the adnexal mass and early ovarian cancerobgyn.med.uky.edu/sites/default/files/the adnexal...
TRANSCRIPT
The Adnexal Mass
The Adnexal Mass
and Early Ovarian Cancer
and Early Ovarian Cancer
Fred Ueland, MD
University of Kentucky
Gynecologic Oncology
Fred Ueland, MD
Fred Ueland, MD
University of Kentucky
University of Kentucky
Gynecologic Oncology
Gynecologic Oncology
“
“
Never give in. Never give
Never give in. Never give
in. Never, never, never,
in. Never, never, never,
never
never
-
-
in nothing great or
in nothing great or
small, large or petty
small, large or petty
-
-
never give in, except to
never give in, except to
convictions of honor
convictions of honor
and good sense.
and good sense.
”
”
Sir Winston Churchill
Sir Winston Churchill

Ovarian Tumors
Ovarian Tumors
Who Cares?
Who Cares?
Surgical costs exceed
Surgical costs exceed
$5,000,000,000 annually
$5,000,000,000 annually
144 million women in USA
144 million women in USA
– 5-10% will undergo a surgical
procedure for a suspected ovarian
neoplasm during their lifetime
30 million women over age 50
30 million women over age 50
–
–
17% develop cystic ovarian
17% develop cystic ovarian
tumors
tumors
–
–
2 million have persistent tumors
2 million have persistent tumors

Risk of Malignancy
Risk of Malignancy
Management challenge is an accurate risk
Management challenge is an accurate risk
of malignancy assessment.
of malignancy assessment.
Risk of malignancy within an ovarian
Risk of malignancy within an ovarian
neoplasm varies with age:
neoplasm varies with age:
–
–
10% in children
10% in children
–
–
15% in reproductive age women
15% in reproductive age women
–
–
50% in postmenopausal women
50% in postmenopausal women

Ovarian Tumors
Ovarian Tumors
Premenopausal Women
Premenopausal Women
Non
Non
-
-
inflammatory ovarian tumors
inflammatory ovarian tumors
–
–
70% functional cysts
70% functional cysts
–
–
20% neoplastic
20% neoplastic
–
–
10% endometriomas
10% endometriomas
15% of ovarian neoplasms in reproductive
15% of ovarian neoplasms in reproductive
age women are malignant
age women are malignant
Other
Other
–
–
Inflammatory process, bowel
Inflammatory process, bowel

Ovarian Tumors
Ovarian Tumors
Premenopausal Women
Premenopausal Women
Functional cysts
Functional cysts
–
–
<
<
8 cm
8 cm
–
–
Unilateral
Unilateral
–
–
Simple, unilocular on TVS
Simple, unilocular on TVS
–
–
No ascites
No ascites
Initial repeat TVS 6
Initial repeat TVS 6
-
-
8 weeks
8 weeks
OCPs do not increase likelihood of
OCPs do not increase likelihood of
resolution, but may decrease risk of
resolution, but may decrease risk of
recurrence
recurrence
Ovarian Tumors
Ovarian Tumors
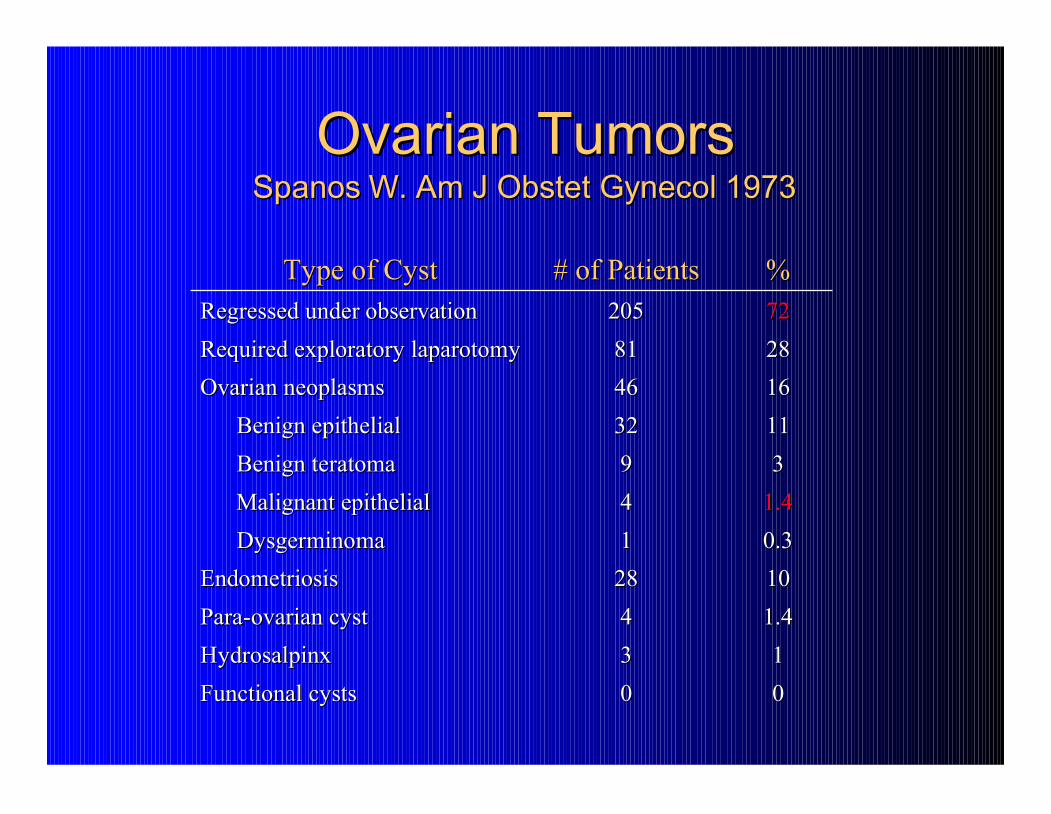
Spanos W. Am J Obstet Gynecol 1973
Spanos W. Am J Obstet Gynecol 1973
0
0
0
0
Functional cysts
Functional cysts
1
1
3
3
Hydrosalpinx
Hydrosalpinx
1.4
1.4
4
4
Para
Para
-
-
ovarian cyst
ovarian cyst
10
10
28
28
Endometriosis
Endometriosis
0.3
0.3
1
1
Dysgerminoma
Dysgerminoma
1.4
1.4
4
4
Malignant epithelial
Malignant epithelial
3
3
9
9
Benign teratoma
Benign teratoma
11
11
32
32
Benign epithelial
Benign epithelial
16
16
46
46
Ovarian neoplasms
Ovarian neoplasms
28
28
81
81
Required exploratory laparotomy
Required exploratory laparotomy
72
72
205
205
Regressed under observation
Regressed under observation
%
%
# of Patients
# of Patients
Type of Cyst
Type of Cyst

Ovarian Tumors
Ovarian Tumors
Modesitt et al, Gyn Oncol 2003
Modesitt et al, Gyn Oncol 2003
Spontaneous Resolution
Spontaneous Resolution
2261
2261
(69%)
(69%)
Cyst + Septum
Cyst + Septum
537 (17%)
537 (17%)
Persistent Cyst
Persistent Cyst
220 (7%)
220 (7%)
Cyst +Solid area
Cyst +Solid area
168 (5%)
168 (5%)
Solid Mass
Solid Mass
21 (0.6%)
21 (0.6%)
Removed by unrelated surgery
Removed by unrelated surgery
40 (1.2%)
40 (1.2%)
3,259
3,259
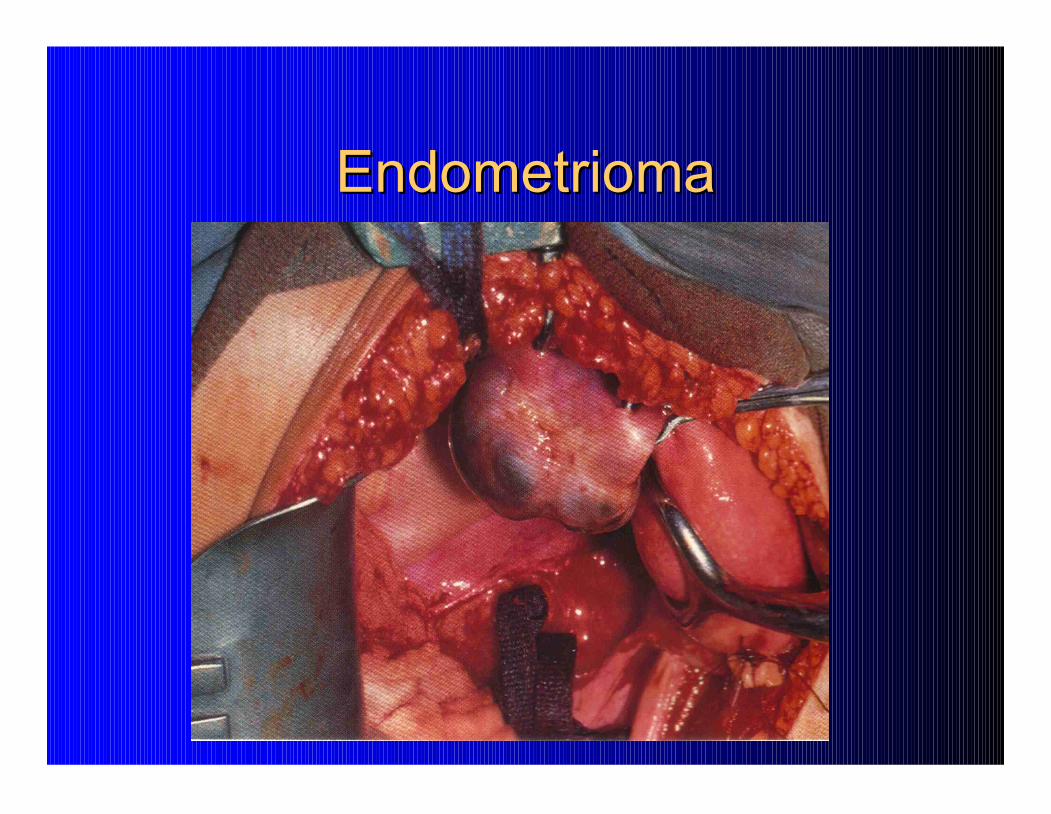
Endometrioma
Endometrioma

Mucinous Cystadenoma
Mucinous Cystadenoma
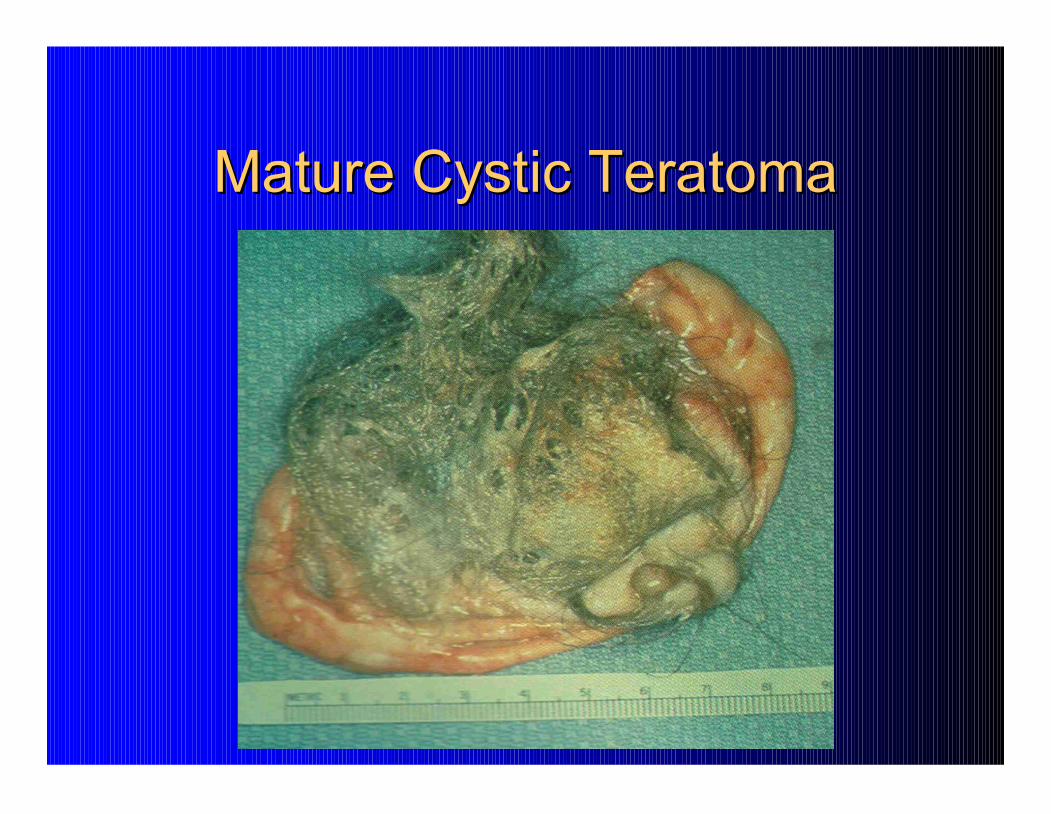
Mature Cystic Teratoma
Mature Cystic Teratoma

Ovarian Dysgerminoma
Ovarian Dysgerminoma

Ovarian Tumors
Ovarian Tumors
Postmenopausal Women
Postmenopausal Women
Benign epithelial tumor
Benign epithelial tumor
Stromal tumor
Stromal tumor
–
–
Granulosa cell
Granulosa cell
–
–
Fibroma
Fibroma
–
–
Thecoma
Thecoma
Epithelial cancer
Epithelial cancer
Metastatic cancer
Metastatic cancer

Ovarian Tumors
Ovarian Tumors
Postmenopausal Women
Postmenopausal Women
50% malignant
50% malignant
Asymptomatic simple cyst < 10 cm with
Asymptomatic simple cyst < 10 cm with
normal CA
normal CA
-
-
125
125
–
–
serial TVS
serial TVS
“Any ovarian tumor in a postmenopausal
“Any ovarian tumor in a postmenopausal
woman that does not meet the above criteria
woman that does not meet the above criteria
should be assumed to be malignant”
should be assumed to be malignant”
–
–
Antiquated?
Antiquated?
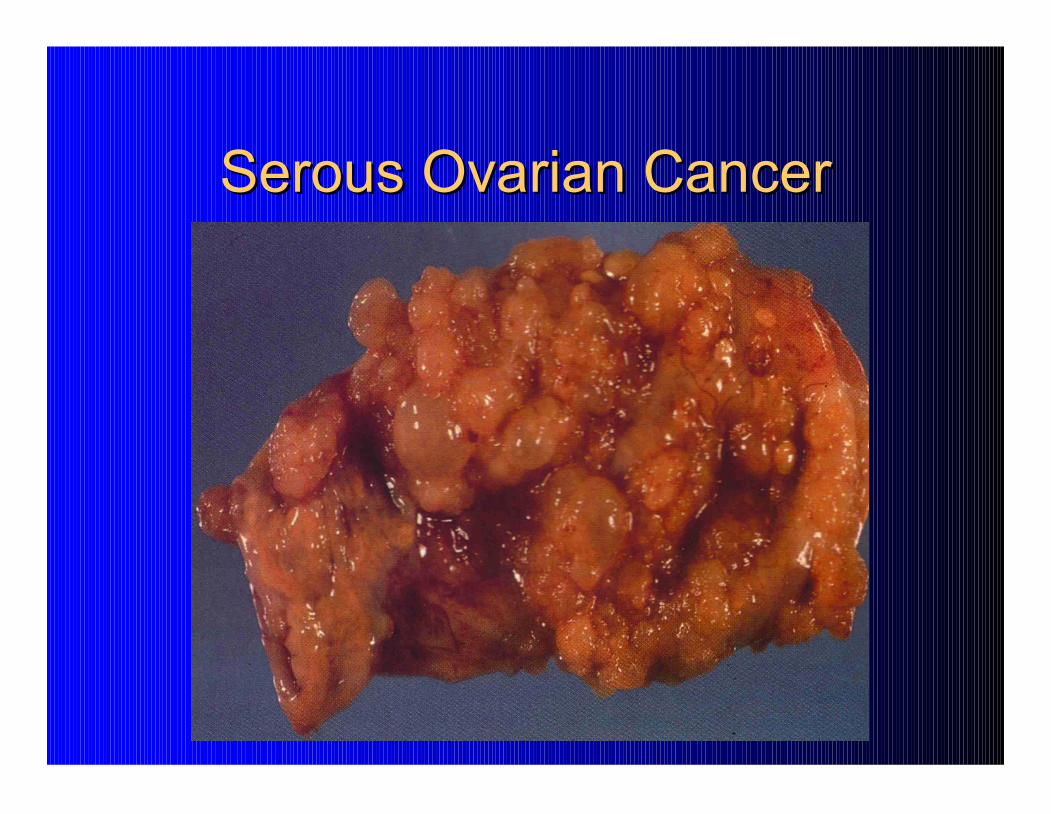
Serous Ovarian Cancer
Serous Ovarian Cancer

Who Gets Referred to a Cancer
Who Gets Referred to a Cancer
Specialist?
Specialist?
Benefits of Surgical Staging?
Benefits of Surgical Staging?
Patients in whom comprehensive surgical
Patients in whom comprehensive surgical
staging confirms early
staging confirms early
-
-
stage disease have a
stage disease have a
better prognosis
better prognosis
than those who were
than those who were
thought to have early stage disease but were
thought to have early stage disease but were
unstaged
unstaged
Accurate identification of women who
Accurate identification of women who
require adjuvant chemotherapy
require adjuvant chemotherapy

Appropriate Staging
Appropriate Staging
Women with
Women with
early stage
early stage
ovarian cancer
ovarian cancer
–
–
N=291
N=291
Complete surgical staging:
Complete surgical staging:
–
–
97% gynecologic oncologists
97% gynecologic oncologists
–
–
52% general obstetrician/gynecologists
52% general obstetrician/gynecologists
–
–
35% general surgeons
35% general surgeons
McGowan L, et al. Obstet Gynecol 1985;65:568-72.

Referral Patterns
Referral Patterns
Utah Cancer Registry: 848 new ovarian cancers
Utah Cancer Registry: 848 new ovarian cancers
diagnosed 1992
diagnosed 1992
-
-
1998
1998
Only 39% were
Only 39% were
ever
ever
seen by a Gyn Onc
seen by a Gyn Onc
Patients with advanced disease had significant
Patients with advanced disease had significant
survival advantage when managed by Gyn Onc
survival advantage when managed by Gyn Onc
(median survival 26 mo vs. 15 mo, p < 0.01)
(median survival 26 mo vs. 15 mo, p < 0.01)
Age < 40, age > 70, and residence in a rural area
Age < 40, age > 70, and residence in a rural area
were not seen by a gynecologic oncologist
were not seen by a gynecologic oncologist
Carney ME, et al. Gynecol Oncol 2002;84:36
Carney ME, et al. Gynecol Oncol 2002;84:36
-
-
42.
42.

Value of Specialists
Value of Specialists
Meta
Meta
-
-
analysis (18 studies) concluded marked benefit with
analysis (18 studies) concluded marked benefit with
Gynecologic Oncologist (
Gynecologic Oncologist (
Giede
Giede
2005)
2005)
–
–
Complete surgical staging with early stage disease
Complete surgical staging with early stage disease
–
–
Optimal cytoreductive surgery with advanced disease
Optimal cytoreductive surgery with advanced disease
–
–
Improved median and overall survival
Improved median and overall survival
Others supporting GO involvement:
Others supporting GO involvement:
–
–
NCCN guidelines
NCCN guidelines
–
–
SGO, ACOG
SGO, ACOG
–
–
SOGC clinical practice guidelines
SOGC clinical practice guidelines
–
–
NIH consensus statement
NIH consensus statement
–
–
London Medical Advisory statement
London Medical Advisory statement

Suggestive of Malignancy
Suggestive of Malignancy
ACOG, SGO
ACOG, SGO
Examination
Examination
–
–
Fixed or nodular
Fixed or nodular
Imaging study
Imaging study
–
–
Mostly solid tumor or distant mets
Mostly solid tumor or distant mets
–
–
Ascites
Ascites
CA
CA
-
-
125
125
–
–
premenopausal
premenopausal
> 200
> 200
–
–
postmenopausal
postmenopausal
> 35
> 35
Im et. al. Obstet Gynecol , 2005
Im et. al. Obstet Gynecol , 2005

So How Do I Know Who Gets
So How Do I Know Who Gets
Referred and Who Doesn’t?
Referred and Who Doesn’t?
Examination
Examination
Imaging
Imaging
Serum
Serum
Pelvic Examination
Pelvic Examination

Pelvic Examination
Pelvic Examination
Inaccuracy
Inaccuracy
Patient age
Patient age
≥
≥
55
55
–
–
30%
30%
Patient weight
Patient weight
≥
≥
200 lb
200 lb
–
–
9%
9%
Uterine weight
Uterine weight
≥
≥
200 g
200 g
–
–
16%
16%
Ueland et al, Gyn Oncol 2005
Ueland et al, Gyn Oncol 2005

So How Do I Know Who Gets
So How Do I Know Who Gets
Referred and Who Doesn’t?
Referred and Who Doesn’t?
Examination
Examination
Imaging
Imaging
Serum
Serum
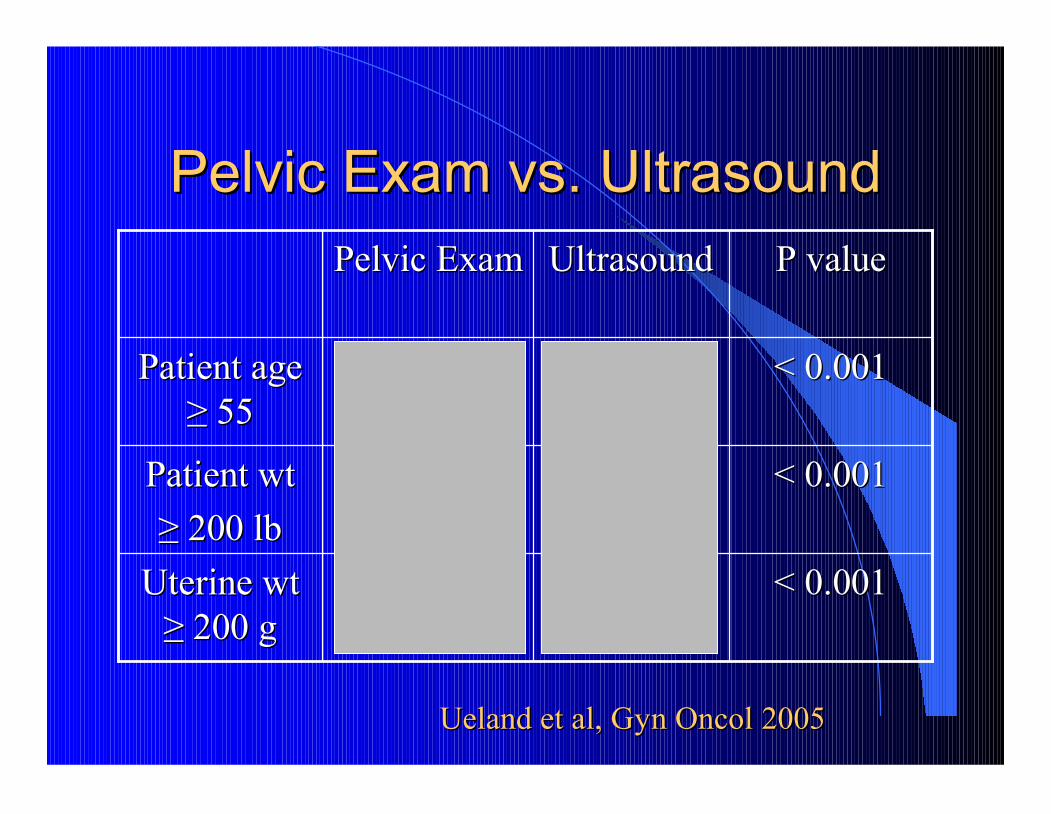
Pelvic Exam vs. Ultrasound
Pelvic Exam vs. Ultrasound
< 0.001
< 0.001
0.80
0.80
0.16
0.16
Uterine wt
Uterine wt
≥
≥
200 g
200 g
< 0.001
< 0.001
0.73
0.73
0.09
0.09
Patient wt
Patient wt
≥
≥
200 lb
200 lb
< 0.001
< 0.001
0.74
0.74
0.30
0.30
Patient age
Patient age
≥
≥
55
55
P value
P value
Ultrasound
Ultrasound
Pelvic Exam
Pelvic Exam
Ueland et al, Gyn Oncol 2005
Ueland et al, Gyn Oncol 2005
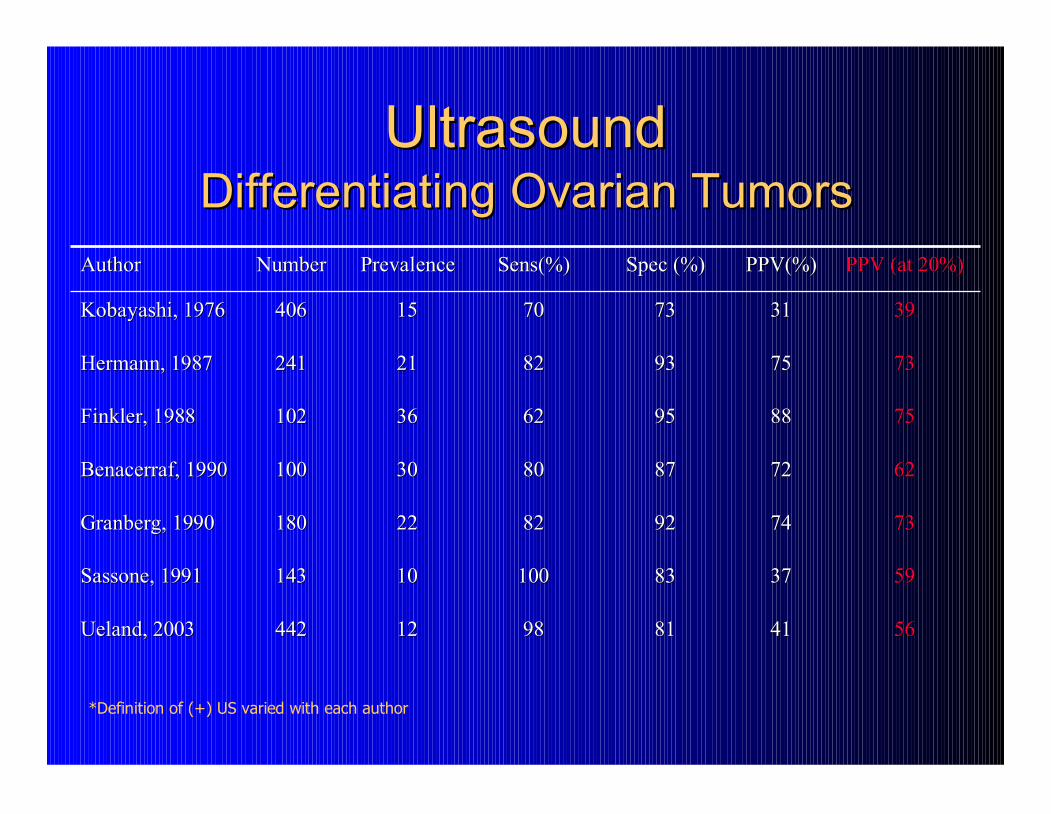
Ultrasound
Ultrasound
Differentiating Ovarian Tumors
Differentiating Ovarian Tumors
*Definition of (+) US varied with each author
56
56
41
41
81
81
98
98
12
12
442
442
Ueland, 2003
Ueland, 2003
59
59
37
37
83
83
100
100
10
10
143
143
Sassone, 1991
Sassone, 1991
73
73
74
74
92
92
82
82
22
22
180
180
Granberg, 1990
Granberg, 1990
62
62
72
72
87
87
80
80
30
30
100
100
Benacerraf, 1990
Benacerraf, 1990
75
75
88
88
95
95
62
62
36
36
102
102
Finkler, 1988
Finkler, 1988
73
73
75
75
93
93
82
82
21
21
241
241
Hermann, 1987
Hermann, 1987
39
39
31
31
73
73
70
70
15
15
406
406
Kobayashi, 1976
Kobayashi, 1976
PPV (at 20%)
PPV (at 20%)
PPV(%)
PPV(%)
Spec (%)
Spec (%)
Sens(%)
Sens(%)
Prevalence
Prevalence
Number
Number
Author
Author

Sonographic Characteristics
Sonographic Characteristics
Ovarian Tumors
Ovarian Tumors
Unilateral
Unilateral
Simple (MI < 5)
Simple (MI < 5)
Doppler
Doppler
–
–
PI > 1.0, RI > 0.4
PI > 1.0, RI > 0.4
–
–
Peripheral flow
Peripheral flow
No ascites
No ascites
Resolution
Resolution
Bilateral
Bilateral
Complex (MI
Complex (MI
≥
≥
5)
5)
–
–
Partly solid
Partly solid
–
–
Internal papillations
Internal papillations
Doppler
Doppler
–
–
PI < 1.0, RI < 0.4
PI < 1.0, RI < 0.4
–
–
Central flow
Central flow
Ascites
Ascites
Persistence or growth
Persistence or growth
Benign
Benign
Malignant
Malignant

Kentucky Morphology Index
Kentucky Morphology Index
Ueland et al Gyn Oncol 2003
Ueland et al Gyn Oncol 2003
UK gynecologic
UK gynecologic
ultrasound database
ultrasound database
442 women with
442 women with
confirmed ovarian
confirmed ovarian
tumor
tumor
–
–
Morphology Indexing
Morphology Indexing
–
–
Color Flow Doppler
Color Flow Doppler
–
–
Surgery
Surgery

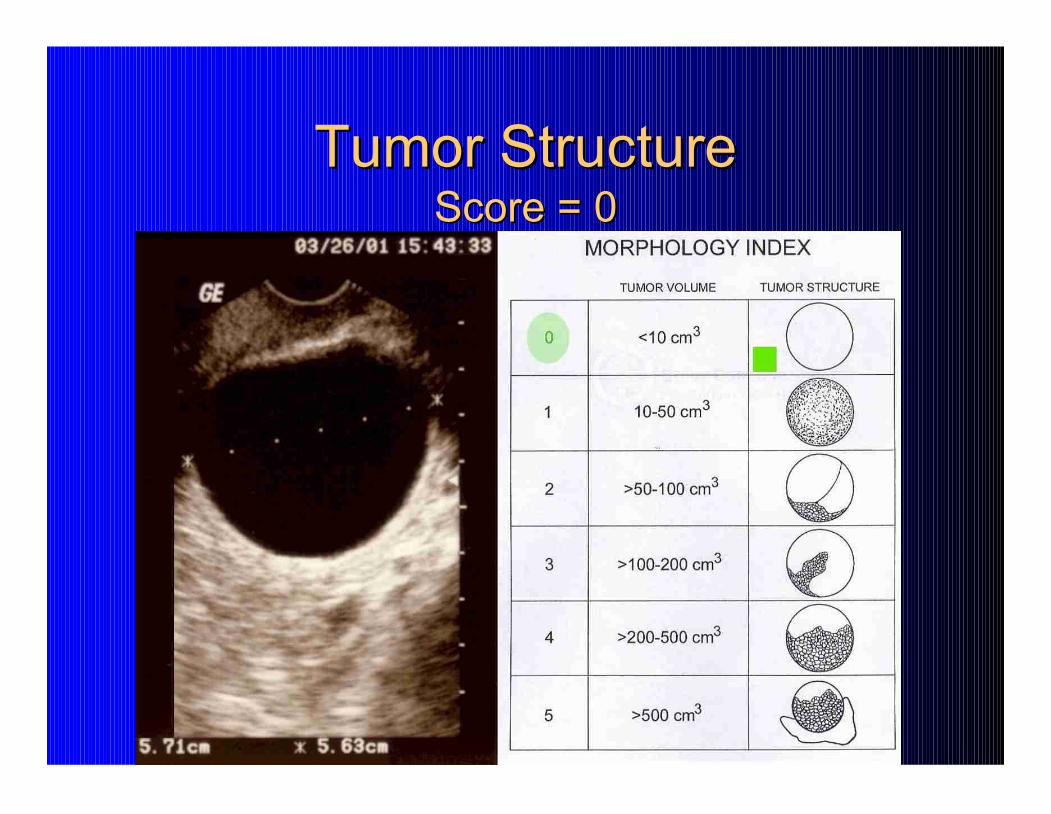
Tumor Structure
Tumor Structure
Score = 0
Score = 0

Tumor Structure
Tumor Structure
Score = 3
Score = 3

Tumor Structure
Tumor Structure
Score = 5
Score = 5
Morphology Index
Morphology Index
Total Score (0
Total Score (0
-
-
4)
4)
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4
% Benign
% Cancer

Morphology Index
Morphology Index
Total Score (5
Total Score (5
-
-
10)
10)
0
10
20
30
40
50
60
70
80
90
100
5 6 7 8 9 10
% Benign
% Cancer
20
32
38
92
77
83

Kentucky Morphology Index
Kentucky Morphology Index
MI
MI
< 5
< 5
benign
benign
MI
MI
≥
≥
5
5
malignant
malignant

Kentucky Morphology Index
Kentucky Morphology Index
Sensitivity
Sensitivity
0.981
0.981
Specificity
Specificity
0.807
0.807
Positive predictive value
Positive predictive value
0.409
0.409
Negative predictive value
Negative predictive value
0.997
0.997
Accuracy
Accuracy
0.828
0.828
Disease Prevalence = 12%
Disease Prevalence = 12%
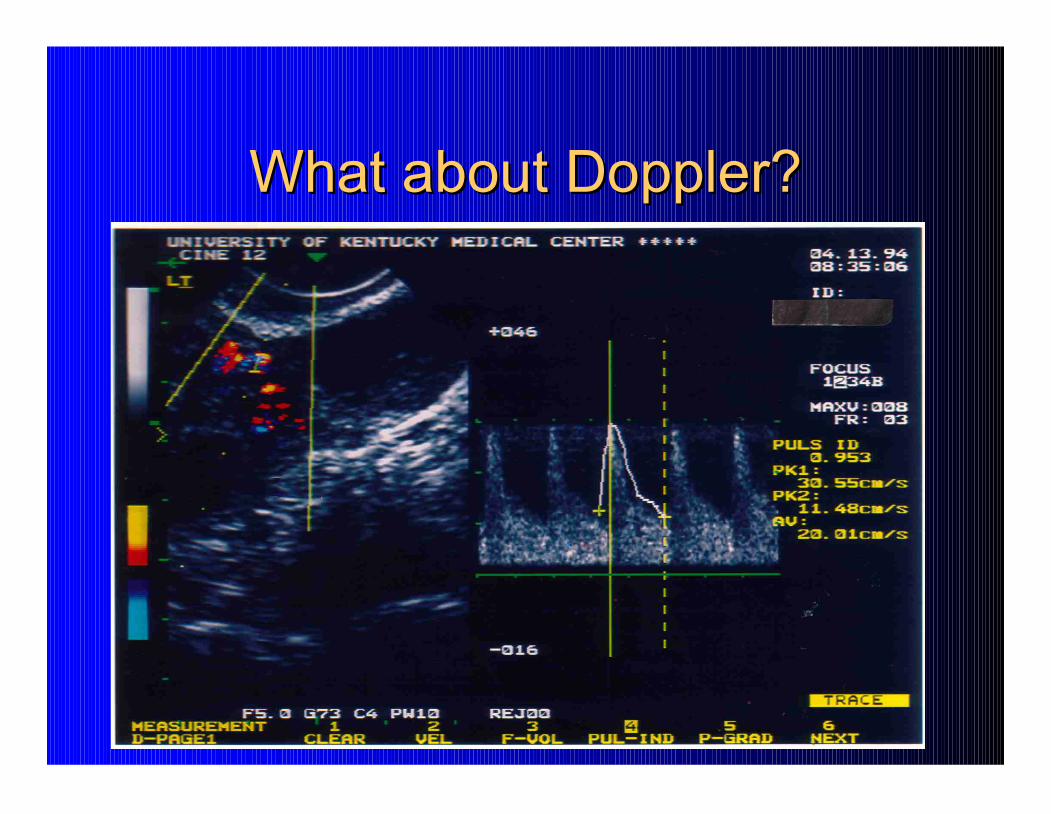
What about Doppler?
What about Doppler?

Doppler
Doppler
0.997
0.997
0.409
0.409
0.807
0.807
0.981
0.981
MI
MI
0.854
0.854
0.056
0.056
0.640
0.640
0.163
0.163
No flow
No flow
0.867
0.867
0.222
0.222
0.867
0.867
0.222
0.222
RI < 0.4
RI < 0.4
0.905
0.905
0.288
0.288
0.776
0.776
0.528
0.528
PI < 1.00
PI < 1.00
NPV
NPV
PPV
PPV
Spec
Spec
Sens
Sens

θ
θ
f
f
0
0
= transmitted US frequency
= transmitted US frequency
v cos
v cos
θ
θ
= target velocity
= target velocity
TVS probe
TVS probe
c
c
= velocity of surrounding medium
= velocity of surrounding medium
vessel
vessel
∆
∆
f = 2f
f = 2f
0
0
v (cos
v (cos
θ
θ
) / c
) / c

Doppler Reproducibility
Doppler Reproducibility
∆
∆
f = 2f
f = 2f
0
0
v (cos
v (cos
θ
θ
) / c
) / c
Is the angle of insonation constant (
Is the angle of insonation constant (
θ
θ
)?
)?
–
–
2 to 3 fold change for
2 to 3 fold change for
∆
∆
θ
θ
(from 30
(from 30
°
°
-
-
80
80
°
°
)*
)*
–
–
Optimal angle and frequency depends on depth
Optimal angle and frequency depends on depth
of vessel
of vessel
Is each Doppler measurement of the same
Is each Doppler measurement of the same
vessel? Are these vessels straight?
vessel? Are these vessels straight?
*J Vasc Surg 1990; 11:688
*J Vasc Surg 1990; 11:688
-
-
94
94

Ultrasound Conclusions
Ultrasound Conclusions
1.
1.
MI
MI
≥
≥
5
5
40% malignant
40% malignant
2.
2.
MI < 5
MI < 5
0.3% malignant
0.3% malignant
3.
3.
Doppler adds little
Doppler adds little

Other Imaging
Other Imaging
CT scan abdomen and pelvis
CT scan abdomen and pelvis
–
–
IV and PO contrast
IV and PO contrast
–
–
CT
CT
-
-
guided biopsy
guided biopsy
Accuracy exceeds 90% for solid tumors
Accuracy exceeds 90% for solid tumors
What about high risk cystic tumors?
What about high risk cystic tumors?
MRI
MRI
PET
PET

CT Scan
CT Scan
Omental cake
Ovarian tumor
So How Do I Know Who Gets
So How Do I Know Who Gets
Referred and Who Doesn’t?
Referred and Who Doesn’t?
Examination
Examination
Imaging
Imaging
Serum
Serum
CA
CA
-
-
125
125
Antigen derived from:
Antigen derived from:
–
–
coelomic
coelomic
epithelium (pericardium, pleura, peritoneum)
epithelium (pericardium, pleura, peritoneum)
–
–
mullerian
mullerian
epithelium (tubal, endometrial,
epithelium (tubal, endometrial,
endocervical
endocervical
)
)
Two different assays
Two different assays
–
–
Assay I
Assay I
<
<
35 U/ml
35 U/ml
–
–
Assay II < 20 U/ml
Assay II < 20 U/ml
Expressed by 80% non
Expressed by 80% non
-
-
mucinous EOC
mucinous EOC
FDA
FDA
-
-
approved to follow the progress of cancer treatment
approved to follow the progress of cancer treatment
–
–
Neither a screening nor a diagnostic test
Neither a screening nor a diagnostic test
Normal CA
Normal CA
-
-
125 values (low sensitivity)
125 values (low sensitivity)
–
–
50% of early stage ovarian cancers
50% of early stage ovarian cancers
–
–
20
20
-
-
25% of advanced stage ovarian cancers
25% of advanced stage ovarian cancers
–
–
Mixed mullerian tumors, clear cell cancers
Mixed mullerian tumors, clear cell cancers

CA
CA
-
-
125
125
Non
Non
-
-
specific
specific
Benign ovarian cysts
Benign ovarian cysts
Uterine leiomyomata
Uterine leiomyomata
Pelvic inflammatory
Pelvic inflammatory
disease
disease
Endometriosis
Endometriosis
Adenomyosis
Adenomyosis
Pregnancy
Pregnancy
Menstruation
Menstruation
Ascites
Ascites
Heart failure
Heart failure
Liver failure
Liver failure
Renal failure
Renal failure
Peritoneal tuberculosis
Peritoneal tuberculosis
Diverticulitis
Diverticulitis
Pancreatitis
Pancreatitis
Recent abdominal or
Recent abdominal or
thoracic surgery
thoracic surgery
Other malignancies
Other malignancies
So Again, What Should I Do?
So Again, What Should I Do?
Surgical removal of ovarian
Surgical removal of ovarian
tumor if symptomatic or
tumor if symptomatic or
high risk
high risk
imaging
imaging
Sonographic
Sonographic
observation if
observation if
asymptomatic, low risk MI
asymptomatic, low risk MI
–
–
6 wks, 3 mo, 6 mo
6 wks, 3 mo, 6 mo
CT scan abdomen/pelvis if
CT scan abdomen/pelvis if
suspect malignancy
suspect malignancy
High Risk Indicators
High Risk Indicators
Ultrasound
Ultrasound
(Ueland et al, 2003; Sassone et al, 1991)
(Ueland et al, 2003; Sassone et al, 1991)
–
–
Internal papillary projection
Internal papillary projection
–
–
Cystic and solid, solid
Cystic and solid, solid
–
–
Ascites
Ascites
CT Scan/MRI
CT Scan/MRI
(Kurtz et al 1999)
(Kurtz et al 1999)
–
–
Cystic and solid, solid
Cystic and solid, solid
–
–
Ascites
Ascites
CA
CA
-
-
125
125
(Roman et al, 1997)
(Roman et al, 1997)
–
–
Premenopausal >100 U/mL
Premenopausal >100 U/mL
–
–
Postmenopausal >35 U/mL
Postmenopausal >35 U/mL

Laparoscopy
Laparoscopy
Ovarian Tumor
Ovarian Tumor
Laparoscopy
Laparoscopy
Guidelines
Guidelines
Prepared for laparotomy
Prepared for laparotomy
–
–
Informed consent
Informed consent
Surgical technique
Surgical technique
–
–
Abdominopelvic inspection, biopsy
Abdominopelvic inspection, biopsy
–
–
Washings
Washings
–
–
Tumor removal and containment with endoscopic bag
Tumor removal and containment with endoscopic bag
–
–
No morcellation, please
No morcellation, please
–
–
Intraoperative frozen section
Intraoperative frozen section
Principles
Principles
Ovarian Tumor
Ovarian Tumor
Laparoscopy
Laparoscopy
Be principled
Be principled
–
–
Do not delay treatment to “confirm diagnosis” at
Do not delay treatment to “confirm diagnosis” at
laparoscopy
laparoscopy
–
–
For high risk tumor, consider referral to specialist
For high risk tumor, consider referral to specialist
–
–
Informed consent for surgery includes explanation of
Informed consent for surgery includes explanation of
alternatives
alternatives
–
–
“What would I do for my mother?”
“What would I do for my mother?”

Ovarian Cancer
Ovarian Cancer
Incidence and Mortality
Incidence and Mortality
Data from the
Data from the
American Cancer
American Cancer
Society
Society
200 Kentucky deaths from ovarian cancer in 2006
200 Kentucky deaths from ovarian cancer in 2006

Stage and Outcome
Stage and Outcome
50%
50%
Overall
Overall
0
0
-
-
20%
20%
15
15
IV
IV
15
15
-
-
30%
30%
55
55
III
III
65%
65%
6
6
II
II
95%
95%
24
24
I
I
Survival
Survival
Percent
Percent
Stage
Stage
American
American Cancer Society

Ovarian Cancer
Ovarian Cancer
Symptoms
Symptoms
Survey distributed to 1500 women who
Survey distributed to 1500 women who
subscribe to
subscribe to
CONVERSATIONS!,
CONVERSATIONS!,
a
a
newsletter about ovarian carcinoma
newsletter about ovarian carcinoma
1725 surveys returned
1725 surveys returned
Median age 52 years
Median age 52 years
70% had stage III or IV disease
70% had stage III or IV disease
Goff, B, et al. Cancer 2000;89:2068
Goff, B, et al. Cancer 2000;89:2068
-
-
75.
75.
Ovarian Cancer
Ovarian Cancer
Symptoms
Symptoms
95% of patients reported having symptoms
95% of patients reported having symptoms
prior to diagnosis
prior to diagnosis
–
–
Abdominal 77%
Abdominal 77%
–
–
Gastrointestinal 70%
Gastrointestinal 70%
–
–
Pain 58%
Pain 58%
–
–
Constitutional 50%
Constitutional 50%
–
–
Urinary 34%
Urinary 34%
–
–
Pelvic 26%
Pelvic 26%
Ovarian Cancer
Ovarian Cancer
Symptoms
Symptoms
Asymptomatic prior to diagnosis
Asymptomatic prior to diagnosis
–
–
Stage I/II
Stage I/II
–
–
11%
11%
–
–
Stage III/IV
Stage III/IV
–
–
3%
3%
Women who ignored their symptoms were
Women who ignored their symptoms were
more likely to be diagnosed with advanced
more likely to be diagnosed with advanced
stage disease
stage disease
Ovarian Cancer
Ovarian Cancer
Symptoms
Symptoms
Factors associated with delay in diagnosis
Factors associated with delay in diagnosis
–
–
Omission of pelvic exam at first visit
Omission of pelvic exam at first visit
–
–
Multiple symptoms
Multiple symptoms
–
–
Missed diagnosis: no problem, depression, stress, IBS, or
Missed diagnosis: no problem, depression, stress, IBS, or
gastritis
gastritis
–
–
No imaging or CA
No imaging or CA
-
-
125
125
–
–
Younger age
Younger age
Type of health care provider seen initially, insurance,
Type of health care provider seen initially, insurance,
and specific symptoms did not correlate with a delay
and specific symptoms did not correlate with a delay
in diagnosis
in diagnosis

Cancer History
Cancer History
Ovarian cancer
Ovarian cancer
Breast cancer
Breast cancer
Endometrial cancer
Endometrial cancer
Other
Other
BRCA 1,2
BRCA 1,2
HNPCC
HNPCC
Conclusions
Conclusions
Identify patients at risk
Identify patients at risk
–
–
Cancer history, symptoms, other
Cancer history, symptoms, other
Ovarian examination is often inaccurate
Ovarian examination is often inaccurate
–
–
Age, obesity, large uterus
Age, obesity, large uterus
Stratify risk with ultrasound, other imaging
Stratify risk with ultrasound, other imaging
Informed surgical consent
Informed surgical consent
Consider laparoscopic approach if feasible
Consider laparoscopic approach if feasible

Conclusions
Conclusions
Referral for an adnexal tumor depends on
Referral for an adnexal tumor depends on
risk of malignancy assessment
risk of malignancy assessment
When a Gyn Onc performs surgery for
When a Gyn Onc performs surgery for
early stage ovarian cancer, patients are more
early stage ovarian cancer, patients are more
likely to be accurately staged and receive
likely to be accurately staged and receive
proper adjuvant treatment
proper adjuvant treatment

"Let us have faith that right makes might, and
"Let us have faith that right makes might, and
in that faith, let us, to the end, dare to do
in that faith, let us, to the end, dare to do
our duty as we understand it."
our duty as we understand it."
Lincoln's Cooper Institute Address
Lincoln's Cooper Institute Address
February 27, 1860.
February 27, 1860.