targeted temperature management in the neuro- icu: who should
TRANSCRIPT
Targeted Temperature Management in the Neuro-ICU: Who should be cooled
and why?
Fred Rincon, MD, MSc, MBE FACP, FCCP, FCCM
Associate Professor, Neurology and NeurosurgeryThomas Jefferson University
Division of Critical Care and NeurotraumaPhiladelphia, PA USA

Disclosures
• Financial
- Grant support (Current): Genentech, AHA CRP12050342
- Royalties: Elsevier
• Non-financial
- Research support: Cerner Corporation
• Unlabeled/Unapproved uses
- Most applications of cooling are off-label
My background
• I am a Critical Care Specialist with experience in different fields
• Extensive experience in implementing protocols for TTM in brain injured patients
• No personal experience in neonates
Outline
DefinitionsPathophysiologyEvidenceBench to bedside

From: 11th ICC SCCM. Puerto Rico 2008.
Targeted Temperature Management
NormothermiaHypothermia

Definitions
AUTHOR MILD MOD DEEP
Wong 32-35 26-31 20-25
Varnathan 32-35 26-31 20-25
Zeiner 34-36 28-33 17-27
Reuler 34-36 28-33 17-27
Hammer >32 28-32 20-28
Safar 33-36 28-32 11-27
Werner 34-36 29-33 17-28
From: Werner D. 11th ICC SCCM. Puerto Rico 2008.
Hypothermia

Definitions
STUDY INSULT TARGET TERM
Clifton TBI 33 Moderate
Bernard CA 33 Moderate
HACA CA 32-34 Mild
Todd Aneurysm 32.5-33.5 Mild
Shankaran Neonatal-Asphyxia 33.5 Not defined
Gluckman Neonatal-Asphyxia 33.5 Mild
From: Werner D. 11th ICC SCCM. Puerto Rico 2008.
Hypothermia
Consensus
•Clinical management issues
•Efficacy
•Basic science biology
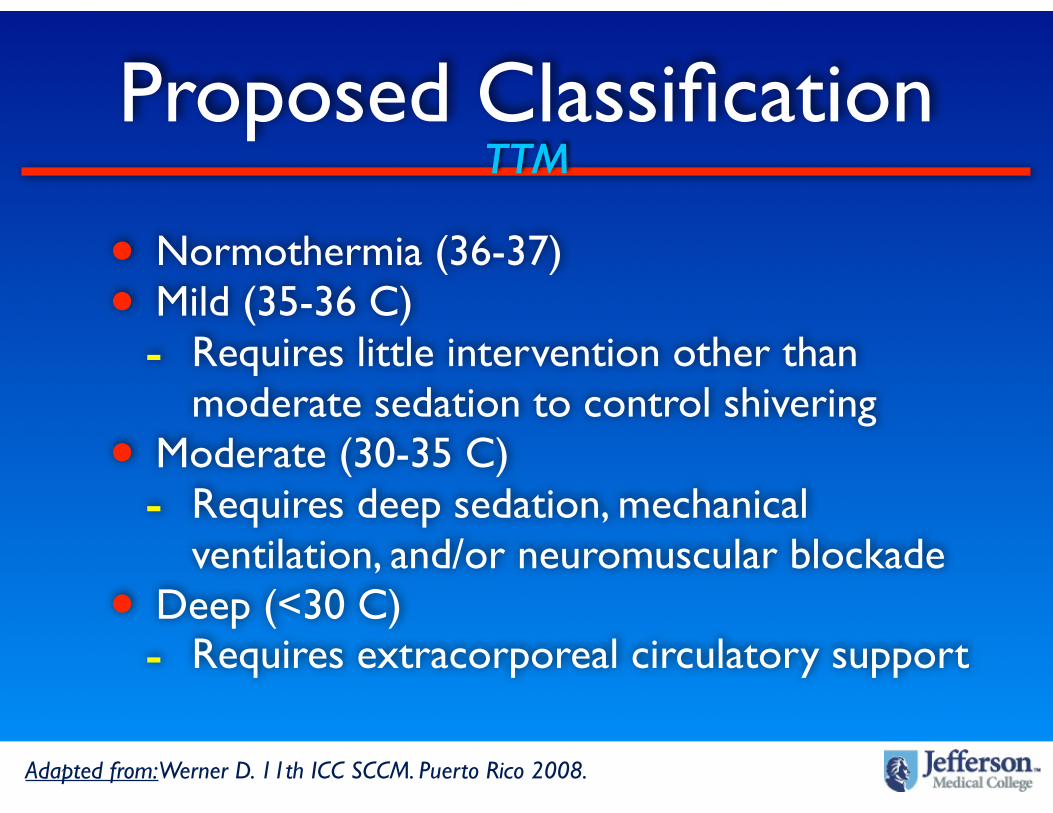
Proposed Classification
• Normothermia (36-37)• Mild (35-36 C)
- Requires little intervention other than moderate sedation to control shivering
• Moderate (30-35 C)- Requires deep sedation, mechanical
ventilation, and/or neuromuscular blockade• Deep (<30 C)
- Requires extracorporeal circulatory support
Adapted from: Werner D. 11th ICC SCCM. Puerto Rico 2008.
TTM

Applications Neuro ICU
Neuroprotection ICP ControlCerebral edema
Hypothermia (30-35 C)Normothermia (36-37 C)
TTM

Experimental Brain Injury
Yamamoto et al. Infarct volume in focal cerebral ischemia in rats. Stroke 2001
Normo
Hypo
Kollmar et al. Stroke 2007
Buki et al. Axonal injury in TBI - rats. Exp Neurol 1999
Normo Hypo
CAMARADES. Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Stroke
Normo Hypo
Chopp et al. Neuronal death in global cerebral ischemia in rats. Stroke 1991
How does mild hypothermia attenuate neuronal death and improve neurological
outcomes when applied AFTER experimental brain injury?
Motor deficits in roedentsKakinohana. Anesthesiology 1999
Hypothermia

From: http://www.irmc.org. Accessed 10/1/10Michenfelder and Thiene. Anesthesiology, 1968
BEFORE injury ,deep and moderate hypothermia
have been used, and continued to be used, for preservation of cellular integrity, mithocondrial
function, and prevention of energy failure
Prevention of Brain InjuryHypothermia
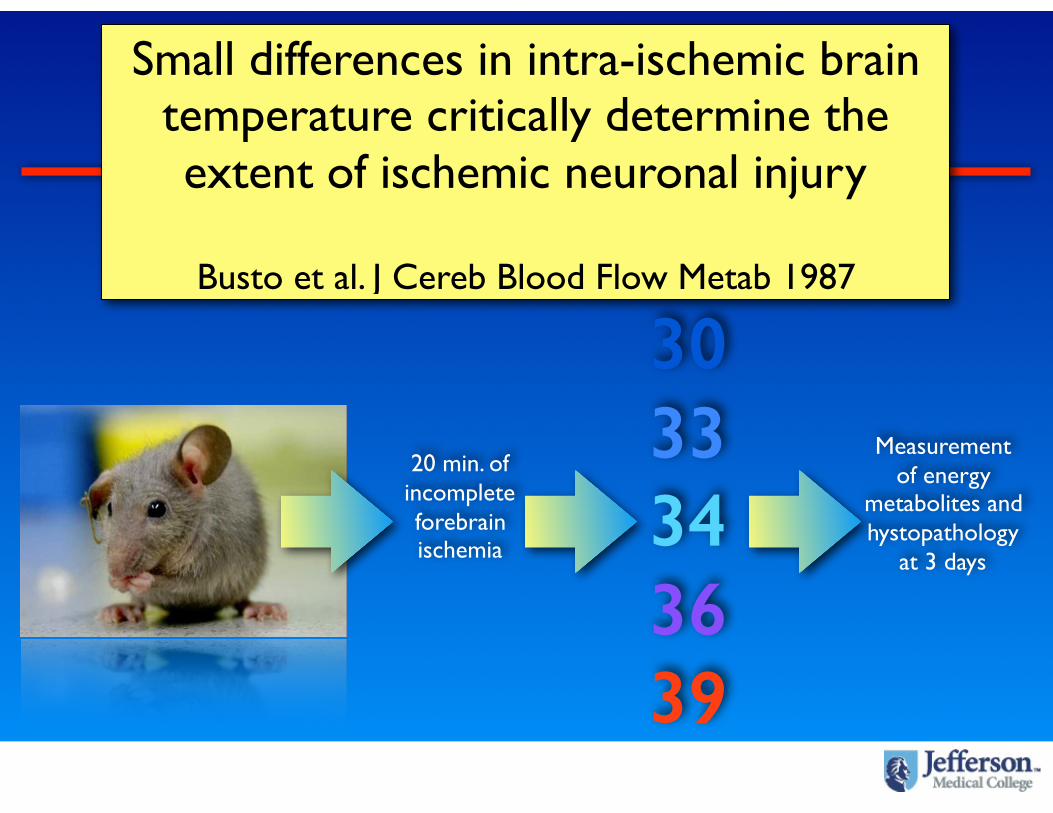
Small differences in intra-ischemic brain temperature critically determine the extent of ischemic neuronal injury
Busto et al. J Cereb Blood Flow Metab 1987
20 min. of incomplete forebrainischemia
30 33 34 36 39
Measurement of energy
metabolites and hystopathology
at 3 days
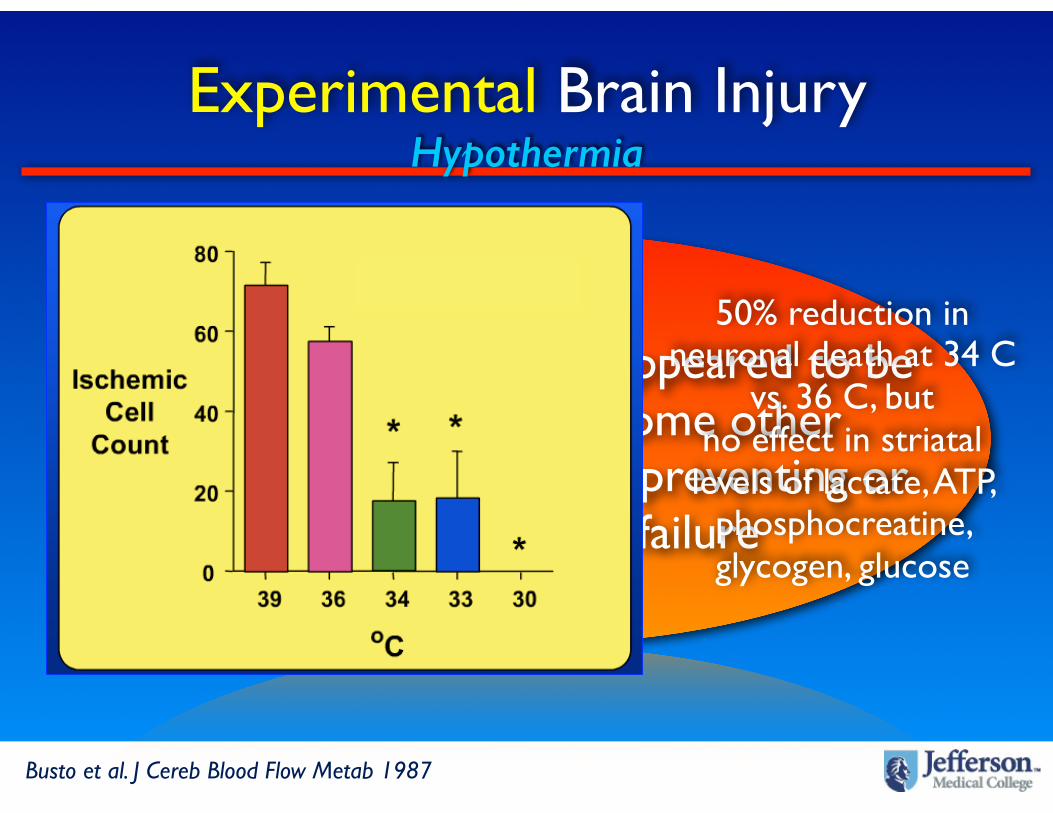
MILD HYPOTHERMIA appeared to be neuroprotective by some other
mechanisms than simply preventing or reversing energy failure
Busto et al. J Cereb Blood Flow Metab 1987
50% reduction in neuronal death at 34 C
vs. 36 C, but no effect in striatal
levels of lactate, ATP, phosphocreatine, glycogen, glucose
Experimental Brain InjuryHypothermia
Therapeutic Hypothermia
Is it blocking secondary injury cascades?
Is it preventing loss of endogenous neuroprotectants?
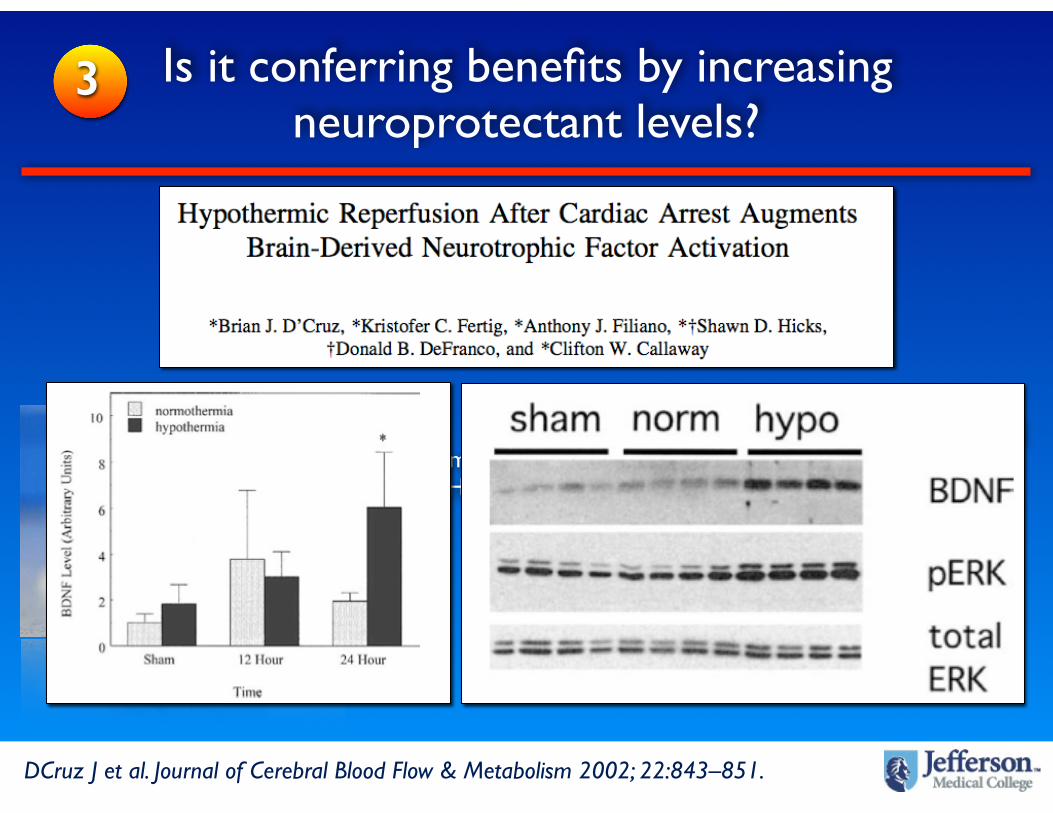
Is it conferring benefits by increasing neuroprotectant levels?
Zhao H.Journal Cereb Blood Flow Metab 2007 & Kochaneck P. 11th ICC SCCM. Puerto Rico 2008.
1
2
3

Therapeutic Hypothermia
Zhao H.Journal Cereb Blood Flow Metab 2007
Therapeutic hypothermia blocks
NUMEROUS secondary injury mechanisms in
experimental brain injury relevant to
critical care medicine

SupressesGlutamate
release
Attenuatesoxidative
stress
Regulatesgene
expression
Attenuatesapoptosis
Blunts inflammatory
response
Limits energyfailure
Atennuatesnitrosative
stressLimits
cytoskeletaldamage Increases
levels ofneurotrop.
AtennuatesMMP
activation
Atennuatesanoxic
depolar.
AtennuatesBBB
injury
LimitsDephos-
phorilation
Mild Therapeutic Hypothermia
Adapted from: Kochaneck P. 11th ICC SCCM. Puerto Rico 2008.
Mechanistic evidence

1 Is it blocking secondary injury cascades?
Mordecai G. J. Neurochem. 65, 1704-1711 (1995)
Hypothermia 30 C

2 Is it preventing loss of endogenous neuroprotectants?
Zhao H. The Journal of Neuroscience, 2005 • 25(42):9794 –9806
AKT= protein kinase B (PKB)
8 min. of asphyxial CAHypothermia 33 C 60 minutes after
ROSC12-24 hr
Measurement of BDNF(Prevents neuronal death)
3 Is it conferring benefits by increasing neuroprotectant levels?
DCruz J et al. Journal of Cerebral Blood Flow & Metabolism 2002; 22:843–851.
MILD-MOD HYPOTHERMIA blocks numerous secondary injury pathways but
has complex mechanistic effects
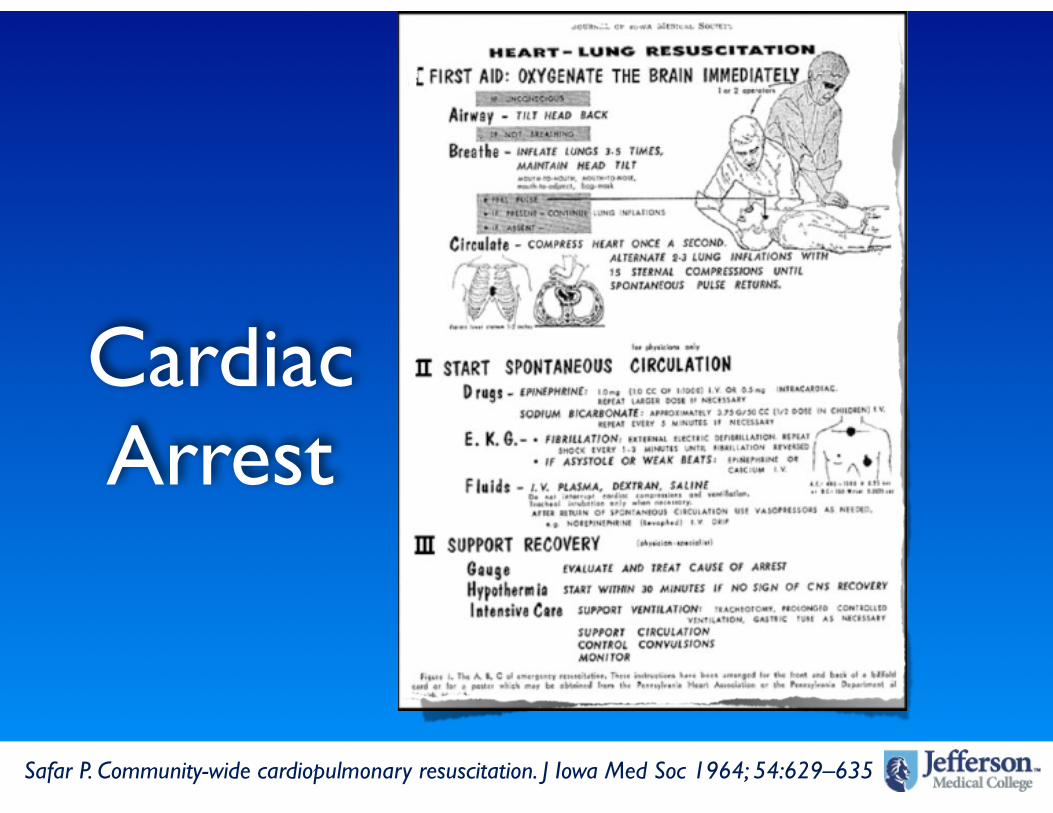
Safar P. Community-wide cardiopulmonary resuscitation. J Iowa Med Soc 1964; 54:629–635
Cardiac Arrest

Holzer M. N Engl J Med 2002;346:549-56.
Cardiac Arrest
Holzer M. Crit Care Med 2005; 33:414–418.
Hypothermia
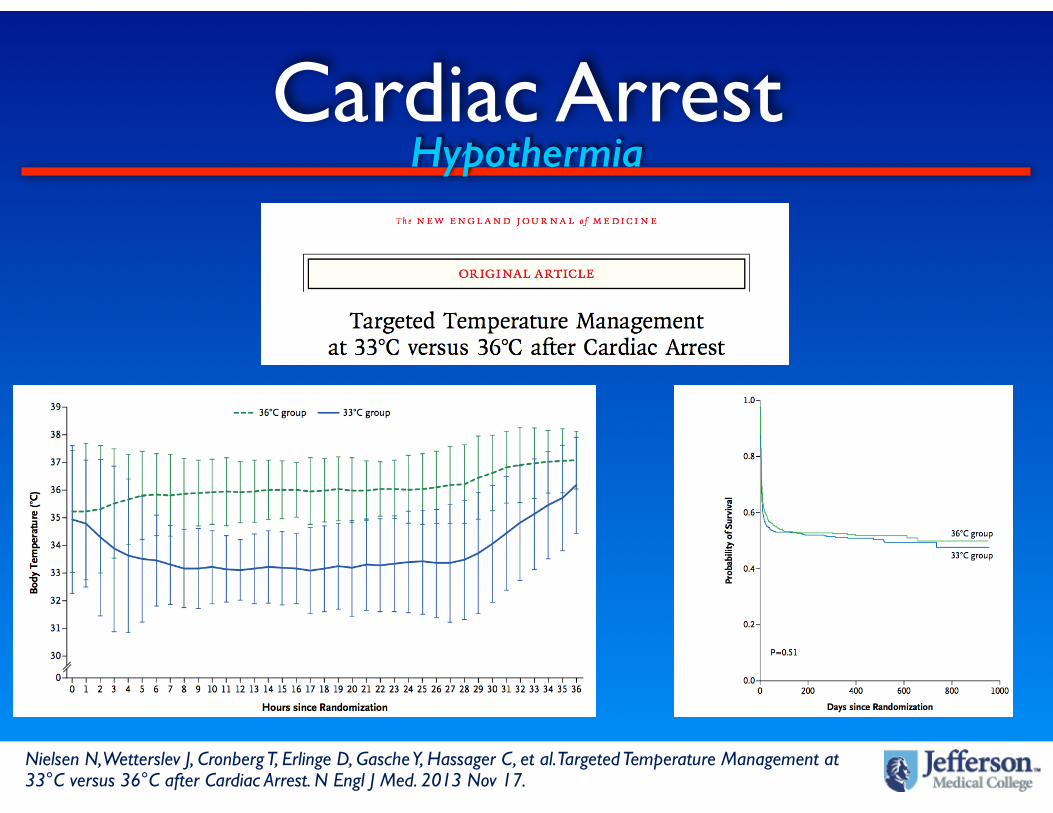
Cardiac ArrestHypothermia
Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, et al. Targeted Temperature Management at 33°C versus 36°C after Cardiac Arrest. N Engl J Med. 2013 Nov 17.

Traumatic Brain Injury

Traumatic Brain InjuryHypothermia

Traumatic Brain Injury
• No effect on outcome
• Significantly reduced ICP
• Increased rate of complications and LOS
N Engl J Med, Vol. 344, No. 8 · February 22, 2001
Hypothermia

Traumatic Brain Injury
Tukotomi T et al. Neurosurgery 52:102-112, 2003
Hypothermia
Traumatic Brain Injury
Polar RCT

Spinal Cord Injury

Spinal Cord Injury
Motor deficits in roedentsKakinohana. Anesthesiology 1999
Hypothermia

Ischemic Stroke
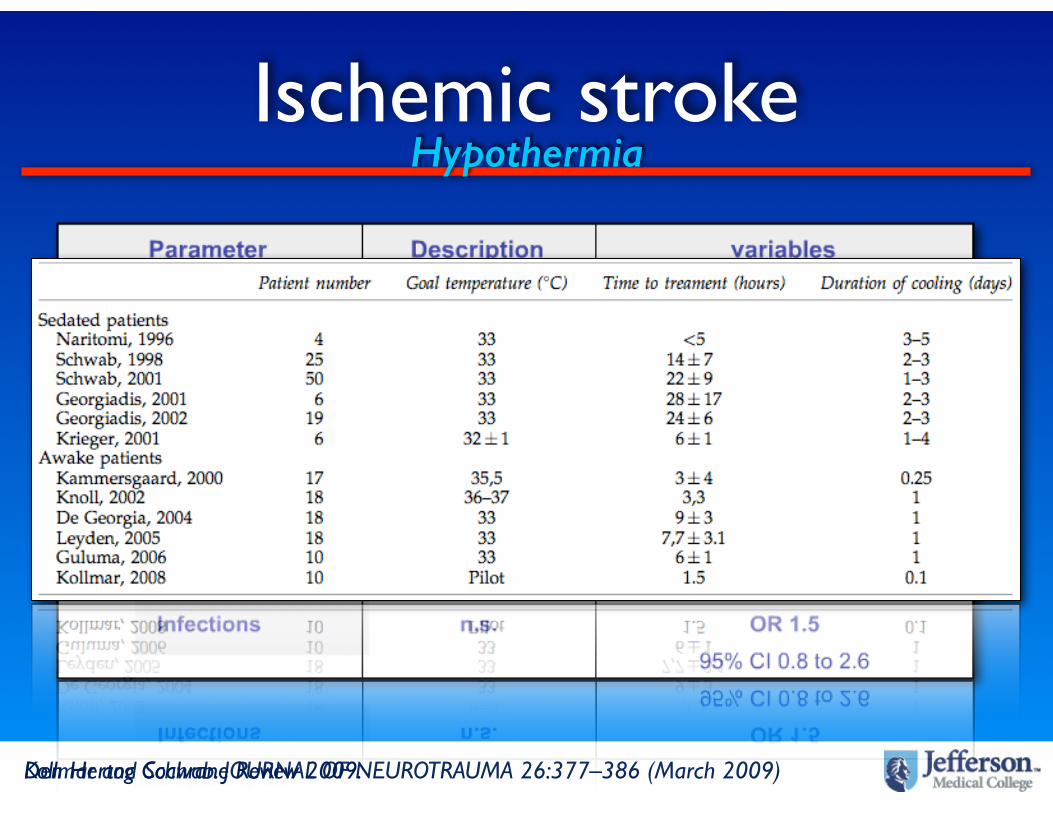
Ischemic stroke
Kollmar and Schwab. JOURNAL OF NEUROTRAUMA 26:377–386 (March 2009)Den Hertog Cochrane Review 2009.
Hypothermia

HypothermiaMalignant MCA Stroke
Schwab S et al. Stroke. 1998;29:2461-2466.
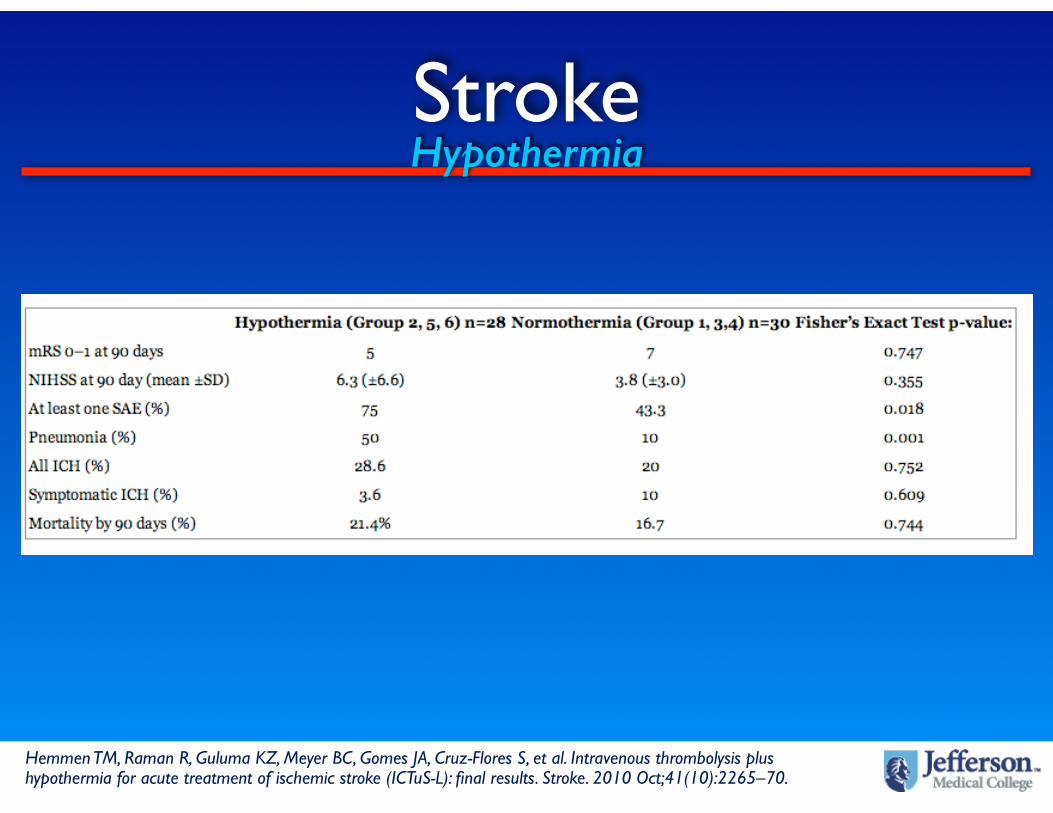
StrokeHypothermia
Hemmen TM, Raman R, Guluma KZ, Meyer BC, Gomes JA, Cruz-Flores S, et al. Intravenous thrombolysis plus hypothermia for acute treatment of ischemic stroke (ICTuS-L): final results. Stroke. 2010 Oct;41(10):2265–70.

Ischemic StrokeFever
Saini M et al. Stroke. 2009;40:00-00.

Ischemic Stroke
http://www.eurohyp.org
RECCLAIM STUDY: Endovascular Management and Cooling
ICH
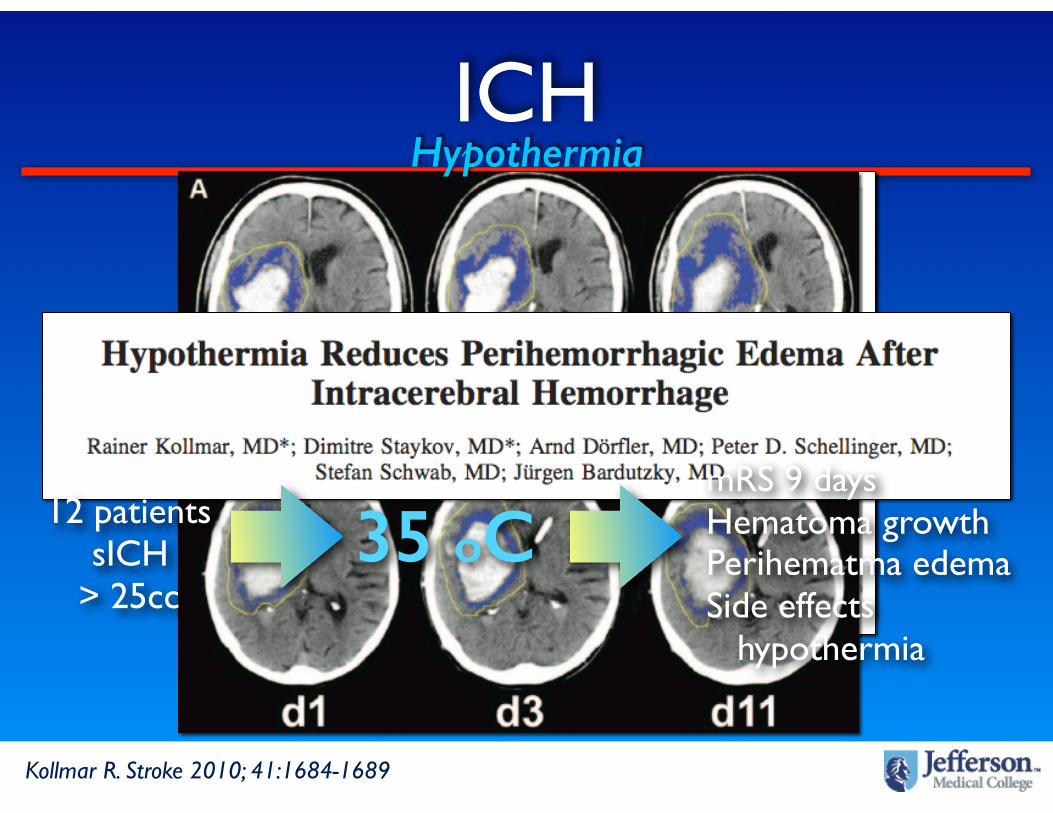
ICHHypothermia
Kollmar R. Stroke 2010; 41:1684-1689
35 oC mRS 9 daysHematoma growthPerihematma edemaSide effects hypothermia
12 patientssICH
> 25cc
ICH
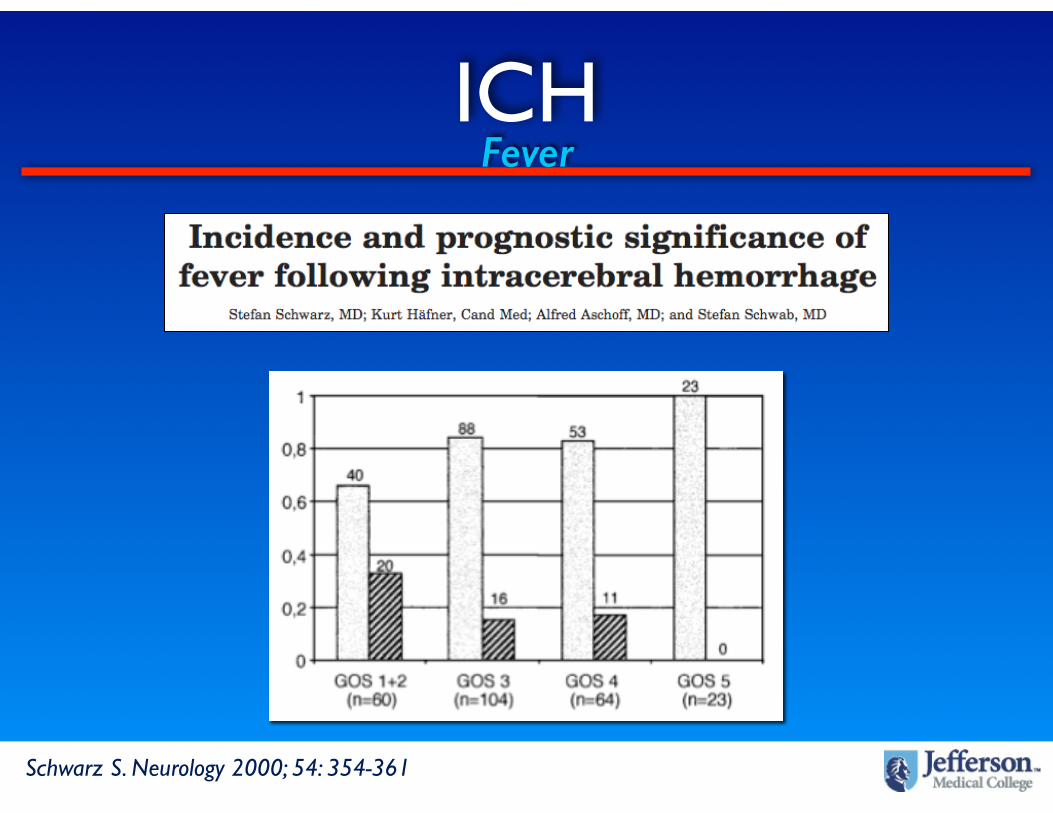
Schwarz S. Neurology 2000; 54: 354-361
Fever
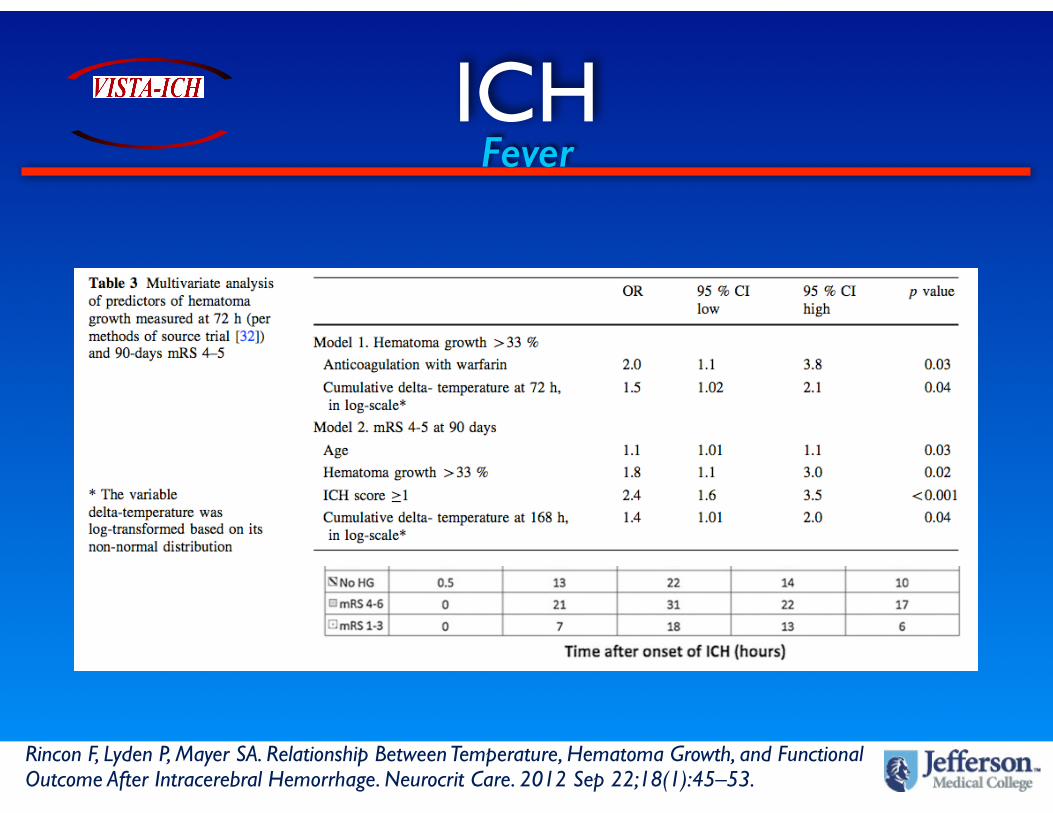
ICHFever
Rincon F, Lyden P, Mayer SA. Relationship Between Temperature, Hematoma Growth, and Functional Outcome After Intracerebral Hemorrhage. Neurocrit Care. 2012 Sep 22;18(1):45–53.

ICH
CINCH
TTM-ICHhttp://clinicaltrials.gov/ct2/show/NCT01607151
http://www.controlled-trials.com/ISRCTN28699995
SAH
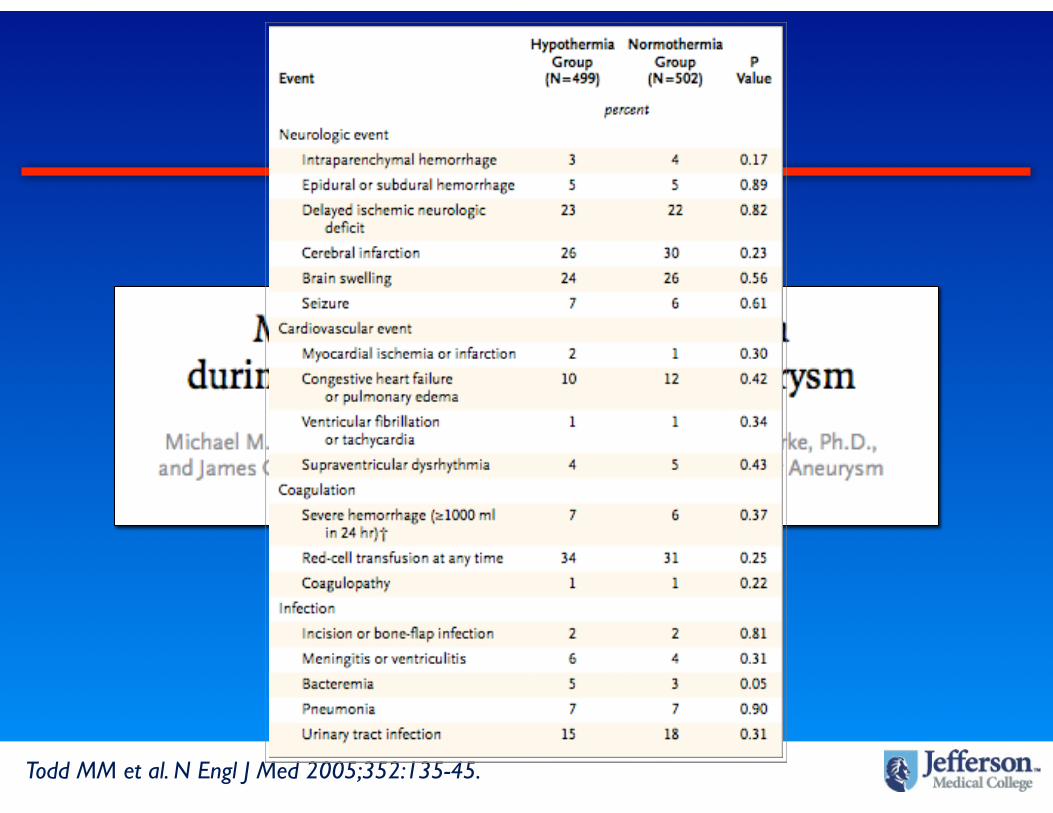
SAH
Todd MM et al. N Engl J Med 2005;352:135-45.
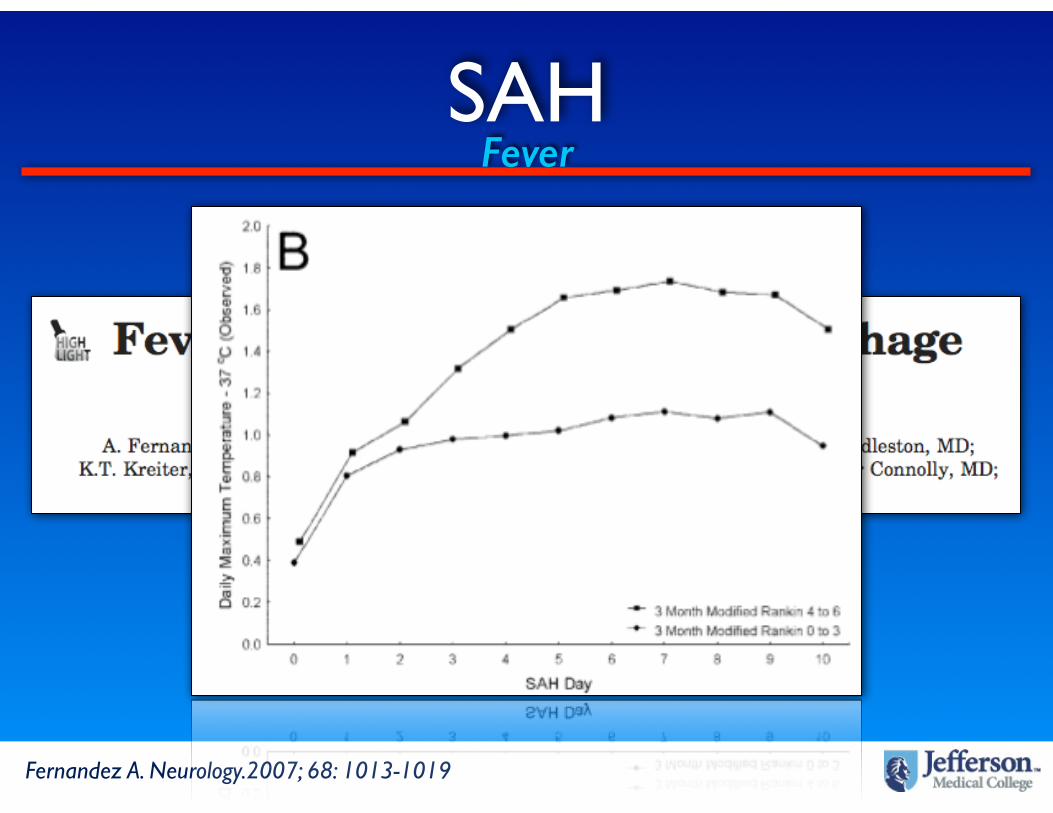
SAHFever
Fernandez A. Neurology.2007; 68: 1013-1019

• Jalan et al (Lancet 1999)
- 7 patients with ALF and intracranial hypertension + cerebral edema
- Moderate hypothermia
- ICP decreased from 45 to 16mmHg
- CPP increased from 45 to 70mmHg
- 3 patients bridged to transplant and all survived
Hepatic Encephalopathy

Hepatic Encephalopathy
Stravitz RT, Larsen FS. Therapeutic hypothermia for acute liver failure. Crit Care Med. 2009 Jul 1;37(Supplement):S258–64.

Status Epilepticus
Status Epilepticus
HYBERNATUS
http://clinicaltrials.gov/show/NCT01359332

Other applications
• Severe sepsis / septic shock
• ARDS
• Radio-contrast nephropathy
• Meningo-encephalitis
• Post-Cardiac surgery shock
• ACS/AMI

Brain InjuryFever
Greer DM. Stroke. 2008;39: 000
14,431

Brain InjuryFever
Rincon F et al. (Unpublished data)
Effect of Early Hyperthermia on Hospital Mortality in Critically-ill Neurological Patients

Brain InjuryFever
Rincon F et al. Significance of admission temperature and impact on mortality in critically-ill neurological patients. Critical Care 2011; 15(Suppl 1): P320 (11 March 2011).
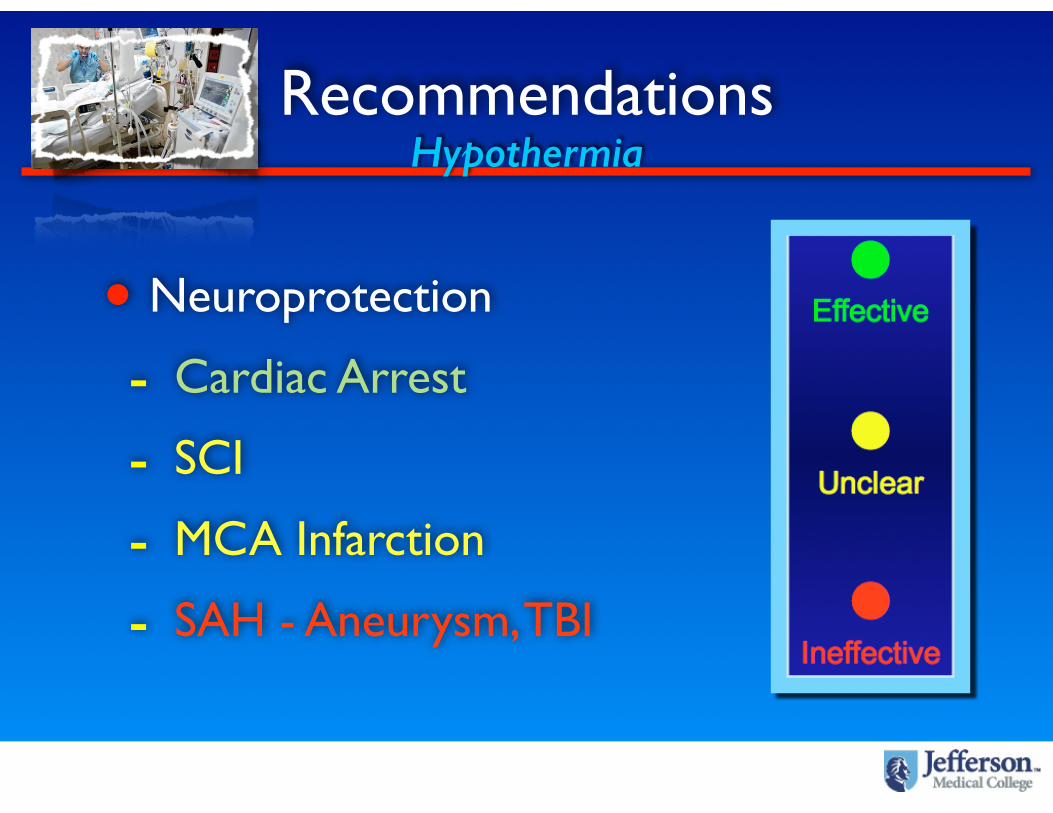
Recommendations
• Neuroprotection
- Cardiac Arrest
- SCI
- MCA Infarction
- SAH - Aneurysm, TBI
Hypothermia
Recommendations
• ICP and mass effect
- TBI?, Hepatic encephalopathy
- MCA infarction
Hypothermia

RecommendationsNormothermia
• Neuroprotection
- All brain injuries
Summary
• Experimental models suggest that hypothermia modulates multiple mechanisms in models of CCM related insults
• Clinical studies mainly in CA, SCI, and TBI (mainly animal) have shown some or clear evidence in clinical outcomes
• Survival after brain injury may depend on the brain remaining “Cool”

Acknowledgements
• Slide segments / portions
• D. Werner, Duke Medical Center
• P. Kochaneck, UPMC
• Sergio Zanotti, Cooper
• SCCM