syamhanin adnan supervisors : prof david …jknj.moh.gov.my/jsm/day1/one dose does not fit all -...
TRANSCRIPT

Syamhanin AdnanSupervisors : Prof David PatersonDr Jason RobertsDr Steven WallisProf Jeffrey Lipman



Case study
PK/PD issues in critically ill
My PhD project : implication into practice
Project 1: The drain study
Project 2 : Amp/sul & MDR-Ab
Project 3 : ARC

Ertapenem in hypoalbuminaemia and ARC

Case 1 – 38yo male (175cm and 92kg) Admitted to ICU with hypoxia post Ivor-Lewis
Oesophagectomy Day 7 – Mediastinitis diagnosis
Tracheo-oesophageal fistula
E. cloacae isolated from ETA
Susceptible mero/erta
Ertapenem prescribed
▪ 1gm IV q12h (EUCAST MIC90 = 0.5-1mg/L)
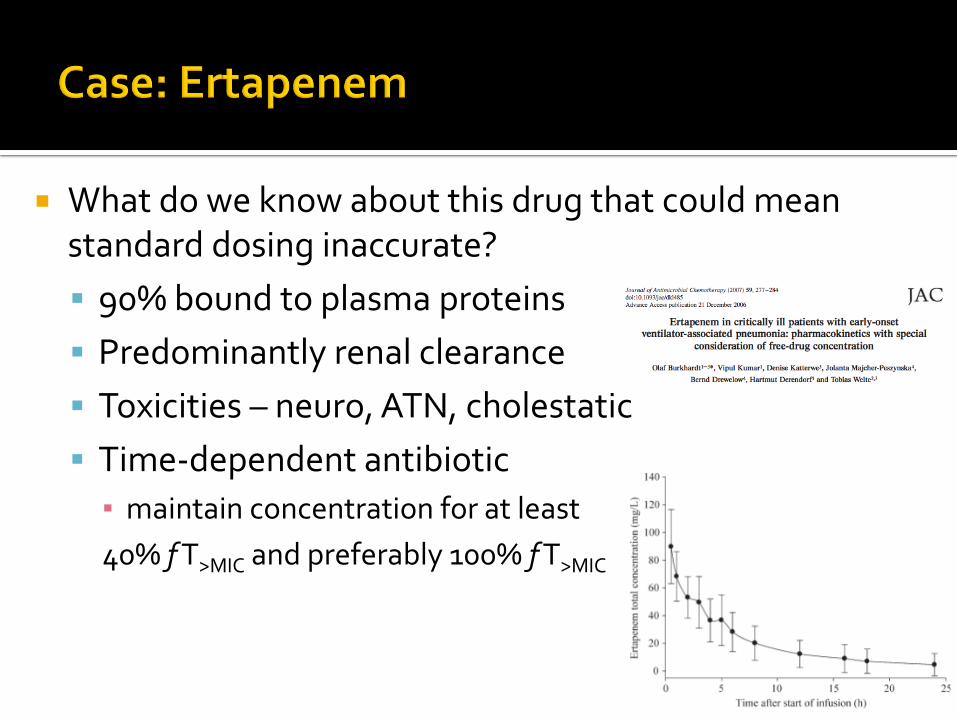
What do we know about this drug that could mean standard dosing inaccurate?
90% bound to plasma proteins
Predominantly renal clearance
Toxicities – neuro, ATN, cholestatic
Time-dependent antibiotic
▪ maintain concentration for at least
40% f T>MIC and preferably 100% f T>MIC
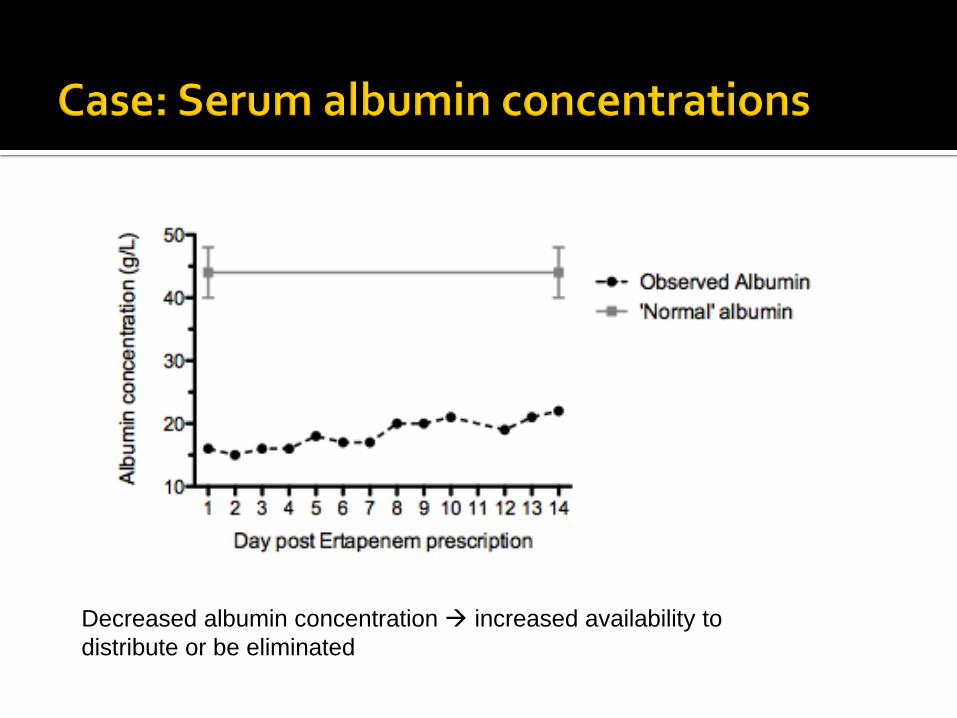
Decreased albumin concentration increased availability to
distribute or be eliminated

Increased CrCL increased clearance of unbound drug

Dose = 1g IV q12h; level actually <0.1mg/L

Dose inc 1g q8h

Dose inc 1g q8h by
extended infusion

Level ‘therapeutic’
(target = 100% f T>MIC)

Day 17, a further E. cloacae isolate (sample collected day 14) was cultured
Ertapenem MIC E-test performed
Now resistant; MIC = 4mg/L Patient changed to meropenem (MIC = 0.3 mg/L) 4/52 course completed with meropenem

Highly protein bound drugs in ICU
PK dramatically changes
~50% of ICU patients have low albumin
Drugs with renal excretion
Clearance can dramatically change
ARC present in ~30% of patients

Lesson learn, the hard way

Demographic : 33 y/o lady CC :
Post trauma D4, MVA (car vs concrete pillar) HOPI
patient as passenger, car driven by a friend (both under alcohol influence and he died)
GCS full upon arrival, intubated later in view of tachypnoea and metabolic acidosis

Past Medical History
Left thyroid nodule (euthyroid on latest TFT) Social/Family History
Divorce with one child
stays with sister
Owns online business Medication
IV Pip/taz on 22/9 and de-escalate to IV Ceftriaxone on 24/9

Issues :
Transected body of pancreas with duodenal perforation (post laparotomy)
Septic shock secondary to pancreatitis
AKI
ARDS (resolved)
Hypoalbuminemia

No Antibiotic Dose Freq Date
start Indication D1 D2 D3 D4 D5 D6 D7 D8 D9 D10 D11 D12 D13 D14
1 Pip/tazobactam 22/9 -24/9 HKL 22/9 23/9 24/9
2 Ceftriaxone 24/9 HKL 24/9
3 Pip/tazobactam 2.25g QID
24/9 –
26/9 Empiric/ 24/9 25/9 26/9
Pancreatitis
4 Imipenem 500mg BD 26/9 Empiric/ 26/9 27/9 28/9 29/9 30/9 1/10 2/10 3/10 4/10 5/10 6/10 7/10 8/10 9/10
13/10 Pancreatitis
10 /
10
11 /
10
12/
10
5 Fluconazole 400mg stat 27/9-3/10 Empiric/ 27/9 28/9 29/9 30/9 1/10 2/10 3/10
200mg od Definitive ?(3/10)
6 Amikacin 750mg od 27/9 Empiric 27/9
1gm od 1/10-8/10 1/10 2/10 3/10 3/10 4/10 5/10 6/10
7 Vancomycin 1g od 29/9-1/10 Empiric 29/9 28/9 29/9 30/9
1g EOD 2/10-9/10 2/10 3/10 4/10 5/10 6/10 7/10 8/10
8Colistiin 2 MU TDS 14/10 CRE
14/
10
15/
10
16/
10
17/
10
18/
10
19/
10

Date Source Pathogen Sensitivity Resistant
26/9
1/10 Blood NG
26/9
29/10 T/Asp NG
26/9 Urine NG
29/9
5/10 Blood NG
29/9
1/10 NPA (Respiratory) NG
29/9
30/9 SP (Abd) Mixed Growth
30/9
3/10 SP (Abd) NG
2/10
7/10 Pleural Fluid NG
2/10
7/10 Abd Fluid NG
3/10 Body Fluid Candida non-albicans Probably contaminant
8/10
14/10 Blood CRE
Tigecycline
Polymycin
Colistin
All carbapenems

No Antibiotic Dose Freq Date
start Indication D1 D2 D3 D4 D5 D6 D7 D8 D9 D10 D11 D12 D13 D14
4 Imipenem 500mg BD 26/9 Post op 26/9 27/9 28/9 29/9 30/9 1/10 2/10 3/10 4/10 5/10 6/10 7/10 8/10 9/10
13/10
WBC 31.5 41.83 37.38 33.53 30.88 30.84 27.31 21.6 14.5 13.7 12.9 14.3
Temperature 38.1 37.6 36.9 38.3 37.8 37.0 38.0 38.0 37.7 37.7 37.5 38.6 37.8
CrCl (ml/min) 35 39 38 34 33 36 47 53 77 73 97 100
Urine output
(ml/hr) 80 60 50 100 50 100 100
10 /
10
11 /
10
12/
10
WBC 14.1 13.2 14.5 12.3
Temperature 38.4 37.7 37.2 37.0
CrCl (ml/min) 118 111 126 147
Urine output
(ml/hr)

Patient have multiple drains :▪ Drain A : 10-50cc, Drain B : 400-550cc, pelvis, pigtail
Elevated renal function ▪ CrCl >100ml/min on D11 of imepenem▪ ICU Pharmacist suggest to increase dose to 1gm bd in view of
penetration and high WBC on D5 of imipenem▪ T/o to HDW on D12 of imipenem
Prolonged duration of imipenem▪ HPB Pharmacist inform that patient already completed D14 of
imipenem on 10/10/2014
CRE isolated on D17 of imipenem


Demographic :68 y/o male CC :
Post trauma, MVA (motorbike vs lorry) HOPI
Refer to HSB
Intubated for poor GCS
Bilateral decompressive craniectomy with EVD insertion

Issues :
Generalized cerebral edema
HAP
Ventriculitis
AF
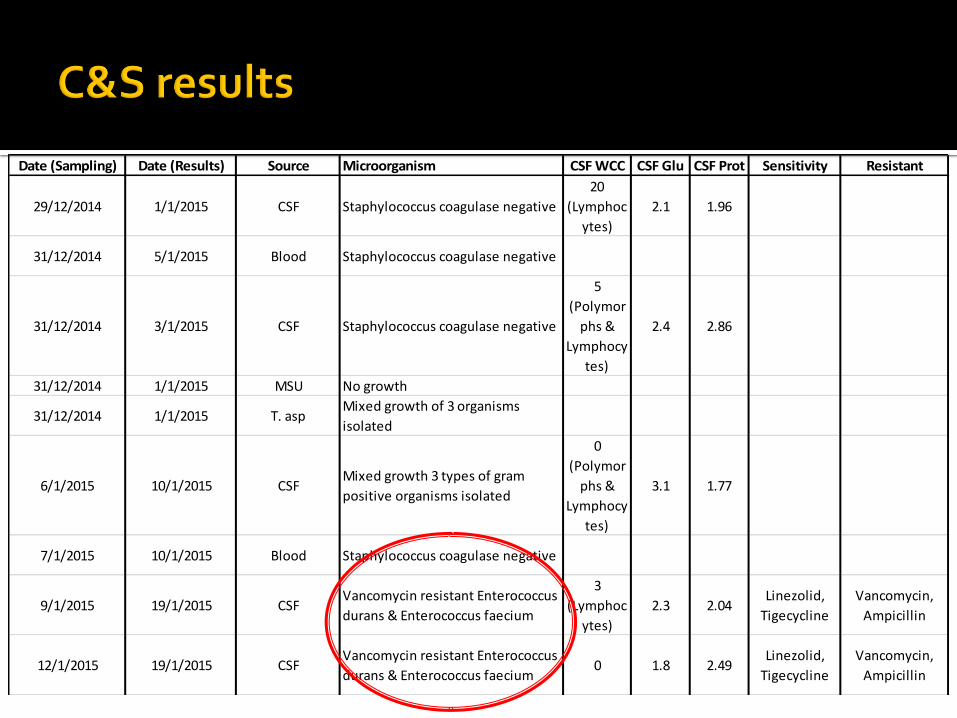
29/12/2014 1/1/2015 CSF Staphylococcus coagulase negative
20
(Lymphoc
ytes)
2.1 1.96
31/12/2014 5/1/2015 Blood Staphylococcus coagulase negative
31/12/2014 3/1/2015 CSF Staphylococcus coagulase negative
5
(Polymor
phs &
Lymphocy
tes)
2.4 2.86
31/12/2014 1/1/2015 MSU No growth
31/12/2014 1/1/2015 T. aspMixed growth of 3 organisms
isolated
6/1/2015 10/1/2015 CSFMixed growth 3 types of gram
positive organisms isolated
0
(Polymor
phs &
Lymphocy
tes)
3.1 1.77
7/1/2015 10/1/2015 Blood Staphylococcus coagulase negative
9/1/2015 19/1/2015 CSFVancomycin resistant Enterococcus
durans & Enterococcus faecium
3
(Lymphoc
ytes)
2.3 2.04Linezolid,
Tigecycline
Vancomycin,
Ampicillin
12/1/2015 19/1/2015 CSFVancomycin resistant Enterococcus
durans & Enterococcus faecium0 1.8 2.49
Linezolid,
Tigecycline
Vancomycin,
Ampicillin
Date (Sampling) Date (Results) Source Microorganism CSF WCC CSF Glu CSF Prot Sensitivity Resistant

Date 1-Jan 2-Jan 3-Jan 4-Jan 5-Jan 6-Jan 7-Jan 8-Jan 9-Jan 10-Jan 11-Jan 12-Jan 13-Jan 14-Jan 15-Jan 16-Jan 17-Jan
Antibiotic
Meropenem 2g Q8H
Vancomycin 1.25g stat &500mg Q12H
Vancomycin 750mg Q12H
Vancomycin 750mg Q8H
Cefo/sulbactam 4g Q8H
Linezolid 600mg Q12H until 6/2
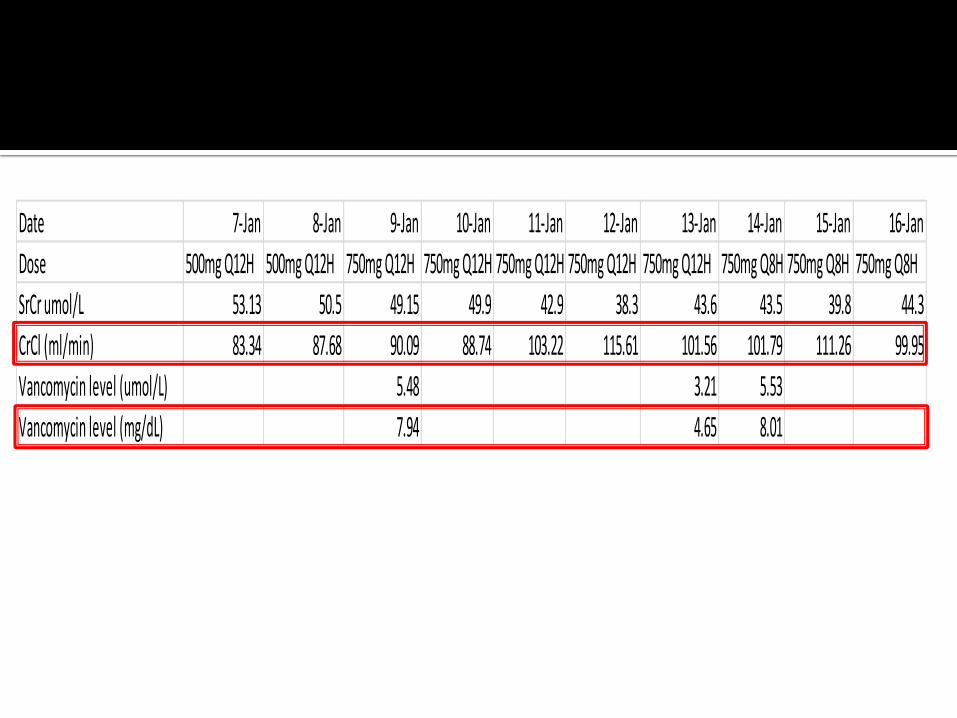
Date 7-Jan 8-Jan 9-Jan 10-Jan 11-Jan 12-Jan 13-Jan 14-Jan 15-Jan 16-Jan
Dose 500mg Q12H 500mg Q12H 750mg Q12H 750mg Q12H 750mg Q12H 750mg Q12H 750mg Q12H 750mg Q8H 750mg Q8H 750mg Q8H
SrCr umol/L 53.13 50.5 49.15 49.9 42.9 38.3 43.6 43.5 39.8 44.3
CrCl (ml/min) 83.34 87.68 90.09 88.74 103.22 115.61 101.56 101.79 111.26 99.95
Vancomycin level (umol/L) 5.48 3.21 5.53
Vancomycin level (mg/dL) 7.94 4.65 8.01

Roberts, J.A. and J. Lipman, Pharmacokinetic issues for antibiotics in the critically ill patient. Crit Care Med, 2009. 37(3): p. 840-51; quiz 859.


49 y/o male
Alleged MVA, referred from HTAR
Cerebral bleed, complicated with ventriculitis
MRSA from nasal swab and sputum
Treated with IV Vancomycin

0
5
10
15
20
25
10-May 11-May 12-May 13-May 14-May
Van
com
ycin
le
vel (
mg/
L)
Patient level
Min level
Max level
1.5g Q8H
1 Q6H
1.75g
incremental dose
2 hour infusion Q6H


0
500
1000
1500
2000
2500
3000
3500
Urine Output (ml)
Urine Output (ml)

10/25/2015 36








Vd : volume in which the total amount of drug
distributed to produce the observed blood
concentrations 13
CL : volume of drug cleared per unit time14

Hydrophilic drugs – Vd consistent with TBW (0.2-0.7 L/kg)
Lipophilic drugs – large Vd(can be variable eg. morphine 3L/kg amiodarone 70L/kg)
▪ Lipophilic drugs have very good distribution throughout body tissue
The volume into which a drug appears to be
distributed with a concentration equal to
that of plasma


Pharmacokinetic issues for antibiotics in the critically ill patient, Jason A. Roberts, B Pharm
(Hons); Jeffrey Lipman, FJFICM, MD, Crit Care Med 2009 Vol. 37, No. 3

-accumulation of fluids in extra-vascular compartment7
Sepsis
Hepatic failure
Fluid resuscitation
Burns
Others
-anti-inflammatory cytokines- capillary leakage
- dehydration-aggressive fluid therapy
Acute Kidney Injury
- impaired sodium excretion
- fluid expansion
- capillary leakage
- i.e pregnancy etc

-40 -50% of critically ill patients had hypoalbuminemia10
- less albumin available causing more free drug initially
- to achieve equilibrium state with the bounded drug, the extra free drug will later distributes into extravascular compartment
-less free drug available to exert pharmacological effect
el Castillo JRE, Elsener J, Martineau GP. Pharmacokinetic modeling of in-feed tetracyclines in pigs using a meta-analytic compartmental approach. Swine Health Prod. 1998;6(5):189-202.
The rate of drug elimination from body
Hydrophilic drugs – predominates through kidneys
Lipophilic drugs – predominates through liver

Acute kidney injury
Liver failure
Cardiovasculardysfunction
- 35% of ICU patient had AKI 8
- AKI patient had reduce glomerular filtration
- impaired drug metabolism- impaired elimination
- impaired perfusion - affecting drug distribution
-26.8% of sepsis patient will be prescribed with renal replacement therapy9

ARC
Increased systemic perfusion and cardiac output due to SIRS
Lead to an increased in renal blood flow
Enhanced renal elimination due to increased renal blood flow
Udy, A.A., et al., Augmented renal clearance: implications for antibacterial dosing in the critically ill. Clin Pharmacokinet, 2010. 49(1): p. 1-16.

Distribution phase
Elimination phase
Vd : volume in which the total amount of drug
distributed to produce the observed blood concentrations
CL : volume of drug cleared per unit time
increasedistribution
causing inadequate
concentrations
decreased elimination
causing accumulation
Consider decrease dose
interval 14
Reduced dose/prolong
interval 14
increased elimination inadequate
concentrations
Consider loading dose15


Project 1 : Dosing of Meropenem and Piperacillin in Patients with indweling surgical drains
Project 2 : Dosing of Ampicillin/Sulbactam in MDR-Ab
Project 2 : Prevalence of Augmented Renal Clearance : Experience in Malaysian Intensive Care Unit


Time concentration profile of meropenem and piperacillin in critically ill patients with indwelling surgical drains
Black lines : plasma concentrations
Grey lines : surgical drain concentrations
Dashed black line : EUCAST MIC breakpoint for P. aeruginosa (2mg/L for meropenem and 16mg/L for piperacillin)

Linear regression analysis showing relationship between drain clearance and output volume of surgical drains
Meropenem(r2=0.89; p=0.05)
Piperacillin (r2=0.63; p=0.20).


Acinetobacter spp is responsible for 25.4% of the organisms isolated in the presence of VAP in Malaysian ICU
Few options available: cefoperazone/sulbactam, ampicillin/sulbactamand/or polymyxin, sulbactam has intrinsic antimicrobial activity against Acinetobacter spp.
Since sulbactam is a bacteriostatic agent, it is recommended for use as high doses; which can increase the risk of toxicity.
Ampicillin is T>MIC; sulbactam : AUC/MIC, emerging data suggests T>MIC
for sulbactam. CLSI MIC breakpoints for ampicillin/sulbactam for susceptible, intermediate and resistant A. baumannii are 8/4 mg/L, 16/8 mg/L and 32/16 mg/L, respectively.
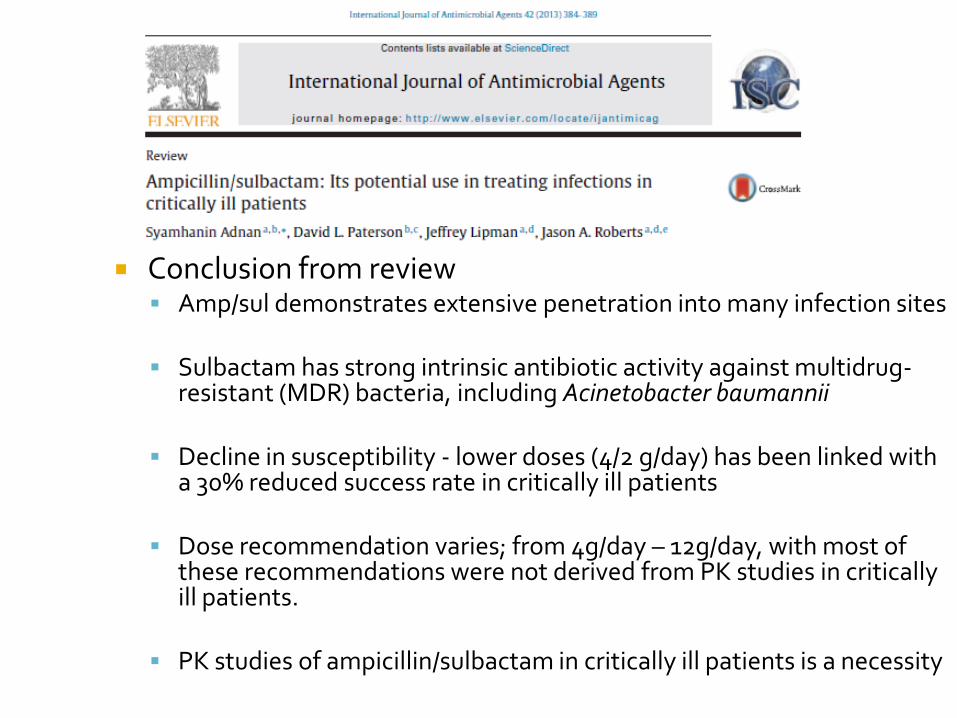
Conclusion from review Amp/sul demonstrates extensive penetration into many infection sites
Sulbactam has strong intrinsic antibiotic activity against multidrug-resistant (MDR) bacteria, including Acinetobacter baumannii
Decline in susceptibility - lower doses (4/2 g/day) has been linked with a 30% reduced success rate in critically ill patients
Dose recommendation varies; from 4g/day – 12g/day, with most of these recommendations were not derived from PK studies in critically ill patients.
PK studies of ampicillin/sulbactam in critically ill patients is a necessity
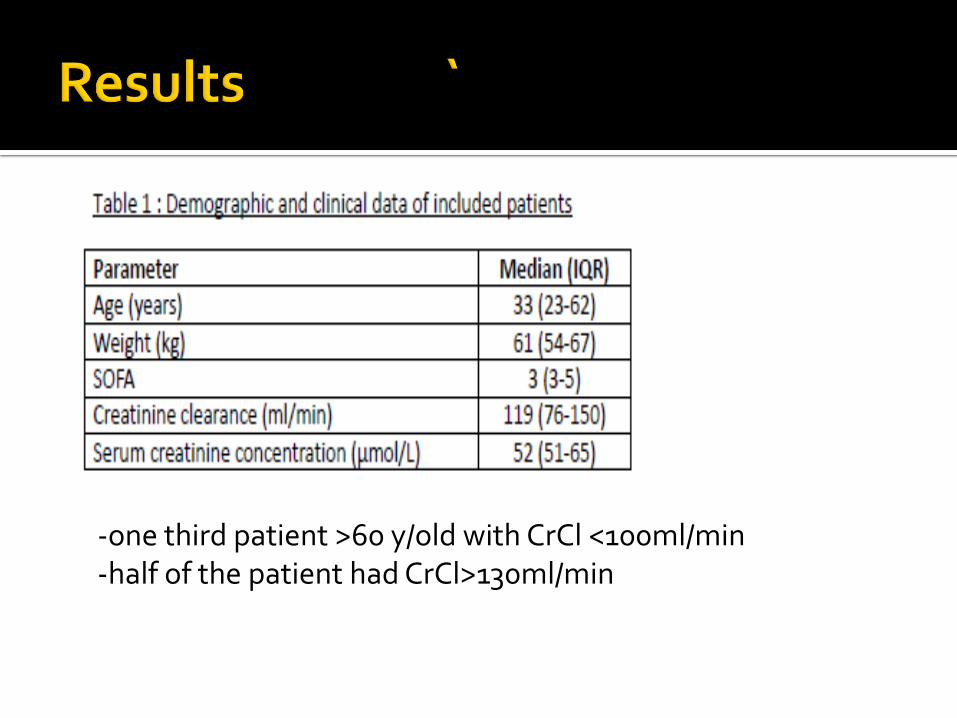
-one third patient >60 y/old with CrCl <100ml/min-half of the patient had CrCl>130ml/min




Significant correlation between drug clearance and renal clearance
risk of excessive drug concentrations with decreased renal function when high doses is used (>50mg amp/>20mg sul)
risk of inadequate drug concentrations with elevated renal function (>130ml/min); <10mg amp/<5mg sul)

Increased drug distribution for amp/sul in critically ill patients
risk of inadequate drug concentrations for those with increased drug distribution (Vd)
some patients did not achieve PK/PD target for sulbactam.

Dosing simulation for sulbactam showed failure to achieve the PK/PD target for MICs ≥ 4 mg/L with our current dosing regimens (6g/day) for patients with GFR ≥ 100 mL/min.
The probability of target attainment was obtained by counting the subjects who achieved 50% fT>MIC.
The target MIC’s were 0.5, 1, 2, 4 and 8 mg/L.

Dose adjustment of ampicillin/sulbactamaccording to the renal function to avoid potential toxicity in impaired renal function
Higher dose required for those patients with potential increased drug distribution
Current amp/sul dosing (12/6g per day) may not be optimal for those patients with creatinine clearance >100ml/min


Dose reduction of renally cleared drugs is common for impaired renal function but not for elevated renal clearance.
Recent article - discontinuation of industry-sponsored clinical trials due to poor outcomes in the study drug arm. Many were younger, higher renal clearances, with
no dose adjustment - may have led to inferior outcomes


Augmented renal clearance, ARC is defined by an elevated creatinine clearance which is used as a surrogate of GFR. Values ≥ 130 ml/min/1.73m2, have been proposed as a useful threshold

Inclusion criteria :1) admission to the ICU with expected length of stay >24 hours, 2) admission serum creatinine concentration <120 µmol/L)3) no history of chronic kidney disease, or renal replacement therapy.
Excluded criteria : 1) absence of invasive haemodynamic monitoring2) absence of an indwelling urinary catheter (IDC) 3) “Risk” stage of AKI (> 1.5 fold increase in serum creatinine from
baseline or urine output< 0.5ml/kg/hr for > 6hrs prior to enrolment





39% of the studied cohort manifested ARC on admission; since the studied cohort only represent 18% of the population - true prevalence of 7%
Trauma patients undergone emergency operations more likely manifest ARC on ICU admission
The majority of ARC patients suffered traumatic brain injury (TBI)
Poor relationship between CG estimated and measured urinary Crcl in ARC patients
Bland-Altman analysis confirms significant bias and imprecision
Bias becomes significantly larger in patients exhibiting ARC

Accurately identifying patients with ARC in the ICU setting is important.
Since bias becomes significantly larger in patients exhibiting ARC, it is suggested that a measured urinary Crcl be used for ICU patients at risk of ARC.

Studies have shown that PK/PD targets may not achieved in ARC patients
Recent simulations of doripenem dosing demonstrated that extended infusions are an effective tool in patients with ARC
Unlike prescribing behaviours in the presence of decreasing GFR, elevated renal clearance is rarely associated with dose modification.

Patient at risk of under-dosing :
Hydrophilic antibiotics in :▪ Fluid overloaded
▪ Drainage
▪ Elevated renal clearance ( young, male, post trauma, neurosurgical patient)
High protein bound antibiotics in hypoalbuminemiapatient
Lipophilic antibiotics in 0bese patient






Quran, Surah Ar-Rahman: 7-9
`..and He made the balance that you may not be inordinate in respect of the measure and keep up the balance with equity and do not make the measure deficient.."

