the development of a severity scale for erythema nodosum ... · 332 0305-7518/16/064053+15 $1.00 q...
TRANSCRIPT

The development of a severity scale for
Erythema Nodosum Leprosum – the
ENLIST ENL severity scale
STEPHEN L. WALKER*, KIRSTY L. KNIGHT**,
VIVEK V. PAI***, PETER G. NICHOLLS****,
MEDHI ALINDA*****, C. RUTH BUTLIN******,
JOYDEEPA DARLONG*******, DEANNA A.
HAGGE********, SABA M. LAMBERT*,*********,
M. YULIANTO LISTIAWAN*****,
ARMI MAGHANOY**********, JOSE A.C.
NERY***********, KAPIL D. NEUPANE********,
PITCHAIMANI*******, ANASTASIA POLYCARPOU*,
ANNA M. SALES***********, MAHESH
SHAH******** & DIANA N.J. LOCKWOOD*
on behalf of the Erythema Nodosum Leprosum International STudy
Group^
*Faculty of Infectious and Tropical Diseases, London School of
Hygiene and Tropical Medicine, London, United Kingdom
** Royal United Hospitals Bath NHS Foundation Trust, Bath,
United Kingdom
*** Bombay Leprosy Project, Mumbai, India
**** Faculty of Health Sciences, University of Southampton,
Southampton, United Kingdom
***** Dr Soetomo General Hospital, Surabaya, Indonesia
****** The Leprosy Mission International, Bangladesh
******* The Leprosy Mission Hospital, Purulia, India
******** Anandaban Hospital, Kathmandu, Nepal
********* ALERT Center, Addis Ababa, Ethiopia
********** Leonard Wood Memorial Center for TB and Leprosy
Research, Cebu, Philippines
*********** FIOCRUZ, Rio de Janeiro, Brazil
Accepted for publication 8 June 2016
^ The other members of the Erythema Nodosum Leprosum International STudy (ENLIST) Group at the time ofthe meeting referred to in this manuscript are listed in the acknowledgements.
Correspondence to: Steve Walker, Faculty of Infectious and Tropical Diseases, London School of Hygiene andTropical Medicine, Keppel Street, London WC1E 7HT (e-mail: [email protected])
Lepr Rev (2016) 87, 332–346
332 0305-7518/16/064053+15 $1.00 q Lepra
Summary
Introduction: Erythema nodosum leprosum (ENL) is a severe, multi-system
complication of leprosy which is difficult to manage. The evidence for effective
treatment is limited and defining outcome measures for clinical trials is difficult.
There are no validated measures of disease severity and so we wished to develop a
clinical severity scale.
Methods: Three published scales that had been used in ENL research were applied
to patients with ENL at six leprosy referral centres. An analysis of the clinical features
associated with ENL severity was performed on data obtained from the ENLIST 1
study. A meeting of experienced leprosy researchers was held to incorporate the
findings from the scale testing and data analysis into a clinical severity scale for ENL
Results: None of the three scales used were found to be ideal but some features of
each were incorporated into a new scale along with novel items felt to be appropriate.
A final 16 item scale – the ENLIST ENL Severity Scale was agreed by the meeting
participants and detailed notes and definitions developed.
Conclusions: We have developed a new severity measure for ENL which we
propose to subject to formal validation.
Introduction
Erythema nodosum leprosum (ENL) is a severe, inflammatory, painful, multisystem
complication of lepromatous leprosy. ENL causes significant morbidity. Patients are treated
with immunomodulatory drugs, particularly corticosteroids, which are used for prolonged
periods of many months or years. Many patients require high doses of corticosteroids to
control their disease and this leads to complications and deaths associated with long-term use
of these drugs.1 Thalidomide is very effective but is not available in many countries or is
severely restricted because of the risk of teratogenicity. Affordability may also limit the use
of thalidomide in some countries. The identification of other agents for controlling ENL is a
priority.2
The Erythema Nodosum Leprosum International STudy (ENLIST) Group aims to improve
the understanding of the mechanisms which cause ENL, improve the evidence to guide
treatment decisions of individuals with ENL and improve access to effective treatments.3
The development of a quantitative measure to assess the severity of ENL has been
highlighted as a priority research area.3 A tool which enables clinicians to accurately assess
the severity of ENL would be useful in defining outcomes for clinical trials. It would facilitate
the even distribution of patients with similar disease severity between the arms of clinical
trials. A measure of ENL severity could also be used in treatment guidelines to indicate the
need for therapy. A quantitative measure of ENL severity may be a useful prognostic tool.
Our objective was to critique existing scales and if necessary develop a clinical severity
scale for ENL which could be subjected to formal validation.
Methods
A meeting of leprosy experts from eight leprosy endemic countries was organised by the
ENLIST Group and hosted by the Bombay Leprosy Project in Mumbai, India form 7–9th
ENLIST ENL Severity Scale 333

April 2015.4 The aims of the meeting with respect to developing a severity scale for ENL
included: reviewing the results of the ENLIST 1 study of the clinical features of ENL,
reviewing published severity scales of ENL and agreeing on the scale items to be tested in the
validation of a severity scale of ENL. The 13 clinical leprosy workers who participated in the
scale development at the meeting had a total of 218·5 years (Range 3-30) experience of
working with patients with ENL.
In the 4 weeks prior to the meeting three published severity scales for ENL (see Appendix 3),
none of which had been validated, were applied to patients at leprosy referral centres in five
leprosy endemic countries (Brazil, Ethiopia, India, Nepal and the Philippines). The scales were
chosen because they resulted in a quantitative measure and had featured in publications of
original research of ENL within 10 years of the meeting.
The case definition of ENL employed was a patient diagnosed with leprosy has ENL if
he/she had crops of tender cutaneous or subcutaneous lesions. In the absence of cutaneous
signs ENL could also be diagnosed if a patient with leprosy had fever or malaise and
histological features consistent with ENL in a tissue biopsy.
Each patient with ENL to whom the scales were applied was categorised by another
assessor, an experienced physician who examined them, as having mild, moderate or severe
ENL. No attempt was made to standardise severity assessments between assessors. The
nature of ENL was defined as:
. acute for a single episode lasting less than 24 weeks,
. recurrent if a patient experienced a second or subsequent episode of ENL occurring
28 days or more after stopping treatment for ENL
. chronic if occurring for 24 weeks or more during which a patient has required ENL
treatment either continuously or where any treatment free period had been 27 days or less.1
The assessor who determined the severity of ENL in an individual was blinded to the scores
that had been determined by the other assessor using the three scales. At the meeting, the face
and content validity and ease of application of each scale was discussed. The scales chosen
were: the prototype of the “Reaction Severity Assessment”5 developed as part of the ILEP
Nerve Function Impairment and Reaction (INFIR) Cohort Study,6 the ‘modified Ramu’
scoring system reported in a controlled trial of thalidomide in Chandigarh, India7 and a scale
described by Haslett et al. in a study of the effects of thalidomide in Nepali patients with
ENL.8 In each scale the higher the score the more severe the ENL.
The prototype of the ‘Reaction Severity Assessment’ was used because it had more items
relating to ENL than the final published version.5 We simplified the prototype by removing
two items which referred to the ‘maximum motor impairment’ and the ‘maximum sensory
impairment’. This scale, which we shall refer to as the ‘modified van Brakel’ scale, had 14
items and the range of possible scores was 0 to 64 for males and 0 to 59 for females. Each item
scored 0, 1, 3 or 5 though for three items the maximum score possible was three and for one
item 0, 1 or 5 were the possible scores. Two minor changes were made to the ‘modified
Ramu’ scale. The assessment of temperature was changed from Fahrenheit to Celsius and the
number of affected joints in the ‘arthritis’ item was clarified. The range of scores possible was
0 to 18 in males and 0 to 17 in females. The possible scores for each item are not uniform in
this scale with ranges of possible scores of 0 or 1, 0–2, 0–3 and 0 or 3. The ‘Haslett’ scale
which uses cutaneous signs was not changed and the range of scores possible was 0 to 31.
This scale scored each of seven anatomical regions 0-3 depending on the extent of the
S.L. Walker et al.334

cutaneous lesions of ENL (in terms of the proportion of each region involved). The score was
increased by a further 10 if an individual had ‘blistered, pustular, or ulcerated’ ENL skin
lesions at any site.
We did not attempt to calculate the item to total score correlation of the three scales, their
internal consistency nor reliability.
Data from the cross-sectional ENLIST 1 study were analysed to identify clinical features
of ENL that were significantly associated with severity.9
A new severity scale was then devised incorporating the best of each of the three
published scales and other items the group deemed important. A round table expert discussion
of each component item and the scoring system was conducted and the scale modified until a
consensus was reached. The proposed scale was called the ENLIST ENL Severity Scale.
Detailed notes were taken during this discussion which enabled explanatory notes and
definitions for the scale to be developed.
A pilot exercise in which the draft version of the ENLIST ENL Severity Scale was
applied to patients with ENL in the clinic of the Bombay Leprosy Project from April 18th to
July 2nd 2015 with the objective of ensuring that the scale could be used easily and any areas
of uncertainty clarified prior to a formal validation exercise. The same methodology was
employed as in the earlier work with the three published scales.
The anonymised data were entered into an Excel database and analysed using Stata 14
(StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
The differences between groups was assessed using odds ratios, the Mann Whitney test, Chi
squared test or ANOVA. The level for statistical significance was set at P # 0·05. A
univariate ordered logistic regression analysis of clinical features of ENL in the ENLIST 1
study was followed by a multilevel ordered logistic (MOL) regression analysis using
purposeful selection of those features that achieved P , 0·25 in the univariate analysis.10
The study was routine. The data collected pertained to the standard of care at each centre
and no ethical approval was necessary.
Results
TESTING THE THREE PUBLISHED SCALES
Forty-three patients with a median age of 32 years were examined. There were almost four
times as many men as women studied. The type of ENL and physician determined severity is
recorded in Table 1.
All three scales showed an increase in score as ENL became more severe (Figures 1a, 1b
and 1c). The differences in the scores of patients with mild and moderate disease were
significantly different for each of the three scales (modified van Brakel P ¼ 0·008, modified
Ramu P ¼ 0·018 and Haslett P ¼ 0·01). However only the modified van Brakel scale
demonstrated a statistically significant difference between the scores of patients classified as
having moderately severe ENL and those with severe ENL (P ¼ 0·017).
CRITIQUE OF THE THREE PUBLISHED SCALES BY ENLIST MEETING ATTENDEES
During the group discussion it was felt that some of items used in the ‘modified van Brakel’
were vague such as the distinction between ‘Chronic’, ‘Mild, acute’ and ‘Definite’ for some
items relating to extracutaneous involvement. It was also felt that there was too great a
ENLIST ENL Severity Scale 335

weighting in favour of neurological features. The ‘modified Ramu’ scale was felt to have
good face and content validity but again suffered from imprecise language in the description
of items particularly of the skin. The Haslett scale was felt to lack content validity because it
only included the cutaneous features of ENL. The items in the Haslett scale were felt to be
clear although it was argued by some that attempting to determine the proportion of the area
of a region involved may not be easy (Table 2).
ORDERED LOGISTIC REGRESSION ANALYSIS OF ENLIST 1 DATA
A univariate analysis of the association between ENL severity and the presence of feelings of
depression, new nerve function impairment, any nerve function impairment, fever (greater
than 37·58C), presence of vesicles or bullae or pustules, ulcerated skin lesions, more than 20
ENL skin lesions, the presence of oedema, the presence of oedema at two or more sites,
dactylitis, arthritis, dactylitis and arthritis, orchitis, lymphadenitis, rhinitis, any extra-
cutaneous involvement and severe pain (a score of four or five on the Wong-Baker Pain
Rating Scale11) was performed and presented to the group (Table 3).
Three variables reached statistical significance in the MOL regression analysis: fever,
ENL skin lesions with a vesicular, bullous or pustular morphology and severe pain.
THE ENLIST ENL SEVERITY SCALE
From the discussion a new 14 item scale was drafted which incorporated items and features
from all three scales as well as novel items. The features of ENL that were deemed important
to include in a new scale were: an assessment of pain associated with ENL and a measure of
wellbeing. The new items that were incorporated to reflect these features were a Visual
Analogue Scale (VAS) of pain12 and the Arizona Integrative Outcomes Scale (AIOS) which
is also a VAS.13 The scoring of the responses to the pain VAS were based on published
values14 and for convenience the same system was used for the AIOS although no such values
exist for this tool. Both instruments were to be translated into the relevant languages.
Table 1. Description of patients with ENL and outcome of the three published scales. IQR ¼ interquartile range
Number (n=43) (%)
Modified van Brakel (Median
Score [IQR])
Modified Ramu (Median Score
[IQR])
Haslett (Median Score [IQR])
Male:Female 3·8:1 ------ ------- ------
Median age (years [Range]) 32 [18–75] ------ ------ ------
Physician determined severity
Mild 11 (25·6) 8 [10] 1 [3] 4 [4]
Moderate 11 (25·6) 15 [8] 4 [5] 10 [11]
Severe 21 (48·8) 25 [14] 7 [4] 12 [17]
Type of ENL Acute 11 (25·6) 17 [11] 4 [5] 6 [15]
Recurrent 9 (20·9) 12 [4] 3 [3] 8 [7]
Chronic 23 (53·5) 20 [19] 6 [5] 12 [15]
S.L. Walker et al.336

0
10
20
30
40
Mod
ified
van
Bra
kel S
core
MILD MODERATE SEVERE
0
5
10
15
Mod
ified
Ram
u Sc
ore
MILD MODERATE SEVERE
0
10
20
30
Has
lett
Scor
e
MILD MODERATE SEVERE
(a)
(b)
(c)
Figure 1. a, b, c Scores across severity groups for (a) Modified van Brakel scale, (b) Modified Ramu scale and (c)Haslett scale.
ENLIST ENL Severity Scale 337

The new scale was circulated to all participants and on the final day a consensus meeting
was held where each of the 14 items in the draft scale were discussed in detail including the
scores that should be applied. The outcome was a 16 item scale. An additional item,
urinalysis, was included to reflect renal involvement. Two items representing new motor and
new sensory impairment replaced a single item relating to nerve function impairment (NFI) in
general. ‘New’ for this purpose was defined as NFI occurring since the start of the current
episode of ENL. An ‘episode’ of ENL is the onset of new or deterioration in established ENL
symptoms.
The item for fever was the subject of much discussion. It was accepted that it was an
important item to include. Many patients complain of fever but often no elevation in
temperature is demonstrable at the time of examination. This was an important finding of the
ENLIST 1 study.9 It was agreed that the item should include a score for patient reported
history of fever as well as a documented elevated temperature at the time of the examination.
PILOT STUDY OF THE ENLIST ENL SEVERITY SCALE
The 22 individuals who were included in this part of the study are described below in Table 4.
The scale was deemed to be easy to use in the clinical setting albeit more time consuming
than the three used in the previous exercise.
Table 2. Critique of three published ENL severity scales
Feature of scale Modified van Brakel Modified Ramu Haslett
Face validity Good Good Good
Content validity Good Good Limited
Number of unclear items/Total number of items
5/14 3/8 0/8
Ease of use Simple Simple Very simple
Table 3. Results of multivariate analysis of the clinical features of ENL in the univariate analysis with P , 0·25
ENL severity (Mild-Moderate-Severe
UnivariateOdds Ratio 95% CI P
Proportional Odds Ratio 95% CI P
New nerve function impairment
1·91 0·89–4·09 0·096 1·14 0·6–2·14 0·693
Any nerve function impairment
0·34 0·15–0·81 0·014 0·75 0·4–1·41 0·371
Fever >37·5ºC 6·87 3·15–14·96 <0·001 5·69 2·82–11·46 <0·001
Vesicles/Bullae/Pustules 3·84 1·40–10·56 0·009 3·52 1·59–7·8 0·002
Oedema 0·57 0·29–1·11 0·098 0·76 0·43–1·35 0·344
Oedema at two or more sites
2·32 1·09–4·91 0·028 1·62 0·84–3·14 0·152
Orchitis 2·67 0·85–8·37 0·092 1·98 0·8–4·88 0·139
Any extracutaneous involvement
4·84 1·7–13·79 0·003 2·10 0·99–4·45 0·052
Severe pain 3·09 1·74–5·49 <0·001 3·42 2·07–5·66 <0·001
S.L. Walker et al.338

The median scores of individuals increased as ENL was judged more severe (Figure 2).
There was no statistically significant difference between the scores of those with mild and
moderate ENL (P ¼ 0·088) nor those with moderate and severe disease (P ¼ 0·129).
However there was a significant difference (P ¼ 0·028) when three severity groups were
analysed together.
The only change to the scale following the pilot process was to reverse the AIOS so that
the positive outcome was on the left hand side rather than the right. This was to reduce any
confusion with measuring and scoring the outcomes of the two VASs.
Discussion
We have developed and piloted a new scale for measuring the severity of ENL which builds
on previously published scales to which we are indebted. We acknowledge that the number of
Table 4. Description of patients with ENL and outcome of ENLIST ENL Severity Scale. IQR ¼ interquartile range
Number in pilot study (n=22) (%)
ENLIST ENL Severity Scale (Median Score
[IQR]) (n=21)
Male:Female 6·3:1 ------
Median age (years [Range]) 28 [18–51] ------
Ridley Jopling Borderline lepromatous leprosy
12 (54·5) ------
Lepromatous leprosy 10 (45·5) ------
Physician determined severity
Mild 4 (18·2) 9·5 [4]
Moderate 10 (45·5) 14 [8]
Severe 8 (36·4) 20 [5]
Type of ENL Acute 10 (45·5) 13 [10]
Recurrent 8 (36·4) 18 [5]
Chronic 4 (18·2) 10·5 [5·5]
5
10
15
20
25
ENLI
ST E
NL
Seve
rity
Scal
e Sc
ore
Mild Moderate SevereFigure 2. Scores across severity groups for the prototype ENLIST ENL Severity Scale.
ENLIST ENL Severity Scale 339

individuals in the scale assessment exercise (n ¼ 43) and the pilot exercise (n ¼ 22) is small
and that male patients are over represented compared with our large, previous study,9
however useful information was obtained from both.
During the development of the ENLIST ENL Severity Scale we assessed the utility of
three previously published scales and incorporated elements of them we felt were successful.
The analysis of the ENLIST 1 data also helped inform the scale by demonstrating the
importance of pain as a potential marker of ENL severity. We also took a novel approach by
incorporating a history of fever into the scale in addition to demonstrable fever at the time of
examination.
The 16 item ENLIST ENL Severity Scale is a prototype (see Appendix 1.) and may
change following formal validation when some items may prove to be redundant. The scale is
easy to use but we accept that incorporating two VASs into this severity measure make it
more time consuming. One of the main reasons for piloting the scale was to ensure that there
were no problems with respect to translation and interpretation of the VASs, particularly the
AIOS which has not been validated outside of the United States. One of the advantages of
including a validated measure such as the pain VAS is that it may also serve as an ‘anchor
scale’ along with another gold standard such as expert opinion during a formal validation
study.15
The ENLIST ENL Severity Scale is not currently gender neutral because one item,
‘Orchitis due to ENL’, relates solely to males. During the validation of the scale it will be
important to determine whether this item is useful or not. This will require the analysis to be
conducted for men and women separately in the first instance. Should the item prove to
be indispensable then a male and female version of the scale will be produced. The results of
separate scales will need to be interpreted in light of this. The alternative would be to use a
conversion factor.
We have developed a User Guide of detailed accompanying notes (see Appendix 2.) to
facilitate application of the scale and we will continue to scrutinise and improve these where
necessary.
The ENLIST ENL Severity Scale is now being formally tested to assess validity,
reliability and minimal clinically important difference in six centres affiliated with the
ENLIST Group. We hope that the final scale will prove useful in both laboratory and clinical
research and in the assessment of patients in routine clinical settings.
Acknowledgements
The membership of the ENLIST Group also includes: Marivic Balagon, Shimelis N. Doni,
Annamma John, David Khan, Milton Moraes, Pawan Parajuli, Euzenir Sarno, Digafe
Tsegaye.
Funding
The workshop was funded by the Novartis Foundation with additional support from Cipla.
Dr Walker is supported in part by a grant from the Hospital and Homes of St. Giles.
The funders had no role in study design, data collection and analysis, decision to publish,
or preparation of the manuscript.
S.L. Walker et al.340

References
1 Walker SL, Lebas E, Doni SN et al. The mortality associated with erythema nodosum leprosum in Ethiopia:a retrospective hospital-based study. PLoS Negl Trop Dis, 2014; 8: e2690.
2 Van Veen NH, Lockwood DN, van Brakel WH et al. Interventions for erythema nodosum leprosum. CochraneDatabase Syst Rev, 2009; (3): CD006949.
3 Walker SL, Saunderson P, Kahawita IP, Lockwood DN. International workshop on erythema nodosum leprosum(ENL) - consensus report; the formation of ENLIST, the ENL international study group. Lepr Rev, 2012; 83:396–407.
4 Walker S, Lockwood D. Erythema Nodosum Leprosum International Study Group: 3rd ENLIST Meeting Report,Mumbai, 7th-9th April 2015. Lepr Rev, 2015; 86: 407–411.
5 Feuth M, Brandsma JW, Faber WR et al. Erythema nodosum leprosum in Nepal: a retrospective study of clinicalfeatures and response to treatment with prednisolone or thalidomide. Lepr Rev, 2008; 79: 254–269.
6 van Brakel WH, Nicholls PG, Lockwood DN et al. A scale to assess the severity of leprosy reactions. Lepr Rev,2007; 78: 161–164.
7 Kaur I, Dogra S, Narang T, De D. Comparative efficacy of thalidomide and prednisolone in the treatment ofmoderate to severe erythema nodosum leprosum: a randomized study. Australas J Dermatol, 2009; 50: 181–185.
8 Haslett PA, Roche P, Butlin CR et al. Effective treatment of erythema nodosum leprosum with thalidomide isassociated with immune stimulation. J Infect Dis, 2005; 192: 2045–2053.
9 Walker SL, Balagon M, Darlong J et al. ENLIST 1: An International Multi-centre Cross-sectional Study of theClinical Features of Erythema Nodosum Leprosum. PLoS Negl Trop Dis, 2015; 9: e0004065.
10 Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. SourceCode Biol Med, 2008; 3: 17.
11 Wong DL, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs, 1988; 14: 9–17.12 Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain),
Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill PainQuestionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), andMeasure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken), 2011; 63(Suppl11): S240–252.
13 Bell IR, Cunningham V, Caspi O et al. Development and validation of a new global well-being outcomes ratingscale for integrative medicine research. BMC Complement Altern Med, 2004; 4: 1.
14 Jensen MP, Chen C, Brugger AM. Interpretation of visual analog scale ratings and change scores: a reanalysis oftwo clinical trials of postoperative pain. J Pain, 2003; 4: 407–414.
15 Clark LA, Watson D. Constructing validity: basic issues in objective scale development. PsychologicalAssessment, 1995; 7: 309–319.
ENLIST ENL Severity Scale 341

Appendix 1. ENLIST ENL Severity Scale
ITEM
SCORES
0 1 2 3 SCORE
1 VAS – Pain (mm)
0 1–39 40–69 70–100
2 VAS Wellbeing (mm)
0 1–39 40–69 70–100
3 Fever None (37·5 or less)
No fever now but history of fever in last 7 days
37·6–38·5 38·6 or higher
4 Number of ENL skin lesions
None 1–10 11–20 21 or more
5 Inflammation of ENL skin lesions
Non tender
Redness Painful Complex
6 Extent of ENL skin lesions
0 1–2 regions 3–4 regions 5–7 regions
7 Peripheral oedema
None 1 site of Hands or Feet or Face
2 sites All three sites (Hands and Feet and Face)
8 Bone pain None Present on examina-tion but does not limit activity
Sleep or activitydisturbed
Incapacitating
9 Inflammation of Joints and/or digits due to ENL
None Present on examina-tion but does not limit activity
Sleep or activitydisturbed
Incapacitating
10 Eye inflamma-tion due to ENL
None redness or pain redness and pain
Blurring and/or reduced vision
11 Orchitis due to ENL
None Tenderness Pain on walking or movement
Pain at rest
12 Lymphadeno-pathy due to ENL
None Enlarged Pain or tenderness
Pain or tender-ness in 2 or more groups
13 Nerve tender-ness due to ENL
None Absent if attention distracted
Present even if attention distracted
Patient with-draws limb on examination
14 Number of nerves with NEW sensory NFI due to ENL
None 1 2 3 or more
15 Number of nerves with NEW motor NFI due to ENL
None 1 2 3 or more
16 Urinalysis for protein
None Trace 1 or 2+ 3+
TOTAL
S.L. Walker et al.342
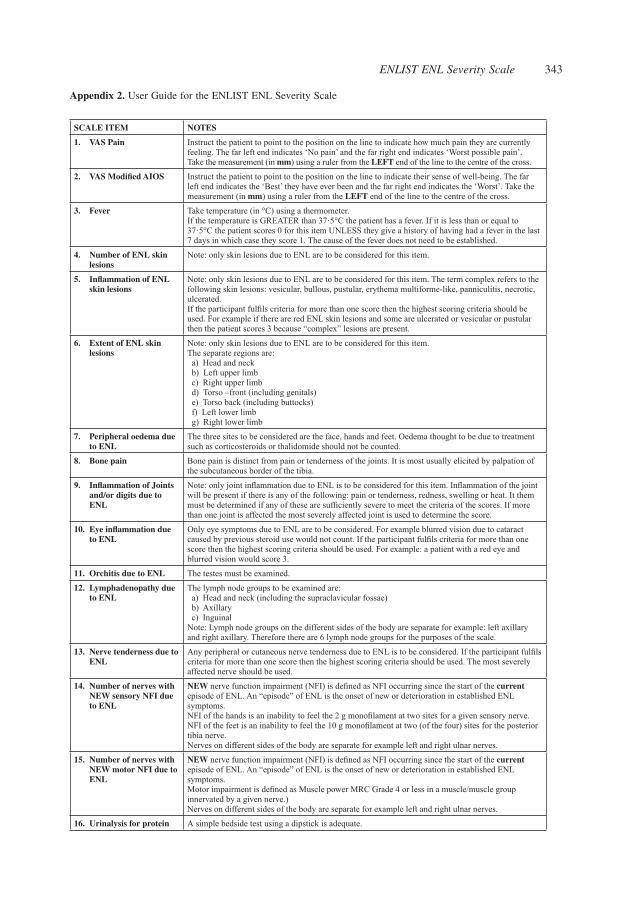
Appendix 2. User Guide for the ENLIST ENL Severity Scale
SCALE ITEM NOTES
1. VAS Pain Instruct the patient to point to the position on the line to indicate how much pain they are currently feeling. The far left end indicates ‘No pain’ and the far right end indicates ‘Worst possible pain’.Take the measurement (in mm) using a ruler from the LEFT end of the line to the centre of the cross.
2. VAS Modified AIOS Instruct the patient to point to the position on the line to indicate their sense of well-being. The far left end indicates the ‘Best’ they have ever been and the far right end indicates the ‘Worst’. Take the measurement (in mm) using a ruler from the LEFT end of the line to the centre of the cross.
3. Fever Take temperature (in °C) using a thermometer. If the temperature is GREATER than 37·5°C the patient has a fever. If it is less than or equal to 37·5°C the patient scores 0 for this item UNLESS they give a history of having had a fever in the last 7 days in which case they score 1. The cause of the fever does not need to be established.
4. Number of ENL skin lesions
Note: only skin lesions due to ENL are to be considered for this item.
5. Inflammation of ENL skin lesions
Note: only skin lesions due to ENL are to be considered for this item. The term complex refers to the following skin lesions: vesicular, bullous, pustular, erythema multiforme-like, panniculitis, necrotic, ulcerated.If the participant fulfils criteria for more than one score then the highest scoring criteria should be used. For example if there are red ENL skin lesions and some are ulcerated or vesicular or pustular then the patient scores 3 because “complex” lesions are present.
6. Extent of ENL skin lesions
Note: only skin lesions due to ENL are to be considered for this item.The separate regions are: a) Head and neck b) Left upper limb c) Right upper limb d) Torso –front (including genitals) e) Torso back (including buttocks) f) Left lower limb g) Right lower limb
7. Peripheral oedema due to ENL
The three sites to be considered are the face, hands and feet. Oedema thought to be due to treatment such as corticosteroids or thalidomide should not be counted.
8. Bone pain Bone pain is distinct from pain or tenderness of the joints. It is most usually elicited by palpation of the subcutaneous border of the tibia.
9. Inflammation of Joints and/or digits due to ENL
Note: only joint inflammation due to ENL is to be considered for this item. Inflammation of the joint will be present if there is any of the following: pain or tenderness, redness, swelling or heat. It them must be determined if any of these are sufficiently severe to meet the criteria of the scores. If more than one joint is affected the most severely affected joint is used to determine the score.
10. Eye inflammation due to ENL
Only eye symptoms due to ENL are to be considered. For example blurred vision due to cataract caused by previous steroid use would not count. If the participant fulfils criteria for more than one score then the highest scoring criteria should be used. For example: a patient with a red eye and blurred vision would score 3.
11. Orchitis due to ENL The testes must be examined.
12. Lymphadenopathy due to ENL
The lymph node groups to be examined are: a) Head and neck (including the supraclavicular fossae) b) Axillary c) InguinalNote: Lymph node groups on the different sides of the body are separate for example: left axillary and right axillary. Therefore there are 6 lymph node groups for the purposes of the scale.
13. Nerve tenderness due to ENL
Any peripheral or cutaneous nerve tenderness due to ENL is to be considered. If the participant fulfils criteria for more than one score then the highest scoring criteria should be used. The most severely affected nerve should be used.
14. Number of nerves with NEW sensory NFI due to ENL
NEW nerve function impairment (NFI) is defined as NFI occurring since the start of the current episode of ENL. An “episode” of ENL is the onset of new or deterioration in established ENL symptoms.NFI of the hands is an inability to feel the 2 g monofilament at two sites for a given sensory nerve.NFI of the feet is an inability to feel the 10 g monofilament at two (of the four) sites for the posterior tibia nerve.Nerves on different sides of the body are separate for example left and right ulnar nerves.
15. Number of nerves with NEW motor NFI due to ENL
NEW nerve function impairment (NFI) is defined as NFI occurring since the start of the current episode of ENL. An “episode” of ENL is the onset of new or deterioration in established ENL symptoms.Motor impairment is defined as Muscle power MRC Grade 4 or less in a muscle/muscle group innervated by a given nerve.)Nerves on different sides of the body are separate for example left and right ulnar nerves.
16. Urinalysis for protein A simple bedside test using a dipstick is adequate.
ENLIST ENL Severity Scale 343

For patients with newly diagnosed ENL, recurrent ENL or those on treatment for ENL
whose symptoms require an increase in current or additional treatment
Acute ENL is a single episode of ENL of less than 24 weeks duration
Recurrent ENL: is a second or subsequent episode of ENL occurring 28 days or more after
stopping treatment for ENL
Chronic ENL: is ENL occurring for 24 weeks or more during which a patient has required
ENL treatment either continuously or where any treatment free period has been 27 days or
less.
Appendix 3. Data collection tool used for the assessment of the three published scales
Details
Gender (Male/Female)
Age (years)
Physician determined Severity (Mild/Moderate/Severe)
Type of ENL (Acute/Recurrent/Chronic)
S.L. Walker et al.344

‘modified’ van Brakel et al. Leprosy Review 2007;78:161-4 (Range Males 0-59, Females 0-54)
ITEM 0 1 3 5 SCORE
Degree of inflammation of nodules
None Tender nodule (s) Painful nodule (s) Ulceration
Number of nodules
None ≤10 >10 >50/uncountable
Inflammation of lymph nodes due to current reaction
None Chronic Mild, acute Definite
Inflammation of joints due to current reaction
None Chronic Mild, acute Definite
Inflammation of eye due to currentreaction
None Chronic Mild, acute Definite
Inflammation of testis due to current reaction
None Chronic Mild, acute Definite
Bone pain due to current reaction
None Chronic Mild, acute Definite
Fever due to reaction (°C)
<37·5 37·5–38·9 >39 ---------
Peripheral oedema due to reaction
None Oedema not affecting function
Oedema affecting function
---------
Number of limbs with peripheral oedema
None 1 2 or more ----------
Nerve pain None Mild, does not limit activity
Sleep or activity disturbed
Incapacitating
Nerve tender-ness on gentle palpation
None Mild tenderness or paraesthesia, absent if attention distracted
Present, even if attention distracted
Severe, patient withdraws limb forcibly
Degree of new nerve enlarge-ment, in nerves previously known to be normal)
No new nerve enlargement or borderline
Definite new enlargement
----------- Nerve abscess
Number of nerves showing recent sensory or motor function impairment
None 1 2 or 3 4 or more
TOTAL
ENLIST ENL Severity Scale 345

“modified Ramu”. Kaur et al. Australasian Journal of Dermatology 2009;51:181-5 (Range Males 0-18, Females 17)
ITEM 0 1 2 3 SCORE
Fever (°C) --------------- 36·9–37·7 37·8–38·8 ≥38·9
Extent of inflammatory skin lesions, that is, exacerbation of lesions, erythema nodosum leprosum etc
--------------- Scattered lesions involv-ing the upper arms/thighs, face or part of the trunk
More extensive lesions affect-ing two limbs (upper/lower limbs), trunk with occasional pustulation
Widespread extensive lesions with postulation and ulceration
Neuritis Absent Neuritis of single nerve
Neuritis of more than one nerve trunk
-----------------
Arthritis Absent ≤2 joints 3–4 joints 5 or more joints
Orchitis Absent Involved --------------- -----------------
Scleritis Absent Involved --------------- -----------------
Lymphadenitis Absent Single node ≤2 cm
More than one node, ≥2·5 cm
-----------------
Internal organ involve-ment (liver/kidney/any other)
Absent ----------------- ----------------- Present
TOTAL
Haslett et al. Journal of Infectious Diseases 2005;192:2045-53 (Range 0-31)
Location of skin lesions Extent of lesions on region involved SCORE
0 1 2 3
HEAD None <25% 25–75% >75%
TORSO – FRONT None <25% 25–75% >75%
TORSO – BACK None <25% 25–75% >75%
LEFT UPPER LIMB None <25% 25–75% >75%
RIGHT UPPER LIMB None <25% 25–75% >75%
LEFT LOWER LIMB None <25% 25–75% >75%
RIGHT LOWER LIMB None <25% 25–75% >75%
SUBTOTAL
Any ulcerated or blistered or pustular skin lesion/s at ANY site?
IF YES ADD 10 POINTS
TOTAL
S.L. Walker et al.346