the brooke surgery the brooke surgery patient pack... · the brooke surgery. the brooke surgery ....
TRANSCRIPT

The Brooke Surgery THE BROOKE SURGERY 20 Market St Hyde SK14 1AT
Tel: 0161 368 3312 Fax: 0161 368 5670 www.brookesurgery.co.uk Twitter:@brookesurgery
Dr. J M Dirckze M.B.Ch.B. (Leeds 1982) M.R.C.G.P. Male
Dr. R Patel M.B.Ch.B. (Manchester 1985) M.R.C.G.P. Male
Dr. A Faruq M.B.Ch.B (Wales 1995) M.R.C.G.P. Male Dr. R Fletcher M.B.Ch.B (Manchester 2005) M.R.C.G.P. Male
DR. L. M. PRESTON M.B.CH.B (MANCHESTER 1995) FEMALE DR. W.K.TSANG M.B.CH.B (SHEFFIELD 1995) FEMALE
DR. F. Amin M.B.CH.B (MANCHESTER 2015) FEMALE
Dr. R. Anis M.B.Ch.B (Manchester 2016) Female
Please note to register at this practice you will need 2 forms of identification, one from each list below:
List A
Passport
Picture Driving Licence
Official Picture ID
List B
Utility Bill, less than 3 months old (not mobile phone)
Lease/Rental Agreement
Rent Book
Inland Revenue correspondence
Welcome to The Brooke Surgery
Your appointment with a member of our nursing team is on …………………………………………….
Please note that you will not be registered with this practice until you have attended for this appointment.
If for any reason you are unable to attend, please telephone the surgery to cancel 0161 368 3312 and rearrange your appointment.
If you do not attend your new patient appointment we will assume that you have decided not to register with us and your application will be destroyed.
We will consider other forms of correspondence that proves your address/identification. The final decision rests with
the Practice Manager.

Surgery opening times The surgery is open all day Monday to Friday from 8:00am to 6:00pm we work through lunchtime everyday Thursdays 8:00am to 9.00pm Appointments can be made online, telephoning, or by calling in at the surgery. We have an Out of Hours service for Prebookable appointments held at Thornley Medical Centre in Hyde operating from 6:30pm – 8pm Mon – Fri and 9am – 12noon Sat to Sun.
Appointments Consultations are available at least two weeks in advance. You will normally be able to see a doctor, nurse or health care assistant within 48 hours. We will always see medically urgent patients the same day.
Facilities for the disabled There is access to the surgery for the disabled and a specially adapted toilet for their use.
Training & Teaching We are an approved training practice, and have experienced doctors as well as medical & nursing students attending the practice, who may be present at your consultation. Should you prefer this not to be the case, simply inform reception. We close at 12 noon on one afternoon monthly for staff training, and the specific day will beadvised by notices in the practice, Facebook -The Brooke Surgery,Hyde and Twitter @brookesurgery and our website www.brookesurgery.co.uk
Home visits Please telephone the surgery before 10:30am for a visit if your illness prevents you from attending the surgery. To assist the doctor we ask that you give the receptionist as much information as possible.
Out of hours Tameside & Glossop CCG are responsible for arranging medical cover out of normal hours. In an emergency always telephone the surgery number. If you feel that you can wait until the next day then contact the surgery on any weekday and if urgent, you will be seen that day.
Reception Team
Jeanette, Susan, Karen, Mechelle,
Lorna, Marie and Jodie
Practice Management
Practice Manager – Kathryn LeyDeputy Manager – Lisa Moran
Reception - Jeanette Mather
Administration – Chris Turner
Nursing – Penny Gowland
Nurses
Nurse Practitioner: Penny Gowland
Nurse: Louise WestmerlandNurse: Pranamee Das
Health Care Assistant: Sue Cavanagh Health Care Assistant: Jade McLarenHealth Care Assistant: Zoe Cockburn
Administration Team
Chris, Kerry, Siobhan, Rebecca and Shannon
Reception & Admin staff Our team of receptionists have attended specific courses to help you make the best use of the facilities at the practice. All staff involved in reception, clerical and admin duties are here to help you. They may need to ask you further details when you telephone; this is to ensure that we can assist you as speedily as possible. They are bound by the same rules of confidentiality as the doctors and nurses.

We also have district nurses, health visitors and midwives visiting the practice to see patients.
Prescriptions Repeat prescriptions are available for any patient who is on long-term medication authorised by the doctor, and all repeat prescriptions will be available within 24 hours of correct ordering. Prescription handed in before 10am will be ready for collection after 2pm on the same day. Prescriptions after 10am will be ready for collection after 2pm the following working day. Repeat medication requests should be made using the tear off slip provided with your prescription or on line. Please only request repeat medications within a week of their due date. We will however try to accommodate one off requests.
Request your repeat prescriptions online
Request your repeat prescriptions quickly online by logging into your account and simply
ticking the appropriate boxes. You can review the progress of your repeat prescriptions and
any message that the practice may have sent to you.
Please note that medication requests cannot be made by telephone, though you can register with a chemist of your choice to arrange ordering and delivery. You will need to make an appointment to see the doctor for any medication other than that on your authorised repeat slip. Please make an appointment to see the practice pharmacist for a medication review when requested to do so.
Accessing your Medical Records
You are able to access your medical records online. For further information please speak to the reception team or complete the application form found in our waiting area or on our website at www.brookesurgery.co.uk and bring in together with your photo ID
New patients All new patients will be asked to complete a lifestyle questionnaire and book an appointment with the Practice Nurse or HCA for a health check in order to register. The health check gives us the opportunity to meet you and your Family and inform you about the practice.
If you move Please let us know your new address. If you move outside the practice area, we will advise you how to register with a new doctor.
Private medical examinations Examinations for fitness to drive, pre-employment, vehicle license and insurance medicals etc. Are carried out by special appointment with your doctor, and a separate fee is payable.
Patients’ rights, responsibilities & personal health information Patients have a right of confidentiality and we ensure that the information we hold is secure and only available to appropriate health professionals involved in your care. Patients & staff have a right to courteous treatment and we ask everybody to respect this when in the surgery. The practice operates a zero tolerance policy towards verbal or physical aggression. We have a duty of care to look after our staff and our patients.
Suggestions, complaints or concerns relating to the practice, its staff or the services offered, should be advised to the Kathryn Ley, Practice Manager who will provide you with a timely response to them.
Action: IF YOU HAVE A NOMINATED PHARMACY FOR ELECTRONIC PRESCRIPTIONS, YOU MUST INFORM THAT PHARMACY IF YOU DECIDE TO MOVE AS YOUR PRESCRIPTIONS WILL
AUTOMATICALLY GO THERE!
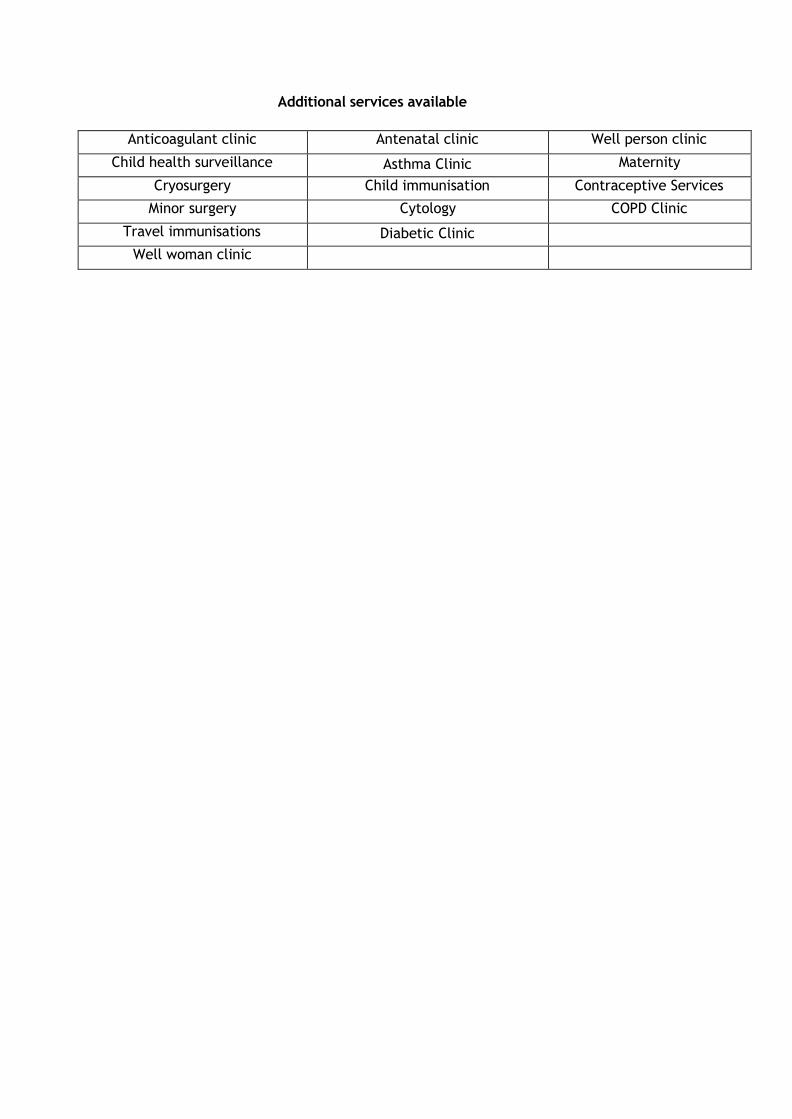
Additional services available
Anticoagulant clinic Antenatal clinic Well person clinic
Child health surveillance Asthma Clinic Maternity
Cryosurgery Child immunisation Contraceptive Services
Minor surgery Cytology COPD Clinic
Travel immunisations Diabetic Clinic
Well woman clinic

The Brooke Surgery New Patient Registration Form
Full Name: Telephone Number:
Mr / Mrs / Miss / Ms / Other…….. Work Number
Address and Postcode Mobile Number:
E-mail Address. By adding an email address
you are agreeing to be contacted by email :
Next of Kin: Relationship to you:
Next of Kin Contact Number:
Date of Birth: Previous / Mother’s surname if different:
Town & Country of Birth
Marital Status:
Gender: Male: Female:
Occupation:
Names & ages of children
If returning from Armed Forces:
Your Service or Personnel Number Your Enlistment Date
Your height:
Feet / inches cm Your weight:
Stones / lbs. kg
Your Religion:
C of E Catholic Other Christian (state) Buddhist Hindu Muslim
Sikh Jewish Jehovah’s Witness No religion Other religion (state)
Your Ethnic Origin: (select one)
White (UK) 9i0
White (Irish) 9i1%
White (Other) 9i2%
Please complete this confidential questionnaire (one for each member of the family to be registered with the Practice).
Please complete in BLOCK CAPITALS and tick the boxes as appropriate.
If you are newly arrived in this country, please bring your passport to confirm your date of birth and entitlement to NHS treatment.
Please complete a separate form for each family member to be registered.
Today’s Date:
Are you a carer:

Caribbean 9i3
African 9i4
Asian 9i5 Other Mixed Background 9i6%
Indian / Brit Indian 9i7
Pakistani Brit Pakist
/ ani 9i8
Banglades Banglades
hi / Brit hi 9i9
Other Asian Background 9iA%
Other Black Background
Chinese 9iE
Other 9iF%
Ethnic Category not stated 9iG
Your main or 1st
language English
Spoken / Understood: (select one)
Hindi Gujurat i Urdu Bengali /Sytheti
Punjabi
Polish Ukrainian French German Spanish Other: (Please Specify)
Your Medical Background:
What illnesses hav you had & When?
e
What operations ha you had and When
ve ?
Do you have any medical problems at
present?
Please list any tablets, medicines or other treatments you are
currently taking: (incl. dose + frequency)
Do you require an alternative correspondence format? Braille
Large Print
Audio Tape
Are there any serious diseases that affect your Parents, Brothers or Sisters (tick all that apply)
Diabetes Heart Attack Heart attack under age of 60 Bowel Cancer
Breast Cancer High Blood Pressure Asthma Stroke
Thyroid Disorder Any other important Family Illness?
Children ONLY
What immunisations have you had? (please tick all
that apply)
Diphtheria Measles German Measles Tetanus Polio MMR
Whooping Cough Pre-school booster Triple vaccine (Diphtheria, Tetanus & Pertussis) – 3 doses
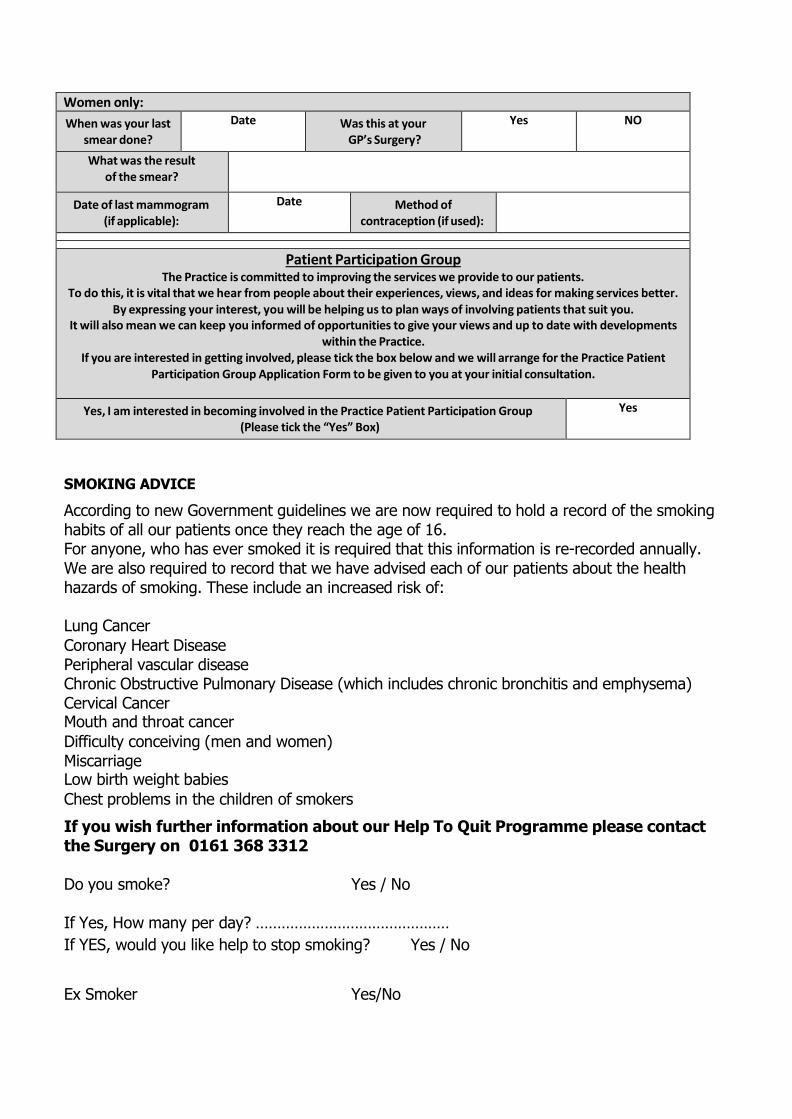
Women only:
When was your last smear done?
Date Was this at your GP’s Surgery?
Yes NO
What was the result of the smear?
Date of last mammogram (if applicable):
Date Method of contraception (if used):
Patient Participation Group The Practice is committed to improving the services we provide to our patients.
To do this, it is vital that we hear from people about their experiences, views, and ideas for making services better. By expressing your interest, you will be helping us to plan ways of involving patients that suit you.
It will also mean we can keep you informed of opportunities to give your views and up to date with developments within the Practice.
If you are interested in getting involved, please tick the box below and we will arrange for the Practice Patient Participation Group Application Form to be given to you at your initial consultation.
Yes, I am interested in becoming involved in the Practice Patient Participation Group (Please tick the “Yes” Box)
Yes
SMOKING ADVICE
According to new Government guidelines we are now required to hold a record of the smoking habits of all our patients once they reach the age of 16. For anyone, who has ever smoked it is required that this information is re-recorded annually. We are also required to record that we have advised each of our patients about the health hazards of smoking. These include an increased risk of:
Lung Cancer
Coronary Heart Disease Peripheral vascular disease Chronic Obstructive Pulmonary Disease (which includes chronic bronchitis and emphysema) Cervical Cancer Mouth and throat cancer
Difficulty conceiving (men and women) Miscarriage Low birth weight babies
Chest problems in the children of smokers
If you wish further information about our Help To Quit Programme please contact the Surgery on 0161 368 3312
Do you smoke? Yes / No
If Yes, How many per day? ………………………………………
If YES, would you like help to stop smoking? Yes / No
Ex Smoker Yes/No

Patient Signature:
Signature on behalf of Patient:
Thank you for completing this form
For more information about the services we offer, please refer to your new patient pack
Your physical examination will include having your height, weight and blood pressure taken, and a specimen of urine for testing (it would be helpful if you would bring a specimen with you when coming to the Practice). The Consultation will also establish relevant past medical and family history, including: Medical factors - illnesses, immunisations, allergies, hereditary factors, screening tests, current health Social factors - employment, housing, family circumstances
Lifestyle factors - diet and exercise, smoking, alcohol and drug abuse.

Page 1 of 2
This is one unit of alcohol…
…and each of these is more than one unit
Section 1 (FAST) 0 1 2 3 4 Your score
How often have you had 6 or more units if female, or 8 or more if male, on a single occasion in the last year? Never Less than
monthly Monthly Weekly Daily or almost daily
Section 1 Fast Score
If score is 0, finish here. If score is 1 or more please complete Section 2
Section 2 (FAST) 0 1 2 3 4 Your score
How often during the last year have you failed to do what was normally expected from you because of your drinking?
Never Less than monthly Monthly Weekly
Daily or almost daily
How often during the last year have you been unable to remember what happened the night before because you had been drinking?
Never Less than monthly Monthly Weekly
Daily or almost daily
Has a relative or friend, doctor or other health worker been concerned about your drinking or suggested that you cut down?
No Yes, but
not in the last year
Yes, during
the last year
Section 1 FAST Score
Section 2 FAST Score
Total FAST Score
If Total FAST Score is Less than 4 finish here. If Total FAST Score is 4 or More please complete Section 3 on Page 2
Page 2 of 2
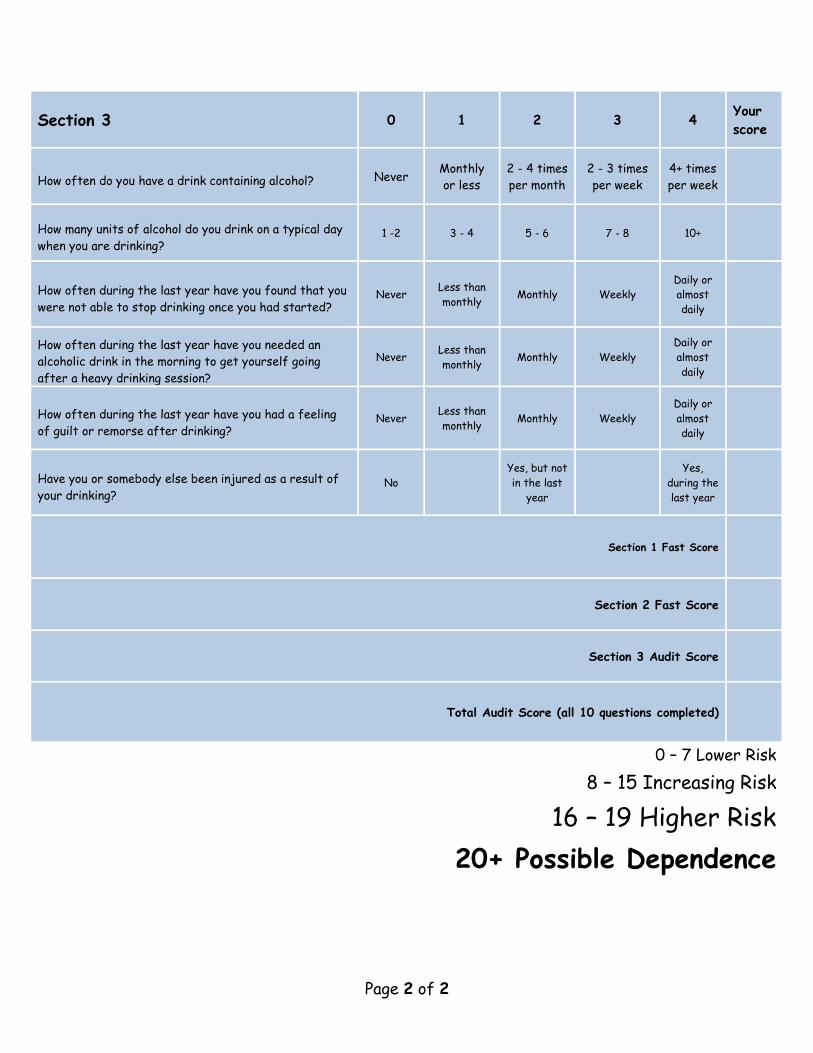
Section 3 0 1 2 3 4 Your score
How often do you have a drink containing alcohol? Never Monthly or less
2 - 4 times per month
2 - 3 times per week
4+ times per week
How many units of alcohol do you drink on a typical day when you are drinking?
1 -2 3 - 4 5 - 6 7 - 8 10+
How often during the last year have you found that you were not able to stop drinking once you had started?
Never Less than monthly Monthly Weekly
Daily or almost daily
How often during the last year have you needed an alcoholic drink in the morning to get yourself going after a heavy drinking session?
Never Less than monthly Monthly Weekly
Daily or almost daily
How often during the last year have you had a feeling of guilt or remorse after drinking?
Never Less than monthly Monthly Weekly
Daily or almost daily
Have you or somebody else been injured as a result of your drinking?
No Yes, but not in the last
year
Yes, during the last year
Section 1 Fast Score
Section 2 Fast Score
Section 3 Audit Score
Total Audit Score (all 10 questions completed)
0 – 7 Lower Risk
8 – 15 Increasing Risk
16 – 19 Higher Risk 20+ Possible Dependence

Family doctor services registration GMS1
Patient’s details Please complete in BLOCK CAPITALS and tick as appropriate
Surname
Date of birth First names
NHS Previous surname/sNo.
Male Female Town and countryof birth
Home address
Postcode Telephone number
Please help us trace your previous medical records by providing the following informationYour previous address in UK Name of previous doctor while at that address
Address of previous doctor
If you are from abroadYour first UK address where registered with a GP
If previously resident in UK, Date you first camedate of leaving to live in UK
If you are returning from the Armed ForcesAddress before enlisting
Service or EnlistmentPersonnel number date
If you are registering a child under 5
I wish the child above to be registered with the doctor named overleaf for Child Health Surveillance
If you need your doctor to dispense medicines and appliances*
I live more than 1 mile in a straight line from the nearest chemist
I would have serious difficulty in getting them from a chemist
Signature of Patient Signature on behalf of patient Date________/_________/_________
Mr Mrs Miss Ms
042017_003 Product Code: GMS1
* Not all doctors are authorised to dispense medicines
NHS Organ Donor registrationI want to register my details on the NHS Organ Donor Register as someone whose organs/tissue may be used for transplantation after my death. Please tick the boxes that apply.
Any of my organs and tissue or
Kidneys Heart Liver Corneas Lungs Pancreas Any part of my body
Signature confirming my agreement to organ/tissue donation Date ________/________/________
For more information, please ask at reception for an information leaflet or visit the websitewww.uktransplant.org.uk, or call 0300 123 23 23.
NHS Blood Donor registrationI would like to join the NHS Blood Donor Register as someone who may be contacted and would be prepared to donate blood.Tick here if you have given blood in the last 3 years Signature confirming consent to inclusion on the NHS Blood Donor Register Date ________/________/________
For more information, please ask for the leaflet on joining the NHS Blood Donor RegisterMy preferred address for donation is: (only if different from above, e.g. your place of work)
Postcode:
HA use only Patient registered for GMS CHS Dispensing Rural Practice
GMS1_072017_004 Family Doctor Services Registration_tearoff.indd 1 20/07/2017 14:27

Family doctor services registration GMS1
To be completed by the doctorDoctors Name HA Code
I have accepted this patient for general medical services For the provision of contraceptive services
I have accepted this patient for general medical services on behalf of the doctor named below who is a member of this practice
Doctors Name, if different from above HA Code
I am on the HA CHS list and will provide Child Health Surveillance to this patient or I have accepted this patient on behalf of the doctor named below, who is a member of this practice and is on the HA CHS list and will provide Child Health Surveillance to this patient.
Doctors Name, if different from above HA Code
I will dispense medicines/appliances to this patient subject to Health Authority’s Approval
I am claiming rural practice payment for this patient. Distance in miles between my patient’s home address and my main surgery is
I declare to the best of my belief this information is correct and I claim the appropriate payment as set out in the Statement of Fees and Allowances. An audit trail is available at the practice for inspection by the HA’s authorised officers and auditors appointed by the Audit Commission.
Authorised Signature
Name Date _______/_______/_______
Practice Stamp
SUPPLEMENTARY QUESTIONS
PATIENT DECLARATION for all patients who are not ordinarily resident in the UKAnybody in England can register with a GP practice and receive free medical care from that practice.
However, if you are not ‘ordinarily resident’ in the UK you may have to pay for NHS treatment outside of the GP practice. Being ordinarily resident broadly means living lawfully in the UK on a properly settled basis for the time being. In most cases, nationals of countries outside the European Economic Area must also have the status of ‘indefinite leave to remain’ in the UK.
Some services, such as diagnostic tests of suspected infectious diseases and any treatment of those diseases are free of charge to all people, while some groups who are not ordinarily resident here are exempt from all treatment charges.
More information on ordinary residence, exemptions and paying for NHS services can be found in the Visitor and Migrant patient leaflet, available from your GP practice.
You may be asked to provide proof of entitlement in order to receive free NHS treatment outside of the GP practice, otherwise you may be charged for your treatment. Even if you have to pay for a service, you will always be provided with any immediately necessary or urgent treatment, regardless of advance payment.
The information you give on this form will be used to assist in identifying your chargeable status, and may be shared, including with NHS secondary care organisations (e.g. hospitals) and NHS Digital, for the purposes of validation, invoicing and cost recovery. You may be contacted on behalf of the NHS to confirm any details you have provided.
Please tick one of the following boxes:
a) I understand that I may need to pay for NHS treatment outside of the GP practice
b) I understand I have a valid exemption from paying for NHS treatment outside of the GP practice. This includes for example, an EHIC, or payment of the Immigration Health Charge (“the Surcharge”), when accompanied by a valid visa. I can provide documents to support this when requestedc) I do not know my chargeable status
I declare that the information I give on this form is correct and complete. I understand that if it is not correct, appropriate action may be taken against me.A parent/guardian should complete the form on behalf of a child under 16.
Signed: Date: DD MM YY
Print name:Relationship to patient:
On behalf of:
Complete this section if you live in another EEA country, or have moved to the UK to study or retire, or if you live in the UK but work in another EEA member state. Do not complete this section if you have an EHIC issued by the UK.NON-UK EUROPEAN HEALTH INSURANCE CARD (EHIC), PROVISIONAL REPLACEMENT CERTIFICATE (PRC) DETAILS and S1 FORMS
Do you have a non-UK EHIC or PRC? YES: NO: If yes, please enter details from your EHIC or PRC below:
If you are visiting from another EEA country and do not hold a current EHIC (or Provisional Replacement Certificate (PRC))/S1, you may be billed for the cost of any treatment received outside of the GP practice, includingat a hospital.
Country Code:
3: Name
4: Given Names
5: Date of Birth DD MM YYYY
6: Personal Identification Number
7: Identification number of the institution
8: Identification number of the card
9: Expiry Date DD MM YYYY
PRC validity period (a) From: DD MM YYYY (b) To: DD MM YYYY
Please tick if you have an S1 (e.g. you are retiring to the UK or you have been posted here by your employer for work or you live in the UK but work in another EEA member state). Please give your S1 form to the practice staff.
How will your EHIC/PRC/S1 data be used? By using your EHIC or PRC for NHS treatment costs your EHIC or PRC data and GP appointment data will be shared with NHS secondary care (hospitals) and NHS Digital solely for the purposes of cost recovery. Your clinical data will not be shared in the cost recovery process.
Your EHIC, PRC or S1 information will be shared with The Department for Work and Pensions for the purpose of recovering your NHS costs from your home country.
GMS1_072017_004 Family Doctor Services Registration_tearoff.indd 2 20/07/2017 14:27

Your emergency care summary
Summary Care Record – your emergency care summary
The NHS in England is introducing the Summary Care Record, which will be used in emergency care.
The record will contain information about any medicines you are taking, allergies you suffer from and any bad reactions to medicines you have had to ensure those caring for you have enough information to treat you safely.
Your Summary Care Record will be available to authorised healthcare staff providing your care anywhere in England, but they will ask your permission before they look at it. This means that if you have an accident or become ill, the doctors treating you will have immediate access to important information about your health.
Your GP practice is supporting Summary Care Records and as a patient you have a choice:
• Yes I would like a Summary Care Record – you do not need to do anything and aSummary Care Record will be created for you.
• No I do not want a Summary Care Record – enclosed is an opt out form. Pleasecomplete the form and hand it to a member of the GP practice staff.
If you need more time to make your choice you should let your GP Practice know.
For more information talk to GP practice staff, visit the website www.nhscarerecords.nhs.uk or telephone the dedicated NHS Summary Care Record Information Line on 0300 123 3020.
Additional copies of the opt out form can be collected from the GP practice, printed from the website www.nhscarerecords.nhs.uk or requested from the dedicated NHS Summary Care Record Information Line on 0300 123 3020.
You can choose not to have a Summary Care Record and you can change your mind at any time by informing your GP practice.
If you do nothing we will assume that you are happy with these changes and create a Summary Care Record for you. Children under 16 will automatically have a Summary Care Record created for them unless their parent or guardian chooses to opt them out. If you are the parent or guardian of a child under 16 and feel that they are old enough to understand, then you should make this information available to them.

Your emergency care summary
OPT-OUT FORM CONFIDENTIAL
Request for my clinical information to be withheld from the Summary Care Record
If you DO NOT want a Summary Care Record please fill out the form and send it to your GP
practice
A. Please complete in BLOCK CAPITALS
Title................................................................. Surname / Family name ...........................................................................................................
Forename(s)...................................................................................................................................................................................................................
Address ...........................................................................................................................................................................................................................
Postcode ...................................................... Phone No...................................................... Date of birth ................................................
NHS Number (if known) ............................................................................................................................................................................................
B. If you are filling out this form on behalf of another person or a child, their GP practice will consider this request. Please ensure you fill out their details in section A and your details in section B
Your name..................................................................................................................................... Your signature.............................................
Relationship to patient ............................................................................................................ Date ................................................................
What does it mean if I DO NOT have a Summary Care Record?
NHS healthcare staff caring for you may not be aware of your current medications, allergies you suffer from and any bad reactions to medicines you have had, in order to treat you safely in an emergency.
Your records will stay as they are now with information being shared by letter, email, fax or phone.
If you have any questions, or if you want to discuss your choices, please: • phone the Summary Care RecordInformation Line on0300 123 3020;• contact your local Patient AdviceLiaison Service (PALS); or• contact your GP practice.
FOR NHS USE ONLY
Actioned by practice: yes/no Date ...............................................................
Ref: 4705

IMPORTANT CHANGES TO
YOUR MEDICAL RECORDS
GP practices across England will soon be
required to supply patients’ personal and
confidential medical information, on a regular
and continuous basis, to the Health and Social
Care Information Centre (HSCIC).
The data upload is due to commence in March
2014 and all households should receive a
leaflet (‘Better information means better care’)
through their letterbox about this in January.
Details from your medical record will be
extracted from the practice in a form that can
identify you, and will include your NHS number,
date of birth, postcode, gender and ethnicity,
together with your medical diagnoses (including
cancer and mental health), their complications,
referrals to specialists, your prescriptions, your
family history, details of your vaccinations and
screening tests, your blood test results, your
body mass index, and your smoking/alcohol
habits.
This programme is called care.data, and the
information uploaded will be used for purposes
other than your direct medical care (so-called
“secondary uses”).
Medical staff treating you in GP surgeries,
hospitals, A&E and out-of-hours centres will not
use, or be able to use, this database. However,
the uploaded data is likely to be made available
to organisations outside of the NHS, such as
universities and commercial organisations.
Under the Health and Social Care Act 2012, GP
practices have no choice but to allow the HSCIC
to extract this information.
Once the data has been extracted, the GP
practice is no longer the data controller for that
information, and cannot control or protect in any
way how that information is used, shared or who
has access to it.
Although GP practices cannot object to this
information leaving the practice, individual
patients and their families can instruct their
practice to prohibit the transfer of their data, i.e.
you have the right to opt-out.
If you do nothing, i.e. you do not opt out, then
your medical information will be extracted and
uploaded to the HSCIC.
Once uploaded, you will not be able to get this
data deleted by the HSCIC. So if you want to
opt out, you need to act now.
To opt out, simply fill in your details on the form
to the right of this page, cut it out and post it or
drop it in to your GP practice, marked for the
attention of your GP. If you wish to opt out your
children or other members of your family for
whom you are responsible, you can add their
details on the back of the form.
This is not the Summary Care Record. The two
databases are very different. Opting out of one
database does not mean that you have
automatically opted out of the other.
Further information about the care.data
programme is available online - details overleaf.
Dear Doctor,
I am writing to give notice that I refuse consent for my identifiable information and the identifiable information of those for whom I am responsible [delete as appropriate] to be transferred from your practice systems for any purpose other than our medical care.
Please take whatever steps necessary to ensure my confidential personal information is not uploaded and record my dissent by whatever means possible.
This includes adding the ‘Dissent from secondary use of GP patient identifiable data’ code (Read v2: 9Nu0 or CVT3: XaZ89) to my record as well as the ‘Dissent from disclosure of personal confidential data by Health and Social Care Information Centre’ code (Read v2: 9Nu4 or CTV3: XaaVL).
I am aware of the implications of this request, understand that it will not affect the care we receive and will notify you should I change my mind.
Signature:
Full name:
Address:
Postcode:
Date of birth:
NHS number (if known):
Space for additional patient details overleaf
IPO
RTA
NT
CH
AN
GES T
O
YO
UR
MED
CA
L R
EC
OR
DS
Ple
ase
read —
you m
ay
need t
o a
ct
NO
W
Additional patient details
Please take whatever steps necessary to ensure the following people’s confidential personal information is not uploaded from your practice and record my dissent on their behalf by whatever means possible.
You can provide details of other family members you wish to opt out on a seperate sheet, but make sure this form is attached.
FIND OUT MORE
This leaflet was written with the help of Dr
Neil Bhatia, GP. We recommend you visit his
website www.care-data.info which provides
a more comprehensive view of the
care.data programme than the ‘Better
information means better care’ leaflet you
may have seen.
NHS England does provide some more
details at www.nhs.uk/caredata and the
Health and Social Care Information Centre
also has a page describing how it handles
your confidential medical information at
www.hscic.gov.uk/patientconf
Opting out will have no effect on your
medical care. If you are unsure what to do,
opt out now. You can discuss this with your
doctor at your next appointment and, if you
are satisfied, you can opt back in at any point.
Copies of this leaflet for you to print or e-mail
to friends and family can be downloaded
from http://optout.care-data.info
NOTES
Patient’s full name:
Address (if different):
Postcode:
Date of birth:
NHS number (if known):
M
I

The Brooke Surgery
20 Market Street
Hyde SK14 1AT Dr R Patel Dr W Tsang Dr J Dirckze Dr R Fletcher
Dr A Faruq
Application for online access to my medical record
Surname Date of birth
First name
Address
Postcode
Email address
Telephone number Mobile number
I wish to have access to the following online services (please tick all that apply):
1. Booking appointments
2. Requesting repeat prescriptions
3. Accessing my medical record
I wish to access my medical record online and understand and agree with each statement (tick)
1. I have read and understood the information leaflet provided by the practice
2. I will be responsible for the security of the information that I see or download
3. If I choose to share my information with anyone else, this is at my own risk
4. I will contact the practice as soon as possible if I suspect that my accounthas been accessed by someone without my agreement
5. If I see information in my record that is not about me or is inaccurate, I willcontact the practice as soon as possible
Signature Date
For practice use only Patient NHS number
Practice computer ID number
Identity verified by (initials)
Date Method Vouching
Vouching with information in record
Photo ID and proof of residence
Authorised by Date
Date account created
Date passphrase sent
Level of record access enabled Prospective
Retrospective All
Limited parts
Contractual minimum
Notes / explanation
v4 4 February 2015