the cardiac cycle & heart sounds jennifer kwan. disclaimer please note: audio files are not the...
TRANSCRIPT

The Cardiac Cycle&
Heart SoundsJennifer Kwan

DISCLAIMER
Please note: audio files are not the best in terms of quality, but they are available for you to use with headphones.

Key principles
• Blood flow depends on pressure gradients
• Pressure gradient = a difference between 2 pressures
• Pressure gradients in the heart depends on contractile
forces
• Blood pressure maintained by pumping of the heart
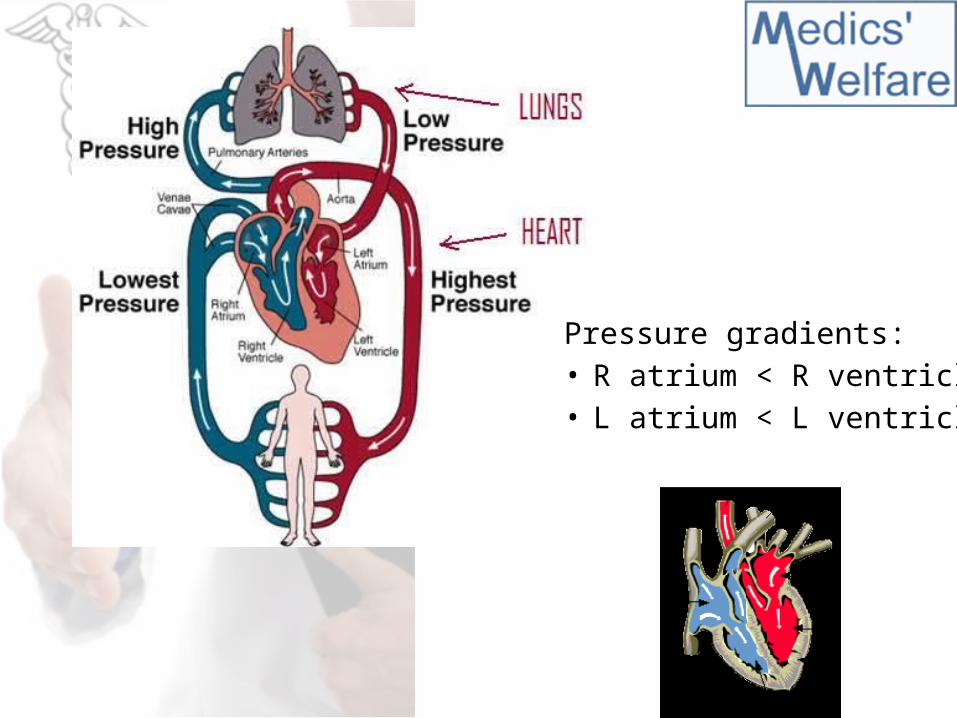
Pressure gradients:• R atrium < R ventricle• L atrium < L ventricle

Early diastole: atrial filling
• Ventricular relaxation
• Arterial pressure > ventricles = SL valves closed
• Ventricular pressure > atria = AV valves closed
Atrial filling and distension

Mid diastole: ventricular filling
• Atrial pressure > ventricles = AV valves open
• Blood returning from the veins flows passively from atria to ventricles
• 80% ventricular filling
SL valves are still closed
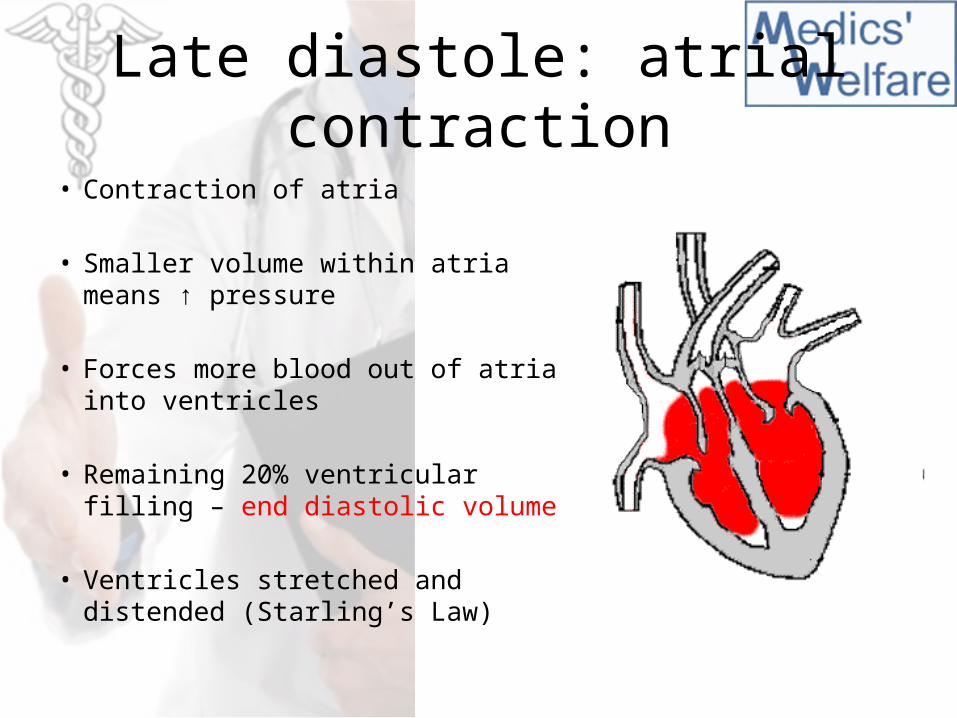
Late diastole: atrial contraction• Contraction of atria
• Smaller volume within atria means ↑ pressure
• Forces more blood out of atria into ventricles
• Remaining 20% ventricular filling – end diastolic volume
• Ventricles stretched and distended (Starling’s Law)

Early systole: ventricular contraction
• Atria remain relaxed from now on
• Ventricles begin to contract
• Ventricular pressure > atria = AV valves closed *1st heart sound*
Ventricles continue contracting but SL valves closed too
• Isovolumetric contraction

Late systole: ventricular contraction
• Isovolumetric contraction ↑ ventricular pressure rapidly
• Ventricular pressure > arteries = SL valves open
• Rapid ejection phase = pulse
• Ventricles still contracting so ventricular pressure still rises
AV valves still closed

Early diastole again• Ventricles begin to relax
• Arterial pressure > ventricles = SL valves closed *2nd heart sound* - end systolic volume
Ventricles continue relaxing but AV valves closed too
• Isovolumetric relaxation
• Arterial pressure maintained by elasticity
Cardiac cycle animated

Pressure changes
c
a v

Heart sounds
• 1st and 2nd heart sound – “lub” and “dub”3rd heart sound common in children 4th heart sound pathological
• Auscultation – turbulent blood flow not valve closure!
• Quality of 1st heart sound = longer, lower pitchQuality of 2nd heart sound = shorter, higher pitch “snap”

Heart murmurs
• Blood flow laminar = silent
• If it strikes obstruction, its flow becomes turbulent
• This generates abnormal heart sounds = murmurs
• In the heart, murmurs usually indicate valve problems(In children and elderly, murmurs can be physiological due to
thin walls that vibrate with rushing blood)

Sites of auscultation

ValvesAtrioventricular valves
Semilunar valves
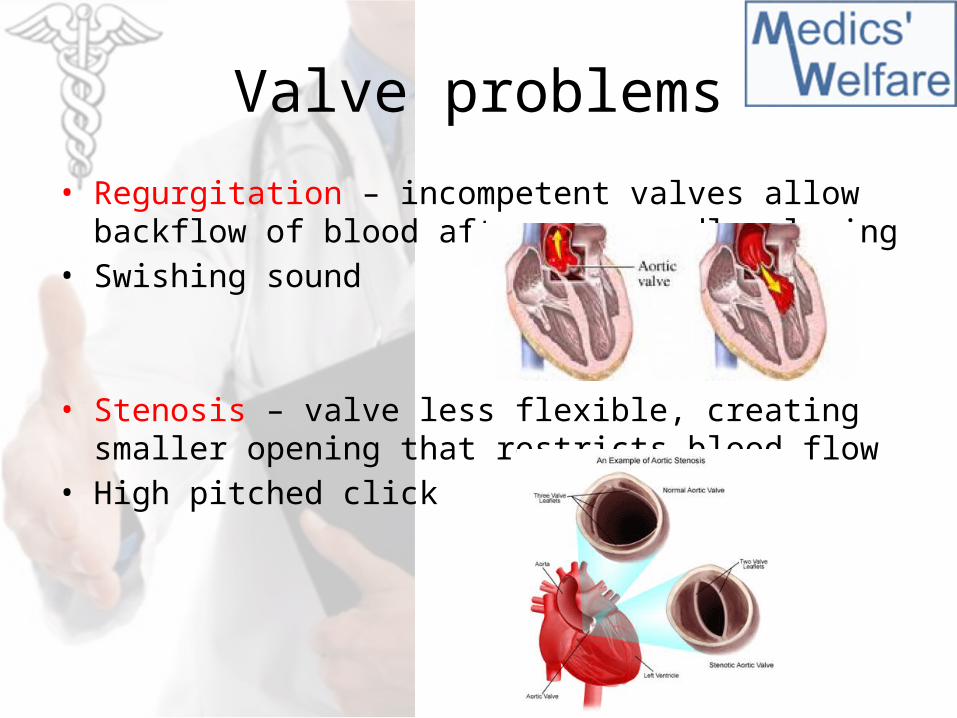
Valve problems
• Regurgitation – incompetent valves allow backflow of blood after supposedly closing
• Swishing sound
• Stenosis – valve less flexible, creating smaller opening that restricts blood flow
• High pitched click

Timing of murmurs
PASS and PAID
• Pulmonary, Aortic Stenosis = Systolic
• Pulmonary, Aortic Incompetency = Diastolic
Reverse for AV valves:(i.e. Mitral, Tricuspid stenosis = Diastole
Mitral, Tricuspid Incompetency = Systole)

Effect of respiration on murmurs
• Inspiration– ↑ negative pressure in thorax, so more venous return– Accentuates right- sided murmurs: pulmonary & tricuspid
• Ask patient to breathe in, hold, then auscultate
• Expiration– thoracic volume, so more blood pushed out of lungs– Accentuates left-sided murmurs: aortic & mitral
• Ask patient to breathe in, out, hold, then auscultate

Mitral regurgitation
• Systolic murmur
• As ventricle contracts, backflow through mitral valve
• Auscultate in axilla

Mitral stenosis
• Diastolic murmur
• As atrial pressure > ventricles, passive blood flow through small opening
• Auscultate 5th IC space, mid-clavicular linePatient rolls to leftUse bell

Aortic regurgitation
• Diastolic murmur
• As ventricle relaxes, arterial pressure > ventricles, backflow through aortic valve
• Auscultate 5th IC space, left sternal edgePatient leans forwardBreathe in, out, and hold

Aortic stenosis
• Systolic murmur
• As ventricles contract, forces blood through smaller aortic opening
• Auscultate carotidsUse bellBreathe in, out, and hold

Thank you!
Question time