the ckd patient in the office or er - peterborough ... talk 2016 dr... · the ckd patient in the...
TRANSCRIPT

The CKD patient in the office or ER
Dr. Vincent Cheung Nephrologist
Peterborough Regional Renal Program November 9th , 2016

Presenter Disclosure
• Dr. Vincent Cheung
• Relationships with commercial interests (in past 2 years):
• Grants/Research Support: none
• Speakers Honoraria: Servier, Janssen
• Consulting Fees: none
• Other: none

Disclosure of Commercial Support
• This presentation has received no financial on in-kind support
• Potential for conflict (s) of interest:
Dr. Cheung has not received any payment or funding in-kind for this program

Mitigating Potential Bias
• Where possible recommendations are supported by evidence
• Off label options are clearly indicated as such
• Many agents discussed are non proprietary

Objectives
• A Fib and NOACs in CKD
• Diuretics in CKD
• Treatment of Gout and Hyperuricemia in CKD
• Hyperkalemia
• Vaccines in CKD

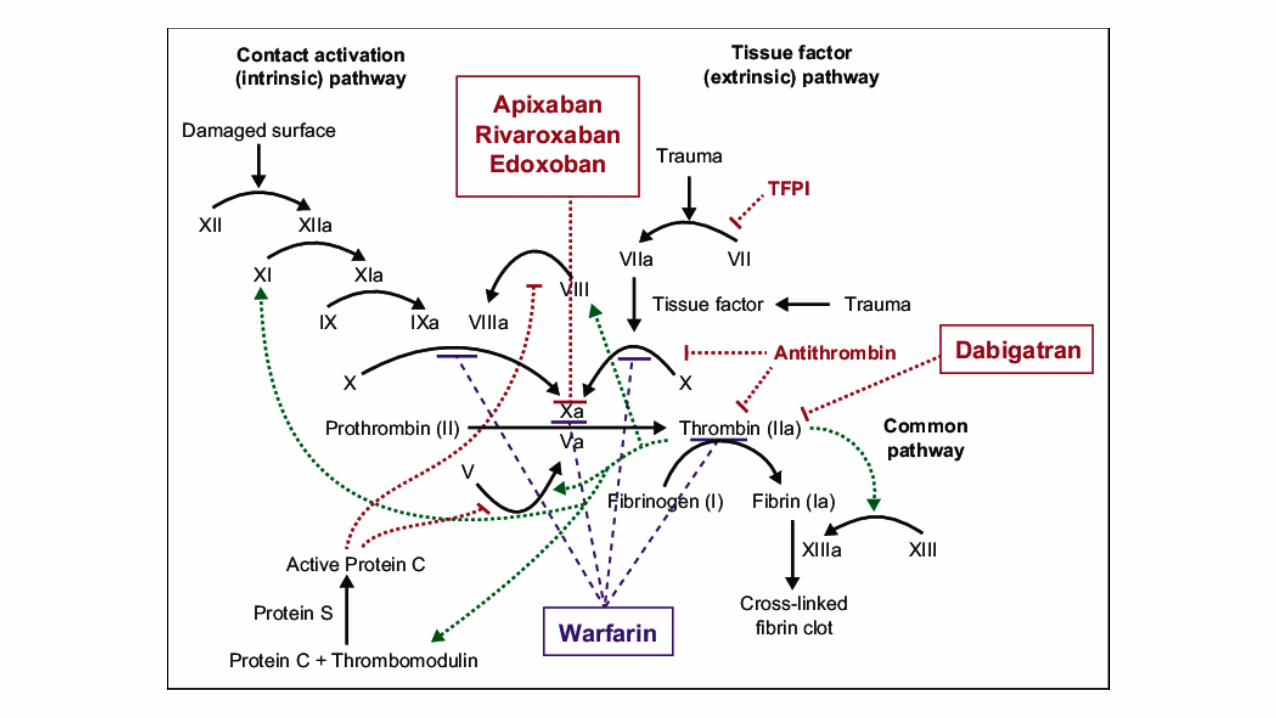
Atrial Fibrillation and Non Vit K Oral Anticoagulants in CKD

Effect on all stroke
Anticoagulation with Warfarin reduces ischemic stroke risk in Nonvalvular Atrial Fibrillation in the general population


NOACs vs. Warfarin • No need for blood testing/dose titration
• No interaction with food
• Less drug interactions
• Rapid onset of action, short half-life
• Equivalent (?better) risk reduction for ischemic stroke
• Better safety profile
• Little evidence/experience in advanced CKD/ERSD
• Lack of reversibility/antidote

Lancet. 2014 Mar 15;383(9921):955-62.
Relative risk 0.81

Lancet. 2014 Mar 15;383(9921):955-62.
Relative risk 0.86

Chronic Kidney Disease
• Increased risk of stroke (RR 3.7 in CKD, RR 5.8 in ESRD)
• Increased prevalence of atrial fibrillation
• CKD/ESRD patients largely excluded from trials
• Increased risk of bleeding if treated with anticoagulation
• Effect of anticoagulation on stroke risk in advanced CKD not clear – no direct randomized trial data

Risk of bleeding with anticoagulation increases with decreasing GFR
Jun M et al, BMJ 2015: 350, h246
Median follow-up 2.1 years

Sardar et al, Can J Cardiol, 2014
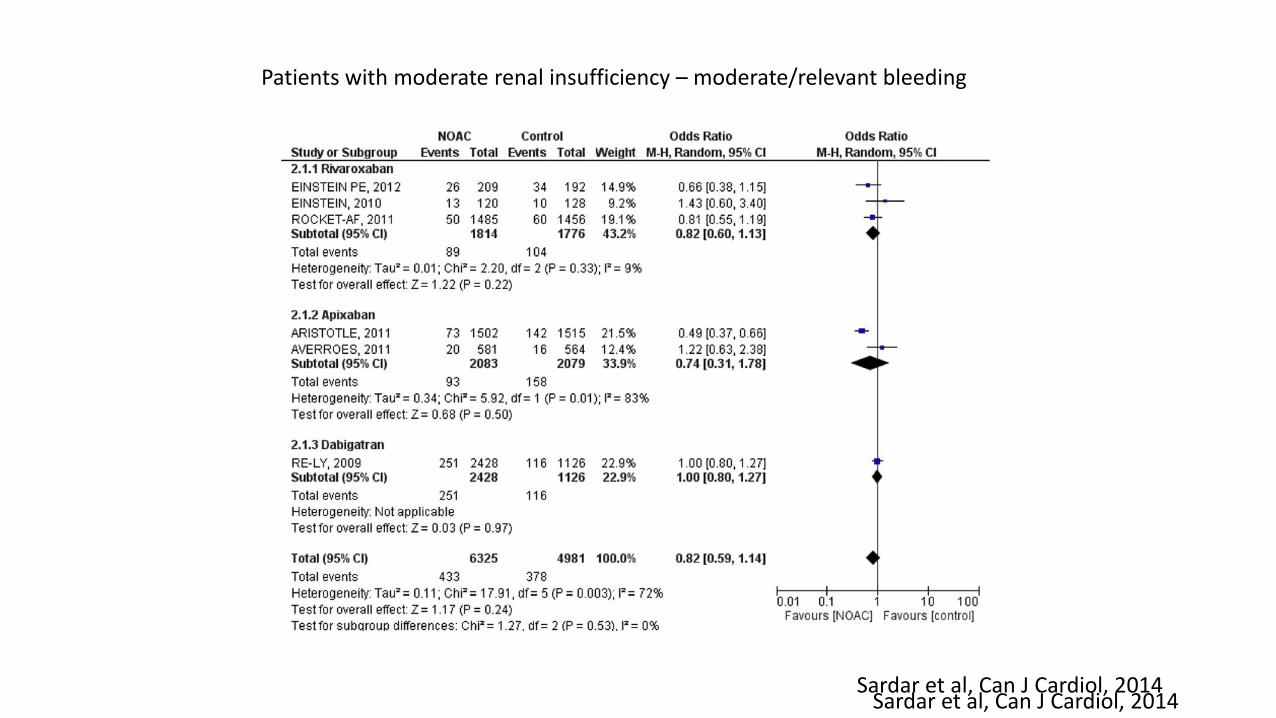
Patients with moderate renal insufficiency – moderate/relevant bleeding
Sardar et al, Can J Cardiol, 2014 Sardar et al, Can J Cardiol, 2014
Stroke risk Bleeding risk
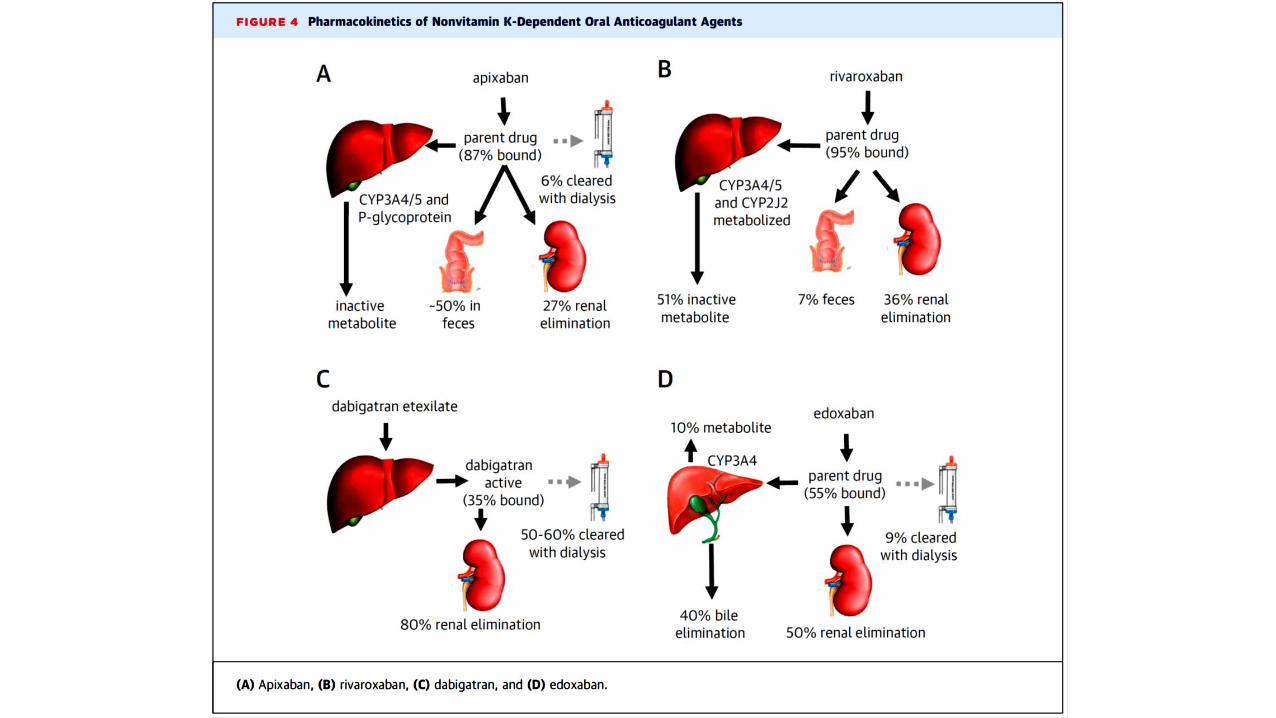

Dosing considerations for NOACs in CKD
FDA: indication for CrCl >15, and HD pt as of Jan 2014
FDA: indication for CrCl 15-30 – dose 75 mg bid
FDA: indication for CrCl 15-30 – dose 15 mg od

Conclusions - NOACs
• Patients with CKD have a greater risk of stroke and bleeding
• For CKD 3 and above (CrCl >30), there is benefit to anticoagulation, and NOACs are as efficacious and as safe as warfarin
• For patients with stage 4 and 5 CKD, benefit for stroke is unclear, and risks of bleeding high. If anticoagulation is pursued, warfarin is indicated. NOACs off label.
• Patients with CKD treated with anticoagulation require close monitoring of INR, renal function, signs of bleeding

Diuretic dosing considerations in CKD

Furosemide
• Loop diuretic • Introduced 1966 • Excretion 2/3 renal 1/3 hepatic • Half life 100 minutes
Diuretic resistance
Dose response characteristic
• Dose threshold
• All or none response
Distal Adaptation

Dose response curves
Graded response Threshold response R
esp
on
se
Dose
Res
po
nse
Dose

Furosemide dose-response curve
Uri
ne
pro
du
ctio
n in
6 h
rs
Dose
40 80 120 160 200 240 280

Furosemide dose-response curve
40 80 120 160 200 240 280
Worsening heart and/or renal function
Uri
ne
pro
du
ctio
n in
6 h
rs
Dose

Furosemide dose-response curve
40 80 120 160 200 240 280
Uri
ne
pro
du
ctio
n in
6 h
rs
Dose

40 80 120 160 200 240 280
Urine p
rod
uction in 6
hrs
Dose
A
B
C
Furosemide changed from 80 mg po od to 40 mg po bid

From Knauf & Mutschler Klin. Wochenschr. 1991 69:239-250
70%
20%
5%
4.5%
0.5% Volume 1.5 L/day
Urine Na 100 mEq/L Na Excretion 155 mEq/day
100% GFR 140 L/day
Plasma Na 140 mEq/L Filtered Load 26,100 mEq/day
CA Inhibitors Proximal tubule
Loop Diuretics Loop of Henle
Thiazides Distal tubule
Antikaliuretics
Collecting duct
Thick Ascending Limb

Diuretic sliding scale
• Escalating or declining loop diuretic dose dictated by daily weight
• Can incorporate thiazide diuretic as maintenance or rescue to counter adaptation
• Can incorporate potassium supplement to compensate for increased potassium losses
• Patient feedback and self management

Diuretic Sliding Scale WEIGHT FUROSEMIDE ZAROXOLYN POTASSIUM
less than 167 No Furosemide, take in more salt
167 to 168 No Furosemide
169 to 170 80 mg in AM 1 tab
171 to 173 80 mg in AM and PM 2 tabs
174 to 176 120 mg in AM and PM 2.5 mg 2 tabs
177 to 179 160 mg in AM and PM 5 mg 2 tabs bid
greater than 180 200 mg in AM and PM, call MD 10 mg 2 tabs bid
40 80 120 160 200 240 280
Urin
e p
rod
uctio
n in
6 h
rs
Dose
A
B
C

Management of Gout/Hyperuricemia in CKD

Hyperuricemia and Gout in CKD
• Common issue in CKD • Decreased uric acid excretion due to reduced GFR • Hyperuricemia associated with metabolic syndrome • Frequent use of drugs which increase uric acid: Diuretics, Low dose ASA, Beta
blockers, cyclosporine/tacrolimus
• Similar to management in general population, but with considerations regarding drug selection and dosing
• Acute gout
• Uric acid lowering for prevention

Anti-inflammatory treatment of acute gout
- Initiate treatment as early as possible
- Consider renal function and comorbidities in drug selection
- Do not start or alter urate lowering therapy during acute episode

Anti-inflammatory treatment of acute gout • NSAID
• Avoid in patients on anticoagulation • Watch renal function, consider temporary reduction/withdrawal of ACE/ARB
to avoid AKI • Adverse effects: Volume retention, renal dysfunction, peptic ulceration, hypertension,
increased CV risk
• Colchicine • Lower dose in patients with CrCl<30, avoid in patients with CrCl<10 • Less effective if late presentation • Adverse effects: Diarrhea, sensimotor neuromyopathy, myelosuppression
• Corticosteroids • Oral or parenteral • Relapse likely if stopped too soon • Adverse effects: Volume retention, hyperglycemia, thrush, peptic ulceration, Weight gain,
sleep disturbance, AVN Hip, osteoporosis, cataracts

Urate Lowering Therapy
• Start 1-2 week after acute attack treated with anti-inflammatory therapy
• Anti-inflammatory prophylaxis for 6 – 9 months recommended to avert flare
• Aim for uric acid level 360
• Continue indefinitely

Urate Lowering Therapy
• Allopurinol • Max dose 300 mg daily for CrCl 20-50, 200 mg for CrCl < 20
• Can cause rash, pruritis, elevated LFTs, hypersensitivity reaction
• Febuxostat • For use if intolerant to Allopurinol
• No data for CrCl < 30
• Probenecid • Uricosuric, use only with CrCl > 50
Reducing Hyperuricemia
• Reduce diuretics, especially thiazides
• Consider once daily or alternate day loop diuretic dose
• Low purine diet
• Weight loss/exercise
• Consider switching ACE/ARB to Losartan
• Consider stopping ASA

Am J Kidney Dis 47:51-59.

Hyperkalemia

Emergent treatment of Hyperkalemia
peaked T wave increased PR interval
flat or absent P wave sine wave
widened QRS ventricular standstill

Emergent treatment of Hyperkalemia
• Membrane stabilization Calcium Gluconate 1 gm IV push over 2 min. Effect lasts 30 - 60 min. Contraindication if on Digoxin
• Shifting strategies Beta agonist: Ventolin puffer or mask. Effects last 30 – 60 min. Caution if cardiac ischemia or tachycardia.
Alkalinization: IV Na Bicarbonate
Insulin
• Excretion/Removal Gut: Kayexalate/Ca resonium. Effect onset 4-6 hours
Kidney: Loop/Thiazide diuretics. Effect onset 4-6 hours
Dialysis Time to machine ???

Emergent treatment of Hyperkalemia
1. Give calcium IV and/or Ventolin
2. Start IV D5 with 3 amp/L NaBicarb and 20 u/L insulin R and run at 75 to 150 cc/h
3. Start Kayexalate 30 gm q2h x 3 and/or Lasix 40-160 mg IV
4. Check glucose and K+ q1h x 4
5. Watch ECG/monitor

Vaccines for CKD

Vaccines for CKD
• Inactivated Influenza Vaccine
• 23 Valent Pneumococcal Vaccine
• Hepatitis B Vaccine
Live vaccines should be avoided in transplant patients, and others on immunosuppressive medications

Sick Day Medication Advice

Sick Day Medication Advice
• Pre-emptive temporary withdrawal of certain medications during period of dehydrating illness
• Diarrhea, vomiting, poor intake
• Excessive heat exposure, bowel prep, high output ostomy
• Instruct patients to stop ACE, ARBs, diuretics, NSAIDs and NSAID creams, SGLT2 inhibitors to avert renal failure and hypotension
• Stop metformin, gliclazide, rosuvastatin, ??NOACs
• Can resume usual meds when better