term paper_big data and ontarios primary care sector (00000003)
TRANSCRIPT

B
BIG DATA AND ONTARIO’S
PRIMARY CARE SECTOR
By
July 2014
Emmanuel Casalino, CPHIMS-CA
Radwan El Ali, MD, MBA
University of Toronto
School of Continuing Studies

1
TABLE OF CONTENTS
ABSTRACT ......................................................................................................................................... 3
BACKGROUND .................................................................................................................................... 4
CURRENT STATE ................................................................................................................................ 6
PRIMARY CARE @ A GLANCE ........................................................................................................... 6
VALUE FOR MONEY ......................................................................................................................... 8
THE TRANSFORMATION JOURNEY .................................................................................................... 9
BEST PRACTICES ........................................................................................................................... 10
FUTURE STATE ................................................................................................................................. 12
IMAGINE FOR A MOMENT ................................................................................................................ 12
BACK TO REALITY .......................................................................................................................... 14
MOVING FORWARD ....................................................................................................................... 17
KEY TERMS ...................................................................................................................................... 20
END NOTES...................................................................................................................................... 21

2

3
ABSTRACT
The paper looks at the potential role of Big Data in a primary care context, with a specific
Ontario focus. It looks at the impact of Big Data in helping to:
Support clinical decision making
Enhance practice workflow
Improve continuity of care from the patient‟s perspective
This paper examines concepts and opportunities beyond what is generally promised by
eHealth – i.e., having the right information, about the right person, at the right time. It examines
how data from the health sector, academia, social media, NGOs and a variety of non-traditional
health sources can help improve clinical outcomes for patients and society as a whole.
It compares and contrasts what data is readily available within a typical EMR-enabled family
practice against a similar yet hypothetical practice that is enabled with Big Data

4
BACKGROUND
Primary care in Ontario has undergone significant change over the past several years, and has
evolved significantly from the days when most family physicians worked as solo practitioners,
used paper charts to manage patient information, and depended on their own professional
judgment to make clinical decisions. Today, family doctors typically work in multi-disciplinary
teams i including nurse practitioners, social workers, and dietitians. They use electronic
medical record (EMR) systems to electronically capture and share patient data and are moving
away from a „fee for service‟ compensation model towards an outcomes-based framework.
The province‟s Excellent Care for All Act (2010) is transformative in that it recognizes the
patient as the centre of Ontario‟s health system and acknowledges that healthcare decisions
should be based on evidence. The Act focuses on better access to care, enhancing
community-care delivery, improving integration by bringing services to the patient, and
ensuring that information follows them as they move through the system. Through policy
directives, family physicians are being asked to be ”more accountable for health outcomes by
embedding quality improvement initiatives in clinic settings”i.
Most modern healthcare system have and continue to invest in technology to assist in
automating clinical practice workflows, and records management – this is considered
foundational to achieving transformational objectives and promisesii.
Bending the cost curve is seen as a strategic imperative to sustaining a viable and effective
healthcare system – one that can meet the needs and expectations of Ontarians. Health care
spending in Canada is expected to double between 2000 and 2020, and is likely to outpace
growth in overall public expenditures by a 2:1 ratioiii. Canada‟s ageing population has a direct
relationship to this cost pressure, with the Conference Board of Canada predicting that per
capita expenditure will double over the same period for people currently aged 55 to 64. The
same report also outlines “advances in technology‟” such as diagnostics, and new drug
regimens that contribute to improved health outcomes. These are also expected to increase
overall health expenditures.
Big Data is being view as a quintessential game changer for primary care. Rather than bending
the cost curve, it may be used to get ahead of it by enhancing:
PREVENTATIVE CARE: Helping to avoid and/or delay the onset of chronic diseases;
improving patients‟ quality of life while having a direct and positive impact on health
system costs
QUALITY OF CARE: Interweaving clinical evidence and best practices into care
decisions; using the collective knowledge of leading experts at the point of care to help
guide care decisions

5
PATIENT CARE CO-MANAGEMENT: Enabling a more robust dialogue and treatment
planning between individuals, family members and the care team
DECISION SUPPORT: Improving the variety, volume, and velocity of data available to
clinicians i.e. breaking down the silos, and contextualizing the data into meaningful
information to support more informed care decisions.
POPULATION HEALTH MANAGEMENT: Leveraging the volumes of data that is
collected, managed, and stored across the health system to improve surveillance
capabilities, and to investigate and ultimately improve outcomes for condition / disease
specific patients.
“When you have extensive data you can query and analyze, you can
ask, what‟s going on? In healthcare, it means finding out what‟s
working and what‟s not working, and the latter is absolutely key.”
- Richard Alverez, CEO and President (former), Canada Health
Infoway
Yet, while healthcare remains one of the most information intense sectors iv, it continues to rely
heavily on paper and even when practices deploy systems they remain “islands of automation
in a sea of paper”v. Today, family physicians‟ care decisions about their patients is based
primarily on: what they know, what they observe and what they are told. What they don‟t know
is precisely that – What They Don‟t Know.
Consider the following: for a typical patient engagement, a family physician:
Knows what drugs they prescribed, but doesn‟t know
what drugs the Specialist also seeing the patient has
ordered
Knows that they have renewed a prescription, but
doesn‟t know that patient has never had the drug
dispensed at a pharmacy
Knows that they have ordered a lab test for blood sugar,
but doesn‟t know that this same test was just completed
during a recent hospital visit
Knows and is monitoring the patient‟s waist / hip ratio,
but doesn‟t know that recent evidence has discounted
this an effective diabetes risk factor
Knows that the patient typically presents with high blood
pressure, but doesn‟t know that the patient is actively monitoring their own pressure at
home and is showing normal ranges on a regular basis
6
Knows that there is no family history of cancer, but doesn‟t know that the patient is
carrying a genetic marker that makes them predisposed to lymphoma
When you consider that “90 percent of all the data in the world has been generated over the
last two years”vi and the healthcare system in the United States reached 150 exabytes in
2011vii, it is clear that the debate is not if Big Data will play a role in enhancing primary care, but
how Big Data will be leveraged to transform the system.
CURRENT STATE
The Ontario healthcare sector is a large, complex and data rich sector in which the information
is fragmented and highly siloed. National and provincial leaders recognize the importance of
liberating patient data and thus making it available where and when it is needed to make more
informed clinical decisions that are based on the latest evidence.
To that end, Ontario is investing hundreds of millions towards the creation of Electronic Health
Records (EHRs). These investments will translate into better access to timely and
comprehensive data, enhanced coordination of care delivery, improved continuity of care and
health outcomes, and enhanced population health management. This paper will focus on the
data aspects of healthcare rather than the clinical characteristics of the healthcare sector in
Ontario.
PRIMARY CARE @ A GLANCE
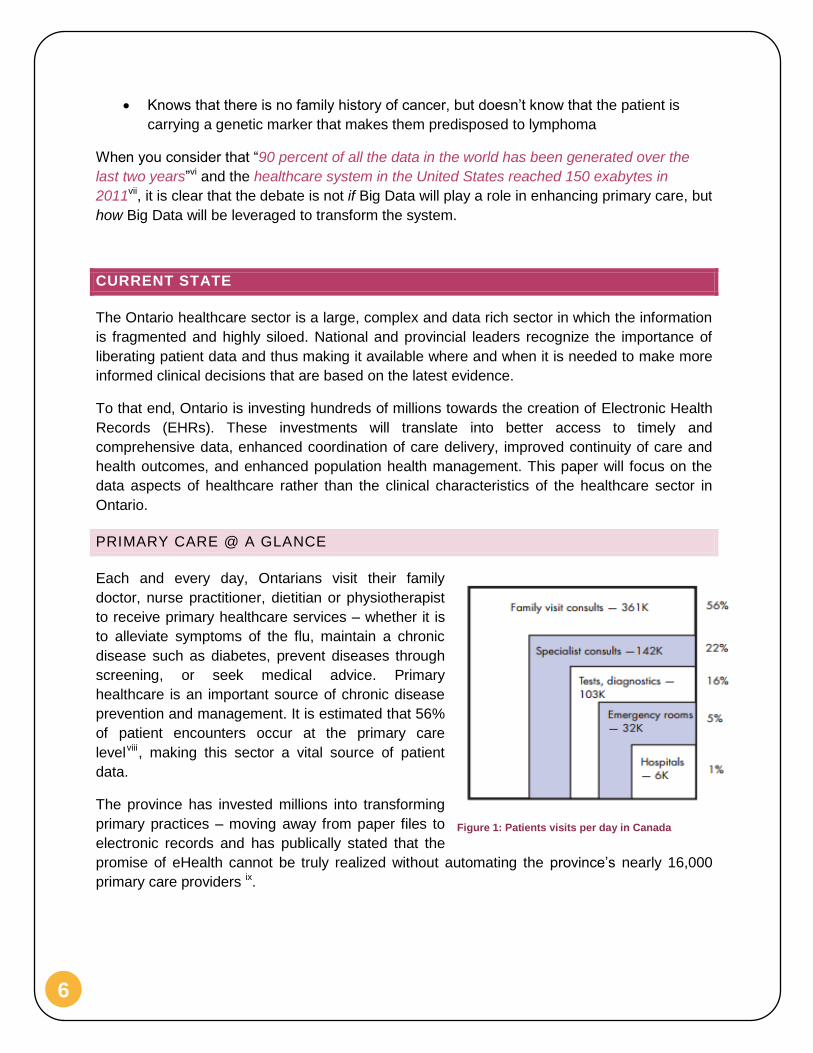
Each and every day, Ontarians visit their family
doctor, nurse practitioner, dietitian or physiotherapist
to receive primary healthcare services – whether it is
to alleviate symptoms of the flu, maintain a chronic
disease such as diabetes, prevent diseases through
screening, or seek medical advice. Primary
healthcare is an important source of chronic disease
prevention and management. It is estimated that 56%
of patient encounters occur at the primary care
levelviii, making this sector a vital source of patient
data.
The province has invested millions into transforming
primary practices – moving away from paper files to
electronic records and has publically stated that the
promise of eHealth cannot be truly realized without automating the province‟s nearly 16,000
primary care providers ix.
Figure 1: Patients visits per day in Canada
7
Consider:
13,000,000+ Ontarians
10,600 primary care physiciansx and 1,867xi nurse-practitioners are active across
Ontario
Every day Ontario‟s primary care clinicians see 150,000 patients
75% of primary care physicians have adopted or enrolled to adopt an Electronic
Medical Record (EMR) within their practicexii
More than 25% of primary care clinicians continue to use paper files to manage patient
records
There are 13 certified EMR products in Ontario
Primary care clinicians represent the first line of care for the vast majority of Ontarians, and
often care for patients over the course of many years –resulting in deep and trusted
relationships. As a result, primary care clinicians are in a unique position within the health
system of being able to collect and manage health data over a span of years. They are able to
witness how a patient‟s health progresses overtime and see patterns of behaviour that could
influence their health status. The challenge facing the health system is this vital data is housed
in thousands of sites, by thousands of unconnected systems, and many hundreds of disparate
applications.
Ontario has what could be classified as the perfect storm from Big Data perspective – lots and
lots of available data that cannot be readily accessed or analyzed.
“We have been referring to Ontario‟s collection of healthcare
providers as a „system‟. In reality, the province has a series of
disjointed services working in many different silos. The Ministry of
Health and Long-Term Care must work with its healthcare providers,
administrators and stakeholders to co-ordinate roles, simplify the
pathways of care and improve the overall patient experience”
Don Drummon, Commission on the Reform of Ontario‟s Public
Services

8
VALUE FOR MONEY
According to the Ontario Budget for the year 2013,
38.3% of the total expenses are related to the
healthcare sector which accounts to $48.9 Billionxiii.
Furthermore, the Canadian Institute for Health
Information (CIHI) forecasted that the health
expenditure in Ontario will be $79.7 Billion by 2013,
of which the public sector expenditure will be $54
Billion or 67.7% of the total health expenditurexiv.
There is growing concern over the affordability of
Ontario‟s health system, with related expenditures
consistently outpacing the growth in GDPxv.
In spite of the level of investment, there are
questions as to whether sufficient value is being
realized. Ontario does not fare well when compared against other Organization for
Economic Co-operation and Development (OECD) jurisdictions who can offer comparable
or even enhanced health outcomes while investing less on a per capital basis. A recent
OECD study of 34 countries placed Canada as the sixth most expensive system in 2009.
Despite the level of expenditures, the Canadian health system does not fare well from a
value for money perspective according to a 2010 Commonwealth Fund Reportii. It placed
Canada second last, ranking only ahead of the United States.
Consider:
Canadian health expenditures are expected toxvi:
o rise by 5.2% in annual growth by 2020 due to primarily demographic factors
o account for 42% of governmental revenues by 2020, up from 31% in 2000
o grow by 58% by 2020, compared to growth in other government spending of
17%
Those 65 and older are estimated to double to more than 4 million by 2036 xvii
80% of Ontarians above the age of 45 suffer from at least one chronic disease, with the
prevalence and cost expected to grow as our population ages xviii
8,700 Ontarians will have been diagnosed with colorectal cancer, with approximately
3,350 dying from it each year. 30% of targeted Ontarians were properly screened for
the disease.xix
61% of women in Ontario aged 50 to 74 were screened for breast cancer with
mammographyxx
Figure 2: Ontario Budget 2013

9
55% of healthcare costs can be attributed to the management of chronic diseases
across Ontario xxi
5% of patients account for two-thirds of healthcare costs xxii
Ontario must do more to offer more comprehensive services at more affordable rates – the
success of our very economy requires it, and Ontarians demand it. There is consensus among
subject matter experts that technology is key to getting ahead of the cost curve; allowing
Ontario to offer high quality health services at affordable rates.
THE TRANSFORMATION JOURNEY
Today, according to OntarioMD more than 75% of community based physicians, “have or are in
the process of adopting an Electronic Medical Record (EMR)”. This is an important
advancement that will allow the liberation of primary care data from the traditional confines of
what was the family physician file room. EMR data contains highly pertinent information to
clinicians outside of the practice. Sadly, it is the norm that when a patient is admitted into an
emergency room or even a long-term care facility, attending clinicians have little to no
knowledge of the patient‟s: current medications, family history, existing diagnoses, past
surgeries, allergies, or procedures performed.
The transformation journey is akin to OntarioMD‟s Maturity Model as depicted in Figure 3:
OntarioMD EMR Maturity Model The first step along the transformation journey is to move away from
paper records and to equip primary care clinicians with an EMR to support the electronic
capture, management and sharing of patient data. As the practice matures it adopts more
advanced capabilities to automating workflow, managing diseases, analyzing and reporting on
patient cohorts, and improving quality outcomes through advanced analytics.
Consider:
Approximately a quarter of Ontario‟s primary
care physicians operate in a purely paper-
based environment
Ontario currently lacks a provincial:
o Medication repository, preventing
access to comprehensive
prescription histories for patients
o eReferral offering, preventing
advances on how patients are
referred to specialists on how data
can follow the patient
o Immunization repository, preventing access to comprehensive history of
immunizations
Figure 3: OntarioMD EMR Maturity Model

10
Primary care clinicians can now access lab results from a provincial repository (i.e. the
Ontario Laboratories Information System), but it currently holds 75% of labs completed
across the province
Provincial infrastructure to allow and support the exchange of information between care
delivery organizations / clinicians is not readily available
Personal Health Information Protection Act (PHIPA) imposes consent obligations on the
sharing of health information
The lack of key provincial assets is inhibiting the flow of patient data between care providers.
Today, primary care clinicians have restricted access to a full view of the patient‟s relevant
medical history and procedures. The promise of Big Data does not seem to be a realistic
objective for this sector of the health system due to the current restrictions.
BEST PRACTICES
The picture is not entirely bleak as the province has several initiatives underway to help
improve data quality. Health Quality Ontario (HQO) is an independent government agency that
is currently working with different stakeholders across Ontario to “provide leadership on a
coordinated and sustainable approach to measure and report on primary care performancexxiii”.
Their goal is ambitious in terms of determining indicators for quality, efficiency, effectiveness
and other considerations. In addition they are aiming to define and capture these indicators
from their different sources and create the technological infrastructure required to capture,
analyze and report on these indicators at both a system and practice level.
Recent advancements are enabling the extraction of EMR data to support secondary uses
such as clinical research. Some examples include:
Better Outcomes and Registry Network (BORN) is currently extracting maternal and
child data to support its mandate surrounding: new born screening and researchxxiv
Ontario Best Practices Research Institute (OBRI) is currently capturing data from
practice locations treating patients with Rheumatologic diseases xxvfor research and
best practices purposes.
The Canadian Cardiovascular Harmonization of National Guidelines Endeavour (C-
Change) initiative is a national initiative focused on the advancement, promotion and
harmonization of cardio vascular disease guidelines. C-CHANGE is working on
promoting these guidelines and implementing them at both a patient and primary care
physician levelxxvi
Canadian Primary Care Sentinel Surveillance Network (CPSSN) is an initiative to work
with participating primary care physicians to capture, analyze and provide insight on the
quality of care provision and how selected chronic diseases and neurologic conditions
are treatedxxvii.
11
When you have extensive data you can query and analyze, you can
ask, what‟s going on? In healthcare, it means finding out what‟s
working and what‟s not working, and the latter is absolutely key.”
- Richard Alverez, CEO and President (former), Canada Health
Infoway

12
FUTURE STATE
IMAGINE FOR A MOMENT
Mark is a sixty year old who was recently admitted into hospital for congestive heart failure,
where he was treated and released two days later. The hospital recommended that Mark be
referred to a cardiologist, be placed into a Telehomecare program, and was ePrescribed an
ACE inhibitor.
The eReferral system identifies Dr. Strul as the most appropriate cardiologist to handle the
referral – based on models that take into consideration factors such as proximity, wait time,
qualifications, patient ratings on social media, etc. An eReferral is sent to Dr. Strul‟s practice
accompanied with relevant details.
As part of the Telehomecare program, Mark is required to measure his weight and blood
pressure twice a day via Bluetooth-enabled devices, which send results to a Telehomecare
Nurse Practitioner.
Three days after being discharged, Mark‟s weight has suddenly increased by 3 lbs. New
evidence from the Heart and Stroke Foundation is suggesting= – based on Mark‟s height,
weight and age – that a weight gain of 2.5 lbs. or more is an indicator of fluid retention and
highly dangerous for CHF patients. The Telehomecare Nurse Practitioner‟s Case Management
System (CMS) monitors emerging evidence, notices the weight gain pattern, and issues an
immediate alert. When reviewing the alert she notices that while Mark was prescribed
medication at the hospital, there is no indication that it was filled.
Given the severity of the situation, the CMS automatically redirects the alert to Dr. Rodin who is
Mark‟s family doctor. Five days ago, Dr. Rodin was sent an electronic notification that Mark
was admitted into hospital and was able to remotely monitor his situation as he received both
hospital and Telehomecare reports on a daily basis directly into his Electronic Medical Record
(EMR).
Dr. Rodin, the Nurse Practitioner, Dr. Strul, and Mark convene a web-based consultation to
discuss his sudden wait gain. On the videoconference, Mark confirms that he did not have time
to get his prescription filled – both the Nurse Practitioner and Dr. Rodin agree this is the likely
cause for his weight gain. Both doctors‟ EMRs received the ePrescription notice, and based on
recent evidence from the United States as well as Mark‟s genetic make-up, they recommend
the drug digoxin instead. It has less risk of a negative interaction with his current medications
and medical history.
The care team agrees on the course of action, and the ePrescription is updated and the closest
pharmacy is notified and delivers the medication to Mark within hours. Mark is told to continue
monitoring his weight and blood pressure and for the moment there is no need to go to the
emergency room. Mark‟s follow-up visit with Dr. Strul is cancelled as the consultation was

13
completed electronically and his medical record is updated – and readily available should his
situation change.
Dr. Rodin participates in a clinical research studies into clinical guidelines for CHF and
Diabetes and has agreed to submit anonymized patient data on a monthly basis. In return he
receives a report that demonstrates how well he is doing against established targets and in
comparison with other providers with similar patient cohort profiles.
Later that month, Dr. Rodin reviews his on-line performance report. It shows that his diabetic
patients are being effectively managed and there is a positive trend regard compliance with
clinical guidelines. However, the report has identified an anomaly with respects to patients who
are booked for their annual foot exam. It forecasts that he will be out of compliance on this key
measure. He opens the list of patients that are due for a foot exam, and sends each a text
reminding them to book an online appointment.

14
BACK TO REALITY
While progress is being made, for the vast majority of
patient interactions across Ontario‟s health system,
information does not readily flow between provider
organizations. Figure 4: Islands of Data depicts the reality
of the current health system. Patient data captured during
a patient encounter, for the most part, remains captive
within the organization‟s four walls.
The current reality is preventing many of the advantages
and benefits described with the fictional Mark‟s
experience. The inability to amass timely and relevant
data are creating „white spaces‟ or gaps of important
information that could be used to advance healthcare
delivery via enhanced analytics and machine learning
opportunities. Current information gaps are preventing /
inhibiting:
a. EFFECTIVE DATA EXCHANGES
What was a near real-time referral in the future state, can currently take days if not weeks.
Family doctors are forced to fax referral requests, wait possibly days to hear back and only
to hear that the specialist is not accepting new patients. Data is not being exchanged in a
manner that can be readily repurposed unless manually re-entered by the receiving
practice.
Patient‟s personal and healthcare information remains fragmented across the continuum of
care, due to the lack of effective system integration capabilities. Machine learning, whether
structured or unstructured, is therefore limited to a finite set of data. Even the highly
respected Institute of Clinical Evaluative Sciences (ICES) which has the mandate gaining
insights and learnings on clinical practices and health outcomes has resorted to using
encrypted discs to gain access to primary care data. Also, due to systemic barriers and
limited budgets, they are restricted to gathering data from 300 of 10,600 primary care
physicians; representing 300,000 of 13,000,000 Ontariansxxviii.
For an industry that is so information intensive the lack of affordable / suitable data
analytics is truly surprising. EMRs typically have limited and unsophisticated data analytics
/ reporting tools. All too often primary care clinicians are forced to download EMR data into
Excel spreadsheets or Access databases to perform rudimentary analytics. In some cases,
EMRs actually prevent data extracts and force clinicians to use vendor-offered services.
What is not surprising is the business intelligence industry that is starting to form around
primary care here in Ontario and across North America. While a welcome addition, these
start-ups are not likely to have access to province-wide data thus restricting the amount
and variety of data sets they can leverage.
Figure 4: Islands of Data
15
Bottom line: The lack of end-to-end integration within the primary care sector is a key
barrier to achieving the promise and hope of Big Data.
b. DATA ANALYSIS / MACHINE LEARING
In the fictional future state scenario data was being consumed and used to detect patterns
and EMRs used machine learning techniques to suggest care plan recommendations.
Today clinical guidelines are typically stored on the doctor‟s office shelf, and are usually out
of date as new guidelines are published as new evidence is discovered. These paper-
based artifacts typically are not consumable by health applications. As such, the latest
guidelines or „business rules‟ cannot be readily used to support analytics or other reporting
functions. Mark was able to avoid complications and re-admittance into hospital because
the CMS was able to: notice patterns in the data and with updated clinical rules in play
facilitate an action to issue an alert.
The Canadian Institute for Health Information (CIHI) piloted the Primary Health Care
Voluntary Reporting System (PHC VRS) with 300 EMR-enabled primary care clinicians to
capture, analyze and report on compliance against established guidelines. In 2013 CIHI
concluded that “the process of extracting, manipulating and analyzing non-standardized
EMR data is not sustainable or affordable” xxix as it is labour intensive and might introduce
“data quality risks” The PHC VRS was eventually decommissionedxxx.
Current reports cannot be produced in a timely manner due to data collection barriers, and
often analysis is looking at events that occurred 6 months ago. Analysis is often highly
retrospective and cannot be effectively used to support quality improvement initiatives.
Data collected to inform clinical guidelines is also dated, and is not from a representative
sample.
The quality of the data collected and managed in EMRs is also a big challenge as data is
typically captured in a non-standardized and often unstructured (e.g., free form) manner.
For example, if a patient is diabetic, the physician can put the diagnosis as DM, DM type 2,
Diabetic, or diabetes. The adage “garbage in, garbage out” comes into play in the current
state and as a result makes data extraction / analysis highly burdensome and costly.
Data quality issues are a key contributing factor for the inability to exchange primary care
data in support of clinical and administrative decisions being made across the health
sector. The amount of effort and costs needed to „cleanse‟ the data for reuse is
insurmountable. And, it is unclear if clinicians would rely on or even trust data that was
extracted from other sources.
Bottom line: The inability to collect primary care data and the quality of the data itself are
key barriers in realizing the benefits that machine learning could offer.
16
c. POPULATION HEALTH MANAGEMENT
Surveillance is at the heart of avoiding / mitigating any outbreak of a contagious disease.
Key to effective surveillance is data from sentinel systems such as primary care EMRs,
hospital information systems, social media, laboratory systems and drug information
systems. The current health system is populated with disparate systems that are not
interconnected or easily interoperable.
The SARS scare in 2003 was a clear example of our health systems limitations. We could
not ask or answer basic questions such as who is sick, who is at risk, who was / was not
immunized, what is the absenteeism rates at work and school, is the virus changing, how
have patients responded to care, what care was provided and will there be enough supply
of vaccines to meet tomorrow‟s demand?
Pockets of data warehouses exist across the health system, but each contains data to help
satisfy the objectives and mandates of the associated organizations (i.e., public health,
hospitals, MOHLTC). Each is not interconnected or able to exchange data for analysis or
monitoring.
Bottom line: Ontario does not have access to the depth nor breadth of information
necessary for a truly effective public / population health surveillance capacity - a key barrier
to an effective population health capability in Ontario.

17
MOVING FORWARD
The promise that Big Data holds in enhancing primary care is both compelling and motivating.
Big Data will allow care to be delivered in ways that we have not yet begun to imagine, and this
potential cannot be ignored.
Currently, healthcare providers are faced with data from multiple data sources for the purpose
of primary and secondary healthcare provision, quality and research. With the huge volume of
data, the exponential velocity, and the different data format and standards, Big Data tools can
play a tremendous role in the consolidation of this data, the extraction, transferring and loading
(ETL) of this data into the proper data warehouses and spreading it across different servers,
which eliminate data loss and system failure. Furthermore, big data tools can facilitate real time
retrieval of information by the primary care physicians, and real time decision support at the
point of care. This will eventually lead to improvement in healthcare provision, reduction if not
elimination of waste in healthcare such as redundant diagnostic tests and imaging, wait time,
resource underutilization and thus lead to reduction of healthcare costs.
However, it is important to choose the proper Big Data tools and take into consideration the
anticipated responsiveness that is related to the utilization and retrieval of data (i.e. how fast
would you like the data query to take place). Furthermore, there are lots of challenges that
need to be taken into consideration in the implementation of Big Data; some are specific to big
data and some are common to data in general. Some of the main challenges are the growing
need for security and privacy protection, yet the need to be in compliance with the increased
scrutiny of the legal and regulatory requirements such as the Personal Health Information
Protection Act. Some examples to clarify this point are as follows:
Consolidation of this huge volume of data from different sources, faces more privacy
concerns than if the data is dispersed over its initial multiple repositories;
Figure 5: Bridging the Information Gap
Acute Care
Primary Care
Public HealthAcademia
MedicalDevices
Social Media
Rx
Labs
Continuing Care
Helping to enhance:• population health management • personalized medicine• evidence-based care• health system management• surveillance / outbreak prevention• continuity of care• patient safety• patient satisfaction
Big Data :Bridging the Information Gap

18
Data transmission from different sources needs to happen through secure channels.
The bigger the number of the data sources and transmission channels, the higher the
change of a breach in security; and
Composable risk is associated with the consolidation of data from different data sources
which might lead to personal information identification
Furthermore, a huge challenge that faces implementation of big data in healthcare is related to
data governance and patient consent. iWho is the custodian of the data?Who can share the
data and under which circumstances? Is the purpose to obtain, provision of care, quality
improvement or research? Is patient consent, implicit, explicit or required?
In conclusion, big data can help improve the efficiency of the healthcare system, improve the
quality of care, enhance patient safety and bend the cost curve. An all-inclusive approach
needs to be implemented at the provincial, regional, system and practice level to deal with the
proper questions and challenges the healthcare system faces. An appropriate solution needs
to be implemented in order to meet the increasing demand for healthcare services from an
aging population with complex care demands.
Where is all the knowledge we lost with information?
- T.S. Elliot
Technology is dominated by two types of people: those who understand
what they do not manage, and those who manage what they do not
understand.
- Archibald Putt

19

20
KEY TERMS
BORN Better Outcomes and Registry Network
CHF Congestive Heart Failure
CIHI Canadian Institute for Health Information
CMS Case Management System
EHR Electronic Health Record
EMR Electronic Medical Record
HQO Health Quality Ontario
ICES Institute for Clinical Evaluative Sciences
PHIPA Personal Health Information Protection Act
VRS Voluntary Reporting System

21
END NOTES
i Ministry of Health and Long-Term Care, Family Health Teams ii Commonwealth Fund, 2012 Report
iii The Conference Board of Canada, The Future Cost of Health Care in Canada, 2000 to 2020
iv Health Care Information Systems: A Practical Approach for Health Care Management
v Physician eHealth Technology Roadmap, August 2010
vi Big Data, for better or worse, SINTEF, May 2013
vii Transforming Health Care Through Big Data, Institute for Health Technology Transformation
viii The CMA‟s 5-year strategy for health information technology investment in Canada; 2010; Canadian
Medical Association ix Physician Technology Roadmap, eHealth Ontario, 2010
x Primary Care in Ontario: reforms, investments and achievements, OMA
xi CIHI Nursing Data 2012
xii OntarioMD
xiii 2013 Ontario Budget
xiv National Health Expenditure Trends, 1975 to 2013, Canadian Institute for Health Information
xv Ontario needs better value for money in healthcare, Toronto Star, April 20, 2014
xvi The Future Cost of Canada
xvii 2012 – 2036 Ontario and Its 49 Census Divisions; Spring 2013, Ministry of Finance, Ontario
xviii Preventing and Managing Chronic Disease: Ontario‟s Framework; May 2007, Ministry of Health &
Long Term Care. xix
Cancer Care Ontario, Colorectal Cancer Screening Program web site xx
Cancer Care Ontario, Breast Cancer Screening Program web site xxi
Preventing and Managing Chronic Disease: Ontario‟s Framework; May 2007, Ministry of Health &
Long Term Care. xxii
Ministry of Health and Long-Term Care, Health Link‟s web site xxiii
Health Quality Ontario xxiv
eHealth Ontario Annual Business Plan (2014-15) xxv
Ontario Best Practices Institute
xxvi Canadian Cardiovascular Harmonization of National Guidelines Endeavour
xxvii Canadian Primary Care Sentinel Surveillance Network
xxviii Institute of Clinical Evaluative Sciences, Electronic Medical Record Administrative Data Linked
Database) xxix
Insights and Lessons Learned From the PHC VRS Prototype; 2013; Canadian Institute for Health
Information xxx
President‟s Quarterly Report and Review of Financial Statements as at December 31, 2013;
Canadian Institute for Health Information