaireforms. Other common indications were gastric ulcers in 35and duodenal ulcers in 23 (Table 1).
The operations were totally laparoscopic in 94 (79%)and laparoscopic assisted in 24 (21%) of the patients. Inlaparoscopic-assisted cases, the hand-sewn anastomoseswere fashioned between duodenum and proximal transectedstomach with the usual technique as in open surgery througha 5-cm transverse muscle-splitting incision over the duode-nal cap in patients with Billroth I gastrectomy. In patientswith Billroth II gastrectomy, a 5-cm left subcostal muscle-splitting incision was made to perform the gastrojejunos-tomy. The anastomoses were completed totally laparoscopi-cally using staples (Endo GIA) in 60 (51%) patients. Thecombination of Endo GIA and intracorporeal hand-sewntechnique was used in 55 (46%) cases in whom the anasto-moses were performed by Endo GIA and side openingswere closed with laparoscopic suturing material. The anas-tomoses were performed totally hand-sewn in three (3%)cases. The mean number of endoscopic staples (Endo GIA)used was five, ranging from four to 16.
Conversion to open surgery was mandatory in six (5%)cases because of bleeding in three, stapler failure in one,transection line too close to the esophagus in one, and in-ability to localize the ulcer site in one.
The average duration of the surgery was 215 min, rang-ing from 90 to 360 min. In the postoperative period, theaverage time to mobilize patient was 28 h, commencementof liquid intake 3 days, solid food 5 days, and the meanhospital stay 8 days. Return to normal daily activities tookan average of 17 days (Table 2).
Postoperative complications were anastomotic obstruc-tion in four (4%), bleeding in two (2%), anastomoticleak in three (3%), and sepsis in two (2%). Othercomplications were duodenal stump leak in one (1%)
and gastric atony in one (1%). There were two operation-related mortalities; duodenal stump leakage with sepsisin one patient and subhepatic abscess and death at reopera-tion in the other. One patient died of AIDS-related pneu-monia.
Laparoscopic gastrectomy was considered superiorto open technique by 10 of 16 surgeons contributing tothis study because of faster recovery, less pain, andbetter cosmesis. According to four of those who responded,it was an expensive and long operation. Two surgeonswere uncertain due to the small number in their personalseries.
Discussion
Laparoscopic gastrectomy has been performed by a numberof surgeons around the world and many modifications to theoriginal technique have been described. Besides the totallyintraperitoneal laparoscopic gastrectomy, laparoscopic-assisted gastrectomy either by gasless technique (elevatingthe abdominal wall with U-shaped retractor) or insufflatingthe abdomen by CO2 has been practiced by some authors[12]. The laparoscopic approach can now be extendedto other related operations such as Billroth I gastrec-tomy, wedge resection, and total gastrectomy [1, 7, 10, 12–14].
Indications for laparoscopic Billroth II gastrectomy in-clude: (1) chronic duodenal or pyloric channel ulcer whichhas failed to heal after adequate medication andHelicobac-ter pylori eradication; biopsy must be taken to exclude ma-lignancy; (2) failure of benign gastric peptic ulcer to healafter 3 months of well-supervised and compliant medicaltreatment; (3) bleeding gastric ulcer after failure of endo-scopic hemostasis; (4) a perforated benign gastric ulcer withminimal soilage; (5) early gastric cancer, and (6) palliativeresection in advanced gastric carcinoma [3, 5, 8]. Relativecontraindications are previous upper abdominal surgery andsevere cardiopulmonary disease. Indications for laparoscop-ic Billroth I gastrectomies are the same as for Billroth IIgastrectomies. Technically, in most cases of Billroth I pro-cedures, dissection and resection phases are carried out un-der the conditions of pneumoperitoneum, but the gastroduo-denostomy is done by open technique through a small in-cision in the right upper quadrant [1, 12]. Wedge resectionscan easily be performed with endostaplers and are mainlyindicated in benign tumors of the stomach [9] and selectedearly gastric cancers [8].
The indications for laparoscopic gastrectomy has beenexpanded to early gastric cancer and palliative resections of
Table 1. The indications for operation
IndicationPatients,n 4 118 (%)
Gastric cancer 46 (38)Gastric ulcer 35 (30)Duodenal ulcer 23 (19)Gastric + duodenal ulcer 5 (4)Benign gastric tumor 3 (3)Non-Hodgkin’s lymphoma 2 (2)Tubulovillous adenoma 1 (1)Angiodysplasia 1 (1)Gastric volvulus 1 (1)Pancreatic rest 1 (1)
Table 2. Postoperative recovery
Average time(range)
Mobilization of patient (hours) 28 (6–192)Liquid intake (days) 3 (1–6)Solid intake (days) 5 (2–12)Hospital stay (days) 8 (3–30)Return to daily activities (days) 17 (9–90)
651

advanced gastric cancer. However, the gastric malignanciesshould be carefully evaluated and selected for laparoscopicapproach. Thus, in early gastric cancer, partial resection,intragastric mucosal resection, or distal partial gastrectomycan be performed. Laparoscopic palliative resection for ad-vanced gastric carcinoma is also feasible. The place of thelaparoscopic approach in stage II and III gastric carcinomasis still uncertain. In these cases a meticulous and extensivenodal dissection can improve survival. Melotti and Azagra,however, reported encouraging preliminary results in theseintermediate stages [2, 11]. The general surgical communityremains unconvinced and longer follow-up and bigger trialsare required.
There are certain advantages to laparoscopic gastrec-tomy. It holds promise of less pain, less immobility, quickeralimentation, less wound and respiratory complications, andearly return to normal daily activities. Therefore, this tech-nique is patient-friendly. On the other hand, with the tech-nology we have today, it is still quite a technical challengeto the surgeon. In addition, the high cost of endoscopicstapling devices is an important drawback of this technique.However, this can be overcome when surgeons improvetheir hand suturing skills. Many suturing assist devices arenow available to make laparoscopic anastomosis less daunt-ing.
Most surgeons performing this operation were im-pressed by the prompt recovery, earlier mobilization, andprompt recovery of gut function in the successful cases.However, the real benefit of this procedure will not be sci-entifically proven for some time due to difficulties in col-lecting large numbers of cases and documenting them. Arandomized controlled trial comparing open and laparo-scopic gastrectomy will also be difficult to carry out as theindications in benign disease are shrinking as a consequenceof the proven effectiveness ofHelicobacter pylorieradica-tion therapy.
This is very preliminary data. Therefore, we can notdraw very definitive conclusions from this study. It justdocuments the preliminary efforts of surgeons around theworld experimenting with this new technique. We are surethat in 5–10 years, the situation will become clearer becausemore data, and more scientific presentation of data, will beavailable.
This data, however, has historical value because it is the
first worldwide survey of this very new procedure. Fifty to100 years from now, when people look back, they will atleast have some information as to how this procedure startedand spread around the world.
Acknowledgment.The authors wish to thank the following surgeons whocontributed to this international study: JS Azagra (Belgium), DL Fowler(USA), JR Mauras (France), G Melotti (Italy), Y Nagai (Japan), N Kat-khouda (USA), V Lange (Germany), D Litwin (Canada), D Rosin (En-gland), M Suppiah (Malaysia), G Szinicz (Germany), JF Uddo, Jr (USA),DI Watson (Australia), T Wuttichai (Thailand), CZ Zheng (China).
References
1. Anvari M, Park A (1994) Laparoscopic-assisted vagotomy and distalgastrectomy. Surg Endosc 8: 1312–1315
2. Azagra JS, Goergen M (1994) Laparoscopic total gastrectomy. In:Meinero M, Melotti G, Mouret PH (eds) Laparoscopic surgery. Mas-son, Milano, pp 289–296
3. Goh P (1994) Laparoscopic Billroth II gastrectomy. Semin LaparoscSurg 1(3): 171–181
4. Goh P, Kum CK (1993) Laparoscopic Billroth II gastrectomy: a re-view. Surg Oncol 2(Suppl 1): 13–18
5. Goh P, Kum CK (1995) Laparoscopic Billroth II gastrectomy. In:Phillips HP, Rosenthal RJ (eds) Operative strategies in laparoscopicsurgery. Springer, New York, pp 155–158
6. Goh P, Tekant Y, Kum CK, Isaac J, Ngoi SS (1992) Totally intra-abdominal laparoscopic Billroth II gastrectomy. Surg Endosc 6: 160
7. Kitano S, Iso Y, Moriyama M, Sugimachi K (1994) Laparoscopic-assisted Billroth I gastrectomy. Surg Laparosc Endosc 4(2): 146–148
8. Kitano S, Shimoda K, Miyahara M (1995) Laparoscopic approaches inthe management of patients with early gastric carcinomas. Surg Lapa-rosc. Endosc 5(5): 359–362
9. Llorente J (1994) Laparoscopic gastric resection for gastric leiomyo-ma. Surg Endosc 8: 887–889
10. Lointer P, Leroux S, Ferrier C, Dapoigny M (1993) A technique oflaparoscopic gastrectomy and Billroth II gastrectomy. J LaparoendoscSurg 3(4): 353–364
11. Melotti G, Meniero M, Tammborrino E (1994) Gastric resection forcancer. In: Meinero M, Melotti G, Mouret PH (eds) Laparoscopicsurgery. Masson, Milano, pp 273–282
12. Uyama I, Pgiwara H, Takahara T, Kato Y, Kikuchi K, Iida S (1994)Laparoscopic and minilaparotomy Billroth I gastectomy for gastriculcer using an abdominal wall-lifting method. J Laproendosc Surg4(6): 441–445
13. Uyama I, Ogiwara H, Takahara T, Kato Y, Kikuchi K, Iida S (1995)Laparoscopic Billroth I gastrectomy for gastric ulcer: technique andcase report. Surg Laparosc Endosc 5(3): 209–213
14. VanHouden CE (1994) Laparoscopic bilateral truncal vagotomy, an-trectomy, and Billroth I anastomosis for prepyloric ulcer. Surg Lapa-rosc Endosc 4(6): 457–460
652