the effect of 4-week rehabilitation on heart rate variability and qtc interval in patients with...
TRANSCRIPT

1
ORIGINAL RESEARCH
The Effect of 4-week Rehabilitation on Heart Rate Variability and QTc Interval in Patients with Chronic Obstructive Pulmonary DiseaseEva Zupanic,1 Ina Zivanovic,1 Jurij Matija Kalisnik,2 Viktor Avbelj,3 and Mitja Lainscak4,5
1 Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia
2 Department of Cardiovascular Surgery, University Medical Center Ljubljana, Ljubljana
3 Department of Communication Systems, Jožef Stefan Institute, Ljubljana, Slovenia
4 Division of Cardiology, University Clinic of Pulmonary and Allergic Diseases Golnik, Golnik, Slovenia
5 Division of Applied Cachexia Research, Department of Cardiology, Charité Campus Virchow-Klinikum, Berlin, Germany
Keywords: chronic obstructive pulmonary disease, heart rate variability, QT interval, rehabilitation, exercise training
Abbreviations: 6MWT = 6-min walk test, 6MWT-CRD = clinically relevant difference in 6MWT, COPD = chronic obstructive pulmonary disease, ECG = electrocardiogram, FEV1 = forced expiratory volume in one second, GOLD = global initiative for chronic obstructive lung disease, HF = high frequency power, HRV = heart rate variability, ICS = inhalatory corticosteroids, ISWT = incremental shuttle walking test, ISWT-CRD = clinically relevant difference in ISWT, LF = low frequency power; LF/HF = ratio LF/HF, LTOT = long-term oxygen therapy, MRC = Medical Research Council dyspnea scale, NN-interval = interval between two adjacent R-waves preceded by P-waves, nuHF = high frequency power in normalized units HF/(TP-VLF), nuLF = low frequency power in normalized units LF/(TP-VLF), PEF = peak expiratory fl ow, PIF = peak inspiratory fl ow, pNN50 = percentage of pairs of adjacent NN intervals differing by more than 50 ms, QTc = corrected QT-interval, RMSSD = the square root of the mean of the sum of the squares differences between adjacent NN intervals, SABA = short acting beta agonists, SDNN = standard deviation of all NN intervals, SGRQ = St. George’s respiratory questionnaire, SGRQ-CRD = clinically relevant difference in SGRQ, TP = total power, VC = vital capacity, VLF = very low frequency power.
Correspondence to: Mitja Lainscak, MD, PhD, Associate Professor of Internal Medicine, Division of Cardiology, University Clinic of Pulmonary and Allergic Diseases Golnik, Golnik 36, SI-4204 Golnik, Slovenia, phone: +386 4 2569 483, fax +386 4 2569 117, email: [email protected]
Abstract
Chronic obstructive pulmonary disease negatively affects the autonomic
nervous system and increases risks of arrhythmias and sudden cardiac death.
Electrocardiogram (ECG) recordings were used to compare parameters of heart
rate variability and QTc interval in patients with COPD and healthy individuals.
The effects of a 4-week program of rehabilitation in patients with COPD were also
evaluated by comparing pre- and post-rehabilitation ECGs with age- and sex-
matched control COPD patients not participating in the program. Heart rate, average
NN, SDNN, RMSSD, pNN50, TP, LF, HF, LF/HF, and QTc were analyzed. Rehabilitation
effects were evaluated using the St. George’s respiratory questionnaire (SGRQ),
the 6-min walk test (6MWT), and the incremental shuttle walking test (ISWT). In
comparison with the healthy individuals, the patients with COPD had higher heart
rate (p < 0.05) and reduced average NN, SDNN, RMSSD, pNN50, HF, LF, and TP (all p <
0.05) but similar QTc interval (p = 0.185). During rehabilitation, SDNN and TP (p <
0.05 for both) increased, as did the results for 6MWT, ISWT, and SGRQ (all p < 0.05).
No signifi cant change of QTc interval was observed within or between the two
groups of patients with COPD. Change in SDNN correlated with a clinically relevant
difference in SGRQ (r = 0.538, p = 0.021). It is concluded that patients with COPD
demonstrate reduced parameters of heart rate variability and that these can be
improved in a rehabilitation program, thus improving health-related quality of life.
COPD, 00:1–11, 2014ISSN: 1541-2555 print / 1541-2563 onlineCopyright © Informa Healthcare USA, Inc.DOI: 10.3109/15412555.2014.898046
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with a two- to four-fold increased risk of death from cardiovascular diseases (1). Patients have an increased risk of congestive heart failure, acute myocardial infarc-tion, atrial fi brillation, hospitalization due to atrial fi brillation, and mortality due to stroke and other arrhythmias (1, 2). Furthermore, patients with COPD demonstrate disrupted autonomic refl exes and neurohormonal activation with enhanced sympathetic tone at rest (3, 4). Th e activity of sympathetic nerves may be aff ected by recurrent hypoxemia, hypercapnia, increased intrathoracic pressure swings resulting from airway obstruction, increased respiratory eff ort, systemic infl ammation, and the use of betasympathomi-metics (3). Autonomic dysfunction may trigger a self-perpetuating cycle con-tributing to the pathogenesis of COPD, and may be associated with increased cardiovascular morbidity and mortality (3, 4).
Among the studies that established the presence of autonomic dysfunc-tion in patients with COPD, several utilized markers of heart rate variability
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Copyright © 2014 Informa Healthcare USA, Inc
2 Zupanic et al.
(HRV) (5–10). Prolongation of the corrected QT inter-val (QTc) (> 440 ms) has also been associated with autonomic neuropathy in patients with hypoxemic COPD (11), whereas in patients with COPD, prolonged QTc remained predictive of poor patient survival when adjusted for age, sex, stage according to the global initia-tive for chronic obstructive lung disease (GOLD), body-mass index, and smoking (12).
Prognosis of COPD remains poor (13), as few inter-ventions have demonstrated benefi cial eff ects in terms of patient-related outcome. However, rehabilitation has an established role in management of COPD, with sev-eral ancillary eff ects (14) such as the positive modula-tion of HRV. Studies to date (15–17) have focused on various outpatient exercise programs and aquired data using Polar heart rate receivers, which could serve as an attractive data acquisition alternative for assessment of R-R interval and evaluation of HRV (18).
All the studies reported signifi cant increase in dif-ferent time-domain HRV parameters, whereas power spectral analysis revealed no increase or gave contrast-ing results.
To our knowledge, no studies to date in patients with COPD have assessed the eff ects of a comprehensive inpatient rehabilitation program using electrocardio-gram (ECG)-derived HRV parameters and QTc. Th e aims of our study were: (1) to compare HRV and QTc in patients with COPD and healthy individuals, (2) to assess changes of HRV and QTc in patients with COPD after comprehensive inpatient rehabilitation as com-pared with COPD controls.
Methods
Study designTh e study was designed as (1) a cross-sectional obser-vational study comparing HRV and QTc in patients with COPD and healthy individuals, (2) a prospective pseudo-randomized control study comparing HRV and QTc in COPD patients before and after a 4-week com-prehensive rehabilitation program with a control group of COPD patients without rehabilitation but in a similar time frame. We also compared the change in HRV and QTc in the rehabilitation group with clinical param-eters used for assessment of rehabilitation effi cacy. Th e National Medical Ethics Committee of the Republic of Slovenia approved all the study protocols (approval nr. 54/03/12), and informed consent was obtained from all study participants prior to data collection.
Study participants and data collectionWe recorded 20-min ECGs in 121 subjects enrolled in the study and 62 of these were further analyzed (Figure 1). For patients with COPD, we required a defi nite diag-nosis of COPD and an indication for rehabilitation. Healthy individuals were defi ned as persons without known chronic disease except well controlled arterial hypertension or hypercholesterolemia. Exclusion crite-
ria for all participants in the study were: absence of sinus rhythm, diagnosis of diabetes mellitus or chronic heart failure, long-term beta-blocker therapy, ECG recording inappropriate for HRV analysis (e.g., too many exter-nal disturbances or supraventricular extrasystoles) or incomplete ECG recording (e.g., loss of data, participant declined participation). In COPD patients, we excluded one patient with pulmonary disease other than COPD. We excluded 19 healthy individuals due to relevant smoking history or because of non-matching for sex and age with patients with COPD (Figure 1).
Th e group with COPD who underwent rehabilitation comprised of 18 patients referred to a 4-week compre-hensive rehabilitation program at the University Clinic of Pulmonary and Allergic Diseases Golnik between March 2011 and May 2012. ECGs were recorded at the beginning (on 2nd day ± 1 day) and at the end (on 27th day ± 1 day) of rehabilitation. Th e control group of patients with COPD comprised 13 age- and sex-matched candidates for rehabilitation who did not take part in the program at that time; their ECGs were recorded in an identical time interval, during which time the patients lived at home and attended to their daily activities. Th ese two groups together represented all the included patients with COPD (n = 31).
Th e group of healthy individuals comprised 31 age- and sex-matched persons without a diagnosis of COPD; they had a maximum smoking history of 3 pack-years but no active smoking at the time of the study. Th e healthy individuals’ group had their ECGs recorded once only.
Rehabilitation programTh e University Clinic of Pulmonary and Allergic Dis-eases Golnik off ers a comprehensive rehabilitation program for patients with COPD, with priority given to patients waiting for lung transplantation and patients with COPD stage GOLD 3 or 4. In the fi rst days of the program patients undergo physiological and psycho-logical evaluation using the Medical Research Council dyspnea scale (MRC), St. George’s respiratory question-naire (SGRQ), 6-min walk test (6MWT), incremental shuttle walking test (ISWT), peak inspiratory and expi-ratory fl ow measurements (PIF, PEF), cycloergometry, and densitometry. Th e rehabilitation program is deliv-ered 5 days per week under the supervision of physio-therapists and is comprised of (1) inspiratory (Respifl o™spirometer) and expiratory (Th reshold™ PEP) muscle training and exercises for diff erent breathing techniques (e.g., diaphragmatic, chest, apical) (20–25 minutes twice daily), (2) cycloergometry (20–35 minutes twice daily), which is occasionally accompanied by stair climbing exercises, (3) treadmill workout (10–25 minutes daily), (4) electrostimulation of the quadriceps muscle (25 min-utes twice daily), (5) exercises for fl exibility and strength of upper extremities and thoracic muscles (30 minutes daily). Patients are also instructed about relaxation tech-niques and how to expectorate mucus from the airways.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Heart rate variability in COPD 3
www.copdjournal.com
All participants have regular assessment session and/or program with psychologists, dieticians, and social work-ers, which can be upgraded with additional sessions if needed. Th e intensity of bicycle ergometer training is determined by the supervising physician and is based on initial exercise testing (19, 20).
Treadmill workout intensity was determined using a progressive treadmill test where the slope is gradually increased with respect to patient’s pulse, oxygen satu-ration and patient’s subjective perception of exertion. Th e exercise slope is set to 80% of the maximal incli-nation reached and may be adjusted during training to fi t a patient’s current exercise capacity. Quadriceps muscle electrostimulation intensity is adjusted indi-vidually during each session according to a patient’s threshold for pain and slowly increased during the course of rehabilitation. Th e respiratory muscle train-ing, breathing technique training, exercises for fl ex-ibility and strength of upper extremities and thoracic
muscles program and intensity is initially same for all participants, and is adjusted according to patient pref-erences and ability.
At the end of the 4-week rehabilitation program, patients repeat the initial testing to evaluate their prog-ress and success. Th e following thresholds were set for a clinically relevant diff erence: (1) SGRQ-CRD (clinically relevant diff erence in SGRQ) = reduction of 4 units or more (21); (2) 6MWT-CRD (clinically relevant diff er-ence in 6MWT) = increase of 30 m in distance walked (22); (3) ISWT-CRD (clinically relevant diff erence in ISWT) = increase of 47.5 m in distance walked (23).
ECG recordingTwenty-minute ECG recordings were obtained using the mobile 12-lead electrocardiograph Cardiax PC ECG (IMED Ltd.), self-adhesive chest electrodes, limb clamps, and a personal computer. Patients were in supine position 15 minutes prior to recording and were
Figure 1. Flowchart for patient selection.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Copyright © 2014 Informa Healthcare USA, Inc
4 Zupanic et al.
asked to relax, breathe normally, refrain from moving and talking, but to keep awake during the procedure.
Data acquisition and analysisTh e ECG recordings were analyzed at Th e Jožef Stefan Institute in Ljubljana, Slovenia. RR intervals were deter-mined using NevroEKG software (developed by the Jožef Stefan Institute and the Department of Neurology, University Medical Center Ljubljana) and displayed on Poincaré plots, enabling recognition of cardiac arrhyth-mias. Only NN intervals (RR intervals in which adjacent R-waves are preceded by P-waves) can be used in the spectral analysis methods that were used in the analysis (24), therefore individual premature beats were replaced with interpolated ones, and recordings with too many rhythm disturbances resulting from premature beats or external disturbances were discarded.
Th e GET_HRV program from PhysioToolkit (Physi-oNet http://www.physionet.org) was used for calcula-tion of time- and frequency-domain parameters of HRV (25). Time-domain parameters included the standard deviation of all NN intervals (SDNN), the square root of the mean of the sum of squares diff erences between adjacent NN intervals (RMSSD), and the percentage of pairs of adjacent NN intervals diff ering by more than 50 ms (pNN50). Frequency-domain parameters included absolute powers (ms
2): total power (TP, 0.0033–0.40
Hz); very low frequency power (VLF, 0.0033–0.04 Hz); low frequency power (LF, 0.04–0.15 Hz); and high fre-quency power (HF, 0.15–0.40 Hz). We also determined the LF/HF ratio (LF/HF), LF in normalized units (nuLF =LF/(TP-VLF), and HF in normalized units (nuHF =HF/(TP-VLF). QT intervals were determined from the initial parts of recordings using Cardiax program ver-sion 3.50 (IMED Ltd.). QTc intervals were calculated using Framingham’s formula (QTc = QT + 0.154 (1 − RR)) (26).
Statistical analysisContinuous data are reported as mean and standard deviation. Characteristics of the study participants were compared between groups using the independent samples Student’s t-test for continuous variables and Fisher’s exact test for categorical values. Baseline HRV parameters and QTc were compared between groups using the independent samples Student’s t-test. Baseline and outcome HRV parameters and QTc within groups were compared using a paired samples t-test. Changes of HRV parameters and QTc were compared between groups using the independent samples Student’s t-test. In the case of quadratic values (TP, HF, LF) and values derived from them (nuHF, nuLF, LF/HF), a logarith-mic transformation was performed (ln(x + 1)) and the transformed values were tested using the independent samples Student’s t-test.
Changes in TP, HF, LF, and LF/HF were tested using the exact Mann–Whitney test. Th e association of changes in HRV parameters and clinical test results (SGRQ, 6MWT,
ISWT) was assessed using Pearson’s correlation. Com-parison of HRV parameters, QTc length and rehabilita-tion outcome was performed for patients with or without long-term oxygen therapy (LTOT). Th e level of statistical signifi cance was set at p < 0.05. SPSS (Statistical Package for Social Sciences) for Windows 19.0 (SPSS Inc., Chicago IL, USA) was used for the analysis.
Results
Characteristics of the study participantsTh e demographic and anthropometric characteristics, pulmonary function, and comorbidities of the 62 sub-jects included in the study are shown in Table 1. Healthy individuals and patients with COPD diff ered in smoking preference, therapy for COPD and therapy with ACE-inhibitors. Th ere was a signifi cant diff erence in vitamin D therapy between healthy participants and patients with COPD and between both COPD groups. No other signifi cant intergroup diff erences were recorded, including no intergroup diff erences between therapy in calcium-channel blockers, statins or oral steroids and other pharmacological agents (Appendix Table A1).
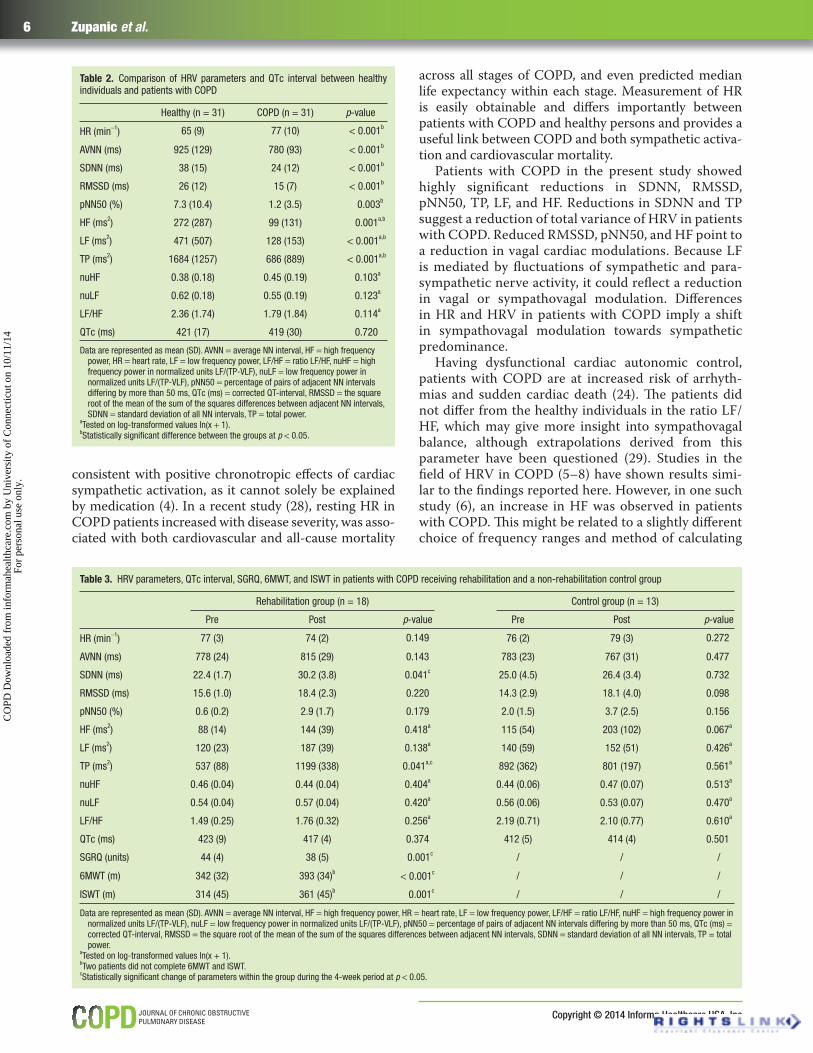
Comparison of HRV markers and QTc in healthy individuals and patients with COPDTh e group of healthy individuals and the patients with COPD showed signifi cant diff erences in HR (p < 0.001), average NN, SDNN, and RMSSD (all p < 0.001), pNN50 (p = 0.003), TP and LF (both p < 0.001), and HF (p =0.001) (Table 2). We found QTc prolongation in ECGs of 13 (42%) patients with COPD and 7 (27%) healthy par-ticipants, although the diff erence was not statistically signifi cant (p = 0.185).
Effect of rehabilitation on HRV parameters, QTc, and clinical testsAt baseline, there were no signifi cant diff erences in HR, HRV, or QTc between the COPD rehabilitation group and the COPD control group (all p > 0.05). After the 4-week period, SDNN changed signifi cantly in the reha-bilitation group (p = 0.041) but not in the control group (p = 0.732) (Table 3, Figure 2). TP also changed signifi -cantly in the rehabilitation group (p = 0.041) compared with the control group (p = 0.561) (Table 3). Th ere were highly signifi cant changes in all clinical test results (SGRQ, 6MWT, ISWT all p ≤ 0.001) within the rehabilitation group: mean SGRQ decreased by 6 units, mean 6MWT increased by 51 m and mean ISWT by 47 m.
As displayed in Figure 2, two patients in the rehabili-tation group had a drop in SDNN during rehabilitation. Th e fi rst patient’s SDNN decreased by 14.7 ms, HR increased by 6 beats per minute, SGRQ decreased by 2 units, 6MWT increased by 5 m and ISWT decreased by 20 m. Th e second patient’s SDNN decreased by 6.7 ms, HR remained unchanged, SGRQ decreased by 2 units, 6MWT increased by 60 m, ISWT increased by 10 m.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Heart rate variability in COPD 5
www.copdjournal.com
Other HRV parameters and QTc showed no significant changes within either group, includ-ing comparison of patients with or without LTOT. Comparison of changes in HRV parameters and QTc that occurred during the 4-week period did not find any statistically significant differences between the groups.
Correlation between HRV, QTc, and clinical testsA signifi cant positive correlation was found between changes in SDNN and clinically relevant diff erences in SGRQ (SGRQ-CRD) (r = 0.538, p = 0.021) – Table 4, Figure 3, whereas no correlation was found between the change in SDNN and change in SGRQ – Table 4 and Figure 4. Th e p-value was 0.069 for the associa-tion between QTc and SGRQ change (ΔQTc, ΔSGRQ) and 0.074 for the association between SGRQ-CRD and change in RMSSD (ΔRMSSD). Th ere was no important correlation between HRV parameters and QTc interval in the 6MWT or ISWT.
Discussion
Compared with healthy individuals, patients with COPD showed reduced time-domain HRV parameters and frequency-domain parameters HF, LF, and TP, implying a shift towards sympathetic predominance. After 4 weeks of comprehensive rehabilitation, the patients performed signifi cantly better in all clinical tests (SGRQ, 6MWT, ISWT) and showed signifi cant increases in SDNN and TP, suggesting a general improvement of HRV, which cor-related with improvement in health-related quality of life.
HR and HRV in COPDCompared with the healthy individuals’ group, the group with COPD had a signifi cantly higher HR, with an average of 77 beats/min, and a signifi cantly lower aver-age NN, its reciprocal value. Other studies (6, 27) have demonstrated similar HRs, diff ering from the present study by a maximum of ± 10 beats/min. Th e fi nding of elevated HR is common in patients with COPD and most
Table 1. Comparison of the characteristics of the healthy individuals and patients with COPD and comparison of the rehabilitation group and non-rehabilitation control group
Characteristics of participantsHealthy(n = 31)
COPD(n = 31) p-value
Rehabilitation(n = 18)
COPD controls(n = 13) p-value
Demographic and anthropo-metric data
Male sexa 13 (42%) 13 (42%) 1.000 7 (39%) 6 (46%) 0.727
Age (years)b 60 (8) 61 (7) 0.671 60 (8) 61 (7) 0.721
Active smokersa 0 4 (13%) / 2 2 1.0
Pack-yearsb 0.1 (0.6) 39.3 (26.2) / 40.2 (27.8) 37.9 (24.7) 0.822
Body-mass indexb 26.5 (3.2) 25.8 (6.7) 0.608 24.0 (5.6) 28.3 (7.5) 0.080
Pulmonary function
GOLD stage III or IVa / 21 (68%) / 13 (87%) 8 (62%) 0.701
VC (%)b / 74 (16) / 74 (19) 75 (13) 0.999
FEV1 (%)b / 37 (20) / 35 (23) 40 (16) 0.465
TI (%)b / 37 (14) / 35 (14) 40 (13) 0.428
Co-morbidities Arterial hypertensiona 6 (19%) 11 (35%) 0.255 5 (28%) 6 (46%) 0.449
HLPa 5 (16%) 7 (23%) 0.749 4 (22%) 3 (23%) 1.0
Pharmacological therapy
ICSa 0 24 (77%) / 14 (78%) 10 (77%) 1.0
SABAa 0 24 (77%) / 15 (83%) 9 (69%) 0.413
LABAa 0 27 (87%) / 17 (94%) 10 (77%) 0.284
Tiotropiuma 0 23 (74%) / 15 (83%) 8 (61%) 0.228
Ipratropiuma 0 12 (39%) / 5 (28%) 7 (54%) 0.262
Theophyllinea 0 7 (23%) / 4 (22%) 3 (23%) 1.0
Montelukasta 0 2 (6%) / 1 (6%) 1 (8%) 1.0
LTOTa 0 8 (26%) / 5 (28%) 3 (23%) 1.0
ACEia 4 (13%) 12 (39%) 0.040 7 (39%) 5 (38%) 1.0
CCBa 2(6%) 6 (19%) 0.255 3 (17%) 3 (23%) 0.676
Statinsa 4 (13%) 7 (23%) 0.301 4 (22%) 3 (23%) 0.558
Oral steroidsa 0 4 (13%) 0.113 4 (22%) 0 0.120
Vitamin Da 1 (3%) 8 (26%) 0.026 8 (44%) 0 0.010
Data are represented as mean (SD). p-values for comparison of smoker status and therapy between healthy individuals and patients with COPD are not listed because these were confound-ing parameters with p-values < 0.001. ACEi = angiotensin converting enzyme inhibitors, CCB = calcium channel blockers, FEV1 (%) = forced expiratory volume in 1 s calculated according to the normative values, HLP = hyperlipidemia, IC S = inhalatory corticosteroids, LABA = long-acting beta agonists, LTOT = long-term oxygen therapy, PPI = proton pump inhibitors, SABA = short-acting beta agonists, TI (%) = Tiffeneau index calculated according to normative values, VC (%) = vital capacity calculated according to normative values.
ap-values calculated using Fisher’s exact test.bp-values calculated using the independent samples Student’s t-test.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.
Copyright © 2014 Informa Healthcare USA, Inc
6 Zupanic et al.
Table 2. Comparison of HRV parameters and QTc interval between healthy individuals and patients with COPD
Healthy (n = 31) COPD (n = 31) p-value
HR (min−1) 65 (9) 77 (10) < 0.001b
AVNN (ms) 925 (129) 780 (93) < 0.001b
SDNN (ms) 38 (15) 24 (12) < 0.001b
RMSSD (ms) 26 (12) 15 (7) < 0.001b
pNN50 (%) 7.3 (10.4) 1.2 (3.5) 0.003b
HF (ms2) 272 (287) 99 (131) 0.001a,b
LF (ms2) 471 (507) 128 (153) < 0.001a,b
TP (ms2) 1684 (1257) 686 (889) < 0.001a,b
nuHF 0.38 (0.18) 0.45 (0.19) 0.103a
nuLF 0.62 (0.18) 0.55 (0.19) 0.123a
LF/HF 2.36 (1.74) 1.79 (1.84) 0.114a
QTc (ms) 421 (17) 419 (30) 0.720
Data are represented as mean (SD). AVNN = average NN interval, HF = high frequency power, HR = heart rate, LF = low frequency power, LF/HF = ratio LF/HF, nuHF = high frequency power in normalized units LF/(TP-VLF), nuLF = low frequency power in normalized units LF/(TP-VLF), pNN50 = percentage of pairs of adjacent NN intervals differing by more than 50 ms, QTc (ms) = corrected QT-interval, RMSSD = the square root of the mean of the sum of the squares differences between adjacent NN intervals, SDNN = standard deviation of all NN intervals, TP = total power.
aTested on log-transformed values ln(x + 1).bStatistically signifi cant difference between the groups at p < 0.05.
Table 3. HRV parameters, QTc interval, SGRQ, 6MWT, and ISWT in patients with COPD receiving rehabilitation and a non-rehabilitation control group
Rehabilitation group (n = 18) Control group (n = 13)
Pre Post p-value Pre Post p-value
HR (min−1) 77 (3) 74 (2) 0.149 76 (2) 79 (3) 0.272
AVNN (ms) 778 (24) 815 (29) 0.143 783 (23) 767 (31) 0.477
SDNN (ms) 22.4 (1.7) 30.2 (3.8) 0.041c 25.0 (4.5) 26.4 (3.4) 0.732
RMSSD (ms) 15.6 (1.0) 18.4 (2.3) 0.220 14.3 (2.9) 18.1 (4.0) 0.098
pNN50 (%) 0.6 (0.2) 2.9 (1.7) 0.179 2.0 (1.5) 3.7 (2.5) 0.156
HF (ms2) 88 (14) 144 (39) 0.418a 115 (54) 203 (102) 0.067a
LF (ms2) 120 (23) 187 (39) 0.138a 140 (59) 152 (51) 0.426a
TP (ms2) 537 (88) 1199 (338) 0.041a,c 892 (362) 801 (197) 0.561a
nuHF 0.46 (0.04) 0.44 (0.04) 0.404a 0.44 (0.06) 0.47 (0.07) 0.513a
nuLF 0.54 (0.04) 0.57 (0.04) 0.420a 0.56 (0.06) 0.53 (0.07) 0.470a
LF/HF 1.49 (0.25) 1.76 (0.32) 0.256a 2.19 (0.71) 2.10 (0.77) 0.610a
QTc (ms) 423 (9) 417 (4) 0.374 412 (5) 414 (4) 0.501
SGRQ (units) 44 (4) 38 (5) 0.001c / / /
6MWT (m) 342 (32) 393 (34)b < 0.001c / / /
ISWT (m) 314 (45) 361 (45)b 0.001c / / /
Data are represented as mean (SD). AVNN = average NN interval, HF = high frequency power, HR = heart rate, LF = low frequency power, LF/HF = ratio LF/HF, nuHF = high frequency power in normalized units LF/(TP-VLF), nuLF = low frequency power in normalized units LF/(TP-VLF), pNN50 = percentage of pairs of adjacent NN intervals differing by more than 50 ms, QTc (ms) = corrected QT-interval, RMSSD = the square root of the mean of the sum of the squares differences between adjacent NN intervals, SDNN = standard deviation of all NN intervals, TP = total power.
aTested on log-transformed values ln(x + 1).bTwo patients did not complete 6MWT and ISWT.cStatistically signifi cant change of parameters within the group during the 4-week period at p < 0.05.
consistent with positive chronotropic eff ects of cardiac sympathetic activation, as it cannot solely be explained by medication (4). In a recent study (28), resting HR in COPD patients increased with disease severity, was asso-ciated with both cardiovascular and all-cause mortality
across all stages of COPD, and even predicted median life expectancy within each stage. Measurement of HR is easily obtainable and diff ers importantly between patients with COPD and healthy persons and provides a useful link between COPD and both sympathetic activa-tion and cardiovascular mortality.
Patients with COPD in the present study showed highly signifi cant reductions in SDNN, RMSSD, pNN50, TP, LF, and HF. Reductions in SDNN and TP suggest a reduction of total variance of HRV in patients with COPD. Reduced RMSSD, pNN50, and HF point to a reduction in vagal cardiac modulations. Because LF is mediated by fl uctuations of sympathetic and para-sympathetic nerve activity, it could refl ect a reduction in vagal or sympathovagal modulation. Diff erences in HR and HRV in patients with COPD imply a shift in sympathovagal modulation towards sympathetic predominance.
Having dysfunctional cardiac autonomic control, patients with COPD are at increased risk of arrhyth-mias and sudden cardiac death (24). Th e patients did not diff er from the healthy individuals in the ratio LF/HF, which may give more insight into sympathovagal balance, although extrapolations derived from this parameter have been questioned (29). Studies in the fi eld of HRV in COPD (5–8) have shown results simi-lar to the fi ndings reported here. However, in one such study (6), an increase in HF was observed in patients with COPD. Th is might be related to a slightly diff erent choice of frequency ranges and method of calculating
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Heart rate variability in COPD 7
www.copdjournal.com
Parameters of HRV that increased signifi cantly dur-ing rehabilitation were SDNN and TP. Th ese measure-ments represent total variance and are also time- and frequency-domain correlates (24). SDNN is one of the top two prognostic time-domain parameters of HRV (24), and its improvement therefore represents an important eff ect of rehabilitation. SDNN has also been shown to increase after 12 weeks of high intensity train-ing (16) and after 7 weeks of resistance training (17). Th e TP value increased close to that in the healthy individu-als, also confi rming a positive eff ect of rehabilitation.
TP has not been addressed in previous rehabilitation studies, although it has been utilized in other fi elds. Sig-nifi cant decreases in TP were observed after coronary artery bypass surgery and its use in evaluation of surgical techniques has been demonstrated (30). In the present
normalized values, or to the use of a parametric test or, as has been suggested (5), may be an eff ect of medica-tion withdrawal.
Changes in clinical test results and HRV after rehabilitation
As expected, the patients performed signifi cantly better in all clinical tests after 4 weeks of rehabilitation. Th e average improvement in SGRQ and 6MWT results are within limits for a clinically relevant diff erence, as reported recently (21, 22). Although the ISWT distance increased 0.5 m less than the minimum clinically rel-evant diff erence (23), it was nevertheless a statistically signifi cant improvement. Th e results demonstrate that rehabilitation was successful in terms of increasing exer-cise capacity and health-related quality of life.
Figure 2. Change in SDNN in patients with COPD receiving rehabilitation and in the COPD control group.
Table 4. Correlation between change in QTc, SDNN, and RMSSD and tests of rehabilitation outcome in patients with COPD receiving rehabilitation
ΔSGRQ Δ6MWT ΔISWT SGRQ-CRD 6MWT-CRD ISWT-CRD
ΔQTc r = −0.369p = 0.132
r = 0.174a
p = 0.519r = 0.364a
p = 0.166r = 0.369p = 0.132
r = 0.197a
p = 0.465r = 0.320a
p = 0.226
ΔSDNN r = −0.244p = 0.329
r = 0.076a
p = 0.779r = 0.420a
p = 0.106r = 0.539p = 0.021b
r = 0.193a
p = 0.474r = 0.190a
p = 0.481
ΔRMSSD r = −0.024p = 0.925
r = 0.330a
p = 0.213r = 0.242a
p = 0.367r = 0.432p = 0.074
r = 0.352a
p = 0.182r = 0.107a
p = 0.693
r = Pearson’s correlation coeffi cient, ΔQTc = change in corrected QT-interval, ΔRMSSD = change in the square root of the mean of the sum of the squares differences between adjacent NN intervals, ΔSDNN = change in standard deviation of all NN intervals, ΔSGRQ = change in St. George’s respiratory questionnaire, SGRQ-CRD = clinically relevant difference in SGRQ, Δ6MWT =change in 6-min walk test, 6MWT-CRD = clinically relevant difference in 6MWT, ΔISWT = change in incremental shuttle walking test, ISWT-CRD = clinically relevant difference in ISWT.
aTwo patients did not complete 6MWT and ISWT.bStatistically signifi cant correlations at p < 0.05.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Copyright © 2014 Informa Healthcare USA, Inc
8 Zupanic et al.
study, a great part of the increase in TP was attributable to VLF, but little is known about physiological correlates of this parameter (24). Th e improvements in several HRV parameters may indicate improvement in physical fi tness (24), the eff ects of rehabilitation on COPD as a systemic disease, or changes in autonomic system activ-ity; the improvements may also be fl uctuations.
Even with the benefi cial eff ects on HRV, it needs to be noted that rehabilitation cannot restore the HRV parameters to a level as seen in healthy individuals. Th is implies a need for additional research on the revers-ibility of HRV changes in COPD, linked to their etiol-
ogy and pathophysiology in the disease, and the scope of improvement possible with various modalities and duration of rehabilitation. According to our results, and considering the problems with small sample statistical analysis, the LTOT seems not to have clinically relevant implication.
Th is study has demonstrated a correlation between the change in SDNN and SGRQ-CRD, confi rming the concept that changes in HRV are linked to effi cacy of rehabilitation. Th e patients took part in a compre-hensive rehabilitation program, therefore the initial improvements in a test evaluating health-related qual-ity of life and its correlation with a total HRV parameter was expected. Similarly, in a study (15) on the eff ects of aerobic exercise training on HRV in patients with COPD, a correlation was observed between changes in 6MWT distance and RMSSD during submaximal ambulation.
Additionally, we observed a decrease in SDNN in two patients receiving rehabilitation (Figure 2). Such fi nding needs to be interpreted in light of limited or no rehabili-tation benefi t as demonstrated by the exercise capacity tests and quality of life questionnaires. Also, a higher average HR at follow-up recording could contribute to reduction of SDNN (31).
QTc interval in COPD and changes after rehabilitationAmong the 31 patients with COPD, 13 (42%) showed pro-longation of QTc interval. In a larger study (12), QTc pro-longation was found in 37% of 1001 patients with COPD, which suggests that the patients in the present study were comparable, in that aspect, to a larger population of patients. Nevertheless, the average QTc in the present patients was not prolonged and did not signifi cantly diff er from QTc length in the healthy individuals.
Similarly, the average QTc of the COPD rehabilita-tion group was 443 ms before and 432 ms after reha-bilitation. Th e decrease during the program was not signifi cant, but no extensive prolongation was present at baseline. In a study of HRV and QT parameters after off -pump coronary artery bypass surgery (30), changes in HRV parameters and QT variability index were observed, with no signifi cant changes occuring in mean QT or QTc, thus the former might be more sensitive indicators of autonomic function. On the other hand, in a study (32) on the eff ects of an intensive 6-month training program on QTc in an elderly population, changes in the level of repolarization were observed to occur later in the course of clinical improvement, and the importance of adequate rehabilitation for the long term was stressed. Prolongation of QTc has been demonstrated to increase mortality risk in a healthy population (33) and in hypoxemic patients with COPD (11) and has been linked to autonomic neuropathy in COPD (11). Th us, further research into the eff ect of rehabilitation on this parameter in a larger group of patients or a group undergoing a longer rehabilitation program is warranted.
Figure 3. Correlation between clinically relevant difference in St. George’s respiratory questionnaire (SGRQ-CRD) and change in SDNN in the patients with COPD receiving rehabilitation.
Figure 4. Correlation of change in St. George’s respiratory questionnaire and change in SDNN in the patients with COPD receiving rehabilitation (r = −0.244 p =0.329). A negative change in SGRQ represents improvement.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Heart rate variability in COPD 9
www.copdjournal.com
Study limitationsTh e results of the study need to be interpreted with regard to some limitations. First, the number of subjects is inversely related to statistical power, in particular for variables with high intersubject variability (34). However, this issue is shared with other studies in the fi eld, where similarly small numbers of patients were recruited.
Second, breathing depth and frequency were not con-trolled during recordings (29). Bartels et al. (35) showed HRV in COPD is reproducible in 5-minute recordings with controlled respiratory rate and oxygen saturation. Studies on how a fi xed respiratory rate aff ects HRV in general are inconsistent: it may lower LF (36), increase HF (23), cause upset and loss of vagal tone (37). Mental eff ort may contribute to HF decrease (38). In COPD, controlled breathing for 20 minutes might increase sym-pathetic tone. Controlled breathing tailored to the indi-vidual's resting breathing pattern could have improved our study. Even so, rehabilitation participants all had average breathing rates of 9-20 breaths per minute, within which HF diff ers at most by very small amounts when comparing spontaneous and metronome-guided breathing (39).
Last, there were diff erences between patients and healthy individuals in therapy shown or speculated to aff ect HRV (ACE-inhibitors, inhaled beta-agonists, cor-ticosteroids and anticholinergic drugs) and vitamin D, the latter not shown to aff ect HRV. Primary concerns for interpretation of our results represent ACE-inhibi-tors, which have the potential to increase time-domain indexes, mostly through an increase HF and/or decrease LF (40–42). Even with anticipated protective eff ect, the diff erence in indices of HRV between healthy individu-als and patients with COPD was signifi cant (Table 2), suggesting that COPD indeed worsens HRV parameters to a signifi cant extent.
Clinical implicationsTh e ECG is a simple, reliable and noninvasive bedside investigation and it has been suggested that it might become a routine investigation in management of COPD (12, 25). In particular, 20-min ECGs are advantageous as they are also suitable for subsequent non-linear HRV analyses in a time frame where stationary conditions are feasible. For fi eld tests and clinical practice, Polar heart rate monitors could serve as an attractive alternative, provided we do not need information beyond R-R inter-vals and estimates of HRV.
Th e established initial diff erences in HRV between patients with COPD and healthy individuals demon-strate how HRV analysis might be useful for determina-tion of autonomic dysfunction and even risk assessment in COPD. Future studies should assess the long-term eff ects of rehabilitation-induced ECG changes and the potential implications for patient-related outcome. Comparison of stationary and ambulatory rehabilita-tion programs would also be relevant for implications in clinical practice.
Conclusions
Compared with healthy individuals, patients with COPD demonstrate reduced parameters of HRV, and quantifi -cation of these parameters allows determination of the level of autonomic dysfunction in this disease. Compre-hensive rehabilitation not only improves exercise capac-ity and health-related quality of life in these patients but also improves several HRV parameters. Th e fi ndings of this study confi rm that HRV is potentially useful for determination and even quantifi cation of autonomic dysfunction in patients with COPD. Further research on how HRV could be used in risk assessment and evalua-tion of therapeutic intervention is therefore warranted.
Declaration of Interest Statement
Th e authors report no confl icts of interest. Th e authors are responsible for the content and writing of this paper. Th e research was supported by funding from the European Union Seventh Framework Programme (FP7/2007-2013) under Grant Agreement No. 241558 (SICA-HF).
References 1. Curkendall SM, DeLuise C, Jones JK, et al. Cardiovascular
disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada: cardiovascular disease in COPD patients. Ann Epidemiol 2006; 16(1):63–70.
2. Lainscak M, Dagres N, Filippatos GS, et al. Atrial fi brillation in chronic non-cardiac disease: where do we stand? Int J Cardiol 2008; 128(3):311–315.
3. Van Gestel AJ, Steier J. Autonomic dysfunction in patients with chronic obstructive pulmonary disease (COPD). J Th orac Dis 2010; 2(4):215–222.
4. Andreas S, Anker SD, Scanlon PD, et al. Neurohumoral activation as a link to systemic manifestations of chronic lung disease. Chest 2005; 128(5):3618–3624.
5. Stein PK, Nelson P, Rottman JN, et al. Heart rate variability refl ects severity of COPD in PiZ α1-antitrypsin defi ciency. Chest 1998; 113(2):327–333.
6. Volterrani M, Scalvini S, Mazzuero G, et al. Decreased heart rate variability in patients with chronic obstructive pulmonary disease. Chest 1994; 106(5):1432–1437.
7. Gunduz H, Talay F, Arinc H, et al. Heart rate variability and heart rate turbulence in patients with chronic obstructive pulmonary disease. Cardiol J 2009; 16(6):553–559.
8. Chen WL, Chen GY, Kuo CD. Hypoxemia and autonomic nervous dysfunction in patients with chronic obstructive pulmonary disease. Respir Med 2006; 100(9): 1547–1553.
9. Van Gestel AJ, Kohler M, Steier J, et al. Cardiac autonomic dysfunction and health-related quality of life in patients with chronic obstructive pulmonary disease. Respirology 2011; 16(6):939–946.
10. Tükek T, Yildiz P, Atilgan D, et al. Eff ect of diurnal variability of heart rate on development of arrhythmia in patients with chronic obstructive pulmonary disease. Int J Cardiol 2003; 88(2–3):199–206.
11. Stewart AG, Waterhouse JC, Howard P. Th e QTc interval, autonomic neuropathy and mortality in hypoxaemic COPD. Respir Med 1995; 89(2): 79–84.
12. Bones U, Zabret M, Sarc I et al. Electrocardiogram analysis and survival of patients with chronic obstructive pulmonary disease. Chest 2011; 140(4_Meeting abstracts):575A.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Copyright © 2014 Informa Healthcare USA, Inc
10 Zupanic et al.
13. Sarc I, Jeric T, Ziherl K, et al. Adherence to treatment guidelines and long-term survival in hospitalized patients with chronic obstructive pulmonary disease. J Eval Clin Pract 2011; 17(4):737–743.
14. Bolton CE, Bevan-Smith EF, Blakey JD, et al. British Th oracic Society guideline on pulmonary rehabilitation in adults: accredited by NICE. Th orax 2013; 68 Suppl 2:ii1–ii30.
15. Borghi-Silva A, Arena R, Castello V, et al. Aerobic exercise training improves autonomic nervous control in patients with COPD. Respir Med 2009; 103(10):1503–1510.
16. Camillo CA, Laburu Vde M, Gonçalves NS, et al. Improvement of heart rate variability after exercise training and its predictors in COPD. Resp Med 2011; 105(7):1054–1062.
17. Ricci-Vitor AL, Bonfi m R, Fosco LC, et al. Infl uence of the resistance training on heart rate variability, functional capacity and muscle strength in the chronic obstructive pulmonary disease. Eur J Phys Rehabil Med 2013; 49(6):793–810.
18. Weippert M, Kumar M, Kreuzfeld S, et al. Comparison of three mobile devices for measuring R-R intervals and heart rate variability: Polar S810i, Suunto t6 and an ambulatory ECG system. Eur J Appl Physiol 2010; 109(4):779–786.
19. Spruit MA, Singh SJ, Garvey C, et al. An offi cial American Th oracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med 2013; 188(8):e13–64.
20. Gloeckl R, Marinov B, Pitta F. Practical recommendations for exercise training in patients with COPD. Eur Respir Rev 2013; 22(128):178–186.
21. Jones PW. Interpreting thresholds for a clinically signifi cant change in health status in asthma and COPD. Eur Respir J 2002; 19(3):398–404.
22. Polkey MI, Spruit MA, Edwards LD, et al. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important diff erence for death or hospitalization. Am J Respir Crit Care Med 2013; 187(4):382–386.
23. Singh SJ, Jones PW, Evans R, et al. Minimum clinically important improvement for the incremental shuttle walking test. Th orax 2008; 63(9):775–777.
24. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J 1996; 17(3):354–381.
25. Goldberger AL, Amaral LA, Glass L, et al. PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation 2000; 101(23):E215–220.
26. Sagie A, Larson MG, Goldberg RJ, et al. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol. 1992; 70(7):797–801.
27. Warnier MJ, Rutten FH, Numans ME, et al. Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease. COPD 2013; 10(1):62–71.
28. Jensen MT, Marott JL, Lange P, et al. Resting heart rate is a predictor of mortality in COPD. Eur Respir J 2013; 42(2):341–349.
29. Eckberg DL. Sympathovagal balance. A critical appraisal. Circulation 1997; 96:3224–3232.
30. Kalisnik JM, Avbelj V, Trobec R, et al. Assessment of cardiac autonomic regulation and ventricular repolarization after off -pump coronary artery bypass grafting. Heart Surg Forum 2006; 9(3):E661–E667.
31. Billman GE. Th e eff ect of heart rate on the heart rate variability response to autonomic interventions. Front Physiol 2013; 4:222.
32. Schuit AJ, Dekker JM, de Vegt F, et al. Eff ect of physical training on QTc interval in elderly people. J Electrocardiol 1998; 31(2):111–116.
33. de Bruyne MC, Hoes AW, Kors JA, et al. Prolonged QT interval predicts cardiac and all-cause mortality in the elderly. Th e Rotterdam Study. Eur Heart J 1999; 20(4):278–284.
34. Pinna GD, Maestri R, Torunski A, et al. Heart rate variability measures: a fresh look at reliability. Clin Sci (Lond) 2007; 113(3):131–140.
35. Bartels MN, Jelic S, Gonzalez JM, et al. Reproducibility of heart rate and blood pressure variability in patients with chronic obstructive pulmonary disease. Clin Auton Res 2004; 14(3):194–196.
36. Kobayashi H. Does paced breathing improve the reproducibility of heart rate variability measurements? J Physiol Anthropol 2009; 28(5):225–230.
37. De Meersman RE, Reisman SS, Daum M, et al. Infl uence of respiration on metabolic, hemodynamic, psychometric, and R-R interval power spectral parameters. Am J Physiol 1995; 269(4 Pt 2):H1437–1440.
38. Sloan RP, Korten JB, Myers MM. Components of heart rate reactivity during mental arithmetic with and without speaking. Physiol Behav 1991; 50(5):1039–1045.
39. Bloomfi eld DM, Magnano A, Bigger JT Jr, et al. Comparison of spontaneous vs. metronome-guided breathing on assessment of vagal modulation using RR variability. Am J Physiol Heart Circ Physiol 2001; 280(3):H1145–1150.
40. Kontopoulos AG, Athyros VG, Papageorgiou AA, et al. Eff ect of angiotensin-converting enzyme inhibitors on the power spectrum of heart rate variability in post-myocardial infarction patients. Coron Artery Dis 1997; 8(8–9):517–524.
41. Kontopoulos AG, Athyros VG, Didangelos TP, et al. Eff ect of chronic quinapril administration on heart rate variability in patients with diabetic autonomic neuropathy. Diabetes Care 1997; 20(3):355–61.
42. Athyros VG, Didangelos TP, Karamitsos DT, et al. Long-term eff ect of converting enzyme inhibition on circadian sympathetic and parasympathetic modulation in patients with diabetic autonomic neuropathy. Acta Cardiol 1998; 53(4):201–209.
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.

Heart rate variability in COPD 11
www.copdjournal.com
Table A1. Pharmacological therapy in study participants
Healthy(n = 31)
COPD(n = 31)
Rehabilitation(n = 18)
COPD controls(n = 13)
Thiazide and thiazide-like diuretics 1 2 3 3
Loop diuretics 1 3 4 0
ARBs 1 0 0 0
Bisphosphonates 4 0 4 0
Calcium carbonate 5 0 5 2
PPI 6 1 7 2
NSAID 2 4 6 4
Antihistamines 2 1 0 1
BDZ 0 3 1 2
Warfarin 0 2 2 0
Ezetimibe 0 1 0 1
Tamsulozine 0 1 0 1
Casodex 0 1 0 1
Opioid analgetics 1 1 0 1
SSRI 1 1 0 1
Mirtazapine 0 1 1 0
Flupentixol 0 1 0 1
AED 0 1 0 1
AED – antiepileptic drugs; ARBs - angiotensin receptor blockers; BDZ – benzodiazepines; NSAID - non-steroidal anti-infl ammatory drugs; PPI – proton pumb inhibitors; SSRI - selective serotonin reuptake inhibitors.
No intergroup differences were observed.
Appendix
CO
PD D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/1
1/14
For
pers
onal
use
onl
y.