“t · martin czerny, university hospital zurich, ... eacts daily news is pleased to announce the...
TRANSCRIPT

Theofficialnewspaperofthe27thEACTSAnnualMeeting2013 Sunday 6 October
Martin Czerny, University Hospital Zurich, Switzerland
Diseaseoftheaortaisnowbeingrecognizedasdistinctentityincreasinginincidence.Itisacknowledgedthatthe
managementofbothacuteandchronicaorticconditionsnowhavesuchabroadevidencebasethatspecialistknowledge,trainingandskillsarerequiredtoprovidebestpatientcare.Thespecialismtraversesallagegroups;youngpatientsaremostlyaffectedbyconnectivetissuediseases(CTS),middle-agedpatientsareaffectedbydegenerationofbicuspidaorticvalveswithorwithoutaneurysmalformationofthesinusofValsalvaortheascendingaortacausedbyaccompanyingmedialdegeneration,whereaselderlypatientsmayalsodevelopthesamephenotypeofdisease(aorticvalveandascendingaorta)butduetootherunderlyingpathomechanisms,predominantlyatherosclerosisandcalcificdegeneration.
Endovascularstentinghasbroadenedaortictherapeuticsandhasledtodevelopmentofmanyalternativetreatmentapproachesusingisolatedstentingandhybridstent-surgerytechniques.Someofthemhavebecomeroutineandmaybejudgedasvalidatedandstandardized.
However,betterunderstandingofthelimitationsofendovasculartherapyaswellasacknowledgementoftheexcellentresultsforconventionalaorticsurgerymustbeconsideredbeforeexpandingendovascularoptionstoallaorticpathologiesofnewpatientpopulations.Amultidisciplinaryapproachmayclearlyservetochoosetheadequatetreatmentmodalityin
theindividualsettingascomplicationsinducedmightnotbehandledinanadequatefashionbynon-cardiacsurgeons(e.g.endovasculartreatmentofascendingaorticpathology).
Thelogicalconsequenceoftheevolutionofaorticsurgeryandtoreconcileheterogeneityoftreatmentmodalitiesisthecreationofaorticcenterscapableoftreatingtheentireorganwithalldiagnosticandtherapeuticoptions.Theleadersofsuchcentersarelikelytobecardio-vascularsurgeonswithexperienceinbothcardiacandvascularsurgicaldisciplinesincludingendovascularskills.
Byabroadsurgicaltrainingprogramwithaclearanddefinedaiminadefinedtimeperiod,leavingroomforboth,surgery,endovasculartherapyandscience,youngpeoplemusthavethechancetodevelopandmature.Itisourtasktodefinethefutureandtopavethewayforthegenerationstocome.
Wire or knife? Not to go where the puck is but to go where the puck will be
Plenary Session: Life is short and the art long 08:30 Hall D
In this issueIn this issueIntra- cardiac and vascular ultrasoundEnrico Ferrari outlines the benefits of these two imaging modalities2
Tuberculosis Piotr Yablonski discusses the tactics and results of treating patients with different forms of MDR and XDR and the role of individualised treatment4
Fallot Giovanni Stellin states that pulmonary valve integrity can be preserved during early ToF repair by utilising balloon dilation 6
Proximal TADAdriana Gittenberger-de Groot
examines thoracic aortic disease and explains the embryology of the aorta - from cells to an organ 8
Patient adherence Jo Cook reports on the role of the primary care team and the role they play in a patient’s adherence to
their medication. 12
Donor shortage Thierry Carrel argues that DCDD grafts are useful in overcoming the shortage of donor organs 18
CMR or PET for surgery?Rafael Sadaba looks at the benefits of both CMR and PET imaging modalities when assessing
a patient’s for coronary artery surgery 19
EACTS Academy Events in 2014 21
Floorplan 24
EACTS 2014 25
“T hesuccessofaValve-in-Valveprocedureisbasedoncorrectidentificationof
thesurgicalvalve,choosingthecorrectsizeoftheTAVIvalveanditssubsequentaccurateplacement,”saidBapat.“Surgicalvalvesvaryinappearanceunderfluoroscopy,structureandalsointheirinternaldiameter.Similarly,TAVIvalvesdifferintheirappearancesandavailablesizes.KnowledgeaboutallthesurgicalvalvesthathavebeenimplantedinthelasttwodecadesisminimalbutrelevanttotheValve-in-Valvetherapy.”
SHVs and TAVI valvesUsingtheValve-in-ValveApp,userscannowfamiliarisethemselveswithimportantdesigninformationaboutvariousstentedandstentlessSHVsandTAVIvalves.TheycanselectaspecificvalveandalabeledsizeandfindoutwhichsizeofTAVIvalve
couldbeusedandhowitisbestplacedduringaValve-in-Valveprocedure.Ifthevalvetypeisunknown,theappalsoguidestheuserthroughaseriesofstepswheretheycanidentifythesurgicalvalvetypeandthenusetheinformationavailableforit.
“TheValve-in-Valveappreducestheneedtotrawlthroughvastamountsofliteraturetofindinformationspecifictotheclinicalscenario,”explainedBapat.“TheapplicationnavigatestheuserthroughimportantaspectsofsurgicalandTAVIvalvedesign,whicharevitalforasuccessfulValve-in-Valveprocedureandlogicallystepsthroughthepossiblecombinationstogivetheuserspecificinformationneededtoperformtheprocedure.”
Valve-in-Valve MitralBapatandcolleagueshavealsoreleasedthesecondappinthisseries–Valve-in-ValveMitral,specifictothevalvesandringsusedinthemitralposition.Inadditiontotheinformationaboutmitral
valvesandrings,theappprovidesimportantdifferencesbetweenanaorticValve-in-ValveandamitralValve-in-Valveprocedure.
“Attheheartoftheideaiseducationthatisfreetouseandtheinformationisalsoavailablewithouttheneedforaninternetconnectionandwillenhancetheusersunderstandingofvarious
aspectsofthisprocedure,”BapattoldEACTS Daily News.“Wehopethiswillresultinimprovedresultsandbetteroutcomesforpatients.”
AnAndroidversionoftheappisplannedtobereleasedinOctober2013.
EACTS Daily News is pleased to announce the 2013 EACTS Techno College Innovation Award was won by Dr Vinayak Nilkanth Bapat (Guys and St. Thomas’ Hospital, London, UK), for the ‘Valve-in-Valve’ app that provides information specific for a clinical scenario, quickly and simply and helps in the planning of and performing, a Valve-in-Valve case.
Valve-in-Valve app wins 2013 EACTS Techno College Innovation Award
Vinayak Bapat
Martin Czerny
Domenico Pagano Chair of the QUIP
Elka Humphrys QUIP Project Manager
In2012EACTSestablishedaQualityImprovementProgramme(QUIP)toencourageimprovementofclinicaloutcomesforpatients,andtopromote
theimportanceofintegratingqualityimprovementinitiativesintodailyclinicalpractice.
TheprogrammereliesontheparticipationofEACTSmembersandsincethelaunchoftheQUIP,sixmemberledgroupshavebeenestablishedtosupportprojectswithintheprogramme;theNetworkforOutcomesResearch,PublishingOutcomes,ClinicalConsensus&Guidelines,Education,Nursing&AlliedHealthProfessions,andPerfusion.ItisthankstoyoureffortsseenthisyearthatworknowspansallfourEACTSDomainsandincludessurgeons,perfusionists,nurses,andalliedhealthprofessionalsworkingtowardsimprovingclinicaloutcomesforpatients.
Projectswithinthegroupsarenowprogressingandinitialresultswillbe
presentedinvarioussessionsduringthisyear’sAnnualMeeting,includingtheAcquiredCardiacDiseasePostgraduateEducationsessionsonSunday,Tuesday’sfocussessiononoptimisingtrainingforbetterpatientoutcome,andthroughouttheDomainprogrammes.FurtherinformationonallprojectsandgroupswillbeavailableattheEACTSexhibitionstand(HallXL,Booth148),andamemberoftheQUIPteamwillbeavailableonthestandatthefollowingtimestoansweranyspecificquestions.nSunday6October: 17:00-19:00nMonday7October: 09:00-10:00
13:00-14:00 15:45-16:30
nTuesday8October: 09:00-10:00 13:00-15:15
We thank all members currently contributing to QUIP projects, and we look forward to working with many more members in the future. Your support will lead to more quality improvement projects and will increase the difference we can make to our patients.
EACTS Quality Improvement Programme
Togetinvolvedinanyofthecurrentprojectsortojoinoneofthegroupsforfutureprojects,visittheEACTSexhibitionstand(HallXL,Booth148)atthe27thAnnualMeetingandspeaktotheQUIPteam.
Alternatively,nominateyourselfforinvolvementintheQUIPviatheMyProfiletabinyourEACTSUserArea:www.eacts.org/user-area
2 Sunday 6 October 2013 EACTS Daily News
Sunday 6 October
Postgraduate Course
Plenary Session: Life is short and the art long
Hall D
J.L. Pomar, Barcelona; T. Sundt, Boston
08:30 Attentiontodetailinadumbed-downworld Paul Sergeant
08:50 Overregulationoranarchy? David Barron
09:15 Trainingisbrokenandthereisnoquickfix Michael Dusmet
09:35 WireorKnife?Nottogowherethepuckisbuttogowherethepuckwillbe Martin Czerny
Acquired Cardiac Disease
10:30 Session 1: Imaging in Mitral valve repair
Hall D
Moderator: J Pepper, London; V. Delgado, Leiden
10:30 Does3Dchocardiographyenhancedecisionmaking? Jolanda Kluin
10:50 Howdowegetthebestoutofmagneticresonanceimaging Philip Kilner
11:10 Directvieworvideo-scopicimaging Ludwig Muller
11:30 Image-baseddecision-makingincomplexmitralvalverepair Patrick Perier
12:30 Session 2: Imaging in Transcutaneous valve interventions
Hall D
Moderators: C. Ruiz, New York; F. Beyersdorf, Freiburg
12:30 Planningtranscatheteraorticvalveimplantationprocedures:theroleofimaging Peter Wenaweser
12:55 Intraoperativeguidanceintranscatheteraorticvalveimplantationprocedures Joerg Kempfert
13:20 Intracardiacandintravascularultrasound Enrico Ferrari
13:40 Image-guidedtransseptalpuncture Alec Vahanian
14:05 Image-guideddecisionmakingformitralinterventions Joerg Seeburger
14:30 Session 3: Imaging in Coronary Artery Surgery
Hall D
Moderators: T.A. Folliguet, Nancy; A. Vahanian, Paris
14:30 Catheter-basedimaging(OCT;IVUS) Simon Davies
14:50 Assessmentofviability(magneticresonanceimaging,positronemissiontomography) Rafael Sádaba
15:10 Myocardialassessment:Echocardiography Victoria Delgado
15:30 Graftassessment:intra-operativeimaging Syed Rehman
15:50 ImagingfortheHybridapproach Rashmi Yadav
16:10 RoleoftheHeartTeamapproach Sacha Salzberg
14:00 Circulating viewpoints
Hall E2
14:00 Introduction A.P. Kappetein, Rotterdam
14:05 PrideandPrejudiceincardio-thoracicsurgery B.E. Keogh, London
14:35 TalesofatravellingsurgeoninAfrica P. Simon, Vienna
10:25 Session 1: Improving Perfusion
Hall F1
Moderators: F. Merkle, Berlin; A. Liebold, Ulm
10:30 Antegradeandretrogradeautologousprimingwithconventionalbypasssystems Korneel Vandewiele
10:50 Clinicalexperiencewithminimizedbypasssystemsinaorticsurgery:theHammersmithtechnique John Mulholland
11:10 Cellsaversduringcardiolpulmonarybypass:savingbloodandreducinginflammation Anders Jeppsson
11:30 Howtopreventairembolismduringvalvesurgery? Manuel Antunes
11:50 Toclamportoinflate:thehandlingofmyocardialperfusioninMICS Johannes Bonatti
12:10 Simultaneousbrain,heartandbodyperfusioninaorticarchsurgery Christoph Benk
12:30 Session 2: Safety in perfusion
Hall F1
Moderators: A. Jeppsson, Gothenburg; C. Hamilton, Vogtareuth
12:30 Failureduringcardiopulmonarybypass:howtohandledifficultsituations Gino Gerosa
Continued on page 4
Aorticstenosis(AS)isacommonlife-threateningcondition
thatisanunder-appreciatedyetseriousandgrowingpublichealthproblem1.Asiswidelyknowninthecardiacsurgerycommunity,manypatientswithvalvediseasearenotreferred,oftenwithdisastrousconsequences.AtEdwardsTM,wearecommittedtoraisingawarenessofASundertreatmentamongreferringcommunities,byimplementingeducationalprogramsandsymposiaacrossEuropeanconferencesthatincludeadvertisingtoreferringphysicians(GPs,cardiologists,andgeriatricians),andtargetededucationthroughscientificandlaypressarticles,e-learning,andpartnershipswithkeyprofessionalsocieties.Onceapatientisreferred,EdwardsTMisdedicatedtoprovidingyouwiththebestoptionsforminimallyinvasivetechniquesthroughcontinuedinnovationinsurgicalandtranscatheterheartvalvedevicesanddeliverysystems.
ASmayprogressrapidly.TherearenomedicationstoreverseAS,andtreatmentoptionsandtimingmatter.Withouttreatment,symptomaticpatientswithsevereASsurviveanaverageof2–3years.Surgicalaorticvalvereplacement(SAVR)isthegoldstandardtreatment
forsevereASandshouldbeperformedpromptlyaftersymptomonset2.However,whileSAVRremainstheAStreatmentofchoiceformostpatients,morethanathirdofpatientsisdeniedsurgery5-10(Figure).PractitionersarereluctanttoconsiderSAVRinolderpatientsorinthosedeemedunfitforsurgeryduetomajorcardiacdysfunctionandcomorbidities,orduetohighoperativeriskandlowlifeexpectancy2,9.Inthepast,thesepatientswouldnotbetreatedorevenreferred.However,thisischangingthankstominimallyinvasivetechniquesincludingtranscatheteraorticheartvalveimplantation(TAVI),
whichisnowperformedroutinelyatcertifiedheartcenters.Since2012,theEuropeanSocietyofCardiologyandEuropeanAssociationforCardio-ThoracicSurgeryrecommendTAVIinitsguidelinesformanagementofAS.TAVIisindicatedinpatientswithseveresymptomaticASwhoarenotsuitableforsurgery,asassessedbyamultidisciplinaryheartteam.Thisdecision-makingapproachisparticularlyadvisableinthemanagementofhigh-riskpatients2.
AllhealthcareprovidersmanagingpatientswithASsymptomsneedtoensurethatthesepatientsare
appropriatelyreferredtoamultidisciplinaryheartteam,receiveadefinitivediagnosis,andareawareoftheirtreatmentoptions,whetherSAVRorTAVI.WithEdwardsTM’rapidinnovationinbothSAVRandTAVItechnologiestocontinuallylessentheinvasivenessofAStreatment,ourgoalistoensurethatthereisaproductsuitableforeverypatient,irrespectiveoftheirdiseaseprogression.
ThereisanencouragingtrendsincetheintroductionofTAVIwhichisanincreaseinpractitionerawarenessofAS,withacorrespondingincreaseintotalreferralsandAStreatmentviaboth
surgicalandtranscathetermodalities11.
HealthcarepractitionersshouldthereforenotweakentheireffortstoreduceASundertreatment:thingsareontherightpath.References
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvu-lar heart diseases: a population-based study. Lancet 2006;368:1005-11.2. Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451-96.3. Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr., Faxon DP, Freed MD, et al. 2008 Focused up-date incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardi-ology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardio-vascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008;118:e523-661.4. Ross J, Jr., Braunwald E. Aortic stenosis. Circu-lation 1968;38:61-7.5. Iung B, Baron G, Tornos P, Gohlke-Barwolf C, Butchart EG, Vahanian A. Valvular heart disease in the community: a European experience. Curr Probl Cardiol 2007;32:609-61.6. Bach DS, Cimino N, Deeb GM. Unoperated pa-tients with severe aortic stenosis. J Am Coll Cardiol 2007;50:2018-9.7. Bouma BJ, van Den Brink RB, van Der Meulen JH, Verheul HA, Cheriex EC, Hamer HP, et al. To oper-ate or not on elderly patients with aortic stenosis: the decision and its consequences. Heart 1999;82:143-8.8. Charlson E, Legedza AT, Hamel MB. Decision-making and outcomes in severe symptomatic aortic stenosis. J Heart Valve Dis 2006;15:312-21.9. Iung B, Cachier A, Baron G, Messika-Zeitoun D, Delahaye F, Tornos P, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J 2005;26:2714-20.10. Pellikka PA, Sarano ME, Nishimura RA, Malouf JF, Bailey KR, Scott CG, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aor-tic stenosis during prolonged follow-up. Circulation 2005;111:3290-5.11. Malaisrie SC, Tuday E, Lapin B, Wang E, Lee R, McGee EC, et al. Transcatheter aortic valve implanta-tion decreases the rate of unoperated aortic stenosis. Eur J Cardiothorac Surg 2011;40:43-8.
Enrico Ferrari University Hospital of Lausanne, Switzerland
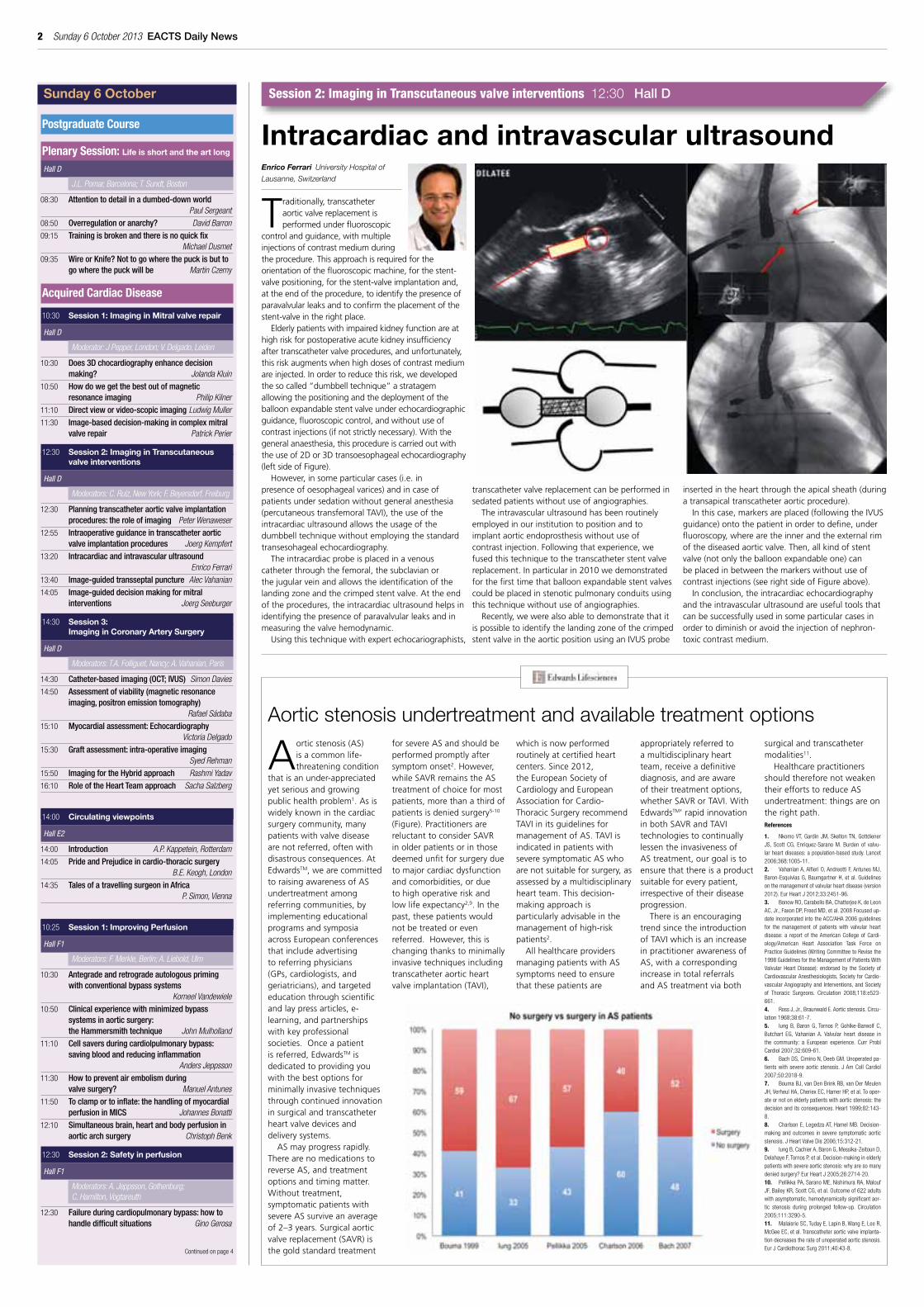
Traditionally,transcatheteraorticvalvereplacementisperformedunderfluoroscopic
controlandguidance,withmultipleinjectionsofcontrastmediumduringtheprocedure.Thisapproachisrequiredfortheorientationofthefluoroscopicmachine,forthestent-valvepositioning,forthestent-valveimplantationand,attheendoftheprocedure,toidentifythepresenceofparavalvularleaksandtoconfirmtheplacementofthestent-valveintherightplace.
Elderlypatientswithimpairedkidneyfunctionareathighriskforpostoperativeacutekidneyinsufficiencyaftertranscathetervalveprocedures,andunfortunately,thisriskaugmentswhenhighdosesofcontrastmediumareinjected.Inordertoreducethisrisk,wedevelopedthesocalled“dumbbelltechnique”astratagemallowingthepositioningandthedeploymentoftheballoonexpandablestentvalveunderechocardiographicguidance,fluoroscopiccontrol,andwithoutuseofcontrastinjections(ifnotstrictlynecessary).Withthegeneralanaesthesia,thisprocedureiscarriedoutwiththeuseof2Dor3Dtransoesophagealechocardiography(leftsideofFigure).
However,insomeparticularcases(i.e.inpresenceofoesophagealvarices)andincaseofpatientsundersedationwithoutgeneralanesthesia(percutaneoustransfemoralTAVI),theuseoftheintracardiacultrasoundallowstheusageofthedumbbelltechniquewithoutemployingthestandardtransesohagealechocardiography.
Theintracardiacprobeisplacedinavenouscatheterthroughthefemoral,thesubclavianorthejugularveinandallowstheidentificationofthelandingzoneandthecrimpedstentvalve.Attheendoftheprocedures,theintracardiacultrasoundhelpsinidentifyingthepresenceofparavalvularleaksandinmeasuringthevalvehemodynamic.
Usingthistechniquewithexpertechocariographists,
transcathetervalvereplacementcanbeperformedinsedatedpatientswithoutuseofangiographies.
Theintravascularultrasoundhasbeenroutinelyemployedinourinstitutiontopositionandtoimplantaorticendoprosthesiswithoutuseofcontrastinjection.Followingthatexperience,wefusedthistechniquetothetranscatheterstentvalvereplacement.Inparticularin2010wedemonstratedforthefirsttimethatballoonexpandablestentvalvescouldbeplacedinstenoticpulmonaryconduitsusingthistechniquewithoutuseofangiographies.
Recently,wewerealsoabletodemonstratethatitispossibletoidentifythelandingzoneofthecrimpedstentvalveintheaorticpositionusinganIVUSprobe
insertedintheheartthroughtheapicalsheath(duringatransapicaltranscatheteraorticprocedure).
Inthiscase,markersareplaced(followingtheIVUSguidance)ontothepatientinordertodefine,underfluoroscopy,wherearetheinnerandtheexternalrimofthediseasedaorticvalve.Then,allkindofstentvalve(notonlytheballoonexpandableone)canbeplacedinbetweenthemarkerswithoutuseofcontrastinjections(seerightsideofFigureabove).
Inconclusion,theintracardiacechocardiographyandtheintravascularultrasoundareusefultoolsthatcanbesuccessfullyusedinsomeparticularcasesinordertodiminishoravoidtheinjectionofnephron-toxiccontrastmedium.
Intracardiac and intravascular ultrasoundSession 2: Imaging in Transcutaneous valve interventions 12:30 Hall D
Aortic stenosis undertreatment and available treatment options

4 Sunday 6 October 2013 EACTS Daily News
Piotr Yablonskii President of the Association of Thoracic Surgeons of Russia
Relationtosurgicaltreatmenthaschangedovertime.Successoftherapeutictreatmentanddecreaseinthe
incidenceoftuberculosisintheworldinthemid-20thcentury,thatfindingsuggeststhatsurgicaltechniquemaybeexcludedfromthemanagementofpatientswithtuberculosis.However,theepidemicofMDRandXDRtuberculosishaschangedthepresentationofeventhemostactivesupportersoftheconservativeapproach.Now,WHOTaskforcegrouphasformulatedthemainindicationsforsurgicaltreatment.Whichsummarizedasfollows:1)LocalizedformsofcavitaryTBwithcontinuousmycobacteriumtuberculosisexcretionconfirmedbybacteriologicalexaminationanddrugsusceptibilitytesting(DST)after4-6monthsofsupervisedanti-TBchemotherapy.2)M/XDR-TBcharacterizedbyanti-TBchemotherapy’sfailure3)ComplicationsandsequelaeofTBprocess(includingM/XDR-TB)4)Otherindications.
Atthesametime,avarietyofclinicalformsoftuberculosiscanbeconsidered
thesurgeryintheseComplexcases.SecondandthirdpointsaremostcomplicatedcasesofTB-surgery.InourpresentationonSunday6thOctoberentitled:“Complextuberculosiscases”,wewillshowthetacticandresultsofthetreatmentofpatientswithdifferentformsofMDRandXDR-tuberculosis.Therewillbethreecases.
First case –male,45yearsoldwithrapidlyprogressionoftuberculosisintheleftlungandcavernoustuberculosisofupperlobeofrightlung.Previously,
patientwasdiagnosed,asMDRTB,complicatedwithpyopneumothorax.Periodofdrugtherapywas18months,accordingDST.Chesttubewasinsertedintothepatienttwicebeforeadmissiontothehospital.Leftpneumonectomywithextrapleuraldissectionwasdoneasfirststepofsurgicalpartoftreatment.Earlypostoperativeperiodwascomplicatedsmallbronchopleuralfistula.Itwasclosedafterconservativetreatment.Rightupperposteriorthree-ribsthoracoplastywasdoneaftertwomonths.Long-termfollow-upwasuneventful,duringallperiodMBTinsmearsabsent.
Second case–male,32yearsoldwithXDRpulmonarytuberculosis.CTscanrevealeddestructionofcompletelyleftlungandcavernoustuberculosisofupperrightlobe,complicatedpulmonarybleeding.Previousperiodoftherapywas54months,accordingtoDST.Firstly,endobronchialvalvewasinsertedintheupperrightbronchus.Thesecondstepofmanagementofpatient,leftpneumonectomywithextrapleuraldissectionwasdone.Postoperativeperiodwasuneventful.But,despiteofendobronchialblockingcavernousinupperrightlobewaspersisting.
Accordingthis,rightupperposteriorfour-ribsthoracoplastywasdone.Six-monthfollow-upnotrevealanysignsofprogressionofTB.ConversioninonemonthafterlastoperationandallperiodafterMBTinsmearsabsent.
Third case –male,59yearsoldwithMDRpulmonarytuberculosis,complicatedaspergillosisoflung.Historyofdiseasebegan36yearsago,whenpatientwastreatedthrowrightupperlobectomywithantibacterialtherapyaccordingtoDSTfromcavitarytuberculosis.Butafter27yearspulmonarybleedingwasdiagnosedanddiagnosisofMDRtuberculosisandaspergillosiswasconfirmed.Nineyearspatientdeclineallsuggestionofsurgery.Afteradmissionofpatientinclinic,CTscanrevealedcavityinlowlobeofrightlungandinthemiddleofcavityaspegillomawasdiagnosedtoo.Completionrightpneumonectomywasdone.Long-termfollow-upwasuneventful,duringallperiodMBTinsmearsabsent.
ThegoodresultsoftreatmentcanbecomethebasisforfurthercarefulstudyofallthepossibilitiesofsurgicaltreatmentofpatientswithComplexMDRandXDRpulmonarytuberculosis.
The new face of the old problem
13:50 Session 3: Transplant/mechanical assist
Hall F1
Moderators: J. Mulholland, London; G. Gerosa, Padua
13:50 Cardiactransplantationwithnon-heart-beatingheartdonors:futurestrategyorfantasy Thierry Carrel
14:10 Long-termsupportwithleftventricularassistdeviceinelderlypatients Bart Meyns
14:30 Donorextracorporeallifesupportforimprovedorganpreservation Guillaume Lebreton
14:50 TheOrganCareSystem:amulticentrestudy Martin Strüber
15:10 Session 4: Pro/ Con:Use of Intra-aortic balloon support during ECMO/ECLS
Hall F1
Moderators: T. Carrel, Berne; G. Lebreton, Paris
15:10 Pro Arnt Fiane
15:30 Con Peter Nielsen
15:50 EuropeanPerfusionRegistry:Aplatformforperfusionqualityimprovement Luc Puis
Nurses, Nurse Practitioners and Physician Assistants Programme
08:45 Session 1: Moving Borders
Hall K
Moderators; T Bartley, Birmingham; D Bordingggaard, Odense
08:45 Welcome Leslie Hamilton; Richard Van Valen
08:55 NursinginAustria M Burscher
09:05 Video-assistedthoracoscopiclobectomyenhancesrecoveryandreducestheneedforphysiotherapyinterventionscomparedtothoracotomy Paula Agostini
09:25 PatientunderstandingandexperienceoftheirSternotomyandthePromotionofWoundHealing Libby Nolan
09:45 Thepatient,theGP,theprimarycareteam:theirrelationship,adherencetotreatmentandtheimplicationsforresearch Jo Cook
10:05 Postoperativemobilisation C Brun Thorup
10:25 Transcatheraorticvalveimplantation,theEuropeanperspective Bo Kjeldsen
10:40 Thetranscatheteraorticvalveimplantationdebate;theviewfromthealliedprofessionals Nicolas Van Mieghem
11:15 Session 2: Moving Borders
Hall K
Moderators: C Bannister, Southampton; M Hoffmann, Kalsruhe
11:15 TheAmericanperspective D Lizotte
12:00 IntroducingPAsinGermanyandtheirroleinthechain Craig Matthews
12:20 Postlungsurgeryrehabilitation P Nikkelsen
12:40 Education:Thoracic:MorbusGorhan M Brunott
13:00 Lunch:UpdateonEQUIP D Pagano, T Bartley
14:00 Session 3: Non-surgical skills for teams in theatre
Hall K
Faculty: S Patterson Brown; N Maran, Edinburgh
Basic Science
10:30 Session 1: The enemy from within
Hall P
Moderators: K. T. Preissner, Giessen; J. Vaage, Oslo
10:30 MitochondrialDNA:adangeroussignalintheheart? Marte Bliksoen
11:10 Damagingnatureofendogenousribonucleicacidincardiacischaemia/reperfusioninjury. K. Preissner
13:00 Session 2: A look into the future
Hall P
Moderators: P. Dohmen, Leipzig; J. Vaage, Oslo
13:00 Thefutureofvalvesurgery P. Dohmen, Leipzig
13:30 Thefutureofmyocardialrevascularization P. Sergeant, Leuven
14:00 Transplantationofengineeredhearttissueasabiologicalcardiacassistdevice F. Schlegel, Leipzig
14:40 Session 3: Bleeding
Hall P
Moderators: T. Tonnessen, Oslo; M. Sousa Uva, Lisbon
14:40 Thebasicsofbleedingandhaemostasisincardiacsurgery A. Jeppsson
Continued from page 2
Continued on page 6
Cardiopulmonarybypass (CPB) isakeycontributor topatientoutcomes incardiacsurgeryandhasasignificantimpactondirectandindirectcostsof
healthcare.Inachangingscenariowherecardiacsurgerypatientsaremorecomplexand
costcontainmentpressureisincreasing,interestinoptimizedperfusionstrategiesisrapidlygrowing.ThegoalistominimizethenegativeimpactofCPBonpatientoutcomeswhilereducingcostsofcare.
Formorethan40years,SorinGrouphasbeenleadinginnovationincardiacsurgery, offering products and solutions to help clinicians address the keychallengesofdailyclinicalpractice.
Afewshortmonthsfollowingthe launchof itsnewlydesignedperfusionelectronic charting system, Sorin Connect™, Sorin Group reinforces itscommitment to innovation by launching a complete new family of adultoxygenator systems, Sorin INSPIRE™ along with its Goal-Directed Perfusionsystem,SorinHeartLink™atEACTS2013.
The new INSPIRE family of oxygenators has been designed to meet alladult patient needs and to support different perfusion practices. The INSPIREfamily provides clinicians with new options to improve patient outcomes incardiopulmonarybypass,allowingthemtosafelyandcomfortablyrunperfusionwithpowerfulandconsistentperformance.
ThenewINSPIREfamilyoffersseveralkeybenefitstoclinicians:nAnunprecedentedchoiceofthemostcompletefamilyofadultoxygenators,
fullymodularandflexiblen Thefirstandonly6LPMmaximumratedbloodflowoxygenatorsystems,
representingtheidealsolutionforoptimizedperfusioninawidepatientpopulation
n Highlyefficientoxygenatorswithpowerfulandconsistentperformanceupto8LPM,allowingtosafelyandcomfortablytreatalladultpatientswithonedevice
n Minimizedimpactonhemodilution,whichcontributestodecreasedbloodtransfusionsandimprovedclinicaloutcomesduringandaftercardiopulmonarybypass(CPB)
n Superiorgaseousmicroemboli(GME)handlingincomparisontocompetitivedesigns,helpingtoprotectpatientsfromapotentialsourceofneurologicaldamageafterCPB
n Adual-chamberreservoir,allowingacomprehensiveapproachtoenhancedbiocompatibilitythankstoitsuniquedesign,tothephosphorylcholinePH.I.S.I.OcoatingandtoitseasyconnectiontoSorinXTRA®
AutotransfusionSystem.n TheHeartLinkcardavailableinINSPIRE
PTSfortheactivationoftheHeartLinksystemfunctionalities,includingGDPMonitorTM
Before launching this new family, theINSPIRE oxygenator systems have beenextensivelyevaluatedclinicallyinaglobalMarketAssessmentStudyofover2.000patients.Reductioninprimingvolume,reservoirperformance,gasexchangeandheatexchangewere consistently ratedas themost compelling featuresof theINSPIREdevices.Thestudyreportedthatwhencomparedtocurrentoxygenatorsystems,INSPIREdevicesreducedprimingvolumeanddeliveredhigherhematocritduringCPB.
INSPIRE isakeycomponentofthenewHeartLinksystem,whichfacilitatesimprovementboth inpatientoutcomesand in thedailyperfusionpracticebyunlocking synergies between the key system components: S5/C5 heart-lungmachines,CONNECTperfusionchartingsystem, INSPIREfamilyofoxygenatorsandXTRAautotransfusionsystemandbyenablingtheimplementationofGoal-DirectedPerfusion.
For further information, please visit the Sorin Group booth #114.
Session 2: Challenging infectious diseases 12:30 Room I
Sorin Group launches a complete new family of adult oxygenators at eAcTS 2013
Piotr Yablonskii
Syed M Rehman John Radcliffe Hospital, Oxford
BothESC/EACTSandNICE(UK)haveissuedguidelinesrecommendingtheuseofintra-operativegraftevaluation.Technicalerrorisacontributingfactortograftfailure
andtheintra-operativegraftfailureratereportedintheliteratureis4%.Identificationoffailedgraftsbeforeleavingtheoperatingtheatregivessurgeonstheopportunitytorevisesuchgraftsandpotentiallypreventtheassociatedpoorclinicaloutcomeswhichincludemyocardialinfarctionanddeath.Conventionalangiographyisthegoldstandardfordemonstratinggraftpatency.However,itisnotpracticalforroutineintra-operativeuseduetoincreasedresourceimplicationsofpersonnel,facilities,timeandcost.Inaddition,ithasrisksduetobeinginvasiveand
requiringpotentiallynephrotoxiccontrast.Twotechniquesthataremorecommonlyusedinpracticeareintra-operativefluorescenceimaging(IFI)andtransittimeflowmetry(TTFM).
IFIusesindocyaninegreendye,which,wheninjectedintothebloodstream,bindsimmediatelytoplasmaproteinsandemitslightwhenilluminatedwithanear-infraredlightsource.Thisfluorescenceiscapturedonavideocamerawhichprovidesareal-timeimagesimilartoconventionalangiography.
TTFMisbasedontheprincipleoftransit-timeultrasoundtechnology.Itusesaflowprobe,whichholdsthegraftperpendiculartotwoultrasonictransducersandafixedacousticreflectorhousedwithintheprobe.Theultrasoundpulsesignalstransmittedfromthetransducerspropagatebothupstreamanddownstreamofthedirectionofbloodflowthroughthereflector.Theintegratedtransittime
thatmeasuresthedifferencebetweenthedurationtakenforsignaltravelbetweenthetwotransducersisusedtoprovideaprecisemeasureofflowvolume.
Specificmeasurementstakenaremeangraftflow,diastolicflowindex(thepercentageoftotalflowoccurringindiastolewhichshouldexceed50%ofmeangraftflow)andpulsatilityindexwhichisanestimateoftheresistancetograftflow.
Asummaryoftheliteraturedemonstratesthatintra-operativeimagingissafeanddoesnecessitategraftrevisionin3.4%(IFI)and5.4%(TTFM)ofcases.ThereisevidencethatahighpulsatilityindexrecordedwithTTFM,indicatingunsatisfactorygraftflow,isassociatedwithsignificantlygreatermajoradversecardiaceventsandmortality.
AnanalysisbytheUK’sNationalInstituteforHealthandClinicalExcellencesuggeststhatroutineuseofTTFMwouldresultinacostsavingofapproximately€135perpatient.Theuseofintra-operativeimagingforgraftevaluationisanimportantconceptforcardiacsurgeonstobefamiliarwithandtoconsideremployingintheirroutinepracticeofcoronaryarterybypassgraftsurgery.
Graft assessment: Intra-operative imaging
Session 3: Imaging in Coronary Artery Surgery 14:30 Hall D


6 Sunday 6 October 2013 EACTS Daily News
Session 3: Complex surgery 15:30 Room F2
Giovanni Stellin University of Padua, Padua, Italy
earlytetralogyofFallot(ToF)repairhasbeenadvocatedsincemanyyearstoavoidthedeleteriouseffectsof:chroniccyanosisandspells,systemic-to-pulmonaryartery
shuntsandtheirconsequences,chronicRVoverloadandmyocardialcompensatoryhypertrophy.Atransatrial-transpulmonaryapproachavoidsalargerventriculotomyintotheRVbody,whenneeded.
InourInstitution,ToFrepairhasbeenperformedinyounginfantssincetheearly’80;earlyone-stagetrans-atrialrepair(within3-4monthsofage)sincetheearly’90.Afurtherevolutionofourtechniqueshasbeenrecentlydeveloped(2007)forsavingtheanatomicintegrityofthenativepulmonaryvalve(PV).
A‘classic’repairincludestheincisionofPVannulus,whenhypoplastic,leadinginevitablytoachronicpulmonaryregurgitationwithRVdilatationandfailure,inthelongterm.
BetweenJune,2007andDecember,2012,69patientsunderwentToFrepairinourInstitution.In39ofthem,balloonvalvedilatationandPVpreservationwasattempted.Itwassuccessfulin34.Thistechniqueincludes:1 PVcommissurotomy2 RVOTmusclebundlesresectionuptothePV
annulus3 TranstricuspidPVballoondilatation4 VSDpatchclosure5 PVreconstruction
Inhospitalandfollow-upresultswerecomparedtoasimilargroupof30patientswhounderwent“classicrepair”bymeansofatransannularpatch,duringthesameperiod.
Ourresultsshowthatwiththenewdilatationtechnique,PVcompetenceandRVfunctionarebetterpreserved,atdischargeandatthefollow-up.
WeconcludethatPVintegrityandfunctioncanbepreserved,inselectedpatients,duringearlyToFrepair,byconcomitantPVballoondilatationandPVreconstruction,leadingtoanimprovedRVfunction,inthemid-term.
Balloon dilatation right ventricular outflow tract in Fallots repair
Giovanni Stellin
Professional Development
10:00 Session 1: Teach the Teacher
Room 1
Moderators: G. Kitchingman, London; P. Newman, London
10:00 Introductions:Whoyouare;Yourteachingexperience;Whatyouwanttogainfromtheday
10:30 Learningstylesandteaching:Learningstyles;Overcomingbarrierstolearning
11:30 TheTeachingProcess:Whylearningobjectivesareimportant;Designingyoursessiontoengageyourlearners;Textureofcontent;Deliveringforoptimalimpact;Yourplatformskills;Measuringyourteachingeffectiveness?validation
12:15 Teachingtechniques:Afocusedstructure:‘KIM’;Gaininglearnerinteractioningroups;Usingquestions;Theeighttrainerbehaviours
14:00 Session 2: Teach the Teacher
Room 1
Moderators: G. Kitchingman, London; P. Newman, London
14:00 Whathaveyoulearned?Shortobservedtrainingsessionsandfeedback;Actionsforpersonaldevelopement
Thoracic
10:30 Session 1: Interactive Session on the Management of Challenging Mediastinal Cases
Room I
Moderator: F Melfi, Pisa; P.E. van Schil, Edegem
Illustrative cases will be presented by each speaker and discussed in an interactive way10:30 Cliff K C Choong
10:50 Jens Rückert
11:10 Pala Rajesh
11:30 Alan Sihoe
12:30 Session 2: Challenging infectious diseases
Room I
Moderators: D. Subotic, Belgrade; M. Lucchi, Pisa
12:30 Complextuberculosiscases Piotr Yablonskii
12:50 Fromaneasy-to-treattuberculosistoanightmare Alan Sihoe
13:10 Lunghydatidosis Dragan Subotic
13:30 Decendingnecrotisingmediastinitisfromodontogenicinfectiontoperitonitis Dejan Stojakov
14:00 Session 3: Controversies in sympathetic surgery
Room I
Moderator: E. Belcher, Oxford; D Mathisen, Boston
Illustrative cases will be presented by each speaker and discussed in an interactive way14:00 Gaetano Rocco
14:20 Jan Coveliers
14:40 Peter B Licht
15:15 Session 4: Major complications after thoracic surgery
Room I
Moderators: P.B. Rajesh, Birmingham; D. Mathisen, Boston
15:15 AmericanExperience(MajorAirway) Douglas Mathisen
15:30 EuropeanExperience(MajorAirwayandLung) Philippe Dartevelle
15:45 UnitedKingdomExperience(Pleura,ChestwallandBronchus) Maninder Kalkat
16:00 AustralianExperience(Airways,LungandMediastinum) Cliff K C Choong
Congenital
10:30 Session 1: Double outlet right ventricle
Room F2
Moderators: R. Jonas, Washington; B. Maruszewski, Warsaw
10:30 Morphologyofdoubleoutletrightventricle Andrew Cook
10:50 Classificationanddecisionmaking Damien Bonnet
11:10 Novel3Dimagingofdoubleoutletrightventricle Andrew Taylor
11:30 Methodsofsurgicalrepair Emile Bacha
11:50 WhatarethelimitsofBiventricularrepair Francois Lacour-Gayet
12:10 Long-termoutcomeandreoperation Virginie Lambert
Continued from page 4
Continued on page 8
S. Salzberg Heart Clinic Zurich, Klinik Hirslanden, Zurich, Switzerland
M. Emmert University Hospital Zurich, Switzerland
Surgicalrevascularizationremainsthetreatmentof choice for complex 3-vessel coronary
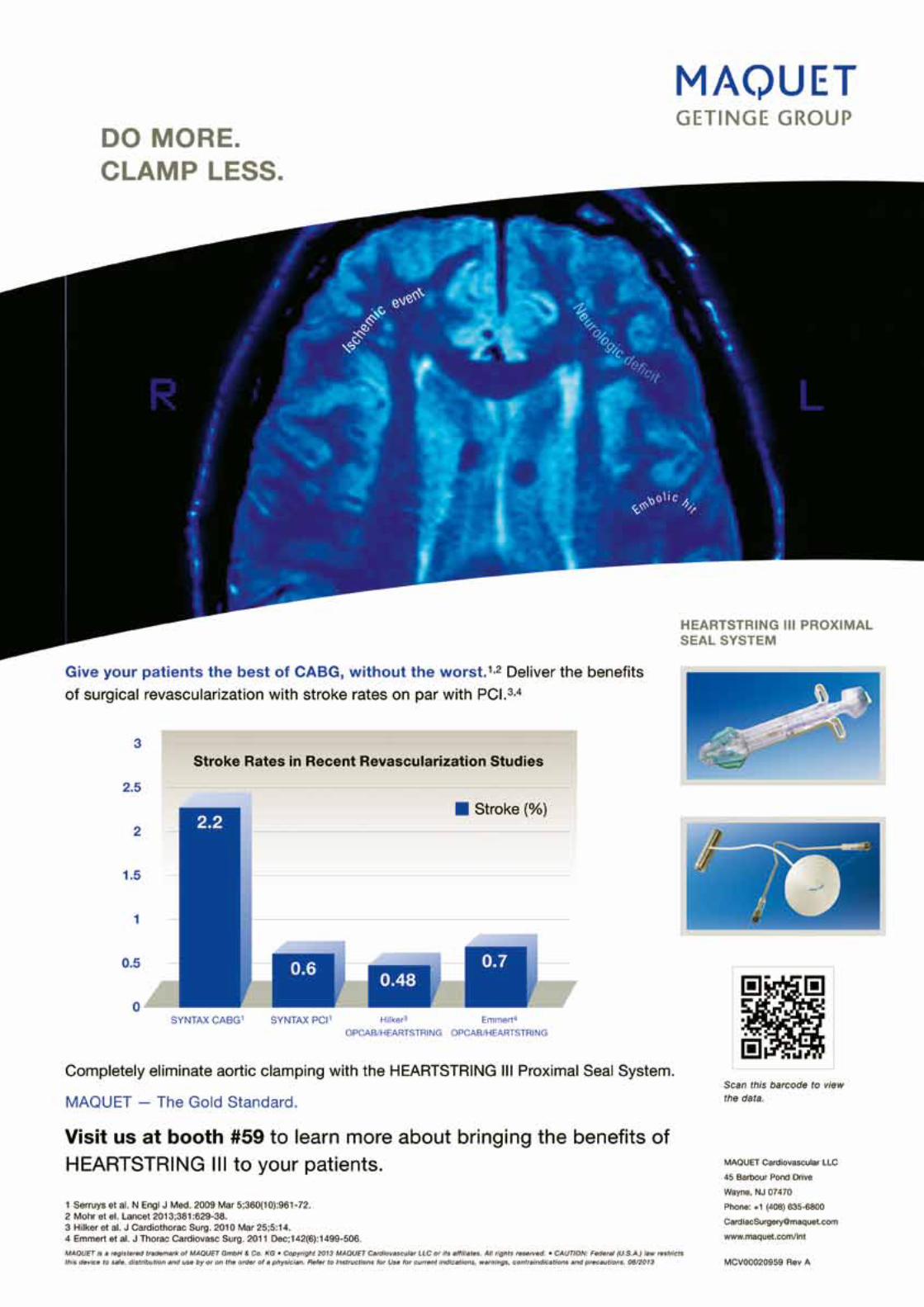
disease,leftmaincoronaryarteryinvolvementordiabetesmellitus.However,coronaryarterybypassgrafting (CABG) is limitedbyconcernabout thehigher stroke rate compared with PCI. Reportsof inferior neurological outcomes for CABG vs.PCIhaveprimarilyresultedfromstudiesinwhichconventional on-pump CABG techniques wereused,ratherthanoff-pumptechniqueswithaorticno-touchstrategies.
A growing body of evidence supportsclampless off-pump approaches to surgical
revascularization inordertominimizeneurologicinjury. By eliminating manipulation and aorticcross-clamping required for cardiopulmonarybypass,off-pumpcoronaryarterybypass(OPCAB)results in a lower incidence of stroke comparedto conventional CABG, particularly whenperformed in combinationwith complete in-situgrafting(doubleinternalmammaryarteryand/orT-orY-Grafting).Whileoff-pumpinsitugraftinghas been proposed as the ‘standard of care’ toreduce neurological complications, it may notbe applicable in everypatient. Inmany cases toachieve complete revascularization the use offreegrafts (arterialorvenous)requiringproximalanastomosis is necessary. In these situations,proximal anastomosis can be done without apartial clampbyusing theHEARTSTRINGdevice(MAQUET,SanJose,CA,UnitedStates).
In a propensity-matched analysis of 4314patients undergoing surgical revascularization atthe University Hospital Zurich, stroke incidencewassignificantly lowerwhenHEARTSTRINGwasused to perform proximal anastomoses during
OPCAB rather than the partial camp. Of note,thestrokeratefortheHEARTSTRINGgroupwascomparable to that of patients who underwentcompletelyno-touchinsitugrafting.(Figure1)
The use of the HEARTSTRING device can besafely implemented into routine clinical practicewithlittlelearningcurveandsignificantlyminimizesthe occurrence of stroke and other neurologicalcomplications compared with partial- or sidebite clamping. The combination of OPCAB andclamplessstrategieseitherusingcompleteinsitugraftingtechniquesorclamplessdevicessuchasHEARTSTRING for proximal anastomosis reducesstroke to levels comparable to PCI, representingasignificantadvanceoverconventionalon-pumpCABG.(Figure2)
Whileaorticcrossclamping(A)duringstandardon-pumpCABGaswellaspartialclampingusinga side-bite clamp during OPCAB (B) are wellestablishedasimportantriskfactorsforstroke,aclamplesstechniqueforproximalanastomosis(C)applyingtheHEARTSTRINGdeviceisaneffectivetoolforstrokereduction.
Only by these means can surgeons achievestroke rates similar or even lower than for PCI,henceendingthedebateaboutearlyneurologicaloutcomesafterCABG.References
1 Emmert MY, Seifert B, Wilhelm M, Grünenfelder J, Falk V, Salzberg SP. Aortic no-touch
technique makes the difference in off-pump coronary artery bypass grafting. J Thorac
Cardiovasc Surg. 2011 Dec;142(6):1499-506.
2 Emmert MY, Salzberg SP, Seifert B, Scherman J, Plass A, Starck CT, Theusinger O, Hoerstrup
SP, Grünenfelder J, Jacobs S, Falk V. Clampless off-pump surgery reduces stroke in patients
with left main disease. Int J Cardiol. 2012 Jun 21. [Epub ahead of print].
cABG comes with comparable stroke to PcI if the aorta is not clamped
Figure 1 – Stroke Rate by Operative Procedure in 4314 CABG Patients Figure 2 – Alternative Approaches to Proximal Anastomosis

8 Sunday 6 October 2013 EACTS Daily News
Session 1: Proximal thoracic aortic disease – variations on a theme 10:30 Room E1
Adriana C. Gittenberger-de Groot Leiden University Medical Center, Leiden, the Netherlands
Duringcardiovasculardevelopmentinthehumanembryotheheartstartstobeatataboutthreeweeksofdevelopment.Atthattimepointtheheart,linedby
endocardium,isconnectedtothebodyoftheembryoatthevenouspolewherebloodofthesinusvenosusenterstheheartandatthearterialpolewherethebloodispumpedintoanaorticsacwhichisconnectedtoasystemofpharyngealoraorticarcharteries.Initiallythesearteriesaresolelylinedbyendothelium,whichiscontinuouswiththeendocardium.Toaddstrengthtothevascularwall,sothatitcanmanagehaemodynamicflowandpressure(althoughextremelylowintheembryo),smoothmusclecells(SMCs)arerecruitedtothevesselwall.
TheseSMCshaveaheterogeneousmesodermaloriginthatvariesalongthelengthoftheaorta.Duetospecificaorticpathologyinthevarioussegmentsitisofinteresttoinvestigatethesecontributionsandifpossibletheirspecificmorphogeneticbackground.Itisknownthatbesidesacontributionfromthesplanchnicmesoderm(currentlyreferredtoasanteriorsecondheartfield)neuralcrestcellsplayanimportantrolebesidesincontributingSMCs,alsoinseptationoftheaorticsacintoanascendingaorta
andapulmonarytrunk.Ahithertoneglectedsourcefortheintrapericardialpartoftheaortaarethearterialepicardiumderivedcells(EPDCs).Allthreecelltypesarenotonlyrelevantfortheformationofthemediaofthegreatarteriesbutalsoplayaroleintheformationofthemyocardialoutflowtract,outflowtractseptationandtheformationofthesemilunarvalvesfromtheendocardialoutflowtractcushions.
Studyofthehistopathologyofaneurysmformation(ordilation)oftheascendingaortashowsthattheaorticwallisintrinsicallydifferentinpatientswithatricuspidvalve(TAV)orabicuspidvalve(BAV)whichmightreflectadifferenceincontributionaswellas(epi)geneticdisturbanceinoneormoresmoothcellcomponents.IngeneralthedilatedaorticwallinTAVshowsmoresignsofinflammationandageing,whereastheBAVaorticwallhasanimmaturephenotype.
Thelatterisalreadyobviousinthenon-dilatedaorticwall.Aspecificdifferenceinproteinexpressionpatternsseemstosupportadifferenceinasusceptibleandanon-susceptibleBAVaorticwallfordilation.Followingtheseobservationsthereisalsoacaseforspecificpathologyoftheaorticarch(includingcoarctationoftheaorta)anddescendingaorta.ImplicationsforthetimingandchoiceofthesurgicalapproachinaorticreconstructivesurgeryandRossprocedureswillbeshortlyeludedto.
TheworkisperformedinamultidisciplinaryandmulticentreresearchgroupconsistingoftheDepartmentofAnatomyandEmbryology(ProfessorMarcoDeRuiter,MoniqueJongbloed),DeptartmentofCellBiology(ProfessorMarieJoseGoumans),DeptartmentofSurgery(JanLindeman),Cardiology(ProfessorAdrianaGittenberger-deGroot)andThoracicSurgery(NimratGrewal,ProfessorRobertKlautz,MeindertPalmen)allfromtheLeidenUniversityMedicalCentre(LUMC),theDeptartmentofThoracicSurgery(ProfessorAdBogers)ErasmusUniversityRotterdam,theNetherlandsandfurthermoretheDeptartmentofThoracicSurgery(ProfessorHansSievers,SalahMohamed)fromtheUniversitatsklinikumSchleswig-Holstein,Germany.
Proximal thoracic aortic disease-variations on a themeembryology of the aorta – from cells to an organ
Adriana Gittenberger-de Groot
Session 3: Complex surgery 15:30 Room F2
M.G.Hazekamp Leiden University Medical Center, the Netherlands
A videoisshownwhereinasix-week-oldinfantwithaorticarchinterruptiontypeB-2,malalignmentVSD(IAA-
VSD)andLVOTobstructionundergoesrepairoftheseanomaliesbymeansofaRoss-Konnoprocedureandrepairoftheaorticarch.
AorticarchinterruptionwithVSDisknowntobeassociatedtoobstructionoftheLVOT.However,inthemajorityofcasesLVOTobstructionbecomessignificantatalaterstageandtypically,aorticarchrepairandVSDclosureissufficientasafirstprocedure.WhenLVOTobstructionoccurslaterandafterinitialrepairofIAA-VSD,theRoss-
Konnoprocedureprovidesagoodsolution,especiallywhentheaorticvalvecannolongerbepreservedand/ortheLVOTshowstunnel-likenarrowing.
Inourpatienttheaorticvalveannulardiameterwasnomorethan3,4mm’satabodyweightof4,300gram(Z-score:–4)whichimplicatedthatsimplearchrepairandVSDclosurewouldbeinsufficient.BiventricularrepaircouldonlybeobtainedbyeitherRoss-KonnowitharchrepairorbyaYasuiprocedurewhereNorwoodandRastellitechniquesarecombined.Eachofthesetechniqueshasitsadvantagesanddisadvantages:thedisadvantagesoftheRoss-KonnobeingpossiblelatedilatationofthepulmonaryautograftandahighertechnicalcomplexitywhileanextracardiacRVtopulmonaryartery
conduitisapotentialdisadvantageoftheYasuioperation1,2.
Withanexperienceofnowover30Ross-Konnoproceduresthisapproachwasdecidedfor:afterremovalofaorticandpulmonaryrootstheoutletseptumwasresected,resultinginawideopenLVOT.WhenharvestingthepulmonaryautograftpartoftheanteriorwalloftheRVhadremainedattachedandwasusedtoclosetheVSDwhileatthesametimeaugmentingtheLVOT.A14mmbovinejugularveingraft(Contegra,MedtronicInc.,Minnesota,USA)wasusedasanorthotopicRVtoPAconduit.Withtheuseofaxenopericardialpatchanewaorticarchwascreatedadaptingitsproximalparttothewiderpulmonaryautograft.FiveyearslaterthepatientremainsingoodconditionwithawideopenLVOT,noinsufficiencyofthe
pulmonaryautograftandanunalteredRVtoPAconduit.References
1 Management options in neonates and infants with critical left ven-
tricular outflow tract obstruction. Alsoufi B, Karamlou T, McCrindle BW,
Caldarone CA. Eur J Cardiothorac Surg. 2007; 31:1013-21.
2 Ross and Yasui operations for complex biventricular repair in infants
with critical left ventricular outflow tract obstruction. Hickey EJ, Yeh T Jr,
Jacobs JP, Caldarone CA, Tchervenkov CI, McCrindle BW, Lacour-Gayet
F, Pizarro C. Eur J Cardiothorac Surg. 2010; 37: 279-88
Ross-Konno operation with concomitant aortic arch repair
M.G.Hazekamp
Marte Bliksøen and Marte Guro Valen University of Oslo, Norway
T heinnateimmunesystemmaynotdistinguishbetweenselfandnon-
self,butratherreactupondanger.Wehavepatternrecognitionreceptorsinourimmunecellsandalsoinnon-professionalimmunecellssuchascardiomyocyteswhichmayreactupondanger.Onewell-knowntypeofpatternrecognitionreceptorsarethetoll-likereceptorfamily.Patternrecognitionreceptorsrecognizemolecularpatternsonbacteriaandviruses,andprobablyalsoendogenousfragmentsofinjuredcells.Toll-likereceptors2and4arewellcharacterizedascontributorstowardsinjury
inacutemyocardialischemiaandheartfailuredevelopment.Toll-likereceptor9islesswellcharacterizedintheheart.ItisknowntorecognizebacterialDNA.Toll-likereceptorssignalthroughthetranscriptionfactornuclearfactorkappaB1.
Mitochondriaareevolutionaryendosymbiotsofbacteria,andcontaintheir
ownDNAwhichissimilartobacterialDNA.WewonderedifmitochondrialDNAinjuredbymyocardialischemiacouldactasadangersignalandevokeanimmuneresponsethroughtoll-likereceptor9signaling.Incardiactissue,wefoundthatmitochondrialDNAisinjuredbyischemia.Itleaksintothecirculationinhumanswith
acutemyocardialinfarctionundergoingrevascularizationwithPCI,andfromisolatedmouseheartswithinducedischemia2.Thecardiomyocyteexpressestoll-likereceptor9.ThecardiomyocytetakesupmitochondrialDNAfragmentsandinternalizesthem.CardiomyocytesstimulatedwithmitochondrialDNAhaveanincreasedcelldeath,signalingthroughtoll-likereceptor9andnuclearfactorkappaB.Themechanismofdeathmaybethroughalteredmitochondrialmembranepotential.
Wearecurrentlyexploringifcardioplegicarrestandreperfusionduringopenheartsurgery(CABG)leadstoleakageofmitochondrialDNAintothecoronarycirculation.Pilotstudiesindicatethatthisisthe
case.Furthermore,pilotstudiesindicatethatmitochondrialDNArepairenzymesareactivatedbycardioplegiaandreperfusioninleftventricularbiopsies,wheretoll-likereceptor9isupregulated.MitochondrialDNAleakingintothecirculationafteropenheartproceduresmaypotentiallycontributetothewhole-bodyinflammatoryresponseseenaftermajorsurgery.InhibitionofmitochondrialDNAmaypotentiallyalleviatepostoperativeinflammation.References
1 Valen G, Yan Z-Q, Hansson GK. Nuclear Factor kappa-B
and the heart. Journal of American College of Cardiology
2001;38;307-314.
2 Bliksøen M, Mariero LH,Ohm I, Haugen F, Yndestad A,
Solheim S, Seljeflot I, Ranheim T, Aukrust P, Valen G, Vinge
LE. Mitochondrial DNA released into the circulation during
myocardial infarction may be immunogenic. Int J Cardiol
2012;158:132-134.
Mitochondrial DNA: a danger signal in the heart?
Guro Valen
Session 1: The enemy from within 10:30 Hall P
13:30 Session 2: Rheumatic and congenital mitral valve disease
Room F2
Moderators: C. Brizard, Melbourne; J.V. Comas, Madrid
13:30 Morphologyofrheumaticandcongenitalmitralvalvedisease Andrew Cook
13:45 Surgeryforcongenitalmitralvalvestenosis Pedro Del Nido
14:00 Surgeryforcongenitalmitralvalveregurgitation Emre Belli
14:15 Surgeryforrheumaticmitralvalvedisease Kirsten Finucane
14:30 Whatcanwelearnfromtheadultmitralvalvesurgeons? Robert Dion
15:30 Session 3: Complex surgery
Room F2
Moderators: E Bacha, New York; O Ghez, London
15:30 Ross-Konnowitharchrepair Mark Hazekamp
15:40 Doubleoutletrightventriclewithnon-committedventricularseptaldefect Emre Belli
15:50 NikaidoProcedure Viktor Hraska
16:00 TheSenningProcedure David Barron
16:10 Aorticrootrestorationwithasub-aorticring Domenico Mazzitelli
16:20 BalloondilatationrightventricularoutflowtractinFallotsrepair Giovanni Stellin
Vascular Disease Domain
10:30 Session 1: Proximal thoracic aortic disease – variations on a theme
Room E1
Moderators: M. Borger, Leipzig; M. Grabenwöger, Vienna
10:30 Embryologyoftheaorta–fromcellstoanorgan Adriana Gittenberger-de Groot
10:45 Updateonvalveandaorticguidelines Ruggero De Paulis
11:00 Bicuspidaorticvalveinaorticdissection Christian D. Etz
11:15 Aorticvalvediseaseinconnectivetissuedisorders Duke Cameron
11:30 TheRossoperation–why,who,howandhownotto Alain Prat
13:00 Session 2: EACTS/STS aortic – Part I: Circulation management, temperature and neuroprotection
Room E1
Moderators: J.E. Bavaria, Philadelphia; J. Bachet, Paris
13:00 Temperaturemanagementandneuroprotectioninaorticsurgery?TheEuropeanperspective Thierry Carrel
13:15 Visceralprotectionduringsurgeryofthethoracicaorta:thesafetyofmoderatehypothermia Davide Pacini
13:30 Selectiveantegradecerebralperfusionwithdifferentbloodflowrates:aretheredifferencesincerebraltissueoxygenationandmeancerebralbloodflowvelocity? Reto Basciani
13:45 Temperaturemanagementandneuroprotectioninaorticsurgery–theAmericanperspective Edward Chen
14:00 Anewindicatorofpostoperativedelayedawakeningaftertotalaorticarchreplacement Tomonori Shirasaka
14:15 Aorticarchsurgeryforoctogenarians:Isitjustified? Hiroshi Kurazumi
15:00 Session 3: EACTS/STS aortic – Part II: Circulation management, temperature and neuroprotection
Room E1
Moderators: J Coselli, Houston; C Mestres, Barcelona
15:00 Unilateralvs.bilateralperfusionforcerebralprotection–theneedforaprospectiverandomizedtrial Paul Urbanski
15:15 Differentialselectivehypothermicintercostalarteryperfusion:anewmethodforconfirmingspinalcordperfusionduringthoracoabdominalaorticaneurysmrepair Yoshikatsu Saiki
15:30 CurrentpracticeofneuroprotectioninEurope–TheEACTSsurveyinEurope Ruggero De Paulis
15:45 Embolismisemergingasamajorcauseofspinalcordinjuryafterdescendingandthoracoabdominalaorticrepairwithacontemporaryapproach Hiroshi Tanaka
16:00 CurrentpracticeofneuroprotectioninJapan–TheEACTSsurveyinJapan Yukata Okita
16:15 Finalremarksandclose
Continued from page 6
Marte Bliksøen
Mitochondrial DNA: a danger signal in the heart?

10 Sunday 6 October 2013 EACTS Daily News
Klaus T Preissner Justus-Liebig-University, Giessen, Germany
Duringacutemyocardialinfarction,cardiomyocytedeathoccursandhasapredominantimpactonthequalityoflifeandsurvivalofpatientssufferingfrom
coronaryarterydisease,themosteminentsinglecauseofdeathinindustrializedcountries.Duetotheocclusionofcoronaryvesselsbyarterioscleroticplaquematerial,largelydecreasedoxygensupply(termedischemia)ofthemyocardiumdeterminesthediseaseoutcome.Despitereopening/reperfusionofstenosedvessels,amajororgandamageremains.Theinitialmechanistictriggersofthismyocardial“ischemia/reperfusion(I/R)injury”remaingreatlyunexplained.Wehaveuncoveredandcharacterizedhypoxia/ischemia-drivenmechanismsthatarethebasisforthepathogeneticphenomenaofI/Rinjuryintheheart.
Basedonpreviouslyreporteddatafromourgroup,extracellularRNA(eRNA,derivedduringvascularinjury,celldeathetc.)servesasanimmediatealarmsignalofstressedordamagedtissue,therebypromotingthrombosis,inflammationoroedemaunderpathologicalconditions.Hereweshowthatfactorsfromthedamagedcardiactissueitself,inparticulareRNAandtumor-necrosis-factor-a(TNF-a),maydictateI/Rinjury.Followingmyocardialischemia/reperfusion(I/R)inmiceorI/RinducedintheisolatedLangendorffratheart,increasedeRNAlevelswerefoundtogetherwithcardiacinjurymarkers.Likewise,eRNAwasreleasedfromcardiomyocytesunderhypoxiaandsubsequentlyinducedTNF-aliberationbyactivationofTNF-aconvertingenzyme(TACE)andprovokedcardiomyocytedeath.Conversely,TNF-apromotedeRNAreleaseespeciallyunderhypoxia,feedingaviciouscelldamagingcycleduringI/R.AdministrationofRNase1orTAPI(TACE-inhibitor)preventedcelldeathandmyocardialinfarction.Likewise,RNase1
significantlyreducedI/R-mediatedenergyexhaustion,openingofmitochondrialpermeabilitytransitionporesaswellasoxidativedamageincardiomyocytes.Finally,adramaticincreaseofendogenousvascularRNase1inhumansubjectswasachievedbyinducingnon-invasiveintermittentlimbI/Rusinganexternaloccluder,therebyprovingtheimpactoftheeRNA/RNasesysteminremoteischemicpreconditioning.
Basedontheaccumulationofinvitroandin vivofindings,non-toxic,thermostableRNase1orTAPI(inhibitorofTACE/ADAM17)mayoffernovelandsafetreatmentstopreventtissueandorgandamage,asshownherefortheheart.Theuncoveredfundamentalpatho-mechanismsarelikelyoperativeinotherorgansandtissuesaswell,suchthattheproposedinterventionshavemajorimpactfortheapplicationofnoveltherapeuticregimeninmedicine.AlthoughendothelialcellsasamajorsourceofvascularRNase1doproduceandsecretethenucleaseintothebloodstream,itsnormalconcentrationisinsufficienttocombattheacutelife-threateningsituationofI/Rinjury.However,initialclinicalstudiesrevealedadramaticincreaseofendogenousvascularRNase1inhumansubjectsbyinducingnon-invasiveintermittentlimbI/Rusinganexternaloccluder.
Damaging nature of endogenous RNA in cardiac ischemia/reperfusion injury
Session 1: The enemy from within 11:10 Hall P
Klaus Preissner
Session 2: EACTS/STS aortic session: Part I 13:00 Room E1
Davide Pacini Department of Cardiac Surgery, S.Orsola-Malpighi Hospital, University of Bologna, Bologna, Italy.
Antegradeselectivecerebralperfusion(ASCP)providesexcellentprotectionofthebrainduringaorticarchsurgery1-5and
differentstrategiesarecurrentlyinusebasedonindividualsurgicalexperience6-10.Althoughtheidealdegreesofsystemichypothermiaandtheoptimalflowrateofcerebralperfusionarenotfullyestablished,moderatesystemichypothermiaappearstobeasafeandreliabletoolforbrainprotection11,12.
However,theissueofdistalorganprotectionwiththistechniqueremainstobeclarified.TheaimofthestudywastoretrospectivelyevaluatetheoutcomeofaorticarchsurgeryusingASCPatdifferentsystemictemperaturesinordertoassesstheeffectivenessofthemoderatehypothermia(26°Cofnasopharyngealtemperature)invisceralorganprotection.Forthisreasonweincludedpatientswhounderwentelectivethoracicaortarepair;andexcludedpatientswhohadearlypost-operativelowcardiacoutputsyndromebecausethisconditionaffectsvisceralorganfunction.
Threehundredandfourpatientswere
enrolledinthestudyanddividedintotwogroupsbasedondegreeofsystemichypothermiaduringHCA:GroupAwithnasopharyngealtemperaturemaintainedat25°Corlower(194patients)andGroupBwithnasopharyngealtemperaturehigherthan25°C(110patients).
Theoverallin-hospitalmortalitywas4.6%(14patients)withoutsignificantdifferencebetweengroups.Therewerealsonodifferencesintheincidenceof
postoperativecomplications.Creatinine,aspartateaminotransferase
(AST),alanineaminotransferase(ALT)andbilirubin,wereexaminedpreoperativelyandpostoperativelyasbiochemicalmarkersofvisceraldysfunction.Renaldysfunctionwasdefinedbyapostoperativeserumcreatininelevelofatleast2.0mg/dloranincreaseincreatininetotwicethebaselinelevel.Liverdysfunctionwasdefinedasapostoperativebilirubinlevelgreaterthan2.5mg/dloranincreaseofASTandALTvaluesgreaterthantwicethebaselinelevel.
Twenty-fivepatients(8.2%)hadisolatepostoperativerenaldysfunctionandforty-one(13.5%)hadassociatedrenalandliverdysfunctionwithoutsignificantdifferencesinincidencebetweenthetwogroups.Isolatedliverdysfunctionoccurredin69patients(22.7%).TheincidencewashigheringroupA(25.8%)thaningroupB(17.3%);however,thedifferencedidnotreachstatisticalsignificance.
Atmultivariateanalysis,CPBtimelongerthan180minuteswastheonlyindependentriskfactorofrenalandhepato-renaldysfunction(OR=2.16;CI1.21-3.86;P=0.010),andtemperaturewasnotfoundtobeariskfactor.Instead,atemperature>25Cwasshowntobeanindependentprotectivefactorforliver
dysfunction(Figure1).Thissuggeststhereductionofreperfusionorganinjuriesinwarmertemperatures,especiallywhensurgicalproceduresarecompletedwithinatimeperiodofvisceralcirculatoryarrestnotexceeding60minutes13.
Inconclusion,moderatesystemichypothermiaatanasopharyngealtemperature>25°Chasbeendemonstratedtobenolesseffectivethanlowerhypothermiclevelsinvisceralorganprotection.Moreover,moderatehypothermiaat26°Cshouldbepreferred
forperiodsofvisceralischemialessthan60minutesbecauseitmayreducereperfusionorganinjury.References
1. Bachet J, Guilmet D, Goudot B, Dreyfus GD, Delentdecker P, Brodaty D, Dubois C: Antegrade cerebral perfusion with cold blood: a 13-year experience. Ann Thorac Surg 1999, 67(6):1874-1878; discussion 1891-1874.2. Griepp RB: Cerebral protection during aortic arch surgery. J Thorac Cardio-vasc Surg 2001, 121(3):425-427.3. Kazui T, Yamashita K, Washiyama N, Terada H, Bashar AH, Suzuki K, Suzuki T: Aortic arch replacement using selective cerebral perfusion. Ann Thorac Surg 2007, 83(2):S796-798; discussion S824-731.4. Harrington DK, Walker AS, Kaukuntla H, Bracewell RM, Clutton-Brock TH, Faroqui M, Pagano D, Bonser RS: Selective antegrade cerebral perfusion at-tenuates brain metabolic deficit in aortic arch surgery: a prospective random-ized trial. Circulation 2004, 110(11 Suppl 1):II231-236.5. Pacini D, Di Marco L, Leone A, Tonon C, Pettinato C, Fonti C, Manners DN, Di Bartolomeo R: Cerebral functions and metabolism after antegrade selec-tive cerebral perfusion in aortic arch surgery. Eur J Cardiothorac Surg 2010, 37(6):1322-1331.6. Di Bartolomeo R, Pacini D, Di Eusanio M, Pierangeli A: Antegrade selective cerebral perfusion during operations on the thoracic aorta: our experience. Ann Thorac Surg 2000, 70(1):10-15; discussion 15-16.7. Urbanski PP, Lenos A, Bougioukakis P, Neophytou I, Zacher M, Diegeler A: Mild-to-moderate hypothermia in aortic arch surgery using circulatory arrest: a change of paradigm? Eur J Cardiothorac Surg 2012, 41(1):185-191.8. Spielvogel D, Etz CD, Silovitz D, Lansman SL, Griepp RB: Aortic arch re-placement with a trifurcated graft. Ann Thorac Surg 2007, 83(2):S791-795; discussion S824-731.9. Misfeld M, Leontyev S, Borger MA, Gindensperger O, Lehmann S, Legare JF, Mohr FW: What is the best strategy for brain protection in patients undergoing aortic arch surgery? A single center experience of 636 patients. Ann Thorac Surg 2012, 93(5):1502-1508.10. Zierer A, Detho F, Dzemali O, Aybek T, Moritz A, Bakhtiary F: Antegrade cerebral perfusion with mild hypothermia for aortic arch replacement: sin-gle-center experience in 245 consecutive patients. Ann Thorac Surg 2011, 91(6):1868-1873.11. Pacini D, Leone A, Di Marco L, Marsilli D, Sobaih F, Turci S, Masieri V, Di Bartolomeo R: Antegrade selective cerebral perfusion in thoracic aorta surgery: safety of moderate hypothermia. Eur J Cardiothorac Surg 2007, 31(4):618-622.12. Khaladj N, Peterss S, Oetjen P, von Wasielewski R, Hauschild G, Karck M, Haverich A, Hagl C: Hypothermic circulatory arrest with moderate, deep or pro-found hypothermic selective antegrade cerebral perfusion: which temperature provides best brain protection? Eur J Cardiothorac Surg 2006, 30(3):492-498. 13. Qing M, Vazquez-Jimenez JF, Klosterhalfen B et al. Influence of tempera-ture during cardiopulmonary bypass on leukocyte activation, cytokine balance, and post-operative organ damage. Shock 2001; 15:372-377.
Visceral organ protection in aortic arch surgery: safety of moderate hypothermia
Davide Pacini
Figure 1: Multivariate analysis
NeW smartcanulas® for MIcS and ecMOBy Prof. Ludwig K. von Segesser Cardio-Vascular Research, CHUV, Lausanne, Switzerland
The original idea for the developmentof the smartcanula® was to build a
peripheral vascular access device providingfull flow with gravity drainage alone.The consecutively developed “collapsedinsertion and expansion in situ” principleresulted in temporary caval stenting withshape-memorymaterials(Fig.1),andprovedto be most promising for superior venousdrainageduringcentralandremoteaccessCPB for standard and minimally invasivecardiac surgery, complex cardio-thoracicprocedures,andECMO.Fiftypercenthigherflowsandcompletecardiacunloading(Fig.2)canbeachievedwiththeself-expandingsmartcanula® S although introducedthroughperipheralveins.Lateron,itturnedout that smaller smartcanulas® compatiblewithcentrifugalpumpsorvacuumprovidealso superiorperformanceas compared to
traditionalpercutaneouscannulas:The MICS smartcanula® ST is designed
forperipheralcannulationofthecavalaxiswithpercutaneous techniquesandcanbeused in combination with a centrifugalpump or vacuum for augmentation. TheMICS smartcanula® ST comes in 24F, and20F configurationswith several lengths. ItisCE-markedforroutineuseup-to6hours.
The ECMO smartcanula® STC isdesigned forperipheral cannulationof thecavalaxiswithpercutaneoustechniquesandcanbeconnecteddirectlytoan integratedpump-oxygenator structure. The ECMOsmartcanula® STC comes in 24F, and 20Fconfigurationswithseverallengths.ItisCE-markedforlongertermuseup-to28days.
The original smartcanula® S designedfor gravity drainage can also be used incombination with the smart dilator set(8F-24F)whereasthesyntheticsmartcanula®Pismadeforroutineusewithcentralaccess.Forbetterflow,checkout:
www.smartcanula.com
Fig. 1: The smartcanula® is built from shape-memory materials and changes its configuration once inserted into a vessel:
superior performance results!

12 Sunday 6 October 2013 EACTS Daily News
Jo Cook John Radcliffe Hospital, Oxford, UK
AsaResearchNursecurrentlyworkingontheArterial
RevascularisationTrial(ART),followinguppatientsfor10yearspostcardiacsurgery;Ihaveidentifiedseveralinterestingtrendsthroughthetelephoneconversations,withpatients,aspartoftheirfollow-up:nPatient’snon-adherencetomedicationand
treatmentpostdischargefollowingCABGnVariationinGP’smonitoringof
cardiovascularrisknImplicationsforresearchIhaveusedthedatafromourcohortof427patients,recruitedattheJohnRadcliffehospitalinOxfordandhavechosentolookataspirinandstatinmedicationandGPsurgeryvisits
nTheArterialRevascularisationTrial(ART)isaUniversityofOxford,multi-centre,international,randomisedcontroltrial;fundedbyboththeMRCandBHF.
nProfessorDPTaggartistheprincipleinvestigatorforARTandhasbeenextremelysupportiveandencouragingwiththiswork.
nTheaimofARTistoevaluatewhethertheuseofbothIMA’sduringCABGimprovessurvivalandreducestheincidenceofrecurrentchestpainand/ortheneedforfurtherintervention,comparedtousingoneIMA.
n3,102patientswererecruitedin28centresandsevencountries.
nPatientswererandomisedtoeitherSIMA(SingleIMA)orBIMA(BilateralIMA)andondischargearefollowedupbytelephoneandpostyearlyfor10years.
nTheprimaryoutcomeissurvivalat10years;secondaryendpointsincludeclinicalevents,reinterventionandcost
effectiveness.MypresentationhighlightstheimportanceofsecondarypreventionandbothGPandpatientapproachestothis;datafromourpatientcohort
regardingthereasonsfor‘nottakingmedication’and‘notregularlyseeingtheirGP/practicenurse’.
Ihavealsoidentifiedsomefutureconsiderations,namely,whatpercentageofdataisaffectedbythepatient’snon-adherenceandGP’svaryingadherencetoguidelinesandhowsignificantisthiswhenanalysingcardiacevents,readmissionsandreinterventions.
ItisimportanttonotethatalthoughthefigurespresentedshowahighcompliancewithbothmedicationandGPsurgeryvisits,forthepurposesofthispaperandcertainlyfromanursingperspective,IamfocusingonthepercentageofpatientsNOTadheringandexaminingthereasonsbehindthiswhichmayhaveimplicationsforbothresearchandnursingpractice.Thisisacommentarypaperonlyaimedtoraisesomeinterestingpointsfordiscussion.
The patient, the GP, the primary care team: their relationship, adherence to treatment and the implications for research
Figure 1
Nicolas M Van Mieghem Thoraxcenter, ErasmusMC, Rotterdam, The Netherlands
ItonlytookonedecadefortheTranscatheterAorticValveImplantation(TAVI)technologytosurgetoanestablishedtreatmentstrategyforapotentiallyvastgroupofpatientswithsymptomaticaorticvalvestenosis.Afteragradualbuild-upbymeansofcasereportsand
single-centrecohortstudies,largenationalandinternationalregistriespavedthewaybydemonstratingproceduralsafetyandshort-termefficacy.TherandomizedPlacementofAorticTranscatheterValves(PARTNER)trialcreatedtheevidentrationalfundamentsfortheEuropeanSocietyofCardiology(ESC)andEuropeanAssociationofCardio-ThoracicSurgery(EACTS)toformulateastrongrecommendationforTAVIinpatientswithsymptomaticsevereASwhoaredeemedinoperableandidentifyTAVIasalternativetosurgicalvalvereplacementiftheoperativeriskisconsideredtobehigh.Absolutelyfundamentaltotheserecommendationsisthe
installmentofatruemulti-disciplinaryheartteamconsistingofacoreminimumofinterventionalcardiologistsandcardiacsurgeonsandideallycompletedbycardiacimagingspecialistsand(cardiac)anesthesiologists.AsaninterventionalcardiologistIthereforeshouldconsidermyselfanalliedprofessionaltomycardiacsurgerycolleagues.Butbordersarefading.TransfemoralTAVIproceduresareconsideredthestrategyoffirstchoiceinmostcentersandcanbeperformedbybothcardiologistsandsurgeons.InErasmusMedicalcenter–asintheHeliosCenterinHamburg-alsothetransaxillaryapproachhasbeenexecutedincompletepercutaneousfashionusingpercutaneoussuturebasedclosuredevices.Inallhonesty,we,inErasmusMC,haveabandonedthispercutaneousapproach;theaxillaryarterydidnotseemappropriateforthesekindsofsuturebasedclosuredevicesanddefinitelyprovedinferiortoasurgicalcut-downandcontrolledaccess.
Maybefuturedevelopmentsindedicatedclosuredevicesforlargearteriotomiesprovemorereliable.Thatbeingsaidinthetransapicalscene,
interestingnewclosuredevicesseemtoworkandmayconverttransapicalTAVIintoacompletelypercutaneoustechnique.Itmayevenrejuvenatethetransapicalaccessoption,makingitmoreaccessibletocardiologistsandimportantlylesspainfultopatients.
Onadifferentnote,three-dimensionalimagingmaycontributesignificantlytobetterTAVIoutcomebydemonstratingreductionsintheincidenceofmoderatetosevereparavalvularaorticregurgitationandevenimprovingsurvival.ClearlythestagehasbeensettoexploretheefficacyandsafetyofTAVIinpatientswithaloweroperativerisk.Howtodetermineapatient’sriskisstillamatterofdebate.ClearlytheestablishedriskmodelsliketheSocietyofThoracicSurgeons(STS)scoreorthe(logistic)EuropeanSystemforCardiacOperativeRiskEvaluation(EuroSCORE)comeshortinrisk-estimatingoctogenarianswithascalaofco-morbidities.Still,thecurrentlyongoingorrecentlycompletedSURgicalreplacementandTranscatheterAorticValveImplantation(SURTAVI)andPARTNERIIhavebeenrelyingontheSTSscoreof4toidentifyapatientashavingatleastintermediateoperativerisk.TheuseofanSTSscoreforriskstratifyingpotentialTAVIcandidatesmaybeaflawasitignoresrelativelycommonriskvariablessuchasfrailty,hostilechestandporcelainaorta.Regardless,ifPARTNERIIandSURTAVIconfirmthenon-inferiorityofTAVItoSAVRthenextimportantmissinglinkwillbethedurabilityofTHV.ThefollowingyearswillcertainlyzoominonthispieceoftheTAVIpuzzle.
The transcatheter aortic valve implantation debate The view from the allied professionals
Session 1: Moving Borders 08:45 Hall K
Session 1: Moving Borders 08:45 Hall K
Session 2: Moving Borders 11:15 Hall K
David Lizotte Rockingham Memorial Hosptial, Harrisonburg, VA, USA
Inthemid-1960s,physiciansandacademicsintheUnitedStatesrealizedtherewasashortageofprimarycarephysicians.EugeneA.SteadJr.,MD,oftheDukeUniversityMedicalCenter,puttogether
thefirstclassofPhysicianAssistants(PA)in1965,basingthecurriculumofthisfirst-of-its-kindprogramonhisknowledgeofthefast-tracktrainingofdoctorsduringWorldWarII.Inkeepingwiththistheme,heselectedNavycorpsmenwhohadreceivedconsiderablemedicaltrainingduringtheirmilitaryserviceasmembersofhisfirstclass.ThefirstPAclassgraduatedfromtheDukeUniversityPAprogramonOct.6,1967.ThePAconceptgainedacceptanceandbackingbytheUSgovernmentasearlyasthe1970sforitwasseenasacreativesolutiontophysicianshortages.Thephysiciancommunityhelpedsupporttheprofessionandfacilitatedthedevelopmentofaccreditation
standards,establishinganationalcertificationandstandardizedexamination,anddevelopingcontinuingmedicaleducationrequirements.
JohnWebsterKirklin,MD,awellknowcardiothoracicsurgeon,foundedthefirstformaleducationalprogramtotrainsurgicalphysicianassistants.Dr.Kirklinandhiswife,Dr.MargaretKirklin,theprogram’sfirstAcademicDirector,startedtheUniversityofAlabamaatBirmingham’sSurgeonAssistanttrainingprogramin1967.ThefocusoftheprogramwasinspiredbyDrKirklin’spositionasaleaderincardiacsurgeryandprovidedanemphasisoncardiacsurgicaltraining.ThisenabledmanyPAstoenterthespecialtyofcardiothoracicsurgeryintheUnitedStates.Overthecourseofthenext46years,PAsbecameanintegralpartofthecardiothoracicsurgicalteam.Wearefirstassistantsinallcardiothoracicsurgeriesfromthesimplestmediastinoscopiestothemostcomplexaorticsurgeriesandtransplantation.Wehavebeenpartnersinthe
developmentandimplementationofnewandexcitingtechnologiesthatdirectlybenefitcardiothoracicsurgerypatients,themostnotablebeingendoscopicvesselharvesting.Weperforminvasiveproceduresindependentlysuchaschesttubeplacement,centralandarteriallineplacement,thoracentesis,Swan-GanzplacementandIABPplacement.WeareactiveparticipantsinthecareofthecardiothoracicsurgicalpatientinallarenasincludingtheICUandstepdownfloorswheretheyoftenfunctionashouseofficers.PAservicesarebillabletoinsuranceandPAsareabletoprescribemedicationsinall50states.
AswefaceagrowingphysicianshortageintheUnitedStatesforourspecialty,ourservicesareevermoreindemand.Weareproudofourhistoryandanticipatewithgreatexcitementourfuture.Inatimeofneedphysicianswithgreatvisioncreatedapathforthedevelopmentofourprofessionthatremainsgroundedintheteamapproach.Aswefaceournext50yearsasaprofession,wearepoisedtoplayanevengreaterandexpandingroleinhealthcaredeliveryintheUnitedStates.
The American perspective
David Lizotte
European Quality Improvement Programme
T heNursing&AlliedHealthProfessionsgroupisoneofthesixgroupssupportedbytheEACTSQualityImprovementProgramme,toimproveoutcomesforpatientsacrossEurope.ThegroupischairedbyTaraBartley(Birmingham,UK)andaimsto
createaframeworkfordeliveringhighqualitynursingcareacrossEurope.Thegrouparecurrentlyworkingwithnursingandalliedhealth
professionalteamstodefinepracticesthatarealreadyinplacetodeliverqualitycaretopatients,andtoidentifykeyareasforimprovingcarefor
patients.Colleagueshavebeenaskedtoprovidedetailsofanycurrentdepartmentalprotocolsthatareinplacetodeliverqualitystandardcare,andtosuggestareaswherequalityimprovementinitiativescouldimproveoutcomesforpatients.Anonlinesurveyhasalsobeendevelopedtoseekpractitionerperspectiveonqualityissuesinrelationtopatientoutcomes(www.eacts.org/quip/outcomes-survey).Colleaguesfromnursing,surgicalcarepractitioners,physicianassistants,pharmacists,physiotherapistsandmembersofthemultidisciplinaryteamareencouragedtoparticipate,asthesurveywillprovidevaluableinformationfortheproject.
AnupdateontheEuropeanQualityImprovementProgrammewillbegivenaspartoftoday’sPostgraduateEducationsession:Nurse,NursePractitionersandPhysicianAssistantsProgramme.Amemberofthe
qualityimprovementteamwillalsobeavailableattheEACTSexhibitionstand(HallXL,Booth148)atthefollowingtimestoanswerquestions:nSunday6October: 17:00–19:00nMonday7October: 09:00–10:00
13:00–14:00 15:45–16:30
nTuesday8October: 09:00–10:00 13:00–15:15
JenavalveAdvert
14 Sunday 6 October 2013 EACTS Daily News
Charlotte Brun Thorup Aalborg University Hospital
Aftertheimplementationofsupportiveprecautionsforpatients,followingsternotomyincardiacsurgery,aneedfor
knowledgeaboutthepatients’experiencesaroseAliteraturereviewrevealedthatnostudiesexistedwhichfocusedonthepatients’experiences,livingwithprecautionsaftercardiacsurgery.Aim:Toexplore.
Aftermidlinesternotomypatientsare
instructedonactivityprecautionstoavoidsternalwoundcomplications.InDepartmentofCardiothoracicSurgery,CenterforCardiovascularResearch.AalborgUniversityHospital,wedidquestionhowrestrictivethoseprecautionsshouldbe,sincetheymightleadtoadecreaseinqualityoflifeinthepostoperativeperiod.Aliteraturereview(CINAHL,PubMed,CochraneLibraryandPedro)weremaderesultinginthefollowingprecautions:navoidstretchingbotharmsbackwardsat
thesametimefor10days
nloadedactivityshouldbedonewiththeelbowsclosetothebody
nonlymovearmswithinpainfreerangenuselegrollingwithcounterweighting
whengettinginandoutofbednprotectsternumwhencoughingby
crossingthearmsina“selfhugging”posture
nusesupportivesternalvestwhencoughingconstantlyorwhenBMI≥35,and
nusesupportivebrawhenbreastcup≥D.Wefoundnoevidencetosupportweightlimitationregardingactivity,aslongastheupperarmsarekeptclosetothebody,andactivitywithinpain-freerange.Coughisconsideredthemostimportantsinglemechanicalstressfactorcausinginstability.
Afterimplementingtheseprecautions
weperformedastudyonhowpatientsexperiencelivingwiththeseprecautionsaftercardiacsurgery.Thestudyconsistedofsemi-structuredinterviewswithpatientssixtoeightweeksaftercardiacsurgery.Patients’experienceswereexpressedinthefollowingthemes.“Logicalorbodilyexperiencedmeaningoftheprecautions”,“Cognitiveorphysicalcomprehensionoftheprecautions”and“difficultyinmanagingtheprecautions”.Alltogether,thepatientsexperienceddifficultieswithmanagingtheprecautionsinthepostoperativeperiod,butstilltheyusedtheprecautionsasguidelines.Theyweremotivatedbythepromiseofapositiveachievement,oravoidanceofnegativeresults.Thepatientsalsosuggestedamoreindividualfocus.
Postoperative mobilisation after sternotomy
Bart Meyns University Hospital Leuven, Leuven, Belgium
Forambulatorychronicheartfailure
patientsrefractorytomedicationandwhoarenotappropriatecandidatesfor,orhavefailed,cardiacresynchronization,therearefewoptionsavailable.LVADsareintendedforthesickestpatients,butduetotheinvasivenessofthesurgery,oftenarenotconsideredforelderlypatientswhomayalsobefrail.
ArecentanalysisfromtheINTERMACSdatarevealedthatolderage(definedas
>70years)isanindependentpredictorofmortalityduringfollow-upafterLVADimplantation.Nonetheless,midtermsurvivalintheoldercohortwasstillreasonable(63%attwoyears)1.
Withthisinmind,theconceptofalessinvasivesupportoptionisattractiveforthefrailelderlypatient.
TheSYNERGYCirculatorySupportSystemissuchadevice.Asamicro-bloodpump–approximatelythesizeandweightofaAAbattery–theSYNERGYSystempumpsupto4.25L/minofbloodandreducestheheart’sworkload,improvingbloodflowtovitalorgans.Thesystemissurgicallyimplantedusingamini-thoracotomy,withthemicro-pumpplacedinapacemaker-likepocket.Itisdesigned
totreatambulatorychronicheartfailurepatientsclassifiedasINTERMACS4-6(i.e.non-inotropedependent).
WerevieweddatafromtheCEMarkEuropeantrialoftheSYNERGYSystem,andcomparedoutcomesforpatients≥70yearsandthose<70years,in54patientsoverafive-yearenrollmentperiod2.
Themaindifferencebetweengroupswasthebaselinetherapy;theolderpatientshadagreatertendencytobetreatedwithallpossibledevicetherapiespriortoconsideringcirculatorysupport.Additionally,itwasobservedthattheyoungerpatientsdemonstratedashorterlengthofsupport(averagedurationof188days)inabridgetotransplantscenarioasopposedtoolderpatients(averagedurationof337days),
wherecirculatorysupportwasmostcertainlyviewedasdestinationtherapy.
Thedatashowthatolderandyoungerpatientsexperiencesimilarimprovementsinhemodynamics(pulmonarycapillarywedgepressure-9±16vs-10±8mmHg;CO+1.0±0.7vs0.9±1.0l/min;PVR-1.2±1.5vs0.8±1.7Wood)andfunctionalstatus,includingsimilaraverageimprovementinthesix-minutewalktest(107±120vs130±121m).Theoveralladverseeventratewascomparable,althougholderpatients,asobservedinpreviousanalyses,hadasomewhathigherrateofbleeding.Infectionsrelatedtothedeviceordrivelinealsowerelimitedintheoldercohorttoaratecomparabletotheyoungerpopulation.Despiterenalfunctionbeingcompromised
intheolderpatients,thisdidnotresultinahigherrateofacutefailurepost-operativelyorinthelongrunofchronicsupport.
Theseoutcomesshowusthatminimally-invasivecirculatorysupport,benefitsyoungerandolderpatientsequallywell,andiswell-suitedasbothanearlyinterventionandanefficacioustreatmentforfrailambulatorychronicheartfailurepatients.References
1 Atluri P, Goldstone A, Kobrin D, Cohen J, MacArthur J, Howard J, Jessup
M, Rame E, Acker M, Woo J. Ventricular assist device implant in the elderly is
associated with increased, but respectable risk: a multi-institutional study. Ann
Thorac Surg 2013;96:141-147.
2 Barbone A, Pini D, Rega F, Ornaghi D, Vitali E, Meyns B. Circulatory support
in elderly chronic heart failure patients using the Circulite Synergy system. Eur
J Cardiothorac Surg 2013;44:207-212.
Long-term assist with LVAD in elderly patients
John Mulholland Hammersmith Hospital, Imperial College Health Science Centre, London, UK
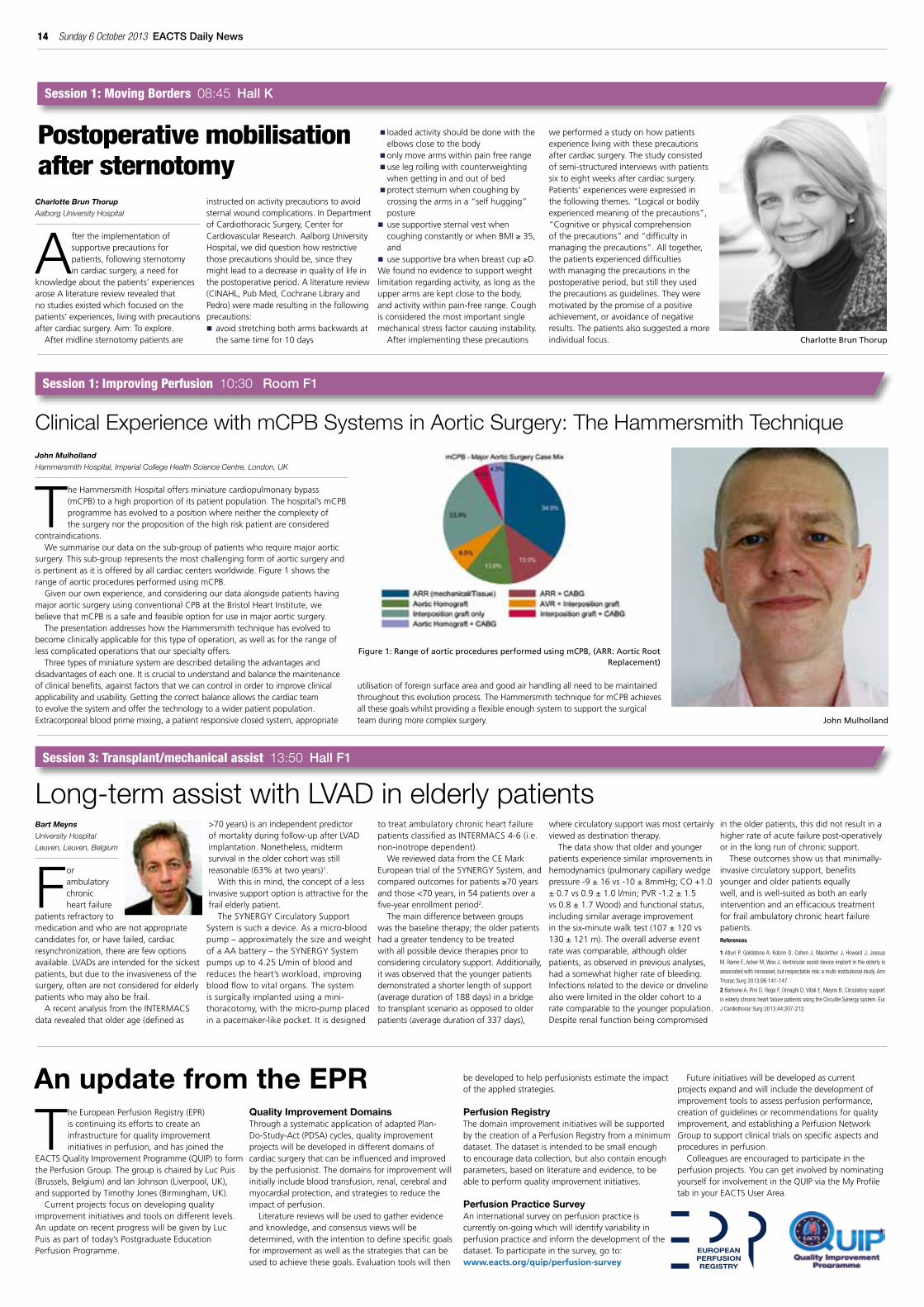
TheHammersmithHospitaloffersminiaturecardiopulmonarybypass(mCPB)toahighproportionofitspatientpopulation.Thehospital’smCPBprogrammehasevolvedtoapositionwhereneitherthecomplexityofthesurgerynorthepropositionofthehighriskpatientareconsidered
contraindications.Wesummariseourdataonthesub-groupofpatientswhorequiremajoraortic
surgery.Thissub-grouprepresentsthemostchallengingformofaorticsurgeryandispertinentasitisofferedbyallcardiaccentersworldwide.Figure1showstherangeofaorticproceduresperformedusingmCPB.
Givenourownexperience,andconsideringourdataalongsidepatientshavingmajoraorticsurgeryusingconventionalCPBattheBristolHeartInstitute,webelievethatmCPBisasafeandfeasibleoptionforuseinmajoraorticsurgery.
ThepresentationaddresseshowtheHammersmithtechniquehasevolvedtobecomeclinicallyapplicableforthistypeofoperation,aswellasfortherangeoflesscomplicatedoperationsthatourspecialtyoffers.
Threetypesofminiaturesystemaredescribeddetailingtheadvantagesanddisadvantagesofeachone.Itiscrucialtounderstandandbalancethemaintenanceofclinicalbenefits,againstfactorsthatwecancontrolinordertoimproveclinicalapplicabilityandusability.Gettingthecorrectbalanceallowsthecardiacteamtoevolvethesystemandofferthetechnologytoawiderpatientpopulation.Extracorporealbloodprimemixing,apatientresponsiveclosedsystem,appropriate
utilisationofforeignsurfaceareaandgoodairhandlingallneedtobemaintainedthroughoutthisevolutionprocess.TheHammersmithtechniqueformCPBachievesallthesegoalswhilstprovidingaflexibleenoughsystemtosupportthesurgicalteamduringmorecomplexsurgery.
clinical experience with mcPB Systems in Aortic Surgery: The Hammersmith Technique
John Mulholland
Figure 1: Range of aortic procedures performed using mCPB, (ARR: Aortic Root Replacement)
Session 1: Moving Borders 08:45 Hall K
Charlotte Brun Thorup
Session 3: Transplant/mechanical assist 13:50 Hall F1
Session 1: Improving Perfusion 10:30 Room F1
TheEuropeanPerfusionRegistry(EPR)iscontinuingitseffortstocreateaninfrastructureforqualityimprovementinitiativesinperfusion,andhasjoinedthe
EACTSQualityImprovementProgramme(QUIP)toformthePerfusionGroup.ThegroupischairedbyLucPuis(Brussels,Belgium)andIanJohnson(Liverpool,UK),andsupportedbyTimothyJones(Birmingham,UK).
Currentprojectsfocusondevelopingqualityimprovementinitiativesandtoolsondifferentlevels.AnupdateonrecentprogresswillbegivenbyLucPuisaspartoftoday’sPostgraduateEducationPerfusionProgramme.
Quality Improvement DomainsThroughasystematicapplicationofadaptedPlan-Do-Study-Act(PDSA)cycles,qualityimprovementprojectswillbedevelopedindifferentdomainsofcardiacsurgerythatcanbeinfluencedandimprovedbytheperfusionist.Thedomainsforimprovementwillinitiallyincludebloodtransfusion,renal,cerebralandmyocardialprotection,andstrategiestoreducetheimpactofperfusion.
Literaturereviewswillbeusedtogatherevidenceandknowledge,andconsensusviewswillbedetermined,withtheintentiontodefinespecificgoalsforimprovementaswellasthestrategiesthatcanbeusedtoachievethesegoals.Evaluationtoolswillthen
bedevelopedtohelpperfusionistsestimatetheimpactoftheappliedstrategies.
Perfusion Registry ThedomainimprovementinitiativeswillbesupportedbythecreationofaPerfusionRegistryfromaminimumdataset.Thedatasetisintendedtobesmallenoughtoencouragedatacollection,butalsocontainenoughparameters,basedonliteratureandevidence,tobeabletoperformqualityimprovementinitiatives.
Perfusion Practice SurveyAninternationalsurveyonperfusionpracticeiscurrentlyon-goingwhichwillidentifyvariabilityinperfusionpracticeandinformthedevelopmentofthedataset.Toparticipateinthesurvey,goto:www.eacts.org/quip/perfusion-survey
Futureinitiativeswillbedevelopedascurrentprojectsexpandandwillincludethedevelopmentofimprovementtoolstoassessperfusionperformance,creationofguidelinesorrecommendationsforqualityimprovement,andestablishingaPerfusionNetworkGrouptosupportclinicaltrialsonspecificaspectsandproceduresinperfusion.
Colleaguesareencouragedtoparticipateintheperfusionprojects.YoucangetinvolvedbynominatingyourselfforinvolvementintheQUIPviatheMyProfiletabinyourEACTSUserArea.
An update from the EPR

EACTS Daily News Sunday 6 October 2013 15
Virginie Lambert Centre Chirurgical Marie Lannelongue, Le Plessis Robinson, France
Double-outletrightventricle(DORV)includesawidespectrumofanatomicsubtypesrequiringavarietyofsurgicalapproachesforrepair.Themostcomplexformsremain
asurgicalchallengeintermsofoperativetechniquesandregardingthechoiceofthesurgicalprocedure.
Indeed,thewisdomofextendingbiventricularrepairtoborderlineanatomiccandidateswithhypoplasticleft-sidedstructuresoranon-subaorticventricularseptaldefectisstillquestioned.Someauthorspromotesingle-ventriclerepairsincesomebiventricularrepair,especiallyRastelli-typereconstruction,isassociatedwithhigherlatemortalityandreinterventionthaninFontanrepair.Bycontrast,othersarguethat,althoughtheFontanoperationhaveledtoimprovedearlyandmidtermresults,the
functionalstateofpatientsfollowingtheFontanoperationdeteriorateswithtime,andpushtheindicationsofbiventricularrepairasfaraspossible.
However,moststudiesshowedanimprovementinlong-termoutcomesforpatientswithDORVandafavourableinfluenceofcontemporaryeraextendedtoeventhosepatientswithcomplexforms.Latemortalityislowwithanoverall10-and15-yearsurvivalof80-90%reportedinthelargestseries.Arrhythmiashavebeenrecognizedasacauseforlatedeathswithincreasingsurgicalage,postoperativeventriculararrhythmiasandcompleteheartblockassignificantriskfactors.
Moreover,mortalityandmorbidityareassociatedwithanyreoperationwhetherexpected(eg,rightventricle-pulmonaryarteryconduitchange)orunplanned.Theneedforreoperationafterrepairremainsanimportantchallengesincerisksanalysispredictthatathirdofpatientswillundergo
reinterventionwithin15yearsfromrepair.Themajorityofreinterventionsweredirectedatreliefofrightventricleoutflowtractobstruction,butresidualorrecurrentleftventricleoutflowtractobstructionisalsodocumentedin13-15%ofpatients.Patientswithsubaorticventricularseptaldefectsareatlowestriskforreoperationatcontrarytothosewithnon-committedventricularseptaldefect.
Inthelatter,amongthemostsevere,theprogressivelydevelopingsubaorticstenosisisamajorconcern,involving26%ofthem.Inthesecases,thereoperationshouldnotonlyaimtorelievetheobstruction,butalsotostreamlinetheleftventricleoutflowpathwayusinganextendedseptoplasty,anadaptedtechniquetotreatthiscomplicationwithgoodresults.FunctionalstatusremainspromisinginserieswiththebigmajorityofpatientsinNewYorkHeartAssociationclassIorIIwithoutanymedicaltreatmentatlastcontrol.
Double outlet right ventricle: long-term outcome and reoperations
SorinGroupispleasedtoannouncetheEuropeanlaunchofSoloSmart,abiologicalaorticpericardialheartvalve.
Solo Smart is the evolution of the SorinFreedomSolo valvewhichhasbeenon themarket since 2004. Designed to maximizehemodynamic performance and ease ofimplantation,SoloSmartbehavesjustlikeahealthynativevalve restoringthequalityoflifeofpatients.
Solo Smart features a temporarystent that gives support and facilitatesimplantation.Thetemporarystentmaintainsvalve geometry and symmetry within theaortic root to simplify implant procedureand suturing. Once the valve is suturedto the aortic root, the temporary stent isremovedleavingthestentlessvalveinplace.Solo Smart provides all the benefits of anative-like valve, now with a stented-likeimplantability.
Solo Smart was designed to mimic thenative aortic valve and preserve the aorticroot physiology to maximize hemodynamicperformance. This unique bioprosthesisis a totally biological heart valve withno synthetic material and it is implantedin supra-annular position which allowsthe alignment of the valve orifice to thepatient annulus. It ensures a physiologicalblood flow through the annulus providingexcellent hemodynamics in terms of EOAandmeanandpeakgradientswhichremainstableover the follow-upperiod.This leadsto a remarkable clinical improvement aswellastosignificant leftventricularreverseremodeling with a fast left ventricularrestoration.
SorinGroup isveryproudofthecomingintroduction of Solo Smart valve to themarket,anuniquetechnologythatprovidesan excellent alternative to physiciansmanaging the care of patients with aorticvalve disease. The introduction of SoloSmartisanimportantmilestoneforSorinasitcontinuesthelegacyofprovidingsurgeonswithmarket-leadingheartvalveoptions.
Forfurtherinformation,pleasevisittheSorinGroupbooth#114.
Sorin Group Solo Smart Tissue Heart Valve: Introducing New Treatment Options
Session 1: Double outlet right ventricle 10:30 Room F2
16 Sunday 6 October 2013 EACTS Daily News
Sarah Longnus, Hendrik Tevaearai, Thierry Carrel University Clinic for Cardiovascular Surgery, Inselspital, Berne University Hospital and University of Berne, Switzerland
Althoughthenumberofpatientswithindicationstocardiactransplantationhasconsistentlyincreasedoverthelastdecade,
donororganavailabilityhasremainedstable,resultinginachronicshortageofcardiacgrafts1.InEUcountriesattheendoftheyear2010,3,290patientswereregisteredonwaitinglistsforhearttransplantation2.Inthefollowingyear,atotalof2,024hearttransplantswereperformedand412patientsdiedwhileawaitingcardiactransplantation1,indicatingawaitinglistmortalityofapproximately12%peryear.
Onestrategyforincreasingcardiacgraftavailabilityistouseorgansobtainedwithdonationafterdeclarationofcirculatorydeath(DCDD),inadditiontothose
obtainedwithconventionaldonationafterbraindeath.WithDCDD,increasesindonorsupplyareexpectedtoincreasebyapproximately17%foradults3and42%forpediatricpatients4.Furthermore,recentreportsoftransplantationandex vivoresuscitationofDCDDheartsattesttothefeasibilityofthisapproach.However,giventheexquisitesensitivityofthehearttoinjuryfollowingwarmischemia,useofDCDDcardiacgraftsrequiresparticularconsideration.
Oneoftheseveralfocusesofourresearch(www.cardiovascular-research.ch)isaimedatidentifyingclinicallyapplicableapproachesthati)limitcardiacinjuryfollowingwarmischemiaandreperfusion,andii)enableearlyevaluationofDCDDcardiacgraftsfortransplantsuitability.Inthiscontext,wehaveachievedkeymilestonesthatsupportourvisionofDCDD-basedcardiactransplantationbecoming,oneday,areality:1.Clinicallyapplicablemeansofprolonging
thetoleranceofheartstowarmischemia
provideagreaterwindowofopportunityfortheapplicationofadditionalprotectivemeasuresanduseofDCDDcardiacgrafts.Wehavedemonstratedthatslightlyreducingmyocardialtemperaturedramaticallyincreasesthisperiodofischemictolerance(40minutesforalocaltemperatureof32°C,versus20minutesat37°C)5.
2.Clinicallyapplicablemeansthatpreventthedevelopmentofreperfusioninjuryenableimprovedpost-ischemichemodynamicrecovery.Wealsoreportthatmechanical-postconditioning–inducedmechanisms,appliedtonormothermichearts(37°C)placedunderglobal(noflow)ischemiaformorethan25minutes,permitdramaticincreasesinfunctionalrecoveryrates(manuscriptinpreparation).
3.Clinicallyapplicablemeanstoevaluategraftsatthetimeofprocurementreliablyandreproduciblypredictfunctionalrecoveryaftertransplantation.Alistofbiochemicalandhemodynamic
parametershasbeenidentifiedthat,whenmeasured5–10minutesafterprocurementofischemichearts,enablespredictionsubsequentpost-ischemicrecovery6,7.
TheuseofDCDDgraftsisanattractiveandrealisticapproachtowardsovercomingthedonororganshortageandhasrecentlymotivatedthedevelopmentofseveralclinicalprotocolsforprocurementoforgansotherthantheheart.DeterminingthepreciseinterventionsthatwouldguaranteeoptimalcontractilefunctionoftransplantedDCDDheartsiscertainlyachallenge.Nevertheless,basedon
laboratoryexperienceandencouragedbyrecentclinicalresults,wefeelconfidentthatcardiactransplantationwillsoonrelyonasignificantpercentageofDCDDorgans.References
1. Council of Europe, Ed: R. Matesanz. (2012) Newsletter Transplant. in Inter-national Figures on Donation and Transplantation – 20112. Council of Europe, Ed: R. Matesanz. (2011) Newsletter Transplant. in Inter-national Figures on Donation and Transplantation – 2010 3. Osaki S, Anderson JE, Johnson MR, Edwards NM and Kohmoto T. (2010) Eur J Cardiothorac Surg 37: 74-79
4. Koogler T and Costarino AT Jr. (1998) Pediatrics 101: 1049-1052
5. Stadelmann M, Dornbierer M, Clément D, Gahl B, Dick F, Carrel TP, Tevaearai
HT, Longnus SL. (2013) Transplant Int 26(3):339-48
6. Dornbierer M, Stadelmann M, Sourdon J, Gahl B, Cook S, Carrel TP, Tevaea-
rai HT, Longnus SL. (2012) PLoS One 7(8):e436-42
7. Sourdon J, Dornbierer M, Huber S, Gahl B, Carrel TP, Tevaearai HT, Longnus
SL. (2013) Eur J Cardiothorac Surg 44(1):e87-96
Thierry Carrel, Sarah Longnus, Hendrik Tevaearai
Session 3: Transplant/mechanical assist 13:50 Room F1
Heart transplantation with donation after circulatory declaration of death (DCDD)
Hiroshi Kurazumi Yamaguchi University Graduate School of Medicine, Yamaguchi, Japan
Theprogressanddevelopmentofthemedicaltherapyledtheincreasinglifespanallovertheworld,whichhasresultedina
significantincreaseinthenumberofpeopleagedmorethan80years.Elderlypatientsoftenpresentadditionalco-morbidconditions,andpastreportshaveindicatedthatcardiacsurgeryinelderlypatientsisassociatedwithsignificantoperativemortalityandmorbidity.Cardiovascularsurgeonsoftenhesitatetoperformaorticarchsurgeryonelderlypatients,assumingpoorclinicaloutcomes,becausethoracicaorticsurgeryisthoughttobeamoreinvasiveprocedurerelativetoothertypesofcardiacsurgery.Consequently,elderlypatientsmightbedeniedaorticarchsurgerydespitetheriskofsuddendeathduetotheruptureofaneurysm.
Inthisstudy,weevaluatedearlyclinicaloutcomesofsurgicaltreatmentforaorticarchdisease,mid-termsurvivalandQOLinoctogenarianpatients.49consecutivepatientsolderthan80
yearswhowerereferredtoourinstitutionsenrolledthisstudy.Ofthesepatients,20underwentsurgicalintervention(surgicalgroup)and29weretreatedmedically(medicalgroup).Kaplan-Meiersurvivalanalysiswasperformedbetweentwogroups,andresultswerecomparedwith
age-matchedpopulationdata.TheriskfactorsformortalityweredeterminedbyaCoxregressionanalysis.
Thepatientcharacteristicsatbaselinewerenotsignificantlydifferentbetweenthetwogroups.Inthesurgicalcases,conventionaltotalaorticarchreplacement
wasperformedin15patients,debranchedTEVARintwo,andChimneyTEVARinthree.Emergencyprocedurewasperformedinthreepatients.Nohospitaldeathsoccurredinthesurgicalgroup.Reoperationforbleedingwasobservedintwopatientsandprolongedmechanicalventilationwas
observedinfourpatients.Five-yearsurvivalwas61.5%inthesurgicalgroupand13.6%inthemedicalgroup(p=0.02).Freedomfromaorta-relateddeathatfive-yearwas92.3%inthesurgicalgroupand32.4%inthemedicalgroup(p=0.01).Therewerenodifferencesinthefive-yearsurvivalbetweenpatientsundergoingsurgicalinterventionandthoseintheage-matchedpopulation(p=0.08),whereasthefive-yearsurvivalwassignificantlylowerinpatientswhoreceivedmedicaltherapyrelativetotheage-matchedpopulation(P<0.001).Medicaltherapywasthesoleriskfactorformortality(Oddsratio:3.19,p=0.03).
Theoverallsurvivalwashigherinthesurgicalgroup,aswasthefreedomfromaorta-relateddeath,suggestingthattheavoidanceofaorta-relateddeathduetothesurgicalinterventioncontributestothesuperiorlong-termsurvivalofthesurgicalgroup.Ourdataclearly
indicatethatsurgicaltreatmentforthoracicarchaneurysmreversestheprognosis,eveninoctogenarians.
Inconclusion,surgicalinterventionforaorticarchdiseaseinoctogenarianscanyieldsatisfactoryearlyclinicaloutcomesandacceptablemid-termsurvivalwithadequatedailyactivity.Ourstudyindicatesthatamongoctogenarians,agealoneshouldnotdisqualifyapatientfromreceivinganaorticarchintervention.
Edward Chen Emory University, Atlanta, USA
Aorticarchsurgeriesrepresentcomplexprocedures.Successfuloutcomedependsonawell-plannedandcoordinated
operativestrategytowardcerebralprotection,myocardialprotectionandlowerbodyperfusion.Neurologicinjuryfollowingtheseoperationscanbeduetothromboembolicdiseaseresultinginfocalorpermanentneurologicdeficitsorglobalcerebralischemiaresultinginnonfocalortemporaryneurologicdeficits.Contemporarymethodsofbrainprotectionareaimedatreducingbothtypesofinjury.
Cerebralprotectiontechniquesduringaorticarchsurgeryhavetraditionallyincludeddeephypothermiccirculatoryarrestaloneorincombinationwithretrogradecerebralperfusionandmorerecently,selectiveantegradecerebralperfusion(SACP).Theoptimalstrategyofcerebralprotectioncontinuestobedebatedwithoutstandingresultsbeingreportedwithuseofbothretrogradeandantegradecerebralprotectionfromhighvolumecentersofexcellence.Nonetheless,therehasbeentremendousshiftinthepreferredcirculationmanagementstrategyoverthelast10yearsacrosstheworldandcertainlyintheUnitedStates.
Moderatehypothermiccirculatoryarrestincombinationwithselectiveantegradecerebralperfusionhasrecentlyemergedasanacceptabletechniqueofcirculationmanagementandcerebralprotectionforaorticarchsurgeryrequiringanopendistalanastomosis.Since2004,atourinstitution,althoughwecontinuetousedeephypothermiaandretrogradecerebralperfusionforisolatedspecificclinicalandanatomicsituations,weprimarilyemployatechniqueofmoderatehypothermiccirculatoryarrestusinguSACPviarightaxillaryarterycannulationforthemajorityofarchreconstructioncases.
Inourinstitutionalexperience,we
foundthatselectiveantegradecerebralperfusioncombinedwithmoderatehypothermiccirculatoryarrestresultedinpermanentandtemporaryneurologicdeficitratesof3.2%and4.1%,respectively,forhemiarchreconstruction.Theaveragetemperatureatwhichcirculatoryarrestwasoriginallyinitiatedwas26.5degreesCelsius.Inadditiontodiscussingourresultsinthesettingofelectivesurgery,theresultsofthiscirculationmanagementstrategyinthesettingofemergenttypeAdissectionwillalsobereviewed.Finally,wewillalsopresentourexperiencewhenutilizingthesetechniqueswithmorecomplextotalarchreconstruction.
Aortic arch surgery in octogenarians: Is it justified?
Hiroshi Kurazumi
Edward Chen
Session 2: EACTS/STS aortic session: Circulation management, temperature and neuroprotection 13:00 Room E1
Session 2: EACTS/STS aortic – Part I: Circulation management, temperature and neuroprotection 13:00 Room E1
Temperature management and neuroprotection in aortic surgery – the American perspective

EACTS Daily News Sunday 6 October 2013 17
Session 2: Challenging infectious diseases 12:30 Room I
Alan D L Sihoe The University of Hong Kong, Queen Mary Hospital, Hong Kong SAR, China.
TherearemanyreasonswhyTuberculosis(TB)isnotconsideredamajorconcernbymanythoracicsurgeonsnowadays.ItsprevalenceintheDevelopedWorldhasfallendramatically
sinceitsheydayacenturyago.AndwhenpatientsdopresentwithTB,themainstayofmanagementisoverwhelminglybypharmacotherapy.Onlyrarelyaretherecasesofmulti-drugresistantTBforwhichanti-microbialsareinsufficientandthoracicsurgeonsarecalledupontotreat.
Ontheotherhand,therearealsomanyreasonswhyTBremainsanever-presentpartofthoracicsurgicalpractice.Firstly,itispreciselybecauseoftheeffectivenessofpharmacotherapythatmostTBpatientssurvivetheiracuteinfection–buttheflipsideofthiscoinisthatmorethenliveonwiththesequelaeand
complicationsofTB.Theseincludemanypresentationsforwhichthoracicsurgicalmanagementisrequired:empyema,pneumothorax,airwaystenosis,andsoon.Secondly,theeaseoftravelaroundtheworldmeansthatitwillneverbepossibletocompletelyeliminateTBinanygivenregion,providedcarriersfromTB-prevalentregionscanstillenter.Eveninthe21stCentury,itmaycomeasasurprisetosomethatmanycountrieslistedasendemicforTBarefoundintheDevelopedWorld,andthattheincidenceofTBinsomecountriesintheWestisactuallyrisingratherthanfalling.Clearly,TBwillcontinuetofeatureinthecasemixofthoracicsurgerycentersworldwideformanyyearstocome.
ThemajorityofTB-relatedconditionsrequiringthoracicsurgeryarerelativelybenignandeasy-to-treat.Theoperativetechniquesaresimilartothoseusedforsimilarconditionswithnon-TBetiology.However,thechallengeposedtothoracicsurgeonsliesinthenatureofthemycobacteriumitselfand
theparticularinfluenceithasoninflammationandhealing.Therelativedifficultyineradicatingtheinfection,thegranulomatousreactionandsooncanquicklyturnacaseof‘simple’surgicalmanagementintoaclinicalquagmire.
Inthesession,DrAlanSihoewillbepresentingacasefromHongKongthatillustrateshowTBcantransformeventhemostseeminglystraightforwardmanagementintoadrawn-outmarathonoffrustration.Treatingayoungmanwithapneumothoraxspiralledintomonthsofcomplications–whichthoughnotlife-threateningbecamequality-of-life-damaging.Delegateswillbewelcometodiscussexperiencesandopinionsonthiscase.
Clinical dangers are caused not just by danger, but also frustration
A nightmare with TB begins with a simple chest X -ray
TheE-vitaOPENPLUShybridstentgraftsystemcombines surgical vascular reconstruction
withmodern,minimallyinvasiveaorticstenting.This unique prosthesis simplifies previoustherapeutic techniques which impose a severestrain on the patients with their two-stageprocedureandinvasiveness.ByusingE-vitaOPENPLUS, theoperativeprocedure canbe reducedtoasingleinterventionfromwhichbothpatientandsurgeon,benefitinequalmeasure.
E-vita OPEN PLUS allows the so calledoptimized “Frozen Elephant Trunk Technique”to treat complex lesions of the thoracic aortaduring a single-stage procedure by combiningendovascularstentingofthedescendingthoracicaorta with conventional surgery. After mediansternotomyandundercirculatoryarrestthearchis opened. The E-vita OPEN PLUS stent graftsystemisintroducedinanantegradefashionintothe descending aorta over a previously placedstiff guide wire. By using the proven Squeeze-to-Release deployment mechanism the hybridstentgraft canbedeployed safeandprecisely.Aftersurgicalfixationofthestentgraftportionby a circumferential suture line the infoldedsurgical cuff canbeeasily evertedand suturedtoanothervasculargraftorusedforaorticarchreconstruction.
The E-vitaOPENPLUS stentgraft system isavailableindiametersfrom24to40mmaswellasindifferentlengthsofthesurgicalcuffportion(50, 70mm) and stent graft portion (130mm,150mm and 170mm). The one-piece hybridstentgraftismadeofbloodtightpolyesterandsupported by nitinol springs in the stent graftsection. Thanks to a special weaving processthesurgicalcuffisprimarilybloodtightwithoutanyimpregnationorpre-clotting.Thenewmorecompact delivery system allows easy handlingandprecisepositioningofthestentgraft.
Foundedin2000,JOTEChasbecomefirmlyestablished on the market as a specialist foraortic disease. The product portfolio containsnumerous solutions for life-threateningaortic and peripheral vascular diseases. TheproductionisbasedinGermany,atthecompanyheadquarters inHechingen.Direct salesunitesarelocatedinSwitzerland,Italy,SpainandPolandand an international network of distributorsguaranteeworldwidemarketpresence.
PleasevisittheJOTECboothno.29and30atEACTS2013tolearnmoreabouttheE-vitaOPENPLUSstentgraftsystem.
From an easy-to-treat tuberculosis to nightmare
The Hybrid Stent Graft System e-vita OPeN PLUS
18 Sunday 6 October 2013 EACTS Daily News
Thierry Carrel University Hospital Berne, Switzerland
Themethodsofcerebralprotectionandneuromonitoringofthebrainfunctionduringsurgeryinvolvingtheaorticarchhave
beenconsiderablyrefinedduringthelast15years;thefavourableeffecthasbeenatremendousdecreaseofmortalityandneurologicalmorbidityinexperiencedcenters.However,theoptimalmanagementisstillmatterofdiscussion;therearemainlythreetopicstobediscussed:1.Thelevelofhypothermia2.Thetypeofcerebralperfusion3.ThemethodsofmonitoringHistorically,deephypothermiccirculatoryarresthasbeenthegoldstandardforproceduresontotheaorticarchbutthereareseveralnegativeeffects,forinstanceprolongedperfusiontimeanddisturbancesofthecoagulationsystem.Thisisoneofthemainreasonwhymoderatehypothermiahasmostrecentlygainedincreasingconsideration.Nowadays,asubstantialnumberofsurgicalteams
avoiddeephypothermiaandproceedwithcoretemperaturearound26to30°C,evenifprolongedperiodofcirculatoryarrestarerequired.Insomeinstances,distalperfusionisperformedtoavoidadverseeffectsonthespinalchordandtheabdominalorgans.
Antegradeselectivecerebralperfusionhasbeendemonstratedtoattenuatepostoperativeneurologicalinjury,whichstillremainsthemaincauseofmortalityandmorbidityfollowingsurgicalaorticproceduresincludingtheaorticarch.Protectiveeffectsofhypothermiccerebralperfusionincludeinhibitionofneuronexcitationaswellasdischargeofexcitableamino-acids,andthereby,preventionofanincreaseinintercellularcalciumions,hyperoxidationoflipidsincellmembranes,andfinallyfreeradicalproduction.However,perfusionpressure,flowmanagementaswellastemperatureoftheperfusatearestillunderdiscussionaswellasthetypeofperfusion(throughbothcommoncarotidarterieswithspecialcatheters(bilateral)orusingthearterialinflowcanulaofthecardiopulmonary
bypasscircuit(unilateral)).Mosteffortstodocumenttheuse
andefficacyofretrogradedeliveryofcerebralperfusionforbrainprotectionhavefailed.Infewstudies,advantagesrelatedonlytotheremovalofembolicdebrisfromthebackflowthroughthearterialsystem.
Finallytheoptimaltechniqueofneuromonitoringhasnotbeendefinedyet.Themostcommonmethodsare:EEG,nearinfraredspectroscopy(NIRS),TranscranialdopplerandjugularSO
2assessment.
Onepromisingapproachtoimprovethequalityofneuromonitoringmightbethesocalled“wholeheadmonitoringofcerebraloxygenation“,asusedalreadytodayforneurovascularinterventions.Thesettingincludes16transmitters/receiversand52NIRSchannelswithcontinuouswavetechnologyusingthreewavelengthsof780,805and830nm:thismethodsallowingsimultaneousassessmentofcerebraloxygenationinallbrainsegmentshasbeenvalidatedduringneuro-angiographicprocedures.
Session 2: EACTS/STS aortic session: Circulation management, temperature and neuroprotection 13:00 Room E1
Neuroprotection and neuromonitoring during surgery involving the aortic arch: the European perspective
Figure: a multichannel registration system can increase the sensitivity of
detection of cerebral mal-oxygenation during hypothermia and selective
cerebral perfusion
Dejan Stojakov Clinic for digestive surgery, Clinical center of Serbia, Belgrade, Serbia
Descendingnecrotizingmediastinitis(DNM)islife-threateningdisease,originatingfrominfectioninoralcavityandneck.Fascialplansinneckdivideneckin
severalcompartments,and,desendingdeepintomediastinum,createpathwayforspreadingoddeepneckinfectiontomediastinum.UnusualcaseofDNMtypeIIB(accordingEndo’sclassification),originatingfromodontogenicinfection,withbilateralpleuralempyema,anddiffuseperitonitisduetosubdiaphragmalextensionofmediastinalinfection.InthisreportseveralimportantissuesindiagnosisandtreatmentofDNMaredisscused.
Young(33yearsold),otherwisehealthy,femalepatient,sufferedfromtoothache,swellingandpaininleftsubmandibularregion,andincreasebodytemperature.Aftertwodaysshewasadmittedinregionalhospital,andtreatmentwithwidespectrumantibioticsandtransoralincisionanddrainageofsubmandibularabscessarestarted.Patientconditionwasimproved.Leftparapharyngealabscesswasrevealedbyneckultrasoundaftersevendays,butclinicallytherewerenoobviuossignsofdeepneckinfection,patientwasafebrileandingoodgeneralcondition.Threedayslaterpatientsufferredfromdyspnea,cough,withoutincreaseofbodytemperature,withoutclinicalyevidentsignsofdeepneckinfection.Afteranothertwodaysgeneralconditionofpatientwasrapidlyworsenedand
CPCRprocedurewereappliedaftercardiacarrest.ChestX-raxconfirmedmassivebilateralpleuraleffusions.
Thoracocenthesisconfirmedpusinbothpleuralcavities,andbilateralchesttubewasplacedandbigammountofpusevacuated(left-2,500ml;right-1,500ml).CTscanoftheneck,thoraxandupperabdomenrevealedabscessintheleftparapharyngealspace,gasinleftcarotidsheet,signsofinfectioninallmediastinalcompartments,smallammountofeffusioninbothpleuralcavities,bilaterallunginfiltrates,gasbellowtheleftlobeoftheliverandfluidinomentalbursa.DiagnosisofDNMwithbilateralpleuralempyema,andperitonitiswasestablished,andtheneedforaggressivesurgicaldebridement.
Weperformedagressivesurgicaldebridementusingbilateralanteriorcervicotomy,bilateralsynchronousanterolateralthoracotomy,anduppermedianlaparotomy.Bilaterallungdecorticationwasperformed,debridementofnonviableinfectedneckandmediastinaltissue,cervicomediastinalandabdominallavage,withplacementofmultipleneck,mediastinal/chestandabdominaldrains,tracheostomyandgastrostomy.Postoperativecervicomediastinalirrigationcontinuedfortwoweeks.PatientdevelopedbilateralVAPandwasmechanicalventilationofthelungwasperformedfor26days.Steadyimprovementwasnoticed,andsixfollow-upMDCTscansshowedrecoveryofintrathoracicandabdominalinfection.Patientwasdischargedhomeaftertwomonths.Aftersixmonthsshedevelopedstenosisofdistaltrachea,whichsuccessfullytreated.
Thisillustrativecaseshowsrareclinicalentity,difficultiesinestablishingdiagnosisduringatypicalclinicalpresentationofDNM,possibilityofsubdiaphragmalextensionofmediastinalnecrotizinginfection,andchallengiesinthetreatment.
Descending necrotizing mediastinitis — from odontogenic infection to peritonitis
Session 2: Challenging infectious diseases 12:30 Room I

EACTS Daily News Sunday 6 October 2013 19
Session 2: Imaging in Transcutaneous valve interventions 12:30 Hall D
Jörg Kempfert Keckhoff Clinic Bad Nauheim, Germany
Transcatheteraorticvalveimplantation(TAVI)hasseenarapidevolutionduringthe
lastfewyears.Today,ithastobeconsideredasastandardalternativetotreatelderlyhigh-riskpatientssufferingfromaorticstenosis.Incomparisontosurgicalaorticvalvereplacement(AVR),TAVIchallengestheoperatorwitha‘closedchest’situationnotallowingforanydirectviewontotheoperatingfield.Thus,sophisticatedimagingtoolsarecrucialinordertoobtainthemostoptimaloutcome.
Inregardtopreoperativeplanningmulti-dimensionalaorticannulusmeasurementsiskey
toobtainexactTAVIprosthesissizingwhichiscrucialtoavoidrelevantparavalvularleaks.Typically,thisisperformedbasedonmultislice-CT(MSCT)and2D/3Dtransesophagealechocardiography(TEE).Inaddition,anatomicalsuitabilityofthedesiredaccesshastobeassessedespeciallyincaseofatransvascularapproachtominimizeratesofmajorvascularcomplications.Again,MSCTplaysacrucialroleforthatpurposesupplementedbypotentialangiographyorMRI-scans.
Intraoperatively,“classic”imageguidanceismainlybasedonhigh-qualityfluoroscopytopreciselypositionandimplantthevariousTAVIprosthesesavailabletoday.Inaddition,TEEishelpfulduringtheimplantationitselfandespeciallyforfunctionalassessmentofthevalveperformance.
Overthelastyears,several‘new’imageguidanceoptionshavebeendeveloped.Thesesystemseitherrelyonare-registrationofthepreoperativeMSCTdataset(PhillipsHeartNavigator),utilizeconventionalrootangiographyindifferentplanes(PaieonC-THV)orfacilitateautomaticsegmentationbasedonarotationangiographyspin(SiemensSyngoValveGuide).TheseadvancedimagingconceptshelptofindthemostoptimalC-armangulation,allowfordedicatedoff-lineplanningandofferadditionalreal-timeoverlayguidanceduringpositioningandimplantationoftheTAVIdevices.
Insummary,TAVIoutcomeisclearlylinkedtosophisticatedimaging.AvarietyofdifferentconceptareconstantlydevelopingtoprovideadditionalimagebasedguidanceduringTAVIprocedures.
Example of the Siemens Syngo ValveGuide system: (A) root reconstruction and detection of landmarks including visualization of calcification patterns (B) template planning (C) online overlay
Intraoperative guidance in TAVI procedures
Rafael Sádaba Hospital de Navarra, Pamplona, Spain
P atientswithchronicischemicleftventriculardysfunctionmayhaveasubstantialamountofviable,hibernating
myocardium.Theconceptofhibernationimpliesadownregulationofcontractilefunctionasanadaptationtoareductioninmyocardialbloodflowthatservestomaintainmyocardialintegrityandviabilityduringpersistentischemia
Coronaryrevascularizationinthesepatientsmayresultinimprovementofleftventricularfunction.Onthecontrary,intheabsenceofviability,leftventricularfunctionwillnotimprovefollowingrevascularization.
Thepresenceofmyocardialviabilityisalsorelatedtoprognosis.Patientswithviablemyocardiumwhoundergorevascularizationappeartohavebetterprognosisthanpatientswithviablemyocardiumwhoaretreatedmedically.Reciprocally,patientswithischemicheartdiseasewhoarerevascuralizedandhaveviablemyocardium,appeartohavebetteroutcomesthanthosewithnoviablemyocardium.
Accordingly,assessmentofviabilityisimportantinthetherapeuticdecision-makingprocessofpatientswithchronicischemicleftventriculardysfunction.
Variousnoninvasiveimagingtechniquesareavailableforthedetectionofviablemyocardium,includingnuclearimagingwithpositronemissiontomographyandmagneticresonanceimaging.
Positron emission tomographyPositronemissiontomography(PET)isaradionuclideimagingtechniquethatallowsquantitativeassessmentofregionalmyocardialfunction.Itismainlyusedtoassessviabilityofdissynergicmyocardium,bymeansofcombinedimagesofflow
(commonlywith13NammoniumorRubidium82)andmetabolism(withfluordeoxyglucose).Themismatchpattern,withanincreaseinfluordeoxyglucosemetabolisminhypoperfusedregions,isindicativeofviability.Thematchpattern(adecreaseinflowandmetabolisminthesameareas)isindicativeofnecrosis.
Cardiac magnetic resonanceCardiacmagneticresonance(CMR)isanimportanttoolfortheevaluationofmyocardialviabilityandscarinpatientswithischemicleftventriculardysfunction.Thereareanumberofparameters
whichareusefulInordertoevaluatemyocardialviability.Theseareend-diastolicwallthickness,contrast(gadoliniumbased)perfusion,delayedcontrastenhancementanddobutamineevaluationofcontractilereserve.Myocardialsegmentswithanend-diastolicwallthicknesslessthan5,5mmmostlikelyrepresenttransmuralscarformation,andcontractilefunctionwillnotimproveaftermyocardialrevascularization.Gadoliniumlateenhancementgivesanideaofscartransmurality.Scarringoflessthan
25%ofwallthicknessisagoodindicatorofviability,whereasifitismorethan75%thelikelihoodoffunctionalrecoveryispoor.
Inischemicheartfailure,CMR
hyperenhancementasamarkerofmyocardialscarcloselyagreeswithPETdata.Althoughhyperenhancementcorrelateswithareasofdecreasedflowandmetabolism,itseemstoidentifyscartissuemorefrequentlythanPET.WhileCMRiscontraindicatedinpatientswithmetallicimplants,ithastheadvantagesoflessexpenseandnoradiationoverPET.Therefore,CMRisconsideredapromisingdiagnostictoolfordetectingnonviabletissueinpatientswithadvancedcoronaryarterydisease.
Imaging in coronary artery surgery: Assessment of viability with cardiac magnetic resonance and positron emission tomography
Session 3: Imaging in Coronary Artery Surgery 14:30 Hall D
Assessment of viability is important in the therapeutic decision-making process
of patients with chronic ischemic left ventricular dysfunction.

20 Sunday 6 October 2013 EACTS Daily News
Session 1: Proximal thoracic aortic disease – variations on a theme 10:30 Room E1
Session 2: A look into the future 13:00 Room P
Ruggero De Paulis, Raffaele Scaffa European Hospital, Rome, Italy
Newevidenceiscontinuouslyaccumulatingonriskstratification,diagnosticmethodsandtherapeuticoptionsjustifyingtheneedforanupdateonpracticeguidelines.The
EuropeanSocietyofCardiologypresentedguidelinesformanagementofvalvediseasein2007andupdatedin2012.DuringthesameperiodaseriesofAmericanSocietypublishedtheirguidelinesinthetreatmentofthoracicaorticdiseaseandjustrecently(2013)theSocietyofThoracicSurgeonsreportedcombinedguidelinestooptimalmanagementofaorticvalveandascendingaorta.Asmalldifferenceamongreports
representsanaturalchangeovertimeoraslightlydifferentpractice.
Howaorticvalvediseaseismanagedcontinuestoevolve,withnovelapproachesforbothaorticvalvestenosisandregurgitation.Thereisacompleteconsensusthattheseverityofaorticvalvedisease,whetherstenosisorinsufficiencyneedstobeassessedbyquantitativemeasurementandthesevaluesaremoreandmorebetterdefined.Foranaorticvalvestenosis(AS)thetimingofsurgicaltreatmentisbasedonthesymptomaticstatusandtheseverityofthedisease.Currentguidelinesrecommendaorticvalvereplacement,asaclassIindication,onlyinsevereASforsymptomaticpatientsorforasymptomaticpatientswithsystolicLVdysfunction.Hence,anaccurategradingofASseverity
ismandatoryforclinicaldecision-making.Todate,noneoftheparametersdefinedtogradeAScanbeappliedasasinglecriterion.AcrucialstepintheevaluationoftheseverityofASistheanalysisoftheflowacrossthevalve.Indailypractice,theassessmentofASseverityshouldintegratetheflow-gradientpatterntotheclassicmeasurementofAVA.Innormalflow-highgradientandinlowflow-highgradientthesymptomaticpatientsareclassicallyreferredforAVR,whereaswhenasymptomatic,themanagementofthesepatientsunderlinestheneedforoptimizedriskstratification.Insymptomaticpatientswithlow-flow,low-gradientandreducedEF,indicationwillmainlydependonevidenceofflowreservewhileitisimportanttorecognizetheparadoxicallow-flow,low-gradientwithnormalEFin
ordernottodenysurgerytoasymptomaticpatient.Quitesimilarly,inseverechronicaorticregurgitation
(AR)asdefinedbyquantitativemeasuresofvenacontracta,effectiveregurgitantorificeorregurgitantvolume,allsymptomaticpatientsrequiresurgery,regardlessoftheirLVfunctionanddilation;inasymptomaticpatientsAVRisindicatedwhenLVejectionfractionEF<50%(classI).
Aneurysmaldilationoftheascendingaortaand/oraorticrootisoneoftheprimarypathologiesnecessitatingsurgicalinterventionontheascendingaorta.Nowadaysoutcomesforascendingaortaandarchreplacementareexcellentforelectiverepair;however,resultsdeterioratefornon-electivestatus,suggestingthatincreasedscreeningand/orloweringthresholdsforelectiveinterventioncouldpotentiallyimproveoutcomes.Forpatientswithoutconnectivetissuedisorders,currentguidelinesstillrecommendedsurgeryatmaximumdiameterof5.5cmorforayearlyincrease>0.5cm/yr.(ClassI,levelC)whetherdegenerative,chronicdissection,orpenetratingulcers.Forpatientswithbicuspidvalveelectivesurgeryisrecommendedwhenthediameterexceed5cmor2.5cm/m2(ClassI,levelC).Onlyincasethepatientsneedsurgerybecauseofvalvediseasethisthresholdisloweredto4.5cm.InpatientswithMarfansyndromethethresholdremainat5.0cm(ClassI,levelC)butisloweredto4.5cmasClassIIa,settingthebasisforamorerestrictiveapproachthatisalreadyplacedat4.2cmforpatientswithLoeys-Dietzsyndrome(ClassIIa,levelC).Inthispeculiargroupofpatientswithconnectivetissuedisorders(andsomesubgroupsofbicuspidvalvecouldalsobeassimilated)othermorerestrictiveformulasbasedoncross-sectionalareatoheightratiooronageandindividualriskfactorsarecurrentlyunderevaluationandmightcontributetofurtherrefiningcurrentguidelines.Lowerthresholdsofaorticdiametersbegintobeconsideredinlow-riskpatientsandinanexperiencedCentres.
Finally,forcompletenessitmustbesaidthattheusageofTAVIhasintroducedthemultidisciplinaryapproachintotheguidelinesandisexpectedtocontributetosomechangestothecurrentapproachbasedoncosts,newerdevices,andcompetition.
Schlegel F.1,2,3#, Leontyev S.1#, Spath C.1,4, Schmiedel R.1, Nichtitz M. 1, Boldt A.3, Rübsamen R.2 , Salameh A.1, Kostelka M. 1, Mohr F.-W.1, Dhein S.1 1 Heart Centre Leipzig, Germany; 2 University Leipzig, Germany; 3 Translational Centre for Regenerative Medicine, Leipzig, Germany
Weestablishedamethodforengineeringhearttissueforthetreatmentofdilativecardiomyopathy(DCM)inan
in vivoratmodel.Therefore,engineeredhearttissue(EHT)wascreatedasaringfromneonatalratcardiomyocytes,collagen,matrigelandmedia.AftercultivationtimeelectricallystimulatedEHTcontractedspontaneously(0.5-2Hz)anddevelopedforceof0.444±0.124mN.HistologicalinvestigationshowedthepresenceofTroponinIandCx43positiveelongatedcross-straitedcardiomyocytesandpreformedvascularstructuresintheEHTinvitro(figure1).EHTwasimplantedaroundthebeatingheartof
13SpraqueDawleyratswithdoxorubicininducedDCM.Additionally,12animalswithDCMunderwentashamsurgery.Priorandaftersurgerytheheartfunctionwascontrolledbyechocardiographyandinvasivehaemodynamicmeasurement(dp/dtmax)byMillarcatheterundercontrolconditionsandunderdobutamine(0.2mg/kg)forstimulationofβ-adrenergicsystem.SubsequentlytheheartswereexplantedandpreparedfortheLangendorffsystemandelectricalmappinganalysis.Therefore,256electrodeswereplacedaroundtheheartandwemeasuredthecardiacactivationtime.Finally,histologicalinvestigationsoftheEHTandtheheartwereperformed.InEHT-treatedDCMrats84%survivedandinshamtreatedanimals58%(p=0.3).Priortosurgery,fractionalshortening(FS)wassignificantlydecreasedascomparedtohealthyanimals(healthy:43.2±1.3%vs.DCM32.9±0.9%,p<0.05).30daysafterEHTimplantationFSincreasedby+4.61.3%.Incomparison,shamtreatedanimalsexhibitedfurtherdecreaseinFS(-
7.53.7%,p=0.002).Contractilityanalysisrevealed
thatthedobutamineinducedincreaseincontractility(healthy:12350±1619mmHg/s)wascompletelyabolishedinDCM(+7050±1045mmHg/s),butwasrestoredbyEHT-therapy(12579±2892mmHg/s),butnotbyshamtherapy(+5824±543mmHg/s).Furthermore,mappinganalysisrevealed
anelectricalsynchronisationofEHTwiththenativemyocardium.TherewerenoarythmogenicfociandnosignificantdelaysintotalactivationtimeandnochangesinpeaktopeakamplitudedetectablebetweenEHTandnativeheart.Moreover,EHTwasmacroscopically(seefigure2)andhistologicallyintegratedintotherecipientheartandconnectedtothecoronarysystemwhichwasshown
byintracoronarydyeinjectionandredbloodcellscontainingvesselsinEHTin vivo.Additionally,wefoundsignificantinductionofvascularendothelialgrowthfactor(VEGF)-expressionafterEHT-therapy,comparedtoshamtreatedanimals.TheseresultsareinagreementwiththefindingofsignificantlyenhancedcapillarydensityinEHT-treatedheart,sothatthataparacrineVEGFproductionmaycontributetothebeneficialeffectsofEHT-therapyviaanangiogeneticeffectintherecipientheart.ImplantedEHTshowedorganisedcollagenstructure,elasticfibres,andcontainsTroponinIandCx43positiveelongatedcardiomyocytes.
Inconclusion,thiscouldmeanthatthetherapeuticeffectprobablyisnotonlyduetoenhancedcontractility,butmaybeexplainedbyacombinationofincreasedelasticforces(elasticfibresintheEHT),paracrineeffectslikeincreaseinVEGF,aslightlyincreasedcoronaryflowinDCM-EHTvs.DCM-shamhearts,andthecontractilityoftheEHTitself.
Treatment of dilated cardiomyopathy using engineered heart tissue (eHT) as biological cardiac assist device
Session 1: Imaging in Mitral valve repair 10:30 Hall D
Jolanda Kluin UMC Utrecht, The Netherlands
Anatomicandfunctionalstudyofthepreoperativeregurgitatingmitralvalveisessentialfordecidingthetimingandsuitabilityofsurgicalrepair.Althoughstandard
techniquesformitralregurgitationevaluationhavebeenofvalue,theirreproducibilityandaccuracyarelimitedinsomepatientgroups.
Thegoalofdiagnosticimagingistoprovideaquantitativemeasureofthesizeoftheregurgitantlesion.Reproducibleandaccuratequantificationofmitralvalveregurgitationremainsanongoingclinicalchallenge.AssessingthedegreeofmitralregurgitationmightbedifficultwithTTEor2DTEEespeciallyincaseswitheccentricormultiplejets.
From3DcolorDopplervolumetricdatasets,wecannowroutinelymeasurethevenacontractaarea,ameasurethataccuratelyquantifies
theeffectivefloworificearea(ERO)inbothfunctionalandorganicmitralvalvedysfunction.Inaddition,methodstorapidlyderivethree-dimensionalPISAmeasureshaverecentlybeencommercializedandcliniciansandinvestigatorsarecurrentlygainingexperiencewiththesepromisingnewtechniques.Thereisanexcellentcorrelationbetween3DanatomicEROderivedregurgitantvolumeandmitralregurgitantvolumecalculatedbycardiacmagneticresonance.
Precisecharacterizationofthemitralvalveiscrucialforguidingthemanagementofpatientswithmitralvalveprolapse.Fromwatchfulwaitingtovalverepair,differentoptionsmaybeconsideredonthebasisofthepossibilityofrepair.Echocardiographyremainstheexaminationofchoiceforsuchevaluation.Accurateechocardiographicevaluationofthemitralvalvemightbecomplexandrequiresadvancedoperatortrainingandexperiencetoprovideanaccurate3Danalysisofthevalve.Withexperience,thisanalysisisusuallyachievedfrommultiple2Dimages,mentallyreconstructedtoforma3Dimage.Byusing3DTEEimages,less-
experiencedcardiologistsandcardiothoracicsurgeonscanbypassthestepofmentalreconstructionfrom2Dimagesanddescribeandunderstandmitralvalveprolapsemoreaccurately.Furthermore,2DTEEislimited,especiallyinthediagnosisofmorecomplexvalvesforwhichrepairismoredifficult.3DTEEmaybeofvalueinsuchselectedcasestoimprovecharacterizationofmitralvalvephysiopathologyandtoalertsurgeonstotheneedformorecomplexoperation(egcommissuralprolapse)thanmaybeindicatedby2Dexamination.Finally,infunctionalmitralregurgitation,quantitative3Dechocardiographicparametersmeasuringleafletdeformation,asaresultoftethering,canoffermechanisticcluesalongwithprognosticinformationonthedurabilityofcertainmitralvalveapproaches.
3Dechocardiographyisonitswaytobeavaluabletoolinmitralregurgitationassessment.Itassuresbetterquantificationinpatientswitheccentricormultiplejets,andbettercharacterizationinpatientswithfunctionalmitralregurgitationorinpatientswithcomplexvalves.
Does 3D echocardiography enhance decision making?
Valve and aortic guidelines
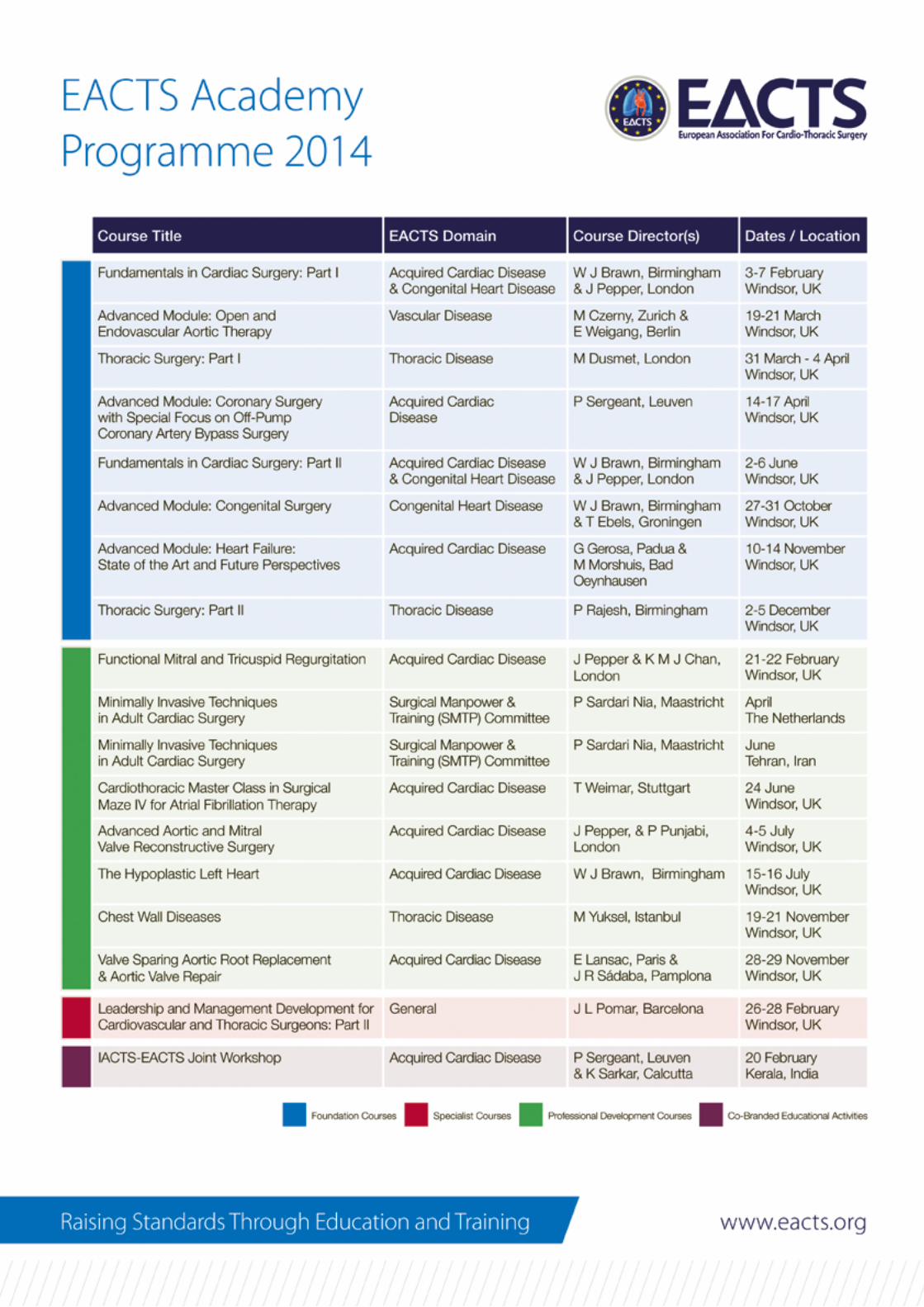
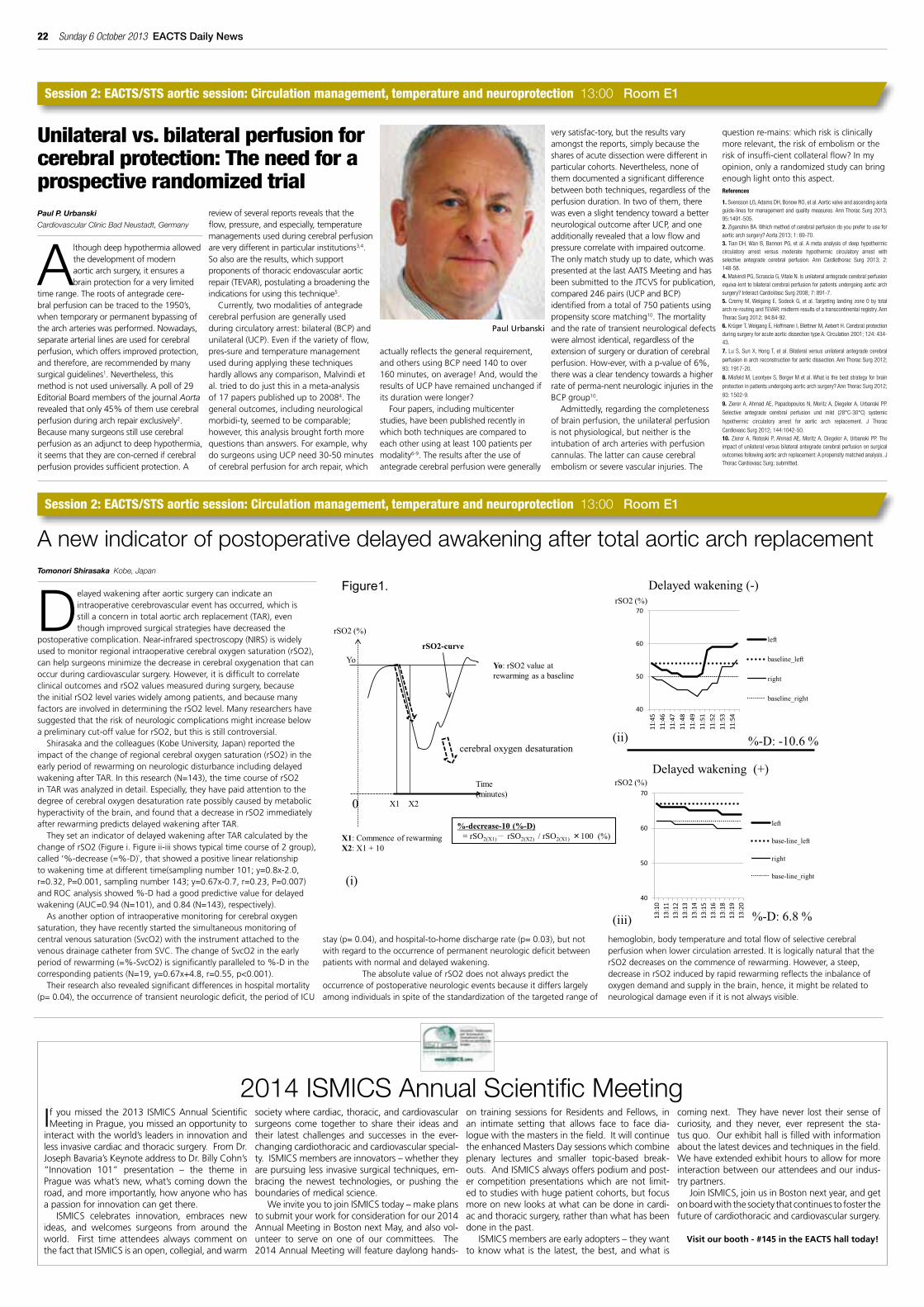
22 Sunday 6 October 2013 EACTS Daily News
Session 2: EACTS/STS aortic session: Circulation management, temperature and neuroprotection 13:00 Room E1
Session 2: EACTS/STS aortic session: Circulation management, temperature and neuroprotection 13:00 Room E1
Paul P. Urbanski Cardiovascular Clinic Bad Neustadt, Germany
Althoughdeephypothermiaallowedthedevelopmentofmodernaorticarchsurgery,itensuresabrainprotectionforaverylimited
timerange.Therootsofantegradecere-bralperfusioncanbetracedtothe1950’s,whentemporaryorpermanentbypassingofthearcharterieswasperformed.Nowadays,separatearteriallinesareusedforcerebralperfusion,whichoffersimprovedprotection,andtherefore,arerecommendedbymanysurgicalguidelines1.Nevertheless,thismethodisnotuseduniversally.Apollof29EditorialBoardmembersofthejournalAortarevealedthatonly45%ofthemusecerebralperfusionduringarchrepairexclusively2.Becausemanysurgeonsstillusecerebralperfusionasanadjuncttodeephypothermia,itseemsthattheyarecon-cernedifcerebralperfusionprovidessufficientprotection.A
reviewofseveralreportsrevealsthattheflow,pressure,andespecially,temperaturemanagementsusedduringcerebralperfusionareverydifferentinparticularinstitutions3,4.Soalsoaretheresults,whichsupportproponentsofthoracicendovascularaorticrepair(TEVAR),postulatingabroadeningtheindicationsforusingthistechnique5.
Currently,twomodalitiesofantegradecerebralperfusionaregenerallyusedduringcirculatoryarrest:bilateral(BCP)andunilateral(UCP).Evenifthevarietyofflow,pres-sureandtemperaturemanagementusedduringapplyingthesetechniqueshardlyallowsanycomparison,Malvindietal.triedtodojustthisinameta-analysisof17paperspublishedupto20084.Thegeneraloutcomes,includingneurologicalmorbidi-ty,seemedtobecomparable;however,thisanalysisbroughtforthmorequestionsthananswers.Forexample,whydosurgeonsusingUCPneed30-50minutesofcerebralperfusionforarchrepair,which
actuallyreflectsthegeneralrequirement,andothersusingBCPneed140toover160minutes,onaverage!And,wouldtheresultsofUCPhaveremainedunchangedifitsdurationwerelonger?
Fourpapers,includingmulticenterstudies,havebeenpublishedrecentlyinwhichbothtechniquesarecomparedtoeachotherusingatleast100patientspermodality6-9.Theresultsaftertheuseofantegradecerebralperfusionweregenerally
verysatisfac-tory,buttheresultsvaryamongstthereports,simplybecausethesharesofacutedissectionweredifferentinparticularcohorts.Nevertheless,noneofthemdocumentedasignificantdifferencebetweenbothtechniques,regardlessoftheperfusionduration.Intwoofthem,therewasevenaslighttendencytowardabetterneurologicaloutcomeafterUCP,andoneadditionallyrevealedthatalowflowandpressurecorrelatewithimpairedoutcome.Theonlymatchstudyuptodate,whichwaspresentedatthelastAATSMeetingandhasbeensubmittedtotheJTCVSforpublication,compared246pairs(UCPandBCP)identifiedfromatotalof750patientsusingpropensityscorematching10.Themortalityandtherateoftransientneurologicaldefectswerealmostidentical,regardlessoftheextensionofsurgeryordurationofcerebralperfusion.How-ever,withap-valueof6%,therewasacleartendencytowardsahigherrateofperma-nentneurologicinjuriesintheBCPgroup10.
Admittedly,regardingthecompletenessofbrainperfusion,theunilateralperfusionisnotphysiological,butneitheristheintubationofarcharterieswithperfusioncannulas.Thelattercancausecerebralembolismorseverevascularinjuries.The
questionre-mains:whichriskisclinicallymorerelevant,theriskofembolismortheriskofinsuffi-cientcollateralflow?Inmyopinion,onlyarandomizedstudycanbringenoughlightontothisaspect.References
1. Svensson LG, Adams DH, Bonow RO, et al. Aortic valve and ascending aorta guide-lines for management and quality measures. Ann Thorac Surg 2013; 95:1491-505.2. Ziganshin BA. Which method of cerebral perfusion do you prefer to use for aortic arch surgery? Aorta 2013; 1: 69-70. 3. Tian DH, Wan B, Bannon PG, et al. A meta analysis of deep hypothermic circulatory arrest versus moderate hypothermic circulatory arrest with selective antegrade cerebral perfusion. Ann Cardiothorac Surg 2013; 2: 148-58. 4. Malvindi PG, Scrascia G, Vitale N. Is unilateral antegrade cerebral perfusion equiva-lent to bilateral cerebral perfusion for patients undergoing aortic arch surgery? Interact CardioVasc Surg 2008; 7: 891-7.5. Czerny M, Weigang E, Sodeck G, et al. Targeting landing zone 0 by total arch re-routing and TEVAR: midterm results of a transcontinental registry. Ann Thorac Surg 2012; 94:84-92. 6. Krüger T, Weigang E, Hoffmann I, Blettner M, Aebert H. Cerebral protection during surgery for acute aortic dissection type A. Circulation 2001; 124: 434-43.
7. Lu S, Sun X, Hong T, et al. Bilateral versus unilateral antegrade cerebral
perfusion in arch reconstruction for aortic dissection. Ann Thorac Surg 2012;
93: 1917-20.
8. Misfeld M, Leontyev S, Borger M et al. What is the best strategy for brain
protection in patients undergoing aortic arch surgery? Ann Thorac Surg 2012;
93: 1502-9.
9. Zierer A, Ahmad AE, Papadopoulos N, Moritz A, Diegeler A, Urbanski PP.
Selective antegrade cerebral perfusion und mild (28°C-30°C) systemic
hypothermic circulatory arrest for aortic arch replacement. J Thorac
Cardiovasc Surg 2012; 144:1042-50.10. Zierer A, Risteski P, Ahmad AE, Moritz A, Diegeler A, Urbanski PP. The impact of unilateral versus bilateral antegrade cerebral perfusion on surgical outcomes following aortic arch replacement: A propensity matched analysis. J Thorac Cardiovasc Surg; submitted.
Unilateral vs. bilateral perfusion for cerebral protection: The need for a prospective randomized trial
Tomonori Shirasaka Kobe, Japan
Delayedwakeningafteraorticsurgerycanindicateanintraoperativecerebrovasculareventhasoccurred,whichisstillaconcernintotalaorticarchreplacement(TAR),eventhoughimprovedsurgicalstrategieshavedecreasedthe
postoperativecomplication.Near-infraredspectroscopy(NIRS)iswidelyusedtomonitorregionalintraoperativecerebraloxygensaturation(rSO2),canhelpsurgeonsminimizethedecreaseincerebraloxygenationthatcanoccurduringcardiovascularsurgery.However,itisdifficulttocorrelateclinicaloutcomesandrSO2valuesmeasuredduringsurgery,becausetheinitialrSO2levelvarieswidelyamongpatients,andbecausemanyfactorsareinvolvedindeterminingtherSO2level.Manyresearchershavesuggestedthattheriskofneurologiccomplicationsmightincreasebelowapreliminarycut-offvalueforrSO2,butthisisstillcontroversial.
Shirasakaandthecolleagues(KobeUniversity,Japan)reportedtheimpactofthechangeofregionalcerebraloxygensaturation(rSO2)intheearlyperiodofrewarmingonneurologicdisturbanceincludingdelayedwakeningafterTAR.Inthisresearch(N=143),thetimecourseofrSO2inTARwasanalyzedindetail.Especially,theyhavepaidattentiontothedegreeofcerebraloxygendesaturationratepossiblycausedbymetabolichyperactivityofthebrain,andfoundthatadecreaseinrSO2immediatelyafterrewarmingpredictsdelayedwakeningafterTAR.
TheysetanindicatorofdelayedwakeningafterTARcalculatedbythechangeofrSO2(Figurei.Figureii-iiishowstypicaltimecourseof2group),called‘%-decrease(=%-D)`,thatshowedapositivelinearrelationshiptowakeningtimeatdifferenttime(samplingnumber101;y=0.8x-2.0,r=0.32,P=0.001,samplingnumber143;y=0.67x-0.7,r=0.23,P=0.007)andROCanalysisshowed%-Dhadagoodpredictivevaluefordelayedwakening(AUC=0.94(N=101),and0.84(N=143),respectively).
Asanotheroptionofintraoperativemonitoringforcerebraloxygensaturation,theyhaverecentlystartedthesimultaneousmonitoringofcentralvenoussaturation(SvcO2)withtheinstrumentattachedtothevenousdrainagecatheterfromSVC.ThechangeofSvcO2intheearlyperiodofrewarming(=%-SvcO2)issignificantlyparalleledto%-Dinthecorrespondingpatients(N=19,y=0.67x+4.8,r=0.55,p<0.001).
Theirresearchalsorevealedsignificantdifferencesinhospitalmortality(p=0.04),theoccurrenceoftransientneurologicdeficit,theperiodofICU
stay(p=0.04),andhospital-to-homedischargerate(p=0.03),butnotwithregardtotheoccurrenceofpermanentneurologicdeficitbetweenpatientswithnormalanddelayedwakening.
TheabsolutevalueofrSO2doesnotalwayspredicttheoccurrenceofpostoperativeneurologiceventsbecauseitdifferslargelyamongindividualsinspiteofthestandardizationofthetargetedrangeof
hemoglobin,bodytemperatureandtotalflowofselectivecerebralperfusionwhenlowercirculationarrested.ItislogicallynaturalthattherSO2decreasesonthecommenceofrewarming.However,asteep,decreaseinrSO2inducedbyrapidrewarmingreflectstheinbalanceofoxygendemandandsupplyinthebrain,hence,itmightberelatedtoneurologicaldamageevenifitisnotalwaysvisible.
A new indicator of postoperative delayed awakening after total aortic arch replacement
Paul Urbanski
Delayed wakening (-)
Delayed wakening (+)
%-D: 6.8 %
%-D: -10.6 %
40
50
60
70
11:4
5 11
:46
11:4
7 11
:48
11:4
9 11
:51
11:5
2 11
:53
11:5
4
left
baseline_left
right
baseline_right
40
50
60
70
13:1
0 13
:11
13:1
2 13
:13
13:1
4 13
:15
13:1
6 13
:18
13:1
9 13
:20
left
base-line_left
right
base-line_right
rSO2 (%)
rSO2 (%)
rSO2 (%)
%-decrease-10 (%-D) = rSO2(X1) rSO2(X2) / rSO2(X1) 100 (%)
Time(minutes)
X1 X2
cerebral oxygen desaturation
X1: Commence of rewarmingX2: X1 + 10
Yo: rSO2 value at rewarming as a baseline
0
YorSO2-curve
(i)
(ii)
(iii)
Ifyoumissed the2013 ISMICSAnnualScientificMeetinginPrague,youmissedanopportunityto
interactwiththeworld’sleadersininnovationandlessinvasivecardiacandthoracicsurgery.FromDr.JosephBavaria’sKeynoteaddresstoDr.BillyCohn’s“Innovation 101” presentation – the theme inPraguewaswhat’snew,what’scomingdowntheroad,andmoreimportantly,howanyonewhohasapassionforinnovationcangetthere.
ISMICS celebrates innovation, embraces newideas, and welcomes surgeons from around theworld. First time attendees always comment onthefactthatISMICSisanopen,collegial,andwarm
societywherecardiac,thoracic,andcardiovascularsurgeons come together to share their ideas andtheir latest challenges and successes in the ever-changingcardiothoracicandcardiovascularspecial-ty.ISMICSmembersareinnovators–whethertheyarepursuinglessinvasivesurgicaltechniques,em-bracing the newest technologies, or pushing theboundariesofmedicalscience.
WeinviteyoutojoinISMICStoday–makeplanstosubmityourworkforconsiderationforour2014AnnualMeetinginBostonnextMay,andalsovol-unteer to serve on one of our committees. The2014AnnualMeetingwillfeaturedaylonghands-
on training sessions forResidentsandFellows, inan intimate setting that allows face to face dia-loguewiththemastersinthefield.ItwillcontinuetheenhancedMastersDaysessionswhichcombineplenary lectures and smaller topic-based break-outs.AndISMICSalwaysofferspodiumandpost-er competitionpresentationswhicharenot limit-edtostudieswithhugepatientcohorts,butfocusmoreonnewlooksatwhatcanbedoneincardi-acandthoracicsurgery,ratherthanwhathasbeendoneinthepast.
ISMICSmembersareearlyadopters–theywanttoknowwhat isthe latest,thebest,andwhat is
comingnext.Theyhavenever losttheirsenseofcuriosity, and they never, ever represent the sta-tusquo.Ourexhibithallisfilledwithinformationaboutthelatestdevicesandtechniquesinthefield.Wehaveextendedexhibithourstoallowformoreinteractionbetweenourattendeesandourindus-trypartners.
JoinISMICS,joinusinBostonnextyear,andgetonboardwiththesocietythatcontinuestofosterthefutureofcardiothoracicandcardiovascularsurgery.
Visit our booth - #145 in the EACTS hall today!
2014 ISMIcS Annual Scientific Meeting
• Track all cardiac surgery procedures• Automated op notes/discharge summaries• Integrated risk modelling – EuroScore II• CUSUM, VLAD and Funnel Plot analysis• Unlimited longitudinal follow-up• Export to national registries
CardiaC Surgery databaSe Software for HoSpitalS aNd NatioNal regiStrieS
Delete
OM2 Routine graft Long SV Average (1.5–2.0mm) Scattered disease
Procedure Site Local Procedure Graft Conduit Coronary VesselSize
Coronary Vessel Quality
Distal RCA Routine graft Radial artery Average (1.5–2.0mm) Diffuse disease
Prox LAD Endarterectomy Free LIMA Average (1.5–2.0mm) Diffuse disease
Date of Operation: 07 September 2012 Selected Patient : John Nemo
Next Page
Exit Application
Previous PagePrevious Page
Dendrite Clinical SystemsCopyright © 2012
Proximal RCA
MidRCA
DistalRCA
Proximal circumflexProximal
circumflex
Distalcircumflex
LMS
OM1
OM2
Circumflex-PDA
Proximal LAD
MidLAD
DistalLAD Aortic
root
Aortic arch
Ascending aorta Descending
aorta
Abdominal aorta
Reveal • Interpret • Improve
The Hub – Station Road – Henley-on-Thames – RG9 1AY – United KingdomPhone: +44 1491 411 288 – e-mail: [email protected] – www.e-dendrite.com
PleasevisitDendrite onStand 97hereatEACTS 2013foradatabasedemonstration

24 Sunday 6 October 2013 EACTS Daily News
16
15
26
73
111
5149 6765 8280
92A991A
1381136
1461144
6361
25
46
53 69 84
58 86
887559
114
112
116
60
9077
79
3598
15911581157115611551154153115211511150149
101
12
93
140
148
126
124
122
128
130
132
6462
838168665250
74B74A
11
10
9
8
7
6
5
4
3
1
17
18
19
20
21
22
23
24
27
28
29
30
31
32
33
34
92B991B
95
96
97
3799
1391137
1471145
102
103
104
105
106
107
108
Catering and refreshments
10 SHVD–TheSocietyforHeartValveDisease
77 Siemens,HealthcareSector
108 Smartcanula
114 SorinGroupItalia
116 StJudeMedical
31 StarchMedical
137 STS–TheSocietyofThoracicSurgeons
21 SunshineHeart
79 Symetis
128 TerumoEuropeCardiovascularSystems
132 ThoratecCorporation
66 TianjinPlasticsResearchInstitute
4 TianjinWelcomeMedicalEquipment
80 TransonicEurope
105 ValveXchange
26 Vivostat
15 WexlerSurgical
149 WisepressOnlineBookshop
6 WLGore&Associates
18 WolfVision
50 WSPCHS–WorldSocietyforPediatricandCongenitalHeartSurgery
BoothCompanyName
BoothCompanyName
138 3-DMatrixEurope
24 A&EMedicalCorporation
144 AATS–AmericanAssociationforThoracicSurgery
126 AbbottVascularInternational
8 ACUTEInnovations
46 Admedus
19 AdvancisSurgical
51 AndocorNV
9 APACVS–AssociatonofPhysicianAssistantsinCardiovascularSurgery
93 AsanusMedizintechnik
88 AtriCureEurope
122 BBraunSurgical
27–28BaxterHealthcare
69 BerlinHeart
67 BioCerEntwicklungs
139 BiointegralSurgical
61 BiometMicrofixation
17 BioVentrix
7 CRBard
81 CardiaInnovation
37 CardiaMed
101 CardioMedical
158–9Carmat
92b ChaseMedical
150–3CircuLite
157 ClearCatheterSystems
106–7CookMedical
12 CorMatrixCardiovascular
74b Correx
58 CryolifeEuropa
136 CTSNet
20 DeSoutterMedical
98 Delacroix-Chevalier
97 DendriteClinicalSystems
EACTS-Euromacs
148 EACTS–TheEuropeanAssociationforCardio-ThoracicSurgery
112 EdwardsLifesciences
111 Estech
73 Ethicon–Johnson&JohnsonMedical
130 Eurosets
1 FehlingInstruments
91a gebemedDeutschland
35 GebruederMartin
75 GeisterMedizintechnik
3 GeneseeBioMedical
32 GEOMEDMedizin-Technik
92a GlobalCommunication
146 Gunze
82 HamamatsuPhotonicsDeutschland
49 HeartandHealthFoundation
52 HeartHugger/GeneralCardiacTechnology
124 HeartWare
91b ImaCor
83 Integra
145 ISMICS–InternationalSocietyforMinimallyInvasiveCardiothoracicSurgery
140 JenaValveTechnology
29–30JOTEC
63–64KarlStorz
95–96LepuMedicalTechnology
99 LSISolutions
5 Mani
59 MaquetCardiopulmonary
22 MasterSurgerySystems
147 MDDMedicalDeviceDevelopment
53 Medafor
74a MedexResearch
84 Medistim
90 MedosMedizintechnik
60 MedtronicInternationalTrading
154–5MiCardiaCorporation
23 NeoChord
86 On-XLifeTechnologies
16 OxfordUniversityPress
11 PCR
25 PetersSurgical
156 Posthorax
68 Praesidia
34 Qualiteam
65 Redax
62 RTISurgical
33 RumexInternational
102–4ScanlanInternational
Floor plan
ENTRANCE

26 Sunday 6 October 2013 EACTS Daily News
Learnmoreabout thedesign, implantationandclinicalresultsofthe3fEnable®SuturelessValve
and Engager®, the next generation surgical TAVIplatformthroughpresentationsbyexpertsfollowedbyawetlabandasimulationworkshop.
Over the past few years, new technologieshave expanded the treatment options forcardiacsurgeonstotreatpatientssufferingfromaortic stenosis such as transcatheter aortic valvereplacementandmorerecentlywithnewsurgicalsuturelessvalves.
Following the recent introduction of theEngagertransapicalaorticvalvesysteminEuropeand the growing interest in sutureless valves
such as the 3f Enable® valve, Medtronic seizesthe opportunity of this year’s EACTS to inviteattendeestotheMedtronicExperienceCentretoattendaseriesofpracticalworkshopsfocusedonthesenewtechnologies.
Each workshop will start with a presentationof the 3f Enable® sutureless valve by professorOttoDapunt1followedbyawet-labduringwhichparticipants will have the opportunity to implantthevalveonpighearts.
The workshop will then continue with apresentationofthenewEngagertransapicalaorticvalve system by Dr. Hendrik Treede2, Pr. MichaelHilker3andPr.EhudSchwammenthal4followedby
sizingandimplantationsimulation.More than offering a practical experience,
each workshop will be an opportunity to helpsurgeons use their best judgement to matchthe appropriate product with the appropriatepatientthroughdiscussionswithexpertsonpre-proceduralplanning,scientificresultsandpatientindications.
EACTSattendeeswillingtoparticipatetooneoftheseworkshopsareinvitedtocontactaMedtronicrepresentativeattheMedtronicboothordirectlyatthereceptionoftheMedtronicExperienceCentrelocatedintheLounge3atlevel01oftheAustriaCentre.
3 Workshops:nMonday07October:
from09:00to11:00n Tuesday08October:
from09:00to11:00andfrom14:00to16:00
Please visit the Medtronic Experience Centreat your convenience for simulation stationson minimally invasive OPCAB, cannulation,perfusionsystemsand transcatheteraorticvalvereplacementsystems.1 Pr. Otto Dapunt, Clinic for Heart Surgery at Klinikum Oldenburg, Germany
2 Dr. Hendrik Treede- Hamburg University Hospital, Germany
3 Pr. Michael Hilker- Universität Klinikum Regensburg, Germany
4 Pr. Ehud Schwammenthal- Tel Aviv University- Israël
Test-Drive Medtronic’s Latest Solutions for Patients with Aortic Stenosis
PublisherDendriteClinicalSystems
Editor in ChiefPieterKappetein
Managing [email protected]
Industry [email protected]
Design and [email protected]
Managing [email protected]
Head OfficeTheHubStationRoadHenley-on-Thames,RG91AY,UnitedKingdomTel+44(0)1491411288Fax+44(0)1491411399Websitewww.e-dendrite.com
Copyright2013©:DendriteClinicalSystemsandtheEuropeanAssociationforCardio-ThoracicSurgery.Allrightsreserved.Nopartofthispublicationmaybereproduced,storedinaretrievalsystem,transmittedinanyformorbyanyothermeans,electronic,mechanical,photocopying,recordingorotherwisewithoutpriorpermissioninwritingoftheeditor.
EACTSDaily News