thalassemia and hemoglobinopathies edna d’souza product specialist clinical diagnostic division
TRANSCRIPT

Thalassemia and Hemoglobinopathies
Edna D’SouzaProduct Specialist
Clinical Diagnostic Division

Hemoglobinopathies


Types of defects Thalassemia
Sickle cell anemia Hb EHb DHb QHb J Hb C
Hb Lepore Hb H

Caste groups that have a higher carrier rate
Sindhis and Punjabis from Northern India,
Bhanushali’s, Kutchis, Lohana’s from Gujarat,
Mahar’s, Neobuddhist’s, Koli’s and Agri’s from Maharashtra,
Gowda’s and Lingayat’s from Karnataka

Scenario of Hb S carrier incidence in India
(Mohanty & Colah et al, 2010)

HEMOGLOBIN E
3 - 50%
5 -35 %
HEMOGLOBIN D
2 %

India: Average Incidence of thalassemia carriers -3.9% (varying from 1-
17%) 1 in 25 Carriers in India!!!! 30-40 million carriers.
Affected births/yr Thalassemia major- 9000-10000 (1-2 majors born every hour ) Sickle Cell Disease-~5000
Thalassemia –National Problem

ThalassemiasAre a group of autosomal recessive disorders characterized by the
complete absence or defect in the synthesis of the globin chains.
β- thalassemia presents itself in three forms:
β thalassemia trait asymptomatic condition wherein there is mild microcytic , hypochromic anemia
β thalassemia major
β thalassemia intermedia
The patient suffers from the disorder. Is unable to synthesize hemoglobin and requires blood transfusion to survive beginning as early as 6 months of ageGenotypically they are similar to thal majors. However phenotypically they are not dependent on regular transfusions.

thalassemia major: production of -globin chains is severely impaired
Patients with thalassemia major need blood transfusions every 3-4 weeks to maintain their hemoglobin levels
Due to transfusions they are at a risk of: Blood transfusion related infections
like hepatitis C, hepatitis B , HIV
Iron overload with a damage to all vital organs like heart, lung , liver , kidney etc.
The survival of individuals who have been well transfused and treated with appropriate chelation extends beyond 30 years.
clinical presentation
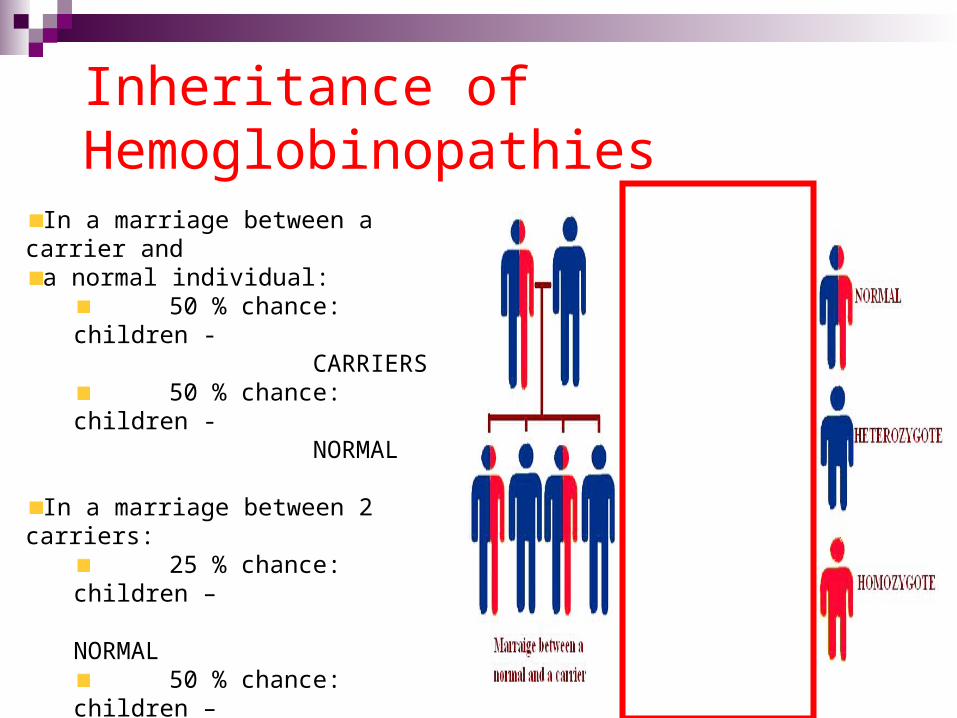
Inheritance of Hemoglobinopathies
In a marriage between a carrier and
a normal individual: 50 % chance: children
- CARRIERS
50 % chance: children - NORMAL
In a marriage between 2 carriers: 25 % chance: children
–
NORMAL50 % chance: children
–
CARRIERS 25 % chance: children
–
HOMOZYGOTES

How to avoid baby with Thalassemia major Follow only 2 simple steps Step 1: Get your partner and yourself tested for
thalassemia before marriage. Step 2: If both your partner and you are
thalassemia minors, consult your doctor for prenatal diagnostic test.
•A complete Blood count test
•A Hemoglobin HPLC analysis to estimate Hb A2 levels.
What test is required to detect Thalassemia

Hb A
Hb F
Hb A2
Adult~ 94-96
%0- 1%
1.8-3.5%
Thal Minor
90-92% 1-5% 4-8%
Percentage of hemoglobins

Variant II hemoglobin testing system
Fully automated, High-throughput
hemoglobin analyzer Providing an integrated
method for sample preparation, separation and determination of the relative percent of specific hemoglobins in whole blood.

Why HPLC ???FEATURE HPLC ElectrophoresisQuantification Yes, Objective No, Subjective
Automation Yes Manual and Laborious
Data Storage Convenient Not convenient
Optimization Calibrators and QC Sera Not optimised
Multianalyte More clinical info from each assay
Requires both acid and alkaline ELP
Operator toOperator Variation
None Yes
Time Taken 6.5 min/sample Couple of hours to entire day.
Sample capacity
100, continuous sample loading facility
Fixed depending on the wells
Number of steps
One Many
Reporting format
Printable Chromatogram with complete information
Electrophoresis strip only shows band separations

9 STEPS to prepare hemolysate
Time taken >40 MINUTES
PER SAMPLE
On Bio-Rad VARIANT II capped primary tubes are directly loaded.
Time taken1 STEP – 1 MINUTE -
PER SAMPLE
Sample Preparation
Chances of manual error are
high
Complete automation No manual error introduced

Results required to be interpreted by an experienced technician
Misinterpretation of bands is possible resulting in incorrect diagnosis
FEATURE HPLC ELECTROPHORESIS
Quantification Yes, Objective No, Subjective
ELECTROPHORESISV/S
HPLC
Accurate quantification of Hb A2 and Hb F
Reproducibility of results

Along with manual errors , the time taken in reporting could be almost a day
FEATURE HPLC ELECTROPHORESIS
Automation Complete Manual and Laborious
Primary tube sampling
Automated bar-code reading
ELECTROPHORESISV/S
HPLC
Time required to report results highly reduced

Electrophoresis strips information needs to be manually fed into the report
For quantitation of bands additional densitometer required
FEATURE HPLC ELECTROPHORESIS
Data Storage Convenient Not convenient
LAN
LAN
Lab Network
ELECTROPHORESISV/S
HPLC
All the information of the sample chromatogram is directly transferred onto the report
Complete information of all the percentages of the various hemoglobins on the report

FEATURE HPLC ELECTROPHORESIS
Multianalyte More clinical info from each
assay
Requires both acid
And alkaline ELP
Hb S/Hb D
Hb D
Hb S
ELECTROPHORESISV/S
HPLC
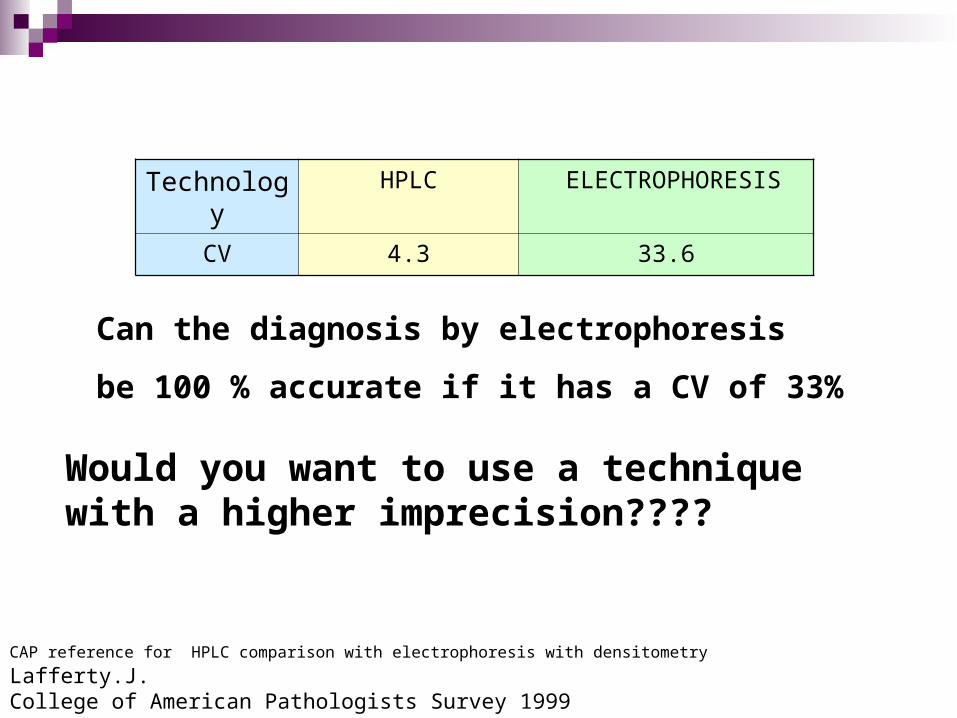
Technology HPLC ELECTROPHORESIS
CV 4.3 33.6
Would you want to use a technique with a higher imprecision????
Can the diagnosis by electrophoresis
be 100 % accurate if it has a CV of 33%
CAP reference for HPLC comparison with electrophoresis with densitometry Lafferty.J. College of American Pathologists Survey 1999
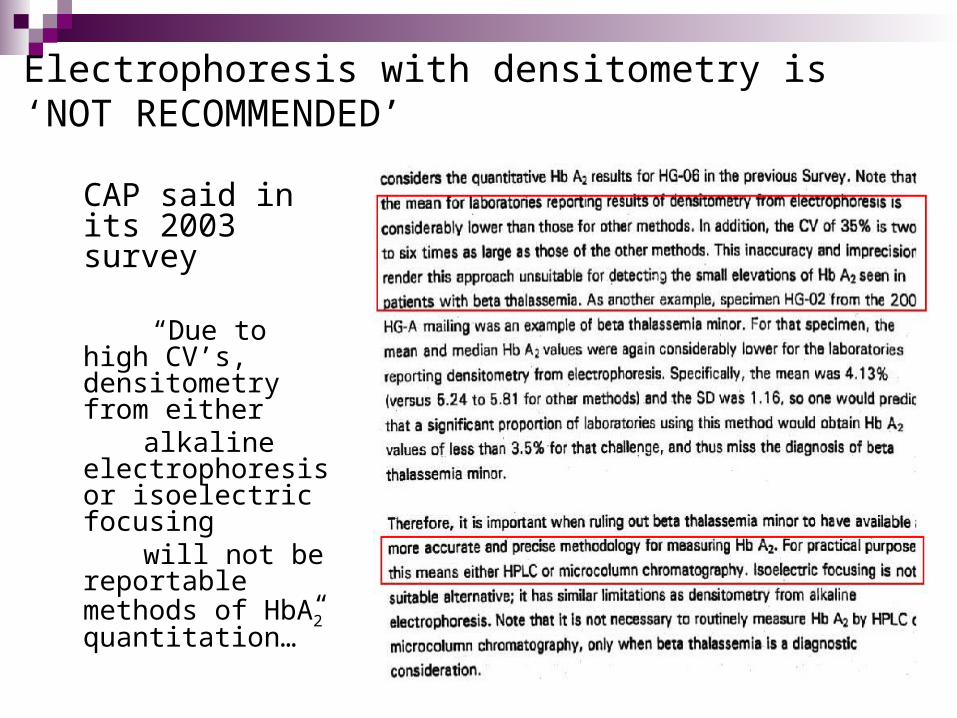
Electrophoresis with densitometry is ‘NOT RECOMMENDED’
CAP said in its 2003 survey
“Due to high CV’s, densitometry from either
alkaline electrophoresis or isoelectric focusing
will not be reportable methods of HbA2 quantitation…”

Evaluation of VariantCollege of American Pathologists
Analyzed 1,370 consecutive samples over a 1-year period using an automated Bio-Rad HPLC system and compared the results with standard methods
HPLC analysis detected 3 abnormal Hb patterns without corresponding gel abnormalities
HPLC is more sensitive than the standard methods for the detection of Hb variants and can be considered for routine use by hospital or clinical reference laboratories.
Improved Hemoglobin Analysis
by High-Performance Liquid Chromatography


β-thalassemia trait
Hb S trait
Hb E trait Hb D-Punjab trait
Variant II Chromatogram Reports

screen forthalassemia
New births of beta-thalassemia major can be prevented
do it the right way
The screening test needs to done only once in a person’s life
but done the right way THANK YOU
urgent need to identify all carriers
screen forthalassemia