thalassemia treatment update
TRANSCRIPT

AUBHO-2015
Vip Viprakasit, MD, DPhil (Oxon)Thalassaemia Center & Department of Paediatrics
Faculty of Medicine Siriraj HospitalMahidol University
Bangkok, THAILAND
“What ‘s new in Hematology: Thalassemia”

Agenda
• A new Guideline for TDT-TIF 2014
• A new information on current management
- What’s new!! on iron chelators
• A new future treatment on horizon
- New approach and new paradigm shift
- New diagnosis & future
Agenda
• A new Guideline for TDT-TIF 2014
• A new information on current management
- What’s new!! on iron chelators
• A new future treatment on horizon
- New approach and new paradigm shift
- New diagnosis & future

The TIF Thalassemia Management Guidelines in a nutshell
• Published and endorsed by the Thalassaemia International Federation (TIF), Nicosia, Cyprus
• Currently in its 3rd edition (published in 2014 since 1980s’)• Current edition exclusive to transfusion-dependent
thalassemia (TDT)− Guidelines for the management of non-transfusion-dependent
thalassemia (NTTD) published separately in 2013• Ed. Taher A, Vichinsky E, Musallam KM, Cappellini MD, Viprakasit V
• Guidelines mainly targeting HCPs− Separate guidelines published for
• emergency care • Nursing staff

More importantly…Moving from
independent expert opinion
To evidence-based practice

Evolving change in the direction of thalassemia management
Looking at the total patient population
Looking at the individual patient
Considering the patient status today
Considering the patient journey until today
Managing iron overload Managing an iron overload profile
Treating a patient Supporting a human
Acting as a physician Acting as a team
IOL, iron overload; TIF, Thalassaemia International Federation.
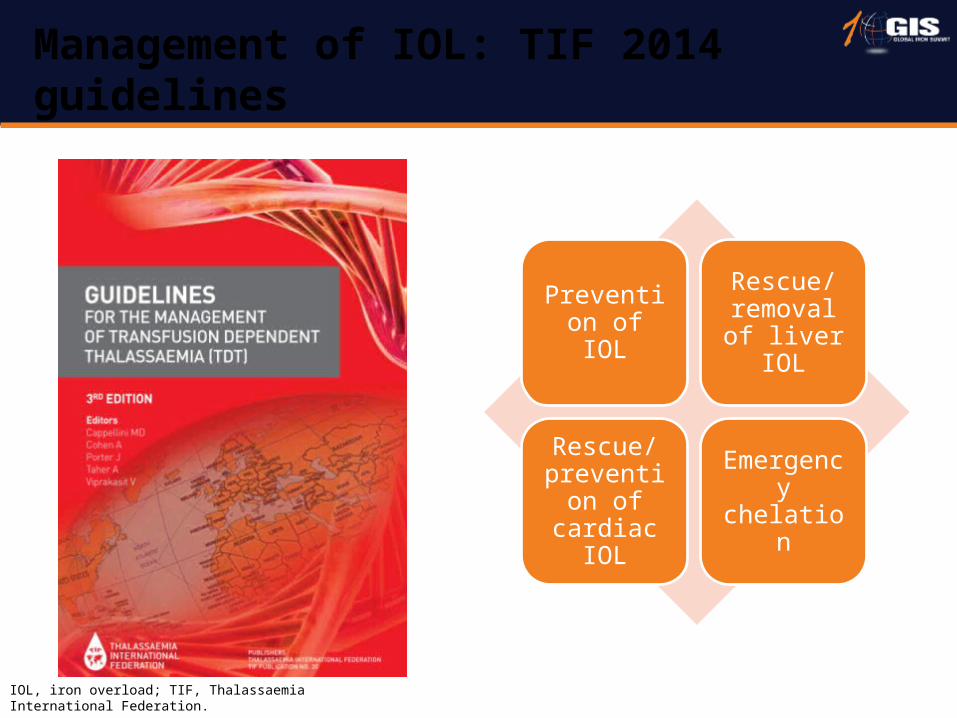
Management of IOL: TIF 2014 guidelines
Prevention of IOL
Rescue/ removal of liver IOL
Rescue/ prevention of cardiac
IOL
Emergency chelation
Agenda
• A new Guideline for TDT-TIF 2014
• A new information on current management
- What’s new!! on iron chelators
• A new future treatment on horizon
- New approach and new paradigm shift
- New diagnosis & future
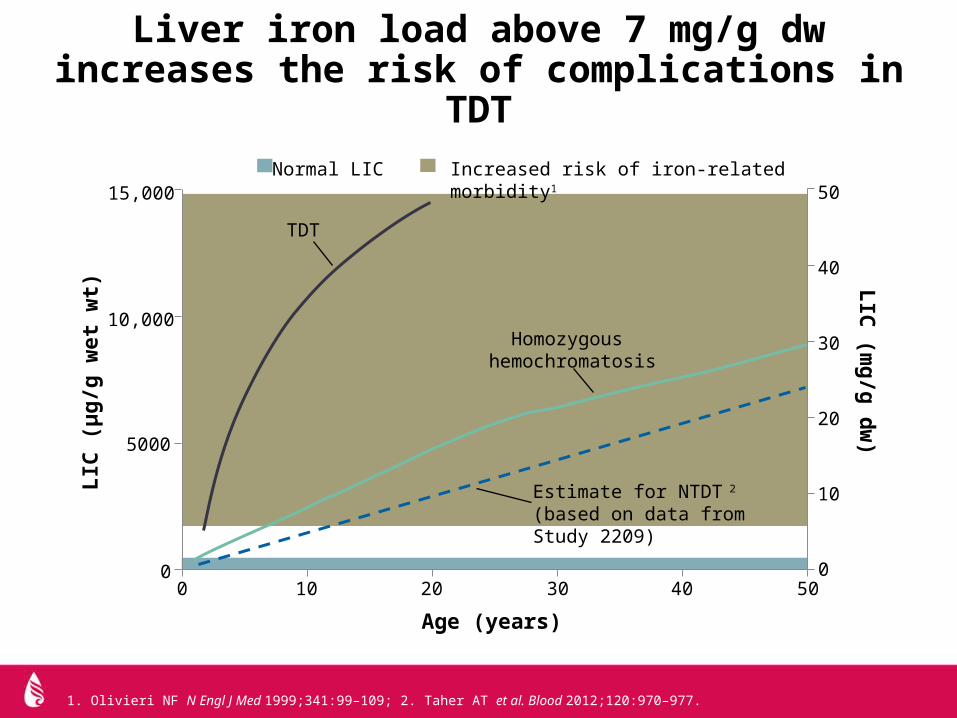
Liver iron load above 7 mg/g dw increases the risk of complications in TDT
1. Olivieri NF N Engl J Med 1999;341:99–109; 2. Taher AT et al. Blood 2012;120:970–977.
Homozygous hemochromatosis
Estimate for NTDT 2
(based on data from Study 2209)
Age (years)
LIC
(μg/
g w
et w
t)
TDT
LIC (m
g/g dw)
Increased risk of iron-related morbidity1Normal LIC15,000
10,000
5000
00 10 20 30 40 50
0
10
20
30
40
50

Liver enzyme concentrations increase at LIC >15 mg Fe/g dw
Jensen PD et al. Blood 2003;101:91-96.
AST, U
/L
16.8
Fe
mg/
g dr
y w
t
Liver iron, µmol Fe/g
SF, µg/L
240
200
160
120
80
40
00 100 200 300 400 600500
240
200
160
120
80
40
00 100 200 300 400 600500
100
10100 1000 10,000
100
10100 1000 10,000
ALT
, U/L
R2=0.55P<0.0001
R2=0.62P<0.0001
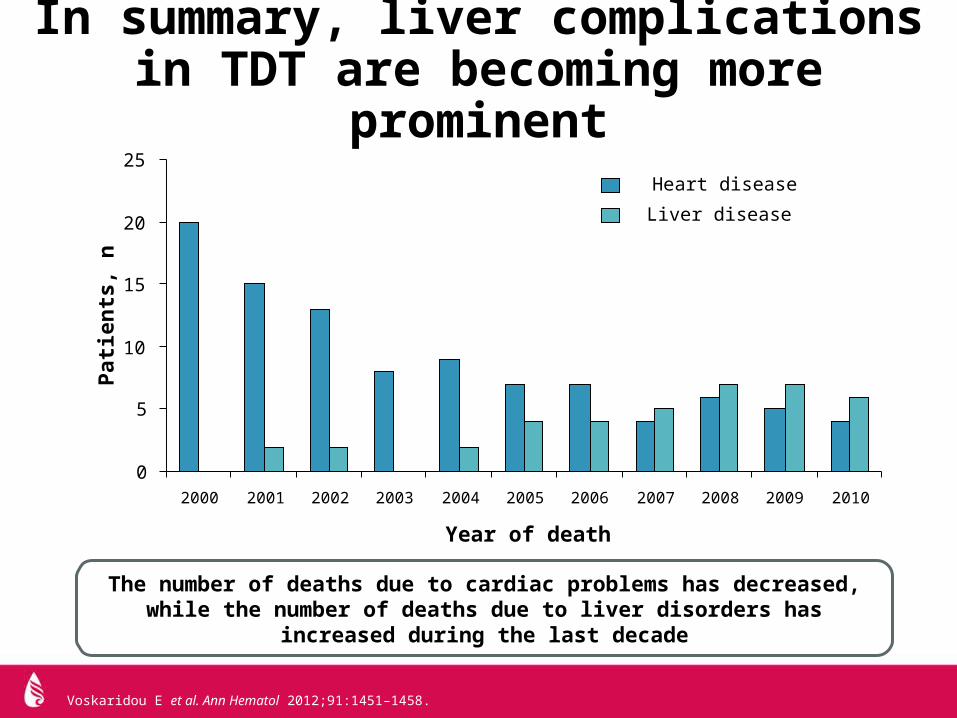
In summary, liver complications in TDT are becoming more prominent
Voskaridou E et al. Ann Hematol 2012;91:1451–1458.
0
5
10
15
20
25
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Heart disease
Liver disease
Year of death
Patie
nts,
n
The number of deaths due to cardiac problems has decreased, while the number of deaths due to liver disorders has increased during the last decade
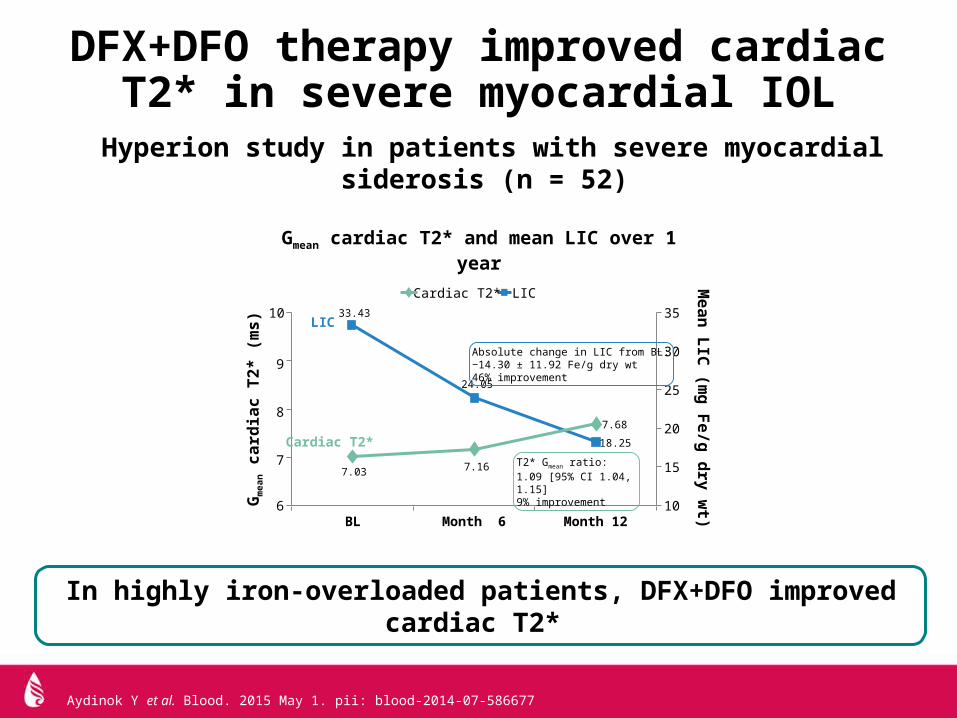
DFX+DFO therapy improved cardiac T2* in severe myocardial IOL
Aydinok Y et al. Blood. 2015 May 1. pii: blood-2014-07-586677
Gmean cardiac T2* and mean LIC over 1 year
6
7
8
9
10
BL Month 6 Month 1210
15
25
30
35
20
Gm
ean c
ardi
ac T
2* (m
s)M
ean LIC (m
g Fe/g dry wt)
LICCardiac T2*33.43
24.05
18.25
7.68
7.167.03
Absolute change in LIC from BL:−14.30 ± 11.92 Fe/g dry wt46% improvement
T2* Gmean ratio:1.09 [95% CI 1.04, 1.15]9% improvement
In highly iron-overloaded patients, DFX+DFO improved cardiac T2*
Hyperion study in patients with severe myocardial siderosis (n = 52)
Cardiac T2*
LIC
Compared to current formulation– more bioavailable: 14 mg DFX FCT equals 20 mg of
DFX DT – lower biovariability and more limited food effect
Different posology – tablets of 90, 180, and 360 mg DFX FCT corresponding
to 125, 250, and 500 mg tablets DFX DT No lactose in DFX FCT: improved GI safety?
– to be evaluated in the 2201 trial
DFX DT, deferasirox dispersible tablets (Exjade®);DFX FCT, deferasirox film-coated tablets, “new formulation”.
New deferasirox formulation: film-coated tablets (FCT)

AE, adverse event; GI, gastrointestinal. Available from: clinicaltrials.gov/ct2/show/NCT02125877?term=deferasirox&rank=31. Accessed March 2015.
F2201 trial evaluates the safety (and efficacy) of deferasirox FCT
Primary objective: to evaluate the overall safety, measured as frequency and severity of AEs and changes in laboratory values in patients with TDT or MDS (IPSS-R Very low, Low, or Intermediate risk)
Secondary objectives (both formulations) – selected GI AEs– pharmacokinetics– patient-reported outcomes (satisfaction, palatability, and GI symptoms)– patient compliance (using pill count and a daily diary)
Screening (including wash out)
14 days
Deferasirox DTtaken as per local label (n = 75)
Follow-up
Follow-upDeferasirox FCTtaken with or after food (n = 75)
24 weeks
24 weeks
1 month
1 month
Ran
dom
izat
ion

Basel, March 30, 2015 - Novartis announced today that the US Food and Drug Administration (FDA) has approved JadenuTM (deferasirox) tablets, a new oral formulation of Exjade® (deferasirox) tablets for oral suspension, for the treatment of chronic iron overload due to blood transfusions in patients 2 years of age and older, and chronic iron overload in non-transfusion-dependent thalassemia syndromes (NTDT) in patients 10 years of age and older. Jadenu is the only once-daily oral iron chelator that can be swallowed whole.
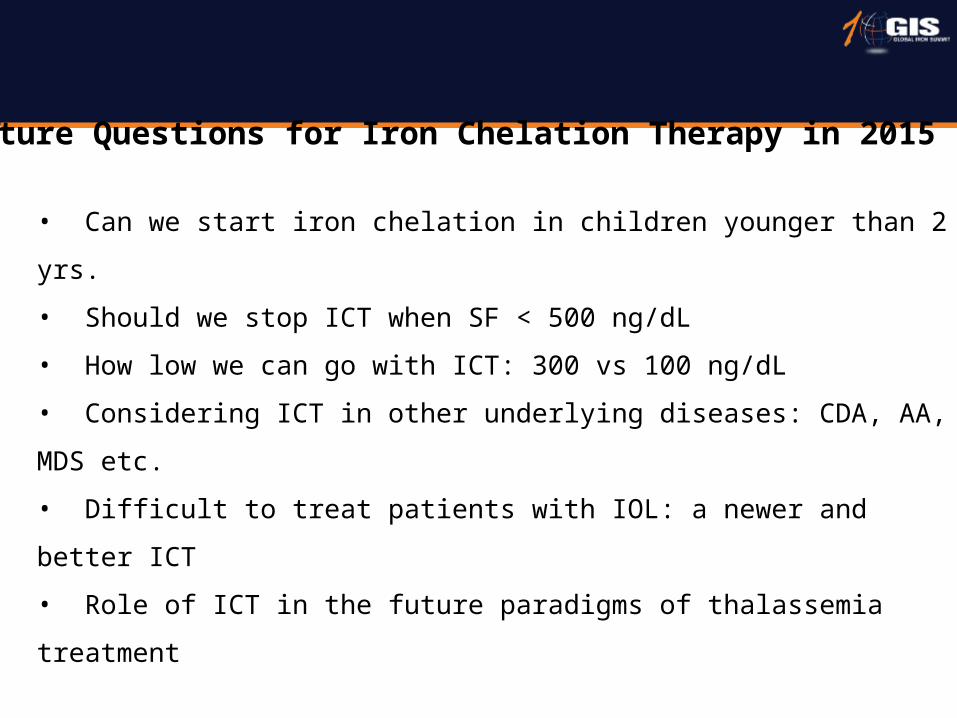
Future Questions for Iron Chelation Therapy in 2015
• Can we start iron chelation in children younger than 2 yrs.
• Should we stop ICT when SF < 500 ng/dL
• How low we can go with ICT: 300 vs 100 ng/dL
• Considering ICT in other underlying diseases: CDA, AA, MDS etc.
• Difficult to treat patients with IOL: a newer and better ICT
• Role of ICT in the future paradigms of thalassemia treatment
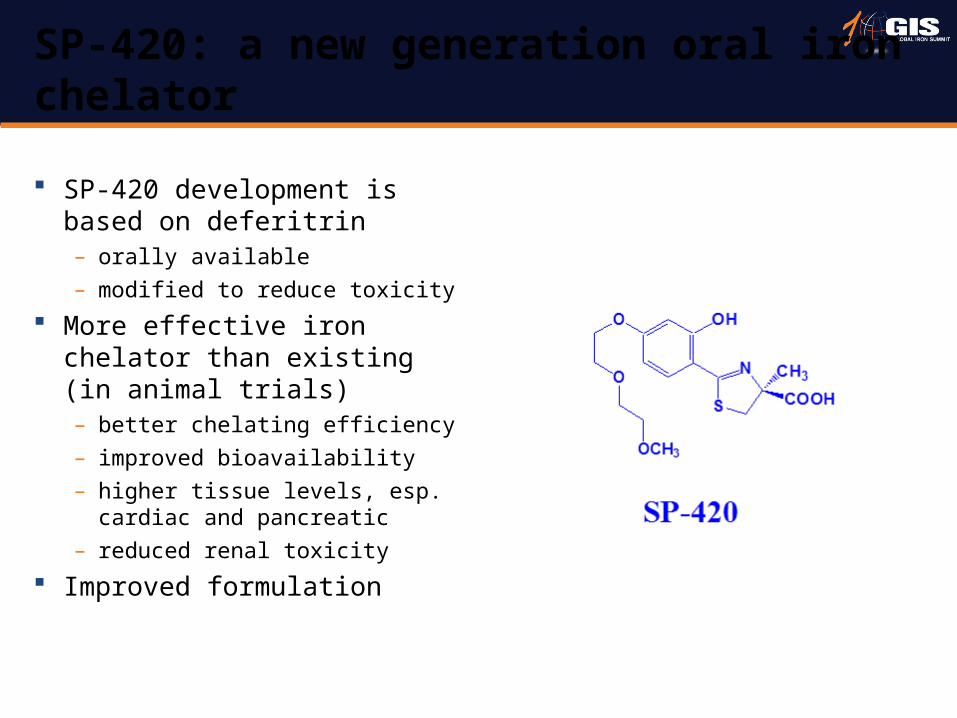
SP-420 development is based on deferitrin – orally available– modified to reduce toxicity
More effective iron chelator than existing (in animal trials)– better chelating efficiency – improved bioavailability– higher tissue levels, esp.
cardiac and pancreatic– reduced renal toxicity
Improved formulation
SP-420: a new generation oral iron chelator
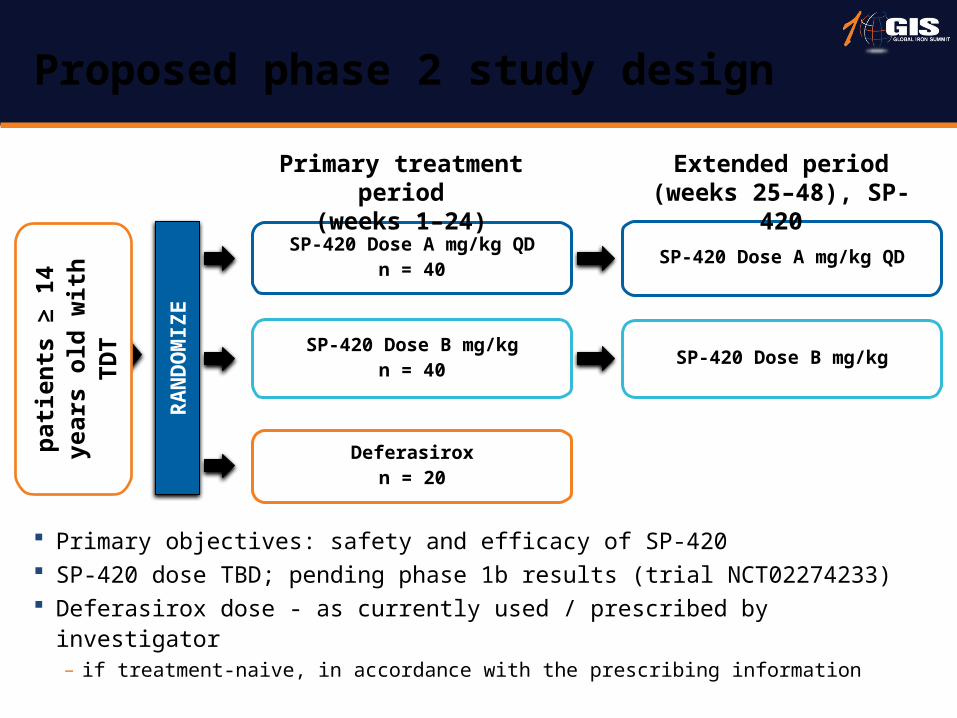
Primary objectives: safety and efficacy of SP-420 SP-420 dose TBD; pending phase 1b results (trial NCT02274233) Deferasirox dose - as currently used / prescribed by investigator
– if treatment-naive, in accordance with the prescribing information
Proposed phase 2 study design
RA
ND
OM
IZE
SP-420 Dose A mg/kg QDn = 40 SP-420 Dose A mg/kg QD
SP-420 Dose B mg/kgn = 40 SP-420 Dose B mg/kg
Deferasiroxn = 20
Extended period(weeks 25–48), SP-420
Primary treatment period(weeks 1–24)
patie
nts
≥ 14
yea
rs
old
with
TD
T

• Derivative of desazadesferrithiocin• Polyethers chosen to increase hydrophilicity• Very high affinity and selectivity for iron• Orally bioavailable • FBS0701 chosen for pharmacological,
pharmacokinetic and toxicity profile • Iron chelating efficiency 23% in primates
FBS0701: A New Promising Drug?
Rienhoff et al. Haematologica 2011;96:521–5; Hahn et al. J Am Chem Soc 1990;112:1854–60; Anderegg & Raeber J Chem Soc Chem Commun 1990;17:1194–6; Bergeron et al. J Med Chem. 2008; 51: 3913–23

FBS0701/Ferrikin/SH602/Deferithiozine
Causing renal cell carcinoma in mouse model
Agenda
• A new Guideline for TDT-TIF 2014
• A new information on current management
- What’s new!! on iron chelators
• A new future treatment on horizon
- New approach and new paradigm shift
- New diagnosis & future

Ineffective Erythropoiesis

RBC Hemolysis: Oxidative stress
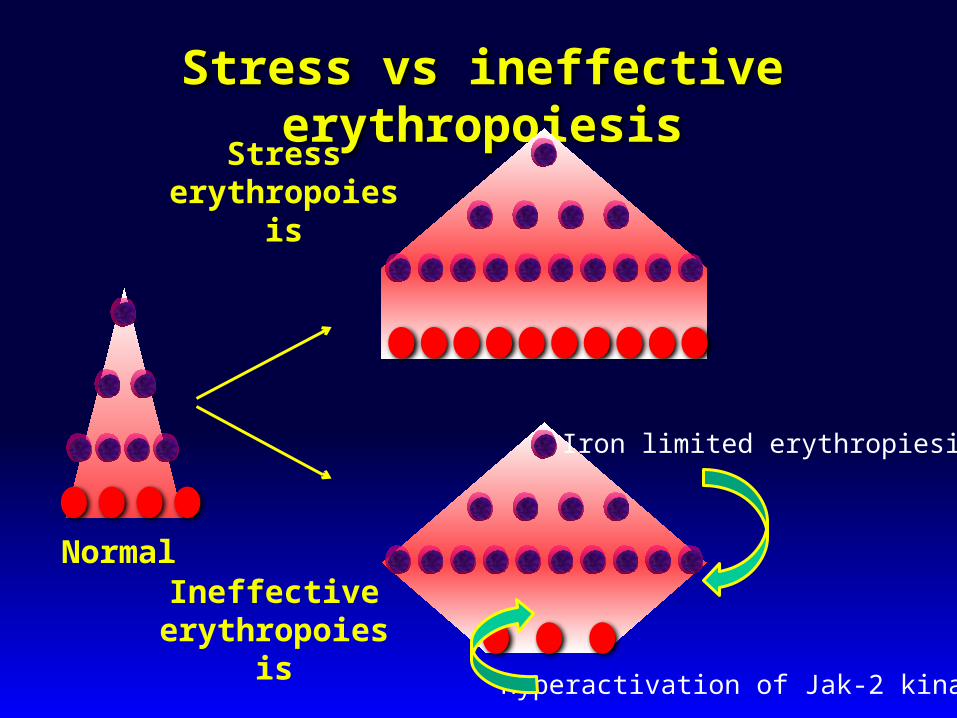
Stress vs ineffective erythropoiesis
Normal
Stress erythropoiesis
Ineffectiveerythropoiesis
Iron limited erythropiesis
Hyperactivation of Jak-2 kinase
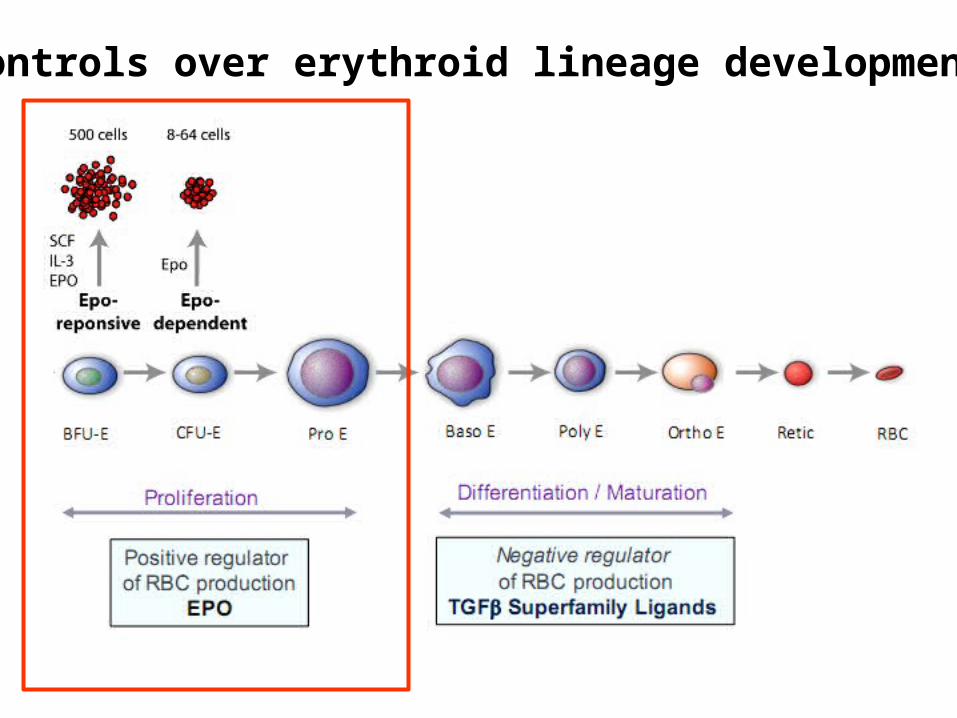
Controls over erythroid lineage development
ActRIIB, activin receptor type Iib. Suragani R, et al., Nat Med. 2014;20:408-14.
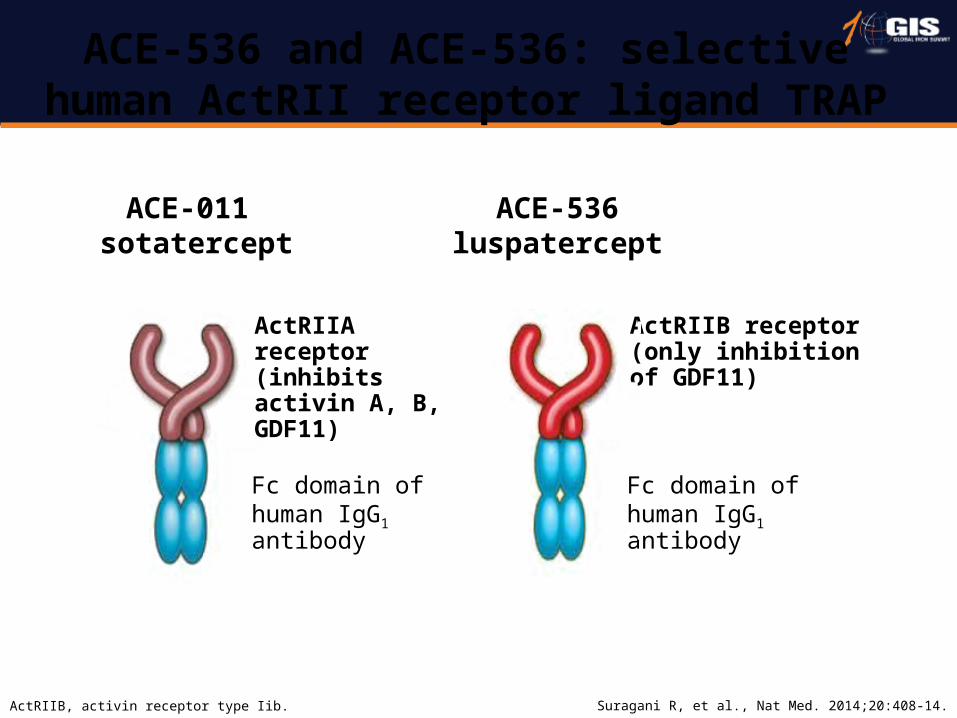
ACE-536 and ACE-536: selective human ActRII receptor ligand TRAP
ActRIIB receptor(only inhibition of GDF11)
Fc domain of human IgG1 antibody
ACE-536luspatercept
ActRIIA receptor (inhibits activin A, B, GDF11)
Fc domain of human IgG1 antibody
ACE-011 sotatercept

* s.c. injection once every 3 weeks.25 patients: 18 NTDT; 7 TDT.NTDT, non-transfusion-dependent thalassaemia; TDT, transfusion-dependent thalassaemia.
Porter J, et al. EHA 2014. Haematologica. 2014;99 Suppl 1:abstract S662.
Phase 2a interim results: sotatercept* improves anaemia and has a favourable safety profile
Sotatercept increased Hb levels in NTDT patients, decreased transfusion requirement in TDT patients, and has a favourable safety profile
≥ 1 g/dL increase ≥ 2 g/dL increase0
20
40
60
80
1000.1 mg/kg (n = 6)0.3 mg/kg (n = 6)0.5 mg/kg (n = 6)0.75 mg/kg (n = 4)
Maximum change in Hb during the first 9 weeks
Sotatercept
Patie
nts
(%)
Maximum change in Hb in NTDT patients during the first 9 weeks
Interim data as of 7 February 2014.Hb values are not included if measured within 2 weeks after transfusion.
≥ 20% reduction ≥ 50% reduction0
20
40
60
80
100 0.1 mg/kg (n = 2)0.3 mg/kg (n = 3)0.5 mg/kg (n = 2)0.75 mg/kg (n = 3)
Sotatercept
Reduction in transfusion burden in TDT patients
Change in transfusion burdenb
Interim data as of 7 February 2014.a Transfusion burden evaluated up to the last known efficacy record, adjusted to 168 days.
b Change in transfusion burden (units/168 days) from baseline.
a
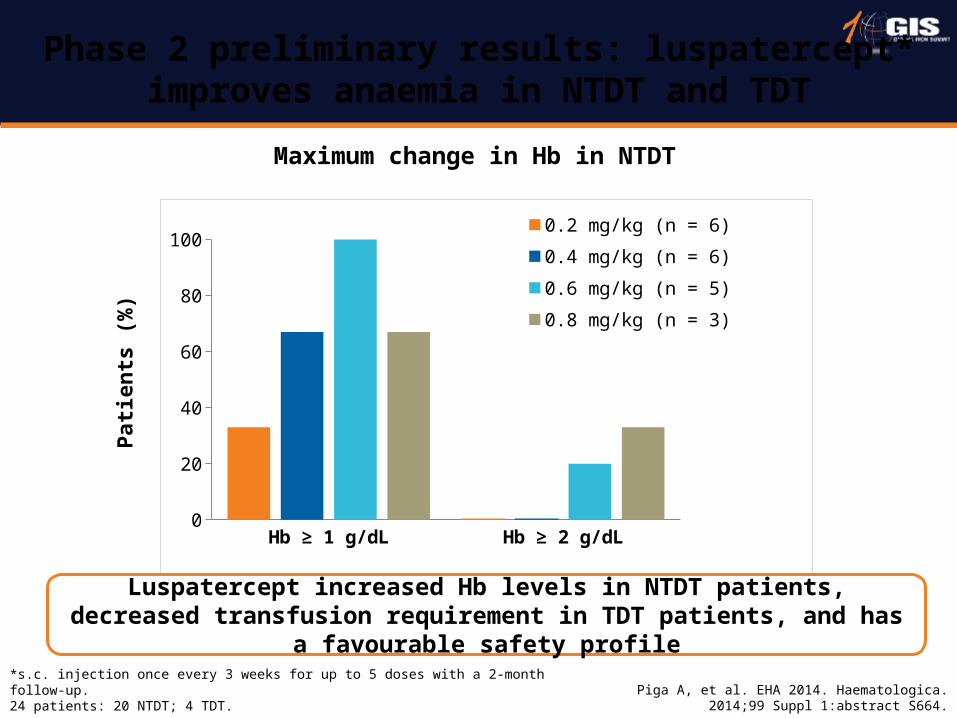
*s.c. injection once every 3 weeks for up to 5 doses with a 2-month follow-up.24 patients: 20 NTDT; 4 TDT.
Piga A, et al. EHA 2014. Haematologica. 2014;99 Suppl 1:abstract S664.
Phase 2 preliminary results: luspatercept* improves anaemia in NTDT and TDT
Hb ≥ 1 g/dL Hb ≥ 2 g/dL0
20
40
60
80
1000.2 mg/kg (n = 6)
0.4 mg/kg (n = 6)
0.6 mg/kg (n = 5)
0.8 mg/kg (n = 3)
Patie
nts
(%)
Luspatercept increased Hb levels in NTDT patients, decreased transfusion requirement in TDT patients, and has a favourable safety profile
Maximum change in Hb in NTDT
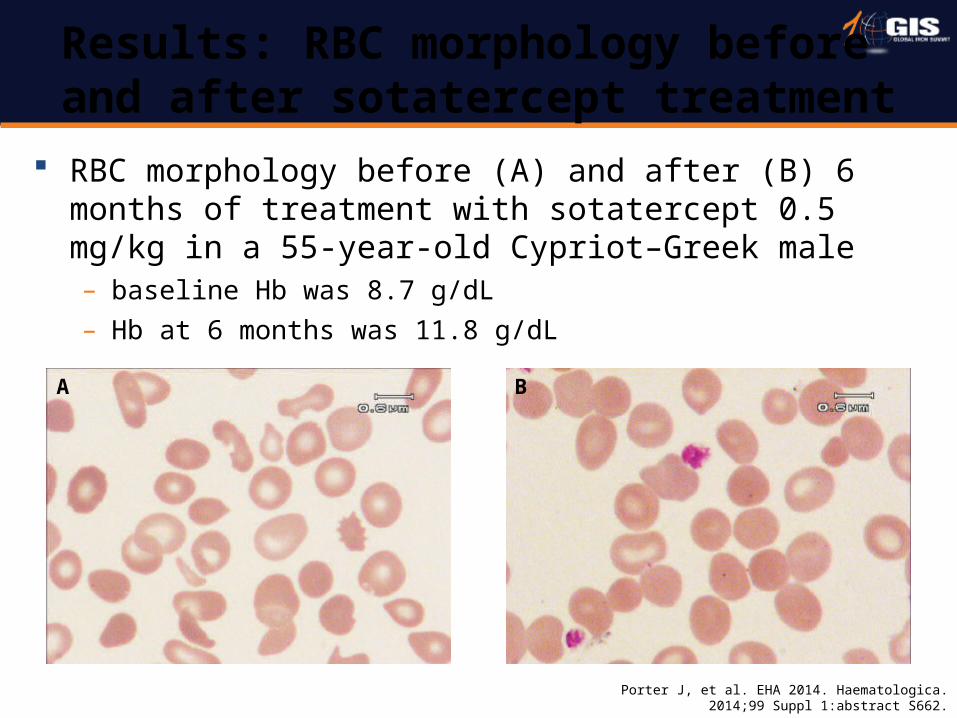
RBC morphology before (A) and after (B) 6 months of treatment with sotatercept 0.5 mg/kg in a 55-year-old Cypriot–Greek male– baseline Hb was 8.7 g/dL– Hb at 6 months was 11.8 g/dL
Porter J, et al. EHA 2014. Haematologica. 2014;99 Suppl 1:abstract S662.
Results: RBC morphology before and after sotatercept treatment
A B
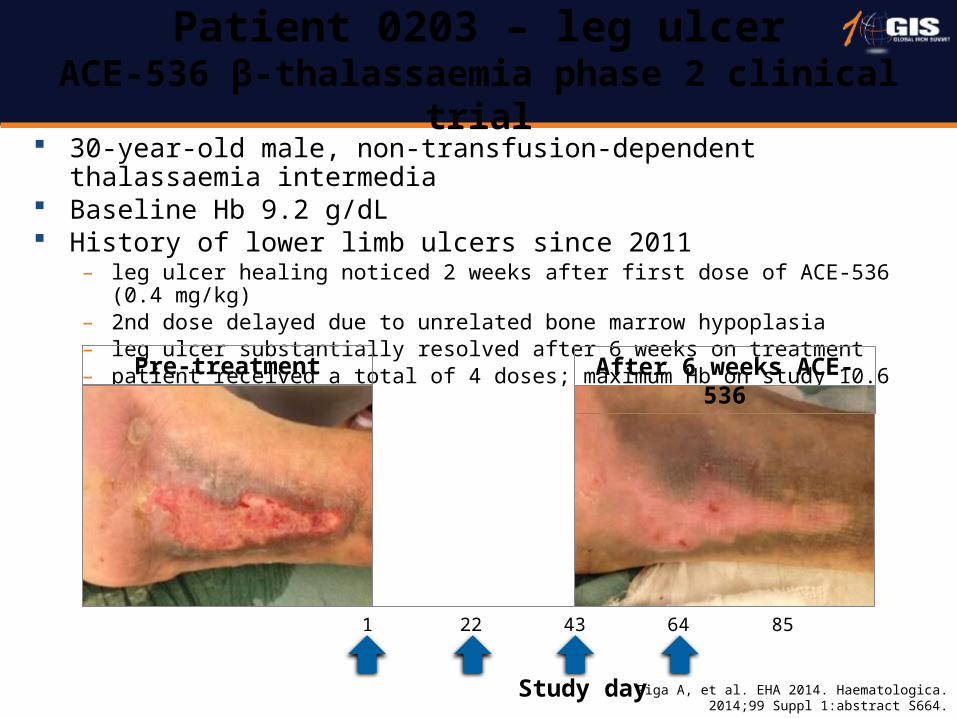
30-year-old male, non-transfusion-dependent thalassaemia intermedia Baseline Hb 9.2 g/dL History of lower limb ulcers since 2011
– leg ulcer healing noticed 2 weeks after first dose of ACE-536 (0.4 mg/kg) – 2nd dose delayed due to unrelated bone marrow hypoplasia– leg ulcer substantially resolved after 6 weeks on treatment– patient received a total of 4 doses; maximum Hb on study 10.6 g/dL
Piga A, et al. EHA 2014. Haematologica. 2014;99 Suppl 1:abstract S664.
Patient 0203 – leg ulcerACE-536 β-thalassaemia phase 2 clinical trial
Pre-treatment After 6 weeks ACE-536
Study day
1 22 43 64 85
Care – prevention of complications: Improving ICT– early control of complications through a rigorous
follow-up and treatment– control of ineffective erythropoiesis: Jak-2, Activin inh.
Cure– SCT: Haploidentical– gene therapy
Future landscape of haemoglobinopathic treatment

Our Lab teamAcknowledgement: Vip’s team at Siriraj Hospital