the distribution and character of glomerular · pdf filedistribution et aspects des...
TRANSCRIPT

Kidney International, Vol. 2 (1972), p. 33—50
The distribution and character of glomerular
deposits in systemic lupus erythematosus
ISABEL DUJOVNE, VICTOR E. POLLAK, CONRAD L. PIRANI and MARTIN G. DILLARD
Department of Pathology and the Renal Division, Department of Medicine,Michael Reese Hospital and Medical Center and the University of Chicago, Pritzker School of Medicine,
Chicago, Illinois
The distribution and character of glomerular deposits in systemiclupus erythematosus. Forty renal biopsy specimens from 24patients with systemic lupus erythematosus were examined indetail to assess the amount, character, and distribution ofdeposits in the glomeruli. Semiquantitative electron microscopicand immunohistologic methods were used. The results werecorrelated with clinical and histological findings. Deposits werenot randomly distributed. Rather, there was some relationshipbetween increasing amounts of subendothelial and mesangialdeposits. Subendothelial deposits were found only in activedisease and were extensive only in the presence of extensivemesangial deposits. Contrary to expectation, there was an inverserelationship between the extent of subendothelial and subepi-thelial deposits. Extensive subendothelial deposits were foundonly with the most active histological changes and three of fourpatients with extensive subendothelial deposits died within weeks.Subendothelial deposits contained a wide variety of plasmaproteins including, not only the immune globulins and D1Cglobulin, but also fibrinogen, albumin, and transferrin. Ingeneral, the clinical course of patients with extensive subepithelialdeposits and intramembranous deposits was benign. Subepithelialdeposits were found to contain only immune globulins and J31Cglobulin. Serial studies revealed the long term persistence ofsubepithelial deposits. By contrast, in patients who survived,subendothelial deposits disappeared with time and treatment.
Distribution et aspects des dépôts glomérulaires dans le lupusérythémateux disséminé. Quarante biopsies rénales chez 24malades atteints de lupus érythémateux disséminé ont étéexaminées en detail afin d'évaluer la quantité, I'aspect et Iadistribution des dépôts dans le glomérule. Des méthodes semi-quantitatives, immunohistologiques et de microscopie électro-nique, ont été employees. Les résultats ont etC correlCs avec lesconstatations cliniques et histologiques. Les dCpôts n'étaient pasdistribuCs au hasard. Ii y avait plutôt une certaine relation entreles importances croissantes des dépôts sous endothéliaux etmésangiaux. Les dépôts sous endothéliaux n'étaient trouvés quedans les lupus actifs et n'étaient Ctendus qu'en presence dedCpôts mésangiaux vastes. Contrairement a toute attente il yavait une relation inverse entre l'importance des depots sous
Received for publication January 3, 1972;accepted in revised form April 3, 1972.© 1972, by the International Society of Nephrology.
33
endothéliaux et sous CpithCliaux. Les depOts sous endothéliauxCtendus n'ont etC trouvés que dans les cas comportant les modi-fications histologiques les plus accentuées et 3 des 4 maladeschez qui ces depOts sous endothéliaux etendus ont été observessont morts en quelques semaines. Les depOts sous endotheliauxcontenaient une grande variété de protCines plasmatiques com-prenant non seulement les immunoglobulines et la D1C globulinemais aussi le fibrinogCne, l'albumine et Ia transferrine. D'unefaçon génCrale, l'évolution clinique des malades ayant des depOtssous épithéliaux Ctendus et des depOts intramembraneux CtaitbCnigne. Les depOts sous épithCliaux ne contenaient que desimmunoglobulines et de la j31C globuline. Les etudes itCrativesont montrC Ia persistance a long terme des depOts sous CpithC-liaux. Au contraire, chez les malades qui ont survécu les depOtssous endotheliaux ont disparu au cours du temps et sous traite-ment.
Renal disease is now regarded as a serious complicationand major cause of death in patients with systemic lupuserythematosus. With the development of the percutaneousrenal biopsy technique it has been possible to study theearly stages of the disease, to correlate clinical and histo-logic findings and to evaluate the effects of treatment [1—6].
Ultrastructural changes observed in lupus nephritisinclude thickening of the glomerular capillary basementmembrane, an increased number of all glomerular cellswith prominence of cytoplasmic organelles, extensiveelectron dense deposits, and fusion of foot processes [6—12].Electron dense deposits are seen in the mesangial and sub-epithelial locations and may be most striking in the sub-endothelial position. The reasons for the variability in theamount and location of the deposits are not yet clearlyunderstood [13]. Organized deposits with a "finger print"pattern are found occasionally [12]. In the endothelialcytoplasm microtubular formations are common [14—16]and are considered by some to be of viral origin.
By immunofluorescence microscopy the presence ofgamma globulin, 1C globulin, and fibrinogen has beenshown in the glomerular lesions of patients with systemic

34 Dujovne et al
lupus erythematosus [17—21]. These observations have ledto the conclusion that the glomerular lesions of systemiclupus erythematosus result from the deposition of circulat-ing immune complexes. This view has been reinforced by thedemonstration that gamma globulin eluted from the gb-meruli contains a higher proportion of antinuclear and anti-DNA activity than does the circulating gamma globulin[22, 23], by the detection in some cases of DNA and anti-DNA in the glomerular deposits [23] and in the circulation[24], and by the association of active renal disease withhigh titers of anti-DNA antibodies and low serum comple-ment levels [25].
In previous studies it has also been shown that certaintypes of histological changes are associated with rapid andprogressive renal disease whereas other changes progresslittle if at all over a period of a few years [4, 6]. It is thepurpose of this paper to describe the amount, characterand distribution of deposits in the glomeruli of kidneysfrom patients with systemic lupus erythematosus and todetermine the relationship between their nature and extenton the one hand, and the clinical and histologic evidencefor active lupus nephritis on the other. Their significancefor prognosis and therapy are also discussed.
Material and Methods
Selection of materialfor study. Systemic lupus erythema-tosus was diagnosed on the basis of a spectrum of clinicaland laboratory findings [1, 4]. Material from patients whowere considered to have unequivocal evidence of systemiclupus erythematosus is included in this paper; that fromany patient in whom the diagnosis was thought to be"probable" or "possible" systemic lupus erythematosusis excluded. Since 1957 we have performed renal biopsieson patients with systemic lupus erythematosus with theobjective of defining whether or not renal disease waspresent and, when present, its precise nature. Biopsies havealso been done to assess the response to treatment. Tissuewas usually, but not invariably, taken and stored for elec-tron microscopic and immunohistologic examination.
The present study demanded semiquantitative analysisof the biopsy specimen by light microscopy and by electronmicroscopy and/or immunohistology. From among thebiopsies taken between 1963 and 1971, only those wereselected in which the material was adequate to performsemiquantitative analyses with at least two, and preferablyall three techniques. Thus, the material reported in thispaper represents only a fraction of the biopsies taken.Tissue from 24 patients was evaluated. In 12 instances asingle biopsy specimen was available while two or morebiopsy specimens were available from the remaining12 patients. Therefore a total of 40 biopsy specimens wereexamined.
Light microscopy. A portion of the tissue was fixed inZenker formalin; sections 2 to 3 g in thickness werestained with hematoxylin and eosin (H & B), alcian blue
periodic acid Schiff (PAS), Masson's trichrome, and silvermethenamine. The sections were analyzed semiquantitativelyand the degree of renal damage and overall activity gradedfrom 0 to 4+, by methods previously described [26, 27].
Electron microscopy. A second portion of tissue wascut into 1 mm cubes, fixed in 2.5% glutaraldehyde, post-fixed in 1 % osmium tetroxide and embedded in Epon.Thick survey sections were stained with toluidine blue.Ultrathin sections were stained with uranyl acetate andlead citrate [27]. At least two glomeruli and, wheneverpossible, three to four glomeruli were studied in the RCAEMU-3 electron microscope. The following features wereanalyzed in every glomerulus to evaluate the cellularchanges, size and location of deposits and the appearanceof the mesangial matrix and of the basement membrane.
1. Endothelial, mesangial and epithelial cells: number ofcells, their nuclei and cytoplasm, mitochondria, rough andsmooth endoplasmic reticulum, the Golgi apparatus andthe presence of vacuoles, cytolysosomes and fibrils. In theendothelial cells the character of the fenestrae and thepresence of microtubular structures was recorded. In thevisceral epithelial cells the appearance of the foot processes(discrete, focal, or diffuse fusion, cellular membrane andvilbous transformation) was evaluated.
2. Mesangial matrix: amount and texture and presenceof collagen fibres.
3. Basement membrane: thickness, contour, texture anddefects (gaps).
4. Electron dense deposits: a semiquantitative methodwas used to evaluate the extent and location of deposits.Completely sclerosed glomeruli were not analyzed. Toobtain an appropriate sample of the nature and extent ofthe deposits, which are often distributed focally and seg-mentally, several low magnification electron micrographswere taken of every glomerulus to cover the entire portionavailable regardless of the findings. Based on their location,four types of electron dense deposits were found: subendo-thelial, intramembranous, subepithelial and mesangial.The extent of each was graded from 0 to 4+ : occasionalvery small or questionable deposits; + =occasional (1 to 2)small but definite deposits; 2 + =several (>3) smalldeposits; 3 + =several (>3) large fused deposits; and4 + = asingle large fused deposit occupying more than 50%of the circumference of a loop or most of the surface of amesangial area. The findings in each capillary loop andmesangial area were graded in this manner. The final gradeassigned for each biopsy was the average of all glomerulistudied which, in turn, was obtained from the grades foreach individual loop or mesangial area.
Immunohistological studies. A third portion of tissue wascut into 1 mm cubes, plunged into isopentane precooled inliquid nitrogen, substituted in acetone, and embedded inparaffin according to the technique of Post [28, 29]. Sec-tions 0.5 l in thickness were cut in the cryostat with aglass knife. They were incubated with antisera prepared inthe rabbit and directed against human albumin, transferrin,

Glomerular deposits in lupus nephritis 35
IgG (y chain), 1gM (js chain), IgA (c chain), icand ? chains,J1C globulin, and fibrinogen. All antisera gave singleprecipitin arcs when tested by immunoelectrophoresis andimmunodiffusion. Some antisera were conjugated withfluorescein isothiocyanate [30] and a single layering techni-que was used. With other antisera a double layering techni-que was employed. The tissue was first incubated with anunconjugated rabbit antiserum and then with a fluoresceinisothiocyanate conjugated goat antirabbit globulin serum.
The sections were examined at magnifications up to1250 x with the Leitz Ortholux microscope using anOsram HBO 200 mercury vapor burner and UG-l andUV absorbing filters. Photographs were taken withAnscochrome ASA 200 film. The findings were describedin detail and the observations summarized in a standardprotocol. Fluorescence was considered to be either absent,present segmentally or focally, or present diffusely. Equi-vocal or faint fluorescence was scored as 0. Thirteenbiopsies were studied by this method.
After the slides were photographed, the coverslips wereremoved and after fixation in 5% glutaraldehyde, the sec-tions were stained with periodic acid-Schiff (PAS)-hema-toxylin; the identical field was then photographed onEktachrome film. Precise localization of proteins wasachieved by comparison of the two photographs of theidentical field. With this thin sectioning technique, it wasusually possible to examine most glomeruli serially withall the antisera used. Positive results were checked byappropriate blocking experiments. After the initial observa-tions had been completed and for purposes of the presentstudy, all paired photographs were re-examined systematic-ally, thereby providing a re-assessment of the accuracy ofstructural localization within the glomerulus.
Five biopsies were studied by a technique making use ofgoat antirabbit globulin serum conjugated with peroxidaseby the technique of Avrameas [31]. The peroxidase markerwas made visible by staining with diamino-benzidine [32].The sections were then stained with PAS-hematoxylin andwere examined by light microscopy. With this techniqueprecise localization of proteins was easily achieved [33].
Four biopsies were examined in duplicate. In the firstlayer several antisera made in the rabbit and directedagainst human proteins were used. The duplicate slideswere then incubated with a goat anti-rabbit globulin serumconjugated either with fluorescein isothiocyanate or withperoxidase. Identical localization of proteins was observedwith both methods.
Results
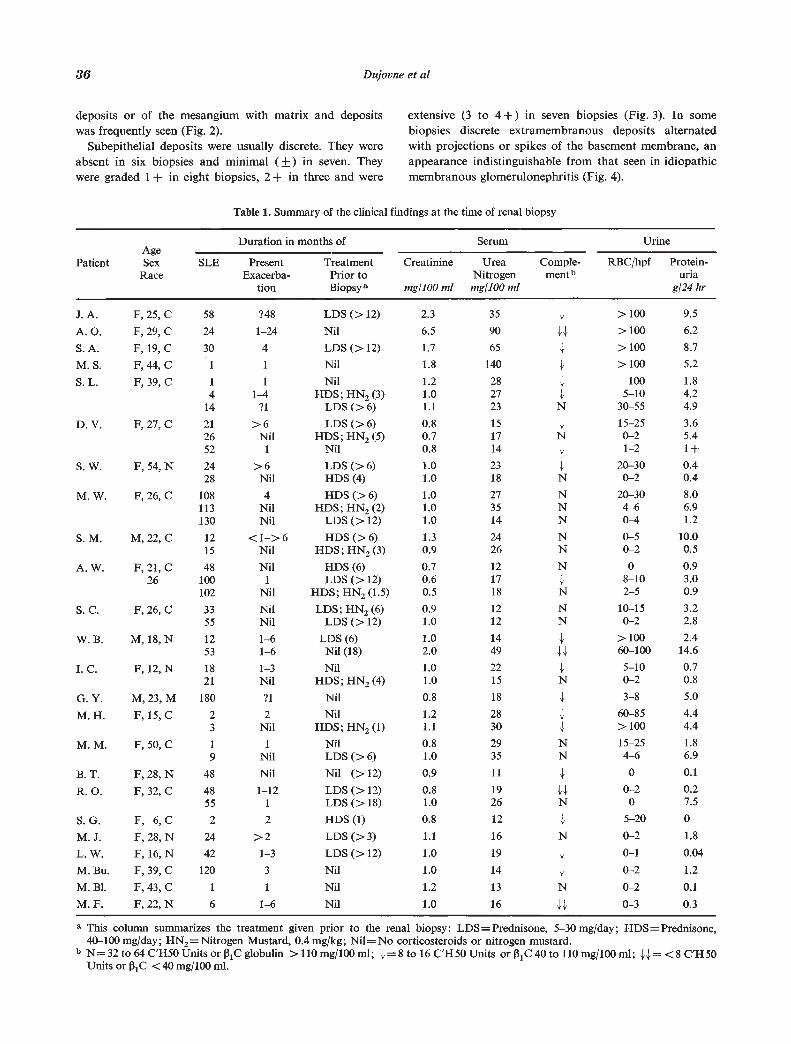
Clinical findings (Table 1). The 24 patients had been illwith systemic lupus erythematosus for periods varying fromone to 180 months before the biopsy was taken and werebeing treated as follows: prednisone — 5 to 30 mg/day(LDS), 13 biopsies; prednisone — 40 to 100 mg/day (HDS),six biopsies; HDS and nitrogen mustard —0.4 mg/kg (HN2),
seven biopsies; LDS and HN2, one biopsy; no treatment,13 biopsies.
Patient G.Y. was known to have had systemic lupuserythematosus with renal involvement for many years.About eight weeks prior to the renal biopsy, he developeda thrombosis of the inferior vena cava which extendedabove the orifices of the renal veins.
Light microscopic findings (Table 2). The followingpatterns of glomerular involvement [4, 34] were identifiedin the 40 biopsies: active lupus glomerulonephritis (25 biop-sies); healed and inactive lupus glomerulonephritis (7 biop-sies). In two patients, A.W. and M.M., the changes werepredominantly those of membranous glomerulonephro-pathy, but they are classified in the active lupus glomerulo-nephritis group because there was definite focal increasedcellularity.
Active lesions were characterized by segmental andfocal hypercellularity associated with local necrosis,karyorrhexis and fibrinoid changes. Hematoxyphil bodiesand hyalin thrombi were found occasionally; extracapillarycell proliferation with crescent formation was noted in themore severe cases. Interstitial edema and interstitial plasmacell infiltration were also considered as evidence of activity.Basement membrane changes and glomerular sclerosiswere prominent in the inactive lesions. The renal tubulescontained hyaline casts and the cytoplasm of their liningepithelium showed hyalin droplet changes in some cases.There were no significant abnormalities of the blood vessels.Interstitial fibrosis was minimal or mild even in the longstanding cases.
Electron microscopic observations (Table 3). Electronmicroscopy was performed on 31 renal biopsies. Electrondense deposits that were finely granular and stained darkerthan the lamina densa were found in four different locations:between the glomerular basement membrane and the endo-thelial cells; between the basement membrane and theepithelial cells; within the glomerular basement membrane;in the mesangial area predominantly in the mesangialmatrix. Organized "finger print" deposits were occasionallyseen.
Subendothelial deposits were absent in seven biopsies andminimal in nine biopsies; they were graded 1 + in eightbiopsies, 2 + in three biopsies and were extensive (3 to 4+)in four biopsies (Fig. 1). This corresponds to the "wireloop" by light microscopy. In these subendothelial depositsmaterial with the characteristics of polymerized fibrin wasseen in two of the four biopsies with the most extensivedeposits (4+).
Electron dense deposits were seen in every biopsy in themesangial area regardless of the activity or severity of thedisease. They were graded as equivocal (±) in five biopsies,mild (1 +) in seven, moderate (2+) in 11 and moderatelysevere or severe (3 to 4+) in eight (Figs. 1 and 2). Themesangial matrix was increased in every case. Collagenfibers were present in the mesangial area in four biopsies.Circumferential subendothelial extension of the mesangial
36 Dujovne et a!
deposits or of the mesangium with matrix and depositswas frequently seen (Fig. 2).
Subepithelial deposits were usually discrete. They wereabsent in six biopsies and minimal (±) in seven. Theywere graded 1 + in eight biopsies, 2 + in three and were
extensive (3 to 4+) in seven biopsies (Fig. 3). In somebiopsies discrete extramembranous deposits alternatedwith projections or spikes of the basement membrane, anappearance indistinguishable from that seen in idiopathicmembranous glomerulonephritis (Fig. 4).
Table 1. Summary of the clinical findings at the time of renal biopsy
a This column summarizes the treatment given prior to the renal biopsy: LDS =Prednisone, 5—30mg/day; HDS = Prednisone,
Duration inAge
Patient Sex SLE Present
months of Serum Urine
Treatment Creatinine Urea Comple- RBC/hpf Protein-Race Exacerba-
tionPrior toBiopsy a mg/100 ml
Nitrogenmg/100 ml
ment' uriag/24 hr
LA. F,25,C 58 ?48 LDS(>12) 23 35 4, >100 9.5
A.O. F,29,C 24 1—24 Nil 6.5 90 44, >100 6.2
S.A. F, 19,C 30 4 LDS(>12) 1.7 65 4, >100 8.7
M.S. F,44,C I I Nil 1.8 140 4, >100 5.2
S.L. F,39,C 1
414
1
1—4
?l
NilHDS;HN2(3)
LDS (>6)
1.21.01.1
282723
4,
4
N
1005—10
30—55
1.84.24.9
D. V. F, 27, C 212652
>6Nil1
LDS(>6)HDS;HN2(5)
Nil
0,80.70.8
151714
4,
N4,
15—25
0—2
1—2
3.65.41+
S.W. F,54,N 2428
>6Nil
LDS(>6)HDS(4)
1.01.0
2318
4,
N20—30
0—2
0.40.4
M. W. F, 26, C 108113130
4NilNil
HDS(>6)HDS; HN2(2)
LDS(>12)
1.01.01.0
273514
NNN
20—304—6
0—4
8.06.91.2
S.M. M,22,C 1215
<1—>6Nil
HDS(>6)HDS; HN2(3)
130.9
2426
NN
0—5
0—2
10.00.5
A. W. F, 21, C26
48100102
Nil1
Nil
HDS (6)LDS (>12)
HDS; HN2 (1.5)
0.70.60.5
121718
N4N
08—102—5
0.93.00.9
S. C. F, 26, C 3355
NilNil
LDS; HN2 (6)LDS (>12)
0.91.0
1212
NN
10—15
0—2
3.22.8
W.B. M, 18,N 1253
1—6
1—6LDS(6)Nil (18)
1.02.0
1449
44,4
>10060—100
2.414.6
I. C. F, 12, N 1821
1—3
NilNil
HDS;HN2(4)1.01.0
2215
4N
5—10
0—2
0.70.8
G. Y. M, 23, M 180 ?l Nil 0.8 18 1 3—8 5.0
M.H. F, 15,C 23
2Nil
NilHDS;HN2(l)
1.21.1
2830
44
60—85
>1004.44.4
M. M. F, 50, C 1
91
NilNilLDS(>6)
0.81.0
2935
NN
15—25
4-61.86.9
B.T. F,28,N 48 Nil Nil (>12) 0.9 11 4, 0 0.1
R. 0. F, 32, C 4855
1—121
LDS (>12)LDS(>18)
0.81.0
1926
44N
0—20
0.27.5
S.G. F, 6,C 2 2 HDS(1) 0.8 12 4 5—20 0
M.J. F,28,N 24 >2 LDS(>3) Li 16 N 0—2 1.8
L. W. F, 16, N 42 1—3 LDS (>12) 1.0 19 4 0—1 0.04
M. Bu. F, 39, C 120 3 Nil 1.0 14 4 0—2 1.2
M.B1. F,43,C 1 1 Nil 1.2 13 N 0—2 0.1
M. F. F, 22, N 6 1—6 Nil 1.0 16 44 0—3 0.3
40—100 mg/day; HN2= Nitrogen Mustard, 0.4 mg/kg; Nil= No corticosteroids or nitrogen mustard.b N=32 to 64 C'H50 Units or 131C globulin >110 mg/I® ml; 4=8 to 16 C'HSO Units or 131C 40 to 110 mg/i® ml; 44= <8 C'HSO
Units or 31C <40 mg/i® ml.

Glomerular deposits in lupus nephritis 37
Fig. 1. Patient S. A. There are massive subendothelial deposits of electron dense material (D). Abundant deposits are also seen inthe mesangial (M) areas. The deposits and the swelling of the endothelial cells (END) contribute to a marked narrowing of the capillarylumen which contains a red blood cell (RBC). Within the cytoplasm of an endothelial cell (arrow) is a formation of microtubularstructures (Insert). The basement membrane (BM) is normal and the foot processes are partially fused (magnification x 7520;insert x 46320).
Intramembranous deposits were equivocal or absent in13 biopsies, present to a moderate degree (1 to 2+) in nineand prominent (3 to 4+) in nine (Fig. 5). They were fre-quently associated with extramembranous deposits, some-times involving the entire thickness of the basement mem-brane, giving the impression of a gap or interruption of itscontinuity (Fig. 5). Partial or complete gaps in the base-ment membrane with direct contact between visceralepithelial and endothelial or mesangial cells were occasion-ally seen. In a few biopsies deposits in any site, and partic-ularly those in an intramembranous position, had a pale"washed out" appearance.
The character of the glomerular cells did not vary greatlyfrom biopsy to biopsy, whether or not deposits were seenadjacent to these cells. The capillary lumens were narrowedby enlargement of the mesangial areas and by swelling ofthe endothelial cells. The fenestrae were reduced in number.The endothelial cytoplasm contained prominent mito-chondria and abundant cytolysosomes and vacuoles, someof which appeared as infoldings of the plasma membrane.Microtubular structures (Fig. 1) were observed in the
endothelial cytoplasm of 15 biopsies from 12 patients;they were numerous in four biopsies . The mesangial cellswere increased in size. Most had a prominent Golgi appara-tus and endoplasmic reticulum as well as an increasednumber of free ribosomes. Within the visceral epithelialcells numerous intracytoplasmic dense bodies were common.There was abundant rough surfaced endoplasmic reticulumand free ribosomes (Fig. 3). The intracytoplasmic fibrilswere also prominent. This morphologic evidence suggestsincreased activity of the cells and was obvious when theglomerular disease was more severe. There was focal footprocess fusion and occasional villous transformation wasnoted. In the areas where subepithelial deposits werepresent, there was increased density of the foot processes.In some glomeruli this was very prominent and the cell
1 This is a lesser frequency than reported by others [14—16]. Thepresent study was not designed to assess these structures andelectron micrographs were taken and examined primarily toillustrate the distribution of deposits. A higher prevalencewould undoubtedly have been observed if studies had beendirected specifically toward identification of these structures.
•wa,crs•pct ;4WA,

38 Dujovne et a!
Table 2. Summary of selected light microscopic changes in 40 renal
a The findings are graded on a scale 0 to + + + +; F= focal.
membrane of the epithelial cell could not be identifiedgiving the impression of continuity between the epimem-branous dense deposits and the dense material in theepithelial cell cytoplasm (Fig. 6). In one case electron densedeposits were seen within the wall of arterioles.
Immunohistological findings (Tables 3 and 4). The resultsfrom 22 biopsies are summarized in Tables 3 and 4 and
Figs. 7—9. In all four biopsies with active lupus glomerulo-nephritis of 3 + to 4 + severity extensive deposits werefound. In all biopsies some abnormality was found in thesubendothelial, subepithelial, intramembranous and mesan-gial positions. The subepithelial deposits contained allthree immunoglobulins and f31C globulin, but no fibrinogen.The subendothelial deposits contained considerable amounts
Patient Date of Biopsy Basement
Glomerulus
Intra-Capillary Hyaline Karyorrhexis Hema-Membrane Cells Thrombi toxyphilThickening Bodies
*1412
413
*1*2413
*1*2dtl*2*3411
*2*1*2*3441
*2*1*3141
*2
J. A.
A. 0.S. A.
M. S.
S. L.S. L.S. L.
D. V.D. V.D. V.
S. W.S. W.
M.W.M.W.M.W,
S.M.S. M.
A. W.A. W.A. W.
S.C.S.C.W. B.W. B.
IC.I. C.
G.Y.M.H.M.H.M.M.M.M.B. T.
R. 0.R. 0.S. G.
M.J.L. W.
M.Bu.M.BI.
M. F.
4/11/68 + ++++ ++ ++5/27/68 + +++ +++ ++++ ++++
12/24/69 ++ ++++ + ++++ +++9/30/71 ++ +++ +++ +++4/18/687/02/686/27/69
00
000
++0+
000
7/10/6712/28/672/02/70
++++ 0
0
++0 0
0
12/14/664/04/67
+d
+++ 00
++0
+0
12/06/675/08/68
10/10/69
++++
++++
++++
00
+++0
000
1/22/704/14/70
00
+0 0
9/19/631/22/683/07/68
+++++++++++
++0
000
0+0
0+0
5/04/663/04/68
++
++++
++
+0
00
1/03/686/17/71
+++
+++
0+
0+
0
3/04/716/28/71
++
+ 00 0
00
11/05/69 ++ + 0 0 0
2/16/703/16/70
00
++++
00
++
00
10/24/636/18/64
++++++
00
00
00
4/21/70 0 0 0 0
2/13/689/26/68
+ +0
00
+0
00
12/16/68 0 0 0 0
3/10/71 0 0 0 0
6/10/71 0 0 0
3/12/71 0 0 0
4/01/68 0 0 0 0 0
11/22/68 0 0 0 0 0

Glomerular deposits in lupus nephritis
biopsy specimens from 24 patients with systemic lupus erythematosus a
39
of all proteins studied including fibrinogen. All proteinsstudied were also observed in the mesangium.
In patients with active glomerulonephritis of lesserseverity (+ or + +), deposits were found in the sub-epithelial position in seven, in the subendothelial positionin five, within the basement membrane in only one and inthe mesangium in all eight. The deposits were more fre-
quently segmental in the glomerulus and were, in general,more striking in the subepithelial than in the subendo-thelial position. In only two instances was fibrinogendetected in the subendothelial position. Focal depositswere noted in the subepithelial, intramembranous andmesangial positions in some of the glomeruli in the threebiopsies with healed active lupus glomerulonephritis.
Interstitial tissue .Histologic
Extra- Edema Inflammation Fibrosis severity
.Histologic
activityFibrinoid GlomerularSclerosis capillary
Cells grade grade
++ + ++ + + + ++++ +++++++ + +++ + ++ ++ ++++ +++++++ + +++ +++ ++++ ++ ++++ +++++++ 0 + +++ ++ ++ +++ ++++
00
0++
+
+++
++
00+
+0+
E+
+++++
++++
++++
+++00
++++
++
+++00
000
+++0
+0+
+++++++
+++0+
00
+++
+0
00
+ E ++++
+++
0
+++++
++0 0
0
++++
++
++
++++++
+++++
+0
+0
+++
00
00
00
+++
++0
+++
0 000
000
+++
0
±+
++++++++
+++
000
++
+0
00
0±
±+
++
++
0+++
0++
0++
±+++
0++++
±+
++++
+++++
++0
0±
00
0+
±0
±+
+±
+0
± + ± + ++ ++ ++ +00
0±
±±
±±
±0
±±
++++
++
+0
++
00
00
00
±±
++++
±±
0 ± 0 0 0 + E 000
0±
+0
+0
±0
00
±0
+0
0 0 0 0 0 0 ± ±0 + 0 ± + + ± ±± 0 ± 0 0 0 ± 00 + 0 0 0 + E 00 0 0 0 0 0 0 00 0 0 0 +F EF 0 0

40 Dajovne eta!
Table 3. Summary of the site, nature; and degree of glomerular deposits
AUN ++++
Histo-
Patient logicDiagnosisa
Histo-logic
Activity
Deposits
Subendothelial Subepithelial Intramembranous Mesangial
EMb IFC EM IF EM IF EM IF
J. A.
A. 0.S. A.
M. S.
AUN ++++ +++AGN ++++ ++++
AUN ++++
+++ U,ji,B,F
N.D.AIb, U, M,A, B, T, F
+++ Alb,U,M,A, B, T, F
++ N.D.++ N.D.
N.D. F
S.L $1 AUNS.L $2 AUNS.L. $3 AUN
++++
++
th U,Bo N.D.+ U,M,A,B
+++ U,A,13
o N.D.+ N.D.
N.D. U, M, A, f3
d N.D.g.t,B
D.V. $1 AUN +++D.V. $2 HUN 0
+ B ++++ AIb,U,M,a, B, f++ Na ++++ N.D.
+ F ++++ Alb,U,M,A, B, T, F
+++ U,A43 ++++ U,M,A,B, F, T
o N.D. ++ N.D.+ N.D. ++ N.D.
N.D. None N.D. Aib, U, A,J3, F, t
+ N.D.+ None
N.D.
0N.D.
NoneN.D.N.D.N.D.N.D.None
++++
±+++
++
++±+
++0+++
++++
N.D.±±
+++++++N.D.
+++
++++++++++++
0+
+++ND.
NoneN.D.N.D.N.D.N.D.i, B
N.D.U, i, B
N.D.N.D.N.D.
N.D.N.D.
U, BU, j.t, A, B
o N.D.o None
N.D. Noneo N.D.o N.D.
+ N.D.+ N.D.
N.D. None
+++ Na+++ alb,U,13,t
± N.D.++++ ND.++++ ND.
++ Na+ N.D.O None
N.D. U,A,B
N.D. None
D.V. $3S.W. $1S.W. $2M.W. $ IM.W. $2M.W.$3
S.M. $1SM. $2A.W. $1A.W. $2A.W. $3S.c. $1S.c. $2W.B. $1W.B. $3
LC. $1
LC. $2U. Y.M.H. $1M.H. $2M.M. $1M.M. $2B. T.
R.0. $1R.O. $2S. U.
M. J.L. W.
M.Bu.M.Bl.M. F.
AUNAUNHUNAUNAUNAUN
AUNHUNAUNAUNHUNAUNAUNAUNAUN
AUN
HUNAUNAUNAUNAUNHUNHUN
UUUUUUNN
+ N.D.O None
± N.D.± N.D.± N.D.
+ N.D.+ N.D.+ U,j3
N.D. U,M,A,B, F,
+ N.D. U,M,A,B, F,
O ± N.D.+ ± y,13+ ++ U,MJ3+ + 'y,A,Jl,t± 0 N.D.± 0 N.D.O 0 None
+ + 7O 0 None
++ ND.++ alb,U,B,
f, TN.D. Ujt, 13, T
± N.D.± N.D.
++ ND.+ N.D.
N.D. Alb,Uj.t,B, F
+ N.D.+ jt,F+ N.D.+++ Na+++ Na
+++ Na++ Na+ alb,U,T
N.D. U,M,A,B, F
N.D. alb, U, M,A, II, F, T+++ Na
++ U,M,B,f± U,j.s,B,f± yj3,f,t++ Na+ N.D.+ None
++ alb,yj3,f,t++ alb,I3,f
N.D. 7, ii, 13
+ N.D.++ U,p,B
+ U,M,A,B+ U,M,a,B++ Na± N.D.+ 7,l3± l'sO None
+++++++
±0
++++++++
000
N.D.0
N.D.N.D.N.D.
± ±± N.D.O 0
O N.D.O N.D.O N.D.
N.D.U, BNoneNoneN.D.N.D.
7, l's, 13
7, I)13
N.D.NoneNoneNoneNoneNone
N.D.13
NoneNonealbNone
0N.D.
0N.D.N.D.N.D.
N.D.NoneNoneNoneNone
13
++N.D.
±ND.N.D.N.D.
N.D.7, j,t, a, 3, f
NoneNone
Aib, .t, t
a Histologic Diagnosis: AUN= active lupus glomerulonephritis; HUN= healed and inactive lupus glomerulonephritis; U= minimalglomerular change; N = no abnormality.
b EM =electron microscopy graded from 0 to + + + +; N.D. =not done.IF = immunofluorescence microscopy. The letters represent protein present in each location, capital letters indicate widespreadfluorescence in that site (+ to + +); lower case letters indicate segmental or focal. Abbreviations: Albumin (AIb, alb); Heavy chains(U, A, M; y, a, l.t); I31C globulin (B; 13); Transferrin (T; t); Fibrinogen (F; f).

Glomerular deposits in lupus nephritis 41
Fig.2. Fig.3.
Fig. 2. Patient S. C., second biopsy. Circumferential extension(M1) of the mesangial matrix (M) to the periphery of a capillary.Abundant circumferential deposits (D1), apparently extendingfrom those in the mesangial area (D), are present. The endothelialcell (En) is swollen and the capillary lumen (L) is markedlynarrowed. (magnification x 5860).
Fig. 3. Patient M. S. Segment of glomerular capillary withseveral subepithelial deposits (arrows) along the basementmembrane (BM). The foot processes are completely fused andthe visceral epithelial cell (Ep) contains an increased amount ofendoplasmic reticulum. In the capillary lumen (L) there is anelectron dense structure consistent with a degenerated "naked"nucleus probably a hematoxyphil body (HB). (magnification>c 8200).
Fig. 4. Patient S. M., second btopsy. Segment of glomerularcapillary containing red blood cells (RBC) on the right. Theendothelium (E) is normal. The basement membrane (B) containsnumerous small deposits (D). Larger subepithelial deposits (D)separated by "spikes" of basement membrane are also present.The foot processes are partially fused (magnification x 14100). Fig. 4.
• a
1.
C S
t 4'
s
A4'
•i.
:ad
tb
t_••
:

42 Dujovne et al
Fig. 5. Patient M. S. Segment of glomerular capillary wall with asubendothelial deposit (D) in direct continuity with a subepithe-hal deposit (D1) across the basement membrane (BM). Theendothelial cells (En) are swollen and the foot processes of thevisceral epithelial cell (Ep) are completely fused (magnificationx 14500).
Fig. 6. Patient A. W., second biopsy. Segment of glomerularcapillary wall with intramembranous (D) and subepithelial (D1)deposits. Note that the visceral epithelial cell (Ep) is in closeproximity to the subepithelial deposit and has an indistinct cellmembrane and a very dense cytoplasm. L, capillary lumen; US,urinary space (magnification x 25400).
Table 4. Summary of immunohistologic findingsa
Histologicdiagnosis
Histologicactivity
No.of
Biop-sies
Deposits.
Subendothelial.
Subepithehal Intramembranous .Mesangial
7b a j.t 131C F ? a 131C F y a ji 131C F y a ji fl1C F
Active ++++ 4 4 3 3 4 4 4 3 1 3 0 2 2 0 2 1 4 3 4 4 3glomerulo— (1) (1) (2) (1) (1) (1) (1) (1)
nephritis
+—++ 8 32212(2) (4)
52351(1) (1) (3) (2)
10010 72233(1) (2) (4) (4)
Healed
(0—±)
3 00000 10010(1) (1) (1)
10000(1) (1) (2)
10001(2) (1)
Minimal 0—+ 5 00000 00000 00000 00000glomerular (1) (1) (1) (1) (2) (2) (1) (1) (3) (3)
changes
Normal 0 2 00000 00000(1) (1)
00000 00000(1)
a The number of biopsies in which the protein was found widespread is indicated on the first line. In parentheses, on the second lineis the number of biopsies in which the protein was distributed segmentally.
b Abbreviations: y, a, t= Heavy chains of IgG, IgA, 1gM; 31C= 31C globulin; F= fibrinogen.
There were no subendothelial deposits in these bi- sponded well with that of the heavy chains. All 22 biopsiesopsies. were also studied with antisera directed against albumin
Of the seven biopsies considered to be normal or to have and transferrin, proteins presumably not involved in anyminimal glomerular changes, small segmental deposits immunologic reaction. In none was albumin or transferrinwere present in only two. detected in the subepithelial or intramembranous position.
Thirteen biopsies were examined with antiserum directed In a few cases, particularly those with severe active gb-against the light chains K and ?; their distribution corre- merulonephritis, albumin and transferrin were found in

CcD.--
Glomerular deposits in lupus nephritis 43
Fig. 7. Patient I. C., first biopsy. Photomicrograph of a glomerulus showing the distribution of IgG (y chain) in a 0.5 gifrozensubstituted section treated as follows: (1) incubated with rabbit antiserum to human y chain; (2) incubated with a peroxidase con-jugated goat antiserum to rabbit globulin; (3) incubated with diaminobenzidine; (4) fixed in gluteraldehyde; (5) stained with PAS-hematoxylin. Note the very widespread distribution of IgO in the glomerular capillary walls. At higher magnification it was clearlyevident that this was in the subendothelial position (magnification x 440).
subendothelial deposits. Albumin and transferrin wereobserved in the mesangium in about half of the biopsiesstudied and appeared most prominently in severely damagedglomeruli.
In general there was a good correlation between theimmunohistologic and electron microscopic findings.Deposits were more difficult to detect within the glomerularbasement membrane by immunohistology than by electronmicroscopy. This was probably due to the difficulty inprecisely localizing fluorescence or peroxidase within theglomerular basement membrane at the magnificationspossible. Of the six biopsies in which material immuno-reactive with antifibrinogen serum was found in the sub-endothelial position, three were studied by electron micro-scopy. Polymerized material with the electron microscopiccharacteristics of fibrin was noted in two.
Relationship between deposits and histologic findings.A relationship between histologic activity and clinicalevidence of active lupus nephritis has been reported
previously [4, 35] and was noted in the present series ofbiopsies (Fig. 10). Except in those biopsies taken afterprolonged treatment and in which there was no histologicevidence of activity, histologic severity paralleled histologicactivity. There was no relationship between histologicactivity, on the one hand, and the extent of subepithelial orintramembranous deposits, on the other (Fig. 11). Intra-membranous deposits were present both in active lupusglomerulonephritis and in healed and inactive disease aftertreatment. They were prominent in five of the seven latterbiopsies. The correlation between histologic activity andthe extent of subendothelial and mesangial deposits wasonly a rough one; however, extensive subendothelial depos-its were seen only with the most active histologic lesions andsubendothelial deposits were virtually absent in healed andinactive lesions after treatment. Moreover, in all patientswho died with severe active lupus glomerulonephritis,extensive subendothelial deposits were found in the biopsytaken within weeks of death.

44 Dujovne et a!
Fig. 8. Patient M. S. The distribution of I1C globulin is shown in a single severely damaged glomerulus. It is predominantly alongthe glomerular capillary wall in some areas and is in the centrilobular or mesangial region in many places, particularly in the necroticareas (arrows). Immunoperoxidase technique with PAS-hematoxylin (magnification x 480).Insert A. Detail showing the subendothelial and mesangial distribution of t3IC globulin in two capillary loops. The arrows point tothe basement membrane (magnification x 800).Insert B. Area from the same glomerulus incubated with antiserum to IgG (y chain). Note the subendothelial IgG giving the appearanceof a "wire loop" (magnification x 800).

Fig. 9. Patient S. M., second biopsy. The distribution of IgG (y chain) is shown. There is an area of sclerosis in the glomerulus.Note the segmental distribution of IgG along some capillary walls. The patent glomerular capillaries contain IgG as demonstratedby the immunoperoxidase technique with PAS-hematoxylin (magnification x 360).Inserts A and B. In a few areas the basement membrane (BM) is normal. A single subendothelial deposit (S END in insert A)containing IgG can be clearly seen. Elsewhere there is segmental but widespread IgG in the subepithelial and intramembranouspositions (magnification x 630).

3
02b0
0Ca
CaAs .3Ca0V-e.5 •
• S. S
. 30000
0
4 5.>..
5 5SCS
C.)
. :°Øo
0±1
Fig. 12. Interrelationship between the extent of deposits in various positions in the glomerulus. See legend to Fig. 10 for symbols.
The deposits did not seem to be distributed randomlyin the several positions (Fig. 12). There was some relation-ship between increasing amounts of subendothelial andmesangial deposits. Inactive disease, subendothelial depositswere extensive only in the presence of extensive mesangialdeposits. In general, there was an inverse relationshipbetween the extent of the subendothelial and subepithelialdeposits (Fig. 13). Extensive subendothelial deposits occur-red in association with the most active histologic changesand three of the four patients with extensive subendothelialdeposits died within weeks of the renal biopsy, In generalthe clinical course of patients with extensive subepithelial
deposits was benign. A single exception to these relation-ships was observed in the renal biopsy of patient M.S.This patient had fatal hyperacute lupus nephritis and thebiopsy was unusual in that there were many large obviousdefects or gaps in the glomerular basement membrane.
The deposits could not be quantitated as readily byimmunohistology and similar comparisons could not bemade by this technique. One striking finding, however, wasobserved in the four biopsies with the most active histologiclesions (4+). In all, the subendothelial deposits wereparticularly prominent and far more extensive than thesubepithelial deposits. Material immunoreactive with
46
4
Dujovne et a!
4.5S..
S.5
5
•.5•
S.
555 5 4 •5 S
- S.. 5 3 •5 5
- S. 2 5 •
...0*AOA-AAA
55 1—.o
0 Ljo A iA
S
S•S 5
0±1Subepithelial
2 3
deposits40±1
Subendothelial2 3 4
deposits
+
0
. 05••S•
A
!A 0AA Ao 0
0 1
3
3-j4
' 41
. • 2
3 4Intramembranous deposits
5.S
-±-2
S.5.-. $5
— S 5
AAA •o04 ?A 41
2 3 4Mesangial deposits
+2
Clinical activity
Fig. 10. Interrelationship between clinical activity and the histo-logic activity of the renal disease. The symbols used in this andthe following two figures are: open circle (o), normal kidney orminimal glomerular change; closed circle (.), active lupusglomerulonephritis; closed triangles (A), active glomerulone-phritis which, following treatment, has healed.
' S 4
•A
4+0L
0
Fig. 11. Interrelationship between histologic activity and extentof deposits. See legend to Fig. 10 for symbols.
—S
-S0 5A S0 0
- A AA
0 SA 55
Ca
Ca0C)-e
biaCa
+
0'
— •AA S
—50 5. 5A0 50
—SA SAA0 SA
I I I I0±1 2 3 4Subepithelial deposits
555 5 4 5Ca
Ca03 AAA S. S-e
Can0
: • l • ':
I
Subendothelial
I2
I3
deposits
I4
— 00.Ao •0.A0
I0±1Subepithelial
•I I2 3
deposits
I40

Fig. 13. Interrelationship between sub-endothelial and subepithelial deposits andhistologic activity.
Glomerular deposits in lupus nephritis 47
antifibrinogen serum was prominent in the subendothelialdeposits in these four instances, but was not seen in thesubepithelial position.
Discussion
Aggregates of electron dense material are prominent inthe glomeruli in various diseases [36, 37]. For example, inacute poststreptococcal glomerulonephritis and in mem-branous glomerulonephropathy they are predominantlyepimembranous, contain gamma globulin and comple-ment and are assumed to result from deposition of circu-lating antigen-antibody complexes. On the other hand,experimental work [38] suggests that when glomerularbasement membrane is the antigen, the locally formedantigen-antibody complexes are deposited along the innerportion of the basement membrane. In diabetic nephro-pathy, by contrast, deposits rich in lipoproteins and otherproteins are seen in the subendothelial position and areregarded as insudative in nature. In most reports in whichthe nature of the deposits has been studied by immuno-fluorescence microscopy, it should be noted that thelocation of the deposits in the glomerular wall could nothave been determined precisely, because of the thickness(4 to 6 j.L) of the sections.
In patients with systemic lupus erythematosus, depositshave been reported within and on both sides of the gb-merular basement membrane and in the mesangial matrix.The demonstration of gamma globulin, complement, andanti-DNA in the deposits has led to the conclusion thatthey represent antigen-antibody complexes. The present
study confirms that electron dense deposits, gamma globulinand complement are deposited in all positions in theglomerular capillary wall in lupus nephritis (Table 3).
Evolution of the deposits with time and treatment. Theelectron microscopic observations made at varying stagesin the evolution of lupus nephritis and after treatmentsuggest that extensive subendothelial deposits occurredonly in the most active disease. Three of the four severestcases died of renal failure within weeks. In other patientssubendothelial deposits tended to decrease in prominenceor disappear following therapy (Fig. 11). In one patient(W.B.) a recrudescence of severe lupus nephritis wasaccompanied by the appearance of extensive subendo-thelial deposits and renal failure leading to death withinfour weeks of the biopsy.
In serial biopsy studies, deposits in the mesangiumchanged less than did the subendothelial deposits. Sub-epithelial deposits appeared to undergo relatively fewchanges with time; once present, they persisted. Only inpatient M.M. was there a significant decrease in the extentof the deposits in a second biopsy. With time they appearedto become incorporated into the glomerular basementmembrane in a manner similar to that seen in idiopathicmembranous glomerulonephropathy [39] and to becomeless electron dense in some. When extensive subepithelialdeposits were the predominant finding there appeared tobe little clinical or histologic progression of the diseaseover long periods of time. For example, there were extensivesubepithelial deposits in a biopsy taken from patient A.W.in 1963. The patient had one episode of active lupus gb-merulonephritis in 1968, but apart from this episode has
++++
.c +++. ++++0
+

48 Dujovne et a!
been in good health with little proteinuria and normalfunction from 1963 to 1971.
Intracapillary cell proliferation decreased in some patientsafter treatment. Mesangial matrix seemed to increase withtime and collagen was seen in the mesangial area close tothe mesangial cytoplasm on only three occasions in biopsiestaken after treatment. There were occasional gaps orinterruptions in the glomerular basement membrane withdirect contact between intra- and extracapillary cells, oftenin places where subepithelial, intramembranous or trans-mural deposits were present. The gaps appeared to be theresult of damage produced by the deposits. In the visceralepithelial cells, cytophagolysosomes appeared to be morecommon adjacent to the gaps.
The nature of the deposits has been elucidated in partby the immunohistochemical studies. The subepithelialdeposits were found to contain immune globulins and1C globulin, but no fibrinogen, albumin, or transferrin.These findings are consistent with the view that thesedeposits represent antigen-antibody complexes. The intra-membranous deposits were more difficult to define byimmunohistologic techniques but they seemed to consistpredominantly or exclusively of gamma globulins andcomplement. In both the mesangium and the subendothelialposition, the immunohistochemical studies indicated thatthere were, in many instances, deposits of material immuno-reactive with antiserum to albumin, to transferrin, and tofibrinogen, as well as to the immune globulins and fI1Cglobulin. In glomeruli in which necrosis of a segment ofthe tuft was observed, all plasma proteins studied weredetected in the necrotic areas. Deposits in the mesangialand in the subendothelial position are usually thought torepresent antigen-antibody complexes. The present observa-tions suggest that subendothelial deposits might well heinsudative lesions.
Mesangial deposits were found even in biopsies withminimal or no light microscopic changes. When mesangialdeposits are small they may represent evidence of a normallyfunctioning mesangium rather than evidence of activedisease [13]. Rowever, proliferation of mesangial cellsor an increase in mesangial matrix was a common findingand emphasizes the reactive properties and importance ofthe mesangium in systemic lupus erythematosus. Themesangium plays a role in removing large molecules orcomplexes circulating in the glomerular capillaries, eitherby the phagocytic properties of mesangial cells or by wayof the spongy material of the mesangial matrix [40—42].The first site of deposition of circulating macromoleculesin the glomeruli seems to take place in the mesangialregions [41—43]; but material deposited there may spillover into the subendothelial space (lamina rara intema) indirect continuity with the mesangium only when thephagocytic properties and/or storage capacity of mesangialcells and matrix are exceeded. Projections of mesangialcytoplasm and/or matrix peripherally between the endo-thelium and capillary basement membrane occurred
frequently in our material. In some instances the so-calledsubendothelial deposits appeared in reality to be depositswithin the mesangium extending circumferentially aroundthe capillaries. Evidence for endothelial vesicular intra-cytoplasmic transport [44, 45] was occasionally seen, butdid not seem to play a major role in the formation ofsubendothelial deposits.
Both intra- and epimembranous deposits underwentrelatively little change with time or following treatmentwhile subendothelial deposits decreased markedly. It ispossible that subendothelial deposits can be removed byactivity of the mesangial cells in a direction opposite tothat in which they are formed. The discordance betweenthe extent and severity of subendothelial and subepithelialdeposits on the one hand, and the concordance of sub-endothelial and mesangial deposits on the other, alsosuggests the possibility that disappearance of large sub-endothelial aggregates may be by a pathway through themesangium rather than through the basement membrane.In favor of this possibility is the complete disappearance ofsubendothelial deposits after treatment, whereas mesangialdeposits persist longer and only rarely disappear com-pletely. There was also evidence that the decrease or disap-pearance of subendothelial deposits was associated with anincrease of intra- and/or epimembranous deposits. Recentexperimental evidence [46] suggests that cortisone mayprevent transmigration of complexes from the blood to thesubepithelial portion of the capillaries and that it maytherefore, indirectly, facilitate removal of deposits bymesangial cell activity from the subendothelial areas. Thepersistence of deposits in the subepithelial region is notexplained. This finding is similar to that observed in otherdiseases such as idiopathic membranous glomerulonephro-pathy. To a limited extent, subepithelial deposits may beremoved by visceral epithelial cells themselves as demon-strated by the frequent disruption of their plasma mem-brane, condensation of the cytoplasm immediately aroundthe deposits and the common finding of cytophagolyso-somes. Occasionally, intramembranous and subepithelialdeposits seemed to be less dense or had a "washed out"appearance with time or following treatment.
The results of this study appear to reflect reasonablyaccurately the character and behavior of glomerulardeposits in various stages of lupus nephritis. The findingsmust be interpreted with caution because of certainunavoidable limitations. First, renal disease had beenpresent clinically in all but two patients for varying periodsof time before the first biopsy was taken. Therefore, theearliest stages of several patterns of glomerular diseasemay have not been adequately represented in this seriesof cases. Second, varying amounts of prednisone andnitrogen mustard had been administered to 13 patientsfor varying periods of time before the first biopsy wastaken. As a result the distribution and composition of thedeposits may have been somewhat modified. Third,because of the well known focal and segmental distribution
Glomerular deposits in lupus nephritis 49
of the glomerular lesions, a qualitative and quantitativeevaluation, especially of the immunohistologic and electronmicroscopic findings has obvious limitations related tosampling.
The results of this study indicate that glomerular depositsper se should not be interpreted as evidence of activedisease unless they are either located subendothelially orpresent in massive amounts after treatment. Persistence ofsubepithelial and intramembranous deposits withouthistologic evidence of active disease indicates that cortico-steroids and immunosuppressive agents have a greatereffect on the cellular response than on these deposits, orthan on the basic disease process. An alternative possibilityis that treatment induces changes in the chemical and/orphysical characteristics of the deposits not detectable bythe methods used in this study.
Acknowledgements
Presented in part at the 3rd Annual Meeting of the Amer-ican Society of Nephrology, Washington, D.C., December,1969. This work was supported in part by N.I.H. grantAM 10314. Dr. Dillard's work was supported by USPHSFellowship AM 44140; his present address is Departmentof Medicine, Howard University, Washington, D.C.Dr. Dujovne's present address is Laprida 1717-4° A,Buenos Aires, Argentina. We thank Mrs. Hilda Sanders,Mrs. Jean Makowski and Mrs. Elena Sileikis for technicalassistance.
Reprint requests to Dr. ConradL. Pirani, Department ofPathology, Michael Reese Hospital, 29th and Ellis Avenue,Chicago, Illinois 60616, U.S.A.
References
1. MUEHRCKE RC, KARK RM, PIRANI CL, POLLAK YE: Lupusnephritis: A clinical and pathologic study based on renalbiopsies. Medicine 36:1—147, 1957
2. SOFFER U, SOUTHREN AL, WEINER HE, WOLF RI: Renalmanifestations of systemic lupus erythematosis: A clinicaland pathologic study of 90 cases. Ann mt Med 54:215—228,1961
3. ROTHFIELD NF, MCCLUSKEY RT, BALDWIN DS: Renal dis-ease in systemic lupus erythematosus. New EngI J Med269:537—544, 1963
4. POLLAK YE, PIRANI CL, SCHWARTZ FD: The natural historyof the renal manifestations of systemic lupus erythematosus.J Lab C/in Med 63:537—550, 1964
5. ZWEIMAN B, KORNBLUM J, CORNOG J, HILDRETH EA: The
prognosis of lupus nephritis. Role of clinical-pathologiccorrelations. Ann mt Med 69:441—459, 1968
6. BALDWIN DS, LOWENSTEIN J, ROThFIELD NF, GALLO G,MCCLUSKEY RT: The clinical course of the proliferativeand membranous forms of lupus nephritis. Ann mt Med 73:929—942, 1970
7. FARQUHAR MG, VERNIER RL, GooD RA: An electronmicroscopic study of the glomerulus in nephrosis, glomerulo-
nephritis, and lupus erythematosus. J Exp Med 106:649—660, 1957
8. PIRANI CL, MANALIGOD JR: The kidneys in collagen dis-eases in The Kidney, edited by MosroFi KF, Baltimore,Williams & Wilkins, 1966
9. COMERFORD FR, COHEN AS: The nephropathy of systemiclupus erythematosus. Medicine 46:475—490, 1967
10. GRISHMAN E, CiiuRo J, MAUTNER W, SUZUKI Y: Pathologyof lupus nephritis. J Mount Sinai Hosp 30:117—126, 1963
11. SPARGO B, ARNOLD JD: Glomerular extrinsic membranousdeposits with the nephrotic syndrome. Ann NY Acad Sci86:1043—1063, 1960
12. GRISHMAN E, PoRusH JC, ROSEN SM, CHURG J: Lupusnephritis with organized deposits in the kidneys. Lab Invest16:717—725, 1967
13. KOFFLER D, AGNELLO V, CARR RI, KUNKEL HG: Variable
patterns of immunoglobulin and complement deposition inthe kidneys of patients with systemic lupus erythematosus.Am JPath 56:305—316, 1969
14. GYORKEY F, MIN KW, SINKOvIcs JG, GYORKEY P: Systemiclupus erythematosus and myxovirus. New Engi J Med 280:333—336, 1969
15. GARANUCIS JC, KOMOROWSKI RR, BERNHARD GC, STRAUM-FJORD JY: Significance of cytoplasmic microtubules in lupusnephritis. Am J Path 64:1—12, 1971
16. HURD ER, EIGENBRODT D, WORTHEN H, STRUNK SS, ZirrM: Glomerular cytoplasmic tubular structures in renalbiopsies of patients with systemic lupus erythematosus andother diseases. Arth Rheum 14:539—550, 1971
17. VAZQUEZ JJ, DIXON FJ: Immunohistochemical study oflesions in rheumatic fever, systemic lupus erythematosusand rheumatoid arthritis. Lab Invest 6:205—207, 1957
18. MELLORS RC, ORTEGA LG, HOLMAN HR: Role of gammaglobulin in the pathogenesis of renal lesions in systemiclupus erythematosus and chronic membranous glomerulo-nephritis, with an observation of the lupus erythematosuscell reaction. J Exp Med 106:191—202, 1957
19. PARONETrO F, KOFFLER D: Immunofluorescent localizationof immunoglobulins, complement, and fibrinogen in humandiseases. I. Systemic lupus erythematosus. J C/in Invest 44:1657—1664, 1965
20. SVEC K, BLAIR JD, KAPLAN MH: Immunopathologic studiesof systemic lupus erythematosus (SLE). I. Tissue boundimmunoglobulins in relation to serum immunoglobulin insystemic lupus and in chronic liver disease with LE cellfactor. J C/in Invest 46: 558—568, 1967
21. MCCLUSKEY RT, VASSALLS P, GALLO G, BALDWIN DS: Animmunofluorescent study of pathogenic mechanisms inglomerular diseases. New Engi J Med 274:695—701, 1966
22. KRISHNAN C, KAPLAN MH: Immunopathologic studies ofsystemic lupus erythematosus. II. Antinuclear reaction ofglobulin eluted from homogenates and isolated glomeruli ofkidneys from patients with lupus nephritis. J C/in Invest 44:
1657—1664, 1967
23. KOFFLER D, SCHUR PH, KUNKEL HG: Immunologic studiesconcerning the nephritis of systemic lupus erythematosus.JExp Med 126: 607—623, 1967
24. TAN EM, SCEUR PH, CARR RI, KUNKEL HG: Deoxyribo-nucleic acid (DNA) and antibodies to DNA in the serumof patients with systemic lupus erythematosus. J C/in Invest45:1732—1740, 1966

50 Dujovne et a!
25. TOWNESAS, STEWART CR, JE, OSLER AG: Immunologicstudies of systemic lupus erythematosus. II. Variations ofnucleoprotein reactive gamma globulin and hemolytic serumcomplement levels with disease activity. Bull Johns HopkinsHosp 112:202—219, 1963
26. PIRANI CL, POLLAK yE, SCHWARTZ FD: The reproducibilityof semiquantitative analyses of renal histology. Nephron 1:230—237, 1964
27. PIRANI CL, SALINAS-MADRIGAL L: Evaluation of percutan-
eous renal biopsy in Pathology Annual, New York, Appleton-Century-Croft, 1968, p. 249
28. POST RS: A technique for cutting thin sections from solventsubstituted paraffin embedded tissues. Cryobiology 1:261—269, 1965
29. POLLAK YE, Ooi BS, PESCE AJ: The distribution of serumalbumin in the diseased human nephron as demonstratedby immunofluorescence. J Lab C/in Med 76:357—373, 1970
30. MARSHALL JD, EVELAND WC, SMITH CW: Superiority offluorescein isothiocyanate (Riggs) for fluorescent antibodytechniques with a modification of its application. Proc SocExp Biol Med 98: 898—900, 1958
31. AVRAMEAS 5: Coupling of enzymes to proteins with glutar-aldehyde. Use of the conjugates for the detection of antigensand antibodies. Immunochemistry 6:43—52, 1969
32. GRAHAM RC, KARNOVSKY MJ: Glomerular permeability.Ultrastructural cytochemical studies using peroxidases asprotein tracers. J Exp Med 124:1123—1133, 1966
33. NORRIs SH, MoDEsToRR, PESCE AJ, CLYNED, POLLAKYE:Antibody-enzyme conjugates: the preparation of inter-
molecular conjugates of horseradish peroxiclase and gammaglobulin and their application to immunohistology of therenal cortex. J Histochem Cytochem (Submitted)
34. POLLAK YE, PIRANI CL: Renal histologic findings in sys-temic lupus erythematosus. Mayo Clinic Proc 44:630—644,1969
35. POLLAK YE, PIRANI CL, KARK RM: Effect of large doses ofprednisone on the renal lesions and life span of patients withlupus glomerulonephritis. J Lab C/in Med 57:495—511, 1961
36. CHURG J: Electron microscopic aspects of renal pathologyin Structural Basis of Renal Disease, edited by BECKER EL,New York, Hoeber, 1968, p. 132
37. BUIRKHOLDER PM: Immunology and immunohistopathologyof renal disease in Structural Basis of Renal Disease, editedby BECKER EL, New York, Hoeber, 1968, p. 197
38. MCCLUSKEY RT, VASSALLI P: Experimental glomerular dis-eases in The Kidney: Morphology, Biochemistry, Physiology,edited by ROUmLER C, MULLER AF. New York, AcademicPress, Vol. 2, 1969, p. 84
39. EHRENREICH T,CHURGJ: Pathology of membranous nephro-pathy in Pathology Annual, 1968, p. 145
40. MENEFEE MG, MUELLER GB, BELL AL, MYERS LK: Trans-port of globulin by the renal glomerulus. J Exp Med 120:1129—1138, 1964
41. LATTA H, MAUNSBACH AB, MADDEN SC: The centrolobularregion of the renal glomerulus studied by electron micro-scopy. J Ultrastruct Res 4:455—472, 1960
42. FARQUHAR MG, PALADE GE: Functional evidence for theexistence of a third cell type in the renal glomerulus. J CellBiol 13:55—87, 1962
43. MICHIELSEN P, CREEMERS J: The structure and function ofthe glomerular mesangium in Ultrastructure of the Kidney,edited by DALTON AJ, HAGUENAUF, New York, AcademicPress, 1967, p. 57
44. FAITH GC, TRUMP BF: The glomerular capillary wall inhuman kidney disease: acute glomerulonephritis, systemiclupus erythematosus, and preeclampsia-eclampsia. Labinvest 15:1682—1719, 1966
45. BROWNE JT, HUTT MP, REGER JF, SMITH SW: Localizationof "fibrinoid" deposit in lupus nephritis. An electronmicro-scopic demonstration of glomerular endothelial cell phago-cytosis. Arth Rheum 6:599—614, 1963
46. GERMUTH FJ, JR, VALDES AJ, SENTEREIT LB, POLLACK AD:A unique influence of cortisone on the transit of specificmacromolecules across vascular walls in immune complexdisease. Bull Johns Hopkins Hosp 122:137—153, 1968