surgical management of - denver, colorado · surgical management of ... pancreaticoduodenectomy •...
TRANSCRIPT

Surgical management of cystic pancreatic neoplasms
Csaba Gajdos, MD

Survey Question # 1• 33 yo female with h/o
pancreatitis• 3.3 cm cystic lesion in the
pancreas• Previous attempted
endoscopic drainage over 1 yr ago
• Constant abdominal pain (4-5/10)
• EUS reveals mucin and papillary epithelial cells

Survey Question # 2• 61 yo female with 2
months h/o new onset epigastric pain
• CT A/P reveals 1.3cm cystic lesion in the body and 0.5 cm lesion in the head of pancreas
• EUS finds mucin in first lesion
• Her symptoms are gone after “cleaning her bowels”

Survey Question # 2

Pancreatic Cystic Lesions
• Cystic neoplasms represent about 10% of pancreatic neoplasms
• The proportion of pancreatic resections nearly doubled (from 16% to 30%) in certain tertiary care hospitals in the last 15 years

Pancreatic Cystic Lesions
Allen PJ Ann Surg 2006

Pancreatic Cystic Lesions
• Increasingly recognized –Widespread use and improved cross
sectional imaging• Spectrum of benign to malignant lesions
–Pseudocysts–Serous cystadenomas–Mucinous cystadenomas–Intraductal papillary mucinous
neoplasm (IPMN)
Pancreatic Cystic Lesions History
• Symptoms related to lesion?– Pain– Obstructive jaundice– Weight loss
• Pancreatitis– past or present?
Pancreatic Cystic LesionsDecision Points
• Differential diagnosis of the cyst– Neoplastic vs. Non-neoplastic– Risk of malignancy
• Likelihood of harm – With and without testing– With and without treatment
• Particularly relevant for asymptomatic patient
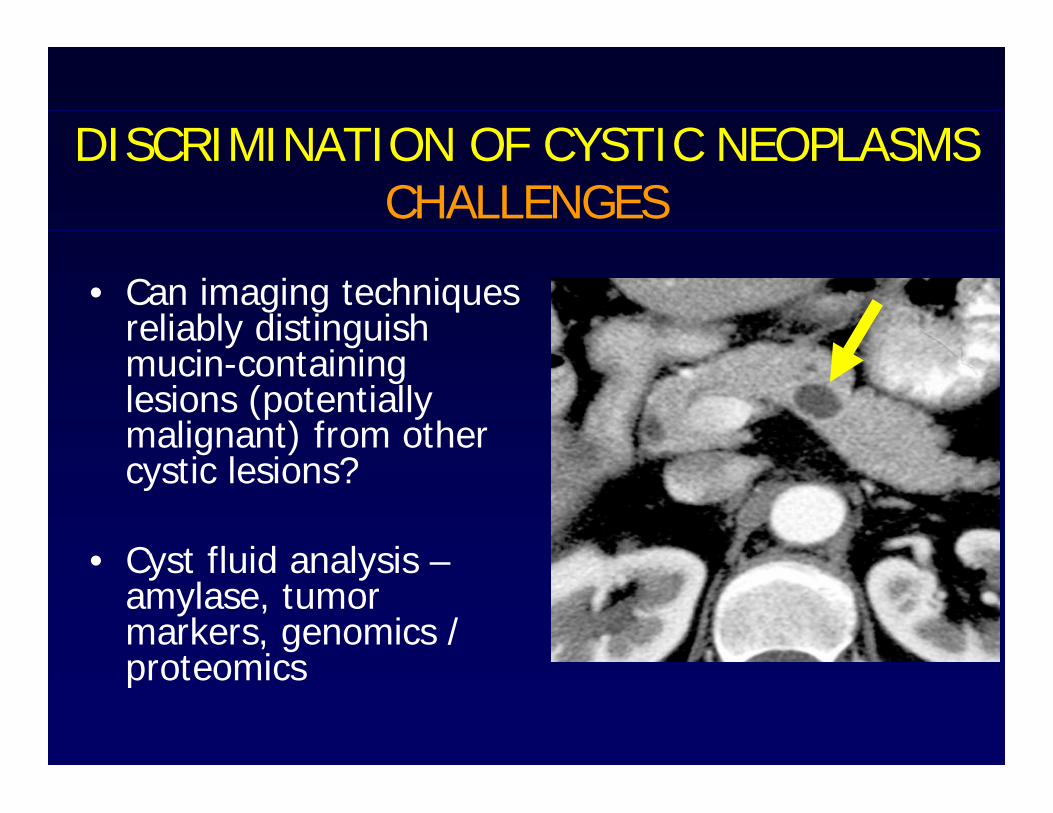
DISCRIMINATION OF CYSTIC NEOPLASMSCHALLENGES
• Can imaging techniques reliably distinguish mucin-containing lesions (potentially malignant) from other cystic lesions?
• Cyst fluid analysis –amylase, tumor markers, genomics / proteomics
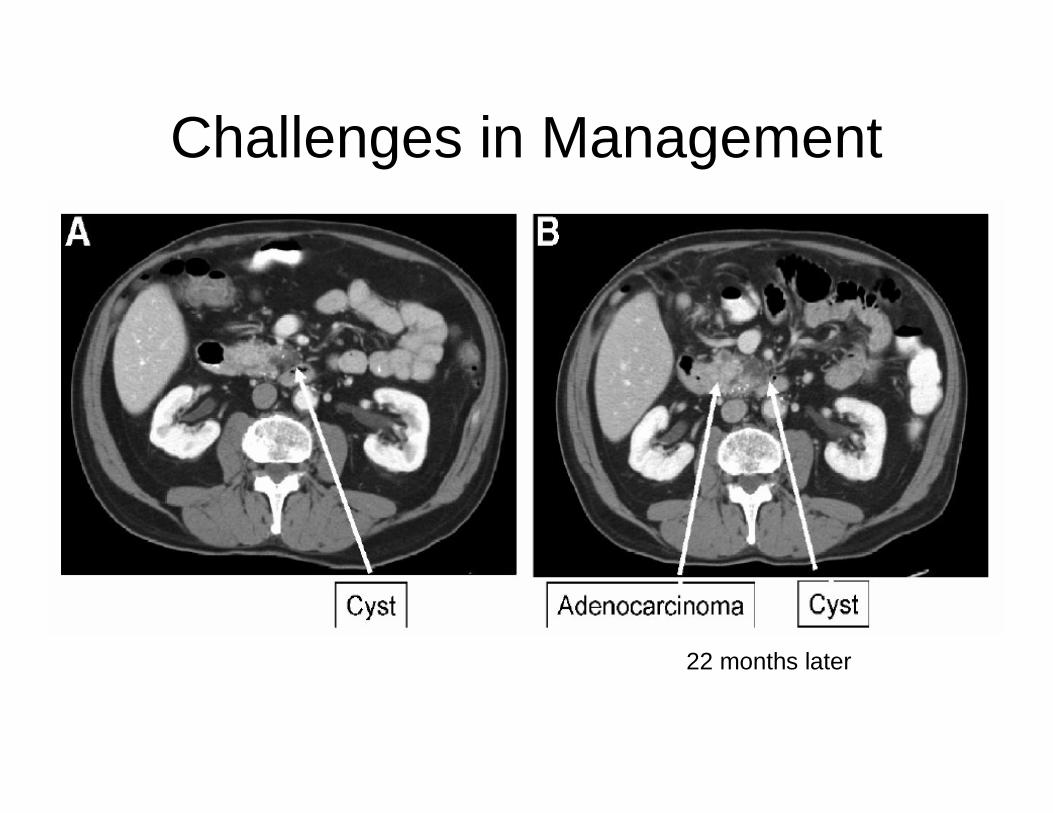
Challenges in Management
22 months later

Challenges in Management
• “Neither randomized control trials or systematic reviews of RCTs (level 1 evidence) nor cohort studies or reviews of cohort studies (level 2 evidence) have been published. Only one report fit the criteria for level 3 evidence (case control study)”
• After additional review and analysis, we considered only six reports to be “cornerstone papers” of merit for the final review”
Bassi C et al. J Gastrointest Surg 2008


Differential DiagnosisPseudocyst
Clinical• Gender• Age• Ethanol abuse• Pancreatitis history• Malignant potential• Location Imaging studies• Septae• Locularity• Calcifications
• Male• Variable• Yes• common• No• Variable
• Variable• Unilocular (usually)• None (adjacent parenchyma)
Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639--653 653

Pseudocyst
Mucinous Cystadenoma

Differential DiagnosisSerous Cystadenoma
Clinical• Gender• Age• Ethanol abuse• Pancreatitis history• Malignant potential• Location Imaging studies• Septae• Locularity• Calcifications
• Female (2-3:1)• 60’s• No association• Uncommon• No (rare)• Evenly distributed
• Yes• Multiple small (usually)• Yes (central sunburst or stellate)
Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639--653653

SEROUS CYSTADENOMA
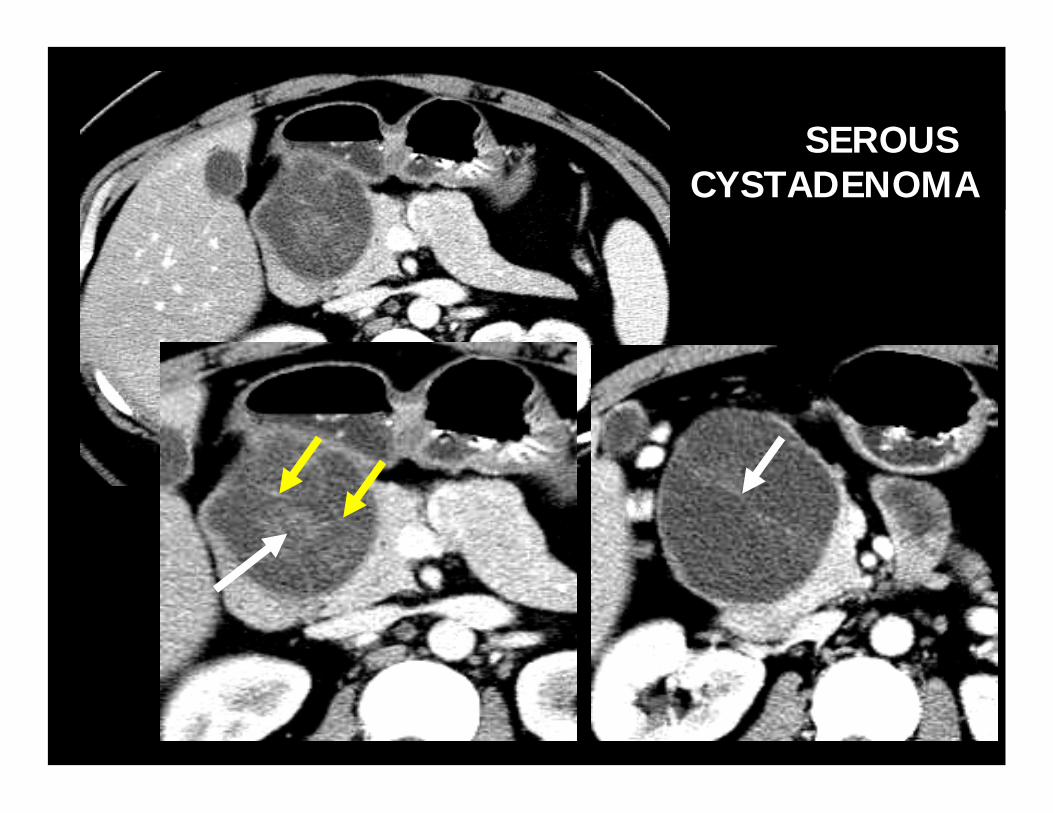
SEROUS CYSTADENOMA


Histology

Differential DiagnosisMucinous cystadenoma
Clinical• Gender• Age• Ethanol abuse• Pancreatitis history• Malignant potential• Location Imaging studies• Septae• Locularity• Calcifications
• Female • Adenoma (50-60’s) Ca (60-70)• No association• Uncommon• Yes• Variable
• Yes• Multilocular (usually)• Yes (peripheral, curvilinear)
Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639--653653


Histology

Mucinous Cystadenocarcinoma

Mucinous Cystadenocarcinoma

Differential DiagnosisIntraductal Papillary Mucinous
NeoplasmClinical• Gender• Age• Ethanol abuse• Pancreatitis history• Malignant potential• Location Imaging studies• Septae• Locularity• Calcifications
• Male (3-4:1)• 60’s• No association• Uncommon• Yes• Variable
• No• Multiocular (usually)• No
Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639Levy MJ, Clain JE. Clin Gastroenterol Hepatol 2004;2(8):639--653653

Histology

Curved reformat- IPMT-Main Duct Type

IPMT- SIDE BRANCH TYPE

IPMN vs. MCN
• Can we distinguish them preoperatively?– Ovarian stroma
• Risk of malignancy 6-36% (less if stroma)
• Criteria for resection of IPMN– Main duct: MPD<15mm, mural nodules– Branch duct: >3cm, mural nodules– Mixed types
Tanaka et al. Pancreatology 2006;6:17-32

IPMN: Branch Duct vs Main Duct
• Prevalence of cancer:–Main duct: invasive 43% (70% if CIS included)–Branch duct 15% (25% if CIS included)
• May be difficult to differentiate MCN from side branch IPMN
–Similar low malignancy risk?–Different risk of multifocality and need for
surveillance
Tanaka et al. Pancreatology 2006;6:17-32

Size < 1 cm Size 1-3 cm Size > 3 cm
MR or thin
slice CT
In 1 year
Size
< 1 cm
Size
1-2 cm
EUS and MRCP or ERCP
High-risk stigmata:Mural nodules
Dilated main duct
Positive cytology
No
MR or CT1-2 cm every 6-12 mo*
2-3 cm every 3-6 mo
Sumptomatic, size > 3cm or positive high-risk stigmata
No Yes
Resection
Yes
Tanaka et al. Pancreatology 2006;6:17-32
International Consensus Guideline on IPMN Management
*The interval of follow-up can be lengthenedafter 2 years of no change

SOLID PSEUDOPAPILLARY TUMOR
** *

SPPTP

Diagnostic Features of Pancreatic Cystic Lesions


Pancreatic Cystic LesionsPotential Management Strategies
• Additional Imaging Studies– CT– MRI (MRCP may show ductal communication with IPMN)– EUS +/- FNA
• Cyst fluid Characterization• Risk/Benefit assessment of surgical resection• Watchful Waiting


Table 1. Characteristics of Pancreatic Cystic Neoplams with Low Risk of Malignancy as Described in The Published International Guidelines*
1. Asymptomatic
2. Size < 30 mm
3. Main Pancreatic Duct Dilation < 6mm
4. No solid component within or associated with cyst on imaging
* Tanaka et al. Pancreatology 2006;6:28
Pancreatic Cystic LesionsDoes Size Matter?
• Retrospective study from MGH• 86 pts with cysts 3 cm or smaller• 48 operated; 38 monitored• 75 benign; 8 borderline malignant, 3
carcinoma in situ (PPV 87% for size)• Unilocular cysts PPV benign 97%• Septations poor for prediction of malignancy
PPV 20%
Sahani DV et al. Radiololgy 2006;238:912-919.

Pancreatic Cystic LesionsRole of EUS
• Endosonographic architecture – Not sufficient for accurate
classification– Solid mass and invasive tumor –
malignant• EUS appearance
– Serous: numerous small cysts with thin septae
– Mucinous: macrocystic-- uni- or multilocular
– IPMN: mural nodules may show invasive features and target for FNA
Pancreatic Cystic LesionsCyst fluid Characterization
• EUS FNA: safe and well tolerated <1% complication rate– Technique: limit passes, antibiotics
• Fluid analysis– Cytology: insensitive– Amylase/Lipase: confusing– Tumor Markers: CEA most useful
Pancreatic Cystic Lesions:The Cooperative Pancreatic Cyst Study
• 341 patients EUS + FNA• 112 surgical resection (68 mucinous, 7 serous, 27
inflammatory, 5 endocrine, 5 other)• ROC analysis: cyst fluid CEA > 192 ng/ml –
differentiate mucinous vs. non-mucinous (AUC .79)• CEA better than EUS morphology or cytology (50-
60%)• Cyst fluid CEA most accurate test to identify mucinous
lesion
Brugge et al. Gastroenterology 2004;126:1330Brugge et al. Gastroenterology 2004;126:1330--1336 1336

Pancreatic Cyst IdentifiedPancreatic Cyst Identified
SymptomaticSymptomatic
Surgical CandidateSurgical Candidate
MonitorMonitor EUSEUS
MonitorMonitor FNAFNA
SurgerySurgery MonitorMonitor
ResectionResection EUS +/EUS +/-- FNA to FNA to support support benign benign etiology etiology
(pseudocyst)(pseudocyst)
NO/BorderlineYes
CT diagnostic for serous lesionCT diagnostic for serous lesion
““DiagnosticDiagnostic”” for for serous lesionserous lesion
Mucinous Non-Mucinous
Yes No
NoYes
NoYes

Pancreatic Cystic Lesions
• Diagnostic Testing should influence management– Does EUS +/- FNA change surgical decision-making?– Costs and risks
• Collaborative approach with endoscopist, radiologist, pancreaticobiliary surgeon and GI pathologist
– Frozen sections for IPMN margins problematic• Patient must be actively involved in understanding
risks and uncertainties• Critical need for prospective, controlled data to provide evidence
based diagnostic and therapeutic strategies

Pancreatic Cystic LesionsWhat the future holds
• Improved diagnosis– Cyst fluid molecular analysis
• Gene markers• Mutational analysis• Proteomics (Crnogorac-Jurcevic T. et al
Gastroenterology. 129(5):1454-63, 2005)• Telomerase (Mishra G et al. GIE 2006;63:648-54)
– Trucut biopsy– Ethanol Lavage
Absolute criteria for who should/should not undergo surgical resection for a cystic pancreatic neoplasm do not currently exist
Rational approach:-All symptomatic patients who are reasonable operative risks should undergo surgical resection (in one a study malignant lesion was found in 40% of symptomatic pts compared to 17% of asymptomatic counterparts)
-Asymptomatic patients:-much less clear-things that push towards resection:
-any solid component in the cyst-CEA in cyst fluid elevated (79% specific for mucin-producingtumor (MCN or IPMT))
- good operative risk

Must balance risk of operation with risk of developing maligancy in tumor (numbers from operative series- so may not represent truly asymptomatic lesions)
Risk of malignancy:
• Serous cystadenomas (no malignant risk)
• Mucinous cystic neoplasms (MCN): about 8-30% have an invasive component: risk of malignant degeneration unknown-can occur even up to 15-20 years after diagnosis
• Intraductal mucinous papillary neoplasms (IPMN): about 1/3 have an invasive component; risk of malignant degeneration unknown; alsocan occur many years after presentation

Surgical Approaches to Cystic Neoplasms
• Lesion in head/neck/uncinate process: pancreaticoduodenectomy
• Lesion in body/tail: distal pancreatectomy and splenectomy
• Lesions diffusely involving the gland or involving the head and extending into the body: total pancreatectomy

Serous Cystadenoma• Indications for Surgery
-symptoms-large size*-inability to distinguish a serous cystic neoplasm from a mucinous lesion
• *Series of 106 pts (MGH)Rate of growth of lesion (24 pts had serial radiography)– < 4 cm: median growth of 0.12 cm per year– > 4 cm: median growth of 1.98 cm per year
Tseng et al. Ann Surg 2005; 242: 413-419.

Mucinous Cystic Neoplasms (MCN)• Series of 163 pts. from MGH and University of Verona• ovarian stroma required for diagnosis• Median size 5 cm. Average age 45 yrs. • 12% had invasive cancer. • All invasive cancers > 3cm; 84% of these had a solid
component• Argued all MCNs should be surgically resected
- avoid life-long monitoring- authors assume that all (or most) small MCN
progress to cancer over time
• Surgical complication rate: 49% overall morbidity, with a 24% pancreatic fistula rate, and 10% of patients requiring an interventional radiology procedure or re-operation.
Crippa et al. Ann Surgery 2008

Main duct IPMN or Mixed Variant IPMN
• Risk of malignancy thought to approach 70%
• Current recommendations are for surgical resection regardless of presence of symptoms

Branch Duct IPMN
• Resect if :>3 cm in sizesymptomsmural nodules
In the absence of these 3 criteria, observation may be indicated


Pancreaticoduodenectomy (Whipple procedure)

Distal Pancreatectomy

Total Pancreatectomy

Decision to operate a balance between risk of surgery and risk of cancer
Complications from Pancreatic Surgery
Death rate1) Whipple 1-3%2) Distal pancreatectomy 0.5%3) Total pancreatectomy 1-3%
Risk of diabetes1) Whipple 8-10% (removing 50% of gland)2) Distal pancreatectomy (can remove up to 70% and not get diabetes if remainder of gland is normal)3) Total pancreatectomy 100%

Surgical Resection
1) Serous cystadenomano follow-up needed
2) Non-invasive MCNno follow up needed
3) Invasive MCN (adenocarcinoma)treat like pancreatic adenocarcinoma

Surgical Resection- IPMN
• Two main typesmain ductside branch
Goal is complete resection with negative surgical margin
We rely on intraoperative frozen section in operating room

IPMN• Need to decide how you will approach a positive
margin in the operating room and discuss possible scenarios with the patient
• Frozen section margin status• Negative: operation complete• Positive for non-invasive IPMN (adenoma): proceed with further
resection, and total pancreatectomy if indictated, or consider surveillance program*
• Positive for carcinoma in situ or invasive IPMN: proceed with further resection, and total pancreatectomy if indicated*
(factors such as patient age, compliance, co-morbiditiescome into play)

IPMN
• Both main duct and side branch type IPMN’s can recur: all patients need to be enrolled in a surveillance program (CT or EUS)
• recurrence with negative margin: 7-10%

Thanks to Dr. Diane Simeone for mentoring me in pancreas surgery and for sharing her slides