systemic hypertension definitions of hypertension elevated arterial blood pressure is a major cause...
TRANSCRIPT

SYSTEMIC SYSTEMIC HYPERTENSIONHYPERTENSION

SYSTEMIC HYPERTENSIONSYSTEMIC HYPERTENSION
Definitions of hypertension
Elevated arterial blood pressure is a major cause of premature vascular disease leading to cerebrovascular events, ischaemic heart disease and peripheral vascular disease.
Blood pressure is the pressure exerted by the blood against the walls of the blood vessels, especially the arteries.
It varies with the strength of the heartbeat,
the elasticity of the arterial walls, the volume and viscosity of the blood,
and a person's (health, age, and physical condition

Age
onset between 30 - 50 years of age increases over 65 years of age sex - males in young adulthood and early
middle age females after the age of 55 years

The prevalence
hypertensions is higher among blacks and older persons, especially older women
Hypertension increased with age, and is higher in young men than in young women, although the reverse is true in older adults.
Hypertension - IntroductionHypertension - Introduction
Silent Killer – painless complications It is the leading risk factor –MI, HF, CRF
Stroke Responsible for the majority of office visits, Number one reason for drug prescription. 25% of population Complications bring to diagnosis but late…
This requires the heart to work harder than normal to circulate blood through the blood vessels.
Blood pressure is summarised by two measurements, systolic and diastolic
which depend on whether the heart muscle is contracting (systole) or relaxed between beats (diastole).

Normal blood pressure at rest is within the range of 100-140mmHg systolic (top reading) and 60-90mmHg diastolic (bottom reading).
High blood pressure is said to be present if it is persistently at or above 140/90 mmHg.

Ideal Mean Aterial Pressure
(MAP) is defined as 93 mm of mercury, which corresponds to 120/80 and can be calculated by MAP = DP + 1/3 (SP-DP).
Mean Arterial blood pressure depends on the flow of blood from the heart (cardiac output) and the resistance to flow in the small arteries and microscopic resistance vessels (arterioles)
Regulation of BP:Regulation of BP:
BP = Cardiac Output x Peripheral Resistance Endocrine Factors
– Renin, Angiotensin, ANP, ADH, Aldosterone. Neural Factors
– Sympathetic & Parasympathetic Blood Volume
– Sodium, Mineralocorticoids, ANP Cardiac Factors
– Heart rate & Contractility.
Classification of blood of blood pressure
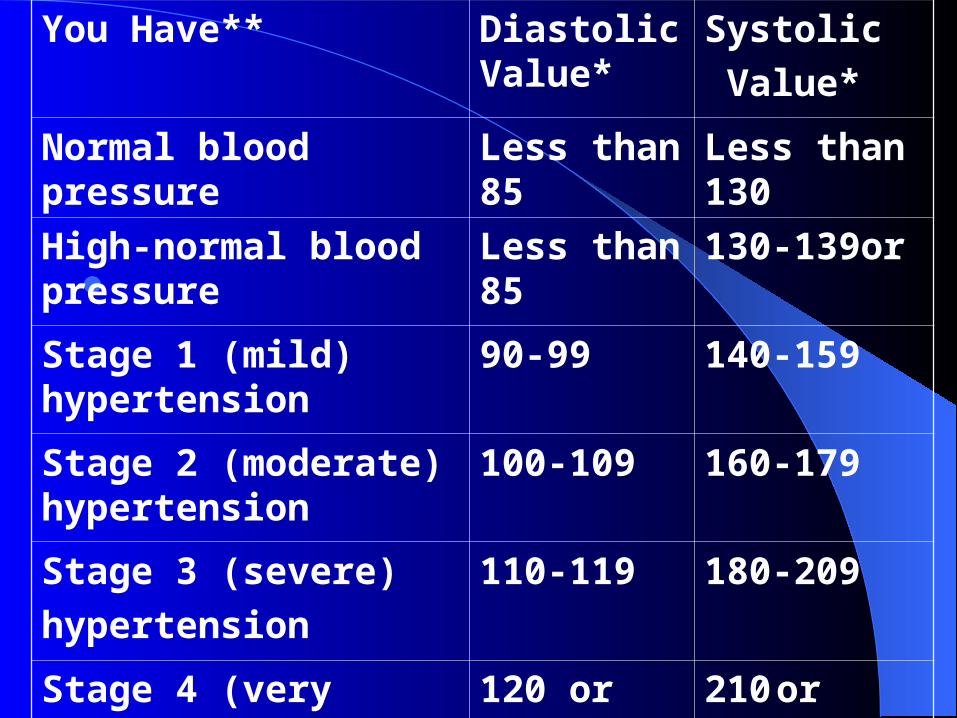
You Have** Diastolic Value*
Systolic
Value*
Normal blood pressure Less than 85 Less than 130
High-normal blood pressure
Less than 85 130-139or
Stage 1 (mild) hypertension
90-99 140-159
Stage 2 (moderate) hypertension
100-109 160-179
Stage 3 (severe)
hypertension
110-119 180-209
Stage 4 (very severe)
hypertension
120 or higher
210 or higher

Signs and symptoms
Hypertension is rarely accompanied by any symptoms, and its identification is usually through screening, or when seeking healthcare for an unrelated problem. A proportion of people with high blood pressure reports
headaches (particularly at the
back of the head and in the morning),
lightheadedness, vertigo, tinnitus (buzzing or hissing in the ears), altered vision or fainting episodes
These symptoms however are more likely to be related to associated anxiety than the high blood pressure itself

Control of Blood Pressure:Control of Blood Pressure:
BPCardiac Output
PeripheralResistance
Blood VolumeNa+, Aldosterone
VasoconstrictorsAngiotensin II
CatecholaminesVasodilatorsPg & Kinins
Local FactorspH, Hypoxia
Neural FactorsAdrenergic – Consß Adrenergic - Dil
Cardiac FactorsRate & Contract..
Humoral Factors
Peak blood pressure
Peak blood pressure levels in humans occur during the mid morning (at about 10:00 AM) then decrease progressively throughout the remainder of the day to reach a trough value the following morning at around 3:00 AM

Definition of Circadian Rhythm
Circadian rhythms are daily cycles of physiology and behavior that are driven by an endogenous oscillator with a period of
approximately one day

Normally, circadian rhythms
are synchronized with the 24.0 h environment by stimuli which alter the phase of the underlying brain circadian pacemaker.
For most organisms, including mammals, the primary phase-shifting stimulus is light

These processes include :--sleep-wake cycles, -body temperature, -blood pressure,-release of hormones. This activity is controlled by the biological
clock, which is located in the supra-chiasmtic nuclei of the hypothalamus in human brains.
It is highly influenced by natural dark-light cycles, but will persist under constant environmental conditions. Examples: Disruptions to the circadian rhythm can cause problems with the sleep-wake cycle
Circadian rhythms are regulated by three components :
(1) the circadian pacemaker or "clock", (2) an input mechanism which allows the
clock to be reset by environmental stimuli, and
(3)an output mechanism which regulates physiological and behavioral Processes
Hypertension types Primary Hypertension, High blood pressure of
unidentified cause, Accounts for 90% of cases of high blood pressure. The identified risk factors in primary hypertension are as follows , age onset between 30 - 50 years of age , increases over 65 years of age, sex - males in young adulthood and early middle age, females after the age of 55 years
Secondary Hypertension is High blood pressure in which the cause can be identified.
Etiology Etiology
1- Essential:In more than 95% of cases, an underlyingcause cannot be found. Proposed mechanismsinclude:Excess renal sodium retentionOver activity of sympathetic nervous
systemRenin angiotensin excessHyperinsulinemiaAlterations in vascular endothelium

Factors contributing to the development of Essential hypertension
•Genetic Factors: hypertension is more common in some families and in some ethnic groups like African Americans
•Environmental factors include obesity, alcohol, lack of exercise and excess salt
• Emotional stress can cause quite large increases in blood pressure. Prominent amongst the physiological responses to stress is an increase in activity
in the sympathetic nerves • Postural changes exert stresses on the
cardiovascular system requiring effective reflex responses to constrict arteries and veins and stimulate the heart, to control blood pressure, maintain brain blood flow, and prevent loss of consciousness

• Regular over-consumption of alcohol can raise blood pressure dramatically, as well as
cause an elevation upon withdrawal
The severity of obstructive sleep apnea syndrome OSAS is an independent factor
correlated to diurnal hypertension

pathophysiology
There is some evidence that supports a hypothesis that the primary fault in the patho-physiology of hypertension is a defect in the:-
calcium binding of the plasma membrane of the cells of a pressure-regulating center in the nervous system.
2- Secondary hypertension2- Secondary hypertension Renal: These account for over 80% of the cases of
secondary hypertension. The common causes are diabetic nephropathy, chronic glomerulonephritis, adult polycystic disease, chronic tubulointerstitial nephritis, and renovascular disease.
Endocrinal: These include Conn's syndrome, adrenal hyperplasia,
acromegaly, Phaeochromocytoma, Cushing's syndrome. Drugs and toxins Pregnancy-induced hypertension Vascular: coarctation of aorta, vasculitis

Children
Hypertension in neonates is rare, occurring in around 0.2 to 3% of neonates,
blood pressure is not measured routinely in the healthy newborn
Hypertension is more common in high risk newborns.
A variety of factors, such as gestational age, postconceptional age and birth weight needs to be taken into account when deciding if a blood pressure is normal in a neonate
Hypertensive crises
Severely elevated blood pressure (equal to or greater than a systolic 180 or diastolic of 110 — sometime termed malignant or accelerated hypertension) is referred to as a "hypertensive crisis", as blood pressures above these levels are known to confer a high risk of complications.
People with blood pressures in this range may have no symptoms, but are more likely to report headaches (22% of cases)and dizziness than the general population
Other symptoms accompanying a hypertensive crisis may include :-
1-visual deterioration2-breathlessness due to heart failure 3-general feeling of malaise due to renal
failure4-Most people with a hypertensive crisis are
known to have elevated blood pressure, but additional triggers may have led to a sudden rise
emergency hypertensive"malignant hypertension", is diagnosed
when there is evidence of :-1- direct damage to one or more organs as a
result of the severely elevated blood pressure.
1-This may include hypertensive encephalopathy, caused by brain swelling and dysfunction,

characterized by:-
- headaches
-altered level of consciousness (confusion or drowsiness).
-Retinal papilloedema
-fundal hemorrhages

-exudates are another sign of target organ damage.
-Chest pain may indicate heart muscle damage (which may progress to myocardial infarction) or sometimes aortic dissection,
-tearing of the inner wall of the aorta. -Breathlessness, cough, and the
expectoration of blood-stained sputum are characteristic signs of pulmonary edema, the swelling of lung tissue due to left ventricular failure

-inability of the left ventricle of the heart to adequately pump blood from the lungs into the arterial system
In pregnancy
Hypertension occurs in approximately 8-10% of pregnancies
Most women with hypertension in pregnancy have pre-existing primary hypertension, but high blood pressure in pregnancy may be
the first sign of pre-eclampsia, a serious condition of the second half of pregnancy and puerperium.[

Pre-eclampsia is characterised by
increased blood pressure the presence of protein in the urineIt occurs in about 5% of pregnancies and is
responsible for approximately 16% of all maternal deaths globally
Pre-eclampsia also doubles the risk of perinatal mortality
] Usually there are no symptoms in pre-eclampsia and it is detected by routine screening.
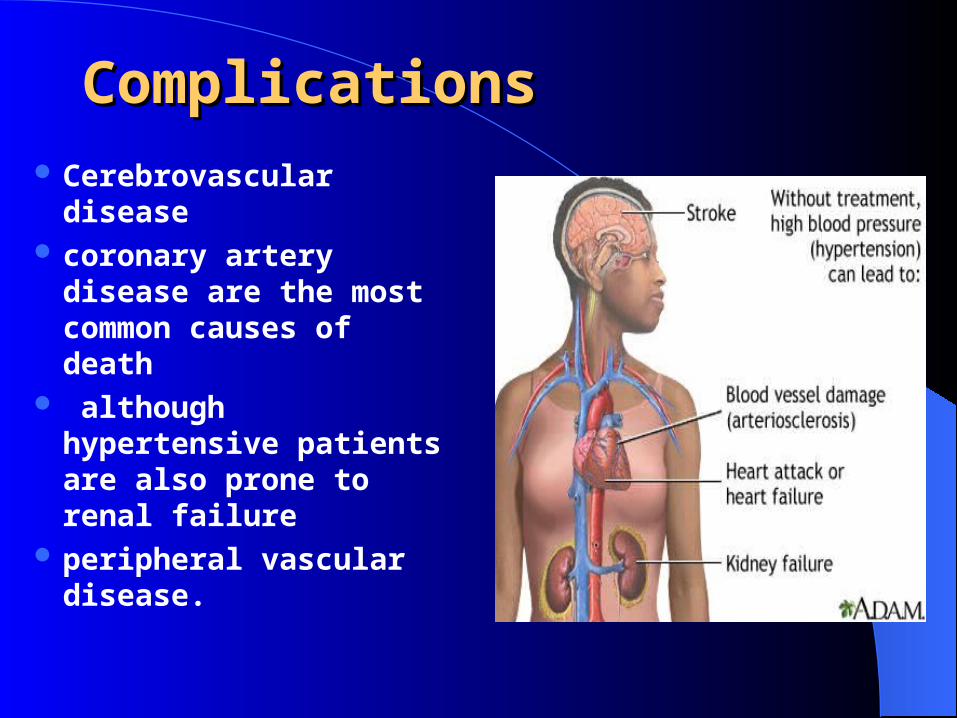
ComplicationsComplications
Cerebrovascular disease
coronary artery disease are the most common causes of death
although hypertensive patients are also prone to renal failure
peripheral vascular disease.
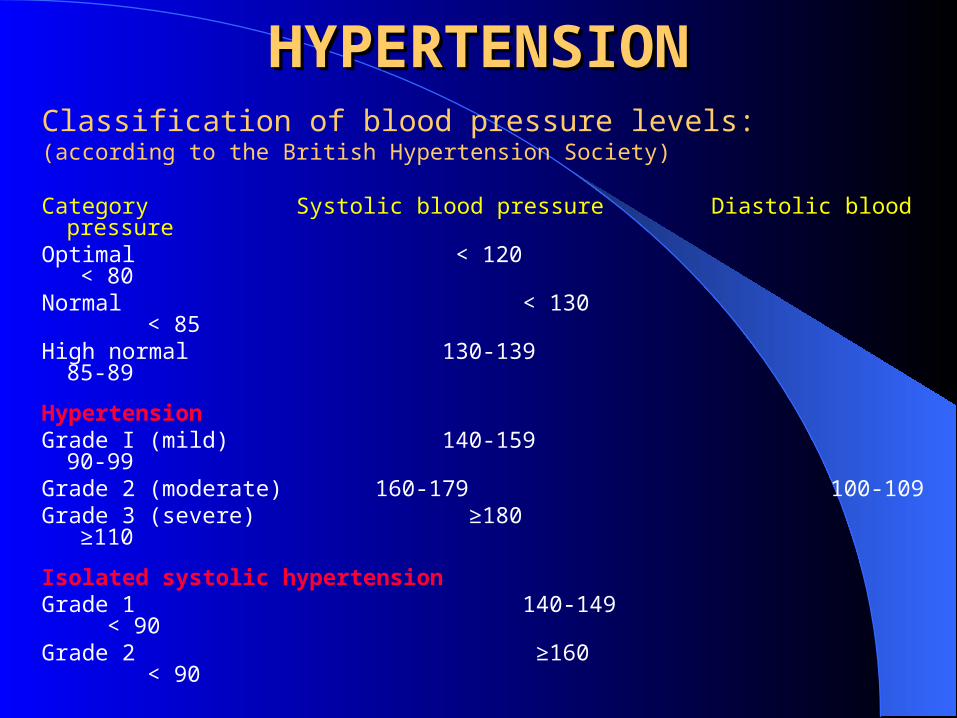
HYPERTENSIONHYPERTENSIONClassification of blood pressure levels:(according to the British Hypertension Society)
Category Systolic blood pressure Diastolic blood pressureOptimal < 120 < 80Normal < 130 < 85High normal 130-139 85-89
HypertensionGrade I (mild) 140-159 90-99Grade 2 (moderate) 160-179 100-109Grade 3 (severe) ≥180 ≥110
Isolated systolic hypertensionGrade 1 140-149 < 90Grade 2 ≥160 < 90
HISTORYHISTORYThe patient with mild hypertension is
usually asymptomatic. Attacks of sweating headaches palpitations. Higher levels of blood pressure may be
associated with, epitasis or nocturnal. Breathlessness may be present owing to left
ventricular hypertrophy or cardiac failure.

INVESTIGATIONSINVESTIGATIONS
Routine investigation of the hypertensive
patient should include: ECG Urine stix test for protein and blood Fasting blood for lipids (total and high-
density lipoprotein cholesterol) and glucose Serum urea, creatinine and electrolytes.

Investigation of selected casesInvestigation of selected cases
Chest X-ray Ambulatory BP recordingEchocardiogram Renal ultrasoundRenal angiographyUrinary catecholaminesUrinary cortisol and dexamethasone
suppression testPlasma renin activity and aldosterone

PreventionMuch of the disease burden of high blood
pressure is experienced by people who are not labelled as hypertensive.
population strategies are required to reduce the consequences of high blood pressure and reduce the need for antihypertensive drug therapy.
Lifestyle changes are recommended to lower blood pressure, before starting drug therapy.

maintain normal body weight for adults (e.g. body mass index 20–25 kg/m2)
reduce dietary sodium intake to <100 mmol/ day (<6 g of sodium chloride or <2.4 g of sodium per day)
Engage in regular aerobic physical activity such as brisk walking (≥30 min per day, most days of the week)
limit alcohol consumption to no more than 3 units/day in men and no more than 2 units/day in women
consume a diet rich in fruit and vegetables (e.g. at least five portions per day)
Effective lifestyle modification may lower blood pressure as much an individual antihypertensive drug.
Combinations of two or more lifestyle modifications can achieve even better results.

ManagementLifestyle modifications includesdietary changesphysical exercise weight loss.
If hypertension is high enough to justify immediate use of medications, lifestyle changes conjunction with medication.
Anti-inflammatory approaches should be a promising strategy for treating both hypertension and atherosclerosis
Different programs aimed to reduce:-
psychological stress such as biofeedback relaxation or meditation
Dietary change such as a low sodium diet is beneficial. A long term (more than 4 weeks) low sodium diet in
Also, the DASH diet, a diet rich in nuts, whole grains, fish, poultry, fruits and vegetables
diet is also rich in potassium, magnesium, calcium, as well as protein
Non-pharmacological Non-pharmacological treatmenttreatment
Weight reduction - BMI should be < 25 kg/m2 Low-fat and saturated fat diet Low-sodium diet - < 6 g sodium chloride per day Limited alcohol consumption - ≤ 21 units/week for
men and ≤ 14 units/week for women eating plan, which is rich in potassium and
calcium Chronic intake of diets rich in pomace olive oil
improves endothelial dysfunction in spontaneously hypertensive
Diets rich in fruits and vegetables reduce blood pressure
Dynamic exercise –At least 30 minutes' brisk walk per dayIncreased fruit and vegetable consumptionReduce cardiovascular risk by stopping
smoking increasing oily fish consumption.
Pharmacological treatment should be Pharmacological treatment should be
based on the followingbased on the following The initiation of antihypertensive therapy in
subjects with sustained systolic blood pressure (BP) ≥ 160 mmHg, or sustained diastolic BP ≥ 100 mmHg.
In patients with diabetes mellitus, the initiation of antihypertensive drug therapy if systolic BP is sustained ≥ 140 mmHg, or diastolic BP is sustained ≥ 90 mmHg.

In non-diabetic hypertensive subjects, treatment goals: BP < 140/85 mmHg. In some hypertensive subjects these levels may be difficult to achieve.
Most hypertensive patients will require a combination of antihypertensive drugs to achieve the recommended targets.
In most hypertensive patients, therapy with statins and aspirin to reduce the overall cardiovascular risk burden.
Glycaemic control should be optimized in diabetics (HbA1c < 7%).
Anti-hypertensive medications are not effective for everyone
costly and result in adverse effects that impair quality of life and reduce adherence.
Moreover, abnormalities associated with high BP, such as insulin resistance and hyperlipidaemia, may persist or may even be exacerbated by some anti-hypertensive medications.

Pharmacological Treatment Pharmacological Treatment
Several classes of drugs are available to treat
hypertension. The usual are:
(a) ACE inhibitors or Angiotensin receptor antagonists
(b) Beta-blockers
(c) Calcium-channel blockers
(d) Diuretics
(e) Other drugs as α-blocker, direct vasodilator, or centrally acting drugs
Choice of antihypertensive therapy
The choice of antihypertensive therapy is usually dictated by
cost, convenience, the response to treatment and freedom of
side effects

Co morbid conditions may have an important influence on
initial drug selection e.g.Β-blocker in anginaThiazide diuretics and calcium
antagonists in elderly peopleACE in heart failure, post MI, type 1
diabetic nephropathyARBs in type 2 diabetic nephropathy,
intolerance to ACEα-blocker in benign prostatic
hypertrophy

Aerobic exercises
Aerobic exercises may play an important role in the treatment of blood pressure of
hypertensive individuals treated in the long run

Exercises
For many years, physical inactivity has been recognized as a risk factor for coronary heart disease (CHD) and most recommendations suggest regular physical activity as a part of the strategy in preventing/reducing CHD
Physical Activity
Regular physical activity is the first treatment recommended
to lower BP and improve cardiovascular health,
The effect of physical activity on SBP and DBP is unequal. With increased levels of activity there is an almost linear increase in SBP, whereas DBP tends to decrease

Moderate-intensity (40–70% VO2 max) aerobic exercise is associated with a significant reduction of blood pressure in hypertensive and normotensives participants and in overweight, as well as normal-weight participants
reducing :_1-regional sympathetic outflow,
2- total peripheral resistance3- heart rate.
- exercise has been shown to augment vagal tone, endothelium-mediated vasodilatation
- insulin sensitivity and mood - and to lower cholestero
-Resistive exercise training has been shown to decrease SNS activity
-increase baroreflex sensitivity (an index of reflex vagal control of the heart which
carries relevant patho physiological
-High intensity training may paradoxically increase arterial stiffness in healthy
middle-aged -

In hypertension, sympathetic activation represents a mechanism potentially responsible for the day-night blood
pressure difference evening exercise significantly reduced the
nighttime blood pressure, Irrespective of a morning exercise period
nitric oxides release by moderate exercises as a vasodilator on endothelium cell of blood vessels that increases blood
flow while lowering blood pressure.
Decreases in catecholamine and total peripheral resistance,
improved insulin sensitivity,
and alterations in vasodilators and vasoconstrictors are some of the postulated explanations for the
antihypertensive effects of exercise
sympathy inhibition and enhanced vagal activity

increase in diastolic blood pressure of more than 10 mmHg during or after exercise represents a coronary artery disease.
SummarySummary
• Hypertension is the commonest cause of major morbidity,
but less than a quarter of patients are adequately treated.
• A reduction in cardiovascular disease mortality and
morbidity can be achieved through improved treatment
and control of hypertension.
• A greater choice of drugs are available for hypertension
than for other chronic diseases.
• Rational choice of single and combination drugs facilitated
by understanding their effects on the renin system, but
systematic trial and error may still be necessary.
