tendon
DESCRIPTION
TRANSCRIPT

T en on healing variables
repairgrafting
mansoor khanAugust,
2010
HMC Plastic& reconstruction
d
muscle to the bone
glistening structurebetween muscle
& bone whichtransmit force from
“”

collagen
fibrils
fibers
fasciles
tertiary bundles
Tendons
endotenon
histology of tendons

Loose areolar tissue
encasing tendon in low mechanical stress area
Paratenon..?

Paratenon
Loose areolar
tissue containing
collagen & inner
lining of synovial
cells, containing
synovium like
fluid bathing the
tendon.
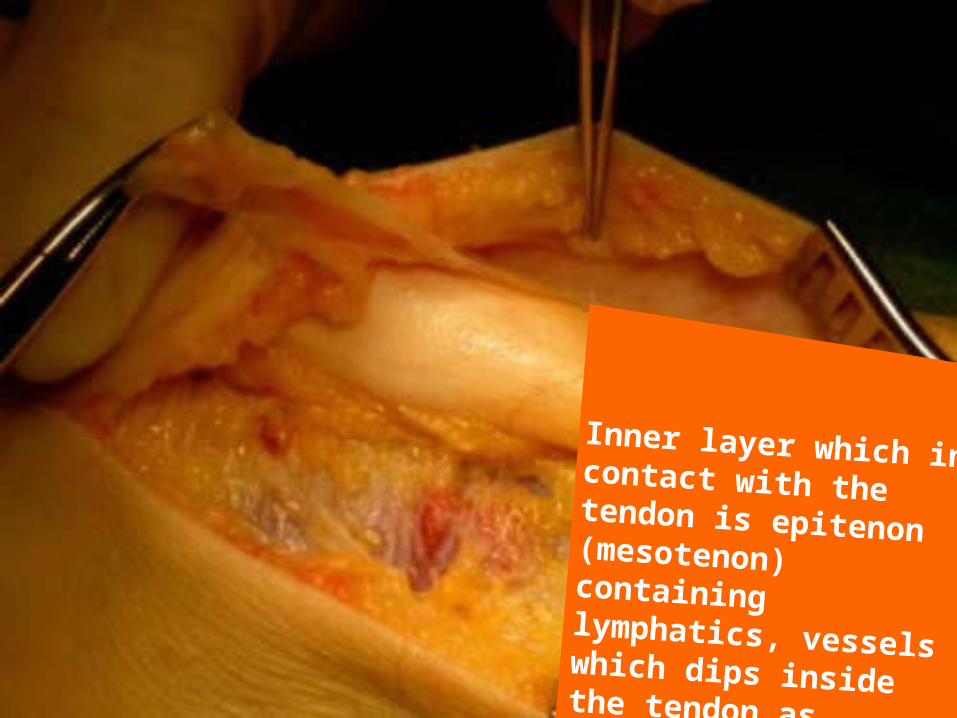
Inner layer which in contact with the tendon is epitenon (mesotenon) containing lymphatics, vessels which dips inside the tendon as endotenon.
Tendon Sheath..?
a dense fibrous
tissue tunnel
enclosing tendon in
high mechanical
stress area
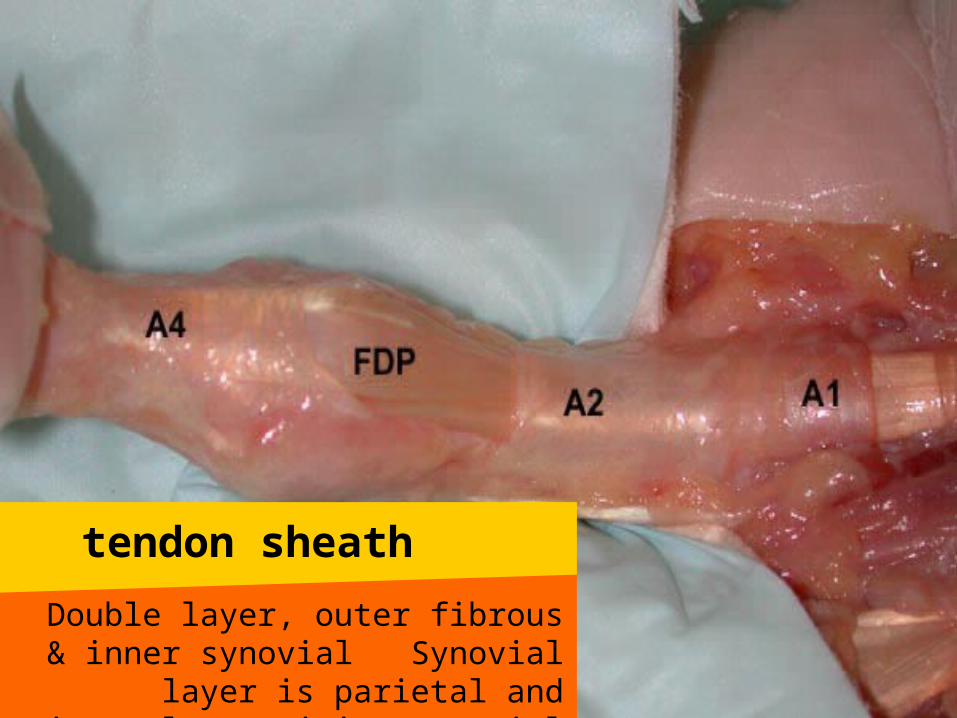
Double layer, outer fibrous & inner synovial Synovial layer is parietal and visceral
containing synovial fluid
tendon sheath
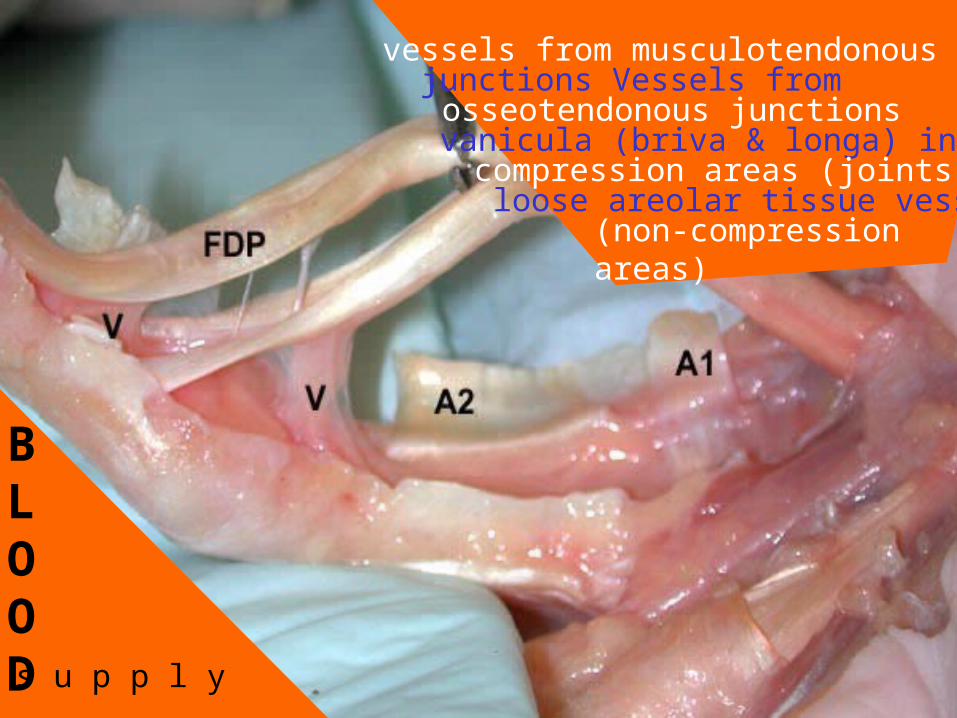
BLOOD
vessels from musculotendonousjunctions Vessels fromosseotendonous junctions
vanicula (briva & longa) incompression areas (joints),
loose areolar tissue vessels(non-compression areas)
s u p p l y

nutrition
sources
vincular blood vesse
ls
synovial fluid blood vesse
ls
Tendon & tendon graft healing
clot and fibrin plug seals the tendon gap
macrophages/neutrophils appears
Inflammatory phase
(48-72 hours):
Stitch provide the whole strength
cells migrate into the wound from, peritenon (extrinsic healing), epitenon/endotenon/tenocytes
(intrisic healing) Becomes fibroblasts produce collagen
Prolif
erativ
e phase
(5 d
ays-4 w
ks):
Tendon & tendon graft healing
Stitch provide the whole strength
Strength is shifted to the scar gradually
rem
odelling p
hase
(4 w
ks-2years
):
Tendon & tendon graft healing
Idea of tendon’s incapability of intrinsic healing leading to extrinsic healing and
adhesions formation CHANGED
Both intrinsic & extrinsic healing are responsible but we have to minimize extrinsic healing to prevent adhesions
intrinsic
...?
extrin
sic..?

T endon healing modulators
hyluronic acid improves healing

Indications: Lacerations with intact soft tissue, Digital re-implantation, Tendon laceration with fractured bones
Goals: Tendon healing,
effortless gliding, full joint motion
Tendon
Repair
mobile digit with minimal scare at least one digital nerve intactmeticulous surgical techniqueco-operative patientcareful graduated mobalization
requirmentsrepair

Guid
elines
Meticulous/atraumatic
techniqueplace
sutures in
the
avascular
portion
anteriorly, good exposure
as retrieval
leads to
trauma, core suture with
4/0 monofilament and 3/0 if
early active
motion
planned, aim for smooth
repair edges

Guidelines
Epitenon su
ture
s decre
ases
external h
ealing
(adhesions),
adds to
strength
,
Modified kessler +
epitenon su
ture
(low
breaking st
rength
& lo
w
gliding re
sistance
) are
adequate when pass
ive
mobilizatio
n is planned
Multistra
nd repair
(high
breaking st
rength
& lo
w
gliding re
sistance
) when
active m
obilizatio
n
Blood supply:
Critical factor for final
results Hypovascularity
> decreased matrix >
decreased strength >
decreased motion > greater
adhesions
variables of tendon healing
Preservation/
reconstruction of flexor
sheath: A2 & A4 must
Sheath
reconstruction restores
nutrition, lu
brication
variables
of tendon
healing
Increases healing, collagen deposition and remodelling, pumping of nutrients inside the tendon, disruption of early vascular budding & adhesions frmation
Early Motion & tensile strength
variables
of tendon
healing
strengthP roportional
number strands
Eight strand
Kessler repairFour strand
cruciate
VS
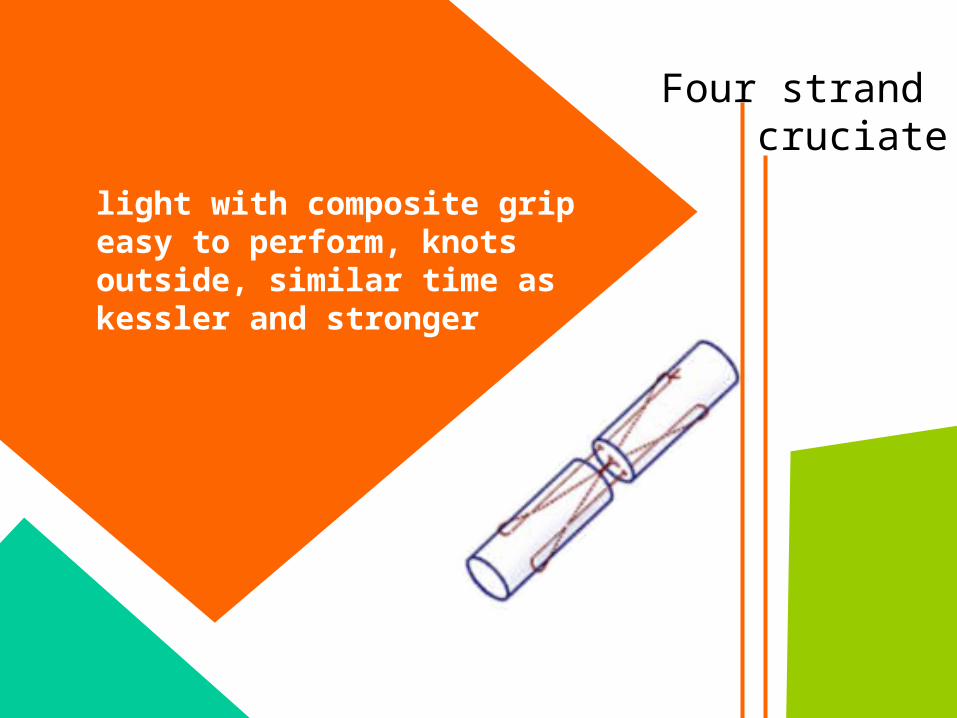
Four strand cruciate
light with composite grip easy to perform, knots outside, similar time as kessler and stronger

tendo ng rafting
When tendon ends can’t be approximatedNecrotic stump
graftingTendon
Indications
Complete wound healing with adequate soft tissue coverageAbsent edema/induration Satisfactory & stable Skeletal alignmentFull range of passive motion of joint
Requirements

absence of indicationsadherent extensor tendons
planned capsulotomy
Contr
ain
dic
ati
ons:

DONOR
SITES
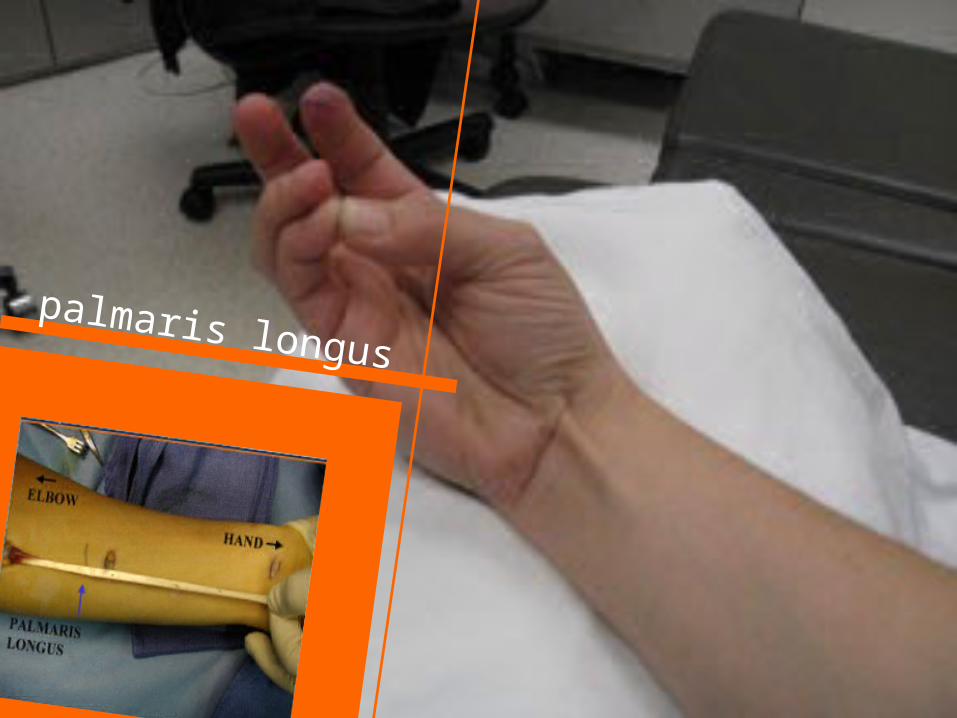
palmaris longus
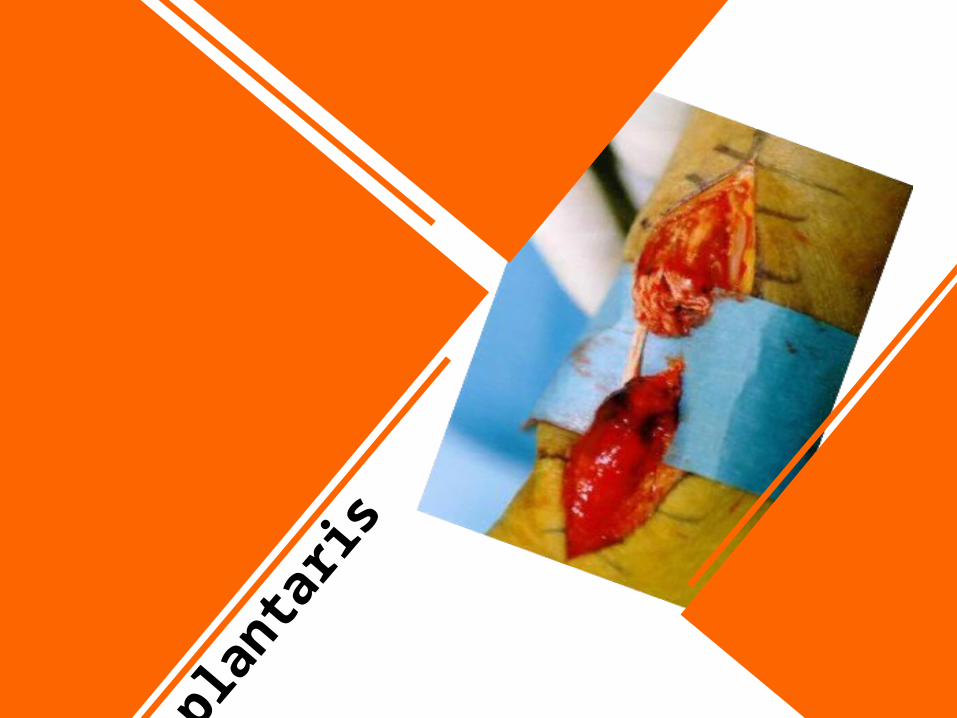
plan
taris
ext
enso
r
dig
itoru
m

tendon lengthening techniques
tendon lengthening techniques
tendon lengthening techniques
tendon lengthening techniques
tendon Lengthening/shotening
techniques

Z tenotomy for tendon
lengthening
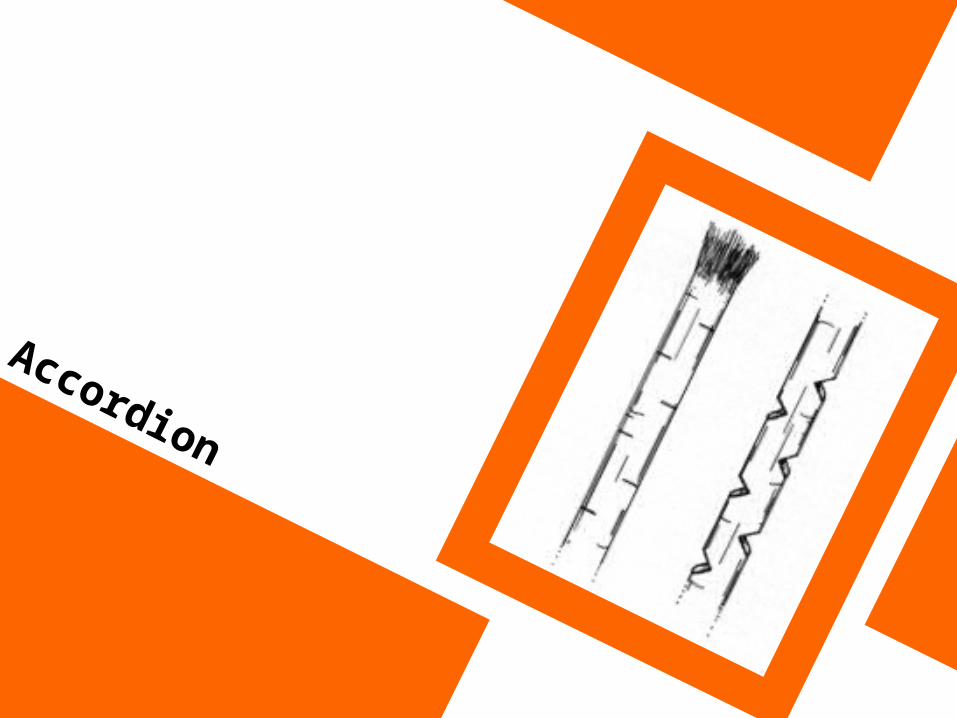
Accordion technique

Modified Z
tenotomy
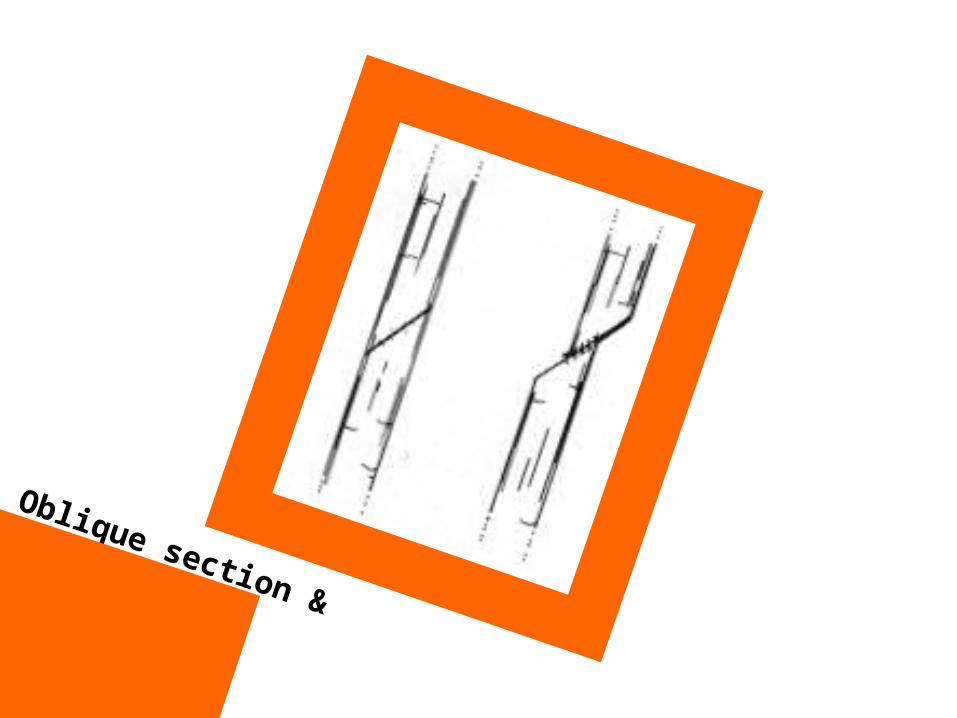
Oblique section &
sliding

Wed
ge s
ection
rese
ctio
n
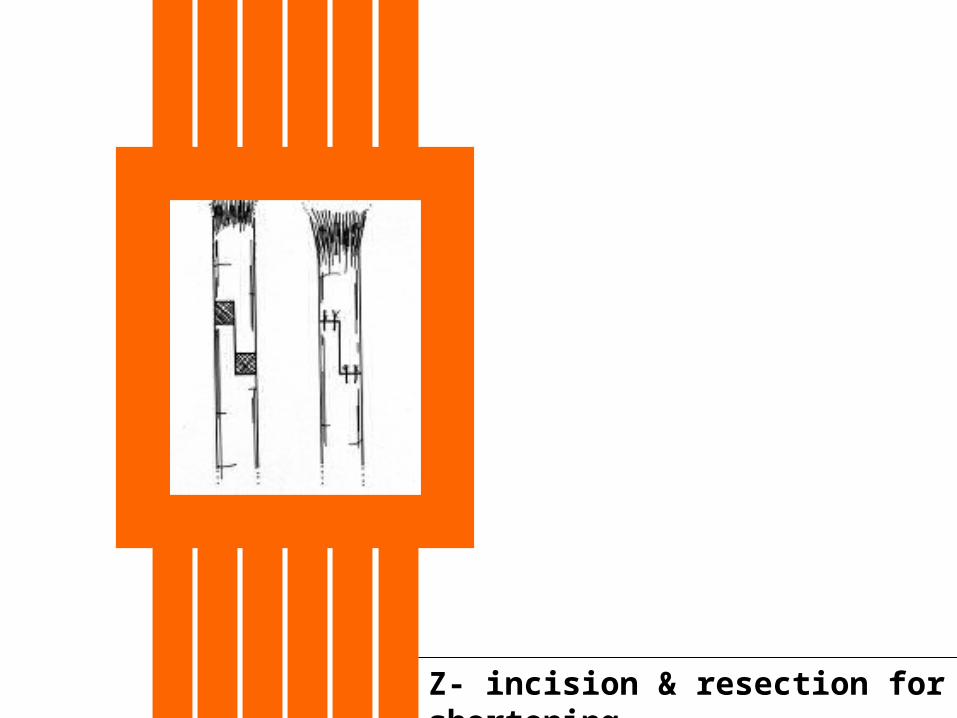
Z- incision & resection for shortening
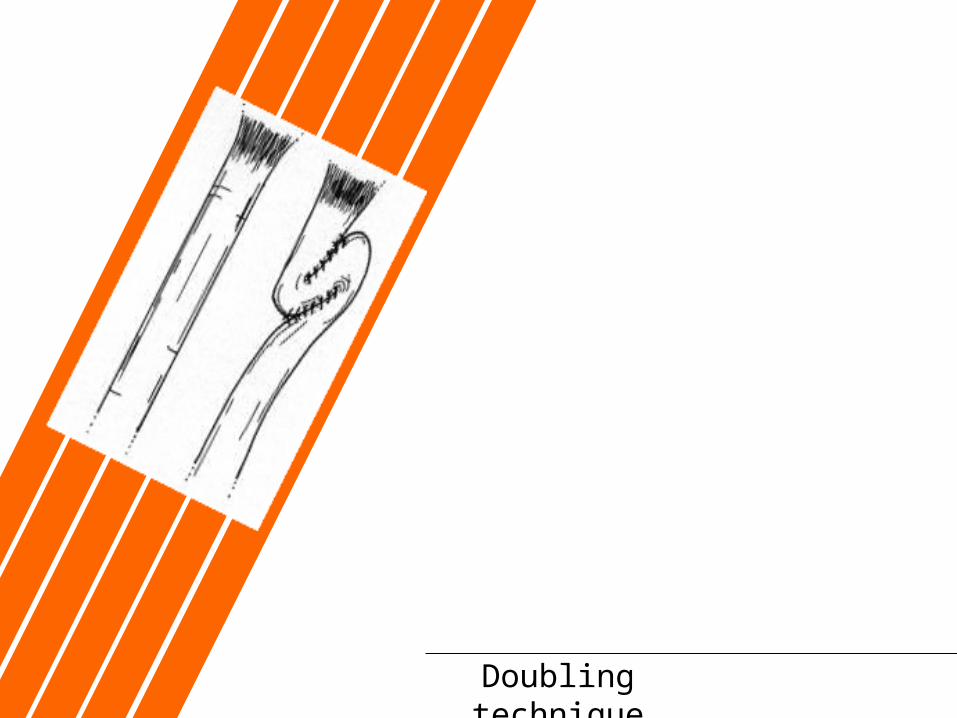
Doubling technique
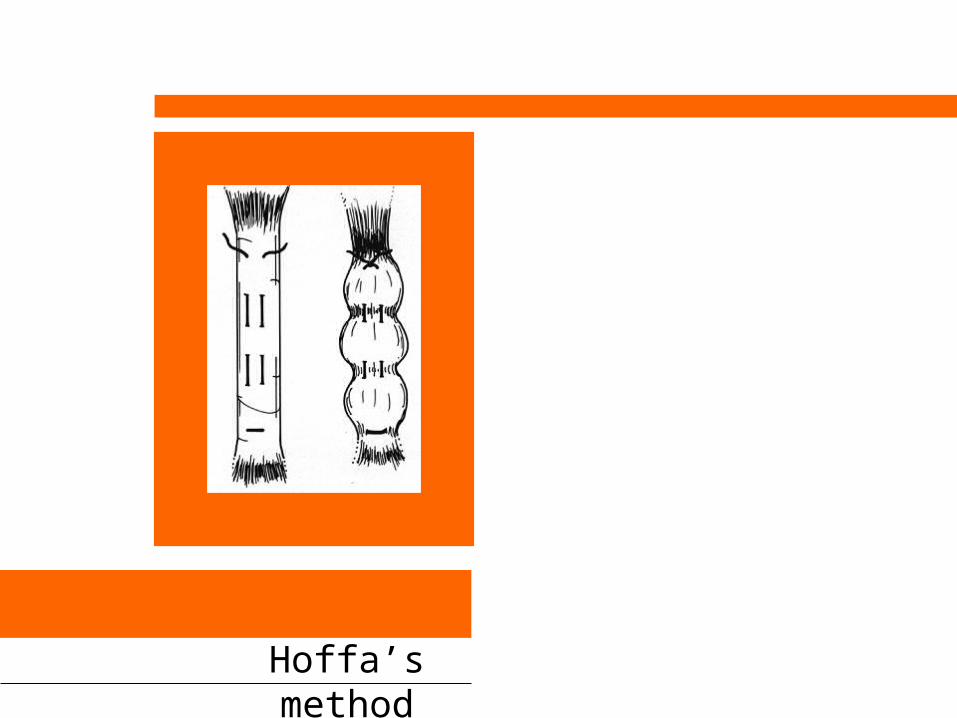
Hoffa’s method