systemic ubiquitin release after blunt trauma and burns ... · systemic ubiquitin release after...
TRANSCRIPT

Systemic Ubiquitin Release After Blunt Trauma and Burns:Association With Injury Severity, PosttraumaticComplications, and SurvivalMatthias Majetschak, MD, PhD, Siegfried Zedler, PhD, Arwed Hostmann, MD,Luis T. Sorell, PhD, Mayur B. Patel, MD, Lissette T. Novar, MPH, Robert Kraft, MD, Fahim Habib, MD,Marc A. de Moya, MD, Wolfgang Ertel, MD, Eugen Faist, MD, and Ulrich Schade, PhD
Background: Recent data suggestthat ubiquitin (Ub) is systemically re-leased after trauma, has pleiotropic effectson host defense mechanisms, and that Ubadministration reduces fluid shifts into tis-sues during inflammation. Ub release af-ter burns (B) has not been studied and itsassociation with injury severity and out-come after blunt trauma (T) is unknown.Thus, we evaluated Ubs association with in-jury severity and outcomes after B and T.
Methods: Injury severity was as-sessed with the Injury Severity Score (ISS)in T and burn size (% total body surfacearea, %TBSA) in B. A total of 129 T (ISS:26 � 13) and 55 B (46% � 18% TBSA)were observed for sepsis/multiple organ fail-ure (MOF) and survival. In B, sequentialorgan failure assessment scores were docu-
mented daily. Fifty volunteers served ascontrols (C) Ub serum levels were mea-sured on day 0 (admission), 1, 3, 5, and 7by enzyme-linked immunosorbent assay.Data were analyzed using bivariate or par-tial correlation analyses, t test, and analysisof variance with Tukey post-hoc test formultiple comparisons (two-tailed p < 0.05).
Results: Ub was significantly ele-vated in patients. Peak levels (ng/mL)were detectable on day 0 (C: 118 � 76; T:359 � 205; B: 573 � 331) and increasedwith increased ISS, %TBSA, and presenceof inhalation injury. In T, Ub normalizedby day 3, but remained elevated in B. In B,Ub correlated significantly negative withsequential organ failure assessment scores(r: �0.143; p � 0.0147), sepsis/MOF de-velopment (r: �0.363; p � 0.001), and
survival (r: �0.231; p � 0.009). Comparedwith B who recovered uneventfully, Ublevels were significantly lower on days 1 to7 and on days 5/7 in B who developedsepsis/MOF or died, respectively.
Conclusion: Ub concentrations re-flect the extent of tissue damage. Alongwith Ubs previously described anti-inflammatory properties, this study sug-gests that its systemic release is protective,that burn patients who develop sepsis/MOFhave a relative Ub deficiency and that Ubcould play an important role during thephysiologic response to burn injury.
Key Words: Fluid shifts, Capillaryleak, Organ failure, Tissue damage, Im-mune modulation.
J Trauma. 2008;64:586–598.
Ubiquitin (Ub) is a small, heat stable, and highly con-served protein in all eukaryotic cells.1–3 It fulfills itsmajor biologic role through covalent ligation (ubiqui-
tylation or ubiquitination) to intracellular proteins, and thuslabels the target protein for degradation via the proteasome orreversibly regulates the targeted protein’s function.3 Today,ubiquitylation is regarded as the second most common post-translational protein modification after phosphorylation.4–6
Although the discovery of Ub introduced this protein as amolecule with extracellular actions,1 little attention has sincebeen paid to its possible role outside the cell. Ub is a naturalconstituent of extracellular fluids, such as serum, plasma, or
cerebrospinal fluid, and increased extracellular concentra-tions have been described in some diseases.1,7–12 However,no pathophysiologic role was attributed to extracellular Ub inthese studies.
Recently, we showed that Ub is systemically released aftertrauma and sepsis in patients, that it is involved in the regulationof leukocyte function and inhibits the lipopolysaccharide-(LPS)-evoked tumor necrosis factor-� and interleukin-8 re-sponse of blood and isolated peripheral blood mononuclear cellsin vitro.13,14 Because other investigators provided evidence thatit also regulates growth and apoptosis, and possesses antimicro-
Submitted for publication October 1, 2007.Accepted for publication December 4, 2007.Copyright © 2008 by Lippincott Williams & WilkinsFrom the Divisions of Trauma and Surgical Critical Care (M.M., L.S.,
M.B.P., L.T.N., F.H., M.A.D.M.), DeWitt Daughtry Family Department ofSurgery, University of Miami Miller School of Medicine, Miami, Florida;Department of Surgery (S.Z., R.K., E.F.), Klinikum Grosshadern, Ludwig-Maximilians-University of Munich, Munich, Germany; Department ofTrauma and Reconstructive Surgery (A.H., W.E.), Charite-University Hos-pitals Berlin, Campus Benjamin Franklin, Berlin, Germany; and SurgicalResearch (F.U.S.), Department of Trauma Surgery, University HospitalDuisburg-Essen, Essen, Germany.
M. de Moya is currently affiliated to Department of Surgery, Massa-chusetts General Hospital, and M.B. Patel is affiliated to Department ofGeneral Surgery, Duke University Medical Center.
Supported by grants MA 2474/2-2 from the Deutsche Forschungsge-meinschaft (DFG) and 6123-1035-00-B contract W81XWH-05-1-0585 fromthe USAMRAA.
Presented at the 66th Annual Meeting of the American Association forthe Surgery of Trauma, September 27–29, 2007, Las Vegas, Nevada.
Address for reprints: Matthias Majetschak, MD, PhD, Divisions ofTrauma and Surgical Critical Care, DeWitt Daughtry Family Department ofSurgery, University of Miami Miller School of Medicine, 1800 NW 10thAvenue, Miami, FL 33136; email: [email protected].
DOI: 10.1097/TA.0b013e3181641bc5
The Journal of TRAUMA� Injury, Infection, and Critical Care
586 March 2008

bial activity,15–17 extracellular Ub may have pleiotropic effectson host defense mechanisms. Subsequently, we were able toconfirm Ubs immune modulatory properties in vivo and showedthat it has profound anti-inflammatory effects in various modelsof infectious and noninfectious inflammation.18–22 Altogether,these data suggest that Ub is an endogenous anti-inflammatorymediator that could play an important role during the inflamma-tory response to mechanical and thermal injury. However, itsassociation with injury severity and outcomes in blunt traumapatients is unknown and Ub release after thermal injuries has notbeen studied. Therefore, we conducted a prospective observa-tional trial in blunt trauma and burned patients to evaluatewhether Ubs systemic concentrations are associated with injuryseverity, development of severe posttraumatic complications,and survival.
PATIENTS AND METHODSPatients, Participants, and Study Protocol
The Institutional Review Boards of the Universities ofMiami, Berlin, Munich, and Essen approved the protocol thatwe used. Informed consent was obtained from all partici-pants. The study population comprised of 129 patients withblunt injuries and 55 patients with burns who were admittedto the emergency room of the participating hospitals, and of50 healthy blood donors. Exclusion criteria were age under18 years, hospital admission later than 6 hours after injury,transfer from other hospitals and severe preexisting infec-tious, and immunologic or cardiovascular diseases that re-quired long-term medication. Sixty-six blunt trauma patientswere recruited in Miami, 53 in Berlin, and 10 in Essen.Burned patients were recruited in Munich. Healthy blooddonors were recruited in Miami (n � 20), Munich (n � 20),and Essen (n � 10). Blood donors (age: 43 � 11 years[mean � SD]; 68% male), had no signs of infection at least4 weeks before the blood draw.
All patients requiring surgical intervention received stan-dard surgical care and postoperative intensive care unit (ICU)treatment according to the standard treatment protocols of theindividual hospitals. For the assessment of injury severity inblunt trauma patients, the Injury Severity Scores (ISS) werecalculated based on the final patient records.23 In burnedpatients injury severity was assessed by the percentage of atleast second-degree burned total body surface area (%TBSA),as documented in the patient records. All patients were pro-spectively observed for the development of severe sepsis,septic shock, or multiple organ failure (sepsis/MOF). Severesepsis and septic shock were diagnosed according to theAmerican College of Chest Physicians/Society of CriticalCare Medicine (ACCP/SCCM) consensus conference criteria.24
MOF was diagnosed using a scoring system modified accord-ing to Goris et al.25–27 In brief, failure of a single organ wasassumed when the following criteria were present for at least3 consecutive days: lung, mechanical ventilation with posi-tive end-expiratory pressure (PEEP) �10 cm H2O and/or
FIO2 �0.4; heart, dopamine �700 �g or catecholamine treat-ment; kidney, hemofiltration or hemodialysis; liver, bilirubin�102 �mol/L or aspartate aminotransferase (AST) �100U/L; blood, hemorrhagic diathesis or leukocytes �60 k/�L or�2.5 k/�L; gastrointestinal, parenteral nutrition; brain, treat-ment for increased intracranial pressure. MOF was diagnosedwhen these criteria were fulfilled for two or more organs.Because MOF without positive criteria of severe sepsis orseptic shock after blunt trauma and burns was expected to berare, these posttraumatic complications were combined anddocumented as sepsis/MOF positive or negative. In addition,in burned patients the sepsis-related organ failure or sequen-tial organ failure assessment (SOFA) scores28,29 were calcu-lated daily and the volumes of fluids infused and urine outputwere documented.
Duration of ICU treatment and hospital survival weredocumented based on the final patient records. The epidemi-ologic and clinical characteristics of the blunt trauma andburned patients are shown in Table 1.
Venous blood samples (1–2 mL) were drawn immedi-ately after admission to the emergency room (day 0) and inthe morning of the subsequent days 1, 3, 5, and 7 between 7AM and 9 AM along with the routine laboratory work-up.Because blood samples could not be obtained from eachpatient at each individual time point, the exact number ofanalyzed blood samples is provided for each time point in theResults section. Blood samples were collected in serum testtubes, which were in routine use in the participating hospitals,serum prepared according to the standard hospital proceduresand stored at -70°C until further analysis. After all bloodsamples were collected and patient data recorded, Ub serumconcentrations were determined with the investigatorsblinded to the patient-related data.
Ubiquitin Enzyme-Linked ImmunosorbentAssay (ELISA)
Ub serum concentrations were quantified with a compet-itive ELISA, in which biotinylated Ub and Ub in the testsample compete for a limited number of binding sites in the
Table 1 Epidemiologic and Clinical Characteristics ofthe Patient Populations
Trauma Burns
N 129 55Age 45 � 20 46 � 18Male (%) 72.8 83.6ISS 26 � 13 N/ATBSA (%) 0 39 � 16
with inhalation injury 0 34.5ICU (d) 21 � 29 47 � 83Sepsis/MOF 20.1% 45.5%Mortality 12.4% 23.6%
Data are means � SD or percentages.
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 587

anti-Ub antibody according to that shown in Refs. 14 and 18to 22. In brief, microtiter plates (Nalge Nunc International,Rochester, NY) were coated with anti-Ub (Sigma-Aldrich,St. Louis, MO) and incubated for 18 hours at 4°C. The plateswere washed three times with 0.05% Tween 20 in phosphatebuffered saline and were incubated with blocking buffer(0.5% bovine serum albumin [Sigma-Aldrich] 0.05% Tween20, in phosphate buffered saline) for 1.5 hours. After washingthree times, 50 �L of the standards or samples were mixedwith 50 �L of biotinylated Ub (Boston Biochem, Boston,MA) and placed in the plates. Each sample was tested in eightdilutions. Dilutions for the standard curve and the test sam-ples were prepared in blocking buffer. After incubation for1.5 hours the plates were washed again and a peroxidase-labeled anti-biotin antibody (Amersham Biosciences, Buck-inghamshire, UK) was added. After incubation for 1.5 hoursthe plates were washed again and 100 �L 3, 3�, 5, 5�,tetramethylbenzidine ELISA solution (Sigma-Aldrich) wasadded. After incubation for 20 to 40 minutes, the reaction was
stopped by addition of 100 �L HCl and optical densities weremeasured using a micro-ELISA autoreader (�Quant, Bio-TekInstruments Inc., Winooski, VT; test filter: 450 nm; referencefilter: 540 nm). The Ub concentration in the test sample wascalculated with the KC4 for windows program, version 3.02(Bio-Tek Instruments Inc.), from a four-parameter logistic fitemploying Ub as standard (0–1700 ng/mL, Sigma-Aldrich).The correlation coefficients for each standard curve were0.98 to 1. This ELISA predominantly detects free Ub.Comparison of Ub concentrations measured by ELISA andwestern blot showed that concentrations determined byELISA were 107% � 9% (n � 4) of the concentrations forfree Ub that were determined by western blot. Thus, be-cause of some cross-reactivity with ubiquitylated proteins,the ELISA measurements overestimate the concentrationof free Ub by approximately 7%. Addition of purifiedhemoglobin to the assay did not affect measurements. Therecovery of Ub in spiked serum and plasma was 94% to105%.
0 1 2 3 4 5 6 7
0
100
200
300
400
500
DAY AFTER TRAUMA
ng/m
L
0 1 2 3 4 5 6 7
0
100
200
300
400
500
600
700
800
900
DAY AFTER BURNS
ng/m
L
A B
0 1 2 3 4 5 6 7
0
100
200
300
400
500
DAY AFTER TRAUMA
ng/m
L
0 1 2 3 4 5 6 7
0
100
200
300
400
500
DAY AFTER TRAUMA
ng/m
L
0 1 2 3 4 5 6 7
0
100
200
300
400
500
DAY AFTER TRAUMA
ng/m
L
Berlin Essen Miami
a
a/ba/ba/b
b
c
a
bb
b
bb
Fig. 1. Ubiquitin serum concentrations in blunt trauma and burned patients during a 7-day observation period. Time points not sharing thesame letter are significantly different (analysis of variance/Tukey). Data are mean � SEM. (A) F, Blunt trauma patients, day 0: n � 116,day 1: n � 66; day 2: n � 63, day 5: n � 58, day 7: n � 26. �, Healthy blood donors, n � 50. Inserts, time course of Ub serum levelsin patients recruited at the different study sites. (B) f, Burned patients, day 0: n � 37; day 1: n � 46; day 2: n � 45, day 5: n � 41, day7: n � 37. �, Healthy blood donors, n � 50.
The Journal of TRAUMA� Injury, Infection, and Critical Care
588 March 2008
Statistical AnalysisData are described as mean � SD and are presented in
the graphs as mean � SEM along with the exact number ofmeasurements to improve the interpretation of the data.30
Differences in Ub serum concentrations were analyzed usingStudent’s t test or analysis of variance with Tukey post hoccorrection to correct for multiple testing. Correlations wereassessed using Spearman correlation coefficients (rs) andpartial correlation coefficients (rp) that describe the relation-ship between two variables while controlling for the effects of
one or more additional variables. Statistical analyses werecalculated with the SPSS for windows program (SPSS Inc.,Chicago, IL). Differences were considered significant on atwo-tailed p � 0.05 level.
RESULTSThe time course of Ub serum concentrations in trauma and
burned patients is shown in Figure 1A and B. Ub serum levels weresignificantly elevated in both patient populations, as compared withhealthy volunteers (n � 50, 118 ng/mL � 76 ng/mL Ub). Ub serum
ctrl. 0 1-9 10-19 20-29 30-39 40+0
100
200
300
400
500
600
700
aab
b
b
b
b
c
ISS
ng/m
L
ctrl. <25 25-35 36-45 46+ Yes No0
100
200
300
400
500
600
700
800
900
1000
a
ab
bc
c c
noitalahniASBT%injury
*
ng/m
L
0 1-7 8-21 22+ ≤30 >300
100
200
300
400
500
ab
bb
0
300
600
900Trauma Burns
a
*
ICU days
ng/m
L ng/mL
A B
C
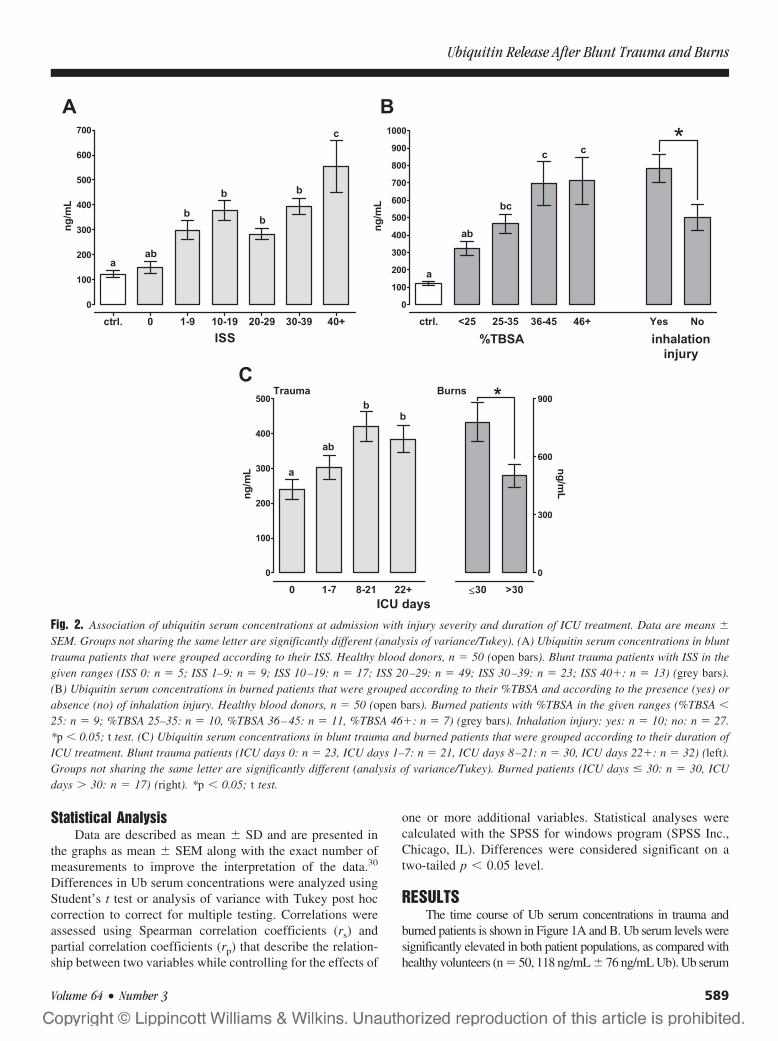
Fig. 2. Association of ubiquitin serum concentrations at admission with injury severity and duration of ICU treatment. Data are means �
SEM. Groups not sharing the same letter are significantly different (analysis of variance/Tukey). (A) Ubiquitin serum concentrations in blunttrauma patients that were grouped according to their ISS. Healthy blood donors, n � 50 (open bars). Blunt trauma patients with ISS in thegiven ranges (ISS 0: n � 5; ISS 1–9: n � 9; ISS 10–19: n � 17; ISS 20–29: n � 49; ISS 30–39: n � 23; ISS 40�: n � 13) (grey bars).(B) Ubiquitin serum concentrations in burned patients that were grouped according to their %TBSA and according to the presence (yes) orabsence (no) of inhalation injury. Healthy blood donors, n � 50 (open bars). Burned patients with %TBSA in the given ranges (%TBSA �
25: n � 9; %TBSA 25–35: n � 10, %TBSA 36–45: n � 11, %TBSA 46�: n � 7) (grey bars). Inhalation injury: yes: n � 10; no: n � 27.*p � 0.05; t test. (C) Ubiquitin serum concentrations in blunt trauma and burned patients that were grouped according to their duration ofICU treatment. Blunt trauma patients (ICU days 0: n � 23, ICU days 1–7: n � 21, ICU days 8–21: n � 30, ICU days 22�: n � 32) (left).Groups not sharing the same letter are significantly different (analysis of variance/Tukey). Burned patients (ICU days � 30: n � 30, ICUdays � 30: n � 17) (right). *p � 0.05; t test.
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 589

A B
C D
0 1 3 5 7
0
100
200
300
400
500
malefemale
DAY AFTER TRAUMA
ng/m
L
0 1 3 5 7
0
100
200
300
400
500 < 30 yrs30-50 yrs> 50 yrs
DAY AFTER TRAUMAng
/mL
0 1 3 5 7
0
50
100
150
200
250
300
350
400
450
500
550
sepsis/MOFno sepsis/MOF - ISS matchedno sepsis/MOF
DAY AFTER TRAUMA
ng/m
L
0 1 3 5 7
0
100
200
300
400
500
600
diedsurvived - ISS matchedsurvived
DAY AFTER TRAUMA
ng/m
L
Fig. 3. Ubiquitin serum concentrations after blunt trauma by gender, age, sepsis/MOF, and survival. Data are means � SEM. (A) Female (day0: n � 31, day 1: n � 19; day 2: n � 18, day 5: n � 17, day 7: n � 8) (open bars). Male (day 0: n � 85, day 1: n � 47; day 2: n � 45, day5: n � 41, day 7: n � 18) (grey bars). (B) Less than 30 years (day 0: n � 31, day 1: n � 20; day 2: n � 21, day 5: n � 18, day 7: n � 7) (openbars). Thirty to 50 years (day 0: n � 40, day 1: n � 21; day 2: n � 19, day 5: n � 18, day 7: n � 6) (light grey bars). More than 50 years (day0: n � 45, day 1: n � 22; day 2: n � 21, day 5: n � 20, day 7: n � 10) (dark grey bars). (C) No sepsis/MOF (ISS: 24�13 [mean � SD]; day0: n � 91, day 1: n � 48; day 2: n � 45, day 5: n � 42, day 7: n � 15) (striped bars). No sepsis/MOF - ISS matched (ISS: 29 � 10 [mean �
SD]: day 0: n � 69, day 1: n � 41; day 2: n � 39, day 5: n � 38, day 7: n � 13) (white bars). Sepsis/MOF (ISS: 33 � 11 [mean � SD]: day0: n � 25, day 1: n � 12; day 2: n � 13, day 5: n � 13, day 7: n � 8) (grey bars). (D) Survived (ISS: 24 � 12 [mean � SD[; day 0: n � 101,day 1: n � 58; day 2: n � 54, day 5: n � 50, day 7: n � 22) (striped bars). Survived - ISS matched (ISS: 30 � 8 [mean � SD]: day 0: n � 71,day 1: n � 46; day 2: n � 43, day 5: n � 41, day 7: n � 16) (white bars). Died (ISS: 33 � 11 [mean � SD]: day 0: n � 15, day 1: n � 8; day2: n � 9, day 5: n � 8, day 7: n � 8) (grey bars).
The Journal of TRAUMA� Injury, Infection, and Critical Care
590 March 2008

concentrations and their time-dependent changes after blunt traumawere similar in patients from all study sites (Fig. 1A, inserts). Peaklevels were detectable at admission (day 0, n � 116, 359 ng/mL �205 ng/mL) and normalized within 3 days after blunt trauma.
Burned patients showed significantly higher Ub serumconcentrations at admission (day 0, n � 37, 573 ng/mL �331 ng/mL) than blunt trauma patients (p � 0.001). In con-trast to trauma patients, Ub serum concentrations in burnedpatients remained elevated within the 7 days observationperiod.
The initial Ub serum concentrations (day 0) correlatedsignificantly with injury severity and duration of ICU treat-ment after blunt trauma (ISS: rs � 0.25, p � 0.0063; ICU[days]: rs � 0.21, p � 0.029) and burns (%TBSA: rs � 0.413,p � 0.017; presence of inhalation injury: rs � 0.568, p �0.001; ICU [days]: rs � -0.411, p � 0.041).
Figure 2A shows the initial Ub serum levels after blunttrauma when patients were grouped according to their ISS.Although Ub levels increased with an increase in ISS, theydid not differentiate patients with an ISS of 1 to 9 up topatients with an ISS of 30 to 39. Only trauma patients with anISS of more than 39 had significantly higher Ub serum levels(n � 13, 592 ng/mL � 377 ng/mL) than all other injuredpatients (ISS 1–9 [n � 9]: 305 ng/mL � 108 ng/mL; ISS10–19 [n � 17]: 370 � 165; ISS 20–29 (n � 49): 319ng/mL � 155 ng/mL; ISS 30–39 [n � 23]: 377 ng/mL � 158
ng/mL). Similarly, blunt trauma patients who did not requireICU treatment (ISS: 13 � 11) had significantly lower Ubserum levels at admission (289 ng/mL � 141 ng/mL) thanpatients with more than 7 days of ICU treatment (ISS: 30 �11; 420 ng/mL � 238 ng/mL) (Fig. 2C).
When burned patients were grouped according to their%TBSA Ub serum levels on day 0 increased from 321 ng/mL � 91 ng/mL with �25% TBSA (n � 9) to 465 ng/mL �175 ng/mL (n � 10), 697 ng/mL � 412 ng/mL (n � 11) and713 ng/mL � 356 ng/mL (n � 7) with 25% to 35%TBSA,35% to 46%TBSA, and more than 46%TBSA, respectively(Fig. 2B). Furthermore, the presence of inhalation injury wasassociated with significantly higher Ub concentrations (Fig.2B; no inhalational injury [n � 27]: 506 ng/mL � 342ng/mL; inhalational injury [n � 10]: 782 ng/mL � 254ng/mL; p � 0.029). Surprisingly, the initial Ub serum levelswere significantly lower in burned patients who required ICUtreatment for more than 30 days (36% � 10% TBSA; 501ng/mL � 193 ng/mL) than in patients with a shorter durationof ICU treatment (43% � 14% TBSA;779 ng/mL � 774ng/mL; p � 0.03) (Fig. 2C).
Ub concentrations showed no sex or age-related differ-ences and no differences between blunt trauma patients withand without development of sepsis/MOF or blunt traumasurvivors and nonsurvivors at any time point (Fig. 3).
Because we did not detect time-related changes of Ubserum levels after burns, the correlations between Ub con-centrations, %TBSA, fluid balance (fluids infused minusurine output), age, sex, SOFA scores, and outcomes wereanalyzed for the 7 days observation period (Table 2). In abivariate correlation analysis, Ub levels correlated signifi-cantly positive with %TBSA and negative with SOFA scoresand sepsis/MOF development. As expected, %TBSA, age,fluid balance, and SOFA scores also correlated with out-comes. Thus, we used partial correlation analyses to adjustUbs correlation with outcome for possible confounding fac-tors (Table 3). When correlations with sepsis/MOF develop-ment and survival were corrected for the effects of all othervariables, Ub concentrations, as well as age and %TBSAcorrelated significantly with sepsis/MOF development andsurvival. In contrast, fluid balances during the entire obser-
Table 2 Correlation of Ubiquitin Serum Concentrations During the 7-d Observation Period With Epidemiologicand Clinical Patient Characteristics After Burns
rs (p) Age Female TBSA (%) FB SOFA Sepsis/MOF Survival
Ub –0.033 (645) 0.11 (0.126) 0.153 (0.033)* 0.065 (0.461) –0.143 (0.047)* –0.155 (0.031)* –0.051 (0.477)Age 0.182 (0.225) –0.154 (0.308) –0.002 (0.979) 0.245 (0.001)* 0.156 (0.302) 0.469 (0.01)*Female –0.119 (0.43) –0.048 (0.577) –0.105 (0.118) –0.258 (0.08) 0.086 (0.572)TBSA (%) 0.300 (0.001)* 0.312 (0.001)* 0.393 (0.007)* 0.375 (0.01)*FB 0.067 (0.438) 0.046 (0.597) 0.229 (0.007)*SOFA 0.55 (0.001)* 0.432 (0.001)*Sepsis/MOF 0.459 (0.001)*
* Significant correlations.rs, Spearman correlation coefficient; p, level of statistical significance; Ub, ubiquitin serum concentrations; FB, fluid balance (volumes
infused minus urine output per 24 h); sepsis/MOF, development of sepsis/multiple organ failure.
Table 3 Partial Correlation Analyses of UbiquitinSerum Concentrations, Clinical and EpidemiologicPatient Characteristics With Outcomes After Burns
rp (p) Sepsis/MOF Survival
Ub –0.363 (0.001) –0.231 (0.009)TBSA (%) 0.246 (0.005) 0.448 (0.001)FB 0.003 (0.970) 0.112 (0.211)Age 0.233 (0.009) 0.547 (0.001)Female –0.282 (0.001) –0.016 (0.855)SOFA 0.319 (0.001) 0.285 (0.001)
rp, partial correlation coefficients controlling for the effects of allother variables; FB, fluid balance (fluids infused minus urine output per24 h); Ub, ubiquitin serum concentrations; sepsis/MOF, development ofsepsis/multiple organ failure; p, level of statistical significance.
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 591
vation period did not show independent correlations withthese outcomes.
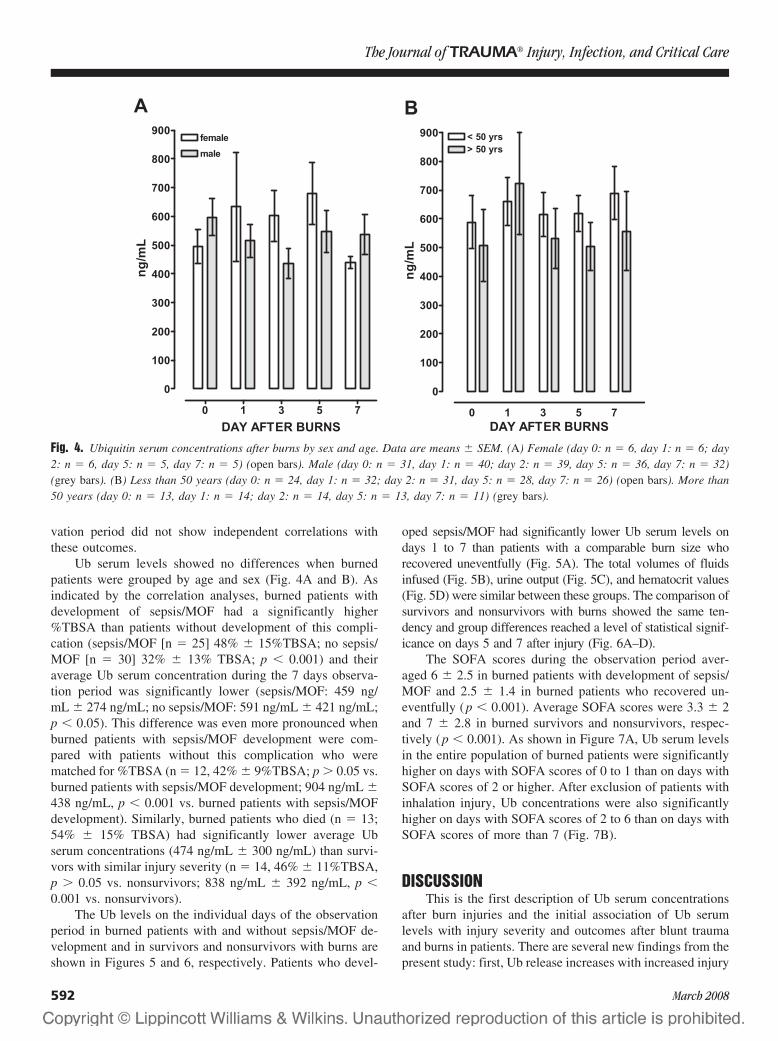
Ub serum levels showed no differences when burnedpatients were grouped by age and sex (Fig. 4A and B). Asindicated by the correlation analyses, burned patients withdevelopment of sepsis/MOF had a significantly higher%TBSA than patients without development of this compli-cation (sepsis/MOF [n � 25] 48% � 15%TBSA; no sepsis/MOF [n � 30] 32% � 13% TBSA; p � 0.001) and theiraverage Ub serum concentration during the 7 days observa-tion period was significantly lower (sepsis/MOF: 459 ng/mL � 274 ng/mL; no sepsis/MOF: 591 ng/mL � 421 ng/mL;p � 0.05). This difference was even more pronounced whenburned patients with sepsis/MOF development were com-pared with patients without this complication who werematched for %TBSA (n � 12, 42% � 9%TBSA; p � 0.05 vs.burned patients with sepsis/MOF development; 904 ng/mL �438 ng/mL, p � 0.001 vs. burned patients with sepsis/MOFdevelopment). Similarly, burned patients who died (n � 13;54% � 15% TBSA) had significantly lower average Ubserum concentrations (474 ng/mL � 300 ng/mL) than survi-vors with similar injury severity (n � 14, 46% � 11%TBSA,p � 0.05 vs. nonsurvivors; 838 ng/mL � 392 ng/mL, p �0.001 vs. nonsurvivors).
The Ub levels on the individual days of the observationperiod in burned patients with and without sepsis/MOF de-velopment and in survivors and nonsurvivors with burns areshown in Figures 5 and 6, respectively. Patients who devel-
oped sepsis/MOF had significantly lower Ub serum levels ondays 1 to 7 than patients with a comparable burn size whorecovered uneventfully (Fig. 5A). The total volumes of fluidsinfused (Fig. 5B), urine output (Fig. 5C), and hematocrit values(Fig. 5D) were similar between these groups. The comparison ofsurvivors and nonsurvivors with burns showed the same ten-dency and group differences reached a level of statistical signif-icance on days 5 and 7 after injury (Fig. 6A–D).
The SOFA scores during the observation period aver-aged 6 � 2.5 in burned patients with development of sepsis/MOF and 2.5 � 1.4 in burned patients who recovered un-eventfully (p � 0.001). Average SOFA scores were 3.3 � 2and 7 � 2.8 in burned survivors and nonsurvivors, respec-tively (p � 0.001). As shown in Figure 7A, Ub serum levelsin the entire population of burned patients were significantlyhigher on days with SOFA scores of 0 to 1 than on days withSOFA scores of 2 or higher. After exclusion of patients withinhalation injury, Ub concentrations were also significantlyhigher on days with SOFA scores of 2 to 6 than on days withSOFA scores of more than 7 (Fig. 7B).
DISCUSSIONThis is the first description of Ub serum concentrations
after burn injuries and the initial association of Ub serumlevels with injury severity and outcomes after blunt traumaand burns in patients. There are several new findings from thepresent study: first, Ub release increases with increased injury
A B
0 1 3 5 7
0
100
200
300
400
500
600
700
800
900
malefemale
DAY AFTER BURNS
ng/m
L
0 1 3 5 7
0
100
200
300
400
500
600
700
800
900 < 50 yrs> 50 yrs
DAY AFTER BURNSng
/mL
Fig. 4. Ubiquitin serum concentrations after burns by sex and age. Data are means � SEM. (A) Female (day 0: n � 6, day 1: n � 6; day2: n � 6, day 5: n � 5, day 7: n � 5) (open bars). Male (day 0: n � 31, day 1: n � 40; day 2: n � 39, day 5: n � 36, day 7: n � 32)(grey bars). (B) Less than 50 years (day 0: n � 24, day 1: n � 32; day 2: n � 31, day 5: n � 28, day 7: n � 26) (open bars). More than50 years (day 0: n � 13, day 1: n � 14; day 2: n � 14, day 5: n � 13, day 7: n � 11) (grey bars).
The Journal of TRAUMA� Injury, Infection, and Critical Care
592 March 2008

severity after mechanical and thermal injury. Second, highamounts of Ub are systemically released in burned patients.Third, in contrast to blunt trauma patients, Ub is not clearedfrom the systemic circulation within the first week in burnedpatients. Fourth, Ub serum levels in burned patients whodevelop sepsis/MOF and in those who die after burns arelower than in patients with comparable injury severity whorecover uneventfully or survive. Fifth, low Ub concentrationsare associated with a higher degree of organ dysfunction orfailure after burns.
The Ub serum concentrations and their time-relatedchanges that were detected by ELISA in the present studyconfirm our initial measurements in a small number ofblunt trauma patients, that were detected previously usinga competitive binding immunoassay.13 The finding that Ubserum levels at admission correlate with injury severity inboth trauma populations indicates passive release from
damaged tissues as its major cellular source. Because weshowed recently that the lung is among the organs thatcontain the highest concentrations of free intracellular Ubper gram of tissue, the increased Ub serum concentrationsin burned patients with additional inhalation injury furthersupport this assumption.31 In line with cell damage asmajor cellular source of Ub, we did not detect any age orsex-related differences after blunt trauma or burns. Incontrast to the ISS that was used to assess injury severityin blunt trauma patients, %TBSA is a measure of theoverall size of injured tissue. Thus, the stronger correlationbetween Ub levels and %TBSA than between Ub levelsand ISS further indicates Ub as a marker of cell damage.Because the serum half-life of extracellular Ub is approx-imately 1 hour,18 –20 the finding that it is not cleared fromthe systemic circulation after burns suggests ongoing celldamage for at least 1 week.
* *
0 1 3 5 7
0
200
400
600
800
1000
1200 * *
no sepsis/MOFno sepsis/MOF - %TBSA matched
sepsis/MOF
DAY AFTER BURNS
ng/m
L
0 1 2 3 4 5 6 7
0
5000
10000
15000
20000
25000
DAY AFTER BURNS
fluid
s (m
L/24
h)
0 1 2 3 4 5 6 7
0
1000
2000
3000
4000
5000
6000
7000
8000
DAY AFTER BURNS
urin
e ou
tput
(mL/
24h)
A
B DC
0 1 2 3 4 5 6 7
25
30
35
40
45
50
DAY AFTER BURNS
HK
T (%
)
Fig. 5. Ubiquitin serum concentrations and fluid balance in burned patients with and without sepsis/MOF development. Data are means �
SEM. (A) Ubiquitin serum concentrations. No sepsis/MOF (day 0: n � 20, day 1: n � 23; day 2: n � 23, day 5: n � 21, day 7: n � 19)(stripped bars). No sepsis/MOF – %TBSA matched (day 0: n � 6, day 1: n � 11; day 2: n � 11, day 5: n � 10, day 7: n � 10) (white bars).Sepsis/MOF (day 0: n � 17, day 1: n � 23; day 2: n � 22, day 5: n � 20, day 7: n � 18) (grey bars). *p � 0.05 (analysis of variance/Tukey).(B–D) Same patients as in (A). No sepsis/MOF (open circles). No sepsis/MOF – %TBSA matched (open squares). Sepsis/MOF (grey circles).(B) Fluids infused (mL/24 h). (C) Urine output (mL/24 h). (D) Hematocrit (%).
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 593

Because it has been shown that Ub is also stored togetherwith catecholamines in secretory granules of chromaffin cellsin the adrenal medulla and secreted with catecholamines intothe circulation upon chromaffin cell stimulation, its releaseduring the stress response could also contribute to its sys-temic concentrations.17 However, patients who were admittedto the emergency room after an accident but did not sufferfrom any injuries (ISS 0) did not show a significant increasein Ub serum concentrations, as compared with healthy vol-unteers. Thus, the contribution of Ub that is actively secretedduring the stress response to its overall concentration in thesystemic circulation after blunt trauma and burns is probablysmall.
Although Ub serum levels were not associated with sep-sis/MOF development or survival after blunt trauma, signif-icantly lower Ub concentrations were detectable in burned
patients with poor outcomes and Ub concentrations afterburns correlated significantly negative with SOFA scores.This association with poor clinical outcome and organ dys-function or failure explains the negative correlation of itsconcentrations with the duration of ICU treatment.
We showed previously that Ub has multiple anti-inflammatory effects in vitro and in vivo. Ub inhibited theLPS evoked tumor necrosis factor-� and interleukin-8 re-sponses of whole blood and peripheral blood mononuclearcells in vitro and in vivo13,14,18 and also enhanced theanti-inflammatory Th2 tissue cytokine response during in-flammation in vivo.22 These immunologic effects wereaccompanied by a significant reduction of third spacing offluids in models of endotoxic shock, traumatic shock, andlung ischemia-reperfusion injury.18 –22 Although the exactmechanism of Ubs actions is currently not known, it was
0 1 3 5 7
0
200
400
600
800
1000
1200 * *
survivedsurvived - %TBSA matched
died
DAY AFTER BURNS
ng/m
L
0 1 2 3 4 5 6 7
0
5000
10000
15000
20000
25000
30000
DAY AFTER BURNS
fluid
s (m
L/24
h)
0 1 2 3 4 5 6 7
0
1000
2000
3000
4000
5000
6000
7000
DAY AFTER BURNS
urin
e ou
tput
(mL/
24h)
A
0 1 2 3 4 5 6 7
25
30
35
40
45
50
DAY AFTER BURNS
HK
T (%
)
B DC
Fig. 6. Ubiquitin serum concentrations and fluid balance in burned survivors and nonsurvivors. Data are means � SEM. (A) Ubiquitinserum concentrations. Survived (day 0: n � 29, day 1: n � 35; day 2: n � 34, day 5: n � 33, day 7: n � 30) (striped bars). Survived – %TBSAmatched (day 0: n � 8, day 1: n � 14; day 2: n � 13, day 5: n � 12, day 7: n � 13) (white bars). Died (day 0: n � 8, day 1: n � 13;day 2: n � 13, day 5: n � 12, day 7: n � 13) (grey bars). *p � 0.05 (analysis of variance/Tukey). (B–D) Same patients as in (A). Survived(open circles). Survived – %TBSA matched (open squares). Died (grey circles). (B) Fluids infused (mL/24 h). (C) Urine output (mL/24 h). (D)Hematocrit (%).
The Journal of TRAUMA� Injury, Infection, and Critical Care
594 March 2008

shown previously that extracellular Ub can be taken upinto intact cells, followed by covalent ligation of extracel-lular Ub to intracellular proteins.16,32 Because its uptakeshowed saturation kinetics with a Kd value in the low nMrange,32 these data strongly suggest a highly specific re-ceptor through which Ub mediates its actions.
Burn injuries are always associated with a profoundinflammatory response and significant fluid shifts intotissues during the early postburn period, which in turn contrib-ute to the development of organ dysfunction and failure.33–36
Therefore, the findings of the present study suggest that Ubrelease could constitute an endogenous defense mechanism thatis aimed to limit inflammation and possibly impaired microvas-cular permeability. Although effects of Ub on immune functionshave been described at physiologic relevant concentrations, itseffects on fluid shifts were detectable when doses were admin-istered that produced supraphysiologic concentrations.13,14,18–22
This may explain the observation that Ub concentrations werenot associated with fluid balances in the present study. However,because observational studies cannot address any functional as-pects, further mechanistic studies are required to evaluate thishypothesis. In contrast to the homogenous population of patientswith thermal injuries, the heterogeneity of the individual injuriesin blunt trauma patients and the variability of the physiologicresponse to blunt trauma could explain the missing associationof Ub levels with outcomes in this patient population.
Comparison of the fluid balance and hematocrit valuesbetween patients with and without sepsis/MOF or burnedsurvivors and nonsurvivors did not show differences in our
patient population. Thus, high volumes of resuscitationfluids that possibly could have caused a dilution effect inpatients with poor outcomes cannot account for the lowerUb concentrations. Other possible explanations could beincreased renal secretion or Ub consumption. Because weshowed that only 10% of intravenously administered ex-ogenous Ub can be recovered in the urine,20 increasedconsumption appears to be more likely to account for thelower Ub concentrations in burned patients with poor clin-ical outcome. Besides increased proteolytic degradation ofUb as one possible explanation, enhanced uptake couldalso explain the lower concentrations that were associatedwith sepsis/MOF or death after burns.16,32
In conclusion, the findings of the present studystrongly suggest that systemic Ub concentrations reflectthe extent of tissue damage after blunt trauma and burns inpatients. Furthermore, burn patients who develop sepsis/MOF or die seem to have a relative Ub deficiency. Al-though the wide range of Ub serum concentrations ininjured patients shows that its levels will probably not beuseful as a diagnostic or prognostic marker in the clinicalarena, the results of the present study imply that Ub couldplay an important pathophysiologic role during the wholebody response to burn injury and suggest that its systemicrelease is protective. Further mechanistic studies are re-quired to confirm this hypothesis.
Because pharmacologic interventions that prevent fluidleakage into the extravascular compartment after thermalinjury are not available, the results from the present study
0-1 2-6 7+
0
100
200
300
400
500
600
700
800
900
1000
a
bb
SOFA
ng/m
L
0-1 2-6 7+
0
100
200
300
400
500
600
700
800
900
1000 a
b
c
SOFAng
/mL
A B
Fig. 7. Ubiquitin serum levels and SOFA scores in burn patients. Data are means � SEM. Groups not sharing the same letter aresignificantly different (analysis of variance/Tukey). (A) Entire population of burn patients. SOFA 0–1: n � 27; SOFA 2–6: n � 131; SOFA6�: n � 36. (B) Burn patients without inhalation injury. SOFA 0–1: n � 23; SOFA 2–6: n � 83; SOFA 6�: n � 10.
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 595

along with Ubs ability to reduce fluid shifts during infectiousand noninfectious inflammation in vivo18–20,22 provide astrong rationale to assess Ubs therapeutic potential also afterburn injuries.
REFERENCES1. Goldstein G, Scheid M, Hammerling U, Schlesinger DH, Niall HD,
Boyse EA. Isolation of a polypeptide that has lymphocyte-differentiating properties and is probably represented universally inliving cells. Proc Natl Acad Sci USA. 1975;72:11–15.
2. Ozkaynak E, Finley D, Varshavsky A. The yeast ubiquitin gene:head-to-tail repeats encoding a polyubiquitin precursor protein.Nature. 1984;312:663–666.
3. Hershko A, Ciechanover A. The ubiquitin system. Annu RevBiochem. 1998;67:425–479.
4. Ben-Neriah Y. Regulatory functions of ubiquitination in the immunesystem. Nat Immunol. 2002;1:20–26.
5. Sigismund S, Polo S, Di Fiore PP. Signaling throughmonoubiquitination. Curr Top Microbiol Immunol. 2004;286:149–185.
6. Weissman AM. Themes and variations on ubiquitylation. Nat RevMol Cell Biol. 2001;2:169–178.
7. Asseman C, Pancre V, Delanoye A, Capron A, Auriault C. Aradioimmunoassay for the quantification of human ubiquitin inbiological fluids: application to parasitic and allergic diseases.J Immunol Methods. 1994;173:93–101.
8. Takagi M, Yamauchi M, Toda G, Takada K, Hirakawa T, OhkawaK. Serum ubiquitin levels in patients with alcoholic liver disease.Alcohol Clin Exp Res. 1999;23: 76S–80S.
9. Akarsu E, Pirim I, Capoglu I, Deni O, Akcay G, Unuvar N.Relationship between electroneurographic changes and serumubiquitin levels in patients with type 2 diabetes. Diabetes Care.2001;24:100–3.
10. Okada M, Miyazaki S, Hirasawa Y. Increase in plasma concentrationof ubiquitin in dialysis patients: possible involvement in beta 2-microglobulin amyloidosis. Clin Chim Acta. 1993;220:135–144.
11. Akarsu E, Pirim I, Selcuk NY, Tombul HZ, Cetinkaya R. Relationbetween serum ubiquitin levels and KT/V in chronic hemodialysispatients. Nephron. 2001;88:280–282.
12. Manaka H, Kato T, Kurita K, et al. Marked increase in cerebrospinalfluid ubiquitin in Creutzfeldt-Jakob disease. Neurosci Lett. 1992;139:47–49.
13. Majetschak M, Krehmeier U, Bardenheuer M, et al. Extracellularubiquitin inhibits the TNF� response to endotoxin in peripheralblood mononuclear cells and regulates endotoxin hyporesponsivenessin critical illness. Blood. 2003;101:1882–1890.
14. Patel MB, Proctor KG, Majetschak M. Ubiquitin increases instored red blood cell units during storage. J Surg Res. 2006;135:226 –232.
15. Daino H, Shibayama H, Machii T, Kitani T. Extracellular ubiquitinregulates the growth of human hematopoietic cell. Biochem BiophysRes Commun. 1996;223:226–228.
16. Daino H, Matsumura I, Takada K, et al. Induction of apoptosis byextracellular ubiquitin in human hematopoietic cells: possibleinvolvement of STAT3 degradation by the proteasome pathway ininterleukin 6-dependent hematopoietic cells. Blood. 2000;95:2577–2585.
17. Kieffer AE, Goumon Y, Ruh O, et al. The N- and C-terminalfragments of ubiquitin are important for the antimicrobial activities.FASEB J. 2003;17:776–778.
18. Majetschak M, Cohn SM, Obertacke U, Proctor KG. Therapeuticpotential of exogenous ubiquitin during resuscitation from severetrauma. J Trauma. 2004;56:991–1000.
19. Majetschak M, Cohn SM, Nelson JA, Burton EH, Obertacke U,Proctor KG. Effects of exogenous ubiquitin in lethal endotoxemia.Surgery. 2004;135:536–543.
20. Earle SA, Proctor KG, Patel MB, Majetschak M. Ubiquitin reducesfluid shifts after traumatic brain injury. Surgery. 2005;138:431–438.
21. Earle SA, El-Haddad E, Patel MB, Ruiz P, Pham SM, MajetschakM. Prolongation of skin graft survival by exogenous ubiquitin.Transplantation. 2006;82:1544–1546.
22. Garcia-Covarrubias L, Manning EW III, Sorell LT, Pham SM,Majetschak M. Ubiquitin enhances the Th2 cytokine response andattenuates ischemia-reperfusion injury in the lung. Crit Care Med.2008; Jan 18; [E-pub ahead of print] PMID: 18209671.
23. Greenspan L, McLellan BA, Greig H. Abbreviated injury scale andinjury severity score: a scoring chart. J Trauma. 1985;25:64.
24. American College of Chest Physicians—Society of Critical CareMedicine Consensus Conference: definitions for sepsis and organfailure and guidelines for the use of innovative therapies in sepsis.Crit Care Med. 1992;20:864–875.
25. Goris RJ, te-Boekhorst TP, Nuytinck JK, Nuytinck JK, Gimbrere JS.Multiple-organ failure: generalized autodestructive inflammation?Arch Surg. 1985;120:1109–1115.
26. Ertel W, Friedl HP, Trentz O. Multiple organ dysfunction syndrome(MODS) following multiple trauma: rationale and concept oftherapeutic approach. Eur J Pediatr Surg. 1994;4:243–248.
27. Ertel W, Keel M, Marty D, et al. Significance of systemicinflammation in 1,278 trauma patients. Unfallchirurg. 1998;101:520–526.
28. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related OrganFailure Assessment) score to describe organ dysfunction/failure; onbehalf of the Working Group on Sepsis-Related Problems of theEuropean Society of Intensive Care Medicine. Intensive Care Med.1996 22:707–710.
29. Antonelli M, Moreno R, Vincent JL, et al. Application of SOFAscore to trauma patients. Sequential organ failure assessment.Intensive Care Med. 1999;25:389–394.
30. Nagele P. Misuse of standard error of the mean (SEM) whenreporting variability of a sample. A critical evaluation of fouranaesthesia journals. Br J Anaesth. 2003 90:514–516.
31. Patel MB, Majetschak M. Distribution and interrelationship ofubiquitin proteasome pathway component activities and ubiquitinpools in various porcine tissues. Physiol Res. 2007 56:341–350.
32. Majetschak M, Ponelies N, Hirsch T. Targeting the monocyticubiquitin system with extracellular ubiquitin. Immunol Cell Biol.2006;84:59–65.
33. Warden GD. Fluid resuscitation and early management. In: HerndonDN, ed. Total Burn Care. Philadelphia: W.B. Saunders; 1996:53–60.
34. Williams WG, Phillips LG. Pathophysiology of the burn wound. In:Herndon DN, ed. Total Burn Care. Philadelphia: W.B. Saunders;1996:63–70.
35. Klein MB, Hayden D, Elson C, et al. The association between fluidadministration and outcome following major burn: a multicenterstudy. Ann Surg. 2007;245:622–628.
36. Jeschke MG, Mlcak RP, Finnerty CC, Norbury WB, Kulp GA,Herndon DN. Burn size determines the inflammatory andhypermetabolic response. Crit Care. 2007 23;11:R90.
DISCUSSIONDr. Marc G. Jeschke (Galveston, Texas): He presented
that ubiquitin protein expression, ubiquitynilation plays animportant role in our body, is a new marker for severe, forstress and stress response.
When I read through this paper and on this data mythoughts were, is it not just another marker? We have cyto-kines as predictors and as major players in the whole host
The Journal of TRAUMA� Injury, Infection, and Critical Care
596 March 2008

defense response and systemic inflammatory response dis-covered 20 years ago and they failed what they promised.
So my first question leading to this is philosophical. Isubiquitin just another marker that we have, another tool ratherthan ubiquitin has any effect?
The next question I have to you is based on some con-fusion I had reading through your paper. You say ubiquitinreflects, its release reflects the extent of the damage andthe stress. However, when you get burned your basicubiquitin goes down so there seems to be a controversy inyour data and particularly, when you show that inhalationinjury causes an up-regulation of ubiquitin, however, thatis actually good. So is inhalation injury then good for burnpatients?
My next question is how did you measure ubiquitin? It’san ELISA as you mentioned. Is it total? Is it free? Is it bound?Is there a different effect of the ubiquitin that you measure?
And where is ubiquitin produced? That maybe is alsoplays a role when you say inhalation injury increases ubiq-uitin concentration.
And then, lastly, I would like you to elucidate on how isubiquitin released? Is it an active transportation? A passive?Is it just like enzymes when there is cell damage and thenreleases into the system?
And yet again leading to the point, what is the signifi-cance? Do we want to increase ubiquitin levels? Do we wantit decreased? Do we want it affected or do we want to give itor what is the clinical role then of ubiquitin? Again, thankyou very much for discussing this paper.
Dr. Basil A. Pruitt, Jr. (San Antonio, Texas): Interest-ing paper. You imply that it does something to capillarypermeability. How did you assess that? In terms of lungweight? Wet and dry weight lung changes or total bodyfluids? We’d like to hear how you rationalized that.
Dr. Timothy Billiar (Pittsburgh, Pennsylvania): Alongthe lines, some of the mechanistic questions, has the cellsurface receptor for ubiquitin been identified?
Dr. M. Majetschak (Miami, Florida): Thank you verymuch for your comments and questions. With regard to Dr.Jeschke’s questions, we showed that extracellular ubiquitinhas several anti-inflammatory effects in-vitro and in-vivo.Ubiquitin inhibits LPS evoked TNF� and IL-8 production ofleukocytes and a very recent study showed that it enhancesthe Th2 cytokine response in the lung during inflammation.Studies from other investigators showed that it also possessanti-microbial actions. More importantly, we showed inseveral independent animal models that it has beneficialand clinically relevant effects during infectious and non-infectious inflammation. Considering these actions alongwith its highly conserved protein structure and the fact thatthe anti-inflammatory cytokine response evolved relativelylate during evolution, its actions could represent a highlyconserved anti-inflammatory pathway in the innate immunesystem that is aimed to control the evolutionary highly con-served pro-inflammatory response. The wide range of its
serum concentrations in trauma patients shows that the use ofsystemic ubiquitin levels as a diagnostic or prognostic markerin the clinical arena is probably not feasible. Nevertheless, theresults of the present study along with its anti-inflammatoryand clinical relevant effects in-vitro and in-vivo suggest thatthe release of endogenous ubiquitin is protective and implythat burn patients who develop sepsis or multiple organ fail-ure have a ubiquitin deficiency. The next question was inregard to its association with injury severity and inhalationinjury. As presented before, we detected that ubiquitin serumlevels increased with increases in ISS, burn size and also withthe presence of inhalation injury. Thus, there is no inconsis-tency of the results.
The next question was in regard to the ELISA measure-ments. The ELISA is home-made and not commercially avail-able. This assay detects predominantly free ubiquitin. Weknow that it has some cross-reactivity with ubiquitin proteinconjugates which are also present in serum and that themeasurements overestimate the free ubiquitin concentrationsby approximately 5–10%.
In regard to ubiquitins cellular origin and mechanism ofrelease, our previous and the present study strongly suggestpassive release from damaged cells and tissues. We showed,for example, that approximately 30% of ubiquitin that isreleased into CSF after traumatic brain injuries can be attrib-uted to its release from lysed erythrocytes and that the re-maining amounts are probably released from the damagedbrain tissue. On the other hand, Kieffer et al. showed in 2003that ubiquitin is stored together with catecholamines in se-cretory chromaffin granules and released into the circulationupon stimulation of chromaffin cells. Two other reports sug-gested that it may also be secreted by leptomeningeal cellsand hairy cell leukemia cells. However, our finding thatpatients who were admitted to the emergency room but didnot suffer any injuries did not have increased ubiquitin levelssuggest that the amounts of ubiquitin that are released to-gether with catecholamines from the adrenal medulla duringthe stress response is probably very small, as compared to itsrelease due to cell damage. Finally, Dr. Jeschke asked abouta possible clinical role for ubiquitin. Since we showed inmultiple independent and clinically relevant animals studiesthat ubiquitin treatment has profound therapeutic effects aftertrauma and the present study clearly indicates a ubiquitindeficiency in burn patients who develop complications or die,evaluation of its therapeutic efficacy also after burn injuriesappears well justified.
With regard to Dr. Pruitt’s question, we showed thatubiquitin treatment consistently reduced systemic fluid re-quirements to maintain hemodynamics after traumatic andendotoxic shock while hematocrit values were identical inthe control and treatment groups. This was accompaniedby reduced brain edema formation, improved lung me-chanics and oxygenation with ubiquitin treatment. Besidesthis indirect evidence for effects of ubiquitin on fluid
Ubiquitin Release After Blunt Trauma and Burns
Volume 64 • Number 3 597

shifts, we also showed directly that it significantly reducedwet-weight dry-weight ratios of the lung after ischemia-reperfusion injury.
The last question by Dr. Billiar was with regard to a ubiq-uitin receptor. We recently provided initial evidence for a recep-tor for ubiquitin on monocytes that can be up-regulated duringinflammation. We showed that ubiquitin is taken up into thecell and then rapidly conjugated to intracellular proteins, thus
being introduced into the endogenous ubiquitin proteasomesystem of the target cell. This uptake showed saturationkinetics and a Kd value in the very low nanomolar range,which strongly suggests a highly specific receptor mediateduptake process. However, this putative receptor has not beenidentified yet.
Once again, I’d like to thank all discussants for theircomments and questions.
The Journal of TRAUMA� Injury, Infection, and Critical Care
598 March 2008