the cytokines and the b-cell...
TRANSCRIPT
on Maximizing Therapeutic Outcomes
THE CYTOKINES AND THE B-CELL MALIGNANCIES
Thursday, May 4, 2006 Luncheon Program 11:30 am – 1:00 pmBoston Convention & Exhibition CenterGrand Ballroom – WestBallroom LevelBoston, Massachusetts A Division of the Oncology Nursing Society
Join the faculty for a clinical chat at the ONS Booth
1:30 pm - 2:30 pm, Booth #551

Check out CE Central, where you’ll
find detailed information on all the
top-notch educational programming
available through ONS.
Look for the CE Central Catalog
in the mail, or go online for an
updated list of program offerings.
www.ons.org/cecentral
Make it a Win-Win for YOU and YOUR Patients…
• • • • Various Learning Formats
• • • • Wide Range of Topics
• • • • Up-to-Date Information on
Therapies and Treatment Options
• • • • Patient Education
And Much, Much More!
For complete details on all ONS
and OES programs, visit us online at
www.ons.org/cecentral
or call ONS Customer Service at 866-257-4ONS or
412-859-6100.
with evidence-based education
programs from CE CENTRAL!
THE WINNING COMBINATION: ONS EDUCATION + OES = The NEW Center for Education!

A Division of the Oncology Nursing Society
on Maximizing Therapeutic Outcomes
THE CYTOKINES AND THE B-CELL MALIGNANCIES
Table of Contents Program Information ......................................................4
Target Audience ...........................................................4
Program Objectives ......................................................4
Faculty .......................................................................4
Program Schedule ........................................................5
Continuing Education Information ....................................5
Disclosure of Significant Relationships ...............................5
Faculty Biographies .......................................................6
Slides .........................................................................7
References ................................................................55
Glossary ...................................................................56
Commonly Used Medications .......................................57
Hematopoietic Cascade Tool ........................................59
MOAB Lymphoma Tool ................................................60
CE Evaluation Form ....................................................61
DisclaimersThis educational program has been developed and produced by OES, a division of the Oncology Nursing Society.
The opinions expressed in this presentation are those of the participating faculty. It should not be inferred or assumed that they are expressing the views of ONS or of any of the manufacturers of pharmaceuticals mentioned in the program.
Copyright © 2006 ONS. All rights reserved. No part of this program or publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without written permission from the copyright holder.
OES has been assigned meeting space to provide an educational program funded by Berlex Oncology Inc., via an educational grant, during the Oncology Nursing Society’s (ONS) 31st Annual Congress. The Oncology Nursing Society’s assignment of meeting space does not imply product endorsement, nor does the Oncology Nursing Society assume any responsibility for the educational content.
Disclosure of Off-Label UsesSome of the information contained in this program may be inconsistent with product labeling. Therefore, the official package inserts for all products mentioned should be consulted for complete prescribing information and a complete listing of indications, contraindications, warnings, precautions, adverse reactions, and dosage and administration guidelines. Health care providers should exercise their own independent medical judgment in making treatment decisions.
THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
3
Program InformationTreatments for B-cell malignancies have shown great promise in overall survival and in improving quality of life. This case study-based program will examine the latest data in treating follicular lymphoma, large B-cell lymphoma, and chronic lymphocytic leukemia, including chemotherapy and targeted agents. Gain insight into the critical role that antibody-dependent cellular cytotoxicity plays in targeting malignant B-cells and what this means for your practice and your patients. Review how you have treated patients with B-cell malignancies and learn how others are managing similar cases.
Target AudienceThis program is designed for oncology nurses with an interest in learning about novel approaches to treating B-cell malignancies.
Program ObjectivesAt the end of this symposium, the participant will be able to:
1. Discuss the role of the CD-20 antigen in B-cell malignancies.2. Discuss the role of antibody-dependent cell-mediated cytotoxicity (ADCC) in the
treatment of B-cell malignancies.3. Summarize treatment options and their limitation for follicular lymphoma (FL), large
B-cell lymphoma, and chronic lymphocytic leukemia (CLL).4. Summarize data discussing mechanism to delay disease relapse in FL, large B-cell
lymphoma, and CLL.5. Devise a comprehensive plan of care for the patient receiving therapy for FL, large
B-cell lymphoma or CLL, including minimizing adverse events, managing systems, and educating patients.
FacultyProgram ChairMary Browning, RN, OCN®, CCRPSenior Research NurseDepartment of LeukemiaMD Anderson Cancer CenterHouston, Texas
ModeratorElaine DeMeyer, RN, MSN, AOCN®
President and CEO of Creative Cancer ConceptsClinical Instructor, Baylor School of NursingRockwall, Texas
FacultyLisa H. Downs, RN, MSN, CRNP-BCCoordinator, Lymphoma ProgramAbramson Cancer Center at the Hospital of the University of PennsylvaniaPhiladelphia, Pennsylvania
4 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

Continuing Education InformationParticipants will receive 1.8 continuing nursing education credits at the successful completion of the program.
ONS is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s (ANCC) Commission on Accreditation.
Accreditation as an ANCC provider refers only to its continuing-education activities and does not imply ANCC Commission on Accreditation endorsement of any commercial products.
ONS is approved as a provider of continuing education by the California Board of Registered Nursing, Provider #2850.
The contact hours earned from this educational opportunity qualify for initial oncology nursing certification and renewal via ONC-PRO. Visit www.oncc.org for complete details on oncology nursing certification.
This session includes approximately 30 minutes of pharmacology content.
Disclosure of significant relationshipsMary Browning, RN, OCN®, CCRP, has disclosed the following relationship: member of the Berlex Oncology, Inc. Advisory Board.
Elaine DeMeyer, RN, MSN, AOCN®, has disclosed the following relationships: consultant for Berlex Oncology,Inc. and OSI Pharmaceuticals and is on the speakers bureaus for Abraxis Oncology, Amgen, Astra Zeneca, Berlex Oncology, Inc., Merck, MGI Pharma, and Ortho Biotech. She has also received research support from Amgen/ONS research award.
Lisa H. Downs, RN, MSN, CRNP-BC, has disclosed the following relationship: member of the Berlex Oncology, Inc. Advisory Board and a speaker for OES programs supported by Genentech BioOncology.
5
Program Schedule11:30 am Welcome and Program Introduction Mary Browning
11:45 am Case Study I: Follicular lymphoma All Faculty
Case Study II: Large B-cell lymphoma All Faculty
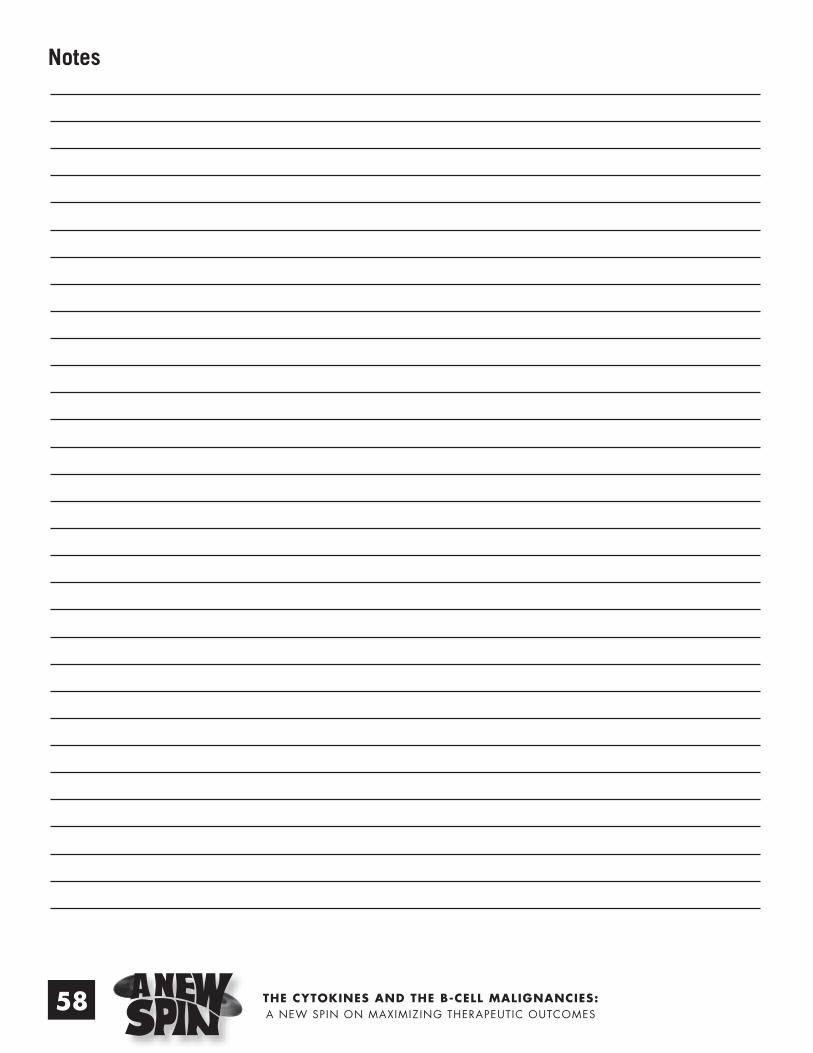
Case Study III: Chronic lymphocytic leukemia All Faculty
12:45 pm Pulling the Cases Together Faculty Panel
Question & Answer Session
1:00 pm Program Concludes
THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
Faculty Biographies
Mary Browning, RN, OCN®, CCRP has been a nurse at MD Anderson Cancer Center in Houston, Texas since 1994 and she has been with the Leukemia Department since 1995. She has focused on the treatment of patients with chronic lymphocytic leukemia by participating in clinical trials since 1998. Ms. Browning assisted with the pivotal trial for alemtuzumab. She is a graduate of Galveston College and Texas Women’s University. Ms. Browning has also co-authored a publication on monoclonal antibodies for a peer-reviewed journal and has written an article titled: Treatment of chronic lymphocytic leukemia with alemtuzumab: a review for nurses in the Oncology Nursing Forum. She is an active member of the Society of Clinical Research Professionals and the Oncology Nursing Society.
Elaine DeMeyer, RN, MSN, AOCN®, has been an oncology nurse for more than eighteen years. She received her first bachelor degree in physiology with a minor in chemistry (1985), from Southern Illinois University in Carbondale. Both her bachelor of nursing (1986) and Master of Science in nursing (1990) were received from St. Louis University. Ms. DeMeyer’s expertise in oncology care was gained through her experience at Baylor University Medical Center in Dallas, Texas, where she practiced as clinical nurse specialist. She also has a clinical faculty appointment at the Louise Harrington School of Nursing at Baylor University. Ms. DeMeyer is an advanced practice oncology nurse (AOCN).
Ms. DeMeyer is the recipient of the Josh Gottheil Bone Marrow Transplant Career Development Award for her excellence in clinical practice. She has also received two mentorship/fellowship awards from ONS and the Clinical Journal of Oncology Nursing. Ms. DeMeyer has published numerous chapters, monographs, and clinical/research articles in peer review journals. She has given more than 100 national lectures on the immune system, novel cancer therapies, and symptom management. Ms. DeMeyer has served as an oncology consultant to numerous teaching hospitals and pharmaceutical/biotech companies. She has worked on four immunology-based monographs that were published through OES, a division of the Oncology Nursing Society.
Lisa H. Downs, RN, MSN, CRNP-BC, is the coordinator of the Lymphoma Program at the University of Pennsylvania Cancer Center. After graduating from Thomas Jefferson University College of Allied Health Professionals in 1991, she accepted a position on the inpatient oncology unit at Jefferson Hospital. She worked on both the inpatient medical oncology unit and the outpatient infusion center. She then graduated from Thomas Jefferson University with a Master’s of Nursing in the family nurse practitioner program in 1998. She took a position shortly after graduation as a nurse practitioner in the Abramson Cancer Center of the University of Pennsylvania in the bone marrow transplant program. Her work since has been in a collaborative practice with Dr. Stephen Schuster, MD. They strive to develop new therapies for lymphomas with a focus on biologic therapies. Over the past several years she has done many presentations on lymphoma and its various treatment modalities. She has educated patients and families as well as health care providers. She has participated in several publications that include case studies, novel treatments of lymphoma, investigations into PET scanning for lymphoma and a chapter for a textbook. Together with Dr. Schuster, she has participated in many clinical trials that focus on novel therapies as well as investigate improving present therapies.
6 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES 7

8 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

9THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

10 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

11THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

12 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

13THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

14 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

15THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

16 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

17THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

18 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

19THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
20 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

21THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

22 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

23THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

24 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

25THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
26 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

27THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

28 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

29THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

30 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

31THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

32 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
Slide not printed due to permissions

33THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

34 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

35THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
36 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

37THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
38 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

39THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

40 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

41THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
42 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

43THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
44 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

45THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

46 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

47THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

48 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
49THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

5150 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

5150 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

52 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

53THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

54 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

ReferencesAlizadeh, A.A., Eisen, M.B., Davis, R.E., Ma, C., Lossos, I.S., Rosenwald, A., et al. (2000). Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature, 403, 503–511.American Cancer Society. (2006). Cancer facts and figures 2006. Atlanta, GA: Author.
Armitage, J.O., & Weisenburger, D.D. (1998). New approach to classifying non-Hodgkin’s lymphomas: Clinical features of the major histologic subtypes. Non-Hodgkin’s Lymphoma Classification Project. Journal of Clinical Oncology, 16, 2780–2795.
Berlex. (2002). Leukine® (sargramostim, GM-CSF) [Prescribing Information]. Richmond, CA: Author.
Byrd, J.C. (1998). Chronic lymphatic leukemia. Seminars in Oncology, 25, 65–74.
Byrd, J.C., Smith, L., Hackbarth, M.L., Flinn, I.W., Young, D., Proffitt, J.H., et al. (2003). Interphase cytogenetic abnormalities in chronic lymphocytic leukemia may predict response to rituximab. Cancer Research, 63, 36–38.
Cheson, B.D., Bennett, J.M., Grever, M., Kay, N., Keating, M.J., O’Brien, S., et al. (1996). National Cancer Institute-sponsored working group guidelines for chronic lymphocytic leukemia: Revised guidelines for diagnosis and treatment. Blood, 87, 4990–4997.
Coiffier, B., Lepage, E., Brière, J., Herbrecht, R., Tilly, H., Bouabdallah, R., et al. (2002). CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. New England Journal of Medicine, 346, 235–242.
Dighiero G. (2002). Is chronic leukemia one disease? Haematologica, 87, 1233–1241.
Dighiero, G., Maloum, K., Desablens, B., Cazin, B., Navarro, M., Leblay, R., et al. (1998). Chlorambucil in indolent chronic lymphocytic leukemia. New England Journal of Medicine, 338, 1506–1514.
Dohner, H., Fischer, K., Bentz, M., Hansen, K., Benner, A., Cabot, G., et al. (1995). p53 gene deletion predicts for poor survival and non-response to therapy with purine analogs in chronic B-cell leukemias. Blood, 85, 1580–1589
El Rouby, S., Thomas, A., Costin, D., Rosenberg, C.R., Potmesil, M., Silber, R., et al. (1993). p53 gene mutation in B-cell chronic lymphocytic leukemia is associated with drug resistance and is independent of MDR1/MDR3 gene expression. Blood, 82, 3452–3459.
Evans, L.S., & Hancock, B.W. (2003). Non-Hodgkin lymphoma. The Lancet, 362, 139–146.
Feugier, P., Van Hoof, A., Sebban, C., Solal-Celigny, P., Bouabdallah, R., Ferme, B., et al. (2005). Long-term results of the R-CHOP study in the treatment of elderly patients with diffuse large B-cell lymphoma: A study by the Groupe d’Etude des Lymphomes de l’Adulte. Journal of Clinical Oncology, 23, 4117–4126.
Fisher, R.I., Miller, T.P., & O’Connor, O.A. (2004). Diffuse aggressive lymphoma. Hematology, 222, 221–236.
Foon, K.A., & Fisher,R.I. (2001). Lymphomas. In E. Beutler, M.A. Lichtman, B.S. Coller, T.J. Kipps, & U. Seligsohn (Eds.), Williams Hematology (6th ed.) (pp. 1237–1262). New York: McGraw-Hill.
Genentech BioOncology. (2005). Rituxan® (rituximab) [Prescribing Information]. South San Francisco, CA: Author.
Hainsworth, J.D., Sharlene, L., Barton, J.H., Houston, G.A., Hermann, R.C., Bradof, F., et al. (2003). Single-agent rituximab as first-line and maintenance treatment for patients with chronic lymphocytic leukemia or small lymphocytic lymphoma. Journal of Clinical Oncology, 21, 1746–1751.
Haioun, C., Itti, E., Rahmouni, A., Brice, P., Rain, J-D., Belhadj, K., et al. (2005). [18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in aggressive lymphoma: An early prognostic tool for predicting patient outcome. Blood, 106, 1376–1381.
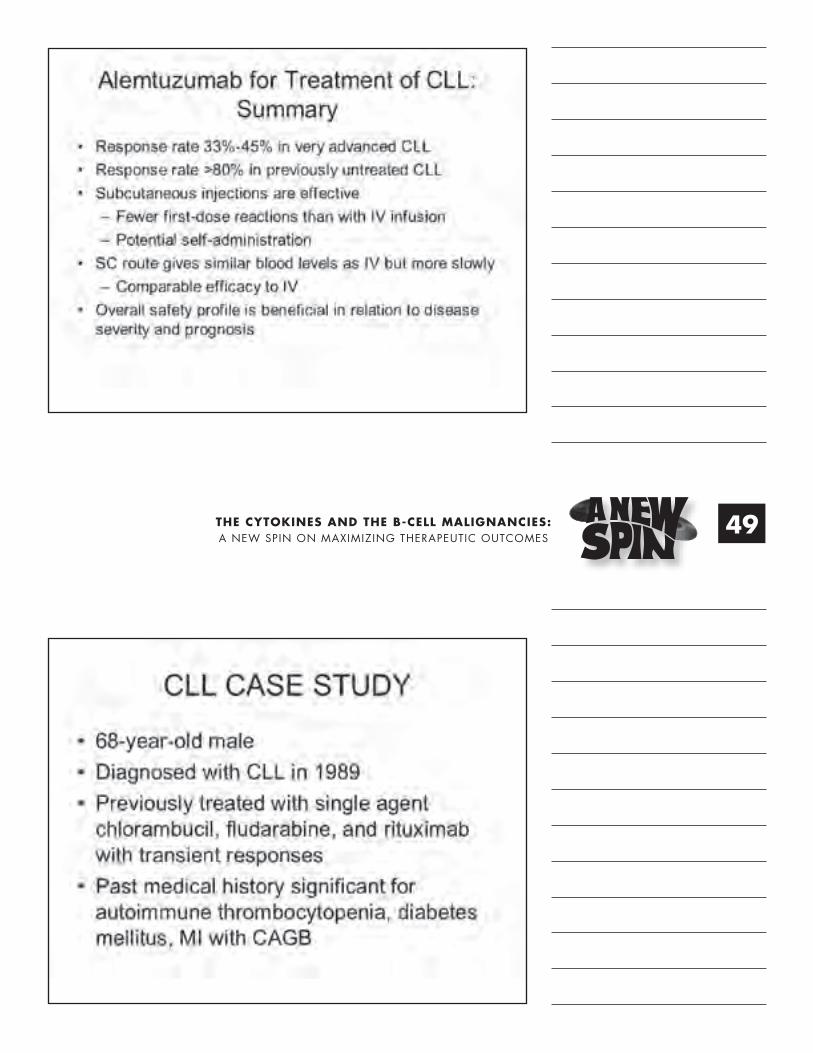
Huhn, D., von Schilling, C., Wilhelm, M., Ho, A.D., Hallek, M., Kuse, R., et al. (2001). Rituximab therapy of patients with B-cell chronic lymphocytic leukemia. Blood, 98, 1326–1331.
Itälä, M., Geisler, C.H., Kimby, E., Juvonen, E., Tjonnfjord, G., Karlsson, K., et al. (2002). Standard-dose anti-CD20 antibody rituximab has efficacy in chronic lymphocytic leukaemia: Results from a Nordic multicentre study. European Journal of Haematology, 69, 129–134.
Janeway, C., Travers, P., Walport, M., & Schlomchik, M. (2001). Immunobiology (5th ed.). New York: Garland Publishing.
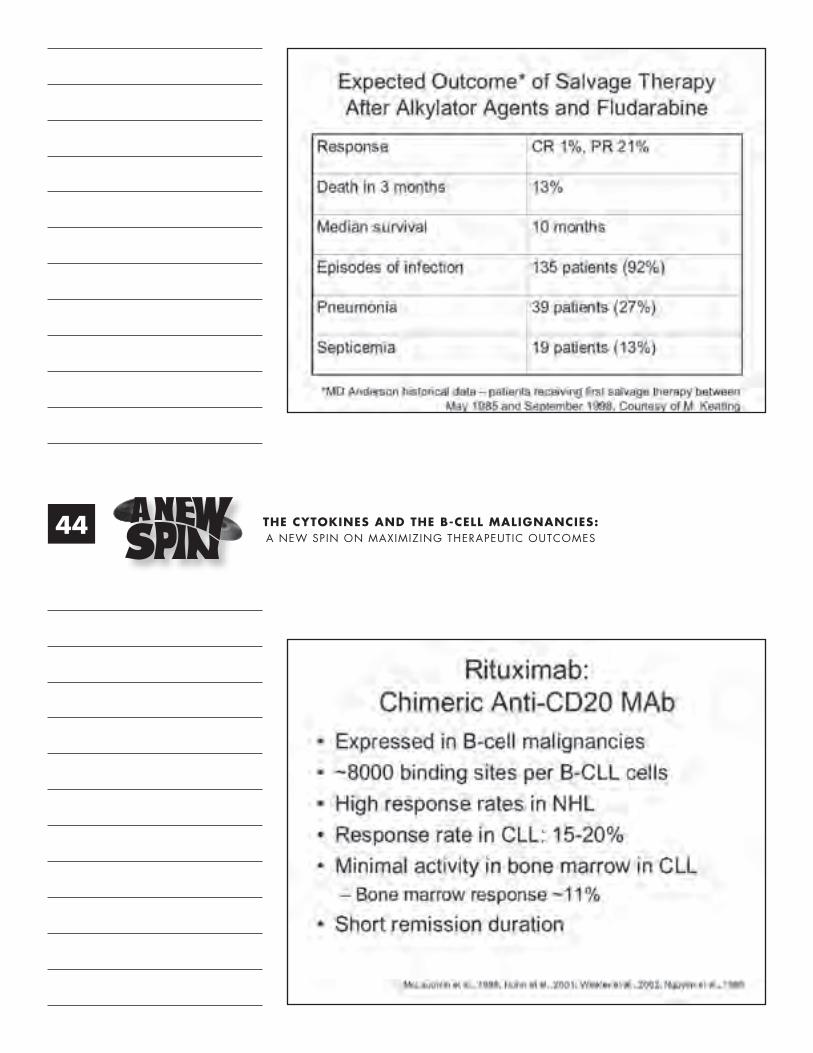
Keating, M.J., Flinn, I., Jain, V., Binet, J-L., Hillmen, P. Byrd, J., et al. (2002). Therapeutic role of alemtuzumab (Campath-1H) in patients who have failed fludarabine: Results of a large international study. Blood, 99, 3554–3561.
Leukemia and Lymphoma Society. (2004). Facts & statistics. Retrieved January 10, 2006, from www.leukemia-lymphome.org/all page?item id=12486.
Lozanski, G., Heerema, N.A., Flinn, I.W., Smith, L., Harbison, J., Webb, J., et al. (2004). Alemtuzumab is an effective therapy for chronic lymphocytic leukemia with p53 mutations and deletions. Blood, 103, 3278–3281.
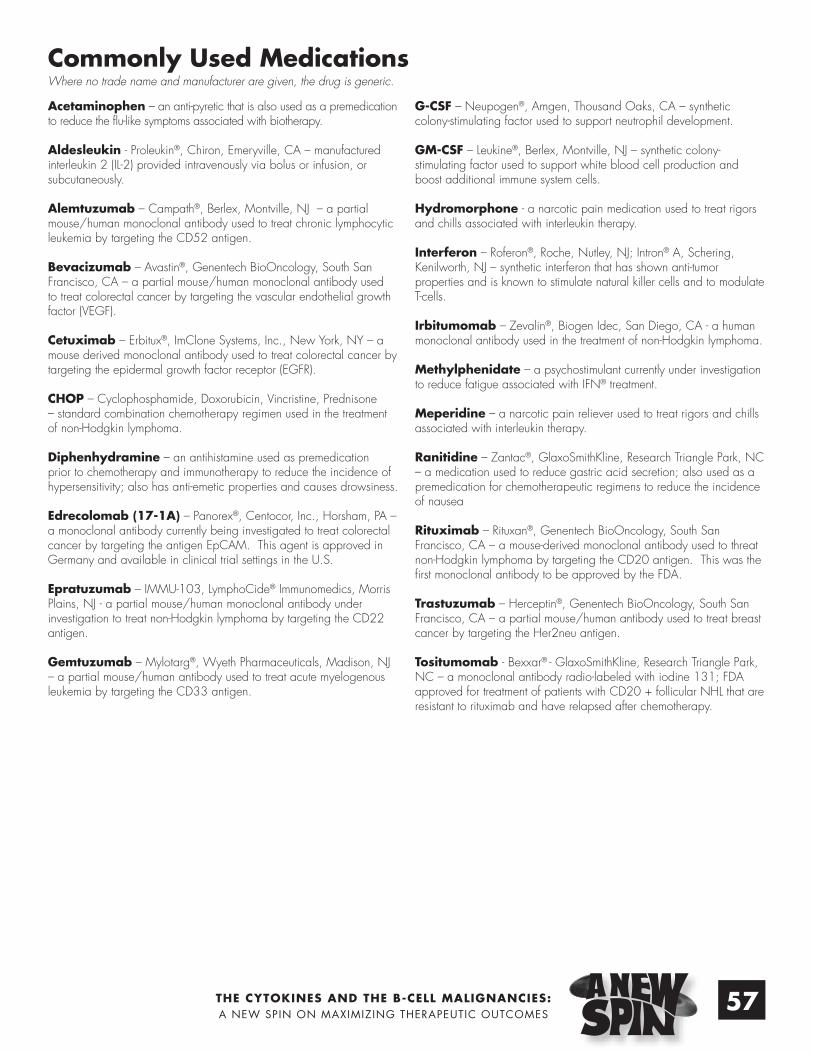
Lundin, J., Kimby, E., Björkholm, M., Broliden, P-A., Celsing, F., Hjalmar, V., et al. (2002). Phase II trial of subcutaneous anti-CD52 monoclonal antibody alemtuzumab (Campath-1H) as first-line treatment for patients with B-cell chronic lymphocytic leukemia (B-CLL). Blood, 100, 768–773.
McLaughlin, P., & Crowley-Norwick, P. (2006). Clinical study phase II: Randomized, open label, phase II trial comparing rituximab plus sargramostim to rituximab monotherapy for treatment of relapsed follicular B-cell lymphoma. Retrieved January 25, 2006, from http://www.clinicaltrials.gov/ct/show/NCT00308087.
McLaughlin, P., & Rodríguez, M. (2001). Rituximab in combination with GM-CSF (Leukine) for patients with recurrent indolent lymphoma [Abstract 2536]. Blood, 98, 605A.
McLaughlin, P., Grillo-Lopez, A.J., Link, B.K., Levy, R., Czuczman, M.S., Williams, M.E., et al. (1998). Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. Journal of Clinical Oncology, 16, 2825–2833.
National Cancer Institute. (2004). SEER cancer stat fact sheets. Retrieved April 26, 2006, from http://seer.cancer.gov/statfacts/html/all.html.
National Comprehensive Cancer Network®. (2005). NCCN clinical practice guidelines in oncology™. Non-Hodgkin’s lymphoma. V. 1.2005. Jenkintown, PA: Authors.
Nguyen, D.T., Amess, J.A., Doughty, H., Hendry, L., & Diamond, L.W., et al. (1999). IDEC-C2B8 anti-CD20 (rituximab) immunotherapy in patients with low-grade non-Hodgkin’s lymphoma and lymphoproliferative disorders: Evaluation of response on 48 patients. European Journal of Haematology, 62, 76–82.
Olivieri, A., Capelli, D., Lucesole, M., Montanari, M., Brunori, M., Gini, G., et al. (2001). A new strategy with CHOP-rituximab (RTX) plus GM-CSF in the salvage treatment of 33 patients with aggressive NHL [Abstract 4709]. Blood, 98, 245b.
A predictive model for aggressive non-Hodgkin’s lymphoma: The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. (1993). New England Journal of Medicine, 329, 987–994.
Rai, K.R., Sawitsky, A., Cronkite, E.P., Chanana, A.D., Levy, R.N., & Pasternack, B.S. (1975). Clinical staging of chronic lymphocytic leukemia. Blood, 46, 219–234.
Rassenti, L.Z., Huynh, L., Toy, T.L., Chen, L., Keating, M.J., Gribben, J.G., et al. (2004). ZAP-70 compared with immunoglobulin heavy-chain gene mutation status as a predictor of disease progression in chronic lymphocytic leukemia. New England Journal of Medicine, 26, 893–901.
Redaelli, A., Laskin, B.L., Stephens, J.M., Botteman, M.F., & Pashos, C.L. The clinical and epidemiological burden of chronic lymphocytic leukaemia. European Journal of Cancer Care,13, 279–287.
Rossmann, E.D., Lundin, J., Lenkei, R., Mellstedt, H., & Osterborg, A. (2001). Variability in B-cell antigen expression: Implications for the treatment of B-cell lymphomas and leukemias with monoclonal antibodies. Hematology Journal, 2, 300–306.
Rozman, C., & Montserrat, E. (1995). Current concepts: Chronic lymphocytic leukemia. New England Journal of Medicine, 333, 1052–1057.
Sehn, L.H., Chhanabhai, M., Fitzgerald, C., Gill, K., Hoskins, P., Klasa, R., et al. (2005). Revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma (DLBCL) treated with rituximab and CHOP (R-CHOP) [Abstract 492]. Blood, 106.
Shanafelt, T., & Call, T. (2004). Current approach to diagnosis and management of chronic lymphocytic leukemia. Mayo Clinic Proceedings, 79, 388–398.
Solal-Céligny, P., Roy, P., Colombat, P., White, J., Armitage, J.O., Arranz-Saez, R., et al. (2004). Follicular Lymphoma International Prognostic Index. Blood, 104, 1258–1265.
Sondel, P.M., & Hank, J.A. (2001). Antibody-directed, effector cell-mediated tumor destruction. Hematology/Oncology Clinics of North America, 15, 703–721.
Stilgenbauer, S., Winkler, D., Krober, A., Kienle, D., Halle, M., Hensel, M., et al. (2004). Subcutaneous Campath-1H (alemtuzumab) in fludarabine-refractory CLL: Interim analysis of the CLL2h study of the German CLL Study Group (GCLLSG) [Abstract 478]. Blood, 104.
Sturm, I., Bosanquet, A.G., Hermann, S., Guner, D., Dorken, B., & Daniel, P.T. (2003). Mutation of p53 and consecutive selective drug resistance in B-CLL occurs as a consequence of prior DNA-damaging chemotherapy. Cell Death and Differentiation, 10, 477–484.
Takvorian, T., & Dipiro, P.J. (2002). Staging of non-Hodgkin’s lymphoma. In Grossbard, M.L. (Ed.), Malignant lymphomas (pp. 67–83). Lewiston, NY: BC Decker.
Venugopal, P., Sivaraman, S., Huang, X.K., Nayini, J., Gregory, S.A., & Preisler, H.D. (2000). Effects of cytokines on CD20 antigen expression on tumor cells from patients with chronic lymphocytic leukemia. Leukemia Research, 24, 411–415.
Venugopal, P., Sivaraman, S., Huang, X.K., Nayini, J., Gregory, S.A., & Preisler, H.D. (2000). Effects of cytokines on CD20 antigen expression on tumor cells from patients with chronic lymphocytic leukemia. Leukemia Research, 24, 411–415.
Villamor, N., Montserrat, E., & Colomer, D. (2003). Mechanism of action and resistance to monoclonal antibody therapy. Seminars in Oncology, 30, 424–433.
Winkler, U., Jensen, M., Manzke, O., Schulz, H., Diehl, V., & Engert, A. (1999). Cytokine-release syndrome in patients with B-cell chronic lymphocytic leukemia and high lymphocyte counts after treatment with an anti-CD20 monoclonal antibody (rituximab, IDEC-C2B8). Blood, 94, 2217–2224.
THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
55

Antibody: Protein, also called immunoglobulin, secreted by the B-cell in response to an antigen.
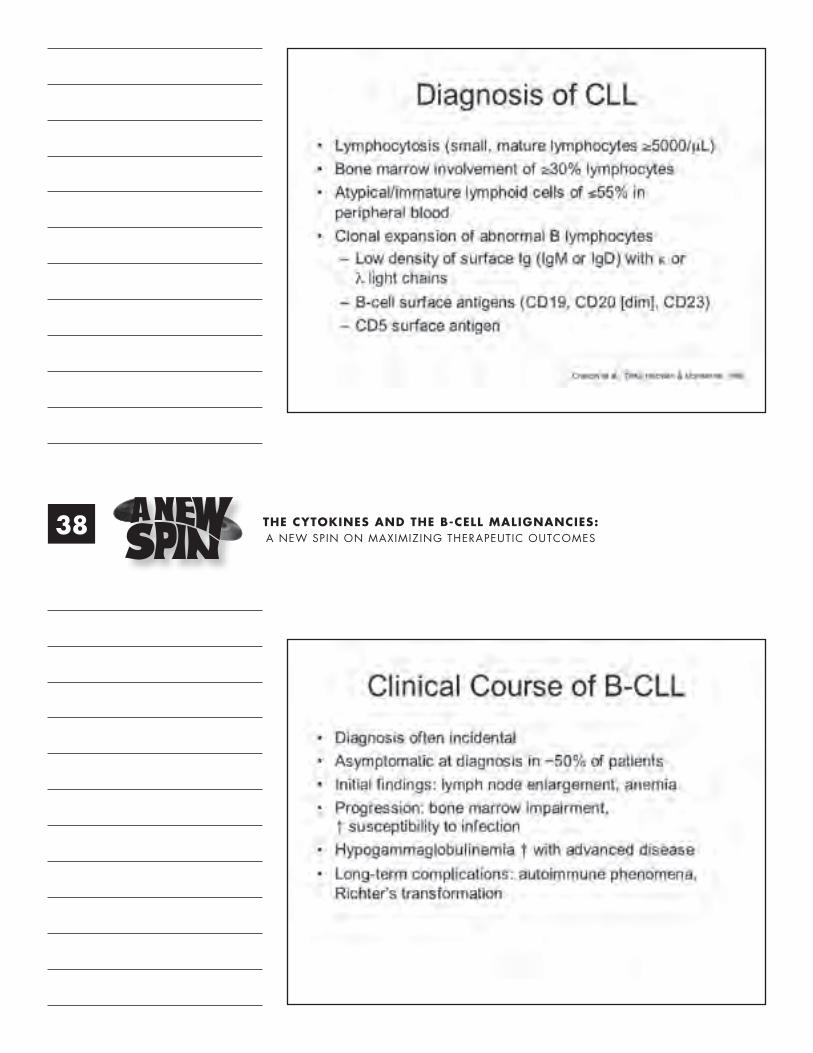
Antibody-Dependent Cellular Cytotoxicity (ADCC): The phenomenon by which antibody-coated pathogens are killed by immune system cells.
Antigen: Any substance (e.g., virus, bacterium, fungus, parasite, tumor cell, transplanted tissue, or cell) that is capable of initiating an immune response.
Antigen-Presenting Cells (APCs): Cells (e.g., macrophages,B-lymphocytes, dendritic cells, other body cells) that “present” antigens in a form that other immune cells recognize and then trigger an immune response.
Apoptosis: Programmed cell death, an active process controlled by cellular signaling.
B-Cells: One of three major classes of lymphocytes. Also calledB-lymphocytes, they transform or mature into plasma cells that secrete antibodies when exposed to a foreign antigen.
Biological Response Modifiers (BRMs): Agents used in biotherapy, classified into four main categories: interferons (INFs), interleukins (ILs), hematopoietic growth factors (HGFs), and monoclonal antibodies (MoAbs).
Biotherapy: Use of agents that affect biologic responses, which may have a direct or indirect effect on a tumor.
Complement: A series of proteins that are involved in mediation of immune responses. The complement cascade is triggered by antibody-antigen reaction.
Complement-Dependent Cytotoxicity (CDC): The activation of compliment proteins to bind and lyse cells coated with an antibody.
Crystallizable Fragment (Fc): Fragment of antibody recognized by effector cells of the immune system.
Cytokines: Regulatory proteins secreted by white blood cells and other cells that can have many effects on immune system cells (acting as intercellular messengers) and the modulation of inflammatory responses.
Dendritic Cells (DCs): Unique white blood cells that are potent antigen-presenting cells, acting as commanders of the immune system. The name originates from the appearance of the cell’s “finger-like” structures, or “tentacles,” that capture antigens to present informationto other immune system cells, especially T-cells.
Effector Cell: An active cell of the immune system responsible for destroying or controlling foreign antigens.
Fragment Binding Antigen (Fab): Section of the antibody molecule containing an antigen-binding site.
Granulocyte Colony-Stimulating Factor (G-CSF): A single lineage hematopoietic growth factor (cytokine) that stimulates the production of granulocytes, primarily neutrophils.
Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF): A multi-lineage hematopoietic growth factor (cytokine) that stimulates the production of: (a)granulocytes, primarily neutrophils, (b)monocytes, which migrate to the tissues to become macrophages, and (c) myeloid-related dendritic cells (DC1s)
Idiotype: The binding region unique to a tumor cell.
Immunotherapy: The use of agents that affect immune responses. The term is often used interchangeably with biotherapy.
Lysis: Rupture and destruction of a cell.
Macrophages: White blood cells that are scavengers; phagocytes, and APCs that are located throughout the body in a variety of tissues. Monocytes that leave the blood stream and enter the tissue are called macrophages.
Monoclonal Antibody: A laboratory-produced substance that locates and binds to specific proteins on cancer cells.
Monocyte: Phagocytic cells that circulate in the blood stream; they leave the bloodstream and migrate into tissues in order to evolve into macrophages.
Natural Killer Cells (NK): One of three major categories of lymphocytes that attack and destroy tumor and infected cells. Termed “natural” killer cells because they do not need to recognize a specific antigen to attack.
Neutrophils: The most common granulocyte and the first to respond to the source of infection. They engulf and kill antigens.
Phagocytosis: The process of ingesting and destroying a virus or other foreign matter by phagocytes.
Plasma Cells: Large antibody-producing cells that develop from B-cells.
Oncofetal: Products normally present during embryonic and fetal development but ones that cease to exist or exist in very low levels in adult tissue. They may be elevated in the presence of malignancy. Examples include CEA (carcinoembryonic antigen) and AFP (alpha-fetal protein).
Opsonization: Process of coating the surface of a pathogen by the antibody to enhance phagocytosis.
T-Cells: One of three major categories of lymphocytes, also called T-lymphocytes, that mediate a cellular immune response against foreignantigens.
Targeted Therapy: A cancer treatment that uses substances to identify and attack specific cancer cells without harming normal cells.
Glossary
56 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
Acetaminophen – an anti-pyretic that is also used as a premedication to reduce the flu-like symptoms associated with biotherapy.
Aldesleukin - Proleukin®, Chiron, Emeryville, CA – manufactured interleukin 2 (IL-2) provided intravenously via bolus or infusion, or subcutaneously.
Alemtuzumab – Campath®, Berlex, Montville, NJ – a partial mouse/human monoclonal antibody used to treat chronic lymphocytic leukemia by targeting the CD52 antigen.
Bevacizumab – Avastin®, Genentech BioOncology, South San Francisco, CA – a partial mouse/human monoclonal antibody used to treat colorectal cancer by targeting the vascular endothelial growth factor (VEGF).
Cetuximab – Erbitux®, ImClone Systems, Inc., New York, NY – a mouse derived monoclonal antibody used to treat colorectal cancer by targeting the epidermal growth factor receptor (EGFR).
CHOP – Cyclophosphamide, Doxorubicin, Vincristine, Prednisone – standard combination chemotherapy regimen used in the treatment of non-Hodgkin lymphoma.
Diphenhydramine – an antihistamine used as premedication prior to chemotherapy and immunotherapy to reduce the incidence of hypersensitivity; also has anti-emetic properties and causes drowsiness.
Edrecolomab (17-1A) – Panorex®, Centocor, Inc., Horsham, PA – a monoclonal antibody currently being investigated to treat colorectal cancer by targeting the antigen EpCAM. This agent is approved in Germany and available in clinical trial settings in the U.S.
Epratuzumab – IMMU-103, LymphoCide® Immunomedics, Morris Plains, NJ - a partial mouse/human monoclonal antibody under investigation to treat non-Hodgkin lymphoma by targeting the CD22 antigen.
Gemtuzumab – Mylotarg®, Wyeth Pharmaceuticals, Madison, NJ – a partial mouse/human antibody used to treat acute myelogenous leukemia by targeting the CD33 antigen.
G-CSF – Neupogen®, Amgen, Thousand Oaks, CA – synthetic colony-stimulating factor used to support neutrophil development.
GM-CSF – Leukine®, Berlex, Montville, NJ – synthetic colony-stimulating factor used to support white blood cell production and boost additional immune system cells.
Hydromorphone - a narcotic pain medication used to treat rigors and chills associated with interleukin therapy.
Interferon – Roferon®, Roche, Nutley, NJ; Intron® A, Schering, Kenilworth, NJ – synthetic interferon that has shown anti-tumor properties and is known to stimulate natural killer cells and to modulate T-cells.
Irbitumomab – Zevalin®, Biogen Idec, San Diego, CA - a human monoclonal antibody used in the treatment of non-Hodgkin lymphoma.
Methylphenidate – a psychostimulant currently under investigation to reduce fatigue associated with IFN® treatment.
Meperidine – a narcotic pain reliever used to treat rigors and chills associated with interleukin therapy.
Ranitidine – Zantac®, GlaxoSmithKline, Research Triangle Park, NC – a medication used to reduce gastric acid secretion; also used as a premedication for chemotherapeutic regimens to reduce the incidence of nausea
Rituximab – Rituxan®, Genentech BioOncology, South San Francisco, CA – a mouse-derived monoclonal antibody used to threat non-Hodgkin lymphoma by targeting the CD20 antigen. This was the first monoclonal antibody to be approved by the FDA.
Trastuzumab – Herceptin®, Genentech BioOncology, South San Francisco, CA – a partial mouse/human antibody used to treat breast cancer by targeting the Her2neu antigen.
Tositumomab - Bexxar® - GlaxoSmithKline, Research Triangle Park, NC – a monoclonal antibody radio-labeled with iodine 131; FDA approved for treatment of patients with CD20 + follicular NHL that are resistant to rituximab and have relapsed after chemotherapy.
Commonly Used MedicationsWhere no trade name and manufacturer are given, the drug is generic.
57THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
58 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES
Notes

59THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

60 THE CYTOKINES AND THE B-CELL MALIGNANCIES:A NEW SPIN ON MAXIMIZING THERAPEUTIC OUTCOMES

A Division of the Oncology Nursing Society
CLASSR O O M O N D E M A N D • FAST,C
ON
VE
NI E
NT
AN
DF
LE
XIB
LE!
•LEARNINGATYOURLEIS
URE•
NO
TR
AV
EL
RE
QU
I RE
D•
ONS Center for Education
Education You Need From a Source You Know
C O N T I N U I N G E D U C A T I O N P R O G R A M S
Get the most current oncology nursing education from ONS!
Our programs are designed by nurses for nurses in a variety of formats that suit your learning style.
Local and Regional Programming Print-Based Materials Online Programs Teleconferences National Conferences
Look to CE Central for the newest cutting-edge cancer treatments!
Check Out ONS Online Distance Learning Courses! Various Topics: Access Devices Cancer Basics Genetics Safe Handling
These highly interactive programs allow you to get the information you want and need. Best of all…It’s all from the comfort of your home at times that are the most convenient for you.
For complete information on all ONS online distance-learning courses visit us at www.ons.org/cecentral.

A Division of the Oncology Nursing Society
OES has been assigned meeting space to provide an educational program funded by Berlex Oncology, Inc., via an educational grant, during the Oncology Nursing Society’s (ONS) 31st Annual Congress. The Oncology Nursing Society’s assignment of meeting space does not imply product endorsement, nor does the Oncology Nursing Society assume any responsibility for the educational content.
This program has been planned and produced by OES, a division of the Oncology Nursing Society.
on Maximizing Therapeutic Outcomes
THE CYTOKINES AND THE B-CELL MALIGNANCIES