texts medicine
TRANSCRIPT
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 1/59
Human eyeFrom Wikipedia, the free encyclopediaJump to: navigation, search
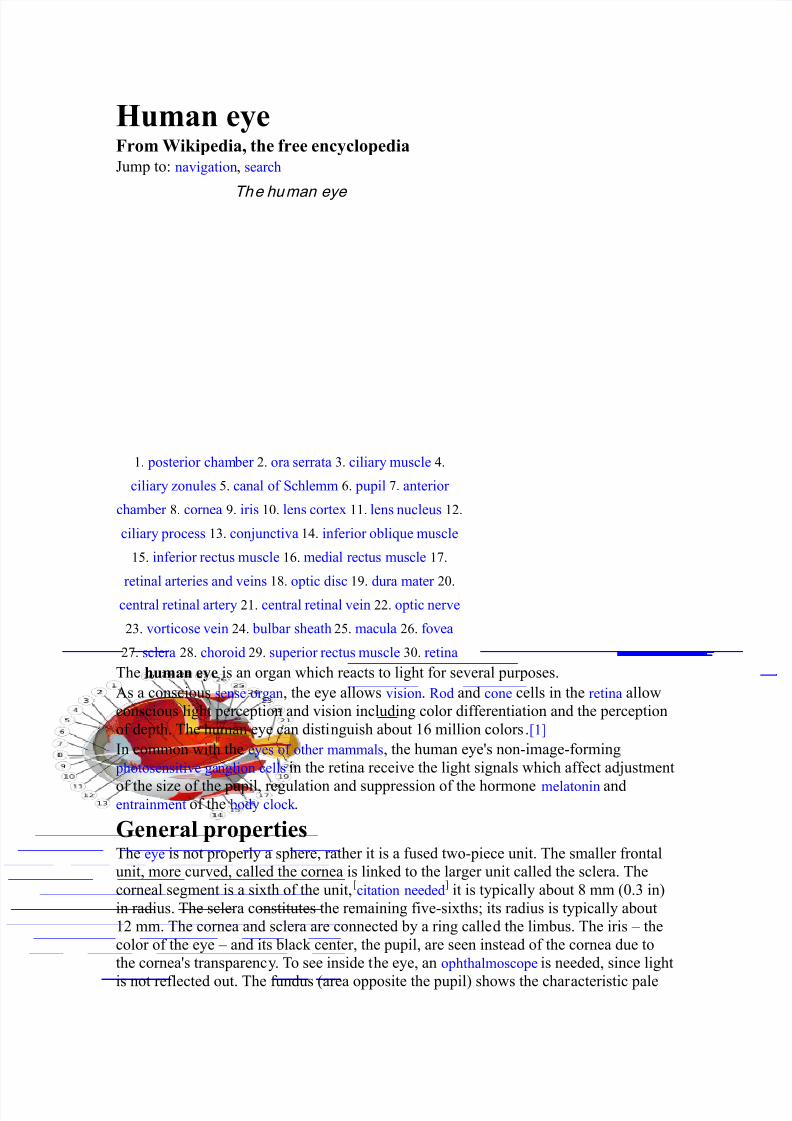
The human eye
1. posterior chamber 2. ora serrata 3. ciliary muscle 4.
ciliary zonules 5. canal of Schlemm 6. pupil 7. anterior
chamber 8. cornea 9. iris 10. lens cortex 11. lens nucleus 12.
ciliary process 13. conjunctiva 14. inferior oblique muscle
15. inferior rectus muscle 16. medial rectus muscle 17.
retinal arteries and veins 18. optic disc 19. dura mater 20.
central retinal artery 21. central retinal vein 22. optic nerve
23. vorticose vein 24. bulbar sheath 25. macula 26. fovea
27. sclera 28. choroid 29. superior rectus muscle 30. retina
The human eye is an organ which reacts to light for several purposes.
As a conscious sense organ, the eye allows vision. Rod and cone cells in the retina allow
conscious light perception and vision including color differentiation and the perception
of depth. The human eye can distinguish about 16 million colors.[1]
In common with the eyes of other mammals, the human eye's non-image-forming
photosensitive ganglion cells in the retina receive the light signals which affect adjustment
of the size of the pupil, regulation and suppression of the hormone melatonin andentrainment of the body clock .
General propertiesThe eye is not properly a sphere, rather it is a fused two-piece unit. The smaller frontal
unit, more curved, called the cornea is linked to the larger unit called the sclera. The
corneal segment is a sixth of the unit, [citation needed
] it is typically about 8 mm (0.3 in)
in radius. The sclera constitutes the remaining five-sixths; its radius is typically about
12 mm. The cornea and sclera are connected by a ring called the limbus. The iris – the
color of the eye – and its black center, the pupil, are seen instead of the cornea due to
the cornea's transparency. To see inside the eye, an ophthalmoscope is needed, since light
is not reflected out. The fundus (area opposite the pupil) shows the characteristic pale
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 2/59
optic disk (papilla), where vessels entering the eye pass across and optic nerve fibers
depart the globe.
[edit] Dimensions
A human eye
The dimensions differ among adults by only one or two millimeters. The vertical
measure, generally less than the horizontal distance, is about 24 mm among adults, at
birth about 16 – 17 mm. (about 0.65 inch) The eyeball grows rapidly, increasing to 22.5 –
23 mm (approx. 0.89 in) by the age of three years. From then to age 13, the eye attains
its full size. The volume is 6.5 ml (0.4 cu. in.) and the weight is 7.5 g. (0.25 oz.)[edit] ComponentsThe eye is made up of three coats, enclosing three transparent structures. The outermost
layer is composed of the cornea and sclera. The middle layer consists of the choroid,
ciliary body, and iris. The innermost is the retina, which gets its circulation from the
vessels of the choroid as well as the retinal vessels, which can be seen in an
ophthalmoscope.
Within these coats are the aqueous humor, the vitreous body, and the flexible lens. The
aqueous humor is a clear fluid that is contained in two areas: the anterior chamber
between the cornea and the iris and exposed area of the lens; and the posterior chamber ,
behind the iris and the rest. The lens is suspended to the ciliary body by the suspensory
ligament (Zonule of Zinn), made up of fine transparent fibers. The vitreous body is a
clear jelly that is much larger than the aqueous humor, and is bordered by the sclera,
zonule, and lens. They are connected via the pupil.[2]
IntestineFrom Wikipedia, the free encyclopediaJump to: navigation, search
In human anatomy, the intestine (or bowel) is the segment of the alimentary canal
extending from the stomach to the anus and, in humans and other mammals, consists of
two segments, the small intestine and the large intestine. In humans, the small intestine is
further subdivided into the duodenum, jejunum and ileum while the large intestine is
subdivided into the cecum and colon.[1]
Structure and function
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 3/59
The structure and function can be described both as gross anatomy and at a microscopic
level. The intestinal tract can be broadly divided into two different parts, the small and
large intestine. Grayish-purple in color and about 35 millimeters (1.5 inches) in
diameter, the small intestine is the first, measuring 6 to 7 meters (20 – 23 ft) long average
in an adult man. Shorter and relatively stockier, the large intestine is a dark reddish
color, measuring roughly 1.5 meters (5 ft) long on average. [2] People will have
different sized intestines according to their size and age.
The lumen is the cavity where digested food passes through and from where nutrients
are absorbed. Both intestines share a general structure with the whole gut, and are
composed of several layers. Going from inside the lumen radially outwards, one passes
the mucosa (glandular epithelium and muscularis mucosa), submucosa, muscularis
externa (made up of inner circular and outer longitudinal), and lastly serosa.
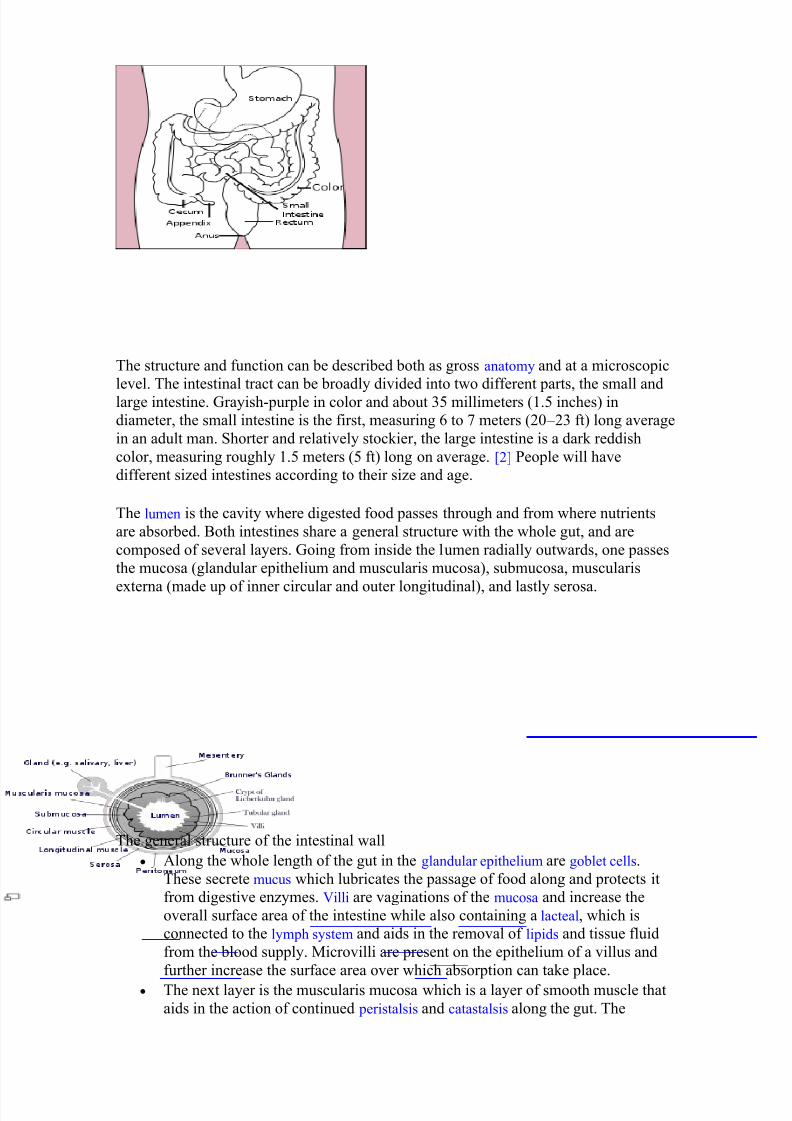
The general structure of the intestinal wall
Along the whole length of the gut in the glandular epithelium are goblet cells.
These secrete mucus which lubricates the passage of food along and protects it
from digestive enzymes. Villi are vaginations of the mucosa and increase the
overall surface area of the intestine while also containing a lacteal, which is
connected to the lymph system and aids in the removal of lipids and tissue fluid
from the blood supply. Microvilli are present on the epithelium of a villus and
further increase the surface area over which absorption can take place.
The next layer is the muscularis mucosa which is a layer of smooth muscle that
aids in the action of continued peristalsis and catastalsis along the gut. The
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 4/59
submucosa contains nerves (e.g. Meissner's plexus), blood vessels and elastic fibre
with collagen that stretches with increased capacity but maintains the shape of
the intestine.
Surrounding this is the muscularis externa which comprises longitudinal and
smooth muscle that again helps with continued peristalsis and the movement of
digested material out of and along the gut. In between the two layers of musclelies Auerbach's plexus.
Lastly there is the serosa which is made up of loose connective tissue and coated
in mucus so as to prevent friction damage from the intestine rubbing against
other tissue. Holding all this in place are the mesenteries which suspend the
intestine in the abdominal cavity and stop it being disturbed when a person is
physically active.
The large intestine hosts several kinds of bacteria that deal with molecules the human
body is not able to break down itself. This is an example of symbiosis. These bacteria
also account for the production of gases inside our intestine (this gas is released as
flatulence when eliminated through the anus). However the large intestine is mainly
concerned with the absorption of water from digested material (which is regulated by
the hypothalamus) and the reabsorption of sodium, as well as any nutrients that may have
escaped primary digestion in the ileum.
BrainFrom Wikipedia, the free encyclopediaJump to: navigation, search
This article is about the brains of all types of animals, including humans. For
information specific to the human brain, see human brain. For other uses, see Brain(disambiguation).
A chimpanzee brain
The brain is the center of the nervous system in all vertebrate, and most invertebrate, animals.[1] Some primitive animals such as jellyfish and starfish have a decentralized
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 5/59
nervous system without a brain, while sponges lack any nervous system at all. In
vertebrates, the brain is located in the head, protected by the skull and close to the
primary sensory apparatus of vision, hearing, balance, taste, and smell.
Brains can be extremely complex. The cerebral cortex of the human brain contains
roughly 15 – 33 billion neurons, perhaps more, depending on gender and age,[2] linked
with up to 10,000 synaptic connections each. Each cubic millimeter of cerebral cortexcontains roughly one billion synapses.[3] These neurons communicate with one another
by means of long protoplasmic fibers called axons, which carry trains of signal pulses
called action potentials to distant parts of the brain or body and target them to specific
recipient cells.
The brain controls the other organ systems of the body, either by activating muscles or
by causing secretion of chemicals such as hormones. This centralized control allows
rapid and coordinated responses to changes in the environment. Some basic types of
responsiveness are possible without a brain: even single-celled organisms may be
capable of extracting information from the environment and acting in response to it.[4]
Sponges, which lack a central nervous system, are capable of coordinated body
contractions and even locomotion.[5] In vertebrates, the spinal cord by itself containsneural circuitry capable of generating reflex responses as well as simple motor patterns
such as swimming or walking.[6] However, sophisticated control of behavior on the
basis of complex sensory input requires the information-integrating capabilities of a
centralized brain.
Despite rapid scientific progress, much about how brains work remains a mystery. The
operations of individual neurons and synapses are now understood in considerable
detail, but the way they cooperate in ensembles of thousands or millions has been very
difficult to decipher. Methods of observation such as EEG recording and functional brain
imaging tell us that brain operations are highly organized, while single unit recording can
resolve the activity of single neurons, but how individual cells give rise to complexoperations is unknown.[7]
FunctionsFrom an organismic perspective, the primary function of a brain is to control the actions
of an animal.[59] To do this, it extracts enough relevant information from sense organs
to refine actions. Sensory signals may stimulate an immediate response as when the
olfactory system of a deer detects the odor of a wolf; they may modulate an ongoing
pattern of activity as in the effect of light-dark cycles on an organism's sleep-wake
behavior; or their information may be stored in case of future relevance. The brain
manages its complex task by orchestrating functional subsystems, which can be
categorized in a number of ways: anatomically, chemically, and functionally.Functional subsystemsThe most straightforward way to categorize the parts of the brain is anatomically, but
there are also several ways to subdivide it functionally. One of the most important of
these is on the basis of the chemical neurotransmitters used by neurons to communicate
with each other. Another is in terms of the way a brain area contributes to information
processing: sensory areas bring information into the brain and reformat it; motor signals
send information out of the brain to control muscles and glands; arousal systems
modulate the activity of the brain according to time of day and other factors.
Pancreas

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 6/59
From Wikipedia, the free encyclopediaJump to: navigation, search
For other uses, see Pancreas (disambiguation).
This article is about the bodily organ. For culinary use of animal pancreas, see
Sweetbread.
Pancreas
1: Head of pancreas
2: Uncinate process of
pancreas
3: Pancreatic notch
4: Body of pancreas
5: Anterior surface of
pancreas
6: Inferior surface of
pancreas
7: Superior margin of
pancreas
8: Anterior margin of
pancreas
9: Inferior margin of

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 7/59
pancreas
10: Omental tuber
11: Tail of pancreas
12: Duodenum
Gray's subject #251 1199
Artery
inferior pancreaticoduodenal artery,
superior pancreaticoduodenal artery,
splenic artery
Vein pancreaticoduodenal veins, pancreatic
veins
Nerve pancreatic plexus, celiac ganglia,
vagus[1]
Precursor pancreatic buds
MeSH Pancreas
Dorlands/Elsevier Pancreas
The pancreas is a gland organ in the digestive and endocrine system of vertebrates. It is
both an endocrine gland producing several important hormones, including insulin,
glucagon, and somatostatin, as well as an exocrine gland, secreting pancreatic juice
containing digestive enzymes that pass to the small intestine. These enzymes help to further
breakdown the carbohydrates, protein, and fat in the chyme.
Contents[hide]
1 Histology
2 Function
o 2.1 Endocrine
o 2.2 Exocrine
o 2.3 Regulation
3 Anatomy of the Pancreas
o 3.1 Position
o 3.2 Parts
o 3.3 Blood Supply
3.3.1 Arterial Supply 3.3.2 Venous Drainage
o 3.4 Lymphatic Drainage
4 Diseases of the pancreas
5 History
6 Embryological development
7 In animals
8 The Pancreas in Popular Culture
9 Additional images
10 References
[edit] Histology
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 8/59
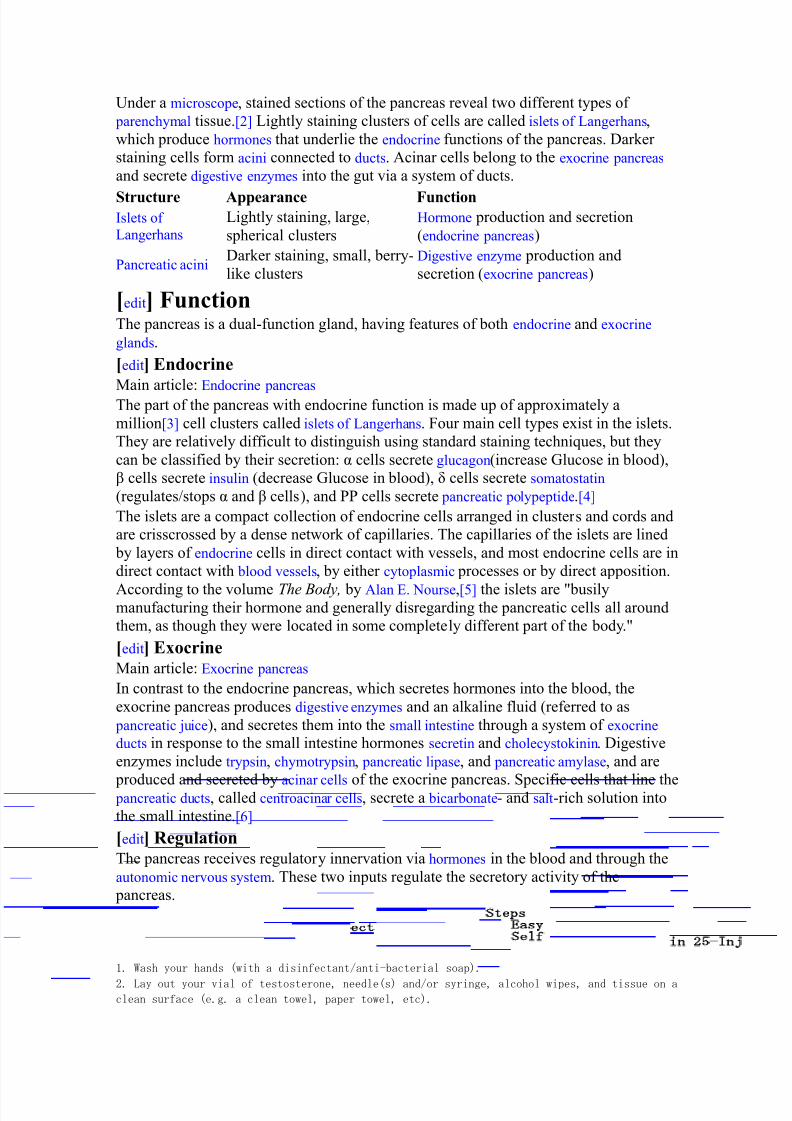
Under a microscope, stained sections of the pancreas reveal two different types of
parenchymal tissue.[2] Lightly staining clusters of cells are called islets of Langerhans,
which produce hormones that underlie the endocrine functions of the pancreas. Darker
staining cells form acini connected to ducts. Acinar cells belong to the exocrine pancreas
and secrete digestive enzymes into the gut via a system of ducts.
Structure Appearance FunctionIslets of
Langerhans Lightly staining, large,
spherical clusters
Hormone production and secretion
(endocrine pancreas)
Pancreatic acini Darker staining, small, berry-
like clusters
Digestive enzyme production and
secretion (exocrine pancreas)
[edit] FunctionThe pancreas is a dual-function gland, having features of both endocrine and exocrine
glands.
[edit] Endocrine
Main article: Endocrine pancreas The part of the pancreas with endocrine function is made up of approximately a
million[3] cell clusters called islets of Langerhans. Four main cell types exist in the islets.
They are relatively difficult to distinguish using standard staining techniques, but they
can be classified by their secretion: α cells secrete glucagon(increase Glucose in blood),
β cells secrete insulin (decrease Glucose in blood), δ cells secrete somatostatin
(regulates/stops α and β cells), and PP cells secrete pancreatic polypeptide.[4]
The islets are a compact collection of endocrine cells arranged in clusters and cords and
are crisscrossed by a dense network of capillaries. The capillaries of the islets are lined
by layers of endocrine cells in direct contact with vessels, and most endocrine cells are in
direct contact with blood vessels, by either cytoplasmic processes or by direct apposition.
According to the volume The Body, by Alan E. Nourse,[5] the islets are "busilymanufacturing their hormone and generally disregarding the pancreatic cells all around
them, as though they were located in some completely different part of the body."
[edit] ExocrineMain article: Exocrine pancreas
In contrast to the endocrine pancreas, which secretes hormones into the blood, the
exocrine pancreas produces digestive enzymes and an alkaline fluid (referred to as
pancreatic juice), and secretes them into the small intestine through a system of exocrine
ducts in response to the small intestine hormones secretin and cholecystokinin. Digestive
enzymes include trypsin, chymotrypsin, pancreatic lipase, and pancreatic amylase, and are
produced and secreted by acinar cells of the exocrine pancreas. Specific cells that line the pancreatic ducts, called centroacinar cells, secrete a bicarbonate- and salt-rich solution into
the small intestine.[6]
[edit] RegulationThe pancreas receives regulatory innervation via hormones in the blood and through the
autonomic nervous system. These two inputs regulate the secretory activity of the
pancreas.
Self-Inject in 25 Easy Steps1. Wash your hands (with a disinfectant/anti-bacterial soap).
2. Lay out your vial of testosterone, needle(s) and/or syringe, alcohol wipes, and tissue on aclean surface (e.g. a clean towel, paper towel, etc).
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 9/59
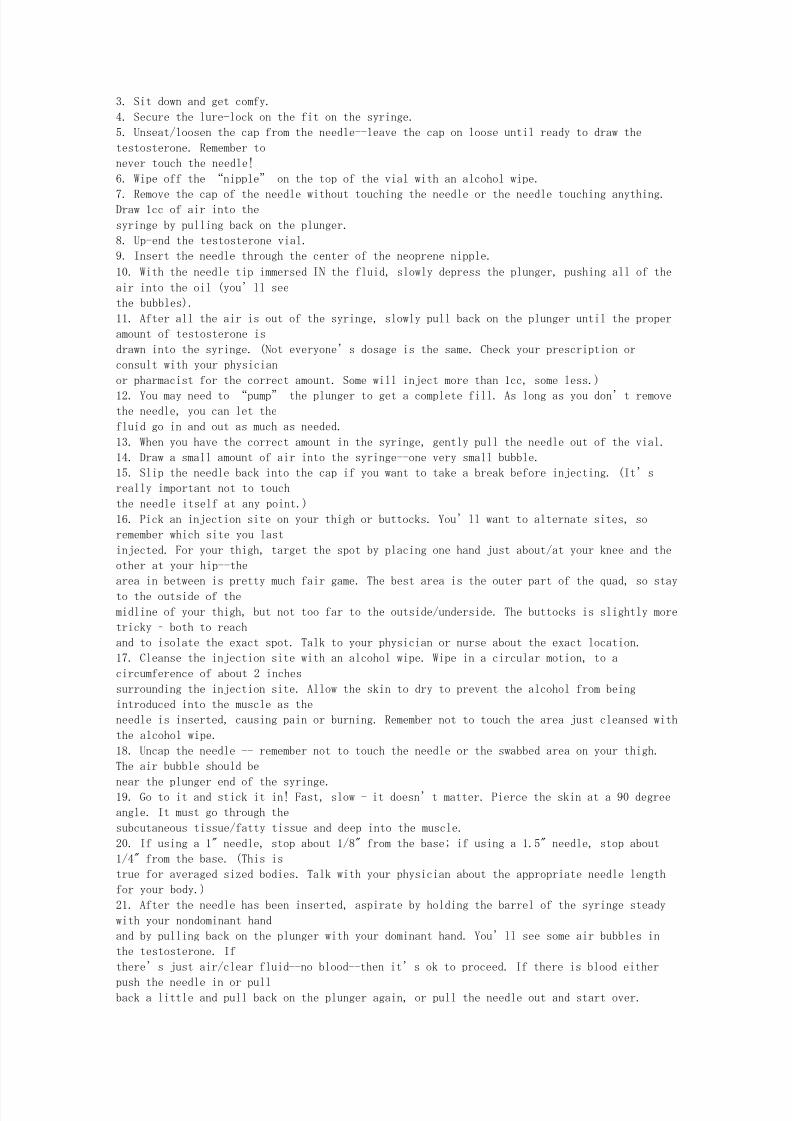
3. Sit down and get comfy.
4. Secure the lure-lock on the fit on the syringe.
5. Unseat/loosen the cap from the needle--leave the cap on loose until ready to draw the
testosterone. Remember to
never touch the needle!
6. Wipe off the “nipple” on the top of the vial with an alcohol wipe.
7. Remove the cap of the needle without touching the needle or the needle touching anything.Draw 1cc of air into the
syringe by pulling back on the plunger.
8. Up-end the testosterone vial.
9. Insert the needle through the center of the neoprene nipple.
10. With the needle tip immersed IN the fluid, slowly depress the plunger, pushing all of the
air into the oil (you’ll see
the bubbles).
11. After all the air is out of the syringe, slowly pull back on the plunger until the proper
amount of testosterone is
drawn into the syringe. (Not everyone’s dosage is the same. Check your prescription or
consult with your physician
or pharmacist for the correct amount. Some will inject more than 1cc, some less.)
12. You may need to “pump” the plunger to get a complete fill. As long as you don’t removethe needle, you can let the
fluid go in and out as much as needed.
13. When you have the correct amount in the syringe, gently pull the needle out of the vial.
14. Draw a small amount of air into the syringe--one very small bubble.
15. Slip the needle back into the cap if you want to take a break before injecting. (It’s
really important not to touch
the needle itself at any point.)
16. Pick an injection site on your thigh or buttocks. You’ll want to alternate sites, so
remember which site you last
injected. For your thigh, target the spot by placing one hand just about/at your knee and the
other at your hip--the
area in between is pretty much fair game. The best area is the outer part of the quad, so stay
to the outside of the
midline of your thigh, but not too far to the outside/underside. The buttocks is slightly more
tricky – both to reach
and to isolate the exact spot. Talk to your physician or nurse about the exact location.
17. Cleanse the injection site with an alcohol wipe. Wipe in a circular motion, to a
circumference of about 2 inches
surrounding the injection site. Allow the skin to dry to prevent the alcohol from being
introduced into the muscle as the
needle is inserted, causing pain or burning. Remember not to touch the area just cleansed with
the alcohol wipe.
18. Uncap the needle -- remember not to touch the needle or the swabbed area on your thigh.
The air bubble should be
near the plunger end of the syringe.19. Go to it and stick it in! Fast, slow - it doesn’t matter. Pierce the skin at a 90 degree
angle. It must go through the
subcutaneous tissue/fatty tissue and deep into the muscle.
20. If using a 1" needle, stop about 1/8" from the base; if using a 1.5" needle, stop about
1/4" from the base. (This is
true for averaged sized bodies. Talk with your physician about the appropriate needle length
for your body.)
21. After the needle has been inserted, aspirate by holding the barrel of the syringe steady
with your nondominant hand
and by pulling back on the plunger with your dominant hand. You’ll see some air bubbles in
the testosterone. If
there’s just air/clear fluid--no blood--then it’s ok to proceed. If there is blood either
push the needle in or pullback a little and pull back on the plunger again, or pull the needle out and start over.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 10/59
22. Holding the syringe steady, inject the testosterone steadily and slowly by depressing the
plunger until all of the
testosterone is injected. The air bubble in the syringe should follow the testosterone and
will “pack” the
testosterone down into your muscle. There will be a slight a “pop” as the bubble leaves the
syringe.
23. Pull the needle out -- again, slow or fast depending upon your preference. (I think it’susually best to pull out slow--
sounds dirty, doesn’t it?!) Sometimes the injection site may bleed a little when you withdraw
the needle, just be
prepared to apply some gentle pressure with some clean tissue(s).
24. Slide the needle back into the cap. (Remember DO NOT reseat the cap by pressing the tip of
the cap towards the
needle’s point.)
25. Dispose of your needles properly in a sharps container.
How To Perform CardiopulmonaryResuscitation (CPR)By Rod Brouhard, About.com Guide
Updated March 29, 2010
About.com Health's Disease and Condition content is reviewed by our Medical Review Board
See More About:
first aid training first aid techniques
cpr
Sponsored Links
SpiderTech TapesAdvanced Pre-cut, Pre-Packaged Kinesiology Taping
Solutionswww.nucapmedical.com
ACLS Test Prep E-LearningACLS exam prep. Cases, hundreds of practice questions, practice
tests.www.focusedmedical.info
"Thumper CPR System"Continous CPR, Fast Deployment Simple Operation, No loss of
CPRwww.michiganinstruments.com
First Aid Ads
CPR Classes CPR Certification CPR Renewal Learning CPR CPR Test
There is no substitute for learning cardiopulmonary resuscitation (CPR), but emergencies don't
wait for training. These instructions are for conventional adult CPR. If you've never been
trained in CPR and the victim collapsed in front of you, use hands-only CPR.
For kids, use the following guidelines:
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 11/59
Infant CPR for kids under 1 year.
Child CPR for kids 1-8 years old.
Not every CPR class is the same. There are CPR classes for healthcare professionals as well as
CPR classes for the layperson. Before you take a CPR class, make sure the class is right for you.
These are the steps to perform adult CPR:
Difficulty: Easy
Time Required: CPR should start as soon as possible
Here's How:
1. Stay Safe! The worst thing a rescuer can do is become another victim. Follow universal
precautions and wear personal protective equipment if you have it. Use common sense
and stay away from potential hazards.
2. Attempt to wake victim. Briskly rub your knuckles against the victim's sternum. If the
victim does not wake, call 911 and proceed to step 3. If the victim wakes, moans, ormoves, then CPR is not necessary at this time. Call 911 if the victim is confused or not
able to speak.
3. Begin rescue breathing. Open the victim's airway using the head-tilt, chin-lift method.
Put your ear to the victim's open mouth:
o look for chest movement
o listen for air flowing through the mouth or nose
o feel for air on your cheek
If there is no breathing, pinch the victim's nose; make a seal over the victim's mouth
with yours. Use a CPR mask if available. Give the victim a breath big enough to make
the chest rise. Let the chest fall, then repeat the rescue breath once more. If the chest
doesn't rise on the first breath, reposition the head and try again. Whether it works on
the second try or not, go to step 4.
4. Begin chest compressions. Place the heel of your hand in the middle of the victim's
chest. Put your other hand on top of the first with your fingers interlaced. Compress
the chest about 1-1/2 to 2 inches (4-5 cm). Allow the chest to completely recoil before
the next compression. Compress the chest at a rate equal to 100/minute. Perform 30
compressions at this rate.
5. Repeat rescue breaths. Open the airway with head-tilt, chin-lift again. This time, go
directly to rescue breaths without checking for breathing again. Give one breath,
making sure the chest rises and falls, then give another. Remember, if the chest doesn't
rise on the first breath, reposition the head before you give the second breath.
6. Perform 30 more chest compressions. Repeat steps 5 and 6 for about two minutes.
7. After 2 minutes of chest compressions and rescue breaths, stop compressions and
recheck victim for breathing. If the victim is not breathing, continue chest
compressions and rescue breaths.
8. Keep going until help arrives.
Tips:
1. If you have acces to an automated external defibrillator, attach it to the victim after
approximately one minute of CPR (chest compressions and rescue breaths).
2. Chest compressions are extremely important. If you are not comfortable giving rescue
breaths, still perform chest compressions!

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 12/59
3. It's normal to feel pops and snaps when you first begin chest compressions - DON'T
STOP! You aren't going to make the victim any worse. Cardiac arrest is as bad as it gets.
4. When performing chest compressions, do not let your hands bounce. Let the chest
fully recoil, but keep the heel of your hand in contact with the sternum at all times.
5. For more information on these steps go to the Emergency Cardiac Care (ECC)
Guidelines from the American Heart Association.
CPR BasicsCardiopulmonary resuscitation (CPR) is a first-aid technique used to keep victims of
cardiopulmonary arrest alive and to prevent brain damage while more advanced medical
help is on the way. CPR has two goals:
keep blood flowing throughout the body
keep air flowing in and out of the lungs
While the modern emergency room has high-tech equipment and an arsenal of drugs to
help treat victims of cardiopulmonary arrest, CPR is a simple technique that requires
little or no equipment. What you do is pretty basic:
Blow into the victim's mouth to push oxygenated air into the lungs. This allows
oxygen to diffuse through the lining of the lungs into the bloodstream.
Compress the victim's chest to artificially re-create blood circulation.
Here are the steps that make up CPR:
Photo courtesy of University of Washington
It sounds pretty simple, but as you can see above, CPR must be performed in a specific,
timed sequence to accurately mimic your body's natural breathing pattern and the wayyour heart pumps. When someone collapses right in front of you, your first reaction is

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 13/59
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 14/59
Cite This!Close
Please copy/paste the following text to properly cite this HowStuffWorks article:
Meeker-O'Connell, Ann. "How CPR Works." 08 January 2001. HowStuffWorks.com.
<http://health.howstuffworks.com/cpr.htm> 18 June 2010.Inside this Article
1. Introduction to How CPR Works
2. Cardiopulmonary Arrest
3. CPR Basics
4. CPR Step-by-Step
5. The ABCs
6. CPR's Role in Rescue
7. See more »
7. CPR and Infectious Disease
8. Lots More Information 9. See all First Aid articles
Health Videos
More Health Videos »
The ABCsHere's a summary of how you might perform CPR on a non-responsive adult (There is
actually a different procedure used to save infants and young children). To learn all
about CPR in detail, so that you could actually practice and perform this life-saving act,
you should sign up for training from an organization like the American Red Cross.
A is for Airway
When you pass out, your tongue relaxes, and it can roll back in your mouth and block
your windpipe. Before you can start CPR on an unconscious person, you'll probably
need move their tongue out of the way. Here's how to clear a blocked airway:
1. Place the palm of your hand across the victim's forehead and push down gently.
2. With the other hand, slowly lift the chin forward and slightly up.
3. Move the chin up until the teeth are almost together, but the mouth is still
slightly open.
Tilting the head back and lifting the chin move the tongue out of the airway. At this
point, you should check again for breathing. If the victim is choking on something, you
may see their chest heave as they try to breathe, but you won't be able to feel or hear air
being exhaled. You'll have to take additional measures to clear out what's blocking
their windpipe, including:
1. Compressing the abdomen with forceful thrusts. This creates pressure that forces
the object up and out of the windpipe.
2. Trying to manually dislodge the object with your fingers.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 15/59
Once this is done, you have to check for signs of breathing again. Just clearing out the
windpipe may sometimes be enough to allow the victim to start breathing on their own!
If the victim starts breathing and moving around on their own, you can stop CPR. If this
doesn't happen, you'll have to help them breath, by providing mouth-to-mouth
resuscitation.
B is for Breathing
Your lungs have one main function: remove carbon dioxide and take up oxygen.
Normally, the muscles in your chest contract and expand your chest cavity, allowing
your lungs to fill up with air. Oxygen and carbon dioxide diffuse across the immense
surface area of your lungs. Finally, your chest muscles relax, and you exhale. (To learn
more about lungs, see How Your Lungs Work ).
Rescue breathing uses your lungs to force air into the victim's lungs at regular
intervals. The timing of each breath (about 1.5 to 2 seconds per breath) mimics normal
breathing. However, the process is much more like blowing up a balloon than real
breathing. You inhale deeply, form a tight seal with your mouth over their mouth, andexhale strongly to push air out of your mouth into theirs. Because you also pinch the
victim's nostrils closed, the air has nowhere to go except down into the lungs, which
expand as they fill with air.
Mouth-to-mouth breathing is hard work. Normally, when you inhale, the chest muscles
drive the process. In artificial respiration, you're working against the victim's relaxed
chest muscles. When the chest muscles are relaxed, the chest cavity is small, keeping
the lungs in a deflated state. As a rescuer, you have to exhale forcefully into the victim's
mouth for 1 to 2 seconds to overcome this resistance. As the lungs fill with air, the
victim's chest is pushed up at the same time; you can actually see it rise. When you
remove your mouth from the victim's and break the air seal, their chest falls and once
again deflates the lungs. As in normal breathing, this results in air being exhaled fromthe victim's mouth.
Does air exhaled from someone else's mouth really provide enough oxygen to save an
unconscious person? Normally, the air you inhale contains about 20 percent oxygen by
volume, and your lungs remove about 5 percent of the oxygen in each breath. The air
you blow into a victim's mouth thus contains about 15 to 16 percent oxygen, which is
more than enough to supply their needs.
After you've given the victim two breaths, you then check to see whether or not they
have a pulse and whether they are able to breathe on their own. This will determine
what you do next.
If the victim . . . you shouldIs breathing and has a
pulse
stop CPR, and stay with them until help
arrives.
Is not breathing and
has a pulsecontinue rescue breathing.
Has no pulse begin chest compressions, alternating
with rescue breathing.
C is for Circulation
If the victim's heart is not beating, all your breathing efforts are for naught; the oxygen
that you're getting into their circulation isn't going anywhere! Once again, you have totake over for a failing organ. This time you essentially become a surrogate heart to
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 16/59
pump oxygenated blood out to the rest of the victim's body. How can you have any
effect on blood flow from outside of the body? All it takes is your hands and some
strength. The steps are simple:
1. Kneeling by the victim, place the heel of your hands one atop the other about .4
to .8 inches (1 to 2 cm) from tip of the breastbone.
2. Using the weight of your body, push the victim's chest down. You shouldcompress their chest 1 to 2 inches (2.54 to 5.08 cm).
3. Hold in this position for half a second, then relax for half a second
4. Repeat steps two and three 29 more times.
5. Give the victim two rescue breaths as you did before to deliver more oxygen to
the blood.
6. Repeat steps 1 through 5 three more times, then check for a pulse.
In reality, all you are doing is squeezing the heart between the breastbone and the
backbone to force blood out. Compressing the chest creates positive pressure inside
the chest that pushes oxygenated blood out of the heart through the aorta. From here, it
travels to the brain and then on to other parts of the body, delivering oxygen forcellular respiration. When you relax, the pressure inside the victim's chest subsides.
Deoxygenated blood moves back into the heart from the veins.
Introduction
Frequently the equine practitioner encounters situations
in which an alternate form of external coaptation
is desirable in the management of injuries of
the lower limb. Traditional fiberglass casts are
ideal for providing rigid coaptation in most cases but
do not allow access to the soft tissues of the limb and
typically require replacement every 3–6 weeks.
A bandage cast is a reusable form of a traditional
cast that maintains rigid stabilization of the limb
yet is amenable to frequent removal and resetting
with the primary advantage of allowing the clinician
access to the underlying soft tissues.
The most common indications for the use of the
bandage cast in our practice are for the management
of severe soft tissue injuries (i.e., tendon lacerations,
extensive wounds over areas under tension) and for
selected orthopedic injuries. We also use the bandage
cast routinely as a form of temporary externalcoaptation for horses recovering from general anesthesia
after undergoing internal fixation for lower
limb fractures.
Case selection is very important when deciding if
a bandage cast has advantages for case management
over traditional casting methods. If instability
of the lower limb exists, it is imperative that the
horse can comfortably and safely stand during the
bandage changes without compromising the integrity
of the repair.
Methods
In most cases, a bandage cast is initially conformed
to the limb while the horse is under general anesthesia

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 17/59
and in association with a surgical repair of
the injury. The bandage cast can be applied in a
standing horse although this is less desirable.
1. A light sterile dressing of conforming gauze is
placed over the incision or wound.
2. Two or three pieces of thin sheet cotton are
gathered together and rolled tightly around
the limb and secured with a roll of brown
gauze. The foot is included. Follow with a
roll of Vetrapa to make a smooth bandage.
3. Place a strip of orthopedic felt around the
proximal cannon bone and secure. Stockinet
is usually not necessary.
4. Apply one roll of casting foamb around the
limb and follow with the desired number of
rolls of fiberglass casting material. Incorporate
the foot and shape as you would a traditional
cast. Provide adequate reinforcementto the bottom of the foot to insure longevity of
the cast.150 2000 / Vol. 46 / AAEP PROCEEDINGS
HOW-TO SESSION
NOTES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVISProceedings of the Annual Convention of the AAEP 2000
5. Optional: Pre-cut the cast with cast cutters
along the medial and lateral aspects (leave the
bottom of the foot intact) and then wrap
tightly with Duct-tape the entire length of the
limb for recovery from anesthesia.6. If the cast was precut, run a scalpel blade
down through the grooves to release the tape
and remove when a bandage change is desired.
If not precut, bivalve the cast under
mild sedation and restraint and pull the cast
apart, lifting the foot out of the bottom.
7. Tend to the incision or wound and replace the
bandage, making sure to wrap firmly so that
the limb will fit back into the cast. Place the
bivalved cast back on the limb and apply duct
tape—an assistant may be required to hold
the two pieces tightly together while the tape
is being applied.
Results and Discussion
All horses have generally tolerated a bandage cast
as they would a traditional cast and have rarely
shown discomfort. Cast sores have been negligible
due to the amount of padding provided by the bandage
material. Length of time of use has ranged
from 3–12 weeks with bandage changes performed
every 3–4 days depending upon the demands of the
particular injury. The most common problems encountered
with the cast are premature wearing ofthe bottom of the cast and occasional difficulty in
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 18/59
refitting the cast if bandage material has been applied
too loosely.
For management of soft tissue injuries in our
practice, the bandage cast has been a very useful
adjunct in the treatment of extensor and flexor tendon
lacerations, open wounds of the fetlock and pastern
joints, severe run-down lacerations, and large
chronic granulating wounds. Orthopedic injuries
managed with a bandage cast include fetlock joint
subluxations, several cases of internal fixation
which required regular wound care, and two cases of
previously repaired cannon bone fractures that subsequently
became unstable in the postoperative period.
In these two cases, general anesthesia for
cast application was undesirable and previously
made bandage casts were applied instead.
For lower limb fractures repaired with internal
fixation (i.e., fractures of the distal cannon or proximalfirst phalanx), a generic bandage cast is fitted
and applied to the limb for anesthetic recovery and
A reusable bivalved bandage cast. then removed shortly thereafter. These casts haveInitial splitting of the bandage cast for future use.
AAEP PROCEEDINGS / Vol. 46 / 2000 151
HOW-TO SESSIONReprinted in the IVIS website with the permission of AAEP Close window to return to IVISProceedings of the Annual Convention of the AAEP 2000
been previously constructed and are tailored to fit
each individual by the amount of bandage material
placed underneath. This method of coaptation for
recovery has been used successfully and safely inapproximately 300 cases in our practice with no
untoward effects.
Conclusion
In summary, a bandage cast offers the clinician the
advantages of rigid external coaptation yet allow for
the opportunity to provide care to the soft tissue
structures of the limb. Additionally, a bandage
cast can be a cost-efficient method of providing external
immobilization for recovery of selected cases
from general anesthesia.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 19/59
Euthanasia
Euthanasia is the deliberate killing of a person for the benefit of that person.
In most cases euthanasia is carried out because the person who dies asks for it, but there are
cases called euthanasia where a person can't make such a request.
Forms of euthanasia
The different types of euthanasia, some of which may be seen as more or less acceptable
depending on your outlook.
Forms of euthanasiaEuthanasia comes in several different forms, each of which brings a different set of rights and
wrongs.
Active and passive euthanasiaIn active euthanasia a person directly and deliberately causes the patient's death. In passive
euthanasia they don't directly take the patient's life, they just allow them to die.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 20/59
This is a morally unsatisfactory distinction, since even though a person doesn't 'actively kill' the
patient, they are aware that the result of their inaction will be the death of the patient.
Active euthanasia is when death is brought about by an act - for example when a person is
killed by being given an overdose of pain-killers.
Passive euthanasia is when death is brought about by an omission - i.e. when someone lets the
person die. This can be by withdrawing or withholding treatment:
Withdrawing treatment: for example, switching off a machine that is keeping a person
alive, so that they die of their disease.
Withholding treatment: for example, not carrying out surgery that will extend life for a
short time.
Traditionally, passive euthanasia is thought of as less bad than active euthanasia. But some
people think active euthanasia is morally better.
Voluntary and involuntary euthanasiaVoluntary euthanasia occurs at the request of the person who dies.
Non-voluntary euthanasia occurs when the person is unconscious or otherwise unable (for
example, a very young baby or a person of extremely low intelligence) to make a meaningful
choice between living and dying, and an appropriate person takes the decision on their behalf.
Non-voluntary euthanasia also includes cases where the person is a child who is mentally and
emotionally able to take the decision, but is not regarded in law as old enough to take such a
decision, so someone else must take it on their behalf in the eyes of the law.
Involuntary euthanasia occurs when the person who dies chooses life and is killed anyway. This
is usually called murder, but it is possible to imagine cases where the killing would count as
being for the benefit of the person who dies.
Indirect euthanasiaThis means providing treatment (usually to reduce pain) that has the side effect of speeding
the patient's death.
Since the primary intention is not to kill, this is seen by some people (but not all) as morally
acceptable.
A justification along these lines is formally called the doctrine of double effect.
Assisted suicideThis usually refers to cases where the person who is going to die needs help to kill themselves
and asks for it. It may be something as simple as getting drugs for the person and putting those
drugs within their reach.
Arguments against euthanasiaThis page sets out the arguments against allowing euthanasia. Could euthanasia ever be safely
regulated? Would legalising euthanasia have knock-on effects?
Overview of arguments against euthanasia
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 21/59
It's possible to argue about the way we've divided up the arguments, and many arguments
could fall into more categories than we've used.
Ethical arguments
Euthanasia weakens society's respect for the sanctity of life
Accepting euthanasia accepts that some lives (those of the disabled or sick) are worthless than others
Voluntary euthanasia is the start of a slippery slope that leads to involuntary
euthanasia and the killing of people who are thought undesirable
Euthanasia might not be in a person's best interests
Euthanasia affects other people's rights, not just those of the patient
Practical arguments
Proper palliative care makes euthanasia unnecessary
There's no way of properly regulating euthanasia
Allowing euthanasia will lead to less good care for the terminally ill
Allowing euthanasia undermines the committment of doctors and nurses to
saving lives
Euthanasia may become a cost-effective way to treat the terminally ill
Allowing euthanasia will discourage the search for new cures and treatments
for the terminally ill
Euthanasia undermines the motivation to provide good care for the dying, and
good pain relief
Euthanasia gives too much power to doctors
Euthanasia exposes vulnerable people to pressure to end their lives Moral pressure on elderly relatives by selfish families
Moral pressure to free up medical resources
Patients who are abandoned by their families may feel euthanasia is the only
solution
Historical arguments
Voluntary euthanasia is the start of a slippery slope that leads to involuntary
euthanasia and the killing of people who are thought undesirable
Religious arguments
Euthanasia is against the word and will of God
Euthanasia weakens society's respect for the sanctity of life
Suffering may have value
Voluntary euthanasia is the start of a slippery slope that leads to involuntary
euthanasia and the killing of people who are thought undesirable
Top
Against the will of GodReligious people don't argue that we can't kill ourselves, or get others to do it. They know that
we can do it because God has given us free will. Their argument is that it would be wrong for usto do so.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 22/59
They believe that every human being is the creation of God, and that this imposes certain limits
on us. Our lives are not only our lives for us to do with as we see fit.
To kill oneself, or to get someone else to do it for us, is to deny God, and to deny God's rights
over our lives and his right to choose the length of our lives and the way our lives end.
The value of sufferingReligious people sometimes argue against euthanasia because they see positive value in
suffering.
Down through the centuries and generations it has been seen that in suffering
there is concealed a particular power that draws a person interiorly close to Christ,
a special grace.
Pope John Paul II: Salvifici Doloris, 1984
The religious attitude to sufferingMost religions would say something like this:
We should relieve suffering when we can, and be with those who suffer, helping
them to bear their suffering, when we can't. We should never deal with the
problem of suffering by eliminating those who suffer.
The nature of sufferingChristianity teaches that suffering can have a place in God's plan, in that it allows the sufferer
to share in Christ's agony and his redeeming sacrifice. They believe that Christ will be present
to share in the suffering of the believer.
Pope John Paul II wrote that "It is suffering, more than anything else, which clears the way for
the grace which transforms human souls."
However while the churches acknowledge that some Christians will want to accept some
suffering for this reason, most Christians are not so heroic.
So there is nothing wrong in trying to relieve someone's suffering. In fact, Christians believe
that it is a good to do so, as long as one does not intentionally cause death.
Dying is good for us
Some people think that dying is just one of the tests that God sets for human beings, and thatthe way we react to it shows the sort of person we are, and how deep our faith and trust in
God is.
Others, while acknowledging that a loving God doesn't set his creations such a horrible test,
say that the process of dying is the ultimate opportunity for human beings to develop their
souls.
When people are dying they may be able, more than at any time in their life, to concentrate on
the important things in life, and to set aside the present-day 'consumer culture', and their own
ego and desire to control the world. Curtailing the process of dying would deny them this
opportunity.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 23/59
Eastern religionsSeveral Eastern religions believe that we live many lives and the quality of each life is set by the
way we lived our previous lives.
Those who believe this think that suffering is part of the moral force of the universe, and that
by cutting it short a person interferes with their progress towards ultimate liberation.
A non-religious viewSome non-religious people also believe that suffering has value. They think it provides an
opportunity to grow in wisdom, character, and compassion.
Suffering is something which draws upon all the resources of a human being and enables them
to reach the highest and noblest points of what they really are.
Suffering allows a person to be a good example to others by showing how to behave when
things are bad.
M Scott Peck, author of The Road Less Travelled , has written that in a few weeks at the end oflife, with pain properly controlled a person might learn
how to negotiate a middle path between control and total passivity, about how to
welcome the responsible care of strangers, about how to be dependent once
again ... about how to trust and maybe even, out of existential suffering, at least a
little bit about how to pray or talk with God.
M Scott Peck
The nature of sufferingIt isn't easy to define suffering - most of us can decide when we are suffering but what is
suffering for one person may not be suffering for another.
It's also impossible to measure suffering in any useful way, and it's particularly hard to come up
with any objective idea of what constitutes unbearable suffering, since each individual will
react to the same physical and mental conditions in a different way.
Top
Sanctity of lifeThis argument says that euthanasia is bad because of the sanctity of human life.
There are four main reasons why people think we shouldn't kill human beings:
All human beings are to be valued, irrespective of age, sex, race, religion, social status
or their potential for achievement
Human life is a basic good as opposed to an instrumental good, a good in itself rather
than as a means to an end
Human life is sacred because it's a gift from God
Therefore the deliberate taking of human life should be prohibited except in self-
defence or the legitimate defence of others
We are valuable for ourselves
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 24/59
The philosopher Immanuel Kant said that rational human beings should be treated as an end in
themselves and not as a means to something else. The fact that we are human has value in
itself.
Our inherent value doesn't depend on anything else - it doesn't depend on whether we are
having a good life that we enjoy, or whether we are making other people's lives better. Weexist, so we have value.
Most of us agree with that - though we don't put it in philosopher-speak. We say that we don't
think that we should use other people - which is a plain English way of saying that we shouldn't
treat other people as a means to our own ends.
We must respect our own valueIt applies to us too. We shouldn't treat ourselves as a means to our own ends.
And this means that we shouldn't end our lives just because it seems the most effective way of
putting an end to our suffering. To do that is not to respect our inherent worth.
Top
The slippery slopeMany people worry that if voluntary euthanasia were to become legal, it would not be long
before involuntary euthanasia would start to happen.
We concluded that it was virtually impossible to ensure that all acts of euthanasia
were truly voluntary and that any liberalisation of the law in the United Kingdom
could not be abused.
We were also concerned that vulnerable people - the elderly, lonely, sick or
distressed - would feel pressure, whether real or imagined, to request early death.
Lord Walton, Chairman, House of Lords Select Committee on Medical Ethics
looking into euthanasia, 1993
This is called the slippery slope argument. In general form it says that if we allow something
relatively harmless today, we may start a trend that results in something currently unthinkable
becoming accepted.
Those who oppose this argument say that properly drafted legislation can draw a firm barrieracross the slippery slope.
Various forms of the slippery slope argumentIf we change the law and accept voluntary euthanasia, we will not be able to keep it under
control.
Proponents of euthanasia say: Euthanasia would never be legalised without proper
regulation and control mechanisms in place
Doctors may soon start killing people without bothering with their permission.
Proponents say: There is a huge difference between killing people who ask for death under appropriate circumstances, and killing people without their permission
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 25/59
Very few people are so lacking in moral understanding that they would ignore this
distinction
Very few people are so lacking in intellect that they can't make the distinction above
Any doctor who would ignore this distinction probably wouldn't worry about the law
anyway
Health care costs will lead to doctors killing patients to save money or free up beds:
Proponents say: The main reason some doctors support voluntary euthanasia is
because they believe that they should respect their patients' right to be treated as
autonomous human beings
That is, when doctors are in favour of euthanasia it's because they want to respect the
wishes of their patients
So doctors are unlikely to kill people without their permission because that contradicts
the whole motivation for allowing voluntary euthanasia
But cost-conscious doctors are more likely to honour their patients' requests for death A 1998 study found that doctors who are cost-conscious and 'practice resource-
conserving medicine' are significantly more likely to write a lethal prescription for
terminally-ill patients [ Arch. Intern. Med., 5/11/98, p. 974]
This suggests that medical costs do influence doctors' opinions in this area of medical
ethics
The Nazis engaged in massive programmes of involuntary euthanasia, so we shouldn't place
our trust in the good moral sense of doctors.
Proponents say: The Nazis are not a useful moral example, because their actions are
almost universally regarded as both criminal and morally wrong
The Nazis embarked on invountary euthanasia as a deliberate political act - they didn't
slip into it from voluntary euthanasia (although at first they did pretend it was for the
benefit of the patient)
What the Nazis did wasn't euthanasia by even the widest definition, it was the use of
murder to get rid of people they disapproved of
The universal horror at Nazi euthanasia demonstrates that almost everyone can make
the distinction between voluntary and involuntary euthanasia
The example of the Nazis has made people more sensitive to the dangers of involuntary
euthanasia
Allowing voluntary euthanasia makes it easier to commit murder, since the perpetrators can
disguise it as active voluntary euthanasia.
Proponents say: The law is able to deal with the possibility of self-defence or suicide
being used as disguises for murder. It will thus be able to deal with this case equally
well
To dress murder up as euthanasia will involve medical co-operation. The need for a
conspiracy will make it an unattractive option
Many are needlessly condemned to suffering by the chief anti-euthanasia
argument: that murder might lurk under the cloak of kindness.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 26/59
A C Grayling, Guardian 2001
Top
Devalues some livesSome people fear that allowing euthanasia sends the message, "it's better to be dead than sick
or disabled".
The subtext is that some lives are not worth living. Not only does this put the sick or disabled at
risk, it also downgrades their status as human beings while they are alive.
The disabled person's perspectivePart of the problem is that able-bodied people look at things from their own perspective and
see life with a disability as a disaster, filled with suffering and frustration.
Some societies have regarded people with disabilities as inferior, or as a burden on society.
Those in favour of eugenics go further, and say that society should prevent 'defective' peoplefrom having children. Others go further still and say that those who are a burden on society
should be eliminated.
People with disabilities don't agree. They say:
All people should have equal rights and opportunities to live good lives
Many individuals with disabilities enjoy living
Many individuals without disabilities don't enjoy living, and no-one is threatening them
The proper approach to people with disabilities is to provide them with appropriate
support, not to kill them
The quality of a person's life should not be assessed by other people
The quality of life of a person with disabilities should not be assessed without providing
proper support first
Opposition to this argumentSupporters of euthanasia would respond that this argument includes a number of completely
misleading suggestions, and refute them:
Dying is not the same as never having been born
The debate is nothing to do with preventing disabled babies being born, or preventing
people with disabilities from becoming parents
Nobody is asking for patients to be killed against their wishes - whether or not those
patients are disabled
The euthanasia procedure is intended for use by patients who are dying, or in a
condition that will get worse - most disabilities don't come under that category
The normal procedure for euthanasia would have to be initiated at the patient's
request
Disabled people who are not mentally impaired are just as capable as able-bodied
people of deciding what they want
Protections will be in place for patients who are mentally impaired, whether through
disability or some other reason
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 27/59
It is possible that someone who has just become disabled may feel depressed enough
to ask for death, which is why any proposed system of euthanasia must include
psychological support and assessment before the patient's wish is granted
All people should have equal rights and opportunities to live, or to choose not to go on
living
Top
Patient's best interestsA serious problem for supporters of euthanasia are the number of cases in which a patient may
ask for euthanasia, or feel obliged to ask for it, when it isn't in their best interest. Some
examples are listed below:
the diagnosis is wrong and the patient is not terminally ill
the prognosis (the doctor's prediction as to how the disease will progress) is wrong and
the patient is not going to die soon
the patient is getting bad medical care and their suffering could be relieved by other
means
the doctor is unaware of all the non-fatal options that could be offered to the patient
the patient's request for euthanasia is actually a 'cry for help', implying that life is not
worth living now but could be worth living if various symptoms or fears were managed
the patient is depressed and so believes things are much worse than they are
the patient is confused and unable to make sensible judgements
the patient has an unrealistic fear of the pain and suffering that lies ahead
the patient is feeling vulnerable
the patient feels that they are a worthless burden on others
the patient feels that their sickness is causing unbearable anguish to their family
the patient is under pressure from other people to feel that they are a burden
the patient is under pressure because of a shortage of resources to care for them
the patient requests euthanasia because of a passing phase of their disease, but is
likely to feel much better in a while
Supporters of euthanasia say these are good reasons to make sure the euthanasia process will
not be rushed, and agree that a well-designed system for euthanasia will have to take all these
points into account. They say that most of these problems can be identified by assessing the
patient properly, and, if necessary, the system should discriminate against the opinions of
people who are particularly vulnerable.
Chochinov and colleagues found that fleeting or occasional thoughts of a desire for death were
common in a study of people who were terminally ill, but few patients expressed a genuine
desire for death. (Chochinov HM, Tataryn D, Clinch JJ, Dudgeon D. Will to live in the terminally
ill. Lancet 1999; 354: 816-819)
They also found that the will to live fluctuates substantially in dying patients, particularly in
relation to depression, anxiety, shortness of breath, and their sense of wellbeing.
Other people have rights too

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 28/59
Euthanasia is usually viewed from the viewpoint of the person who wants to die, but it affects
other people too, and their rights should be considered.
family and friends
medical and other carers
other people in a similar situation who may feel pressured by the decision of thispatient
society in general
Top
Proper palliative carePalliative care is physical, emotional and spiritual care for a dying person when cure is not
possible. It includes compassion and support for family and friends.
Competent palliative care may well be enough to prevent a person feeling any need to
contemplate euthanasia.
You matter because you are you. You matter to the last moment of your life and
we will do all we can to help you die peacefully, but also to live until you die.
Dame Cicely Saunders, founder of the modern hospice movement
The key to successful palliative care is to treat the patient as a person, not as a set of
symptoms, or medical problems.
The World Health Organisation states that palliative care affirms life and regards dying as a
normal process; it neither hastens nor postpones death; it provides relief from pain andsuffering; it integrates the psychological and spiritual aspects of the patient.
Making things better for patient, family and friendsThe patient's family and friends will need care too. Palliative care aims to enhance the quality
of life for the family as well as the patient.
Effective palliative care gives the patient and their loved ones a chance to spend quality time
together, with as much distress removed as possible. They can (if they want to) use this time to
bring any unfinished business in their lives to a proper closure and to say their last goodbyes.
Palliative care should aim to make it easier and more attractive for family and friends to visit
the dying person. A survey (USA 2001) showed that terminally ill patients actually spent the
vast majority of their time on their own, with few visits from medical personnel or family
members.
Spiritual careSpiritual care may be important even for non-religious people. Spiritual care should be
interpreted in a very wide sense, since patients and families facing death often want to search
for the meaning of their lives in their own way.
Palliative care and euthanasia
Good palliative care is the alternative to euthanasia. If it was available to every patient, itwould certainly reduce the desire for death to be brought about sooner.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 29/59
But providing palliative care can be very hard work, both physically and psychologically. Ending
a patient's life by injection is quicker and easier and cheaper. This may tempt people away from
palliative care.
Legalising euthanasia may reduce the availability of palliative care
Some fear that the introduction of euthanasia will reduce the availability of palliative care inthe community, because health systems will want to choose the most cost effective ways of
dealing with dying patients.
Medical decision-makers already face difficult moral dilemmas in choosing between competing
demands for their limited funds. So making euthanasia easier could exacerbate the slippery
slope, pushing people towards euthanasia who may not otherwise choose it.
When palliative care is not enoughPalliative care will not always be an adequate solution:
Pain: Some doctors estimate that about 5% of patients don't have their pain properly
relieved during the terminal phase of their illness, despite good palliative and hospice
care
Dependency: Some patients may prefer death to dependency, because they hate
relying on other people for all their bodily functions, and the consequent loss of
privacy and dignity
Lack of home care: Other patients will not wish to have palliative care if that means
that they have to die in a hospital and not at home
Loss of alertness: Some people would prefer to die while they are fully alert and and
able to say goodbye to their family; they fear that palliative care would involve a level
of pain-killing drugs that would leave them semi-anaesthetised
Not in the final stages: Other people are grateful for palliative care to a certain point in
their disease, but after that would prefer to die rather than live in a state of
helplessness and distress, regardless of what is available in terms of pain-killing and
comfort.
There should be no law or morality that would limit a clinical team or doctor from
administering the frequent dosages of pain medication that are necessary to free
people's minds from pain that shrivels the spirit and leaves no time for speaking
when, at times, there are very few hours or days left for such communication.
Dr. David Roy, Director of the Centre for Bioethics, Clinical Research Institute of
Montreal
Top
Fears about regulationEuthanasia opponents don't believe that it is possible to create a regulatory system for
euthanasia that will prevent the abuse of euthanasia.
Top
It gives doctors too much power

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 30/59
This argument often appears as 'doctors should not be allowed to play God'. Since God
arguments are of no interest to people without faith, it's presented here with the God bit
removed.
Doctors should not be allowed to decide when people die:
Doctors do this all the time
Any medical action that extends life changes the time when a person dies and we don't
worry about that
This is a different sort of decision, because it involves shortening life
Doctors take this sort of decision all the time when they make choices about treatment
As long as doctors recognise the seriousness of euthanasia and take decisions about it
within a properly regulated structure and with proper safeguards, such decisions
should be acceptable
In most of these cases the decision will not be taken by the doctor, but by the patient.
The doctor will provide information to the patient to help them make their decision
Since doctors give patients the information on which they will base their decisions about
euthanasia, any legalisation of euthanasia, no matter how strictly regulated, puts doctors in an
unacceptable position of power.
Doctors have been shown to take these decisions improperly, defying the guidelines of the
British Medical Association, the Resuscitation Council (UK), and the Royal College of Nursing:
An Age Concern dossier in 2000 showed that doctors put Do Not Resuscitate orders in
place on elderly patients without consulting them or their families
Do Not Resuscitate orders are more commonly used for older people and, in the United
States, for black people, alcohol misusers, non-English speakers, and people infected
with Human Immunodeficiency V irus. This suggests that doctors have stereotypes of
who is not worth saving
Top
Pressure on the vulnerableThis is another of those arguments that says that euthanasia should not be allowed because it
will be abused.
The fear is that if euthanasia is allowed, vulnerable people will be put under pressure to end
their lives. It would be difficult, and possibly impossible, to stop people using persuasion or
coercion to get people to request euthanasia when they don't really want it.
I have seen . . . AIDS patients who have been totally abandoned by their parents,
brothers and sisters and by their lovers.
In a state of total isolation, cut off from every source of life and affection, they
would see death as the only liberation open to them.
In those circumstances, subtle pressure could bring people to request immediate,
rapid, painless death, when what they want is close and powerful support andlove.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 31/59
evidence to the Canadian Senate Committee on Euthanasia and Assisted Suicide
The pressure of feeling a burdenPeople who are ill and dependent can often feel worthless and an undue burden on those who
love and care for them. They may actually be a burden, but those who love them may be happy
to bear that burden.
Nonetheless, if euthanasia is available, the sick person may pressure themselves into asking for
euthanasia.
Pressure from family and othersFamily or others involved with the sick person may regard them as a burden that they don't
wish to carry, and may put pressure (which may be very subtle) on the sick person to ask for
euthanasia.
Increasing numbers of examples of the abuse or neglect of elderly people by their families
makes this an important issue to consider.
Financial pressureThe last few months of a patient's life are often the most expensive in terms of medical and
other care. Shortening this period through euthanasia could be seen as a way of relieving
pressure on scarce medical resources, or family finances.
It's worth noting that cost of the lethal medication required for euthanasia is less than £50,
which is much cheaper than continuing treatment for many medical conditions.
Some people argue that refusing patients drugs because they are too expensive is a form of
euthanasia, and that while this produces public anger at present, legal euthanasia provides aless obvious solution to drug costs.
If there was 'ageism' in health services, and certain types of care were denied to those over a
certain age, euthanasia could be seen as a logical extension of this practice.
Arguments in favour of euthanasiaThis page sets out the arguments in favour of allowing euthanasia in certain cases. Should we
accept that euthanasia happens and try to regulate it safely? Do people have the right to
arrange their own deaths?
Overview of arguments in favour of euthanasiaArguments in favour of euthanasia can be broken down into a few main categories:
Arguments based on rights
People have an explicit right to die
A separate right to die is not necessary, because our other human rights imply the right
to die
Death is a private matter and if there is no harm to others, the state and other people
have no right to interfere (a libertarian argument)
Practical arguments It is possible to regulate euthanasia

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 32/59
Death is a private matter and if there is no harm to others, the state and other people
have no right to interfere (a libertarian argument)
Allowing people to die may free up scarce health resources (this is a possible argument,
but no authority has seriously proposed it)
Euthanasia happens anyway (a utilitarian or consequentialist argument)
Philosophical arguments
Euthanasia satisfies the criterion that moral rules must be universalisable
Euthanasia happens anyway (a utilitarian or consequentialist argument)
Is death a bad thing?
Arguments about death itself
Is death a bad thing?
Top
Regulating euthanasiaThose in favour of euthanasia think that there is no reason why euthanasia can't be controlled
by proper regulation, but they acknowledge that some problems will remain.
For example, it will be difficult to deal with people who want to implement euthanasia for
selfish reasons or pressurise vulnerable patients into dying.
This is little different from the position with any crime. The law prohibits theft, but that doesn't
stop bad people stealing things.
Top
People have the right to dieHuman beings have the right to die when and how they want to
In...cases where there are no dependants who might exert pressure one way or
the other, the right of the individual to choose should be paramount. So long as
the patient is lucid, and his or her intent is clear beyond doubt, there need be no
further questions.
The Independent, March 2002
Many people think that each person has the right to control his or her body and life and soshould be able to determine at what time, in what way and by whose hand he or she will die.
Behind this lies the idea that human beings should be as free as possible - and that
unnecessary restraints on human rights are a bad thing.
And behind that lies the idea that human beings are independent biological entities, with the
right to take and carry out decisions about themselves, providing the greater good of society
doesn't prohibit this. Allied to this is a firm belief that death is the end.
Religious objectionsReligious opponents disagree because they believe that the right to decide when a person dies
belongs to God.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 33/59
Secular objectionsSecular opponents argue that whatever rights we have are limited by our obligations. The
decision to die by euthanasia will affect other people - our family and friends, and healthcare
professionals - and we must balance the consequences for them (guilt, grief, anger) against our
rights.
We should also take account of our obligations to society, and balance our individual right to
die against any bad consequences that it might have for the community in general.
These bad consequences might be practical - such as making involuntary euthanasia easier and
so putting vulnerable people at risk.
There is also a political and philosophical objection that says that our individual right to
autonomy against the state must be balanced against the need to make the sanctity of life an
important, intrinsic, abstract value of the state.
Secular philosophers put forward a number of technical arguments, mostly based on the duty
to preserve life because it has value in itself, or the importance of regarding all human beings
as ends rather than means.
Top
Other human rights imply a right to dieWithout creating (or acknowledging) a specific right to die, it is possible to argue that other
human rights ought to be taken to include this right.
The right to life includes the right to die
The right to life is not a right simply to exist
The right to life is a right to life with a minimum quality and value
Death is the opposite of life, but the process of dying is part of life
Dying is one of the most important events in human life
Dying can be good or bad
People have the right to try and make the events in their lives as good as possible
So they have the right to try to make their dying as good as possible
If the dying process is unpleasant, people should have the right to shorten it, and thus
reduce the unpleasantness
People also have obligations - to their friends and family, to their doctors and
nurses, to society in general
These obligations limit their rights
These obligations do not outweigh a person's right to refuse medical treatment
that they do not want
But they do prevent a patient having any right to be killed
But even if there is a right to die, that doesn't mean that doctors have a duty to kill , so
no doctor can be forced to help the patient who wants euthanasia.
The right not to be killedThe right to life gives a person the right not to be killed if they don't want to be.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 34/59
Those in favour of euthanasia will argue that respect for this right not to be killed is sufficient
to protect against misuse of euthanasia, as any doctor who kills a patient who doesn't want to
die has violated that person's rights.
Opponents of euthanasia may disagree, and argue that allowing euthanasia will greatly
increase the risk of people who want to live being killed. The danger of violating the right to lifeis so great that we should ban euthanasia even if it means violating the right to die.
The rights to privacy and freedom of belief include a right to dieThis is the idea that the rights to privacy and freedom of belief give a person the right to decide
how and when to die.
The European Convention on Human Rights gives a person the right to
die
Not according to Britain's highest court.
It concluded that the right to life did not give any right to self-determination over life
and death, since the provisions of the convention were aimed at protecting and
preserving life.
English law already acknowledges that people have the right to dieThis argument is based on the fact that the Suicide Act (1961) made it legal for people to take
their own lives.
Opponents of euthanasia may disagree:
The Suicide Act doesn't necessarily acknowledge a right to die;
it could simply acknowledge that you can't punish someone for succeeding at suicide
and that it's inappropriate to punish someone so distressed that they want to take theirown life.
Euthanasia opponents further point out that there is a moral difference between
decriminalising something, often for practical reasons like those mentioned above, and
encouraging it.
They can quite reasonably argue that the purpose of the Suicide Act is not to allow euthanasia,
and support this argument by pointing out that the Act makes it a crime to help someone
commit suicide. This is true, but that provision is really there to make it impossible to escape a
murder charge by dressing the crime up as an assisted suicide.
Top
Libertarian argumentThis is a variation of the individual rights argument.
If an action promotes the best interests of everyone concerned and violates no one's
rights then that action is morally acceptable
In some cases, euthanasia promotes the best interests of everyone involved and
violates no one's rights
It is therefore morally acceptable
Objections to this argument
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 35/59
Opponents attack the libertarian argument specifically by claiming that there are no cases that
fit the conditions above:
people sometimes think things are in their best interests that are not morally
acceptable
The arguments that euthanasia is intrinsically wrong fit in here people are sometimes wrong about what's in their best interests
people may not realise that committing euthanasia may harm other people
euthanasia may deprive both the person who dies and others of benefits
euthanasia is not a private act - we cannot ignore any bad effects it may have on
society in general
Top
Medical resources
Euthanasia may be necessary for the fair distribution of health resourcesThis argument has not been put forward publicly or seriously by any government or health
authority. It is included here for completeness.
In most countries there is a shortage of health resources.
As a result, some people who are ill and could be cured are not able to get speedy access to the
facilities they need for treatment.
At the same time health resources are being used on people who cannot be cured, and who,
for their own reasons, would prefer not to continue living.
Allowing such people to commit euthanasia would not only let them have what they want, it
would free valuable resources to treat people who want to live.
Abuse of this would be prevented by only allowing the person who wanted to die to intitiate
the process, and by regulations that rigorously prevented abuse.
Objections to this argumentThis proposal is an entirely pragmatic one; it says that we should allow euthanasia because it
will allow more people to be happy. Such arguments will not convince anyone who believes
that euthanasia is wrong in principle.
Others will object because they believe that such a proposal is wide-open to abuse, and would
ultimately lead to involuntary euthanasia because of shortage of health resources.
In the end, they fear, people will be expected to commit euthanasia as soon as they become an
unreasonable burden on society.
Top
Moral rules must be universalisableOne of the commonly accepted principles in ethics, put forward by Immanuel Kant, is that only
those ethical principles that could be accepted as a universal rule (i.e. one that applied to
everybody) should be accepted.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 36/59
So you should only do something if you're willing for anybody to do exactly the same thing in
exactly similar circumstances, regardless of who they are.
The justification for this rule is hard to find - many people think it's just an obvious truth
(philosophers call such truths self-evident). You find variations of this idea in many faiths; for
example "do unto others as you would have them do unto you".
To put it more formally:
A rule is universalisable if it can consistently be willed as a law that everyone
ought to obey. The only rules which are morally good are those which can be
universalised.
The person in favour of euthanasia argues that giving everybody the right to have a good death
through euthanasia is acceptable as a universal principle, and that euthanasia is therefore
morally acceptable.
This alone does not justify euthanasiaThis is sound, but is not a full justification.
If a person wants to be allowed to commit euthanasia, it would clearly be inconsistent for them
to say that they didn't think it should be allowed for other people.
But the principle of universalisability doesn't actually provide any positive justification for
anything - genuine moral rules must be universalisable, but universalisability is not enough to
say that a rule is a satisfactory moral rule.
Universalisability is therefore only a necessary condition, not a sufficient condition for a rule to
be a morally good rule.
So, other than showing that one pre-condition is met, universalisibility doesn't advance the
case for euthanasia at all.
How similar can situations be?Every case is different in some respect, so anyone who is inclined to argue about it can argue
about whether the particular differences are sufficent to make this case an exception to the
rule.
Universal exceptions to universal rulesOddly enough, the law of universalisability allows for there to be exceptions - as long as the
exceptions are themselves universalisable. So you could have a universal rule allowing
voluntary euthanasia and universalise an exception for people who were less than 18 years old.
Top
Euthanasia happens anywayEuthanasia happens - better to make it legal and regulate it properlySounds a bit like "murder happens - better to make it legal and regulate it properly".
When you put it like that, the argument sounds very feeble indeed.
But it is one that is used a lot in discussion, and particularly in politics or round the table in thepub or the canteen.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 37/59
People say things like "we can't control drugs so we'd better legalise them", or "if we don't
make abortion legal so that people can have it done in hospital, people will die from backstreet
abortions".
What lies behind it is Utilitarianism: the belief that moral rules should be designed to produce
the greatest happiness of the greatest number of people.
If you accept this as the basis for your ethical code (and it's the basis of many people's ethics),
then the arguments above are perfectly sensible.
If you don't accept this principle, but believe that certain things are wrong regardless of what
effect they have on total human happiness, then you will probably regard this argument as
cynical and wrong.
A utilitarian argument for euthanasiaFrom a utilitarian viewpoint, justifying euthanasia is a question of showing that allowing people
to have a good death, at a time of their own choosing, will make them happier than the pain
from their illness, the loss of dignity and the distress of anticipating a slow, painful death.
Someone who wants euthanasia will have already made this comparison for themselves.
But utilitarianism deals with the total human happiness, not just that of the patient, so that
even euthanasia opponents who agree with utilitarianism in principle can claim that the
negative effects on those around the patient - family, friends and medical staff - would
outweigh the benefit to the patient.
It is hard to measure happiness objectively, but one way to test this argument would be to
speak to the families and carers of people who had committed assisted suicide.
Opponents can also argue that the net effect on the whole of society will be a decrease inhappiness. The only way to approach this would be to look at countries where euthanasia is
legal. However, as no two countries are alike, it seems impossible to extricate the happiness or
unhappiness resulting from legal assisted suicide, from any happiness or unhappiness from
other sources.
Even if you agree with the utilitarian argument, you then have to deal with the arguments that
suggest that euthanasia can't be properly regulated.
Top
Is death a bad thing?Why ask this question?If death is not a bad thing then many of the objections to euthanasia vanish.
If we put aside the idea that death is always a bad thing, we are able to consider whether
death may actually sometimes be a good thing.
This makes it much easier to consider the issue of euthanasia from the viewpoint of someone
who wants euthanasia.
Why is death a bad thing?
We tend to regard death as a bad thing for one or more of these reasons:
because human life is intrinsically valuable
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 38/59
because life and death are God's business with which we shouldn't interfere
because most people don't want to die
because it violates our autonomy in a drastic way
The first two reasons form key points in the arguments against euthanasia, but only if you
accept that they are true.
The last two reasons why death is a bad thing are not absolute; if a person wants to die, then
neither of those reasons can be used to say that they would be wrong to undergo euthanasia.
People don't usually want to diePeople are usually eager to avoid death because they value being alive, because they have
many things they wish to do, and experiences they wish to have.
Obviously, this is not the case with a patient who wishes to die - and proper regulation will
weed out people who do not really want to die, but are asking for other reasons.
Violation of autonomyAnother reason why death is seen as a bad thing is that it's the worst possible violation of the
the wishes of the person who does not want to die (or, to use philosophical language, a
violation of their autonomy).
In the case of someone who does want to die, this objection disappears.
Being dead, versus not having been bornSome people say that being dead is no different from not having been born yet, and nobody
makes a fuss about the bad time they had before they were born.
There is a big difference - even though being dead will be no different as an experience fromthe experience of not having yet been born.
The idea is that death hurts people because it stops them having more of the things that they
want, and could have if they continued to live.
Someone who makes a request for euthanasia is likely to have a bad quality of life (or a bad
prognosis, even if they are not yet suffering much) and the knowledge that this will only get
worse. If that is the case, death will not deprive them of an otherwise pleasant existence.
Of course, most patients will still be leaving behind some things that are good: for example,
loved ones and things they enjoy. Asking for death does not necessarily mean that they have
nothing to live for: only that the patient has decided that after a certain point, the pain
outweighs the good things.
Abortion is the termination of a pregnancy by the removal or expulsion from the uterus of a
fetus or embryo, resulting in or caused by its death.[2] An abortion can occur spontaneously
due to complications during pregnancy or can be induced, in humans and other species. In the
context of human pregnancies, an abortion induced to preserve the health of the gravida
(pregnant female) is termed a therapeutic abortion, while an abortion induced for any other
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 39/59
reason is termed an elective abortion. The term abortion most commonly refers to the induced
abortion of a human pregnancy, while spontaneous abortions are usually termed miscarriages.
Worldwide 42 million abortions are estimated to take place annually with 22 million of these
occurring safely and 20 million unsafely.[3] While maternal mortality seldom results from safe
abortions, unsafe abortions result in 70,000 deaths and 5 million disabilities per year.[3] One ofthe main determinants of the availability of safe abortions is the legality of the procedure.
Forty percent of the world's women are able to access therapeutic and elective abortions
within gestational limits.[4] The frequency of abortions is, however, similar whether or not
access is restricted.[4]
Abortion has a long history and has been induced by various methods including herbal
abortifacients, the use of sharpened tools, physical trauma, and other traditional methods.
Contemporary medicine utilizes medications and surgical procedures to induce abortion. The
legality, prevalence, and cultural views on abortion vary substantially around the world. In
many parts of the world there is prominent and divisive public controversy over the ethical and
legal issues of abortion. Abortion and abortion-related issues feature prominently in the
national politics in many nations, often involving the opposing pro-life and pro-choice
worldwide social movements (both self-named). Incidence of abortion has declined worldwide,
as access to family planning education and contraceptive services has increased.[5]
Types
A 10-week-old fetus removed from a 44-year-old female diagnosed with early-stage uterine
cancer via a theraputic abortion. The uterus (womb), included the fetus.
SpontaneousMain article: Miscarriage
Spontaneous abortion (also known as miscarriage) is the expulsion of an embryo or fetus due
to accidental trauma or natural causes before approximately the 22nd week of gestation; the
definition by gestational age varies by country.[6] Most miscarriages are due to incorrect
replication of chromosomes; they can also be caused by environmental factors. A pregnancy
that ends before 37 weeks of gestation resulting in a live-born infant is known as a "premature
birth". When a fetus dies in utero after about 22 weeks, or during delivery, it is usually termed
"stillborn". Premature births and stillbirths are generally not considered to be miscarriages
although usage of these terms can sometimes overlap.
Between 10% and 50% of pregnancies end in clinically apparent miscarriage, depending upon
the age and health of the pregnant woman.[7] Most miscarriages occur very early in
pregnancy, in most cases, they occur so early in the pregnancy that the woman is not even
aware that she was pregnant. One study testing hormones for ovulation and pregnancy found
that 61.9% of conceptuses were lost prior to 12 weeks, and 91.7% of these losses occurred
subclinically, without the knowledge of the once pregnant woman.[8]

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 40/59
The risk of spontaneous abortion decreases sharply after the 10th week from the last
menstrual period (LMP).[7][9] One study of 232 pregnant women showed "virtually complete
[pregnancy loss] by the end of the embryonic period" (10 weeks LMP) with a pregnancy loss
rate of only 2 percent after 8.5 weeks LMP.[10]
The most common cause of spontaneous abortion during the first trimester is chromosomalabnormalities of the embryo/fetus,[11] accounting for at least 50% of sampled early pregnancy
losses.[12] Other causes include vascular disease (such as lupus), diabetes, other hormonal
problems, infection, and abnormalities of the uterus.[11] Advancing maternal age and a patient
history of previous spontaneous abortions are the two leading factors associated with a greater
risk of spontaneous abortion.[12] A spontaneous abortion can also be caused by accidental
trauma; intentional trauma or stress to cause miscarriage is considered induced abortion or
feticide.[13]
Induced
A pregnancy can be intentionally aborted in many ways. The manner selected depends chieflyupon the gestational age of the embryo or fetus, which increases in size as it ages.[14] Specific
procedures may also be selected due to legality, regional availability, and doctor-patient
preference. Reasons for procuring induced abortions are typically characterized as either
therapeutic or elective. An abortion is medically referred to as therapeutic when it is
performed to:
save the life of the pregnant woman;[15]
preserve the woman's physical or mental health;[15]
terminate pregnancy that would result in a child born with a congenital disorder that
would be fatal or associated with significant morbidity;[15] or
selectively reduce the number of fetuses to lessen health risks associated with multiple
pregnancy.[15]
An abortion is referred to as elective when it is performed at the request of the woman "for
reasons other than maternal health or fetal disease."[16]
Methods
Gestational age may determine which abortion methods are practiced.
MedicalMain article: Medical abortion
"Medical abortions" are non-surgical abortions that use pharmaceutical drugs, and are only
effective in the first trimester of pregnancy. [citation needed] Medical abortions comprise 10%
of all abortions in the United States[17] and Europe.[citation needed] Combined regimens
include methotrexate or mifepristone, followed by a prostaglandin (either misoprostol or
gemeprost: misoprostol is used in the U.S.; gemeprost is used in the UK and Sweden.) When
used within 49 days gestation, approximately 92% of women undergoing medical abortion with
a combined regimen completed it without surgical intervention.[18] Misoprostol can be used
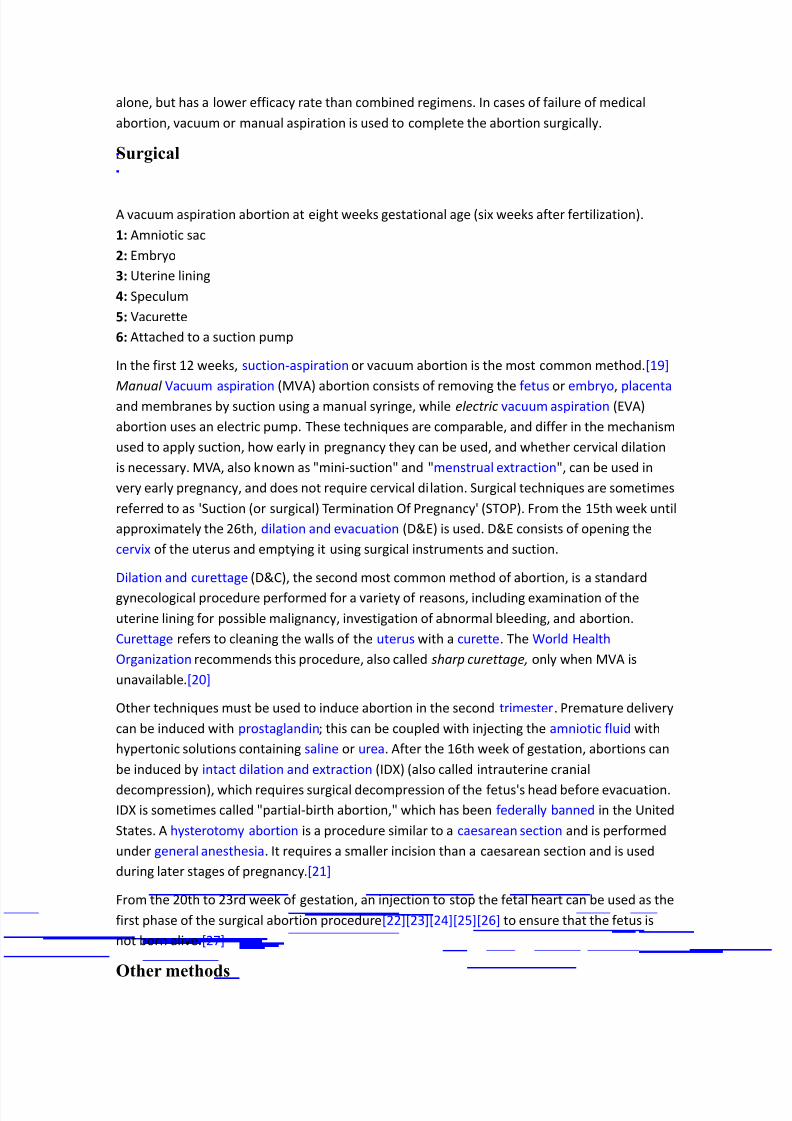
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 41/59
alone, but has a lower efficacy rate than combined regimens. In cases of failure of medical
abortion, vacuum or manual aspiration is used to complete the abortion surgically.
Surgical
A vacuum aspiration abortion at eight weeks gestational age (six weeks after fertilization).
1: Amniotic sac
2: Embryo
3: Uterine lining
4: Speculum
5: Vacurette
6: Attached to a suction pump
In the first 12 weeks, suction-aspiration or vacuum abortion is the most common method.[19]
Manual Vacuum aspiration (MVA) abortion consists of removing the fetus or embryo, placenta and membranes by suction using a manual syringe, while electric vacuum aspiration (EVA)
abortion uses an electric pump. These techniques are comparable, and differ in the mechanism
used to apply suction, how early in pregnancy they can be used, and whether cervical dilation
is necessary. MVA, also known as "mini-suction" and "menstrual extraction", can be used in
very early pregnancy, and does not require cervical dilation. Surgical techniques are sometimes
referred to as 'Suction (or surgical) Termination Of Pregnancy' (STOP). From the 15th week until
approximately the 26th, dilation and evacuation (D&E) is used. D&E consists of opening the
cervix of the uterus and emptying it using surgical instruments and suction.
Dilation and curettage (D&C), the second most common method of abortion, is a standard
gynecological procedure performed for a variety of reasons, including examination of the
uterine lining for possible malignancy, investigation of abnormal bleeding, and abortion.
Curettage refers to cleaning the walls of the uterus with a curette. The World Health
Organization recommends this procedure, also called sharp curettage, only when MVA is
unavailable.[20]
Other techniques must be used to induce abortion in the second trimester. Premature delivery
can be induced with prostaglandin; this can be coupled with injecting the amniotic fluid with
hypertonic solutions containing saline or urea. After the 16th week of gestation, abortions can
be induced by intact dilation and extraction (IDX) (also called intrauterine cranial
decompression), which requires surgical decompression of the fetus's head before evacuation.
IDX is sometimes called "partial-birth abortion," which has been federally banned in the United
States. A hysterotomy abortion is a procedure similar to a caesarean section and is performed
under general anesthesia. It requires a smaller incision than a caesarean section and is used
during later stages of pregnancy.[21]
From the 20th to 23rd week of gestation, an injection to stop the fetal heart can be used as the
first phase of the surgical abortion procedure[22][23][24][25][26] to ensure that the fetus is
not born alive.[27]
Other methods
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 42/59
Historically, a number of herbs reputed to possess abortifacient properties have been used in
folk medicine: tansy, pennyroyal, black cohosh, and the now-extinct silphium (see history of
abortion).[28] The use of herbs in such a manner can cause serious—even lethal—side effects,
such as multiple organ failure, and is not recommended by physicians.[29]
Abortion is sometimes attempted by causing trauma to the abdomen. The degree of force, ifsevere, can cause serious internal injuries without necessarily succeeding in inducing
miscarriage.[30] Both accidental and deliberate abortions of this kind can be subject to criminal
liability in many countries. In Southeast Asia, there is an ancient tradition of attempting
abortion through forceful abdominal massage.[31] One of the bas reliefs decorating the temple
of Angkor Wat in Cambodia depicts a demon performing such an abortion upon a woman who
has been sent to the underworld.[31]
Reported methods of unsafe, self-induced abortion include misuse of misoprostol, and
insertion of non-surgical implements such as knitting needles and clothes hangers into the
uterus. These methods are rarely seen in developed countries where surgical abortion is legal
and available.[32]
Health risksSee also: Health risks of unsafe abortion
Abortion, when legally performed in developed countries, is among the safest procedures in
medicine.[33][34] In such settings, risk of maternal death is between 0.2 –1.2 per 100,000
procedures.[35][36][37][38] In comparison, by 1996, mortality from childbirth in developed
countries was 11 times greater.[39][40][41][42][43][44] Unsafe abortions (defined by the World
Health Organization as those performed by unskilled individuals, with hazardous equipment, or
in unsanitary facilities) carry a high risk of maternal death and other complications.[45] For
unsafe procedures, the mortality rate has been estimated at 367 per 100,000.[46]
Physical health
Surgical abortion methods, like most minimally invasive procedures, carry a small potential for
serious complications.[47]
Surgical abortion is generally safe and the rate of major complications is low[48] but varies
depending on how far pregnancy has progressed and the surgical method used.[49] Concerning
gestational age, incidence of major complications is highest after 20 weeks of gestation and
lowest before the 8th week.[49] With more advanced gestation there is a higher risk of uterine
perforation and retained products of conception,[50] and specific procedures like dilation and
evacuation may be required.[51]
Concerning the methods used, general incidence of major complications for surgical abortion
varies from lower for suction curettage, to higher for saline instillation.[49] Possible
complications include hemorrhage, incomplete abortion, uterine or pelvic infection, ongoing
intrauterine pregnancy, misdiagnosed/unrecognized ectopic pregnancy, hematometra (in the
uterus), uterine perforation and cervical laceration.[52] Use of general anesthesia increases the
risk of complications because it relaxes uterine musculature making it easier to perforate.[53]
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 43/59
Women who have uterine anomalies, leiomyomas or had previous difficult first-trimester
abortion are contraindicated to undertake surgical abortion unless ultrasonography is
immediately available and the surgeon is experienced in its intraoperative use.[54] Abortion
does not impair subsequent pregnancies, nor does it increase the risk of future premature
births, infertility, ectopic pregnancy, or miscarriage.[34]
In the first trimester, health risks associated with medical abortion are generally considered no
greater than for surgical abortion.[55]
Mental healthMain article: Abortion and mental health
No scientific research has demonstrated that abortion is a cause of poor mental health in the
general population. However there are groups of women who may be at higher risk of coping
with problems and distress following abortion.[56] Some factors in a woman's life, such as
emotional attachment to the pregnancy, lack of social support, pre-existing psychiatric illness,
and conservative views on abortion increase the likelihood of experiencing negative feelingsafter an abortion.[57] The American Psychological Association (APA) concluded that abortion
does not lead to increased mental health problems.[58]
Some proposed negative psychological effects of abortion have been referred to by anti-
abortion advocates as a separate condition called "post-abortion syndrome." However, the
existence of "post-abortion syndrome" is not recognized by any medical or psychological
organization.[59][60][61]
IncidenceThe number of abortions performed worldwide has deceased between 1995 and 2003 from
45.6 million to 41.6 million (a decrease from 35 to 29 per 1000 women between 15 and 44
years of age).[3] The greatest decrease has occurred in the developed world with a decrease
from 39 to 26 per 1000 women in comparison to the developing world which had a decrease
from 34 to 29 per 1000 women.[3] Of these approximately 42 million abortions 22 million
occurred safely and 20 million unsafely.[3]
The incidence and reasons for induced abortion vary regionally. Some countries, such as
Belgium (11.2 per 100 known pregnancies) and the Netherlands (10.6 per 100), had a
comparatively low rate of induced abortion, while others like Russia (62.6 per 100) and
Vietnam (43.7 per 100) had a high rate. The world ratio was 26 induced abortions per 100
known pregnancies (excluding miscarriages and stillbirths).[62]
By gestational age and method
Histogram of abortions by gestational age in England and Wales during 2004. Average is 9.5
weeks. (left) Abortion in the United States by gestational age, 2004. (Data source: Centers for
Disease Control and Prevention) (right)
Abortion rates also vary depending on the stage of pregnancy and the method practiced. In
2003, from data collected in those areas of the United States that sufficiently reported
gestational age, it was found that 88.2% of abortions were conducted at or prior to 12 weeks,
10.4% from 13 to 20 weeks, and 1.4% at or after 21 weeks. 90.9% of these were classified as
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 44/59
having been done by "curettage" (suction-aspiration, Dilation and curettage, Dilation and
evacuation), 7.7% by "medical" means (mifepristone), 0.4% by "intrauterine instillation" (saline
or prostaglandin), and 1.0% by "other" (including hysterotomy and hysterectomy).[63] The
Guttmacher Institute estimated there were 2,200 intact dilation and extraction procedures in
the U.S. during 2000; this accounts for 0.17% of the total number of abortions performed that
year.[64] Similarly, in England and Wales in 2006, 89% of terminations occurred at or under 12
weeks, 9% between 13 to 19 weeks, and 1.5% at or over 20 weeks. 64% of those reported were
by vacuum aspiration, 6% by D&E, and 30% were medical.[65] Later abortions are more
common in China, India, and other developing countries than in developed countries.[66]
By personal and social factors
A bar chart depicting selected data from the 1998 AGI meta-study on the reasons women
stated for having an abortion.
A 1998 aggregated study, from 27 countries, on the reasons women seek to terminate their
pregnancies concluded that common factors cited to have influenced the abortion decision
were: desire to delay or end childbearing, concern over the interruption of work or education,
issues of financial or relationship stability, and perceived immaturity.[67] A 2004 study in which
American women at clinics answered a questionnaire yielded similar results.[68] In Finland and
the United States, concern for the health risks posed by pregnancy in individual cases was not a
factor commonly given; however, in Bangladesh, India, and Kenya health concerns were cited
by women more frequently as reasons for having an abortion.[67] 1% of women in the 2004
survey-based U.S. study became pregnant as a result of rape and 0.5% as a result of incest.[68]
Another American study in 2002 concluded that 54% of women who had an abortion wereusing a form of contraception at the time of becoming pregnant while 46% were not.
Inconsistent use was reported by 49% of those using condoms and 76% of those using the
combined oral contraceptive pill; 42% of those using condoms reported failure through slipping
or breakage.[69] The Guttmacher Institute estimated that "most abortions in the United States
are obtained by minority women" because minority women "have much higher rates of
unintended pregnancy."[70]
Some abortions are undergone as the result of societal pressures. These might include the
stigmatization of disabled people, preference for children of a specific sex, disapproval of single
motherhood, insufficient economic support for families, lack of access to or rejection ofcontraceptive methods, or efforts toward population control (such as China's one-child policy).
These factors can sometimes result in compulsory abortion or sex-selective abortion.
Unsafe abortion
Soviet poster circa 1925, promoting hospital abortions. Title translation: "Abortions performed
by either trained or self-taught midwives not only maim the woman, they also often lead to
death."
Main article: Unsafe abortion
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 45/59
Women seeking to terminate their pregnancies sometimes resort to unsafe methods,
particularly where and when access to legal abortion is restricted. The World Health
Organization (WHO) defines an unsafe abortion as being "a procedure ... carried out by persons
lacking the necessary skills or in an environment that does not conform to minimal medical
standards, or both."[71] Unsafe abortions are sometimes known colloquially as "back-alley"
abortions. They may be performed by the woman herself , another person without medical
training, or a professional health provider operating in sub-standard conditions. Unsafe
abortion remains a public health concern due to the higher incidence and severity of its
associated complications, such as incomplete abortion, sepsis, hemorrhage, and damage to
internal organs. It is estimated that 20 million unsafe abortions occur around the world
annually and that 70,000 of these result in the woman's death.[3] Complications of unsafe
abortion are said to account, globally, for approximately 13% of all maternal mortalities, with
regional estimates including 12% in Asia, 25% in Latin America, and 13% in sub-Saharan
Africa.[72] Although the global rate of abortion declined from 45.6 million in 1995 to 41.6
million in 2003, unsafe procedures still accounted for 48% of all abortions performed in2003.[73] Health education, access to family planning, and improvements in health care during
and after abortion have been proposed to address this phenomenon.[74]
History
"French Periodical Pills." An example of a clandestine advertisement published in an 1845
edition of the Boston Daily Times.
Main article: History of abortion
Induced abortion can be traced to ancient times.[75] There is evidence to suggest that,
historically, pregnancies were terminated through a number of methods, including the
administration of abortifacient herbs, the use of sharpened implements, the application of
abdominal pressure, and other techniques.
The Hippocratic Oath, the chief statement of medical ethics for Hippocratic physicians in
Ancient Greece, forbade doctors from helping to procure an abortion by pessary. Soranus, a
second-century Greek physician, suggested in his work Gynaecology that women wishing to
abort their pregnancies should engage in energetic exercise, energetic jumping, carrying heavy
objects, and riding animals. He also prescribed a number of recipes for herbal baths, pessaries,
and bloodletting, but advised against the use of sharp instruments to induce miscarriage due to
the risk of organ perforation.[76] It is also believed that, in addition to using it as a
contraceptive, the ancient Greeks relied upon silphium as an abortifacient. Such folk remedies,
however, varied in effectiveness and were not without risk. Tansy and pennyroyal, for example,
are two poisonous herbs with serious side effects that have at times been used to terminate
pregnancy.
During the medieval period, physicians in the Islamic world documented detailed and extensive
lists of birth control practices, including the use of abortifacients, commenting on their
effectiveness and prevalence.[77] They listed many different birth control substances in their
medical encyclopedias, such as Avicenna listing 20 in The Canon of Medicine (1025) and
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 46/59
Muhammad ibn Zakariya ar-Razi listing 176 in his Hawi (10th century). This was unparalleled in
European medicine until the 19th century.[78][Need quotation to verify]
During the Middle Ages, abortion was tolerated and there were no laws against it.[79] A
medieval female physician, Trotula of Salerno,[80] administered a number of remedies for the
“retention of menstrua,” which was sometimes a code for early abortifacients.[81] Pope SixtusV (1585 –90) is noted as the first Pope to declare that abortion is homicide regardless of the
stage of pregnancy.[82] Abortion in the 19th century continued, despite bans in both the
United Kingdom and the United States, as the disguised, but nonetheless open, advertisement
of services in the Victorian era suggests.[83]
In the 20th century the Soviet Union (1919), Iceland (1935) and Sweden (1938) were among
the first countries to legalize certain or all forms of abortion.[84] In 1935 Nazi Germany, a law
was passed permitting abortions for those deemed "hereditarily ill," while women considered
of German stock were specifically prohibited from having abortions.[85][86][87][88]
Society and cultureAbortion debate
This section needs additional citations for verification.
Please help improve this article by adding reliable references. Unsourced material may be
challenged and removed. (November 2008)
Pro-choice activists near the Washington Monument at the March for Women's Lives in 2004.
(left) Pro-life activists near the Washington Monument at the annual 2009 March for Life in
Washington, DC. (right)Main article: Abortion debate
In the history of abortion, induced abortion has been the source of considerable debate,
controversy, and activism. An individual's position on the complex ethical, moral, philosophical,
biological, and legal issues is often related to his or her value system. The main positions are
one that argues in favor of access to abortion and one argues against access to abortion.
Opinions of abortion may be described as being a combination of beliefs on its morality, and
beliefs on the responsibility, ethical scope, and proper extent of governmental authorities in
public policy. Religious ethics also has an influence upon both personal opinion and the greater
debate over abortion (see religion and abortion).
Abortion debates, especially pertaining to abortion laws, are often spearheaded by groups
advocating one of these two positions. In the United States, those in favor of greater legal
restrictions on, or even complete prohibition of abortion, most often describe themselves as
pro-life while those against legal restrictions on abortion describe themselves as pro-choice.
Generally, the former position argues that a human fetus is a human being with a right to live
making abortion tantamount to murder. The latter position argues that a woman has certain
reproductive rights, especially the choice whether or not to carry a pregnancy to term.
In both public and private debate, arguments presented in favor of or against abortion access
focus on either the moral permissibility of an induced abortion, or justification of lawspermitting or restricting abortion.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 47/59
Debate also focuses on whether the pregnant woman should have to notify and/or have the
consent of others in distinct cases: a minor, her parents; a legally married or common-law wife,
her husband; or a pregnant woman, the biological father. In a 2003 Gallup poll in the United
States, 79% of male and 67% of female respondents were in favor of legalized mandatory
spousal notification; overall support was 72% with 26% opposed.[89]
Abortion lawMain article: Abortion law
See also: Reproductive rights
International status of abortion law: Legal on request Legal for maternal life, health,
mental health, rape, fetal defects, and/or socioeconomic factors Legal for or illegal with
exception for maternal life, health, mental health, rape, and/or fetal defects Illegal with
exception for maternal life, health, mental health and/or rape Illegal with exception for
maternal life, health, and/or mental health Illegal with no exceptions No information
Vertical stripes (various colours): Illegal but unenforced
Before the scientific discovery in the nineteenth century that human development begins at
fertilization,[90] English common law forbade abortions after "quickening", that is, after "an
infant is able to stir in the mother's womb."[91] There was also an earlier period in England
when abortion was prohibited "if the foetus is already formed" but not yet quickened.[92] Both
pre- and post-quickening abortions were criminalized by Lord Ellenborough's Act in 1803.[93]
In 1861, the Parliament of the United Kingdom passed the Offences against the Person Act
1861, which continued to outlaw abortion and served as a model for similar prohibitions in
some other nations.[94]
The Soviet Union, with legislation in 1920, and Iceland, with legislation in 1935, were two of
the first countries to generally allow abortion. The second half of the 20th century saw the
liberalization of abortion laws in other countries. The Abortion Act 1967 allowed abortion for
limited reasons in the United Kingdom (except Northern Ireland). In the 1973 case, Roe v.
Wade, the United States Supreme Court struck down state laws banning abortion, ruling that
such laws violated an implied right to privacy in the United States Constitution. The Supreme
Court of Canada, similarly, in the case of R. v. Morgentaler, discarded its criminal code
regarding abortion in 1988, after ruling that such restrictions violated the security of person
guaranteed to women under the Canadian Charter of Rights and Freedoms. Canada later struckdown provincial regulations of abortion in the case of R. v. Morgentaler (1993). By contrast,
abortion in Ireland was affected by the addition of an amendment to the Irish Constitution in
1983 by popular referendum, recognizing "the right to life of the unborn".
Current laws pertaining to abortion are diverse. Religious, moral, and cultural sensibilities
continue to influence abortion laws throughout the world. The right to life, the right to liberty,
the right to security of person, and the right to reproductive health are major issues of human
rights that are sometimes used as justification for the existence or absence of laws controlling
abortion. Many countries in which abortion is legal require that certain criteria be met in order
for an abortion to be obtained, often, but not always, using a trimester-based system toregulate the window of legality:
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 48/59
In the United States, some states impose a 24-hour waiting period before the
procedure, prescribe the distribution of information on fetal development, or require
that parents be contacted if their minor daughter requests an abortion.[95]
In the United Kingdom, as in some other countries, two doctors must first certify that
an abortion is medically or socially necessary before it can be performed.
In Canada, a similar requirement was rejected as unconstitutional in 1988.
Other countries, in which abortion is normally illegal, will allow one to be performed in the
case of rape, incest, or danger to the pregnant woman's life or health.
A few nations ban abortion entirely: Chile, El Salvador, Malta, and Nicaragua, with
consequent rises in maternal death directly and indirectly due to pregnancy.[96][97]
However, in 2006, the Chilean government began the free distribution of emergency
contraception.[98][99]
In Bangladesh, abortion is illegal, but the government has long supported a network of
"menstrual regulation clinics", where menstrual extraction (manual vacuum aspiration) can be performed as menstrual hygiene.[100]
In places where abortion is illegal or carries heavy social stigma, pregnant women may engage
in medical tourism and travel to countries where they can terminate their pregnancies. Women
without the means to travel can resort to providers of illegal abortions or try to do it
themselves. [101]
In the US, about 8% of abortions are performed on women who travel from another state.[102]
However, that is driven at least partly by differing limits on abortion according to gestational
age or the scarcity of doctors trained and willing to do later abortions.
Sex-selectiveMain article: Sex-selective abortion
Sonography and amniocentesis allow parents to determine sex before childbirth. The
development of this technology has led to sex-selective abortion, or the targeted termination
of female fetuses.
It is suggested that sex-selective abortion might be partially responsible for the noticeable
disparities between the birth rates of male and female children in some places. The preference
for male children is reported in many areas of Asia, and abortion used to limit female births has
been reported in China, Taiwan, South Korea, and India.[103]
In India, the economic role of men, the costs associated with dowries, and a common Indian
tradition which dictates that funeral rites must be performed by a male relative have led to a
cultural preference for sons.[104] The widespread availability of diagnostic testing, during the
1970s and '80s, led to advertisements for services which read, "Invest 500 rupees [for a sex
test] now, save 50,000 rupees [for a dowry] later."[105] In 1991, the male-to-female sex ratio in
India was skewed from its biological norm of 105 to 100, to an average of 108 to 100.[106]
Researchers have asserted that between 1985 and 2005 as many as 10 million female fetuses
may have been selectively aborted.[107] The Indian government passed an official ban of pre-
natal sex screening in 1994 and moved to pass a complete ban of sex-selective abortion in
2002.[108]
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 49/59
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 50/59
were purebred dominant. His experiments led him to make two generalizations, the Law of
Segregation and the Law of Independent Assortment, which later became known as Mendel's
Laws of Inheritance.
Mendel did read his paper, Experiments on Plant Hybridization, at two meetings of the Natural
History Society of Brünn in Moravia in 1865. When Mendel's paper was published in 1866 inProceedings of the Natural History Society of Brünn,[8] it had little impact and was cited about
three times over the next thirty-five years. (Notably, Charles Darwin was unaware of Mendel's
paper, according to Jacob Bronowski's The Ascent of Man.) His paper was criticized at the time,
but is now considered a seminal work.
Life after the pea experimentsAfter Mendel completed his work with peas, he turned to experimenting with honeybees, in
order to extend his work to animals. He produced a hybrid strain (so vicious they were
destroyed), but failed to generate a clear picture of their heredity because of the difficulties in
controlling mating behaviours of queen bees. He also described novel plant species, and theseare denoted with the botanical author abbreviation "Mendel".
After he was elevated as abbot in 1868, his scientific work largely ended as Mendel became
consumed with his increased administrative responsibilities, especially a dispute with the civil
government over their attempt to impose special taxes on religious institutions.[9] At first
Mendel's work was rejected, and it was not widely accepted until after he died. At that time
most biologists held the idea of blending inheritance, and Charles Darwin's efforts to explain
inheritance through a theory of pangenesis were unsuccessful. Mendel's ideas were
rediscovered in the early twentieth century, and in the 1930s and 1940s the modern synthesis
combined Mendelian genetics with Darwin's theory of natural selection.
Mendel died on January 6, 1884, at age 61, in Brno, Moravia, Austria-Hungary (now Czech
Republic), from chronic nephritis. Czech composer Leoš Janáček played the organ at his funeral.
After his death the succeeding abbot burned all papers in Mendel's collection, to mark an end
to the disputes over taxation.[10]
Rediscovery of Mendel's work
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 51/59
Dominant and recessive phenotypes. (1) Parental generation. (2) F1 generation. (3) F2
generation.
It was not until the early 20th century that the importance of his ideas was realized. By 1900,
research aimed at finding a successful theory of discontinuous inheritance rather than blending
inheritance led to independent duplication of his work by Hugo de Vries and Carl Correns, andthe rediscovery of Mendel's writings and laws. Both acknowledged Mendel's priority, and it is
thought probable that de Vries did not understand the results he had found until after reading
Mendel.[2] Though Erich von Tschermak was originally also credited with rediscovery, this is no
longer accepted because he did not understand Mendel's laws.[11] Though de Vries later lost
interest in Mendelism, other biologists started to establish genetics as a science.[2]
Mendel's results were quickly replicated, and genetic linkage quickly worked out. Biologists
flocked to the theory, even though it was not yet applicable to many phenomena, it sought to
give a genotypic understanding of heredity which they felt was lacking in previous studies of
heredity which focused on phenotypic approaches. Most prominent of these latter approaches
was the biometric school of Karl Pearson and W.F.R. Weldon, which was based heavily on
statistical studies of phenotype variation. The strongest opposition to this school came from
William Bateson, who perhaps did the most in the early days of publicising the benefits of
Mendel's theory (the word "genetics", and much of the discipline's other terminology,
originated with Bateson). This debate between the biometricians and the Mendelians was
extremely vigorous in the first two decades of the twentieth century, with the biometricians
claiming statistical and mathematical rigor, whereas the Mendelians claimed a better
understanding of biology. In the end, the two approaches were combined as the modern
synthesis of evolutionary biology, especially by work conducted by R. A. Fisher as early as 1918.
Mendel's experimental results have later been the object of considerable dispute.[10] Fisher
analyzed the results of the F2 (second filial) ratio and found them to be implausibly close to the
exact ratio of 3 to 1.[12] Only a few would accuse Mendel of scientific malpractice or call it a
scientific fraud—reproduction of his experiments has demonstrated the validity of his
hypothesis—however, the results have continued to be a mystery for many, though it is often
cited as an example of confirmation bias. This might arise if he detected an approximate 3 to 1
ratio early in his experiments with a small sample size, and continued collecting more data until
the results conformed more nearly to an exact ratio. It is sometimes suggested that he may
have censored his results, and that his seven traits each occur on a separate chromosome pair,
an extremely unlikely occurrence if they were chosen at random. In fact, the genes Mendelstudied occurred in only four linkage groups, and only one gene pair (out of 21 possible) is
close enough to show deviation from independent assortment; this is not a pair that Mendel
studied. Some recent researchers have suggested that Fisher's criticisms of Mendel's work may
have been exaggerated.[13][14]
What is Parkinson s Disease
Return to Index Return to Alphabetical Contents
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 52/59
What Is Parkinson's Disease?Abraham Lieberman, M.D.
Parkinson's disease (PD) is a progressive disorder of the nervous system. With an annual
incidence of approximately 20 new cases per 100,000 people, the prevalence is 200 cases per
100,000 people or 0.2%. There are 1,000,000 or more people with PD in the United States;
more patients than with multiple sclerosis, amyotrophic lateral sclerosis, muscular dystrophy
and myasthenia gravis combined.
PD is generally age-specific; it is estimated that approximately 1% of the population over age
60 has PD. The occurrence of PD around age 60 suggests the disease may be time-locked to
certain age-related changes in the nervous system. However, PD does occur in young people.
Approximately 10% of all patients develop symptoms before age 50. This suggests that in
addition to any changes related to aging, there are specific changes related to the disease.
PD is characterized by four main features: rigidity or stiffness of the arms, legs or neck; tremor,
usually of the hands; bradykinesia or slowness and reduction of movement; and postural
instability (loss of balance). Other symptoms may accompany the main features, including
depression, dementia or confusion, postural deformity, speech and swallowing difficulty,
drooling, dizziness on standing, impotence, urinary frequency and constipation.
When rigidity, tremor, slowness of movement and loss of balance dominate, when the course
of the disease is slow with disability occurring 10 to 20 years after diagnosis, and when there is
no obvious cause, then the condition is referred to as idiopathic PD. Patients with the above
features, on post-mortem examination, show loss of the dark, pigmented neurons (nerve cells)
in two areas of the brain: the substantia nigra (latin for "black substance") and the locus
ceruleus ("blue substance"). The dead and dying cells contain Lewy bodies. While Lewy bodies
are found in other diseases, the diagnosis of idiopathic PD can only be made with certainty if
Lewy bodies are found in the substantia nigra and locus ceruleus after death.
Paralleling the loss of nerve cells in the substantia nigra is the loss of dopamine, a chemical
which carries messages from one nerve cell to another. The loss of dopamine is most marked in
that part of the brain called the striatum (or "stripped substance"). The striatum consists of two
parts: The caudate nucleus and the putamen. Primary treatment of PD consists of giving
levodopa (in the U.S. via Sinemet or a generic form thereof), which is converted to dopamine in
the substantia nigra and the striatum, and replaces the missing dopamine. Patients with
idiopathic PD usually respond well to levodopa. In fact, a successful response to levodopa
confirms the clinical diagnosis of PD.
When early in the disease there is a mixture of the main features with other symptoms; when
the course of the disease is rapid with marked disability occurring within five years; or when
there is no response to levodopa, the condition is called Parkinson Disease Plus (PD+). The term
"PD+" encompasses a number of disorders including Progressive Supranuclear Palsy (PSP),
Cortico-Basilar Degeneration (CBD) and MultiSystem Atrophy (MSA). MultiSystem Atrophy
includes the Shy-Drager Syndrome (SDS), Striatonigral Degeneration (SND) and
OlivoPontoCerebellar Atrophy (OPCA). The PD+ disorders differ from idiopathic PD in that,
although there is a loss of nerve cells in the substantia nigra, the main changes occur
elsewhere. Though symptoms may resemble PD, Lewy bodies are not found in these disorders.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 53/59
There are also a number of disorders with parkinsonian features for which the cause is known
and which have a variable rate of progression and response to levodopa. These disorders are
referred to as Parkinson Syndrome (PS) and include multiple small strokes and poisoning by
manganese, carbon monoxide and cyanide. PS also includes pugilistic parkinsonism, a disorder
of professional boxers who receive multiple blows to the head and in whom symptoms
progress even after they stop fighting. Pugilistic parkinsonism affected Jack Dempsey, Joe Lewis
and, more recently, Muhammad Ali.
In addition to the above disorders, which are permanent, there are several drug induced
Parkinson disorders that are reversible on stopping the drug. Drugs that cause PS include
tranquilizers such as chlorpromazine (Thorazine), fluphen-zine (Prolixin) and haloperidol
(Haldol). In addition, drugs such as metochlopramide (Reglan) and prochlorperazine
(Compazine), used to treat nausea but similar to the tranquilizers, may also cause PS. These
drug-induced disorders are not associated with a loss of nerve cells in the substantia nigra and
differ from the permanent PS associated with the nerve toxin MPTP which does result in loss of
nerve cells in the substantia nigra.
Diagnosis
The diagnosis of PD is based on finding a combination of rigidity, tremor, slowness of
movement and lack of balance. The patient is often brought to the physician by the spouse and
may not even be aware of any symptoms. The patient's lack of awareness may represent denial
or a real inability to perceive the physical symptoms or depression. Computed tomography (CT)
or magnetic imaging (MRI) are useful in excluding other causes of symptoms such as tumors ormultiple small strokes. MRI is especially useful in excluding shrinkage of the brainstem and
cerebellum, conditions that may be associated with some of the PD+ disorders.
Primary Features
While seldom the main symptom, rigidity is one of the four primary symptoms and is
experienced as a stiffness of the limbs. In PD, rigidity is greater in the limbs whereas in PD+,
rigidity is greater in the neck and trunk.
Tremor, at rest, is usually the earliest and most prominent symptom of PD, and is present inapproximately 70% of patients. It is usually the symptom that brings the patient to the doctor.
Patients with tremor usually have a longer and more "benign" course than patients without
tremor. The tremor, initially, can involve one side more than the other and the hands more
than the feet. The tremor is usually present when the limbs are resting; when the patient is
seated with his/her hand supported or when the patient is walking with hands hanging loosely.
The tremor usually stops when the muscles are activated. For some patients, the tremor may
be more prominent when maintaining a posture (postural tremor). Occasionally the tremor
may increase during movement (kinetic tremor) or the tremor may be prominent during
writing (writing tremor). Postural or kinetic tremor are more common in Essential Tremor (ET)
than in PD. Several types of tremor can coexist in PD including resting, postural, kinetic and
writing tremor.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 54/59
Bradykinesia is the most disabling symptom of PD. Bradykinesia includes slowness and loss of
movement, delays in starting to move, frequent stoppages of movement, fatigue and inability
to perform two movements at once, e.g. swinging the arms while walking. The PD patient who
is bradykinetic differs from the patient who is weak or paralyzed. Weakness or paralysis is an
inability to move because of a lack of power. The PD patient has enough power to move, but
cannot move rapidly.
Postural instability results from impairment of the balance reflexes that are responsible for
correcting equilibrium in response to positional changes. In PD, as a result of postural
instability, patients fall easily. Postural instability may be experienced when a patient attempts
to turn or enter a doorway.
The disturbance in walking in PD is characterized by short steps and results from a combination
of rigidity, bradykinesia and postural instability.
Click here for Symptoms of Parkinson's.
Secondary Features
Secondary features may not be disabling and occur in less than 50% of patients. However,
secondary features like speech and swallowing difficulty can become disabling.
Dementia, characterized by disorientation, confusion and memory loss, occurs in
approximately 30% of patients with PD. Its prevalence increases with age and may be related to
Alzheimer Disease (AD). The dementia of PD may be aggravated by treatment with levodopa
and other drugs, especially anticholinergic and amantadine. The psychiatric side effects ofantiparkinson drugs include an excited, confusional state with delusions or hallucinations.
Depression is frequent in PD, occurring in 50 to 75% of all patients. In 50% of these patients,
the depression is severe enough to require psychological consultation or treatment with
antidepressant drugs. Depression, in PD, may be either a reaction to having a chronic illness or
it may be caused by a chemical imbalance. Supporting the idea that depression is a chemical
imbalance are observations that depression may precede the other symptoms and that there
may be no relationship between the severity of the depression and the severity of PD.
Facial masking results from a combination of bradykinesia and rigidity of the facial muscles.
Disappearance of facial masking may be the earliest sign of successful treatment.
Speech difficulty may include a decrease in volume, a tendency for words to run together and
slurring. The speech difficulty may vary from slight to marked. Some degree of swallowing
difficulty is present in many patients, but severe swallowing difficulty is uncommon, though it
may occur in late PD. Speech and swallowing difficulties result from a combination of rigidity
and bradykinesia in the muscles of the throat and mouth.
Other secondary symptoms include:
Drooling and oily skin are common symptoms but are not disabling.
Dizziness, in PD, is related to a drop in blood pressure on standing and may be aggravated bylevodopa and dopamine agonists.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 55/59
Shortness of breath results from a combination of chest wall rigidity and abnormal, drug-
induced muscle movement.
Urinary problems occur in PD, usually taking the form of urgency. In elderly men, such urgency
is more likely to result from an enlarged prostate.
Constipation, a common symptom in the elderly, is frequent in PD and may be worsened by
drugs, especially anticholinergic and amantadine.
Impotence, another common symptom of the elderly, is also frequent in PD.
Symptoms of burning or cold sensations, muscle cramps and joint pains also occur in PD.
The gold standard for confirming the diagnosis of idiopathic PD is finding Lewy bodies in the
nerve cells of the substantia nigra after death. Approximately 75% of patients who are
diagnosed with PD are found, after death, to have Lewy bodies. The inverse of the above is that
25% of patients who are diagnosed as having typical PD are found, after death, not to have
Lewy bodies. This means that although Lewy bodies are, at present, the best markers for PD,
their presence (or absence) is still not conclusive.
At least 60% of the nerve cells in the substantia nigra and 80% of the dopamine in the striatum
must be lost before the first symptoms of PD appear. This indicates that the process of PD, as
distinct from the recognized disease, is on-going for many years before it is diagnosed. The idea
that there are a large number of seemingly "normal" people who have PD and who may, if they
live long enough, develop PD symptoms, challenges physicians to develop methods for
identifying these people so that treatment to slow progression, with drugs such as selegiline
(Eldepryl), can start before PD becomes obvious.
Click here for secondary symptoms.
Cause
Research on the cause of PD centers on why the nerve cells in the substantia nigra and locus
ceruleus die early while nerve cells in other areas are not affected. The presence of pigment
(neuromelanin) in these nerve cells may provide clues since the pigment in these cells is
derived from dopamine. An unrecognized environmental toxin (similar to MPTP) or a genetic
defect may accelerate the loss of pigment. As nerve cells die throughout the course of PD,identifying the cause and halting the progress is a research priority.
Given how common PD is and how easily it can be recognized, it is surprising that the first
description of PD was in 1817. This suggests that it may be related to an environmental toxin, a
product of the industrial revolution. If environmental toxins are responsible for PD there should
be variations in the occurrence of PD in different areas of the world. The occurrence of PD is
similar in most Western countries, but less in the Mediterranean countries, Japan and China.
Although there are no geographical clusters that would unequivocally establish an
environmental cause, there is enough supportive data to encourage the continuation of
environmental studies.
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 56/59
One observation linking environmental toxins to PD is a lower incidence of cigarette smokers
among PD patients. This suggests there may be a substance in cigarette smoke that protects
against an environmental toxin. Another observation linking environmental toxins to PD is the
higher occurrence of PD in rural areas, where more herbicides and pesticides are used than in
urban areas.
If PD is inherited, such a tendency might be revealed in studies of twins. In a study of 43 pairs
of identical twins and 19 pairs of non-identical twins, in which one of the twins had PD, it was
found that in only one identical twin pair did both twins have PD. Thus, the frequency of PD in
identical twins was similar to what would be expected by chance alone. Other studies also
failed to reveal an increased occurrence of PD in families. For a long time, then, it was believed
that whatever the role of genetics was, it was subtle. Recently, appreciating that there may be
a long delay in the appearance of the symptoms of PD, and using techniques such as positron
emission tomography (PET) to detect PD before it can be recognized by a physician, the
assumption that PD is not inherited is being questioned. While the exact role of genetics is
unknown, it is more important than previously suspected.
The major finding linking PD to environmental toxins is the identification of the chemical MPTP
as a cause of a permanent disorder similar to PD. The role of MPTP surfaced in 1977, when
parkinsonism developed in a young man. Although no cause for the disease could be found,
drugs were suspected. The patient committed suicide and his autopsy revealed loss of nerve
cells in the substantia nigra. Subsequently, Dr. William Langston identified several patients with
parkinsonism who had also been using drugs that contained MPTP. This observation, and
subsequent observations by Langston and Burns that MPTP caused parkinsonism in monkeys,
revolutioned thinking about PD. Whether MPTP or similar compounds play a role in causing PD
is not known. The study of MPTP, however, has led to new insights into PD and in formulatingstrategies for halting its progress.
The virus that caused encephalitis (sleeping sickness) also caused symptoms resembling PD.
This disorder is described in the book and movie by Oliver Sacks: "Awakenings." The
parkinsonian symptoms caused by the virus appeared, in some, during the actual epidemic
(1919 to 1926) while for others, symptoms appeared several years later: Post encephalitic
parkinsonism. The viral disease progressed more slowly than PD. In the substantia nigra, there
was greater loss of nerve cells, but without Lewy bodies. Although other viruses can, though
rarely, cause parkinsonism, many studies have failed to reveal a virus as the cause of idiopathic
PD.
Professional boxers who receive multiple, severe blows to the brain may develop a Parkinson
Syndrome that is progressive. Severe head injuries with prolonged coma can result in a variety
of movement disorders including Parkinson's Syndrome.
The mean age of onset of PD is 60 years. Thus, though not applicable to young-onset patients,
age-related changes may be important in looking for the cause of PD, including:
Age-related losses of nerve cells and pigment in the substantia nigra that peak at age 60. Since
the pigment may protect the dopamine containing nerve cells from the effects of MPTP, toxins
or free radicals, the loss of pigment may predispose the brain of older people to PD.

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 57/59
Age-related loss of dopamine in the striatum. Although the distribution of the age-related
dopamine loss in the striatum is different from the loss in PD, the age-related dopamine loss,
coupled with the disease-related dopamine loss, may make the older brain more vulnerable to
PD.
Age-related increase in the amount of the enzyme MAO-B. The increase in brain MAO-B maypromote the formation of toxic free radicals.
Age-related increase of brain iron and an even greater increase of iron in PD. Brain iron is
undetectable at birth, gradually increasing through the first three decades and concentrating in
the substantia nigra and globus pallidus. Brain iron remains stable until the sixth or seventh
decade when there is a further increase, particularly in the striatum. Iron is absorbed through
the gut and transported into the brain by a protein called transferrin. Iron is stored within the
support cells (glia), where it is bound to another protein, ferritin.
When iron is bound to protein it is harmless. When iron is not bound it is reactive and
promotes the formation of free radicals. Several reports indicate that the increased iron in PD isfree. Although there is evidence that the increased iron has a role in PD it is possible that the
increased iron in PD is a secondary phenomenon.
Disorders Similar to PD
There are several disorders which, at one time or another in their course, may be mistaken for
PD. These disorders may begin differently from PD, progress more rapidly and respond poorly
or not at all to levodopa. Tremor at rest is usually not part of these disorders. Some of these
disorders, especially the PD+ disorders, may be distinguished from PD by the presence of
increased iron in the striatum on MRI. While it is probable that these disorders will be shown
to have causes different from PD, it is conceivable that, ultimately, they may be shown to have
the same cause.
Progressive Supranuclear Palsy (PSP)
PSP begins at about the same time as PD. It is one of the more common PD+ syndromes, with
an occurrence approximately 1% of PD. PSP progresses more rapidly than PD with disability
occurring after 3 to 10 years. PSP begins with falls, eye movement abnormalities and slurred
speech. Tremor is usually absent. Click here for more information.
Multisystem Atrophy (MSA)
There are several disorders which, when well developed, are easily distinguishable from PD.
These disorders are called Multisystem Atrophy (MSA) because, unlike in PD, more than one
system degenerates. The Shy-Drager Syndrome, Striato-Nigral Degeneration and
OlivoPontoCerebellar Atrophy are often grouped under Multisystem Atrophy.
Shy-Drager Syndrome
The main feature of the Shy-Drager Syndrome is dizziness on standing, with an occasional
patient actually blacking out. This results from a drop in blood pressure on standing andreflects a loss of tone of the blood vessels that regulate blood pressure. Many patients with PD
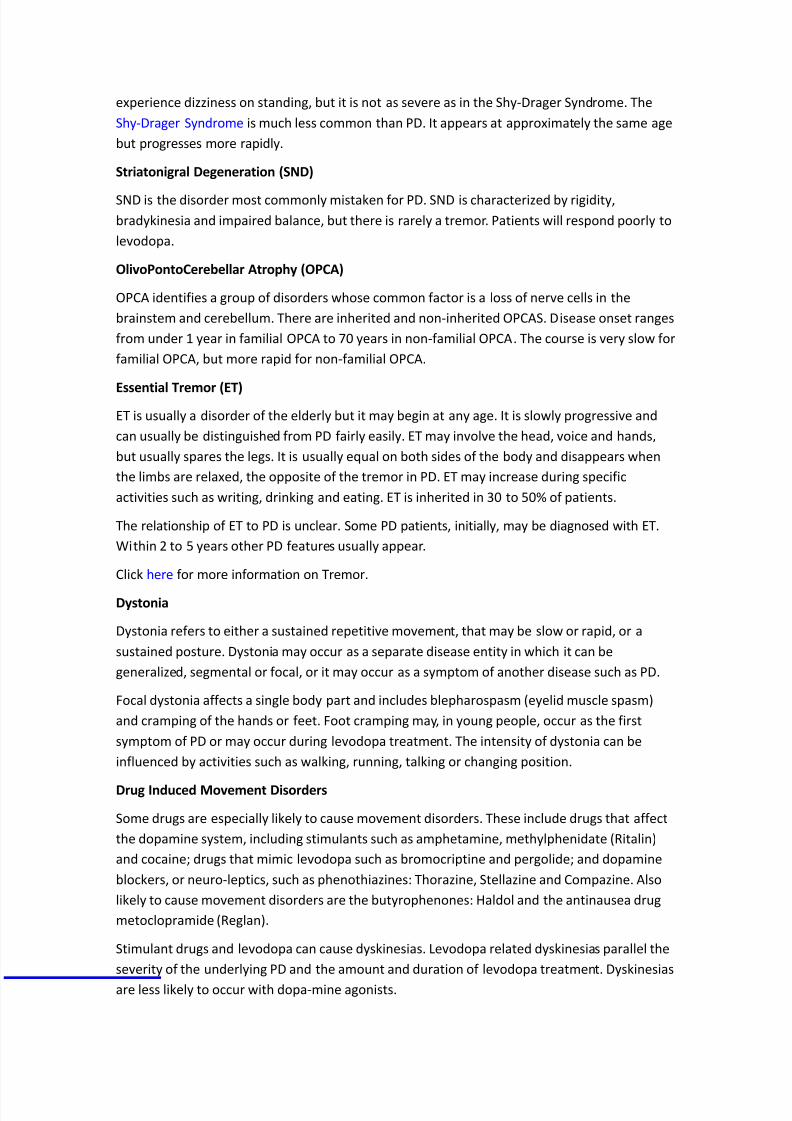
8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 58/59

8/13/2019 Texts Medicine
http://slidepdf.com/reader/full/texts-medicine 59/59
Tremor may be caused or aggravated by many drugs including steroids, anti-asthma drugs,
caffeine, lithium, nicotine, thyroid hormones, certain anti-depressant drugs and anticonvulsant
drugs such as valproic acid (Depakoate). Alcohol may both lessen and aggravate tremors.
http://www.pdcaregiver.org/WhatIsParkinsons.html