the determinants of self-medication: from urban vietnam · pdf filethe determinants of...
TRANSCRIPT

TheDeterminantsofSelf-Medication:EvidencefromUrbanVietnamæ
NguyenTrongHoaiGThangDangGG
June2016
Abstract. This study examines the primary determinants of self-medications among urban citizens in Ho Chi Minh City, Vietnam. Toachieve the researchobjective, thequestionnaire isdesigned toelicit therespondents’ necessary information using in-depth personal interviews.Employing logistic models the paper finds that the probability of self-medication is positively associated with the respondents’ high schooldegree or vocational certificate, married status, and income while it isnegatively related to employed status, the number of children, thegeographicaldistance fromhome to thenearesthospital,doingexercise,andlivinginacentralregion.Meanwhile,usingPoissonmodelsthepaperfinds that the frequencyof self-medication ispositively associatedwiththe respondents’ high school and vocational, married, income, andchronicdiseasewhilethefrequencyofself-medicationisadverselyrelatedto male, employed, children number, distance, being close to healthprofessionalandcentralareas.
hÉywords:Self-medication;HoChiMinhCity;Vietnam
----------------------------------------G= ProfessorofEconomics,UniversityofEconomicsHoChiMinhCity(UEH).Correspondingaddress: @59C Nguyen Dinh Chieu Street, District 3, Ho Chi Minh City, Vietnam. E-mail:[email protected]= Lecturer, School of Economics, University of Economics Ho Chi Minh City (UEH).Corresponding address: @1A Hoang Dieu Street, Phu Nhuan District, Ho Chi Minh City,Vietnam.E-mail:[email protected].†ThefinancialsupportfromtheRockefellerFoundationisgratefullyacknowledged.

2
“Thedesiretotakemedicineisperhapsthegreatestfeaturewhichdistinguishesmanfromanimals”
SirWilliamOsler(Cushing1925)
1 IntroductionSelf-medication has beenwidely used as a common approach to illnesstreatments in the developed world over many years ago (Jones 1976;Bennadi 2014). An increased incidence of self-medication is alsorecognizedfromthedevelopingworld(WHO2000a,2015;Shankaretal.2002).This study empirically investigates the fundamentaldeterminantsof self-proscribed medication among urban citizens in Ho Chi MinhCity,Vietnam-adevelopingandtransitioncountryinSoutheastAsia.
Self-medication is understood as the behavior of using any medicinalproducts without prescription in order to resolve minor deseases orsymptomsthatarerecognizedbymedicinecustomers(Hernandez-Juyoland Job-Quesada 2002). Self-medication is relatively popular in areaswheremedicinesorpharmaceuticalproductsarepredominantlyavailable.The commonness of self-medication can be explained for the reduceddemandfordoctorvisits.
Self-medicationcangeneratebenefitsforbothindividualsandthesocietywhen it is correctly practiced (WHO 2000b). For example, self-medication allows individuals and households manage their healthproblems with the low costs and the saved time. Meanwhile, self-medicationprobablycontributetothepublichealthsystem intheaspectof decreasing the burden for public health facilities. However, self-medicationalsoimposessomepotentialrisksrelatedtoside-effectsofthemisuseofmedicines such as incorrectdiagnosis, inappropriatedurationof using medicines, or drug resistance, abusing the medicines withoutprofessional advice (WHO 2000b). Obviously, self-medication isprobably unavoidable in some situations so that individuals orhouseholds have certain incentives to purchase medicines to treat theirillnesseswithoutprescriptions(WHO2000b).
Previous statistics has shown that self-medication uses range from 2percentto99percentamongvariouscountries(Shehnazetal.2014).For

3
example, there is about 38.5 percent of repspondents who use self-
medication among children and adolescents in Germany (Du 2009).Meanwhile,deMeloetal. (2006) find that there isabout21.5percentofrespondentswhouseself-medicationinasurveyforruralPortugal.
Also, theprevalenceof self-medication isa fact indevelopingcountries.Vietnamissofarnotanexception.Researchonself-medicationhoweveris rarely conducted in developing countries although it is a commonphenomenon there. Hence, this study contributes to the existingliteratureonthislineofresearch.
Vietnam considerablyhas a largepopulation.Healthcare for its citizensbecomes one of the most important problems facing the country.However,Vietnamisalsoadevelopingcountrieswherethepublichealthsystem is seemingly insufficient for the tremendous demand forhealthcareandtheresource-constrainedhouseholdsaredominantwithinthe economy.This contextofdevelopmentprogress stage stylized for adevelopingcountrylikeVietnamapparentlyaffectsitscitizens’behaviorsin choosing the treatments for illness problems and probably self-medicationalsoanimportantmeasure.
Inaddition,thebigsizeofmarketformedicalproductsandtherelaxablestatus of legal aspect for medicine trades allow self-medication beingcommonphenomenon in the society as ameasure forpeople to resolvetheirhealthproblems.Understanding theprimarydeterminantsof self-medication is therefore important inVietnam.That is this study’smainpurpose.
It is important to understand the fundamental determinants of self-medicationinordertorecommendpublichealthpoliciesaimedtoreducepharmaceutical product-related health-risk among citizens. In addition,evidence-based understands of factors related to self-medicationbehaviors promote the awareness of potential health hazards of usingmedicineswithoutdoctoralconsultances.
Chang and Trivedi (2003) is a quantitative study on self-medication inVietnam and find that the behavior of self-prescribed medication issignificantly affectedby income andhealth insurance status.ThispaperusessurveydatafromVietnamLivingStandardSurveys(VLSS)of1997-1998 in Vietnam to disclose that both income and health insurancenegatively correlate to self-medication among Vietnamese citizens.Becauseof the limitationofavailabledata, theymostly focuson income
4
and insurance status as two main determinants of self-medicatingbehaviors.This approach therefore is probably questionable because ofthe possible omitted variables that are crucial to understand theinfluential factors of self-medication in a developing country likeVietnam. In this study,we provide amore in-deep investigation of thedeterminantsof self-medication inVietnam. Inparticular,we relate thewide potential socio-economic factors to the behaviors of self-medication.Todothis,wedesignthequestionnairetoelicit informationon the characteristics of respondents as well as their self-prescribedmedicatingbehaviorsinHoChiMinhCity,Vietnam.
Theremainderofthepaper isorganizedasfollow.Section2reviewstheexisting literature in the topic of self-medication factors for bothdevelopedanddevelopingcountries.Insection3,theresearchdesignandthesampleofdatausedtoachievetheresearchobjectivearepresented.Inparticular,thestructureofthequestionnaireisdescribedandthemethodofdata collection isdiscussed. Section 4 shows the empricalmethodofestimation that is the specifications of econometric models that isemployed in this study. Next, in the empirical results are discussed insection5.Finally,concludingremarksaremadeinsection6.
2 LiteratureReviewThe investigation of determinants of self-medication is increasinglyconducted in developed countries (Grigoryan 2006; Grigoryan et al.2008)anddevelopingnationsaswell (WHO2000a,2015;Shankaretal.2002).
WHO (1998) sytemmatically provides a relatively possible factors thatare potentially related to self-medication behaviors. In particular, thesefactors are grouped into eight groups including socio-economiccharacteristics, lifestyle,accessibility, illnessmanagement,environmentaland pulic health conditions, demographic and epidemiologicalcharacteristics, health sector reforms, and medicine availability. Thisframeworkhasapplied inmanyempiricalstudiesonthis lineofresearchto disclose the important determinants of self-medication in bothdevelopedanddevelopedcountries.
Yusuff and Omarusehe (2011) provide an investigation of keydeterminants of self-medication with othordox and herbal medicines
5
amongpregnantwomen in Ibadan,Nigeria.The results suggest that theself-medication is significantly associated with age and occupationalstatus of respondents. In addition, the lack of knowledge on inverseoutcomesstemmingfromtheuseofself-medicationnegativelyaffectsthebehaviorsofself-medicationinNigeria.
Ramalhinhoetal. (2014)giveanattemptof relating importantvariablesto self-medication with antibiotics in the Algarve Region of Portugal.There are three groups of respondents’ possible variables used in thisstudyincludesocio-demographicvariables,variablesrelatedtohealthandthehealthsystem,andbehavioralvariables.The findingsshow thatnon-prescriptionacquisition,ageandgenderarestronglyassociatedwith theself-medicatingbehaviorswithantibiotics.
Figueirasetal.(2000)isanotherinvestigationofthedeterminantsofnon-prescription medicine uses in Spain. The study relates socio-economicfactorsofrespondentstotheirself-medicationdecisions.Theresultsfindthatgender,marriage status,and residential locationareprimary factorsof self-medication in Spain. Particularly, respondents who are female,singlemarriage status, and urban residents cogently tend to havemoreself-medicationthanothers.
Grigoryan et al. (2008) examine the relationship between predisposingfactors (attitudes and knowledge concerning antibiotic use and self-medication) and enabling factors (countrywealth andhealthcare systemfactors) and self-medication with antibiotics in 12 European countries.The results indicate that the more likely behavior of self-medication ishighly correlated with highly perceived beliefs on useful treatments ofself-medicationwithantibioticsforminorailmentsandbronchitisfortheindividuallevel.Also,theavailabilityofantibioticsispositivelyrelatedtothe behavior of self-medication of an individual. At a macro level, thestudy reveals that thewealthydegreeof countrywhere repondents livehasanegativeimpactonitscitizens’likelihoodofself-medication.
Setiawan et al. (2012) evidently argue that the possibility of self-medicationusedependsonpublicpolicies from thegovernment relatedto regulating and monitoring the dispensation of medicines and drugswithinthecountry.Themorelikelythegovernmentfailstoregulateandsupervise informal markets for medicines and drugs, the more poorcitizens tend to have self-medication. This study is implemented inYogyakartacityofIndonesia.

6
deMeloetal. (2006)show that thesignificant factorsofself-medicatingbehaviorsamongruralPortugees includeage,typeofhealthconsultants,and the duration of time waited to meet doctors and other healthprofessional services. Importantly, the study also finds that there existsthe seasonal fator of self-medication, for some specific deseases,particularly cough and cold preparations, dermatologicals, and anti-inflammatoryandanti-rheumaticproducts.
In addition tooriginal studiesofdeterminantsof self-medication, therearesomesystematicreviewstudiesonthistopic.Forinstance,Shehnazetal. (2014) provide a comprehensive review of the factors of self-medication behaviors among adolecents aged 13-18 years using 163primary studies. The results in particular show that the prevalentdeterminants of self-medication among adolecents consist of femalegender,olderage,maternaleducation,andfamilialpractices.Inaddition,headache, allergies, and fever are frequently the most self-medicatedhealth problems among deseases or symptoms. Meanwhile, Eticha andMesfin (2014) produce a cross-sectional study of self-medication inMekelle,Ethiopia.The results indicate that thehighprobabilityof self-medication is associated with some certain health problems such asheadache, fever,gastrointestinaldiseasesand respiratory tract infections.Also,some typesofmedicalproductsaremore frequentlyused forself-medication such as analgesics/antipyretics, gastrointestinal drugs,respiratorydrugsandoralrehydrationsaltthanothers.
Some studies also find that self-medication is predominantly populousamong people who have knowledge related to medical or phamarcysciences. Alam et al. (2015) evidently show that the likelihood of self-medicationisconsiderablyhighamongmedicalandphamarcystudentsinBangladesh. This populous phenomenon is clearly characterized for adevelopingcountry likeBangladeshalthough itpotentiallypromotesthemisuseofmedicinesevenamongeducatedcitizens.
Asimilarresult isdemonstrated inNepal(Gyawalietal.2015).Notablythe results find that the dominant medicines among self-medicationincludepainkillerswith73.2percent,antipyreticswith68.8percent,andantimicrobials with 56.2 percent of the total sample of respondents.Pavyde ̇etal.(2015)findthatrespondentsaremale,fromruralareas,andsinglepersons aremore likely to self-medicatewithusing antibiotics inLithuania.
7
3 ResearchDesignandtheSampleResearchDesign
Inorder toexamine the fundamentaldeterminantsof self-medication inurbanVietnam, thequestionnaire isdesigned toelicit informationaboutrespondents’ characteristics.The key variables in the questionnaire arearrangedintothreemainfollowinggroups.
(1) Socio-economic characteristics of respondents: This group includesinformation on age, gender, education level, marital status,employmentstatus,andincome.
(2) Informationonhealthcare systems:Thissectionprovidesquestionsinordertoelicittheeffectofcharateristicsofhealthcaresystemsontherespondents’decisionsofself-medicationinVietnamsuchastherespondents’insurancestatus.
(3) Self-medicationbehaviors:Thisgroupconsistsofquestionsinordertoobtaininformationrelatedtoself-medicationbehaviors.Thesearehealth status, the number of doctor visits, the number of self-medication, insurance purchase, the reasons for using self-medication, the types of diseases for self-medication, the effect ofinformation disclosure or external advices on self-medicationbehaviors, the popular places to buy medicines, the methods therespondents usemedicines, knowledge on the effect of using self-
medication on respondents’ health, and the respondents’ lifestylesuchasexerciseactivities.
The full questionnaire is presented in theAppendix 2 at the end of thispaper. The survey is administered in Ho Chi Minh City, one of thebiggestcitiesinVietnam.Face-to-faceinterviewsareimplemented.
HoChiMinhCity is the largest city inVietnamwith a population ofabout at least 8 millions of people. Ho Chi Minh City has seen acollectionofsocitieswithawiderangesof income,education,andothersocio-demographiccharacteristicsoftheircitizens.Toconstructasamplethat is representative for thepopulation in the city, thehouseholdswasrandomlychoosenfromvariousareasincludingthecentralareasandsub-urbanones aswell, areaswith the richhouseholds and thosewithpoorhouseholds. Ho Chi Minh City is a good case study for investigatingurbancitizens’self-medicatingbehaviorsforurbanVietnam.
8
TheSample
Thesamplesizeof241respondentsisachieved.Themeanageisabout30yearsold.Approximately42percentoftherespondentsismaleandabout58percent is female.Thedescriptivestatisticsof thesample ispresentedinTable1.
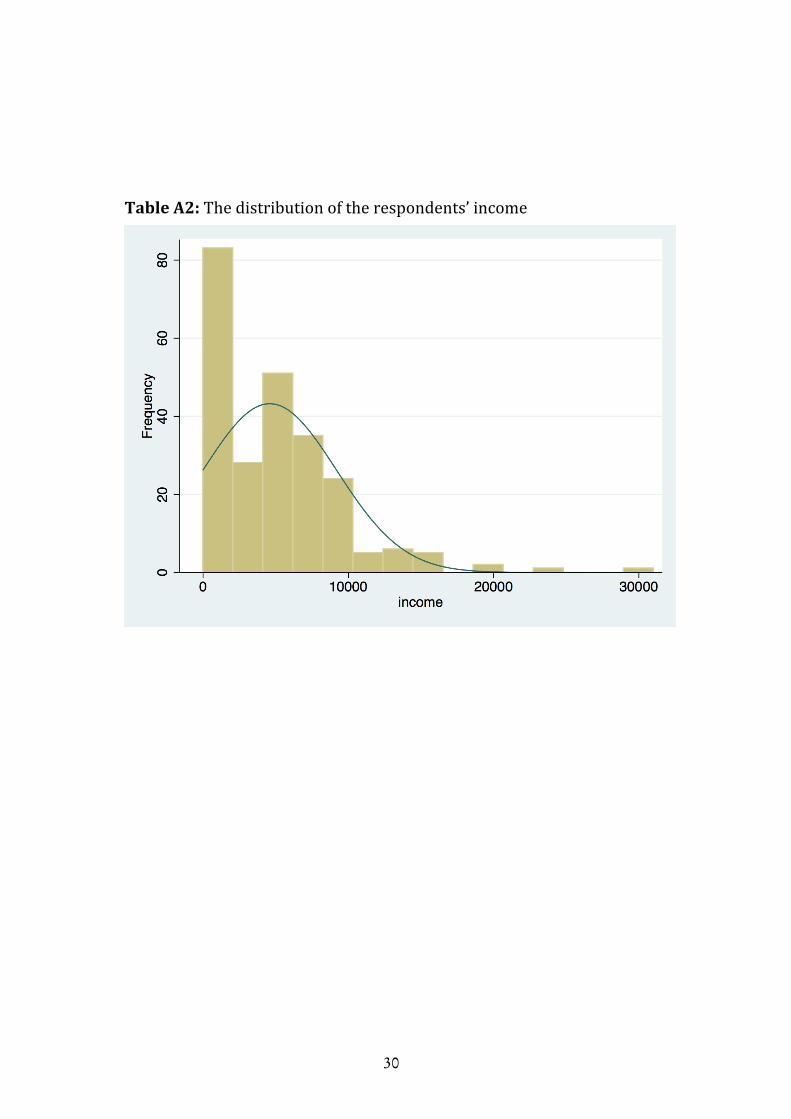
Amongtherespondents,18percenthasthedegreeoflowerorsecondaryschoolasthehighestdegreeofeducationwhilethecorrespondingfiguresforhighschoolorvocationalandtertiaryeducationare39percentand43percent respectively. There are about 32 percent and 68 percent ofrespondentswithbeingmarriedandemployedrespectively.TheaveragemonthlyincomeoftherespondentisaboutVND4.6million.
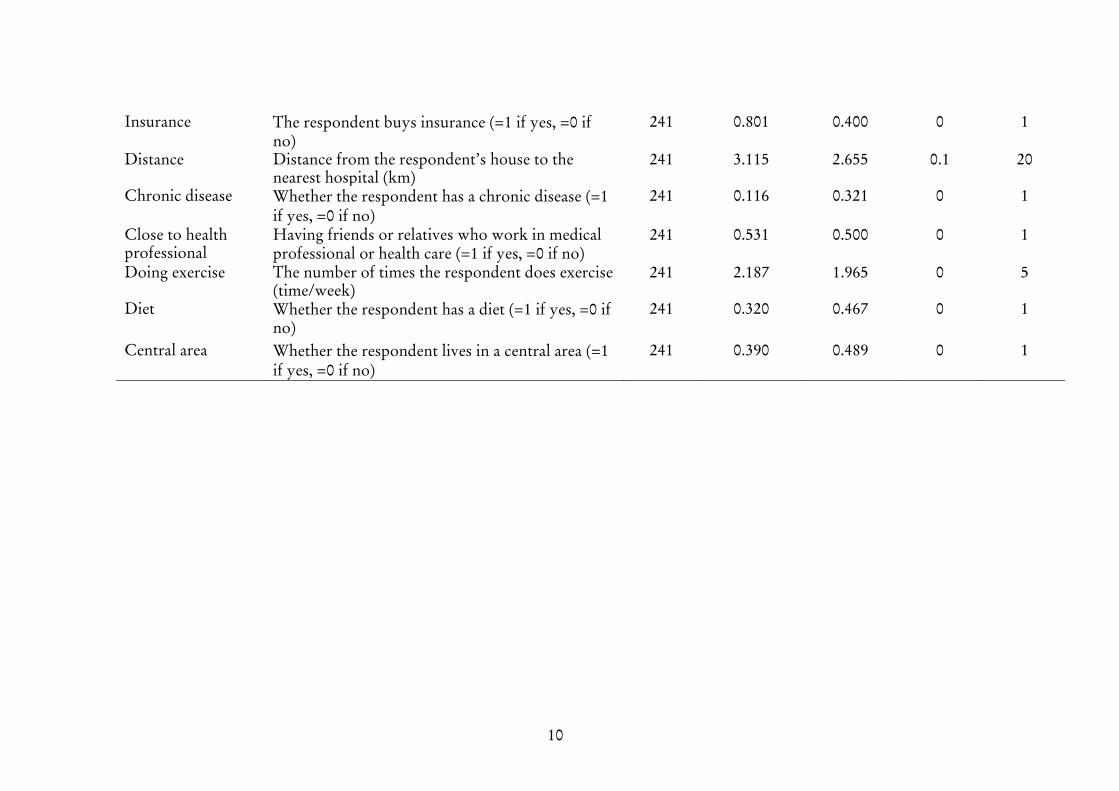
Approximately 11.6 percent of the respondents state that they havechronicdiseases.About53percentofthemhaverelativesorfriendswhoareworkingtheheathindustryorhavehealthcarerelatedjobs.Regardinginformationon the respondents’ lifestyle,one respondentdoesexerciseswithameanfrequencyofnearly2.2timesperweekandabout32percentoftherespondentshavediet.Meanwhile,thereisabout39percentoftherespondents living in the central areas of Ho Chi Minh City. Moreinformation on the sample and highlighting variables is presented in^ééÉåÇáñ==1.
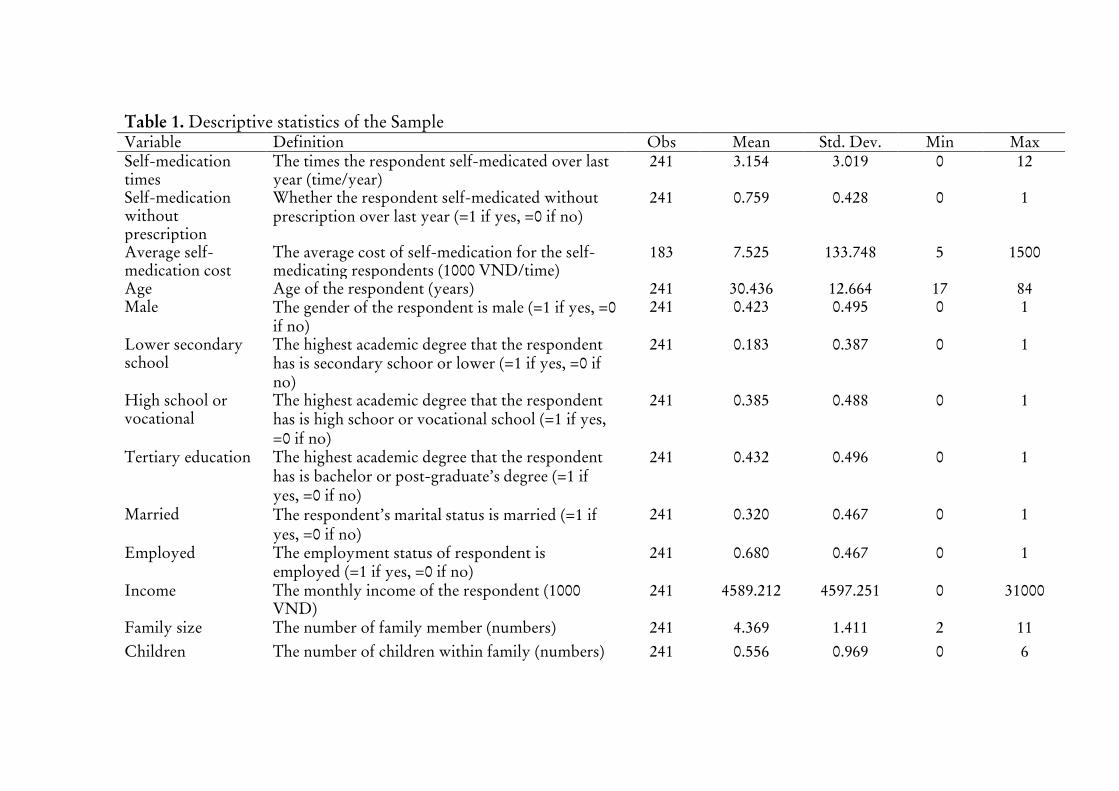
Table1.DescriptivestatisticsoftheSampleVariable Definition Obs Mean Std.Dev. Min MaxSelf-medicationtimes
Thetimestherespondentself-medicatedoverlastyear(time/year)
241 3.154 3.019 0 12
Self-medicationwithoutprescription
Whethertherespondentself-medicatedwithoutprescriptionoverlastyear(Z1ifyes,Z0ifno)
241 0.759 0.428 0 1
Averageself-medicationcost
Theaveragecostofself-medicationfortheself-medicatingrespondents(1000VND/time)
183 7.525 133.748 5 1500
Age Ageoftherespondent(years) 241 30.436 12.664 17 84Male Thegenderoftherespondentismale(Z1ifyes,Z0
ifno)241 0.423 0.495 0 1
Lowersecondaryschool
Thehighestacademicdegreethattherespondenthasissecondaryschoororlower(Z1ifyes,Z0ifno)
241 0.183 0.387 0 1
Highschoolorvocational
Thehighestacademicdegreethattherespondenthasishighschoororvocationalschool(Z1ifyes,Z0ifno)
241 0.385 0.488 0 1
Tertiaryeducation Thehighestacademicdegreethattherespondenthasisbachelororpost-graduate’sdegree(Z1ifyes,Z0ifno)
241 0.432 0.496 0 1
Married Therespondent’smaritalstatusismarried(Z1ifyes,Z0ifno)
241 0.320 0.467 0 1
Employed Theemploymentstatusofrespondentisemployed(Z1ifyes,Z0ifno)
241 0.680 0.467 0 1
Income Themonthlyincomeoftherespondent(1000VND)
241 4589.212 4597.251 0 31000
Familysize Thenumberoffamilymember(numbers) 241 4.369 1.411 2 11Children Thenumberofchildrenwithinfamily(numbers) 241 0.556 0.969 0 6
10
Insurance Therespondentbuysinsurance(Z1ifyes,Z0ifno)
241 0.801 0.400 0 1
Distance Distancefromtherespondent’shousetothenearesthospital(km)
241 3.115 2.655 0.1 20
Chronicdisease Whethertherespondenthasachronicdisease(Z1ifyes,Z0ifno)
241 0.116 0.321 0 1
Closetohealthprofessional
Havingfriendsorrelativeswhoworkinmedicalprofessionalorhealthcare(Z1ifyes,Z0ifno)
241 0.531 0.500 0 1
Doingexercise Thenumberoftimestherespondentdoesexercise(time/week)
241 2.187 1.965 0 5
Diet Whethertherespondenthasadiet(Z1ifyes,Z0ifno)
241 0.320 0.467 0 1
Centralarea Whethertherespondentlivesinacentralarea(Z1ifyes,=Z0ifno)
241 0.390 0.489 0 1

4 EstimationMethodsIn this study, there are two types of data for the dependent variable,which areproxies for self-medication, includingbinarydata (where therespondentself-medicatedoverthelastyear)andcountdata(thenumberof times the respondents use self-medication as the treatment for theirillnessproblemover the lastyear).Corresponding to each typeofdatafor thedependentvariable, therearecorrespondingempiricalmodels.Inparticular,forbinarydependentvariable,the logitandprobitmodelsareemployed to estimate the probability of the pharmacy visit withoutprescriptions.Meanwhile,Poisson regression is employed in the caseofusingthecount-datadependentvariable.
Theestimationmethodsfortheprobabilityofself-medication
Thelogitmodelisspecifiedasbelow:
!" = #$ %" = 1 &' = ()!(*&′')
,+()!(*&′')(1)
where!" isthelikelihoodofusingself-medicationfromtherespondent(0<!" <1),and& isthevectorofcontrolvariables.
Thealternativemodel for thebinarydependentvariable isprobitmodelthatisspecifiedasfollows:
!" = #$ %" = 1 &' = - *&′' (2)
where- *&′' is the cumulative distribution function for the standard
normal.
Theestimationmethodsforthefrequencyofself-medication
Thepoissonregressionmodel isused forestimate the frequencyofself-medicationconditionalon thedistributionof thedependentvariableonthe vector of covariates and parameters of interests, that is called thePoissondistribution:
#$ %" &' = (−/" /"%"
%"! (3)
12
where%" = 0, 1, 2, …is the number of self-medication times, and/is theintensityorrateparameterwithit’smeanparameterizationispresentedasbelow:
/" = ()! *&′' (4)
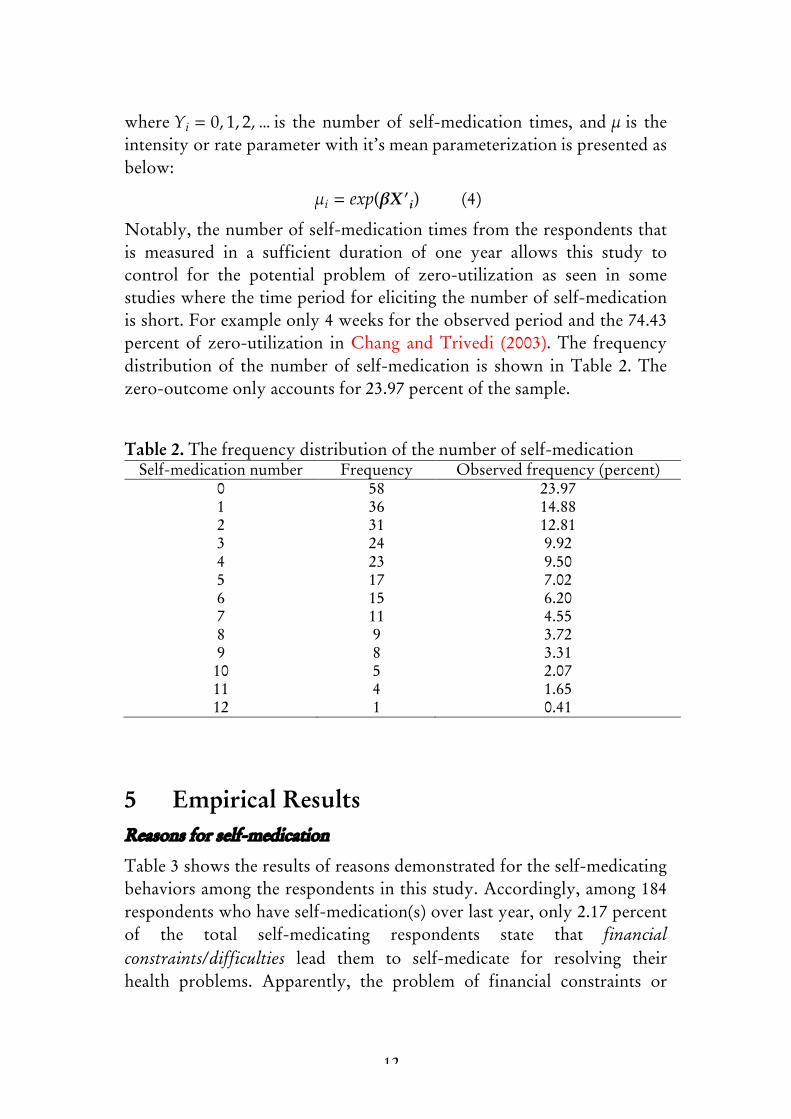
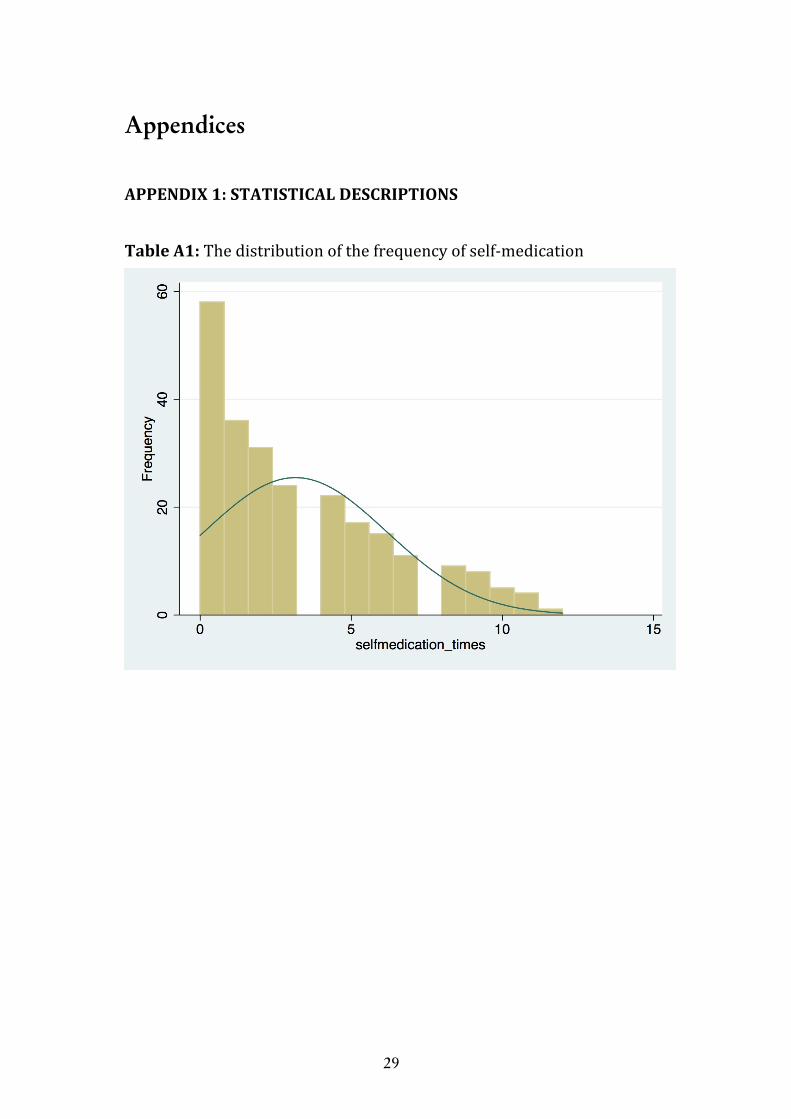
Notably,thenumberofself-medicationtimesfromtherespondentsthatis measured in a sufficient duration of one year allows this study tocontrol for the potential problem of zero-utilization as seen in somestudieswherethetimeperiodforelicitingthenumberofself-medicationisshort.Forexampleonly4weeksfortheobservedperiodandthe74.43percentof zero-utilization inChang andTrivedi (2003).The frequencydistributionof thenumberof self-medication is shown inTable 2.Thezero-outcomeonlyaccountsfor23.97percentofthesample.
Table2.Thefrequencydistributionofthenumberofself-medicationSelf-medicationnumber Frequency Observedfrequency(percent)
0 58 23.971 36 14.882 31 12.813 24 9.924 23 9.505 17 7.026 15 6.207 11 4.558 9 3.729 8 3.3110 5 2.0711 4 1.6512 1 0.41
5 EmpiricalResultsReasonsforself-medication
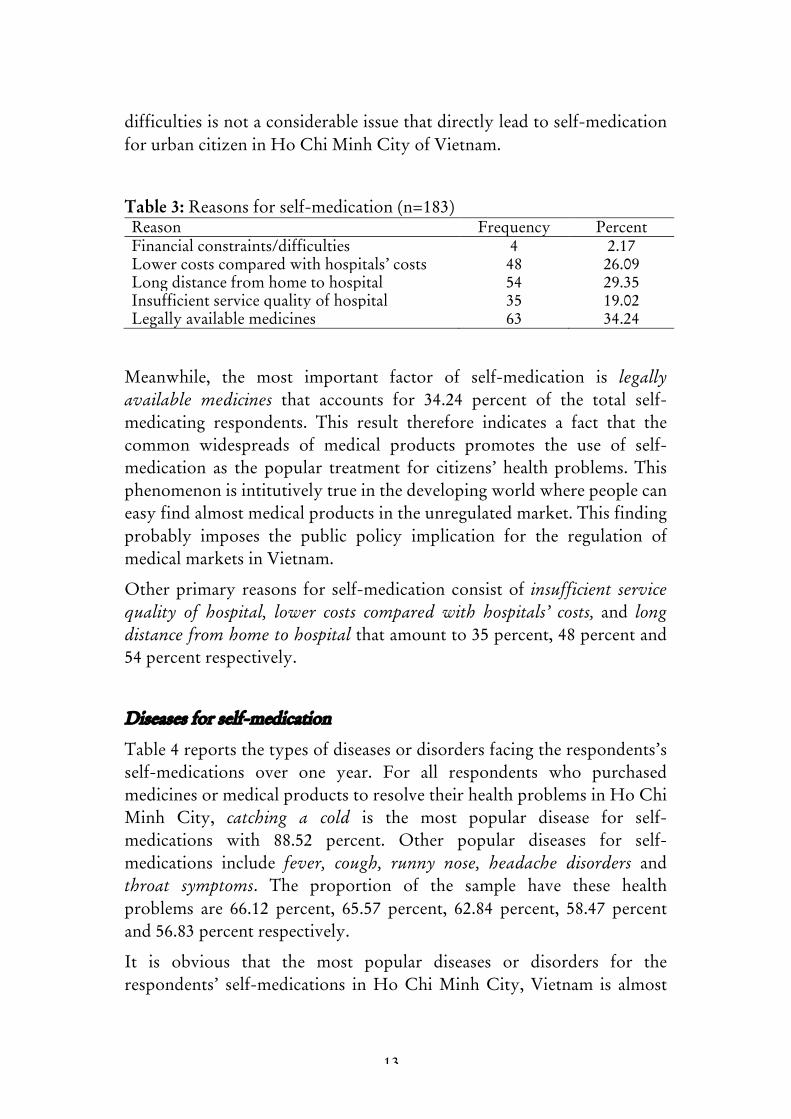
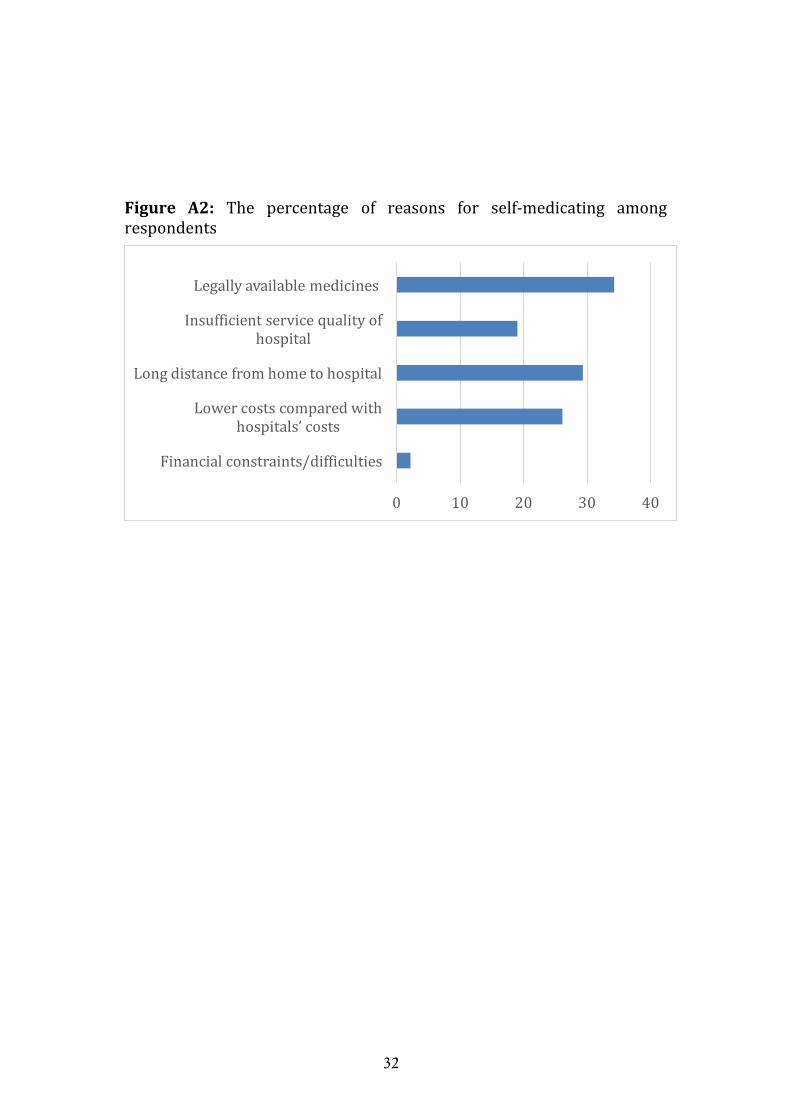
Table3showstheresultsofreasonsdemonstratedfortheself-medicatingbehaviorsamongtherespondents inthisstudy.Accordingly,among184respondentswhohaveself-medication(s)overlastyear,only2.17percentof the total self-medicating respondents state that financialconstraintsLdifficulties lead them to self-medicate for resolving theirhealth problems. Apparently, the problem of financial constraints or
13
difficultiesisnotaconsiderableissuethatdirectlyleadtoself-medicationforurbancitizeninHoChiMinhCityofVietnam.
Table3:Reasonsforself-medication(nZ183)Reason Frequency PercentFinancialconstraints/difficulties 4 2.17Lowercostscomparedwithhospitals’costs 48 26.09Longdistancefromhometohospital 54 29.35Insufficientservicequalityofhospital 35 19.02Legallyavailablemedicines 63 34.24
Meanwhile, the most important factor of self-medication is legallyavailable medicines that accounts for 34.24 percent of the total self-medicating respondents. This result therefore indicates a fact that thecommon widespreads of medical products promotes the use of self-medication as the popular treatment for citizens’healthproblems.Thisphenomenonisintitutivelytrueinthedevelopingworldwherepeoplecaneasyfindalmostmedicalproductsintheunregulatedmarket.Thisfindingprobably imposes the public policy implication for the regulation ofmedicalmarketsinVietnam.
Otherprimary reasons for self-medication consistof insufficient servicequality of hospital, lower costs compared with hospitals’ costs, and longdistancefromhometohospitalthatamountto35percent,48percentand54percentrespectively.
Diseasesforself-medication
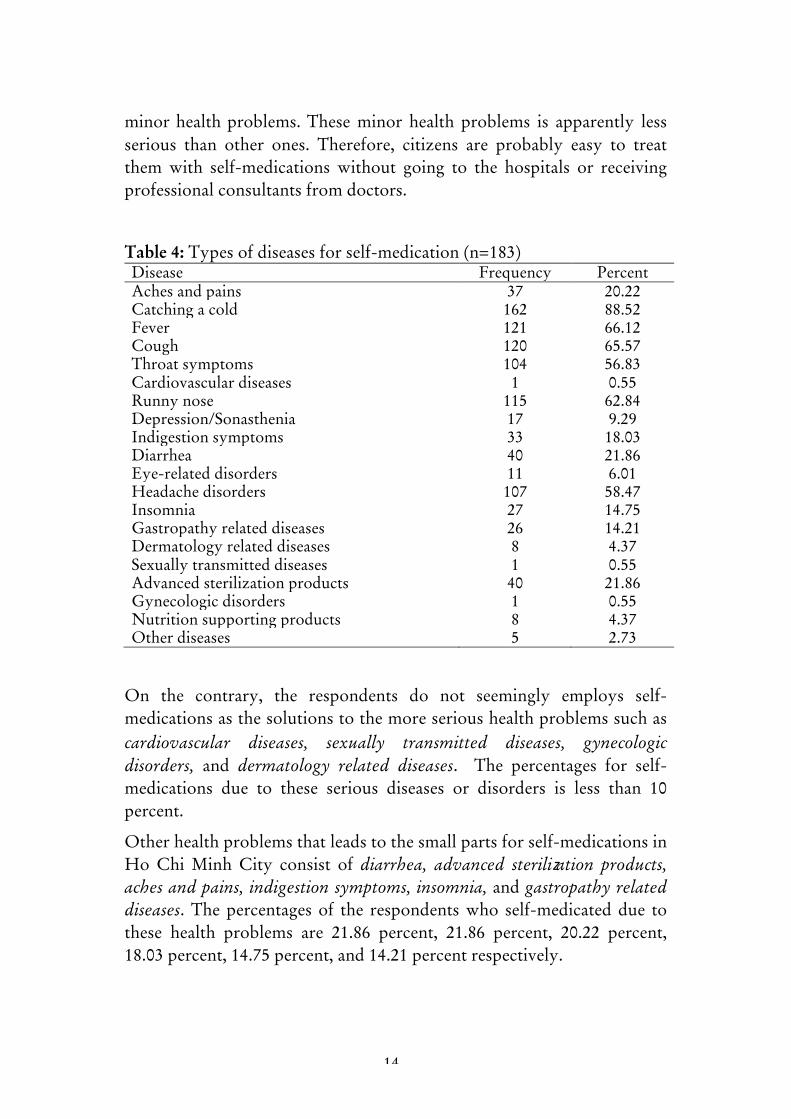
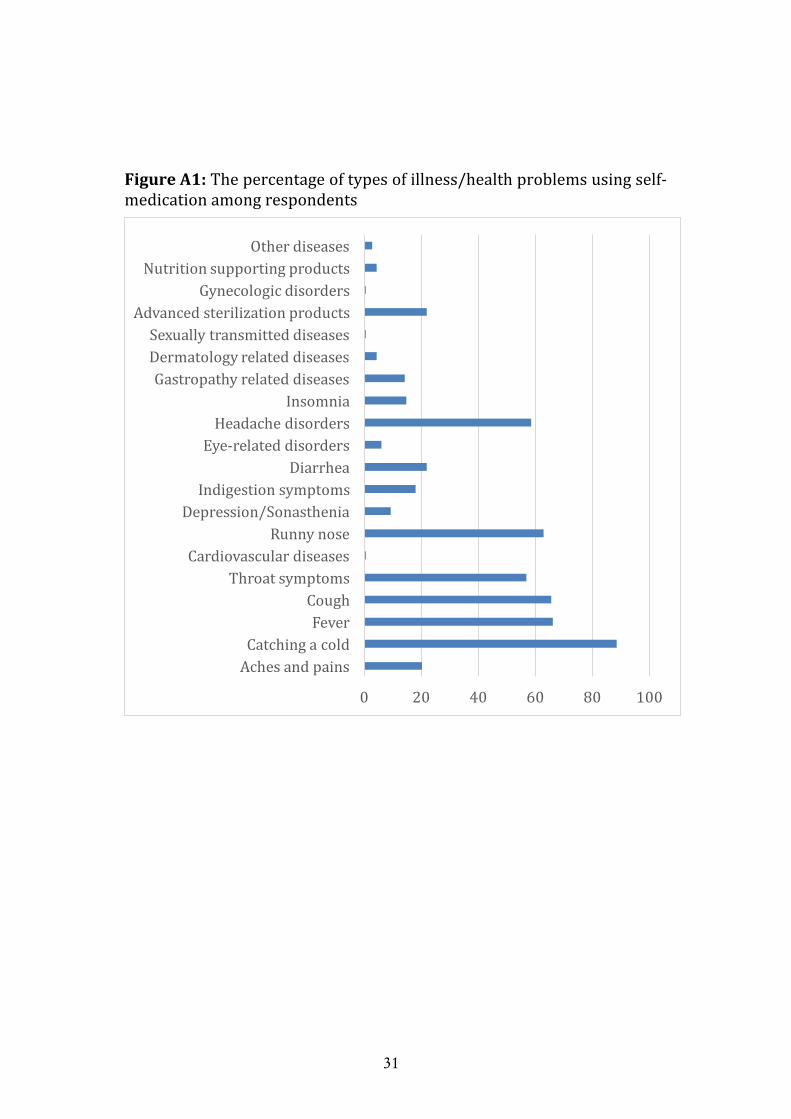
Table4reportsthetypesofdiseasesordisordersfacingtherespondents’sself-medications over one year. For all respondents who purchasedmedicinesormedicalproductstoresolvetheirhealthproblemsinHoChiMinh City, catching a cold is the most popular disease for self-medications with 88.52 percent. Other popular diseases for self-medications include fever, cough, runny nose, headache disorders andthroat symptoms. The proportion of the sample have these healthproblems are 66.12 percent, 65.57 percent, 62.84 percent, 58.47 percentand56.83percentrespectively.
It is obvious that the most popular diseases or disorders for therespondents’ self-medications inHoChiMinhCity,Vietnam is almost
14
minorhealthproblems.Theseminor health problems is apparently lessserious than other ones. Therefore, citizens are probably easy to treatthem with self-medications without going to the hospitals or receivingprofessionalconsultantsfromdoctors.
Table4:Typesofdiseasesforself-medication(nZ183)Disease Frequency PercentAchesandpains 37 20.22Catchingacold 162 88.52Fever 121 66.12Cough 120 65.57Throatsymptoms 104 56.83Cardiovasculardiseases 1 0.55Runnynose 115 62.84Depression/Sonasthenia 17 9.29Indigestionsymptoms 33 18.03Diarrhea 40 21.86Eye-relateddisorders 11 6.01Headachedisorders 107 58.47Insomnia 27 14.75Gastropathyrelateddiseases 26 14.21Dermatologyrelateddiseases 8 4.37Sexuallytransmitteddiseases 1 0.55Advancedsterilizationproducts 40 21.86Gynecologicdisorders 1 0.55Nutritionsupportingproducts 8 4.37Otherdiseases 5 2.73
On the contrary, the respondents do not seemingly employs self-medicationsasthesolutionstothemoreserioushealthproblemssuchascardiovascular diseases, señually transmitted diseases, gynecologicdisorders, and dermatology related diseases. The percentages for self-medications due to these serious diseases or disorders is less than 10percent.
Otherhealthproblemsthatleadstothesmallpartsforself-medicationsinHoChiMinhCity consist of diarrhea, advanced sterilization products,achesandpains, indigestionsymptoms, insomnia,andgastropathyrelateddiseases.Thepercentagesof the respondentswho self-medicateddue tothese health problems are 21.86 percent, 21.86 percent, 20.22 percent,18.03percent,14.75percent,and14.21percentrespectively.

15
Another finding is that there isa97.27percentofrespondentswhoself-
medicated over the last year buy medicines without presriptions frompharmacist-ownedstores.
Probablityofself-medication
Table 5 reports the results from logistic models for the probability ofself-medication in this study. The study uses both logit and probitmodelstoproducetheestimationresults.Usingprobitmodelinadditionto logitmodel isoneway to conduct a robustness testof the resultsofestimation.
In addition, there are two types of empirical models including simplemodel and full model. For simple model, some crucial dependentvariables that are characterized for socio-demographic characteristicsofthe respondents are included such as age, gender, education, maritalstatus, employment status, income, the number of children as thedependents, the geographic distance between home and the nearesthospital,andwhethertherespondentdoexercises.Infullmodel,allotherindependentvariblesinadditionthosefromsimplemodelareincludedinthemodelssuchas familysize, insurancestatus,whether therespondentare with chronic disease, whether the respondent is close to healthprofessional, whether the respondent has diet, and whether therespondent lives incentralareasor locates in suburbanareasofHoChiMinhCity.
In column (1) the results for the simple logit model show that amongindependent variables included in simple models, some variables arestatistically significant for the probability of self-medication at thetraditional levels including high school or vocational (pY0.05), married(pY0.05), employed (pY0.1), log of income (pY0.05), children number(pY0.01),distance(pY0.05),anddoingeñercise(pY0.05).
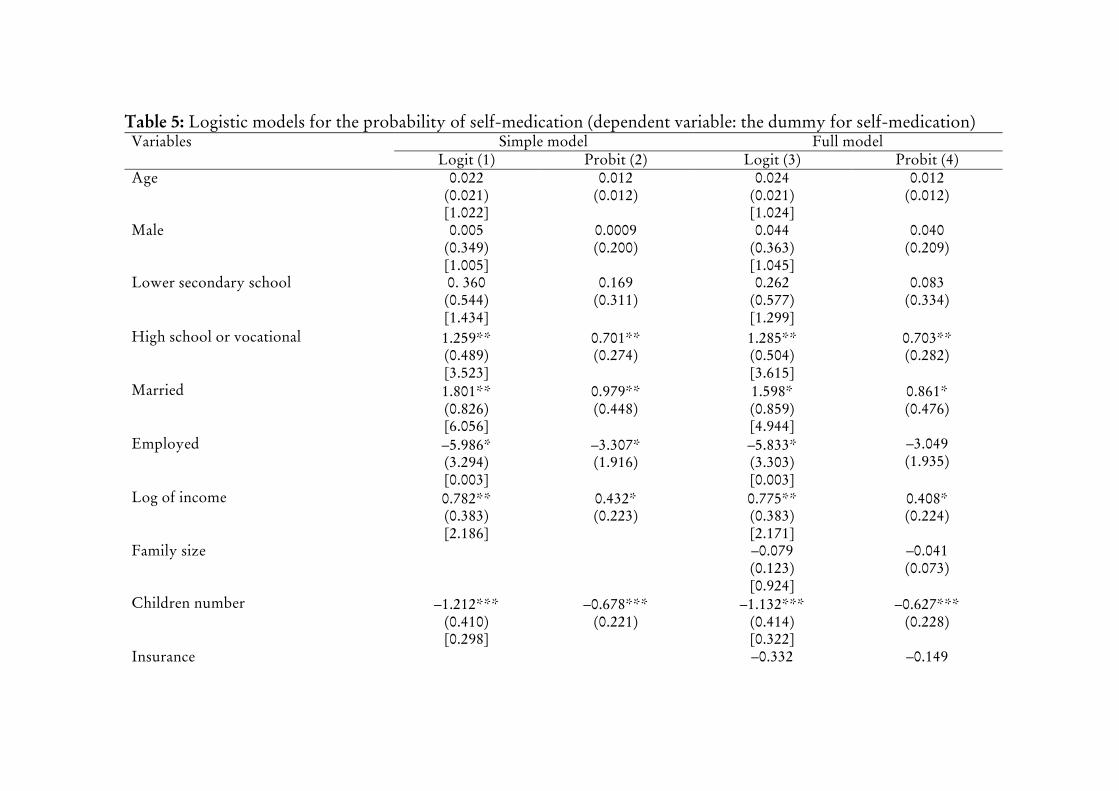
Table5:Logisticmodelsfortheprobabilityofself-medication(dependentvariable:thedummyforself-medication)Variables Simplemodel Fullmodel
Logit(1) Probit(2) Logit(3) Probit(4)Age 0.022
(0.021)[1.022]
0.012(0.012)
0.024(0.021)[1.024]
0.012(0.012)
Male 0.005(0.349)[1.005]
0.0009(0.200)
0.044(0.363)[1.045]
0.040(0.209)
Lowersecondaryschool 0.360(0.544)[1.434]
0.169(0.311)
0.262(0.577)[1.299]
0.083(0.334)
Highschoolorvocational 1.259GG=(0.489)[3.523]
0.701GG=(0.274)
1.285GG(0.504)[3.615]
0.703GG=(0.282)
Married 1.801GG=(0.826)[6.056]
0.979GG(0.448)
1.598G(0.859)[4.944]
0.861G=(0.476)
Employed –5.986G=(3.294)[0.003]
–3.307G=(1.916)
–5.833G(3.303)[0.003]
–3.049(1.935)
Logofincome 0.782GG(0.383)[2.186]
0.432G(0.223)
0.775GG=(0.383)[2.171]
0.408G=(0.224)
Familysize –0.079(0.123)[0.924]
–0.041(0.073)
Childrennumber –1.212GGG(0.410)[0.298]
–0.678GGG(0.221)
–1.132GGG=(0.414)[0.322]
–0.627GGG=(0.228)
Insurance –0.332 –0.149
17
(0.472)[0.717]
(0.269)
Distance –0.147GG=(0.058)[0.863]
–0.087GG=(0.035)
–0.165GGG=(0.061)[0.848]
–0.095GGG=(0.036)
Chronicdisease –0.082(0.592)[0.921]
–0.063(0.339)
Closetohealthprofessional –0.388(0.361)[0.678]
–0.221(0.207)
Doingexercise –0.174GG=(0.087)[0.840]
–0.101GG=(0.050)
–0.170G=(0.092)[0.844]
–0.100G=(0.054)
Diet 0.168(0.418)[1.183]
0.127(0.242)
Centralarea –0.615G=(0.354)[0.540]
–0.330(0.204)
Constant 0.524(0.766)[1.689]
0.389(0.442)
1.517(1.052)[4.557]
0.903(0.603)
Loglikelihood –114.861 –115.134 –111.971 –112.466PseudoR2 0.136 0.134 0.158 0.154Observations 241 241 241 241
Note:G=pY=0.1,GG=pY0.05,GGG=pY=0.01.Tertiaryeducationisomittedvariable.Standarderrorsareinparenthesesandoddsratiosareinbrackets.
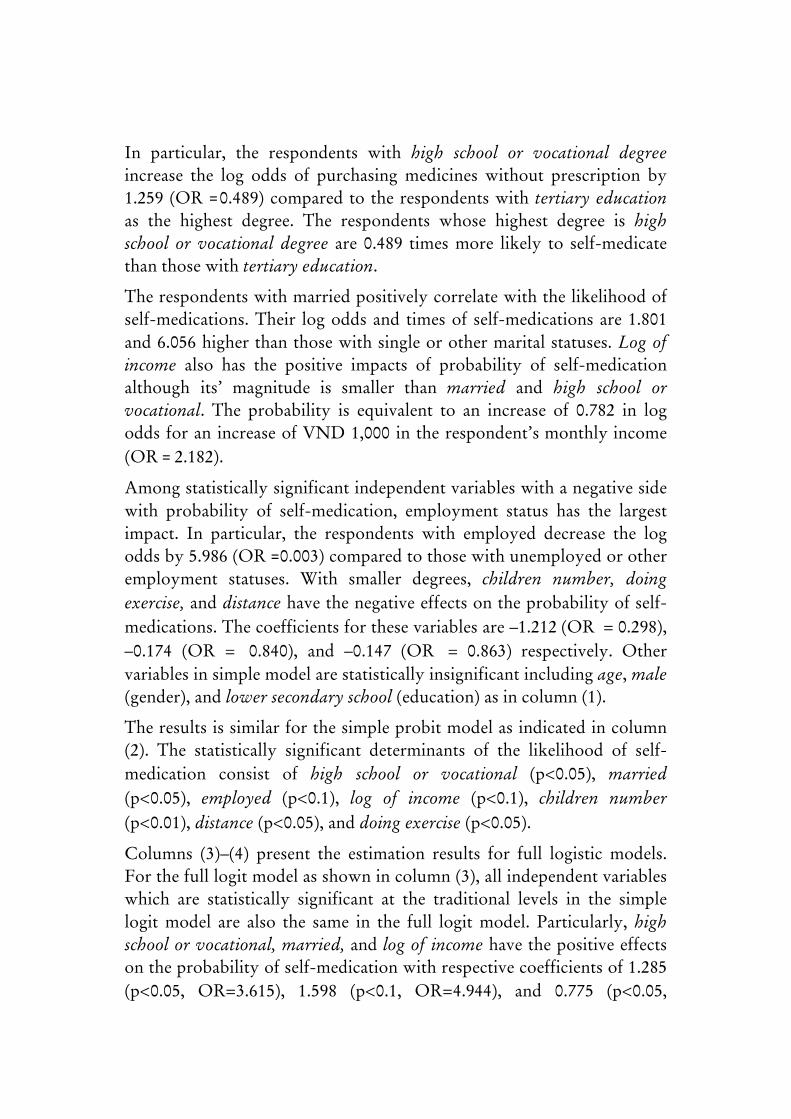
In particular, the respondents with high school or vocational degreeincrease the log odds of purchasing medicines without prescription by1.259 (OR =0.489)compared to the respondentswith tertiary educationas the highest degree. The respondents whose highest degree is highschool or vocational degree are 0.489 timesmore likely to self-medicatethanthosewithtertiaryeducation.
Therespondentswithmarriedpositivelycorrelatewiththe likelihoodofself-medications.Their logodds and timesof self-medications are1.801and6.056higher than thosewithsingleorothermaritalstatuses.Logofincome also has the positive impacts of probability of self-medicationalthough its’ magnitude is smaller than married and high school orvocational. The probability is equivalent to an increase of 0.782 in logodds foran increaseofVND1,000 in therespondent’smonthlyincome(OR=2.182).
Amongstatisticallysignificantindependentvariableswithanegativesidewith probability of self-medication, employment status has the largestimpact. In particular, the respondents with employed decrease the logoddsby5.986(OR=0.003)comparedtothosewithunemployedorotheremployment statuses. With smaller degrees, children number, doingeñercise,anddistancehavethenegativeeffectsontheprobabilityofself-
medications.Thecoefficientsforthesevariablesare–1.212(OR= Z0.298),–0.174 (OR Z= 0.840), and –0.147 (OR= Z 0.863) respectively. Othervariablesinsimplemodelarestatisticallyinsignificantincludingage,male(gender),andlowersecondaryschool(education)asincolumn(1).
Theresults issimilarforthesimpleprobitmodelas indicated incolumn(2). The statistically significant determinants of the likelihood of self-
medication consist of high school or vocational (pY0.05), married(pY0.05), employed (pY0.1), log of income (pY0.1), children number(pY0.01),distance(pY0.05),anddoingeñercise(pY0.05).
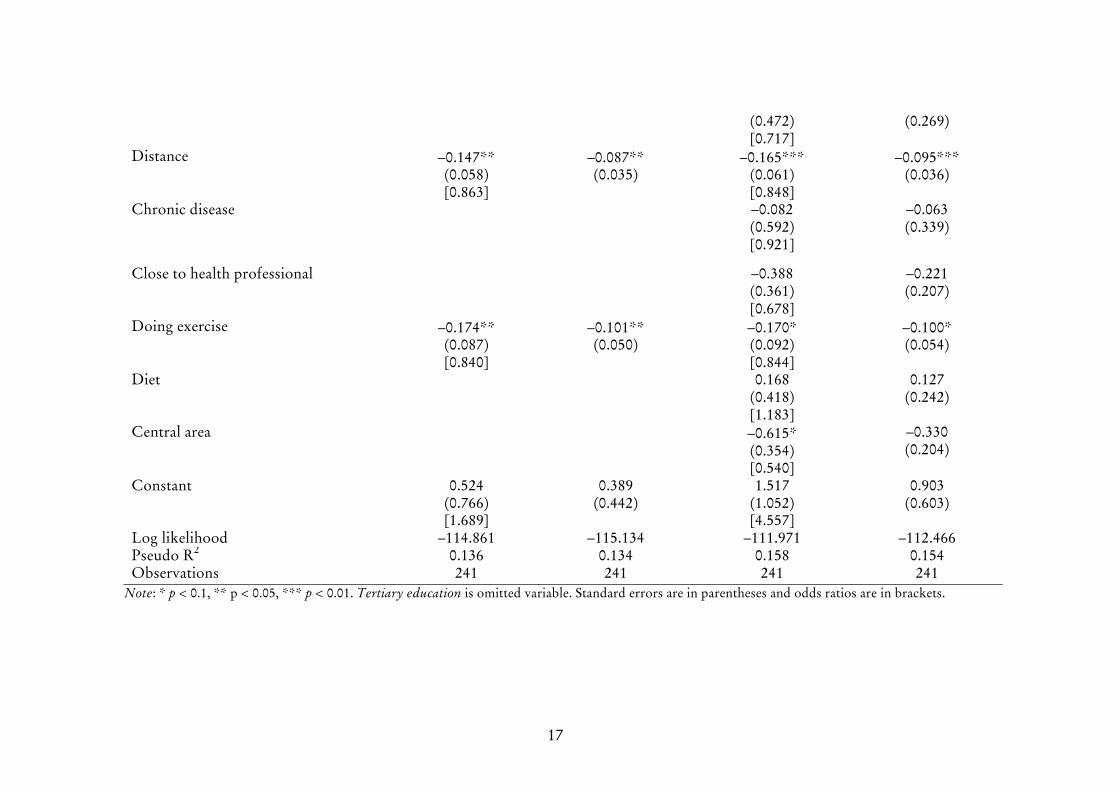
Columns (3)–(4) present the estimation results for full logistic models.Forthefulllogitmodelasshownincolumn(3),allindependentvariableswhich are statistically significant at the traditional levels in the simplelogitmodel are also the same in the full logitmodel.Particularly, highschoolorvocational,married,and logof incomehave thepositiveeffectsontheprobabilityofself-medicationwithrespectivecoefficientsof1.285(pY0.05, ORZ3.615), 1.598 (pY0.1, ORZ4.944), and 0.775 (pY0.05,

19
ORZ2.171) on the one hand. On the other hand, the independentvariables that have statistically significant and negative impacts on thelikelihood of self-medication include employed with a coefficient of –
5.833 (pY0.1,ORZ0.003), children number with a coefficient of –1.132(pY0.01, ORZ0.322), distance with a coefficient of –0.165 (pY0.01,ORZ0.848), and doing eñercise with a coefficient of –0.170 (pY0.1,ORZ0.844).
Among additional control variables included in the full model, centralarea is statistically significant (pY0.1) and has a negative effect on theprobability of self-medication. Specifically, the respondents living in acentralareaofHoChiMinhCityhaveadecreaseof0.615inthelogoddsof theprobabilityof self-medication compared to those from suburbanareas (ORZ0.540). Other additional covariates are statisticallyinsignificant at any traditional level. These variables are family siòe,insurance,chronicdisease,closetohealthprofessional,anddiet.
Generally, there are certain variables that have statistically significanteffects on the likelihood of self-medication include high school orvocational,married,employed, logof income, childrennumber,distance,doing exercise, and central area. The findings demonstrate that therespondent with high school degree or vocational certificate, marriedstatus, or larger income tends on average to have more possibility topurchase medicines without prescriptions to resolve her or his healthproblems. In contrast, with being employed, having more one child,longerdistance fromhome to thenearesthospital,doingexercise, livinginacentralregion,therespondentonaveragedecreasestheprobabilityofself-medicationinHoChiMinhCity,Vietnam.
Frequencyofself-medication
Table 6 presents the results from poisson models for the frequency ofself-medication in this study. There are also simple and full models ofestimationinthissection.
For simple model as indicated in column (1) of Table 6, almostindependentvariablearestatisticallysignificantattraditionallevelexceptfor age, lower secondary school, and doing eñercise. The Poissonregressionmodelproduceshenceahighfittothedata inthisstudy.Theestimates are reasonable to indicate the crucial role of the respondents’
20
socio-demographic characteristics as the primary determinants of thenumberofpharmacyvisitswithoutmedicalprescription.
Itisclearthatfemaleonaveragehavealargernumberofself-medicationcomparedtomale.Inparticular,themalerespondentis0.442timeofself-medication less than the female. The negative association with thenumber of pharmacy visits without prescription are also found invariables such as employed, children number and distance. Specifically,the respondentwithbeing employed,havingmoreone child,orhavingone more km to the nearest hospital from home tends to decrease thenumberofself-medicationcompared to thecounterpartby3.254,0.294,and0.031timesrespectively.
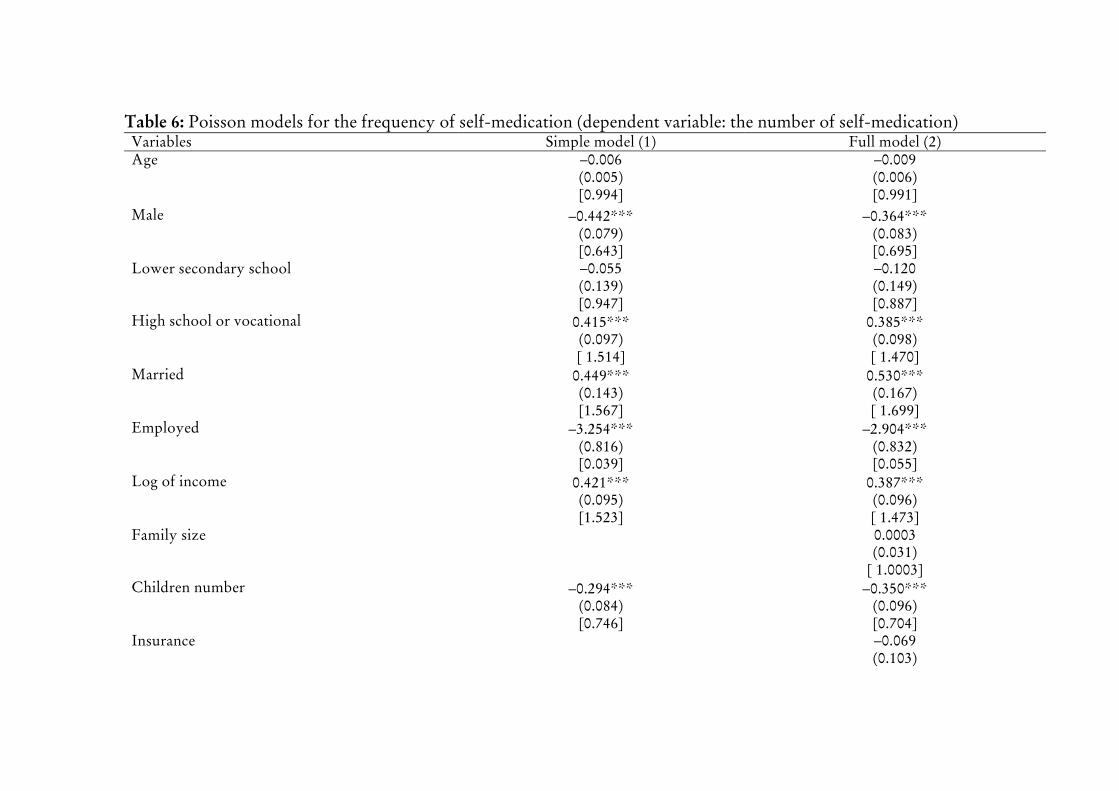
Table6:Poissonmodelsforthefrequencyofself-medication(dependentvariable:thenumberofself-medication)Variables Simplemodel(1) Fullmodel(2)Age –0.006
(0.005)[0.994]
–0.009(0.006)[0.991]
Male –0.442GGG(0.079)[0.643]
–0.364GGG(0.083)[0.695]
Lowersecondaryschool –0.055(0.139)[0.947]
–0.120(0.149)[0.887]
Highschoolorvocational 0.415GGG(0.097)[1.514]
0.385GGG(0.098)[1.470]
Married 0.449GGG(0.143)[1.567]
0.530GGG(0.167)[1.699]
Employed –3.254GGG(0.816)[0.039]
–2.904GGG(0.832)[0.055]
Logofincome 0.421GGG(0.095)[1.523]
0.387GGG(0.096)[1.473]
Familysize 0.0003(0.031)
[1.0003]Childrennumber –0.294GGG
(0.084)[0.746]
–0.350GGG(0.096)[0.704]
Insurance –0.069(0.103)
22
Note:G= pY= 0.1,GG= pY0.05,GGG= pY= 0.01.Tertiary education isomittedvariable.Standard errors are inparentheses and incidence rate ratios are inbrackets.
[0.933]Distance –0.031GG
(0.015)[0.969]
–0.037GG(0.016)[0.964]
Chronicdisease 0.546GGG(0.113)[1.726]
Closetohealthprofessional –0.191GG(0.076)[0.826]
Doingexercise –0.001(0.020)[0.999]
0.006(0.021)[1.006]
Diet 0.018(0.090)[1.019]
Centralarea –0.248GGG(0.082)[0.780]
Constant 1.140GGG(0.171)[3.127]
1.346GGG(0.246)[3.842]
Loglikelihood –608.480 –587.399PseudoR2 0.076 0.108Observations 241 241
Inanotherpattern,high schoolorvocational,married,and logof incomeare positively related to the frequency of self-medication. In particular,the respondent with having the degree of high school or vocationalcertificate, being married status, or have one more VND 1,000 ofmonthlyincomeisonaveragehasthehighernumberofself-medicationsbyrespectively0.415,0.449,and0.421timescomparedtothecounterpartwith tertiary education, singleorothermaritual status,or less thanonemoreVND1,000ofmonthlyincome.
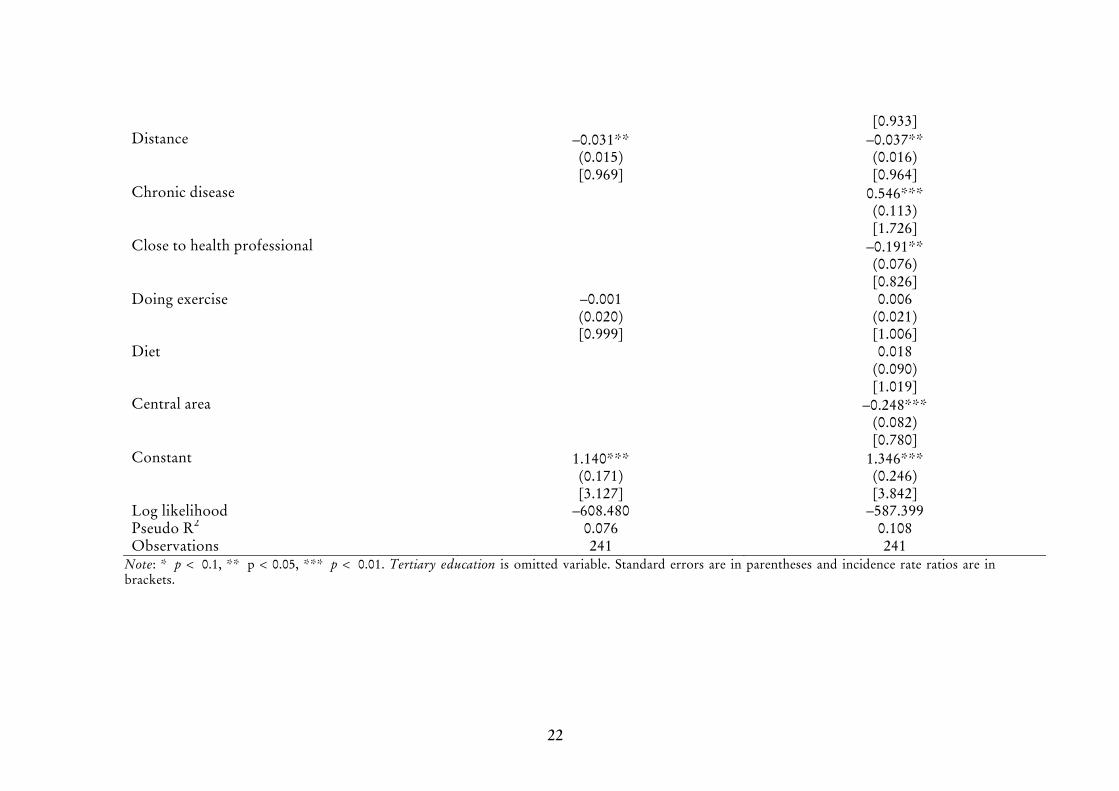
Column (2)ofTable6presents theestimationresults for the fullmodelof Poisson regression. It is apparently that when additional covariatesincluded in the full model, the pattern of estimation results do notchange. This finding can show that the estimation results are highlyrobust.
In particular, among addition variables, chronic disease (pY0.01) ispositively correlated with the frequency of pharmacy visits withoutprescription. The repsondent with having chronic health problems onaverage has more the frequency of self-medication by 0.546 timescomparedtothecounterpartobservation.Onthecontrary,closetohealthprofessional (pY0.05) and central area (pY0.01) decrease the number ofself-medicationby0.191and0.248timesrespectively.Meanwhile,familysiòe, insuranceanddietarestatisticallyinsignificantforanyconventionallevelamongadditionalvariables.
Ingeneral,both simple and fullmodelsofPoisson regression recognizethe important variables that are statistically significant related to thefrequencyofself-medication from thesampleofrespondents inHoChiMinhCity,Vietnam. Inparticular,high school andvocational,married,log of income, and chronic disease are positively associated with thenumber of self-medication. Meanwhile, male, employed, childrennumber, distance, close to health professional, and central area areadversely related to the frequency of self-medication. Other variablesincluding age, lower secondary school, family siòe, insurance, doingeñercise,anddietarestatisticallyinsignificantatanyconventionallevel.
6 ConcludingRemarks

24
Thisstudyshowsthatself-medicationisprevalentasapopulartreatmentfor illnessesamongurbancitizens fromHoChiMinhCity inVietnam,developingcountryinSoutheastAsia.
Thisstudyrecognized importantdeterminantsofself-medicationamongrespondents in Ho Chi Minh City. In particular, the findings indicatethathighschooldegreeorvocationalcertificate,marriedstatus,or largerincome are positively related to the probability of self-medication. Incontrast, being employed, havingmore one child, longer distance fromhometothenearesthospital,doingexercise,livinginacentralregionarenegativelyassociatedwiththeprobabilityofself-medication.
The study also finds that high school and vocational,married, income,and chronicdisease arepositively associatedwith the frequencyof self-medication.Meanwhile,male,employed,childrennumber,distance,closeto health professional, and central area are adversely related to thefrequencyofself-medicationinHoChiMinhCity,Vietnam.
It is important to show that there is a difference in the association ofgender on self-medication using various dependent variables. Whilegender isnotsignificantlyrelated to theprobabilityofsel-medication, itisassociatedwiththefrequencyofself-medicationinHoChiMinhCity,Vietnam.Hencetheimplicationisthechoiceofproxyforself-medicationcanconsiderablyinfluencetheresult.
Apparently, there are some common factors associated with self-medicationasindicatedfromtheexistingliteraturethatarealsofoundinthis study such as employment status (de Moraes et al. 2011), income(Awadetal.2005),schooling level (Awadetal.2005).Importantly, thispaper shows that gender is not significantly associated with theprobabilityof self-medication inVietnam asother studies’ findings, forinstancesdeMoraes et al. (2011) inurbanBrazil,Awad et al. (2005) inSudan,andGarofaloetal.(2015)inurbanItaly.Meanwhile,theresultisthat is respondents with chronic disorders are not associated with theprobability self-medication is supportedby the finding fromdeMoraesetal.(2011)inurbanSouthernBrazil.
Thispaperevidentlyprovidesmore important factson thedeterminantsof self-medicating behaviors from developing countries, especially inurban areaswheremedicines andmedicalproducts arewidely traded inthemarkets.Vietnam is an important and interesting case for investingthisresearch topicbecauseof its’processoftransitionfromtheplanning

25
economy to the market-oriented system including the health careactivities.
The findings from this study alsoprovide some significant implicationsforpublicpolicyinthemanagementofself-medication,especiallyforthedevelopingcountrieslikeVietnam.Firstly,themanagementofqualityofmedicinesandmedicalproductsisimportanttominimizetheside-effectsof self-medication when self-medication as a convenient approach tominorillnessesorhealthproblemsissofarseeminglyunavoidableinthesociety. Secondy, the public provision of necessary information on theguideforself-medicationisalsocrucialforcitizensinordertomaximizethepositive effectsof self-medication anddecreaseor evenbetter avoiditsadverseimpactsaswell.
However, thisstudyalso facesomecertain limitations.Firstly, thesmallsampledoesnotthisstudyallowtoconductmorerobustnesschecksforthe results using various sub-samples based on different ranges orcategories of income, education, location for instance among otherrespondents’ and communities’ characteristics. Secondly, this studyemploysthecross-sectionaldataandthereforeitdoesnotrevealthelong-term trends of self-medicating behaviors of urban citizens. Theselimitations is necessary to be indicated as the research gaps for furtherstudies.
ReferencesAlam, N., Saffoon, N., and Uddin, R. 2015. Self-medication among
medical and pharmacy students in Bangladesh. _j` ResearchNotes8:763.
Awad,A.,Eltayeb, I.,Matowe,L.,andThalib,L.2005.Self-medicationwith Antibiotics and Antimalarials in the community ofKhartoumState,Sudan.gçìêå~ä= çÑ= mÜ~êã~Åó= C= mÜ~êã~ÅÉìíáÅ~ä=pÅáÉåÅÉë8(2):326–331.
Bennadi,D.2014.Self-medication:Acurrentchallenge.gçìêå~ä= çÑ= _~ëáÅ=~åÇ=`äáåáÅ~ä=mÜ~êã~Åó5:19-23.
Chang, F. R., and Trivedi, P. K. 2003. Economics of self-medication:theoryandevidence.HealthEconomics12(9):721-739.
26
CushingH.1925.TheLlifeofSirWilliamOsler (2ndedition).Oxford:OxfordUniversityPress.
deMoraes,A.C.,Delaporte,T.R.,Molena-Fernandes,C.A.,andFalcão,M. C. 2011. Factors associated with medicine use and selfmedication are different in adolescents. CLINICS 66(7): 1149–1155.
Du, Y., and Knopf, H. 2009. Self-medication among children andadolescents in Germany: results of the National Health Surveyfor Children and Adolescents (KiGGS). _êáíáëÜ= gçìêå~ä= çÑ=`äáåáÅ~ä=mÜ~êã~ÅçäçÖó68:599–608.
Eticha T., and Mesfin K. 2014. Self-Medication Practices in Mekelle,Ethiopia.PLoSONE9(5):e97464.
Figueiras, A., Caamano, F., and Gestal-Otero, J. J. 2000. Socio-demographicfactorsrelatedtoself-medicationinSpain.EuropeanJournalofEpidemiology16:19–26.
Garofalo,L.,Giuseppe,G.D.,andAngelillo,I.F.2015.Self-MedicationPracticesamongParentsinItaly._áçjÉÇ= oÉëÉ~êÅÜ= fåíÉêå~íáçå~äKhttp://dx.doi.org/10.1155/2015/580650.
Grigoryan L., Haaijer-Ruskamp F. M., Burgerhof J. G., Mechtler R.,DeschepperR.,Tambic-AndrasevicA.,AndrajatiR.,MonnetD.L., Cunney R., Di Matteo A., Edelsein H., Valinteliene R.,Alkerwi A., Scicluna E., Grzesiowski P., Bara A. C., Tesar T.,CizmanM.,CamposJ.,LundborgC.S.,andBirkinJ.2006.Self-
medication with antimicrobial drugs in Europe. EmergingInfectiousDiseases12:452–459.
Grigoryan, L., Burgerhof, J. G. M., Degener, J. E., Deschepper, R.,Lundborg,C. S.,Monnet,D.L., Scicluna,E.A.,Birkin J., andHaaijer-Ruskamp, F. M. 2008. Determinants of self-medicationwithantibiotics inEurope: the impactofbeliefs,countrywealthand the healthcare system. Journal of AntimicrobialChemotherapy61:1172–1179.
Gyawali,S.,Shankar,P.R.,Poudel,P.P.,andSaha,A.2015.Knowledge,Attitude and Practice of Self-Medication Among Basic ScienceUndergraduateMedicalStudents inaMedicalSchool inWesternNepal. JournalofClinicalandDiagnosticResearch9(12):FC17-FC22.
27
Hernandez-Juyol,M., and Job-Quesada J.R. 2002.Dentistry and self-
medication:Acurrentchallenge.MedOral7:344–347.
JonesR.V. 1976. Self-medication in a small community. Journal of theRoyalCollegeofGeneralPractitioners26:410-413.
Nunes deMelo,M.,Madureira,B.,NunesFerreira,A.P.,Mendes,Z.,Miranda Ada, C., and Martins, A. P. 2006. Prevalence of self-medication in rural areas of Portugal. Pharmacy World andScience28(1):19-25.
Pavyde ̇,E.,Veikutis,V.,Mačiulienė,A.,Mačiulis,V.,Petrikonis,K.,andStankevičiusE.2015.PublicKnowledge,BeliefsandBehavioronAntibiotic Use and Self-Medication in Lithuania. InternationalJournalofEnvironmentalResearchandPublicHealth12:7002-7016.
Ramalhinho,I.,Cordeiro,C.,Cavaco,A.,andCabrita,J.2014.Assessingdeterminants of self-medication with antibiotics amongPortuguesepeopleintheAlgarveRegionInternationalJournalofClinicalPharmacy36:1039–1047.
Setiawan,E.,Hasanbasri,M.,andTrisnantoro,L.2012.Howshouldthehealth system react to informal drug dispensaries? The case ofself-medication in Yogyakarta Province. _j`= mìÄäáÅ= eÉ~äíÜ12(2):A16.
Shankar,P.R.,ParthaP.,andShenoyN.2002.Selfmedicationandnon-
doctorprescriptionpracticesinPokharavalley,WesternNepal:aquestionnairebasedstudy._j`=c~ãáäó=mê~ÅíáÅÉ3:17.
Shehnaz,S.I.,AgarwalA.K.,andKhanN.2014.Asystematicreviewofself-medication practices among adolescents. Journal ofAdolescentHealth55(4):467-483.
WHO(WorldHealthOrganization).2015.Theroleofthepharmacistinself-care and self-medication. Available from:http://apps.who.int/medicinedocs/pdf/whozip32e/whozip32e.pdf.
WHO(WorldHealthOrganization).1998.Theroleofthepharmacist inself-care and self-medication. Report of the 4th WHOConsultativeGroupon theRoleof thePharmacist,TheHague,TheNetherlands,August.
28
WHO (World Health Organization). 2000a. WHO Guidelines for theregulatory assessment of medicinal products for use in self-medication.WHODrugInformation14(1):18-26.
WHO (World Health Organization). 2000b. The benefits and risks ofself-medication.WHODrugInformation14(1):1-2.
Yusuff,K.B.,andOmarusehe,L.2011.Determinantsofselfmedicationpractices among pregnant women in Ibadan, Nigeria.InternationalJournalofClinicalPharmacy33:868–875.
29
AppendicesAPPENDIX1:STATISTICALDESCRIPTIONSTableA1:Thedistributionofthefrequencyofself-medication
30
TableA2:Thedistributionoftherespondents’income
31
FigureA1:Thepercentageoftypesofillness/healthproblemsusingself-medicationamongrespondents
0 20 40 60 80 100
AchesandpainsCatchingacold
FeverCough
ThroatsymptomsCardiovasculardiseases
RunnynoseDepression/SonastheniaIndigestionsymptoms
DiarrheaEye-relateddisordersHeadachedisorders
InsomniaGastropathyrelateddiseasesDermatologyrelateddiseasesSexuallytransmitteddiseases
AdvancedsterilizationproductsGynecologicdisorders
NutritionsupportingproductsOtherdiseases
32
Figure A2: The percentage of reasons for self-medicating amongrespondents
0 10 20 30 40
Financialconstraints/difficulties
Lowercostscomparedwithhospitals’costs
Longdistancefromhometohospital
Insufficientservicequalityofhospital
Legallyavailablemedicines
33
APPENDIX2:THEQUESTIONNAIREWeare the researchers fromUniversityofEconomicsHoChiMinhCity(UEH).Weareimplementingastudyonhealthcareandthebehaviorofself-medicationamongcitizens.Wewouldliketointerviewyouinorderto elicit related information. We promise that we use surveyedinformation for the scientific purposes andwe do not publicly discloseyourinformation.Doyouagreewithusthesetermsandarewillingtobeourrespondent?�YesàLet’sbegintheinterview�NoàStoptheinterview.Nameofrespondent:Address:Phonenumber:ID:____Nameofemerator:Dateofinterview:Duration:___hour___minute
SECTION1:INFORMATIONONDEMOGRAPHIC-SOCIO-ECONOMICCHARACTERISTICSOFTHERESPONDENT
QUESTION1:Howoldareyou?_____yearsQUESTION2:Whatisyourgender?�Male�Female�Other
34
QUESTION3:Whatisyourschoolingyears?_____yearsQUESTION4:Pleaseindicateyourhighestqualification?
□ Going to primary school butnothavingdegree
□ Going to vocational schoolbutnothavingcertificate
□ Completing and having theprimaryschool’sdegree
□ Completingandhaving thevocational school’scertificate
□ Going secondary school butnothavingdegree
□ Going university but nothavingdegree
□ Completing and having thesecondaryschool’sdegree
□ Completingandhaving thebachelor’sdegree
□ Going high school but nothavingdegree
□ Goingpost-graduateschoolbutnothavingdegree
□ Completing and having thehighschool’sdegree
□ Completingandhaving thepost-graduate’sdegree
QUESTION 5: [For whom has tertiary education] Have you studiedmedicalscienceorrelatedmajor?�Yes�NoQUESTION6:Doyouhavefriendsorrelativeswhowork inthemedicalprofessional(doctor,nursing…)?□Yes□NoQUESTION7:Whatisyourmaritalstatus?□Single□Married□Divorced□OthersQUESTION8:Howmanypeopleyourfamilycurrentlyhas?Familymembernumber:______peopleChildrennumber:____peopleQUESTION9:Whatisyourcurrentemploymentstatus?□Part-timeemployment(self-employmentorpaidjob)□Full-timeemployment(self-employmentorpaidjob)
35
□Unemployment□Retired□Home-working□StudentsQUESTION10:Whatisyourmonthlyaveragelevelofincome?
□ From VND 0 to under VND2,000,000
□ From VND 16,000,000 tounderVND18,000,000
□ From VND 2,000,000 tounderVND4,000,000
□ From VND 18,000,000 tounderVND20,000,000
□ From VND 4,000,000 tounderVND6,000,000
□ From VND 20,000,000 tounderVND22,000,000
□ From VND 6,000,000 tounderVND8,000,000
□ From VND 22,000,000 tounderVND24,000,000
□ From VND 8,000,000 tounderVND10,000,000
□ From VND 24,000,000 tounderVND26,000,000
□ From VND 10,000,000 tounderVND12,000,000
□ From VND 26,000,000 tounderVND28,000,000
□ From VND 12,000,000 tounderVND14,000,000
□ From VND 28,000,000 tounderVND30,000,000
□ From VND 14,000,000 tounderVND16,000,000
□ From VND 30,000,000 andover
QUESTION 11: Do you participate in an organization in medicalactivities/publichealthandhealthcare?□Yes□No□Unknown
SECTION2:SELF-MEDICATIONBEHAVIORSQUESTION12:Didyoufaceanyhealthproblemoverlastyear?�Yes�No�Unknown QUESTION13:Howmanytimesdidyouvisitdoctors(includingstayinghospitals)overlastyear?_____times
36
QUESTION14:Didyoubuymedicinebyyourselfinordertoresolvesomehealthproblems?�Yes�NoQUESTION 15: How many times did you self-medicate from medicineshopsoverlastyear?_____timesQUESTION16:Doyoubuymedicineswithdoctors’prescription?�Yes�NoQUESTION 17: Do you take part in which on among the followinginsurancesystems?�Statesocialinsurance�Privateinsurance�Idon’tbuyinsurance�Idon’tknowQUESTION18:Onaverage,howmuchdidyoucost forone timeofself-medication?VND:_____QUESTION19:Whicharethereasonsforyourself-medications?(Youcanchoosemorethanoneoption)�Financialconstraint/difficulties�Lowercostscomparedwithhospitals’costs�Longdistancefromhometohospital�Insufficientservicequalityofhospital�Legallyavailablemedicines�Otherreasons(pleaseindicate):____________QUESTION20:Whichdiseasedoyouuseself-medicationtotreatfor?�Achesandpains�Catchingacold�Fever�Cough�Throatsymptom�Cardiovasculardisease�Runnynose�Depression/Sonasthenia�Indigestionsymptoms
37
�Diarrhoea�Eye-relateddisorders�Headachedisorders�Insomnia�Gastropathyrelateddiseases�Dermatologyrelateddiseases�Sexuallytransmitteddiseases�AdvancedSterilizationProducts�Gynecologicdisorders�Nutritionsupportingproducts�Other:_______QUESTION21:Wheredoyoubuymedicinesbyyourself?�Pharmacist-ownedstore�Hospital’spharmacystore�Onlinetransaction�Supermarket/gloceries�Other:________QUESTION22:Doyoubuymedicinesfortreatingchronicdisease?�YesàDisease:______�NoQUESTION23:Doyoudoexerices�Yes�No�Idon’tknowQUESTION24:Howaboutyourfrequencyofdoingexercises?�Daily�Everytwo-day�Everyfour-day�Onceaweek�Other:_______QUESTION25:Doyouhavedietforbeingbetterhealth?�Yes�No�Idon’tknow

38