the 2014 non-st-elevation mi guidelines—what’s new … · 2014 aha/acc guideline for the ......
TRANSCRIPT

The 2014 Non-ST-elevation MI Guidelines—What’s new and relevant to
clinical practice?
Jeffrey L. Anderson, MD, FACC, FAHA, MACP Professor of Internal Medicine, University of Utah
Associate Chief of Cardiology, Intermountain Medical Center Director of Cardiovascular Research, Intermountain Heart Institute
Vice-Chair of Research, Department of Internal Medicine, Intermountain Medical Center
Objectives:
• Describe the epidemiological and pathology of NSTEMI • Review pre-hospital measures and ED diagnosis in possible
NSTEMI • Describe decision making for invasive vs. noninvasive therapies
The 2014 Non-ST-Elevation-Acute Coronary Syndrome Guidelines—
What’s New and Relevant to Clinical Practice?
Jeffrey L Anderson, MD, FACC, FAHA, MACP
Intermountain Heart Institute Intermountain Medical Center Murray, Utah

Disclosures: Member of “Advances in ACS Expert Consensus Panel” (unrestricted CME grant from Sanofi-Aventis); Consultant, Medicines Company (minor)

Pathophysiology of Non-ST-elevation and ST-elevation Acute Coronary Syndromes
STEMI NSTEMI
HeartSite.com. http://www.heartsite.com/html/cad.html
Cross Section Longitudinal Section
Clot Totally Blocking Channel
Cross Section Longitudinal Section
Clot Partially Obstructing
Channel Ruptured Plaque

Hospitalizations in the U.S. Due to Acute Coronary Syndromes
Acute Coronary Syndromes
1.83 Million Hospital Admissions - ACS
UA/NSTEMI STEMI
1.42 million admissions per year
0.41 million admissions per year
National Hospital Discharge Survey. National Center for Health Statistics/Centers for Disease Control and Prevention 2007. 3

2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes
Sept 23, 2014

6
Key Management Questions
1. Dx/Pathway? STEMI? UA/NSTEMI? Prob/Poss UA? (history, exam, ECG)
2. Risk? (troponin, ECG; TIMI, GRACE risk scores) 3. General management: bedrest, aspirin, O2, NTG,
beta-blocker, morphine (?) 4. Initial strategy?
a. Invasive? B. Initial conservative/medical? 5. Antiplatelet: Clopidogrel? Prasugrel? Ticagrelor?
Glycoprotein IIb/IIIa inhibitor? 6. Anticoagulant: UFH? LMWH? Bival? Fonda?

Troponin Levels Predict Risk of Mortality in UA/NSTEMI
Antman EM et al. N Engl J Med. 1996;335:1342-1949.
1 . 0 1 . 7
3 . 4 3 . 7
6 . 0
7 . 5
0
1
2
3
4
5
6
7
8
0 t o < 0 . 4 0 . 4 t o < 1 . 0 1 . 0 t o < 2 . 0 2 . 0 t o < 5 . 0 5 . 0 t o < 9 . 0 ≥ 9 . 0
Morta
lity at
42 da
ys; %
of pa
tients
831 174 148 134 50 67
% %
% %
%
%
C a r d i a c t r o p o n i n I ( n g / mL )

8
TIMI Risk Score 1. Age ≥65 y*
2. ≥3 CAD risk factors (high cholesterol, family history, hypertension, diabetes, smoking)*
3. Prior coronary stenosis ≥50%
4. Aspirin in last 7 days
5. ≥2 anginal events ≤24 h
6. ST-segment deviation*
7. Elevated cardiac markers* (Troponin or CK-MB)
Antman EM, et al. JAMA. 2000;284(7):835-842.
Number of Predictors
0
5
10
15
20
25
30
35
40
45
0/1 2 3 4 5 6/7
% D
eath
/ M
I / U
rgen
t Rev
asc
at 1
4 d

Non-ACS Causes of Elevated Troponin • Heart failure • Shock: septic, hypovolemic, cardiogenic • Injury: cardiac contusion, surgery, ablation, shocks • Inflammation: myocarditis, pericarditis • Cardiomyopathies: infiltrative, stress, hypertensive, hypertrophic • Aortic dissection, severe aortic stenosis • Tachycardias • Pulmonary: embolism/hypertension, respiratory failure • Neurologic: stroke, intracranial hemorrhage • Renal failure

AHA/ACC NSTE-ACS Guidelines: Early Risk Stratification
Perform rapid determination of likelihood of ACS, including a 12-lead ECG within 10 min of arrival at an ED. Perform serial ECGs at 15- to 30-min intervals during the first hour in symptomatic patients with initial non-diagnostic ECG. Measure cardiac troponin (cTnI or cTnT) in all patients with symptoms consistent with ACS. Measure serial cardiac troponin I or T at presentation and 3-6 h after symptom onset in all patients with symptoms consistent with ACS to identify a rising and/or falling pattern. Use risk scores to assess prognosis in patients with NSTE-ACS
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)

Troponin-I Testing at Intermountain for Probable or Possible NSTE-ACS

AHA/ACC NSTE-ACS Guidelines: General Early Hospital Care
Administer supplemental oxygen only with oxygen saturation <90%, respiratory distress, or other high-risk features for hypoxemia. Administer sublingual NTG every 5 min x 3 for continuing ischemic pain, then assess need for IV NTG. Administer oral beta blockers within the first 24 h in the absence of HF, low-output state, risk for cardiogenic shock, or other contraindications to beta blockade. Calcium channel blockers are recommended for ischemic symptoms when beta blockers are not successful, are contraindicated, or cause unacceptable side effects. Initiate or continue high-intensity statin therapy in patients with no contraindications.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)

High-Intensity Statin and Peri-PCI MI Meta-analysis of 13 Randomized Studies
Test for heterogeneity: Chi2 = 9.02, df = 11 (P = 0.62), I2 = 0%. Test for overall effect: Z = 4.67 (P < 0.00001). OR = odds ratio. Patti G, et al. Circulation. 2011;123:1622-1632.
Study No. of Patients With
Event/Total No. of Patients OR (fixed) 95% CI
Weight %
OR (fixed) 95% CI High-dose statin Controls
ARMYDA 3/76 9/77 4.86 0.31 (0.08 – 1.20) ARMYDA-ACS 5/86 9/85 4.83 0.52 (0.17 – 1.63) ARMYDA-RECAPTURE 7/192 15/191 8.20 0.44 (0.18 – 1.11) Bozbas 1/59 0/34 0.35 1.77 (0.07 – 44.64) Briguori 27/226 37/225 18.48 0.69 (0.40 – 1.18) Cay 0/153 16/146 9.52 0.03 (0.00 – 0.43) Hara 6/15 7/22 1.13 1.43 (0.24 – 8.64) Jia 0/113 0/115 Not estimable Kinoshita 2/21 4/21 2.05 0.45 (0.07 – 2.76) NAPLES II 32/339 52/329 27.05 0.56 (0.35 – 0.89) STATIN-STEMI 13/86 17/85 8.21 0.71 (0.32 – 1.58) Veselka 10/100 12/100 6.11 0.81 (0.33 – 1.98) Yun 12/225 17/220 9.21 0.67 (0.31 – 1.44) Total (95% CI) 100.0 0.56 (0.44 – 0.71)
10 5 2 1 0.5 0.2 0.1 Favors
high-dose statin Favors controls

Considerations for Choice of Stategy Immediate invasive Refractory angina strategy Signs/symptoms of HF, new/worsening mitral regurgitation (within 2 h) Hemodynamic instability
Recurrent angina/ischemia at rest or low-level activity _____________________ Sustained VT or VF________________________________ Ischemia-guided Low-risk score (e.g., TIMI 0/1, GRACE <109) strategy Low-risk, troponin-negative females _____________________ Patient/clinician preference and no high-risk features_____ Early invasive strategy None of above, but GRACE risk score >140 (within 24 h) Temporal change in troponin _____________________ New or presumably new ST depression________________ Delayed invasive None of the above but diabetes mellitus strategy Renal insufficiency (GFR <60 ml/min/1.73 sq-m) (within 25-72 h) Reduced LV systolic function (EF<0.40)
Early post-infarction angina PCI within 6 months Prior CABG GRACE score 109-140; TIMI score >=2.
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 ; Sept 23, 2014

Time (months) 0 1 2 3 4 5 6
0
4
8
12
16
20
% P
atie
nts
Conservative: Invasive:
O.R 0.78 95% CI (0.62, 0.97) P=0.025
19.4% 15.9%
TACTICS: Invasive vs Conservative Rx for Definite UA/NSTEMI Primary Endpoint: Death, MI, Rehospitalized for ACS at 6 Mo
Cannon CP et al. N Engl J Med. 2001;344:1879-1887.

*Low/intermediate risk=GRACE score <140 High risk=GRACE score ≥140 Early: Within 24 h (mean, 15 h); Delayed: After 36 h (mean, 50 h)
TIMACS: Timing of PCI in NSTE-ACS Rates of death, MI, or stroke within 6 mo by GRACE score:
HR (95% CI), early vs delayed invasive strategy
Mehta SR et al. N Engl J Med. 2009;310:2165-2175.
EARLY (%)
DELAYED (%)
Hazard Ratio (95% CI) P
Low/Intermediate (n=2070) 7.6 6.7 1.12 (0.88–
1.56) 0.48
High (n=961) 13.9 21.0 0.65 (0.48–
0.89) 0.006

Mechanisms of Platelet Aggregation and Antiplatelet Therapies in ACS
ADP = adenosine diphosphate, TXA2 = thromboxane A2, COX = cyclooxygenase. Adapted from Schafer AI. Am J Med. 1996;101:199-209.
Collagen Thrombin
TXA2
TXA2
ADP phosphodiesterase
ADP
(Aggregation) Gp IIb/IIIa
Activation
COX
clopidogrel
prasugrel
ticagrelor
aspirin
dipyridamole
cAMP
Heparins IIb/IIIa inhibitors


Aspirin Evidence: Secondary Prevention
Antithrombotic Trialist Collaboration. BMJ 2002;324:71–86
Category % Odds Reduction Acute MI Acute CVA Prior MI Prior CVA/TIA Other high risk CVD
(e.g. unstable angina, heart failure) PAD
(e.g. intermittent claudication) High risk of embolism (e.g. Afib) Other (e.g. DM) All trials
1.0 0.5 0.0 1.5 2.0 Control better Antiplatelet better
Effect of antiplatelet treatment* on vascular events**
*Aspirin was the predominant antiplatelet agent studied **Include MI, stroke, or death

Aspirin Evidence: Dose and Efficacy
0.5 1.0 1.5 2.0
500-1500 mg 34 19
160-325 mg 19 26
75-150 mg 12 32
<75 mg 3 13
Any aspirin 65 23
Antiplatelet Better
Antiplatelet Worse
Aspirin Dose No. of Trials (%) Odds Ratio for
Vascular Events
0 P<.0001
Indirect comparisons of aspirin doses on vascular events in high-risk patients
Antithrombotic Trialist Collaboration. BMJ 2002;324:71-86

Non-enteric-coated aspirin (162-325 mg/d) should be given to all NSTE-ACS patients promptly after presentation, and a maintenance dose (81-325 mg/d) should be continued indefinitely.
In NSTE-ACS patients unable to take aspirin because of hypersensitivity or GI intolerance, a loading dose of clopidogrel followed by a daily maintenance dose should be administered.
It is reasonable to use an aspirin maintenance dose of 81 mg per day in preference to higher maintenance doses in patients with NSTE-ACS treated either invasively or with coronary stent implantation
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
Aspirin Therapy for NSTE-ACS I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III

P2Y12 Inhibitor Basic Pharmacology
Clopidogrel Prasugrel Ticagrelor
Class Thienopyridine Thienopyridine Triazolopyrimidine
Reversibility Irreversible Irreversible Reversible
Activation Prodrug, limited by metabolism
Prodrug, not limited by metabolism
Active drug
Onset of Effect^ 2-4 hours 30 minutes 30 minutes
Duration of Effect 3-10 days 5-10 days 3-4 days
Withdrawal before major surgery
5 days 7 days 5 days
Hamm CW, et al. Eur Heart J. 2011. ^ 50% inhibition of platelet aggregation 22

0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
Cu
mu
lati
ve H
azar
d R
Clopidogrel + ASA*
3 6 9
Placebo + ASA*
Months of Follow-Up
P = 0.00009† N = 12,562
0 12
* In addition to other standard therapies.
The CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Clopidogrel in NSTE-ACS with Medical Therapy: MI/Stroke/CV Death
Overall Relative Risk
Reduction
20%
CURE
0.15
0.10
0.05
0.0 0 100 200 300 400
Days of follow-up
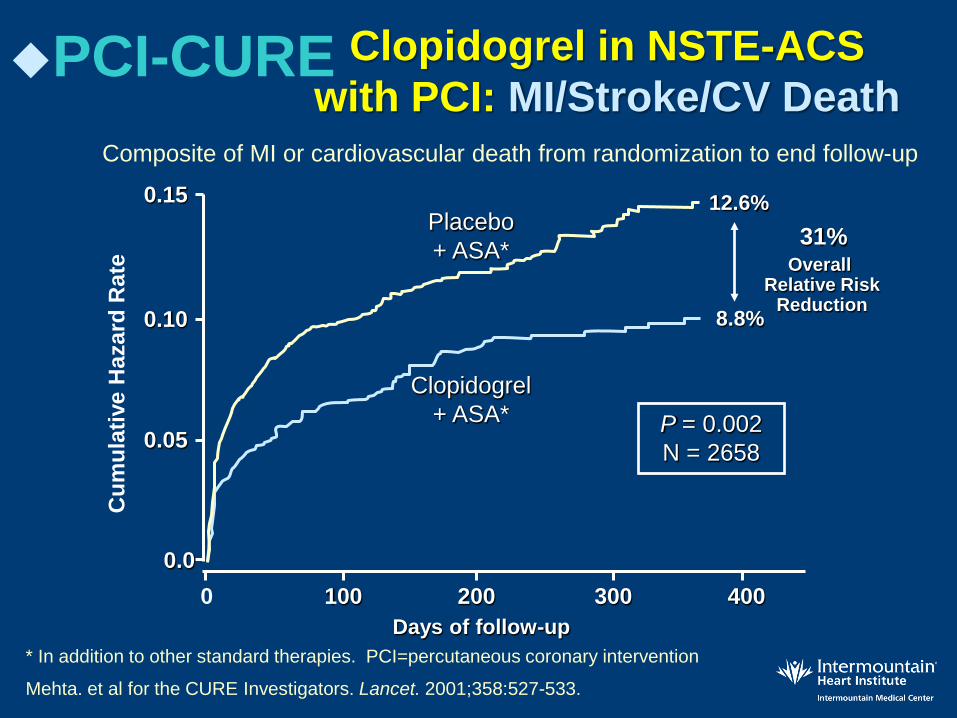
12.6%
8.8%
P = 0.002 N = 2658
Clopidogrel + ASA*
Placebo + ASA*
Cum
ulat
ive
Haz
ard
Rat
e
* In addition to other standard therapies. PCI=percutaneous coronary intervention
Mehta. et al for the CURE Investigators. Lancet. 2001;358:527-533.
Composite of MI or cardiovascular death from randomization to end follow-up
PCI-CURE
Overall Relative Risk
Reduction
31%
Clopidogrel in NSTE-ACS with PCI: MI/Stroke/CV Death

Placebo + ASA*
N = 6303
Clopidogrel + ASA*
N = 6259
Major bleeding 2.7% 3.7% †
Life-threatening bleeding 1.8% 2.2% ‡
Non–life-threatening bleeding 0.9% 1.5% §
• Minor bleeding 2.4% 5.1%
End Point
* In addition to other standard therapies. † P = 0.001; ‡ P = NS; § P = 0.002; P < 0.001.
The CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
CURE: Bleeding Results

Days
Cum
ulat
ive
Haz
ard
0.0
0.01
0.
02
0.03
0.
04
0 3 6 9 12 15 18 21 24 27 30
Clopidogrel: Double vs Standard Dose Primary Outcome: PCI Patients
Clopidogrel Standard
Clopidogrel Double
HR 0.85 95% CI 0.74-0.99
P=0.036
15% RRR
CV Death, MI or Stroke
Mehta. ESC 9/09

Variability in Antiplatelet Effect : Clopidogrel versus Prasugrel
IPA = inhibition of platelet aggregation Adapted from Brandt JT et al. Am Heart J. 2007;153:66.e9-e66.e16. Storey RF. Eur Heart J Suppl. 2008;10(suppl D):D30-D37.
-20
0
20
40
60
80
100
IPA
at 24
Hou
rs, %
Response to Prasugrel 60 mg
Response to Clopidogrel 300 mg
Clopidogrel Responder Clopidogrel Non-responder
Inte
rpat
ient
Varia
bilit
y Interpatient Variability
n = 64

TRITON-TIMI 38: Study Design
Double-blind: at cath, PCI planned
ACS (STEMI or UA/NSTEMI) & Planned PCI ASA
PRASUGREL 60 mg LD/ 10 mg MD
CLOPIDOGREL 300 mg LD/ 75 mg MD
1o endpoint: CV death, MI, Stroke 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic
Median duration of therapy - 12 months
N= 13,600
Wiviott SD et al. Am Heart J. 2006;152:627-35.

Prasugrel vs Clopidogrel for NSTE-ACS and STEMI: TRITON-TIMI 38 Primary Results:
CV Death, MI, Stroke
0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81 P=.0004 Prasugrel
Clopidogrel
HR 0.80 P=.0003
HR 0.77 P=.0001
Days
Prim
ary
End
Poin
t, %
12.1 (781)
9.9 (643)
NNT=46
ITT=13,608
Adapted from Wiviott SD, et al. N Engl J Med. 2007;357(20):2001-2015.

Primary endpoint = first occurrence of CV death, MI, or stroke
n Hazard Ratio Prasugrel
(%) Clopidogrel
(%) Females 320 13.6 20.5 Males 883 9.7 13.6
Age <75 979 9.3 13.0 Age ≥75 224 17.2 28.0
No Hx of DM 856 10.6 11.0 Hx of DM 347 11.7 27.0
UA/NSTEMI 893 12.1 15.2 STEMI 390 9.0 17.1
BMS only 571 10.7 17.0 DES 560 11.3 13.7
CrCl ≥60 1013 8.4 12.3 CrCI <60 176 26.2 31.7
TRITON-TIMI 38 Study: Subgroups
Murphy. Eur Heart J. 2008;29:2473-2479.
Prasugrel better
Clopidogrel better
0.2 1 5

TRITON TIMI 38 Bleeding Events – Safety Cohort (n=13,457)
% E
vent
s
ARD 0.6% HR 1.32 P=0.03
NNH=167
ARD 0.5% HR 1.52 P=0.01
ARD 0.2% P=0.23
ARD 0% P=0.74
ARD 0.3% P=0.002
Clop 0 (0) % Pras 6 (2.3)% (P=0.02)
Wiviott SD et al. N Engl J Med. 2007;357:2001-2015.
Life Threatening
TIMI Major Bleeds
Clopidogrel Prasugrel
0.9
2.4
1.4
0
2
4 ICH in patients with prior stroke/TIA (n=518)
0.9 1.1
0.1 0.4 0.3 0.3
Nonfatal Fatal ICH
1.8

32 32
TRITON-TIMI 38: Net Clinical Benefit Bleeding Risk Subgroups
Post hoc analysis
OVERALL
≥60 kg
<60 kg
<75
≥75
No
Yes
0.5 1 2
Prior Stroke / TIA
Age
Wgt
Risk (%) + 37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel Better HR
Pint = .006
Pint = .18
Pint = .36
Wiviott SD, et al. N Engl J Med. 2007;357(20):2001-2015.

PLATO study design
Primary endpoint: CV death + MI + Stroke Primary safety endpoint: Total major bleeding
6–12-month exposure
Clopidogrel If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI)
Ticagrelor 180 mg loading dose, then 90 mg bid maintenance; (additional 90 mg pre-PCI)
NSTE-ACS (moderate-to-high risk), STEMI (if primary PCI) Clopidogrel-treated or -naive; randomized within 24 hours of index event (N=18,624)
PLATO study design
James S et al. Am Heart J. 2009;157:599-605.
All patients received aspirin

PLATO: Ticagrelor vs. Clopidogel in NSTEMI and STEMI ACS
No. at risk
Clopidogrel Ticagrelor
9,291 9,333
8,521 8,628
8,362 8,460
8,124
Days after randomisation
6,743 6,743
5,096 5,161
4,047 4,147
0 60 120 180 240 300 360
12 11 10 9 8 7 6 5 4 3 2 1 0
13 C
V de
ath,
MI,
or C
VA in
cide
nce
(%)
9.8
11.7
8,219
HR 0.84 (95% CI 0.77–0.92), p=0.0003
Clopidogrel
Ticagrelor
K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval NEJM 09; 361:1045

No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,560
8,678
8,405
8,520
8,177
Days after randomisation
6,703
6,796
5,136
5,210
4,109
4,191
0 60 120 180 240 300 360
6
5
4
3
2
1
0
7
Cum
ulat
ive
inci
denc
e (%
)
Clopidogrel
Ticagrelor
5.8
6.9
8,279
HR 0.84 (95% CI 0.75–0.95), p=0.005
0 60 120 180 240 300 360
6
4
3
2
1
0
Clopidogrel
Ticagrelor
4.0
5.1
HR 0.79 (95% CI 0.69–0.91), p=0.001
7
5
9,291
9,333
8,865
8,294
8,780
8,822
8,589
Days after randomisation
7079
7119
5,441
5,482
4,364
4,419 8,626
Myocardial infarction Cardiovascular death
Cum
ulat
ive
inci
denc
e (%
)
PLATO: Secondary efficacy endpoints

PLATO: Non-invasive and Invasive Therapy Subgroups
0
4
8
12
16
20
0 60 120 180 240 300 360 Days after Randomization
Card
iova
scul
ar d
eath
, MI,
or S
trok
e (%
)
14.3%
12.0% HR 0.85 P=.04
Non-invasive Invasive
James SK, et al. BMJ. 2011.
Ticagrelor Clopidogrel
10.7%
9.0% HR 0.84 P=.0025

PLATO Major Bleeding: Non-CABG vs CABG
Kapl
an-M
eier e
stim
ated
rate
(%
)
Wallentin L et al. N Engl J Med. 2009;361:1045-1057.
P=0.026
P=0.025
NS
NS
Non-CABG PLATO major
bleeding
8
7
6
5
4
3
2
1
0 Non-CABG TIMI major bleeding
CABG PLATO major
bleeding
CABG TIMI major bleeding
4.5
3.8
2.8
2.2
7.4 7.9
5.3 5.8
Ticagrelor Clopidogrel

Ticagrelor Interaction with Aspirin Dose: HR Compared with Clopidogrel
Aspirin Dose (mg/day)
Hazard Ratio 95% CI
>= 300 1.45 1.01 – 2.09 >100 – <300 0.99 0.70 – 1.40 <=100 0.77 0.69 – 0.86
Warning: Aspirin Dose and Ticagrelor Effectiveness: Maintenance doses of aspirin above 100mg reduce the effectiveness of ticagrelor and should be avoided. After any initial dose, use with aspirin 75-100 mg per day (FDA-approved prescribing information, July 2011)

Summary • ASA 81 mg is the preferred dose after the initial
dose in ED or cath lab • Medically managed ACS
– Ticagrelor and clopidogrel indicated • Ticagrelor with superior efficacy/mortality
reduction – Prasugrel not indicated
• Invasively managed ACS – Ticagrelor, prasugrel, clopidogrel indicated – Ticagrelor, prasugrel superior efficacy
(ticagrelor mortality reduction) to clopidogrel with increased bleeding
• Duration of DAPT: generally one year

A loading dose of a P2Y12 receptor inhibitor (clopidogrel, prasugrel, or ticagrelor) should be given before the procedure in patients undergoing PCI with stenting.
It is reasonable to use ticagrelor in preference to clopidogrel for maintenance P2Y12 treatment in patients with NSTE-ACS who undergo an early invasive strategy or ischemia-guided strategy.
It is reasonable to choose prasugrel over clopidogrel in NSTE-ACS patients who undergo PCI and are not at high risk of bleeding.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
P2Y12 Inhibitors in NSTE-ACS with PCI/Stents
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)

A P2Y12 inhibitor (either clopidogrel or ticagrelor) in addition to aspirin should be given for up to 12 months for patients treated with either an early invasive or initial ischemia-guided strategy. It is reasonable to use ticagrelor in preference to clopidogrel for P2Y12 treatment in patients with NSTE-ACS who undergo an early invasive or ischemia-guided strategy. P2Y12 inhibitor therapy (clopidogrel, prasugrel, or ticagrelor) should be continued for at least 12 mo in post-PCI patients treated with coronary stents.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
P2Y12 Inhibitor Therapy in NSTE-ACS (continued)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)

Early Discontinuation of Antiplatelet Therapy is An Important Risk Factor for
Stent Thrombosis
ST = stent thrombosis
Iakovou I et al. JAMA. 2005;293:2126-2130.
UA Thrombus Diabetes Unprotected Left Main
Bifurcation Lesion
Renal Failure
Prior Brachytherapy
Overall ST=1.3% (P=0.09, n=2229)
1.4 2.0 2.5 3.3 3.6 6.2
8.7
29.0
0
10
20
30
Premature Antiplatelet
Discontinuation
Inci
denc
e of
ST
(%)

If the risk of morbidity from bleeding outweighs the anticipated benefit of a recommended duration of P2Y12 inhibitor therapy after stent implantation, earlier discontinuation (e.g., <12 months) of P2Y12 inhibitor therapy is reasonable In patients referred for elective CABG, clopidogrel and ticagrelor should be discontinued for at least 5 days before surgery (LOE: B) and prasugrel for at least 7 days before surgery (LOE:C)
I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I IIa IIa IIa IIb IIb IIb III III III IIa IIa Ia IIb IIb I III III I
P2Y12 Inhibitor Therapy in NSTE-ACS (continued)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III

In patients with NSTE-ACS, anticoagulation, in addition to antiplatelet therapy, is recommended for all patients irrespective of initial treatment strategy. Treatment options include: --Enoxaparin (LOE:A) --Bivalirudin (LOE:B) --Fondaparinux (LOE:B) --Unfractionated heparin (LOE:B) If PCI is performed while the patient is on fondaparinux, an additional anticoagulant with anti-IIa activity (either UFH or bivalirudin) should be administered because of the risk of catheter thrombosis (LOE:B)
I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I IIa IIa IIa IIb IIb IIb III III III IIa IIa Ia IIb IIb I III III I
Anticoagulant Therapy for NSTE-ACS
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2014 AHA/ACC NSTE-ACS Guideline. Circulation 2014 (Epub ahead of print, Sept 23, 2014)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III

Post-hospital systems of care designed to prevent hospital readmissions should be used to facilitate the transition to effective, coordinated outpatient care for all patients with NSTE-ACS. An evidence-based plan of care that promotes medication adherence, timely follow-up, appropriate dietary and physical activities, and compliance with secondary prevention should be provided to patients with NSTE-ACS. Annual influenza vaccination for all patients.
2014 AHA/ACC NSTE-MI Guidelines
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
General Plan of Outpatient Care for Patients with NSTE-ACS
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III

Secondary Prevention* Recommendations COR LOE
Lipid management with lifestyle modification and lipid-lowering therapy
Beta blocker therapy
RAAS blocker therapy
Lifestyle modification I B
Statin therapy—mod/high intensity
I A
For 3 y in pts with normal LVF All pts with EF<40, HF, prior MI
I B A
ACEI if HTN, DM, EF<40, CKD Use ARBs if intolerant of ACEIs
I A
Blood pressure control (with a blood pressure goal of <140/90 mm Hg)
Lifestyle modification I B
Pharmacotherapy I A
Diabetes management (e.g., lifestyle modification and pharmacotherapy) coordinated with the patient’s primary care physician and/or endocrinologist.
I C
Complete smoking cessation I A
In addition, referral to a cardiac rehabilitation program (IB). *Comprehensive secondary prevention recommendations in the ACC/AHA Secondary Prevention and Risk Reduction 2011 and 2013 Updates and 2012 SIHD Guidelines GNL 2011

Performance Matters! Association Between Hospital Guideline
Adherence and In-hospital Mortality in CRUSADE
Adapted with permission from Peterson ED, et al. JAMA. 2006;295(16):1912-1920.
NSTE ACS = non–ST-segment elevation ACS.
8
7
6
5
4
3
2
1
0 1 2 3 4
In-H
ospi
tal M
orta
lity,
%
Hospital Composite Guideline Adherence Quartiles
NSTE ACS
CRUSADE = Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines.

Impact of Adherence to Evidence-based
Therapies: Effect on 6-month Survival in the GRACE Registry Cohort*
OR = odds ratio *Registry of patients with ACS
Chew DP et al. Heart. 2010;96:1201-1206.
0.80 (0.52-1.26)
0.74 (0.48-1.13)
0.59 (0.39-0.90)
0.51 (0.33-0.78)
0.40 (0.26-0.62)
0.27 (0.16-0.44)
0.31 (0.17-0.57)
NUMBER OF THERAPIES (vs 0 or 1 therapy)
2 therapies
3 therapies
4 therapies
5 therapies
6 therapies
7 therapies
8 therapies
OR (95% CI)
0 0.5 1 1.5 2 OR

CONCLUSION
Early Diagnosis, Risk Stratification,
Strategy Selection, and Appropriate
Antithrombotic and Other Guideline-
Directed Medical Therapy Make a
Difference in ACS Outcomes!
Equally Important is Aggressive
Secondary Prevention after Discharge!