thalassemia study in indiashodhganga.inflibnet.ac.in/bitstream/10603/77029/11/12_chapter-3.pdf ·...
TRANSCRIPT

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
47
Gorgan, Iran. Screening for Thalassemia and Hemoglobinopathies in Canada observed by
Bijayini et al. (2010). The observations and study on BT was studied by Cao and Galanello
(2010). James et al., (2010) elevated exhaled carbon monoxide concentration in
hemoglobinopathies and its relation to red blood cell transfusion therapy. Hira et al. (2011).
Find out the complications in thalassemia patients receiving blood transfusion. Thompson et
al., (2011) investigated the red cell alloimmunization in a diverse population of transfused
patients with thalassemia. Recently, Abdelmohsen (2011) studied the exhaled carbon
monoxide concentration in beta-thalassemia and its relation to red blood cell transfusion
therapy in pediatrics. Cappellini et al., (2011) observed iron chelation with deferasirox in
adult and pediatric patients with thalassemia major. Recently Arıca et al. (2012) evaluate the
hemoglobinopathy screening results of a six year period in Turkey. Fabrice et al (2012),
observed the genetic modifiers of beta-thalassemia and clinical severity as assessed by age at
first transfusion. Marion et al. (2012) studied the 0-thalassemia deletion in a Greek patient
with HbH disease and β-thalassemia trait. Yixuan et al. (2012) studied genetic correction of
β-thalassemia patient-specific iPS cells and its use in improving hemoglobin production in
irradiated SCID mice.
Thalassemia study in India
Sood et al. (1993) in his report of ICMR Task Force study, he studied on thalassemia in
India. The burden of haemoglobinopathies in India studied by Balgir (2000). Krishnamurti
(2000) in his report he observed the hemoglobin E-beta-thalassemia in Northeast India. Vaz
et al. (2000) finds the distribution of BT mutations in the Indian population. Piplani (2000)
observed the hemoglobin E disorders in North East India. Genetic epidemiology of the sickle
cell anaemia in India observed by Balgir (2001). Raj et al. (2001) studied an indigenously
manufactured rapid immunochromatographic test for detection of HBsAg. A screening test
for beta thalassemia trait pointed out by Mehta (2002). Agarwal et al. (2003) observed the
prenatal diagnosis in beta-thalassemia in India. Clinico-hematological profile of HbE
syndrome in adults and children studied by Tyagi et al. (2004). Safety of oral iron chelator
desferiprone in young thalassemics observed by Naithani et al. (2005).
Balgir (2005) in his ten years cohort study he studied the Spectrum of haemoglobinopathies
in the state of Orissa. Clinical and radiological study of oro-facial manifestations in
Thalassaemia studied by Patil (2006). Aberrant heterosis in haemoglobinopathies with special
reference to β -thalassemia and structurally abnormal haemoglobins E and S in Orissa, India.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
48
find out by Balgir (2007). Bangal et al. (2009) observed the recurrent pregnancy loss due to
Haemoglobinopathy. Quais Mujawar et al. (2009) in his case study he reported haemoglobin
E-beta thalassemia at Bijapur, South India. Recently, Sharma and Pancholi (2010) studied the
management of TM by oral Iron Chelators.
Newborn Screening in India is studied by Seema Kapoor and Madhulika Kabra (2010). In
2010, Balgir found the phenotypic diversity of sickle cell disorders with special emphasis on
public health genetics in India. Singh et al., (2010) studied the effect of wheat grass tablets on
the frequency of blood transfusions in Thalassemia Major.
2.4 Transfusion transmitted Diseases
Orofacial complications in thalassemia
Pusaksrikit et al. (1987) finds the occlusion of the teeth in thalassemic patients. Drew and
Sach (1997) studied the management of thalassemia induced skeletal facial deformity. Effects
of thalassemia major on components of the craniofacial complex studied by Bassimitci
(1996). Agha (2000) evaluates the maxillofacial anomalies in Beta thalassemia major.
Hypoparathyroidism and intracranial calcification in b-thalassemia major observed by
Zafeiriou et al. (2001). Abu Alhaija et al. (2002) observed the cephalometric measurements
and facial deformities in subjects with beta-thalassaemia major. Singh and
Venketasubramanian (2004) studied the recurrent cerebral infarction in beta thalassaemia
major. Amini et al. (2007) studied the craniofacial morphology of Iranian children with TM.
Salehi et al. (2007) studied the prevalence of Orofacial complications in Iranian Patients with
β -Thalassemia Major. In 2008, Ashraf evaluates the oro-maxillofacial changes in major
thalassemia. Verma et al. (2007) studied the intracranial calcification in beta thalassemia
Major. Srdjan et al. (2008) observed the consanguineous marriages and endemic malaria, can
inbreeding increase population fitness.
Malaria in thalassemic patients
Nittis and Spiliopulos (1937) Studied that Mediterranean anemia may be a peculiar form of
malaria. A selective advantage for survival in individuals with the thalassemia trait in regions
where malaria is endemic. The RBCs of patients with Hb H disease have also shown a
suppressive effect on the growth of the parasites. This effect is not observed in α thalassemia
trait. Fawdry (1944) his studies focused on conducted Greeks and on Cyprus concluded that
malaria played no part in the causation of disease.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
49
Dover and Schultz (1971) studied the transfusion-induced malaria. Transfusion-induced
malaria from an asymptomatic carrier observed by Najem and Sulzer (1976). In 1980, Joishy
and Lopez observed the transfusion-induced malaria in a splenectomized β-thalassemia major
patient and blood donor screening methods. Willcox et al. (1983) in his case study he
observed the Plasmodium falciparum malaria in haemoglobin S and beta-thalassemia traits.
Luzzi et al. (1991) finds the surface antigen expression on Plasmodium falciparum-infected
erythrocytes is modified in alpha- and beta-thalassemia. In 1993, Snounou et al. finds the
high sensitivity of detection of malaria parasites by the use of nested polymerase chain
reaction. Black et al. (1994) pointed out the mixed infections with Plasmodium falciparum
and P. malariae and fever in malaria. Williams et al. (1996) observed the high incidence of
malaria in alpha-thalassemic children.
Allen et al. (1997) studied the alpha -thalassemia protects children against disease caused by
other infections as well as malaria. Weatherall (1997) observed the correlation of the
thalassemia and malaria. Aluoch (1997) observed the higher resistance to Plasmodium
falciparum infection in patients with homozygous sickle cell disease in western Kenya. The
α+-thalassaemias are some of the best recognized malaria-protective polymorphisms. Flint et
al. (1998) studied the population genetics of the haemoglobinopathies. Williams (1999)
observes the mechanisms of malaria protection in the thalassemia syndromes.
Research involving both population and case-control studies has provided strong evidence
that the high frequency of the milder varieties of alpha-thalassemia is related to protection
against P. falciparum malaria (Weatherall and Clegg, 2002). Seed et al. (2005) reviewed the
status and potential role of laboratory testing to prevent transfusion-transmitted malaria.
Williams et al. (2005) observed the negative epistasis between the malaria-protective effects
of alpha+-thalassemia and the sickle cell trait. Kitchen and Chiodini (2006) observed the
blood transfusion transmitted malaria. Wambua et al. (2006) find out the effect of α +-
thalassemia on the Incidence of Malaria and other diseases in children living on the coast of
Kenya. May et al. (2007) studied the hemoglobin variants and disease manifestations in
severe P. falciparum. Transfusion-transmitted infections like hepatitis B, C, HIV, malaria and
syphilis studied by Hira et al, (2011).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
50
Hepatitis/ Viral infections
Sumathy et. al, (1992) studied dipstick immunobinding enzyme-linked immunosorbent assay
for serodiagnosis of hepatitis B and delta virus infections. Ali et al. (2003) studied the
frequency of hepatitis C virus antibodies in blood donors in combined military hospital,
Quetta, at Pakisthan. Hepatitis C virus seropositivity in repeatedly transfused TM patients
studied by Muhammad et al. (2004). Zandieh et al. (2005) observed the Transfusion
Transmitted Virus (TTV) infection in thalassemic patients.
Spleenectomy
Cohen et. al (1980a) studied the transfusion requirements and splenectomy in thalassemia
major. Serum Levels of cytokines in poly-transfused patients with Beta-Thalassemia major:
Relationship to Splenectomy studied by Mohga et al. (2011). Al-Salem et al. (1989) studied
the splenectomy in children with sickle cell disease and thalassemia. Management of
thalassemia major by partial splenectomy studied by Bonani and Bahador (1994). Post-
splenectomy infection in Cooley’s anemia observed by Smith et al. (1964). Kheradpir MH,
Albouyeh M. Partial splenectomy in the treatment of thalassemia major studied by Kheradpir
et al. (1985). Moyamoya syndrome in a splenectomized patient with beta-thalassemia
intermedia observed by Sanefuji et al. (2006). Phrommintikul et al. (2006) observed the
Splenectomy and the risk factor for pulmonary hypertension in patients with thalassemia.
Other diseases and complications
Study of hepatitis B and C., prevalence and liver function in multiply transfused thalassemics
and their parents by author William et al. in 1992. Prati (2000) studied the benefits and
complications of regular blood transfusion in patients with beta-thalassemia major. In India
the study of fractures in transfusion dependent beta thalassemia by the author Basanagoudar
et al. (2001). Bruria et al. (2003) finds out the sleep disruption and objective sleepiness in
children with Thalassemia and congenital dyserythropoietic anemia. Lo et al. (2005)
observed the platelet alloimmunization after long-term red cell transfusion in transfusion-
dependent thalassemia patients. Masaya et. al (2010) studied the aortic valve replacement in a
patient with Alpha-Thalassemia. Kattamis et al. (1979) observed the chelation therapy and
ferritin levels in patients with homozygous β-thalassemia. Ghosh et al. (2000) he observed
the pseudomonas meningitis in adult, multitransfused thalassemia major patient.
Improvement in liver pathology of patients with β-thalassemia treated with Deferasirox for at
least 3 Years observed by Deugnier et al., (2011).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
51
3. PURPOSE OF THE STUDY
Due to lack of education, awareness and information, thousands of children with thalassemia
are born each year and the number is growing day by day. No one can feel the pain and
sufferings except thalassemic children themselves and their parents. Thalassemic and their
parents are waiting for proper and uninfected blood transfusion, medication, laboratory tests
and clinical management needed to erase the shadow of miseries and hanging sword of death
on their heads.
The purpose of this study is to determine the extent of transfusion-induced complications like
transmition of malaria and other diseases like HCV, HBsAg, VDRL, HIV and
microorganisms among blood transfused thalassemic children from Solapur District,
Maharashtra State, India during August-2008 to July 2010.
A secondary purpose was to examine risk factors associated with blood transfusion in
thalassemiac patients. Possible risk factors are: gender, age, family history, genetic
classification, pathophysiology, symptoms, incidence of Alloimmunization in frequently
transfused thalassemic and to evaluate factors which may influence the development of
antibodies, transfusion transmitted diseases. In addition, other complications, medications,
and number of blood transfusions will be determined. For the purpose of this analysis,
patients were considered not at risk of malaria, other disease and complications after
receiving proper nutrition, time to time blood transfusion and medication.
The entire survey study is to was carried out under the observations of medical officer from
thalassemia transfusion centre, Indian Red Cross Society, Gopabai Damani Blood Bank,
Solapur Maharashtra, India. The present research work focused on awareness about
thalassemia, its prevention and its medical care. This study will helps to establish and develop
a collaborative network of national and international thalassemia affected individuals,
medical and scientific communities involved in the field; health-related organizations and
pharmaceutical industries.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
52
4. OBJECTIVES
• To survey the thalassemic patients in different parts of Solapur district, Maharashtra
State, India.
• The aim of this thesis is to approach some of the existing problems related to the
scientific implementation of diagnosis, treatment and prevention by survey method,
possibly contributing to their solution.
• The current study aims to survey the effect of blood transfusion-induced or transmitted
malaria, other protozoan diseases and complications in thalassemia patient from Solapur
District.
• To avoid adverse reactions prevalence of infectious agents should safeguard the quality of
blood transfusion services. Blood donation practices, donor selection, and product
screening constitute some of the most important strategies that contribute to the safety
and adequacy of blood.
• The long term objective of this research is to develop in Solapur District, a National
referral center for blood transfusion in patients with thalassemia for proper monitoring of
better health care, to insist neonatal screening, regular laboratory tests, medication, proper
guidance for nutrition, health, awareness and proper education about the disease and
medication to the thalassemic patients countrywide.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
53
5. RESULTS AND DISCUSSION
This study was done on 125 clinically proved cases of thalassemia. They were of the age
group between 6 months to 18 years, 73 being male and 52 female. They were from different
parts of Solapur District, Maharashtra State (Table 4 and 4a).
The present study was carried out in the following blood banks and hospitals.
1) Indian Red Cross Society, Gopabai Damani Blood Bank, Solapur.
2) Hedgewar Blood Bank, Solapur
3) Sou Sarjubhai Bajaj Blood Bank, Sub Branch Indian Red Cross Society, Pandharpur,
District-Solapur.
4) Shriman Rambhai Shah Blood Bank, Sub Branch, Indian Red Cross Society, Barshi,
District- Solapur.
5) Chatrapati Shivaji Rugnalaya, Government Hospital, Solapur.
Geographical distribution of thalassemia in Solapur District
The thalassemia patient’s code, patient’s initials, sex, diagnosis, Taluka wise distribution at
Solapur District, height, weight, growth and mortality shown in Table-4. The Taluka wise
geographical distribution of thalassemia patients and their prevalence percentage was shown
in Table-4a and Figure-3. The Talukawise distribution of thalassemia patients as follows:
Akkalkot: thalassemia major patients were five; total (4.00%)
Barshi: thalassemia major patients were five; total (6.40%)
Karmala: one BTI and TM three, total four patients (3.20%)
Madha: BTI three and TM two, total five patients (4.00%)
Malshirus: BTI one and TM three, total four (3.20%)
Mangalvedha: BTI two and TM four, Total six ((7.20%)
Mohol: BTMi two and TM four, total six (6.40%)
North Solapur: BTI one and TM two, total three (2.40%)
Pandharpur: BTI one, BTMi one and TM fifteen (12.00%)
South Solapur: BTI one, BTMi two and TM eleven, total fourteen (11.20%)
Sangola: BTMi one and TM four, Total five (4.80%)
Solapur city: SCT one, BTI one, TM 19, total forty two (35.20%).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
54
Table 4. Showes total number of thalassemia patient, with their code, initials, sex, diagnosis,
locality, height (Inch), weight (Kg), growth and mortality.
Patient
Code
Patient
Initials Sex Taluka Diagnosis
Height
(Inch)
Weight
(Kg)
Growth
Mortality
1 BMH F Akkalkot TM 24 7 Yes No
2 MAD M Mohol TM 24 8 Yes No
3 MPA F Solapur TM 24 8 Yes No
4 KPR F Solapur TM 26 9 Yes No
5 JSS F Solapur TM 25 9 Yes No
6 JP F S. Solapur TM 24 8 Yes No
7 GDD F S. Solapur TM 30 10 Yes No
8 DSS M Pandharpur BTI 34 8 Yes No
9 KLB F Solapur TM 32 10 Yes No
10 SGS M Malshirus TM 32 10 Yes No
11 MTM F Solapur TM 30 8 Yes No
12 PST M Solapur TM 36 12 No No
13 SSS M Mohol TM 32 10 Yes No
14 KSS M Solapur TM 34 12.5 Yes No
15 NA F Solapur TM 24 8.5 Yes No
16 MAR F Solapur TM 38 13.5 Yes No
17 STS F Sangola TM 38 13 Yes No
18 SSS M Solapur TM 34 15 Yes No
19 CRR M Akkalkot TM 32 10 Yes No
20 KSS M Solapur TM 40 12 Yes No
21 GSA M Solapur TM 41 20 No No
22 BSR F Pandharpur TM 37 12 Yes No
23 CNT M S. Solapur BTMi 34 12 Yes No
24 BKG F S. Solapur TM 36 10.5 Yes No
25 SOS1 M S. Solapur TM 37 13 Yes No
26 SOS2 M S. Solapur TM 36 12.5 Yes No
27 SSS M Malshirus TM 43 17 No No
28 BLM M N. Solapur BTI 42 15 No No
29 JPA F Solapur TM 37 14 Yes No
30 TRM M Mangalvedha TM 40 13 Yes No
31 PYR M Mangalvedha BTI 43 15 No No
32 RGS M Malshirus BTI 43 18.5 No No

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
55
Table 4. Continued…
Code
Patient
Initials Sex Taluka Diagnosis
Height
(Inch)
Weight
(Kg) Growth Mortality
33 MPP F Pandharpur TM 46 20 No No
34 GPO M Solapur TM 40 15 Yes No
35 TRI M Barshi TM 38 14 Yes No
36 KNS M N. Solapur TM 43 15 Yes No
37 VDS M Solapur TM 42 17 Yes No
38 PSB F Solapur BTMi 44 17.5 Yes No
39 RSB M Mangalvedha TM 42 16 Yes No
40 IVY F Pandharpur TM 41 14 Yes No
41 ARM M S. Solapur BTI 37 14 Yes No
42 GAR M Pandharpur TM 43 20 Yes No
43 KSM M S. Solapur TM 41 23 Yes No
44 KAV F Barshi TM 48 23 No No
45 PUA F Solapur TM 44 21 Yes No
46 DRS M Pandharpur TM 41 17 Yes No
47 BMN M Solapur TM 42 16 Yes No
48 LAB M Solapur TM 44 16 Yes No
49 VDS M Solapur TM 44 20 Yes No
50 SVP M Pandharpur BTMi 45 17.5 Yes No
51 KAN F Solapur TM 36 12 No No
52 SSS F Mohol TM 41 16 Yes No
53 BUT M Karmala TM 45 18 Yes No
54 MA M Sangola BTMi 36 20 Yes Yes
55 RSS M Mohol BTMi 44 20 Yes No
56 BNB M Solapur TM 43 15 Yes No
57 IAS M Solapur TM 45 15 Yes No
58 ISY M Pandharpur TM 44 13 Yes No
59 TAS M Madha BTI 48 15 No No
60 PAM F Solapur TM 45 20 Yes No
61 QSA M Karmala BTI 48 20 No No
62 BSR M Akkalkot TM 36 12 Yes Yes
63 RST F Solapur TM 45 16 Yes No
64 QAS F Karmala TM 47 22 Yes No

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
56
Table 4. Continued…
Code
Patient
Initials Sex Taluka Diagnosis
Height
(Inch)
Weight
(Kg) Growth Mortality
65 GAM M Solapur TM 42 25 Yes Yes
66 PHM M Solapur TM 49 24 Yes No
67 GPS F Barshi TM 49 23 Yes No
68 SV M Solapur TM 36 15 Yes No
69 NDN F Pandharpur TM 47 25 Yes No
70 MLD M Solapur TM 49 23 Yes No
71 PPV F S. Solapur TM 53 24 No No
72 MVM M Madha TM 50 28 Yes No
73 KAS M Barshi TM 44 20 Yes No
74 CYS M Solapur SCT 50 19 Yes No
75 LS M Solapur TM 44 13 Yes Yes
76 GSS F Solapur TM 48 21 Yes No
77 CGR M S. Solapur TM 42 22 Yes No
78 RS M madha TM 44 22 Yes Yes
79 JSS F Akkalkot TM 46 20 Yes No
80 TNJ F S. Solapur TM 46 22 Yes No
81 MPT F Solapur TM 47 21 Yes No
82 BHH M Malshirus TM 48 25 Yes No
83 BSM M Solapur TM 54 30 No No
84 NRB F Pandharpur TM 53 28 Yes No
85 HNK M Akkalkot TM 52 28 Yes No
86 KVM M Mangalvedha BTI 45 33 Yes No
87 NSA M Sangola TM 48 28 Yes No
88 WAS M Solapur BTI 51 24 Yes No
89 NAP M Mangalvedha TM 52 27 Yes No
90 MSS M Sangola TM 50 25 No No
91 LSD M S. Solapur BTMi 53 27 Yes No
92 ISS F Solapur BTMi 51 22 Yes No
93 SAN F Mohol TM 45 20 Yes Yes
94 GSM F Solapur TM 48 20 Yes No
95 RKT F Solapur TM 49 21 Yes No

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
57
Table 4. Continued…
Code
Patient
Initials Sex Taluka Diagnosis
Height
(Inch)
Weight
(Kg) Growth Mortality
96 RP M Pandharpur TM 44 22 Yes Yes
97 KSM M Pandharpur TM 58 28 Yes No
98 MRR F N. Solapur TM 52 20 Yes No
99 KPS F Solapur TM 59 30 No No
100 MMM F Barshi TM 54 26 Yes No
101 KBM F Mangalvedha BTI 48 23 Yes Yes
102 KJ F Solapur TM 48 20 Yes Yes
103 NPN F Pandharpur BTI 48 22 Yes Yes
104 KAA F Solapur TM 52 28.5 Yes No
105 PAD M Mohol TM 65 26.5 Yes Yes
106 HSD F Barshi TM 53 26 Yes Yes
107 GAS M Madha BTI 58 40 Yes No
108 KSS M Pandharpur BTI 58 35 Yes No
109 RYS M Sangola TM 51 26 Yes No
110 LSD F S. Solapur BTMi 63 45 No No
111 DML M Mohol BTMi 58 30 Yes No
112 SS M Pandharpur TM 58 32 Yes Yes
113 PKM M Barshi TM 52 28 Yes No
114 MGM M Madha BTI 54 31 Yes Yes
115 OBC F Karmala TM 55 29 Yes Yes
116 PVD M Mohol TM 65 36 Yes No
117 KKM F Mangalvedha BTI 62 35.5 No No
118 KR F Mangalvedha TM 48 30 Yes Yes
119 JVS M Sangola TM 60 30 Yes Yes
120 TAN F Solapur TM 60 38 No No
121 CLP F Solapur BTI 61 35 No No
122 DAM M Mangalvedha TM 48 39 Yes No
123 RVS M Solapur TM 56 30 Yes No
124 DRD F Barshi BTMi 56 30 Yes No
125 JSS F S. Solapur TM 60 33 No Yes

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
58
Table 4a. Taluka wise geographical distribution and prevalence percentage of thalassemia
patients in Solapur District.
Parameter Sex SCT BTI BTMi TM Total Patients %
Akkalkot M 00 00 00 03 03
F 00 00 00 02 02
T 00 00 00 05 05(4.00)
Barshi M 00 00 00 03 03
F 00 00 00 05 05
T 00 00 00 08 08(6.40)
Karmala M 00 01 00 01 02
F 00 00 00 02 02
T 00 01 00 03 04(3.20)
Madha M 00 03 00 02 05
F 00 00 00 00 00
T 00 03 00 02 05(4.00)
Malshirus M 00 01 00 03 04
F 00 00 00 00 00
T 00 01 00 03 04(3.20)
Mangalvedha M 00 02 00 04 06
F 00 00 00 03 03
T 00 02 00 07 09(7.20)
Mohol M 00 00 2 04 06
F 00 00 00 02 02
T 00 00 02 06 08(6.40)
North Solapur M 00 01 00 01 02
F 00 00 00 01 01
T 00 01 00 02 03(2.40)
Pandharpur M 00 02 01 05 08
F 00 01 00 06 07
T 00 03 01 11 15(12.00)
South Solapur M 00 01 02 04 07
F 00 00 00 07 07
T 00 01 02 11 14(11.20)
Sangola M 00 00 01 04 05
F 00 00 00 01 01
T 00 00 01 05 06(4.80)
Solapur City M 01 01 00 19 21(28.76)
F 00 00 00 23 23(44.23)
T 01 01 00 42 44(35.20)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
59
Type of thalassemic patients in Solapur District
In our study, Sickle cell thalassemia was: male 1(1.36%), female 0(00%), Total 1(0.8%); BTI
was: male 12(16.43%), female 4(7.69%), Total 16(12.8%); BTMi was: male 06(8.21%),
female 4(7.69%), Total 10(8.0%); TM was: male 54(73.97%), female 44(84.61%), Total
98(78.4%); (Table- 4b and Figure- 4). The results compared the trequency of β-thalassemia
trait and other hemoglobinopathies in northern and western India with the reports of Nishi et
al., (2010). There was maximum number of 98(98.4%) cases of TM as compared to BTMi
10(8.0%), BTI 16(12.8%) cases and SCT 1(0.8%) was observed. No cases of α thalassemia
were observed in our research work.
Table- 4b. Showed type of thalassemic patients entering the study (n=125)
Type of thalassemic
patient
Sex
Number of
patients (%)
Prevalence %
SCT
M 1 0.80
F 0 0.00
Total 1 0.8
BTI
M 12 9.6
F 4 3.2
Total 16 12.8
BTMi
M 6 4.8
F 4 3.2
Total 10 8.0
TM
M 54 43.2
F 44 35.2
Total 98 78.4
Total patients
M 73 58.4
F 52 41.6
Total M+F 125 100

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
60
Transfusion History:
All the 125 patients considered in our study were under regular blood transfusion therapy.
Age:
The age range of thalassemia patients (Table-4a) in our study was from 6 months to 18 years.
The mean age was around 8.75 years. Under age group 6 months-3 years, there were 19
male, 15 female patients and total male and female patients were 34(27.2%) observed. The
patients between 4-6 years age group was male 12, female 6 and total male and female
patients are 18(14.4%). In the age group of 7-10 years, the male patients are 22, female 11
and the total male and female patients were 33(26.4%) observed. The age group of 11-13
years, 9 male and 11 female patients observed, the total male and female patients were
20(16%). In the age group between 14-16 total 7 male and 3 female patients were observed,
the total male and female patients are 10(8%). In the age group between 17-18 years Male 4,
female 6 and total 10(8%) thalassemic patients were observed. Maximum patients [
34(27.2%)] were in the age group of 6 months to 3 years of age and minimum patients
[10(8%)] in both age group of 14-16 and 17-18 years age.
Sex:
Our study comprised of 73 (58.4%) males and 52(41.6%) females (Table- 4b) Thus, a higher
incidence of thalassemia in males was observed.
Height
The mean of Height of thalassemia patients showed in Table- 5 and Figure- 5. The mean
height of male patients were (45.43%) and female (44.67%). The total mean heigh of male
and female patients were (45.12%). The Height to Weight Ratio Chart is compared the data
from Disabled World. (2007).
Weight
The mean weight (Kg) of thalassemia patients showed in Table-5 and Figure-5. The average
mean weight of the male thalassemic patients were (20.45%) and female (20.38%) observed.
The total mean weitht of male and female patients were (20.42%). The observations of mean
height were showed the stunting of growth in thalassemic patients.
Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
61
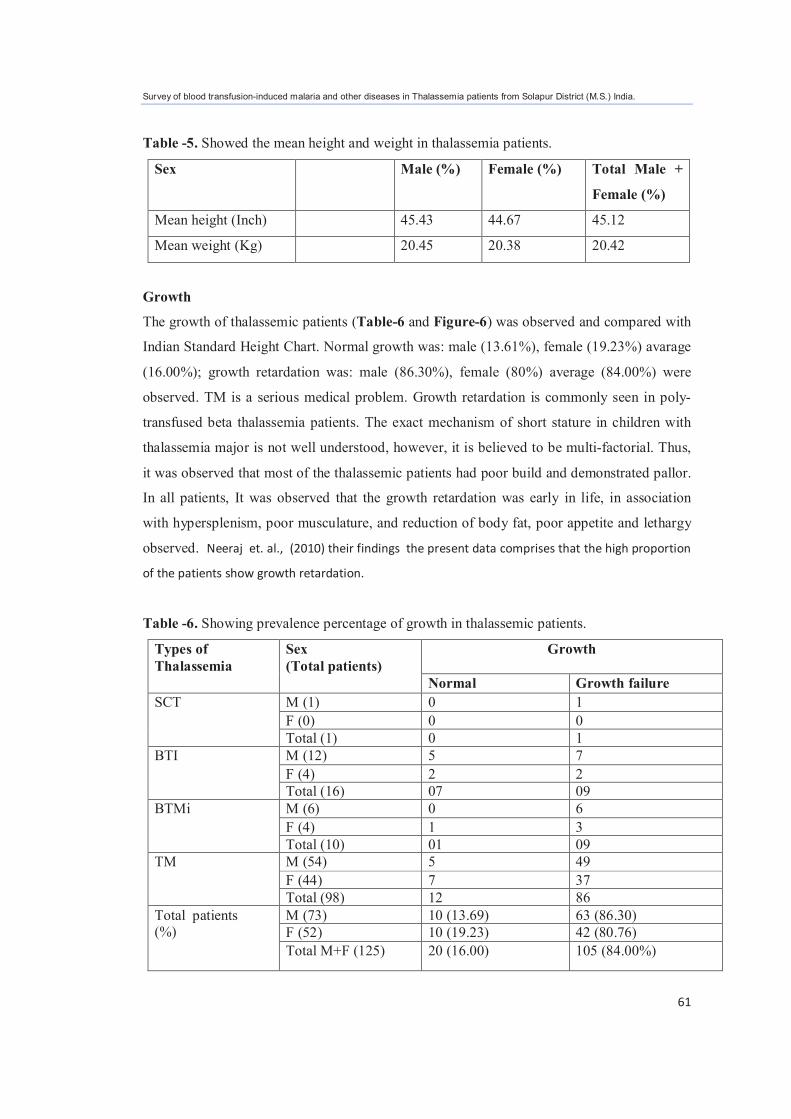
Table -5. Showed the mean height and weight in thalassemia patients.
Sex Male (%) Female (%) Total Male +
Female (%)
Mean height (Inch) 45.43 44.67 45.12
Mean weight (Kg) 20.45 20.38 20.42
Growth
The growth of thalassemic patients (Table-6 and Figure-6) was observed and compared with
Indian Standard Height Chart. Normal growth was: male (13.61%), female (19.23%) avarage
(16.00%); growth retardation was: male (86.30%), female (80%) average (84.00%) were
observed. TM is a serious medical problem. Growth retardation is commonly seen in poly-
transfused beta thalassemia patients. The exact mechanism of short stature in children with
thalassemia major is not well understood, however, it is believed to be multi-factorial. Thus,
it was observed that most of the thalassemic patients had poor build and demonstrated pallor.
In all patients, It was observed that the growth retardation was early in life, in association
with hypersplenism, poor musculature, and reduction of body fat, poor appetite and lethargy
observed. Neeraj et. al., (2010) their findings the present data comprises that the high proportion
of the patients show growth retardation.
Table -6. Showing prevalence percentage of growth in thalassemic patients.
Types of
Thalassemia
Sex
(Total patients)
Growth
Normal Growth failure
SCT
M (1) 0 1
F (0) 0 0
Total (1) 0 1
BTI
M (12) 5 7
F (4) 2 2
Total (16) 07 09
BTMi
M (6) 0 6
F (4) 1 3
Total (10) 01 09
TM
M (54) 5 49
F (44) 7 37
Total (98) 12 86
Total patients (%)
M (73) 10 (13.69) 63 (86.30)
F (52) 10 (19.23) 42 (80.76)
Total M+F (125) 20 (16.00) 105 (84.00%)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
62
Pedigree history of thalassemia patients
The pedigree of the 125 thalassemia patient and their families was represented in Figure-7.
Families are indicated with the name of the proband. Only initials of examined subjects were
reported. The observations in this pedigree support the hypothesis that the genes associated
with hemoglobin S, hemoglobin C and "classical thalassemia" are either very closely linked
or true alleles. The pedigree can identify family members who may be at risk of having
thalassemia disease or trait and should therefore be tested. A genetic counselor may also
identify a history of other conditions that may have a genetic component.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
63
Figure-7. Pedigree of thalassemia patient’s family.
Note: Number indicates patient’s case number and initials indicate patient’s names.
1 BMH
7 GDD
2 MAD
8 DSS
3 MPA
9 KLB
4 KPR
10 SGS
5 JSS
11 MTM
6 JP
12 PST

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
64
Figure-7. Continued..
13 SSS
19 CRR
14 KSS
20 KSS
15 NA
21 GSA
16 MAR
22 BSR
17 STS
23 CNT
18 SSS
24 BKG

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
65
Figure-7. Continued..
25 SOS1
31 PRY
26 SOS2
32 RGS
27 SSS
33 MPP
28 BLM
34 GPO
29 JPA
35 TRI
30 TRM
36 KNS

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
66
Figure-7. Continued..
37 VDS
43 KSM
38 PSB
44 KAV
39 RSB
45 PUA
40 IVY
46 DRS
41 ARM
47 BMN
42 GAR
48 LAB

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
67
Figure-7. Continued..
49 VDS
55 RSS
50 SVP
56 BNB
51 KAN
57 IAS
52 SSS
58
53 BVT
59 TAS
54 GHS
60 PAM

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
68
Figure-7. Continued..
61 QSA
67 GPS
62 BSR
68 SV
63 RST
69 NDN
64 QAS
70 MLD
65 GAM
71 PPV
66 PHM
72 MVM

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
69
Figure-7. Continued..
73 KAS
79 JSS
74 CYS
80 TNJ
75 LS
81 MPT
76 GSS
82 BHH
77 CGR
83 BSM
78 RS
84 NRB

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
70
Figure-7. Continued..
85 HNK
91 LSD
86 KVM
92 ISS
63 SAN
87 NSA
93 SAN
88 WAS
94 GSM
89 NAP
95 RKT
90 MSS
96 RP

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
71
Figure-7. Continued..
97 KSM
103 NPN
98 MRR
104 KAA
99 KSP
105 PAD
100 MMM
106 HSD
101 KBM
107 GAS
102 KJ
108 KSS

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
72
Figure-7. Continued..
109 RYS
115 OBC
110 LSD
116 PVD
111 DML
117 KKM
112 SS
118 KP
113 PKM
119 JVS
114 MGM
120 TAN

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
73
Figure-7. Continued..
121 CLP
124 DRD
122 DAM
125 JSS
123 RVS

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
74
Education
The literacy percentage (Table-7 and Figure-8) in thalassemia patients was: educated male
(65.75%), female (63.46%) avarage (64.8%); below four years of age- male (8.21%), female
(19.23%) avarage (12.8%); uneducated male (26.02%), female (17.30%) avarage (22.4%).
The majority (>22.4%) of thalassemia patients were illiterate with only 1.6% with a higher
education. General health education for those, suffering from thalassaemia, which will help
prevention and spread of thalassemia (Qamruz and Salahuddin, 2006). The present data
analyzed with the reports of Pakbaz et al., (2010), he observed the education and employment
status of children and adults with thalassemia in North America. Due to lack of education,
awareness and information, thousands of children with thalassemia are born each year and the
number is growing day by day. No one can feel the pains of sufferings except thalassemic
children themselves and their parents. Thalassemic and their parents are waiting for proper
and uninfected blood transfusion, medication, laboratory tests and clinical management
needed to erase the shadow of miseries and hanging sword of death on their heads.
Table-7. Showing the education in thalassemic patient
Sex Class Male Female Total Male + Female (%)
Education
LKG 2 2 4
UKG 1 1 2
1st 10 1 11
2nd 3 5 8 3rd 7 2 9
4th 4 1 5 5th 3 7 10
6th 4 7 11
7th 6 1 7
8th 0 3 3
9th 3 1 4 10th 5 2 7
11th 0 2 2 12th 0 0 0
B.A -I 0 1 1
*Below 4 Yr Total %
6 10 16
Uneducated Total %+ Below 4 Yr
19 + *6 = 25
9 +*10 =19 28 + *16 =44
Educated Total % 48 (65.75) 33 (63.46) 81 (64.8)
*Below 4 years patients considered as uneducated

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
75
Skin coloration
The skin color change (Table- 8 and Figure- 9) in thalassemia patients was: fair male
(23.28%), female (26.92%) avarage (24.8%); wheatish male (53.42%), female (59.61%)
avarage (56.0%); brownish male (4.10%), female (0.00%) total (2.4%); blackish male
(19.1%), female (13.46%) avarage (16.8%) were observed.
Table- 8. Showing the skin color of thalassemic patient.
Sex Male (%) Female (%) Total Male +
Female (%)
Skin colour
Fair 17 (23.28) 14 (26.92) 31(24.8)
Wheatish 39 (53.42) 31 (59.61) 70 (56.0)
Brownish 3 (4.10) 0 (0.00) 3 (2.4)
Blackish 14 (19.1) 7 (13.46) 21 (16.8)
Hearing and visual impairment
There was no hearing and visual impairement (Table-9 and Figure-10). Due to proper diet,
medication and regular blood transfusion, these complications are not seen in all thalassemia
patients.
Psychological impaired
The psychological study of all thalassemia patients showed in (Table-9 and Figure-10). In
the present observations all male patients were normal (100%), in female only one was
psychological impaired. In India Atika et al. (2006) observed the psychosocial problems in
thalassemic childrens and their families. It is evident from the findings of our study that
besides the clinical burden, thalassemic have to shoulder very low psychosocial burden
associated with the disease. There was no any correlation between the psychological burden
and the sex.
Table-9. Showing hearing, visual and psychological complications in thalassemia patients.
Sex Parameter Male (%) Female (%) Total Male +
Female (%)
Hearing Normal 73 (100.0) 52 (100.0) 125 (100.0)
Ophthalmological Normal 73 (100.0) 52 (100.0) 125 (100.0)
Psychology
Normal 73 (100.0) 51 (98.7) 124 (99.2)
Abnormal 00 (0) 01(1.92) 1 (0.8)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
76
Consanguineous marriage:
Consanguineous means having similar blood. A marriage between close relatives is referred
to as a consanguineous marriage. The cases of consanguineous marriage (Table-11 and
Figure-11) in thalassemia patients were: male parents 33(45.20%), female parents
30(57.69%) total 63(50.4%); Non consanguineous marriage were observed in male parents
40(54.79%), female parents 22(42.30%) total 62(49.6%). The observations showed the
consanguinity rate was very high (>49%) in both male and female. The results indicate the
need for implementing a comprehensive genetic preventive program for the eradication of
thalassemia in Solapur District. Neeraj et. al. (2010), he observed the consanguinity
marriages of thalassemic patients in Muslim and Sindhi religion. The observations showed the
consanguinity rate was very high (>49%) in male and female. The results indicate the need for
implementing a comprehensive genetic preventive program for the eradication of thalassemia in
Solapur District.
Table 11. Showing prevalence percentage of the consangunous marriages in the parents of
the thalassemic patient.
Sex Male (%) Female (%) Total Male + Female (%)
Consanguinity
Yes 33 (45.20) 30 (57.69) 63 (50.4)
No 40 (54.79) 22 (42.30) 62 (49.6)
Ethnicity
Religion wise percentage of thalassemia (Table-12 and Figure-12). It was very high in
Hindu and muslin as compared to Jain and Sindhi community.
Table-12. Showing the percentage of ethnicity in thalassemic patients.
Ethnicity Male (%) Female (%) Total Male + Female (%)
Hindu 59 (80.82) 42 (80.76) 101 (80.8)
Jain 1 (1.36) 00 (0.00) 1 (0.8)
Muslim 12 (16.43) 10 (19.23) 22 (17.6)
Sindhi 1 (1.36) 00 (0) 1 (0.8)
Diet
There was no any correlation between the diet and sex (Table-13 and Figure-13).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
77
Table-13.. Showing prevalence percentage of thalassemic patients’ diet.
Sex Diet Male (%) Female (%) Total Male + Female (%)
Diet
Vegetarian 23 (31.50) 20 (38.46) 43 (34.4)
Non vegetarian 50 (68.49) 32 (61.53) 82 (65.6)
Orofacial complications
The prevalence of orofacial complications (Table-14) in Thalassemia patients was: rodent
face (Figure-14) male (73.97%), female (75.00%) total (74.4%); saddle nose (Figure-14a)
male (79.45%), female (90.38%) total (84.00%); maxillary protrusion (Figure-14b) male
(79.45%), female (82.69%) total (80.8%); Upper anterior teeth spacing (Figure-14c) male
(52.05%), female (53.84%) total (52.8%); Anterior open bite (Figure-14d) male (69.86%),
female (78.84%) total (73.6%); deep bite (Figure-14e) male (90.41%), female (1.92%) total
(53.6%); Mucosal discoloration (Figure-14f) male (0.00%), female (1.92%) total (0.8%);
respectively. In this study, Upper anterior teeth spacing and deep bite was observed, more
than the normal population especially in older patients, which is due to rotation of mandible
and protrusion of maxilla leading to over growth of upper anterior teeth of maxilla.
The anterior open bite was slightly more than normal population. Regular and repeated
blood-infusion keeping the hemoglobin in an appropriate level (at least 10g/dl), along with
iron removal can prevent face and skull deformities. There was not any relationship between
the complications and sex. Skull and face deformities can be closely related to the patient's
age. Most of the patients were in the first and second decade of life. Early diagnosis and
blood transfusion caused less prevalence of rodent face. The orofacial complications in
patients with thalassemia major were similar to findings of other studies (Drew and Sach,
1997; Agha and Shabandy, 2000). The results of orofacial complications in thalassemic
patients showed that the rate of rodent face, maxillary protrusion, Anterior open bite, and
saddle nose increased with age. This was quite predictable because the maxilla is one of the
most common bones affected by thalassemia (Kliegman and Behromon, 2002). The
evaluation of oro-maxillofacial changes in major thalassemia observations were similar to
results reported by Salehi (2007) and Ashraf et al., (2008). Overall, it indicated a reduction in
complications during last decades, which was due to early diagnosis, treatment, and regular
follows up. The orofacial complications, the data was corroborated with the reports of of
Kremer (1986).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
78
Table-14. Showing the sex wise prevalence of orofacial complications in thalassemic
patients.
Parameter Sex Yes
SCT
No
SCT
Yes
BTI
No
BTI
Yes
BTMi
No
BTMi
Yes
TM
No
TM
Yes
(%)
No
(%)
Rodent
face
M 0 1 9 3 5 1 40 14 54
(73.97)
19
(26.02)
F 0 0 3 1 4 0 32 12 39 (75)
13 (25)
T 0 1 12 4 9 1 72 26 93 (74.4)
32 (25.6)
Saddle nose
M 0 1 11 1 6 0 41 13 58 (79.45)
15 (20.54)
F 0 0 3 1 3 1 41 3 47 (90.38)
5 (9.61)
T 0 1 14 2 9 1 82 16 105 (84)
20 (16)
Maxillary protrusion
M 0 1 11 1 6 0 41 13 58 (79.45)
15 (20.54)
F 0 0 4 0 3 1 36 8 43 (82.69)
9 (17.30)
T 0 1 15 1 9 1 77 21 101
(80.8)
24
(19.2)
Maxillary
anterior
teeth
spacing
M 0 1 5 7 3 3 30 24 38
(52.05)
35
(47.94)
F 0 0 4 0 2 2 22 22 28
(53.84)
24
(32.87)
T 0 1 9 7 5 5 52 46 66
(52.8)
59
(47.2)
Anterior
open bite
M 0 1 10 2 6 0 35 19 51
(69.86)
22
(30.13)
F 0 0 4 0 2 2 35 9 41
(78.84)
11
(21.15)
T 0 1 14 2 8 2 70 28 92
(73.6)
33
(26.4)
Deep bite
M 0 1 1 11 0 6 6 48 66 (90.41)
7 (9.58)
F 0 0 0 4 0 4 1 43 1 (1.92)
51 (98.07)
T 0 1 1 15 0 10 7 91 67 (53.6)
58 (46.6)
Mucosal
discolorati
-on
M 0 1 0 12 0 6 0 54 0
(0)
73
(100)
F 0 0 0 4 0 4 1 43 1
(1.92)
51
(98.07)
T 0 1 0 16 0 10 1 97 1
(0.8)
124
(99.2)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
79
Hematological Parameters
Hematological parameters: WBC count, RBC count, Hb, HCT, MCV, MCH, HCHC and
platelets count were measured using Sysmex cell counter (Wild and Bain, 2001).
RBC morphology
In present survey it was observed that morphology of RBC were abnormal in all 125
thalassemic patients. The morphology of RBC was showed in Figure-15. The following
types of the RBC morphology were observed:
1) Hypochromasia: Red blood cell with a decreased concentration of hemoglobin
2) Macrocytosis: Larger than normal red blood cell
3) Microcytosis: Decrease in the red cell size. Red cells are smaller than ± 7µm in diameter.
4) Anisocytosis: RBC are of unequal size.
5) Poikilocytosis:
a) Target cells: Red cells have an area of increased staining which appears in the area of
central pallor.
b) Ovalocytes: oval shape red blood cell
c) Tear drop cells: Red cells are shaped like a tear drop or pear.
d) Acanthocytosis: RBCs with irregularly spaced projections, these projections very in
width but usually bear a rounded end. These types of cells were observed in splenectomized
thalassemic patients.
e) Sickle Cells: Sickle shaped red cells. Only one male patient was observed sickle cell beta
thalassemia (Hb-S disease).
6) Elliptocytosis: RBCs are oval or elliptical in shape. Long axis is twice the short axis.
7) Envelope form cell: Some of RBCs are overlapped.
8) Basophilic stippling: Large numbers of small basophilic inclusions in RBCs.
WBC, RBC, Hb, HCT, MCV, MCH, MCHC, platelets and Alloimmunization
The normal reference value was showed in Table-15. Hematological parameters were
observed by using cell counter (Sysmex KX21), the report showed in the Table-15.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
80
Table-15. Showing the normal reference value of WBC, RBC, Hb, HCT, MCV, MCH,
HCHC and Platelets.
Parameters Age Normal range male Normal range female
WBC 1 Year
2-18 Years
6-18x103/µl
3.5-11x103/µl
6-18x103/µl
3.5-11x103/µl
RBC 6-11 months
1-11 Years
12-18 Years
3.9-5.5 x106/µl
3.8-4.8 x106/µl
4.1-5.2 x106/µl
3.9-5.5 x106/µl
3.8-4.8 x106/µl
4.1-5.0 x106/µl
Hb 6 months-8 Years
9-11 Years
12-18 Years
11.2-14.1g/dl
12-15g/dl
11.7g/dl
12.2-14.1g/dl
12-15g/dl
11.5-15.3g/dl
HCT 6 months to 18 Years 45-62% 37-48%
MCV 6 months-8 Years
9-11 Years
12-18 Years
68-85 fl
75-87 fl
77-95 fl
68-85 fl
75-87 fl
77-95 fl
MCH
6 months-8 Years
9-11 Years
12-18 Years
24-30 pg
26-32 pg
27-34 pg
24-30 pg
26-34 pg
27-34 pg
MCHC
6 months- 11Years
12-18 Years
32-37 g/dl
32-37 g/dl
32-37 g/dl
32-36 g/dl
Platelets 6 months to 18 Years 1.5-4.5x103/µl 1.5-4.5x10
3/µl

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
81
Table-15. Showing the hematological parameters in the thalassemic patients.
Patient’s
Code
WBC X
103 /
µl
RBC
X106 /
µl
HGB X
g/ dl
HCT
% MCV fl
MCH
pg
MCHC
g/dl
Platelet
X103 /µl
Alloimmu
-nization
1 15.76 3.88 10.06 29.2 75.63 26.16 34.56 551.66 Neg
2 6.76 3.07 7.7 22.83 74.5 25.2 33.83 416.33 Neg
3 6.76 2.61 6.16 18.8 72 23.63 32.86 95.33 Neg
4 7.5 3.36 8.26 24.4 73 24.73 33.83 322 Neg
5 14.36 3.97 10.83 31.23 78.63 27.26 34.66 580 Neg
6 6.93 3.62 6.16 26.56 73.43 24.96 34 263.33 Neg
7 6.26 2.89 7.46 21.2 77.53 26.1 33.63 278.33 Neg
8 9.1 3.91 10.06 29.86 76.16 25.66 33.63 294.33 Neg
9 5.93 2.89 7.06 21.26 75.13 25.16 33.4 343.33 Neg
10 15.9 3.03 7.53 22.8 74.86 24.7 32.9 652 Neg
11 5.2 2.42 5.9 18.1 74.7 24.6 32.9 147.66 Neg
12 4.56 2.59 6.4 19.56 75.9 25 32.86 284 Neg
13 9.63 3.11 7.66 22.56 72.43 24.6 33.96 390.66 Neg
14 17.2 2.5 6.46 19.6 78.53 25.96 33.1 478 Neg
15 12.1 2.69 7.46 21.43 79.46 27.7 34.9 485.66 Neg
16 6.2 2.58 6.66 20 77.56 25.83 33.3 262.66 Neg
17 10.7 3.19 8.63 25.76 80.63 26.93 33.43 385.66 Neg
18 17.8 3.65 10.1 29.4 79.96 27.43 34.36 477 Neg
19 5.8 2.92 6.7 22.96 73.13 23.16 31.7 185.33 Neg
20 9.9 3.73 8.73 26.96 72.3 23.36 32.4 240 Neg
21 11.1 2.79 8.83 22.96 81.9 31.1 37.9 472.66 Neg
22 6.66 3.15 7.3 22.9 72.4 23.03 31.8 386.66 Neg
23 14.7 2.7 7.1 20.46 75.76 26.36 35.13 377.33 Neg
24 7.96 2.96 7.66 22.73 76.33 18.43 33.73 309.66 Neg
25 13.1 3.3 8.56 25 75.66 25.93 34.26 259.66 Neg
26 10.2 2.77 7.6 21.86 78.73 27.36 34.73 164 Neg
27 5.63 2.87 7.26 21.7 77.36 25.86 33.46 293.66 Neg
28 10 3.83 9.93 29.26 76.53 25.96 33.93 341 Neg
29 7.76 3.51 8.3 25.7 72.56 23.36 29.53 286.66 Neg
30 6.93 3.65 9.5 27.5 75.2 25.96 34.56 345 Neg
31 8.76 3.2 8.43 25.46 79.63 26.36 33.1 371.66 Neg

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
82
Table-15. Continued..
Patient’s
Code
WBC X
103 /
µl
RBC
X106 /
µl
HGB X
g/ dl
HCT
% MCV fl
MCH
pg
MCHC
g/dl
Platelet
X103 /µl
Alloimmu
-nization
32 6.3 3.8 7.33 24.23 63.7 19.26 30.23 344.66 Neg
33 10.26 3.38 8.66 25.9 77.86 26.1 33.5 169.66 Neg
34 6.76 2.6 6.6 19.83 76.03 25.23 33.45 167.33 Neg
35 6.26 3.62 9.53 28.5 78.5 26.2 33.4 128.33 Positive
36 7.46 2.98 8.16 23.76 79.43 27.26 34.33 276 Neg
37 10.6 3.21 8.86 27.86 80.8 27.63 34.2 249 Neg
38 5.63 2.87 7.26 21.7 77.46 25.86 33.46 293.66 Neg
39 13.96 3.6 9.43 28.7 79.56 26.13 32.86 283.66 Neg
40 8.2 3.09 8.03 24.06 77.93 26.06 33.46 300 Neg
41 6.93 3.84 9.83 29.5 76.8 25.6 33.3 270 Neg
42 9.4 3.54 8.1 25.3 71.23 22.76 28.6 267.66 Neg
43 8.3 3.47 8.23 25.23 72.63 23.73 32.63 322.66 Neg
44 4.43 3.46 7.9 24.8 71.56 22.8 31.8 339.66 Neg
45 41.4 3.06 7.63 23.66 77.3 24.93 32.23 624 Neg
46 6.16 3.28 8.53 25.73 78.63 26.1 33.1 324.66 Neg
47 6.2 2.49 6.2 18.33 78.66 26.7 33.9 270.66 Neg
48 10.06 3.31 8.73 25.83 77.9 26.2 33.66 269 Neg
49 8.5 2.66 7.26 21.03 78.8 27.23 34.56 298.66 Neg
50 8.56 3.02 8.06 23.93 79.26 26.7 33.66 373.33 Neg
51 7.26 2.83 8.13 22.9 80.73 28.5 35.2 309.33 Neg
52 6.33 2.84 6.96 21.3 74.7 24.43 32.66 170 Neg
53 5.43 2.56 6.8 20.16 78.76 26.6 33.76 307.66 Neg
54 6.36 3.48 9.43 26.73 76.83 27.16 35.3 289 Neg
55 8.86 3.13 8.4 26.2 81.33 26.83 33 236 Neg
56 7.23 2.85 7.16 21.73 76.2 25.13 33.03 246.33 Neg
57 7.7 3.98 11.23 33.63 83.73 28.06 33.53 131.33 Neg
58 8 3.25 8.23 23.9 73.5 25.3 34.3 388.33 Neg
59 8.46 4.17 10.33 30.6 73.36 24.76 33.76 207.66 Neg
60 6.43 2.81 7.7 22.56 80.13 27.36 34.13 407.66 Neg
61 5.3 2.64 6.76 20.23 76.13 25.36 33.26 193.66 Neg
62 5.7 3.35 9.03 25.3 75.6 25.3 35.76 271 Neg
63 14.26 3.69 9.56 29 78.73 25.93 32.96 490 Positive
64 23.9 3.49 9.13 28.03 80.36 26.2 32.6 530.33 Neg
65 13.46 3.22 8.43 25.56 79.26 26.13 33.03 1014 Neg

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
83
Table-15. Continued..
Patient’s
Code
WBC X
103 /
µl
RBC
X106 /
µl
HGB X
g/ dl
HCT
% MCV fl
MCH
pg
MCHC
g/dl
Platelet
X103 /µl
Alloimmu
-nization
66 11.03 2.77 7.43 21.83 78.7 26.83 34.06 445.66 Neg
67 4.63 3.68 9.26 28.23 76.73 25.16 32.83 267.33 Neg
68 7.5 3.18 8.16 24.2 76.36 25.8 33.76 305.33 Neg
69 8.3 3.1 8.6 26.4 85 27.73 32.56 423.16 Neg
70 4.56 2.6 7.53 22.66 86.93 28.83 33.13 301.66 Neg
71 7.73 2.78 6.86 21.16 76.36 24.7 32.3 244 Neg
72 6.1 2.91 7.16 21.7 74.33 24.7 33.16 259.66 Neg
73 10.3 3.24 8.03 24.7 75.03 24.36 32.43 396.66 Neg
74 7.1 3.34 8.46 25.16 75.43 25.43 33.66 284 Neg
75 24.56 2.26 6.7 19.3 85.36 29.7 34.86 510.33 Neg
76 5.83 3.27 9.1 27.26 83.1 27.8 33.46 207.66 Neg
77 8.3 2.84 6.9 20.46 72.4 24.53 34.6 537.66 Neg
78 5.56 2.86 6.66 19.4 72.5 23.43 32.33 161 Neg
79 8.76 2.99 7.53 22.93 77.16 25.43 32.9 269.33 Neg
80 4.83 2.33 6.3 18.53 79.3 26.93 33.9 280 Neg
81 7.33 2.97 7.63 23.26 78.6 25.8 32.83 417.33 Neg
82 6.5 2.8 7.23 21.76 77.8 25.86 38.23 187.66 Neg
83 2.46 4.15 10.96 31.53 76.6 26.36 34.7 157.33 Neg
84 6.56 2.92 6.7 21.3 73.6 19.4 31.56 358 Neg
85 7.76 2.11 4.8 15.23 72 7.4 21.5 137.66 Neg
86 7.7 3.34 8.3 25.06 75.03 24.9 33.1 443.33 Neg
87 7.76 3.35 7.2 23.43 69.63 21.53 30.7 374.33 Neg
88 4.66 2.33 6.13 18.8 80.2 26.06 32.5 234.33 Neg
89 14.06 2.93 7.93 24 81.33 26.86 33.1 208.66 Neg
90 15.4 2.95 8.1 24.5 82.4 26.5 32.6 702 Neg
91 4.46 2.3 6.73 20.8 91 29.33 32.26 233.66 Neg
92 5.76 2.39 6 18.33 76.96 25.2 32.7 174.33 Neg
93 6.16 2.08 5.7 16.83 80.73 27.26 33.8 94 Neg
94 5.76 2.7 6.8 20.3 75.76 25.1 33.13 250.33 Neg
95 5.26 3.35 6.13 18.36 70.86 23.53 33.13 194 Neg
96 7.36 3.38 8.66 24.86 73.66 25.63 34.66 261 Neg
97 6.8 2.85 7.93 23.13 80.86 27.73 34.33 237 Neg
98 5.2 3.45 7.5 23.66 68.4 21.66 31.7 342.33 Neg

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
84
Table-15. Continued..
Patient’s
Code
WBC X
103 /
µl
RBC
X106 /
µl
HGB X
g/ dl
HCT
% MCV fl
MCH
pg
MCHC
g/dl
Platelet
X103 /µl
Alloimmu
-nization
99 18.43 3.2 8.13 25.46 79.63 25.43 30.8 1027 Neg
100 6.3 2.36 6.33 19.36 81.9 26.76 32.73 151.66 Neg
101 7.7 3.5 9.03 27.03 76.06 25.5 33.43 382 Neg
102 5.36 2.71 7.16 20.5 75.73 26.5 34.9 186 Neg
103 26.3 2.46 7.06 20.8 84.56 28.73 33.96 471.33 Neg
104 4.83 2.8 7.26 21.7 78.33 26.2 33.5 329.33 Neg
105 25.6 2.67 6.3 20.66 77.4 23.5 30.33 686.66 Neg
106 15.9 2.79 7.53 23.3 82.93 26.9 32.36 898 Neg
107 9.73 4.06 9.06 28.4 68.33 22.33 32.73 126.33 Neg
108 4.16 2.01 5.33 16.5 82.06 26.56 32.33 177.33 Neg
109 29.96 2.59 7.13 21.9 84.7 27.63 32.6 332 Neg
110 4.8 2.62 6.9 21.5 82.16 26.36 32.06 255.33 Neg
111 7.1 2.92 7.5 22.5 77.46 26.6 33.6 321.33 Neg
112 24.8 2.36 7 19.96 84.6 29.66 35.06 489.66 Neg
113 5.5 2.89 7.23 22.1 76.76 25.13 32.73 129 Neg
114 5.5 2.45 5.76 17.73 72.4 23.56 32.5 274 Neg
115 5.53 2.13 5.53 16.63 78.1 25.9 33.16 201.66 Neg
116 21.83 3.21 8.4 26.1 81.5 26.23 32.2 748 Neg
117 7.5 3.01 7.36 22.3 74.1 24.43 32.96 271.66 Neg
118 5.4 3.09 8.16 22.8 74.16 26.73 35.86 199.33 Neg
119 27.4 2.69 7.1 21.93 81.83 26.5 32.33 868 Neg
120 4.03 2.31 5.73 11.03 77.93 24.73 31.73 201.66 Neg
121 23.66 2.44 6.7 20.53 84.36 27.56 32.66 692.66 Neg
122 4.6 2.77 6.66 20.8 78.2 25.06 32.6 220 Neg
123 17.4 3.13 8 24.56 78.46 25.53 32.56 549.33 Neg
124 3.06 1.86 4.8 14.76 79.33 25.8 32.5 105.33 Neg
125 12.1 3.43 9.16 18.46 78.06 26.66 34.23 862.66 Neg

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
85
WBC Count
The WBC counts of thalassemic patients were showed in the Table-16 and Figure-16 . The
low WBC count was not found in any patients. The normal WBC was 80.80% in male and
female, high WBC count was 19.20% in male and female patients.
Table-16. Showing the prevalence percentage of WBC count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
WBC count (%)
Normal (%) High (%) Low (%)
SCT
M (1) 1(100.00) 00(00.00) 00(00.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total(1) 1(100.00) 00(00.00) 00(00.00)
BTI
M (12) 12 (100.00) 00(00.00) 00(00.00)
F (4) 2(50.00) 2(50.00) 00(00.00)
Total (16) 14(87.50) 2 (12.50) 00(00.00)
BTMi
M (6) 5(83.30) 1(16.60) 00(00.00)
F (4) 4(100.00) 00(0.00) 00(00.00)
Total (10) 9(90.00) 1(10.00) 00(00.00)
TM
M (54) 39(72.22) 15(27.77) 00(00.00)
F (44) 38(86.36) 6(13.63) 00(00.00)
Total (98) 77(78.57) 21(21.42) 00(00.00)
Total patients %
M (73) 57(78.08) 16(21.91) 00(00.00)
F (52) 44(84.61) 08(15.38) 00(00.00)
Total M+F (125) 101(80.80) 24(19.20) 00(00.00)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
86
RBC Count
The RBC count was showed in Table-17 and Figure-17. In all 125 thalassemia patients,
normal RBC count was: male (6.84%), female (1.92%) avarage (4.80%); high RBC count
was not fount in either sex; low RBC count was male (93.15%), female (98.06%) total
(95.2%). Red cells carry oxygen to the tissues, when RBCs are low, the body does not get
enough oxygen and a person may feel tired or short of breath, heart beat faster than normal.
In all majority thalassemia patient’s skin color may be pale due to very low range of red
blood cells. The results shows that the absent beta globin chain synthesis, resulting in reduced
Hb in red blood cells (RBC), decrease RBC production leading to anemia.
Table-17. Showing the RBC count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
RBC (%)
Normal High Low
SCT
M (1) 00(00.00) 00(00.00) 01 (100.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total (1) 00(00.00) 00(00.00) 01(100.00)
BTI
M (12) 03(25.00) 00(00.00) 09 (75.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (16) 03(18.75) 00(00.00) 13(81.25)
BTMi
M (6) 00(00.00) 00(00.00) 06(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 00(00.00) 10(100.00)
TM
M (54) 02(3.84) 00(00.00) 52(96.29)
F (44) 01(2.27) 00(00.00) 43(97.72)
Total (98) 03(3.06) 00(00.00) 95(96.93)
Total patients %
M (73) 05 (6.84) 00(00.00) 68(93.15)
F (52) 01(1.92) 00(00.00) 51(98.06)
Total M+F (125) 06(4.80) 00(00.00) 119(95.2)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
87
Hemoglobin level
The Hb level was shown in Table-18 and Figure-18. In all type of thalassemic patients Hb
level was very low. Not a single patient reported normal or high Hb.
Table-18. Showing the prevalence percentage of Hb in thalassemic patients.
Types of
Thalassemia
Sex
(Total patients)
Hb (%)
Normal High Low
SCT
M (1) 00(00.00) 00(00.00) 1(100.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total 00(00.00) 00(00.00) 01(100.00)
BTI
M (12) 00(00.00) 00(00.00) 12(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (16) 00(00.00) 00(00.00) 16(100.00)
BTMi
M (6) 00(00.00) 00(00.00) 06(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 00(00.00) 10(100.00)
TM
M (54) 00(00.00) 00(00.00) 54(100.00)
F (44) 00(00.00) 00(00.00) 44(100.00)
Total (98) 00(00.00) 00(00.00) 98(100.00)
Total patients
M (73) 00(00.00) 00(00.00) 73(100.00)
F (52) 00(00.00) 00(00.00) 52(100.00)
Total M+F (125) 00(00.00) 00(00.00) 125(100.00)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
88
HCT (Hematocrit or Pack cell volume)
The HCT level was shown in Table-19 and Figure-19. In all type of thalassemic patients
HCT count was very low. Not a single patient was with normal or with high HCT.
Table-19. Showing the prevalence percentage of HCT count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
HCT (%)
Normal High Low
SCT
M (1) 00(00.00) 00(00.00) 1(100.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total 00(00.00) 00(00.00) 01(100.00)
BTI
M (12) 00(00.00) 00(00.00) 12(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (16) 00(00.00) 00(00.00) 16(100.00)
BTMi
M (6) 00(00.00) 00(00.00) 06(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 00(00.00) 10(100.00)
TM
M (54) 00(00.00) 00(00.00) 54(100.00)
F (44) 00(00.00) 00(00.00) 44(100.00)
Total (98) 00(00.00) 00(00.00) 98(100.00)
Total patients
M (73) 00(00.00) 00(00.00) 73(100.00)
F (52) 00(00.00) 00(00.00) 52(100.00)
Total M+F (125) 00(00.00) 00(00.00) 125(100.00)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
89
MCV (Mean Corpuscular Volume)
The MCV count was shown in Table-20 and Figure-20. In all types of thalassemic patients
MCV count was very low inn male (98.63%); female (100.00%). Only one BTMi male
patient was observed with high MCV. None of the patients showed MCV in normal range.
Table-20. Showing prevalence percentage of MCV count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
MCV count (%)
Normal High Low
SCT
M (1) 00(00.00) 00(00.00) 1(100.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total 00(00.00) 00(00.00) 01(100.00)
BTI
M (12) 00(00.00) 00(00.00) 12(100.00)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (16) 00(00.00) 00(00.00) 16(100.00)
BTMi
M (6) 00(00.00) 01(16.60) 05(83.33)
F (4) 00(00.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 01(10.00) 09(90.00)
TM
M (54) 00(00.00) 00(00.00) 54(100.00)
F (44) 00(00.00) 00(00.00) 44(100.00)
Total (98) 00(00.00) 00(00.00) 98(100.00)
Total patients
M (73) 00(00.00) 01(1.38) 72(98.63)
F (52) 00(00.00) 00(00.00) 52(100.00)
Total M+F (125) 00(00.00) 01(0.80) 124(99.20)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
90
MCH (Mean cell hemoglobin)
The MCH was shown in Table-21 and Figure-21. In total the MCH count was normal in
majority patients. In nineteen patients MCH was observed below normal.
Table-21. Showing the percentage MCH count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
MCH (%)
Normal High Low
SCT
M (1) 01(100.00) 00(00.00) 00(00.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total 01(100.00) 00(00.00) 00(00.00)
BTI
M (12) 09(75.00) 00(00.00) 03(25.00)
F (4) 04(100.00) 00(00.00) 00(00.00)
Total (16) 13(81.25) 00(00.00) 03(18.75)
BTMi
M (6) 06(100.00) 00(00.00) 00(00.00)
F (4) 04(100.00) 00(00.00) 00(00.00)
Total (10) 10(100.00) 00(00.00) 00(00.00)
TM
M (54) 45(83.33) 01(1.85) 08(14.81)
F (44) 36(81.81) 00(00.00) 08(18.18)
Total (98) 81(82.65) 01(1.02) 16(16.32)
Total patients
M (73) 61(83.56) 01(1.36) 11(15.06)
F (52) 44(84.61) 00(00.00) 08(15.38)
Total M+F (125) 105(84.00) 01(0.80) 19(7.20)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
91
MCHC count
The MCHC was shown in Table-22 and Figure-22. In total 125 thalassemia patients MCHC
normal was: male (75.34%), female (73.07%) avarage (74.40%); high MCHC count: male
(17.80%), female (1.92%) total (19.20%); low MCHC count was male (6.84%), female
(5.76%) total (15.38%).
Table-22. Showing the MCHC count in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
MCHC (%)
Normal High Low
SCT
M (1) 1(100.00) 00(00.00) 00(00.00)
F (0) 00 (00.00) 00(00.00) 00(00.00)
Total 01(100.00) 00(00.00) 00(00.00)
BTI
M (12) 11(91.66) 00(00.00) 01(8.33)
F (4) 04(100.00) 00(00.00) 00(00.00)
Total (16) 15(93.75) 00(00.00) 01(6.25)
BTMi
M (6) 06(100.00) 00(00.00) 00(00.00)
F (4) 04(100.00) 00(00.00) 00(00.00)
Total (10) 10(100.00) 00(00.00) 00(00.00)
TM
M (54) 49(90.75) 00(00.00) 05(9.25)
F (44) 37(84.09) 00(00.00) 07(15.90)
Total (98) 86(87.75) 00(00.00) 12(12.24)
Total patients
M (73) 67(91.78) 00(00.00) 6(8.21)
F (52) 45(86.53) 00(00.00) 07(13.46)
Total M+F (125) 112(89.0) 00(00.00) 13(10.04)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
92
Platelets Count
The Platelet count was shown in Table-23 and Figure-23. In total 125 thalassemia patients
Platelets normal count was: male (75.34%), female (73.07%) total (74.40%); high Platelets
count: male (17.80%), female (1.92%) total (19.20%); low Platelets count was male (6.84%),
female (5.76%) total (15.38%). Overall the normal range platelet count is more than that of
the high range observed in twenty four patients and below range were eight in thalassemia
patients. The data corroborated with the results of Shivashankara et. al., (2008).
Table-23. Showing the prevalence percentage of platelet count in thalassemic patients.
Types of
Thalassemia
Sex
(Total patients)
Platelet count (%)
Normal High Low
SCT
M (1) 01(100.00) 00(00.00) 00(00.00)
F (0) 00(00.00) 00(00.00) 00(00.00)
Total 01(100.00) 00(00.00) 00(00.00)
BTI
M (12) 11(91.66) 00(00.00) 01(8.33)
F (4) 02(50.00) 02(50.00) 00(00.00)
Total (16) 13(81.25) 02(12.50) 01(6.20)
BTMi
M (6) 06(100.00) 00(00.00) 00(00.00)
F (4) 03(75.00) 00(00.00) 01(25.00)
Total (10) 09(90.00) 00(00.00) 01(10.00)
TM
M (54) 37(5.55) 13(24.07) 04(7.40)
F (44) 33(75.00) 09(20.45) 02(4.54)
Total (98) 70(71.42) 22(22.44) 06(6.12)
Total patients
M (73) 55(75.34) 13(17.80) 05(6.84)
F (52) 38(73.07) 11(1.92) 03(5.76)
Total M+F (125) 93(74.40) 24(19.20) 08(15.38)
Serum Ferritin Level:
The survey reports observed that the Serum ferritn levels are increased in all thalassemic
patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
93
Blood Transfusion in thalassemic patients
Age of first blood transfusion
After diagnosis of thalassemia, blood transfusion was given to all patients. The survey reports
observed that the age of first blood transfusion varies.
Amount of blood transfusion
In thalassemic patients the blood was given on the basis of the patient’s age, weight and the
depending on the Hb percentage. Normally 200 ml blood was transfused at the time.
Frequency of blood transfusion
In thalassemic patients the frequency of blood transfusion were varies and depends upon the
Hb percentage. In some patient’s transfusion was given after two weeks and in some it was
given after three weeks or a month.
Pre and post blood transfusion Hb level.
The pre and post transfusion Hb level was shown Table-24 and Figure-24 a and 24b. Before
blood transfusion, low Hb level were observed in both patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
94
Table-24. Showing the mean percentage of pre and post Hb and HCT count in thalassemia
patients.
Patient
Code
Patient
Initials Sex Diagnosis Pre Hb Post Hb Pre HCT Post HCT
1 BMH F TM 7.17 7.85 21.51 23.55
2 MAD M TM 6.33 7.75 18.99 23.25
3 MPA F TM 7.3 8.7 22.05 26.1
4 KPR F TM 6.98 8.15 20.94 24.45
5 JSS F TM 7.45 8.7 22.35 26.1
6 JP F TM 7.65 8.9 22.95 26.7
7 GDD F TM 7.2 8.4 21.6 25.2
8 DSS M BTI 6.79 7.9 20.37 23.7
9 KLB F TM 8.25 9.45 24.75 28.35
10 SGS M TM 7.17 8.95 21.51 26.85
11 MTM F TM 6.96 9.57 18.78 28.71
12 PST M TM 6.9 8.2 20.7 24.6
13 SSS M TM 8.05 9.3 24.15 27.9
14 KSS M TM 7.35 8.55 22.05 25.65
15 NA* F TM 7.3 8.5 21.9 25.5
16 MAR F TM 8.35 10.85 25.05 32.55
17 STS F TM 7.4 8.8 22.2 26.4
18 SSS M TM 5.67 6.87 17.02 20.62
19 CRR M TM 8.75 9.85 26.25 29.55
20 KSS M TM 6.5 8 19.5 24
21 GSA M TM 8.7 9.95 26.1 29.85
22 BSR F TM 7.5 8.75 22.5 26.5
23 CNT M BTMi 7.4 8.7 22.2 26.1
24 BKG F TM 6.8 8.6 20.4 25.8
25 SOS1 M TM 9.3 10.35 27.9 31.05
26 SOS2 M TM 8.5 9.75 25.5 29.25
27 SSS M TM 9.15 10.3 27.45 30.9
28 BLM M BTI 7.75 8.9 23.25 26.7
29 JPA F TM 8.35 9.6 25.05 28.8
30 TRM M TM 9.1 10.25 27.3 30.75
31 PYR M BTI 8.25 9.55 24.75 28.65
32 RGS* M BTI 8.5 9.65 25.5 28.95
33 MPP* F TM 8.3 9.5 24.9 28.5
34 GPO* M TM 8.15 9.25 24.45 27.75
35 TRI M TM 8.7 9.8 26.1 29.4

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
95
Table-24. Continued..
Patient
Code
Patient
Initials Sex Diagnosis Pre Hb Post Hb Pre HCT Post HCT
36 KNS M TM 8.7 8.95 26.1 26.85
37 VDS M TM 8.9 9.9 26.7 29.7
38 PSB F BTMi 9.75 9.75 29.5 29.1
39 RSB M TM 9.01 10.3 27.03 30.9
40 IVY F TM 8.7 8.95 20.4 23.7
41 ARM M BTI 9.2 10.35 27.6 31.05
42 GAR M TM 9.55 10.75 28.65 32.25
43 KSM M TM 9 10.2 27 30.6
44 KAV F TM 9.2 10.3 2706 30.9
45 PUA F TM 8.5 9.6 25.5 28.8
46 DRS M TM 8.06 9.25 24.15 27.75
47 BMN M TM 7.25 8.4 21.75 25.2
48 LAB M TM 8.8 10.1 26.4 30.3
49 VDS M TM 8.9 9.2 26.7 27.6
50 SVP M BTMi 8.75 9.95 26.25 29.85
51 KAN F TM 8 9.25 24 27.75
52 SSS F TM 8.35 9.55 25.05 28.65
53 BUT M TM 7.4 8.15 22.2 24.45
54 MA M BTMi 7.9 9.3 23.7 27.9
55 RSS M BTMi 9.85 11 29.55 33
56 BNB M TM 7.7 8.85 23.1 26.55
57 IAS M TM 8.23 10.35 24.69 31.05
58 ISY M TM 7.85 9 23.55 27
59 TAS M BTI 9.45 10.7 28.35 32.1
60 PAM F TM 8.5 9.75 25.5 29.25
61 QSA M BTI 8.2 9.45 24.6 28.35
62 BSR M TM 6.75 8 20.25 24
63 RST F TM 7.1 8.4 21.3 25.2
64 QAS* F TM 9.7 10.8 29.1 32.4
65 GAM M TM 7.45 8.6 22.35 25.8
66 PHM M TM 8.85 10 26.55 30
67 GPS F TM 9.1 10.25 27.3 30.75
68 SV M TM 8.45 9.6 25.35 28.8
69 NDN F TM 8.6 9.75 25.8 29.25
70 MLD M TM 8.45 9.65 25.35 28.95

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
96
Table-24. Continued..
Patient
Code
Patient
Initials Sex Diagnosis Pre Hb Post Hb Pre HCT Post HCT
71 PPV F TM 8.9 101 26.7 30.3
72 MVM M TM 8.95 10.2 26.85 30.6
73 KAS* M TM 8.85 10.05 26.55 30.15
74 CYS M SCT 7.65 8.9 22.95 26.7
75 LS M TM 6.85 8 20.55 24
76 GSS F TM 8.55 9.75 25.55 29.55
77 CGR* M TM 5.72 6.45 17.16 19.35
78 RS* M TM 5.2 6.45 15.6 19.3
79 JSS F TM 8.4 9.45 30 28.35
80 TNJ F TM 6.9 8 20.7 24
81 MPT F TM 8.15 9.3 24.45 27.9
82 BHH M TM 7.3 8.5 21.9 25.5
83 BSM M TM 9.5 10.8 28.5 32.4
84 NRB F TM 8.35 9.5 25.05 28.5
85 HNK M TM 8.8 9.3 26.4 27.9
86 KVM M BTI 8.5 9.75 25.5 29.25
87 NSA M TM 8.25 9.5 24.75 28.5
88 WAS M BTI 7.75 8.85 23.25 26.55
89 NAP M TM 8.3 9.5 24.9 28.5
90 MSS M TM 9.35 10.65 28.5 31.95
91 LSD M BTMi 7.85 9.1 23.55 27.3
92 ISS F BTMi 9 10.2 27 30.6
93 SAN F TM 7.1 8.3 21.3 24.9
94 GSM F TM 6.15 7.7 18.45 23.1
95 RKT F TM 6.2 8.25 18.6 24.75
96 RP* M TM 6.6 7.8 19.8 23.4
97 KSM M TM 8.2 9.4 24.6 28.2
98 MRR F TM 7.65 9 22.95 27
99 KPS F TM 8.65 8.7 28.54 26.1
100 MMM F TM 6.4 7.65 19.2 22.95
101 KBM F BTI 6.2 7.45 18.6 22.35
102 KJ* F TM 10 30 11.2 33.6
103 NPN F BTI 7.45 8.7 22.35 26.1
104 KAA F TM 7.95 9.15 23.85 27.45
105 PAD M TM 8.85 10.17 26.55 30.51

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
97
Table-24. Continued..
Patient
Code
Patient
Initials Sex Diagnosis Pre Hb Post Hb Pre HCT Post HCT
106 HSD F TM 8.3 9.45 24.9 28.35
107 GAS M BTI 8.9 11.05 26.7 33.15
108 KSS M BTI 6.95 8.25 20.85 24.75
109 RYS M TM 8.1 9.35 24.3 27
110 LSD F BTMi 7.75 9 23.25 28.05
111 DML M BTMi 8.35 9.55 25.5 28.65
112 SS* M TM 8.1 9.4 24.3 28.2
113 PKM M TM 9.05 10.25 27.15 30.75
114 MGM M BTI 8.1 9.3 24.3 27.9
115 OBC F TM 7.9 9.1 23.7 23.4
116 PVD M TM 8.8 9.95 26.4 29.85
117 KKM F BTI 8.5 9.8 25.5 29.4
118 KR F TM 8.3 9.5 24.9 28.5
119 JVS M TM 7.4 9.65 22.2 28.95
120 TAN F TM 7.9 9.2 23.7 27.3
121 CLP F BTI 8.1 9.4 24.3 27.6
122 DAM M TM 6.6 7.7 19.8 23.1
123 RVS M TM 8 9.2 24 27.6
124 DRD F BTMi 6.5 7.8 19.5 23.4
125 JSS* F TM 8.6 9.75 25.8 29.25

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
98
Table-24a. Indicated the pre and post blood transfusion Hb range in thalassemia patients.
Types of
Thalassemia
Sex
(Total patients)
Pre Hb range (%)
Post Hb range (%)
Normal Low Normal Low
SCT
M (1) 00(00.00) 01(100.00) 00(00.00) 01(100.00)
F (0) 00(00.00) 00(00.00) 00(00.00) 00(00.00)
Total 00(00.00) 01(100.00) 00(00.00) 01(100.00)
BTI
M (12) 00(00.00) 12(100.00) 00(00.00) 12(100.00)
F (4) 00(00.00) 04(100.00) 00(00.00) 04(100.00)
Total (16) 00(00.00) 16(100.00) 00(00.00) 16(100.00)
BTMi
M (6) 00(00.00) 06(100.00) 00(00.00) 06(100.00)
F (4) 00(00.00) 04(100.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 10(100.00) 00(00.00) 10(100.00)
TM
M (54) 00(00.00) 54(100.00) 00(00.00) 54(100.00)
F (44) 00(00.00) 44(100.00) 00(00.00) 44(100.00)
Total (98) 00(00.00) 98(100.00) 00(00.00) 98(100.00)
Total
patients
M (73) 00(00.00) 73(100.00) 00(00.00) 73(100.00)
F (52) 00(00.00) 52(100.00) 00(00.00) 52(100.00)
Total M+F (125) 00(00.00) 125(100.00) 00(00.00) 125(100.00)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
99
Pre and post blood transfusion HCT Count
The pre and post transfusion HCT count was shown in Table-24b and Figure-24 c and 24 d.
Before and after transfusion of blood, all thalassemic patients observed low HCT.
Table -24b. Showing pre and post blood transfusion HCT range in thalassemic patients
Types of
Thalassemia
Sex
(Total patients)
HCT Pre (%) HCT Post (%)
Normal Low Normal Low
SCT
M (1) 00(00.00) 01(100.00) 00(00.00) 01(100.00)
F (0) 00(00.00) 00(00.00) 00(00.00) 00(00.00)
Total 00(00.00) 01(100.00) 00(00.00) 01(100.00)
BTI
M (12) 00(00.00) 12(100.00) 00(00.00) 12(100.00)
F (4) 00(00.00) 04(100.00) 00(00.00) 04(100.00)
Total (16) 00(00.00) 16(100.00) 00(00.00) 16(100.00)
BTMi
M (6) 00(00.00) 06(100.00) 00(00.00) 06(100.00)
F (4) 00(00.00) 04(100.00) 00(00.00) 04(100.00)
Total (10) 00(00.00) 10(100.00) 00(00.00) 10(100.00)
TM
M (54) 00(00.00) 54(100.00) 00(00.00) 54(100.00)
F (44) 00(00.00) 44(100.00) 00(00.00) 44(100.00)
Total (98) 00(00.00) 98(100.00) 00(00.00) 98(100.00)
Total patients
M (73) 00(00.00) 73(100.00) 00(00.00) 73(100.00)
F (52) 00(00.00) 52(100.00) 00(00.00) 52(100.00)
Total M+F (125) 00(00.00) 125(100.00) 00(00.00) 125(100.00)
Malaria
The details of the screening of positive malaria patients are reported in Table-25.and Figure-
25. The prevalence was very less in thalassemic patients from Solapur District. Only one Beta
thalassemia intermedia male patient was observed Malaria positive out of 125 patients.
Transfusion-induced malaria may be a serious threat to the life in a group of special patients:
those who require many transfusions, those who have been treated with immunosuppressants,
and those who have undergone splenectomy. We observed transfusion-induced malaria in a
β-thalassemia major patient who had undergone splenectomy. Existing guidelines for
screening and excluding donors who have or have had malaria are inadequate, and serologic
screenings are too costly. We suggest some guidelines that may help prevent transfusion-

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
100
induced malaria, other diseases and complications. The present research data on malarial
infection in thalassemic patients from Solapur District can be corroborated with the reports of
Asian population study of Choudhury, et al. (1990). O'Donnell et al., (2009). This study also
got the less prevalence percentage of P. vivax.
Modiano et al. (1991) studied the protection against malaria morbidity in alpha-thalassemia
gene in a Nepalese population. Shear et al. (1998) in their studies they observed the
transgenic mice expressing human fetal globin are protected from malaria by a novel
mechanism. Roth et al. (1998) in their observation, malaria in beta-thalassemic mice and
their effects of the transgenic human beta-globin gene. The observations in this study were
that in SCT, BTI, BTMI and TM patients in Solapur District, were resistance to malaria due
to polytransfusion of blood.
Table-25. Prevalence of transfusion-induced malaria in thalassemic patients
Types of
Thalassemia
Sex (Total
patients)
Plasmodium
vivax (%)
P.
falciparum
(%)
P. malaria
(%)
P. ovale
(%)
SCT
M (1) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
F (0) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (1) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
BTI
M (12) 01 (08.33) 00 (00.00) 00 (00.00) 00 (00.00)
F (4) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (16) 01(6.25) 00 (00.00) 00 (00.00) 00 (00.00)
BTMi M (6) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
F (4) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (10) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
TM
M (54) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
F (44) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (98) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total patients
M (73) 01 (1.36) 00 (00.00) 00 (00.00) 00 (00.00)
F (52) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total M+F
(125)
00 (00.80) 00 (00.00) 00 (00.00) 00 (00.00)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
101
Transfusion –induced HCV, HIV, HBsAg and VDRL
The results of HCV, HIV, HBsAg and VDRL positive thalassemia patients showed in Table-
26; 27 and Figure-26. The HCV positive percentage was: male 8(10.95%), female 3(5.76%)
total 11(8.80%). The HIV positive and VDRL positive percentage was nil in all thalassemia
patients. The HBsAg positive percentage was: male 00(0.00%), female 2(5.76%) total
2(02.40%). The reports on tansfusion-induced pathoges are high frequency in splenectomized
patients, they acquired viruses such as HIV, syphilis, hepatitis B and C, iron overload and
defective adaptive/innate immune response (Smith et al., 1964; Piga and Monasterolo, 2001;
Ali et al., 2003;). Di Marco et al., (2008) reported that, in thalassemics, the severity of liver
damage (i.e. the finding of fibrosis and histological signs of cirrhosis) was clearly related to
persistent HCV infection. The reports observed and compared with study of Beeraj et. al.,
(2010) showed that the children suffering from beta-thalassemia major require repeated blood
transfusions which may be associated with dangers like iron overload and contraction of
infections such as HIV, HCV, and HBsAg which ultimately curtail their life span. On the
other hand, inadequate transfusions lead to severe anemia and general fatigue and debility.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
102
Table-26. Prevalence of transfusion-induced malarial parasites, HCV, HIV, HBsAg, VDRL
and complications in the spleen and liver.
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
1 Neg Neg NR Neg NR Normal Normal
2 Neg Neg NR Neg NR Normal Normal
3 Neg Neg NR Neg NR
Moderate
enlarge Normal
4 Neg Neg NR Neg NR Normal Normal
5 Neg Neg NR Neg NR Normal Normal
6 Neg Neg NR Neg NR Normal Normal
7 Neg Neg NR Neg NR Normal Normal
8 Neg Neg NR Neg NR Normal Normal
9 Neg Neg NR Neg NR Normal Normal
10 Neg Neg NR Neg NR Normal Normal
11 Neg Neg NR Neg NR Normal Normal
12 Neg Neg NR Neg NR Normal Normal
13 Neg Neg NR Neg NR Normal Normal
14 Neg Neg NR Neg NR
Moderate
enlarge Normal
15 Neg Neg NR Neg NR Normal Normal
16 Neg Neg NR Neg NR Normal Normal
17 Neg Neg NR Neg NR Normal Normal
18 Neg Neg NR Neg NR
Moderate
enlarge Normal
19 Neg Neg NR Neg NR
Mild
enlarge Normal
20 Neg Neg NR Neg NR Normal Normal
21 Neg Neg NR Neg NR Normal Normal
22 Neg Neg NR Neg NR Normal Normal
23 Neg Neg NR Neg NR Normal Normal
24 Neg Neg NR Neg NR Normal Normal
25 Neg Neg NR Neg NR Normal Normal
26 Neg Neg NR Neg NR Normal Normal
27 Neg Neg NR Neg NR Normal Normal
28 Neg Neg NR Neg NR Normal Normal
29 Neg Neg NR Neg NR Normal Normal
30 Neg Neg NR Neg NR Normal Normal
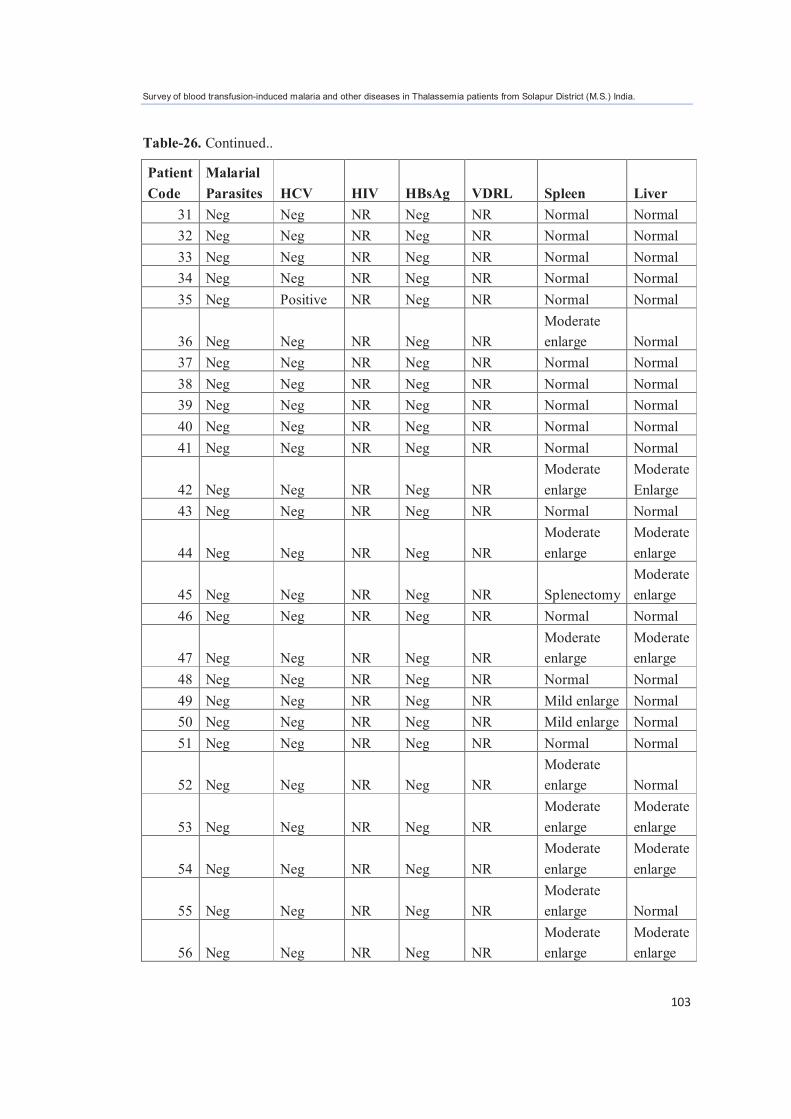
Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
103
Table-26. Continued..
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
31 Neg Neg NR Neg NR Normal Normal
32 Neg Neg NR Neg NR Normal Normal
33 Neg Neg NR Neg NR Normal Normal
34 Neg Neg NR Neg NR Normal Normal
35 Neg Positive NR Neg NR Normal Normal
36 Neg Neg NR Neg NR
Moderate
enlarge Normal
37 Neg Neg NR Neg NR Normal Normal
38 Neg Neg NR Neg NR Normal Normal
39 Neg Neg NR Neg NR Normal Normal
40 Neg Neg NR Neg NR Normal Normal
41 Neg Neg NR Neg NR Normal Normal
42 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
Enlarge
43 Neg Neg NR Neg NR Normal Normal
44 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
45 Neg Neg NR Neg NR Splenectomy
Moderate
enlarge
46 Neg Neg NR Neg NR Normal Normal
47 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
48 Neg Neg NR Neg NR Normal Normal
49 Neg Neg NR Neg NR Mild enlarge Normal
50 Neg Neg NR Neg NR Mild enlarge Normal
51 Neg Neg NR Neg NR Normal Normal
52 Neg Neg NR Neg NR
Moderate
enlarge Normal
53 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
54 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
55 Neg Neg NR Neg NR
Moderate
enlarge Normal
56 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
104
Table-26. Continued..
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
57 Neg Neg NR Neg NR Mild enlarge Normal
58 Neg Neg NR Neg NR Mild enlarge Normal
59 Neg Neg NR Neg NR Normal
Moderate
enlarge
60 Neg Neg NR Neg NR Normal
Moderate
enlarge
61 Neg Neg NR Neg NR Normal Normal
62 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
63 Neg Neg NR Neg NR Normal Normal
64 Neg Neg NR Neg NR Splenectomy Normal
65 Neg Positive NR Neg NR
Moderate
enlarge
Moderate
enlarge
66 Neg Neg NR Neg NR Normal Normal
67 Neg Neg NR Neg NR Normal Normal
68 Neg Neg NR Neg NR Normal Normal
69 Neg Neg NR Neg NR Normal Normal
70 Neg Neg NR Neg NR
Moderate
enlarge Normal
71 Neg Neg NR Neg NR Mild enlarge
Moderate
enlarge
72 Neg Neg NR Neg NR Mild enlarge
Mild
enlarge
73 Neg Neg NR Neg NR
Moderate
enlarge Normal
74 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
105
Table-26. Continued...
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
75 Neg Neg NR Neg NR
Moderate
enlarge Normal
76 Neg Neg NR Neg NR Mild enlarge
Moderate
enlarge
77 Neg Neg NR Neg NR
Moderate
enlarge Normal
78 Neg Neg NR Neg NR
Moderate
enlarge
Mild
enlarge
79 Neg Neg NR Neg NR Normal Normal
80 Neg Neg NR Neg NR Mild enlarge
Mild
enlarge
81 Neg Neg NR Neg NR Normal Normal
82 Neg Neg NR Neg NR
Moderate
enlarge Normal
83 Neg Neg NR Neg NR Normal Normal
84 Neg Neg NR Neg NR Normal Normal
85 Neg Neg NR Neg NR
Moderate
enlarge Normal
86 Neg Neg NR Neg NR Normal Normal
87 Neg positive NR Neg NR
Moderate
enlarge Normal
88 Neg Positive NR Neg NR
Moderate
enlarge
Mild
enlarge
89 Neg Neg NR Neg NR Splenectomy Normal
90 Neg Neg NR Neg NR Splenectomy Normal

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
106
Table-26. Continued...
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
91 Neg Neg NR Neg NR Normal Normal
92 Neg Neg NR Neg NR Mild enlarge Normal
93 Neg Neg NR Neg NR
Highly
enlarge
Moderate
enlarge
94 Neg Neg NR Positive NR Mild enlarge
Mild
enlarge
95 Neg Neg NR Neg NR
Moderate
enlarge Normal
96 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
97 Neg Neg NR Neg NR Normal Normal
98 Neg Positive NR Neg NR Mild enlarge
Moderate
enlarge
99 Neg Neg NR Neg NR Splenectomy Normal
100 Neg Neg NR Neg NR Splenectomy Normal
101 Neg Neg NR Neg NR
Moderate
enlarge Normal
102 Neg Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
103 Positive Neg NR Neg NR
Moderate
enlarge
Moderate
enlarge
104 Neg Neg NR Neg NR Mild enlarge
Moderate
enlarge
105 Neg Positive NR Neg NR Splenectomy Normal

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
107
Table-26. Continued...
Patient
Code
Malarial
Parasites HCV HIV HBsAg VDRL Spleen Liver
106 Neg Positive NR Neg NR Splenectomy Normal
107 Neg Neg NR Neg NR Normal Normal
108 Positive Positive NR Neg NR Splenectomy
Mild
enlarge
109 Neg Neg NR Neg NR Mild enlarge
Mild
enlarge
110 Neg Neg NR Positive NR Normal Normal
111 Neg Neg NR Neg NR Mild enlarge
Moderate
enlarge
112 Positive positive NR Neg NR
Moderate
enlarge Normal
113 Neg Neg NR Neg NR Normal Normal
114 Neg Neg NR Neg NR Mild enlarge Normal
115 Positive Neg NR Neg NR Normal Normal
116 Neg Neg NR Neg NR Splenectomy Normal
117 Neg Neg NR Neg NR Normal Normal
118 Neg Neg NR Neg NR
Moderate
enlarge
Mild
enlarge
119 Neg Neg NR Neg NR Splenectomy Normal
120 Neg Neg NR Neg NR Normal Normal
121 Neg Positive NR Neg NR Splenectomy
Mild
enlarge
122 Neg Positive NR Neg NR
Moderate
enlarge
Moderate
enlarge
123 Neg Neg NR Neg NR Splenectomy Normal
124 Neg Neg NR Neg NR Splenectomy Normal
125 Neg Neg NR Positive NR Splenectomy Normal

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
108
Table-26a. Showing prevalence percentage of transfusion-induced pathogens like HCV,
HIV, HBsAg and VDRL.
Types of
Thalassemia
Sex
(Total patients)
HCV
Positive
(%)
HIV
Positive
(%)
HBsAg
Positive
(%)
VDRL
Positive
(%)
SCT
M (1) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
F (0) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (1) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
BTI
M (12) 02 (16.66) 00 (00.00) 00 (00.00) 00 (00.00)
F (4) 01 (25.00) 00 (00.00) 00 (00.00) 00 (00.00)
Total (16) 03 (18.75) 00 (00.00) 00 (00.00) 00 (00.00)
BTMi
M (6) 00 (00.00) 00 (00.00) 00 (00.00) 00 (00.00)
F (4) 00 (00.00) 00 (00.00) 01 (25.00) 00 (00.00)
Total (10) 00 (00.00) 00 (00.00) 01 (10.00) 00 (00.00)
TM
M (54) 06 (11.11) 00 (00.00) 00 (00.00) 00 (00.00)
F (44) 02 (04.54) 00 (00.00) 02 (04.54) 00 (00.00)
Total (98) 08 (8.16) 00 (00.00) 02 (2.04) 00 (00.00)
Total Positive
patients
M (73) 8 (10.95) 00 (00.00) 00 (00.00) 00 (00.00)
F (52) 3 (05.76) 00 (00.00) 03 (05.76) 00 (00.00)
Total M+F (125) 11 (8.80) 00 (00.00) 03 (02.40) 00 (00.00)
Liver
The liver of thalassemic patients was observed under three categories normal, mild
enlargement, moderate enlargement. Table-27 and Figure-27. Normal liver percentage was:
male 56(76.71%), female 38(73.07%) and in both male and female were 94(75.20%); mild
enlargement of liver: male 5(6.84%), female 4(7.69%) avarage 9(7.20%); moderate
enlargement of liver: male 12(16.43%), female 10(19.23%) avarage 22(17.60%). Liver
toxicity can occur as a direct consequence of iron toxicity and from transfusion-acquired
hepatitis. Liver function must be routinely screened in thalassemia patients on chronic
transfusion. The results compired with the observations of (Aach et al., 1991), due to blood
transfusions, many patients with β-thalassemia are infected with either hepatitis C virus (HCV) or
hepatitis B virus (HBV).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
109
Hyperthyroidism
The hyperthyroidism was not found in any patients Table-27a. .
Alloimmunization
The alloimmunization (Table-27 and Figure-27a) was observed in male 1(1.36%), female
1(1.92%) avarage being 2(16.66%). This study includes red cell alloimmunization rate among
thalassemia patients on regular blood transfusion. Post-storage leukodepleted blood was used
for transfusion. It is not a standard practice in various centers to give phenotype-matched red
cells to patients with thalassemia. The use of phenotype matched blood is given only in
patients who have developed alloantibodies. Alloimmunization was an important finding in
patients with β-major-Thalassemia.
TM patients managed by regular transfusion regimen may develop anti-red cell
alloimmunization. If the alloantibodies are hemolyzing in nature, transfusion reaction may
occur, and provision of blood thereafter requires matching of the relevant blood group in
addition to `ABO" and Rh `D` matching. The hemolyzing nature of antibodies should be
determined in patients who develop these antibodies, and transfusion should be arranged
accordingly. Data regarding the impact of platelet refractoriness on morbidity and mortality
for thrombocytopenic patients are inconsistent. Failure to achieve platelet counts greater than
5 X 109/L significantly increases the probability of life-threatening bleeding. The rate of red
blood cell alloimmunization is relatively low in thalassemia patients. The age at first blood
transfusion and splenectomy were not statistically significant as risk factors for
alloimmunization in this study.
Patients were treated with immunosupressive drugs including prednisolone, intravenous
immunoglobulin, cyclosporine A and azathioprine and now all of them are in healthy
condition. Walker et al. (1989) observed the alloimmunization following blood transfusion.
Thompson et al. (2011) studied the Red cell alloimmunization in a diverse population of
transfused patients with thalassaemia. Iron level tests and serum ferritin tests were not done
time to time after and before blood transfusion by the patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
110
Table-27. Showing the size of liver, hyperthyroidism and alloimmunization in thalassemic
patients.
Types of
Thalassemia
Sex
(Total
patients)
Liver Hyperthy
-roidism
Positive
Alloimmu-
nization
Positive
Normal Mild Moderate
SCT
M (1) 00 00 01 00 00
F (0) 00 00 00 00 00
Total (1) 00 00 01 00 00
BTI
M (12) 09 02 01 00 00
F (4) 02 01 01 00 00
Total (16) 11 03 02 00 00
BTMi
M (6) 04 00 02 00 00
F (4) 04 00 00 00 00
Total (10) 08 00 02 00 00
TM
M (54) 43 03 08 00 01
F (44) 32 03 09 00 01
Total (98) 75 06 17 00 02
Total
Positive
Patients (%)
M (73) 56
(76.71)
05
(06.84)
12 (16.43) 00
(00.00)
01
(01.36)
F (52) 38
(73.07)
04
(07.69)
10 (19.23) 00
(00.00)
01
(01.92)
Total M+F
(125)
94 (75.20) 09 (07.20) 22 (17.60) 00
(00.00)
02 (16.66)
Spleen and splenectomy
Table-28 and Figure-28 summarizes the spleen of thalassemic patients. It was observed
under five categories namely, normal, mild enlargement, moderate enlargement, highly
enlarged and splenectomy (removal of spleen). Normal size spleen percentage was: male
33(45.20%), female 28(53.84%) avarage 61(48.80%); Mild enlargement of spleen: male
9(12.32%), female 7(13.46%) avarage 16(12.80%); moderate enlargement of spleen: male
24(32.87%), female 8(15.38%) avarage 32(25.60%); highly enlargement of spleen: male
0(0.00%), female 1(1.92%) avarage 1(0.80%); splenectomy was: male7(9.58%), female
8(15.38%) avarage 15(12.00%). A highly enlarged spleen was observed in only one patient,

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
111
in sixteen patients spleen was mildly enlarge and in thirty two patients spleen was moderately
enlarge. In our series of 125 thalassemia patients, 15(12.00%) patients had undergone
splenectomy due to heavy iron overload by poly-transfusion. When the spleen continues to
enlarge, hypersplenism results and corrective measures such as splenectomy are required.
Spleen filters abnormal blood cells and removes them from the circulatory system; diseases
that result in abnormal red cells will cause the spleen to enlarge. Sickle cell disease,
thalassemia, and spherocytosis are examples of diseases that form unusually shaped cells that
cannot easily maneuver through the small blood vessels and capillaries of the body. If they
are not removed by the spleen, these abnormal cells can cause blood clots and decrease
circulation. However, removing them causes the spleen to swell and enlarge, the observations
are compired the reports of eMedicineHealth (2011). Splenomegaly is a common
complication caused mainly by massive erythropoieses the results corroborated with reports
of Cappellini et al., (2000a). Splenectomy is essential when spleen is highly enlarged. The
findings of Al-Salem et al. (1989); Smith et al. (1964); Sanefuji et al. (2006); Kheradpir et
al. (1985) and Phrommintikul et al. (2006) also corroborated with present data.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
112
Table-28. Showing spleen enlargement in present study.
Types of
Thalassemia
Sex
(Total
patients)
Spleen
Normal Mild Moderate Highly
Enlarged
Spleenectomy
SCT
M (1) 00 00 01 00 00
F (0) 00 00 00 00 00
Total (1) 00 00 01 00 00
BTI
M (12) 09 01 01 00 01
F (4) 01 00 02 00 01
Total (16) 10 01 03 00 02
BTMi
M (6) 02 02 02 00 00
F (4) 02 01 00 00 01
Total (10) 04 03 02 00 01
TM
M (54) 22 06 20 00 06
F (44) 25 06 06 01 06
Total (98) 47 12 26 01 12
Total Positive
Patients (%)
M (73) 33
(45.20)
09
(12.32)
24 (32.87) 00
(00.00)
07
(09.58)
F (52) 28
(53.84)
07
(13.46)
08 (15.38) 01
(01.92)
08
(15.38)
Total
M+F
(125)
61
(48.8)
16
(12.80)
32 (25.60) 01
(0.80)
15
(12.00)
Medication
As documented in Table-29 and Figure-29, the thalassemic patients mediacation was: Anti
TB; Desirox-500mg male (0.00%), female (1.92%) avarage (0.8%); Asunra 400mg male
(1.36%), female (1.92%) avarage (16.0%); Aurvedic male (2.73%), female (0.00%) avarage
(16.0%); Calcium-X; Kelfer male (0.00%), female (1.92%) avarage (0.8%); Calpol; Bevon
male (1.36%), female (0.00%) avarage (0.8%); Dyton; Folvite male (1.36%), female (0.00%)
total (0.8%); Folvite male (6.84%), female (25.0%) avarage (14.4%); Insulin male (1.36%),
female (0.00%) total (0.8%); Kelfer male (17.80%), female (7.69%) avarage (13.6%); Kelfer;
Folvite male (0.00%), female (1.92%) avarage (0.8%); Loser male (1.36%), female (0.00%)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
113
total (0.8%); no medication male (54.73%), female (59.61%) avarage (56.8%). Total fifty four
patients were gives treatment with different drugs by suggestions of the medical experts, the drugs
are namely anti TB drugs, Desirox-500mg, Asunra, ayurvedic treatment, Calcium-X; Kelfer,
Calpol, Bevo, Dyton, Folvite, Insulin.
Table-29. Showing the medication given for thalassemic patients.
Sex Medication Male (%) Female (%) Total Male +
Female (%)
Medication
Anti TB; Desirox-500mg 0 (0.00) 1 (1.92) 1 (0.8)
Asunra 400mg 1 (1.36) 1 (1.92) 2 (16.0)
Aurvedic 2 (2.73) 0 (0.00) 2 (16.0)
Calcium-X; Kelfer 0 (0.00) 1 (1.92) 1 (0.8)
Calpol; Bevon 1 (1.36) 0 (0.00) 1 (0.8)
Dyton; Folvite 1 (1.36) 0 (0.00) 1 (0.8)
Folvite 5 (6.84) 13 (25.0) 18 (14.4)
Insulin 1 (1.36) 0 (0.00) 1 (0.8)
Kelfer 13 (17.80) 4 (7.69) 17 (13.6)
Kelfer; Folvite 0 (0.00) 1 (1.92) 1 (0.8)
Loser 1 (1.36) 0 (0.00) 1 (0.8)
No 40 (54.73) 31 (59.61) 71 (56.8)
Mortality
The mortality rates of study patients were also examined during the study period (Table-30
and Figure-30) showing probably age specific mortality. In 6-10 years the mortality rate was:
male 5(6.84%); female (0.00%); avarage 5(4%). The mortality rate was: male 3(3.10%);
female 5(9.61%); avarage 8(6.4%) in age between 11-15 Years and 16-18 years: male
2(2.73%); female 3(5.76%); avarage 5(4%). This leads to increased mortality during 11-15
years of age. As a result, transfusional iron overload can cause increased morbidity and premature
mortality in thalassemia patients. The results compared with the findings of the Olivieri and
Brittenham (1997) and Darbari et al. (2006). The greater the transfusion requirement, the greater the
risk of premature mortality was observed during the study. The only way to prevent the disease
and reduce the morbidity and mortality is by educating the patients and parents. For this
reason in this present study, awareness among parents of thalassemic patients regarding the
disease was evaluated. Epidemiological transition caused by improvements in hygiene,

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
114
nutrition, proper medication, blood transfusions and control of infection that has reduced
childhood mortality.
Table-30. Showing the prevalence percentage of mortality in thalassemic patients.
Types of
Thalassemia
Sex
(Total patients)
Mortality
6 Months
to 5 Years
6 Years -
10 Years
11 Years- 15
Years
16 Years to
18 Years
SCT
M (1) 00 00 00 00
F (0) 00 00 00 00
Total (1) 00 00 00 00
BTI
M (12) 00 00 00 01
F (4) 00 00 02 00
Total (16) 00 00 02 01
BTMi M (6) 00 01 00 00
F (4) 00 00 00 00
Total (10) 00 01 00 00
TM
M (54) 0 04 03 01
F (44) 00 00 03 03
Total (98) 00 04 06 04
Total patients
(%)
M (73) 00 (0.00) 05 (6.84) 03(4.10) 02 (2.73)
F (52) 00 (0.00) 00 (0.00) 05 (9.61) 03 (5.76)
Total M+F (125) 00 (0.00) 05(4.0) 08 (6.4) 05 (4.00)
Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
115
6. SIGNIFICANCE OF THE STUDY
The results showed that the high prevalence of thalassemia was observed in the Solapur
District.
Screening of children, pregnant women, and individuals visiting public health facilities is
effective in identifying individuals at risk who require further testing. A simple CBC count,
with emphasis on the RBC counts and indices, including the mean corpuscular volume
(MCV), mean corpuscular Hb (MCH), and RBC distribution width (RDW), is the main
component of such screening processes. Persons suspected to be positive for thalassemia are
checked for elevated levels of Hb for confirmation. In some situations, this simple method
was not adequate, and further testing, including analyses of globin chain synthesis, must be
performed to reach a final diagnosis.
To safeguard the quality of blood transfusion services , the recommendations of WHO and
other agencies should be taken into considerations.
At the time of study, some patients were unaware of their diabetes status. The patients did not
know that their blood was infected by pathogenic organisms. The thesis data was also helpful
for all thalassemic patients in Solapur District and in Country to plan carrier screening,
counseling, awareness of the diseases, prenatal diagnosis and related services. The
information provided here was very useful for efficient evaluation of novel treatment
methods, educational, informational purposes and management strategies of potential benefit
for children and adults with thalassemia.
Further devotement of new methodology, research plans and directs research and research
training and career development programs, on the causes, prevention, and treatment of blood
diseases, including anemias, sickle cell disease, and thalassemia.
Present research work was helpful for extending knowledge of the thalassemia, its prevention
and treatment. It may also prove useful for policy makers, health professionals, patients and
parents, and the community at large.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
116
It will also proved helpful for screening the right of every patient for equal access to quality
medical care, and the safety and adequacy of blood. This research work is intended for a wide
audience with the expectation that national health authorities, policy-makers, scholars,
researchers, health workers and others committed to the advancement of public health in the
Asian region will make good use of it.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
117
7. CONCLUSION
Over 125 patients affected by thalassemia live in Solapur District, Maharashtra, India.
Thalassemia is a blood disease and is common in both sexes. Thalassemia was suspected in
all these patients with age six months to eighteen years, the prevalence percentage of TM was
more than the BTI, BTMi and SCT. The prevalence percentage of thalassemia in specific
ethnic groups. In Solapur District the high frequency of thalassemic patients were observed in
the area of Solapur City, Pandharpur Taluka and in South Solapur as compared to other
Talukas.
In our study, only one SCT patient was found, total BTI patients were sixteen, BTMi were
four and TM were ninety eight. Hence the prevalence percentage of TM were very high in
Solapur District as compared to SCT, BTI and BTMi.
Patients present with pallor, poor appetite, poor growth, lethargy and irritability was
observed. Only one mentally challenged female patient was observed. As thalassemia has an
impact on the different psychosocial life aspects, it is very essential to provide psychosocial
support, including progress of the disease in the patients and parents for clear understanding.
In the present study, the age of thalassemia patients was in between the range of 6 months to
18 years. The mean age was around 8.75 years. The numbers of patients in the age group 6
months to 3 years are more. There were 19 Male and 15 female with t avarage 34(27.2%)
patients in 6 months-3 years age group. Patients between 4-6 years, 12 Male and 6 female
with avarage 18(14.4%); patients in 7-10 years, Male 22, female 11, avarage 33(26.4%); in
11-13 years Male 9 female 11 total 20(16%); in between 14-16 age Male7, female 3, avarage
10(8%); in 17-18 years Male 4, female 6, avarage 10(8%), Maximum patients was:
34(27.2%) were in the age group of 6 months 3 years and minimum patients were : 10(8%) in
both age group of 14-16 and 17-18 years age.
The present study comprised of males and females. A higher incidence of thalassemia was
observed in male than female. Thalassemia was the serious medical problem. In the present
research work, the findings are the failure to thrive after six months of age, stunting in height
and weight. It indicates majority thalassemic patients showed poor growth in poly-transfused
beta thalassemia patients. The observations showed the consanguinity rate was very high

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
118
(>49%) in male and female. That indicates the need for implementing a comprehensive
genetic preventive program for the eradication of thalassemia in Solapur District.
As per the pedigree analysis of the patients observed, most of the parents were thalassemia
minor. The majority (>22.4%) of thalassemia patients were illiterate with only 1.6% with a
higher education. Only one case was reported under psychological burden. It is evident from
the findings of our study that besides the clinical burden, thalassemic have to shoulder very
low psychosocial impact associated with the disease. There was no any correlation between
the psychological impact and the gender. Furthermore, the concept of non-directive genetic
counseling is incompatible with a campaign against consanguineous marriage. The
prevalence percentage was very high in Hindu and muslin as compared in Jain and Sindhi
community. In the present study the non vegetarian thalassemic patients are more than the
vegetarian. Rodent face and saddle nose are more in thalassemic patients as compared to
maxillary protrusion, maxillary anterior teeth spacing and anterior open bite. Only one case
was observed in mucosal discoloration. There was not any relationship between the
complications and sex but skull and face deformities can be closely related to the patient's
age.
In conclusion the hematological parameters vary as compared to normal ranges. The normal
WBC was 80.80% and below normal range percentage of WBC was observed nil in all
patients as compared to high WBC count (>19%). RBC count above range was nil in both
sexes. But in TM patients RBC count below normal was observed in majority patients
(>95%). RBC indices showed microcytic anemia. TM is characterized by reduced Hb level
(<7 g/dl). Hematological investigations revealed the low Hb levels <8.0 g/dL (falling further
with increasing age and severity) with severe microcytosis and hypochromia and increase
target cells in the peripheral film.
All thalassemic patients’ hemoglobin, HCT count was very low, not a single patient was
observed in normal and with high range. MCV count was very low (>99%) in majority
patients. The MCH and MCHC readings was normal in majority patients but nineteen
patients MCH and thirteen patients MCHC was observed below range. Overall the normal
range platelet count is more than that of the high range observed in twenty four patients and
below range was eight in thalassemia patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
119
The pre and post transfusion normal hemoglobin and HCT count was nil in all patients but
below range was observed in all patients, which is comparable to studies conducted by other
authors. Electrophoresis is a gold standard for the diagnosis of thalassemia but it is not
available at all places. Thus several attempts have been made to diagnose the condition by
using red cell indices.
Only the history of one thalassemic patient was showed Plasmodium vivax infection due to
blood transfusion. Recently available kits are useful for testing the positive malarial cases and
it helps to prevent transfusion-induced malaria, other diseases and other complications. This
extensive and well-executed study concludes that SCT, BTI, BTMi, and TM protect
individuals against acquiring malarial infection, They become symptomatic but develop very
low parasite densities. However, the study also concludes that the risks of developing severe
malaria, especially malarial anaemia, are reduced in people with SCT,BTI, BTMi and TM
patients and they reduced risk of malaria-specific mortality.
The HIV positive and VDRL positive percentage was nil in all thalassemia patients. The
HBsAg positive observed 2.40%. The HCV positive were observed 8.80% due to blood
transfusion.
The mild liver enlargement was observed in nine patients and moderate enlarge liver was
observed in twenty two patients. Liver function and hepatitis serology must be routinely
screened in thalassemia patients on chronic transfusion.
The hyperthyroidism was not seen in any thalassemic patients, but the alloimmunization was
observed in one male and one female. A highly enlarged spleen was observed in only one
patient, in sixteen patients spleen was mild enlarge and in thirty two patients spleen was
moderately enlarge. Total fifteen patients were done splenectomy due to heavy iron overload
by poly-transfusion. Total fifty four patients were given treatment with different drugs by
suggestions of the medical expert, the drugs are namely anti TB drugs, Desirox-500mg,
Asunra, ayurvedic treatment, Calcium-X; Kelfer, Calpol, Bevo, Dyton, Folvite, Insulin,
Loser whichever necessary. For supportive treatment mainly by blood transfusion and
medications is freely available in various blood banks at Solapur.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
120
The age group of 6-10 years the mortality rate in male were 6.84%; female 0.00%, in the age
between 11-15 Years and 16-18 years: male 2.73%, female 5.76%, avarage 4%. This leads to
increased mortality during 11-15 years of age. As a result, transfusion iron overload can
cause increased morbidity and premature mortality in thalassemia patients.
In conclusion, blood transfusion therapy and optimal safety of transfused blood are the key
concepts in the protocol of treatment of thalassemia. The maintenance of red cell viability
and function during storage, to ensure sufficient transport of oxygen, maintainance of
appropriate hemoglobin level was essential. Avoidance of adverse reactions, including
transmission of infectious agents like malarial parasites, other pathogenic protozoans, HCV,
HIV, HBsAg, VDRL, microorganisms and other complications are essential.
Intake of Milk, a rich source of calcium, should be at least 500 ml daily, particularly because
it helps to prevent osteoporosis. In Thalassemia, although most of the iron overload is due to
blood transfusions, a small amount of iron is also absorbed from the diet. The absorption of
iron is higher when the hemoglobin is low. Iron chelators such as Desferal and Deferiprone
not only bind iron but also some Zinc and excrete it in the urine. The main nutritional sources
of Zinc are animal foods (meat and dairy products) and wholemeal cereals. In thalassemia,
because of the excess iron in the body, there is a higher risk of oxidative damage. The main
antioxidants are vitamin E, vitamin C, carotenoids and flavonoids are to be given to patients.
Knowing the results of thalassemia screening can impact decisions for prenatal diagnosis
before marriage and well before pregnancy. In conclusion this thesis offers various types of
data that may be useful in management and prevention of thalassemia in India and abroad.
Future research directions
The goal for future research in thalassemia is not only to introduce new strategies of
diagnosis and treatment of thalassemia but also to discover ways to prevent transfusion-
induced malaria, HCV, HIV, HBsAg, VDRL and other complications in thalassemic patients.
Current work deals with specific complications in thalassemia patients such as orofacial
complications, consigunity, ethnicity, hyperthyroidism, Alloimmunization, Hb level at pre
and post blood transfusions, anthropologic measurements, hematological study and
transfusion-induced or transmitted pathogens, complications in liver, spleen,
alloimmunization etc. Efforts should be towards promoting awareness of thalassemia

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
121
amongst the public and health professionals, and promoting the establishment and
improvement of policies aimed at the prevention and medical treatment of thalassemia.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
122
LIST OF ABBREVIATIONS
Symbol Abbreviations
α Alpha
HBA Adult Hemoglobin
β Beta
BT Beta thalassemia
TM Beta-Thalassemia Major
BTMi Beta Thalassemia Minor
BTI Beta Thalassemia Intermedia
CBC Complete Blood Count
0C Degree Celsius
δ Delta
ε Epsilon
F Female
γ Gamma
gm Gram
HCT Hematocrite
HgB Hemoglobin
HBA2 Hemoglobin A2
HbF hemoglobin F (Fetal hemoglobin)
HbS hemoglobin S (Sickle hemoglobin)
HBsAg Hepatitis B Surface Antigen
HCV Hepatitis C Virus
HIV Human Immunodeficiency Virus
Kg Kilogram
M Male
M.C.V. Mean Cell Volume
M.C.H. Mean Cell Hemoglobin
M.C.H.C. Mean Cell Hemoglobin concentration
µ micro
µg micro-gram
µl Micro-Liter
ml Milliliter
Neg Negative
NR Non Reactive
NS Not seen
% Percentage
R.B.C. Red blood cells
SCT Sickle cell thalassemia
θ Theta
VDRL Venereal Disease Research Laboratory
W.B.C. White blood Cells
ζ Zeta

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
123
REFERENCES
Aach, R. D., Stevens, C. E., Hollinger, F. B., Mosley, J. W., Peterson, D. A., Taylor, P.
E., Johnson, R. G., Barbosa, L. H. and Nemo, G. J. (1991): Hepatitis C virus infection in
post-transfusion hepatitis. An analysis with first and second generation assays. N. Engl. J.
Med. 325(19): 1325-1329.
Abdalla Hazza. (2006): Dental development in subjects with Thalassemia major. J.
Contemp.Dental Practice. 7(4): 80-83.
Abdelmohsen Ahmed Abdelmohsen Nayel. (2011): Study of exhaled carbon monoxide
oncentration in beta-thalassemia and its relation to red blood cell transfusion therapy in
pediatrics. Thesis, Master Degree in Pediatrics Faculty of Medicine, Ain Shams University.
Abolfazl Mahyar., Parviz Ayazi., Ali-Asghar Pahlevan., Hoshyar Mojabi., Mohammad-
Reza Sehhat. and Amir Javadi. (2010): Zinc and Copper status in children with beta-
thalassemia major. Ir. J. Pediatr. 20(3): 297-302.
Abu Alhaija, E. S., Hattab, F. N. and Al-Omari, M. A. (2002): Cephalometric
measurements and facial deformities in subjects with beta-thalassemia major. Eur. J. Orthod.
24: 9-19.
Aditi Bandyopadhyay., Sanmay Bandyopadhyay., Jayasri Basak., Bama Charan
Mondal., Anjali Angelika Sarkar., Sunipa Majumdar., Mani Kanchan Das., Sharmila
Chandra., Ashis Mukhopadhyay., Mamtaj Sanghamita., Kusagradhi Ghosh. and Uma
B. Dasgupta. (2004): Profile of beta-thalassemia in eastern India and its prenatal diagnosis.
Prenat. Diagn. 24(12): 992-996.
Agha hoseini F shabandy M (2000): Evaluation of maxillofacial anomalies in B-tha-
lassemia major [PhD Thesis]. Dental school, Tehran University of Medical Sciences, Iran.
Agarwal, M. B. (2003): ICL 670: A new oral cheater: A major breakthrough in treatment of
thalassaemia. Ind. J. Hematol. Blood Trans. 31: 26-28.
Agarwal, M. B., Mehta, B. C. (1982): Genotypic analysis of symptomatic thalasaemic
syndromes. J. Post Graduate Med. 28(1): 1-3.
Agarwal, S., Gulati, R. and Singh, K. (1997): Hemoglobin E-beta thalassemia in Uttar
Pradesh. Ind. Pediatr. 34: 287-292.
Agarwal, S., Gupta, A., Gupta, U. R., Sarwai, S., Phadke, S. and Agarwal, S. S. (2003):
Prenatal diagnosis in beta-thalassemia: an Indian experience. Fetal Diagn. Ther. 18: 328-
332.
Agha hoseini F. and shabandy, M. (2000): Evaluation of maxillofacial anomalies in β-
thalassemia major [PhD Thesis]. Dental school, Tehran University of Medical Sciences, Iran.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
124
Ahmed, S., Saleem, M., Sultana, N., Raashid, Y., Waqar, A., Anwar, M., Modell,
B., Karamat, K. A. and Petrou, M. (2000): Prenatal diagnosis of beta thalassaemia in
Pakistan: experience in a Muslim country. Prenat. Diagn. 20(5): 378–383.
Ali. N., Nadeem, M., Qamar, A., Qureshi, A. H. and Ejaz, A. (2003): Frequency of
hepatitis C virus antibodies in blood donors in combined military hospital, Quetta. Pak. J.
Med. Sci. 19(1): 41-44.
Alice Nyakeriga (2005): Relation of nutritional status, immunity, hemoglobinopathy and
falciparum malaria infection. Dissertation, Wenner-Grens institut för experimentell biologi
Stockholms, Universitet, Stockholm.
Allen, S. J., O’Donnell, A., Alexander, N. D., Alpers, M. P., Peto, T. E., Clegg, J. B.
and Weatherall, D. J. (1997): Alpha -thalassemia protects children against disease caused
by other infections as well as malaria. Proc. Nat. Acad. Sci. USA. 94(26): 14736-14741.
Al-Salem, A. H., Khawaja, Al-Fadel M., Grant, C. and Al-Awami B. (1989):
Splenectomy in children with sickle cell disease and thalassemia. Ind. J. Pediatr. 56: 747-
752.
Altay, C. and BaBak, A. N. (1995): Molecular basis and prenatal diagnosis of
hemoglobinopathies in Turkey. Int. J. Pediatr. Hematol. / Oncol. 2: 283-290.
Aluoch, J. R. (1997): Higher resistance to Plasmodium falciparum infection in patients with
homozygous sickle cell disease in western Kenya. Trop. Med. Int. Health. 2: 568-571.
Amini, F., Jafari, A., Eslamian, L. and Sharifzadeh S. (2007): A cephalometric study on
craniofacial morphology of Iranian children with beta-thalassemia major. Orthod. Craniofac.
Res. 10: 36-44.
Androulla Eleftheriou (2007): About Thalassemia. Published by the Thalassemia
International Federation, Nicosia.
Angastiniotis, M. A. and Hadjiminas M. G. (1981): Prevention of thalassemia in Cyprus.
Lancet. 1: 369–371.
Arıca S.G., Turhan E., Ozer C., Arıca V., Silfeler D.B., Silfeler I. and Altun A.B. (2012):
Evaluation of hemoglobinopathy screening results of a six year period in Turkey. Int. J.
Collaborative Res. Internal Medicine Public Health. 4(2):145-151.
Ashraf Sayyedi, Fereydoun Pourdanesh, Bahador Sarkari, and Sayyed Hesamedin
Nabavizadeh. (2008): Evaluation of oro-maxillofacial Changes in major thalassemia. Inside
Dentistry. 4(2). URL: http://www.dentalaegis.com/id/2008/02/white-paper-evaluation-of-oro-
maxillofacial-changes-in-major-thalassemia.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
125
Atika Khurana., Sudha Katyal. and R. K. Marwaha. (2006): Psychosocial burden in
Thalassemia. Ind. J. Pediatr. 73(10): 877-880.
Aydinok, Y., Erermis, S., Bukusoglu, N., Yilmaz, D. and Solak, U. (2005): Psychosocial
implications of thalassemia major. Pediatr. Int. 47(1): 84-89.
Balgir, R. S. (1995): The clinical and hematological profile of sickle cell disease cases in
India. Ind. Pract. 48: 423–432.
Balgir, R. S. (2000): The burden of hemoglobinopathies in India and the challenges ahead.
Curr. Sci. 79: 1536–1547.
Balgir, R. S. (2001): Genetic epidemiology of the sickle cell anaemia in India. Ind. Pract.
54: 771–776.
Balgir, R. S. (2005): Spectrum of hemoglobinopathies in the state of Orissa, India: a ten
years cohort study. J. Assoc. Phys. Ind. 53: 1021–1026.
Balgir, R. S. (2007): Aberrant heterosis in hemoglobinopathies with special reference to β–
thalassemia and structurally abnormal haemoglobins E and S in Orissa, India. J. Clin. Diagn.
Res. 122–130.
Balgir, R. S. (2010): Phenotypic diversity of sickle cell disorders with special emphasis on
Public health genetics in India. Curr. Sci. 98(8): 25.
Banerji. (1999): URL: http://www.drbanerji-fertilityclinic.com/researchprograms.html
Bangal, V., Kwatra, A., Raghav, S. and Modi, H. (2009): Recurrent pregnancy loss due to
haemoglobinopathy (Thalassemia). Pravara Med. Rev. 4(1).
Bassimitci, S., Yucel-Eroglu E. and Akalar M. (1996): Effects of thalassemia major on
components of the craniofacial complex. Brit. J. Orthodo. 23: 157–162.
URL: http://www.pravara.com/pmr/pmr-4-1-7.pdf
Basanagoudar, P., Shivinder S. Gill., Mandeep S. Dhillon. and Ram K. Marwaha.
(2001): Fractures in transfusion dependent beta-thalassemia – An Indian study. Singapore
Med. J. 42(5): 196-199. URL: http://www.sma.org.sg/smj/4205/4205a2.pdf
Bennett, R. L., Steinhaus, K. A., Uhrich, S. B., OSullivan, C. K., Resta, R. G., Lochner-
Doyle D. (1995): Recommendations for standardized human pedigree nomenclature.
Pedigree standardization task force of the national society of genetic counselors. Am. J. Hum.
Genet. 56:745–752. URL: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1801483/
Beris, P., Darbellay, R. and Extermann, P. (1995): Prevention of beta-thalassaemia major
and Hb Bart’s hydrops fetalis Syndrome. Seminars in Hematol. 32: 244-261.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
126
Bernini, L. F. (2001): Geographic distribution of á thalassemia: In Steinberg MH, Forget B,
Higgs DR, Nagel RL, eds. Disorders of hemoglobin. Genetics, pathophysiology and clinical
management. Cambridge: Cambridge Univ. Press. Pp 878–894.
Berry, C. L. and Marshall W. C. (1967): Iron distribution in the liver of patients with
thalassemia major. Lancet. 1031-1033.
Bijayini Behera., Purva Mathur., Kamran Farooque., Vijay Sharma., Nidhi Bhardwaj.
and Yashwant K. Thakur. (2010): Carrier screening for thalassemia and
hemoglobinopathies in Canada. JOINT SOGC–CCMG. Ind. J. Pediatr. 77: 807-808. URL:
http://medind.nic.in/icb/t10/i7/icbt10i7p807.pdf
Bianca, Maria Ricerca, Arturo, Di Girolamo and Deborah, Rund. (2009): Infections in
Thalassemia and Hemoglobinopathies: Focus on Therapy-Related Complications. Medit. J.
Hemat Infect. Dis. 1(1):
Birgens, H. (2000): Screening for hemoglobinopathies at a knowledge center in Copenhagen
resources should be allocated to solve a growing health problem in the Nordic countries.
Lakartidningen. 97: 2752–2754.
Black, J., Hommel, M., Snounou, G. and Pinder, M, (1994): Mixed infections with
Plasmodium falciparum and P. malariae and fever in malaria. Lancet. 343: 1095.
Blumberg, N. and Gettings K. F. (2003): WBC reduction of RBC transfusions is associated
with decreased incidence of RBC alloimmunization. Transfusion. 43: 945-52.
Boone, K. E. and Watters, D. A. (1995): The incidence of malaria after splenectomy in
Papua New Guinea. Br. Med. J. 311(7015): 1273.
Bonani, S. A. and Bahador, A. (1994): Management of thalassemia major by partial
splenectomy. Pediatr. Surg. Int. 9: 350-352.
Borgna-Pignatti C., Vergine, G., Lombardo, T., Cappellini, M. D., Cianciulli, P.,
Maggio, A., Renda, D., Lai, M. E., Mandas, A., Forni, G., Piga, A. and Bisconte, M. G.
(2004): Hepatocellular carcinoma in the thalassemia syndromes. Br. J. Haematol. 124: 114-
117.
Bothwell, T. H., Charlton, R. W. et al. (1979): Iron metabolism in man. Oxford, Blackwell
Scientific Publications.
Bradford, W. L. and Dye, J. (1936): Observations on the morphology of the crythmytes in
Mediterranean disease thalassemia (Erythtoblastic anemia of Cooley). J. Pediatr. 9: 3 12-13.
Brecher, G. and Cronkite, E. P. (1950): Morphology and enumeration of human blood
platelets. J. Appl. Physiol. 3: 365.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
127
Bruria Freidman, Asher Tal, Josef Kapelushnik. (2003): Sleep disruption and objective
sleepiness in children with thalassemia and congenital dyserythropoietic anemia. Arch.
Pediatr. Adolesc. Med. 157: 1-7.
Buzzal.com, (2011): URL:http://www.buzzle.com/articles/thalassemia-symptoms.html. (Last
Accessed March, 2011).
Caffey, (1937): The skeletal changes in the chronic hemolytic anemias. Am. J. Roentgenol.
Radium Ther. Nuclear Med. 37: 293-324.
Caminopetros, J. (1938): Recherché sur I’anemie erythroblastique infantile des peoples de
la Mediterranee del la maladie. Ann. Med. 43: 104-125.
Canatan, D., Ratip, S., Kaptan, S. and Cosan R. (2003): Psychosocial burden of b-
thalassemia major in Antalya, South Turkey. Soci. Sci. Med. 56: 815-819.
Cappellini, M. D., Bejaoui, M., Agaoglu, L., Canatan, D., Capra, M., Cohen, A.,
Drelichman, G., Economou, M., Fattoum, S., Kattamis, A., Kilinc, Y., Perrotta, S., Piga,
A., Porter, J. B,, Griffel, L., Dong, V., Clark, J. and Aydinok Y. (2011): Iron chelation
with deferasirox in adult and pediatric patients with thalassemia major: efficacy and safety
during 5 years' follow-up. Blood. 118(4): 884-893.
Cappellini, N., Cohen, A., Eleftheriou, A., Piga, A. and Porter, J. (2000): Eds. Guidelines
for the clinical management of thalassemia. Nicosia, Cyprus: Thalassemia International
Federation. Available at http://www.thalassaemia.org.cy/Publications.htm
Cappellini, M. D., Cohen, A., Piga, A., Bejaoui, M., Perrotta, S., Agaoglu, L., Aydinok,
Y., Kattamis, A., Kilinc, Y., Porter, J., Capra, M., Galanello, R., Fattoum, S.,
Drelichman, G., Magnano, C., Verissimo, M., Athanassiou-Metaxa, M., Giardina, P.,
Kourakli-Symeonidis, A., Janka-Schaub. G., Coates. T., Vermylen, C., Olivieri, N.,
Thuret, I., Opitz, H., Ressayre-Djaffer, C., Marks, P. and Alberti, D. (2006): A phase 3
study of deferasirox (ICL670), a once-daily oral iron chelators, in patients with beta-
thalassemia. Blood. 107:3455-3462.
Cappellini, M. D., Robbiolo, L., Bottasso, B. M., Coppola, R., Fiorelli, G. and Mannucci,
A. P. (2000a): Venous thromboembolism and hypercoagulability in splenectomized patients
with thalassemia intermedia. Br. J. Haematol. 111: 467-473.
Cappellini Maria-Domenica., Alan Cohen., Androulla Eleftheriou., Antonio Piga., John
Porter., Ali Taher., et al. (2008): Guidelines for clinical management of the thalassemia,
Revised Edition. Thalassemia Int. Fed. Nicosia, Cyprus.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
128
Caughey, Aaron B., Hopkins, Linda M. and Norton, Mary E. (2006): Chorionic villus
sampling compared with amniocentesis and the difference in the rate of pregnancy loss.
Obst. Gynecol. 108(3):612-616.
Cao, A. and Galanello, R. (2010): Beta-thalassemia. Genet Med. 12(2): 61-76.
Choudhury, N. J. et al., (1990): Post-transfusion malaria in thalassaemia patients. Blut. 61:
314–316.
Choudhry, V. P., Lal, A., Pati, H. P. and Arya, L. S. (1997): Hematological responses to
hydroxyurea therapy in multi transfused thalasaemic children. Ind. J. Pediatr. 64: 395-398.
Chouhan, D. M. (1983): The thalassaemia syndromes in India. Ind. J. Haematol. 1:17.
Cimaz, R., Mensi, C., D'Angelo, E., Fantola, E., Milone, V., Biasio, L. R., Carnelli, V.
and Zanetti, A. R. (2001): Safety and immunogenicity of a conjugate vaccine against
haemophilus influenza type b in splenectomized and nonsplenectomized patients with Cooley
anaemia. J. Infect. Dis. 183(12): 1819-1821.
Cohen, A., Markenson, A. L. and Schwarz, E. (1980a): Transfusion requirements and
splenectomy in thalassemia major. J. Pediatr. 97: 100-102.
Cohen, A. R., Glimm, E. and Porter, J. B. (2008): Effect of transfusional iron intake on
response to chelation therapy in beta-thalassemia major. Blood. 111: 583–587.
Colah, R., Surve, R., Nadkarni, A., Gorakshakar, A., Phanasgaonkar, S., Satoskar P.
and Mohanty, D. (2005): Prenatal diagnosis of sickle syndromes in India: dilemmas in
counseling. Prenat. Diagn. 25(5): 345-349.
Cooley, T. B. and Lec, P. (1925): A series of cases of splenomegaly in children with anemia
and peculiar bone changes. Trans. Am. Pediatr. Soc. 37: 29.
Cooley, T. B. (1927): Von Jaksch’s anemia. Am. J. Dis. Child. Chicago. 33: 786.
Cooley's Anemia Foundation. (2010): http://www.thalassemia.org (Last Accessed
December, 2010).
Costin, G, Kogut, M. D., Hyman, C. B. and Ortega, J. A. (1979): Endocrine abnormalities
in thalassaemia major. Am. J. Dis. Child. 133: 497.
Coulter, W.H. (1956): High speed automatic blood cell counter and cell size analyser. Proc.
Nat. Electronics Conference. 12: 1034-1042
Cunningham, M. J., Macklin, E. A., Neufeld, E. J. and Cohen, A. R. (2004):
Complications of β-thalassemia major in North America. Blood. 104: 34-39.
Curtain, C. C., Kidson, C., Gajdusek, D. C. and Gorman, J. G. (1962): Distribution
pattern, population genetics and anthropological significance of thalassemia and abnormal
hemoglobins in Melanesia. Am. J. Phys. Anthropol. 20: 475.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
129
Darbari, D. S., Kple-Faget, P., Kwagyan, J., Rana, S., Gordeuk, V. R. and Castro, O.
(2006): Circumstances of death in adult sickle cell disease patients. Am. J. Hematol. 8: 858-
863.
Dauphinee, D. and Langley, G. R. (1967): Thalassemia in Canadians. Can. Med. Ass. J.
96: 309.
Deugnier, Y., Turlin, B., Ropert, M., Cappellini, M. D., Porter, J. B., Giannone, V.,
Zhang, Y., Griffel, L. and Brissot, P. (2011): Improvement in liver pathology of patients
with beta-thalassemia treated with Deferasirox for at Least 3 Years. Gastroenterol.
Di Marco. V., Capra, M., Gagliardotto, F. et. al. (2008): Liver disease in chelated
transfusion-dependent thalassemic: the role of iron overload and chronic epatitis C.
Haematologica. 93:1243-1246.
Dover, A. S. and Schultz, M. G. (1971): Transfusion-induced malaria. Transfusion.
11(6):353-357.
Drew, S. J. and Sach, S. A. (1997): Management of thalassemia induced skeletal facial
deformity. J. Oral Maxfac. Surg. 55(1): 1331-1339.
Dumars, K. W., Boehm, C., Eckman, J. R., Giardina, P. J., Lane, P. A. and Shafer, F. E.
(1996): For the Council of Regional Networks for Genetic Services (CORN). Practical guide
to the diagnosis of thalassemia. Am. J. Med. Genet. 62: 29–37.
eMedicineHealth (2011): Enlarged splee. URL-http://www. emedicinehealth. com /
enlarged_spleen_ splenomegaly/article_em.htm
Emedicinehealth.com.(2006): URL:http://www.emedicinehealth.com/malaria/page2_em.
htm (Last Accessed August, 2011).
Elena Fabbri., Gian Luca Forni., Giulia Guerrini. and Caterina Borgna-Pignatti.
(2009): Pseudoxanthoma elasticum-like syndrome and thalassemia: An update. Dermatol.
Online J. 15(7). URL: http://dermatology.cdlib.org/1507/case_reports/pxe/fabbri.html
El-Hazmi, M. A. and Warsy, A.S. (1999): Appraisal of sickle-cell and thalassaemia genes
in Saudi Arabia. East Mediterr. Health J. 5(6):1147-1153.
Elliott Vichinsky. and Laurice Levine. (2008): Standards of care guidelines for
thalassemia. Children’s Hospital and Res. Center Oakland.
Eshghi, P., Alavi, S., Ghavami, S. and Rashidi, A. (2007): Growth impairment in beta-
thalassemia major: the role of trace element deficiency and other potential factors. J. Pediatr.
Hematol. Oncol. 29(1): 5-8.
European Committee for Clinical Laboratory Standards. (1984): Standard for specimen
collection part I: Blood Containers. ECCLs Documents. Beuth Verlag. Berlin. 1(1): 1-6.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
130
Fabrice Danjou., Franco Anni., Lucia Perseu., Stefania Satta., Carlo Dessi'., Maria
Eliana Lai., Paolo Fortina., Marcella Devoto and Renzo Galanello. (2012): Genetic
modifiers of beta-thalassemia and clinical severity as assessed by age at first transfusion.
Haematol. 053504.
Fawdry, A. L. (1944): Erythroblastic anaemia of childhood (Cooley’s anaemia) in Cyprus.
Lancet. 1: 171–176.
Ferrara, M., Matarese, S. M., Borrelli, B., Perrotta, A., Simeone, G., Greco, N., D.
Iarussi and Esposito, L. (2004): Cardiac involvement in beta-thalassemia major and beta-
thalassemia intermedia. Hemoglobin. 28(2): 123-129.
Fessas, P. (1987): Prevention of thalassemia and haemoglobin S syndromes in Greece. Acta
Haematol. 78: 168–172.
Filosa, A., Di Maio S., Vocca, S., Saviano, A., Esopotito, G. and Pagono, L. (1997):
Longitudinal monitoring of bone mineral density in thalassemia patients: Genetic structure
and osteoporosis. Acta Pediatr. 86: 342-346.
Flint, J., Harding, R. M., Boyce, A. J. and Clegg, J. B. (1998): The population genetics of
the haemoglobinopathies. Baillieres Clin. Haematol. 11: 1–51.
Freundlich, M. H. and Gerarde, H. W. (1963): A new, automatic, disposable system for
blood counts and haemoglobin. Blood. 21: 648.
Fuchsa, G. J., Tienboona, P., Khaledc, M. A., Nimsakula, S., Linpisarna, S., Faruquec,
A. S. G., Yutrabootra, Y., Dewiera, M. and Suskindb R. M. (1997): Nutritional support
and growth in thalassaemia major. Arch. Dis. Child. 76: 509-512.
Fuchs, G. J., Tienboon, P., Linpisarn, S., Linpisarn, S., Nimsakul, S., Leelapat, P.,
Tovanabutra, S., Tubtong, V., DeWier, M. and Suskind, R. M. (1996): Nutritional
factors and thalassemia major. Arch. Dis. Child. 74(3):224-227.
Galanello, R. and Origa, R. (2008): Once-daily oral deferasirox for the treatment of
transfusional iron overload. Ex. Rev. Clin. Pharma. 1:231-240.
Galanello and Origa (2010): Beta-thalassemia. Orphanet J. Rare Dis. 5:11.
Galanello, R., Piga, A., Forni, G. L. et al. (2006): Phase II clinical evaluation of
deferasirox, a once-daily oral chelating agent, in pediatric patients with beta-thalassemia
major. Haematol.91:1343–1351.
Nishi, Madan., Satendra Sharma., Sood, S. K., Roshan, Colah and Bhatia, H. M. (2010):
Frequency of β-thalassemia trait and other hemoglobinopathies in northern and western India.
Ind. J. Human Genetics. 16:116-125.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
131
GeneReviews. (2009): http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=gene&part=a-
thal.
Ghazi Omar Tadmouri, B. S. (1994): In Agricultural Engineering, the American University
of Beirut, MS. in Biology, Boðaziçi Univ.
Ghosh, K., Daar, S., Hiwase, D. and Nursat N. (2000): Primary pseudomonas meningitis in
adult, multitransfused thalassemia major patient. Haematol. 30: 69-72.
Giardina., Vincenzo Pascali. (1999): Resistance to Falciparum malaria in α-thalassemia,
oxidative stress, and hemoglobin oxidation. Am. J. Physical Anthropol. 109(2): 269–273.
Giardine, B., Van Baal, S., Kaimakis, P., Riemer, C., Miller, W., Samara, M., Kollia,
P., Anagnou, N. P., Chui, D. H., Wajcman, H., Hardison, R. C. and Patrinos, G. P.
(2007): HbVar database of human hemoglobin variants and thalassemia mutations. Hum.
Mutat. Update. 28(2): 206.
Gupta, R., Singh, B., Rusia, U. and Goyal, S. (2010): Red cell alloimmunization in
routinely transfused patients of beta thalassemia major. Int. J. Blood Trans. Ind. 1(1): 1-4.
Hahalis, G., Alexopoulos, D., Kremastinos, D. T. and Zoumbos, N. C. (2005): Heart
failure in beta thalassemia syndromes: a decade of progress. Am. J. Med. 118: 957-967.
Hamilton R. W. Schwartz E. Atwater J. and Ersler A. J. (1971): Acquired hemoglobin H-
disease N. Eng. J. Med. 285: 1217-1221.
Height to Weight Ratio Chart . (2007): Disabled World. URL: http://www.disabled-
world.com/artman/publish/height_weight.shtml">Height to Weight Ratio Chart</a>
Higgs, D. R., Thein, S. L. and Woods, W. G. (2001): The molecular pathology of the
thalassaemias. In: Weatherall DJ, Clegg B, Eds. The thalassemia syndromes. 4th ed. Oxford,
England: Blackwell Science, 133-191.
Hira Tahir., Syeda Amna Shahid. and Khawaja Tahir Mahmood. (2011): Complications
in thalassemia patients receiving blood transfusion. J. Biomed. Sci. Res. 3(1): 339-346.
Hossain Uddin Shekhar, Yearul Kabir, Mosharaf Hossain, Mesbah Uddin, Kaniz-
Khatun-E-Jannat, Hossain, S. and Shahjalal, H. (2007): Blood transfusion-mediated viral
infections in thalassemic children in Bangla. J. Med.l Sci. 7:131-135.
International Committee for Standardization in Haematology. (1983): Protocol for
evaluation of automated cell counters. Clin. Lab. Haematol. 6: 69.
Irwin Gross (2010): Laboratory studies in the diagnosis of iron deficiency, Latent iron
deficiency and iron deficient Erythropoiesis . Eastern Maine Medical Center,
URL:http://www.iron.sabm.org

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
132
Itano, H. A. and Pouling, L. (1961): Thalassemia and abnormal human hemoglobin. Nature.
191: 398-399.
Jamal, R. (2004): The burden of thalassemia in Malaysia. Kuala Lumpur. First Nat.
Thalassemia Seminar. May 8-9.
James, E. B., Vreman, H. J., Wong, R. J., Stevenson, D. K. and Vichinsky, E. (2010):
Elevated exhaled carbon monoxide concentration in hemoglobinopathies and its relation to
red blood cell transfusion therapy. Pediatr. Hematol. Oncol. 27(2):112-121.
Jensen, C. E., Tuck, S. M., Agnew, J. E., Koneru, S., Morris, R. W., Yardumian, A., et
al. (1998): High prevalence of low bone mass in thalassemia major. Br. J. Hematol. 103:
911-915.
Joishy, S. K. and Lopez, C. G. (1980): Transfusion-induced malaria in a splenectomized β-
thalassemia major patient and review of blood donor screening methods. Am. J. Hematol.
8: 221–229.
Joy, Ho P. and Thein, S. L. (2000): Gene regulation and deregulation: a β globin
perspective. Blood Rev. 14: 78-93.
Kan, Y. W., Nathan, D. G., Cividalii, G. and Frigoletto, F. (1974): Intrauterine diagnosis
of thalassemia. Ann. N. Y. Acad. Sci. 232: 145-151.
Kan, Y. W., Dozy, A. M., Trecartin, R. and Todd, D. (1977): Identification of a
nondeletion defect in a-thalassemia. N. Engl. J. Med. 297: 1081-1084.
Kaplan, E., Werther, R. and Castano, F. A. (1964): Dental and oral findings in Cooley’s
anemia: a study of fifty cases. Ann. N. Y. Acad. Sci. 119: 664–666.
Kattamis, C., Lagos, P. and Langona, E. (1979): Chelation therapy and ferritin levels in
patients with homozygous β-thalassemia. In : The management of Genetic Disorders, ed by
C. Papadatos and C. Bartsokas. Alan R. Liss Inc., New York. Pp 351-359.
Khattak, M. F. and Saleem, M. (1992): Prevalence of heterozygous beta thalassemia in
Northern areas of Pakistan. J. Pak. Med. Asso. 42: 32-34.
Kheradpir, M. H. and Albouyeh, M. (1985): Partial splenectomy in the treatment of
thalassemia major. Z. Kinderchir. 40: 195-198.
Khurana, A., Katyal, S. and Marwaha, R. K. (2006): Psychosocial Burden In
Thalassemia. Ind. J. Pediatr. 73: 877-880.
Kitchen, A. D. and Chiodini, P. L. (2006): Review malaria and blood transfusion. Vox
Sang. 90(2):77-84.
Kliegman, R. M. and Behromon, R. E. (2002): Nelson Essential of Pediatrics. 4th ed.
Saunders Co. 662-663.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
133
Kor-anantakul, O., Suwanrath, C. T., Leetanaporn, R., Suntharasaj, T., Liabsuetrakul,
T. and Rattanaprueksachart, R. (1998): Prenatal diagnosis of thalassemia in
Songklanagarind Hospital in southern Thailand. Southeast Asian J. Trop. Med. Public Health.
29: 795–800.
Kremer, B. H. and Gotzfried, H. F. (1986): Orofacial changes in beta-thalassemia major.
Dtsch Z Mund Kiefer Gesichtschir.10(5): 382-390.
Krishnamurti, L. (2000): Few reports of hemoglobin E/beta-thalassemia in Northeast India:
under diagnosis or complete exclusion of beta-thalassemia by hemoglobin E. J. Pediatr.
Hematol. Oncol. 22(6): 558-563.
Kumar, R. M., Riak, D. E. and Khurana, A. (1997): Beta thalassemia major and successful
pregnancy. J. Reprod. Med. 42: 294-298.
Kumar, S., Rana, M., Handoo, A., Saxena, R., Verma, I. C., Bhargava, M. and Sood, S.
K. (2007): Case report of HbC/beta(0)-thalassemia from India. Int. J. Lab. Hematol. 9(5)
:381-385.
Kunkel, H. G., Ceppellini, R.. Muller-Ederhard, U. and Wolf, J. (1957): Observations on
the minor basic hemoglobin components in the blood of normal individuals and patients with
thalassemia. J. Clin. Invest. 3: 1615-1616.
Lange, K., Westlake, J. and Spence, M. A. (1976): Extensions to pedigree analysis. III.
Variance components by the scoring method. Ann. Hum. Genet. 39(4): 485-491.
Laopodis, V., Kritikos, E., Rizzoti, L., Stefanidis, P., Klonaris, P. and Tzardis, P.
(1998): Laparoscopic splenectomy in beta-thalassemia major patients. Advantages and
disadvantages. Surgical Endoscopy. 12(7): 944-947.
Leonardi, B., Margossian, R., Colan, S. D. and Powell, A. J. (2008): JACC Cardiovasc.
Imaging. 1(5): 572-578.
Leung, T. N., Lau, T. K. and Chung, T. K. H. (2005): Thalassemia screening in pregnancy.
Curr. Opin. Obstet. Gynecol. 17: 129–134.
Lewis, S. M. Wardle, J., Cousins, S. and Skelly, J.V. (1979): Platelet counting-
development of a reference method and a reference preparation. Clin. Lab. Haematol. 1:
227.
Linda J. Vorvick. (2010): http://www.nlm.nih.gov/medlineplus/thalassemia.html, U.S.
National Library of Medicine (Last seen July, 2011).
Lo, S. C, Chang, J. S., Lin, S. W., and Lin, Dong-Tsamn. (2005): Platelet
alloimmunization after long-term redcell transfusion in transfusion-dependent thalassemia
patients. Transfusion. 45: 761-765.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
134
Lodish, H. F. and Jacobsen, M. (1972): Regulation of hemoglobin synthesis. Equal rates of
translation and termination of α- and β-globin chains. J. Biol. Chem. 247: 3622-3629.
Lookopoulos, D. and Kollia, P. (2001): Worldwide distribution of â Thalassemia: In:
Steinberg M. H, Forget B, Higgs D.R, Nagel R.L, eds. Disorders of hemoglobin. Genetics,
pathophysiology, and clinical management. Cambridge: Cambridge University Press. Pp
861–877.
Low, L. C. K. (1997): Hormone and growth abnormalities in untreated and treated beta
thalassemia. J. Pediatr. Endocrinol. Metab. 10: 175-180.
Luzzi, G. A., Merry, A. H., Newbold, C. I., Marsh, K., Pasvol, G, et al. (1991): Surface
antigen expression on Plasmodium falciparum-infected erythrocytes is modified in alpha- and
beta-thalassemia. J. Exp. Med. 173: 785–791.
Madan N Sharma., S. Rusia U., Sen S. and Sood S. K. (1998): Beta thalassemia mutation
in Northern India (Delhi). Ind. J. Med. Res. 107: 134-141.
Maggio, A., D'Amico G., et al. (2002): Deferiprone versus deferoxamine in patients with
thalassemia major: a randomized clinical trial. Blood Cells Mol. Dis. 28(2): 196–208.
Mahadik, C., Kapadia, C., Yagnik, H., Sukumaran, P. K. and Merchant, S. (1986): One
tube osmotic fragility as a useful screening test for thalassemia carriers- A field experience.
Ind. J. Hematol. 4: 62-64.
Maheswari, M., Arora, S, Kabra, M. and Menon, P. S. N. (1999): Carrier screening and
prenatal diagnosis of b-thalassemia. Ind. Pediatr. 36: 1119-1125.
Maram, E. S., Amiri, Z. M. and Haghshenas, M. (2000): Effectiveness of osmotic fragility
screening with varying saline concentrations in detecting thalassemia trait. Ir. J. Med. Sci. 25:
56-58.
Marion Phylipsen., Jan Traeger-Synodinos., Martijn van der Kraan., Peter van Delft.,
Greet Bakker., Mariska Geerts., Emmanuel Kanavakis., Alexandra Stamoulakatou.,
Markissia Karagiorga., Piero C. Giordano and Cornelis L. Harteveld. (2012): A novel
0-thalassemia deletion in a Greek patient with HbH disease and β-thalassemia trait. Europ.
J. Haematol. 88(4): 356–362.
Marwah, R. K, and Lal, A. (1994): Present status of hemoglobinopathies in India. Ind.
Pediatr. 31: 267-271.
Masaya, Oi., Naoko Nagano., Tadamasa Miyauchi., Noboru Ishikawa. and Hitoshi
Kasegawa. (2010): Aortic valve replacement in a patient with alpha-thalassemia Tadashi
Omoto, Takeo Tedoriya, Yasuyuki Kondo, Hirofumi Izuka. Ann. Thorac. Cardiovasc. Surg.
16(5): 365-366.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
135
Masera, G., Monguzzi, W., Tornotti, G., Lo Iacono, B., Pertici, S. and Spinetta, J.
(1990): Psychosocial support in thalassemia major: Monza Center's experience. Haematol.
75(5): 181-190.
May, J., Evans, J. A., Timmann, C., Ehmen, C., Busch, W., Thye, T., Agbenyega, T.
and Horstmann, R. D. (2007): Hemoglobin Variants and Disease Manifestations in
Severe Falciparum Malaria. J. Am. Med. Asso. 297(20): 2220-2226.
Mehta, B. C. (2002): NESTROFT: A screening test for beta thalassemia trait. Ind. J. Med.
Sci. 56: 537-545.
Mehta, B. C. and Pandya, B. G. (1987): Iron status of beta thalassemia carriers. Am. J.
Hematol. 24: 137–141.
Mendelian Inheritance in Man. (1999): Method of estimation of donor ’s haemoglobin by
copper sulphate method. Technical Manual of American Association of Blood Banks, 13th
edition. Pp 711-712. (URL: http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=141900).
Modell, B., Khan, M. and Darlison, M. (2000): Survival in beta-thalassemia major in the
UK: Data from the UK Thalassemia register. Lancet. 355: 2051-2052.
Modell, B. and Petrou M. (1983): The problem of hemoglobinopathies in India. Ind. J.
Haematol. 1-5.
Modell, C. B. (1976): Management of thalassemia major. Br. Med. Bull. 32: 270-276.
Modiano, G., Morpurgo, G., Terrenato, L., Novelletto, A., Di Rienzo, A., et al. (1991):
Protection against malaria morbidity: Near-fixation of the alpha-thalassemia gene in a
Nepalese population. Am. J. Hum. Genet. 48: 390–397.
Mohammad Reza Rabie., Narges Mirbehbahani. and Azam Jahazi. (2010): Frequency
of beta thalassemia trait and carrier in Gorgan, Iran. Flora Vafai. Pak. J. Med. Sci. 26: 40-42.
Mohga Shfik., Hayat Sherada., Yehia Shaker., Mie Afify., Howayda Ali Sobeh. and
Samar Moustafa. (2011): Serum levels of cytokines in poly-transfused patients with beta-
thalassemia major: Relationship to splenectomy. J. Am. Sci. 10(10): 20.
Muhammad Younus., Khalid Hassan., Nadeem Ikram., Lubna Naseem., Hassan Abbas
Zaheer. and Muhammad Farooq Khan. (2004): Hepatitis C virus seropositivity in
repeatedly transfused thalassemia major patients. Int. J. Pathol. 2(1):20-23.
NACA (2008): Safe Blood Transfusion. The National AIDS Coordinating Agency. Gaborone,
Botswana.
Nadeem Ikram, Khalid Hassan, Muhammad Younas, Samina Amanat. (2004): Ferritin
levels in patients of beta thalassaemia major. Int. J. Pathol. 2(2):71-74.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
136
Naithani, R., Chandra, J. and Sharma, S. (2005): Safety of oral iron chelator desferiprone
in young thalassemics. Eur. J. Hematol. 74: 217-220.
Najem, G. R. and Sulzer, A. J. (1976): Transfusion-induced malaria from an asymptomatic
carrier. Transfusion. 16(5):473-476.
Nathan, D. G. and Gunn, R. B. (1966): Thalassemia: the consequences of unbalanced
hemoglobin synthesis. Am. J. Med. 41: 815-830.
Naveed, M. (1995): Clinical, Biochemical and molecular characterization of thalassemia
syndromes in Uttar Pradesh, India. PhD thesis; Sanjay Gandhi Postgraduate Institute of
Medical Sciences, Lucknow.
Neeraj Shah, Anupa Mishra, Dhaval Chauhan, Vora, C. and Shah, N. R. (2010): Study
on effectiveness of transfusion program in thalassemia major patients receiving multiple
blood transfusions at a transfusion centre in Western India. Asian J. Transfus. Sci. 4(2): 94–
98.
Neufeld, E. J. (2006): Oral chelators’ deferasirox and deferiprone for transfusional iron
overload in thalassemia major: new data, new questions. Blood. 107:3436–3441.
Nittis, S. and Spilopulos, G. (1937): Similarity of erythroblastic anaemia and chronic or
congenital malaria. Am. J. Dis. Child. 54: 60-72.
O'Donnell, A., Premawardhena, A., Arambepola, M., Samaranayake, R., Allen, S. J.,
Peto, T. E. A., Fisher, C. A., Cook, J., Corran, P.H., Oliveri, N. F. and Weatherall, D. J.
(2009): Interaction of malaria with a common form of severe thalassemia in an Asian
population. Proceedings of the National Academy of Sciences. URL: http:// www.pnas.org.
106(44): 18716-18721.
Olivieri, N. G. and Brittenham, G. M. (1997): Iron-chelating therapy and the treatment of
thalassemia. Blood. 89:739-761.
Olivieri NF. (1999); The β-Thalassaemias. N. Engl. J. Med. 341(2): 99-109.
Pakbaz, Z., Treadwell, M., Kim, H. Y., Trachtenberg, F., Parmar, N., Kwiatkowski, J.
L., Cunningham, M. J., Martin, M., Sweeters, N., Neufeld, E. J., Giardina, P. J.,
Olivieri, N., Yamashita, R. C. and Vichinsky, E. (2010): Education and employment status
of children and adults with thalassemia in North America. Pediatr. Blood Cancer. 55(4): 678-
683.
Panigrahi, I., Ahmed, R. P., Kannan, M., Kabra, M., Deka, D. and Saxena, R. (2005):
Cord blood analysis for prenatal diagnosis of thalassemia major and hemophilia. Ind.
Pediatr.42: 577- 581.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
137
Panos Englezos. (2005): Prevention of Thalassaemias and Other Haemoglobin Disorders.
Published by Thalassaemia International Federation, Cyprus, 2.
Parfrey, P. S., Barnett, M., Sachs, J. A., Pollock, D. J. and Turnbull, A. L. (1981): Iron
overload in beta-thalassaemia minor. A family study. Scand. J. Haematol. 27: 294–302.
Patil Shilpa. (2006): Clinical and radiological study of oro-facial manifestations in
Thalassaemia. Dissertation, Rajiv Gandhi University of Health Sciences, Karnataka,
Bangalore.
Pauling, L., Itano, H. A., et al. (1949): Sickle cell anemia a molecular disease. Science.
110(2865): 543-548.
Pennell, D. J., Berdoukas, V., Karagiorga, M., Ladis, V., Piga, A., Aessopos, A.,
Gotsis, E. D., Tanner, M. A., Smith, G. C., Westwood, M. A., Wonke, B. and Galanello,
R. (2006): Randomized controlled trial of deferiprone or deferoxamine in beta-thalassemia
major patients with asymptomatic myocardial siderosis. Blood. 107: 3738–3744.
Phaedon, F. (1987): Prevention of thalassemia and haemoglobin S syndromes in Greece.
Acta Haematol. 78: 168–172.
Phrommintikul, A., Sukonthasarn, A., Kanjanavanit, R. and Nawarawong, W. (2006):
Splenectomy: a strong risk factor for pulmonary hypertension in patients with thalassemia.
Heart. 92(10): 1467-1472.
Piga, G., Donato, G. and Monasterolo, G. (2001): Administration and effectiveness of
desferrioxamine. Presented at the Eighth International Conference on Thalassemia and the
Hemoglobinopathies. Athens Greece.
Piga, A., Galanello, R., Forni, G. L., Cappellini, R. O., Zappu, A., Donato, G., Bordone,
E., Lavagetto, A., Zanaboni, L., Sechaud, R., Hewson, N., Ford, J. M., Opitz, H. and
Alberti, D. (2006): Randomized phase II trial of deferasirox (Exjade, ICL670), a once-daily,
orally-administered iron chelators, in comparison to deferoxamine in thalassemia patients
with transfusional iron overload. Haematol. 91: 873–880.
Piomelli, S., Karpatkin, M. H., Arzanian, M. and Zamani M. H., Becker. and Geneiser,
N. (1974): Hypertransfusion regimen in patients with Cooley's anemia. Ann. N.Y. Acad. Sci.
232: 186-192.
Piplani, S. (2000): Hemoglobin E disorders in North East India. J. Ass. Physicians Ind. 48:
1082-1084.
Porter, J. B. (2001): Practical management of iron overload. Br. J. Haematol. 115(2):239-
252.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
138
Prati, D. (2000): Benefits and complications of regular blood transfusion in patients with
beta thalassemia major. Vox-Sang. 79(3): 129-137.
Pratima Raju., Minal Chaudhary., Vijay Wadhwan. (2009): Evaluation of Oral
manifestations as correlates in Thalassemia major cases in current dental practice in Central
part of India. The Internet J. Hematol. 6(2). URL:http://www. ispub.com/
journal/the_internet_journal_of_hematology/volume_6_number_2_37/article/evaluation-of-
oral-manifestations-as-correlates-in-thalassemia-major-cases-in-current-dental-practice-in-
central-part-of-india.html
Pratt, S. C., Daly, M. J. and Kruglyak, L. (2000): Exact multipoint quantitative-trait
linkage analysis in pedigrees by variance components. Am. J. Hum. Genet. 66(3): 1153-1157.
Propper, R. D., Button, L. N. and Nathan, D. G. (1980): New approaches to the
transfusion management of thalassemia. Blood. 55: 55-60.
Pusaksrikit, S., Isarangkura, P. and Hathirat, P. (1987): Occlusion of the teeth in
thalassemic patients. Birth Defects Orig. Artic Ser. 23: 429-433.
Qamruz Zaman and Salahuddin. (2006): Association between the education and
thalassemia: A statistical study. Pak. J. Stat. Oper. Res. 2(2): 103-110.
Quais Mujawar., Sadashiva Ukkali., Malagi, N. N. and Thobbi, A. N. (2009):
Haemoglobin E- beta thalassaemia. A case report from Bijapur, South India. Al Ameen J.
Med. Sci. 2 (1): 82 -84.
Rachmilewitz, E. and Schrier, S. L. (2001): Pathophysiology of β thalassemia. In disorders
of hemoglobin: genetics, pathophysiology, and clinical management. M.H. Steinberg, B.G.
Forget, D.R. Higgs, and R.L. Nagel, editors. Cambridge University Press. Cambridge, United
Kingdom. Pp 233–251.
Rahman, M. and Lodhi, Y. (2004): Prospects and future of conservative management of
beta thalassemia major in a developing country. Pak. J. Med. Sci. 20: 105-112.
Raj, A. A., Subramaniam, T., Raghuraman, S. and Abraham, P. (2001): Evaluation of an
indigenously manufactured rapid immunochromatographic test for detection of HBsAg. Ind.
J. Pathol. Microbiol. 44(4): 413–414.
Rajendran, R. and Sivapathasundaram, B. (2007): Diseases of blood and blood-forming
organs. In: Shafer’s textbook of Oral Pathology, 5th edition. Elsevier publications. Pp 1049-
1050.
Renzo Galanello., Androulla Eleftheriou., Joanne Traeger-Synodinos., John Old., Mary
Petrou. and Michael Angastiniotis. (2005): Prevention of thalassaemias and other
haemoglobin disorders. Thalassaemia International Federation, Nicosia, Cyprus,

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
139
Rietti, F. (1925): Sugli itteri emolitici primitivi. Atti. Accad. Sci. Mediche e Naturali.
Ferrara. 2-14.
Riewpaiboo, A., Bunyadharokul, S., Chaikledkaew, U. and Torcharus, K. (2010):
Budget impact of the thalassemia management under the national health security scheme in
Thailand. Mahidol Univ. J.Pharmaceut. Sci. 37(1-2): 28-39.
Sharma R. N. and Pancholi, S. S. (2010): Oral iron chelators: A new avenue for the
management of thalassemia major. J. Curr. Pharmaceut. Res. 1: 1-7.
Roth, E. F., Shear, H. L., Costantini, F., Tanowitz, H. B. and Nagel, R. L. (1998):
Malaria in beta-thalassemic mice and the effects of the transgenic human beta-globin gene
and splenectomy. J Lab. Clin. Med. 111(1):35-41.
Roy, R. N., Banerjee, D., Chakraborty, K. N. and Basu, S. P. (1971): Observations on
radiological changes of bones in thalassaemia syndrome. J. Ind. Med. Ass. 57(3): 90-95.
Ruffo, G. B., Borsellino, Z., Cuccia, L., Marocco, M. R., Gagliardotto, F. and Tarantino,
R. (2010): Long-term chelation therapy with deferasirox: effects on cardiac iron overload
measured by T2* MRI. Clin. Drug Investig. 30(4): 267-273.
Salehi, M. R., Farhud, D. D., Tohidast, T. Z. and Sahebjamee, M. (2007): Prevalence of
orofacial complications in iranian patients with β -thalassemia major. Ir. J. Publ. Health. 36
(2): 43-46.
Sanefuji, M., Ohga, S., Kira, R., Yoshiura, T., Torisu, H. and Hara, T. (2006):
Moyamoya syndrome in a splenectomized patient with beta-thalassemia intermedia. J. Child
Neurol. 21(1): 75-77.
Sangani, B., Sukumaran, P. K., Mahadik, C., Yagnik, H., Telang, S., Vas, F., Oberroi,
R.A., Modell, B. and Merchant, S. M. (1990): Thalassemia in Bombay: The role of medical
genetics in developing countries. Bull. WHO. 68(1): 75-81.
Sassa, S. (2004): Why heme needs to be degraded to iron, biliverdin IXalpha, and carbon
monoxide? Antioxid Redox Signal. 6(5): 819-24.
Schrier, S. L. (1997): Pathobiology of thalassemic erythrocytes. Curr. Opin. Hematol. 4(2):
75–78.
Schuette, J. L. and Uhlmann, W. R. (1998): Lessons in history: obtaining the family history
and constructing a pedigree. In: Baker DL, A guide to genetic counseling. J. Wiley and Sons.
New York.
Seed, C. R., Kitchen, A. and Davis, T. M. (2005): Review the current status and potential
role of laboratory testing to prevent transfusion-transmitted malaria. Transfus. Med. Rev.
19(3): 229-240.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
140
Seema Kapoor, and Madhulika Kabra. (2010): Newborn screening in India: Current
perspectives. Ind. Pediatr. 219(47).
Shah, A. (2004): Thalassemia Syndromes. Ind. J. Med. Sci. 58: 445-449.
Shah Dheeraj., Panna Choudhury., Dubey, A. P. (1999): Current trends in management of
the beta thalassemias. Ind. Pediatr. 36: 1229-1242.
Shaikha Salim Al-Arrayed. (2010): Beta Thalassemia Frequency in Bahrain: A Ten Year
study. Bahrain Med. Bull. 32:(2).
Sharma, B. K., Choudhury, P. and Dubey, A. P. (1990): Desferrioxamine: It's use in iron
chelation in thalassemia. Ind. Pediatr. 27: 314-319.
Shear, H. L., Grinberg, L., Gilman, J., Fabry, M. E., Stamatoyannopoulos, G.,
Goldberg, D. E. and Nagel, R. L. (1998): Transgenic mice expressing human fetal globin
are protected from malaria by a novel mechanism. Blood. 92(7): 2520-2526.
Shinton, N. K., England, J. M. E. and Kennedy, D.Y. (1982): Guidelines for evaluation of
instruments used in hematological laboratories. J. Clin. Pathol. 35: 1095.
Shivashankara, A. R., Jailkhani, R. and Kini, A. (2008): Hemoglobinopathies In Dharwad,
North Karnataka: A Hospital-Based Study. J.Clin.Diagnost. Res. 2:593-599.
Siamopoulou-Mavoidou A., Movridis, A., Galanakis, E., Vasakos, S., Fatourou, H. and
Lapatsanis, P. (1992): Flow rate and chemistry of parotid saliva related to dental caries and
gingivitis in patients with thalasaemic major. Int. J. Pediatr. Dent. 2(2): 93-97.
Singh, H., Pradhan, M., Singh, R. L., Phadke, S., Naik, S. R., Aggarwal, R. and Naik, S.
(2003): High frequency of hepatitis B virus infection in patients with β-thalassemia receiving
multiple transfusions. Vox Sanguinis. 84: 292–299.
Singh, K., Pannu M. S., Singh, P. and Singh, J. (2010). Effect of wheat grass Tablets on
the frequency of blood transfusions in Thalassemia Major. Ind. J. Pediatr. 77(1): 90-91.
Singh, R. and Venketasubramanian, N. (2004): Recurrent cerebral infarction in beta
thalassaemia major. Cerebrovasc. Dis. 17(4): 344-345.
Sirchia, G., Zanella, A., Parravicini, A., Morelati, F., Rebulla, P. and Masera, G. (1995):
Red cell alloantibodies in thalassemia major. Results of an Italian cooperative study.
Transfusion. 25: 110-112.
Smith, C. H., Erlanson, M. E., Sterin, G. and Scholman, I. (1960): The role of
spenectomy in the management of thalassemia. Blood. 15: 197-211.
Smith, C. H., Erlandson, M. E., Stern, G. and Hilgartner, M. W. (1964): Post-
splenectomy infection in Cooley’s anemia. Ann. N. Y. Acad. Sci. 119: 748-757.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
141
Smith, C. H., Scholman, I., Ando, R. E. and Stern, G. (1955): Studies in Mediterranean
(Cooley’s anemia) I. Clinical and hemato aspects of spenectomy with special reference to
fetal hemoglobin synthesis. Blood. 10: 582-599.
Somchai Insiripong., Sunya Prabriputaloong. and Nittaya Wisanuyothin. (2009):
Thalassemic mothers and their babies. Southeast Asian J. Trop. Med. Publ. Health. 40(2).
Sood, S. K., Madan, N., Colah, R., Sharma, S. and Apte, S. V. (1993): Collaborative study
on thalassemia. Report of ICMR Task Force Study, Indian Council of Medical Research,
New Delhi.
Snounou, G., Viriyakosol, S., Zhu, X. P., Jarra, W, Pinheiro, L., do Rosario, V. E.,
Thaithong, S. and Brown, K. N. (1993): High sensitivity of detection of malaria parasites
by the use of nested polymerase chain reaction. Mol. Biochem. Parasitol. 61: 315–320.
Spirito, P., Lupi, G. and Melevendi, C. (1990): Restrictive diastolic abnormalities
identified by Doppler echocardiography in patients with thalassemia major. Circulation. 82:
88-94.
Srdjan Denic, Nicolas Nagelkerke and Agarwal M. M. (2008): Consanguineous marriages
and endemic malaria: can inbreeding increase population fitness. Malaria J. 7: 150.
Sturgeon, P., Itano, H. A. and Bergren, W. R. (1955): Clinical manifestations of inherited
abnormal hemoglobin. I. The interaction of haemoglobin-S with haemoglobin D. Blood. 10:
389-396.
Sturgeon, P., Iteno, H. and Bergren, W. R. (1955a): Genetic and biochemical studies of
intermediate type of Cooley’s anemia. Br. J. Hematol. 4: 264-277.
Sturgeon, P., Itano, H. A. and Valentine, H. N. (1952): Chronic hemolytic anemia
associated with thalassemia and sickling trait. Blood. 7: 350.
Sukumaran, P.K. and Master (1973): The distribution of abnormal haemoglobins in the
Indian population. In proceedings of the First Conference of the Indian Society of Human
Genetics vol. 1: Human population genetics in India, Bombay. Orient Longman. 91-111.
Sumathy, S., Thyagarajan, S. P., Latif, R., Madanagopalan, N., Raguram, K.,
Rajasambandam, P. et al. (1992): A dipstick immunobinding enzyme-linked
immunosorbent assay for serodiagnosis of hepatitis B and delta virus infections. J. Virol.
Methods. 38(1): 145–152.
Svishcheva, G. R. (2007): Analysis of quantitative trait loci using hybrid pedigrees:
quantitative traits of animals. Genetika. 43(2): 265-275.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
142
Sylvie Langlois Jason C. Ford., Vancouver, B. C., David Chitayat. and Toronto. (2008):
Carrier screening for thalassemia and hemoglobinopathies in Canada. Joint Sogc–Ccmg
Clinical Practice Guideline. Canada.
Tabatabei, M., Kamkar, M. and Habibzadeh, M. R. (2003): Metabolic and endocrine
complications in beta-thalassemia major; a multicenter study in Tehran. Boshehr Med. J.
5(1): 72-73.
Tanner, J. M., Whitehouse, R. H. and Takaishi, M. (1966): Standards from birth to
maturity for height, weight, height velocity, and weight velocity: British children, 1965, Part
II. Arch. Dis. Child. 41: 613.
Thakur (Mahadik) C., Vaz, F., Banerjee, M., et al. (2000): Prenatal diagnosis of beta-
thalassaemia and other haemoglobinopathies in India. Prenat. Diag. 20: 194-201.
Thakemgpol, K., Fucharoen, S. et al. (1992): Liver tissue injury secondary to iron overload
in beta thalasscmia /hemoglobin E disease. Southem Asian J. T. Med. Publ. Health. 23(2):
1015.
The Swedish Information Centre for Rare Diseases. (2005): URL:
http://www.socialstyrelsen.se/rarediseases/thalassemia (Last seen December, 2010).
Thein, S. L. (1992): Dominant beta thalassemia: molecular basis and pathophysiology. Br. J.
Haematol. 80:273-277.
Thompson, A. A., Cunningham, M. J., Singer, S. T., Neufeld, E. J., Vichinsky, E.,
Yamashita, R., Giardina, P., Kim, H.Y., Trachtenberg, F., Kwiatkowski, J. L. and for
the Thalassemia Clinical Research Network Investigators (2011). Red cell
alloimmunization in a diverse population of transfused patients with thalassaemia. Brit. J.
Haematol. 153: 121–128.
Thool, A. A., Walde, M. S., Shrikhande, A. V. and Talib, V. H. (1998): A simple
screening test for the detection of heterozygous thalassemia. Ind. J. Pathol. Microbiol. 41:
423-426.
TRIP Report. (2006): Available from: http://www.tripnet.nl. ISBN-10: 978-90-78631-02-
06.
Tsiantis, J., Dragonas, Th. and Richardson, C. (1996): Psychosocial problems and
adjustment of children with j -thalassemia and their families. Eur. Child Adolescent Psychiat.
5: 193-203.
Tyagi, S., Pari, H. P., Choudhry, V. P. and Saxena, R. (2004): Clinico-hematological
profile of HbE syndrome in adults and children. Hematol. 9: 57-60.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
143
Urbinati, F., Madigan, C. and Malik, P. (2006): Pathophysiology and therapy for
haemoglobinopathies. Part II: thalassaemias. Expert. Rev. Mol. Med. 8(10): 1-26.
Valentine, W. N. and Neel, J. V. (1944): Hematological and genetic study of transmission
of thalassemic of thalassemia. Arch. Itern. Med. 74: 186-196.
Varaswala, N. Y., Old, J. M., Ventakateshanz, S. R. and Weatherall, D. J. (1991): The
spectrum of beta thalassemia mutations in the Indian subcontinent on the basis of prenatal
diagnosis. Brit. J. Hematol. 78: 242-247.
Vaz, F. E., Thakur, C. B., Banerjee, M. K. and Gangal, S. G. (2000): Distribution of
etathalassemia mutations in the Indian population referred to a diagnostic center.
Hemoglobin. 24: 181–194.
Vecchio, F. (1946): Sulla resistenza della emoglobina alla denaturazione alcalina in alcune
sindromi empatiche. Pediatria. (Napoli) 5: 545-549.
Verma, S., Saxena., A. K. and Marwaha, R. K. (2007): Intracranial calcification in beta
thalassemia Major. Ind. Pediatr. 44: 856-858.
Vichinsky, E. (2001): Consensus document for transfusion-related iron overload. Semin.
Hematol. 38(1): 2-4.
Vogel, M., Anderson, L. J., Holden, S., Deanfield, J. E., Pennell, D. J. and Walker, J. M.
2003): Tissue Doppler echocardiography in patients with thalassemia detects early
myocardial dysfunction related to myocardial iron overload. Eur. Heart J. 24(1): 113-119.
Von Jaksch R. (1889): Leukemia and leukocytosis in childhood. Wein. Klin. Wchns. 2: 435.
Wadia, M. R., Phanasgaokar, S. P., Nadkarni, A. H., Surve, R. R., Gorakshakar, A. C.,
olah, R. B. and Mohanty, D. (2002): Usefulness of automated chromatography for rapid
fetal blood analysis for second trimester prenatal diagnosis of beta-thalassemia. Prenat.
Diagn. 22(2): 153-157.
Walker, R. H., Lin, D. T. and Hartrick, M. B. (1989): Alloimmunization following blood
transfusion. Arch. Pathol. Lab. Med. 113: 254-261.
Walter, P. B., Fung, E. B., Killilea, D. W., et al. (2006): Oxidative stress and inflammation
in iron-overloaded patients with beta-thalassaemia or sickle cell disease. Br. J. Haematol.
135: 254–263.
Weel, F., Jackson, I. T., Crookendale, W. A., McMichan, J. (1987): A case of thalassemia
major with gross dental and jaw deformities. Brit. J. Oral Maxillofacial Surg. 25: 348-352.
Weatherall, D. J. (1997): Thalassemia and malaria, revisited. Ann. Trop. Med. Parasitol. 91:
885-890.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
144
Weatherall, D. J. and Clegg, J. B. (1981): The thalassemia Syndromes. Oxford: Blackwell
Scientific Publications Inc. 148-320.
Weatherall, D. J., Clegg, J. B. (2001): Inherited haemoglobin disorders: an increasing
global health problem. Bull. WHO. 79(8): 704-12.
Weatherall, D. J. and Clegg, J. B. (2001): The thalassemia syndromes. Malden,
Massachusetts: Blackwell Science.
Weatherall, D.J. and Clegg, J.B. (2002): Genetic variability in response to infection. In
Malaria and after. Paeds. Immunity, 3, 331–337.
Weiner, E. (2003): Red cell disorders: Impaired phagocyte antibacterial effectors functions
in β-thalassemia: A likely factor in increased susceptibility to bacterial infections. Hematol.
8(1): 35-40.
Whipple, Ci. H. and Bradford, W. L. (1932): Racial or familial anemia of children
associated with fundamental disturbances of bone and pigment metabolism (Cooley-Von
Jaksch). Am. J. Dis. Child. 44: 336-365.
Whipple, G. H. and Bradford, W. L. (1936): Mediterranean disease–Thalassemia
(erythroblastic anemia of Cooley); associated pigment anomalies simulating
hemochromatosis. J. Pediatr. St. Louis. 9: 279-311.
White, J. M., Richards, R., Jelenski, G., Byrne, M. and Ali, M. (1986): Iron state in alpha
and beta-thalassemia trait. J. Clin. Pathol. 39: 256-259.
Whitcher, B. R. (1925): Proc. N. Y. Path. Soc. 15: 25.
Wikipedia. (2008): URL: http://en.wikipedia.org/w/index.php?title=Thalassemia&
action=edit
Wild, B. J. and Bain, B. J. (2001): Investigations of abnormal hemoglobins and thalassemia.
In: Dacie JV, Lewis SM, eds. Dacie and Lewis Practical Hematology. 9th ed. Edinburgh:
Churchill Livingstone. Pp 231-238.
Willcox, M., Bjo¨rkman, A., Brohult, J., Pehrson, P. O., Rombo, L. and Bengtsson, E.
(1983): A case-control study in northern Liberia of Plasmodium falciparum malaria in
haemoglobin S and beta-thalassaemia trait. Ann. Trop. Med. Parasitol. 77: 239-246.
Williams, T. N. (1999): Mechanisms of malaria protection in the thalassemia syndromes
[dissertation]. London: University of London. pp. 269 Available from the Bodlean Library,
University of Oxford, Oxford, UK.
Williams, T. N., Maitland, K., Bennett, S., Ganczakowski, M., Peto, T. E., Newbold, C.
I., Bowden, D. K., Weatherall, D. J. and Clegg, J. B. (1996): High incidence of malaria in
thalassaemic children. Nature. 383: 522–525.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
145
Williams, T. N., Mwangi, T. W., Wambua, S., Peto, T. E., Weatherall, D. J., Gupta, S.,
Recker, M., Penman, B. S., Uyoga, S., Macharia, A., Mwacharo, J. K., Snow, R. W. and
Marsh, K. (2005): Negative epitasis between the malaria-protective effects of
alpha+thalassemia and the sickle cell trait. Nat. Genet. 37: 1253-1257.
William, T. N., Wonke, B. and Donohue, S. M. (1992): A study of hepatitis B and C.
prevalence and liver function in multiply transfused thalassemics and their parents. Ind.
Pediatr. 29(9): 1119-1124.
Wintrobe, M. M. and Lee, G. R. (1999): Wintrobe's clinical hematology. Baltimore,
Williams and Wilkins.
Wong, V., Ma, H. K., Todd, D., Golbus, M. S., Dozy, A. M. and Kan, Y. W. (1978):
Diagnosis of homozygous alphathalassemia in cultured amniotic-fluid fibroblasts. N. Engl. J.
Med. 298: 669-670.
Wood, J. C., Kang, B. P., Thompson, A., Patricia G., Paul H., Tara G., Carole P.
and Thomas D. C. (2010): The effect of deferasirox on cardiac iron in thalassemia major:
impact of total body iron stores. Blood. (4): 537–543.
Wood, J. C. and Noetzli, L. (2010): Cardiovascular MRI in thalassemia major. Ann. N. Y.
Acad. Sci. 1202: 173-179.
World Health Organization. (2005): UNICEF. Annex 3: Maps. In: World Malaria Report
2005.Geneva, Switzerland: World Health Organization and UNICEF Press. Pp 281–286.
World Health Organization. (1983): Human Genetics Programme. Division of
Communicable Diseases. Community control of hereditary anemia’s: memorandum for a HO
meeting. Bull. WHO. 61: 63-80.
WHO (2001): HepatitisB Assays: Operational Characteristics http://www.who.int/
diagnostics_laboratory/evaluations/en/hep_B_rep1.pdf
WHO/UNICEF/UNU. (2001): Iron deficiency anaemia: assessment, prevention, and control.
A guide for programme managers. Geneva, Switzerland: World Health Organization
(WHO/NHD/01.3, 2001).
WHO/March of Dimes. (2006): Report of a joint meeting, May 5-15.
Wambua, S., Mwangi, T. W., Kortok, M., Uyoga, S. M., Macharia, A.W., Jedidah, K.
Mwacharo, David J. Weatherall, Robert W. Snow, Kevin Marsh, Thomas N. Williams.
(2006): The effect of α +-thalassaemia on the incidence of malaria and other diseases in
children living on the Coast of Kenya . PLoS Med. 3(5).
Xu, X., Liao, C., Liu, Z., Huang Y., Zhang, J., Li, J., Peng, Z., Qiu, L. and Xu, Q.
(1996): Antenatal screening and fetal diagnosis of beta-thalassemia in a Chinese population:

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
146
prevalence of the beta-thalassemia trait in the Guangzhou area of China. Hum. Genet. 98:
199–202.
Yeşim Aydinok, Sukran Darcan, Aziz Polat, Kaan Kavakli, Güngör Nişli, Mahmut
Çoker, Mehmet Kantar and Nazan Çetingul. (2002): Endocrine complications in patients
with β‐thalassemia major. J. Trop. Pediatr. 48(1): 50-54.
Yi Kong., Suiping Zhou., Anthony J. Kihm., Anne M. Katein., Xiang Yu., David A.
Gell., Joel P. Mackay., Kazuhiko Adachi., Linda Foster-Brown., Calvert S. Louden.,
Andrew J. Gow. and Mitchell J. Weiss. (2004): Loss of α-hemoglobin–stabilizing protein
impairs erythropoiesis and exacerbates β-thalassemia. J. Clin. Invest. 4(10): 1457–1466.
Yixuan Wang, Chen-Guang Zheng, Yonghua Jiang, Jiqin Zhang, Jiayu Chen,
Chao Yao, Qingguo Zhao, Sheng Liu, Ke Chen, Juan Du, Ze Yang and Shaorong Gao.
(2012): Genetic correction of β-thalassemia patient-specific iPS cells and its use in improving
hemoglobin production in irradiated SCID mice. Cell Res. 22:637–648.
Zafeiriou, D., Athanasiou, M., Katzos, G., Economou, M. and Kontopoulos, E. (2001):
ypoparathyroidism and intracranial calcification in b-thalassemia major. J. Pediatr. 138: 411.
Zandieh, Babaahmadi, B., Pourfathollah, A., Galedari, H., Emam, J. and Jalalifar M. A.
(2005): Transfusion transmitted virus (TTV) infection in thalasaemic patients. Ir. J. Publ.
Health. 34(4): 24-28.
………………………………………………………………………………………………..

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
147
ANNEXES
Aproval letter as a Technical Supervisor (Component Section) at blood bank.
Food and Drug Administration, Government of Maharashtra, Pune, approved by me as a
Technical Supervisor (Component Section) at blood bank last 10 Years. Letter Reference No.
Med/Prod/805/07/2 Dated 12th March 2007.
Thalassemic Patients Data Bank
Thalassemic patients’ data sheet, photography, consent forms, all reports and peripheral
blood smear slides were deposited at Protozoology Laboratory, Dr. Babasaheb Ambedkar
Marathwada University, Aurangabad, Maharashtra, India.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
148
LIST OF PUBLICATIONS
1. Patil S.S., Nikam S.A., Dama S.B., Chondekar R.P., Kirdak R.V. and Dama L.B.
(2011). Prevalence of hepatitis-B surface antigen (HBsAg) positivity in Solapur District,
Maharashtra State, India. Bangladesh Journal of Medical Science. 10(2): 91-94. (ISSN:
1607-0755 EISSN: 2076- 0299).
2. Nikam S.V., Dama S.B., Saraf S.A., Jawale C.S., Kirdak R.V., Chondekar R.P.,
Patil S. S., Deshmukh P.S., Shaikh F.I., and Dama L.B. (2011). Prevalence of red cell
alloimmunization in repeatedly transfused patients with Β- Thalassemia in Solapur
District, Maharashtra State, India. UGC-Sponsored Proceedings of the National-Level
Workshop cum Seminar on ‘Bio-Resources for Bio-Industries and Economic Zoology’,
January- 2011, Solapur, Maharashtra, India. 1-3. (ISBN 81-903603-6-1).
3. Wath M. R., Chondekar R. P., Saraf S. A And Dama S. (2011). Antimicrobial
Evaluation of Three Species Of Cassia Siamea L. UGC-Sponsored Proceedings of the
National-Level Workshop cum Seminar on ‘Bio-Resources for Bio-Industries and
Economic Zoology’, January- 2011, Solapur, Maharashtra, India. 4-6. (ISBN 81-903603-
6-1).
4. Mohd Iliyas., Shaikh, F. I., Quazi Salim., Sayri Abdula and Dama, S. B. (2011).
Behavioral assessment of heavy metal on freshwater crab Barytelphusa cunicularis.
UGC-Sponsored Proceedings of the National-Level Workshop cum Seminar on ‘Bio-
Resources for Bio-Industries and Economic Zoology. 52-54, (ISBN 81-903603-6-1).
5. Tembhurkar V.R., Chintawar S.S., Dama S.B., Arvikar P.G. and Dama L.B. (2012).
Detection of respiration deficiency mutants of Saccharomyces cerevisiae by MBRT test.
DAV International Journal of Science. 1(1): 29-31. ISSN: 2277-5536 (Print); 2277-5641
(Online).
6. Nikam S.V., Dama S.B., Jawale C.S., Deshmukh P.S., Patil S.S. , Tembhurkar V.R.
and Dama L.B. (2012). Height and weight correlation in thalassemic patients from
Solapur District, Maharashtra, India. DAV International Journal of Science. 1(1): 54-57.
ISSN: 2277-5536 (Print); 2277-5641 (Online).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
149
Figure -1. Global distribution of thalassemia, hemoglobins S, C, D and E.
Figure-2. A- Map of India

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
150
B-Map of Maharashtra
C- Map of Solapur Solapur District.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
151
Figure-3. Showing the Talukawise geographical distribution and prevalence percentage of
the thalassemic patients in Solapur District.
Figure -4. Showed type of thalassemic patients entering the study (n=125)
Figure-4a. Showing prevalence percentage of different types of thalassemia in Solapur
District age between 6 months to 18 years.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
152
Figure -5. Showing the mean height (Inch) and weight (Kg) in thalassemia patients.
Figure- 6. Showing prevalence percentage of growth in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
153
Figure-8. Showing the education in thalassemic patient.
Figure-9. Showing the prevalence percentage of the skin color in thalassemia patients

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
154
Figure- 10. Showing the prevalence percentage of hearing, visual impairement and
psychological complications in thalassemia patients.
Figure-11. Showing prevalence percentage of the consanguineous marriages in the parents of
the thalassemic patient.
Figure 12. Showing the prevalence percentage of ethnicity in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
155
Figure-13. Showing prevalence percentage of thalassemic patients’ diet.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
156
Figure-14. Prevalence of orofacial complications in thalassemia patients: Rodent face.
Figure -14a. Prevalence of orofacial complications in thalassemia patients: Saddle nose.
Figure-14b. Prevalence of orofacial complications in thalassemia patients: Maxillary
protrubution.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
157
Figure-14c. Prevalence of orofacial complications in thalassemia patients: Maxillary anterior
teeth spacing.
Figure -14d. Prevalence of orofacial complications in thalassemia patients: Anterior open
bite
Figure-14e. Prevalence of orofacial complications in thalassemia patients: Deep bite.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
158
Figure-14f. Prevalence of orofacial complications in thalassemia patients: Mucosal
discoloration.
Figure- 15.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
159
Figure-15. Photomicrograph of a blood film. Sickle cell thalassemia. (Black arrow
indicates: target cells; Green arrow indicates: distorted tear drop cells; Blue arrow:
hypochromic microlytic cells).
Figure15a. Photomicrograph of a blood film. β-thalassemia Intermedia. (Black arrow
indicates: target cells; Green arrow: distorted tear drop cells; Brown arrow: echinocytes;
Blue arrow: hypochromic microlytic cells).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
160
Figure- 15. Continued...
Figure-15c. Photomicrograph of a blood film. β-thalassemia minor. (Green arrow
indicates: hypochromasia, anisochromasia and anisocytosis).

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
161
Figure-15d. Photomicrograph of a blood film. Thalassemia Major. Shows
hypochromasia, anisochromasia and anisocytosis and numerous poikliocytes and cell
fragments. (Black arrow indicates: target cells; Green arrow indicates: hypochromasia,
anisochromasia and anisocytosis; Red arrow: envelope form cell)
Figure- 15. Continued..
Figure -15e. .Photomicrograph of a blood film. Thalassemia Major, after splenectomy.
Shows many target cells grossly deficient in haemoglobin. The relatively dark staining
target cells are normal cells, which have been transfused. (Black arrow indicates: target
cells)

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
162
Figure-16. Showing the prevalence percentage of WBC count in thalassemia patients.
Figure-17. Showing prevalence percentage of RBC count in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
163
Figure-18. Showing the prevalence percentage of Hb in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
164
Figure-19. Showing the prevalence percentage of HCT count in thalassemia patients.
Figure-20. Showing prevalence percentage of MCV count in thalassemia patients.
Figure-21. Showing the prevalence percentage MCH count in thalassemia patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
165
Figure-22. Showing the range of MCHC in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
166
Figure-23. Showing the prevalence percentage of platelet count in thalassemic patients.
Figure-24a. Showing the range of pre transfusion Hb in thalassemic patients.
Figure-24b. Showing the range of post transfusion Hb in thalassemic patients
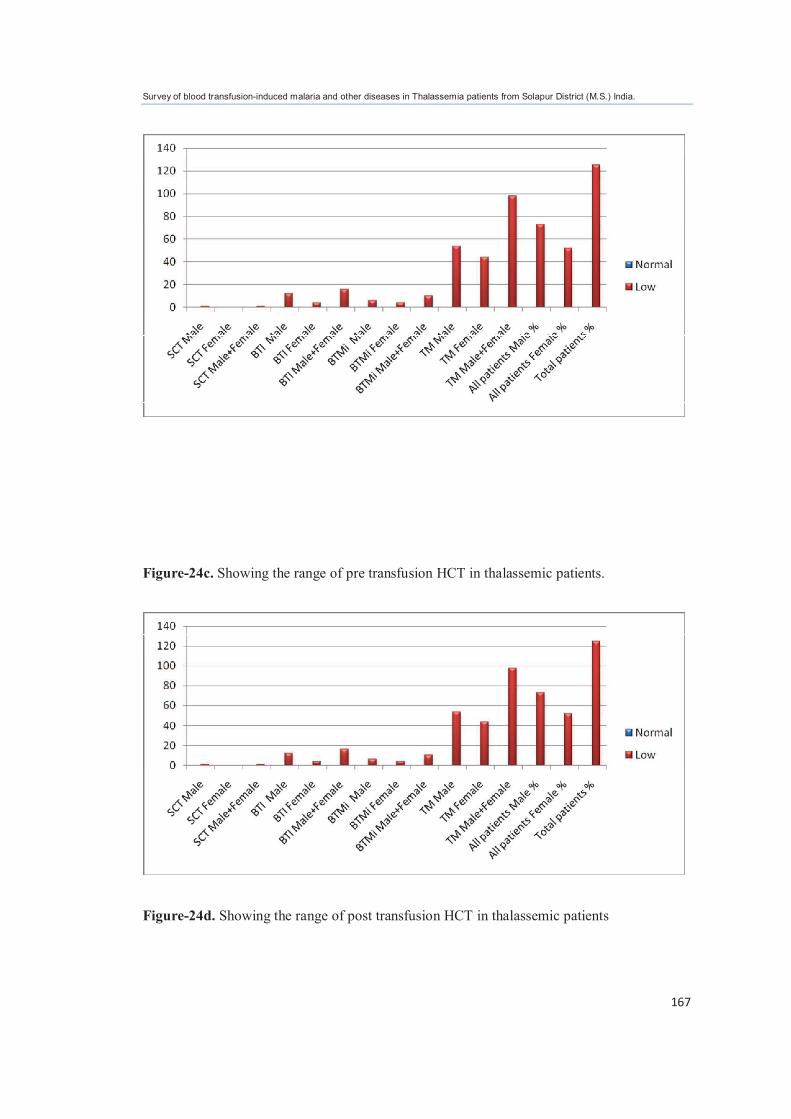
Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
167
Figure-24c. Showing the range of pre transfusion HCT in thalassemic patients.
Figure-24d. Showing the range of post transfusion HCT in thalassemic patients

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
168
Figure-25. Showing prevalence Percentage of malaria history in thalassemic patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
169
Figure-26. Showing prevalane percentage of HCV, HIV, HBsAg and VDRL in thalassemia
patients
Figure-27. Showing prevalence percentage of liver dysfunction in thalassemia patients
Figure-27a. Showing prevalence percentage of hyperthyroidism and alloimmunization in
thalassemia patients

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
170
Figure-28. Showing prevalence percentage of spleen and splenectomized thalassemic
patients
Figure-29. Showing the medication in thalassemia patients.

Survey of blood transfusion-induced malaria and other diseases in Thalassemia patients from Solapur District (M.S.) India.
171
Figure-30. Showed the mortality rates of thalassemic patients during the study period.