the development and implementation of a direct...
TRANSCRIPT

QUALITY REPORT
69|
AUTHORSJeffrey R. Van Blarcom, MD,1,2 Rajendu Srivastava, MD, FRCP(C), MPH,1 DayValena Colling,3 and Christopher G. Maloney, MD, PhD4,5e
1Department of Pediatrics and 5Division of Pediatric Inpatient Medicine, University of Utah School of Medicine, Salt Lake City, Utah; and 2Division of Inpatient Medicine, 3Department of Information Systems, and 4Associate Chief Medical Offi cer, Primary Children’s Medical Center, Salt Lake City, Utah
KEY WORDScommunication, continuity of care/transitions, teamwork/interprofessional cooperation
ABBREVIATIONSED: emergency department; PCMC: Primary Children’s Medical Center
www.hospitalpediatrics.orgdoi:10.1542/hpeds.2013-0019
Address correspondence to Jeffrey R. Van Blarcom, MD, Department of Pediatrics, Uni-versity of Utah School of Medicine, Division of Inpatient Medicine, Primary Children’s Medical Center, 100 North Mario Capecchi Dr, Salt Lake City, UT 84113. E-mail: [email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154 - 1663; Online, 2154 - 1671).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
Health care reform and changes in the levels and models of reimbursement have resulted in hospitals focusing on effi ciency and examining patient fl ow, especially in emergency departments (EDs). Improving the throughput of patients in the ED has been addressed in various ways, including the development of direct admission systems in which patients needing admission but not emergent care can bypass the ED altogether. The development process of such systems has not been addressed in the medical literature. We review the development and implementation of a direct admission system at a tertiary care hospital, including a review of existing direct admission systems. Our new direct admission system replaced a confusing, ill-defi ned process that was a perceived and later survey-confi rmed source of frustration for all involved and a source of resource waste and delays in care. This study also highlights a collaborative process among hospital personnel, including hospitalists, to address hospital effi ciency in a meaningful way. The described process can be generalized to other hospitals.
Hospitals are under increasing pressure to improve the effi ciency of health care delivery,1 especially in light of national health care reform2 and its impact on hos-pital reimbursement,3 notably a de-emphasis on fee-for-service payment and a movement toward payment based on the quality of the care provided rather than on the quantity of care provided.4 The emphasis on effi ciency has neces-sitated an assessment of hospital admission and occupancy patterns in an effort to optimize patient fl ow (movement of patients into, between, and out of hospital departments and/or units).5,6 Enhancing patient fl ow is of particular importance to emergency departments (EDs), where patient overcrowding has been rec-ognized as a signifi cant problem diminishing ED care delivery capabilities7 and decreasing patient satisfaction.8,9 Patients in the ED awaiting admission reduce overall ED throughput.10,11 This is being addressed in a variety of ways, includ-ing streamlining admission procedures with the creation of innovative admission protocols12,13 and new hospital units such as observation units14,15 and “fast-track” units.16,17 However, there is a paucity of literature describing the development and use of a process to improve patient fl ow in the ED by the direct admission of patients to the inpatient setting, bypassing the ED entirely.
Our hospital recognized an opportunity to optimize a portion of patient fl ow by creating a formalized system for the direct admission of patients to the inpatient setting. The opportunity for improvement became apparent from anecdotal direct admission process concerns voiced by ED and referring physicians and from a survey of referring physicians, who acknowledged that many patients felt to need admission but not emergent care were unnecessarily being sent to the ED.
The objective of our quality improvement study was to design and implement a direct admission system to improve patient fl ow and referring physician satisfaction.
The Development and Implementation of a Direct Admission System at a Tertiary Care Hospital
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
70 | VOLUME 4 • ISSUE 2 www.hospitalpediatrics.org
METHODSSetting
The intervention was conducted at Primary Children’s Medical Center (PCMC), an academic children’s hospital in Salt Lake City, affi liated with the Department of Pediatrics, University of Utah. PCMC is a 289-bed hospital serving as a community pedi-atric hospital for Salt Lake County and a tertiary care pediatric hospital for Utah, Wyoming, Idaho, Montana, and Nevada. PCMC is owned and oper-ated by Intermountain Healthcare, a regional, nonprofi t, integrated health care delivery system.18
Planning the Intervention
A direct admission project team was assembled in 2006 to investigate the scope of the problem. Regular team members included stakeholders in the admission process at PCMC: the associate medical director, the chief nursing offi cer, a nursing supervisor, 2 individuals from the systems improve-ment department, an ED physician, and a pediatric resident. Several ad hoc consultants were involved, including a pediatric critical care physician, a refer-ring physician, an education specialist, and individuals from hospital informa-tion systems and telecommunications.
A questionnaire regarding admis-sions to PCMC was developed and distributed to referring physicians (physicians noted to be the primary care provider or referring physician of record for ≥2 inpatients at PCMC in the 12 months before the survey) via electronic and standard mail. A Likert scale was used to gauge their satisfac-tion with the process of directly admit-ting patients to PCMC compared with admitting patients by sending them to
the ED. Free-text comments were also elicited.
Representatives of each stakeholder group were interviewed about direct admissions at PCMC. Stakeholder interviewees were identifi ed differ-ently depending on stakeholder group.
Each referring physician who had fi led an unsolicited direct admission related complaint was interviewed, along with a convenience sample of interviewees from each of these stakeholder groups: hospital administration, hospitalists, ED leadership (nursing and physi-cian), nursing supervisors, housestaff, and referring physicians who had not fi led complaints. Twenty-three inter-views were conducted. Interviewee responses were condensed into 2 principle concerns.
The fi rst principle concern was “inef-fi cient contacts,” which referred to the numerous and variably produc-tive phone calls made by referring physicians in their attempts to facili-tate a direct admission through vari-ous PCMC personnel, none of whom seemed enabled to make admission decisions. The second principle con-cern was referring physicians’ feel-ings of being disrespected by PCMC personnel.
The preintervention direct admis-sion process at PCMC was defi ned, including the role of each stakeholder group and the process decisions made. Interviews of individuals of each stakeholder group were performed, as noted, as were direct observations of stakeholders in the process of facili-tating direct admissions. Stakeholders’ diffi culties and concerns were docu-mented, and time and case volume data were obtained. The project team produced a diagram that displayed the
multiple contacts and time needed to perform a direct admission (Fig 1). In light of the collected data, the project team determined that a formalized direct admission system was needed.
Direct admission systems in existence at other hospitals were identifi ed. Representatives from these hospi-tals were interviewed by telephone. A comparison of the identifi ed systems is presented in Table 1.
The direct admission project team had the responsibility of selecting the most appropriate system to test for the intervention, implementing a sys-tem, and overseeing the system after implementation.
Several key principles were estab-lished for the direct admission process. A system that operated 24 hours a day, 7 days a week was desired because this was felt to be the most convenient for referring physicians. The deci-sion to admit the patient was left in the hands of the referring physician, who was considered an expert on the needs of the patient. The “admissions offi cer” (the on-call hospitalist) was considered an expert on the hospital’s resources and ability to provide for the needs of the patient as conveyed by the referring physician. Also, it was felt that the experience and knowledge of the involved parties were suffi cient to determine the needs of the patient, so the core project team did not require that the patient be seen within a cer-tain time frame before direct admission and did not standardize the interroga-tion of the referring physician by the admissions offi cer.
The Intervention
A call center system, in which cus-tomer service representatives act as a hub connecting all other necessary
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
71|
personnel, was chosen. This sys-tem model addressed the needs of referring physicians, fi t our existing resources best, and was the least expensive to implement and oper-ate with those existing resources. In addition, the project team felt that this type of system, which more heavily involves a physician, was superior in that it allows for direct communica-tion between the referring physician and the accepting physician, which likely results in better patient hand-offs. Other noted advantages of this type of system were its timeliness, ability to standardize calls, and ease of record keeping, especially the record-ing of calls. Disadvantages were a lack
of medical knowledge of the initial call taker, the possibility of a low volume of calls that would not merit continuous clerical staffi ng, and a risk of confu-sion due to multiple individuals enter-ing and exiting the conversation at different times.
Several of the resources necessary for a call center system already existed at PCMC. An in-house physician group (the University of Utah Division of Pediatric Inpatient Medicine) was will-ing to provide the needed round-the-clock physician resources. A readily accessible call center (the Intermoun-tain Healthcare Physician Referral Center) was willing to contract with PCMC for services and to provide
system-specifi c clerical personnel and the necessary training. The PCMC nurs-ing supervisors, with their real-time knowledge of bed space and nurs-ing resources, were willing to provide round-the-clock nursing coverage. An information tracking system (Patient Tracker)20 was in use at PCMC and was accessible to all involved person-nel. Patient Tracker was fl exible and allowed for a new module and soft-ware to be added for the new system.
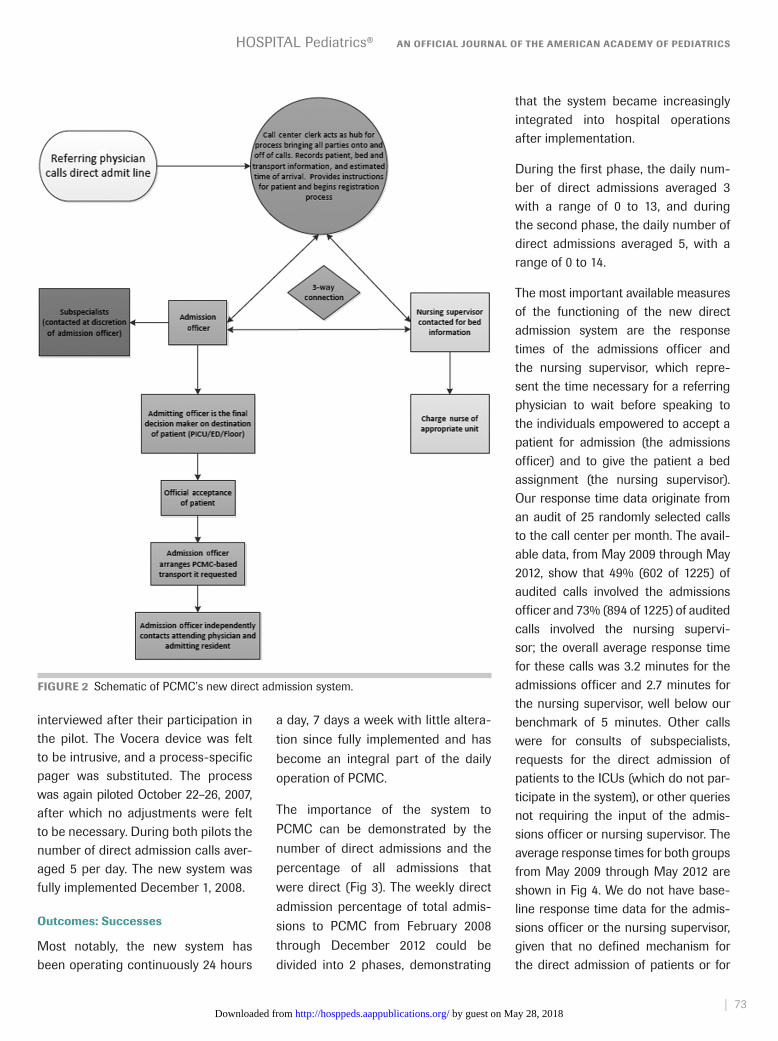
The new system is detailed in Fig 2. A recognizable and memorable phone number was chosen (801-66ADMIT). To engage the new system, refer-ring physicians phoned the call cen-ter and spoke with a dispatcher, who
FIGURE 1 Diagram of the contacts and time involved in facilitating a direct admission at PCMC before our intervention. AR, attending resident; NS, nurse supervisor.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
72 | VOLUME 4 • ISSUE 2 www.hospitalpediatrics.org
took primary responsibility for the caller. The dispatcher simultaneously paged the nursing supervisor and contacted the admissions offi cer via a hands-free communication device (Vocera, Vocera Communications, San Jose, CA). The referring physician, the admissions offi cer, and the nurs-ing supervisor were connected by the dispatcher and discussed the needs of the patient, including transporta-tion. The admissions offi cer recorded patient-specifi c clinical information, and the nursing supervisor recorded the patient’s disposition and any spe-cial care needs in Patient Tracker. If the patient was to arrive on foot or by car, he or she was directed to the admit-ting offi ce at PCMC. If the patient was to be transported by PCMC-based Life Flight,21 the on-call pediatric critical care physician was contacted in his or her role as the “control physician” for the patient’s transport because of his
or her ability to stay in contact with the transport team via radio equipment not readily available to the admissions offi cer.
Implementation Plan
The new system was piloted dur-ing daytime hours for 5 sequential days to identify problems and make adjustments, followed by another 5 sequential days to fi nalize the pro-cess. The new system was then fully implemented.
The Study of the Intervention
The project team was charged with the ongoing evaluation of the new system. Criteria to evaluate the suc-cess of the new system and optimize performance were developed and incorporated into a scorecard that was updated and reviewed quarterly. The performance measures centered on the completeness and accuracy of information gathering and distribution
and the response times of the nursing supervisor and the admissions offi cer (from initial page to return call to the call center). A benchmark of 5 min-utes was set for the response time of the admissions offi cer and the nurs-ing supervisor. A follow-up e-mail and paper questionnaire regarding direct admissions at PCMC (again using Likert scale scoring) was dis-tributed to 629 referring physicians 26 months after the system was fully implemented.
RESULTSImplementation
The new direct admission system was piloted during daytime hours September 10–14, 2007. The new sys-tem was well received by the 4 par-ticipating referring physicians and was felt to function well by the par-ticipating admissions offi cer and nursing supervisor, all of whom were
TABLE 1 Comparison of Tasks, Personnel, and Relative Cost for Identifi ed Direct Admission Systems
Task
Call Center System Triage Center System Triage Physician System
Hospital Traffi c Control System
CSR NS AP TN NR AP HO NS TP NS TP
Takes initial call x x x xTakes responsibility for caller x x x xRecords patient demographic information in database
x x x x
Contacts NS and AP x xContacts NS and TP xContacts TP xMakes decision to admit or not x x x xMakes decision on which service to contact to attend
x x x x
Assigns bed, notifi es unit nursing staff
x x x x
Coordinates transport x x x xContacts hospital admitting offi ce
x x x x
Sends confi rmation of placement to referring
physician
x x x x
Relative cost $ $$ $$$ $$$Call center system: such systems were used by Intermountain Healthcare’s Physician Referral Center and the University of New Mexico. Triage center system: such systems were used by the University of Utah Hospitals; Sacred Heart Children’s Hospital, Pensacola, FL; and Exempla Good Samaritan Medical Center, Lafayette, CO. Triage physician system: this system was used at Cincinnati Children’s Hospital, Cincinnati, OH. Hospital traffi c control system: a system proposed by the University of Utah Pediatric Inpatient Medicine Group. AP, attending physician; CSR, customer service representative; HO, hospital operator; NS, nurse supervisor; TN, triage nurse; TP, triage physician.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from
HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
73|
interviewed after their participation in the pilot. The Vocera device was felt to be intrusive, and a process-specifi c pager was substituted. The process was again piloted October 22–26, 2007, after which no adjustments were felt to be necessary. During both pilots the number of direct admission calls aver-aged 5 per day. The new system was fully implemented December 1, 2008.
Outcomes: Successes
Most notably, the new system has been operating continuously 24 hours
a day, 7 days a week with little altera-tion since fully implemented and has become an integral part of the daily operation of PCMC.
The importance of the system to PCMC can be demonstrated by the number of direct admissions and the percentage of all admissions that were direct (Fig 3). The weekly direct admission percentage of total admis-sions to PCMC from February 2008 through December 2012 could be divided into 2 phases, demonstrating
that the system became increasingly integrated into hospital operations after implementation.
During the fi rst phase, the daily num-ber of direct admissions averaged 3 with a range of 0 to 13, and during the second phase, the daily number of direct admissions averaged 5, with a range of 0 to 14.
The most important available measures of the functioning of the new direct admission system are the response times of the admissions offi cer and the nursing supervisor, which repre-sent the time necessary for a referring physician to wait before speaking to the individuals empowered to accept a patient for admission (the admissions offi cer) and to give the patient a bed assignment (the nursing supervisor). Our response time data originate from an audit of 25 randomly selected calls to the call center per month. The avail-able data, from May 2009 through May 2012, show that 49% (602 of 1225) of audited calls involved the admissions offi cer and 73% (894 of 1225) of audited calls involved the nursing supervi-sor; the overall average response time for these calls was 3.2 minutes for the admissions offi cer and 2.7 minutes for the nursing supervisor, well below our benchmark of 5 minutes. Other calls were for consults of subspecialists, requests for the direct admission of patients to the ICUs (which do not par-ticipate in the system), or other queries not requiring the input of the admis-sions offi cer or nursing supervisor. The average response times for both groups from May 2009 through May 2012 are shown in Fig 4. We do not have base-line response time data for the admis-sions offi cer or the nursing supervisor, given that no defi ned mechanism for the direct admission of patients or for
FIGURE 2 Schematic of PCMC’s new direct admission system.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
74 | VOLUME 4 • ISSUE 2 www.hospitalpediatrics.org
the measurement of response times existed before the implementation of the new system. However, the available information gathered during the obser-vation of shareholders facilitating direct admissions before the implementation of the new system suggests that the time required for a referring physician to be connected to individuals defi ni-tively empowered to make admission decisions was either much longer than these times, as noted in Fig 3, or could not be measured.
Although the response rate to both surveys was low, the March 2011 follow-up survey addressing referring physician satisfaction with the new direct admission system showed that the responding physicians’ experience of directly admitting patients to PCMC improved (Table 2).
Outcomes: Problems and Solutions
After system implementation, the proj-ect team received reports of directly
admitted patients who had been transferred to the ICU immediately or shortly after direct admission, raising the concern that some patients had been inappropriately triaged by the system to the inpatient units instead of the ICU. These reports came through the hospital’s adverse event reporting system, for which a case review trigger is the unplanned transfer of a patient to the ICU within 12 hours of admission. Admission offi cers were subsequently encouraged to obtain vital signs on the patients to be directly admitted to identify potentially unstable patients and route them to the ED or the ICU. Data regarding such instances are being collected with the intention of optimizing patient triage if problematic patterns are recognized.
DISCUSSIONDirect admission systems have been developed at many hospitals but the process of how this was done and the effects that the systems have
had have not been well documented. Through an investigation and analysis of direct admission systems existing at other hospitals and an evaluation of our existing resources, a team of stakeholders successfully designed and implemented a new direct admis-sion system for PCMC. Our new sys-tem replaced a confusing process that was ineffi cient and not user-friendly. Available survey data suggest that referring physician satisfaction has improved, and available response time data suggest that referring physicians need to wait, on average, <5 minutes to speak to those empowered to facili-tate a direct admission at PCMC.
We believe that our process of devel-oping a direct admission system by using quality improvement methodol-ogy can be duplicated at other hospi-tals and can thereby improve a portion of a hospital’s patient fl ow. We have documented several system types that may serve as models. Our system was
FIGURE 3 Phased weekly direct admission percentage of total admissions to PCMC, February 2008 through December 2012.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
75|
modeled after an existing system used at a large integrated health care deliv-ery system (Intermountain Healthcare) by using a locally developed clinical information tracking system (Patient Tracker); other system models may be more appropriate to other institutions given existing resources.
Ongoing evaluation is required to ensure that our system is functioning optimally and that referring physician satisfaction continues to improve. Modifi cation of the system may be necessary in the future to optimize patient triage; in particular, the identifi cation of children who would be more appropriately admitted to the ICU.
Our study highlights a collaborative effort among hospital personnel to improve systems within the hospi-tal. Being hospital based, hospitalist
groups have a vested interest in the functioning of hospital operations, including those that involve patient fl ow. As such, the hospitalist group at PCMC was involved in the identifi cation of our direct admission problem and later in the development and integra-tion of a new direct admission system into hospital operations. The increas-ing role of hospitalists has afforded opportunities for services within hospi-tals to cooperate to optimize resource utilization22,23 and to improve patient care.24–26 Collaboration involving hos-pitalists and ED physicians, in particu-lar, has become increasingly important given how their interaction can have a large effect on hospital effi ciency.27
Optimization of the interaction has been undertaken in different ways and has had positive effects on hospital
FIGURE 4 Average monthly response times of the admissions offi cer and nursing supervisor, May 2009 through May 2012.
throughput and patient satisfaction. Chadaga et al developed a hospi-tal medicine ED team that improved patient fl ow in a tertiary care aca-demic center.28 Howell et al improved ED patient fl ow by incorporating hospitalist-led “bed management rounds” in the ICU and active facili-tation of admissions from the ED.29 A combined pediatric ED/inpatient unit that has had positive effects on throughput, billing, and patient satis-faction was developed at a community hospital by Krugman et al.30 These studies highlight the unique position hospitalists occupy and their ability to fi ll new roles and facilitate collaboration to improve hospital effi ciency.31 Although our intervention does not involve ongo-ing collaboration between the ED and the hospitalist group, it was developed with input from both groups.
The documentation of existing direct admission systems and the develop-ment of our system add to the growing focus on hospital throughput and its relation to resource utilization. Further analysis of hospital admission sys-tems, including direct admission sys-tems, would be valuable to the health care community.
Our study has a number of limita-tions. Objectively measuring the suc-cess of our new system has been limited by a lack of data before the intervention. The baseline number of direct admissions and ED vis-its by nonemergent patients felt to need admission before the interven-tion could not be established. Data were also not available to show the time that referring physicians and hospital personnel spent facilitating direct admissions to PCMC before implementation. The total amount of time required to facilitate a direct
TABLE 2 Follow-up Survey Questions
2006 (n = 110), n (%) 2011 (n = 140), n (%) P
Question 1: The ease of the process of directly
admitting patients for inpatient care
Poor or fair 54 (49) 32 (23) <.01 Good, very good, or excellent 56 (51) 108 (77) <.01Question 2: Being able to admit patients for inpatient
care as soon as they need it Poor or fair 33 (30) 18 (13) <.01 Good, very good, or excellent 77 (70) 122 (84) <.01
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
76 | VOLUME 4 • ISSUE 2 www.hospitalpediatrics.org
admission after implementation has not been adequately tracked, so some of the effi ciency of the system cannot be assessed. Given the variability of calls, most notably the variability in a patient’s medical complexity, such time data may not be instructive. The measure of referring physician impressions of the new system was limited by the use of a nonvalidated survey instrument. Although the sur-vey results showed statistical signifi -cance, they may not be refl ective of the referring physicians as a whole because of the low response rates. Arguably the biggest impact of the system is its effect on hospital effi -ciency, particularly in the ED, but this cannot be adequately quantifi ed.
CONCLUSIONSWe have developed a system for the direct admission of patients that has become an integral part of daily opera-tions at PCMC and has improved referring physician satisfaction. We used quality improvement methods to assess the scope of the problem and assembled a varied stakeholder group to design, implement, and evaluate a new direct admission system. Although it is diffi cult to capture preinterven-tion data with this type of intervention, we believe that other programs intent on improving their hospital through-put may fi nd that this study provides guidance.
REFERENCES
1. Chassin MR, Galvin RW. Institute of
Medicine National Roundtable on
Health Care Quality. The urgent need
to improve health care quality. JAMA.
1998;280(11):1000–1005.
2. Goldsmith J. Managing the risks: healthcare
reform’s challenge to hospitals. Healthc
Financ Manage. 2010;64(7):46–50.
3. Mulvany C. Healthcare reform: the good,
the bad, and the transformational. Healthc
Financ Manage. 2010;64(6):52–59.
4. Mayes R. Moving (realistically) from
volume-based to value-based health care
payment in the USA: starting with Medicare
payment policy. J Health Serv Res Policy.
2011;16(4):249–251.
5. Fieldston ES, Ragavan M, Jayaraman B,
Allebach K, Pati S, Metlay JP. Scheduled
admissions and high occupancy at
a children’s hospital. J Hosp Med.
2011;6(2):81–87.
6. Fugate T, Kirby BA, Tackett R. Patient fl ow
takes on new importance with health care
reform. Hosp Case Manag. 2010;18(7):97–
99.
7. Derlet RW, Richards JR. Overcrowding
in the nation’s emergency departments:
complex causes and disturbing effects. Ann
Emerg Med. 2000;35(1):63–68.
8. Probus D, Peach S. Lean-driven
improvements slash wait times, drive up
patient satisfaction scores. ED Manag.
2012;24(7):79–81.
9. Mason D. Slash door-to-doc time, boost
patient approval. Hosp Case Manag.
2011;19(9):142–143.
10. Bazarian JJ, Schneider SM, Newman VJ,
Chodosh J. Do admitted patients held in
the emergency department impact the
throughput of treat-and-release patients?
Acad Emerg Med. 1996;3(12):1113–1118.
11. Paul JA, Lin L. Models for improving
patient throughput and waiting at hospital
emergency departments. J Emerg Med.
2012;43(6):1119–1126.
12. Amarasingham R, Swanson TS, Treichler
DB, Amarasingham SN, Reed WG. A rapid
admission protocol to reduce emergency
department boarding times. Qual Saf Health
Care. 2010;19(3):200–204.
13. Howell EE, Bessman ES, Rubin HR.
Hospitalists and an innovative emergency
department admission process. J Gen
Intern Med. 2004;19(3):266–268.
14. Macy ML, Hall M, Shah SS, et al. Pediatric
observation status: are we overlooking a
growing population in children’s hospitals?
J Hosp Med. 2012;7(7):530–536.
15. Macy ML, Kim CS, Sasson C, Lozon MM,
Davis MM. Pediatric observation units in
the United States: a systematic review. J
Hosp Med. 2010;5(3):172–182.
16. Simon HK, McLario D, Daily R, Lanese C,
Castillo J, Wright J. “Fast tracking” patients
in an urban pediatric emergency depart-
ment. Am J Emerg Med. 1996;14(3):242–244.
17. Rodi SW, Grau MV, Orsini CM. Evaluation of
a fast track unit: alignment of resources and
demand results in improved satisfaction
and decreased length of stay for emergency
department patients. Qual Manag Health
Care. 2006;15(3):163–170.
18. Clayton P, Narus S, Huff S, et al. Building
a comprehensive clinical information
system from components: the approach
at Intermountain Health Care. Methods Inf
Med. 2003;42:1–7.
19. Guinane CS, Sikes JI, Wilson RK.
Using the PDSA cycle to standardize a
quality assurance program in a quality
improvement-driven environment. Jt Comm
J Qual Improv. 1994;20(12):696–705.
20. Maloney CG, Wolfe D, Gesteland PH,
Hales JW, Nkoy FL. A tool for improving
patient discharge process and hospital
communication practices: the “Patient
Tracker.” AMIA Annu Symp Proc.
2007;11:493–497.
21. Holleran RS, Linsler R. Pediatric transport
team: Intermountain Life Flight. Pediatr
Emerg Care. 2006;22(5):374–378.
22. Auerbach AD, Wachter RM, Cheng HQ,
et al. Comanagement of surgical patients
between neurosurgeons and hospitalists.
Arch Intern Med. 2010;170(22):2004–
2010.
23. Cowan MJ, Shapiro M, Hays RD, et al. The
effect of a multidisciplinary hospitalist/
physician and advanced practice nurse
collaboration on hospital costs. J Nurs
Adm. 2006;36(2):79–85.
24. Hemerson P, Izakovic M. Hospitalist-
pharmacist collaboration. A success story
of the integration of a clinical pharmacist
on the multidisciplinary hospitalist team.
Bratisl Lek Listy (Tlacene Vyd). 2011;112(2):
88–91.
25. Sennour Y, Counsell SR, Jones J, Weiner
M. Development and implementation of a
proactive geriatrics consultation model in
collaboration with hospitalists. J Am Geriatr
Soc. 2009;57(11):2139–2145.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

HOSPITAL Pediatrics® AN OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
77|
department team: associations with
throughput, timeliness of patient care, and
satisfaction. J Hosp Med. 2012;7(7):562–566.
29. Howell E, Bessman E, Kravet S, Kolodner
K, Marshall R, Wright S. Active bed
management by hospitalists and emergency
department throughput. Ann Intern Med.
2008;149(11):804–811.
26. Whelan CT. Interventional radiology and the
hospitalist: an opportunity for collaboration.
Semin Intervent Radiol. 2006;23(4):346–349.
27. Pollack CV Jr, Amin A, Talan DA. Emergency
medicine and hospital medicine: a call for
collaboration. Am J Med. 2012;125(8):e1–e6.
28. Chadaga SR, Shockley L, Keniston A,
et al. Hospitalist-led medicine emergency
30. Krugman SD, Suggs A, Photowala HY, Beck
A. Redefi ning the community pediatric hos-
pitalist: the combined pediatric ED/inpatient
unit. Pediatr Emerg Care. 2007;23(1):33–37.
31. Chadaga SR, Maher MP, Maller N, et al.
Evolving practice of hospital medicine
and its impact on hospital throughput and
effi ciencies. J Hosp Med. 2012;7(8):649–654.
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2013-00192014;4;69Hospital Pediatrics
MaloneyJeffrey R. Van Blarcom, Rajendu Srivastava, DayValena Colling and Christopher G.
Tertiary Care HospitalThe Development and Implementation of a Direct Admission System at a
ServicesUpdated Information &
http://hosppeds.aappublications.org/content/4/2/69including high resolution figures, can be found at:
Referenceshttp://hosppeds.aappublications.org/content/4/2/69#BIBLThis article cites 31 articles, 1 of which you can access for free at:
Subspecialty Collections
al_-_communication_skills_subhttp://classic.hosppeds.aappublications.org/cgi/collection/interpersonInterpersonal & Communication Skillsedicine_subhttp://classic.hosppeds.aappublications.org/cgi/collection/hospital_mHospital Medicineof_care_transition_-_discharge_planning_subhttp://classic.hosppeds.aappublications.org/cgi/collection/continuity_Continuity of Care Transition & Discharge Planningion:practice_management_subhttp://classic.hosppeds.aappublications.org/cgi/collection/administratAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
mlhttp://classic.hosppeds.aappublications.org/site/misc/Permissions.xhtin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.hosppeds.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2013-00192014;4;69Hospital Pediatrics
MaloneyJeffrey R. Van Blarcom, Rajendu Srivastava, DayValena Colling and Christopher G.
Tertiary Care HospitalThe Development and Implementation of a Direct Admission System at a
http://hosppeds.aappublications.org/content/4/2/69located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 2154-1663. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 2012. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on May 28, 2018http://hosppeds.aappublications.org/Downloaded from