the effect of smear layer removal on e. faecalis leakage
TRANSCRIPT
RESEARCH ARTICLE Open Access
The effect of smear layer removal on E.faecalis leakage and bond strength of fourresin-based root canal sealersLaura Andriukaitiene1,6*† , Xiaobo Song2†, Nannan Yang3, Lippo V. J. Lassila4, Pekka K. Vallittu4,5 and Eero Kerosuo1
Abstract
Background: The aim of the study was to assess bacterial sealability and bonding ability of methacrylate-basedResilon (RS, SybronEndo), Endo Rez (ER, Ultradent Products Inc), and epoxy-based AH Plus (AH, Dentsply/DeTrey),MTA Fill Apex (MTAF, Angelus Soluções Odontológicas) root canal sealers, and the effect of the smear layer removalon the sealability.
Methods: One hundred thirty root segments were instrumented up to apical size #60 and rinsed with 2.5% NaOCl.Half of the roots were rinsed with 5ml 17% EDTA to remove the smear layer. All the roots were filled with AH, ER,MTAF sealers and gutta-percha, or RS with Resilon cones. After storage at 37°C for 7 days the samples weremounted into bacterial leakage assay for 50 days.Another 100 roots were instrumented and rinsed as described above, split longitudinally, cut into the cervical,middle and apical parts. The sealers were injected through the plastic mould on the dentin surface. After 7 days ofincubation at 37°C, bond strength was tested using a notched-edge test fixture (Crosshead, Ultradent Products Inc.)and a universal testing machine (Lloyd Instruments).
Results: AH revealed the longest mean time for bacterial resistance by 29.4 and 36.8 days (with and without smearlayer, respectively) followed by RS (15.1 and 24.7 days, respectively). The difference between materials wassignificant (p<0.001).Bond strength values ranged from 0.2± 0.1 to 3.5± 0.7 MPa and increased from the apical to the cervical third. Inthe apical third, AH showed the highest mean (SD) bond values 1.4 (0.4) MPa and 1.7 (0.6) MPa (with and withoutsmear, respectively, followed by RS, 0.5 (0.1) MPa and 0.8 (0.1) MPa, respectively. The difference between materialswas significant (p=0.001).
Conclusion: The effect of the smear layer removal on the sealability was material-dependent.
Keywords: Root canal sealers, Bond strength, Bacterial leakage, Smear layer
BackgroundThe main cause of pulpal and periradicular pathosis ismicroorganisms and their by-products in the root canalsystem [1]. Root canal treatment aims to eliminate mi-crobes from an infected root canal and to seal the canalsystem to prevent bacteria ingress from the oral cavity[2] and to entomb any residual bacteria [3].
Ørstavik et al. [4] postulated that a correlation shouldexist between adhesive properties of a root canal sealerand its sealability. Although methacrylate-based sealersEndo Rez (ER, Ultradent Products Inc., South Jordan,UT) and Epiphany/ Resilon (RS, SybronEndo, Orange,CA) produce longer and more frequent resin tags todentinal tubules, compared to epoxy resin-based AHPlus (AH, Dentsply/ DeTrey, Konstanz, Germany), thelatter has shown significantly higher bond strengthvalues [5]. Studies reporting both bond and sealabilityare sparse. Eldeniz et al [5, 6] found no significant differ-ence in the sealability between AH and ER, although AH
* Correspondence: [email protected]; [email protected]†Laura Andriukaitiene and Xiaobo Song contributed equally to this work.1Department of Clinical Dentistry, Faculty of Health Sciences, UiT The ArcticUniversity of Norway, N-9037 Tromso, Norway6Present address: Vilnius, Vilnius, LithuaniaFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Andriukaitiene et al. BMC Oral Health (2018) 18:213 https://doi.org/10.1186/s12903-018-0655-7

had three-times higher bond strength. Similar lack ofcorrelation between bond and sealability has been shownwith AH, compared to a salicylate-based sealer [7, 8].In order to enable disinfectants to reach the bacteria
from the dentinal tubules, the removal of the smearlayer before intracanal medication and filling of root ca-nals is widely advocated [9]. The final rinse of root canalwith NaOCl and 17% EDTA was confirmed as the mosteffective combination in the removal of the smear layer[10]. This was supposed to increase the adhesion andsealability of a filing [11]. But in contrast, Saleh et al. [7]found that EDTA did not increase the bond strength ofany tested materials, including AH. Moreover, the sameresearch group in another study found that the use ofEDTA did not improve the sealability of any of thetested material, including AH and RS [8].The aims of this study were therefore to assess the
bacterial sealability and bonding ability of two meth-acrylate resin-based root canal sealers, ER and RS, andtwo epoxy-based sealers, AH and MTA Fill Apex(MTAF) (Angelus Soluções Odontológicas, Londrina,PR, Brazil), and to test the hypothesis that the removalof the smear layer would improve the sealability.
Materials and MethodsTested materialsTwo methacrylate resin-based sealers Endo Rez (ER,Ultradent Products Inc., South Jordan, UT) and Epiph-any/ Resilon (RS, SybronEndo, Orange, CA) and twoepoxy-based sealers AH Plus (AH, Dentsply/ DeTrey,Konstanz, Germany) and MTA Fill Apex (MTAF) (An-gelus Soluções Odontológicas, Londrina, PR, Brazil)were used in this study.
Selection of the teethA total of 230 human maxillary central incisors ex-tracted for reason not related to this study were used.Periapical radiographs (Bel-Ray II AC, Belmont Equip-ment, Somerset, NJ, USA) were taken in mesio-distaland bucco-lingual planes to exclude severe root canalcalcification, apical curvatures, or any resorptive alter-ation of the canal lumen. All the teeth were subject tosurface disinfection by immersion in 0.5% Chloramine T,followed by removal of all adhering soft tissues and deb-ris by scaling, washed under running tap water, placed indistilled water, and refrigerated at 4C° for 24 hours be-fore use.
Preparation of the samples for bacterial leakage assayThe crowns of 130 teeth were removed with a diamondbur in a high-speed hand piece under water-cooling,leaving 10mm of the root segment. All roots wereinspected for the presence of cracks with a stereomicro-scope under x40 magnification. ProTaper Universal NiTi
rotary files (Dentsply/Maillefer, Ballaigues, Switzerland)were used to prepare each root canal to size #50 andstainless steel K-files (Dentsply/Maillefer) to finish prep-aration up to size #60. The root canals were irrigatedwith 2.5% 3ml NaOCl after the use of each file. All theroots were randomly divided into two groups. Half of in-strumented roots were rinsed with 5ml of 17% EDTAfor 5 min to remove the smear layer [12, 13]. Distilledwater was finally used to rinse the roots thoroughly. Allthe roots were autoclaved at 121+/- 2°C for 20 min.After sterilization, the root canals were dried with sterilepaper points (Dentsply/Maillefer). All the roots with andwithout the smear layer were assigned to eight experi-mental subgroups (n=15) and two control groups (n=5)as shown in Table 1. All the tested sealers were mixedaccording to manufacturer’s instructions and appliedinto the root canals on the master gutta-percha (GP)cone size #60 (Dentsply/Maillefer) or Resilon cones(SybronEndo), respectively. The canals were obturatedwith the lateral condensation method. Additional GPcones size A (Dentsply/Maillefer) were placed after lat-eral compression with same size spreader until the cer-vical part of the root was filled. Eventually excess GPfrom the coronal part was removed with a heated handplugger and condensed vertically. Aseptic techniqueswere employed throughout the procedure. The speci-mens were kept in sealed tubes with sterile water at 37°C for 7 days to allow the sealers to set. The positive con-trols prepared and rinsed with EDTA as described abovewere obturated without a sealer (core material only),simulating poor obturation.
Bacterial leakage assayThe two-chamber microleakage device [8, 14] was usedwith minor modifications. The specimens were insertedthrough a cut tip of 15ml polyethylene tubes (upperchambers), leaving 3mm of the cervical part inside thetube and the remaining part hanging out of it. Meltedsticky wax was first applied on the outer surface of the3mm cervical part, leaving the surface with the canal ori-fice exposed in the experimental and positive controlgroups, but fully covering it in the negative control group.Thereafter the wax was applied on the hanging part of theroot and the tube interface, leaving 3mm of the apical partuncovered similarly in all the groups. These mounts werethen tightly sealed with sticky wax to sterile 50 ml poly-ethylene tubes (lower chambers) containing 8 ml of sterileTrypticase Soy Broth (TSB; Oxoid Ltd, Basingstoke, UK).The apices extruding from the upper chambers werehanging vertically 2mm in the broth.Enterococcus faecalis ATCC 29212 was used as the test
strain. After growing in TSB at 37°C overnight, 3ml ofthe overnight bacterial culture was added to each upperchamber. The mounts were incubated at 37°C for 50
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 2 of 9

days. The bacterial culture in the upper chamber was re-placed with fresh bacterial every second day to maintainbacterial sufficiency and viability. The bottom chambersof all the mounts were checked every second day for tur-bidity, the evidence for bacterial penetration along theroot canal filling.On observation of turbidity, the seal was broken and the
bacterial cultures were then streaked on Trypticase SoyAgar (TSA; EMD Millipore Corporation, Billerica, MA,USA) plates for colony morphology observation and PCRidentification. The bacteria growing on 25 plates, ran-domly chosen from the eight experimental subgroups,were identified by PCR assay with species-specific primerstargeting E. faecalis 16S rRNA [15]. The date of leakagewas recorded for each leaking sample.
Preparation of the samples for bond testingThe method previously described by Jessop [16] wasused with minor modifications for the preparation andtesting of the samples.One hundred teeth were decoronated at the
cement-enamel junction using a slow speeddiamond-watering blade (Ernst Leitz GmbH, Wetzlar,Germany), split longitudinally in the bucco-lingual direc-tion and inspected for presence of cracks with a stereo-microscope under x40 magnification, grounded on awater-irrigated grinding wheel (Struers LaboPol-21) untilsmooth and flat surface, using 2000-grit (FEPA) silicon car-bide paper and cut into three parts: cervical, middle, andapical. Each specimen was fixed in the acrylic resin (Her-aeus Kulzer Dental GmbH, Laboratory Products Division,
Hanau, Germany). All the roots were divided into twogroups according to the final exposed dentin surface treat-ment. In group A, the smear layer was removed by rinsingeach specimen with 3ml 2.5%NaOCl solution for 1min,followed by 3ml 17%EDTA for 1min. Group B specimenswere irrigated for 1min only with 3ml 2.5% NaOCl.Each group was divided into five subgroups: i) AH was
injected into the plastic mould, with 2.4 mm diameter and2mm cylindrical button height (Ultradent Products Inc.South Jordan, UT, USA) on the root dentin bonding sur-face, ii) RS was similarly applied and light-cured for 40 secaccording to manufacturer’s instructions, iii) MTAF andiv) ER were applied as AH, v) composite specimens wereprepared according to manufacturer’s instructions by ap-plying 3M ESPE Scotchbond Etchant, Adhesive and Pri-mer (3M Dental Products, St. Paul, MN, USA) on thedentin specimens. Finally, the composite 3M ESPE FiltecSupreme XP was packed through the mould on the bond-ing surface and light-cured for 20 sec. All the sampleswere left for 8 hours in a water bath at the roomtemperature and the jig was removed. Afterwards theywere placed in an incubator at 37°C and 100% humidityfor 7 days. For comparison, every third crown was usedfor testing the dentin bonding to simulate a restorativeprocedure in a class III standard cavity (1.5 mm deep).
Bond strength testingThe specimens were tested using a notched-edge sheartest fixture (Crosshead, Ultradent Products Inc.) on auniversal testing machine (Lloyd LRX; Lloyd Instru-ments, Fareham Hants, UK) and the results expressed in
Table 1 The tested materials, their codes, and the number of specimens in each group for the bacterial leakage and bond strengthexperiments
Material Code Experiment
Leakage(n)
Bond (n)
Apical Middle Cervical
AH Plus/GP w/ EDTA AH-ns 15 8 8 9
AH Plus/GP w/o EDTA AH-s 15 8 10 10
EndoRez/ w/ EDTA ER-ns 15 7 8 8
EndoRez/GP w/o EDTA ER-s 15 7 7 8
RealSeal/Resilon w/ EDTA RS-ns 15 9 8 9
RealSeal/Resilon w/o EDTA RS-s 15 9 8 9
MTA Fill Apex/GP w/ EDTA MTAF-ns 15 8 9 8
MTA Fill Apex/GP w/o EDTA MTAF-s 15 7 7 7
Composite w/ EDTA Composite-ns - 10 9 10
Composite w/o EDTA Composite-s - 9 9 10
Positive control w/ EDTA PC 5a 30b
Negative control w/o EDTA NC 5c
n number of specimens, GP gutta-percha, w/ with, w/o without, ns smear layer removed, s smear layer left in situaRoot canals obturated with core material only, simulating poor obturationbTested materials were applied on every third crown with class III standard cavity as described abovecNo root canal filling, just sealing coronal and apical part of the root with the sticky wax
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 3 of 9
MPa by diving the force needed to break the bond (N)by the surface area in mm2. Failure modes obtained bythe shear-bond testing were reported and a mean andstandard deviation calculated.
Statistical AnalysisThe group size of 15 was considered appropriate in thisex vivo study. Too limited or inconsistent data in theprevious literature does not allow to estimate a goldenstandard to which the other materials can be compared.In the leakage assay, the Kaplan Meier test for sur-
vival analysis was used. The median time of leakagewas calculated and pairwise comparisons of groupswere performed by using the log-rank test. Bondstrength between the groups was analysed using theTwo-way ANOVA with Tukey’s post hoc test. Datawere entered and analysed by the statistical programpackage IBM SPSS statistics 21.0 (IBM, Somers, NewYork, NY, USA).
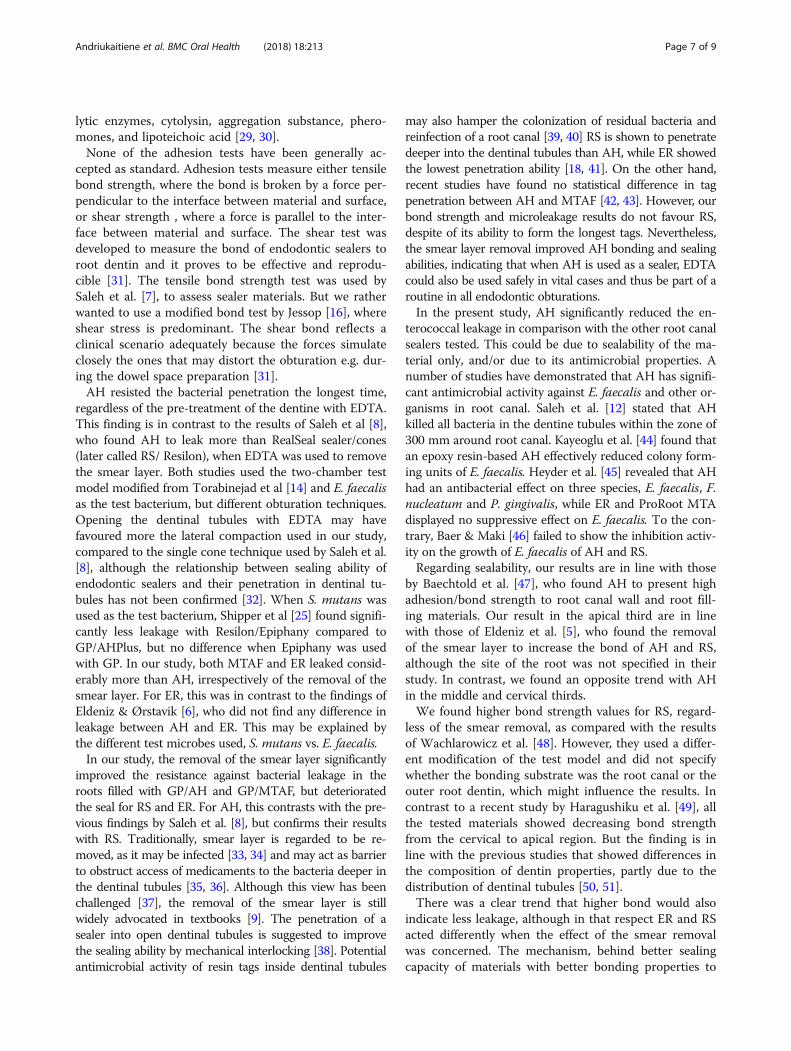
ResultsBacterial leakage assayAll the cell colonies on TSA plates appeared as small,smooth, cream or white colonies with entire edges andwere identical to those of E. faecalis ATCC 29212. ThePCR assay revealed 23 samples showing one band at thesame size as 137 bp of positive control of E. faecalisATCC 29212 and two samples showing one band a bitlower than the positive control (Fig. 1). Further DNA se-quencing confirmed that these two strains were also E.faecalis ATCC 29212 having 99-100% sequence identity.
All the samples leaked within 41 days (range 6-41days), except the negative controls (N=5) whichremained without leakage throughout the 50 days testperiod. All the positive controls (N=5) samples leakedon the second day (Table 2).The Kaplan-Meir survival curves showed that the
AH-ns group significantly differed from all the othergroups (p<0.001; Mantel-Cox Chi-square analysis) (Fig. 2).
Bond strength testAll the tested sealer materials showed an increase inbond strength when going from the apical region to-wards the crown. Bonding to the crown dentin after theremoval of the smear layer with composite resin, used asa reference material, showed the highest strength values,13.7±1.5 MPa (Table 3). The strength values of thesealers bonded to the root canal wall dentine rangedfrom 0.2± 0.1 to 3.5± 0.7 MPa, depending on the mater-ial, location or removal of the smear layer with EDTA(Table 3). The removal of the smear layer increased thebond strength of all the sealers in all thirds of the root,except in the AH group in the cervical and middle thirdof the root and in the MTAF group in the cervical third,but none of the differences were statistically significantwhen tested by Tukey’s pairwise comparisons (P>0.05)(Table 3). In all the tested root dentin sites, the compos-ite resin used for the reference showed significantlyhigher (P<0.001) bonding values (range from 3.1±0.5 to10.8±1.9 MPa) compared to any of the sealers, irrespect-ive of the site of the tooth or the smear layer removal(Table 3). In the apical third, AH showed highest bond
Fig. 1 PCR profiles of 16S rRNA gene from the bacterial samples in lower chamber. The lanes of ladder are 1 kb plus ladder; the lanes of 1-25 aresamples. Neg, the lane of negative control; Pos, the lane of positive control of E. faecalis ATCC 29212 at the size of 137 bp
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 4 of 9

strength from all the tested sealers, and differed signifi-cantly from all other sealers groups (AH-ns vs. RS-nsp=0.001, Tukey’s pairwise comparisons), regardless ofthe smear layer removal (Table 3).
Relationship between shear bond strength and bacterialleakageThere was an obvious overall trend that higher bondstrength values resulted in less bacterial leakage (Fig. 3).In the apical third, the removal of the smear layer in-creased bond strength within all the materials tested, but
had a favourable effect on bacterial sealability with twomaterials only, AH and MTAF.
DiscussionThere are numerous of studies addressed to test the bondstrength separately from the coronal or apical bacterialleakage of the endodontic sealer cements. However, to ourknowledge there is no study that could assess the bondstrength of the sealer and its resistance to the microbialleakage. We tested four sealer cements that are commonlyused in the clinical practice. AH Plus is considered to beas the golden standard. It has very favorable physical prop-erties and it has been widely tested [17]. EndoRez featureslong resin tags into dentinal tubules that might be benefi-cial for the mechanical retention to the root canal dentin[18]. Several bacterial leakage studies reported conflictingfindings between AH Plus and EndoRez [19–23], thereforewe tested both materials as they are still commonly usedin clinical practice. Epiphany (RealSeal) and MTA FillApex are relatively new materials. Epiphany has beenclaimed to have an ability to bond to the dentin wall andthe core material and to form a gap-free solid monobloc,while MTA Flill Apex should exhibit MTA features. Twodifferent irrigation regimes were tested to explore a pos-sible influence of the smear layer to the adhesion as wellas the bacterial leakage and to assess those importantparameters.Dye and isotope penetration, glucose and fluid infiltra-
tion are suggested to assess the coronal leakage [24], butthe two-chamber bacterial method may best simulatethe clinical conditions [8, 14, 25], hence used in thisstudy. Rechenberg et al. [26] recently challenged the val-idity of the two-chamber model, as they found bacterial
Table 2 Proportion of leaked samples and the number ofdays the samples resisted the bacterial leakage, expressed asmean, range, and standard deviation (SD). Four group codes,see Table 1
Material/smear P Mean Range SD D
AH-s 15/15 29.4 23-35 1.0 b
AH-ns 15/15 36.8 30-41 1.1 a
ER-s 15/15 11.8 9-16 0.7 e
ER-ns 15/15 8.7 6-13 0.5 d
RS-s 15/15 24.7 20-37 1.1 b
RS-ns 15/15 15.1 11-20 0.8 c
MTAF-s 15/15 8.9 6-13 0.7 d
MTAF-ns 15/15 13.3 9-18 0.8 c
Positive control 5/5 2 2 0
Negative control 0/5 50 50 0
AH AHPlus, ER EndoRez, RS RealSeal/Resilon, MTAF MTA Fill Apex, s smear layerin situns smear layer removed with EDTA, P proportion of samples leaked, Meanmean time of leakage days, Range range of leakage days, SD Standarddeviation of the leakage days, D Log-rank test (P< 0.05): experimental groupswith different letter are significantly different from each other
Fig. 2 Kaplan Meier cumulative survival curves of samples expressed in number of incubation days resisting the bacterial leakage. Solid line,smear layer left in situ; dotted line, smear layer removed with EDTA. None of the negative control samples leaked in 50 days
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 5 of 9

penetration between sealing wax and the root interfacein both the experimental and control groups after 56days. In contrast, our study showed clear differences inthe experimental groups within 50 days, although theroot parts were similarly covered by wax in each group.They also pointed out improper sample preparation forthe control groups. In our study, we used meltedpre-autoclaved sticky wax to fix samples to upper cham-ber tubes first from the coronal aspect to assure closecontact to the root and the tube. As suggested byDe-Deus [27], we paid attention to a similar design ofthe groups by leaving the root apices uncovered for allthe groups, including the positive and negative controls.
To overcome possible variations in root canal anat-omy, we used upper incisors only. Moreover, theiranatomy was examined using radiographs in twoplanes to exclude those with severe root canal calcifi-cation or fracture lines, or any resorptive alteration ofthe canal lumen.E. faecalis was chosen as the test bacterium, because it
is frequently recovered in persistent periradicular lesions[3, 15, 28]. It shows an ability to penetrate dentin tu-bules, form biofilms on biotic/abiotic surfaces, endureprolonged nutritional deprivation, resist intracanal medi-cation and produce virulence factors that cause persist-ent infection and periradicular inflammation, such as
Table 3 Mean ± standard deviation (SD) of shear-bond strength values (MPa) of four endodontic sealer materials and a compositeresin filling material tested on four different dentin sites, the crown part of the tooth and apical, middle and cervical thirds of theroot canal wall, with and without removing the smear layer using EDTA
Material Apical Middle Cervical Crown P-value
Mean (SD) Mean (SD) Mean (SD) Mean (SD) (sites)
AH-s 1.4(0.4) N=8xa 2.0(0.8) N=10xa 3.5(0.7) N=10xb 3.4(0.4) N=3xb P<0.001
AH-ns 1.7(0.6) N=8xa 1.9(0.4) N=8xa 3.0(0.5) N=9xb 5.7(0.5) N=3xb P<0.001
ER-s 0.2(0.1) N=7ya 0.2(0.1) N=7ya 0.4(0.1) N=8yb 0.7(0.2) N=2yc P<0.001
ER-ns 0.4(0.1) N=7ya 0.5(0.4) N=8ya 0.1(0.4) N=8yb 0.9(0.1) N=3yb P=0.005
RS-s 0.5(0.1) N=9y 0.8(0.1) N=8x 1.0(0.6) N=9y 1.2(0.1) N=3y P=0.360
RS-ns 0.8(0.1) N=9ya 1.0(0.3) N=8xa 1.7(0.5) N=9yb 2.6(0.4) N=3yc P<0.001
MTAF-s 0.2(0.1) N=7ya 0.4(0.1) N=7ya 1.1(0.3) N=7yb 0.9(0.1) N=2yb P<0.001
MTAF-ns 0.3(0.1) N=8ya 0.5(0.1) N=9yb 1.0(0.3) N=8yc 1.1(0.2) N=3yc P<0.001
Comp-s 3.1(0.5) N=9za 4.8(1.3) N=9za 9.6(2.1) N=10zb 11.7(1.2) N=3zb P<0.001
Comp-ns 3.4(0.9) N=9za 5.5(0.8) N=9zb 10.8(1.9) N=10zc 0.7(1.5) N=3zd P<0.001
P-values (material groups) P<0.001 P<0.001 P<0.001
AH AHPlus, ER EndoRez, RS RealSeal/Resilon, MTAF MTA Fill Apex, Comp Composite, s smear layer in situ, ns smear layer removed with EDTA, N number of samplesa-d, pairwise comparison between the dentin sites, Tukey’s testx-z, pairwise comparisons between the material groups, Tukey’s test
Fig. 3 Survival of the bacterial challenge (mean number of days resisting the leakage) of E. faecalis strain in a two-chamber model in relation tothe mean of the shear bond strength (MPa) in the apical third of the root in the presence (red dots) and absence (blue dots) of the smear layer.Dotted line represents the trend. AH, AH Plus/gutta-percha; RS, RealSeal/Resilon; ER, EndoRez/gutta-percha; MTAF, MTA Fill Apex/gutta-percha
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 6 of 9
lytic enzymes, cytolysin, aggregation substance, phero-mones, and lipoteichoic acid [29, 30].None of the adhesion tests have been generally ac-
cepted as standard. Adhesion tests measure either tensilebond strength, where the bond is broken by a force per-pendicular to the interface between material and surface,or shear strength , where a force is parallel to the inter-face between material and surface. The shear test wasdeveloped to measure the bond of endodontic sealers toroot dentin and it proves to be effective and reprodu-cible [31]. The tensile bond strength test was used bySaleh et al. [7], to assess sealer materials. But we ratherwanted to use a modified bond test by Jessop [16], whereshear stress is predominant. The shear bond reflects aclinical scenario adequately because the forces simulateclosely the ones that may distort the obturation e.g. dur-ing the dowel space preparation [31].AH resisted the bacterial penetration the longest time,
regardless of the pre-treatment of the dentine with EDTA.This finding is in contrast to the results of Saleh et al [8],who found AH to leak more than RealSeal sealer/cones(later called RS/ Resilon), when EDTA was used to removethe smear layer. Both studies used the two-chamber testmodel modified from Torabinejad et al [14] and E. faecalisas the test bacterium, but different obturation techniques.Opening the dentinal tubules with EDTA may havefavoured more the lateral compaction used in our study,compared to the single cone technique used by Saleh et al.[8], although the relationship between sealing ability ofendodontic sealers and their penetration in dentinal tu-bules has not been confirmed [32]. When S. mutans wasused as the test bacterium, Shipper et al [25] found signifi-cantly less leakage with Resilon/Epiphany compared toGP/AHPlus, but no difference when Epiphany was usedwith GP. In our study, both MTAF and ER leaked consid-erably more than AH, irrespectively of the removal of thesmear layer. For ER, this was in contrast to the findings ofEldeniz & Ørstavik [6], who did not find any difference inleakage between AH and ER. This may be explained bythe different test microbes used, S. mutans vs. E. faecalis.In our study, the removal of the smear layer significantly
improved the resistance against bacterial leakage in theroots filled with GP/AH and GP/MTAF, but deterioratedthe seal for RS and ER. For AH, this contrasts with the pre-vious findings by Saleh et al. [8], but confirms their resultswith RS. Traditionally, smear layer is regarded to be re-moved, as it may be infected [33, 34] and may act as barrierto obstruct access of medicaments to the bacteria deeper inthe dentinal tubules [35, 36]. Although this view has beenchallenged [37], the removal of the smear layer is stillwidely advocated in textbooks [9]. The penetration of asealer into open dentinal tubules is suggested to improvethe sealing ability by mechanical interlocking [38]. Potentialantimicrobial activity of resin tags inside dentinal tubules
may also hamper the colonization of residual bacteria andreinfection of a root canal [39, 40] RS is shown to penetratedeeper into the dentinal tubules than AH, while ER showedthe lowest penetration ability [18, 41]. On the other hand,recent studies have found no statistical difference in tagpenetration between AH and MTAF [42, 43]. However, ourbond strength and microleakage results do not favour RS,despite of its ability to form the longest tags. Nevertheless,the smear layer removal improved AH bonding and sealingabilities, indicating that when AH is used as a sealer, EDTAcould also be used safely in vital cases and thus be part of aroutine in all endodontic obturations.In the present study, AH significantly reduced the en-
terococcal leakage in comparison with the other root canalsealers tested. This could be due to sealability of the ma-terial only, and/or due to its antimicrobial properties. Anumber of studies have demonstrated that AH has signifi-cant antimicrobial activity against E. faecalis and other or-ganisms in root canal. Saleh et al. [12] stated that AHkilled all bacteria in the dentine tubules within the zone of300 mm around root canal. Kayeoglu et al. [44] found thatan epoxy resin-based AH effectively reduced colony form-ing units of E. faecalis. Heyder et al. [45] revealed that AHhad an antibacterial effect on three species, E. faecalis, F.nucleatum and P. gingivalis, while ER and ProRoot MTAdisplayed no suppressive effect on E. faecalis. To the con-trary, Baer & Maki [46] failed to show the inhibition activ-ity on the growth of E. faecalis of AH and RS.Regarding sealability, our results are in line with those
by Baechtold et al. [47], who found AH to present highadhesion/bond strength to root canal wall and root fill-ing materials. Our result in the apical third are in linewith those of Eldeniz et al. [5], who found the removalof the smear layer to increase the bond of AH and RS,although the site of the root was not specified in theirstudy. In contrast, we found an opposite trend with AHin the middle and cervical thirds.We found higher bond strength values for RS, regard-
less of the smear removal, as compared with the resultsof Wachlarowicz et al. [48]. However, they used a differ-ent modification of the test model and did not specifywhether the bonding substrate was the root canal or theouter root dentin, which might influence the results. Incontrast to a recent study by Haragushiku et al. [49], allthe tested materials showed decreasing bond strengthfrom the cervical to apical region. But the finding is inline with the previous studies that showed differences inthe composition of dentin properties, partly due to thedistribution of dentinal tubules [50, 51].There was a clear trend that higher bond would also
indicate less leakage, although in that respect ER and RSacted differently when the effect of the smear removalwas concerned. The mechanism, behind better sealingcapacity of materials with better bonding properties to
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 7 of 9

dentine, relates to the capability of bonding interfaces toresist stress of the curing contraction of the sealer. Fromthe clinical point of view, our results will favour AH, asit would be desirable to select a sealer material thatapart from justified sealing ability, would also resist anydisturbing mechanical forces e.g. during the dowel spacepreparation.
ConclusionsAs a conclusion, the present study showed that among thefour resin-based sealers tested, the effect of the smearlayer removal on the sealability was material-dependent.AH showed the highest bond and lowest bacterial leakage.As the removal of the smear layer improved both thebond and the sealability for AH, the results suggest theclinical use of EDTA for root canal conditioning also invital cases, if AH is used.
Additional file
Additional file 1: Legislation. (DOCX 16 kb)
AbbreviationsAH: AHPlus; ER: EndoRez; GP: Gutta- percha; MTAF: MTA Fill Apex; n: Numberof specimens; ns: Smear layer removed; RS: Resilon; s: Smear layer left in situ;SD: Standard deviation; w/: with; w/o: without
AcknowledgementsOur thanks go to Hannu Vähänikkilä, PhD for the statistical analysis.
FundingNo funding was received.
Availability of data and materialsThe datasets used and/or analyzed during the current study are availablefrom the corresponding author on reasonable request.
Authors’ contributionsLA designed study, prepared samples and conducted all experiment, shealso wrote the manuscript. XS contributed in bacterial leakage part ofexperiment and participated in manuscript writing. N. Yong contributed inbacterial leakage part and completed PCR identification. LVJL was a leadingadvisor in bond strength experiment design and interpretation of the results,he contributed in manuscript writing. PKV contributed as an advisor inexperiment design and methodology, he also revised the manuscript. EK wasthe main advisor in experiment design and methodology, he contributed inanalyzing the experiment data and writing of the manuscript. All authorsread and approved the final manuscript.
Ethics approval and consent to participateWe declare that we have followed the ethical guidelines stated in thelegislation in Finland in the Act on the Medical Use of Human Organs,Tissues, and Cells, issued by the Ministry of Social Affairs and Health, Finland,in Helsinki on 2nd February 2001, see section 20 amended 30.11.2012 (689/2012) attached and highlighted in yellow. As the teeth were previouslyextracted for therapeutic purposes (treatment not related to this study) andno personal data were used, the permission by the Institute of Dentistry,University of Turku, was found adequate. The document is attached as aseparate file under the title- "Legislation". 3 (Additional file 1). All teeth wereextracted due to therapeutical reason not related with the study at the Instituteof Dentistry, University of Turku. Such teeth are collected, stored under thespecial conditions and used for the further research studies with the Institute"
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Department of Clinical Dentistry, Faculty of Health Sciences, UiT The ArcticUniversity of Norway, N-9037 Tromso, Norway. 2Department of MedicalBiology, Faculty of Health Sciences, UiT The Arctic University of Norway,Tromso, Norway. 3Department of Community Medicine, Faculty of HealthSciences, UiT The Arctic University of Norway, Tromso, Norway. 4Departmentof Biomaterials Science, Institute of Dentistry, University of Turku, Turku,Finland. 5Welfare Division, Turku, Finland. 6Present address: Vilnius, Vilnius,Lithuania.
Received: 4 December 2017 Accepted: 7 November 2018
References1. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of
dental pulps in germ- free and conventional laboratory rats. Oral Surg OralMed Oral Pathol Oral Radiol Endod. 1965;20:340–9.
2. Ørstavik D, Kerekes K, Molven O. Effects of extensive apical reaming andcalcium hydroxide dressing on bacterial infection during treatment of apicalperiodontitis: a pilot study. Int Endod J. 1991;24:1–7.
3. Sundquist G, Figdor D. Endodontic treatment of apical periodontitis. In:Ørstavik D, Pitt Ford TR, editors. Essential Endodontology, 1st edn. Oxford,1998. UK: Blackwell Science Ltd. p. 253.
4. Ørstavik D, Eriksen HM, Beyer-Olsen EM. Adhesive properties and leakage ofroot-canal sealers in vitro. Int Endod J. 1983;16:59–63.
5. Eldeniz AU, Erdemir A, Belli S. Shear bond strength of three resin basedsealers to dentin wall with and without smear layer. J Endod. 2005;31(4):293–6.
6. Eldeniz AU, Ørstavik D. A laboratory assessment of coronal bacterial leakagein root canals filled with new and conventional sealers. Int Endod J. 2009;42:303–12.
7. Saleh IM, Ruyter IE, Haapasalo M, Ørstavik D. The effect of dentinepretreatment on the adhesion of root canal sealers. Int Endod J. 2002;35:859–66.
8. Saleh IM, Ruyter IE, Haapasalo M, Ørstavik D. Bacterial penetration alongdifferent root canal filling materials in the presence or absence of smearlayer. Int Endod J. 2008;41:32–40.
9. Johnson WT, Noblett WC. Cleaning and Shaping, Endodontics: Principlesand Practice. In: Torabinejad M, Walton RE, editors. , vol. 2009. St. Louis:Sounders Elsevier. p. 264–5.
10. Goldman M, Goldman LB, Cavaleri R, Bogis J, Lin PS. The efficacy of severalendodontic irrigating solutions: a scanning electron microscopic study: part2. J Endod. 1982;8:487–92.
11. Zmener O, Banegas G, Pameijer CH. Bone tissue response to amethacrylate-based endodontic sealer: a histological and histometric study.J Endod. 2005;31:457–9.
12. Saleh IM, Ruyter IE, Haapasalo M, Ørstavik D. Survival of Enterococus faecalisin infected dentinal tubules after root canal filling with different root canalsealers in vitro. Int Endod J. 2004;37:193–8.
13. Qian W, Shen Y, Haapasalo M. Quantitative analysis of the effect of irrigantsolution sequences on dentin erosion. J Endod. 2011;37(10):1437–41.
14. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration ofcoronally unsealed endodontically treated teeth. J Endod. 1990;16:566–9.
15. Sun J, Song X, Kristiansen BE, Kjaereng A, Willems RJ, Eriksen HM, SundsfjordA, Sollid JE. Occurrence, population structure, and antimicrobial resistanceof enterococci in marginal and apical periodontitis. J Clin Microbiol. 2009;47(7):2218–25.
16. Jessop NT. "Testing shear bond strength." U.S. Patent No. 6. 2001;916(4):324.17. Schafer E, Bering N, Burklein S. Selected physicochemical properties of AH
Plus, EndoRez and RealSeal SE root canal sealers. Odontology. 2015 Jan;103(1):61–5.
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 8 of 9

18. Chandra SS, Shankar P, Indira R. Depth of penetration of four resin sealersinto radicular dentin tubules : a confocal microscopic study. J Endod. 2012;38(10):1412–6.
19. Drukteinis S, Peciuliene V, Maneliene R, Bendinskaite R. In vitro study ofmicrobial leakage in roots filled with Endo REZ sealer/Endo REZ points and AHPlus sealer/conventional gutta-percha points. Stomatologija. 2009;11(1):21–5.
20. Sevimay S, Kalayci A. Evaluation of apical sealing ability and adaptation todentine of two resin-based sealers. J Oral Rehabil. 2005;32(2):105–10.
21. Dultra F, Barroso JM, Carrasco LD, Capelli A, Guerisoli DM, Pécora JD.Evaluation of apical microleakage of teeth sealed with four different rootcanal sealers. J Appl Oral Sci. 2006;14(5):341–5.
22. Gernhardt CR, Kruger T, Bekes K, Schaller HG. Apical sealing ability of 2epoxy resin-based sealers used with root canal obturation techniques basedon warm gutta-percha compared to cold lateral condensation.Quintessence Int. 2007;38(3):229–34.
23. da Silva Neto UX, de Moraes IG, Westphalen VP, Menezes R, Carneiro E,Fariniuk LF. Leakage of 4 resin-based root-canal sealers used with a single-cone technique. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(2):e53–7.
24. Wu MK, Wesselink PR. Endodontic leakage studies reconsidered. Part I.Methodology, application and relevance. J Endod. 1993;26(1):37–43.
25. Shipper G, Ørstavik D, Teixeira FB, Trope M. An evaluation of microbialleakage in roots filled with a thermoplastic synthetic polymer-based rootcanal filling material (Resilon). J Endod. 2004 May;30(5):342–7.
26. Rechenberg DK, Thurnheer T, Zehnder M. Potential systematic error inlaboratory experiments on microbial leakage through filled root canals: anexperimental study. Int Endod J. 2011;44:827–35.
27. Editorial D-DG. Int. J Endod. 2012;45:1063–4.28. Sedgley CM, Lennan SL, Clewell DB. Prevalence, phenotype and genotype
of oral enterococci. Oral Microb Immunol. 2004;19:95–101.29. Sun J, Sundsfjord A, Song X. Enterococcus faecalis from patients with
chronic periodontitis: virulence and antimicrobial resistance traits anddeterminants. Eur J Clin Microbiol Infect Dis. 2012;31:267–72.
30. Stuart CH, Schwartz SA, Beeson TJ, Owatz CB. Enterococcus faecalis: Its Rolein Root Canal Treatment Failure and Current Concepts in Retreatment. JEndod. 2006;32(2):93–8.
31. Tagger M, Tagger E, Tjan AHL, Bakland LK. Measurements of adhesion ofendodontic sealers to dentin. J Endod. 2002a;28:351–4.
32. Jardine AP, Rosa RA, Santini MF, Wagner M, So MV, Kuga MC, Pereira JR,Kooper PM. The effect of final irrigation on the penetrability of an epoxyresin-based sealer into dentinal tubules: confocal microscope study. ClinOral Investig. 2016;20(1):117–23.
33. McComb D, Smith DC. A preliminary scanning electron microscopic studyof root canals after endodontic procedures. J Endod. 1975;1:238–42.
34. Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopicinvestigation of the smeared layer on root canal walls. J Endod. 1984;10:477–83.
35. Brannstrom M, Johnson G. Effects of various conditioners and cleaningagents on prepared dentin surfaces: a scanning electron microscopicinvestigation. J Prosthet Dent. 1974;31:422–30.
36. Haapasalo M, Ørstavik D. In vitro infection and disinfection of dentinaltubules. J Dent Res. 1987;66:1375–9.
37. Paqué F, Luder HU, Sener B, Zehnder M. Tubular sclerosis rather than thesmear layer impedes dye penetration into the dentine of endodonticallyinstrumented root canals. Int Endod J. 2006;39(1):18–25.
38. Kokkas AB, Boutsioukis AC, Vassiliadis LP, Stavrianos CK. The influence of thesmear layer on dentinal tubule penetration depth by three different rootcanal sealers: An in vitro study. J Endod. 2004;30:100–2.
39. Heling I, Chandler NP. The antimicrobial effect within dentinal tubules offour root canal sealers. J Endod. 1996;22(5):257–9.
40. Bouillaget S, Shaw L, Barthelemy J, Krejci I, Wataha JC. Long-term sealingability of pulp canal sealers, AH-Plus, GuttaFlow and Epiphany. Int Endod J.2008; 41(3):219-226. 34.
41. Mamoofil K, Messer HH. Penetration of dentinal tubules by endodontic sealercements in extracted teeth and in vivo. Int Endod J. 2007;40(11):873–81.
42. Akcai M, Arslan H, Durmus N, Mese M, Capar ID. Dentinal tubule penetrationof AH Plus, iRoot SP, MTA Fillapex, and GuttaFlow Bioseal root canal sealersafter different final irrigation procedures: a confocal microscopy study.Lasers Surg Med. 2016;48:70–6.
43. Kok D, Rosa RA, Barreto MS, Busanello FH, Santini MF, Prereira JR, So MV.Penetrability of AH Plus and MTA Fillapex after endodontic treatment and
retreatment: a confocal laser scanning microscopy study. Microsc Res Tech.2014;77(6):467–71.
44. Kayaoglu G, Erten H. Alac T¸ Ørstavik D. Short-term antibacterial activity ofroot canal sealers towards Enterococcus faecalis. Int Endod J. 2005;38:483–8.
45. Heyder M, Kranz S, Völpel A, Pfister W, Watts DC, Jandt KD, Sigusch BW.Antibacterial effect of different root canal sealers on three bacterial species.Dent Mater. 2013;29:542–9.
46. Baer J, Maki JS. In vitro evaluation of the antimicrobial effect of threeendodontic sealers mixed with amoxicillin. J Endod. 2010;36(7):1170–3.
47. Baechtold MS, Mazaro AF, Crozeta BM, Leonardi DP, Tomazinho FSF,Baratto-Filho F, Haragushiku GA. Adhesion and formation of tags from MTAFillapex compared with AH Plus cement. RSBO. 2014;11(1):71–6.
48. Wachlarowicz A, Joyce AP, Roberts S, Pashley DH. Effect of endodonticirrigants on the shear bond strength of Epiphany sealer to dentin. J Endod.2007;33(2):152–5.
49. Haragushiku GA, Teixeira CS, Furuse AY, Silva Sousa YT, Sousa Neto MD,Silva RG. Analysis of interface and bond strength of resin-based endodonticcements to root dentin. Microscop Res Tech. 2012;75(5):655–61.
50. Watanabe LG, Marshall GW Jr, Marshall SJ. Dentin shear strength: effects oftubule orientation and intratooth location. Dent Mater. 1996;12:109–15.
51. Marshall GW Jr, Marshall SJ, Kinney JH, Balooch M. The dentine substrate:structure and properties related to bonding. J. Dent. 1997;25:441–58.
Andriukaitiene et al. BMC Oral Health (2018) 18:213 Page 9 of 9