the cranky baby the neonatal › wp-content › uploads … · medical center nicu. disclosures no...
TRANSCRIPT
THE CRANKY BABY– THE NEONATAL ABSTINENCE SYNDROME…WITHDRAWAL IN
THE NEONATE
Evelyn Rider, MD – Medical Director Alaska Regional Hospital NICU and NEST Program
And Staff Neonatologist The Children’s Hospital at Providence NICU
Alaska Neonatology Associates, MEDNAX Medical Group

ACKNOWLEDGEMENTS
• Alaska Neonatology Associates Group
• C. Denise Rose, MSN, ANP-Board Certified Neonatology
• William Trawick, ANP-Board Certified Neonatology
• Staff at Alaska Regional Hospital NEST/NICU
• Staff at The Children’s Hospital at Providence/Providence Alaska Medical Center NICU

DISCLOSURES
No conflicts of interest to disclose
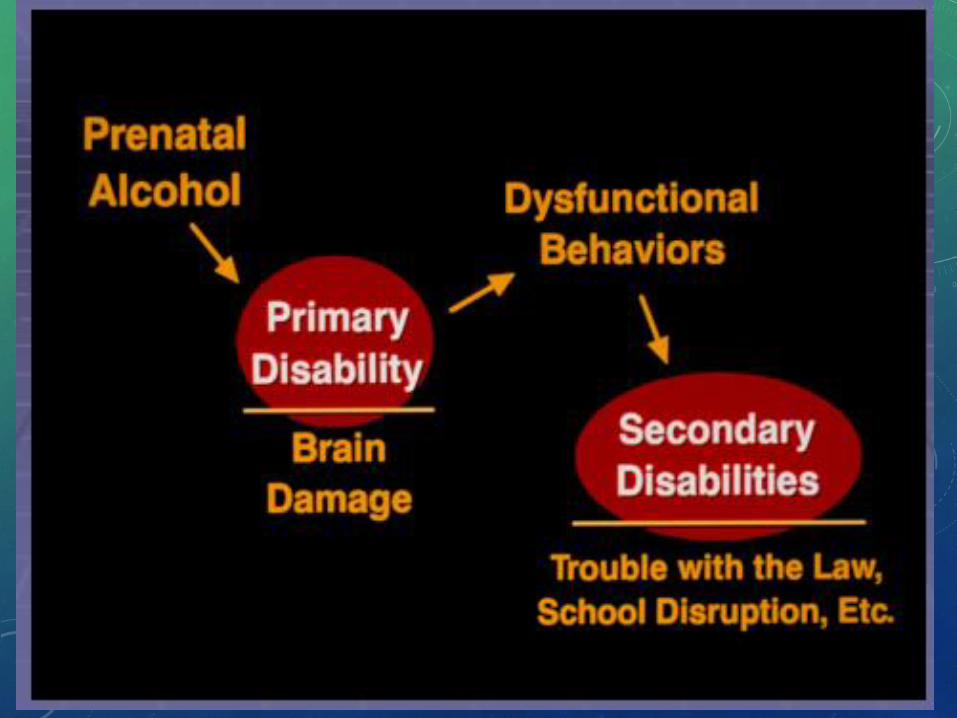
HOW DOES PRENATAL SUBSTANCE ABUSE COUNT AS TRAUMA OR ABUSE TO THE NEWBORN????
• Trauma – a deeply distressing or disturbing experience; physical
injury; an emotional response to a terrible event or experience
• Abuse – verb
• Use (something) to bad effect or for a bad purpose, misuse
• Treat (a person or animal) with cruelty or violence regularly or repeatedly
• Abuse – noun
• Cruel and violent treatment of a person or animal
• Abuse – can be physical, sexual, emotional, verbal or in combination
IMAGINE………..


OBJECTIVES
• Understand the prevalence of prenatal substance abuse and the potential number of pregnancies and babies affected
• Be familiar with Neonatal Abstinence Syndrome
• Understand the effects of maternal prenatal substance abuse on the baby – before, during and after birth
• Discuss the cost to society of substance abuse in pregnancy and its consequences for the mother/baby/family
• Cost of care, Cost in Lost Future Potential for Society
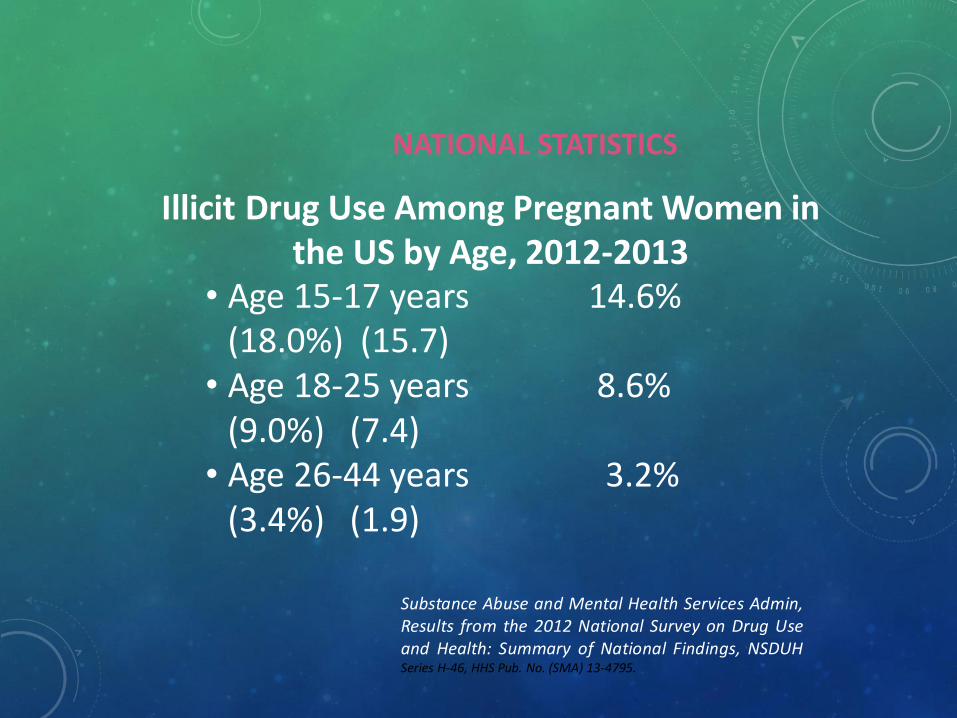
NATIONAL STATISTICS
Illicit Drug Use Among Pregnant Women in the US by Age, 2012-2013
• Age 15-17 years 14.6% (18.0%) (15.7)
• Age 18-25 years 8.6% (9.0%) (7.4)
• Age 26-44 years 3.2% (3.4%) (1.9)
Substance Abuse and Mental Health Services Admin,Results from the 2012 National Survey on Drug Useand Health: Summary of National Findings, NSDUHSeries H-46, HHS Pub. No. (SMA) 13-4795.
WHAT SUBSTANCES ARE ABUSED
SUBSTANCES ABUSED IN PREGNANCY
• Illicit Drugs - Polysubstance Use is the NORM
• Tobacco
• Other Forms of Nicotine
• Alcohol
• Prescription Drugs, especially Narcotics/Opioids

TOBACCO – MARKER FOR OTHER SUBSTANCE ABUSE
• “women who had smoked ….. were 8x more likely to use alcohol or drugs during pregnancy than women who had done neither”
Chasnoff IJ. Screening for substance use in pregnancy: A practical approach for the primary physician. American Journal of Obstet Gynecol.
2001:184:752-8
Prescription Drug Abuse: The white collar drug2nd most commonly abused substances following marijuana
“One in five women enrolled in state Medicaid filled a prescription for opioids during pregnancy.”
Increase in Prescription Opioid Use During Pregnancy Among Medicaid-Enrolled WomenDesai, Rishi J.; Hernandez-Diaz, Sonia; Bateman, Brian T.; More Obstetrics & Gynecology. 123(5):997-1002, May 2014.
“More than 14 percent of pregnant women were prescribed opioids for pain at some time during their pregnancy”
Patterns of Opioid Utilization in Pregnancy in a Large Cohort of Commercial Insurance Beneficiaries in the United StatesBrian T. Bateman, Sonia Hernandez-Diaz, James Rathmell, et.al.Anesthesiology. The Journal of the American Society of Anesthesiologist.February 2014-Volume 120-Issue 2-pA13-A18Doi: 10.1097/01.anes.0000442608.71529.4a
PRESCRIPTION OPIOID EPIDEMIC
• Patrick et al. JAMA. 2012;307(18):1934-1940. Data 2000-2009
• Maternal opiate use increased from 1.19 to 5.63/1000 live births
• Patrick et al Pediatrics 2015;135(5):842-850.
• Rx Data linked to Vital Stats for mothers enrolled in Tennessee Medicaid 2009-2011 (n=112,029 pregnancies)
• ~ 1 in 3 (31,354 = 28%) Pregnant Women used at least 1 opioid
• Quarterly NAS rate increased from ~6 to 10.7/1000 live births
• Compared to Women who did not have opioid Rx:
• Depression (5.3% vs 2.7%)
• Anxiety Disorder (4.3% vs 1.6%)
• Tobacco Use (41.8% vs 25.8%)
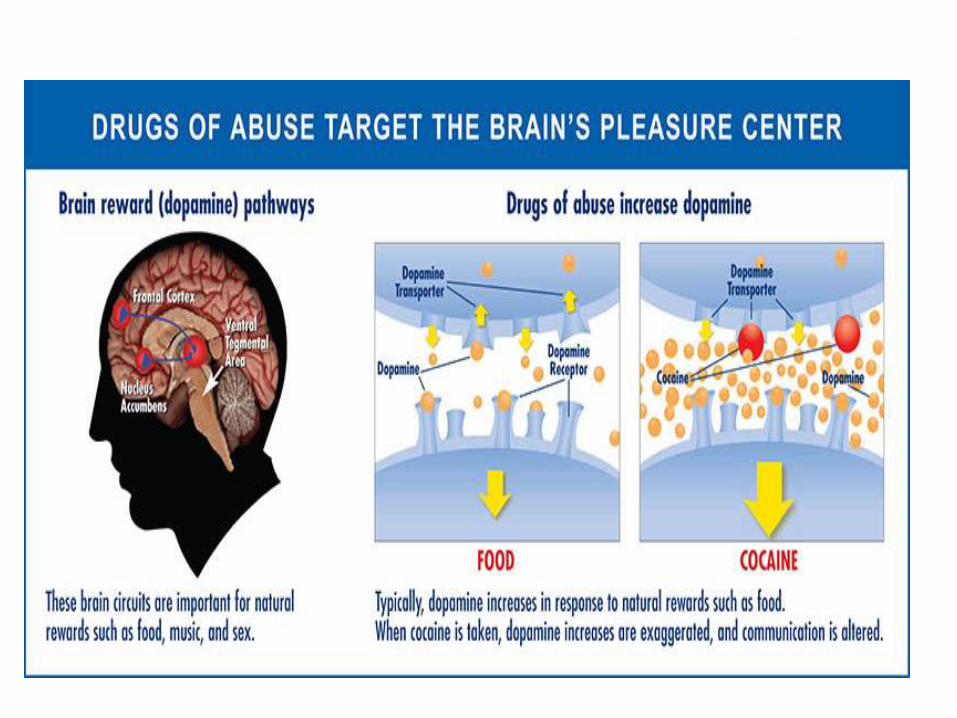
PATHOPHYSIOLOGY – MATERNAL EFFECTS
• Similar mechanism of action for almost all addictive drugs – alteration in pathways for reward.
• Through complex neurochemical interactions, various chemicals act to increase dopaminergic pathways.
• Negative feedback loops created to inhibit dopamine uptake to attenuate the reward mechanism of the brain.

WHAT (LEGAL) DRUG ABUSE MAY LOOK LIKE NOW
AND THIS……………
AND IN SOME STATES, INCLUDING ALASKA, THIS…….(2015 REPORT - 1 IN 14 ALASKA WOMEN USE MARIJUANA)

DETECTION/TESTING
• Urine Drug Screening – Mothers during Pregnancy; time of delivery
• Urine Drug Testing of Newborn – must be done immediately; sampling very time dependent
• Umbilical Cord Tissue Testing – historical exposure
• 12/13 drug panels identify up to 30 different drug and alcohol biomarkers
• Meconium – time dependent; historical exposure
• Hair Analysis (research)
UNITED STATES DRUG TESTING LABORATORIES
1700 SOUTH MOUNT PROSPECT ROAD
DES PLAINES, ILLINOIS 60018
Phone: (847) 375-0770 / Fax: (847) 375-0775
Email: [email protected]
Visit us @ http:// www.usdtl.com
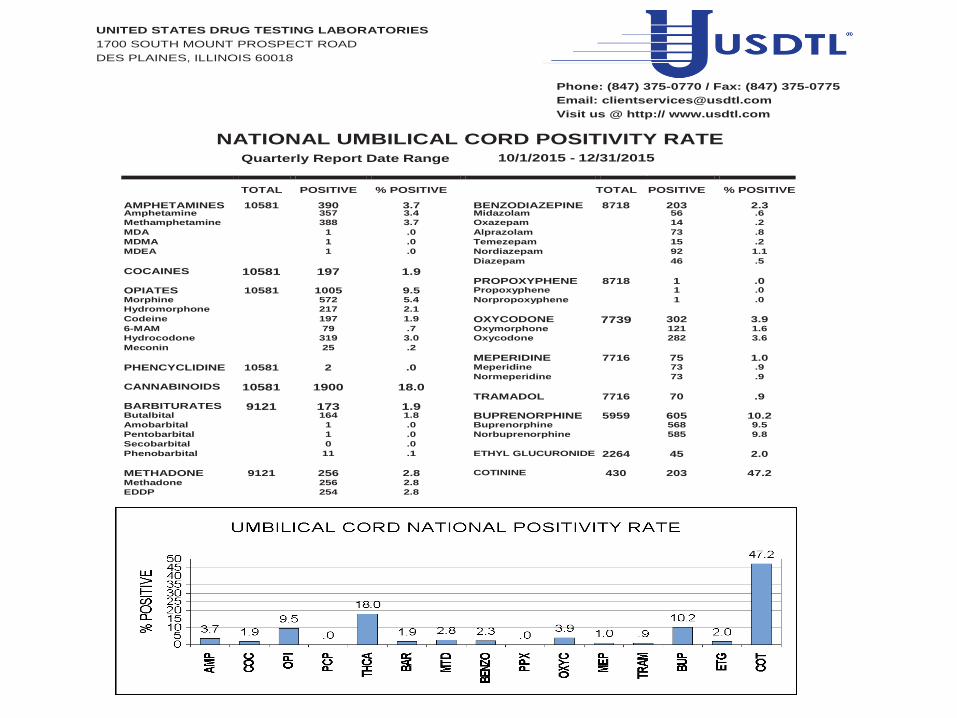
NATIONAL UMBILICAL CORD POSITIVITY RATE Quarterly Report Date Range 10/1/2015 - 12/31/2015
AMPHETAMINES
TOTAL
10581
POSITIVE
390
% POSITIVE
3.7
BENZODIAZEPINE
TOTAL
8718
POSITIVE
203
% POSITIVE
2.3 Amphetamine 357 3.4 Midazolam 56 .6
Methamphetamine 388 3.7 Oxazepam 14 .2
MDA 1 .0 Alprazolam 73 .8
MDMA 1 .0 Temezepam 15 .2
MDEA 1 .0 Nordiazepam 92 1.1
Diazepam 46 .5
COCAINES 10581 197 1.9 PROPOXYPHENE 8718 1 .0 OPIATES 10581 1005 9.5 Propoxyphene 1 .0
Morphine 572 5.4 Norpropoxyphene 1 .0
Hydromorphone 217 2.1 Codeine 197 1.9 OXYCODONE 7739 302 3.9 6-MAM 79 .7 Oxymorphone 121 1.6
Hydrocodone 319 3.0 Oxycodone 282 3.6
Meconin 25 .2 MEPERIDINE 7716 75 1.0 PHENCYCLIDINE 10581 2 .0 Meperidine 73 .9
Normeperidine 73 .9
CANNABINOIDS 10581 1900 18.0 TRAMADOL 7716 70 .9 BARBITURATES 9121 173 1.9 Butalbital 164 1.8 BUPRENORPHINE 5959 605 10.2 Amobarbital 1 .0 Buprenorphine 568 9.5
Pentobarbital 1 .0 Norbuprenorphine 585 9.8
Secobarbital 0 .0 Phenobarbital 11 .1 ETHYL GLUCURONIDE 2264 45 2.0
METHADONE 9121 256 2.8 COTININE 430 203 47.2 Methadone 256 2.8 EDDP 254 2.8
Page 39 of 39 Friday, January 01, 2016
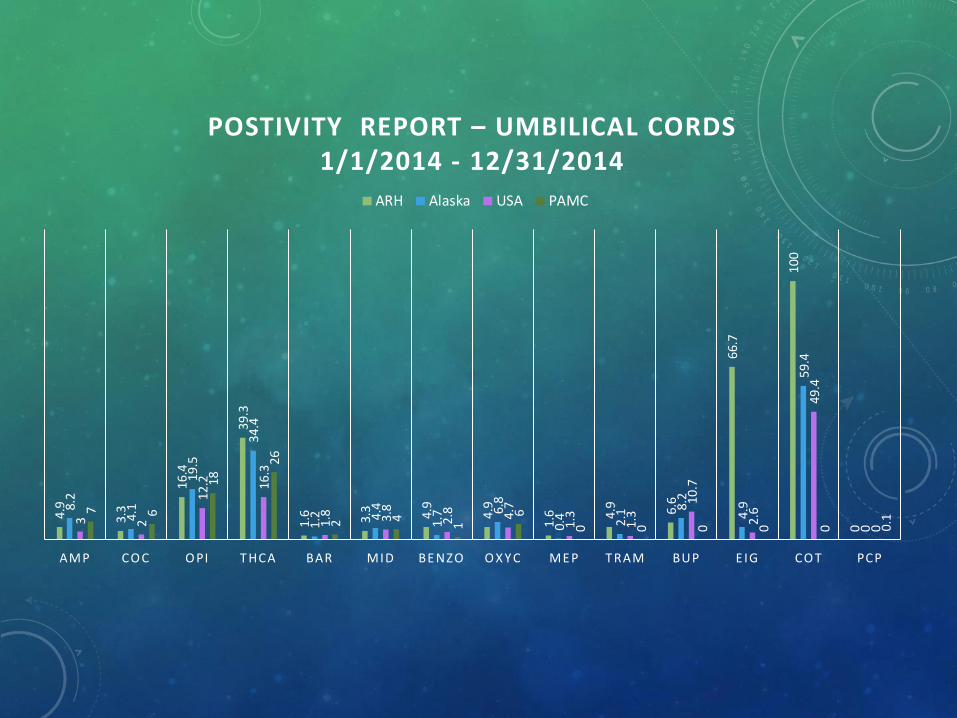
4.9
3.3
16.4
39.3
1.6 3.3 4.9
4.9
1.6 4.
9 6.6
66.7
100
0
8.2
4.1
19.5
34.4
1.2 4
.4
1.7 6.
8
0.4 2.1
8.2
4.9
59.4
0
3 2
12.2 16
.3
1.8 3.8
2.8 4.7
1.3
1.3
10
.7
2.6
49.4
0
7 6
18
26
2 4
1
6
0 0 0 0 0 0.1
AMP CO C O PI T HCA BAR MID BE NZO O X Y C ME P T RAM BUP E IG CO T PCP
POSTIVITY REPORT – UMBILICAL CORDS1/1/2014 - 12/31/2014
ARH Alaska USA PAMC
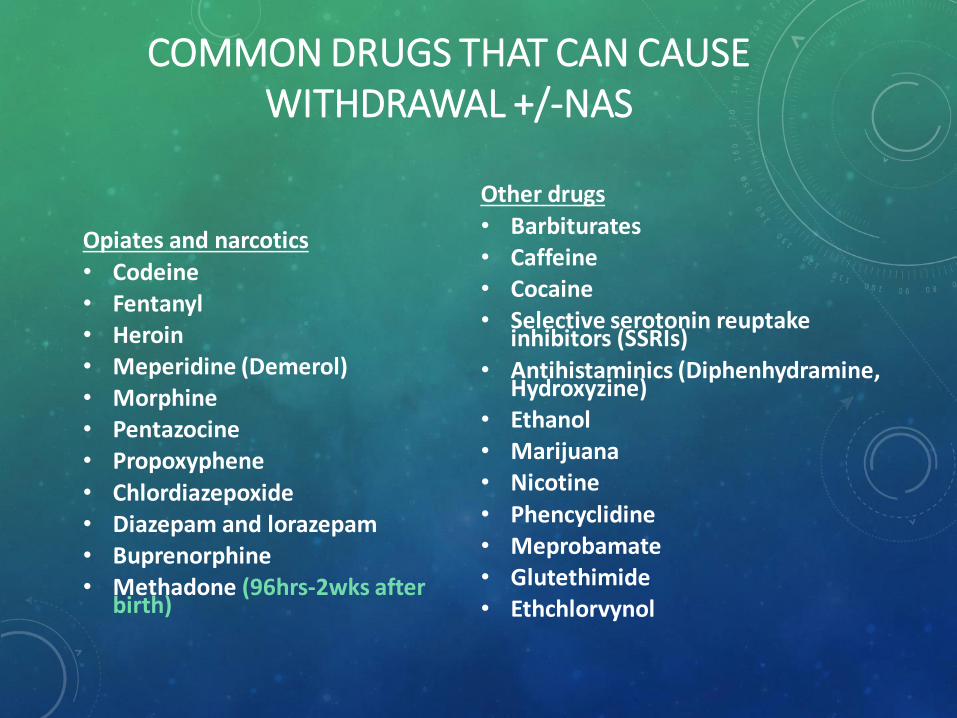
COMMON DRUGS THAT CAN CAUSE WITHDRAWAL +/-NAS
Opiates and narcotics
• Codeine • Fentanyl• Heroin • Meperidine (Demerol) • Morphine • Pentazocine• Propoxyphene
• Chlordiazepoxide• Diazepam and lorazepam• Buprenorphine• Methadone (96hrs-2wks after
birth)
Other drugs
• Barbiturates • Caffeine • Cocaine • Selective serotonin reuptake
inhibitors (SSRIs)
• Antihistaminics (Diphenhydramine, Hydroxyzine)
• Ethanol • Marijuana • Nicotine
• Phencyclidine • Meprobamate• Glutethimide• Ethchlorvynol
EFFECTS ON THE FETUS AND NEWBORN

NATIONAL INSTITUTE ON DRUG ABUSETOPICS IN BRIEF 2011
• Prenatal Exposure to Drugs of Abuse – May 2011 Research Update
• 2008-2009 Combined Data from National Survey on Drug Use and Health
• Confirmed ADVERSE outcomes from exposure to Nicotine, Alcohol, Cocaine, Marijuana and other Illicit Drugs
• However….this statement: “…although use of heroin (an opiate) during pregnancy has been associated with low birth weight, the impact of prescription opiate abuse on pregnancy outcomes is NOT WELL UNDERSTOOD
WHAT WE KNOW IN 2016
• Prescription Opiate Use/Abuse in Pregnancy Results in Neonatal Abstinence Syndrome
• Combined Use with Tobacco, Alcohol, and/or other Illicit Drugs worsen the effects on the fetus and newborn
• Increased prematurity, low birth weight, congenital defects including strokes and brain defects, other complications after birth
• Longer hospital stays and higher cost of care in the hospital and out
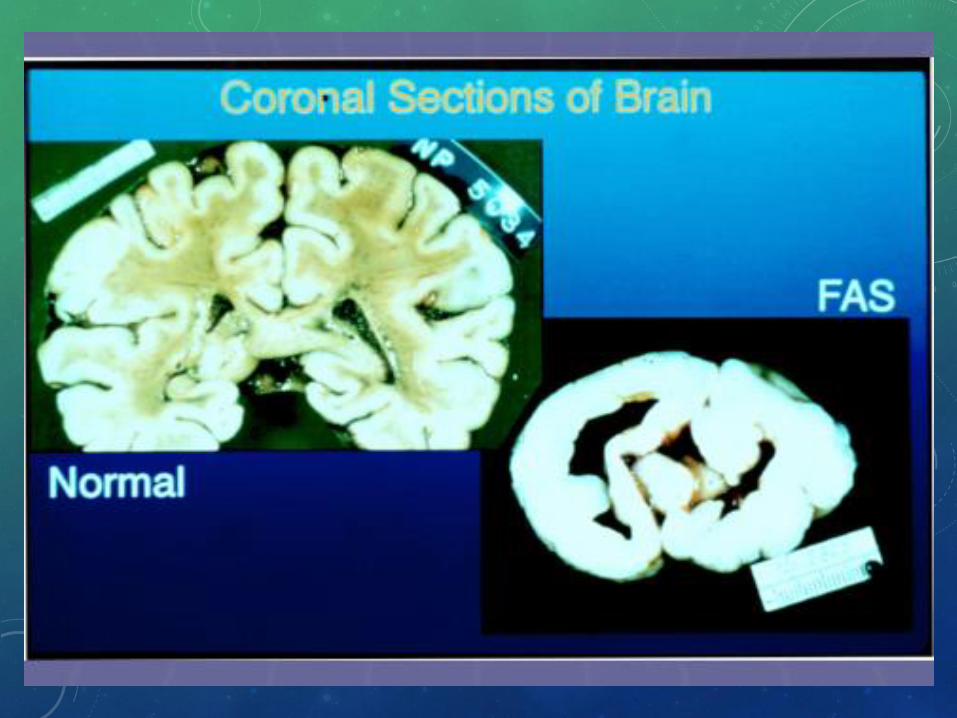
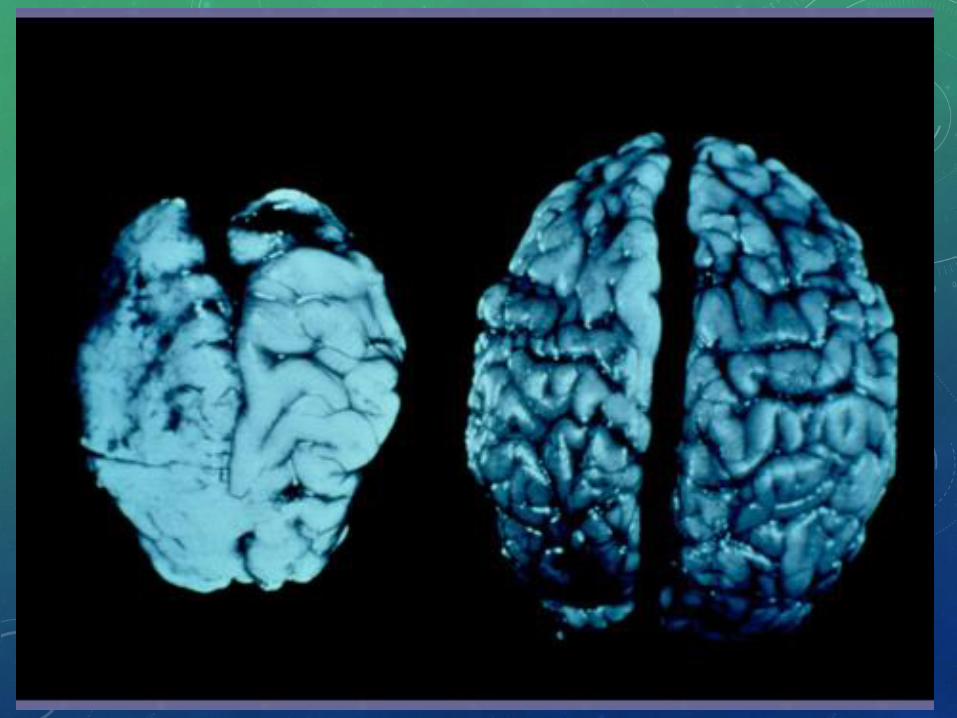
PATHOPHYSIOLOGY – FETAL EFFECTS
• Impact on developing brain most critical.
• Two broad classes of fetal brain insult:
• First 20 wks of gestation – damage during cytogenesis and cell migration
• Second 20 wks – damage during brain growth and differentiation.
• Continuous use - disruption of complicated neural pathways affects developing brain’s ability to learn and mature.
• Other organ effects – especially when polysubstance abuse: strokes, vascular accidents (intestinal complications – atresias, ?gastroschisis), FAS
NEONATAL EFFECTS
• Acute Effects – NAS
• Collection of behavioral and physiological signs and symptoms due to withdrawal from exposure to narcotics
• Long Term Effects – Learning, Social
• Behavioral, related to effects on developing brain (functional/structural), not withdrawal
FETAL/NEONATAL EFFECTS –ACUTE/EARLY
• Withdrawal – like symptoms (behavioral; marijuana, cocaine, meth): irritability, trembling, poor state regulation, poor sleep patterns
• Neonatal Abstinence Syndrome – true withdrawal symptoms that may benefit from pharmacologic therapy
http://d15gtop1hlgyun.cloudfront.net/content/pediatrics/134/2/e547/F2.medium.gif
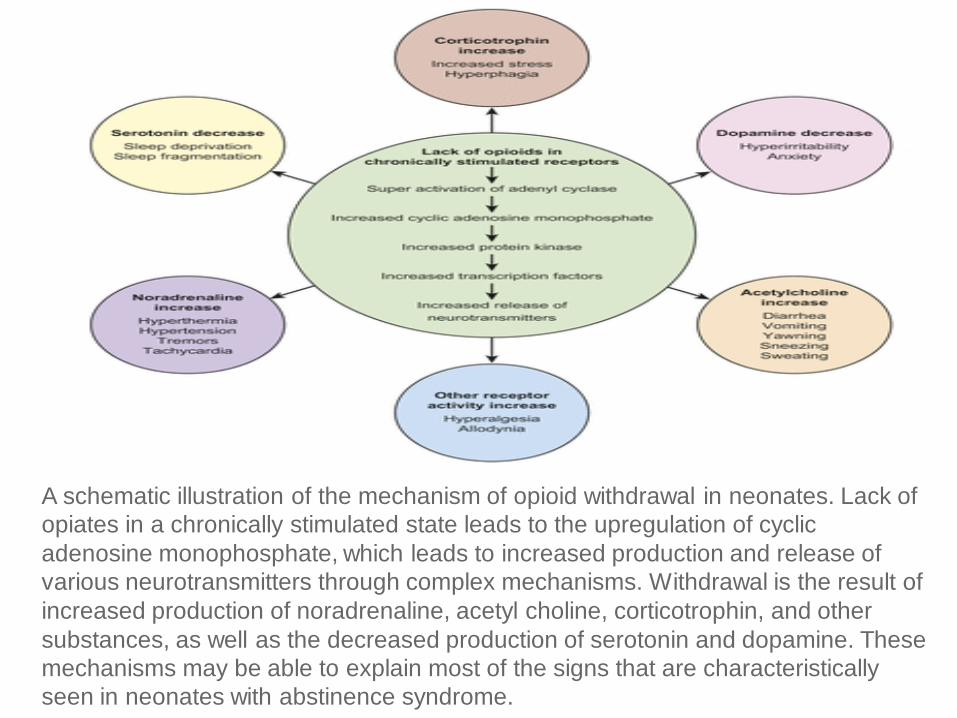
A schematic illustration of the mechanism of opioid withdrawal in neonates. Lack of
opiates in a chronically stimulated state leads to the upregulation of cyclic
adenosine monophosphate, which leads to increased production and release of
various neurotransmitters through complex mechanisms. Withdrawal is the result of
increased production of noradrenaline, acetyl choline, corticotrophin, and other
substances, as well as the decreased production of serotonin and dopamine. These
mechanisms may be able to explain most of the signs that are characteristically
seen in neonates with abstinence syndrome.
NAS SYMPTOMS
Irritability
Crying
Tremor
Hypertonicity
Generalized convulsions or Sz
Sleeplessness
Sweating
GI upset
Loose Stools
Yawning
Sneezing
Hiccups
Excessive Suck
Poor Feeding
Emesis
SCORING SYSTEMS – CHALLENGES IN ASSESSING NAS
• ALL Scoring Systems are based on opiate withdrawal; based on term newborns
• Intended for NAS to determine need for therapeutic intervention – with or without the aid of medication(s)
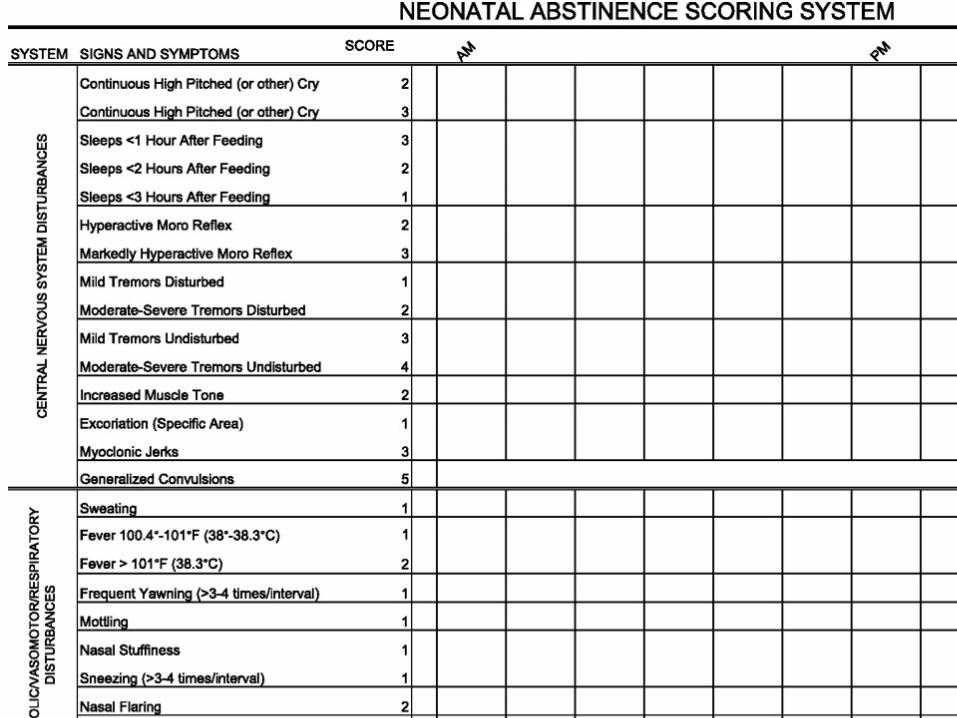
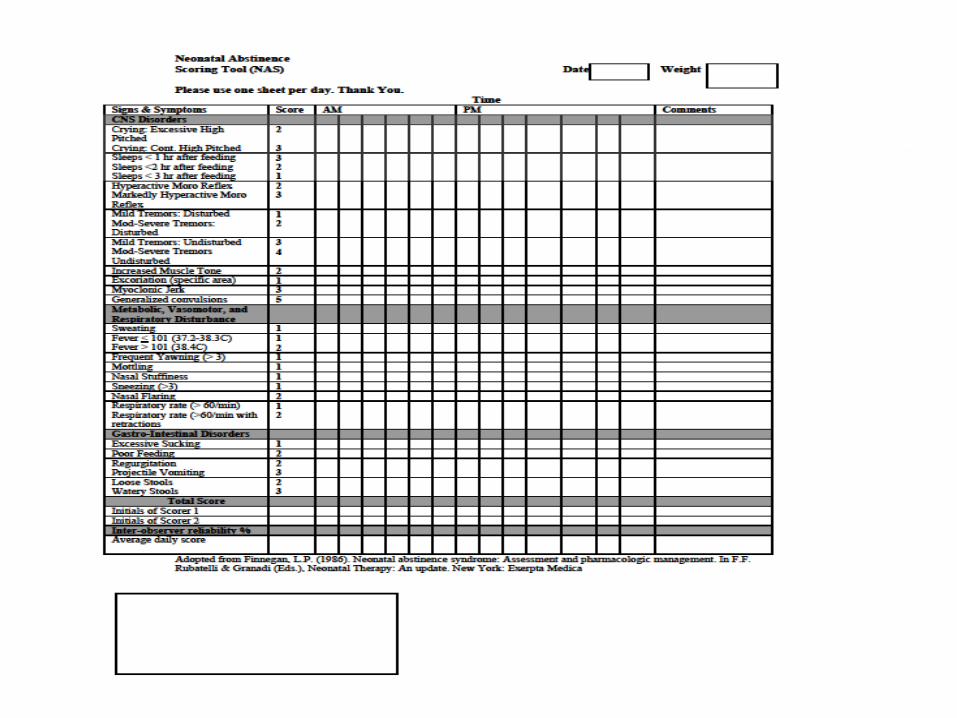
• Gold Standard – Finnegan Scoring System
• 21 items assessed/scored individually
• Inter-rater variability
• Modified Finnegan
• Others –
• Neonatal Withdrawal Inventory
• Neonatal Narcotic Withdrawal Index
• Neonatal Brazelton Neurobehavioral Scales
• Neonatal Network Neurobehavioral Scales
DECISION FOR TREATMENT
• Consistency is important – Protocols help improve outcomes, decrease length of stay
• Train all care givers and audit for maintaining appropriate inter-rater reliability
• Decide which scoring system is best for your facility
• Thresholds for treatment
• Nonpharmacologic/Supportive Treatment
• Pharmacologic Therapy
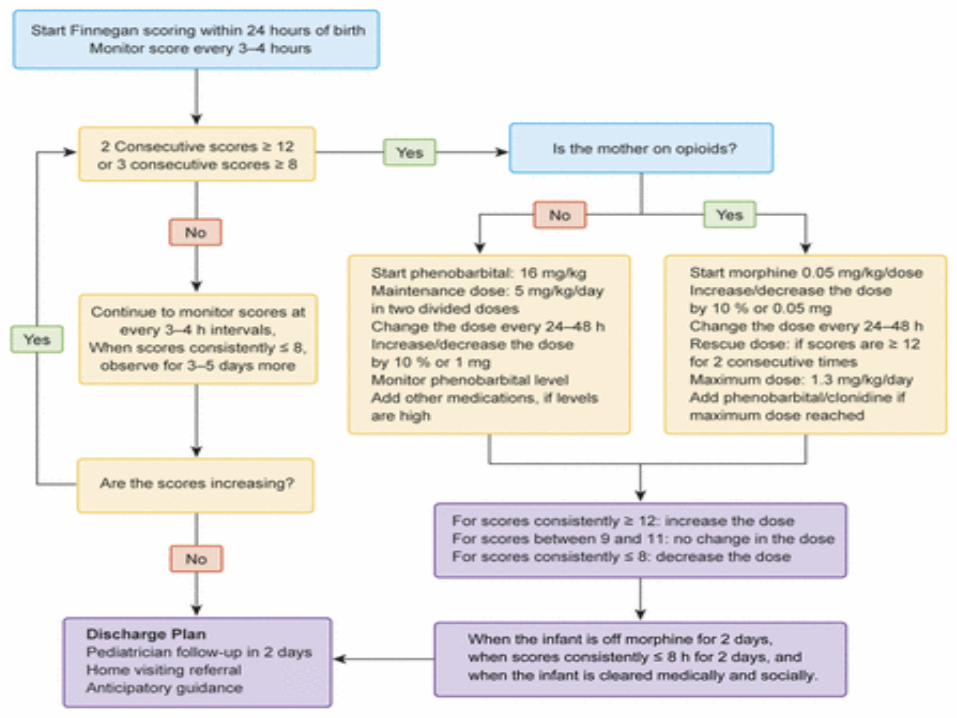
. eFIGURE 3A management plan for NAS in neonates. Medications are to be
initiated, increased, decreased, or discontinued depending on the Finnegan score.
Morphine can be initiated at a higher dose if scores are high; for example, if the
scores are 17 to 20, morphine can be started at 0.12 mg per dose, and if the
scores are ≥25, morphine can be initiated at 0.20 mg per dose.49 Morphine dose
can also be escalated by >10% for higher scores.21 Methadone can be substituted
for morphine for opioid withdrawal. Cardiopulmonary monitoring of the infant is
preferred during the acute stage.
PHARMACOLOGIC TREATMENT OPTIONS FOR NAS
• Morphine
• Phenobarbital
• Clonidine
• Methadone
MANAGEMENT OF THE DRUG EXPOSED NEONATE
• Do not use Naloxone
• Start NAS scoring
• Conservative measures for all
• Pharmacologic therapy if indicated
• Long term follow up – neurodevelopmental sequelae, child safety, family health, learning challenges
• CNS imaging if delayed developmental milestones

LONG-TERM EFFECTS (NOT WITHDRAWAL)
• Early phase: hyperactivity, disturbed sleep and increased lability of state last up to 12 wks- 6months. Hutchings et al
• Difficulty being consoled.
• Abnormal sleep patterns
• increase in rapideye-movement sleep
• decrease in quiet sleep
• increase myoclonus sleep
• Prolonged sucking bursts, fewer pauses, more feeding problems and increased arousal (sleeping, drowsy, alert, fussy/crying)
• More reactive to increases in the level of stress
• Poor tolerance to environmental changes
• Hypertonicity subsides after 6-7 months Hayford et al, Dinges et al
LONG TERM EFFECTS
• Opiate-exposed: a poor response to visual stimuli, decreased orientation to auditory stimuli, and deficient interactive behavior. Wagner et al, Strauss et al
• Methadone-exposed: had a 3.7-fold higher risk of SIDS compared with nonexposed controls Szeto et al, Hutchings et al
• Heroin-exposed: had a 2.3-fold higher risk of SIDS Hutchings et al
• Cocaine-exposed: infants displayed significantly greater state lability and shorter sleep bouts, fussed or cried more often, and spent less time asleep and more time in transitional states. Eiden et al
• Late phase: >7months: impaired organizational and perceptual abilities, poor self-adjustment and in situations requiring motor inhibition, heightened activity Hutchings et al
Date of download: 11/9/2015Copyright © 2015 American Medical
Association. All rights reserved.
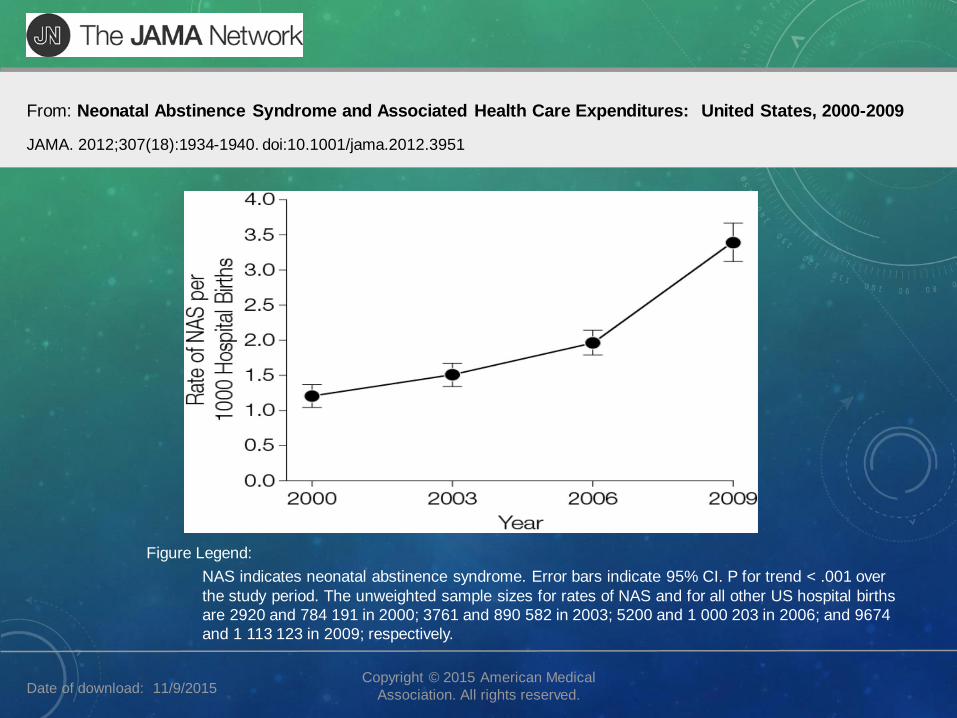
From: Neonatal Abstinence Syndrome and Associated Health Care Expenditures: United States, 2000-2009
JAMA. 2012;307(18):1934-1940. doi:10.1001/jama.2012.3951
NAS indicates neonatal abstinence syndrome. Error bars indicate 95% CI. P for trend < .001 over
the study period. The unweighted sample sizes for rates of NAS and for all other US hospital births
are 2920 and 784 191 in 2000; 3761 and 890 582 in 2003; 5200 and 1 000 203 in 2006; and 9674
and 1 113 123 in 2009; respectively.
Figure Legend:
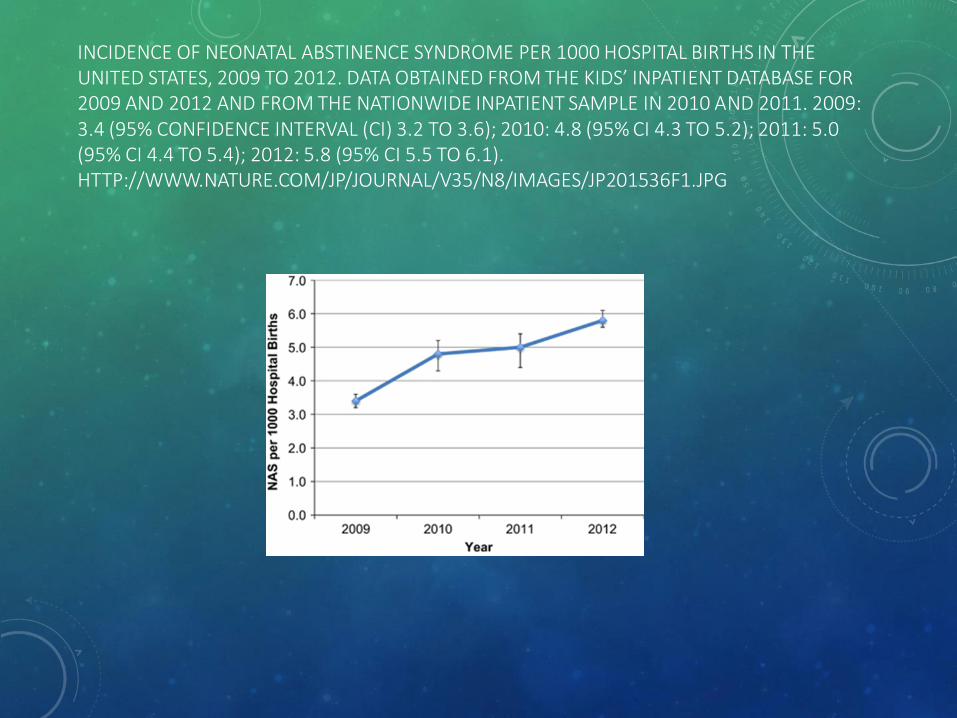
INCIDENCE OF NEONATAL ABSTINENCE SYNDROME PER 1000 HOSPITAL BIRTHS IN THE UNITED STATES, 2009 TO 2012. DATA OBTAINED FROM THE KIDS’ INPATIENT DATABASE FOR 2009 AND 2012 AND FROM THE NATIONWIDE INPATIENT SAMPLE IN 2010 AND 2011. 2009: 3.4 (95% CONFIDENCE INTERVAL (CI) 3.2 TO 3.6); 2010: 4.8 (95% CI 4.3 TO 5.2); 2011: 5.0 (95% CI 4.4 TO 5.4); 2012: 5.8 (95% CI 5.5 TO 6.1). HTTP://WWW.NATURE.COM/JP/JOURNAL/V35/N8/IMAGES/JP201536F1.JPG
WHAT DOES THIS MEAN IN 2009 VS 2012(PATRICK ET AL)?
• 2009:
• 13,539 newborns with NAS
• (95% CI 12,441-14,635)
• OR….. 1 infant born every hour in US with signs of Neonatal Abstinence
• 2012:
• 21,732 newborns with NAS
• (95% CI 20,052-23,413)
• OR….. 1 infant born every 25 minutes in US with signs of Neonatal Abstinence
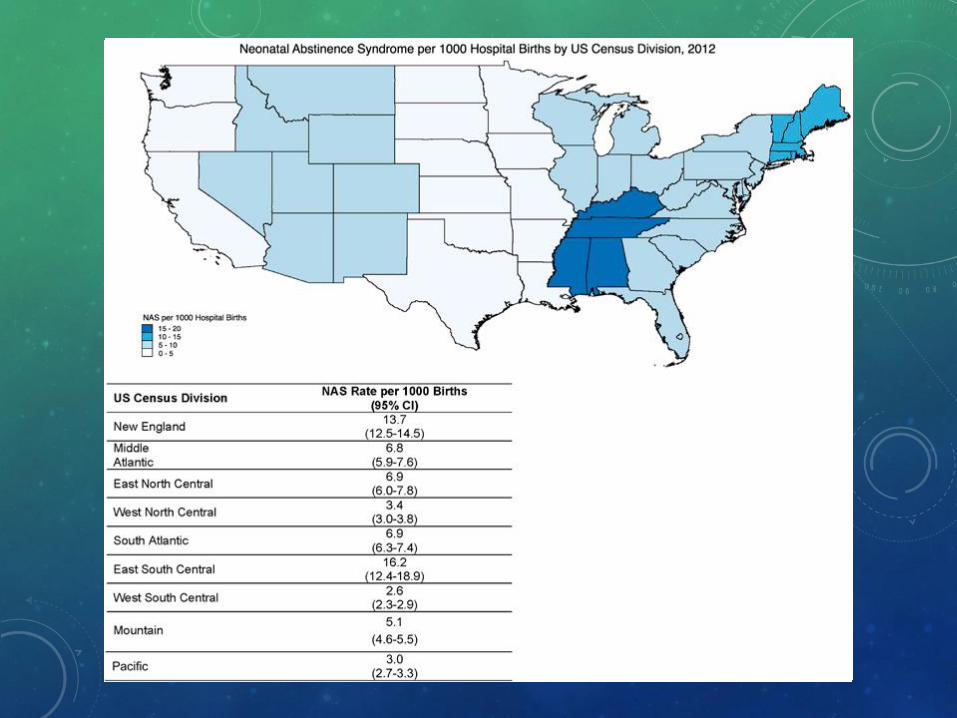
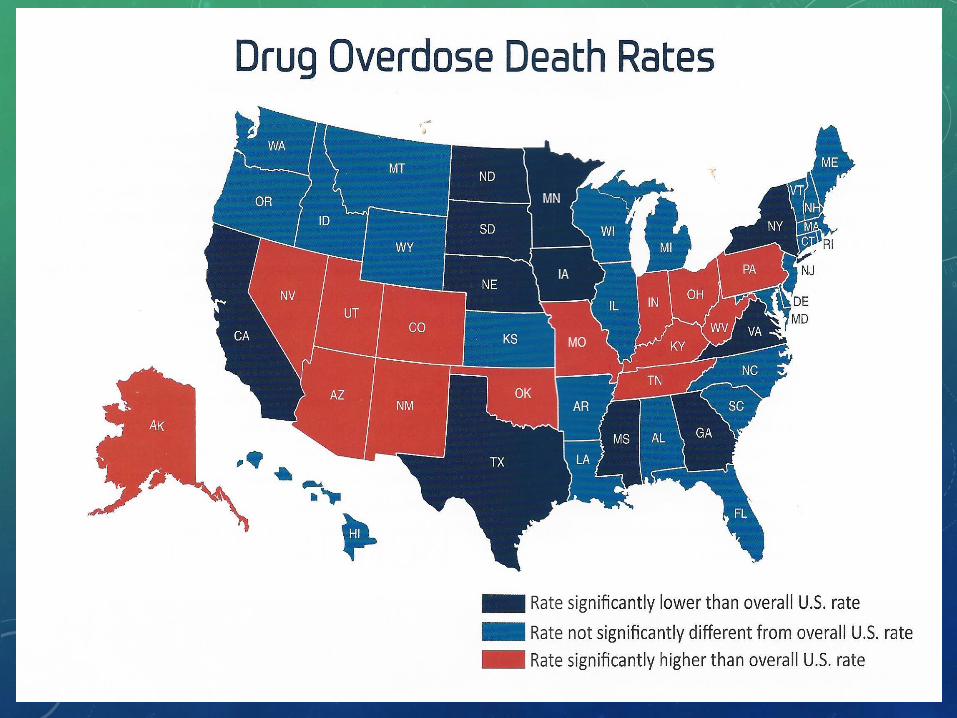
NAS/1000 Live Births US Census Bureau geographic division 2012.
Division 1 (New England): Maine, New Hampshire, Vermont, Massachusetts, Rhode Island and Connecticut. ---13.7Division 2 (mid-Atlantic): New York, Pennsylvania and New Jersey. ---6.8Division 3 (East North Central): Wisconsin, Michigan, Illinois, Indiana and Ohio. ---6.9Division 4 (West North Central): Missouri, North Dakota, South Dakota, Nebraska, Kansas, Minnesota and Iowa. ---3.4 Division 5 (South Atlantic): Delaware, Maryland, Dist of Columbia, Virginia, West Virginia, North Carolina, South Carolina, Georgia and Florida. ---6.9
Division 6 (East South Central): Kentucky, Tennessee, Mississippi and Alabama. ---16.2Division 7 (West South Central): Oklahoma, Texas, Arkansas and Louisiana. Division 8 (Mountain): Idaho, Montana, Wyoming, Nevada, Utah, Colorado, Arizona and New Mexico. ---5.1Division 9 (Pacific): Alaska, Washington, Oregon, California and Hawaii. ---3
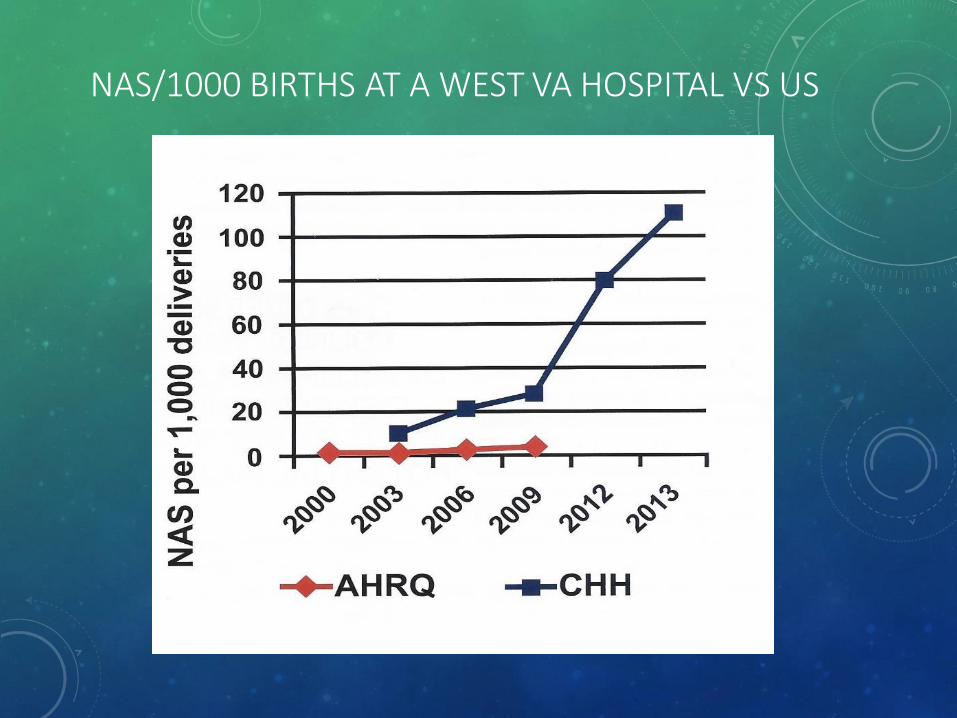
NAS/1000 BIRTHS AT A WEST VA HOSPITAL VS US
FETAL/NEONATAL EFFECTSBABIES WITH NAS HAVE HIGHER RATES OF MEDICAL
COMPLICATIONS LONGER HOSPITAL STAYS
• Prematurity
• Low Birthweight
• Respiratory Complications
• Transient Tachypnea (TTN), Meconium Aspiration, RDS
• Feeding Difficulty
• Seizures
• Jaundice
• Sepsis
COST OF CARE: 2009-2012
• Aggregate Hospital Charges –
• INCREASE from $732 Million $1.5 Billion
• 2012 NAS Cases - 81% attributed to state Medicaid Programs
• 2012 NON-NAS Cases – 46% are Medicaid recipients
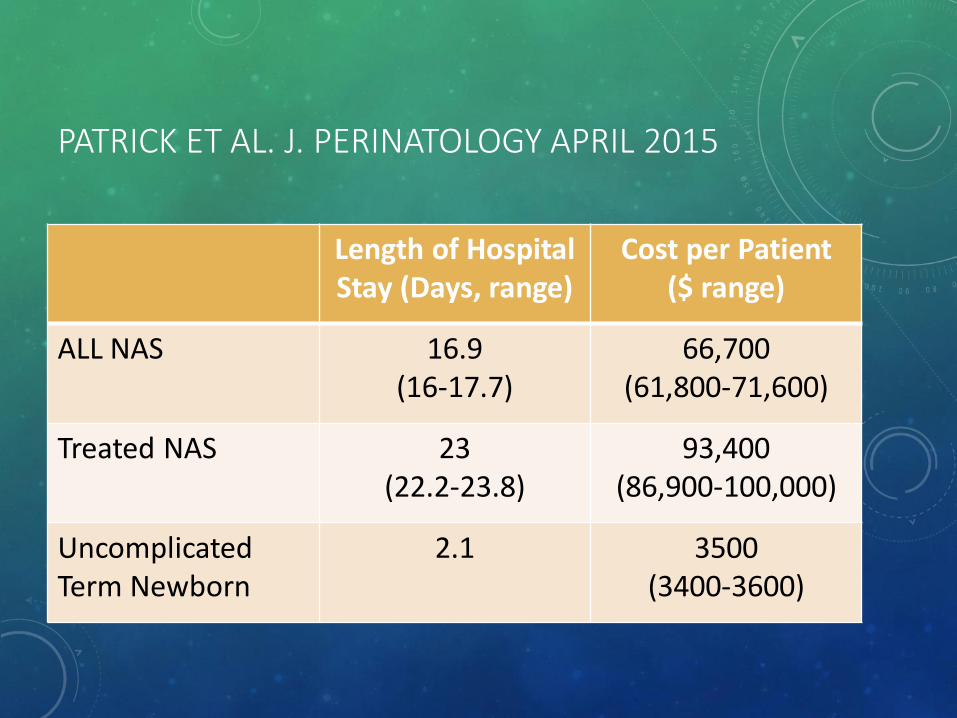
PATRICK ET AL. J. PERINATOLOGY APRIL 2015
Length of Hospital Stay (Days, range)
Cost per Patient ($ range)
ALL NAS 16.9 (16-17.7)
66,700 (61,800-71,600)
Treated NAS 23 (22.2-23.8)
93,400 (86,900-100,000)
Uncomplicated Term Newborn
2.1 3500 (3400-3600)
CONSISTENCY AND COLLABORATIVE WORK MATTER
• Improving Care for Neonatal Abstinence Syndrome. Patrick et al. (Vermont Oxford Network Collaborative Project). Pediatrics (137): May 2016:e20153835.
• 199 participating centers – data collected 2012-2014. Guidelines for care developed and modified.
• NAS focused guidelines increased from 3.7 to 5.1 (6 possible measures) in the centers
• NAS Rx length decreased from 16 days to 15 days
• Infants discharged on medication decreased from 39.7% to 26.5%
• Length of Hospital Stay decreased from 21 days to 19 days
• = savings of ~$170 million in hospital charges (2012 cost)
ALASKA EPIDEMIOLOGY BULLETIN – FEB 2016INCREASE NAS IN ALASKA 2001-2015
• Hospital Discharge Database (HDD) 2001-2012 NAS Diagnosis
• 0.8/1000 (2001) to 5.1/1000 (2012) Live Births
• Medicaid Claim Database 2004-2015
• 1/1000 (2005) to 6.4/1000 (2014) Live Births
• Geographic Variability – highest in ANC (3.6) and SE (3.4)/1000; lowest in SW (1.5) and Northern regions (0.9)/1000 Live Births
• Average Hospitalization Charge $88,869 vs. $12,731 for non NAS < 28 days
• Medicaid primary payor for 78% of HDD-identified infants with NAS
• Statewide NAS rate increased >5 fold in Alaska from 2001-2012
• Underestimates reality – only 67-83% of in state births occur in the hospital
PRENATAL SUBSTANCE ABUSE- SOCIAL DILEMNA
• Attachment disorders
• Vicious cycle of poor bonding, parental neglect, attachment disorders lead to high behavior in children and adolescents
• Altered state regulation, attention, and behavior affect learning
• Unmeasured LOSS to Society – Intellectual Potential, Income Potential, Life Long Effects for the Baby/Family
PRENATAL SUBSTANCE ABUSE- SOCIAL DILEMNA
• Multi-generational social challenges
• Increased incidence of child abuse
• Poor adult role models
• Prenatal effects on developing brain has long lasting effects that last a lifetime
• Dysfunctional/Unsafe home environment -potential exposure to toxic chemicals in home environment; poor parenting skills; vicious cycle
PERINATAL SUBSTANCE ABUSE- SEQUELAE
• Tobacco use can worsen the growth restriction.
• Concurrent exposure to alcohol increases pathologic effects on developing brain.
• Damaging effects on dopaminergic and serotonergic neurons (brain cells/pathways) potentially permanent.
• Selective structural cortical changes as well as dopamine transporter and receptor dependent neurotransmission.

PERINATAL SUBSTANCE ABUSE –POTENTIAL FOR INTERVENTION
• Plasticity in developing brain.
• Supportive environmental influence and positive role modeling can impact children’s outcome.
• Better understanding of longterm effects on learning and behavior to provide optimal intervention at home and school.
NEONATAL ABSTINENCE SYNDROME -POLICY PERSPECTIVE
• 2009 Subtance Abuse and Mental Health Services Administration Report –“Substance-Exposed Infants: State Responses to the Problem”
• Provided a 5-point intervention framework to organize prevention and intervention opportunities for opioid – dependent women and their children
• States attempting to develop Universal Screening Tools to Assess Risk
• Federal Legislation: November 2015 President Obama signed into Law
• Protecting our Infants Act – directs the Secretary of Health and Human Services to identify and make available recommendations for the Dx and Rx of NAS, evaluate and coordinate federal efforts to research and respond to NAS, and assist state health agencies with data collection efforts
KO ET AL. MMWR AUGUST 12, 2016. VOL 65:799-802
• Incidence of Neonatal Abstinence Syndrome – 28 States, 1999-2013
• NAS incidence increased 300% : 1.5 to 6 per 1000 live births
• In 2013, range 0.7/1000 (Hawaii) to 33.4/1000 (W. Va.) hospital births
• Source – State Inpatient Databases, Healthcare Cost and Utilization Project
• Passive surveillance of NAS utilizing public data to help states successfully target prevention and treatment measures.
• Some states (Florida, Georgia, Kentucky and Tennessee have made NAS a reportable condition to state health departments.
• “As part of the Protecting Our Infants Act of 2015 CDC provides technical assistance to states and American Indian tribes to improve NAS surveillance and support implementation of effective public health measures.”
LOCALLY….IN ALASKA
• Between 2008-2014 there were 175 infants treated as
inpatients on the Alaska Neonatology Service between ARH
and PAMC – Alaska Neonatology Database.
• The length of stay in the Neonatal Intensive Care Unit,
related to NAS, was between 3-86 days when corrected for
prematurity.
• Average length of stay was approximately 30 days- After
correction for prematurity.
STATEWIDE COLLABORATIVE WORK WITH VERMONT OXFORD NETWORK NEONATAL ABSTINENCE SYNDROME QUALITY IMPROVEMENT PROJECT -2015
• PAMC led Statewide Collaborative Quality Improvement Initiative involving multiple facilities statewide in Anchorage and Fairbanks
• Each facility participated in webinar based learning modules
• Certificate of Excellence when >90% of staff completed all learning modules
• PAMC, FMH, ARH have all developed guidelines for management of NAS affected babies
• Treatment guidelines include non-pharmacologic and pharmacologic measures
• Pharmacologic guidelines driven by NAS scores, protocol driven to optimize concensus approach
THEN eonatal AbstinenceE valuationS upportT reatment
ALASKA REGIONAL HOSPITAL – Unit within the NICU
The NEST has developed best practice based protocols following an extensive period of research, study, and academic introspection of many past abstinence experiences. Based on the following principles:
Parents should be parenting their own children and the wellness of the family (in it’s entirety) is absolutely critical to the future of these patients.
• The unit is designed so that mother and infant may stay together 24/7• The family will be the primary caretakers of their child.• The NEST provides aggressive and specialized social support services available
with a NEST based Clinical Social Worker.
ARH LOS = 15 days as of 2016 (down from 30 days in 2014)
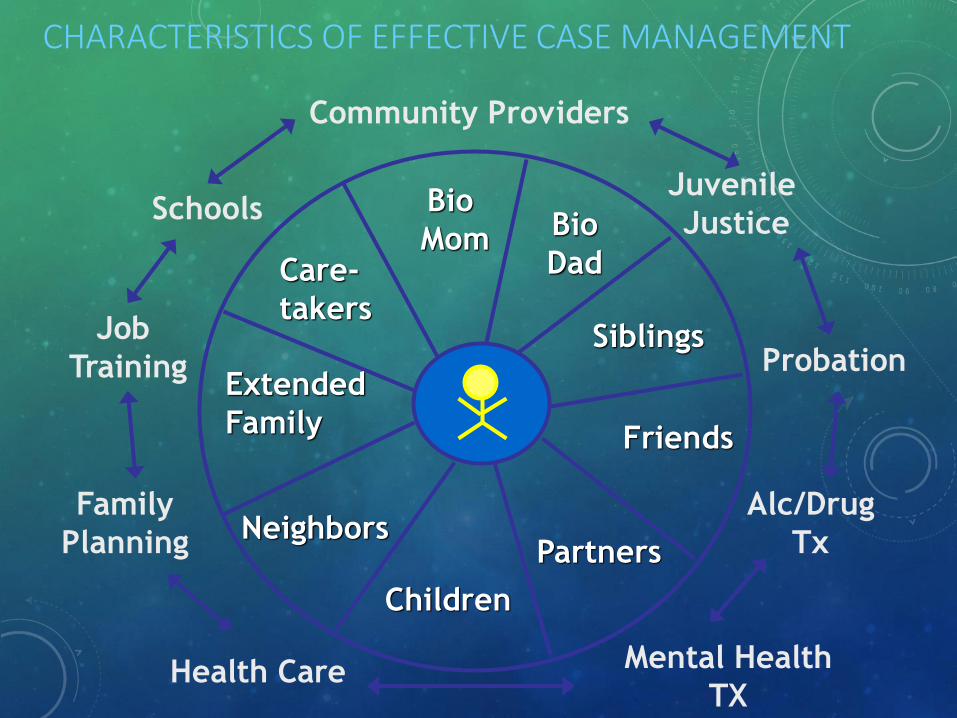
CHARACTERISTICS OF EFFECTIVE CASE MANAGEMENT
Community Providers
Juvenile
Justice
Probation
Alc/Drug
Tx
Mental Health
TXHealth Care
Family
Planning
Job
Training
Schools Bio
Mom Bio
Dad
Siblings
Friends
Partners
Children
Neighbors
Extended
Family
Care-
takers
SO….AS YOU CAN SEE……OUR WORK IS JUST BEGINNING ----
SUBSTANCE ABUSE IS A SOCIETAL PROBLEM THAT POTENTIALLY AFFECTS
ALL OF US.
THANK YOU!
REFERENCES - 1
• 1. Increasing Prevalence of Neonatal Withdrawal Syndrome: Population Study of Maternal Factors and Child Protection Involvement. O’Donnell, et. al. Pediatrics 2009 (123): e615-e621.
• 2. The Opioid Exposed Newborn: Assessment and Pharmacologic Management. Jansson, et.al. J Opioid Management 2009 (5): 47-55.
• 3. Neonatal Abstinence Syndrome after Methadone or BupernorphineExposure. Jones, et al. N. Engl. J. Med 2010 (363): 2320-2331.
• 4. Neonatal Abstinence Syndrome and Associated Health Care Expenditures United States, 2000-2009. Patrick, et.al. JAMA 2012 (307): 1934-1940.
• 5. Neonatal Drug Withdrawal Clinical Report – Policy Statement from AAP. The Committee on Drugs and The Committee on Fetus and Newborn. Pediatrics 2012 (129): e541-e560.
REFERENCES - 2
• 6. Predicting Treatment for Neonatal Abstinence Syndrome in Infants Born to Women Maintained on Opioid Agonist Medication. Kaltenbach et.al. Addiction 2012 (107): 45-52.
• 7. Neonatal Abstinence Syndrome (State of the Art Review Article). Prabhakar. Pediatrics 2014 (134):e547-561.
• 8. The American College of Obstetricians and Gynecologists – Committee on Obstetric Practice. Marijuana Use During Pregnancy and Lactation. ObstetGynecol 2015 (126):234-238.
• 9. Editorial – Neonatal Abstinence Syndrome: A Policy Perspective. Chasnoff and Gardner. J Perinatology 2015 (35): 539-541.
• 10. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States, 2009-2012. Patrick et.al. J Perinatology 2015 (35): 650-655.
REFERENCES - 3
• 11. Protecting our Infants Act – Federal Law Signed by President Obama Nov 2015.
• 12. Prescription Opioid Epidemic and Infant Outcomes. Patrick et.al. Pediatrics (135): 842-850.
• 13. Increasing Incidence of the Neonatal Abstinence Syndrome in US Neonatal ICUs. Tolia et.al. N Engl J med 2015 (372): 2118-2126.
• 14. Neonatal Abstinence Syndrome. Jansson, Lauren M. UpToDateReview Jan 2016.
• 15. Increase in Neonatal Abstinence Syndrome, Alaska, 2001-2015. Young, Margaret. State of Alaska Epidemiology Bulletin Feb. 2016.
• 16. Improving Care for Neonatal Abstinence Syndrome. Patrick et. al. Pediatrics 2016 (137): e20153835.
• 17. Incidence of Neonatal Abstinence Syndrome - 28 States, 1999-2013. Ko et al. MMWR Aug 2016 (65): 799-802.
UNITED STATES DRUG TESTING LABORATORIES
1700 SOUTH MOUNT PROSPECT ROAD
DES PLAINES, ILLINOIS 60018
Phone: (847) 375-0770 / Fax: (847) 375-0775
Email: [email protected]
Visit us @ http:// www.usdtl.com
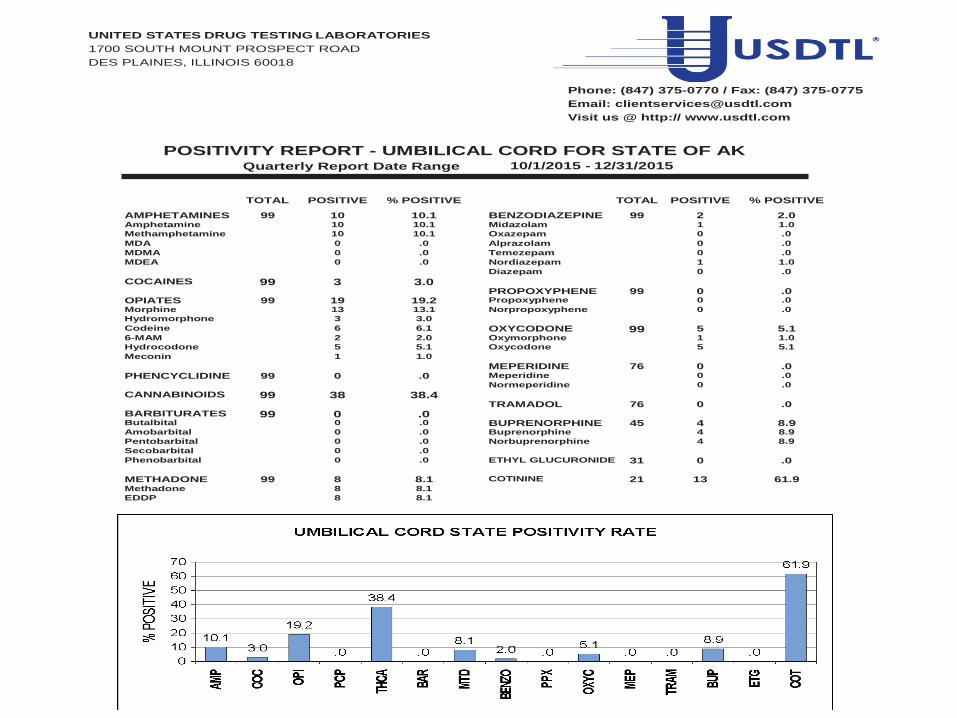
POSITIVITY REPORT - UMBILICAL CORD FOR STATE OF AK Quarterly Report Date Range 10/1/2015 - 12/31/2015
AMPHETAMINES
TOTAL
99
POSITIVE
10
% POSITIVE
10.1
BENZODIAZEPINE
TOTAL
99
POSITIVE
2
% POSITIVE
2.0 Amphetamine 10 10.1 Midazolam 1 1.0
Methamphetamine 10 10.1 Oxazepam 0 .0
MDA 0 .0 Alprazolam 0 .0
MDMA 0 .0 Temezepam 0 .0
MDEA 0 .0 Nordiazepam 1 1.0
Diazepam 0 .0
COCAINES 99 3 3.0 PROPOXYPHENE 99 0 .0 OPIATES 99 19 19.2 Propoxyphene 0 .0
Morphine 13 13.1 Norpropoxyphene 0 .0
Hydromorphone 3 3.0 Codeine 6 6.1 OXYCODONE 99 5 5.1 6-MAM 2 2.0 Oxymorphone 1 1.0
Hydrocodone 5 5.1 Oxycodone 5 5.1
Meconin 1 1.0 MEPERIDINE 76 0 .0 PHENCYCLIDINE 99 0 .0 Meperidine 0 .0
Normeperidine 0 .0
CANNABINOIDS 99 38 38.4 TRAMADOL 76 0 .0 BARBITURATES 99 0 .0 Butalbital 0 .0 BUPRENORPHINE 45 4 8.9 Amobarbital 0 .0 Buprenorphine 4 8.9
Pentobarbital 0 .0 Norbuprenorphine 4 8.9
Secobarbital 0 .0 Phenobarbital 0 .0 ETHYL GLUCURONIDE 31 0 .0
METHADONE 99 8 8.1 COTININE 21 13 61.9 Methadone 8 8.1 EDDP 8 8.1
WITHDRAWAL FROM ? – TIMING OF PRESENTATION
• Alcohol – 3 to 12 hrs old
• Narcotics – 24 to 96 hrs old
• Methadone – most commonly seen medication in the withdrawing infant; symptoms typically by 48-72 hrs of age but sometimes as late as 3 wks due to long half life
• Nicotine – mild; by 24-48 hrs of age
• Buprenorphine (opioid substitue) – by 72 hrs