the art of managing drug-drug interactions in patients ... · ©2017 mfmer | slide-1 the art of...
TRANSCRIPT

©2017 MFMER | slide-1
The ART of Managing Drug-Drug Interactions in Patients with HIVBradley L. Smith, [email protected] Grand RoundsDecember 19, 2017

©2017 MFMER | slide-2
Presentation Objectives• Describe the HIV life cycle and how
antiretroviral medications work to suppress viral replication
• Identify drug-drug interactions with common antiretroviral medications
• Recognize appropriate management strategies for drug-drug interactions in HIV patients

©2017 MFMER | slide-3
Presentation Abbreviations• ART – Antiretroviral Therapy
• AUC – Area under the curve
• CD4 – Cluster of differentiation 4
• CCR5 – C-C chemokine receptor 5
• CXCR4 – C-X-C chemokine receptor 4
• DHHS – Department of Health and Human Services
• DVT – Deep vein thrombosis
• H2RAs – Histamine-2 Receptor Antagonist
• INSTIs – Integrase Inhibitors
• mRNA – messenger RNA
• NNRTIs – Non-Nucleoside Reverse Transcriptase Inhibitors
• NRTIs – Nucleoside Reverse Transcriptase Inhibitors
• PIs – Protease Inhibitors
• P-gp – P-glycoprotein
• PPIs – Proton Pump Inhibitors
• vDNA – viral DNA
• vRNA – viral RNA
• RT – reverse transcriptase

©2017 MFMER | slide-4
HIV Life Cycle – Fusion and Entry
IntracellularExtracellular
CCR5 or CXCR4Viral Nucleocapsid
CD4

©2017 MFMER | slide-5
Current Antiretroviral MedicationsFusion Inhibitor (1)Enfuvirtide (T-20)
CCR-5 Inhibitors (1)Maraviroc (MVC)
IntracellularExtracellular
CCR5 or CXCR4CD4

©2017 MFMER | slide-6
HIV Life Cycle – Transcription and Integration
vRNA
HIV RT
vDNA
Host DNA
Integrase
Nucleus

©2017 MFMER | slide-7
HIV Life Cycle – Transcription and Integration
vRNA
HIV RT
vDNANRTIs (7)Abacavir (ABC)Didanosine (ddI)Emtricitabine (FTC)Lamivudine (3TC)Stavudine (d4T)Tenofovir (TDF)Zidovudine (AZT, ZDV)
NNRTIs (5)Efavirenz (EFV)Etravirine (ETV)Nevirapine (NVP) Rilpivirine (RPV)Delavirdine (DLV)

©2017 MFMER | slide-8
HIV Life Cycle – Transcription and Integration
Host DNA
Integrase
Nucleus
INSTIs (3)Dolutegravir (DTG)Elvitegravir (EVG)Raltegravir (RAL)
vDNA

©2017 MFMER | slide-9
HIV Life Cycle – Transcription and Integration
Nucleus
Host DNA
Integrase
Integrated HIV DNA
Transcriptionto viral mRNA
Transcription to vRNA
Polyprotein Protease
Protease
Protease
Protease
Protease

©2017 MFMER | slide-10
HIV Life Cycle – Cell Exit

©2017 MFMER | slide-11
HIV Life Cycle – Transcription and Integration
Polyprotein ProteaseProtease
PIs (9)Atazanavir (ATV)Darunavir (DRV)Fosamprenavir (FPV)Lopinavir/r (LPV/r)Ritonavir (RTV)Tipranavir (TPV) Indinavir (IDV)Nelfinavir (NFV)Saquinavir (SQV)

©2017 MFMER | slide-12
Current Antiretroviral Medications
NRTIs (7)Abacavir (ABC)Didanosine (ddI)Emtricitabine (FTC)Lamivudine (3TC)Stavudine (d4T)Tenofovir (TDF)Zidovudine (AZT, ZDV)
NNRTIs (5)Efavirenz (EFV)Etravirine (ETV)Nevirapine (NVP) Rilpivirine (RPV)Delavirdine (DLV)
Fusion Inhibitor (1)Enfuvirtide (T-20)
INSTIs (3)Dolutegravir (DTG)Elvitegravir (EVG)Raltegravir (RAL)
CCR-5 Inhibitors (1)Maraviroc (MVC)
PIs (9)Atazanavir (ATV)Darunavir (DRV)Fosamprenavir (FPV)Lopinavir/r (LPV/r)Ritonavir (RTV)Tipranavir (TPV) Indinavir (IDV)Nelfinavir (NFV)Saquinavir (SQV)

©2017 MFMER | slide-13
Common Antiretroviral RegimensNRTIsAbacavir (ABC)Emtricitabine (FTC)Lamivudine (3TC)Tenofovir (TDF)Zidovudine (AZT, ZDV)
NNRTIsEfavirenz (EFV)Etravirine (ETV)Rilpivirine (RPV)
PIsAtazanavir (ATV)Darunavir (DRV)
EnhancersCobicistat (COBI)
INSTIsDolutegravir (DTG)Elvitegravir (EVG)Raltegravir (RAL)
Ritonavir (RTV)
Backbone One Additional Agent

©2017 MFMER | slide-14
Pharmacokinetic Boosting Agents
Cobicistat (COBI)
• No activity against HIV• Less drug interactions
• P-gp inhibitor• 3A4 substrate• 3A4, 2D6 – inhibitor
Ritonavir (RTV)
• HIV activity (PI)• More drug interactions
• P-gp substrate and inhibitor
• 3A4, 2D6 – substrate• 3A4, 2D6 – inhibitor• 1A2, 2C8, 2C9, 2C19,
UGT 1a1 – inducer

©2017 MFMER | slide-15
Single-Tablet Regimens
Positively Aware 2017 HIV Drug Chart. www.positivelyaware.com

©2017 MFMER | slide-16
How many medication targets are there in the HIV life cycle?
A) Three
B) Four
C) Five
D) Six
©2017 MFMER | slide-17
Assessment of ART-related Drug Interactions

©2017 MFMER | slide-18
Assessment of Drug Interactions• Tertiary drug sources interaction checkers• University of Liverpool site
• www.hiv-druginteractions.org• Only checks interactions with ART
• 2017 DHHS HIV Guidelines• Table 17 - Mechanisms of Antiretroviral-Associated
Drug Interactions • Table 18 – ART Drug Interactions by class

©2017 MFMER | slide-19
DHHS HIV Guidelines: Mechanisms of Antiretroviral-Associated Drug Interactions
DTG – DolutegravirEVG – ElvitegravirRAL – Raltegravir
COBI – CobicistatRTV – RitonavirATV – Atazanavir
HIV/AIDS Treatment Guidelines. https://aidsinfo.nih.gov/guidelines

©2017 MFMER | slide-20
DHHS HIV Guidelines: ART Drug Interactions by Class
TPV/r – Tipranavir/ritonavirATV/c – Atazanavir/cobicistatDRV/c – Darunavir/cobicistat RTV – Ritonavir
HIV/AIDS Treatment Guidelines. https://aidsinfo.nih.gov/guidelines

©2017 MFMER | slide-21
Management of ART-related drug interactions

©2017 MFMER | slide-22
Patient Case #1• 56 year old female• Admitted for community acquired pneumonia• Past Medical History:
• HIV• Osteopenia
• Current medications include:• Complera® (RPV/TDF/FTC) once daily at bedtime• Calcium 600mg/Vitamin D3 800IU two tablets daily
• Medicine Service orders:• Continue home medications• Pantoprazole 40mg once daily• Levofloxacin 500mg once daily
RPV – RilpivirineTDF – TenofovirFTC – Emtricitiabine

©2017 MFMER | slide-23
Stomach Acid and Antiretrovirals
• Antacids: ATV 2 hours before or 1 to 2 hours after
• H2RAs: ATV at least 10 hours after• Famotidine < 20mg BID
• PPIs: PPI at least 12 hours before• Omeprazole ≤ 20mg
Boosted-Atazanavir(ATV/c or ATV/r)
Boosted-Atazanavir(ATV/c or ATV/r)
• Antacids: Give 2 hours before or 4 hours after RPV
• H2RAs: Give 12 hours before or 4 hours after RPV
• PPIs: Contraindicated
Rilpivirine(RPV)
Rilpivirine(RPV)

©2017 MFMER | slide-24
Polyvalent Cations and Antiretrovirals
Dolutegravir(DTV)
Elvitegravir(EVG)
Raltegravir(RAL)
CalciumAluminum
MagnesiumIronZinc
Chelation
©2017 MFMER | slide-25
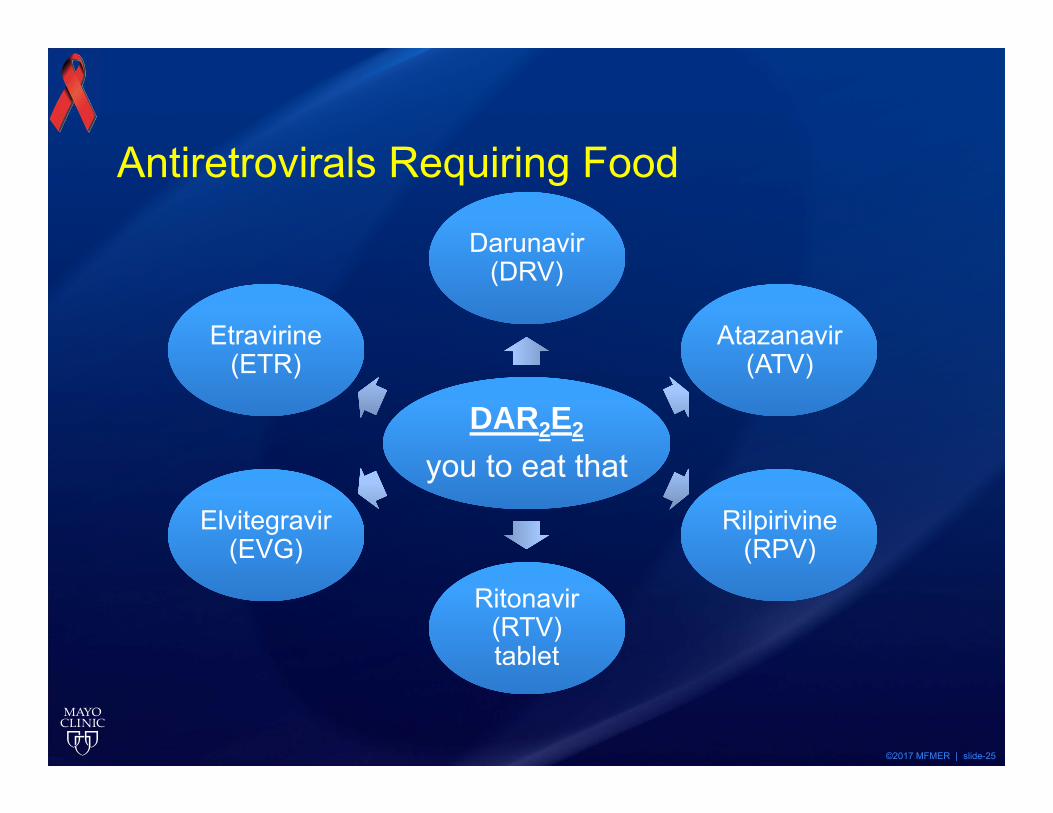
Antiretrovirals Requiring Food
DAR2E2
you to eat thatDAR2E2
you to eat that
Darunavir(DRV)
Darunavir(DRV)
Atazanavir(ATV)
Atazanavir(ATV)
Rilpirivine(RPV)
Rilpirivine(RPV)
Ritonavir (RTV) tablet
Ritonavir (RTV) tablet
Elvitegravir(EVG)
Elvitegravir(EVG)
Etravirine (ETR)
Etravirine (ETR)

©2017 MFMER | slide-26
Antiretrovirals Requiring Food
• Patient Friendly Answer• 400 calories• 10 grams fat
Antiretroviral Food RequirementRilpivirine
(RPV)400k kcal13 g fat
Atazanavir(ATV)
350 - 721 kcal8.2 - 37.3 g fat
Darunavir(DRV)
240 - 925 kcal12 - 56 g fat
Elvitegravir/cobicistat(EVG/c)
373 - 800 kcal20 - 50% fat
Rilpivirine [package insert]. Gilead Sciences, Inc. March 2, 2016Atazanavir [package insert]. E.R. Squibb & Sons, L.L.C. September 24, 2015
Darunavir [package insert]. Janssen Products LP. June 8, 2015Stribild [package insert]. Gilead Sciences, Inc. February 29, 2016
©2017 MFMER | slide-27
Patient Case #1• 56 year old female• Admitted for community acquired pneumonia• Past Medical History:
• HIV• Osteopenia
• Current medications include:• Complera® (RPV/TDF/FTC) once daily at bedtime• Calcium 600mg/Vitamin D3 800IU two tablets daily
• Medicine Service orders:• Continue home medications• Pantoprazole 40mg once daily• Levofloxacin 500mg once daily
RPV – RilpivirineTDF – TenofovirFTC – Emtricitiabine

©2017 MFMER | slide-28
Which is an appropriate recommendation for the management of this patient?A) Complera® (RPV/TDF/FTC) may be given at bedtime
during hospital admission
B) Pantoprazole may be used for stress ulcer prophylaxis
C) Ensure spacing of antiretroviral by at least 4 hours before calcium or 2 hours after
D) A and C
E) All of the above
RPV – RilpivirineTDF – TenofovirFTC – Emtricitiabine

©2017 MFMER | slide-29
Patient Case #2
• 61 year old male patient• Admitted due to right lower extremity DVT• Patient on therapeutic enoxaparin• Orders for transition to oral anticoagulation• Social history:
• Smokes 1 pack per day• Current medication list includes
• Lisinopril 10mg once daily• Tivicay® (DTG) 50mg once daily• Prezcobix® (DRV/r) 800mg/150mg once daily• Truvada® (TDF/FTC) 300mg/200mg once daily
DTG = DolutegravirDRV/r = Darunavir/ritonavirTDF = TenofovirFTC = Emtricitabine

©2017 MFMER | slide-30
Anticoagulation and AntiretroviralsART Apixaban Dabigatran Rivaroxaban WarfarinPIs(Boosted)
Notrecommended
↓ apixaban 50%
Not recommended
Consider alternative
Not recommended
Consider alternative
PI/r: ↓ warfarin possible
Monitor INR closely
COBI Notrecommended
↓ apixaban 50%
No recommended
Not recommended
↑ or ↓ warfarin possible
Monitor INR closely
NNRTIs EFV, ETR, NVP: Consider alternative
EFV, NVP, RPV: No adjustment
ETR: Consider alternative
EFV, ETR, NVP: Consider alternative
RPV: Good
↑ or ↓ warfarin possible
Monitor INR closely
EFV = EfavirenzETR = EtravirineNVP = Nevirapine RPV = Rilpivirine

©2017 MFMER | slide-31
Smoking Cessation and AntiretroviralsART Nicotine
ReplacementVarenicline Bupropion
PIs(Boosted)
Recommended Recommended ↑ Bupropion dose
COBI Recommended Recommended ↑or↓ bupropion possible
NNRTIs Recommended Recommended ↑ Bupropion dose

©2017 MFMER | slide-32
Patient Case #2
• 61 year old male patient• Admitted due to right lower extremity DVT• Patient on therapeutic enoxaparin• Orders for transition to oral anticoagulation• Social history:
• Smokes 1 pack per day• Current medication list includes
• Lisinopril 10mg once daily• Tivicay® (DTG) 50mg once daily• Prezcobix® (DRV/r) 800mg/150mg once daily• Truvada® (TDF/FTC) 300mg/200mg once daily
DTG = DolutegravirDRV/r = Darunavir/ritonavirTDF = TenofovirFTC = Emtricitabine

©2017 MFMER | slide-33
What is your recommendation for an oral anticoagulant?A) Apixaban 10 mg twice daily for 7 days then 5 mg
twice daily
B) Dabigatran 150 mg twice daily
C) Rivaroxaban 15 mg twice daily for 21 days then 20 mg once daily
D) Warfarin 5 mg once daily adjusted per INR results
E) Warfarin 3 mg once daily adjusted per INR results
©2017 MFMER | slide-34
Patient Case #3
• 23 yo male patient newly diagnosed with HIV• Patient is ready to begin antiretroviral therapy• Past medical history:
• Asthma• Seizures
• Social History• Denies smoking, alcohol or illicit drug use
• Current medication list includes• Fluticasone 110mcg 2 puffs twice daily• Phenobarbital 100mg twice daily

©2017 MFMER | slide-35
Corticosteroids and Antiretrovirals
Glucocorticoid metabolism via CYP3A4
RTV, COBI, PIs inhibit CYP3A4
Glucocorticoid accumulation
RTV – RitonavirCOBI – Cobicistat

©2017 MFMER | slide-36
Corticosteroids and Antiretrovirals
Sadarangani S, et al. Interdiscip Perspect Infect Dis. 2014;2014:849432Azevedo L, et al. BMJ Case Rep 2015
Johnson SR et al. J Pediatr 2006;148:386-388Rainsbury PG et al. Pediatr Infect Dis J 2017;36:502-503
Case Age/Sex Antiretrovirals Corticosteroid1 39/male TDF
FTCDRV/r
Inhaled salmeterol/fluticasoneIntranasal fluticasone
2 12/female 3TCAZTLPV/r
Inhaled salmeterol/fluticasone
3 15/male 3TCAZTDRV/r
Ophthalmic dexamethasone
4 48/female TDFFTCATV/r
Injected triamcinolone epidural
3TC = LamivudineDRV/r = Darunavir/ritonavirTDF = TenofovirFTC = Emtricitabine
ATV/r = Atazanavir/ritonavirLPV/r = Lopinavir/ritonavirAZT = Zidovudine

©2017 MFMER | slide-37
Corticosteroids and Antiretrovirals
Alternative corticosteroid options
• Beclomethasone• Flunisolide
Alternative ART options
• NNRTIs• INSTIs (RAL or DTG)
If benefits outweigh risks, consider dose adjustment and monitor closely
RAL = RaltegravirDTG = Dolutegravir

©2017 MFMER | slide-38
Anticonvulsants and AntiretroviralsAnticonvulsant Antiretroviral ActionCarbamazepine PIs, RPV, EVG/c Contraindicated
ETR, RAL AvoidDTG Increase DTG to 50mg twice daily
Phenytoin, Phenobarbital
PIs, RPV, EVG/c ContraindicatedETR, RAL, DTG Avoid
Lamotrigine, Valproic Acid
PIs CautionNNRTIs Okay
Levetirectam safe to use with all antiretrovirals
DTG = DolutegravirRPV = RilpivirineEVG/c = Elvitegravir/cobicistatETR = EtravirineRAL = Raltegravir
©2017 MFMER | slide-39
Patient Case #3
• 23 yo male patient newly diagnosed with HIV• Patient is ready to begin antiretroviral therapy• Past medical history:
• Asthma• Seizures
• Social History• Denies smoking, alcohol or illicit drug use
• Current medication list includes• Fluticasone 110mcg 2 puffs twice daily• Phenobarbital 100mg twice daily
©2017 MFMER | slide-40
What would be an appropriate recommendation for therapy?
A) Genvoya® (EVG/COBI/FTC/TDF) once daily
B) Atripla® (EFV/FTC/TDF) once daily
C) Prezcobix® (DRV/r) once daily plus Descovy® (TAF/FTC) once daily
D) Triumeq® (DTG/ABC/3TC) once daily plus Tivicay® (DTG) 50mg once daily

©2017 MFMER | slide-41
Antiretroviral Drug Interactions Summary• Resources for interactions
• DHHS Table 18
• Cobicistat and Ritonavir
• Acid Suppression• Atazanavir; Rilpivirine
• Food requirement• DAR2E2 you to eat that
• Warfarin – safest anticoagulant
• Corticosteroids• Use beclomethasone
• Levetiracetam – no drug interactions