swede heart prospective registry based randomized clinical trials (r-rct) – a new concept for...
TRANSCRIPT

SWEDE HEART
Prospective Registry based Randomized Clinical Trials (R-RCT) –
a new concept for clinical research
Lessons from the TASTE trial
Stefan James, Uppsala University
Sweden


3 Tricoci P et al. JAMA 2009;301:831-41Tricoci P et al. JAMA 2009;301:831-41
Which Treatment is Best for Whom?High-Quality Evidence is Scarce

11.7%
26.4%
15.3%
13.5%
12.0%
22.9%
6.4%
6.1%
23.6%
0.3%
9.7%
11.0%
19.0%
4.9%
4.8%
0% 10% 20% 30%
AF
Heart failure
PAD
STEMI
Perioperative
Secondary prevention
Stable angina
SV arrhythmias
UA/NSTEMI
Valvular disease
VA/SCD
PCI
CABG
Pacemaker
Radionuclide imaging
Level of Evidence ACurrent Guidelines

SWEDE HEART
SCAARThrombus aspirationin Sweden

Vlaar, P.J. et al. The Lancet 2008; 371:1915-20
TAPAS
Fröbert, O. et al. Int J Cardiol. 2010; 145:572-3
HR (95% CI): 1.21 (1.08-1.35)
/ Swedish registry data
PCI alone (N=16 417)
TA+PCI (N=3 666)

Strengths
• Data quality variable and questionable
• Cannot be used for comparative outcomes research
• Confounding factors can not be adjusted for despite advanced
statistical models
• Ideal for description of standars
• Unselected patient populations –generalizable
• Large number of events – makes it possible to identify rare events
• Inexpensive
Weaknesses
Register studiesObeservational studies (None-inverventional)

RandomizedStudies (RCT)
Non randomizedObservational studies
Randomized Controlled/Clinical Trials - RCT

Weaknesses
Strengths
Correctly designed studies with adequate power are gold standard
Extinguishes confounding
Highly selected populations due to exclusion criteria
Often selected specialized study centers
Often surrogate endpoints
Long time to plan and complete
Expensive
Often sponsored by industry- only studies with economic interest will be
performed
SWEDE HEART
Randomized Clinical Trials- RCT

Is a prosective randomized trial but it uses a clinical registry for one or several major functions for trial conduct.
Register based Randomized Clinical trials- R-RCT

Registry based Randomized Clinical trials - R-RCT
Strengths
• Correctly designed studies with adequate power are gold standard
• Extinguishes confounding
• Unselected patient populations –generalizable
• Large number of events – makes it possible to identify rare events
• Inexpensive
Weaknesses
• Data quality lower
• Variable definition
Number of cases annually: 80 000
RIKS-HIA 73 CCU hospitals, 100%
SCAAR 30 PCI hospitals, 100%
Percutaneous valves 7 hospitals, 100%
Heart surgery 7 hospitals, 100%
Secondary prevention 65 hospitals, 85%
>200 variables
(Baseline data, procedural and outcome measures)
At monitoring: 95-96% agreement between files and registry.

Data entry on line by the operator
Automatic linkage with population registry
Automated data checksClinical background and prior CV disease
Angiographic background data
Administrative data
Name, personal ID number

Two questions need to be answered:
Did the patient consent orally?Are inclusion and no exclusion
criteria met?
Did the patient consent?
Are inclusion and exclusion crieteria met?

Information for consent
Did the patient consent?
Are inclusion and exclusion crieteria met?

Randomize and store data
Did the patient consent?
Are inclusion and exclusion crieteria met?

Randomized
All primary PCI:s
7244 patients
Date
Patients
TASTE inclusion rate
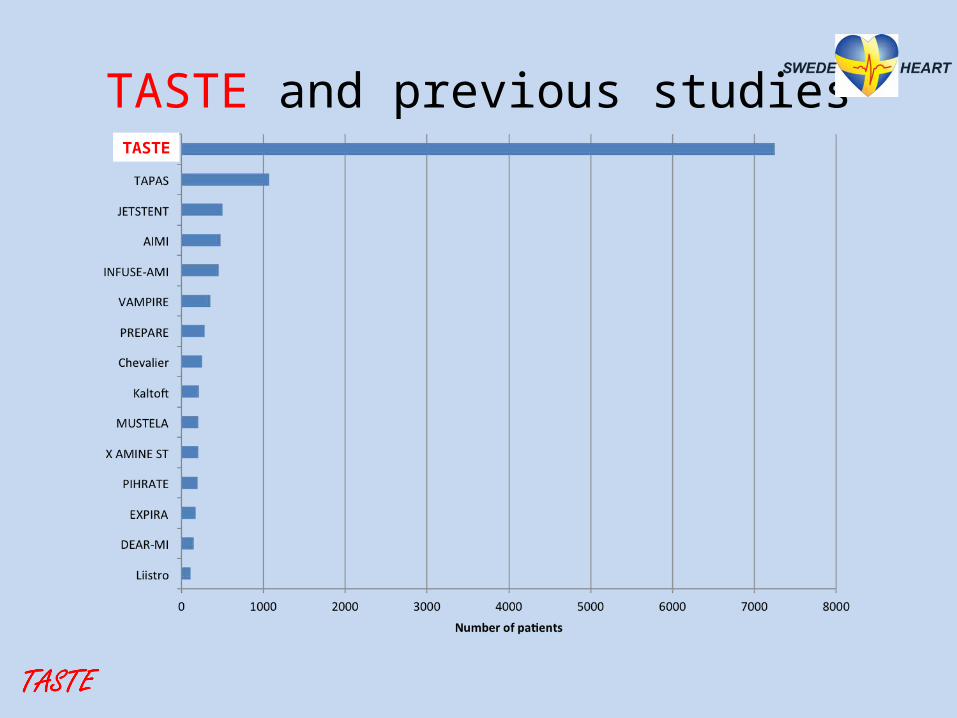
TASTE and previous studiesTASTE

All patients with STEMI in Sweden and Iceland undergoing
primary or rescue PCI. N=11 709 *)
Enrolled in TASTEN=7259
N=3621 assignedto thrombus aspiration
N=3399 underwentthrombus aspirationN=222 underwentconventional PCI
TASTE trial enrollment flow chart
Not enrolled N=4697
N=3623 assignedto conventional PCI
N=3535 underwent conventional PCI
N=1162 underwentthrombus aspiration
N=3445 underwentconventional PCIN=178 underwent
thrombus aspiration
N=3621 werefollowed up
N=3623 werefollowed up
N=1162 werefollowed up
N=3535 werefollowed up
Enrolled in DenmarkN=247
Erroneous enrollments
N=15
Randomized in TASTEN=7244
No patients (0) were lost to follow-up of the
primary outcome!

All-cause mortality up to 1 year
HR up to 1 year 0.94 (0.78 – 1.15), P=0.57
HR up to 30 days 0.94 (0.72 - 1.22), P=0.63

2.72.7
Reinfarction
HR 1 year 0.97 (0.73 – 1.28), P=0.81
HR 30 days 0.61 (0.34 - 1.07), P=0.09
Stent thrombosis
HR 1 year 0.84 (0.50 – 1.40), P=0.51
HR 30 days 0.47 (0.20 - 1.02), P=0.06
Lagerqvist NEJM 2014


New concept for clinical research
Combines the advantages of a clinical registry and
randomized study
Complement to classical RCT –No substitute
•RRCT
•Evaluation of therapeutic options available/used in
routine clinical care
RCTApproval of new
pharmaceutical agents and medical devices
R-RCT vs. classical RCT

• Identify patients• Randomize• Collect baseline and procedure characteristics (CRF)• Assist with and collect consent forms • Identify clinical endpoints (endpoint detection)• Control clinical outcome events (adjudication, CEC)
Some or all parts of trial
What can a registry do?

RCT R-RCT
Strategy +
Device – CE mark, used +
Device, first in man +
Approved drugs used in clinical practise
+
Drugs for new indication + +
New drugs +
Study design

• Simple hypotesis, one question- one answer • Sub-studies limited and simple• Treatment alternatives available • Well defined randomized options• Open lable with blinded evaluation of events (PROBE)• Blind, placebo controlled?
Study design

- Well defined, death optimal
- Clinical
- Complete
- Available (Delay for Swedish hospital admission registry)
- Central clinical event committee (CEC) is needed if not well defined events- particularly for open label trials
Endpoints

Data base
Informed consentRandomisation code
Incl-/exclusion critera
Extra study specificvariables
Clincial register (variabler ex. personual ID) Study database
Alla variabler
Personal ID replaced to study coode
Cannot be changed
Analyse databas
Personal ID replced with study code
Relevant registry variables
Available for registry staff/ PI
Possibility to remove patients from registry
Available for registry staff/ for registry staff/trialists
Not possible to remove patients from a trial
Available
Data checks
All patients kept untial behålls tills ev återtaget samtycke
Other national registries (PAR, LM, )

Study design
Primary Endpoint: 1-year total mortalityAdditional secondary endpoint and sub studies
Data analysis through SWEDEHEART registry and national mortality registry
*Inclusion criteria:• symptoms suggestive of AMI within 6h• SpO2 ≥ 90%• ≥ 30y• ECG changes indicating ischemiaand/or elevated troponin levels

VALIDATE (n=6000) Bivalirudin versus Heparin in NST and ST- Elevation myocardial infarction in patients on modern
antiplatelet therapy in SWEDEHEART,
DETOX-AMI (n=7000)DETermination of the role of OXygen in Acute Myocardial Infarction,
SWEDEPAD (n=2480)SWEdish Drug Elution trial in Peripheral Arterial Disease. DES vs BMS and DEB vs POBA.
IFR SWEDEHEART (n=2000)Instantaneous Wave-Free Ratio versus Fractional Flow Reserve in ACS
PROSPECT-2 (n=1200, hybrid trial)Providing Regional Observations to Study Predictors of Events in the Coronary Tree. Evaluate
future events from cholesterol plaques detected by near infrared spectroscopi
DISCO (n=2480)Evaluate if patients with out of hospital cardiac arrest should undergo routine coronary angiography
U-CARE (n=500)Evaluation of internet based cognitive behavioural therapy (iCBT) versus usual care in patients with
depression/anxiety post MI.
Ongoing R-RCT

• Large need for randomized trials (RCT) particularly for the evaluation of strategies, devices, pharmacological therapies
• Classical RCTs are often not performed in broad representative patient populations
• The national clinical registries are strong networks for collaboration and enroll complete patient populations
• Prospective Registry based Randomized Clinical Trials (RRCT) is a new opportunity for clinical research
• RRCT is ideal for one clinically important hypothesis with reliable hard endpoints
• Large need for randomized trials (RCT) particularly for the evaluation of strategies, devices, pharmacological therapies
• Classical RCTs are often not performed in broad representative patient populations
• The national clinical registries are strong networks for collaboration and enroll complete patient populations
• Prospective Registry based Randomized Clinical Trials (RRCT) is a new opportunity for clinical research
• RRCT is ideal for one clinically important hypothesis with reliable hard endpoints
Conclusions