teaching caregivers to implement speech-generating device
TRANSCRIPT
University of South FloridaScholar Commons
Graduate Theses and Dissertations Graduate School
October 2017
Teaching Caregivers to Implement Speech-Generating Device-Based Mand Training:Evaluating the Efficacy of Behavioral Skills TrainingRachel SubermanUniversity of South Florida, [email protected]
Follow this and additional works at: http://scholarcommons.usf.edu/etd
Part of the Social and Behavioral Sciences Commons
This Thesis is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in GraduateTheses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected].
Scholar Commons CitationSuberman, Rachel, "Teaching Caregivers to Implement Speech-Generating Device-Based Mand Training: Evaluating the Efficacy ofBehavioral Skills Training" (2017). Graduate Theses and Dissertations.http://scholarcommons.usf.edu/etd/7094

Teaching Caregivers to Implement Speech-Generating Device-Based Mand Training: Evaluating
the Efficacy of Behavioral Skills Training
by
Rachel Suberman
A thesis submitted in partial fulfillment of the requirements for the degree of
Master of Arts Department of Child and Family Studies
College of Behavioral and Community Sciences University of South Florida
Major Professor: Catia Cividini-Motta, PhD, BCBA-D Nicole McMillan, PhD, BCBA-D
Raymond Miltenberger, PhD, BCBA-D
Date of Approval: October 9, 2017
Key words: Applied behavior analysis, parent training
Copyright © 2017, Rachel Suberman
DEDICATION
I dedicate this thesis to my family, friends, teachers, and colleagues who displayed
tremendous support as I completed this project. I also dedicate this project to families who give
their children a voice when traditional means of spoken language are ineffective.
ACKNOWLEDGEMENTS
I would like to acknowledge Dr. Catia Cividini-Motta for her guidance and
encouragement throughout the process of completing this project. She has contributed to the field
of Applied Behavior Analysis in many ways and I thank her for her dedication to her students
and the field.

i
TABLE OF CONTENTS
List of Tables iii
List of Figures iv
Abstract v
Introduction 1
Method 6
Participants, Setting, and Materials 6
Measurement and Interobserver Agreement 6
Experimental Design 9
Procedure 9 Preference Assessment 9 Structured Observation 10 Baseline 10 Behavioral Skills Training 11 Behavioral Skills Training Assessment 11 Post Behavioral Skills Training Assessment 12 Behavioral Skills Training Booster Session 12 Post Behavioral Skills Training Booster Session Assessment 12 Generalization Probe 13
Results 14
Discussion 17
References 21
Tables and Figures 27
Appendices Appendix A: Task Analysis: Caregiver Implemented Mand Training Level 1 30 Appendix B: Task Analysis: Caregiver Implemented Mand Training Level 2 31 Appendix C: Task Analysis: Caregiver Implemented Mand Training Level 3a 32
ii
Appendix D: Treatment Integrity Checklist: BST, BST Booster Training Session 33 Appendix E: Treatment Integrity Checklist: Baseline, BST Assessment, Post-BST Assessment, Post-Booster Assessment 34 Appendix F: Social Validity Questionnaire 35 Appendix G: Paired Stimulus Preference Assessment Data Sheet 36 Appendix H: Structured Observation Procedures 38 Appendix I: Sample Script for Training Assistant 39

iii
LIST OF TABLES
Table 1: Child’s Highly Preferred Items 27

iv
LIST OF FIGURES
Figure 1: Percentage of steps correctly implemented during all phases across all caregivers 28
Figure 2: Percentage of independent mands emitted by each child during all phases of the study with each caregiver 29

v
ABSTRACT
Many individuals with developmental disabilities do not develop vocal repertoires. Thus,
teaching the use of an augmentative and alternative communication (AAC) device is imperative.
A speech-generating device (SGD) is an example of an AAC that is universally understood.
Individuals with developmental disabilities have been taught to communicate using such device.
Teaching caregivers to conduct communication training with their children may be one to way to
foster communication in an individual’s natural environment. Thus, the purpose of this study was
to extend previous research by using behavioral skills training (BST) to teach caregivers to
implement SGD-based mand training using an adapted training sequence. Additionally, we
evaluated whether training caregivers to implement mand training with their children resulted in
an increase of independent mands in their children. This study found that BST was effective in
teaching caregivers to implement SGD-based mand training with their children. Additionally,
independent mands increased from pre-training to post-training observations for two children.
Key words: caregiver training, mand training, Proloquo2Go™, speech-generating devices

1
INTRODUCTION
Approximately, 25% to 30% of individuals with autism spectrum disorders (ASD) are
likely to have deficits in communication (Lord & Jones, 2012). Those with a limited
communicative repertoire may engage in problem behavior to access social reinforcers, such as
preferred items or attention (see Beavers, Iwata, & Lerman, 2013 and Hanley, Iwata, & McCord,
2003 for reviews), thus impairing the individual’s independent functioning and social
development (Darrou et al., 2010). Despite the development of various teaching procedures to
promote vocal communication, many individuals with developmental disabilities do not acquire
functional vocal repertoires (National Research Council, 2001). Thus, the use of augmentative
and alternative communication (AAC) aids may be necessary (Durand, 1993; Mirenda, 2003).
Augmentative and alternative communication aids either enhance an individual’s current
vocal speech repertoire (i.e., augment), or act as the individual’s sole modality of communication
(i.e., alternative; Mirenda, 2003). Augmentative and alternative communication aids include
manual signs, picture exchange, and speech-generating devices (SGDs). Manual signs are
classified as a topography-based mode of communication as each manual sign is clearly unique
to the verbal response (Sundberg & Sundberg, 1990). Manual signs have also been referred to as
unaided communication modality (Mirenda, 2003). Many individuals have learned to
communicate using manual signs and some learners have indicated a preference for this
communication modality (Couper et al., 2014; van der Meer, 2012). Although an advantage of
manual signs is that the individual does not require extraneous materials to communicate
(Mirenda, 2003), one drawback is that few community members understand signs, thus limiting

2
the number of individuals with whom the person can communicate (Durand, 1993). In addition,
the need to modify signs due to the person’s limited motor skills can further restrict his or her
verbal community (Durand, 1993; Mirenda, 2003).
Picture exchange and SGDs are selection-based communication modalities (also referred
to as aided communication, Mirenda, 2003), as the learner’s physical response is the same (e.g.,
pointing to or exchanging a picture) for every verbal response (Sundberg & Sundberg, 1990).
Selection-based communication modalities involve the use of equipment (e.g., a picture book or
an electronic device) containing symbols representative of stimuli in the individual’s
environment (Bondy & Frost, 1994; Mirenda, 2003; Schlosser, 2003). Although picture
exchange and SGDs may be more easily understood than manual signs (Durand, 1993), both
communication modes require extraneous stimuli. Thus, they are dependent on the availability of
the communication aid.
To determine the most preferred and effective AAC modality, multiple studies have
compared acquisition and preference for AAC modalities. Results of studies have found that over
75% of participants preferred SGDs to manual signs (van der Meer et al., 2012), and over 88% of
participants preferred SGDs to both manual signs and picture exchange (Couper et al., 2014;
McLay et al., 2015). Additionally, results of some studies have indicated that acquisition of
SGDs required less teaching trials than manual signs (Achmadi et al., 2014; van der Meer et al.,
2012), or both manual signs and picture exchange (Couper et al., 2014). These results provide
support for teaching individuals to communicate using SGDs.
Speech-generating devices are found in a variety of platforms, ranging from modern
devices, such as smartphones and tablets, to equipment specifically designed for AAC voice
output functions, such as Dynavox® and GoTalk® (King et al., 2014; Shane et al., 2012).

3
However, devices such as Dynavox® and GoTalk® have been known to be heavy, expensive,
difficult to use, and stigmatizing for the user, potentially decreasing access and likelihood of use
(Shane et al., 2012). Due to advances in technology, household electronics such as iPads® and
smartphones can now be used as SGDs simply by downloading speech-generating applications.
These devices are less stigmatizing for the user (Durand, 1993; Shane et al., 2012), user friendly,
and more cost effective than the previous SGD models. Thus, leading to greater access and
potentially increased use (King et al., 2014; Kagohara et al., 2013; Shane et al., 2012).
Research has shown that individuals can be taught to use SGDs to emit a variety of
communicative responses including mands (e.g., King et al., 2014; Waddington et al., 2014; Xin
& Leonard, 2015), and intraverbals (e.g., Lorah et al., 2015; Waddington et al., 2014; Xin &
Leonard, 2015). Moreover, the acquisition of SGDs is sometimes associated with an increase in
vocal speech (e.g., Gevarter, et al., 2016; Kasari et al., 2014; Roche et al., 2014). In addition, a
variety of teaching procedures have been employed for teaching individuals to use SGDs such as
discrete trial training (DTT; e.g., King et al., 2014; Sigafoos et al. 2004), naturalistic training
(Sigafoos et al., 2004; Xin & Leonard, 2015), and an interrupted chaining procedure (Sigafoos et
al., 2013). However, behavior analysts usually are responsible for completing communication
training in clinics, schools, or homes, and during therapy hours. Thus limiting the opportunities
for the learner to practice using SGDs. In fact, parents are often not directly involved in language
interventions (Smith, 2011; Hong et al., 2016; U.S. Department of Education, 2014), which
potentially hinder the acquisition, maintenance, and generalization of AAC use. Furthermore,
Smith et al. (2011) suggested that training parents to promote their children’s communication
skills may result in a decrease in the children’s problem behavior.

4
Therefore, one potential way to promote communication acquisition in individuals with
developmental disabilities is to involve caregivers in communication training (Hong, Ganz,
Neely, Gerow, & Ninci, 2016). Limited studies have attempted to teach caregivers to facilitate
SGD-based communication in the natural environment (Hong et al., 2014; Sigafoos et al., 2004).
For instance, Sigafoos and colleagues (2004) taught three caregivers (i.e., mother, sister, and
family friend) to implement SGD-based mand training with an adolescent at home. In this study,
written and verbal descriptions of the target responses combined with observation of sessions
completed by the researchers was effective in training the caregivers to teach SGD-based
communicative responses to the adolescent. Similarly, Hong and colleagues (2014) trained four
caregivers to implement mand training with an adult SGD user through instructions, modeling,
and practice. In both studies caregivers learned to accurately implement SGD-based
communication training. However, the learner’s independent SGD-communication increased
after the caregivers learned to implement training in Sigafoos and colleagues, but not in Hong
and colleagues. Nevertheless, both studies only included one SGD user, used different teaching
procedures, and did not assess for generalization of the skills. Furthermore, only one study
assessed if caregiver training led to an increase in SGD use. Therefore, additional research in this
area is warranted.
A standardized training protocol that may be effective in teaching caregivers to
implement SGD-based mand training with their children is behavior skills training (BST).
Behavioral skills training employs instruction and modeling provided by an expert, rehearsal of
the skills by the learner, and feedback from the expert (e.g., Miltenberger et al., 2004; Sarokoff
& Sturmey, 2004). Behavioral skills training has been shown to be effective in training
caregivers a variety of skills including teaching parents to conduct functional assessments

5
(Shayne & Miltenberger, 2013) and teaching caregivers to implement pedestrian safety skills
training with their children (Harriage, Blair, & Miltenberger, 2016). Furthermore, BST has been
effective in teaching communication partners to correctly implement levels 1, 2, and 3 of the
Picture Exchange Communication System (PECS; Homlitas, Rosales, & Candel, 2014; Rosales,
Stone, & Rehfeldt 2009). Therefore, BST is likely to foster the caregivers’ acquisition of the
procedures involved in teaching children to mand using SGDs.
To date, there is limited research on procedures for teaching caregivers to conduct SGD-
based communication training with their children. Although previous research has employed
components of BST (e.g., modeling and rehearsal) when teaching caregivers to implement mand
training, the efficacy of BST in teaching caregivers to conduct SGD-based communication
training is unknown. Therefore, the purpose of this study was to extend previous research by
using BST to teach caregivers to implement SGD-based mand training using an adapted training
sequence.

6
METHOD
Participants, Setting, and Materials
Three caregiver-child dyads participated in the study. All children were diagnosed with
an ASD and communicated with a SGD consisting of an iPad® with Proloquo2Go™.
Participants were recruited from local ABA service providers in the Tampa area. Dyad 1
consisted of a 39-year-old female and her 9-year-old daughter. The child of dyad 1
communicated with manual signs and a SGD that she had for 2 years. At the time of enrollment
in the study, her caregiver reported that she often selected pictures of preferred items to request
her wants in the home. Dyad 2 consisted of a 35-year-old female and her 12-year-old son. The
child of dyad 2 communicated with manual signs and he had had a SGD for approximately 2
years. His caregiver reported that he rarely used his SGD in their home but that his therapists had
him practice communicating with the SGD during his ABA therapy. Dyad 3 consisted of a 42-
year-old female and her 10-year-old son. The child communicated with vocal approximations
and with his SGD, which he had used for approximately 6 months. His caregiver reported that he
rarely used his SGD in their home but that it was occasionally used in his classroom. None of the
caregivers had ever received formal SGD communication training. Sessions were conducted in
the caregivers’ homes.
Materials included a video camera to record sessions, an iPad® with the application
Proloquo2Go™ used during BST, printed instructions for implementing mand training, several
items identified as preferred for each of the participating children, and data sheets.
Measurement and Interobserver Agreement

7
The primary dependent measure was the percentage of steps implemented correctly on
the task analysis detailing the caregiver target responses for the adapted training sequence for
SGDs (Appendix A, B, C; Bondy & Frost, 1994; King et al., 2014). Each session consisted of
five trials and the task analysis was used to score caregivers’ performance during baseline, BST,
assessments, and probes. The percentage of correct steps was calculated by adding the number of
steps performed correctly, dividing it by the total number of applicable steps, and then
multiplying by 100%. Data were also collected on the duration (time spent in training) of BST.
Caregiver 1 spent 115 min in BST, caregiver 2 spent 130 min in BST and 45 min in BST
booster, and caregiver 3 spent 125 min in BST.
Data were also collected on mands emitted by the children throughout the structured
observation, baseline, and post BST assessments. These data were summarized as the percentage
of independent mands emitted by each child. An independent mand was defined for each child
based on his or her performance during baseline. An independent mand consisted of the child
independently selecting the correct picture sounding the item’s name on the device. Child 2 was
observed to repeatedly select the icon on the device. If this occurred, the caregiver was instructed
to not provide any consequence, remove access to device and continue to the next trial. A
prompted mand was defined as the child not emitting a response within 5 s to complete any part
of the mand sequence. An error was defined as the child emitting an incorrect response. During
the structured observation, an opportunity to mand consisted of any of the following: the child
requesting an item using any mode of communication (vocal, signs, iPad®, gestures), the
caregiver showing a preferred item to the child independently of whether the child then requested
the item using any mode of communication, and the child gaining access to an item without
requesting it.

8
Interobserver agreement was calculated for at least 33% of sessions for each caregiver-
child dyad across each of the assessments and phases. Graduate student observers were trained to
collect interobserver agreement and treatment integrity data by having them review and collect
data on a practice video until their data matched the data collected by the primary observer on at
least 80% of the trials. The observers independently scored sessions by directly observing the
session or by reviewing recorded footage of the sessions. Interobserver agreement was calculated
by totaling the number of agreements from each observer’s data sheet, dividing it by the total
number of agreements and disagreements, and multiplying by 100%.
Interobserver agreement was calculated for 44% of all sessions for dyad 1. Interobserver
agreement for dyad 1 was 98% for the preference assessment, 100% for the pre-training
structured observation, 99% (range 97%-100%) for baseline assessments, 94% (range 87% to
98%) for post-BST assessments, and 89% (range 80% to 97%) for generalization probes.
Interobserver agreement was calculated for 39% of all sessions for dyad 2. Interobserver
agreement for dyad 2 was 100% for the preference assessment, 100% for the pre-training
structured observation, 92% for baseline assessments (range 84% to 100%), 95% (range 92% to
98%) for post-BST assessments, 96% for post-booster BST assessments, and 87% for
generalization probes. Interobserver agreement was calculated for 41% of all sessions for dyad 3.
Interobserver agreement for dyad 3 was 100% for the preference assessment, 89% (range 86% to
94%) for baseline assessments, 92% (range 87% to 96%) for post-BST assessments, and 87% for
generalization probes.
Trained observers assessed treatment integrity by reviewing 33% of sessions across
caregivers. A treatment integrity checklist (Appendix D, E) was used to score session videos or
directly observe sessions. The checklist measured the researcher’s fidelity in implementing the

9
different phases of the study, including baseline, the components of behavioral skills training
such as providing instruction, modeling the correct responses, allowing the caregivers to rehearse
the skills, and providing feedback to the caregivers, post-BST assessments, and probes. The
treatment integrity score was calculated by totaling the number of steps performed correctly,
dividing it by the total number of steps, and multiplying by 100%. Treatment integrity was 100%
across all phases for dyads 1, 2 and 3.
A social validity questionnaire was administered to the caregivers at the end of the study
(Appendix F). The questionnaire contained four questions evaluating the caregivers’ opinions
about the study. Each question was answered using a 5-point Likert scale ranging from 1
(strongly disagree) to 5 (strongly agree). Caregivers 1 and 2 reported agreement or strong
agreement with each question on the social validity questionnaire.
Experimental Design
The experimental design was a nonconcurrent multiple baseline across participants with
generalization probes. The implementation of behavioral skills training was staggered across
caregivers upon stability of data during baseline.
Procedure
Preference assessment. A paired-stimulus preference assessment (Appendix G; Fisher
et al., 1992) was conducted with the participating children to identify preferred edible items
(child 1 and 2) and preferred tangible items (child 3). Prior to beginning the assessment, the
children were provided with a small piece of each edible item or allowed to interact with each
tangible item for up to 30 s. During the preference assessment the items were presented with
every other item once on the right side and once on the left side. During each trial the first item
reached towards by the child was scored as the selected item on that trial and the other item was

10
immediately removed from the table. If after 5 s of presenting the edible or tangible items, the
child had not made a selection, the items were removed for 5 s and the trial was represented a
second time. If on the second time the child did not make a selection, the trial was scored as no
response. The items selected in approximately 70% or more of trials were selected for mand
training. A list of the preferred items identified during the preference assessments was included
on the instructions for mand training presented to the caregivers.
Structured observation. A structured observation of the caregiver-child dyad was
conducted both pre- and post-BST to measure the frequency of independent mands emitted by
the child using his or her SGD (see Appendix H). Preferred items identified during the
preference assessment were within the child’s eyesight but out of reach to set the occasion for the
child to mand. In addition, the child’s SGD was available and functioning. Prior to beginning the
session, the child had the opportunity to use the restroom and the caregiver was instructed to
respond how they normally would to their child’s requests. At the beginning of the session, the
research assistant provided a general verbal prompt to the child (e.g., “if you want something,
please let us know”). Throughout the session, all mands (with or without iPad®) emitted by the
child resulted in access to the requested item. If at any point during the session the child independently accessed a
preferred item without requesting it, he or she was allowed to consume it or play with the item. Sessions continued until the child
had 10 opportunities to mand. The post-training session was conducted approximately 6 weeks
following the generalization probe conducted post-mastery of level 3a.
Baseline. During baseline, each caregiver was given a copy of the task analysis
(Appendix A, B, C) to review for 5 min. Then, they were instructed to demonstrate how they
would encourage their child to request preferred items using their SGD. Each caregiver’s
performance was scored across a session consisting of five trials. No feedback was provided to
caregivers during the baseline sessions.

11
Behavioral skills training. The steps of BST as described by Miltenberger and
colleagues (2004) were used to train caregivers to implement levels 1, 2, and 3a of the adapted
training sequence for SGD. The researcher first reviewed the correct implementation of the steps
of SGD-mand training and provided written instructions to the caregivers (see Appendix A, B,
C). The researcher then modeled the correct responses with a training assistant while the
caregiver observed. Training assistants were provided with a script (Appendix I) detailing their
performance during the role-play to ensure that the researcher had a chance to model the correct
caregiver response to each of the following potential child performances: independent responses,
responses requiring a gestural point, responses requiring full physical guidance, and incorrect
responses (i.e., selecting the picture of a neutral item). After the researcher modeled each
response, the caregivers were given the opportunity to rehearse the responses. Each response was
practiced at least once. If a step was performed incorrectly or the caregiver requested more
opportunities to rehearse, additional trials were conducted. The lead researcher provided positive
and corrective feedback to the caregiver after each trial. Once the caregiver had performed the
response to each scenario correctly in at least one trial, the researcher asked the caregiver if they
felt comfortable conducting these steps. If they stated they felt comfortable, no additional trials
were practiced and their performance was assessed. If they stated they wanted more practice, we
conducted more trials until they reported that they felt comfortable conducting the steps.
Behavioral skills training assessment. During each session of the BST assessment the
training assistant emitted each of the different potential responses at least once. If the caregiver
completed less than 90% of the steps correctly, additional BST training and BST assessment
sessions were completed until the caregiver met mastery criterion by scoring 90% in a session.
12
Post-behavioral skills training assessment. Following the mastery of implementation of
SGD mand training during BST, the researcher conducted an assessment to evaluate the
caregivers’ implementation of SGD mand training with their children. Items identified by the
preference assessment were available to the caregiver. Caregivers’ performances were evaluated
on at least three sessions. If the caregiver completed all steps correctly across the three sessions,
no additional sessions were completed. If the caregivers’ performances were variable but reached
90% on the last session, additional assessment sessions were completed. If the caregivers’
performances were on a decreasing trend, or stable but below 90%, a BST booster session was
conducted with their child in the natural environment followed by a post-BST booster
assessment sessions
Behavioral skills training booster session. During the BST booster session, the same
procedures outlined for BST were implemented. However, training included the caregiver’s child
instead of a training assistant. The lead researcher first discussed with the caregivers their
performance in the previous assessment sessions. Then, the BST components of instruction,
modeling, rehearsal, and feedback were completed until the caregiver correctly conducted the
different responses at least once and upon being asked, stated that she felt comfortable with the
steps.
Post-BST booster session assessment. Upon completion of a BST booster session, the
caregiver’s performance (caregiver 2 only) was reevaluated across three assessment sessions. If
the caregiver scored at least a 90% across three consecutive sessions, no additional sessions were
completed. If the caregiver’s performance was variable but reached 90% on the last session,
additional assessment sessions were completed. If the caregiver’s correct performance was on a
decreasing trend, or was stable but below 90%, additional booster sessions were conducted and

13
performance was reassessed. If necessary, this process continued until the caregiver scored 90%
across three consecutive sessions or for a maximum of 10 BST booster training sessions.
Generalization probe. To test for generalization of the caregivers’ skills, after meeting
mastery criterion during the assessment sessions, the dyads were observed in a novel setting. The
generalization probe consisted of one session following the same procedures as the post-BST
assessment. The generalization probe occurred approximately 1 week after completion of the
post-BST assessment for each level.

14
RESULTS
Table 6 displays the results from the preference assessments. Child 1’s highest preferred
edibles were Slim Jims®, Jimmy Dean® breakfast sausage, Li’l Smokies®, salami, bologna,
chocolate milk, and orange juice. Child 2’s highest preferred edibles were Pirate’s Booty®,
Veggie Straws®, Oreos®, Skittles®, and Rice Krispy Treats®. Child 3’s highest preferred
tangibles were train videos on his iPad, two dinosaur books, a light-up ball, and Bunchems®.
These items were included during all subsequent assessments as items the child could access
contingent on a mand.
Figure 1 depicts the caregivers’ performances during baseline and post-BST training
assessments sessions for levels 1, 2, and 3a of instruction. During baseline caregivers correctly
completed 75% or less of the steps for level 1 and 60% or less of the steps for levels 2 and 3a.
During the post-BST assessment sessions, caregivers completed at least 87% of the steps
correctly across all levels during post-BST assessments suggesting that BST was effective in
increasing their performance of SGD mand training. Finally, caregivers completed at least 80%
of the steps correctly during the generalization probes conducted in a novel setting.
Three baseline sessions were conducted for caregiver 1 for each level of instruction and
following BST caregiver 1 met mastery criteria for all three levels of SGD-based mand training.
Following BST, four post-BST assessments were conducted to demonstrate mastery criterion for
level 1, five for level 2, and three for level 3a. Generalization probes were conducted once
mastery criterion was reached for each level and this caregiver scored above 90% in all three

15
generalization probes conducted in a novel setting. Caregiver 1 spent 35 min in BST for level 1,
45 min for level 2, and 35 min for level 3a, totaling 115 min spent in BST.
Five baseline assessments were conducted for caregiver 2 for each level of instruction.
Caregiver 2 met mastery criterion for levels 1 and 3a following BST and three post-BST
assessment sessions were needed to demonstrate acquisition of these skills. Following BST,
however, caregiver 2’s performance of the steps for level 2 remained below criterion thus a
booster BST session was conducted for level 2. Following the booster BST session, caregiver 2
met mastery criterion for level 2. Caregiver 2 scored 90% in the generalization probe for level 1
and 95% in the generalization probe for levels 2 and 3a. Caregiver 2 spent 60 min in BST for
level 1, 65 min for level 2, 40 min for booster BST for level 2, and 45 min for level 3a totaling
210 min spent in BST for all levels.
Finally, seven baseline sessions were conducted for levels 1 and 3a, and eight sessions
were conducted for level 2 for caregiver 3. Following BST caregiver 3 met mastery criterion for
all three levels of SGD-based mand training and mastery of the skills was demonstrated in three
post-BST assessment sessions. Caregiver 3’s generalization probe scores were between 83% and
88%. Caregiver 3 spent 45 minutes in BST for level 1, 50 min for level 2, and 30 min for level 3a
totaling 125 min spent in BST for all levels.
Figure 2 depicts the percentage of independent mands emitted by each child throughout
all phases of the study. Child 1 emitted independent mands in less than 40% of the opportunities
across the structured observation pre-BST, baseline, post-BST assessments, and generalization
probes however independent manding increased to 80% of opportunities during the post-BST
structured observation. Child 2 emitted independent mands in less than 33% of the opportunities
across the structured observation pre-BST, baseline, post-BST assessments, and generalization

16
probes however during the structured observation post-BST he manded independently in 90% of
opportunities. Child 3 emitted independent mands in less than 33% of opportunities across the
initial structured observation, baseline, post-BST assessments, and generalization probes. The
post-BST structured observation has not been conducted for dyad 3. Overall, the data on
independent mands emitted by the children throughout all phases of the study show that
independent manding was low throughout the first five phases of the study and increased during
the structured observation conducted post-BST for child 1 and 2.

17
DISCUSSION
The current study evaluated the effectiveness of BST in teaching caregivers to conduct
mand training with their children who communicated with a speech generating device consisting
of an Ipad ® with Proloquo2Go™. The results of the study showed that following behavioral
skills training, caregivers correctly implemented mand training with their children. Additionally,
only one of the caregivers, caregiver 2, required a BST-booster session to learn to correctly
implement the mand training protocol. Finally, independent mands increased for child 1 and 2 as
observed during the structured observation completed following BST. These results are
consistent with previous research on BST and caregiver training that has shown that BST is
effective for teaching caregivers a variety of skills, such as how to conduct functional
assessments (Shayne & Miltenberger, 2013) and how implement discrete-trial teaching
(Lafasakis & Sturmey, 2007) and pedestrian safety skills with their children (Harriage et al.,
2016). However, the increase in independent mands observed during the final structured
observation was unexpected. Both child 1 and 2 emitted independent mands in over 80% of
opportunities during the post-BST structured observation even though responding during the
other phases of the study remained at levels similar to the pre-BST structured observation. Given
that the post-BST structured observation was conducted at least 6 weeks following the
completion of the post-BST assessment for level 3a, it is plausible that caregivers may have
continued to implement the mand training steps with their children, leading to an increase in
independent responding.

18
This study adds to previous research evaluating the effectiveness of BST in teaching
adults without behavioral analytic training to implement mand training. For instance, Rosales,
Stone, and Rehfeldt (2009) used BST to teach graduate students and Homlitas, Rosales, and
Candel (2014) taught teachers to implement mand training with individuals communicating
using PECS. Similarly, Sigafoos and colleagues (2004) and Hong and colleagues (2014)
successfully taught caregivers to implement mand training with an adolescent and an adult,
respectively, whose communication modality consisted of a SGD although these studies did not
use BST as the intervention. The current study, however, used BST to teach caregivers to
implement mand training with their child who communicated with SGDs. In addition in our
study the steps for mand training were adapted from the standardized PECS instructions (Bondy
& Frost, 1994). Our study thus replicates previous research using BST to teach adults to
implement mand training and extends previous research by being the first to use BST to teach
caregivers to implement SGD-based mand training with their children.
It is important to consider the variables responsible for the current results. Behavioral
skills training consists of instruction, modeling, rehearsal and feedback (e.g., Miltenberger et al.,
2004; Sarokoff & Sturmey, 2004). During baseline, the caregivers were provided with the
instructions yet access to instructions alone did not result in mastery of the skills thus suggesting
that modeling, rehearsal, and/or feedback was necessary. Previous studies have used components
of BST to teach caregivers to implement SGD-based mand training. For instance, Sigafoos and
colleagues (2004) employed instruction and modeling in their training which resulted in
caregivers successfully implementing the mand training steps with their child. Additionally,
Hong and colleagues (2014) used instructions, modeling, and practice to effectively teach
caregivers SGD-based mand training. Thus it is possible that in the current study caregivers may
19
have acquired the skills through modeling alone or modeling plus rehearsal however because we
evaluated BST we can not draw any conclusions about the efficacy each of its components alone.
Furthermore, each child’s history with a SGD may have impacted the results. All children
had access to an SGD but only child 1 and 2 received ABA therapy. According to caregivers
each of the children used their SGD at least occasionally at school or the clinic where the child
was receiving services. Thus it is possible that the children could use their SGD to communicate
but did not do so at home, yet by experiencing mand training in the home setting the skills they
had previously acquired generalized to this new setting. Future research should assess children’s
skills across settings and consider selecting children whose manding repertoire is limited across
all settings.
Additional limitations of the current study must be discussed. First, caregivers were
instructed on how to implement the adapted steps of mand training for levels 1, 2 and 3a. The
steps of mand training included instructions on how to arrange the environment, entice with a
preferred item, prompt the child to mand, and reinforce the child’s correct response. These steps
did not include procedures for collecting data, evaluating progress, introducing new items, fading
prompts, and providing differential reinforcement for prompted and independent responses.
However the purpose of the study was to evaluate the effects of BST on teaching caregivers to
implement mand training. Although we did not teach all of the steps, given that BST was
effective in teaching caregivers the target skills selected for this study, it is likely that BST would
result in the acquisition of these other responses as well. Second, the steps of mand training did
not include specific guidelines for addressing problem behavior. Anecdotally, problem behavior
in the form of aggression occurred in almost every session for child 2 and 3. We instructed the
caregivers to follow their child’s clinical program in effect at the beginning of this study. If these

20
were nonexistent, we instructed the caregivers to follow best practice procedures (e.g., minimal
attention, redirection to the task). Anecdotal observation suggests that at least in some cases
caregiver performance was lower during sessions in which their child engaged in problem
behavior. Thus future research should consider incorporating steps for addressing problem
behavior that occurs during sessions. Third, we did not collect maintenance data on the
caregiver’s performance and generalization data were only collected across settings. Future
research should consider assessing maintenance and also variables that may impact long term
maintenance of the skills taught to caregivers. Finally, caregiver 3 scores decreased during the
generalization probe, possibly because we did not incorporate common stimuli, other than the
preferred items, between training and generalization settings (Miltenberger, 2012). Future
research should ensure that procedures selected for training are likely to lead to acquisition,
generalization, and maintenance of the skills. This could be accomplished by teaching across
multiple stimuli in the training environment, ensuring the training incorporates common stimuli
from the natural environment, or incorporating stimulus situations that may occur in the natural
environment (Miltenberger, 2012).
In conclusion, this study provides evidence that caregivers can learn to conduct mand
training with their children who use a SGD to communicate. The intervention also led to an
increase in independent mands from the child. This study adds to the body of research on mand
training, BST, and SGD-based communication.

21
REFERENCES
Achmadi, D., Sigafoos, J., van der Meer, L., Sutherland, D., Lancioni, G. E., … Marschick, P. B.
(2014). Acquisition, preference, and follow-up data on the use of three AAC options by
four boys with developmental disability/delay. Journal of Developmental and Physical
Disabilities, 26, 565-583.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders.
(5th ed.). Arlington VA: American Psychiatric Publishing.
Beavers, G. A., Iwata, B. A., & Lerman, D. C. (2013). Thirty years of research on the functional
analysis of problem behavior. Journal of Applied Behavior Analysis, 46, 1–21.
Bondy, A., & Frost, L. (1994). The picture exchange communication systems. Focus on
Autistic Behavior, 9, 1-19.
Calculator, S., & Dollaghan, C. (1982). The use of communication boards in a residential setting.
Journal of Speech and Hearing Disorders, 14, 281-287.
Couper, L., van der Meer, L., Schafer, M. C. M., McKenzie, E., McLay, L., O’Reilly, M.
F., … Sutherland, D. (2014). Comparing acquisition of a preference for manual signs,
picture exchange, and speech-generating devices in nine children with autism spectrum
disorder. Journal of Developmental Neurorehabilitation, 17, 99-109.
Darrou, C., Pry, R., Pernon, E., Michelon, C., Aussilloux, C., & Baghdadli, A. (2010). Outcome
of young children with autism: Does the amount of intervention influence developmental
trajectories? Sage Publications and the National Autistic Society, 14, 663-677.
Durand, V. M. (1993). Functional communication training using assistive devices: Effects on

22
challenging behavior and affect. AAC Augmentative and Alternative Communication, 9,
168-176.
Fisher, W. W., Piazza, C. C., Bowman, L. G., Hagopian, L. P., Owens, J. C., & Slevin, I.
(1992). A comparison of two approaches for identifying reinforcers for persons with
severe and profound disabilities. Journal of Applied Behavior Analysis, 25, 491-498.
Gevarter, C., O’Reilly, M. F., Kuhn, M., Mills, K., Ferguson, R., Watkins, L., … Lancioni, G.
E. (2016). Increasing the vocalizations of individuals with autism during intervention
with a speech-generating device. Journal of Applied Behavior Analysis, 49, 17-33.
Hanley, G. P., Iwata, B. A., & McCord, B. E. (2003). Functional analysis of problem behavior: A
review. Journal of Applied Behavior Analysis, 36, 147–185.
Harriage, B., Blair, K.C., & Miltenberger, R. (2016). An evaluation of parent
implemented in situ pedestrian safety skills intervention for individuals with autism.
Journal of Autism and Developmental Disorders, 46, 2017-2027.
Homlitas, C., Rosales, R., & Candel, L. (2014). A further evaluation of behavioral skills training
for implementation of the Picture Exchange Communication System. Journal of Applied
Behavior Analysis, 47, 198-203.
Hong, E. R., Ganz, J. B., Gilliland, W., & Ninci, J. (2014). Teaching caregivers to implement an
augmentative and alternative communication intervention to an adult with ASD.
Research in Autism Spectrum Disorders, 8, 570-580.
Hong, E. R., Ganz, J. B., Neely, L., Gerow, S., & Ninci, J. (2016) A review of the quality
of primary caregiver-implemented communication intervention research for children with
ASD. Research in Autism Spectrum Disorders, 25, 122-136
Kagohara, D. M., van der Meer, L., Ramdoss, S., O’Reilly, M. F., Lancioni, G. E., ... Sigafoos,

23
J. (2013). Using iPods and iPads in teaching programs for individuals with developmental
disabilities: A systematic review. Research in Developmental Disabilities, 34, 147–156.
Kasari, C., Kaiser, A., Goods, K., Nietfeld, J., Mathy, P., Landa, R., … Almirall, D. (2014).
Communication interventions for minimally verbal children with autism: A sequential
multiple assignment randomized trial. Journal of the American Academy of Child and
Adolescent Psychiatry, 53, 635-646.
King, M. L., Takeguchi, K., Barry, S. E., Rehfeldt, R. A., Boyer, V. E., & Mathews, T. L.
(2014). Evaluation of the iPad in the acquisition of requesting skills for children with
autism spectrum disorder. Research in Autism Spectrum Disorders, 8, 1107-1120.
Lafasakis M. & Sturmey, P. (2007). Training parent implementation of discrete-trial teaching:
Effects on generalization of parent teaching and child correct responding. Journal of
Applied Behavior Analysis, 40, 685-689.
Lorah, E. R., Karnes, A., & Speight, D. R. (2015). The acquisition of intraverbal responding
using a speech generating device in school aged children with autism. Journal of
Developmental and Physical Disabilities, 27, 557-568.
Lord, C. & Jones, R. M. (2012). Annual Research Review: Re-thinking the classification of
autism spectrum disorders. Journal of Child Psychology and Psychiatry, 53, 490-509.
McLay, L., van der Meer, L., Schafer, M. C. M., Couper, L., McKenzie, E., O’Reilly, M.
F., … Sutherland, D. (2015). Comparing acquisition, generalization, maintenance, and
preference across three AAC options in four children with autism spectrum disorder.
Journal of Developmental and Physical Disabilities, 27, 323-339.
Miltenberger, R. G. (2012). Behavior modification: Principles and procedures (5th ed,). Boston,
MA: Wadsworth Publishing.

24
Miltenberger, R. G., Flessner, C., Gatheridge, B., Johnson, B., Satterlund, M., & Egemo,
K. (2004). Evaluation of behavioral skills training procedures to prevent gun play in
children. Journal of Applied Behavior Analysis, 37, 513-516.
Mirenda, P. (2003). Toward functional augmentative and alternative communication for students
with autism: Manual signs, graphic symbols and voice output communication aids.
Language, Speech, and Hearing Services in Schools, 34, 203-216.
National Research Council. (2001). Educating children with autism. Washington, DC: National
Academy Press.
Roche, L., Sigafoos, J., Lancioni, G. E., O’Reilly, M. F., Schlosser, R. W., Stevens, M.,
… Marschik, P. B. (2014). An evaluation of speech production in two boys with
neurodevelopmental disorders who received communication intervention with a speech-
generating device. International Journal of Developmental Neuroscience, 38, 10-16.
Rosales, R., Stone, K., & Rehfeldt, R. A. (2009). The effects of behavioral skills training
on implementation of the picture exchange communication system. Journal of Applied
Behavior Analysis, 42, 541-549.
Sarokoff, R. A. & Sturmey, P. (2004). The effects of behavioral skills training on staff
implementation of discrete-trial teaching. Journal of Applied Behavior Analysis, 37, 535-
538.
Schlosser, R. (2003). Roles of speech output in augmentative and alternative communication:
Narrative review. AAC: Augmentative and Alternative Communication, 19, 5–27.
Sigafoos, J., Lancioni, G. E., O’Reilly, M. F., Achmadi, D., Stevens, M., … Green, V. A.

25
(2013). Teaching two boys with autism spectrum disorders to request the continuation of
toy play using an iPad®-based speech-generating device. Research in Autism Spectrum
Disorders, 7, 923-930.
Sigafoos, J., O’Reilly, M. F., Seely-York, S., Weru, J., Son, S. H., Green V. A., &
Lancioni, G. E. (2004). Transferring AAC intervention to the home. Journal of Disability
and Rehabilitation, 26, 1330-1334.
Shane, H. C., Laubscher, E. H., Schlosser, R. W., Flynn, S., Sorce, J. F., & Abramson, J. (2012).
Applying Technology to Visually Support Language and Communication in Individuals
with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 42,
1228-1235.
Shayne, R. & Miltenberger, R. G. (2013). Evaluation of behavioral skills training for
teaching functional assessment and treatment selection skills to parents. Behavioral
Interventions, 28, 4-21.
Smith, A. L., Romski, M. A., Sevcik, R. A., Adamson, L. B., & Bakeman, R. (2011).
Parent stress and its relation to parent perceptions of communication following coached
language intervention. Journal of Early Intervention, 33, 135-150.
Sundberg, C. T. & Sundberg, M. L. (1990). Comparing topography-based verbal behavior with
stimulus selection-based verbal behavior. The Analysis of Verbal Behavior, 8, 31-41.
Sundberg, M. L. & Partington, J. W. (1998). Teaching language to children with autism
or other developmental disabilities. Pleasant Hill, CA: Behavior Analysts Inc.
U.S. Department of Education, Office of Special Education and Rehabilitative Services, Office

26
of Special Education Programs (2014). 36th Annual Report to Congress on the
Implementation of the Individuals with Disabilities Education Act, (1). Washington, DC:
Author.
van der Meer, L., Kagohara, D., Achmadi, D., O’Reilly, M. F., Lancioni, G., … Sigafoos,
J. (2012). Speech-generating devices versus manual signing for children with
developmental disabilities. Research in Developmental Disabilities, 33, 1658-1669.
Waddington, H., Sigafoos, J., Lancioni, G. E., O’Reilly, M. F., van der Meer, L., Carnett, A.,
… Marschik, P. B. (2014). Three children with autism spectrum disorder learn to perform
a three-step communication sequence using an iPad-based speech-generating device.
International Journal of Developmental Neuroscience, 39, 59-67.
Xin, J. F. & Leonard, D. A. (2015). Using iPads to teach communication skills of
students with autism. Journal of Autism and Developmental Disorders, 45, 4154-416

27
Table 1 Child’s Highly Preferred Items
Child 1 Child 2 Child 3 Li’l Smokies Oreos Bunchems Orange Juice Skittles Train Videos Jimmy Dean Sausage Pirate’s Booty Orange and Blue Light Up Ball Chocolate Milk Rice Krispie Treats Dinosaur Pop-Up Book Salami Veggie Straws Dinosaur Safari Book Bologna

28
Figure 1. Percentage of steps correctly implemented during all phases across all caregivers.

29
Figure 2. Percentage of independent mands emitted by each child during all phases of the study with each caregiver. BST-booster was only necessary for Caregiver 2 thus data on mands is for that assessment is only available for Child 2.

30
Appendix A Task Analysis: Caregiver Implemented Mand Training Level 1
Description
Trial 1 Trial 2 Trial 3 Trial 4 Trial 5
Pre-Session
1. Ensure materials are ready (iPad is functioning, preferred edibles are available, pictures of preferred edibles are programmed in iPad)
Session
2. Place preferred item out of child’s reach but within eyesight
3. Place iPad next to child
4. Stand/sit next to child
5. Hold (entice) item in front of child until child looks at or reaches for item
6. If child independently selects picture of desired item within 5 s of previous step: a. Vocally state name of item and praise (e.g., “good job”) b. Provide larger piece of edible item to child/approximately 20-30 s access to item
7. If child has not pressed icon within 5 s of step 5: a. Provide gestural prompt (e.g., point) towards icon on iPad b. If no response within 5 s after gestural prompt, physically prompt by using hand over hand
guidance to press icon
c. Vocally state the name of the item d. Provide small piece of edible after prompted response or approximately 5 s of access to item
TOTAL SCORE Child response per trial
PREFERRED ITEMS:
31
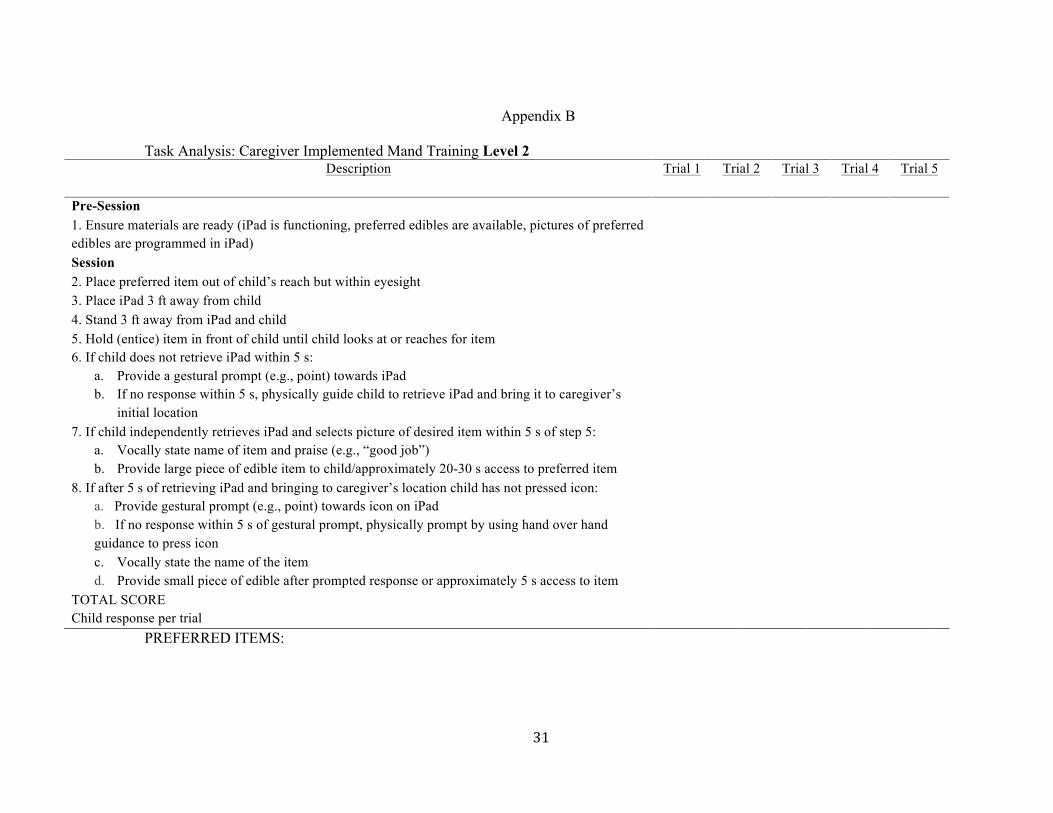
Appendix B Task Analysis: Caregiver Implemented Mand Training Level 2
Description
Trial 1 Trial 2 Trial 3 Trial 4 Trial 5
Pre-Session 1. Ensure materials are ready (iPad is functioning, preferred edibles are available, pictures of preferred edibles are programmed in iPad)
Session 2. Place preferred item out of child’s reach but within eyesight 3. Place iPad 3 ft away from child 4. Stand 3 ft away from iPad and child 5. Hold (entice) item in front of child until child looks at or reaches for item 6. If child does not retrieve iPad within 5 s:
a. Provide a gestural prompt (e.g., point) towards iPad b. If no response within 5 s, physically guide child to retrieve iPad and bring it to caregiver’s
initial location
7. If child independently retrieves iPad and selects picture of desired item within 5 s of step 5: a. Vocally state name of item and praise (e.g., “good job”) b. Provide large piece of edible item to child/approximately 20-30 s access to preferred item
8. If after 5 s of retrieving iPad and bringing to caregiver’s location child has not pressed icon: a. Provide gestural prompt (e.g., point) towards icon on iPad b. If no response within 5 s of gestural prompt, physically prompt by using hand over hand guidance to press icon
c. Vocally state the name of the item d. Provide small piece of edible after prompted response or approximately 5 s access to item
TOTAL SCORE Child response per trial
PREFERRED ITEMS:

32
Appendix C Task Analysis: Caregiver Implemented Mand Training Level 3a
Description Trial 1 Trial 2 Trial 3 Trial 4 Trial 5 Pre-Session 1. Ensure materials are ready (iPad is functioning, preferred edibles are available, pictures of preferred edibles and neutral items are programmed in iPad)
Session 2. Place preferred item out of child’s reach but within eyesight 3. Place iPad 3 ft away from child 4. Stand 3 ft away from iPad and child 5. Hold (entice) item in front of child until child looks at or reaches for item 6. If child does not retrieve iPad within 5 s:
a. Provide a gestural prompt (e.g., point) towards iPad b. If no response within 5 s, physically guide child to retrieve iPad and bring it to caregiver’s
initial location
7. If child independently retrieves iPad and selects picture of desired item within 5 s of step 5: a. Vocally state name of item and praise (e.g., “good job”) b. Provide large piece of edible item to child/approximately 20-30 s access to item
8. If after 5 s of retrieving iPad and bringing to caregiver’s location child has not pressed icon: a. Provide gestural prompt (e.g., point) towards icon on iPad b. If no response within 5 s of gestural prompt, physically prompt by using hand over hand
guidance to press icon
c. Vocally state the name of the item d. Provide small piece of edible after prompted response or 5 s access to item 9. If child selects picture of incorrect item, vocally state “no, we don’t have that” and use hand over hand guidance to prompt child to press correct item
10. Do not provide edible item if incorrect picture chosen TOTAL SCORE Child Response
PREFERRED ITEMS:

33
Appendix D Treatment Integrity Checklist: BST, BST Booster Training Session
Step Description Trial 1 Trial 2 Trial 3 Trial 4 Trial 5
1. Materials present iPad, data sheets, designated “preferred items”/children’s preferred items
2. Materials set up Items at least 3 ft away
3. Researcher provides written instruction
TA provided to caregiver
4. Researcher provides verbal instruction
Verbal review of TA
5. Researcher model trial Researchers implement a trial with the training assistant per the steps of the TA while the
caregiver observes
6. Research instructs caregiver to practice responses
7. Caregiver practices trial With training assistant or child 8. Researcher provides
feedback on performance Researcher reviews with caregiver all steps
implemented correctly and incorrectly
9. Caregiver asked if he/she wants more practice
10. Caregiver given more practice trials
11. Researcher reviews performance in previous assessment
TOTAL SCORE

34
Appendix E
Treatment Integrity Checklist: Baseline, BST Assessment, Post-BST Assessment, Post-Booster Assessment, Generalization Probe
Step Description Trial 1 Trial 2 Trial 3 Trial 4 Trial 5
1. Materials present 1a. iPad functioning
1b. TA 1c. Data sheets 1d. Preferred items 1e. Timer
TA present during baseline only
2. Materials set up 2a. Preferred items 2b. Researcher has data sheets, pen
At least 3 ft from child
3. Researcher provides TA for 5 min 3a. Researcher sets timer 3b. Researcher removes TA
Given to caregiver; TA for level being assessed; only baseline
After 5 min
4. Researcher provides instruction States “encourage you child to request preferred item”
5.
Researcher scores performance Using appropriate TA
6. No feedback provided Researcher does not discuss caregiver performance
TOTAL SCORE

35
Appendix F
Social Validity Questionnaire 1. I enjoyed learning how to help my child communicate with his or her iPad.
1 2 3 4 5 Strongly Disagree Disagree Neutral Agree Strongly Agree 2. I am going to use the skills I learned in the training with my child.
1 2 3 4 5 Strongly Disagree Disagree Neutral Agree Strongly Agree 3. I think that these communication training procedures will improve my child’s communication.
1 2 3 4 5 Strongly Disagree Disagree Neutral Agree Strongly Agree 4. After training I feel comfortable implementing communication training with my child.
1 2 3 4 5 Strongly Disagree Disagree Neutral Agree Strongly Agree 5. I would recommend this training to other parents whose children use iPads to communicate.
1 2 3 4 5 Strongly Disagree Disagree Neutral Agree Strongly Agree

36
Appendix G
Paired Stimulus Preference Assessment Data Sheet
StimulusItems: OverallRank(highest%is#1)1. 2. 3. 4. 5. 6. 7. 8.
Treatment Integrity
Trial
Items (Response)
Correct item placement
Researcher stated
“choose one”
Non-selected
item removed
after selection
If no response
within 5 s, re-present
items
If no response
after second presentation
, score as no response
(NR)
If both items
selected, block and re-present
items/instruction
1 7 8 NR 2 4 6 NR 3 5 7 NR 4 7 3 NR 5 6 8 NR 6 2 3 NR 7 1 8 NR 8 3 4 NR 9 8 6 NR
10 2 1 NR 11 7 4 NR 12 5 1 NR 13 1 4 NR 14 6 3 NR 15 2 6 NR 16 2 4 NR 17 5 8 NR 18 4 1 NR 19 5 6 NR 20 4 2 NR 21 8 7 NR 22 7 2 NR 23 1 6 NR 24 6 1 NR 25 1 3 NR

37
26 3 7 NR 27 7 1 NR 28 6 7 NR 29 1 2 NR 30 3 1 NR 31 1 7 NR 32 5 3 NR 33 2 8 NR 34 8 4 NR 35 3 2 NR 36 6 2 NR 37 7 6 NR 38 8 1 NR 39 3 5 NR 40 1 5 NR 41 8 3 NR 42 4 8 NR 43 8 2 NR 44 4 5 NR 45 4 3 NR 46 5 2 NR 47 3 6 NR 48 6 4 NR 49 5 4 NR 50 4 7 NR 51 7 5 NR 52 2 5 NR 53 8 5 NR 54 3 8 NR 55 6 5 NR 56 2 7 NR

38
Appendix H Structured Observation Procedures
Description Pre-session 1 2 3 4 5 6 7 8 9 10 Pre-Session
1. Ensure iPad is available and functioning
2. Ensure at least 10 preferred items are within child’s eyesight but at least 3 ft from child
3. Ensure child has had opportunity to use restroom (e.g., verbally offer bathroom to child; walk child to bathroom door and offer access)
Session 4. RA vocally prompt caregiver to
respond as he/she normally would to child’s manding
5. RA provides general vocal prompt to child (e.g., “if you want something please let me know”)
6. RA starts timer a. RA only stops timer after child
has 10 mand opportunities or child requests restroom
b. RA restarts timer after child returns from bathroom
7. If child independently mands for item on iPad, provide small amount of edible or 1 min access to tangible a. Score as independent mand
8. If after 2 min with no mand opportunity, RA prompts caregiver to show item for 5 s to child a. If child responds after prompt,
deliver small amount of edible or 1 min of access to tangible
b. Score as prompted mand 9. If child does not respond within 1 min
of caregiver prompt, score as no response
Child Response

39
Appendix I
Sample Script for Training Assistant Session 1: Researcher modeling caregiver observes 1. Independently touch correct icon on iPad to sound name of desired item 2. Require physical guidance (HH) to touch correct icon on iPad 3. Require gestural point to touch correct icon on iPad 4. Require physical guidance (HH) to touch correct icon on iPad 5. Independently touch INCORRECT icon on iPad Session 2: Alternating between researcher modeling and caregiver practicing 6. Require physical guidance (HH) to touch correct icon on iPad Caregiver practice & receives feedback 7. Require gestural point to touch correct icon on iPad Caregiver practice & receives feedback 8. Independently touch correct icon on iPad Caregiver practice & receives feedback 9. Independently touch INCORRECT icon on iPad Caregiver practice & receives feedback 10. Require gestural point to touch correct icon on iPad Caregiver practice & receives feedback Session 3: Alternating between researcher modeling and caregiver practicing 11. Require gestural point to touch correct icon on iPad Caregiver practice & receives feedback 12. Independently touch correct icon on iPad Caregiver practice & receives feedback 13. Require physical guidance (hand-over-hand) to touch correct icon on iPad Caregiver practice & receives feedback 14. Independently touch INCORRECT icon on iPad Caregiver practice & receives feedback 15. Require gestural point to touch correct icon on iPad Caregiver practice & receives feedback BST assessment (to terminate BST) no feedback for caregiver1. Require shoulder prompt to touch correct icon on iPad 2. Require forearm prompt to touch correct icon on iPad 3. Independently touch correct icon on iPad to sound name of desired item 4. Require hand over hand prompt to touch correct icon on iPad 5. Independently touch INCORRECT icon on iPad 6. Independently touch correct icon on iPad to sound name of desired item 7. Require shoulder prompt to touch correct icon on iPad 8. Independently touch INCORRECT icon on iPad 9. Require forearm prompt to touch correct icon on iPad 10. Require hand over hand prompt to touch correct icon on iPad