the effects of a controlled family navigator nurse …effects+of+a...the effects of a controlled...
TRANSCRIPT

The Effects of a Controlled Family Navigator Nurse Directed Intervention Program for Parents Hospitalized with Children Undergoing Allogeneic Haematopoietic Stem Cell Transplantation (HSCT)
Submitted: 31 July 2011
Department of Pediatrics, The Juliane Marie Centre & Department of Hematology, The Finsen Centre The University Hospitals Center for Nursing and Care Research Copenhagen University Hospital, Rigshospitalet
Ph.D. Dissertation Hanne Bækgaard Larsen
F A C U L T Y O F H E A L T H S C I E N C E S U N I V E R S I T Y O F C O P E N H A G E N
Faculty of Health Sciences University of Copenhagen
Academic advisor: Professor, ph.d. Lis Adamsen

PhD Dissertation:
The Effects of a Controlled Family Navigator Nurse Directed Intervention Program for Parents Hospitalized with Children Undergoing Allogeneic Haematopoietic Stem Cell Transplantation (HSCT)
Hanne Bækgaard Larsen
The dissertation will be defended on
Official opponents
• Associate Professor Ole Weis Bjerrum, MD, DMSc Department of Surgery and Internal Medicine, University of Copenhagen Copenhagen, Denmark
• Professor Henrik Hasle, MD, DMSc Department of Pediactrics, Aarhus University Hospital, Skejby Aarhus Denmark
• Professor Kristian Larsen,RN, MSc, Ed.st., Ph.D.
Oslo University College, Faculty of Nursing Oslo, Norway
Scientific Advisors
• Professor Lis Adamsen, RN, MSc. Soc., Ph.D. The University Hospitals Center for Nursing and Care Research Institute of Public Health, Faculty of Health Sciences Copenhagen University, Copenhagen Denmark
• Professor Carsten Heilmann, MD, DMSc Department of Pediatrics, Copenhagen University Hospital, Rigshospitalet Copenhagen, Denmark
• Professor Christoffer Johansen, MD, DMSc, Ph.D. Department of Psychosocial Cancer Research, Danish Cancer Society Copenhagen, Denmark
The University Hospitals Center for Nursing and Care Research (UCSF), Copenhagen University Hospital, Department 7001, Blegdamsvej 9, DK-2100 Copenhagen, Denmark
Tak Undersøgelserne i denne afhandling er gennemført med finansiel støtte fra Børnecancerfonden, Helsefonden, Lundbeckfonden, Gangstedfonden samt Rigshospitalets 2½-årige forskerdelestilling. Tusind tak for jeres støtte og medindlevelse i projektet undervejs. Jeg vil også rette en stor tak til jer forældre og børn, der i forbindelse med jeres behandling med allogen knoglemarvstransplantation har sagt Ja til at dele denne, for jer, svære tid med mig. I har åbnet ikke kun jeres isolationsstue på Rigshospitalet for mig, men også jeres familier. I har haft overskud til at dele jeres bekymringer, følelser, tanker og meninger med mig, svare på spørgsmål og udfylde talrige spørgeskemaer. Hvis I ikke havde udvist det storsind i en svær tid, kunne dette projekt ikke være lykkedes. Jeg ønsker jeg alle det bedste for fremtiden. Jeg er ligeledes dybt taknemmelig og fuld af beundring for den støtte, vejledning og læring jeg har fået gennem min hovedvejleder i ph.d. forløbet Professor Lis Adamsen fra Universitetshospitalernes center for Sygepleje- og Omsorgsforskning (UCSF). Lis, du har en beundringsværdig, utrættelig energi, som du investerer i forskning for derved at medvirke til at ændre verden til det bedre. Dette gør du enten direkte gennem din egen forskning eller ved at investere din tid og kræfter i andres projekter, hvilket i særdeleshed er kommet mig til gode i dette forløb. Lis, det er sjældent at møde mennesker der, i samme grad som dig, er i stand til at holde fanen højt, stille skarpt på de forskningsmæssige problemer, gennemskue svagheder, inspirere, nytænke og vedvarende holde fast i den røde tråd. Disse evner har jeg nydt godt af i dette projekt og det er jeg dig taknemmelig for. Jeg vil ligeledes sige mange tusinde tak til min projektvejleder Professor Carsten Heilmann, Rigshospitalets Juliane Marie Center. Carsten, jeg er dybt taknemmelig for din tro og støtte til mig gennem alle årene, således at jeg har kunnet udvikle mig både i forskerrollen men også som menneske. Du har en særlig evne til at stille skarpt på problemstillingerne, både i forskningen og i sproget. Du er ekspert i at opretholde enkelthed, overskuelighed og stringens i forskningen. Ligeledes går du hverken af banen for en golfbold eller Max Weber, hvilket er et udtryk for din alsidige styrke. Også mange tusinde tak til min bi-vejleder Professor Christoffer Johansen fra Kræftens Bekæmpelse. Christoffer, jeg er meget taknemmelig for den tid og energi du har brugt på mig i forbindelse med dette projekt. Du har en herlig evne til at tænke store tanker i forskningen, det er dejligt befriende. Tak for det. I skal alle have tak for jeres energi, store hjælpsomhed og ikke mindst tid, i forbindelse med dette projekt. Tak til de undervisere som har varetaget undervisningen til forældrene i forbindelse med projektet. I har været utrolig fleksible og har tilpasset tidspunkterne efter forældrenes behov. Først og fremmest vil jeg sige tak til pædagog Lise Auscher, for alt hvad du har lært mig om børn og forældre, og ikke mindst for at du har haft overskud til at formidle denne viden til forældrene i forbindelse med dette projekt. Dernæst vil jeg sige tak til de øvrige undervisere; sygeplejerske Helen Munk for utroligt mange gode tips og ideer til forældrene, psykolog Bo Snedker Boman for at introducere forældrene til kognitiv terapi på en anvendelig måde, og Tine Banke Høgsberg for at dele sin viden og tanker om, hvordan det er at være mor gennem et langt transplantationsforløb. I denne forbindelse vil jeg også sige en stor tak til Ronand McDonald huset på Rigshospitalet, og ikke mindst Karen Bjørløw Jacobsen, for at lægge lokaler til forældreundervisningen. Også Tak til sygeplejerskerne Anne Shaffer Lassen og Camilla Roepstorff, der har været ”stand ins” for mig i forbindelse med varetagelse af den daglige intervention.

Projektet er udført både i Juliane Marie Centret og Finsencentret, hvorfor min tak også går til centerledelsen i Juliane Marie Centeret, centerdirektør Bent Ottesen og centerchefsygeplejerske Sanne Wilsdahl samt centerledelsen i Finsencentret, Centerdirektør Kurt Stig Jensen og centerchefsygeplejerske Jeanette Bech. Tak for jeres støtte til at skabe rammerne for projektudførelsen. Tak til Professor Kjeld Schmiegelow for husly. Desuden tak til sygeplejerskerne og lægerne i afdeling 5061, 4043 og 5002 for at tage godt i mod mig i forbindelse med udførelsen af projektet, for jeres støtte undervejs, og for det store engagement I har i det daglige arbejde med børn og forældre. Sheila Schmidt skylder jeg stor tak for hendes kommentarer og ikke mindst skarpe pen når det gælder det engelske sprog, og ass. Professor Anders Tolver, Institut for grundvidenskab og miljø, LIFE instituttet, for statistiske beregninger, tålmodighed, pædagogisk vejledning og ikke mindst hurtige analyser. Jeg vil også sige en kæmpe stor tak til mine kolleger på Rigshospitalet, sygeplejerskerne Sine Rasmussen, Jeanette Holder, Ann-Mari Bertelsen, Line Pedersen og Heidi Petersen, og sekretær Vivi Ljungberg for at have huset mig på Rigshospitalet i dagligdagen og ikke mindst for jeres engagement i projektet. I har lyttet tålmodigt på dagliglivets små finurligheder og samtidig haft en utrolig indsigt i hvordan problemer kan løses, hvilket jeg har draget stor nytte af. I er nogle uvurderlige ildsjæle. Tak! til alle mine kolleger på UCSF. Til forsker Mary Jarden, Tom Møller, Betina Lund Nielsen og Christina Andersen for at dele denne ph.d. proces med mig, al jeres hjælp, støtte og engagement undervejs og ikke mindst jeres glade grin og gode humør – I er guld værd! Speciel tak til forsker Mary Jarden og forskningsfysioterapeut Kira Bloomquist for oversættelse af spørgeskemaer til projektet. Tak til seniorforsker Julie Midtgård for hjælp til projektbeskrivelsen, til Ingrid Egerod for et evigt godt humør og faglig indsigt og til forsker Dorte Overgaard for faglig gejst og gode snakke. I har alle bidraget med spændende perspektiver. Til alle øvrige medarbejdere i UCSF vil jeg sige tusind tak for mange hyggelige stunder: forskningsfysioterapeuterne Morten Quist, Jacob Uth og Christian Lillelund; ph.d. studerende Jesper Frank Christensen; forskningsassistenterne Pernille Cromhout, Maria Stage og Signe Risom; sygeplejerskerne Mette Leinø, Birgit Nielsen, Birgitte Rasmussen, Jørgen H. Laursen og servicemedarbejder Kjeld Jensen. En helt særlig tak vil jeg give til sekretær Ida Raun-Petersen. Ida du har været en stor del af dette projekt i alle dets faser, du har skrevet interviews ud, åbnet kuverter, sendt artikler, læst korrektur, sat dokumenter op, osv. Du har været en helt uvurderlig støtte, mange tak for dette og dit altid gode humør. Også en stor tak til sekretær Bente Kronborg for at du altid kan finde et par ord for meget, når det nu er det der skal til. Ligeledes tak til bibliotekar Anders Larsen, for assistance til litteratursøgning, referenceopsætning og redigering. Til sidst vil jeg sige mange tusinde tak til min mand Flemming for din tålmodighed, engagement, forståelse og kærlige opbakning gennem hele dette projekt forløb. Uden din hjælp var dette ikke lykkedes. Jeg vil også sige en stor tak til mine forældre Henning og Tove samt til min bror Jesper, min svigerinde Camilla og pigerne, Maja og Lea for jeres opbakning til mig undervejs. Hanne Bækgaard Larsen København, 27. juli 2011
ORIGINAL PAPERS This dissertation is based on the following papers:
I. Larsen HB, Heilmann C, Johansen C, Adamsen L. (2011) An analysis of parental roles during haematopoietic stem cell transplantation of their offspring: a qualitative and participant observational study. Journal of Advanced Nursing. doi: 10.1111/j.1365-2648.2010.05587.x
II. Larsen HB, Heilmann C, Johansen C, Adamsen L. Socially disadvantaged parents of
children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study. Submitted.
III. Larsen HB, Adamsen L, Tolver A, Johansen C, Heilmann C. Supportive Intervention
Program Targeting Parents to Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation (HSCT): a Controlled Study. Manuscript.
The papers are referred to in the text by their Roman numerals.

DANSK RESUMÉ Et kontrolleret family navigator nurse ledet interventionsstudie hos medindlagte forældre til Allogen hæmatopoietisk stamcelletransplanterede (HSCT) børn. Baggrund Medindlagte forældrene er de primære omsorgsgivere hos børn med livstruende sygdomme under behandlingen med allogen hæmatopoietisk stamcelletransplantation (HSCT). Barnets HSCT behandling medfører omfattende fysiske og psykiske bivirkninger, risiko for komplikationer, samt en mortalitet på 22-50%. Litteraturen, egen pilotundersøgelse og kliniske erfaringer viste at forældrene er emotionelt og socialt svært belastede under barnets 4-6 ugers lange indlæggelse i isolation under transplantationsforløb. Der er udført få, ikke konklusive interventionsundersøgelser hvori et mindre antal deltagere (børn/forældre) er inkluderet. Formål, design og intervention Formålet var at undersøge effekten af et multifacetteret understøttende interventions program rettet mod omsorgskapacitet hos medindlagte forældres til børn behandlet med HSCT. Interventionsprogrammet indeholdt ni timers intervention/uge: a) daglig medicinsk information samt emotionelt og social understøttende intervention ved en Family Navigator Nurse (FNN); b) fem timers forældreudvisningsprogram; samt c) fysisk aktivitet for forældre. Teoretisk er undersøgelsen inspireret af et interaktionistisk perspektiv, Hochschild’s teori om familie- og følelsernes sociologi samt kognitiv adfærdsterapi. Metoder og population Udbyttet af interventionsstudiet blev belyst i to kvalitative analyser: 1) ved convenient sampling blev 16 semistrukturerede interviews og otte deltagerobservationsstudier blandt medindlagte forældre inkluderet i en analyse af disses omsorgsroller, og 2) ved quota-sampling blev 21 semistrukturerede interviews og 25 deltagerobservationsstudier hos forældre i interventionsgruppen inkluderet i en analyse af forældrenes væsentligste problemstillinger under medindlæggelsen. Effekten af interventionen blev undersøgt med velvaliderede kvantitative spørgeskemaer (HADS, POMS, CHIP, BASES) ved at sammenligne en forældre interventionsgruppe (N=25) med: 1) en prospektiv forældrekontrolgruppe (N=8) der modtog afdelingens standardpleje, 2) en retrospektiv forældrekontrolgruppe (N=46) til børn behandlet i de foregående 3.5 år, der havde modtaget afdelingens standardpleje. De medindlagte forældre er 56 mødre (71%) og 23 fædre (29%) til 79 børn ( 46% piger og 54% drenge) i alderen 0-20 år ( median 8 år). Der udarbejdet 3 artikler baseret på resultaterne fra interventionsstudiet. Resultater Artikel 1: belyser, vha. kvalitative metoder, tre idealtyper for forælde og omsorg hhv. 1. ekspertise orienterede-, 2. dialog orienterede- og 3. socialt udfordrede forældre. De tre omsorgstyper afspejler forældrenes tilgang til barnets pleje og behandling samt influerer på samarbejdet og kommunikationen mellem barn, forældre og personale. Konflikter opstår når omgivelserne ikke agerer i overensstemmelse med forældrenes omsorgsrationalitet. For at kunne varetage omsorgsudøvelse udfører forældrene samtidig en følelsesmæssig bearbejdning af sig selv, hvilket socialt udfordrede forældre har vanskeligt ved. Artikel 2: viser, de tre problemområder som forældrene angiver som væsentligste at skulle forholde sig til under medindlæggelsen: 1. Den emotionelle belastning forbundet med barnets HSCT 2.

Reorganiseringen af familielivet for at kunne være medindlagt med barnet, og 3. Den økonomiske belastning forbundet med at skulle manøvrerer i det danske socialsystem. Det at have fire eller flere af følgende risikofaktorer: 1) enlig forældre, 2) lav indkomst, 3) lav uddannelsesniveau, 4) begrænset netværk, 5) arbejdsløs, 6) fysisk/psykisk sygdom, og 7) at være at ”nydansker”, medførte, at forældrene befandt sig i en kompleks social, økonomisk og følelsesmæssig belastet situation, hvilket influerede på deres omsorgsevne og krævede omfattende og vedvarende FNN intervention. Artikel 3: afdækker, ved hjælp af spørgeskema HADS effekt af interventionen og udviklingen af forældrenes niveau for angst- og depressivsymptomer i forhold til barnets indlæggelsesforløb. Der fandtes ingen statistisk signifikans i forældrenes angst og depressionsniveau imellem grupperne.. Ved indlæggelsen havde 24% af forældrene en HADS score på over 10, hvilket indikerede et moderat til højt depressions symptomniveau og 39% have et moderat til højt angstsymptom niveau. Blandt forældre i interventionsgruppen blev angstniveauet signifikant reduceret ved følgende dage 0, +14, +21 og +100 fra baseline (dag –7). En tilsvarende reduktion i angstscore under indlæggelse kunne ikke påvises for kontrolgruppen, men på dag 100. Konklusion Allogen HSCT til børn er en kompleks invasiv behandling, som gennemgribende påvirker forældrenes emotionelle og sociale funktion samt forældreomsorgsevne. Dette er det første interventionsstudie rettet mod at understøtte medindlagte forældres omsorgskapacitet under barnets HSCT behandling. FNN interventionen understøttede forældrenes transition mellem hjem og hospitalsindlæggelse, og familiernes vej gennem det komplicerede behandlingsforløb. De tre identificerede idealtyper giver indsigt i forældrenes omsorgsrationalitet for barnet samt nye perspektiver på den komplekse interaktion mellem forældre, barn og sundhedsprofessionelle under HSCT behandlingen. Denne viden kan hjælpe personalet med at identificere gruppen af socialt udfordrede forældre, som har mest udtalt behov for støtte til at håndtere omsorgen for barnet. Samtidig har interventionsstudiet medvirket til at identificere nogle af de samfundsmæssig barrierer der negative påvirker forældrenes omsorgskapacitet.

ENGLISH ABSTRACT The Effects of a Controlled Family Navigator Nurse Directed Intervention Program for Parents Hospitalized with Children Undergoing Allogeneic Haematopoietic Stem Cell Transplantation (HSCT). Background Parents are the primary caregivers of children with a life-threatening disease and who undergo allogeneic haematopoietic stem cell transplantation (HSCT). A child’s HSCT carries the risk of severe physical and emotional complications and a mortality risk of 22-50%. The literature, own pilot study and clinical experience describe these parents as being heavily emotional and socially burdened during the 4-6 weeks of the transplantation process in isolation. Very few inconclusive intervention studies with a small sample size (children/parents) have been carried out in this field. Aim, design and intervention The aim was to investigate the effect of a multifaceted intervention program targeting the care capacity of resident parents for children undergoing HSCT. The intervention program comprised nine hours/week: (a) daily medical information relay, emotional and social support with a Family Navigator Nurse (FNN), b) a five hour education program for parents, and c) physical activity for parents. Theoretically, the study was inspired by an interactive perspective, Hochschold´s theory of family and emotional sociology and cognitive behavioral therapy. Methods and sample The benefits of the intervention study were explored in two qualitative analyses: 1) by convenient sampling; 16 semi-structured interviews and eight participant observation studies among the resident parents were included in an analysis of their caregiving roles, 2) by quota-sampling; 21 semi-structured interviews and 25 participant observation studies among parents in the intervention group were included in an analysis of the parents’ major problems during hospitalization. The effect of the intervention was examined by validated quantitative questionnaires (HADS, POMS, CHIP, BASES) by comparing the parental intervention group (N=25) to: 1) a prospective parental control group (N=8) receiving standard care, and 2) a retrospective parental control group (N=46) to children treated over the past 3.5 years and who received standard care. The residential parents were 56 mothers (72%) and 23 fathers (29%) to 79 children (46% girls and 54% boys) aged 0-20 years (median 8 years) Three papers were developed from the intervention study results. Results Paper 1: highlights, using qualitative methods, three types of parent care, i.e. 1) expertise minded; 2) dialogue minded, and 3) socially challenged parents. The three care types reflect the parents’ approach to their child’s care and treatment as well as the influence of each approach on collaboration and communication between the child, the parents and the staff. Conflicts emerged when actions did not comply with the parents’ rationale for care. In order for the parents to provide childcare, they had to engage in emotional work which was difficult for the socially challenged parents. Paper 2: shows, on the backcloth of qualitative interviews, three major problem areas that the parents faced during hospitalization with their child: 1. the emotional burden associated with the child’s HSCT; 2. the necessary reorganization of family life to accommodate hospitalization with the child; and 3. the economic burden associated with maneuvering within the Danish social welfare

system. Having four or more of the following risk factors: 1) being a single parent; 2) having a low income; 3) having a low education level; 4) having a limited social network; 5) being unemployed; 6) having a physical/psychological illness; and 7) being a new Danish citizen, all led to the parents feeling trapped in a complex socially, economically and emotionally burdensome situation that impacted their ability to care and they demanded continuous and comprehensive FNN intervention. Paper 3: uncovers, by means of the HADS questionnaire, the effect of the intervention process and the development in the parents’ levels of anxiety and depression in relation to the child’s hospitalization process. There was no statistically significant difference between the prospective parental control group and the parental intervention group. At admission, 24% of the parents had HADS scores over 10, which indicates a moderate to severe level of depression and 39% of the parents had a moderate to severe level of anxiety. The anxiety level in the intervention group was reduced significantly on day: 0, +14, +21 and +100 following admission. A similar reduction in anxiety scores during hospitalization could not be seen in the control group, however, a significant reduction was observed on day 100. Conclusion Allogeneic HSCT for children is a complex invasive treatment that deeply affects their parents’ physical, emotional and social functions as well as their care abilities. This is the first intervention study targeting the resident parents’ caring abilities during the child’s HSCT treatment. The FNN intervention supported the parents’ transition between home and hospital and supported the parents during the complex HSCT inpatient treatment course. The three identified ideal types provide an insight into the parents’ care rationale for the child and provide new perspectives on the complex interaction between parents, the child and the caregivers during HSCT treatment. This knowledge may assist staff to identify socially challenged parents who are in most need of assistance in caring for their child. In addition, the intervention study identified barriers within society that negatively affect the parents’ caregiving abilities.

ABBREVIATIONS ANC - Absolute Neutrophil Count
BASES - Behavioural, Affective and Somatic Experience Scale
CHIP - Coping Health Index for Parents
CM - Case manager
EORTC - European Organization for Research and Treatment of Cancer
GvHD - Graft versus Host Disease
FNN - Family Navigator nurse
HADS - Hospital Anxiety and Depression Scale
HLA-typing - Human Leukocyt Antigen - typing
HSCT - Allogeneic Haematopoietic Stem Cell Transplantation
I.V. fluid - Intravenous fluid
LAF - Laminar Air Flow
MD – Medical Doctor
PIG - Parental Intervention Group
PN - Patient navigator
POMS - Profile of Mood States-B
PPCG - Prospective Parental Control Group
RCT - Randomised control trials
RN – Registered Nurse
RPCG - Retrospective Parental Control Group
SEM - Standard Error of Means
SD - Standard Deviation
TBI - Total Body Irradiation
UID – Unique Identification Number
1
TABLE OF CONTENTS 1. INTRODUCTION .................................................................................................................. 1 2. HYPOTHESES AND AIMS ................................................................................................. 1 3. BACKGROUND AND THEORETICAL INSPIRATION ................................................. 2
3.1 Allogeneic Hematopeietic Stem Cell Transplantation 3.2 The pre-HSCT period 3.3 The HSCT inpatient course 3.4 The HSCT inpatient-setting and the parents’ care related tasks 3.5 Emotional distress during the isolation treatment 3.6 Clinical intervention studies of HSCT children 3.7 Clinical intervention studies among parents to HSCT children 3.8 Intervention studies aimed to reduce distress in parents to children with recent cancer
diagnoses 3.9 Pilot study of Danish children previously treated with HSCT and their parents 3.10 Nurses performing the Case Manager/ Patient Navigator function
4. THEORETICAL FRAMEWORK ........................................................................................ 6 4.1 A sociological approach to the family 4.2 Balancing work and home 4.3 Emotional management 4.4 Behavioural and cognitive behavioural therapy inspiration 4.5 Summary
5. MATERIALS AND METHODS ........................................................................................... 8 5.1 Design 5.2 Sample
5.2.1 Excluded parents in the study 5.3 Baseline medical and socio-demographic characteristics of the children and parents 5.4 The supportive intervention 5.4.1 The author’s background and function in the intervention program 5.5 Intervention program 5.6 Principles for the intervention
5.6.1 The daily FNN intervention schedule 5.6.2 The FNN intervention focused on three parent-targeted components 5.6.3 The daily rounds 5.6.4 The supervised, structured group-based education program 5.6.5 Physical activity
5.7 Standard care received by the control groups 5.8 Data collection
5.8.1 Qualitative data collection 5.8.1.1 Participant observation study 5.8.1.2 Semi-structured interviews
5.8.2 Quantitative data collection 5.8.2.1 Data collection schedule and procedures 5.8.2.2 Assessment instruments and questionnaires

2
6. DATA ANALYSES AND INTERPRETATION .................................................................. 18 6.1 Qualitative data analysis 6.2 Quantitative data analysis
7. ETHICAL CONSIDERATIONS .......................................................................................... 19 8. RESULTS ................................................................................................................................ 20
8.1 Paper I 8.2 Paper II 8.3 Paper III
9. DISCUSSION .......................................................................................................................... 23 9.1 Parental roles 9.2 The parental problem areas and risk factors 9.3 The parents’ level of anxiety and depression in relation to the intervention program 9.4 FNN role and dilemmas 9.5 Qualitative methodological considerations and limitations
9.5.1 Sampling in the participant observation study and qualitative interviews 9.5.2 Validation of the participant observational study and semi-structured interviews 9.5.3 Theoretical foundation of the qualitative findings 9.5.4 The researchers role in qualitative research 9.5.5 Transferability
9.6 Quantitative methods advantages and limitations 9.6.1 Advantages 9.6.2 Limitations and bias
10. CONCLUSION, IMPLICATIONS & RECOMMENDATIONS ..................................... 31 11. FUTURE RESEARCH ......................................................................................................... 33 REFERENCE LIST .................................................................................................................... 34 PAPERS I-III APPENDICES
A. Qualitative and quantitative measueres B. Supplementary quantitative analyses C. Approvals
1
1. INTRODUCTION Allogeneic HSCT in children is a complex invasive and sometimes lethal treatment, which carries the risk of multiple physical side-effects and complications. During the 4-6 weeks of hospitalisation, the child must master the physical, emotional and social consequences of the HSCT. The child depends on the parents for around the clock care and support to cope with the treatment. Consequently, the parents are emotionally and socially affected by the child’s HSCT, while they must continue with their responsibilities toward the healthy siblings. This dissertation is based on an intervention study that comprised medical information relay, emotional support and social counselling performed by a Family Navigator Nurse (FNN) and which targeted parents to children treated with allogeneic haematopoietic stem cell transplantation (HSCT). The present dissertation aims to explore the parental position during the child’s HSCT, using qualitative and quantitative methods, and evaluates the benefits of a parent targeted support intervention program. Firstly, the parents’ caregiver role was explored in 16 parents by means of participant observation studies and semi-structured interviews (paper I). Secondly, the parents’ major problems and the benefits of the support intervention program were explored in 21 parents (paper II). Thirdly, to test the effect of the support intervention program, conducted by the FNN using validated questionnaires, a population based clinical controlled trial was conducted among 79 parents to children treated with HSCT. This part of the study compares a parental prospective intervention group (n=25) to 1) to a retrospective parental control group (n=46) and to 2) a prospective parental control group (n=8) (paper III). The study was performed at Finsen Centre and Juliane Marie Centre, Copenhagen University Hospital (Rigshospital) during the period from 2004 to 2009. 2. HYPOTHESES AND AIMS The aim of this dissertation is to investigate the qualitative and quantitative benefits of a support intervention program for resident parents during their child’s 4-6 weeks inpatient treatment with myeloablative allogeneic HSCT. The FNN conducted parental intervention program comprised daily medical information relay, emotional support and social counselling as well as a supervised, structured education program for parents and the possibility for them to engage in physical activity (walking/biking). The hypotheses were, that the intervention would:
• support the parents’ ability to care for their child throughout the course of the HSCT. • identify the parents major problems and test a support intervention program to meet
these problems during the child’s HSCT. • reduce the parents’ level of anxiety and depression during their child’s HSCT.
The main objectives of each research focus (Papers I – III) in this dissertation, include:
• investigating, from an interactionistic perspective, the parents’ experiences and reflections on their parental role while taking care of their child (paper I).
• exploring the major problems faced by parents to children treated with HSCT during the child’s hospitalization and ascertaining how these problems affect the parents’ daily life and the FNN conducted intervention to assist them (Paper II).
• Determining the effect of the intervention program, through use of psychosocial questionnaires and investigating the parents’ levels of anxiety and depression during the child’s HSCT (Paper III).
2
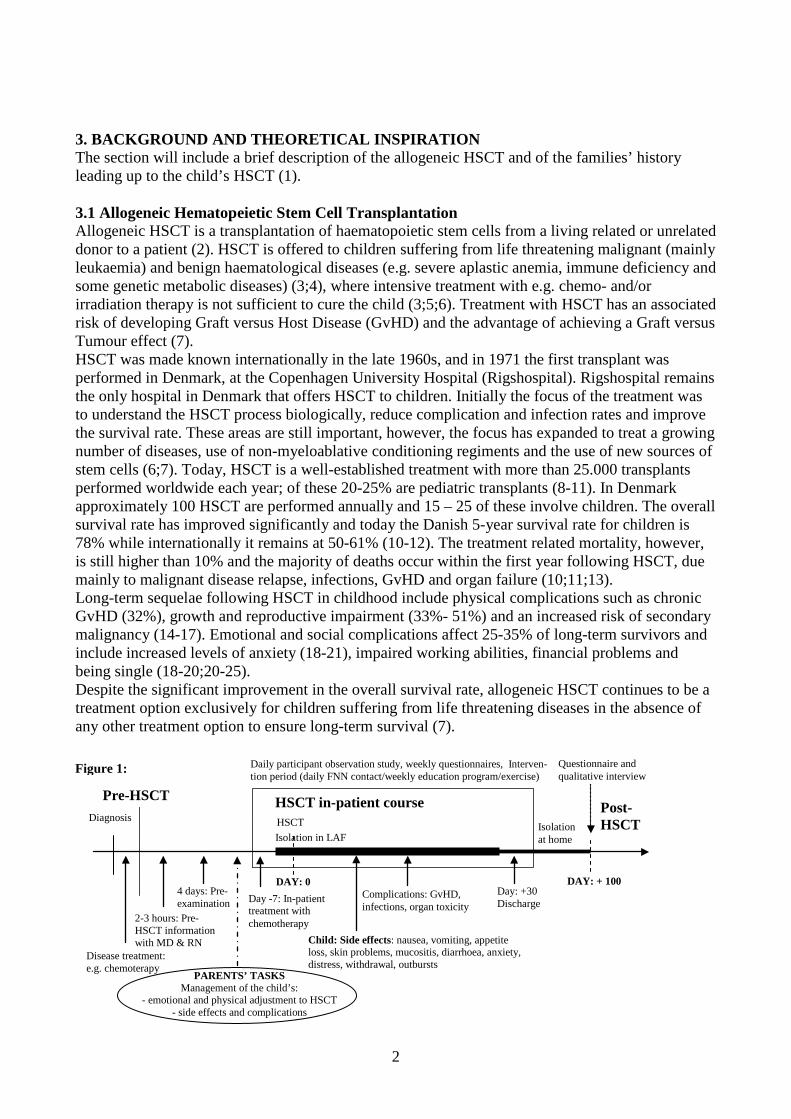
3. BACKGROUND AND THEORETICAL INSPIRATION The section will include a brief description of the allogeneic HSCT and of the families’ history leading up to the child’s HSCT (1). 3.1 Allogeneic Hematopeietic Stem Cell Transplantation Allogeneic HSCT is a transplantation of haematopoietic stem cells from a living related or unrelated donor to a patient (2). HSCT is offered to children suffering from life threatening malignant (mainly leukaemia) and benign haematological diseases (e.g. severe aplastic anemia, immune deficiency and some genetic metabolic diseases) (3;4), where intensive treatment with e.g. chemo- and/or irradiation therapy is not sufficient to cure the child (3;5;6). Treatment with HSCT has an associated risk of developing Graft versus Host Disease (GvHD) and the advantage of achieving a Graft versus Tumour effect (7). HSCT was made known internationally in the late 1960s, and in 1971 the first transplant was performed in Denmark, at the Copenhagen University Hospital (Rigshospital). Rigshospital remains the only hospital in Denmark that offers HSCT to children. Initially the focus of the treatment was to understand the HSCT process biologically, reduce complication and infection rates and improve the survival rate. These areas are still important, however, the focus has expanded to treat a growing number of diseases, use of non-myeloablative conditioning regiments and the use of new sources of stem cells (6;7). Today, HSCT is a well-established treatment with more than 25.000 transplants performed worldwide each year; of these 20-25% are pediatric transplants (8-11). In Denmark approximately 100 HSCT are performed annually and 15 – 25 of these involve children. The overall survival rate has improved significantly and today the Danish 5-year survival rate for children is 78% while internationally it remains at 50-61% (10-12). The treatment related mortality, however, is still higher than 10% and the majority of deaths occur within the first year following HSCT, due mainly to malignant disease relapse, infections, GvHD and organ failure (10;11;13). Long-term sequelae following HSCT in childhood include physical complications such as chronic GvHD (32%), growth and reproductive impairment (33%- 51%) and an increased risk of secondary malignancy (14-17). Emotional and social complications affect 25-35% of long-term survivors and include increased levels of anxiety (18-21), impaired working abilities, financial problems and being single (18-20;20-25). Despite the significant improvement in the overall survival rate, allogeneic HSCT continues to be a treatment option exclusively for children suffering from life threatening diseases in the absence of any other treatment option to ensure long-term survival (7).
DAY: 0 Day: +30 Discharge
HSCT in-patient course HSCT Isolation in LAF
Isolation at home
Pre-HSCT Diagnosis
Post- HSCT
Disease treatment: e.g. chemoterapy
Day -7: In-patient treatment with chemotherapy
DAY: + 100
Daily participant observation study, weekly questionnaires, Interven- tion period (daily FNN contact/weekly education program/exercise)
Questionnaire and qualitative interview
Child: Side effects: nausea, vomiting, appetite loss, skin problems, mucositis, diarrhoea, anxiety, distress, withdrawal, outbursts
Complications: GvHD, infections, organ toxicity
PARENTS’ TASKS Management of the child’s:
- emotional and physical adjustment to HSCT - side effects and complications
2-3 hours: Pre- HSCT information with MD & RN
4 days: Pre-examination
Figure 1:
3
Figure 1 illustrates the traditional breakdown of the HSCT course: 1) The pre-HSCT period, leading up to the transplant, 2) The HSCT inpatient course, from day – 7 to day +100, and 3) The post-HSCT period from day + 100. In addition, figure 1 provides a timeline for important medical events during the HSCT treatment course. The emphasis in this model is on the impact of the HSCT setting, the care related tasks performed by the parents and the impact of the medical treatment on the child’s and the parents’ wellbeing. 3.2 The pre-HSCT period The child’s life threatening disease challenges the stability of the family and places multiple emotional, spiritual, social and organizational stressors on all of its members (26-28). The diagnosis process exposes the child to multiple invasive tests and procedures. To control malignant diseases requires months to yearlong treatment and often includes chemotherapy and/or irradiation. Consequently, the child and the parents must cope with related side-effects such as nausea, vomiting, weight loss or gain, loss of hair, infections, mucositis, pain, diarrhoea, fatigue, and toxic reactions, etc. (26;28). Prior to the HSCT, an eligible family (often sibling) or unrelated register donor must be identified by HLA-typing (29). Approximately four weeks prior to the HSCT, a senior HSCT physician, a transplant coordinator and a nurse inform the parents and the child about the medical rationale, potential side-effects and complications associated with the HSCT. Additionally, the child is hospitalized for four days for a comprehensive health examination. 3.3 The HSCT inpatient course During the first week of admission prior to the child’s HSCT, the conditioning regimen of chemotherapy (in some cases combined with Total Body Irradiation (TBI)) is administered, followed by an infusion of stem cells from the donor. Consequently, the child experiences side- effects and possible complications, including nausea, vomiting, loss of appetite, mucositis, pain, diarrhoea, fatigue and hair loss. The child may experience organ toxicity, GvHD and he/she is treated with immunosuppression to prevent GvHD, antibiotics to prevent infections as well as nutrition and I.V. fluid (3;30;31). When the marrow has engrafted (ANC>0.5 x 109/l) and the child no longer displays acute medical or care related difficulties, then the family is discharged to isolation at home with weekly outpatient visits. 3.4 The HSCT inpatient-setting and the parents’ care related tasks The parents are the primary care givers and source of comfort for the child. Furthermore, they attempt to alleviate the child’s distress during the HSCT course (32). To decrease the risk of infection, the child and one parent (the residential) are isolated behind double locked doors in a Laminar Air Flow (LAF) room from the time of the conditioning to engraftment. The average time spent in protective isolation is 3-4 weeks. If the child has two parents then they may alternate as the resident parent. During admission, the resident parent has comprehensive care responsibilities. This includes around the clock caring for the child’s basic needs (nutrition, liquid, hygiene, activity, comfort etc.) oral care, toilet assistance and administration of oral medicine. These routine tasks must adhere to the hygienic standards of the isolation regime and the parents and the child must learn the standards before performing these basic care tasks themselves. Accordingly, parents mediate between the child and staff 24 hours/day for 4-6 weeks, during medical (invasive) procedures communicatively and by assisting the child to comply with the procedures (33;34). During the HSCT isolation period, the parents are expected to assist the child to comply with the increased basic care needs, the multiple side-effects to the treatment and the invasive medical procedures. In order for the parents to be continuously present at the hospital, they are granted leave

4
of absence from their work while retaining their regular salary which is subsidised by the social authorities (Law on social service § 42 (35)). 3.5 Emotional distress during the isolation treatment At the time of admission to HSCT, 40% of children display anxiety (36), a significant increased level of somatic distress, mood disturbances and a lowered level of activity (30). Phipps et al. (30;37) showed that during the inpatient period, the child’s distress symptoms peak one week following transplantation, and decrease to admission level by four-five weeks after HSCT. Common psychosocial reactions include depression, mood changes, anger, irritability, withdrawal and impaired interaction with others (33;37;38). At the time of admission, 20-66% of parents have a significantly elevated level of distress (39-42), and symptoms of depression and anxiety (18;40;43;44). One study suggested that a high parental level of distress and anxiety influence the parental caring ability, including responsiveness to their child needs and providing support and comfort during stressful situations (45). Parents find it especially stressful when they are unable to ease the child’s fear, shield the child from pain and embrace the child’s emotional reactions (32;34;46). The stress may affect the parents emotionally (e.g. cause secondary anxiety and depression), their parental role, the quality of the care they provide and their ability to make treatment related decisions (32;45). As such, the parents’ psychosocial well-being is interrelated with the child’s adoption of HSCT (19;32;33;42;47). 3.6 Clinical intervention studies of HSCT children In the USA, 60% of the pediatric transplant centres (n=65) offer support groups and 49% provide art-in-medicine programs (e.g. art, play and musical therapy and relaxation) to the child aiming at reducing emotional distress and side-effects. However, the duration or what point in time during the HSCT these interventions are offered is not specified. Apart from two randomised control trials (RCT), the effect of these interventions has not been tested beyond the descriptive level (48-55). Studies have shown that the children like massages and writing/painting can be a method of expressing and processing the HSCT experience. Non of the studies were performed within a Danish or European context (48;53). The most comprehensive, complementary intervention RCT (n=178 families) compared 1) a child-targeted intervention of massage and humour therapy with 2) the child-targeted intervention supplemented by a parent-targeted intervention of massage and relaxation/imagery. The program included at least two hours of intervention per week for four weeks. However, the study did not show any significant effect on the child’s level of somatic distress, on mood disturbance or on the use of analgetic and antiemetic medication (53;56). As such, HSCT child-targeted intervention programs are few in numbers (even less are RCT studies) and include a limited number of children. None of the studies have shown significant positive effects on the child’s well-being. 3.7 Clinical intervention studies among parents to HSCT children The primary research focus on the parents has been an assessment of their levels of distress, anxiety and depression and on coping strategies and factors influencing the parents coping capacity (34;40;41). None of these studies were intervention studies. One RCT study aimed at lowering the parents’ (n=22) levels of distress by offering 90 minutes of education in stress management techniques (education, relaxation, communication) prior to the child’s HSCT (57). The study showed that the intervention group used stress management techniques more frequently than the control group during the child’s HSCT, however, no significant differences between the groups were found.

5
3.8 Intervention studies aimed to reduce distress in parents to children with recent cancer diagnoses Eight complementary intervention studies were identified that aimed to reduce the level of distress, anxiety or depression in parents to children newly diagnosed with cancer (58). The total duration of the intervention was 45 minutes to eight hours /week and included 8-217 parents (58). The studies show a decrease in the parents’ levels of distress and anxiety when they have access to a web-site with medical information (59), participated in discussion sessions (60), and enhancement of their problem solving skills by means of cognitive behavioural therapy (61;62). These studies indicate that interventions where parents could express emotions and enhance their problem solving skills may be effective in reducing parental distress. However, these findings require confirmation in other studies. 3.9 Pilot study of Danish children previously treated with HSCT and their parents As there is limited evidence in the literature for interventions aimed at the parents either to children undergoing treatment with HSCT or children newly diagnosed with cancer, it was decided to perform a pilot study among parents to Danish children treated with HSCT. The aim was to explore the families’ main needs and propose interventions that would diminish the strain on them during the HSCT inpatient period. This study included seven families and was conducted through qualitative semi-structured interviews by the author (HBL). The parents and children (3 months – 3 years following treatment, in average 1 year) were recruited in the HSCT-unit’s outpatient clinic. The parents and children described how complex chains of interrelated interactions between themselves and the staff affected the children’s adjustment to treatment, the parents caring abilities and generated emotional responses. Discontinuity in interaction between the parents with the nursing staff resulted in inconsistent care and medical information relay, causing conflicts related to the care of the child. Parents and the staff’s main priority was the child undergoing HSCT treatment and as such the needs of healthy siblings were disregarded, and parents experienced being isolated in resolving this dilemma. The child’s LAF isolation resulted in the resident parent feeling socially isolated and physical inactive and generated emotional strains of insecurity, frustration and powerlessness. The parents requested that a small team of nurses be assigned to help meet the entire family’s needs. The nurses should provide consistent care, medical information, and assistance in addressing problems on a day-to-day basis. The parents requested a broader perspective on the family’s situation than just the child undergoing HSCT. This request inspired the inclusion of continuous nursing support and the provision of a case manager or patient navigator function. 3.10 Nurses performing the Case Manager/ Patient Navigator function Historically, the Case Manager (CM) and the Patient Navigator (PN) roles emerged from a need to assist patients during transition between and within the health care system and society (63). The CM provides assistance with discharge planning; housing arrangements, medical treatment, daily activities, finances, vocational training and navigation within the decentralized complex community care system (63-65). The role of the PN is to provide individualized assistance to cancer patients, families and caregivers to overcome health care system barriers, to navigate within the system, and to coordinate treatment plans (66). The PN supports the patient along the disease trajectory by streamlining the patients’ care, acting as a liaison between the patient and the medical staff, and advocating for the patients’ with the nurses and physicians (67;68) The expansion of the patient navigator role to include aspects of treatment options and compliance along the illness trajectory requires a person with an extensive nursing background in oncology care. The PN model has proven

6
a success in the early detection and treatment of breast cancer and in reducing the use of hospitals, cost of care and in family burden. The model also provides an increased stability with respect to housing, symptom control and quality of life for patients (66;67;69;70). The multifaceted functions described in the CM and PN models serve as inspiration for the introduction of a family navigator nurse to address the families’ needs during the child’s HSCT. 4. THEORETICAL FRAMEWORK The sociology of the family inspired this dissertation, especially how childcare responsibility is divided between the parents and the state. The theoretical framework is also inspired by a symbolic interactionistic approach (71;72), founded by the Chicago School, and a cognitive behavioural approach (73-75). The Chicago School is characterised by being multidisciplinary, applying methodological diversity in their empirical research and attempting to provide means for people to improve their lives (76;77). Arlie Hochschild, a descendant from the Chicago School, inspired this study with her work on balancing home and work life within the family. Hochschild´s contribution to the sociology of emotions also provides inspiration to the theoretical approach of the social context in emotional management. Behavioural and cognitive behavioural theories lent inspiration to the emotional support provided in the intervention study. 4.1 A sociological approach to the family The State expects the family to perform certain roles and functions while maintaining, transferring and establishing social order within the society. This includes an expectation that the family, as a social institution to care for offspring, also continues its caring role during treatment of life threatening diseases (78). Furthermore, the State has the authority to control the manner in which these care responsibilities are performed and can sanction any failures by e.g. constructing labels such as a “problem family” or ultimately removing the child from the parents’ custody. But, the State also provides the framework and resources for the family to comply with these expectations, e.g. in relation to the child’s HSCT treatment the Danish social law ensures the parents economic compensation while caring for their child. In general, parents have the most enduring influence on the child’s life and socialization. The most enduring influence on children’s lives and socialization derives from the parents’ socio-economic status, child rearing practice, cultural background, religious beliefs and mode of communication (79). The importance of the parent’ s emotional well being and socio-economic status for the child’s adaption to HSCT treatment is indicated in the literature on HSCT (41;42;80-83). However, what factors indirectly or directly influence the parents and the child remain unexplained as do the different patterns of parental adaptation to the caring task and how it is possible to intervene to strengthen the bond between parents and child (84;85). 4.2 Balancing work and home The books, “The time bind” (86) and “The second shift” (87), by sociologist Arlie Hochschild address the dilemma of balancing the expectations and relationship between work and home. She describes the competition that exists between work and family time and the problems related to being “a serious player” at work and a “family man” at home. Within the family, she highlights the relationship between power (actual or perceived) and the bonds of human caring. She studied the myths and strategies developed by couples to live up to inequalities in workloads and the “economics of gratitude” displayed. Hochschild’s theory on the relationship between work and home provides an approach to the dilemma between the different rationalities that govern the work place and the home environment. The relationship between work and home, that Hoshschild describes, holds some resemblance to the relationship the parent describes when addressing the

7
association between the demands from the child’s hospital inpatient treatment and home and as such “economics of gratitude” may be seen among the parents. 4.3 Emotional management Hochschild´s sociology of emotions provides a framework for understanding how emotions are imbedded in the conflict between the body and society. Hochschild’s interactionistic perspective is centred on notions like feeling rules, emotional work and altering of emotions by surface and deep acting. According to Hochschild, every society has a set of cultural rules that governs emotions that are possible to feel, which are appropriate to feel, which are expected to be displayed in a given situation, and how inappropriate emotions are sanctioned (88;89). Emotions are associated with images, ideas and thoughts and can be changed e.g. by changing the cognition, a process referred to as ‘emotional work’. Emotions are manipulated by “surface acting” or “deep acting” (88), the difference being the level of emotional work performed in the given situation. In surface acting, a person changes the outward expression to match a feeling rule, e.g. by smiling instead of showing anger where as in deep acting the cognition of the emotion is changed e.g. by transforming the emotion of anger into empathy (88). Hochchild´s theory on emotions has inspired this dissertation in two ways, i.e. by providing an understanding of the emotions that the parents are expected to express during the HSCT course and by the way that the parents engage in emotional management by using surface and deep acting techniques while interacting with their child. 4.4 Behavioural and cognitive behavioural therapy inspiration In line with Hochschild’s sociology of emotions, cognitive behavioural therapy emphasizes the importance of cognition of thoughts on the fringe of consciousness. These thoughts precede and influence the individual’s emotional reactions and behaviour toward an event (73-75). Problem-solving strategies inspired by cognitive behavioural therapy are founded on a sense of optimism (a positive orientation) that problems can be solved (61). Solving problems requires accurate identification of the problem, the cause of the problem, implementation of a strategy for resolution, and evaluation of the solution (90). Mothers to children who were newly diagnosed with cancer (n=440) were offered an intervention of eight hours duration to learn problem-solving strategies. Compared with a group receiving standard care, their problems solving skills were significantly enhanced when measured at 3 months, e.g. the Social Problem-Solving Inventory (91) and Profile of Mood States (92), however, at 6 months following the intervention the standard care group reached the same lowered level as the intervention group, and at this point there was no significant effect noted from the intervention (61). In adults suffering from anxiety and depression, cognitive behavioural therapy techniques have proven effective in the treatment of emotional disorders within a limited time-frame (5 –12 sessions) (74). In adults diagnosed with cancer the use of cognitive therapy has shown conflicting results (93-97). 4.5 Summary Only children with life threatening diseases are treated with HSCT. HSCT is a complex, invasive and lengthy treatment carried out in isolation, with high morbidity and mortality rates, and requiring comprehensive caregiving by the parents. The increased care needs during the HSCT treatment require a transition in the family’s daily life and induces a high level of emotional and social distress in the parents and the child. During the 4-6 weeks HSCT isolation period, the parents are the primary caregivers around the clock to ensure the child’s adjustment to increased basic care needs, side-effects and treatment complications. The few intervention studies performed among parents to children treated with HSCT have not shown positive significant effects. However,
8
intervention studies aimed at children with cancer and their parents have indicated promising results. Intervention programs have assisted parents in increasing their knowledge and sharing the cancer burden, and enhanced their problem-solving capacity. A Danish pilot study conducted by the author (HBL) indicated a need for a caregiver support intervention study, targeting the parents, by providing continuity in nursing care as well as nursing and medical guidance and by addressing the family’s emotional and social circumstances. The multifaceted function and the continuity described in the CM and PN models inspired the implementation of a family navigator nursing function for families with multiple interrelated problems, such as those families of children treated with HSCT. 5. MATERIALS AND METHODS 5.1 Design This study is a retrospective and prospective controlled study of parents to children treated with HSCT in a population-based (5.5 million) and nationwide study in Denmark. To address the problem of the limited number (n=15-22) of children (aged 0-20 years) undergoing HSCT annually, it was decided to compare three groups of parents: Parental Intervention Group (PIG) was compared to 1) Prospective Parental Control Group (PPCG) receiving the HSCT unit’s standard care, to 2) Retrospective Parental Control Group (RPCG) receiving the HSCT unit’s standard care. The study is designed as a mixed method research using qualitative methods (in-dept semi-structured interviews and participant observation) and quantitative methods (validated questionnaires). 5.2 Sample All resident parents to children (0-20 years) undergoing HSCT in Denmark were eligible for inclusion. The parents were approached during their child’s medical pre-examination (figure 1, HSCT course) and were presented with oral and written study information. Exclusion criteria were: 1) parents to children with a medical prognosis of imminent death, 2) children without a resident parent as the primary caregiver, and 3) a resident parent who was unable to speak Danish. The parents were included in three different consecutive groups (figure 2: Parent flow chart). The retrospective parental control group (RPCG) was recruited in June 2007 among 62 children treated with HSCT from 1 January 2004 to 30 June 2007. Five (8%) children were classified as ineligible (four did not have a resident parent as caregiver and one was excluded due to intensive care treatment). Consequently, 57 parents were contacted by mailed questionnaire and 46 (81%) responded. The prospective parental control group (PPCG) was recruited from 1 July 2007 to 31 October 2007 among 10 children scheduled for HSCT treatment. Two children (20%) did not have a parental caregiver and were excluded. Parents to the remaining eight children were approached for participation and all consented. Two children died within the first 100 days and accordingly six parents (75%) completed the study. The parental intervention group (PIG) (n=25) was recruited from 1 November 2007 to 31 October 2009 among 31 children scheduled for HSCT treatment. Three did not have resident parents as caregivers, two were treated at the intensive care unit (ICU) and one child had parents who did not speak Danish. Consequently, six (19%) children were excluded. Parents to the remaining 25 children were approached for participation in the PIG and all consented. A total of four (19%)

9
parents did not complete the study (two children died, one child had a relapse of the underlying disease, one parent did not adhere to the data collection schedule). Consequently, 21 parents completed the study. 5.2.1 Excluded parents in the study The number of children (n=6) excluded for not having a resident parent, as the primary caregiver was higher than predicted during the study planning. The under-aged children were care for by professional teams of social workers. The caring skills of the social workers were not within the scope of this study. The young adults (18-20 years old) received support from a spouse or friends and likewise, the skills of these resources were not within the scope of this study. The children treated in ICU were not approached for study participation since the unique situation these parents were facing was outside the scope of the intervention program and related study measures. As such, it was considered unethical to include this group of parents in the study. Figure 2: Parent flow chart
Excluded: n=6 0-18 years, no residential parent: n=2 18-19.9 years, no residential parent: n=1 ICU treatment: n=2 (died: day +1, day +48) Language barriers: n=1
Parents approached: n=25 All included
Lost to follow-up: n=4 Drop out: n=1 Relapse: n=1 Died before day +100: n=2 (day +31, day +50)
Day +100 Follow-up: n=21
Parental intervention group: n=31 Parents to child 0-19.9 years Scheduled HSCT: Nov 1, 2007–Oct 31, 2009
Excluded: n=2 0-18 years, no residential parent: n=2
Day +100 Follow-up: n=6
Parents approached: n=8 All included
Lost to follow-up: n=2 Died before day +100: n=2 (day +10, day +57)
Prospective parental control group: n=10 Parents to child 0-19.9 years Scheduled HSCT: Jul 1, 2007–Oct 31, 2007
Parents approached: n=57 By mail questionnaires
Excluded: n=5 0-18 years, no residential parent: n=1 18-19.9 years: no residential parent: n=3 Intensive care unit (ICU) treatment: n=1
Excluded: n=11 Declined to participate: n=2 Did not respond: n=9
Parents included: n=46 Response rate: 81% Qualitative interviews: n=7 (Pilot study)
Retrospective parental control group: n=62 Parents as primary caregiver to child 0-19.9 years, alive HSCT: Jan 1, 2004–Jun 30, 2007

10
5.3 Baseline medical and socio-demographic characteristics of the children and parents Baseline medical and treatment characteristics of the children and socio-demographic characteristics of the 79 resident parents included in the study are described in Paper III, table 2. The socio-demographic characteristics for the PIG are described in Paper II, table I. There were no significant differences in the children’s baseline medical or treatment characteristics between the PIG, the RPCG and PPCG. In general, the children had high performance rates at baseline with a mean Karnofsky score (98)/Lansky play performance score (99) equal to or above 90. A score of 90 indicates the ability to carry on normal activity with minor signs or symptoms of disease or alternatively minor restrictions in strenuous physical activity. There was no significant difference in baseline socio-demographic characteristics between the parents included in the PIG and the two control groups. It should be noted that the parents who completed the data collection measures were the resident primary caregivers, and as such this study includes both maternal and paternal caregivers, (appendix B). 5.4 The supportive intervention 5.4.1 The author’s background and function in the intervention program The FNN role was inspired by the CM (63-65) and the PN (66-69) concepts. The role of the FNN was to carry out the following tasks:
1. facilitate the family’s transition between home and hospital, and the return to home following HSCT;
2. assist the family to navigate through the highly specialized and complex HSCT treatment course; and
3. eliminate barriers that negatively affected the parents’ care for their children. Figure 3: The FNN position in the intervention model
Isolation
Family Navigator Nurse
Foundations etc. Other children
Hospital
Municipality
Medical information relay
Treatment plans, medical complications, side effects
Nursing care
Side effects: nausea, vomiting Oral intake: medicine, fluid, food,
nutritional support Other: skin care, pain, diarrhoea
Emotional well being
Social functioning
Financial difficulties, income compensation, additional financial support, housing
evaluation, social network
Discharge planning Nursing care support to the
child after discharge
HSCT Child
Parents
Physicians
Nurses
Psychologists, social workers, etc
Home care nurses
Social authorities

11
The author (HBL), an educated nurse and sociologist, filled the FNN function during the 2½-year intervention period. The author has extensive nursing care experience within allogeneic HSCT, during the inpatient period and during the outpatient recovery period. However, the author had never worked at the HSCT unit where the intervention program took place. As a FNN the author relayed medical information to the parents as well as providing emotional support and social counselling interventions for the duration of the child’s inpatient period (4-6 weeks). Being able to follow the family allowed for continuity in addressing changes in the child’s medical condition and building trust when addressing the family’s specific problems. Each day the FNN made rounds to the child’s isolation room. Figure 3 illustrates the FNN´s position in the relationship between the parents and the highly specialized hospital treatment staff and social authorities in the parents’ municipalities.
5.5 Intervention program Literature on intervention studies carried out among parents to severely ill children, expert clinicians and recommendations from seven pilot study qualitative interviews inspired the components of the present intervention program. The program targeted parents to children treated with allogeneic HSCT and included three components (table 1):
A. daily medical information relay, emotional support and social counselling by the FNN; B. a supervised, structured education program for parents; and C. a physical activity program for parents (walking/biking).
Table 1: The weekly 9-hour intervention schedule for parents included a FNN conducted controlled intervention program for parents to children treated with allogeneic HSCT, Denmark.
Time Monday Tuesday Wednesday Thursday Friday 9-12 (1 hour)
Medical information relay, emotional support and social counselling intervention by a Family Navigator Nurse
Medical information relay, emotional support and social counselling intervention by a Family Navigator Nurse
Medical information relay, emotional support and social counselling intervention by a Family Navigator Nurse
Medical information relay, emotional support and social counselling intervention by a Family Navigator Nurse
Medical information relay, emotional support and social counselling intervention by a Family Navigator Nurse
14-15 (1 hour)
Physical activity by a Family Navigator Nurse (Cycling)
Physical activity by a Family Navigator Nurse (Walking)
Physical activity by a Family Navigator Nurse (Cycling)
15-16 (1 hour)
Education program
Total direct parents intervention time/day
2 hours 1 hour 2 hours 2 hour 2 hours
Indirect patient intervention by the FNN
Calling, writing letters, etc. to social authorities physicians, nurses, psychologists etc. on behalf of the parents
Calling, writing letters, etc. to social authorities physicians, nurses, psychologists etc. on behalf of the parents
Calling, writing letters, etc. to social authorities physicians, nurses, psychologists etc. on behalf of the parents
Calling, writing letters, etc. to social authorities physicians, nurses, psychologists etc. on behalf of the parents
Calling, writing letters, etc. to social authorities physicians, nurses, psychologists etc. on behalf of the parents
Indirect patient intervention by FNN
1-5 hours/day/ family 1-5 hours/day/ family 1-5 hours/day/ family 1-5 hours/day/ family 1-5 hours/day/ family
As illustrated in table 1, the daily medical information relay, emotional support and social counselling intervention program was estimated to include 1 hour of daily parent contact, however, the time spent by the FNN outside of the child’s isolation room in dealing with the parents and child’s daily problems were not included in this time estimate. Depending on the complexity of the problem, the amount of time spent assisting the families to navigate through the complex medical
12
and social system (phone calls, letters, meetings on behalf of the parents, etc.) ranged from 1 hour/day to 5 hours/day. The highest number of parents included concurrently in the intervention program was three. 5.6 Principles for the intervention 5.6.1 The daily FNN intervention schedule The daily medical information relay, emotional support and social counselling intervention began the day of the child’s admission to HSCT and lasted until discharge, i.e. approximately 4-6 weeks later. The program took place in the child’s isolation room at the HSCT unit and was estimated at one hour daily, five days a week. The intervention was performed as daily rounds to the child’s isolation room. 5.6.2 The FNN intervention focused on three parent-targeted components • The medical information relayed concerned the care tasks assigned to the parents regarding the
child’s physical needs (e.g. nausea, vomiting, appetite loss, skin problems) and the child’s emotional reactions. Being a resource person to the parents, the FNN was also included in medical and care decision-making and in liaising between the parents and the medical staff.
• Daily emotional support focused on the parents’ thoughts and concerns (e.g. frustration, distress and anxiety), negative thoughts (e.g. fear of the child’s death), and the parents’ assessment of own and the child’s well-being.
• The social counselling component addressed the parents’ social and organizational circumstances, e.g. social network support and unresolved financial issues. Assistance was provided to address these problems directly or through the Danish social welfare authorities.
5.6.3 The daily rounds Daily rounds began with a formal dialogue related to the child’s medical condition, changes since yesterday and which changes to expect. This dialogue comprised medical information and education concerning the treatment plan (e.g. chemotherapy, TBI, immunosuppressive treatment), side-effects (e.g. nausea, vomiting, appetite loss, pain, skin reactions) and complications (marrow engraftment, infections, acute and chronic GvHD, etc.). The dialogue included the parents’ perceptions of the information provided to them by physicians’ and nursing staff. Clarifications were provided either by the FNN or by the medical staff. The care related tasks assigned to the parents when the child was in protective isolation were performed according to the HSCT unit’s hygienic requirements. The nursing staff instructed in these hygienic rules (e.g. the child’s body must be washed in a specific order, the child is only allowed limited food items that required sterile handling, etc.). Performance of these tasks was complicated by the side-effects of the treatment. Difficulties related to performing the basic care related tasks will be discussed and analysed below. A strategy for the parents’ care over the following 24-hour period was then developed collaboratively between the FNN, the parents and the nursing staff. If needed, the FNN addressed any special care needs with the nursing staff, e.g. adjustment of medication (pain killers, antiemetica, tests etc.), insertion or removal of tubes, catheters, etc. The emotional care tasks performed by the parents were addressed since one assumption of this dissertation is that the parents´ and children’s emotional strain are interrelated. Children’s emotional reactions to the HSCT treatment, e.g. withdrawal, emotional outburst and fear may affect their cooperation with the parents’ during caregiving. When appropriate, the parents were instructed by the FNN to use behavioural interventions such as contingency management, cognitive/attentional
13
distraction, systematic desensitisation, modelling and behavioural rehearsal to ease the child’s burden. The other assumption in the dissertation is that the child’s medical condition or emotional well being can release emotional responses in the parents, e.g. fear, sadness, anxiety and depression or joy and happiness. When these emotional reactions emerge they can impact the parents’ caring ability and the child’s emotional well-being. The unfamiliarity of a child’s HSCT treatment complicates interpretation of the emotional and medical changes in the child. For example, development of low-grade acute GvHD may be interpreted as a sign of new stem cells engraftment and treatment success whereas high-grade acute GvHD may be interpreted as a severe medical complication causing danger to the child’s life and extended medical treatment. The FNN employed elements of cognitive behavioural therapy and assisted the parents in adjusting to their emotional response to such changes. Special attention was given to parents whose emotional response was influenced by constant fear of the child’s death (e.g. intrusive thoughts). Part of the intervention program was to troubleshoot barriers that affected the parent’s ability to perform the care related tasks. This part of the intervention program included a diversity of actions, e.g.: • addressing financial difficulties with the social authorities (and private foundations), including
phone calls, correspondence and meetings together with or on behalf of the parents. • assessment of the parent’s home in terms of hygienic requirements following HSCT; including
contact with the social authorities to make any required adjustments or to secure alternative housing arrangements.
• mobilizing social network support for the parents either from their own existing social network or through contracts with the social authorities.
• establishing contact with (health) professionals e.g. physicians, psychologists, physiotherapist, hospital priest and home care nurses.
• assisting language impaired parents by contacting other professionals and the social authorities. • Addressing minor issues (ordering or locating special food or drinks for the child, finding lab
results, etc.) 5.6.4 The supervised, structured group-based education program Prior to the HSCT, the parents received 2-3 hours of medical education by a transplant physician and a nurse in HSCT treatment rationale, regarding possible side-effects and complications. The staff nurses instructed the parents (and child) in care aspects and in relation to the child’s protective isolation. During the inpatient period the intervention offered a one-hour group-based educational session for parents each week for five weeks, in a meeting room at the hospital. The sessions aimed primarily at educating the parents on topics relevant to their current situation and secondly to provide them with the opportunity to benefit from each other’s experiences. The topics were based on recommendations made by the parents from the pilot study. Five specialists were charged with the education program: • The FNN led the session ”Role changes in the family when a child is diagnosed with a life
threatening illness” This session included a discussion on changes and challenges in parental roles due to the child’s diagnosis and treatment; including consequences of work, gender, and the social authorities.
• A psychologist led the session “Emotional management”, while paying special attention to thoughts and situations that generate conflicts, and including possible solutions.

14
• A family nurse specialist ran the session “Children’s (and siblings’) reaction to a life threatening diagnosis and subsequent treatment” paying special attention to childrens emotional reactions and possible supportive parental actions.
• A specially trained play therapist led the session “ Child development when severely ill”. This session addressed developmental (social, cognitive and physical) areas that might be impaired due to the child’s illness and treatment, and guided the parents in use of play activities to support the child’s development.
• A mother to a child previously treated with HSCT ran the session “Meeting with peers and what parents find difficult during the child’s treatment period”, addressing the personal experience of having a child treated with HSCT.
5.6.5 Physical activity A physical activity program for parents (three sessions of one hour per week) was offered, with the intent to enhance their psychological well-being. This program was offered as a distraction and not to improve the parents’ physical capacity. Results from the literature indicates beneficial effects of exercise in e.g. healthy individuals and cancer patients’ levels of stress and depression (100;101). The parents were encouraged to use an exercise bike, either in the child’s isolation room or outside in the HSCT unit, at least twice a week during the child’s admission. Once a week parents were encouraged to go for a walk outside the hospital together with the FNN. 5.7 Standard care received by the control groups The parents assigned to the control groups received standard care. All parents were offered an individual 2-3 hours medical information relay session led by a senior physician and a nurse prior to the child’s HSCT. The aim of this session was to explain the medical rationale for HSCT treatment and to inform about special care needs, e.g. isolation requirements. Further medical and care information relay was provided to the parents on a need-to-know basis by the staff. Emotional support was provided by referral and included the option of psychological evaluation primarily for the child and secondly for the parents. If the psychologist recommended further sessions, those were consequently scheduled. Social support to the parents at the hospital was provided by a social worker with special education in laws applicable to the parents’ unique situation. Access to this support was done on the basis of referral and the social worker decided the parents’ needs for further assistance. 5.8 Data collection A combination of qualitative and quantitative methods, described as triangulation, was used in the current study (77;102;103). The qualitative methods were intended to provide a multifaceted insight into the parental perspective on care responsibilities and the effect of the intervention, in order to improve parental support. We applied two qualitative methods, a participant observational study and semi-structured interviews. The participant observational method was derived from social science (71) and provided systematic insight into the parents’ behaviour and interactions in the natural setting of the HSCT unit (104-106). Intervention literature on parents’ involvement in their child’s HSCT has not evaluated the use of qualitative methods. The quantitative methods were intended to provide a broad view of the parents’ levels of anxiety and depression, and to detect the effect of the intervention program. The qualitative measurements were chosen as a point of reference in comparison with international studies.

15
5.8.1 Qualitative data collection Qualitative data were collected as a participant observation study in the PIG, by semi-structured interviews with seven parents from the RPCG, and from all parents in the PRG and PIG at 100 days following the child’s HSCT. The themes investigated by the qualitative methods were developed from the theoretical framework, existing literature and the purpose of the intervention study. Silverman (77) notes that the greatest danger in field work is to seek to report everything. Accordingly, the author (HBL) developed themes for systematic data collection during the participant study and the semi-structured interviews. These themes comprised a set of questions to systematically guide the data collection process. The interactive character of this data collection method allowed for flexibility in the type of information shared and for the parents to freely express thoughts, feelings and concerns. During this process new perspectives on the theme emerged, which provided an in-depth understanding of the parents’ perspectives. 5.8.1.1 Participant observation study In order to document the nature of the FNN intervention, the author (HBL) developed a logbook for each family. In the logbook the FNN kept track of interactions with the parents and other family members. Furthermore, the FNN made daily notes of the child’s medical condition, side-effects and complications and specific areas of the child’s care and treatment were discussed. Emotional expressions by the parents and the child were noted along with the type of intervention performed by the FNN. Special note was made of topics related to the parents’ emotional thoughts and the use of cognitive behavioural techniques. Problems and remedial measures in relation to the parents’ financial, organisational and social network were noted. Apart from documenting direct interactions with the parents, the FNN also noted the time spent in resolving the parents’ problems e.g. contact with nurses and physicians, social workers, psychologists, social authorities, foundations, etc. As such, this daily logbook served to keep track of each family’s problems, progress in finding resolution to the problem and the parents’ adherence to the education and physical activity sessions. The logbook was also used to record field notes from the participant observational study. The purpose of the participant observational study was to provide insight into how the parents, as primary caregivers, ascribed meaning to their behaviour and beliefs during actions and interactions (77;103). One of the aims was to investigate the parents’ reflections on their parental role while taking care of their child. Therefore, prior to the observational study the author (HBL) developed a scheme for observation with respect to the following theme questions (appendix A): • How and by whom are routine child care activities performed? • How do the parents cope with the child’s medical condition practically and emotionally? • How do the parents interact with the child and the staff? • What goals are the parents trying to accomplish by their care and interactions? • What distress factors are perceived as major based on non-verbal and verbal communication?
The logbook also contained a collection of other observations, including parental actions, descriptions of interactions, assumptions and thoughts on patterns that need to be confirmed or explored later. Field notes from the observation study were transcribed after each encounter. The daily observational data were systematically gathered by the author (HBL) among the 25 families included in the PIG by (HBL) (30 minutes - 2 hour/daily, average 90 minutes/day) from baseline to the child’s discharge.

16
5.8.1.2 Semi-structured interviews According to Weber (107;108) it is important to understand the individuals rationale as they motivate their action. The purpose of including semi-structured in-depth interviews was to provide insight into the parental perspective of the problems (77;103) experienced in relation to the child’s HSCT and to evaluate the effect of the intervention program. The interview guidelines were developed by the author (HBL) and explored the following themes (appendix A): • The type of care-related tasks performed by parents. • The care situations found to be stressful during hospitalisation. • How parents, children and staff co-operated and coped with these situations. • Major problems experienced by the parents in relation to the child’s HSCT treatment. • The impact of the child’s HSCT treatment on the parents’ physical, financial and psychosocial
situation. • The type of support needed to enable the parents to provide care for their child. Each group of parents was requested to impart their experience of the intervention program based on their unique position. For example, the RPCG were asked which intervention would have eased their involvement in the HSCT course; the PPCG were asked to provide their perspective on the data collection schedule; and the PIG were asked to evaluate the intervention program. Furthermore, the semi-structured interview included an exploration of important interactions and situations from the participant observational study. All interviews were audio-recorded, transcribed verbatim and checked for accuracy. Prior to the intervention study seven families from the RPCG were approached for participation in the pilot study. The seven semi-structured interviews were held with 6 mothers, 2 fathers and three of the children (11 and 15 years) treated with HSCT. The duration of the semi-structured interview was on average 50 minutes (30 minutes - 90 minutes). These interviews are described in Paper I. The remaining 27 semi-structured interviews (six parents in the PPCG group and 21 in the PIG) were carried out at day 100. Two members of the team (HBL and LA) performed interviews of 25 - 90 minutes (mean 55 minutes) duration, at the hospital. The interviews are included in Paper I & II. 5.8.2 Quantitative data collection 5.8.2.1 Data collection schedule and procedures All of the parents included in the study were assigned a unique identification number (UID) that allowed separation of parental identifiers from information provided from the completed questionnaires. The only persons who had access to both databases were the authors (HBL and CH). Participants in the PPCG and PIG groups completed questionnaires at hospital admission (baseline), and weekly until discharge, and at day 100 following the HSCT (figure 1). The baseline information was gathered prior to entering the intervention program. The weekly questionnaires were coded with the UID number and given to the parents in a closed envelope each Monday and collected the following day by the FNN. If the parents had not responded to the questionnaires they were given an additional 24 hours to complete them. The FNN assisted parents with limited Danish language skills either by reading the questionnaires to them or by explaining unfamiliar words. Participants in the RPCG completed a mailed questionnaire once. Parents who did not respond to the first mailed questionnaire were contacted by mail two weeks following dispatch of the first questionnaire and once by telephone. The anonymized questionnaires were scanned by an outside agency and checked for accuracy and systemic errors.

17
5.8.2.2 Assessment instruments and questionnaires All of the parents completed a self-developed questionnaire (by the author HBL) on socio-demographic information at baseline. The contents of the questionnaire were inspired by validated questionnaires used in social research (109) and methodological considerations when designing the survey questions (110). At baseline, weekly throughout the child’s admission and at day 100 the parents completed the following validated questionnaires: the Hospital Anxiety and Depression Scale (HADS) (111), the Behavioural, Affective and Somatic Experience Scale (BASES) (112;113), Profile of Mood States-B (POMS) (92) and Coping Health Index for Parents (CHIP) (114). To obtain a Danish version of the BASES and CHIP, we used a back and forth translation by two independent bilingual researchers following the recommendation of the EORTC (115). Furthermore, we conducted a semantic equivalence testing of the socio-demographic questionnaire, BASES and Chip with 10 parents to HSCT children in order to further evaluate the face validity (116). (Questionnaires, appendix A). The child’s medical and treatment information (Paper I, II, III) Medical and treatment information on the children were drawn from medical records. This included each child’s gender, age, diagnosis, donor relationship, graft source and performance score by the Karnofsky performance status (98) or Lansky play performance scale (99). The Karnofsky performance scale is a functionality measure including disease status, normal activity ability and general health. The equivalent scale used on the children is based on their play and activity levels. Both scales measure the child’s performance on an 11-point scale (0-100, in intervals of 10), discrimination death (0%) to perfect health (100%). The socio-demographic questionnaire (Paper I, II, III) The parents’ socio-demographic information included: gender of the primary resident caregiver, marital status, level of education, employment status and type, and annual household income. The parents were asked to provide information on their social network and physical well-being including medical history of severe or chronic disease, exercise habits, physical ability to walk, fatigue and the use of sleeping medicine, history of anxiety or depression including the use of pharmaceuticals, use of alcohol and their perception of whether changes in any of these areas were related to the child’s disease or treatment (appendix A). HADS (Paper III) The HADS (111) is a 14- item anxiety and depression screening tool that measures symptoms on a 4-point scale (range 0-3) (111). The results were analysed categorically, discriminating normal (0-7 points), borderline (8-10 points) and moderate to severe symptom levels (11- 21 points) (appendix A). BASES (Paper, III) The 22-item BASES questionnaire repeatedly measures, on a 5-point scale, the acute aspects of the child’s quality of life (112;113). BASES has 5 sub-scales: somatic distress, compliance, mood disturbance, quality of interactions and activity. The parental version of BASES was used on all parents while the children’s version of BASES was used in the PIG and PPCG (appendix A).

18
POMS (Paper III) The POMS (92) shortened (30-item) version measures the psychological state of the parents on a 5-point scale. POMS has 6 sub-scales: tension-anxiety, depression-dejection, anger-hostility, vigor-activity, fatigue-inertia, and confusion-bewilderment (appendix A). CHIP (Paper, III) The CHIP (114) scale (45-items) measures on a 4-point scale (not helpful to extremely helpful) parents’ responses to life when having a seriously/chronically ill child. The CHIP has three sub-scales: 1) maintaining family integration, cooperation and an optimistic definition of the situation, 2) maintaining social support, self-esteem and psychological stability, and 3) understanding the medical situation through communication with other parents and consultation with the medical staff (appendix A). 6. DATA ANALYSES AND INTERPRETATION 6.1 Qualitative data analysis (Paper I, II) Overall the data analysis was inspired by an interationistic perspective in which emphasis is placed on insights into the interrelatedness between the individual’s actions, motivations, rationale and perspectives (71;77). According to the aims, this study included an exploration of parental care provided during a child’s hospitalisation for HSCT, the problems these parents faced and the intervention required to address these problems. Consequently, these themes were included in the participant observational field notes and the semi-structured interview guide. Inspired by Malterud (117) and Lacrosse (118), the data structuring was performed by the use of a coding tree that included different categories and the tree was not complete until these patterns “made sense” (119;120). This included an “open coding” process (118) whereby the meaning units surfaced and formed patterns by questioning the phenomena reflected in the data and by identifying similarities and variations in the data. The categories included in the coding tree were derived both from theoretical inspiration and from the analytical interpretation of the data. When no new categories appeared and when the data indicators did not generate significantly new insights then the theoretical saturation point was reached(118). The open coding process was followed by an “axial coding” process whereby the emerging categories were related and combined across the coding tree into themes(118). This process was followed by “selective coding” (118) whereby the patterns and themes identified were meshed into mega themes or stories. It was decided to present the data from the current study as theoretical stories, i.e. a style that accounts for the complexity of how the categories interrelated. In paper II, we used Silverman’s “tabulation in fieldwork” (121) as inspiration to calculate the parent’s number of risk factors and the FNN intervention hours. The aim was to demonstrate the deviation between parents, through qualitative analysis. Qualitative analysis is a non-linear process in which decontextualisation and recontextualisation are important methods to assure that the identified patterns agree with the context (106;122). In order to confirm and discuss the findings, we used researcher triangulation. Researchers from the team (LA, CH) participated during the participant observation study; the researchers (HBL and LA) performed the semi-structured interviews; the author (HBL) conducted the initial coding and theoretical analysis and these were then confirmed by the other members of the research team (LA, CH, CJ).
19
6.2 Quantitative data analysis (Paper III) This study included three groups of parents: RPCG (n=46), PPCG (n=8) and PIG (n=25). In order to examine the effect of the intervention program, the degree to which the parents participated in the intervention components were measured in percentages of possible intervention days. Prior to statistical analysis, all data were controlled and corrected for systematic and accidental errors. Data from the HADS, BASES, POMS and CHIP questionnaires were coded according to the guidelines of their respective manuals. Fisher’s exact test and Mann-Whitney U test were used to investigate if the intervention and the two control groups were comparable with respect to socio-demographic characteristics and baseline measurements. To investigate whether the socio-demographic characteristics and baseline measurements for the PIG were comparable respectively the RPCG and the PPCG, Fisher’s exact test was used for categorical variables and the Mann-Whitney U Test was used for continuous variables. The efficacy of the intervention program was analysed by comparing the differences between the PIG and the PPCG on the HADS sub-scale using Mann-Whitney U test, supplemented by analysis of the parents’ BASES, POMS and CHIP measures. A secondary analysis was performed to study the within group changes in the PIG and the PPCG from baseline to the weekly test points, and day 100. The weekly measurements of sub-scale scores were analysed using a linear mixed effects model that was validated by residual plots and quantile-quantile plots. The use of a parametric model increases the power of the statistical analysis and accounts for the unbalanced data derived from the uneven number of completed questionnaires from individual parents. Spearman’s tests were used to examine the strength of the relationship between the parents’ HADS scores and sub-scales on rating their child’ well-being (measured by the BASES scale). A statistical analysis was made using “R: A Language and Environment for Statistical Computing” (123) and values of p<0.05 were accepted as statistical significance. Estimates for sub-scale scores at each time point were reported as means, standard errors and standard error of means while changes in HADS scores from baseline were displayed with 95% confidence intervals (CI). 7. ETHICAL CONSIDERATIONS The PRCG included a consecutive cohort of parents to children who were treated during the previous 3½ years and who were alive at the time of the survey. Ideally, the survey should have included all parents to children treated with HSCT during this period, however, it was decided that contacting parents to deceased children would conflict with the principle of non-maleficence (not causing harm). Additionally, if a child in the PPCG or PIG relapsed or died within the study period the parents were not requested to complete the endpoint questionnaire at day +100. The project adhered to the regulations established by the Helsinki II Declaration, the Ethical Guidelines for Nursing Research in the Nordic Countries and all laws and regulations in Denmark. The Regional Ethical Scientific Committee approved the study (File no: 01-206-7216) and the participants provided informed oral and written consent in compliance with requirements of the Committee. The study was filed with the National Data Protection Board (File no: 2007-58-0015), (appendix C)

20
8. RESULTS 8.1 Paper I (Published): An analysis of parental roles during haematopoietic stem cell transplantation (HSCT) of their offspring. A qualitative and participant observational study Using convenient sampling, the findings in this study are based on 16 semi-structured interviews (two from the RPCG, six from the PPCG and eight from the PIG) with the resident parent 100 days following the child’s HSCT treatment. Additionally, the eight parents from the PIG participated in a participant observation study during the child’s isolation period. Theoretically, the analysis was inspired by Weber’s ideal type construction and Hochschild’s interactionistic approach to the sociology of emotions. During the analysis, three ideal types of parental approaches to childcare emerged: 1) expertise-mindedness, 2) dialogue-mindedness, and 3) the approach of the socially challenged parents. The expertise minded parents rationale is based on medical knowledge and the positional control system. The child is subordinated the parents caring rationality and is left little room for abandoning procedures. The parents expect the staff to possess a high degree of medical knowledge and to adhere to procedures and if the staff fails then conflict arises. As such, this type of parents complies with and maintains hospital procedures and ensures preservation of the hospital system. The dialogue minded parents’ rationale for care is based on a personal control system. Accordingly, the parents’ care is subject to negotiation and seeks to include their own and the child’s wishes and emotions. The parents expect the staff to use their medical knowledge to find procedures that encompass their wishes and emotions with respect to childcare, and conflicts arise when these are not taken into consideration. As such, the dialogue-minded parents constantly challenged the hospital’s procedures and attempted to change the hospital system. Being able to manage these two approaches required emotional work by the parents in the form of both surface- and deep-acting. The socially challenged parents failed consistently to adopt either of these two approaches to care and complied with staff expectations. Furthermore, they had difficulties in managing and adhering to hospital procedures. Consequently, the childcare required for HSCT pressured the socially challenged parents to such a degree that they felt incompetent and distressed. These parents were in need of staff support to manage the child’s caregiving and challenged the hospital’s system by the level of support they required to provide care for the child. The current analysis provides a new perspective on the complex interactions that occurred between the parents, the child and staff during the child’s HSCT treatment. 8.2 Paper II (submitted): Socially disadvantaged parents of children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study, Denmark Using the quota sampling strategy, 21 semi-structured interviews and 25 participant observation studies were performed in the PIG and are included in this analysis. Theoretically, the analysis was inspired by a sociological approach to the family and social marginalization. The findings of this analysis showed that during the child’s HSCT treatment the parents mastered three major problems: 1) their emotional strain; 2) re-organizing the family’s daily life to include hospitalization with the child; and 3) their strain of manoeuvring within the Danish welfare system. Having a child treated with HSCT influences the parents emotionally to such a degree that a majority of the parents describe themselves as being in emotional chaos. When in this state, the FNN conducted intervention was needed to support the parents’ caregiving abilities. The parents depended heavily on their social network of family and friends during reorganization of daily life to care for healthy siblings or to support them during the child’s hospitalisation. Families

21
with limited social network support and resources needed FNN intervention to address this need either from within their own social network or through the social authorities. The parents’ care related leave of absence from work included being granted economic compensation by the social authorities. As such, the parents were subordinate to the social authorities’ administration of the law and this resulted in delays and reductions in compensation, which left some families in financial chaos. These families needed FNN intervention to address their financial rights with the social authorities. It was shown during the intervention period that having the following pre-existing risk factors negatively influenced the parents´ ability to address the above-mentioned problems: 1) being a single parent; 2) having a low level income; 3) having a low level education; 4) having a low level of network support: 5) being a student or unemployed; 6) having a physical/psychiatric illness; and 7) ethnicity. Six families with four or more risk factors had complex emotional, social and financial problems that required extensive and persistent intervention by the FNN and that impacted their ability to provide care for the child (figure 4, figure 5). Figure 4: The 7 risk factors among the parents in the intervention group
Figure 5: The number of risk factors divided by family and intervention hours
0123456789
no riskfactors
Onerisk
factor
Two riskfactors
Threerisk
factos
Fourrisk
factors
Five riskfactors
Six riskfactors
SevenRisk
factors
0
5
10
15
20
25
30
Number of families
Interventionhours/week/family
8.3 Paper III (manuscript): Supportive Intervention Program Targeting Parents to Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation (HSCT): A controlled study The aim of this paper was to test the effect of the intervention program on the parents’ levels of anxiety and depression. The PIG (N=25) was compared with two control groups receiving standard care: I) a PPCG (N=8), and II) the RPCG (N=46). The results presented are based on completion of the following questionnaires: a socio-demographic questionnaire, HADS, BASES, POMS and CHIP from admission, weekly through discharge and at day 100. The RPCG performed the same evaluation once, by mail. The FNN intervention was performed in 92% of the expected intervention days. 72% of the parents completed the educational program and 16% participated in the physical activity sessions. The missed FNN intervention sessions were due to logistical problems. Parents to children previously treated with HSCT recommended the physical activity intervention component. However, the
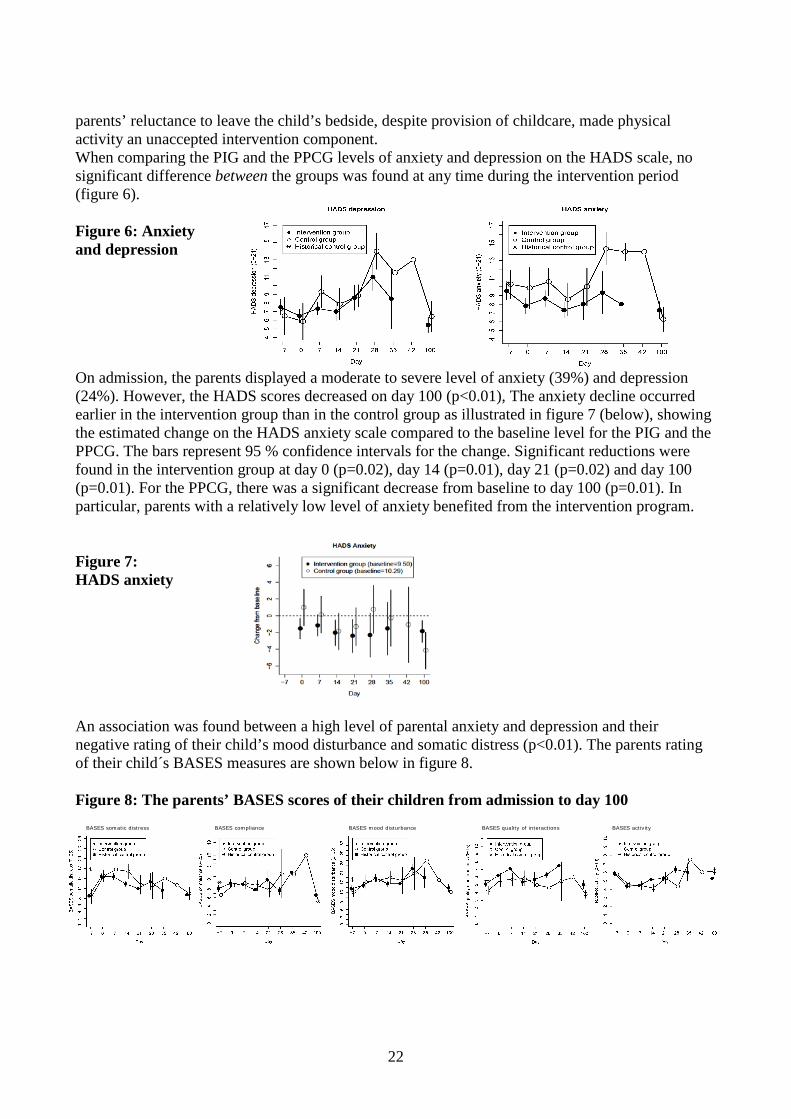
22
parents’ reluctance to leave the child’s bedside, despite provision of childcare, made physical activity an unaccepted intervention component. When comparing the PIG and the PPCG levels of anxiety and depression on the HADS scale, no significant difference between the groups was found at any time during the intervention period (figure 6). Figure 6: Anxiety and depression On admission, the parents displayed a moderate to severe level of anxiety (39%) and depression (24%). However, the HADS scores decreased on day 100 (p<0.01), The anxiety decline occurred earlier in the intervention group than in the control group as illustrated in figure 7 (below), showing the estimated change on the HADS anxiety scale compared to the baseline level for the PIG and the PPCG. The bars represent 95 % confidence intervals for the change. Significant reductions were found in the intervention group at day 0 (p=0.02), day 14 (p=0.01), day 21 (p=0.02) and day 100 (p=0.01). For the PPCG, there was a significant decrease from baseline to day 100 (p=0.01). In particular, parents with a relatively low level of anxiety benefited from the intervention program. Figure 7: HADS anxiety An association was found between a high level of parental anxiety and depression and their negative rating of their child’s mood disturbance and somatic distress (p<0.01). The parents rating of their child´s BASES measures are shown below in figure 8. Figure 8: The parents’ BASES scores of their children from admission to day 100
BASES somatic distress BASES compliance BASES mood disturbance BASES quality of interactions BASES activity

23
9. DISCUSSION Expectations of how parents fulfil the parental role are embedded in their specific time and culture period (124). This dissertation presents the results of an intervention study aimed to improve the basis for parental involvement in their child’s care during HSCT treatment. The dissertation furthermore summarizes the results of an explorative controlled study including 46 parents in a retrospective control group, eight parents in a prospective control group and 25 parents in a prospective intervention group. 9.1 Parental roles: Paper 1 Focus on the parents’ rationale for care was inspired by daily observations and semi-structured interviews with the parents. The analysis included observations of interactions between the parents, the child and the staff, and the parents’ explanation of their rationale for childcare. The participant observation study focused on the parents’ childcare e.g. administering medicine, daily bathing, providing food and liquid, as well as the parents’ reflections on their own caregiving. The focus was inspired by an interactionalistic theoretical approach (72) and participant observation methodology (71;77). Three patterns emerged in the analysis of these data that were further elaborated on by combining Hochschild’s distinction between the positional and personal control system (88) and Weber’s four concepts of ideal type behaviour (the concept “ideal type” captures the essential characteristics of a particular phenomenon) (71;107;108;125). The first two patterns identified were “the expertise mindedness” and “the dialogue mindedness” parental approach to care, and in addition a group of parents who were unable to consistently comply with either a positional and personal control system. In relation to Hochchild’s theory, this latter group comprised “deviants” (77;126) since they were unable to comply with the child’s increased care demands. For example, they were unable to observe the child’s needs for care or based their care on how the HSCT treatment affected themselves and not the child (Paper I & II). The deviant cases are those that are contradictory or unusual cases as opposed to standard cases (71;77). These cases tend to reveal most about a setting or a situation and is an important part of a qualitative analysis (104). Hochschild´s theory does not address situations where either the positional or the personal control systems cannot be applied. Consequently, what characterized this group of parents is what they were unable to perform in contrast with how they performed. Weber’s concepts on the ideal type (71;107;108;125) behaviour were also included in the development of the three parental approaches to care. In this analysis, Weber’s rationale for behaviour is consistent with the two control types described by Hochschild. Contrary to Hochschild, Weber includes descriptions of behaviour that he does not perceive as rational and distinguishes between behaviour based on emotion and tradition (107;108). Based on the parents’ actions and emotional responses during the participant observation study and the parents’ expression of their emotions in relation to performing childcare, this “deviant” group of parents expressed their emotions as governing their caregiving performance and accordingly resemble Weber’s description of behaviour based on emotions. However, this group of parents was also characterized by a discrepancy between their resources and the child’s care demands. The course of this deficit could be related to the parents’ physical, mental, emotional or social capacity. We named this group of parents “the socially challenged parents”. It can be argued that this group of parents are not a genuine ideal type (107;108) since the group is generated from the analysis of deviant cases. However, we found that these parents had enough common characteristics to group them as an ideal type (107;108), as defined in paper I. In the current study (paper I) we show that the parents engaged in emotional work,both through surface- and deep-acting. These findings suggest that sociology of emotions (86-88) as a theoretical approach to exploring the emotional strain of a child’s HSCT can be developed further.
24
The advantage of the analysis on the parental approach to care in an HSCT setting, where all parents must adhere to identical hygienic rules and perform numerous care tasks daily, is that the observer interpretations were diminished regarding whether a care task was performed correctly or not. The disadvantage was that the parents were requested to disregard how they performed these care tasks outside of the hospital setting. This could explain why we were unable to identify a parental approach to care based on tradition, as described by Weber (107;108;125). Accordingly, the distinctions between different parental approaches to care identified in this study may serve as hypotheses that require confirmation and testing in other settings. The analysis also highlighted a group of parents who were in special need of assistance to manage care of the child, i.e. the group of socially challenged parents (paper II). 9.2 The parental problem areas and risk factors: Paper II We identified three major problems that required addressing if the parents were to be able to be with the child during admission to HSCT. These include: the emotional strain of the child’s HSCT; re-organizing family daily life to include hospitalization with the child; and the strain of manoeuvring within the Danish welfare system. The most unexpected finding was financial difficulty posed by the Danish welfare system. In contrast to some western countries (124;127) the Danish state provides, by law, financial security for parents to be actively involved in the child’s care during HSCT. In theory, this law ought to prevent parent’s financial concerns and distress during the child treatment. However, as shown in paper II, the parents experienced that the social authorities’ administration of the law caused reductions and delays in receiving the financial compensation and left them in an insecure financial situation. In the section “the sociological approach to the family” we described the relationship between the State and the family (78). By using this approach, a discrepancy between the State’s intentions with the law (to provide the resources for parents to fulfill their caring obligations) and the social authorities’ administration of the law (governed by an administrative technical rationality(78)) were accentuated in the parents’ everyday life and was seen as financial chaos. Therefore, while transiting from being independent and active in the work force to being full-time caregivers to a severely ill child, the parents were subjected to a second transition. Being granted income compensation, the parents became subordinate to and dependent on the social authorities’ administration of the law and were as such diminished to client status in the social welfare system. Järvinen et al. (128) showed in their analysis of the Danish social welfare system that having a client status is associated with reduced power to define own problems and an increased power given to the social system to control and sanction how parents perform their care responsibilities. As such, the analysis of the parents’ financial difficulties have highlighted a social problem, as what was law intended is contradictory to the parents’ reality. The analysis can be seen therefore as a social critique. The FNN intervention did not intend to fundamentally change the parents’ financial situation but simply to ensure that it did not hinder their parental caring abilities. The parents needed (high-power) assistance during the HSCT course to address their social needs and, as shown by Forinder et al. (129), this need continues years after the child’s HSCT. During this intervention study the FNN observed that the proportion of problems was not evenly distributed between the families. Some families (n=6) needed comprehensive FNN support to solve several interrelated problems that formed complex entities (paper II). We identified seven pre-existing risk factors that influenced the parents’ caregiving abilities during the HSCT of their child: 1) single-parent household; 2) low-level income; 3) low-level education; 4) low-level social network support; 5) student or unemployed status; 6) physical/psychiatric illness; and 7) ethnicity. The interrelatedness between the risk factors and their impact on the parents’ childcare became evident during the participant observational study (paper II). We experienced that parents with four
25
or more risk factors had an increased need for FNN intervention. This is a highly vulnerable group of parents that needs comprehensive assistance both at the hospital, at home and by the social authorities in order to manage care of the child during the complex HSCT treatment. 9.3 The parents’ level of anxiety and depression in relation to the intervention program: paper III In the current study, we were not able to show a significant effect of the intervention program when comparing the PPCG with the PIG. We showed that parents had a high level of anxiety (39%) and depression (24%) at the time of the child’s admission to HSCT, which decreased significantly at day 100. This is a high level of anxiety and depression compared with the general population (130), however, it is in line with findings in other studies (18;41;131-133) among parents to children treated with HSCT. The parents’ levels of anxiety and depression decreased significant following HSCT which is concurrent with findings in studies among parents to children treated with HSCT (18;133;134). We therefore suggest that the parents’ levels of anxiety and depression are interrelated with the threat that the disease and treatment pose on the child’s life. As such, it is questionable to what degree cognitive behavioural therapy techniques will profoundly impact the parents’ levels of anxiety and depression. The genesis of the parents’ anxiety and depression may differentiate from the anxiety and depression treated in relation to own mental disease and where these therapies have proven most effective (94). The interrelatedness between the parents’ and child’s well-being suggest that the best intervention for the parents’ anxiety and depression is to improve HSCT treatment for the child by reducing side-effects and complications and improving the survival rates. However, while treatment improvements progress it may be fruitful to try to adapt a different perspective on the emotional performed by the parents during the child’s HSCT treatment. In paper I we showed, by means of a participant observation study, that parents used both surface and deep acting to a large extent in their interaction with the child and the staff, as described by Hochschild (88). Unfolding the sociology of emotions in a setting such as the HSCT unit may provide new perspectives on the emotional work that is being performed, i.e. how emotions are expressed, suppressed, altered and exchanged (88;96). The benefits of surface acting are that parents are able to modify their facial expressions and body language. They can suppress their feelings by changing their mental focus, e.g. limit their time-frame, assume a happy face, etc. This emotional work enabled the parents to support the child to cope with difficult treatment procedures and to continue working with the staff despite errors occurring, etc. (88;95;96). The disadvantage of the use of surface acting may be an increased level of stress related to the emotional dissonance (88;95). The benefits of deep acting are that inner feelings are modified to match the required emotional expression, and hereby have been argued to reduce stress (88). The disadvantage of deep acting is that the ability to modify feelings may also include modification of bodily needs or emotions that provide important information on the body’s well-being that may require addressing (88). Hochchild´s theory may also provide insight into the emotions that parents are expected to express during the HSCT course and hereby provide a cultural perspective on the organizational expectations of parental emotional management that they as caregivers have to master in addition to their practical caregiver tasks. 9.4 FNN role and dilemmas The role of the FNN was to ease the family’s transition between home and hospital, assist the families to navigate through the highly specialized and complex HSCT treatment and support them on their return home following HSCT. During this process, the FNN was to eliminate barriers that negatively affected the parents’ care of their children. These goals were set up as ideals, since the FNN interventions were exploratory and depended on the specific problems for which the parents

26
needed support. Furthermore, the goals also provided direction for the FNN relationship to and within the field, when trying to empower the parents in caregiving for their children (135). The benefit was the possibility to explore the complexity of parents’ major problems and the boundaries for the FNN intervention. The disadvantage was the FNN’s position as an intermediary within the status hierarchy at the hospital and in relation to the social authorities, and as such not having the highest bargaining power, despite being higher than the parents’ power (135). Before addressing the advantages and limitations of the FNN position, access to the parents of children treated in isolation was required, necessitating a gatekeeping process (104) in the field, and establishing a research identity (77). The author’s (HBL) nursing experience with HSCT patients resolved the gatekeeping barrier (staff and the parents to the HSCT children). The intervention program required finding a position that could satisfy both the researcher and the intervention role yet that could be distinguished from a traditional clinical nursing role. The FNN provided support and guidance to the parents during daily rounds. While doing this, the FNN did not wear a uniform similar to that of the nursing staff but dressed in sterile attire like the parents. This allowed the researcher (also HBL) to undertake an observation study of the parents’ care in their natural setting (71;72;77), while being the person who performed the intervention program. This position is best described as a “participant as observer” role (77;104;136) and the parents consented to participating in the observational study and intervention program. To perform a concurrent participant observation and intervention study requires a balance of the researchers’ involvement in the each situation (137). On the one hand, intervention in a situation changes the possibility of performing “out side” observation of an “untouched” situation. On the other hand intervention provides the FNN with an important “inside perspective” (136) of the parents’ situation, since the FNN needs to address and solve the same problems as the parents,e.g. claims with the social authorities, dissatisfaction with the nursing staff, disagreement with medical procedures, etc. Furthermore, through the intervention, the researcher partakes in defining the setting for the observations, hereby changing the “natural setting” from one that is untouched and uninfluenced. A methodological objection to the notion of a “natural setting” as being uninfluenced by research is that it is an illusion; we attempted instead to describe the degree to which and how the researcher influenced the setting (71;77). This dilemma was resolved over the lengthy intervention period of 2½ years, including numerous interactions that allowed for diversity in possible outcomes in similar situations. The intent of the intervention program was to provide a supplement to standard care. Accordingly, while the staff performed their work, the FNN’s role is best described as that of an “observer as participant” (77;104;136), i.e. observing the interaction between the staff and the family. However, if the FNN observed situations in which nursing related errors occurred (e.g. wrong dosage of medicine, disregarding procedures or providing incorrect information), the research observational role was transformed to a “complete participant” intervention nursing role (77;104;136) In these situations the researcher used the professional nursing power related to the FNN role to address and correct the errors with the nursing staff. Such interactions with the staff confirmed the FNN position as being “on the parents’ side” (136) but “inside” the hospital system and “outside “the HSCT unit staff”, as was the original intention (66;68;69). The FNN position is intended to be a mediating position between the parents and the staff, and accordingly the FNN is able to relate to both sides. This is, however, not the same as agreeing with both sides, and the FNN role requires both surface- and deep-acting as described by Hochschild (88;95;96).The FNN position outside of the regular nursing staff at the unit decreased bargaining power with the nursing group. The parents’ bargaining power was however increased and the introduction of the FNN position may have also provided a small change in the power balance between the parents and the hospital staff and the social authorities (135).
27
9.5 Qualitative methodological considerations and limitations This study is one of only a few intervention studies that target parents to children treated with HSCT and to our knowledge it is the first controlled study that tests the effect of an intervention on the parents’ levels of anxiety and depression during the child’s inpatient period. Additionally, it is the first study to include qualitative methods such as participant observation and semi-structured interviews in determining the benefits and barriers of the intervention. The strength of this study is the controlled study design, including pre-, during- and post-test points by triangulated methods (quantitative and qualitative) that encompass a Danish national cohort of parents to children treated with allogeneic HSCT (103;138;139). All of the parents approached (100%) accepted to be included in the study and the group is representative of parents to children treated with HSCT living in a welfare-based society where medical treatment is free-of-charge (external validity). During the 2½ years of prospective data collection, the care, treatment and procedures related to allogeneic HSCT of children remained the same as did the intervention program and the qualified health professionals treating the children. 9.5.1 Sampling in the participant observation study and qualitative interviews In order to gain in-depth understanding of the parents’ care experience, we used qualitative methods including participant observation carried out during the daily FNN interventions and in-depth semi-structured interviews 100 days following the child’s HSCT (120). This group of parents’ had comprehensive experience as primary caregivers to a child treated with HSCT within the Danish health and welfare system during the hospital treatment period of 4-6 weeks and at home following discharge. As such, this sample of parents possessed the necessary knowledge of the themes under investigation (119). To gain insight into the potential advantages and disadvantages of the intervention program it was important to include a diverse group of parents. This is in line with qualitative sampling strategies concerned with achieving diversity by seeking to including dimensions that are likely to influence the respondents’ experiences and perspectives, such as language skills (140;141).The advantage of including a diverse group of parents was evident in the qualitative part of the study, whereby this group of parents accentuated vital aspects of the parental care role (paper I) as well as their difficulties in manoeuvring within the Danish health and welfare system (paper II). The participant observation study was carried out daily among all parents in the intervention group during the child’s hospitalisation. All parents approached accepted to participate. At day 100, following the child’s HSCT, a total of 27 semi-structured interviews were performed in the prospective control group n=6 and intervention group n= 21. As such, the semi-structured interviews were performed among all of the parents (100%) who completed the intervention study. During the pilot study, seven semi-structured interviews (retrospective control group) were performed. Hereby, 25 participant observational studies and 34 semi-structured interviews provide the basis for the qualitative findings in this study. The number of respondents in this study sufficed to account for essential aspects of the parents’ experiences as caregivers and of their participation in the intervention program. Data saturation (106;117) was reached at different points in the two analyses presented in paper I and II. In paper I, using convenient sampling (77;103) data, the saturation point was reached within the first 12-14 interviews, however, two more interviews were performed. Data saturation (77;103) was decided based on a theoretical saturation point when no new perspectives and insights emerged during the interviews. The use of this sampling strategy required that the data analysis and review be combined with the data collection process.

28
In paper II, it was important to include data from the 21 interviews in the intervention group since this paper addressed the experience of participation in the intervention program and a quota-sampling strategy was applied (77;103). 9.5.2 Validation of the participant observational study and semi-structured interviews In the analysis of the parents’ different approaches to the child’s caregiving (paper I), we combined the data collected during the participant observation study with the parents’ thoughts on care as expressed during the semi-structured interviews. We achieved respondent validation by confirming the observations from the participant observational study in the qualitative interviews. However, qualitative methodology literature questions the extent to which this validation is necessary (105;140;141). The advantage of member checking as a method to achieve internal validation is that the parents are able to correct errors and misinterpretations and elaborate on the observed data with additional information and perspectives. As such, the researcher also gains the advantage of summarizing preliminary findings (126;142). The disadvantage of member checking is that some findings are not easily associated directly with the participants, e.g. findings related to difficult care situations and in which the participants could deny the viability of the data and have them removed from the data material (143). Furthermore, member checking is based on the assumption that there is a fixed truth of reality that can be confirmed by the researcher and the respondent. Qualitative research findings, however, are based on combining and abstracting patterns across individual respondents (105;126;142). In the current study we did not validate by member checking, however, we asked the parents about their perceptions of the child’s medical treatment, as well as the care related tasks and interactions during the HSCT course. By applying qualitative methods we intended to gain a comprehensive understanding of the parents’ complex and multifaceted experience in their parental role through a bottom-up approach (140;141). We explored the tension between the parents’ caregiving and competences and the places where the “…embodied and embedded lived experience meet the clinical reality and current institutional structures and processes” , as expressed by Miller and Crabtree (71). By adding depth and context to the parents’ actions, unseen and unheard dimensions of their care surfaced and as such a new perspective on their rationality of caregiving for their child (paper I). The interpretative process in qualitative research involves creating meaning by identifying patterns and developing a context for understanding the parents’ experiences within a theoretical framework (141). In paper I we described three new ideal types of parental roles and the emotional work required to engage in these roles. In paper II, we described the impact of the parents’ pre-existing risk factors on the care they provided for their child. As such, the use of qualitative methods has generated new hypotheses and insights into the parents’ complex situation. Insights and hypotheses that may be subject to testing in other settings and parental care situations (77;140) The use of qualitative methods explored the changes the child’s treatment posed on the parents’ everyday life, including the parents’ experiences with the Danish social authorities (paper II). The parents’ experience of how the law is administered by the local social authorities include a social critique of the distribution of power and privileges and how they influence the parents caregiving (119). Inclusion of both observational data and semi-structured interview data made it possible to gain in-depth insight into the parents’ perspectives on being a caregiver to a child undergoing HSCT. 9.5.3 Theoretical foundation of the qualitative findings In the current study we did not use computer programs to organize or analyse the data. Instead, we used reflection and critical thinking by content analysis to the point where the patterns “made sense”(119;120). Coding was done by structuring the data into different categories using a coding
29
tree, where some of the themes were identified in advance and some derived from the data (117;120). During this process we were inspired by three different approaches to the systematic analysis of data. In paper I, in order to comprehend the parents’ experiences beyond the descriptive level, the categories were analysed inspired by Hoschchild and Weber’s theoretical framework. In paper II, the theoretical inspiration was derived from the social marginalization theory. During this analysis we used a combination of editing (data-based) and template analysis (theory-based) (106), while identifying the problem areas that the parents were facing during the child’s treatment (paper II). We used a crystallisation analysis style in which the most important aspects of the parents problems were presented (122). During this analysis, the categories identified were cross-checked for conflicting explanations (106) as we were unable to identify quotations from the parents that could be characterized by Weber as expressions of a tradition based rationality (107;108) (paper I). While decontextualising and recontextualising, it was important to assure that the identified patterns remained in agreement with the parental context (106;122). This process can best be described as a Malterud (106) inspired approach where we used the total impression of the data to identify meaning units, followed by identification of the individual meaning units and ending by summarising their importance. 9.5.4 The researchers role in qualitative research Within the qualitative tradition the researcher is actively involved in the study field and interacts with the respondents (106;119;141). Accordingly, the researchers’ skills, training, responsiveness and reflectivity on own engagement (self-critique) becomes important (119;120;141). The initial analysis of the observed patterns was performed by HBL and was re-analysed by the co-author during participation in the daily interactions with the parents (CH, LA) and during the analysis of the semi-structured interviews (LA) (142). However, in order to maintain structure and focus within this research tradition, the qualitative interviews were carried out according to the interview guidelines. All parents were subjected to the same themes in a semi-structured interview guide, however, each group of parents was also interviewed on their particular position in the study. For example, the prospective control group was asked how they experienced filling out weekly questionnaires while the intervention group was asked to reflect on their perception of the different intervention components. Additionally, to support the study’s conformability (106), some of the qualitative interviews were performed by a senior researcher (LA) and during the 2½-year intervention period the FNN was supervised by the other members of the research team (LA, CH and CJ). The internal validity of the study refers to factors that interfere with the study and thereby raising the possibility that the results of the study can be ascribed to other factors than the interventions performed. Ideally, the difference in intervention should be the only source to outcome difference. However, the daily FNN function, highly promoted interaction and intervention between the FNN and the parents in order to support the latter. The risk of this design is that it promotes the therapeutic personality bias (105;120) whereby the FNN influences the parent’s perception of the benefit of the intervention program or the effect of the program is related to the FNN’s personality and not to the intervention program itself (119;141). However, all parents were assigned to the same FNN, which minimized the proficiency bias. In this intervention study, the FNN held dual roles both as the person performing the daily intervention program and the person who was responsible for the qualitative data collection as an integrated part of the qualitative research tradition. 9.5.5 Transferability The transferability of a study relates to the extent to which its findings can be transferred to other groups of parents or settings (106;126;142). The qualitative findings of this study may be

30
transferable to other settings where parents perform comprehensive caregiving tasks for a child with cancer or another chronic disease. Similar to this group of parents, those parents to children with cancer or other chronic diseases e.g. renal, heart or handicaps, have to manage the emotional strain of having a severely ill child and have to reorganize their daily lives in order to comply with the child’s treatment at home or at the hospital (144;145). 9.6 Quantitative methods advantages and limitations 9.6.1 Advantages The advantage of this study is that it had access to all children aged 0-20 years who were treated in Denmark during the 2.5-year data collection period. In addition, all eligible parents (100%) approached to participate in the study accepted. In total, eight parents were included in the prospective control group and 25 in the intervention group. The inclusion of a retrospective control group of parents (n=57) supported the statistical representation of the prospective parental control group. Furthermore, 46 (80%) of the RPCG completed the survey and in general, a 80% response rate on a post enquette survey is considered to be a high response rate (146). Overall, the intervention study was well accepted and only one parent was unable to comply with the study requirements. 9.6.2 Limitations and bias Bias is any systemic error in a study that results in an incorrect estimate of the effect of the intervention program, which is why these should be addressed. The two major groups of bias are selection and misclassification bias. This study was not affected by sampling bias since all of the members of the population meeting the inclusion criteria were included. In addition, the one parent who was unable to adhere to the data collection schedule made the attrition bias minimal and all data were analysed with an intention-to-treat approach (147). In addition, the study was not affected by misclassification bias since all parents included had children treated with HSCT. However, by having the RPCG respond to a questionnaire regarding their experience during their child’s HSCT, we introduced the possibility of a recall bias. Despite nationwide access to parents of children treated with HSCT, a limited number of children (N=41) were treated with HSCT during this period. As such, one weakness of this controlled study was the small sample size (148). In the present study, we were unable to show a significant difference between the intervention and the prospective control group (paper III) on the parents’ levels of anxiety and depression. The inadequate sample size affected the possibility of drawing a negative conclusion of the effect of the intervention program, as confirmed by Altman and Bland who (148) stated: “ Absence of evidence is not evidence of absence”. What Altman and Bland imply is that having a small sample size increases the risk of introducing both a type 1 and 2 error (147). The risk of a type 1 error (false positive) is present, since it is possible that the significant effect on the parents’ levels of anxiety within the group of parents with a relatively low level of anxiety may be ascribed to other factors than an effect of the intervention program. Furthermore, the possibility of a type 2 error (false negative) exist since, it is possible that the inability to show an effect of the intervention program between the groups can be ascribed to the limited statistical power of the study and not to the lacking effect of the intervention program. Accordingly, any positive or negative findings in this study should be interpreted with caution due to the limited sample size, and instead it may be treated as a hypothesis that needs to be tested in a larger sample. As such, the small sample size affected the internal validity of the study, which is the observed difference between the groups, since it challenged the possibility of gaining sufficient statistical
31
power to detect any significant difference and the effects that can be attributed to the intervention (147). Furthermore, it affects the possibility of performing more advanced statistical analysis (147). To increase the number of parents in this study we could have prolonged the study period, including other groups of parents to severely ill children or we could have designed the study as a multi-center trail by, for example, including the other Nordic countries. However, this was not considered a realistic option within the frame and premises of the present Ph.D. dissertation. Alternatively, we could have equalized the sizes of prospective control and intervention groups but in light of the limited number of children this would have reduced the possibility of gaining knowledge on the feasibility of the intervention program components. We chose to include a retrospective parental control group in stead. An advantage of this study is that 100% of the eligible parents accepted inclusion in the study which should minimize the possibility for referral, popularity and sampling bias (139). Surprisingly, the primary exclusion criterion in the present study was not having a resident parent caregiver. Of the possible eligible children, eight (20%) (two from the prospective control group and six from the intervention group) did not have parents who met the inclusion criteria for this study. Despite the limitations related to having a small sample size, we have been able to compare the levels of anxiety and depression present among Danish parents to international findings. Furthermore, this study is limited by not being designed as a RCT, which is considered the “gold standard” (147) for evaluating effectiveness of intervention studies. A RCT design would have included randomisation of participants between the prospective control and the intervention groups, allocation concealment and blinding. In the current study this was not a realistic possibility in a clinical setting where all children were treated in the same unit, and as such it was impossible to use blind participation of parents in either the intervention or the control groups or of the staff. We designed the study such that the prospective control group data were collected prior to the intervention group data. In this way we increased the possibility of introducing a selection bias (147) since the parents did not have an equal option of being assigned to either the control or the intervention group. Additionally, the sequence of allocation was known in advanced. However, with this design we minimized the risk of contamination bias between the groups but concurrently increased the risk that changes in the care affected one group more than the other (147). However, during the study period no changes in the treatment and care protocols were made nor were there changes in the staff’s organization or in the level of support provided to the parents. The external validity refers to what extent the results of a study can be generalized and transferred to other clinical settings or populations of parents and children. Since this study has limited internal validity due to the limited sample size it has also limited external validity. The external validity was also influenced by other factors such as the setting, the selection of the participants and type of intervention which are factors described in detail in relation to the qualitative methods. 10. CONCLUSION, IMPLICATIONS & RECOMMENDATIONS In this first controlled intervention study aimed to assist parents emotionally and socially in managing their child’s HSCT treatment, we showed that parents caregiving abilities are deeply affected by their child’s HSCT treatment. By applying qualitative methods and adopting theoretical inspiration from Hochschild and Weber, three parental ideal types of approach to care emerged: expertise mindedness, dialogue mindedness and the approach of the socially challenged parents. These parental types brought new insight into the relationship between the parents’ rationale on caregiving and their caregiving abilities. Additionally, these parental types provide an understanding of the rationale for care that governs parental interactions with the child and also the approach that staff should take on how to engage with each family. In this analysis, the ‘socially challenged’ parents emerged as a group in special
32
need of staff support in order for them to manage caregiving for their child. The ideal types may provide a new perspective on how different parental rationales for care preserve or challenge the healthcare system. The study findings showed that parents had to master three major problems as a consequence of the child’s HSCT hospitalisation: 1) their emotional strain, 2) re-organizing of the family’s daily life, and 3) the strain of manoeuvring within the Danish welfare system. The parents needed FNN intervention to address their emotional strain and lacking social network support. The parents who were subordinated by the social authorities administration of the law and felt financial chaos, needed FNN intervention to address their rights with the social authorities. In addition, the parent needed medical information relay from the FNN concerning the HSCT treatment and related care tasks. During the study period, a group of six parents were identified with a set of pre-existing multiple interrelated complex problems. This group of parents were characterized by having four or more of the following risk factors: 1) being single parents; 2) having a low level of income; 3) having low level education; 4) having a low level social network: 5) student or unemployed; 6) being physical/psychiatric illness; and 7) ethnicity. These parents’ multiple interrelated pre-existing social circumstances influenced their caregiving ability and they had an increased need for FNN support to manage childcare during HSCT. In this first controlled intervention study that aimed to assist parents in managing their caregiving capabilities, anxiety and depression during their child’s HSCT treatment, we did not observe an effect of the intervention when comparing the intervention group and the prospective control group when using validated questionnaires. However, the analysis was affected by the small sample size. Results showed that the parents experienced a considerable level of anxiety and depression during the child’s HSCT treatment but which decreased after the treatment. In addition, the FNN support intervention seemed to benefit parents with a low level of anxiety at baseline. Clinical implications of the parental roles Considering the parents’ ideal type would benefit medical staff’s understanding, communication and interaction with the parents. When interacting with “expertise minded” parents the staff should adhere to written medical and care procedures both in their action and communication. These parents seek knowledge on correct medical and care procedures and gain a sense of control by knowing that routines are performed correctly. Conflicts arise when staff do not adhere to procedures or do not meet the parents as “equally” skilled in relation to the child’s care and treatment. “Dialogue minded” parents seek knowledge on how to bend procedures and treatment to adhere to their wishes. These parents gain a sense of control when their point of view is considered and conflicts arise when staff is unwilling to negotiate terms for care and treatment. The staff must recognize that “socially challenged” parents need consistent assistance and training from the staff to comply with the child’s increased care needs. In support of the different ideal types of parents it is also recommended that the parents have access to medical information and that this information encompasses nursing care and procedures. An HSCT trained physician and an experienced HSCT nurse should provide this information. Clinical implications of the parental problem areas and risk factors To a varying degree, parents need support from the staff to address changes that the child’s HSCT poses on them. Identifying parents with several pre-existing risk factors is essential since these parents require comprehensive and time-consuming support from the FNN, the staff and the social authorities to address their complex interrelated problems in order to manage care of the child. The FNN (and the parents) experienced that encounters with the social authorities regarding care related problems required considerable high-level power assistance from the hospital. Early identification
33
and support provided to these parents is highly recommended since increasing complexity in the child’s treatment only increases the complexity of the pre-existing problems. Clinical implications of the parents’ levels of anxiety and depression in relation to the intervention program The high level of anxiety and depression found in this study indicate a need for emotional support to the parents during the child’s HSCT, and possibly following the child’s treatment. This includes providing easier access to psychological and psychiatric counselling for the parents, who are in need of professional assistance to manage the strain of their child’s HSCT treatment. 11. FUTURE RESEARCH • The distinctions between different parental ideal-type approaches to care identified in this study
may serve as hypotheses that require confirmation and testing in other settings. The ideal types may bring a new perspective on how the interaction between the parents and the healthcare system influence each other. In this study, we researched the pediatric HSCT treatment from a parental perspective. To gain further insight into how to support children during HSCT, it is recommended that the children’s perspective also be included.
• The parents’ subordination to the social authorities’ administration of the law on care related leave of absence from the work forces some families into financial chaos. This needs to be researched further. A more profound theoretical understanding of the transitions and challenges facing families is suggested, especially when their situation forces them to engage in contact with the social authorities.
• It is recommended that the influence of parental social confounders including financial burdens, social network, work affiliation, etc. be included in research on the family’s situation. Children with chronic or severe diseases are highly dependent on their parents’ caregiving abilities. Risk factors that impact socially challenged parents’ caregiving abilities during treatment, and their long-term consequences, should be explored further.
• Future large-scale studies may apply this intervention model as an outset for further development of intervention models to benefit parents of children receiving HSCT. Further exploration and understanding of the genesis of the parents’ anxiety and depression may be fruitful prior to testing new intervention programs.
34
Reference List
(1) Hansen HP, Tjornhoj-Thomsen T, Johansen C. Rehabilitation interventions for cancer survivors: The influence of context. Acta Oncol 2011 Feb;50(2):259-64.
(2) Wiener LS, Steffen-Smith E, Fry T, Wayne AS. Hematopoietic stem cell donation in children: a review of the sibling donor experience. J Psychosoc Oncol 2007;25(1):45-66.
(3) Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med 2006 Apr 27;354(17):1813-26.
(4) Heilmann CJ, Jacobsen N. [Allogeneic stem cell transplantation in non-malignant diseases]. Ugeskr Laeger 2003 Dec 8;165(50):4850-2.
(5) Loberiza FR, Jr., Serna DS, Horowitz MM, Rizzo JD. Transplant center characteristics and clinical outcomes after hematopoietic stem cell transplantation: what do we know? Bone Marrow Transplant 2003 Mar;31(6):417-21.
(6) Jenq RR, van den Brink MR. Allogeneic haematopoietic stem cell transplantation: individualized stem cell and immune therapy of cancer. Nat Rev Cancer 2010 Mar;10(3):213-21.
(7) Cooper LJ. New approaches to allogeneic hematopoietic stem cell transplantation in pediatric cancers. Curr Oncol Rep 2009 Nov;11(6):423-30.
(8) Schultz KR. Haploidentical transplantation in children. Blood 2010 Apr 29;115(17):3420-1.
(9) Gratwohl A, Baldomero H, Schwendener A, Gratwohl M, Apperley J, Frauendorfer K, et al. The EBMT activity survey 2008 impact of team size, team density and new trends. Bone Marrow Transplant 2010 Mar 29.
(10) Shaw PJ, Kan F, Woo AK, Spellman SR, Aljurf M, Ayas M, et al. Outcomes of pediatric bone marrow transplantation for leukemia and myelodysplasia using matched sibling, mismatched related, or matched unrelated donors. Blood 2010 Nov 11;116(19):4007-15.
(11) Pasquini MC WZ. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR Summary Slides, 2010. http://www.cibmtr.org . 2011. Ref Type: Online Source
(12) Heilmann C. 2011.
Ref Type: Personal Communication (13) Haastrup E, Muller K, Baekgaard H, Heilmann C. Cytomegalovirus infection after
allogeneic stem cell transplant in children. Pediatr Transplant 2005 Dec;9(6):734-40.
(14) Matthes-Martin S, Lamche M, Ladenstein R, Emminger W, Felsberger C, Topf R, et al. Organ toxicity and quality of life after allogeneic bone marrow transplantation in pediatric patients: a single centre retrospective analysis. Bone Marrow Transplant 1999 May;23(10):1049-53.
35
(15) Forinder U, Lof C, Winiarski J. Quality of life and health in children following allogeneic SCT. Bone Marrow Transplant 2005 Jul;36(2):171-6.
(16) Socie G, Mary JY, Esperou H, Robert DV, Aractingi S, Ribaud P, et al. Health and functional status of adult recipients 1 year after allogeneic haematopoietic stem cell transplantation. Br J Haematol 2001 Apr;113(1):194-201.
(17) Vannatta K, Zeller M, Noll RB, Koontz K. Social functioning of children surviving bone marrow transplantation. J Pediatr Psychol 1998 Jun;23(3):169-78.
(18) Barrera M, Boyd-Pringle LA, Sumbler K, Saunders F. Quality of life and behavioral adjustment after pediatric bone marrow transplantation. Bone Marrow Transplant 2000 Aug;26(4):427-35.
(19) Felder-Puig R, di GA, Waldenmair M, Norden P, Winter A, Gadner H, et al. Health-related quality of life of pediatric patients receiving allogeneic stem cell or bone marrow transplantation: results of a longitudinal, multi-center study. Bone Marrow Transplant 2006 Jul;38(2):119-26.
(20) Nespoli L, Verri AP, Locatelli F, Bertuggia L, Taibi RM, Burgio GR. The impact of paediatric bone marrow transplantation on quality of life. Qual Life Res 1995 Jun;4(3):233-40.
(21) Forinder U, Posse E. 'A life on hold': adolescents' experiences of stem cell transplantation in a long-term perspective. J Child Health Care 2008 Dec;12(4):301-13.
(22) Helder DI, Bakker B, de HP, van d, V, Vossen JM, Wit JM, et al. Quality of life in adults following bone marrow transplantation during childhood. Bone Marrow Transplant 2004 Feb;33(3):329-36.
(23) Badell I, Igual L, Gomez P, Bureo E, Ortega JJ, Cubells J, et al. Quality of life in young adults having received a BMT during childhood: a GETMON study. Grupo Espanol de Trasplante de Medula Osea en el Nino. Bone Marrow Transplant 1998 Apr;21 Suppl 2:S68-S71.
(24) Hayden PJ, Keogh F, Ni CM, Carroll M, Crowley M, Fitzsimon N, et al. A single-centre assessment of long-term quality-of-life status after sibling allogeneic stem cell transplantation for chronic myeloid leukaemia in first chronic phase. Bone Marrow Transplant 2004 Sep;34(6):545-56.
(25) Schulz-Kindermann F, Hennings U, Ramm G, Zander AR, Hasenbring M. The role of biomedical and psychosocial factors for the prediction of pain and distress in patients undergoing high-dose therapy and BMT/PBSCT. Bone Marrow Transplant 2002 Feb;29(4):341-51.
(26) Tremolada M, Bonichini S, Altoe G, Pillon M, Carli M, Weisner TS. Parental perceptions of health-related quality of life in children with leukemia in the second week after the diagnosis: a quantitative model. Support Care Cancer 2010 Mar 13.

36
(27) McGrath P, Paton MA, Huff N. Beginning treatment for pediatric acute myeloid leukemia: the family connection. Issues Compr Pediatr Nurs 2005 Apr;28(2):97-114.
(28) McCaffrey CN. Major stressors and their effects on the well-being of children with cancer. J Pediatr Nurs 2006 Feb;21(1):59-66.
(29) Gratwohl A, Baldomero H, Schwendener A, Rocha V, Apperley J, Frauendorfer K, et al. The EBMT activity survey 2007 with focus on allogeneic HSCT for AML and novel cellular therapies. Bone Marrow Transplant 2009 Feb;43(4):275-91.
(30) Phipps S, Dunavant M, Garvie PA, Lensing S, Rai SN. Acute health-related quality of life in children undergoing stem cell transplant: I. Descriptive outcomes. Bone Marrow Transplant 2002 Mar;29(5):425-34.
(31) Loberiza FR, Jr., Lee SJ, Freytes CO, Giralt SA, Van BK, Kurian S, et al. Methodological and logistical considerations to study design and data collection in racial/ethnic minority populations evaluating outcome disparity in hematopoietic cell transplantation. Biol Blood Marrow Transplant 2009 Aug;15(8):903-9.
(32) Melnyk BM. Intervention studies involving parents of hospitalized young children: an analysis of the past and future recommendations. J Pediatr Nurs 2000 Feb;15(1):4-13.
(33) DuHamel KN, Redd WH, Vickberg SM. Behavioral interventions in the diagnosis, treatment and rehabilitation of children with cancer. Acta Oncol 1999;38(6):719-34.
(34) Forinder U. Bone marrow transplantation from a parental perspective. J Child Health Care 2004 Jun;8(2):134-48.
(35) Law on social service § 42. Lov om social service § 42 . https://www.retsinformation.dk/Forms/R0710.aspx?id=135122Size calculater web site: http://www.raosoft.com/samplesize.html . 2011. Ref Type: Online Source
(36) Meyers CA, Weitzner M, Byrne K, Valentine A, Champlin RE, Przepiorka D. Evaluation
of the neurobehavioral functioning of patients before, during, and after bone marrow transplantation. J Clin Oncol 1994 Apr;12(4):820-6.
(37) Phipps S, Dunavant M, Lensing S, Rai SN. Acute health-related quality of life in children undergoing stem cell transplant: II. Medical and demographic determinants. Bone Marrow Transplant 2002 Mar;29(5):435-42.
(38) Andrykowski MA. Psychosocial factors in bone marrow transplantation: a review and recommendations for research. Bone Marrow Transplant 1994 Apr;13(4):357-75.
(39) Dermatis H, Lesko LM. Psychological distress in parents consenting to child's bone marrow transplantation. Bone Marrow Transplant 1990 Dec;6(6):411-7.
(40) Vrijmoet-Wiersma CM, Egeler RM, Koopman HM, Norberg AL, Grootenhuis MA. Parental stress before, during, and after pediatric stem cell transplantation: a review article. Support Care Cancer 2009 Dec;17(12):1435-43.
37
(41) Manne S, DuHamel K, Ostroff J, Parsons S, Martini DR, Williams SE, et al. Anxiety, depressive, and posttraumatic stress disorders among mothers of pediatric survivors of hematopoietic stem cell transplantation. Pediatrics 2004 Jun;113(6):1700-8.
(42) Phipps S, Dunavant M, Lensing S, Rai SN. Psychosocial predictors of distress in parents of children undergoing stem cell or bone marrow transplantation. J Pediatr Psychol 2005 Mar;30(2):139-53.
(43) Jobe-Shields L, Alderfer MA, Barrera M, Vannatta K, Currier JM, Phipps S. Parental depression and family environment predict distress in children before stem cell transplantation. J Dev Behav Pediatr 2009 Apr;30(2):140-6.
(44) Packman W, Weber S, Wallace J, Bugescu N. Psychological effects of hematopoietic SCT on pediatric patients, siblings and parents: a review. Bone Marrow Transplant 2010 Jul;45(7):1134-46.
(45) Grootenhuis MA, Last BF. Adjustment and coping by parents of children with cancer: a review of the literature. Support Care Cancer 1997 Nov;5(6):466-84.
(46) Svavarsdottir EK. Caring for a child with cancer: a longitudinal perspective. J Adv Nurs 2005 Apr;50(2):153-61.
(47) Melnyk BM, Feinstein NF. Mediating functions of maternal anxiety and participation in care on young children's posthospital adjustment. Res Nurs Health 2001 Feb;24(1):18-26.
(48) Burns DS, Robb SL, Haase JE. Exploring the feasibility of a therapeutic music video intervention in adolescents and young adults during stem-cell transplantation. Cancer Nurs 2009 Sep;32(5):E8-E16.
(49) Burns DS, Robb SL, Phillips-Salimi C, Haase JE. Parental perspectives of an adolescent/young adult stem cell transplant and a music video intervention. Cancer Nurs 2010 Jul;33(4):E20-E27.
(50) Clarke SA, Eiser C, Skinner R. Health-related quality of life in survivors of BMT for paediatric malignancy: a systematic review of the literature. Bone Marrow Transplant 2008 Jul;42(2):73-82.
(51) Gunter M. [Art therapy in the psychiatric clinic. A historical analysis of the development of art studios]. Psychiatr Prax 1990 Sep;17(5):163-71.
(52) Kuntz N, Adams JA, Zahr L, Killen R, Cameron K, Wasson H. Therapeutic play and bone marrow transplantation. J Pediatr Nurs 1996 Dec;11(6):359-67.
(53) Phipps S, Barrera M, Vannatta K, Xiong X, Doyle JJ, Alderfer MA. Complementary therapies for children undergoing stem cell transplantation: report of a multisite trial. Cancer 2010 Aug 15;116(16):3924-33.
(54) Sahler OJ, Hunter BC, Liesveld JL. The effect of using music therapy with relaxation imagery in the management of patients undergoing bone marrow transplantation: a pilot feasibility study. Altern Ther Health Med 2003 Nov;9(6):70-4.

38
(55) Sherman AC, Simonton S, Latif U, Nieder ML, Adams RH, Mehta P. Psychosocial supportive care for children receiving stem cell transplantation: practice patterns across centers. Bone Marrow Transplant 2004 Jul;34(2):169-74.
(56) Phipps S. Reduction of distress associated with paediatric bone marrow transplant: complementary health promotion interventions. Pediatr Rehabil 2002 Oct;5(4):223-34.
(57) Streisand R, Rodrigue JR, Houck C, Graham-Pole J, Berlant N. Brief report: parents of children undergoing bone marrow transplantation: documenting stress and piloting a psychological intervention program. J Pediatr Psychol 2000 Jul;25(5):331-7.
(58) Peek G, Melnyk BM. Coping interventions for parents of children newly diagnosed with cancer: an evidence review with implications for clinical practice and future research. Pediatr Nurs 2010 Nov;36(6):306-13.
(59) Svavarsdottir EK, Sigurdardottir AO. Developing a family-level intervention for families of children with cancer. Oncol Nurs Forum 2006 Sep;33(5):983-90.
(60) Kazak AE, Simms S, Alderfer MA, Rourke MT, Crump T, McClure K, et al. Feasibility and preliminary outcomes from a pilot study of a brief psychological intervention for families of children newly diagnosed with cancer. J Pediatr Psychol 2005 Dec;30(8):644-55.
(61) Sahler OJ, Fairclough DL, Phipps S, Mulhern RK, Dolgin MJ, Noll RB, et al. Using problem-solving skills training to reduce negative affectivity in mothers of children with newly diagnosed cancer: report of a multisite randomized trial. J Consult Clin Psychol 2005 Apr;73(2):272-83.
(62) Hoekstra-Weebers JE, Heuvel F, Jaspers JP, Kamps WA, Klip EC. Brief report: an intervention program for parents of pediatric cancer patients: a randomized controlled trial. J Pediatr Psychol 1998 Jun;23(3):207-14.
(63) Dixon L. Assertive community treatment: twenty-five years of gold. Psychiatr Serv 2000 Jun;51(6):759-65.
(64) Schaedle R, McGrew JH, Bond GR, Epstein I. A comparison of experts' perspectives on assertive community treatment and intensive case management. Psychiatr Serv 2002 Feb;53(2):207-10.
(65) Meyer PS, Morrissey JP. A comparison of assertive community treatment and intensive case management for patients in rural areas. Psychiatr Serv 2007 Jan;58(1):121-7.
(66) Freeman HP. Patient navigation: a community based strategy to reduce cancer disparities. J Urban Health 2006 Mar;83(2):139-41.
(67) Wilcox B, Bruce SD. Patient navigation: a "win-win" for all involved. Oncol Nurs Forum 2010 Jan;37(1):21-5.

39
(68) Swanson J, Koch L. The role of the oncology nurse navigator in distress management of adult inpatients with cancer: a retrospective study. Oncol Nurs Forum 2010 Jan;37(1):69-76.
(69) Robinson-White S, Conroy B, Slavish KH, Rosenzweig M. Patient navigation in breast cancer: a systematic review. Cancer Nurs 2010 Mar;33(2):127-40.
(70) Ziguras SJ, Stuart GW. A meta-analysis of the effectiveness of mental health case management over 20 years. Psychiatr Serv 2000 Nov;51(11):1410-21.
(71) Denzin NK, Lincoln YS. The SAGE handbook of qualitative research. 3rd ed ed. Thousand Oaks: Sage Publications; 2005.
(72) Blumer H. Symbolic Interactionism [1969]. In: Calhoun C, editor. Contemporary sociological theory. 2nd ed ed. Malden, MA: Blackwell Pub; 2007.
(73) Beck AT. Cognitive therapy and the emotional disorders. New York: Meridian Book; 1979.
(74) Beck AT, Emery G, Greenberg RL. Anxiety disorders and phobias a cognitive perspective. 15th anniversary ed ed. New York: Basic Books; 2005.
(75) Beck JS. Cognitive therapy for challenging problems what to do when the basics don't work. New York: Guilford Press; 2005.
(76) Adams BN, Sydie RA. Sociological theory. Thousand Oaks, Calif: Pine Forge Press; 2001.
(77) Silverman D. Interpreting qualitative data methods for analyzing talk, text and interaction. 3rd ed ed. London: SAGE; 2006.
(78) Jamrozik A, Nocella L. The sociology of social problems theoretical perspectives and methods of intervention. Cambridge, U.K: Cambridge University Press; 1998.
(79) Schor EL. Family pediatrics: report of the Task Force on the Family. Pediatrics 2003 Jun;111(6 Pt 2):1541-71.
(80) DuHamel KN, Rini C, Austin J, Ostroff J, Parsons S, Martini R, et al. Optimism and life events as predictors of fear appraisals in mothers of children undergoing hematopoietic stem cell transplantation. Psychooncology 2007 Sep;16(9):821-33.
(81) Rini C, Manne S, DuHamel K, Austin J, Ostroff J, Boulad F, et al. Social support from family and friends as a buffer of low spousal support among mothers of critically ill children: A multilevel modeling approach. Health Psychol 2008 Sep;27(5):593-603.
(82) Vrijmoet-Wiersma CM, Kolk AM, Grootenhuis MA, Spek EM, van Klink JM, Egeler RM, et al. Child and parental adaptation to pediatric stem cell transplantation. Support Care Cancer 2009 Jun;17(6):707-14.

40
(83) Barrera M, Atenafu E, Hancock K. Longitudinal health-related quality of life outcomes and related factors after pediatric SCT. Bone Marrow Transplant 2009 Aug;44(4):249-56.
(84) Brown RT, Wiener L, Kupst MJ, Brennan T, Behrman R, Compas BE, et al. Single parents of children with chronic illness: an understudied phenomenon. J Pediatr Psychol 2008 May;33(4):408-21.
(85) Klassen A, Raina P, Reineking S, Dix D, Pritchard S, O'Donnell M. Developing a literature base to understand the caregiving experience of parents of children with cancer: a systematic review of factors related to parental health and well-being. Support Care Cancer 2007 Jul;15(7):807-18.
(86) Hochschild AR. The time bind when work becomes home and home becomes work. 2nd Owl Books ed ed. New York: H. Holt; 2001.
(87) Hochschild AR, Machung A. The second shift. New York: Avon Books; 1990.
(88) Hochschild AR. The managed heart commercialization of human feeling. 20th anniversary ed., with a new afterword ed. Berkeley: University of California Press; 2003.
(89) Hochschild AR. Feeling around the world. Context 7(2), 2008.Reprinted in the Swedish sociological journal, Sociologisk Forskning.http://contexts.org/articles/spring-2008/feeling-around-the-world/ . 2008. Ref Type: Online Source
(90) Varni JW, Katz ER, Colegrove R, Jr., Dolgin M. The impact of social skills training on the
adjustment of children with newly diagnosed cancer. J Pediatr Psychol 1993 Dec;18(6):751-67.
(91) D´Zurilla t.J. NAM. Development an dpreliminary evaluation of the Social Problem-Solving Inventory. Psychological Assessment 1990;2:156-63.
(92) McNair P.M, Lorr M, Doppelman L. Profile of Mood States Manual. San Diego: Education and Industrial Testing Service; 1971.
(93) Boesen EH, Karlsen R, Christensen J, Paaschburg B, Nielsen D, Bloch IS, et al. Psychosocial group intervention for patients with primary breast cancer: A randomised trial. Eur J Cancer 2011 Jun;47(9):1363-72.
(94) Butler A.C., Chapman JE, Forman EM, Beck A. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev 2006;26(1):17-31.
(95) Grandey A A. When "the show must go on": Surface acting and deep acting as determinants of emotional exhaustion and peer-rated service delivery. Academy of Managment Journal 2003;46(1):86-96.
(96) Henderson A. Emotional labor and nursing: an under-appreciated aspect of caring work. Nurs Inq 2001 Jun;8(2):130-8.
(97) Bevans M, Castro K, Prince P, Shelburne N, Prachenko O, Loscalzo M, et al. An individualized dyadic problem-solving education intervention for patients and family
41
caregivers during allogeneic hematopoietic stem cell transplantation: a feasibility study. Cancer Nurs 2010 Mar;33(2):E24-E32.
(98) Schag, C.C, Heinrich RLGPA. Karnofsky performance status revisited: reliability,validity,and guidelines. Journal of Clinical Oncology 1984;2(3):187-93.
(99) Lansky S.B., List MA, Lansky LL, Ritter-Sterr C, Miller DR. The measurement of performance in childhood cancer patients. Cancer 198;60(7):1651-6.
(100) Martinsen. Kropp og sinn. 2. oppl ed. Bergen: Fagbokforlaget; 2005.
(101) Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry 2005 Mar;18(2):189-93.
(102) Foss C, Ellefsen B. The value of combining qualitative and quantitative approaches in nursing research by means of method triangulation. J Adv Nurs 2002 Oct;40(2):242-8.
(103) Teddlie C, Tashakkori A. Foundations of mixed methods research integrating quantitative and qualitative approaches in the social and behavioral sciences. Los Angeles: SAGE; 2009.
(104) Mays N, Pope C. Qualitative research: Observational methods in health care settings. BMJ 1995 Jul 15;311(6998):182-4.
(105) Cohen DJ, Crabtree BF. Evaluative criteria for qualitative research in health care: controversies and recommendations. Ann Fam Med 2008 Jul;6(4):331-9.
(106) Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet 2001 Aug 11;358(9280):483-8.
(107) Weber M. "Objectivity" in Social Science [1904]. In: Calhoun CJ, editor. Classical sociological theory. 2nd ed ed. Malden, MA: Blackwell Pub; 2007.
(108) Weber M. Basic Sociological Terms [1914]. In: Calhoun C, editor. Classical sociological theory.Malden, Mass: Blackwell Publishers; 2002.
(109) Hansen E.J. Danskernes levekår. Kbh.: Hans Reitzel; 1986.
(110) Olsen H. Tallenes talende tavshed.Kbh: Akademisk Forlag; 1998.
(111) Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983 Jun;67(6):361-70.
(112) Phipps S, Hinds PS, Channell S, Bell GL. Measurement of behavioral, affective, and somatic responses to pediatric bone marrow transplantation: development of the BASES scale. J Pediatr Oncol Nurs 1994 Jul;11(3):109-17.
(113) Phipps S, Dunavant M, Jayawardene D, Srivastiva DK. Assessment of health-related quality of life in acute in-patient settings: use of the BASES instrument in children undergoing bone marrow transplantation. Int J Cancer Suppl 1999;12:18-24.

42
(114) McCubbin HI, McCubbin MA, Patterson JM, Cauble AE, Wilson LR, Warwick W. CHIP-Coping Health Inventory for Parents: An Assessment of Parental Coping Patterns in the Care of the Chronically Ill Child. Journal of Marriage and Family 1983 May;45(2):359-70.
(115) Cull A., Spangers M, Bjordal K, Aaronson N, West K, Bottomley. EORTC Qualtiy Of Life Group Transplantation Procedure . [Second Edition]. 2002. ref Type: Online Source
(116) Hunt SM, Bhopal R. Self report in clinical and epidemiological studies with non-English
speakers: the challenge of language and culture . J Epidemiol Community Health 2004 Jul;(58:):618-22.
(117) Malterud K. The art and science of clinical knowledge: evidence beyond measures and numbers. Lancet 2001 Aug 4;358(9279):397-400.
(118) Larossa R. Grounded Theory Methods and Qualitative Family Research. Journal of Marriage and Family 2005;67:837-57.
(119) Chapple A, Rogers A. Explicit guidelines for qualitative research: a step in the right direction, a defence of the 'soft' option, or a form of sociological imperialism? Fam Pract 1998 Dec;15(6):556-61.
(120) Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007 Dec;19(6):349-57.
(121) Silverman D. Doing qualitative reserach. Los Angelse, London, New Delhi, Singapore, Washington DC: SAGE; 2010.
(122) Crabtree BF, Miller WL. Doing qualitative research. Newbury Park, Calif: Sage Publications; 1992.
(123) R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. 2011. Vienna, Austria. Ref Type: Online Source
(124) Waldfogel J. International policies toward parental leave and child care. Future Child
2001;11(1):98-111.
(125) Weber. The protestant ethic and the spirit of capitalism. Dover value ed ed. Mineola, NY: Dover Publications; 2003.
(126) Mays N, Pope C. Qualitative research in health care. Assessing quality in qualitative research. BMJ 2000 Jan 1;320(7226):50-2.
(127) Schuster MA, Chung PJ, Elliott MN, Garfield CF, Vestal KD, Klein DJ. Perceived effects of leave from work and the role of paid leave among parents of children with special health care needs. Am J Public Health 2009 Apr;99(4):698-705.
(128) Järvinen, Mik M. At skabe en klient. 1. udgave ed. Kbh: Hans Reitzel; 2003.
43
(129) Forinder U, Posse E, Winiarski J. Long-term psychosocial support for families of children who have undergone allogeneic stem cell transplant. Soc Work Health Care 2008;47(2):157-73.
(130) Crawford JR, Henry JD, Crombie C, Taylor EP. Normative data for the HADS from a large non-clinical sample. Br J Clin Psychol 2001 Nov;40(Pt 4):429-34.
(131) Manne S, Nereo N, DuHamel K, Ostroff J, Parsons S, Martini R, et al. Anxiety and depression in mothers of children undergoing bone marrow transplant: symptom prevalence and use of the Beck depression and Beck anxiety inventories as screening instruments. J Consult Clin Psychol 2001 Dec;69(6):1037-47.
(132) Manne S, DuHamel K, Ostroff J, Parsons S, Martini DR, Williams SE, et al. Coping and the course of mother's depressive symptoms during and after pediatric bone marrow transplantation. J Am Acad Child Adolesc Psychiatry 2003 Sep;42(9):1055-68.
(133) Nelson AE, Miles MS, Belyea MJ. Coping and support effects on mothers' stress responses to their child's hematopoietic stem cell transplantation. J Pediatr Oncol Nurs 1997 Oct;14(4):202-12.
(134) Phipps S, Dunavant M, Lensing S, Rai SN. Patterns of distress in parents of children undergoing stem cell transplantation. Pediatr Blood Cancer 2004 Sep;43(3):267-74.
(135) Larsen K. Sundhedsprofessionernes kamp - hvorfor opretholde status qou over tid? In: Petersen, Høyen, Axelsen, Callewaert, Hexis - Forum for Samfundsvidenskabelig Forskning, editors. At sætte spor på en vandring fra Aquinas til Bourdieu. 1. udgave ed. Kbh.: Hexis; 2008.
(136) Smith MK. Participant observation and informal education. www.infed.org/research/participant_observation.htm. 1997. Ref Type: Online Source
(137) Hammersley M, Atkinson P. Ethnography, principles in practice. London: Routledge;
1989.
(138) Biesheuvel CJ, Vergouwe Y, Oudega R, Hoes AW, Grobbee DE, Moons KG. Advantages of the nested case-control design in diagnostic research. BMC Med Res Methodol 2008;8:48.
(139) Hartman JM, Forsen JW, Jr., Wallace MS, Neely JG. Tutorials in clinical research: part IV: recognizing and controlling bias. Laryngoscope 2002 Jan;112(1):23-31.
(140) Barbour RS, Barbour M. Evaluating and synthesizing qualitative research: the need to develop a distinctive approach. J Eval Clin Pract 2003 May;9(2):179-86.
(141) Stige B, Malterud K, Midtgarden T. Toward an agenda for evaluation of qualitative research. Qual Health Res 2009 Oct;19(10):1504-16.
(142) Rolfe G. Validity, trustworthiness and rigour: quality and the idea of qualitative research. J Adv Nurs 2006 Feb;53(3):304-10.
44
(143) Cutcliffe JR, McKenna HP. Establishing the credibility of qualitative research findings: the plot thickens. J Adv Nurs 1999 Aug;30(2):374-80.
(144) Gannoni AF, Shute RH. Parental and child perspectives on adaptation to childhood chronic illness: a qualitative study. Clin Child Psychol Psychiatry 2010 Jan;15(1):39-53.
(145) Raina P, O'Donnell M, Rosenbaum P, Brehaut J, Walter SD, Russell D, et al. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005 Jun;115(6):e626-e636.
(146) Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol 1997 Oct;50(10):1129-36.
(147) Akobeng AK. Assessing the validity of clinical trials. J Pediatr Gastroenterol Nutr 2008 Sep;47(3):277-82.
(148) Altman DG, Bland JM. Absence of evidence is not evidence of absence. Aust Vet J 1996 Oct;74(4):311.
ORIGINAL PAPERS:
I. Larsen HB, Heilmann C, Johansen C, Adamsen L. (2011) An analysis of parental roles during haematopoietic stem cell transplantation of their offspring: a qualitative and participant observational study. Journal of Advanced Nursing. doi: 10.1111/j.1365-2648.2010.05587.x
II. Larsen HB, Heilmann C, Johansen C, Adamsen L. Socially disadvantaged parents of
children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study. Submitted.
III. Larsen HB, Adamsen L, Tolver A, Johansen C, Heilmann C. Supportive Intervention
Program Targeting Parents to Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation (HSCT): a Controlled Study. Manuscript.

ORIGINAL RESEARCH
An analysis of parental roles during haematopoietic stem cell
transplantation of their offspring: a qualitative and participant
observational study
Hanne Bækgaard Larsen, Carsten Heilmann, Christoffer Johansen & Lis Adamsen
Accepted for publication 18 December 2010
Correspondence to H.B. Larsen:
e-mail: [email protected]
HanneBækgaardLarsenMSSc(Sociology)RN
Clinical Nurse Advisor
Finsen Centret, Copenhagen University
Hospital, Denmark,
and
Faculty of Health Sciences, University of
Copenhagen, Denmark
Carsten Heilmann MD DMSc
Professor
Juliane Marie Center, Copenhagen University
Hospital, Denmark
Christoffer Johansen MD PhD DMSc
Professor and Head,
Department of Psychosocial Cancer Research,
The Institute of Cancer Epidemiology,
Copenhagen, Denmark,
and NationalCentre for Cancer Rehabilitation
Research, Southern Danish University,
Odense, Denmark
Lis Adamsen MSSc (Sociology) PhD RN
Professor
The University Hospitals Center for Nursing
and Care Research (UCSF), Copenhagen
University Hospital, Denmark
LARSEN H.B. , HEILMANN C., JOHANSEN C. & ADAMSEN L. (2011)LARSEN H.B. , HEILMANN C., JOHANSEN C. & ADAMSEN L. (2011) An anal-
ysis of parental roles during haematopoietic stem cell transplantation of their off-
spring: a qualitative and participant observational study. Journal of Advanced
Nursing 00(0), 000–000. doi: 10.1111/j.1365-2648.2010.05587.x
AbstractAim. The aim of this study was to investigate the parents’ experiences and reflec-
tions on their parental role while taking care of their child.
Background. Parents of children undergoing treatment with allogeneic haemato-
poetic stem cell transplantation for life threatening diseases in protective isolation,
experience distress related to the child’s care. Parents struggle to cope with the stress
related to the child’s disease, treatment and survival possibilities.
Methods. During the period 2007–2009, eight participant studies and 16 in-depth
interviews were performed and analysed using a theoretical ideal type construction
and an interactionistic approach.
Results. Three ideal types of approaches were identified (1) expertise-mindedness,
(2) dialogue-mindedness and (3) the approach of the socially challenged parents.
Expertise-minded parents base their rationality for care and interactions on medical
knowledge. It is important for dialogue-minded parents that emotions are included
in the rationality for care. Being able to manage these two approaches requires
emotional work in the form of both surface- and deep acting from the parents.
Socially challenged parents fail to adapt to either of the two approaches since they
often fail to manage the required emotional work.
Conclusion. The three described ideal types give a new perspective on the complex
interactions that occur between parents, child and staff during treatment with
haematopoetic stem cell transplantation. Understanding the rationality behind the
different approaches adopted by parents may assist medical staff to understand the
parents’ rationality for care of their child and to identify socially challenged parents
who need help in managing the care of their child.
Keywords: HSCT, intervention, nursing, parents, psychosocial, qualitative
� 2011 Blackwell Publishing Ltd 1
J A N JOURNAL OF ADVANCED NURSING

Introduction
Allogeneic haematopoietic stem cell transplantation (HSCT)
is a well-established potentially curative treatment for chil-
dren with malignant and non-malignant diseases. Treatment
related problems and relapse of underlying disease are major
reasons for mortality, with rates ranging from 3% to 50%
(Loberiza et al. 2003, Copelan 2006). Most deaths occur
within the first year post-transplantation (Loberiza et al.
2003). Over the last decades, therapeutic HSCT has
improved, yet there is little knowledge about the parents’
needs in their care giver role, i.e. how they experience and
manage the child’s treatment (Vrijmoet-Wiersma et al.
2009b, Packman et al. 2010).
Multiple factors influence a parent’s emotional state before
and during the child’s HSCT (Manne et al. 2004, Barrera &
Atenafu 2008, Rini et al. 2008). The way parents cope with
the child’s disease and HSCT is important since it has an
impact on the child’s coping with the disease, treatment and
later recovery. Previous studies have focused on parents’
emotional well-being from a psychological perspective
(Manne et al. 2002, Rini et al. 2004, Barrera et al. 2009).
Studies shows that the HSCT procedure is distressing for both
parents and children (Dermatis & Lesko 1990, Barrera et al.
2000, Streisand et al. 2000, Phipps et al. 2005, Jobe-Shields
et al. 2009), who must cope with disease, survival potential,
side effects and treatment complications (Manne et al. 2003,
DuHamel et al. 2004, 2007). Studies focused on the mother’s
emotional well-being gives valuable knowledge about factors
that influence mothers’ coping capacity such as home
environment, family support, personality traits and coping
strategies (Kronenberger et al. 1998, Manne et al. 2004,
Barrera & Atenafu 2008, Rini et al. 2008, Vrijmoet-Wiersma
et al. 2009a).
During the inpatient period, the child and the parents’
HSCT experience is influenced by numerous interactions
between child, parents and medical staff (Manne et al. 2003,
Vrijmoet-Wiersma et al. 2009b), however, this perspective
has not been addressed in the current research (Tremolada
et al. 2009). The objective of this study is to gain knowledge
from a qualitative, interactionistic perspective about parents’
experiences and reflections as primary caregivers on their role
in administering care during the inpatient period of a severely
ill child undergoing HSCT.
Background
Arlie Hochschild’s (2003) concept of positional and personal
control systems was used to analyse interaction between the
parents and children when carrying out medical procedures.
The positional control system is characterized by formal
rules that define the right to make decision, based on formal
attributes, e.g. age, sex and parenthood. The personal
control system is characterized by considering the parent
and child’s emotions when addressing rules. Hochschild’s
concepts of emotional management are used to analyse the
emotional work parents are required to make in their
interactions with the child and the medical staff. Emotional
management requires one to induce (surface acting) or
suppress (deep acting) feelings in order to sustain outward
countenance that coaxes an appropriate state of mind in
others. Max Weber’s (Collins 1985, Weber 2003, Breiner
2007) development of four categories of ideal types of
behaviour, i.e. goal rationale (the best and most efficient way
to achieve a specific goal), value rationale (belief in a certain
value e.g. ethical, religious), emotional rationale (based on
emotions) and traditional rationale (based on traditions)
(Collins 1985) used to highlight common features in parental
experiences and perceptions of their role during the child’s
treatment. Ideal types are theoretical constructions that give
clarity, but do not represent exact empirical reality. Both
Weber’s ideal type constructions and Hochschild’s control
systems were used to classify the parents in different ‘ideal’
types.
The study
Aim
The aim of this study was from an interactionistic perspective
and in the context of the uncertainty with respect to having a
severely ill child treated with HSCT, to explore how parents
manage emotionally and experience their caregiver role
during the child’s course of treatment in the hospital’s
isolation unit.
The hospital HSCT-unit
One centre in Denmark gives allogeneic HSCT for children.
The centre has three transplantation beds in isolated Laminar
Air Flow (LAF) filtered rooms. Annually, 16–25 children
under 18 years are treated with HSCT. Although children are
treated with HSCT for a variety of diseases, the treatment
procedure is highly standardized both nationally and inter-
nationally (Loberiza et al. 2003).
Denmark gives government-sponsored national health
insurance; consequently, all children requiring HSCT are
treated, regardless of the family’s economic and insurance
status. Furthermore, parents receive full income compensa-
tion during the treatment period.
H.B. Larsen et al.
2 � 2011 Blackwell Publishing Ltd

The child is isolated in LAF rooms with double lock
doors from 1 week prior to and 4 weeks following trans-
plantation to avoid infection. The week prior to HSCT, the
child is administered high-dose chemotherapy and in some
cases combined with Total Body Irradiation to ensure
sufficient immuno-suppression and myeloaplasia. The con-
ditioning regiment is followed by an infusion of stem cells
from a donor. At least one parent is present (remains,
sleeps and eats) in the room with the child 24 hours/day,
with brief breaks. They wear sterile attire, surgical masks
and gloves when handling the child. After the nurses’
introduction to the unit’s isolation procedures, the parents
give basic care including preparation of food, bathing,
changing of clothes/-diapers, administration of oral medi-
cines, entertainment etc. The nurses assist the parents when
needed and provide for the child’s special care such as
clinical observation, administration of I.V. fluid and med-
icine, etc.
The intervention programme included the following
components: (1) Daily medical and psychosocial support
to the parents and children; (2) An education programme
for parents; and (3) An exercise programme for parents
conducted at the unit. The interventions programme was
estimated to include nine hours of intervention per week
per family, during the child’s HSCT hospitalization of
4–6 weeks. The daily medical and psychosocial intervention
was the primary intervention. The psychosocial intervention
included daily support dialogues with the parents about the
child’s treatment with HSCT and the parents’ concerns.
The results of the intervention study will be published
elsewhere.
Design
A qualitative, descriptive and exploratory study of parents of
children undergoing allogeneic HSCT while hospitalized was
undertaken. Data were generated from the participant
observational study and the in-depth interviews of the
parents.
Sample
During the period 2007–2009, using convenient sampling
sixteen families were included in this study. At least 100 days
after the child’s HSCT, a semi-structured interview with the
primary caregiver(s) was conducted and a total of sixteen
interviews are included in this study. In addition, a daily
participant observational study during the child’s inpatient
period in isolation in LAF filtered rooms was performed
among eight of the sixteen families.
Recruitment
The sixteen families were recruited during their visit to the
hospital in relation to the child’s treatment. The families all
had children less than 18 years of age who were treated
with allogeneic HSCT and parents as primary caregivers.
All families spoke Danish to such a degree that they could
participate in a semi-structured interview and at the time of
the approach none of the families had terminally ill chil-
dren. The families were contacted by a member of the
research team (HBL) and informed about the current study
orally and by written information. After oral and written
consent arrangement for the interviews was scheduled at an
office in the hospital. The eight families who were also
informed about the daily participant observational study,
all accepted to participate. The acceptance of participating
in the observational study included having a researcher
present together with the child and their parents during the
child’s treatment period in isolation in the LAF-filtered
room.
Participants
Of the sixteen families included in this study ten couples
shared the caregiver burden (including two divorced couples);
five mothers and one father were single primary caregivers
(two were married) during the child’s admission. Data were
obtained from interviews with eleven mothers, four fathers
and one interview with both parents. The children’s mean age
was 7 years, range from 18 months to 15 years. Eleven
children were treated for malignant diseases (ten with acute
leukaemia); three with non-malignant diseases and two with
aplastic anaemia.
Data collection
Participant observational study
The participant observational study method gave insight
into how parents as primary caregivers to the child gave
meaning to their behaviours and beliefs during actions and
interactions (Bogdewic 1999). Prior to the observational
study the researcher HBL developed a scheme including the
following themes: (1) How and by whom routine child care
activities were performed; (2) The child’s medical condition
and how the family coped with these practically and emo-
tionally; (3) The family’s interaction with each other and the
staff; (4) What goal the parents tried to accomplish by their
care and interactions; and (5) What parents perceived as
major distress factors based on non-verbal and verbal
communication. Observational data were systematically
gathered daily (HBL) (30 minutes–2 hour/daily, average
90 minutes/day) from the week before HSCT to the child’s
JAN: ORIGINAL RESEARCH Analysis of parental roles during HSCT of their offspring
� 2011 Blackwell Publishing Ltd 3

discharge (average 49 days). Data collection ended when no
new perspectives were revealed and thereby data saturation
was reached.
Semi-structured interviews
The interview guidelines were developed by HBL and
explored the following themes: (1) The type of care-related
tasks performed by parents; (2) The care situations found to
be stressful during hospitalization; and (3) How parents,
children and staff co-operated and coped with these situa-
tions. The researchers held sixteen semi-structured in-depth
interviews of 25–90 minutes (mean: 50 minutes) duration
with the primary caregivers at the hospital. Two members of
the team HBL and LA performed the interviews. Data col-
lection ended when no new perspectives were revealed and
thereby data saturation was reached.
Ethical considerations
The Regional Ethical Scientific Committee approved of the
study (no: 01 206-7216) and participants signed an informed
written consent.
Data analysis
Participant observational study
When visiting the child’s isolation room daily, the researcher
noted observations related to the predefined themes. Thereby
the key findings were systematically noted during the
observation with the families and the field notes were tran-
scribed following each encounter. During the participant
observational study, it was noted that parents adopted dif-
ferent strategies when they engaged in similar care situations
with their child. This prompted the analysis, of whether
different parent types could be identified. The analysis was
performed using an interactionistical theoretic context. The
two-first ‘ideal types’ of parents ‘the expertise-minded’ and
the ‘dialogue-minded’ were identified early in the process.
The third ideal type, ‘the socially challenged’, was not as
explicitly expressed by the parents and took a longer time to
identify. In order to confirm and discuss these findings,
researchers from the team (LA, CH) participated during the
participant observation study. In the results section below,
observational data are used to illustrate situations and
interactions that were not described by the families during
the interviews.
Semi-structured interviews
Interviews were audio-recorded, transcribed verbatim,
checked for accuracy and read several times prior to data
analysis. The data were categorized according to the themes
in the interview guideline and research question. Data were
then compiled and sorted under different headings to identify
unique predominant features (Malterud 2001a, 2001b). Ini-
tial coding and theoretical analysis were conducted by one
researcher (HBL) and reviewed by other members of the
team. The ideal types of parents identified during the par-
ticipant observational study were confirmed during the
interview by the way the parents explained and expressed
their view and experience with care of the child.
Results
The parents’ approaches to manage the care of their child can
be divided into three categories: (1) expertise-mindedness, (2)
dialogue-mindedness and (3) the approach of the socially
challenged.
The expertise-minded parent
Parents for whom it is important to do everything according
to medical, nursing and the HSCT-unit’s standards are
labelled expertise-minded parents. They seek expert knowl-
edge and challenge the medical staff’s knowledge and
evaluate their answers based on their own knowledge.
Mother of a 6-year-old boy:
You need to know as much as possible about the transplant process.
I’m the type of parent who verifies everything that’s been said, done
or administered on the Internet. I need to know everything, and the
more I know the calmer I am …It’s very complicated and I have
learned an incredible amount about leukaemia, …I can enter into a
qualified discussion with the doctors
Parents know the HSCT-unit’s standards and expect the staff
to adhere to these. If they are not satisfied, these parents enter
into a dialogue with the staff and question their knowledge or
correct them.
Mother of a 13-year-old boy:
You have to keep an eye on them (the staff), to make sure that things
are always done correctly all the time...
Deviations from procedure by nurses may lead to conflicts
between staff, and parents. The parents expect their child to
co-operate with medical procedures and if the child refuses,
then try to convince the child. This, however, increases
pressure on the child, especially if physical force becomes
necessary. Parents leave little space for the child to refuse or
influence procedures, but they take time to comfort the child
if distressed as a result of these procedures.
H.B. Larsen et al.
4 � 2011 Blackwell Publishing Ltd

Mother of a 5-year-old boy:
We learned quickly to be consistent… Parents should know that it is
normal that their child may not co-operate, but that it is essential for
the child to take the pills. We have been very strict even though he
fought, kicked and screamed.
The dialogue-minded parent
Dialogue-minded parents include their emotions and expecta-
tions in their care giving. During discussions with the staff,
they seek to concentrate on procedures that consider the child’s
opinion and minimally compromise the child’s autonomy.
Mother of an 11-year-old boy:
One day I made a deal with my son. If he took one of three pills orally
then the rest could be administered intravenously. I didn’t consider
the nurses in this deal which resulted in a conflict with the nursing
and medical staff, since the procedure prescribed it should be (sic)
taken orally.
Dialogue-minded parents challenge hospital procedures by
questioning their rationale and considering whether they
make sense.
Father of an 11-year-old girl:
She was told - one thing by one nurse, and another thing by the next
nurse. For example she was promised that she would receive the
medicine intravenously but then one nurse said: ‘This is not how we
do it’ and my daughter went completely ballistic. Finally, after a very
long struggle, the doctor said she could have it intravenously.
Dialogue-minded parents try to twist procedures to suit the
child, but their interpretation of these procedures may
conflict with those of the staff. Some parents reject hospital
procedures if they find them irrational or believe them to be
emotionally damaging to their child. They are aware of the
rejecting of a procedure and are willing to take responsibility
for their actions.
Mother of a 6-year-old girl:
I was so afraid that she would break down mentally due to the
pressure by the system which wanted her to follow the rules, that I had
to make a deal with her. If she didn’t want to perform oral hygiene –
we simply skipped it and put an x on the paper, indicating that we had
done it. That way we confirmed our secret alliance against the system.
The socially challenged parent
Parents, who do not have the required physical, mental,
emotional or social capacity to take care of their child when
treated with HSCT, can be described as being socially
challenged. They were able to care for the child before
extensive medical treatment and care were required, but
when the child’s needs increased then it exceeded the parents’
capabilities. The child’s increased needs may affect minor
aspects of a parent’s caring capabilities, however, some are
affected to such degree that they become incapable of caring
for their child. As much, the parent’s resources are challenged
by the child’s increased need for care, and the child becomes a
stress factor. This increases the parent’s resource deficit, he/
she seek support from the staff, but at the same time worry
that they may consider him/her an inadequate caregiver.
Mother of a 9-year-old girl:
I’m so afraid of breaking down. I don’t think I have the strength for
it…I have no energy left – and as you can see I’m about to cry. I can’t
do this anymore, I won’t do this anymore, but I have to be here, since
there is no one else.
During the interview the mother explained that she had not
informed the staff or her family about her feelings since she
was afraid of breaking down and she said that she was
incapable of caring for her daughter:
I became impatient with my daughter… I became tougher and
corrected her more than necessary. I was so tired of being at the
hospital. I felt I had to force my daughter despite the fact that she
fought to the best of her ability. I felt, she wasn’t fighting hard
enough. She was also unhappy because she didn’t do what I had
asked. I didn’t feel good when I screamed at her, especially while she
was so ill.
Conflicts with the staff occur when parents do not follow
hospital guidelines. Contrary to the dialogue-minded parents,
the socially challenged parents do not deliberately decide to
follow or discard a particular procedure, nor do they consider
how this may influence their child’s health. The parents are
not aware that they are not following the established
procedure.
Observational study:
A father to a 3-year-old girl suffering from diarrhoea and ulcerated
buttocks changes her diaper numerous times. Each time he finishes
the procedure the girl cries and complains and he has to repeat the
procedure. Eventually he just leaves the diaper off, allows the
diarrhoea to smear on the girls buttocks, looks distressed, does not
ask for help but waits until he gathers enough energy to change the
diaper again.
Conflicts between the parents and the staff occur when the
parents cannot master the emotional strength to deal with
JAN: ORIGINAL RESEARCH Analysis of parental roles during HSCT of their offspring
� 2011 Blackwell Publishing Ltd 5

unpleasant procedures, while staff requests the parents to
adapt emotionally to the situation. For example a 7-year-old
with a nosebleed is scared and calls for his mother. Even
though the boy and nurses repeatedly ask her to be present
she refuses since she is incapable of dealing with the situation
emotionally. Conflicts between the parents and the child arise
in situations when the parents cannot give the necessary
support and comfort.
Potential conflict situations
In general parents adopt either an expertise-minded or
dialogue-minded approach to the care they give the child.
An expertise-minded parent expects their partner to adapt
the same approach to care of the child as themself and
accordingly to follow procedures. Conflicts between the
parents arise when one parent is dissatisfied with the other
parent’s level of performance. Further conflicts occur when
one parent does not hesitate to correct the other. Conflicts
with the child occur if the child is not willing to follow the
procedures.
If both parents adopt the dialogue-minded approach,
different interpretations of the best way to follow procedures
may lead to conflicts between the parents and with the child.
A mother of an 11-year-old boy:
My son has a very contrary personality and tends to become
hysterical. He makes a big deal out of everything. We would have
conflicts if he didn’t want to shower or he would change the order of
the actions. In these situations my husband became angry and I tried
to be very caring.
The child is used to negotiate deals but during HSCT the
child experiences non-negotiable procedures, such as taking
medicine. In this study we found that when one parent
adopted an expertise- or dialogue-minded approach and the
other parent adopted a socially challenged approach, then
this latter parent took limited or no responsibility for the care
and was seldom present at the hospital.
Mother of an 11-year-old boy:
I didn’t see the boy’s father much when we were at the hospital. He
showed up twice and once drunk. So I could not count on him for
anything.
Surface and deep acting
For parents to be able to adopt either an expertise- or dialogue
minded approach to the care of their child, it is required that
they are able to perform emotional management as described
by Hochschild. The emotional management can either be as
surface acting or deep acting. In surface acting the parents do
not display their real emotions e.g. show a happy face even
though they are sad, and thus disregarding their own emotions
for the sake of the child.
In deep acting is when parents alter their feelings e.g.
suppressing anger and transform it to sympathy due to the
child’s difficult situation.
A father to a 13-year-old boy describes how he attempts deep acting
but ends up performing surface acting towards his son:
When he was under pressure, he became aggressive…He was very
outspoken and I could handle it because I was able to put two and
two together. Deep down I knew he didn’t mean the terrible names he
called me and afterwards he was sad because he could remember the
things he called me. Although I pretended not to be bothered, it was
hard.
In the previous example, where the mother is requested to be
present in the room during her son’s nosebleed is an example
of a request to engage in surface acting for the sake of her
child, but a request the mother is not able to comply.
The care for a severely ill child requires the parents to
engage in emotion management in numerous situations.
Expertise-minded parents engage in deep acting towards their
child when the child is not willing to co-operate with medical
procedures. Thereby the parents’ suppress their emotions in
order to sustain their goal of caring according to the hospitals
procedures. Dialogue-minded parents engage in surface
acting, when their child is not willing to co-operate with
medical procedures and when they are not able to adapt a
hospital procedure into their own and the child’s emotions.
The socially challenged parents find it difficult to engage in
either surface- or deep acting when the child is not willing to
co-operate with the hospitals procedures and as a result are
not able to support the child emotionally, as the nosebleed
example illustrates.
Discussion
The majority of parents in this study opted to be present as
couples and to be equally active in caring for their child
during hospitalization. Future research should include the
male perspective of a hospitalized child, an aspect that is
underplayed in recent research.
In this study, there is a striking resemblance between
Hochschild’s positional control system and the expertise-
minded parents and the personal control system and the
dialogue-minded parents, in how they manage care situa-
tions. Weber’s categories of ‘ideal’ types may explain why the
H.B. Larsen et al.
6 � 2011 Blackwell Publishing Ltd

expertise-minded parents seem to adopt goal-rational action
types and the dialogue-minded parents adopt value-rationale
action types, while the socially challenged parents base their
actions on emotional-rationale, a rationale described by
Weber as an action without rationale. We were not able to
identify Weber’s fourth ideal type (traditional rationale),
among the participating parents. One explanation might be
that the care procedures were highly specialized due to the
isolation requirements and as such the care routines adopted
by the parents prior to the child’s disease, had been
abandoned.
Treatment with HSCT imposes rules and procedures on the
family. Expertise-minded parents accept rules based on
formal attributes, e.g. the hospital system represented by
the staff. If a procedure is not properly followed, they
sanction the staff’s behaviour. In this way expertise-minded
parents help the hospital system to maintain its procedures.
Overall, dialogue-minded parents accept hospital procedures,
the rationale behind them, and the fact that the procedures
are based on formal attributes. However, they do not accept
that emotions and requests are ignored, when they question a
rule or a procedure. Socially challenged parents’ difficulties in
coping with hospital procedures, can further affect their sense
of incompetence and is linked to increased levels of distress as
shown by Oppenheim et al. (2002), Vrijmoet-Wiersma et al.
(2009a), Jobe-Shields et al. (2009). Heightened levels of
stress in parents are linked to factors such as: the child’s
prognosis, health status and coping with the HSCT proce-
dure, and their own emotions, level of coping and resources
(Kronenberger et al. 1998, Streisand et al. 2000, Manne
et al. 2003, Moore & Rauch 2006, DuHamel et al. 2007,
Rini et al. 2008, Packman et al. 2010), i.e. conditions that
were also applicable and influenced the parents in this study.
To give care for the child during stressful situations, parents
must engage surface and deep acting. The three types of
parents engage differently in the emotional management of
Hochschild’s surface- and deep acting. The expertise-minded
parent’s rationale is based on the positional control system; he/
she uses gained medical knowledge and understanding of
formal rules to grasp emotional control. By doing so,
expertise-minded parents are able to perform the emotional
management required to engage in both deep acting (i.e.
suppressing their own and the child’s feelings), and surface
acting (i.e. not losing their temper if procedures are not carried
out correctly). If the procedures are followed correctly it
diminishes the parents’ insecurities and fear. The dialogue-
minded parent’s rationale is based on personal control and it is
important that emotions are taken into consideration during
decision-making in order to gain emotional control.
This forces dialogue-minded parents to engage in situations
requiring surface acting as they often find themselves in
situations where emotions are overruled by the hospital’s
procedures. When emotions are not considered, this type of
parent risks losing emotional control. Similar to the dialogue-
minded parent, the socially challenged parent considers his/her
own and the child’s emotions and tries to incorporate their
desires into hospital procedures. They are overwhelmed by
emotion, rendering them incapable of transforming their
wishes into rational actions. Socially challenged parents may
be characterized by an impaired ability to perform requested
emotional management in the form of surface and deep acting,
which is necessary during their child’s HSCT. This leaves them
feeling powerless which is in line with Oppenheim et al.’s
(2002) study that described the parents feelings of helplessness
or by Jobe-Shields et al.’s (2009) study that shows that parents
with elevated levels of depressive symptoms are the ones who
have most difficulties dealing with the child’s emotional
reactions. The socially challenged parents are afraid to display
their powerlessness to hospital staff because they fear losing
any remaining emotional control or fear that the hospital
system might question their parental abilities.
In clinical practice the parents’ different approaches may
provide the staff with a better understanding of which care
situations parents find difficult, the type of knowledge they
are seeking, facilitate better communication and reduce the
parents’ stress. Since open communication within the family
facilitates the child’s adjustment to the HSCT procedure
(Jobe-Shields et al. 2009), open communication between the
staff and family would facilitate the parents’ adjustment to
the child’s treatment.
The socially challenged parents show most difficulties in
relating to the care. Being in a position to identify that type of
parents would allow the staff to secure appropriate resources,
allow the parents to receive support in coping with the strain
of their child’s care and allow the child to better cope with
the distressing experience of HSCT.
Methodological reflections and study limitations
The combination of the two methods aims to compensate for
bias that presents itself during participant observation or
dialogue. However, a combination of the two methods also
reveals that parents’ actions and statements about their
actions are not always coherent. In this case, members of the
research team interacted with the families and the most
predominant feature formed the basis for the classification
into ideal types. The use of ideal types was chosen with the
intent to give clarity of predominant common features that
parents displayed while caring for the children. However,
ideal types are theoretical constructions and thereby
JAN: ORIGINAL RESEARCH Analysis of parental roles during HSCT of their offspring
� 2011 Blackwell Publishing Ltd 7

categorical and not intended to embrace the complexity of
everyday life (Weber 2003). The parents in this study were all
experienced primary caregivers. They represent a unique
group of parents that possess a long comprehensive experi-
ence of functioning within the hospital setting. The parents’
experience increased their validity in answering the questions
asked in this study.
On one hand the researcher’s familiarity with HSCT
procedures could have induced a bias of having a pre-
understanding of the parents’ social context. On the other
hand, it was an advantage to understand the social context in
which the parents found themselves. The researcher did not
participate in the care of the child in order to avoid ‘going
native’ with the staff or the parents. The parents who
participated in this study participated in an ongoing inter-
vention programme and it could have influenced their actions
in some care situations. However, the participant observation
study duration (90 minutes per day, for 49 days) allowed the
parents to be observed in numerous situations and interac-
tions with the child and the staff.
The patterns formed by the participant observation study
and the interviews were analysed from a theoretical perspec-
tive influenced by Weber’s ideal type construction, and gave a
new understanding of the different approaches adopted by
the parents. Hochschild’s interactionistic perspective high-
lighted important features of the parents’ coping mechanisms
in distressing care situations. This analysis may be applied to
other HSCT settings or care situations where parents and
children are hospitalized for longer periods.
Conclusion
Being able to identify what type of approach-to-care the
parents of children treated with HSCT adopt may help
medical staffs improve interaction and communication and
thereby reduce the parents’ stress. It can assist medical staff in
identifying the socially challenged parents who are most in
need of psychosocial intervention.
The majority of parents in this study form couples equally
involved in the child’s care, which highlights the importance
of including a shared caregiver perspective. This study has
highlighted the importance of analysing parents’ actions and
the implications they have on providing care for their child.
However, there is still a need for further research of the
complex emotional and practical interactions that parents
and children face during the HSCT procedure.
Funding
Danish Cancer Foundation for Children, Danish Health
Foundation, Lundbeck Foundation, Gangsted foundation,
Righospitalet, Copenhagen University Hospital supported
this study.
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
HBL, CH, CJ and LA were responsible for the study concep-
tion and design. HBL and LA performed the data collection.
HBL, CH and LA performed the data analysis. HBL, CJ and
LA were responsible for the drafting of the manuscript. HBL,
CH, CJ and LA made critical revisions to the paper for
important intellectual content. HBL and LA obtained funding.
HBL and LA provided administrative, technical or material
support. HBL and LA supervised the study.
What is already known about this topic
• Parents of children undergoing treatment with
allogeneic hematopoietic stem cell transplantation
(HSCT) for life threatening diseases in protective
isolation, experience distress related to the child’s care.
• Multiple factors influence parents’ emotional state
during the child’s inpatient period, and the way they
cope has an impact on the child’s coping with the
disease, treatment and HSCT.
What this paper adds
• This study has identified three distinct ‘ideal’ types of
parental engagement in the care of a severely ill child:
the expertise-minded, the dialogue-minded and the
socially challenged approach.
• In clinical practice the three different types of parents’
approach to care impact how parents relate to the care
of the child, to the medical staff and to hospital
procedures.
Implications for practice and/or policy
• Understanding the rationality behind the different
approaches adopted by parents may help medical staff
to understand the parents’ rationality for care of their
child.
• Understanding the three types of parents may help staff
to identify socially challenged parents who need help in
managing the care of their child.
H.B. Larsen et al.
8 � 2011 Blackwell Publishing Ltd
References
Barrera M. & Atenafu E. (2008) Cognitive, educational, psychosocial
adjustment and quality of life of children who survive hemato-
poietic SCT and their siblings. Bone Marrow Transplantation 42,
15–21.
Barrera M., Pringle L.B., Sumbler K. & Saunders F. (2000) Quality of
life and behavioural adjustment after pediatric bone marrow
transplantation. Bone Marrow Transplantation 26, 427–435.
Barrera M., Atenafu E. & Hancock K. (2009) Longitudinal health-
related quality of life outcomes and related factors after pediatric
SCT. Bone Marrow Transplantation 44(4), 249–256.
Bogdewic S.P. (1999) Participant observation. In Doing Qualitative
Research, 2nd edn (Crabtree B.F. & Miller W.L., eds), Sage Pub-
lication, Thousand Oaks, CA, pp. 37–70.
Breiner P. (2007) Ideal-types as ‘Utopias’ and impartial political
clarification: Weber and Mannheim on Sociological Prudence. In
Max Weber’s ‘‘Objectivity’’ Reconsidered (McFalls L.H. ed.),
University of Toronto Press, Toronto, pp. 89–116.
Collins R. (1985) Max Weber: A Skeleton Key. Sage Publications,
Newbury Park, CA.
Copelan E. (2006) Hematopoietic stem cell transplantation. New
England Journal of Medicine 354, 17.
Dermatis H. & Lesko L. (1990) Psychological distress in parents
consenting to child¢s bone marrow transplant. Bone Marrow
Transplantation 6, 411–417.
DuHamel K.N., Manne S., Nereo N., Ostroff J., Martini R., Parsons
S., Williams S., Mee L., Sexson S., Wu L., Winkel G., Boulad F. &
Redd W.H. (2004) Cognitive processing among mothers of chil-
dren undergoing bone marrow/stem cell transplantation. Psycho-
somatic Medicine 66, 92–103.
DuHamel K.N., Rini C., Austin J., Ostroff J., Parsons S., Martini R.,
Williams S., Mee L., Sexson S., Winkel G., Boulad F. & Redd
W.H. (2007) Optimism and life events as predictors of fear
appraisals in mothers of children undergoing hematopoietic stem
cell transplantation. Psycho-Oncology 16, 821–833.
Hochschild A.R. (2003) The Managed Heart. University of Califor-
nia Press, Berkeley & Los Angeles, CA.
Jobe-Shields L., Alderfer M.A., Barrera M., Vannatta K., Currier
J.M. & Phipps S. (2009) Parental depression and family environ-
ment predict distress in children before stem sell transplantation.
Journal of Developmental and Behavioral Pediatrics 30(2), 140–
146.
Kronenberger W.G., Carter B.D., Edwards J., Morrow C., Stewart J.
& Sender L. (1998) Psychosocial adjustment of mothers of children
undergoing bone marrow transplantation: the role of stress, coping
and family factors. Children¢s Health Care 27(2), 77–95.
Loberiza F.R. Jr, Serna D.S., Horowitz M.M. & Rizzo J.D. (2003)
Transplant center characteristics and clinical outcomes after
hematopoietic stem cell transplantation: what do we know. Bone
Marrow Transplantation 31, 417–421.
Malterud K. (2001a) The art and sciences of clinical knowledge:
evidence beyond measures and numbers. The Lancet 358, 397–
400.
Malterud K. (2001b) Qualitative research: standards, challenges, and
guidelines. The Lancet 358, 483–488.
Manne S., DuHamel K., Nereo N., Ostroff J., Parsons S., Martini R.,
Williams S., Mee L., Sexson S., Wu L., Difede J. & Redd W.H.
(2002) Predictors of PTSD in mothers of children undergoing bone
marrow transplantation: the role of cognitive and social processes.
Journal of Pediatric Psychology 27(7), 607–617.
Manne S., DuHamel K., Winkel G., Ostroff J., Parsons S., Martini
R., Williams S.E., Mee L., Austin J. & Redd W.H. (2003) Brief
Reports: percieved partner critical and avoidant behaviors as pre-
dictors of anxiety and depressive symptoms among mothers of
children undergoing hemopaietic stem cell transplantation. Journal
of Consulting and Clinical Psychology 71(6), 1076–1083.
Manne S., DuHamel K., Ostroff J., Parsons S., Martini R., Williams
S.E., Mee L., Sexson S., Austin J., Difede J., Rini C. & Redd W.H.
(2004) Anxiety, depressive and posttraumatic stress disorder
among mothers of pediatric survivors of hematopoitic stem cell
transplantation. Pediatrics 113, 1700–1708.
Moore C.W. & Rauch P.K. (2006) Addressing parenting concerns of
bone marrow transplant patients: opening and closing Pandora’s
box. Bone Marrow Transplantation 38(12), 775–782.
Oppenheim D., Valteau-Couanet D., Vasselon S. & Hartmann O.
(2002) How do parents perceive high-done chemotherapy and
autologous stem cell transplantation for their children. Bone
Marrow Transplantation 30(1), 35–39.
Packman W., Weber S., Wallance J. & Bugescu N. (2010) Psycho-
logical effects of hematopoietic SCT on pediatric patients, siblings
and parents: a review. Bone Marrow Transplantation 45(1), 1–13.
Phipps S., Duvant M., Lensing S. & Rai N. (2005) Psychosocial
predictors of distress in parents of children undergoing stem cell or
bone marrow transplantation. Journal of Pediatric Psychology
30(2), 139–153.
Rini C., DuHamel K.N., Austin J., Ostroff J., Boulad F., Parsons
S.K., Martini R., Williams S.E., Mee L., Sexson S. & Redd W.
(2004) Mothers¢ perception of benefit following pediatric stem cell
transplantation: a longitudinal investigation of the role of opti-
mism, medical risk, and sociodemographic resources. Annual of
Behavioural Medicine 28(2), 132–141.
Rini C., Manne S., DuHamel K., Austin J., Ostoff J., Boulad F.,
Parsons S.K., Martini R., Williams S.E., Mee L., Sexson S. &
Redd W.H. (2008) Social support from family and friends as a
buffer of low spousal support among mothers of critically ill
children: a multilevel modeling approach. Health Psychology
27(5), 593–603.
Streisand R., Rodrigue J.R., Houck C., Graham-Pole J. & Berlant N.
(2000) Brief Report: Parents of Children Undergoing Bone Marrow
Transplantation: Documenting Stress and Piloting a Psychological
Intervention Program. Journal of Pediatric Psychology 25(5), 331–
337.
Tremolada M., Bonichini S., Pillon M., Messina C. & Carli M.
(2009) Quality of life and psychosocial sequelae in children
undergoing hematopoietic stem-cell transplantation: a review.
Pediatric Transplantation 13(8), 955–970.
Vrijmoet-Wiersma C.M.J., Kolk A.M., Grootenhuis M.A., Sprek
E.M., van Klink J.M.M., Egeler R.M., Bredius R.G.M. & Koop-
man H.M. (2009a) Child and parental adaption to pediatric stem
cell transplantation. Supportive Care in Cancer 17(6), 707–714.
Vrijmoet-Wiersma C.M.J., Egeler R.M., Koopman H.M., Norberg
A.L. & Grootenhuis M.A. (2009b) Parental stress before, during,
and after pediatric stem cell transplantation: a review article.
Supportive Care in Cancer 17(12), 1435–1443.
Weber M. (2003) The Protestant Ethic and the Spirit of Capitalism.
Dover Publications Inc., New York, USA.
JAN: ORIGINAL RESEARCH Analysis of parental roles during HSCT of their offspring
� 2011 Blackwell Publishing Ltd 9

The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal and with an Impact Factor of 1Æ518 – ranked 9th of 70 in the 2010
Thomson Reuters Journal Citation Report (Social Science – Nursing). JAN has been in the top ten every year for a decade.
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 7,000 libraries
worldwide (including over 4,000 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Early View: rapid online publication (with doi for referencing) for accepted articles in final form, and fully citable.
• Faster print publication than most competitor journals: as quickly as four months after acceptance, rarely longer than seven months.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
H.B. Larsen et al.
10 � 2011 Blackwell Publishing Ltd
1
PAPER II Socially disadvantaged parents of children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study, Denmark. Authors: Hanne Bækgaard Larsen, Carsten Heilmann, Christoffer Johansen, Lis Adamsen Institutions Hanne Bækgaard Larsen, RN, MSc.Soc. Copenhagen University Hospital, Finsen Centret, Copenhagen, Denmark Copenhagen University Hospital, Juliane Marie Center, Copenhagen, Denmark Copenhagen University Hospital, The University Hospitals Center for Nursing and Care Research (UCSF), Copenhagen, Denmark University of Copenhagen, Faculty of Health Sciences, Copenhagen, Denmark Professor Carsten Heilmann, MD, DMSc Copenhagen University Hospital, Juliane Marie Center, unit 4072 Blegdamsvej 9 2100 Copenhagen, Denmark e-mail: [email protected] Professor Christoffer Johansen MD, PhD, DMSc Head, Department of Psychosocial Cancer Research The Institute of Cancer Epidemiology, Strandboulevarden 49 2100 Copenhagen, Denmark e-mail: [email protected] National Centre for Cancer Rehabilitation Research Institute of Public Health Southern Danish University, Odense, Denmark Professor Lis Adamsen, RN, MSc.Soc., PhD Copenhagen University Hospital, The University Hospitals Center for Nursing and Care Research (UCSF), department 7331 Institute of Public Health, University of Copenhagen, Faculty of Health Sciences, Copenhagen Blegdamsvej 9 2100 Copenhagen, Denmark e-mail: [email protected] Corresponding Author: Hanne Bækgaard Larsen, RN, MSc.Soc. The University Hospitals Centre for Nursing and Care Research
2
Copenhagen University Hospital, Department 7331 DK-2100 Copenhagen, Denmark Telephone: +45 3545 7336 Telefax: +45 3545 7399 Email: [email protected] Running header: Socially disadvantaged parents of children treated with allogeneic HSCT.

3
Abstract Purpose: This study, inspired by cognitive therapy, was undertaken to test and develop a daily psychosocial intervention program performed by a case manager nurse (CMN), to support parents during the distressful experience of their child’s Allogeneic Haematopoietic Stem Cell Transplantation (HSCT). Methods: An explorative qualitative analysis of a psychosocial intervention program for parents whose child is under HSCT treatment while hospitalized. Parents to 25 children were included in this study and 21 of these completed a semi-structured interview 100 days following HSCT. Results: Three main problems faced by all parents included 1) the emotional strain of the child’s HSCT; 2) re-organizing of the family’s daily life to include hospitalization with the child; and 3) the financial strain of manoeuvring within the Danish welfare system. The CMN performed daily interventions rounds to ease each of these problems during the study period. Having the following pre-existing risk factors, negatively influenced the parents´ ability to address these problems: 1) being a single parents; 2) low-level income; 3) low-level education; 4) low-level network support: 5) being a student or unemployed; 6) physical/psychiatric illness; and 7) ethnicity. Six families with 4 or more risk factors had complex emotional, social and financial problems that required extensive intervention by the CMN and that impacted their ability to provide care for the child. Conclusion: The parents’ pre-existing risk factors were further complicated by their children’s HSCT. A recommendation for clinical practice is to identify families with multiple interrelated problems and allocate most resources to support these families. Keywords: Nurses, HSCT, Parents, Psychosocial, Intervention, Qualitative.
4
INTRODUCTION Health services in Denmark, including allogeneic Haematopoietic Stem Cell Transplantation (HSCT), is provided free-of-charge (www.denmark.dk). HSCT is a well-established, potentially curative treatment for children with malignant and non-malignant diseases (Loberiza et al., 2003; Copelan 2006). Although there is increased therapeutic success with HSCT, it is an intensive and potentially lethal medical treatment. To ensure sufficient immuno-suppression and myeloaplasia, the child receives conditioning (high-dose chemotherapy/ total body irradiation) one week prior to HSCT, followed by an infusion of stem cells from a donor. To avoid infection, the child is isolated in a laminar air filtered room from the time of conditioning to approximately 4 weeks post-HSCT. To care for the child, at least one parent remains in the room with the child around the clock. Since both parents work outside of the home in more than 95% of Danish families (www.denstoredanske.dk), they receive full income compensation from the social welfare authorities during their child’s HSCT. The child’s HSCT and consequent increased dependency on the parents poses a substantial strain on emotional well-being and family function and at a time when both parties faces uncertain futures (Lesko 1994; Clarke et al., 2008; Manne et al., 2002). How parents manage the challenge is important since it affects the child’s adjustment to HSCT while the way in which the child manages the HSCT also impacts the parents’ level of distress (Lesko 1994; Phipps et al., 2002a, 2002b; Vrijmoet-Wiersma et al., 2009b). Thus, psychosocial adjustment to HSCT and recovery has become a growing concern and the literature indicates a need for supportive interventions for these families (Vrijmoet-Wiersma et al., 2009a; Tremolada et al., 2009; Jobe-Shields et al., 2009). Intervention programs to ease the child’s emotional reactions include art therapy (Günter 2000), play therapy (Kuntz et al., 1996), complementary health promotion (Phipps 2002c) and support group activities (Sherman et al., 2004). Intervention programs supporting the parents´ well-being include psychotherapeutic interventions (Lesko 1994) and parents giving massage therapy to their child (Phipps 2002c). Phipps et al.´s (2010) randomised complementary (humor therapy/massage / relaxation /imagery) intervention study, that included 178 children undergoing HSCT and their parents, is the most comprehensive study to date. However, no differences were found between the groups in this study. No single therapy to date has proven the most beneficial, however, these intervention studies call for further studies and research within these families, and the most promising results included cognitive behavioural therapy (Sherman et al., 2004; Tremolada et al., 2009; Packman et al., 2010). The current psychosocial intervention study was developed to allow a Case Manager Nurse (CMN) to provided daily support to parents with a child undergoing HSCT. Theoretically, the Roy Adaptation Model inspired the intervention study design and especially the notion that a person/family is a bio-psycho-social being in constant interaction with a changing environment; and emphasis of the relationship between stimuli, coping mechanisms and adaptation (Roy & Roberts 1981). Cognitive behavioural therapy inspired the CMN´s daily emotional support targeting the parents (Beck 1979; Beck at al., 1985; Beck 2005). The current intervention study primarily included daily psychosocial support by the CMN and in addition, the parents were offered the option to participate in five one-hours educational and weekly exercise sessions.

5
The aim of this paper is to explore the predominant problems faced by parents of children treated with HSCT during the child’s hospitalisation and to explore how these problems affect the parents’ daily life. A second aim is to illustrate the required intervention by the CMN in assisting the parents. METHODS Design An explorative qualitative analysis of 25 parents to hospitalised children treated with allogeneic HSCT through a psychosocial intervention study. Participants During the period from November 2007 to July 2009, using convenience sampling, all parents to children aged 0 – 19.9 years scheduled for allogeneic HSCT was approached during the child’s initial health examination. In total, 31 children were scheduled for a transplant, however six children were excluded from the study since they did not meet the inclusion criteria (three children did not have a resident parent as caregiver, one family did not speak Danish and two children were excluded for medical reasons). Sample The remaining 25 families consented to participate in the psychosocial intervention program and 21 of them participated in the semi-structured interviews 100 days following the child’s HSCT. Four families were excluded from the semi-structured interview since their children were transferred to a referral hospital for terminal treatment and two families lost their respective children prior to day 100. The main characteristics of the population under study are shown in Table 1. The majority of the children were treated for malignant diseases. Data collection Prior to the child’s HSCT, each of the 25 families provided information about their child’s disease and the families psychosocial functioning. The semi-structured interview guidelines were developed by the authors and explored the parents´ perception of issues related to the child’s HSCT: 1) specific major problems, 2) impact on their physical, financial and psychosocial situation, and 3) support needed to enable them to provide care for their child. Two members of the team (HBL and LA) performed the 21 in-depth interviews of 25 - 90 minutes (mean 50 minutes) duration, at the hospital. Data collection ended when no new perspectives were revealed and thereby data saturation was reached. Intervention program The intervention was estimated to be nine hours weekly per family during the child’s HSCT hospitalisation, over 4-6 weeks. Daily psychosocial support was the primary intervention component. A Case Manager Nurse (CMN) (HBL) provided support to the parents. This CMN had extensive experience with HSCT nursing care and an education in social science. The function included daily rounds with the parents and the child in the child’s isolation room, and which allowed thus building and continuity in addressing the family’s specific problems and changes in the child’s medical condition. The CMN did not participate in the child’s daily care and was not a regular staff member in the HSCT-unit. The intervention focused primarily on the following aspects of the parents’ situation.
6
A. Care tasks assigned to the parents related to the child’s medical condition e.g. nausea, vomiting, appetite loss, skin problems, and the child’s emotional reaction. B. Daily emotional support focused on the parents’ thoughts and concerns (e.g. frustration, distress and anxiety). Special attention was given to schemata of unrealistic negative thoughts (e.g. unrealistic fear of the child’s death) and assessment of own and the child’s well-being. C. The parents’ social and organizational situations e.g. social network support and unresolved financial situation. Assistance was provided to address these problems directly or through the Danish social welfare authorities. The intervention also offered educational sessions for parents (one hour of education per week for five weeks) on topics such as: family changes, children’s reactions, and conflict management. Exercise sessions for parents (three hours per week) were also offered. Data analysis Interviews were audio-recorded, transcribed verbatim, checked for accuracy and read several times prior to data analysis. The data were categorized according to the themes in the interview guidelines and the research aim of this paper. Data were compiled and sorted under different headings to identify unique predominant features (Malterud 2001a, 2001b). Initial coding and theoretical analysis were conducted by one researcher (HBL) and reviewed by other team members. The data were categorized using content analysis, and in accordance with the research questions. To understand the predominant features that surfaced in the analysis, each pattern was analysed separately. Inspired by the Roy Adaptation Model the three most predominant problem areas were analysed in the context of how parents dealt with them. In order to explore the complexity of the problems inspired by the theory of social marginalization (Walker & Walker 1997, Backett-Milburn et al., 2003; Attree, 2006; Davies et al., 2008), the semi-structured data were analysed for interrelatedness with the described problem areas and risk factors that influenced the parents’ problem-solving capacity. Figure 1 illustrates the analysis model. The risk factors formed a pattern that correlated with the time spent during the interventions to assist the parents with the three major problem areas. The parents´ care- giver problems that derived from their respective financial and psychosocial situation were confirmed during the interview when they expressed their view on care of their child. The three predominant themes that emerged were related to the parents’ emotional well-being, their need to reorganize family daily life and their interaction with the social welfare authorities. Three themes are presented in the results below. Ethical considerations The Regional Ethical Scientific Committee approved the study (File no: 01 206-7216) and participants provided informed oral and written consent. RESULTS The results are divided in to two parts: Part I. The three predominant problems identified by the 21 parents during the semi-structured interviews 100 days following the child’s HSCT. During the interviews three predominant themes emerged:
7
1. Diagnosis and subsequent HSCT lead to emotional chaos for parents For some of the families, the time-span from the child’s diagnosis with a life threatening disease to subsequent treatment with HSCT was only a few months. These parents described their emotional state as being: “chocked, sad, confused, overwhelmed, and angry”. “I am so sad, angry and frustrated, that I cannot stand being at the hospital. Every time I see my son I want to take him home and let him die peacefully. I blame my husband for putting him through HSCT and I take my anger out on him”. Other families developed an emotional strategy that they used throughout the HSCT course. “The cancer diagnosis was a chock and the first time was hideous, we were like zombies, but then we decided… our family project is to manage the treatment, to beat the child’s cancer, and to become stronger as a family”. Some families, however, had to develop new emotional strategies. “Prior to the HSCT I felt in control, but suddenly my daughter’s life depended on an unrelated donor, and I panicked… It has been very hard for me to trust a stranger to save my daughter”. Some parents were dissatisfied with how they managed the emotional strain of the child’s HSCT and expressed the impact of it on their ability to care for the child: “I became impatient with my daughter… I became tougher and corrected her more than necessary”. CMN interventions to assist parents in dealing with the emotional strain of the child’s HSCT
• Evaluation of care related tasks performed by the parents (bathing, skin care, administration of food and oral medicine).
• Training and evaluation of the parents in behavioural interventions e.g: contingency management, cognitive/attentional distraction, systematic desensitisation, modelling, and behavioural rehearsal.
• Addressing the parents’ negative thoughts patterns (depression, self-esteem) and emotional reactions (distress, anxiety), including containing the parents’ emotions. Defence mechanisms were not addressed if they did not impact care of the child.
• Referring parents and children to psychological/psychiatric treatment if needed. 2. HSCT leads to disintegration and organisational chaos in the family The parent presence during the child’s HSCT needed to reorganize daily life. Parents relied heavily on support from their social network. A common solution was to rely on the child’s grandparents for assistance. “My parents moved into our house to take care of our two other children so they can continue to go to school while we are here”

8
In some families the grandparents also assisted by taking care of the hospitalized child. “My mother stays with me at the hospital and we take turns caring for my daughter. My father stays at my home and takes care of the two other children…I would not know how to manage if they were not here for me”. In the case of families with a limited social network, re-organizing family life became more complicated. A divorced immigrant mother explains: “My family does not living in the country and my ex- husband has no contact with his family; so we have no-one to help us. My ex-husband stays at the hospital with our daughter and I stay at home with our healthy daughter… I would like to be present and involved in my daughter’s care, though” The daily life reorganization factor for the families occurred mainly prior to the HSCT, however this re-organization was not always sustainable for the duration of the transplant period, which resulted in the need for further rearrangements. “I caught a cold during my son’s HSCT and was not allowed in the unit. So I made a 911 call to a friend and asked him to drop everything and take care of my son at the hospital”. “I needed acute surgery during my daughter’s HSCT. However, I did not want to worry or leave my daughter, so the CMN organized the surgery here at this hospital, while my mother took care of my daughter” CMN interventions to assist parents in the re-organizing the family’s daily life during the child’s HSCT
• Assessment of whether the re-organization of daily family life was sustainable for the entirety of the child’s HSCT, and if not, to assist the parents in identifying long-term solutions.
• Identifying alternative re-organisation solutions when unexpected changes occurred. • Assisting parents with a limited social network to connect with the Danish social welfare
authorities, so that help could be provided either at the hospital or at home following hospital discharge.
3. Diagnosis and subsequent HSCT leads to financial chaos within the family Problems related to the parents’ financial situation became evident as they spoke of their contact with the social welfare authorities. One or both parents had to leave the work force due to their child’s HSCT and their prior income was subsidised by the social welfare authorities. More than half of the parents described facing financial difficulties because of the rigidity of the social system: e.g. disagreement in calculation of the compensation, and delay in receiving the income compensation. ” The income compensation has not yet been granted even though we applied for it five months ago”. “Our income compensation has not been calculated correctly so we have filed several complaints. We have several ring binders at home.... It is time consuming to write the letters, read the law and
9
to deal with the bills we cannot pay, this is time that is taken away from us being with the child and his siblings. The process has been going on for two years and now the bank threatens to put a foreclosure on our house.” Immigrant families also faced problems understanding the social law. One of the fathers explains: “As I do not speak and read the language well, it is difficult to read the law, understand letters from the social welfare authorities and to explain our situation” These parents allocate time and energy in their struggle to control the family’s financial situation. In particular families, financial struggle seemed overwhelming: “My son has been ill for several years and my income compensation is very low. I cannot change it and I cannot continue to live on nothing, so now I borrow money to pay the bills”. “We are newly divorced and have no money, I live in a flat where there are cockroaches and I share a bed with my two daughters. My ex-husband has no place to live and sleeps on a friend’s couch.” CMN intervention to assist parents in solving their financial constraints during the child’s HSCT
• Identifying parents with financial difficulties. If the financial difficulties affected the treatment and recovery of the child, then assist the parents in understanding their options within the social law.
• Communication with the social welfare authorities for additional financial support, e.g. making phone calls, filing applications, arranging and attending meetings with the social welfare authorities.
• Writing grant applications for additional financial supports, toys, and vacations packages following the child’s recovery.
All 21 families who participated in the semi-structured interviews faced the above-mentioned problems. All of the families experienced emotional strain related to their child’s HSCT, had their income subsidised by the social welfare authorities; and faced substantial reorganization in their daily life. The parent’s ability to find useful strategies depended on their personal resources as well as on resources within their social networks. In some families the complexity of the three problems areas affected their ability to find sustainable solutions, resulting in a prolonged chaotic atmosphere. Part II. Risk factors identified prior to the child’s HSCT and faced by the 25 parents influenced their ability to care for their child during HSCT A major characteristic of the families most in need of CMN assistance was the parents’ position within society. The theory of social marginalization specifies at least three risk factors as important: minimal social relationships, limited participation in political activity, limited participation in leisure activities, poor physical or mental health and being poor (Larsen 2004). This inspired the analysis of what risk factors parents possessed prior to the child’s HSCT and how they manage the three predominant problem areas imposed by their child’s HSCT.

10
The following seven risk factors were identified as affecting the parents´ ability to provide care: 1) having a psychiatric or physical diagnosis that affects daily functioning, 2) low level of support from their social networks, 3) being a single parent, 4) low-level of income, 5) low-level of education, 6) being unemployed or a student, and 7) other ethnicity than Danish. Having a psychiatric history combined with the emotional strain of their child’s HSCT resulted in the parents struggling with emotional management and having limited personal resources to provide care for their child. A severe physical illness impaired a parents’ physical ability to perform specific care tasks. A low level of support from a parent’s social network proved to be a risk factor in the parents’ ability to re-organize daily life. This became a more complex task when being a single parent with several children. An annual household income below the national average for the parent’s household type put the parents at financial risk when income compensation was delayed. A low level of education impaired the parents´ communications with authorities, e.g. when requiring income compensation. Being unemployed or a student was a risk factor as these parent types received the lowest income compensation and were most exposed to the greatest financial difficulty. Being of other ethnicity than Danish was a risk factor when combined with an inability to speak Danish. It affected the parents’ ability to communicate with representatives of the health- and social welfare system. The above-mentioned risk factors for the 25 families in the intervention study are listed in Table 1. It is important to note that having one or more of the following risk factor suffice to severely affect the parents’ ability to care for the child. Table 1 The 25 families had a total of 55 risk factors (highlighted in bold). Figure 2 Figure 2 shows the distribution of the seven risk factors described above that affected the 25 families. Based on the parents’ civil status 13 families had a household income below the national average and 12 had a household income equal to or above the average. Low household income was the predominant risk factor, followed by a lack of practical and emotional support and poor health. Figure 3 During the intervention study the CMN noted the amount of time spend each day to assist families in managing the child’s HSCT. When a family had concurrent emotional, organisational and financial problems, the amount of time spent with each family increased. If a family possessed several risk factors in addition to the three problem areas, then the amount of time spent on interventions further increased. This triggered an analysis of the average time spent per week by the CMN in addressing the parents´ risk factors identified prior to HSCT. Figure 3 shows that when a family had four or more risk factors then the time spent intervening doubled compared with families identified with less than three risk factors. The 55 risk factors were not evenly distributed between the 25 families. Six families in total possessed 31 risk factors while the remaining 24 risk factors were distributed between the remaining 19 families. The six families characterised as having four or more of the seven risk factors, were those families in most immediate need of emotional, re-

11
organizational, and financial support. These families each required up to 24 hours of CMN intervention per week during the child’s hospitalization (average 49 days). DISCUSSION A main finding of this study is that all of the parents had addressed the emotional, organizational and financial problems associated with their child’s HSCT. The majority of the families have overcome these problems. Another essential finding is that new challenges arise during the child’s HSCT affecting the family’s emotional, organizational and financial situation. When new challenges are added, the complexity of the problems within the family increases as does the parents´ need for support. Emotional strain on the family In this study, the majority of parents managed the emotional strain emanating from the child’s HSCT. This is explained by Jobe-Shields et al.’s (2009) study in which family cohesion, family expressiveness and low parental depressive symptoms acted as protective factors against child distress. However, the HSCT challenged a subset of parents’ emotional strategies in this study, mainly when changes in the child’s medical treatment and well-being occurred or when the parents were emotional exhausted. The fact that a child’s HSCT is emotionally challenging is demonstrated in the current study and in the literature, where an increased level of distress and depression is found among parents to children treated with HSCT (Phipps et al., 2004; Barrera et al., 2000; Manne et al., 2004). The intervention study showed that parents most in need of support to manage emotional strain were those dealing with a psychiatric illness, a limited social network and/or language barriers, in addition to organizational and financial problems. This finding is concurrent with studies that link parents’ management of a child’s HSCT to their prior emotional well-being, negative life events, personality traits and social support (DuHamel et al., 2007; Phipps et al., 2005; Rini et al., 2008). An essential implication of this finding is that early identification of parents in need of emotional support is important to preventing additional strain. The reorganization of family daily life The parents in this study were expected to care for the child during the HSCT. This places an organizational strain on them. The families relied heavily on support from their own parents to help at home or at the hospital. A subset of parents had a limited social network and felt isolated in the care of their child. The importance of lacking support has been linked to lowered function, heightened stress and perceived vulnerability among mothers (Rini et al., 2008; Vrijmoet-Wiersma et al., 2009a). However, at the time of the child’s cancer diagnosis, no significant differences in problem-solving ability between two-parent and single-parent households have been found (Lobst et al., 2009). In this study, we found that single-parent households with more than one child were more dependent on support from their social network than two-parent households in managing the re-organisation of the family life. In addition, the most challenged were the singles with limited supporting networks. This became more apparent if the re-organisation plans failed during HSCT. Financial challenges imposed in the family during a child’s HSCT Families do not always receive entitled benefits during the transition period from salary earner to receiving income compensation and may experience delays in claim processing (Adelman et al., 2003). The parents in this study, who did not meet the social welfare system’s predefined categories, e.g. business owners or parents with variable incomes, experienced difficulties in
12
justifying their income levels. Regardless, household income delays or reductions place pressure on family life. The most predominant risk factor was household income below the average set by family type as the majority of the parents in this study did not meet the criteria for the poverty level (Aber et al., 1997; Deding & Gerstoft 2009; Statistics Denmark, 2009). The financial strain on this subset of parents was interrelated with a low level of education or being unemployed. Subsequently, these parents’ income levels were frozen for the duration of the child’s treatment. To receive support from the Danish social welfare system, the parents were required to acquaint themselves with the social law to make a solid case (Ploug 2007). Parents found this to be time consuming and difficult especially when they were unfamiliar with the Danish social system and language. The combination of a child’s HSCT with financial strain increases the parents´ risk of impaired emotional well-being. Families with a complex set of interrelated problems Six families in this study required interventions of the highest degree and intensity by the CMN to manage the care of their child. These parents had multiple interrelated complex problems that reinforced each other. Some of the emotional, financial and social network support problems that they parents faced did not emerge as a result of the child’s HSCT but rather, they pre-existent and interrelated with the following risk factors: 1) physical/psychiatric illness; 2) being single parents with a low support level; 3) having a low level income which in combination with having a low education level or unemployment. In addition, Danish as a second language was a challenge when communicating with the social welfare authorities. This study and the literature on this subject, indicates that poor mental health and depression are likely to affect parents’ ability to nurture their children (Aber et al., 1997; Jobe-Shields et al., 2009). Furthermore, a lack of nurturing support during the HSCT, places the child at risk of a range of psychological and social difficulties following treatment (Phipps & Mulhern 1995). In this study, the parents’ pre-existing problems were prolonged and made more complex as a consequence of their child’s HSCT. This finding is in line with Kronenberg et al.´s (1998) study where social and life stresses, aside from the child’s disease, pose a significant threat to the mothers´ acceptance of her child’s HSCT. Being able to identify parents with multiple interrelated problems is important as these problems affect the care provided during the child’s HSCT. Methodological considerations and limitations This study adds to the growing body of studies related to parents´ coping ability during their child’s HSCT. The majority of these studies use quantitative methods and few qualitative methods when addressing this problem. By using semi-structured interviews, we aimed to provide an in-depth understanding of how parents experience, describe and resolve problem areas related to the child’s HSCT, and to provide an understanding of how these problems are interrelated and affected by the parents’ prior and current life. The parents who participated in this study possess a long experience of being parents to a severely ill, hospitalized child treated with HSCT and how this impacts family life. The main problems areas identified in this study are transferable to other parents groups to children who are severely ill or face prolonged hospitalization. This study identified a subset of six parents characterized by multiple interrelated problems, who found it difficult to function without extensive CMN intervention. The complexity of their problems derived from their background of risk factors as well as from the problem areas imposed on then by their child’s HSCT. The risk factors identified through the current study should be confirmed using a larger sample and within other cultures, so that families most in need of CMN support can be identified as early as possible.

13
CONCLUSION Prior to the child’s HSCT parents in the current study possess a number of risk factors that influence their daily life prior to their child’s HSCT, i.e. these included: 1) single-parents household; 2) low-level income; 3) low-level education; 4) low-level social network support; 5) student or unemployed status; 6) physical/psychiatric illness; and 7) ethnicity. In addition, they needed to address at least three new problems areas related to the child’s HSCT. These include: emotional strain on the family; the re-organisation of the family daily life; and financial adjustment to their incomes. This intervention study showed a clear association between the number of risk factors and the extent of support parents required during the child’s HSCT. The families in this study needed emotional support, support to identify resources within their social network /assistance to apply for additional network support from the Danish social welfare authorities, and support to relieve the family’s financial constrains. It is recommended that future clinical practice assess the number of risk factors that parents face prior to their child’s HSCT. Screening to identify families with multiple interrelated problems is suggested and allocating most resources to support these families is strongly suggested. By doing this, families will gain the ability to manage the strain imposed in them by their child’s HSCT. Resources allocation to families most in need may provide a more optimal outcome for children undergoing HSCT as well as during their rehabilitation. Acknowledgements Danish Cancer Foundation for Children, Danish Health Foundation, Lundbeck Foundation, Gangsted foundation, Righospital- Copenhagen University Hospital supported this study.
14
REFERENCES Aber J.L., Bennett N.G., Conley D.C. & Li J. (1997) The effects of poverty on child health and development. Annual Review of Public Health 18, 463-83. Adelman L., Middleton S. & Ashworth P. (2003) Britain’s poorest children: severe and persistent poverty and social exclusion. Save the Children, London, UK. Attree P. (2006) The social costs of child poverty: a systematic review of the qualitative evidence. Children & Society 20, 54-66. Backett-Milburn K., Cunningham-Burley S. & Davis J. (2003) Contrasting lives, contrasting views? understandings of health inequalities from children in differing social circumstances. Social Science & Medicine 57, 613-623. Barrera M., Boyd-Pringle L.A., Sumbler K. & Saunders F. (2000) Quality of life and behavioral adjustment after pediatric bone marrow transplantation. Bone Marrow Transplantation 26, 427-435. Beck A.T., (1979) Cognitive Therapy and the emotional disorders, Meridian, The penguin group, Middlesex, England Beck A.T and Emery G., (1985) Anxiety Disorders and Phobias, A cognitive perspective, Basics Books, The Perseus book group, USA Beck J.S (2005) Cognitive therapy for challenging problems: What to do when the Basics don’t Work. The Guilford Press, New York. Clarke S.A., Eiser C. & Skinner R. (2008) Health-related quality of life in survivors of BMT for paediatric malignancy: a systematic review of the literature. Bone Marrow Transplantation 42, 73-82. Copelan E.A. (2006) Hematopoietic stem cell transplantation. New England Journal of Medicine 354, 1813-1826. Davies B., Davis E., Cook K. & Waters E. (2008) Getting the complete picture: combining parental and child data to identify the barriers to social inclusion for children living in low socio-economic areas. Child Care Health & Development 34, 214-222. Deding M. & Gerstoft F. (2009) Børnefattigdom i Danmark 2002-2006 (Child poverty in Denmark 2002-2006). SFI - The Danish National Center for Social Research, Copenhagen. DuHamel K.N., Rini C., Austin J., Ostroff J., Parsons S., Martini R., Williams S., Mee L., Sexson S., Winkel G., Boulad F., Redd W.H. & Manne S. (2007) Optimism and life events as predictors of fear appraisals in mothers of children undergoing hematopoietic stem cell transplantation. Psycho-Oncology 16, 821-833.

15
Gyldendal (2009). Danmark: familieforhold (Denmark: family conditions). Den Store Danske - Gyldendals åbne encyklopædi [Online]. Available at: http://www.denstoredanske.dk/index.php?sideId=61047 [Accessed 24 September 2010] Günter M. (2000) Art therapy as an intervention to stabilize the defenses of children undergoing bone marrow transplantation. The Arts in Psychotherapy 27, 3-14. Jobe-Shields L., Alderfer M.A., Barrera M., Vannatta K., Currier J.M., and Phipps S (2009) Parental Depression and Family Environment Predict Distress in Children Before Stem Cell Transplantation. Journal of Developmental and Behavioral Pediatrics 30, 140-146 Kronenberger W.G., Carter, B.D., Edwards J., Morrow C., Stewart J. & Sender L. (1998) Psychosocial adjustment of mothers of children undergoing bone marrow transplantation: the role of stress, coping and family factors. Children’s Health Care 27, 77-95. Kuntz N., Adams J.A., Zahr L., Killen R., Cameron K. & Wasson H. (1996) Therapeutic play and bone marrow transplantation. Journal of Pediatric Nursing 11, 359-367. Larsen J.E. (2004) Fattigdom og social eksklusion: tendenser i Danmark over et kvart århundrede (Poverty and social exclusion: tendency in Denmark over a quarter century). SFI - The Danish National Center for Social Research, Copenhagen. Lesko L.M. (1994) Bone marrow transplantation: support of the patient and his/her family. Supportive Care in Cancer 2, 35-49. Loberiza F.R. Jr, Serna D.S., Horowitz M.M. & Rizzo J.D. (2003) Transplant center characteristics and clinical outcomes after hematopoietic stem cell transplantation: what do we know? Bone Marrow Transplantation 31, 417-421. Lobst E.A., Alderfer M.A., Sahler O.J.Z., Askin M.A., Fairclough D.L., Katz E.R., Butler R.W., Dolgin M.J. and Noll R.B.. (2009) Brief Report: Problem Solving and Maternal Distress at the time of the Child´s Diagnosis of Cancer in Two-Parent versus Lone-Parent Households Journal of Pediatric Psychology 34, 8, 817-821 Malterud K. (2001a) The art and sciences of clinical knowledge: evidence beyond measures and numbers. Lancet 358, 397-400. Malterud K. (2001b) Qualitative research: standards, challenges, and guidelines. Lancet 358, 483-488. Manne S., DuHamel K., Nereo N., Ostroff J., Parsons S., Martini R., Williams S., Mee L., Sexson S., Wu L., Difede J. & Redd W.H. (2002) Predictors of PTSD in mothers of children undergoing bone marrow transplantation: the role of cognitive and social processes. Journal of Pediatric Psychology 27, 607-617. Manne S., DuHamel K., Ostroff J., Parsons S., Martini D.R., Williams S.E., Mee L., Sexson S., Austin J., Difede J., Rini C. & Redd W.H. (2004) Anxiety, depressive, and posttraumatic stress
16
disorders among mothers of pediatric survivors of hematopoietic stem cell transplantation. Pediatrics 113, 1700-1708. Packman W., Weber S., Wallance J. & Bugescu N. (2010) Psychological effects of hematopeietic SCT on pediatric patients, siblings and parents, Bone Marrow Transplantation 45, 1134-1146 Ploug N. (2007) Socialt udsatte børn: identifikation, viden og handlemuligheder i daginstitutioner (Socially disadvantaged children: identification, knowledge and scope of action in day care). SFI - The Danish National Center for Social Research, Copenhagen. Phipps S and Mulhern R.K. (1995) Family cohesion and expressiveness promote resilience to the stress of pediatric bone marrow transplant: a preliminary report. Development and Behavioral Pediatrics 16, 257-263 Phipps S., Dunavant M., Garvie P.A., Lensing S. & Rai S.N. (2002a) Acute health-related quality of life in children undergoing stem cell transplant: I. Descriptive outcomes. Bone Marrow Transplantation 29, 425-434. Phipps S., Dunavant M., Lensing S. & Rai S.N. (2002b) Acute health-related quality of life in children undergoing stem cell transplant: II. Medical and demographic determinants. Bone Marrow Transplantion 29, 435-442. Phipps S. (2002c) Reduction of distress associated with paediatric bone marrow transplant: complementary health promotion interventions. Pediatric Rehabilitation 5, 223-234. Phipps S., Dunavant M., Lensing S. & Rai S.N. (2004) Patterns of distress in parents of children undergoing stem cell transplantation. Pediatric Blood Cancer 43, 267-274. Phipps S., Dunavant M., Lensing S. & Rai S.N. (2005) Psychosocial predictors of distress in parents of children undergoing stem cell or bone marrow transplantation. Journal of Pediatric Psychology 30, 139-153. Phipps S., Barrera M., Vannatta K., Xiong X., Doyle J.J., and Alderfer M.A. (2010) Complementary Therapies for Children Undergoing Stem Cell Transplantation. Cancer 116(16), 3924-3933 Rini C., Manne S., DuHamel K., Austin J., Ostroff J., Boulad F., Parsons S.K., Martini R., Williams S.E., Mee L., Sexson S. & Redd W.H. (2008) Social support from family and friends as a buffer of low spousal support among mothers of critically ill children: a multilevel modeling approach. Health Psychology 27, 593-603. Roy C. and Roberts S.L., (1981) Theory construction in nursing. An adaptation model. Englewood Cliffs. N.J. Prentice Hall. Sherman A.C., Simonton S., Latif U., Nieder M.L., Adams R.H. & Metha P. (2004) Psychosocial supportive care for children receiving stem cell transplantation: practice patterns across centers. Bone Marrow Transplantation 34, 169-174.
17
Statistics Denmark (2009) Indkomster 2007: særskilt afsnit om personer med høje og lave indkomster (Income 2007: separate document on people with high and low income). Statistics Denmark, Copenhagen. Tremolada M., Bonichini S., Pillon M., Messina C. & Carli M. (2009) Quality of life and psychosocial sequelae in children undergoing hematopoietic stem-cell transplantation: a review. Pediatric Transplantation 13, 955-970. Vrijmoet-Wiersma C.M.J., Egeler R.M., Koopman H.M., Norberg A.L.& Grootenhuis M.A. (2009b) Parental stress before, during, and after pediatric stem cell transplantation: a review article. Supportive Care in Cancer 17(12), 1435-1443 Vrijmoet-Wiersma C.M., Kolk A.M., Grootenhuis M.A., Spek E.M., van Klink J.M., Egeler R.M., Bredius R.G. & Koopman H.M. (2009a) Child and parental adaptation to pediatric stem cell transplantation. Support Care Cancer 17, 707-714. Walker A. & Walker C. (eds) (1997) Britain divided: the growth of social exclusion in the 1980s and 1990s. Child Poverty Action Group, London.
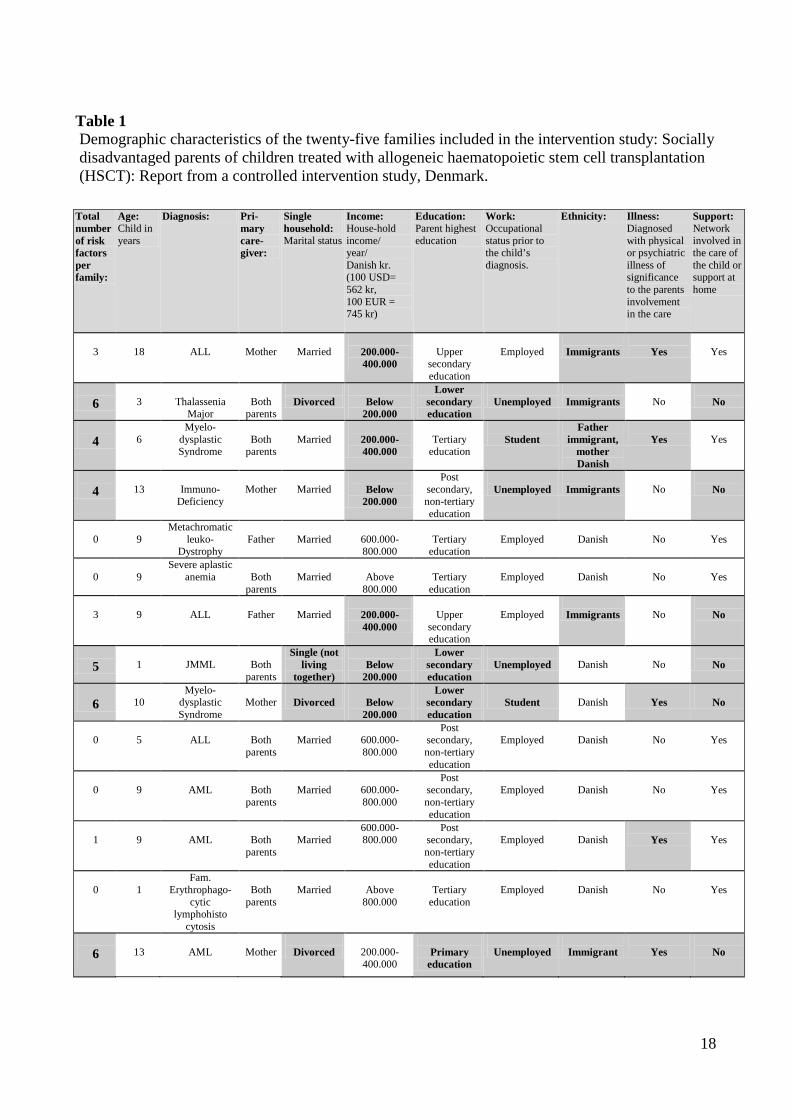
18
Table 1 Demographic characteristics of the twenty-five families included in the intervention study: Socially disadvantaged parents of children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study, Denmark.
Total number of risk factors per family:
Age: Child in years
Diagnosis: Pri-mary care-giver:
Single household: Marital status
Income: House-hold income/ year/ Danish kr. (100 USD= 562 kr, 100 EUR = 745 kr)
Education: Parent highest education
Work: Occupational status prior to the child’s diagnosis.
Ethnicity: Illness: Diagnosed with physical or psychiatric illness of significance to the parents involvement in the care
Support: Network involved in the care of the child or support at home
3
18
ALL
Mother
Married
200.000-400.000
Upper
secondary education
Employed
Immigrants
Yes
Yes
6
3
Thalassenia
Major
Both
parents
Divorced
Below
200.000
Lower secondary education
Unemployed
Immigrants
No
No
4
6
Myelo- dysplastic Syndrome
Both
parents
Married
200.000-400.000
Tertiary
education
Student
Father immigrant,
mother Danish
Yes
Yes
4
13
Immuno-
Deficiency
Mother
Married
Below
200.000
Post secondary, non-tertiary education
Unemployed
Immigrants
No
No
0
9
Metachromatic leuko-
Dystrophy
Father
Married
600.000-800.000
Tertiary
education
Employed
Danish
No
Yes
0
9
Severe aplastic anemia
Both
parents
Married
Above
800.000
Tertiary
education
Employed
Danish
No
Yes
3
9
ALL
Father
Married
200.000-400.000
Upper
secondary education
Employed
Immigrants
No
No
5 1
JMML
Both
parents
Single (not living
together)
Below
200.000
Lower secondary education
Unemployed
Danish
No
No
6
10
Myelo-dysplastic Syndrome
Mother
Divorced
Below
200.000
Lower secondary education
Student
Danish
Yes
No
0
5
ALL
Both
parents
Married
600.000-800.000
Post secondary, non-tertiary education
Employed
Danish
No
Yes
0
9
AML
Both
parents
Married
600.000-800.000
Post secondary, non-tertiary education
Employed
Danish
No
Yes
1
9
AML
Both
parents
Married
600.000-800.000
Post secondary, non-tertiary education
Employed
Danish
Yes
Yes
0
1
Fam. Erythrophago-
cytic lymphohisto
cytosis
Both
parents
Married
Above
800.000
Tertiary
education
Employed
Danish
No
Yes
6
13
AML
Mother
Divorced
200.000-400.000
Primary
education
Unemployed
Immigrant
Yes
No
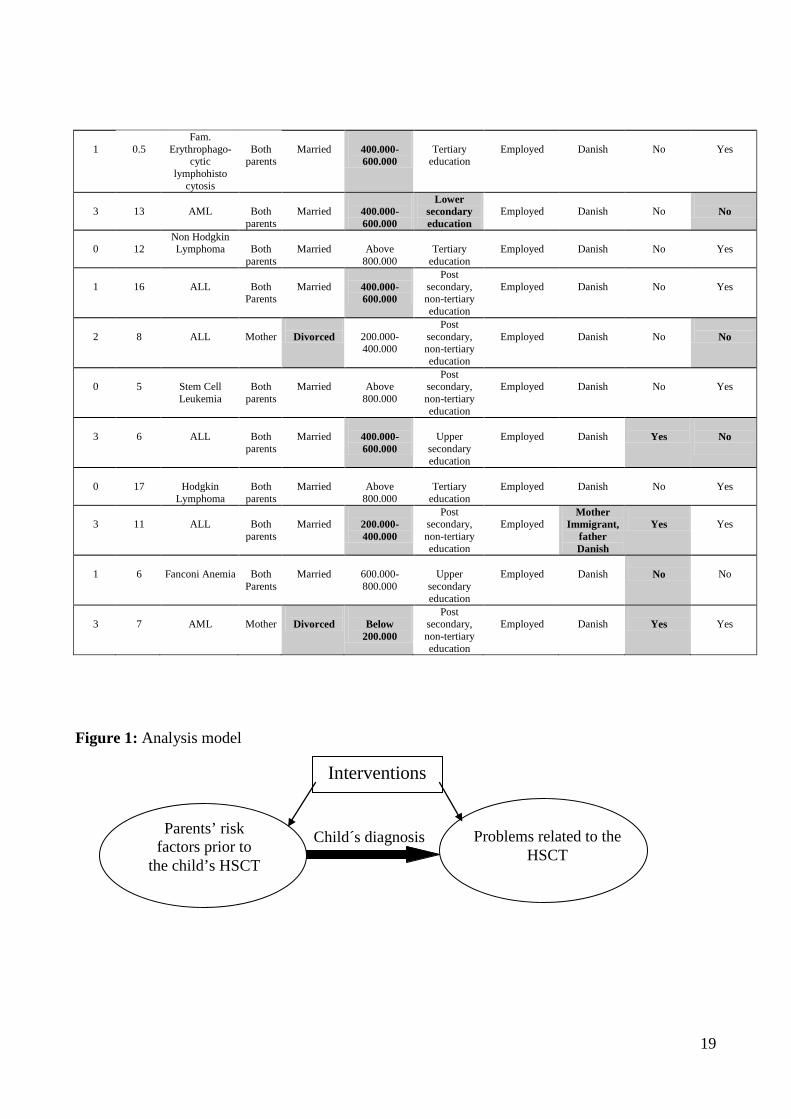
19
1
0.5 Fam.
Erythrophago-cytic
lymphohisto cytosis
Both
parents
Married
400.000-600.000
Tertiary
education
Employed
Danish
No
Yes
3
13
AML
Both
parents
Married
400.000-600.000
Lower secondary education
Employed
Danish
No
No
0
12
Non Hodgkin Lymphoma
Both
parents
Married
Above
800.000
Tertiary
education
Employed
Danish
No
Yes
1
16
ALL
Both
Parents
Married
400.000-600.000
Post secondary, non-tertiary education
Employed
Danish
No
Yes
2
8
ALL
Mother
Divorced
200.000-400.000
Post secondary, non-tertiary education
Employed
Danish
No
No
0
5
Stem Cell Leukemia
Both
parents
Married
Above
800.000
Post secondary, non-tertiary education
Employed
Danish
No
Yes
3
6
ALL
Both
parents
Married
400.000-600.000
Upper
secondary education
Employed
Danish
Yes
No
0
17
Hodgkin
Lymphoma
Both
parents
Married
Above
800.000
Tertiary
education
Employed
Danish
No
Yes
3
11
ALL
Both parents
Married
200.000-400.000
Post secondary, non-tertiary education
Employed
Mother Immigrant,
father Danish
Yes
Yes
1
6
Fanconi Anemia
Both
Parents
Married
600.000-800.000
Upper
secondary education
Employed
Danish
No
No
3
7
AML
Mother
Divorced
Below
200.000
Post secondary, non-tertiary education
Employed
Danish
Yes
Yes
Figure 1: Analysis model
Parents’ risk factors prior to
the child’s HSCT
Problems related to the HSCT
Interventions
Child´s diagnosis

20
Figure 2: Number of risk factors among the 25 families
0
24
68
1012
14
Income Support Illness Ethnicity Work Singlehousehold
Education
Risk factors
Num
ber o
f fam
ilies
Figure 3: Number of families with risk factors and intervention time spend in relation to number of risk factors
0123456789
no riskfactors
Onerisk
factor
Two riskfactors
Threerisk
factos
Fourrisk
factors
Five riskfactors
Six riskfactors
SevenRisk
factors
0
5
10
15
20
25
30
Number of families
Interventionhours/week/family
1
PAPER III Supportive Intervention Program Targeting Parents to Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation (HSCT): A Controlled Study Authors: Authors: Hanne Bækgaard Larsen, Lis Adamsen, Anders Tolver, Christoffer Johansen, Carsten Heilmann Institutions Hanne Bækgaard Larsen, RN, MSc. Soc., Copenhagen University Hospital [Rigshospital], Finsen Center, Copenhagen, Denmark University of Copenhagen, Faculty of Health Sciences, Copenhagen, Denmark The University Hospital Center for Nursing and Care Research (UCSF) Professor Lis Adamsen, RN, MSc.Soc., PhD Copenhagen University Hospital, The University Hospital Center for Nursing and Care Research (UCSF), Department 7331 Institute of Public Health, Faculty of Health Sciences, University of Copenhagen, Blegdamsvej 9 2100 Copenhagen, Denmark e-mail: [email protected] Associate Professor Anders Tolver, MSc, Ph.D. Department of Basic Sciences and Environment Faculty of Life Sciences University of Copenhagen Thorvaldsensvej 40 1871 Frederiksberg C Denmark e-mail: [email protected] Professor Christoffer Johansen MD, PhD, DMSc, Head, Department of Psychosocial Cancer Research Institute of Cancer Epidemiology Strandboulevarden 49 2100 Copenhagen Denmark e-mail: [email protected] Professor Carsten Heilmann, MD, DMSc Copenhagen University Hospital, [Rigshospital], Paediatric Clinic, 4072 Juliane Marie Center Blegdamsvej 9 2100 Copenhagen Denmark e-mail: [email protected]

2
Corresponding Author: Hanne Bækgaard Larsen, RN, MSc. Soc. The University Hospital Center for Nursing and Care Research Copenhagen University Hospital, Department 7331 DK-2100 Copenhagen Denmark Telephone: +45 3545 7336 Telefax: +45 3545 7399 Email: [email protected] Running header: Support Intervention Program Targeting Parents to Children undergoing HSCT

3
Abstract Anxiety and depression were investigated in a controlled nine-hour/week intervention program targeting parents hospitalized with their children who were undergoing Allogeneic Haematopoietic Stem Cell Transplantation (HSCT). The program included daily family navigator nurse support (medical information relay, social counselling, and emotional support), educational and physical activity sessions. The parental intervention group (N=25) was compared with two parental control groups receiving standard care: I) a consecutive prospective group (N=8), and II) a retrospective group (N=57). At admission, the intervention and the prospective control groups completed weekly evaluations to time of discharge and at day100, using HADS and BASES questionnaires. The retrospective control group performed the same evaluation once, by mail. Results: No significant difference was observed between the groups. On admission, the parents displayed a moderate to severe level of anxiety (39%) and depression (24%). However, the HADS scores decreased on day100 (p<0.01). The anxiety decline occurred earlier in the intervention group than in the control group. In particular, parents with a relatively low-level of anxiety benefited from the intervention program. Based on this parent-targeted study, anxiety and depression support interventions and further research are recommended. Keywords: SCT, Parents, Anxiety, Daily, Intervention

4
INTRODUCTION At hospital admission for Allogenic Haematopoietic Stem Cell Transplantation (HSCT), 15-66% of parents experience an elevated level of depression and anxiety (1-7). At discharge, Nelson et al. (5) found that 52% of mothers (N=50) suffered from depression and 18 months following HSCT, Manne et al. (3) found that more than 10% of mothers (N=115) were diagnosed with depressive disorders and 4% with general anxiety disorders. Neither of these studies included comparison groups. Studies have linked the parents’ elevated level of anxiety and depression to the threat that HSCT poses on the child’s life (8-10) and to witnessing treatment related side-effects and complications (11-13). During HSCT, parents perform comprehensive care tasks and deal with the child’s physical and emotional responses to HCST (8;14-19). Concurrently, the parents must deal with changes in the family situation, the needs of healthy siblings, work-related changes, financial burdens and medical information (2;20-22). The complex medical treatment, the transition in the parents’ daily life, the expectations of their caregiving performance combined with the high prevalence suffering from depressive and anxiety symptoms implies unmet psychosocial needs that warrant testing and development through a support intervention program. Only one HSCT parent-targeted intervention study (2) (n=22) that included a control group was identified. Based on validated questionnaires, this study indicated that parents receiving stress management training prior to the child’s HSCT used stress managment techniques more frequently than parents in the control group, however, the results were not significant. Based on these limited data, we set out to conduct a controlled study in order to enhance and support the parents’ caregiving abilities and diminish their levels of anxiety and depression during their child’s HSCT. We had access to the only clinic in Denmark that offers HSCT and this ensured a population-based (5.5. million) and nationwide study. We designed the study to compare the intervention group with two control groups of parents, including three months of follow-up on completion of the intervention. MATERIAL AND METHODS In accordance with the free-of-charge health care system, the 15 to 22 children below the age of 18 years who require HSCT annually are treated at the University Hospital of Copenhagen (Rigshospitalet) (23). By law, at least one parent is granted full financial compensation to care for the child irrespective of their socio-economic status (24). This law is interpreted and administered by the social authorities of the parents’ respective municipalities (21). From the time of conditioning until engraftment, at least one parent is expected to perform around-the-clock child care at the hospital. After introduction to the HSCT unit’s hygienic standards, including the rationale for keeping the child isolated in a laminar air-filtered room for approximately4-6 weeks, the parents provide basic care for the child (assistance with personal hygiene, food preparation, medicine administration and entertainment). Participants To address the problem regarding the limited number of children (aged 0-20 years) undergoing HSCT annually, it was decided to compare three groups of parents: an intervention group and two control groups receiving standard care. All resident parents of children undergoing HSCT in Denmark were eligible for inclusion in the study.
• The retrospective parental control group (RPCG) (N=57) was recruited in June 2007. These parents had a child treated with HSCT during the period from 1. January 2004 to 30. June 2007.
• The prospective parental control group (PPCG) (N=8) was recruited from 1. July 2007 to 31 October 2007.
5
• The parental intervention group (PIG) (N=25) was recruited from 1. November 2007 to 31. October 2009.
Exclusion criteria were: 1) parents to children with a medical prognosis of imminent death, 2) children without a resident parent as primary caregiver, and 3) a parent’s inability to speak Danish. Figure 1: insert As illustrated in figure 1, a total of 62 children (alive) were eligible for the RPCG. However, five (8%) children were classified as ineligible. Consequently, 57 parents were contacted by mailed questionnaire and 46 (81%) responded. Ten children were eligible for participating in the PPCG, however, two (20%) children did not have a parental caregiver. Eight parents consented to participate, two children died within the first 100 days and six parents (75%) completed the study. A total of 31 children were approached for participation in the PIG, however, six (19%) were ineligible. 25 parents consented to participate but four (19%) parents did not complete the study. Intervention program Table 1: insert This program included three parent-targeted components (table 1).
• Daily medical information relay, emotional support and social counselling by a Family Navigator Nurse (FNN)
The case manager and patient navigator theory inspired the FNN function, including troubleshooting of transitional problems faced by parents when attempting to navigate within the complex medical and welfare system (25-27). The FNN intervention component was provided (by HBL) during daily rounds to the isolation rooms where the child and the parent stayed. The FNN provided: 1) medical information that focused on the parental caregiving tasks in relation to the child’s physical needs (e.g. nausea, nutrition, skin problems); 2) emotional support focusing on the parents’ thoughts and concerns (e.g. frustration, distress, anxiety), with particular attention given to negative thoughts (e.g. fear of the child’s death); and 3) social counselling that focused on the parents’ unresolved financial and social networking problems. Each component played a role in the intervention. By these means the FNN improved the parent’s caregiving abilities and provided emotional support inspired by cognitive behavioural therapy (28-30). Following each encounter, the FNN identified each family’s problems that involved co-operatioin from other professionals (nurses, physicians, psychologists, social authorities), and redirected, referred or mediated to resolve these problems.
• The supervised structured education program The parents were offered five one-hour educational sessions on: family changes, children’s reactions, conflict management and child development. A sociologist, a nurse, a psychologist, a play therapist and a parent to a recently transplanted child conducted these sessions.
• Physical activity To attain physical and emotional well-being (31;32) parents were offered three hours of of physical activity (bicycling/walking outside the hospital) per week. The intervention program included nine hours of intervention per family per week for the duration of the child’s 4-6 weeks of hospitalization.

6
Data collection Figure 2: insert Participants in the PPCG and PIG group completed questionnaires at hospital admission (baseline), weekly until discharge and at day 100 following HSCT treatment (Figure 2). Participants in the RPCG completed a mailed questionnaire. Medical and treatment information for the children was obtained by reviewing the medical records. Questionnaires All of the parents completed a questionnaire on socio-demographic factors, the Hospital Anxiety and Depression Scale (HADS) (33), the Behavioural, Affective and Somatic Experience Scale (BASES) (34;35), Profile of Mood States-B (POMS) (36), and Coping Health Index for Parents (CHIP) (37) . Socio-demographic information included: marital, financial, employment and medical status. The HADS is a 14- item anxiety and depression screening tool that measures symptoms on a 4-point scale (range 0-3) (33). The results were analysed categorically for anxiety and depression, discriminating normal (0-7 points), borderline (8-10 points) and moderate to severe symptom levels (11- 21 points). The 22-item BASES questionnaire repeatedly measured, on a 5-point scale, the acute aspects of the child’s quality of life (34;35). BASES has 5 subscales: somatic distress, compliance, mood disturbance, quality of interaction and activity. The parental version of BASES was used in all three groups of parents while the children’s version of BASES was used in the PIG and PPCG. The POMS shortened (30-item) version measured the psychological state of the parents on a 5-point scale. POMS has 6 subscales: tension-anxiety, depression-dejection, anger-hostility, vigor-activity, fatigue-inertia, and confusion-bewilderment (36). The CHIP scale (45-items) measures parents’ responses to life when having a seriously/chronically ill child, on a 4-point scale (not helpful to extremely helpful). The CHIP has three subscales: 1) maintaining family integration, cooperation and an optimistic definition of the situation, 2) maintaining social support, self-esteem and psychological stability, and 3) understanding the medical situation through communication with other parents and consultation with the medical staff (37). To obtain a Danish version of the BASES and CHIP, we used a back and forth translation by two independent bilingual researchers following the recommendation of the EORTC (38). Furthermore, we conducted a semantic equivalence testing with 10 parents to HSCT children to further evaluate the face validity (39). Statistical methods and outcomes The primary endpoint with respect to the efficacy of the intervention program was the overall wellbeing of parents as measured by the HADS, supplemtented by BASES, POMS and CHIP. Fisher’s exact test and Mann-Whitney U test were used to investigate if the intervention and the two control groups were comparable with respect to socio-demographic characteristics and baseline measurements. The purpose of the statistical analyses was to compare the PIG and the PPCG and to study changes within each group from baseline to day 100. Weekly measurements of subscale scores were analysed using a linear mixed effects model and the model was validated using residual plots and quantile-quantile plots. Using a parametric model increases the power of the statistical

7
analysis. Furthermore, this approach takes into account that the data were unbalanced with respect to the number of completed questionnaires from individual parents. Estimated changes from baseline to day 14 and day 100 for the HADS scores were extracted from the mixed model. Spearman’s tests were used to examine the association between HADS scores and subscales on the BASES. A background population of a non-clinical sample of the UK population (n=1792) (40) was identified to further compare the level of HADS in this study. All analyses were performed using “R: A Language and Environment for Statistical Computing” (41) and a significance level of p<0.05. Estimates for subscale scores at each time point are reported with standard errors while changes of HADS scores from baseline are displayed with 95% confidence intervals (CI) in Figure 3. The Regional Ethical Scientific Committee approved the study (File no: 01-206-7216) and the participants provided informed oral and written consent in compliance with requirements of the Committee. The study was filed with the National Data Protection Board (File no: 2007-58-0015). RESULTS Intervention compliance The FNN intervention was performed in 92% of the expected intervention days. 72% of the parents completed the supervised structured educational program and 16% participated in the physical activity sessions. The FNN intervention was a well-accepted intervention component and none of the parents terminated their participation in this component prior to the child’s discharge. Parents to children previously treated with HSCT recommended the physical activity intervention component. Despite provision of childcare, the parents’ were reluctant to leave the child’s bedside to go walking outside of the hospital. Consequently, physical activity became an unaccepted intervention component. Table 2: insert Table 2, shows the medical and treatment characteristics of the children treated with HSCT and the socio-demographic characteristics of the included parents. Table 3: insert Table 3 shows the parents mean HADS, BASES, POMS and CHIP scores at baseline. Compared with baseline scores, the RPCG recall their children’s level of physical distress (p=0.00) and mood disturbance (p=0.01) as being significantly worse than in the PIG. Furthermore, POMS showed that single parents were significantly (p=0,01) more confused than married parents at baseline. In addition, the PPCG were significantly (p=0.01) more confused at 100 days than PIG. The effect of the intervention program When comparing the PIG and the PPCG levels of anxiety and depression on the HADS scale, no significant difference between the groups was found at any time during the intervention period. The parents’ levels of anxiety and depression from admission to day 100 At baseline, there was no significant difference between HADS anxiety (p=0.79) and depression (0.88) scores in the three groups of parents. At admission to HSCT treatment, 39% (CI:23%-56%)
8
of the resident parents (PCG and IG) reported moderate to severe symptoms on the HADS anxiety scale (median 10, lower-quantile 7, upper-quantile 12) compared to 12.6% in the general population (median 6, lower-quantile 4, upper-quantile 9) (40). Concurrently, 24% (CI: 10%-39%) had moderate to severe levels of depression on the HADS scale (median 6, lower-quantile 3.75, upper-quantile 10.25) compared to 3.6% in the general population (median 3, lower-quantile 1, upper-quantile 6) (40). In the RGC, 41 % (CI:22%-60%) (median 10, lower-quantile 6, upper-quantile 15) indicated a moderate to severe level of anxiety and 26 % (CI 9%-43%) (median 7, lower-quantile 4, upper-quantile 11) a moderate to severe level of depression symptoms. A significant decline (p<0.01) on the anxiety scale was found at day 100 and the number of parents with moderate and severe levels of anxiety decreased to 22% (CI: 7%-38%). The number of parents with moderate and severe levels of depression declined to 11% (CI:0%-23%) (p=0.04). Table 4: insert A significant reduction in the HADS anxiety level was observed in the intervention group from baseline to day 0 (p<0.02), day 14 (p<0.01), day 21 (p<0.02) and day 100 (p<0.00) while the decline had borderline significance at day 7 (p<0.08) and day 28 (p=0.08), (table 4, figure 3). No decline showed in the PPCG on the HADS anxiety scale during the hospitalisation but as mentioned a significant decrease was observed at day 100 (p<0.01). Concerning the HADS depression scale, no significant difference (p=0.98) between the intervention and the control groups was found but an overall decline for both groups was observed from baseline to day 100 (p<0.01). Figure 3: insert Splitting the PIG into two groups of equal size, according to the baseline values on the HADS anxiety scale, a significant decrease to day 0 (p<0.04) was found only in the group experiencing a relatively low-level of initial anxiety (Figure 3). Assicoation between the parents HADS level and their rating of the child’s affective and somatic experience To test the interrelatedness between the parents’ levels of anxiety and depression and their rating of the child’s affective and somatic experience, the association between the parents’ HADS scores and their rating of the child’s BASES scores was analysed. Significant associations were found between the increased parents´ HADS anxiety score and the parents’ negative rating of the child’s well-being on the BASES physical distress (p<0.01) and the BASES mood disturbance (p<0.01) scales. Similarly, the parents´ increased HADS depression score was significantly associated with their negative rating of the child’s well-being on the BASES physical distress (p<0.01) and BASES mood disturbance (p<0.01) scale. The association between the HADS anxiety and depression subscales was 0.74 (p<0.01). DISCUSSION We did not observe a significant effect of the intervention program when comparing the PPCG with the PIG. The increased level of anxiety (39%) and depression (24%) among parents at admission indicates that involvement in the child’s HSCT affected them profoundly despite comprehensive support provided by the public social and health system. This finding is in agreement with other studies showing that 18-66% of parents experiencing an increased level of anxiety at the time of the

9
child’s admission (3;5;6). Likewise, the level of depression observed in other studies indicates that 8-35% of parents have an increased level of depression symptoms at admission (1;3;4;6;42). We tested a multi-facetted supportive intervention program targeting parents to children treated with HSCT. The intervention components aimed at supporting the parents’ caregiving abilities and their social, emotional and medical information needs during the child’s 4-6 weeks HSCT inpatient period. The three different approaches used were: 1). Daily FNN parental guidance in which problem-solving techniques inspired by congnitive behavioral therapy, were included in addressing the parents’ caregiving related problems. This included support in identifying problems affecting their childcare, defining and evaluating possible solutions, installing actions and evaluating the effect of their actions. This intervention component was well accepted and performed in 92% of the expected intervention days. 2) The supervised-structured education program introduced various problem solving skills e.g. from a more theoretical approach of influencing thoughts (cognitive behavioural model) (28-30) to practical ideas for possible action. The education program was completed by 72% of the parents. 3) The physical activity program offered parents the possibility of distraction by cycling/walking outside of the hospital. This program was not well accepted and was completed by only 16% of the parents. In the present study we did not perform the problem-solving support intervention as scheduled training sessions (2;43;44); or as a psychotherapeutic intervention program (2). Such programs have been tested in other populations with various effects. It was therefore possible to assume a more structured approach would prove effective in the current study. During the HSCT treatment, the parents faced multiple interrelated complex problems, including reorganization of the family’s daily life to meet the needs of the treatment, healthy siblings, financial strains, etc. (20-22). These types of problems are more manageable than emotional problems with the support of problem-solving skills. Therefore, it is possible that the problems-solving techniques were used to a larger degree to address financial and social network problems than emotional reactions such as anxiety and depression. This notion is supported by Larsen et al.’s (21;22) findings within this population and by Bevans et al.(43) among caregivers to adults HSCT patients. The parents may have found it difficult to applying problem-solving techniques to address their depression and anxiety due to the interrelatedness of their anxiety with the threat the disease and treatment posed on the child’s life (9;45). This threat was constant throughout the HSCT period but decreased with time following the transplant. As such, to some parents the emotional strain was transitory which may explain the significant decrease in their anxiety and depression scores from baseline to day 100 in both the PPCG and the PIG. This finding is in line with findings in other studies (5;6;46) showing that the parents’ levels of anxiety and depression peaked at the time of the child’s admission. Despite this decrease, the number of parents with increased anxiety (22%) and depression (11%) scores at day 100 was still above the level in the general population (47) In a secondary analysis, we found that parents with a relative low level of anxiety at baseline benefited from the intervention program. These parents’ may have used problem-solving skills prior to admission, explaining the significance found in this group. However, this finding needs to be confirmed in other studies. In this study we included the POMS and CHIP questionnaires to be able to provide further elaboration of the parents’ emotional well-being and coping styles, related to the effect of the intervention program. However, the parents sparsely completed these questionnaires during the study which is why further analysis is not possible. In this study 25% of the of families were bilingual (one or both parents having Danish as their second language) (21). These parents found it difficult to differentiate some of positive and negative adjectives used in POMS and the wording of questions in CHIP. This may explain why these questionnaires were sparsely completed compared with the satisfactory completion of the HADS and BASES.
10
The strength of this study is the inclusion of all eligible parents to HSCT children in Denmark Access to only a small sample size, however, limited our study. Our study did not use randomization but two control groups and the PCG, which included only eight parents. However, a small sample size is a well-known challenge in the HSCT field, affecting the possibility of drawing conclusions based on controlled trials. To achieve access to a larger sample size and to reach sufficient statistical power would call for a multi-center trial. It is, however, difficult to perform this type of trial due to national differences in treatment protocols, access to health services and culture. In conclusion, in this first controlled intervention study that aimed to assist parents in managing their anxiety and depression during their child’s HSCT treatment, we did not observe an overall effect of the intervention. Results show that during the child’s HSCT treatment the parents experienced a considerable level of anxiety and depression which decreased after the HSCT treatment. In addition, the support care interventions seemed to benefit parents with a low level of anxiety at baseline. Future large-scale studies may apply this intervention model as an outset for further development of intervention models in order to benefit parents of HSCT children. Conflict of interest The authors declare no conflict of interest. Acknowledgements Danish Cancer Foundation for Children, Danish Health Foundation, Lundbeck Foundation, Gangsted Foundation, Copenhagen University Hospital [Rigshospital] supported this study.

11
Reference List
(1) Manne S, DuHamel K, Ostroff J, Parsons S, Martini DR, Williams SE, et al. Anxiety, depressive, and posttraumatic stress disorders among mothers of pediatric survivors of hematopoietic stem cell transplantation. Pediatrics 2004 Jun;113(6):1700-8.
(2) Streisand R, Rodrigue JR, Houck C, Graham-Pole J, Berlant N. Brief report: parents of children undergoing bone marrow transplantation: documenting stress and piloting a psychological intervention program. J Pediatr Psychol 2000 Jul;25(5):331-7.
(3) Manne S, Nereo N, DuHamel K, Ostroff J, Parsons S, Martini R, et al. Anxiety and depression in mothers of children undergoing bone marrow transplant: symptom prevalence and use of the Beck depression and Beck anxiety inventories as screening instruments. J Consult Clin Psychol 2001 Dec;69(6):1037-47.
(4) Manne S, DuHamel K, Ostroff J, Parsons S, Martini DR, Williams SE, et al. Coping and the course of mother's depressive symptoms during and after pediatric bone marrow transplantation. J Am Acad Child Adolesc Psychiatry 2003 Sep;42(9):1055-68.
(5) Nelson AE, Miles MS, Belyea MJ. Coping and support effects on mothers' stress responses to their child's hematopoietic stem cell transplantation. J Pediatr Oncol Nurs 1997 Oct;14(4):202-12.
(6) Barrera M, Boyd-Pringle LA, Sumbler K, Saunders F. Quality of life and behavioral adjustment after pediatric bone marrow transplantation. Bone Marrow Transplant 2000 Aug;26(4):427-35.
(7) Vrijmoet-Wiersma CM, Egeler RM, Koopman HM, Norberg AL, Grootenhuis MA. Parental stress before, during, and after pediatric stem cell transplantation: a review article. Support Care Cancer 2009 Dec;17(12):1435-43.
(8) Packman W, Weber S, Wallace J, Bugescu N. Psychological effects of hematopoietic SCT on pediatric patients, siblings and parents: a review. Bone Marrow Transplant 2010 Jul;45(7):1134-46.
(9) Grootenhuis MA, Last BF. Adjustment and coping by parents of children with cancer: a review of the literature. Support Care Cancer 1997 Nov;5(6):466-84.
(10) Oppenheim D, Valteau-Couanet D, Vasselon S, Hartmann O. How do parents perceive high-dose chemotherapy and autologous stem cell transplantation for their children. Bone Marrow Transplant 2002 Jul;30(1):35-9.
(11) Cooper LJ. New approaches to allogeneic hematopoietic stem cell transplantation in pediatric cancers. Curr Oncol Rep 2009 Nov;11(6):423-30.
(12) Jenq RR, van den Brink MR. Allogeneic haematopoietic stem cell transplantation: individualized stem cell and immune therapy of cancer. Nat Rev Cancer 2010 Mar;10(3):213-21.
12
(13) Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med 2006 Apr 27;354(17):1813-26.
(14) Jobe-Shields L, Alderfer MA, Barrera M, Vannatta K, Currier JM, Phipps S. Parental depression and family environment predict distress in children before stem cell transplantation. J Dev Behav Pediatr 2009 Apr;30(2):140-6.
(15) Phipps S, Barrera M, Vannatta K, Xiong X, Doyle JJ, Alderfer MA. Complementary therapies for children undergoing stem cell transplantation: report of a multisite trial. Cancer 2010 Aug 15;116(16):3924-33.
(16) Clarke SA, Eiser C, Skinner R. Health-related quality of life in survivors of BMT for paediatric malignancy: a systematic review of the literature. Bone Marrow Transplant 2008 Jul;42(2):73-82.
(17) Phipps S, Dunavant M, Garvie PA, Lensing S, Rai SN. Acute health-related quality of life in children undergoing stem cell transplant: I. Descriptive outcomes. Bone Marrow Transplant 2002 Mar;29(5):425-34.
(18) Lesko LM. Bone marrow transplantation: support of the patient and his/her family. Support Care Cancer 1994 Jan;2(1):35-49.
(19) Mayer DK, Tighiouart H, Terrin N, Stewart S, Peterson E, Jeruss S, et al. A brief report of caregiver needs and resource utilization during pediatric hematopoietic stem cell transplantation. J Pediatr Oncol Nurs 2009 Jul;26(4):223-9.
(20) Moore CW, Rauch PK. Addressing parenting concerns of bone marrow transplant patients: opening (and closing) Pandora's box. Bone Marrow Transplant 2006 Dec;38(12):775-82.
(21) Larsen H.B., Heilmann C, Johansen C, Adamsen L. Socially disadvantaged parents of children treated with allogeneic haematopoietic stem cell transplantation (HSCT): Report from a controlled intervention study, Denmark. 2011. Ref Type: Unpublished Work
(22) Larsen HB, Heilmann C, Johansen C, Adamsen L. An analysis of parental roles during
haematopoietic stem cell transplantation of their offspring: a qualitative and participant observational study. J Adv Nurs 2011 Feb 16.
(23) Heilmann C. 2011. Ref Type: Personal Communication
(24) Danmark: familieforhold (Denmark: family conditions), Den Store Danske - Gyldendals
åbne encyklopædi [Online]. http://www.denstoredanske.dk/index.php?sideId=61047 . 2001. Gyldendal . Ref Type: Online Source
(25) Freeman HP. Patient navigation: a community based strategy to reduce cancer disparities. J
Urban Health 2006 Mar;83(2):139-41.

13
(26) Robinson-White S, Conroy B, Slavish KH, Rosenzweig M. Patient navigation in breast cancer: a systematic review. Cancer Nurs 2010 Mar;33(2):127-40.
(27) Swanson J, Koch L. The role of the oncology nurse navigator in distress management of adult inpatients with cancer: a retrospective study. Oncol Nurs Forum 2010 Jan;37(1):69-76.
(28) Beck AT. Cognitive therapy and the emotional disorders. New York: Meridian Book; 1979.
(29) Beck AT, Emery G, Greenberg RL. Anxiety disorders and phobias a cognitive perspective. 15th anniversary ed ed. New York: Basic Books; 2005.
(30) Beck JS. Cognitive therapy for challenging problems what to do when the basics don't work. New York: Guilford Press; 2005.
(31) Martinsen. Kropp og sinn. 2005;2. oppl.
(32) Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry 2005 Mar;18(2):189-93.
(33) Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983 Jun;67(6):361-70.
(34) Phipps S, Hinds PS, Channell S, Bell GL. Measurement of behavioral, affective, and somatic responses to pediatric bone marrow transplantation: development of the BASES scale. J Pediatr Oncol Nurs 1994 Jul;11(3):109-17.
(35) Phipps S, Dunavant M, Jayawardene D, Srivastiva DK. Assessment of health-related quality of life in acute in-patient settings: use of the BASES instrument in children undergoing bone marrow transplantation. Int J Cancer Suppl 1999;12:18-24.
(36) McNair P.M, Lorr M, Doppelman L. Profile of Mood States Manual. 1971. San Diego, Education and Industrial Testing Service. Ref Type: Online Source
(37) McCubbin HI, McCubbin MA, Patterson JM, Cauble AE, Wilson LR, Warwick W. CHIP-
Coping Health Inventory for Parents: An Assessment of Parental Coping Patterns in the Care of the Chronically Ill Child. Journal of Marriage and Family 1983 May;45(2):359-70.
(38) Cull A., Spangers M, Bjordal K, Aaronson N, West K, Bottomley. EORTC Qualtiy Of Life Group Transplantation Procedure . [Second Edition]. 2002. Ref Type: Online Source
(39) Hunt SM, Bhopal R. Self report in clinical and epidemiological studies with non-English
speakers: the challenge of language and culture. J Epidemiol Community Health 2004 Jul;(58:):618-22.
(40) Crawford JR, Henry JD, Crombie C, Taylor EP. Normative data for the HADS from a large non-clinical sample. Br J Clin Psychol 2001 Nov;40(Pt 4):429-34.
(41) R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. 2011. Vienna, Austria. Ref Type: Online Source
14
(42) Nelson AE, Gleaves L, Nuss S. Mothers' responses during the child's stem cell transplantation: pilot study. Pediatr Nurs 2003 May;29(3):219-23.
(43) Bevans M, Castro K, Prince P, Shelburne N, Prachenko O, Loscalzo M, et al. An individualized dyadic problem-solving education intervention for patients and family caregivers during allogeneic hematopoietic stem cell transplantation: a feasibility study. Cancer Nurs 2010 Mar;33(2):E24-E32.
(44) Sahler OJ, Fairclough DL, Phipps S, Mulhern RK, Dolgin MJ, Noll RB, et al. Using problem-solving skills training to reduce negative affectivity in mothers of children with newly diagnosed cancer: report of a multisite randomized trial. J Consult Clin Psychol 2005 Apr;73(2):272-83.
(45) Melnyk BM. Intervention studies involving parents of hospitalized young children: an analysis of the past and future recommendations. J Pediatr Nurs 2000 Feb;15(1):4-13.
(46) Phipps S, Dunavant M, Lensing S, Rai SN. Patterns of distress in parents of children undergoing stem cell transplantation. Pediatr Blood Cancer 2004 Sep;43(3):267-74.
(47) Groenvold M, Fayers PM, Sprangers MA, Bjorner JB, Klee MC, Aaronson NK, et al. Anxiety and depression in breast cancer patients at low risk of recurrence compared with the general population: a valid comparison? J Clin Epidemiol 1999 Jun;52(6):523-30.

15
Table 1: Weekly intervention schedule for parents in a Family Navigator Nurse (FNN) conducted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark
Monday Tuesday Wednesday Thursday Friday Family Navigator Nurse
intervention 1 hour
Family Navigator Nurse intervention
1 hour
Family Navigator Nurse intervention
1 hour
Family Navigator Nurse intervention
1 hour
Family Navigator Nurse intervention
1 hour Physical Activity
1 hour Physical Activity
1 hour Physical Activity
1 hour Education Program
1 hour
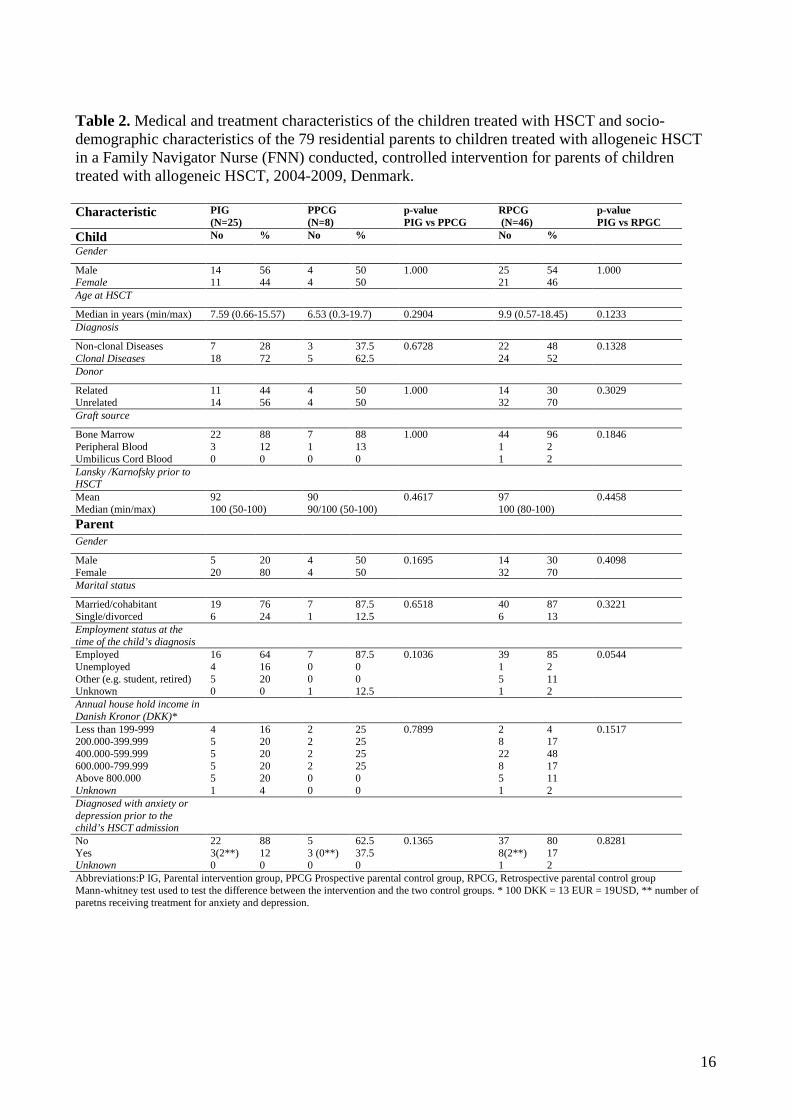
16
Table 2. Medical and treatment characteristics of the children treated with HSCT and socio-demographic characteristics of the 79 residential parents to children treated with allogeneic HSCT in a Family Navigator Nurse (FNN) conducted, controlled intervention for parents of children treated with allogeneic HSCT, 2004-2009, Denmark. Characteristic PIG
(N=25) PPCG (N=8)
p-value PIG vs PPCG
RPCG (N=46)
p-value PIG vs RPGC
Child No % No % No % Gender
Male Female
14 11
56 44
4 4
50 50
1.000 25 21
54 46
1.000
Age at HSCT
Median in years (min/max) 7.59 (0.66-15.57) 6.53 (0.3-19.7) 0.2904 9.9 (0.57-18.45) 0.1233 Diagnosis
Non-clonal Diseases Clonal Diseases
7 18
28 72
3 5
37.5 62.5
0.6728 22 24
48 52
0.1328
Donor
Related Unrelated
11 14
44 56
4 4
50 50
1.000 14 32
30 70
0.3029
Graft source
Bone Marrow Peripheral Blood Umbilicus Cord Blood
22 3 0
88 12 0
7 1 0
88 13 0
1.000 44 1 1
96 2 2
0.1846
Lansky /Karnofsky prior to HSCT
Mean Median (min/max)
92 100 (50-100)
90 90/100 (50-100)
0.4617 97 100 (80-100)
0.4458
Parent
Gender
Male Female
5 20
20 80
4 4
50 50
0.1695 14 32
30 70
0.4098
Marital status
Married/cohabitant Single/divorced
19 6
76 24
7 1
87.5 12.5
0.6518 40 6
87 13
0.3221
Employment status at the time of the child’s diagnosis
Employed Unemployed Other (e.g. student, retired) Unknown
16 4 5 0
64 16 20 0
7 0 0 1
87.5 0 0 12.5
0.1036 39 1 5 1
85 2 11 2
0.0544
Annual house hold income in Danish Kronor (DKK)*
Less than 199-999 200.000-399.999 400.000-599.999 600.000-799.999 Above 800.000 Unknown
4 5 5 5 5 1
16 20 20 20 20 4
2 2 2 2 0 0
25 25 25 25 0 0
0.7899 2 8 22 8 5 1
4 17 48 17 11 2
0.1517
Diagnosed with anxiety or depression prior to the child’s HSCT admission
No Yes Unknown
22 3(2**) 0
88 12 0
5 3 (0**) 0
62.5 37.5 0
0.1365 37 8(2**) 1
80 17 2
0.8281
Abbreviations:P IG, Parental intervention group, PPCG Prospective parental control group, RPCG, Retrospective parental control group Mann-whitney test used to test the difference between the intervention and the two control groups. * 100 DKK = 13 EUR = 19USD, ** number of paretns receiving treatment for anxiety and depression.

17
Table 3: Mean HADS, BASES, POMS, CHIP baseline data of 79 parents in a FNN concucted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark PIG PPCG RPGC
Measure PIG v PPCG
PIG v RPCG
Mean SEM STD Mean SEM STD p Mean SEM STD p HADS Anxiety 9.5 0.95 4.44 10.29 1.16 4.23 0.49 10.34 0.74 4.9 0.58 Depression 7.5 0.92 4.53 6.5 2.17 6.14 0.48 7.28 0.72 4.73 0.82 BASES - Parent Physical distress 8.79 0.85 4.15 8.57 2.15 5.68 0.53 16.81 0.77 5.06 0.00 Compliance 8.13 0.77 3.7 6.62 0.88 2.5 0.32 9.61 0.7 4.29 0.15 Mood disturbance 14.46 1.3 6.38 13.0 1.94 5.13 0.69 18.38 0.93 5.9 0.02 Quality of interaction 5.12 0.36 1.75 4.29 0.6 1.6 0.28 5.59 0.3 1.94 0.37 Activity 5.83 0.28 1.37 5.75 0.25 0.71 0.88 5.83 0.29 1.33 0.81 BASES - Child Physical distress 7.31 0.72 2.89 9.2 2.8 6.26 N/A 16.68 1.05 6.11 N/A Compliance 6.12 0.4 1.65 7.4 1.12 2.51 N/A 9.36 0.67 3.84 N/A Mood disturbance 9.35 0.64 2.62 10.4 1.63 3.65 N/A 14.76 1.1 6.32 N/A Quality of interaction 4.06 0.37 1.52 4.4 0.68 1.52 N/A 5.15 0.38 1.52 N/A Activity 5.82 0.29 1.19 6.2 0.73 1.64 N/A 4.56 0.25 1.44 N/A POMS Tension 6.57 0.83 3.99 6.62 1.72 4.87 0.92 9.24 0.82 5.53 0.06 Depression 4.17 0.75 3.36 4.75 1.36 3.85 0.74 6.02 0.76 5.07 0.2 Anger 4.5 0.66 3.22 4.12 0.89 2.53 0.89 4.93 0.72 4.87 0.72 Vigor 7.67 0.83 4.09 6.86 1.71 4.53 0.67 8.11 0.61 4.03 0.81 Fatigue 5.88 0.73 3.53 6.5 2.15 6.09 0.89 7.49 0.82 5.47 0.36 Confusion 4.96 0.57 2.8 4.75 1.0 2.82 0.89 5.19 0.55 3.59 0.74 CHIP Family integration 33 4.93 8.54 40.33 1.45 2.52 0.4 34.21 1.37 5.95 0.67 Social support 35.25 3.86 7.72 39.67 2.67 4.62 0.34 34.11 1.31 5.57 0.98 Communication 14 1.53 2.65 17 2 2.83 0.5 14 1.01 4.84 1.0 Abbreviations: HADS, Hospital Anxiety and Depression Scale, BASES, Behavioural, Affective and Somatic Experience Scale, POMS, Profile of Mood States-B, CHIP, Coping Health Index for Parents, PIG, Parental intervention group, PPCG Prospective parental control group, RPCG, Retrospective parental control group STD, Standard Deviation, SEM, Standard Error of Means; Mann-whitney test used to test the difference between the intervention and the two control groups. Table 4: Mean of changes from baseline in HADS scores at day 7, day 14 and day 100 following a child HSCT in a FNN conducted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark Day +14 Day +100 PIG PPCG PIG PPCG Scale HADS
Mean change
STD p Mean change
STD p Mean change
STD p Mean change
STD p
Anxiety -2.04 0.76 0.01 -1.87 1.1 0.09 -1.87 0.64 0.00 -4.16 1.1 0.00 Depression -0.38 0.66 0.56 0.53 0.95 0.58 ´1.41 0.57 0.01 -0.9 0.95 0.35 Abbreviations: HADS, Hospital Anxiety and Depression Scale, PIG,parental intervention group, PPCG Prospective parental control group, STD, Standard Deviation

18
Figure 1 shows a diagram of the inclusion process for parents in a Family Navigator Nurse (FNN) conducted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark.
Excluded: n=6 0-18 years, no residential parent: n=2 18-19.9 years, no residential parent: n=1 ICU treatment: n=2 (died: day +1, day +48) Language barriers: n=1
Parents approached: n=25 All included
Lost to follow-up: n=4 Drop out: n=1 Relapse: n=1 Died before day +100: n=2 (day +31, day +50)
Day +100 Follow-up: n=21
Parental intervention group: n=31 Parents to child 0-19.9 years Scheduled HSCT: Nov 1, 2007–Oct 31, 2009
Excluded: n=2 0-18 years, no residential parent: n=2
Day +100 Follow-up: n=6
Parents approached: n=8 All included
Lost to follow-up: n=2 Died before day +100: n=2 (day +10, day +57)
Prospective parental control group: n=10 Parents to child 0-19.9 years Scheduled HSCT: Jul 1, 2007–Oct 31, 2007
Parents approached: n=57 By mail questionnaires
Excluded: n=5 0-18 years, no residential parent: n=1 18-19.9 years: no residential parent: n=3 Intensive care unit (ICU) treatment: n=1
Excluded: n=11 Declined to participate: n=2 Did not respond: n=9
Parents included: n=46 Response rate: 81% Qualitative interviews: n=7 (Pilot study)
Retrospective parental control group: n=62 Parents as primary caregiver to child 0-19.9 years, alive HSCT: Jan 1, 2004–Jun 30, 2007

19
Figure 2 shows the intervention program and data collection schedule for parents included in a Family navigator Nurse (FNN) conducted controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark.
Admission HSCT
Day 100 HADS, BASES POMS CHIP Semi-structured interviews
Day -7 (Baseline) Demographic HADS, BASES, POMS, CHIP
Day 0 HADS, BASES.POMS CHIP
Day 7 HADS, BASES POMS CHIP
Day 14 HADS, BASES POMS CHIP
Day 21 HADS, BASES POMS CHIP
Day 28 HADS, BASES POMS CHIP
HADS, BASES POMS CHIP
Pre-eksamination Informed consent
Abbreviations and legends:
FNN = Family Navigator Nurse intervention (1 hour)
FNN & P = Family Navigator Nurse intervention and Physical Activity (2 hours)
FNN & E = Family Navigator Nurse intervention and Education Program (2 hours)
Demographic = Demographic Questionnaire
HADS = Hospital Anxiety and Depression Scale
BASES = Behavioural, Affective and Somatic Experience Scale
Discharge
Admission
Figure 3 shows the estimated change on the HADS anxiety scale compared to the baseline level for the PIG and the PPCG of parents in a Family Navigator Nurse (FNN) conducted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark. The bars represent 95 % confidence intervals for the change. Significant reductions were found for the intervention group at day 0 (p=0.02), day 14 (p=0.01), day 21 (p=0.02) and day 100 (p=0.01). For the PPCG there was a significant decrease from baseline to day 100 (p=0.01)
APPENDIX A
FNN Logbook
Semistructured interviewguide control group
Semistructured interviewguide intervention group
Questionnaires:
• Socio-Demographic questionnaire • HADS • POMS • BASES • CHIP
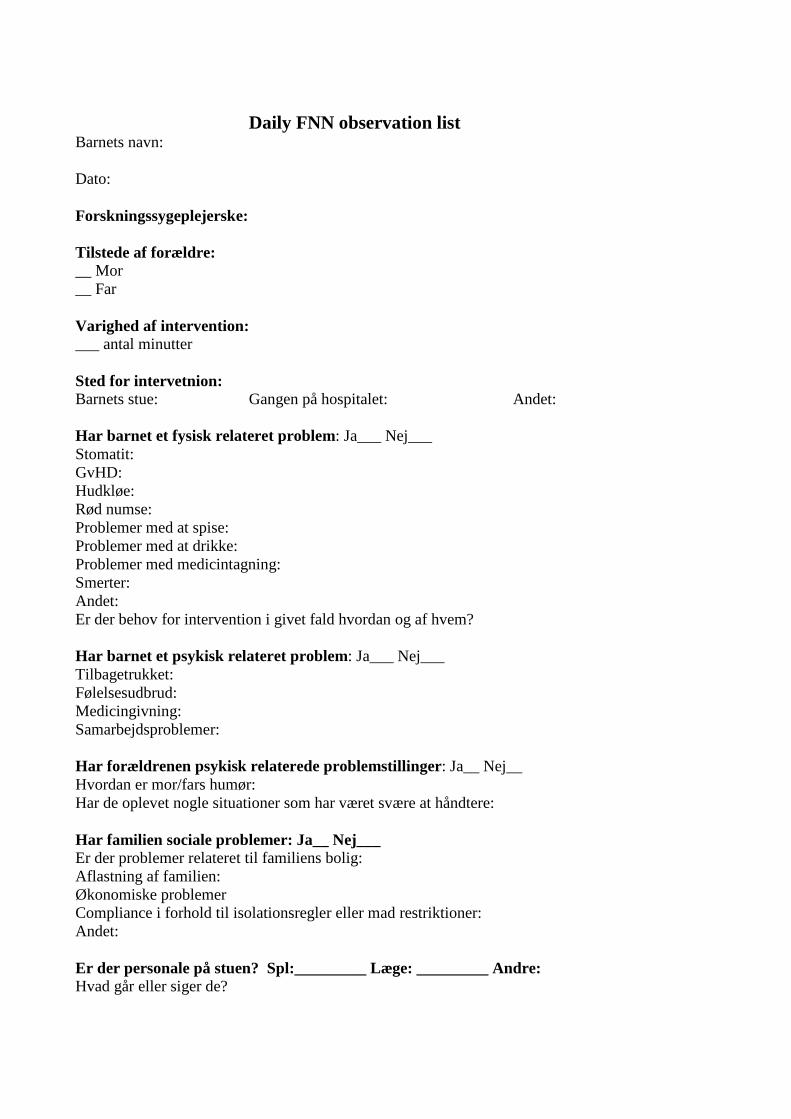
Daily FNN observation list Barnets navn: Dato: Forskningssygeplejerske: Tilstede af forældre: __ Mor __ Far Varighed af intervention: ___ antal minutter Sted for intervetnion: Barnets stue: Gangen på hospitalet: Andet: Har barnet et fysisk relateret problem: Ja___ Nej___ Stomatit: GvHD: Hudkløe: Rød numse: Problemer med at spise: Problemer med at drikke: Problemer med medicintagning: Smerter: Andet: Er der behov for intervention i givet fald hvordan og af hvem? Har barnet et psykisk relateret problem: Ja___ Nej___ Tilbagetrukket: Følelsesudbrud: Medicingivning: Samarbejdsproblemer: Har forældrenen psykisk relaterede problemstillinger: Ja__ Nej__ Hvordan er mor/fars humør: Har de oplevet nogle situationer som har været svære at håndtere: Har familien sociale problemer: Ja__ Nej___ Er der problemer relateret til familiens bolig: Aflastning af familien: Økonomiske problemer Compliance i forhold til isolationsregler eller mad restriktioner: Andet: Er der personale på stuen? Spl:_________ Læge: _________ Andre: Hvad går eller siger de?
Hvad sker der på stuen, hvordan har barnet og forældrene det, er der noget som der skal tages hånd om til i morgen. Hvilke aftaler er der indgået. Daglige noter:
Interventionsundersøgelse – historisk kontrolgruppe Ph.d. studerende Hanne Bækgaard Laursen
1
Interventionsundersøgelse Interviewguide, kontrolgruppe
Da jeg ikke har været involveret i dit barns behandlingsforløb vil jeg gerne bede dig beskrive hvordan du/I har oplevet det. Det jeg specielt er interesseret i at din/jeres beskrivelse af hvorledes du/I har oplevet forløbet fra at dit/jeres barn blev diagnosticeret, den indledende behandling der ledte op til knoglemarvstransplantationen, selve transplantationsforløbet og til hvor I er i dag. Det jeg specielt er interesseret i at jeres hjælp til at finde ud af, er hvorledes man kan støtte og hjælpe såvel børn som forældre til at få en bedre hverdag under transplantationen. Indledningsvis vil jeg gerne have lov til at stille nogle baggrundsspørgsmål om jeres familie. Demografisk oplysningsspørgeskema.
1. Hvis I tænker tilbage, hvordan opdagede I at jeres barn var sygt? 2. Hvad gjorde I? 3. Hvor lang tid gik der fra I opdagede de første symptomer til at diagnosen blev
stillet? 4. Hvordan reagerede I på diagnosen? 5. Hvordan reagerede jeres barn på diagnosen? 6. Hvordan reagerede evt. søskende på diagnose? 7. Hvordan organiserede du/I jeres hverdag således at barnet kunne følge
behandlingen (orlov?, nedsat arbejdstid?, pasning af evt. søskende o.l.) 8. Havde du/I nogen personer omkring jer som støttede jer, og hvordan gjorde de det? 9. Hvornår kom det på tale at jeres barn skulle behandles med en
knoglemarvstransplantation? 10. Hvad var din/jeres umiddelbare tanker om det kommende transplantationsforløb? 11. Hvorledes har du/I forberedt jeg på dette? 12. Hvorledes har du/I forberedt barnet på dette? 13. Hvorledes har I organiseret jer som familie i forbindelse med transplantationen fx
har begge forældre orlov, hvor er evt. søskende. 14. Er der nogle ting du/I ville have forberedt anderledes, med den viden du/I har i dag? 15. Hvordan gik transplantationsforløbet? 16. Var du meget alene på barnets stue under transplantationsforløbet? 17. Har du haft mulighed for at forlade isolationsstuen og benyttede du dig af
muligheden? 18. Hvor aktiv har dit barn været under transplantationsforløbet? 19. Hvordan har din kontakt været til dit barn under transplantationsforløbet? 20. Har der været situationer hvor du/I oplevede at have uoverensstemmelser med
barnet undervejs, kan du evt. beskrive en sådan situation? 21. Hvad har været det sværeste for dig i forbindelse med transplantationsforløbet? 22. Hvad har været sværest for dit barn? 23. Hvordan håndterede du svære situationer? 24. Hvordan har din kontakt til sygeplejerskerne været? 25. Hvordan har barnets kontakt til sygeplejerskerne været? 26. Hvordan har din kontakt til lægerne været? 27. Hvordan har barnets kontakt til lægerne været?

Interventionsundersøgelse – historisk kontrolgruppe Ph.d. studerende Hanne Bækgaard Laursen
2
28. Hvad har fungeret godt i forbindelse med transplantationsforløbet? 29. Har du/I oplevet nogen plejerelaterede situationer som du/I synes har været
vanskelige at håndtere? (fx medicin administration, bad, mad og drikke, skiftning af forbinding o.l.)
30. Hvad mener du/I ville have kunne have hjulpet jer? 31. Har du/I oplevet nogen situationer som har været svære at håndtere
følelsesmæssigt? 32. Hvorledes mener du/I bedst at man kan støtte forældre i forbindelse med et barns
transplantationsforløb? 33. Hvorledes mener du/I bedst at man kan støtte et barn i forbindelse med et
transplantationsforløb? 34. Kan du nævne 5 ting som ville have enten hjulpet dig eller dit barn gennem
transplantationsforløbet?

Interventionsundersøgelse – Interventionsgruppe Ph.d. studerende Hanne Bækgaard Laursen
1
Interventionsundersøgelse Interviewguide, Interventionsgruppe
Jeg er interesseret i at høre din/jeres oplevelse af hvorledes du/I har oplevet transplantationsforløbet. Jeg er interesseret i din/jeres beskrivelse af hvorledes du/I har oplevet forløbet fra at dit/jeres barn blev diagnosticeret, den indledende behandling der ledte op til knoglemarvstransplantationen, selve transplantationsforløbet og til hvor I er i dag. Det jeg specielt er interesseret i at jeres hjælp til at finde ud af, er hvorledes man kan støtte og hjælpe såvel børn som forældre til at få en bedre hverdag under transplantationen.
1. Hvis I tænker tilbage, hvordan opdagede I at jeres barn var sygt? 2. Hvad gjorde I? 3. Hvor lang tid gik der fra I opdagede de første symptomer til at diagnosen blev
stillet? 4. Hvordan reagerede I på diagnosen? 5. Hvordan reagerede jeres barn på diagnosen? 6. Hvordan reagerede evt. søskende på diagnose? 7. Hvordan organiserede du/I jeres hverdag således at barnet kunne følge
behandlingen (orlov?, nedsat arbejdstid?, pasning af evt. søskende o.l.) 8. Havde du/I nogen personer omkring jer som støttede jer, og hvordan gjorde de det? 9. Hvornår kom det på tale at jeres barn skulle behandles med en
knoglemarvstransplantation? 10. Hvad var din/jeres umiddelbare tanker om det kommende transplantationsforløb? 11. Hvorledes har du/I forberedt jeg på dette? 12. Hvorledes har du/I forberedt barnet på dette? 13. Hvorledes har I organiseret jer som familie i forbindelse med transplantationen fx
har begge forældre orlov, hvor er evt. søskende. 14. Er der nogle ting du/I ville have forberedt anderledes, med den viden du/I har i dag? 15. Hvordan gik transplantationsforløbet? 16. Var du meget alene på barnets stue under transplantationsforløbet? 17. Har du haft mulighed for at forlade isolationsstuen og benyttede du dig af
muligheden? 18. Du/I har deltaget i en undersøgelse hvor du/I blev tilbudt at deltage i gåture og
cykeltræning, har I benyttet jer af dette tilbud? 19. Hvordan har tilbudet fungeret for jer i praksis, har I haft mulighed for at
deltage? 20. Hvis du/I skulle nævne nogle positive ting om aktivitetstilbudet, hvad kunne
det være ? 21. Hvis du/I skulle nævne nogle negative ting om aktivitetstilbudet, hvad kunne
det være? 22. Mener du/I at dette er det rigtige tilbud til forældre, eller ville du/I hellere have
haft en anden type af tilbud, som fx? 23. Hvor aktiv har dit barn været under transplantationsforløbet? 24. Hvad mener du/I har haft den største indflydelse på dit barns aktivitetsniveau
(barnets almene tilstand, tilbud til aktiviteter, holdning til hvor meget barnet kan fra fx personalets side)
25. Hvordan har din kontakt været til dit barn under transplantationsforløbet?

Interventionsundersøgelse – Interventionsgruppe Ph.d. studerende Hanne Bækgaard Laursen
2
26. Har der været situationer hvor du/I oplevede at have uoverensstemmelser med barnet undervejs, kan du evt. beskrive en sådan situation?
27. I forbindelse med denne undersøgelse er du/I blevet tilbudt undervisning i barnets reaktioner på sygdom og behandling. Har du haft mulighed for at deltage i den planlagte undervisning? (Hvis nej, hvorfor ikke?)
28. Har du kunnet anvende noget af den viden du har fået i forbindelse med undervisningen i forhold til hvorledes du/I har håndteret situationer hvor der har været uoverensstemmelser mellem dig og dit barn?
29. Hvilke anvisninger har fungeret bedst for dig i relation til dit barn? 30. Hvilke anvisninger har ikke fungeret for dig i relation til dit barn? 31. Er der områder som du mener at undervisningen ikke har dækket, men som
ville have nyttigt for at lette transplantationsforløbet, som fx? 32. Er der områder af undervisningen som ikke har været relevant for dig? 33. Hvad har været det sværeste for dig i forbindelse med transplantationsforløbet? 34. Hvad har været sværest for dit barn? 35. Hvordan håndterede du svære situationer? 36. Hvordan har din kontakt til sygeplejerskerne været? 37. Hvordan har barnets kontakt til sygeplejerskerne været? 38. Hvordan har din kontakt til lægerne været? 39. Hvordan har barnets kontakt til lægerne været? 40. I forbindelse med denne undersøgelse er du/I blevet tilbudt at den
projektansvarlige sygeplejerske, kom hverdag, har du/I benyttet jer af dette tilbud?
41. Hvordan har det fungeret? 42. Hvorledes har I benyttet den projektansvarlige sygeplejerske? 43. Har det været en støtte for jer? 44. Har det været en støtte for jeres barn? 45. Har det været en belastning at have en ekstra person involveret i barnets
forløb? 46. Hvad mener du/I er det vigtigste som den projektansvarlige sygeplejerske har
gjort for jer? 47. Mener du at der er områder som den projektansvarlige sygeplejerske ikke har
dækket, men som hun med fordel kunne have involveret sig I? 48. Mener du at ordningen med en fast sygeplejerske, der følger jer gennem hele
transplantationsforløbet bør være en fast ordning? 49. Hvad har fungeret godt i forbindelse med transplantationsforløbet? 50. Har du/I oplevet nogen plejerelaterede situationer som du/I synes har været
vanskelige at håndtere? (fx medicin administration, bad, mad og drikke, skiftning af forbinding o.l.)
51. Hvad mener du/I ville have kunne have hjulpet jer? 52. Har du/I oplevet nogen situationer som har været svære at håndtere
følelsesmæssigt? 53. Hvorledes mener du/I bedst at man kan støtte forældre i forbindelse med et barns
transplantationsforløb? 54. Hvorledes mener du/I bedst at man kan støtte et barn i forbindelse med et
transplantationsforløb? 55. Kan du nævne 5 ting som ville have enten hjulpet dig eller dit barn gennem
transplantationsforløbet?



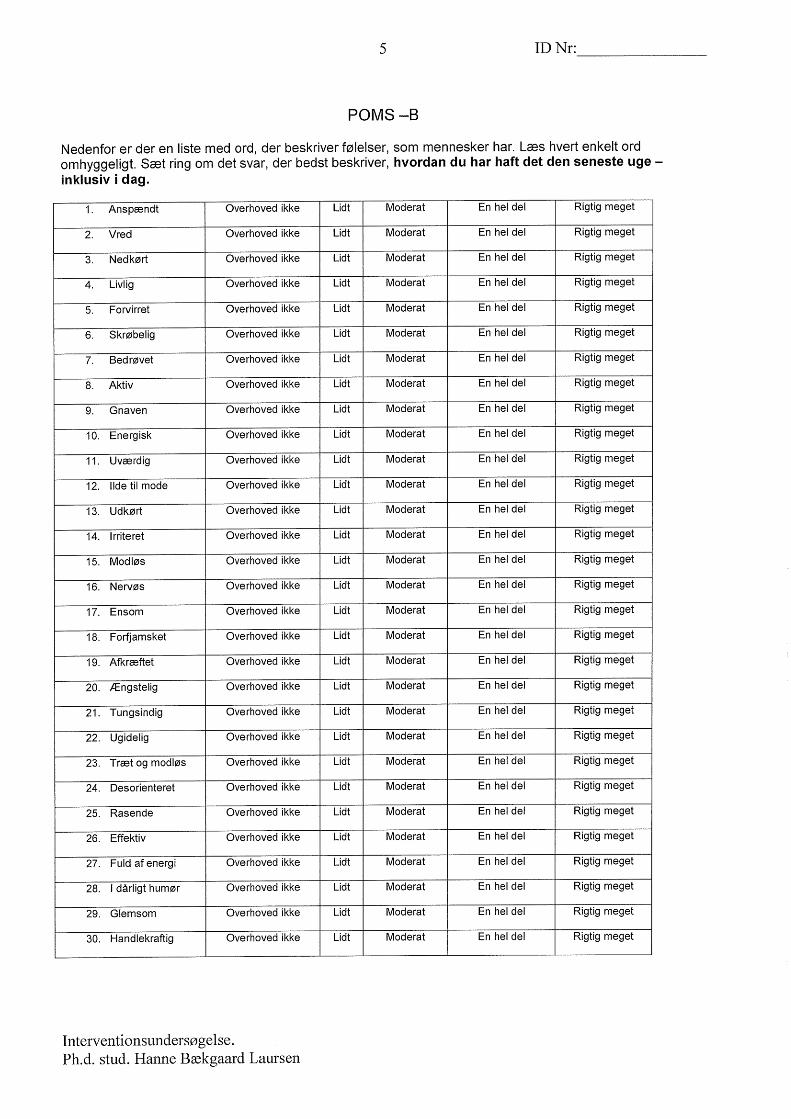
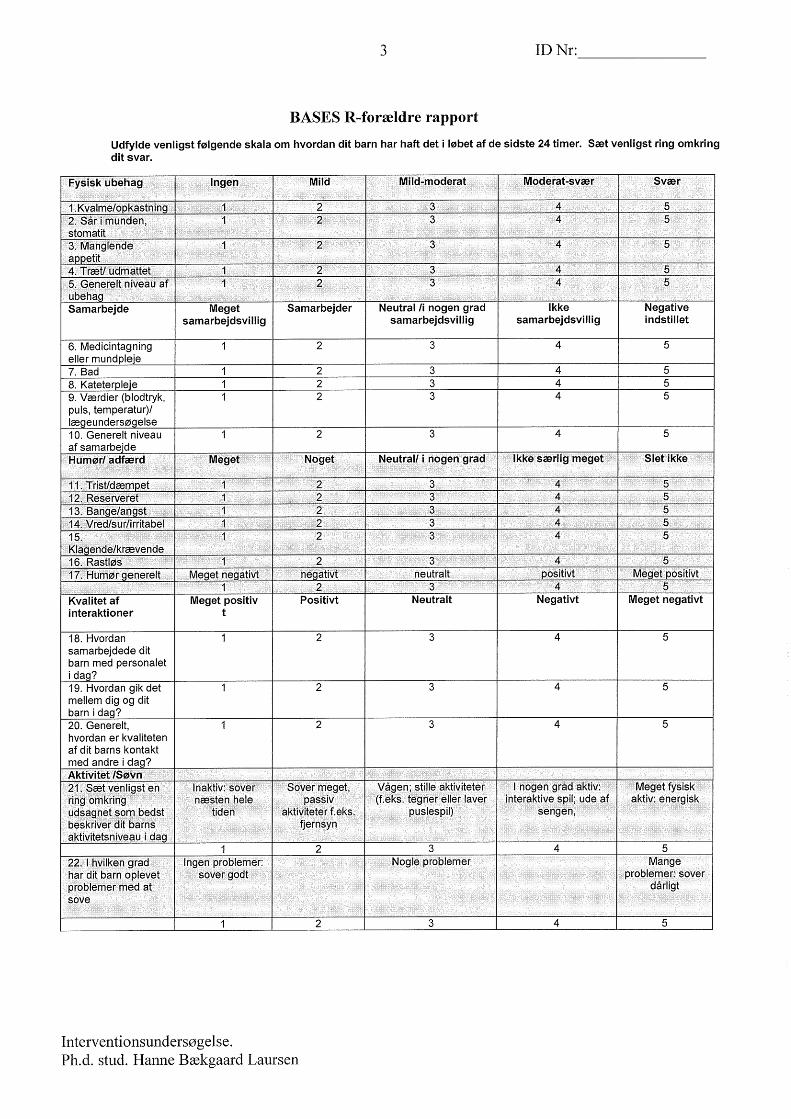
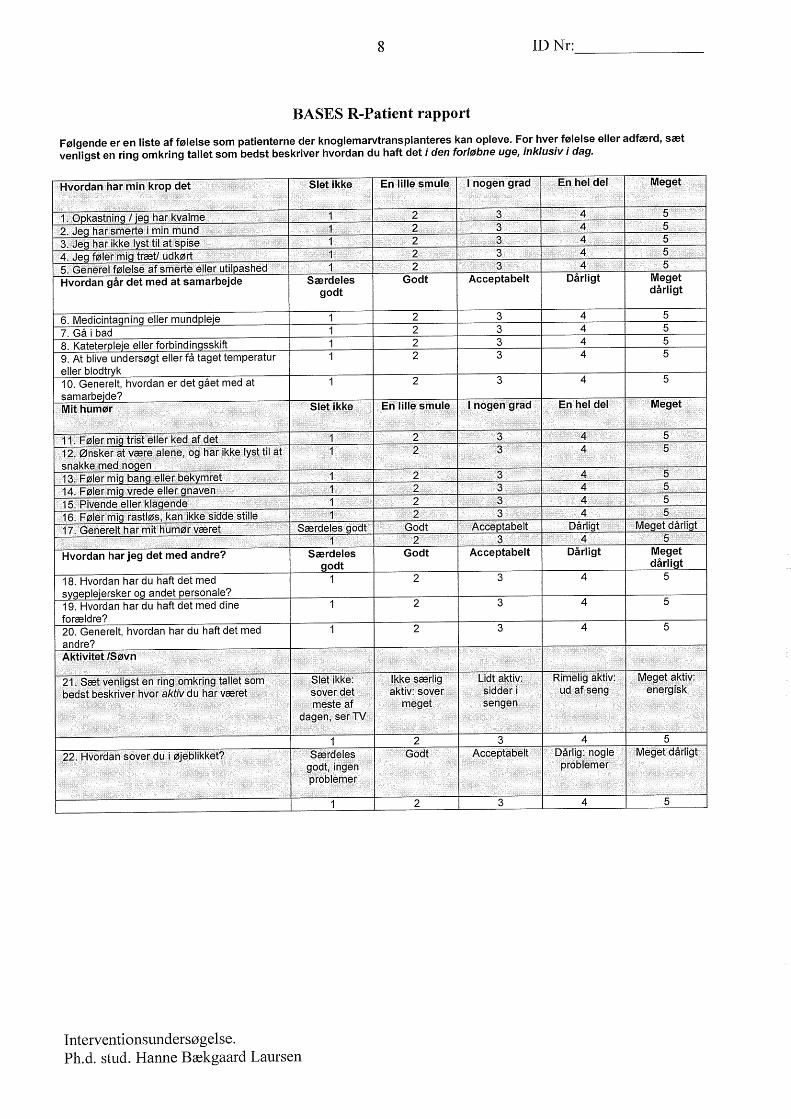



1
APPENDIX B Results of questionnaires: Baseline measurements and supplementary analyses:
• Socio-Demographic questionnaire • HADS • POMS • BASES • CHIP

2
Table 1. Medical and treatment characteristics of the children treated with HSCT and socio-demographic characteristics of the 79 residential parents to children treated with allogeneic HSCT in a Family Navigator Nurse (FNN) conducted, controlled intervention for parents of children treated with allogeneic HSCT, 2004-2009, Denmark. Characteristic PIG
(N=25) PPCG (N=8)
I vs PCG
RPCG (N=46)
I vs RGC
Child
Gender No % No % p No % p Male Female
14 11
56 44
4 4
50 50
1.000 25 21
54 46
1.000
Age at HSCT Median in years (min/max) 7.59 (0.66-15.57) 6.53 (0.3-19.7) 0.2904 9.9 (0.57-18.45) 0.1233 Diagnosis Non-clonal Diseases Clonal Diseases
7 18
28 72
3 5
37.5 62.5
0.6728 22 24
48 52
0.1328
Donor Related Unrelated
11 14
44 56
4 4
50 50
1.000 14 32
30 70
0.3029
Graft source Bone Marrow Peripheral Blood Umbilicus Cord Blood
22 3 0
88 12 0
7 1 0
88 13 0
1.000 44 1 1
96 2 2
0.1846
Lansky /Karnofsky prior to HSCT
Mean Median (min/max)
92 100 (50-100)
90 90/100 (50-100)
0.4617 97 100 (80-100)
0.4458
Parent
Gender Male Female
5 20
20 80
4 4
50 50
0.1695 14 32
30 70
0.4098
Marital status Married/cohabitant Single/divorced
19 6
76 24
7 1
87.5 12.5
0.6518 40 6
87 13
0.3221
Employment status at the time of the child’s diagnosis
Employed Unemployed Other (e.g. student, retired) Unknown
16 4 5 0
64 16 20 0
7 0 0 1
87.5 0 0 12.5
0.1036 39 1 5 1
85 2 11 2
0.0544
Annual house hold income in Danish Kronor (DKK)*
Less than 199-999 200.000-399.999 400.000-599.999 600.000-799.999 Above 800.000 Unknown
4 5 5 5 5 1
16 20 20 20 20 4
2 2 2 2 0 0
25 25 25 25 0 0
0.7899 2 8 22 8 5 1
4 17 48 17 11 2
0.1517
Diagnosed with anxiety or depression prior to the child’s HSCT admission
No Yes Unknown
22 3 0
88 12 0
5 3 0
62.5 37.5 0
0.1365 37 8 1
80 17 2
0.8281
Abbreviations: PIG,Parental Intervention Group, PPCG Prospective Parental Control Group, RPCG, Retrospective Parental Control Group Mann-whitney and test used to test the difference between the intervention and the two control groups.

3
Table 2: Mean HADS, BASES, POMS, CHIP baseline data of 79 parents in a FNN conducted, controlled intervention to parents of children treated with allogeneic HSCT, 2004-2009, Denmark PIG PPCG PRGC
Measure N=25
N=8
PIG v PPCG
N=46
PIG v RPCG
Mean SEM SD Mean SEM SD p Mean SEM SD p HADS Anxiety 9.5 0.95 4.44 10.29 1.16 4.23 0.49 10.34 0.74 4.9 0.58 Depression 7.5 0.92 4.53 6.5 2.17 6.14 0.48 7.28 0.72 4.73 0.82 BASES - Parent Physical distress 8.79 0.85 4.15 8.57 2.15 5.68 0.53 16.81 0.77 5.06 0.00 Compliance 8.13 0.77 3.7 6.62 0.88 2.5 0.32 9.61 0.7 4.29 0.15 Mood disturbance 14.46 1.3 6.38 13.0 1.94 5.13 0.69 18.38 0.93 5.9 0.02 Quality of interaction 5.12 0.36 1.75 4.29 0.6 1.6 0.28 5.59 0.3 1.94 0.37 Activity 5.83 0.28 1.37 5.75 0.25 0.71 0.88 5.83 0.29 1.33 0.81 BASES - Child Physical distress 7.31 0.72 2.89 9.2 2.8 6.26 N/A 16.68 1.05 6.11 N/A Compliance 6.12 0.4 1.65 7.4 1.12 2.51 N/A 9.36 0.67 3.84 N/A Mood disturbance 9.35 0.64 2.62 10.4 1.63 3.65 N/A 14.76 1.1 6.32 N/A Quality of interaction 4.06 0.37 1.52 4.4 0.68 1.52 N/A 5.15 0.38 1.52 N/A Activity 5.82 0.29 1.19 6.2 0.73 1.64 N/A 4.56 0.25 1.44 N/A POMS Tension 6.57 0.83 3.99 6.62 1.72 4.87 0.92 9.24 0.82 5.53 0.06 Depression 4.17 0.75 3.36 4.75 1.36 3.85 0.74 6.02 0.76 5.07 0.2 Anger 4.5 0.66 3.22 4.12 0.89 2.53 0.89 4.93 0.72 4.87 0.72 Vigor 7.67 0.83 4.09 6.86 1.71 4.53 0.67 8.11 0.61 4.03 0.81 Fatigue 5.88 0.73 3.53 6.5 2.15 6.09 0.89 7.49 0.82 5.47 0.36 Confusion 4.96 0.57 2.8 4.75 1.0 2.82 0.89 5.19 0.55 3.59 0.74 CHIP Family integration 33 4.93 8.54 40.33 1.45 2.52 0.4 34.21 1.37 5.95 0.67 Social support 35.25 3.86 7.72 39.67 2.67 4.62 0.34 34.11 1.31 5.57 0.98 Communication 14 1.53 2.65 17 2 2.83 0.5 14 1.01 4.84 1.0 Abbreviations: HADS, Hospital Anxiety and Depression Scale, BASES, Behavioural, Affective and Somatic Experience Scale, POMS, Profile of Mood States-B, CHIP, Coping Health Index for Parents, PIG, intervention group, PPCG Prospective control group, RPCG, Retrospective control group SEM, Standard Error of Means, SD, Standard Deviation Mann-whitney test used to test the difference between the intervention and the two control groups.
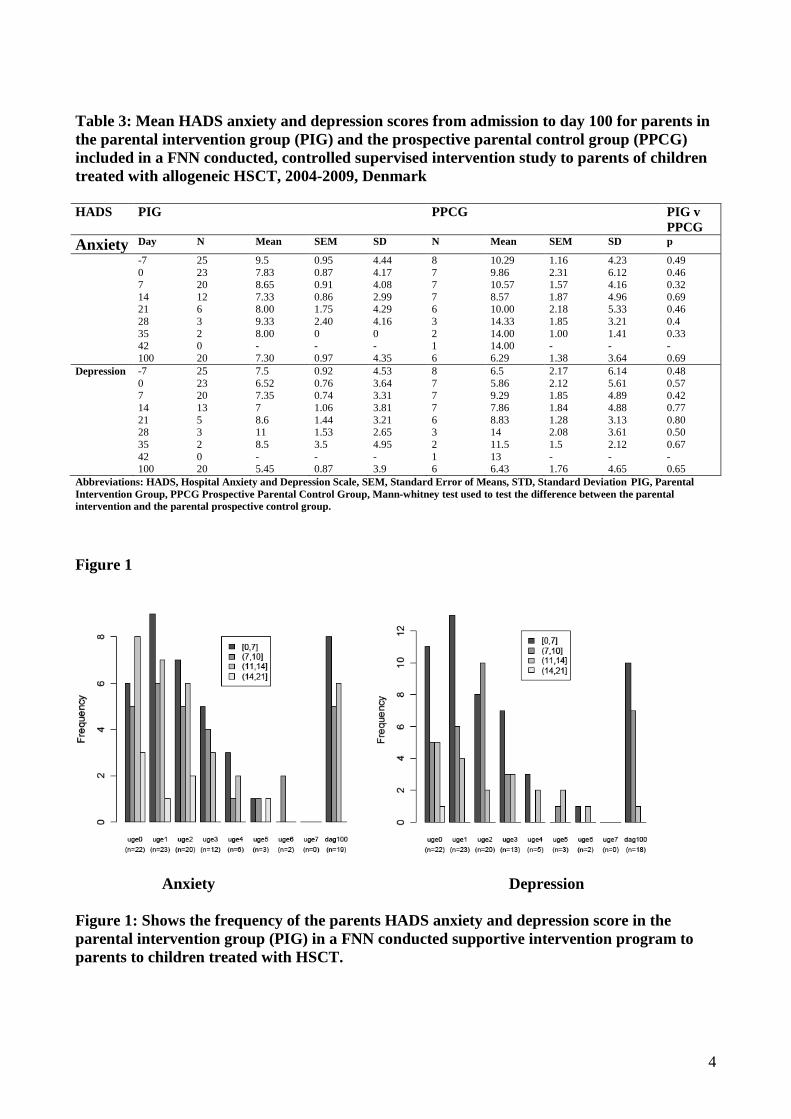
4
Table 3: Mean HADS anxiety and depression scores from admission to day 100 for parents in the parental intervention group (PIG) and the prospective parental control group (PPCG) included in a FNN conducted, controlled supervised intervention study to parents of children treated with allogeneic HSCT, 2004-2009, Denmark HADS PIG PPCG PIG v
PPCG Anxiety Day N Mean SEM SD N Mean SEM SD p
-7 25 9.5 0.95 4.44 8 10.29 1.16 4.23 0.49 0 23 7.83 0.87 4.17 7 9.86 2.31 6.12 0.46 7 20 8.65 0.91 4.08 7 10.57 1.57 4.16 0.32 14 12 7.33 0.86 2.99 7 8.57 1.87 4.96 0.69 21 6 8.00 1.75 4.29 6 10.00 2.18 5.33 0.46 28 3 9.33 2.40 4.16 3 14.33 1.85 3.21 0.4 35 2 8.00 0 0 2 14.00 1.00 1.41 0.33 42 0 - - - 1 14.00 - - - 100 20 7.30 0.97 4.35 6 6.29 1.38 3.64 0.69 Depression -7 25 7.5 0.92 4.53 8 6.5 2.17 6.14 0.48 0 23 6.52 0.76 3.64 7 5.86 2.12 5.61 0.57 7 20 7.35 0.74 3.31 7 9.29 1.85 4.89 0.42 14 13 7 1.06 3.81 7 7.86 1.84 4.88 0.77 21 5 8.6 1.44 3.21 6 8.83 1.28 3.13 0.80 28 3 11 1.53 2.65 3 14 2.08 3.61 0.50 35 2 8.5 3.5 4.95 2 11.5 1.5 2.12 0.67 42 0 - - - 1 13 - - - 100 20 5.45 0.87 3.9 6 6.43 1.76 4.65 0.65 Abbreviations: HADS, Hospital Anxiety and Depression Scale, SEM, Standard Error of Means, STD, Standard Deviation PIG, Parental Intervention Group, PPCG Prospective Parental Control Group, Mann-whitney test used to test the difference between the parental intervention and the parental prospective control group. Figure 1
Anxiety Depression
Figure 1: Shows the frequency of the parents HADS anxiety and depression score in the parental intervention group (PIG) in a FNN conducted supportive intervention program to parents to children treated with HSCT.

5
Table 4: Mean parent BASES scores of their children from admission to day 100 for parents in the parental intervention group (PIG) and the prospective parental control group (PPCG) included in a FNN conducted, controlled supervised intervention study to parents of children treated with allogeneic HSCT, 2004-2009, Denmark BASES Parent
PIG PPCG PIG v PPCG
Day N Mean SEM SD N Mean SEM SD p Physical distress -7 25 8.79 0.85 4.15 7 8.57 2.15 5.68 0.53 0 22 14.55 0.88 4.13 8 14.75 1.9 5.37 0.84 7 21 14.52 0.99 4.53 6 16.67 2.45 5.99 0.54 14 13 12.38 0.93 3.36 7 16.14 2.12 5.61 0.2 21 7 11 1.59 4.2 6 12.17 2.88 7.05 0.97 28 3 13 2.52 4.36 2 12 4 5.66 0.8 35 2 10.5 2.5 3.54 2 14 7 9.9 1 42 0 - - - 1 12 - - - 100 19 9.11 0.52 2.26 6 9.5 1.98 4.85 0.56 Compliance -7 25 8.13 0.77 3.7 20 6.62 0.88 2.5 0.32 0 20 9.4 1.01 4.52 7 8.86 2.22 5.87 0.63 7 18 9.17 1.04 4.4 7 9.43 1.34 3.55 0.71 14 12 7.83 0.85 2.95 7 8.86 1.28 3.39 0.54 21 5 10.2 2.35 5.26 6 7.83 1.72 4.22 0.57 28 3 7.67 0.88 1.53 3 11.67 5.66 9,81 1 35 1 12 - - 2 11.5 6.5 9.19 1 42 0 - - - 1 16 - - - 100 19 6.63 0.61 2.67 6 5.14 0.14 0.38 0.18 Mood disturbance -7 25 14.46 1.3 6.38 7 13.0 1.94 5.13 0.69 0 21 15.9 1.05 4.82 7 17.29 2.69 7.13 0.85 7 18 18.83 1.57 6.65 7 17.86 1.63 4.3 0.85 14 12 16.5 1.18 4.08 5 19 2.53 5.66 0.52 21 6 16.5 1.84 4.51 4 17.75 5.39 10.78 1 28 3 22.67 2.03 3.51 3 20.67 6.69 11.59 0.8 35 2 19 4 5.66 1 26 - - 0.67 42 0 - - - 1 18 - - - 100 20 14.8 1.55 6.91 6 13.14 1.64 4.34 0.76 Quality of interaction -7 25 5.12 0.36 1.75 8 4.29 0.6 1.6 0.28 0 23 6.22 0.43 2.04 8 5.62 0.84 2.39 0.43 7 21 7.1 0.43 2. 26 7 5.71 0.81 2.14 0.15 14 13 5.38 0.49 1.76 7 5.86 0.99 2.61 0.68 21 7 5.71 0.49 2.43 6 5 0.93 2.28 0.68 28 3 6.33 0.92 0.58 3 4.87 0.88 1.53 0.3 35 2 7.5 0.33 2.12 2 5.5 -2.5 3.54 0.67 42 0 - - - 1 6 - - - 100 19 5.05 0.52 2.27 6 3.83 0.54 1.33 0.27 Activity -7 25 5.83 0.28 1.37 8 5.75 0.25 0.71 0.88 0 22 4.36 0.3 1.4 8 4.5 0.38 1.07 0.79 7 20 4.45 0.34 1.5 7 4.43 0.48 1.27 0.93 14 13 5.15 0.4 1.46 7 4.14 0.4 1.07 0.22 21 7 5.29 0.29 0.76 6 5.33 0.67 1.63 0.93 28 3 6.33 0.33 0.58 3 4.33 1.45 2.52 0.5 35 2 6 1 1.41 2 7.5 0.5 0.71 0.67 42 0 - - - 1 6 - - - 100 20 5.3 0.16 0.73 6 6.14 0.4 1.07 0.07 Abbreviations: BASES, parent version: Behavioural, Affective and Somatic Experience Scale, SEM, Standard Error of Means, STD, Standard Deviation PIG, Parental Intervention Group, PPCG Prospective Parental Control Group Mann-whitney test used to test the difference between the intervention and the control group.

6
Table 5: The children’s mean BASES scores from admission to day 100 for children of parents included in the parental intervention group (PIG) and the prospective parental control group (PPCG) in a FNN conducted, controlled supervised intervention study to parents of children treated with allogeneic HSCT, 2004-2009, Denmark BASES Child
PIG PPCG PIG v PPCG
day N Mean SEM SD N Mean SEM SD p Physical distress -7 7.31 0.72 2.89 9.2 2.8 6.26 0 15 13.8 0.98 3,78 6 15.83 1.96 4.79 0.43 7 14 12.71 1.26 4.7 5 16.4 3.09 6.91 0.31 14 9 12.56 1.33 4 5 15.4 2.88 6.43 0.46 21 3 11 1.73 3 4 12.5 4.17 8.35 0.91 28 3 11.33 0.88 1.53 2 16 4 5.66 0.4 35 1 12 - - 1 20 - - 1 42 0 - - - 0 - - - - 100 19 8.42 0.46 2.01 5 9.8 2.16 4.82 0.91 Compliance -7 6.12 0.4 1.65 7.4 1.12 2.51 0.67 0 14 9.36 0.98 3.65 6 8.5 1.59 3.89 0.81 7 14 9.29 1.15 4.29 4 9.25 2.13 4.27 0.6 14 8 7.25 0.9 2.55 5 8.2 1.39 3.11 1 21 3 8.33 3.33 5.77 4 7.75 2.43 4.86 1 28 3 7.33 1.85 3.21 2 6 0 0 1 35 1 13 - - 1 5 - - - 42 0 - - - 0 - - - - 100 19 5.89 0.42 1.82 5 5.2 0.2 0.45 0.64 Mood disturbance -7 9.35 0.64 2.62 10.4 1.63 3.65 0 15 11.27 0.99 3.84 5 12 1.92 4.3 0-72 7 14 12.97 0.98 3.65 5 12.8 1.39 3.11 0.61 14 9 11.44 0.8 2.4 5 14.8 1.46 3.27 0.05 21 3 12.67 2.33 4.04 3 11.33 3.85 6.66 0.9 28 3 13.67 2.96 5.13 1 10 - - 1 35 2 13.5 1.5 2.12 1 15 - - - 42 0 - - - 0 - - - - 100 19 10.42 0.95 4.14 5 10.4 1.25 2.79 0.58 Quality of interaction -7 4.06 0.37 1.52 4.4 0.68 1.52 0 15 5.73 0.45 1.75 6 5.33 0.99 2.42 0.72 7 14 6.21 0.51 1.89 5 6 1.27 2.83 0.75 14 9 5.89 0.63 1.9 5 5.4 1.12 2.51 0.7 21 4 5.75 1.38 2.75 4 4.5 1.5 3 0.49 28 3 4.67 1.2 2.08 2 4.5 1.5 2.12 1 35 1 9 - - 1 3 - - - 42 0 - - - 0 - - - - 100 19 4.58 0.45 1.95 5 4.6 0.68 1.52 0.91 Activity -7 5.82 0.29 1.19 6.2 0.73 1.64 0 15 5.13 0.36 1.41 6 4.83 0.54 1.33 0.64 7 14 5.43 0.37 1.4 5 5 0.71 1.58 0.67 14 9 5.78 0.43 1.3 5 5.2 0.97 2.17 0.75 21 4 6.25 0,48 0.96 4 5.25 0.86 1.71 0.57 28 3 7 0.58 1 2 5.5 1.5 2.12 0.5 35 2 7.5 0.5 0.71 1 8 - - 1 42 0 - - - 0 - - - - 100 19 5.63 0.17 0.86 5 6.2 0.2 0.45 0.11 Abbreviations: BASES Child version, Behavioural, Affective and Somatic Experience Scale, Standard Deviation PIG, Parental Intervention Group, PPCG Prospective Parental Control Group Mann-whitney test used to test the difference between the intervention and the control group.
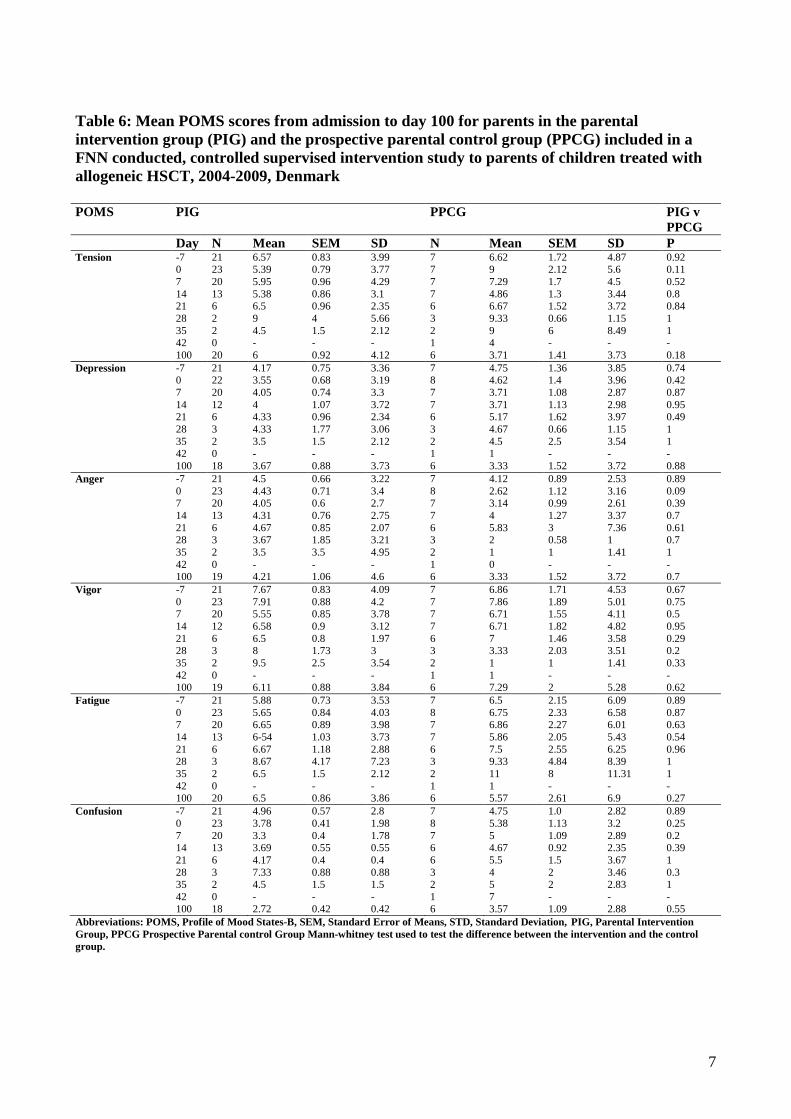
7
Table 6: Mean POMS scores from admission to day 100 for parents in the parental intervention group (PIG) and the prospective parental control group (PPCG) included in a FNN conducted, controlled supervised intervention study to parents of children treated with allogeneic HSCT, 2004-2009, Denmark POMS PIG PPCG PIG v
PPCG Day N Mean SEM SD N Mean SEM SD P Tension -7 21 6.57 0.83 3.99 7 6.62 1.72 4.87 0.92 0 23 5.39 0.79 3.77 7 9 2.12 5.6 0.11 7 20 5.95 0.96 4.29 7 7.29 1.7 4.5 0.52 14 13 5.38 0.86 3.1 7 4.86 1.3 3.44 0.8 21 6 6.5 0.96 2.35 6 6.67 1.52 3.72 0.84 28 2 9 4 5.66 3 9.33 0.66 1.15 1 35 2 4.5 1.5 2.12 2 9 6 8.49 1 42 0 - - - 1 4 - - - 100 20 6 0.92 4.12 6 3.71 1.41 3.73 0.18 Depression -7 21 4.17 0.75 3.36 7 4.75 1.36 3.85 0.74 0 22 3.55 0.68 3.19 8 4.62 1.4 3.96 0.42 7 20 4.05 0.74 3.3 7 3.71 1.08 2.87 0.87 14 12 4 1.07 3.72 7 3.71 1.13 2.98 0.95 21 6 4.33 0.96 2.34 6 5.17 1.62 3.97 0.49 28 3 4.33 1.77 3.06 3 4.67 0.66 1.15 1 35 2 3.5 1.5 2.12 2 4.5 2.5 3.54 1 42 0 - - - 1 1 - - - 100 18 3.67 0.88 3.73 6 3.33 1.52 3.72 0.88 Anger -7 21 4.5 0.66 3.22 7 4.12 0.89 2.53 0.89 0 23 4.43 0.71 3.4 8 2.62 1.12 3.16 0.09 7 20 4.05 0.6 2.7 7 3.14 0.99 2.61 0.39 14 13 4.31 0.76 2.75 7 4 1.27 3.37 0.7 21 6 4.67 0.85 2.07 6 5.83 3 7.36 0.61 28 3 3.67 1.85 3.21 3 2 0.58 1 0.7 35 2 3.5 3.5 4.95 2 1 1 1.41 1 42 0 - - - 1 0 - - - 100 19 4.21 1.06 4.6 6 3.33 1.52 3.72 0.7 Vigor -7 21 7.67 0.83 4.09 7 6.86 1.71 4.53 0.67 0 23 7.91 0.88 4.2 7 7.86 1.89 5.01 0.75 7 20 5.55 0.85 3.78 7 6.71 1.55 4.11 0.5 14 12 6.58 0.9 3.12 7 6.71 1.82 4.82 0.95 21 6 6.5 0.8 1.97 6 7 1.46 3.58 0.29 28 3 8 1.73 3 3 3.33 2.03 3.51 0.2 35 2 9.5 2.5 3.54 2 1 1 1.41 0.33 42 0 - - - 1 1 - - - 100 19 6.11 0.88 3.84 6 7.29 2 5.28 0.62 Fatigue -7 21 5.88 0.73 3.53 7 6.5 2.15 6.09 0.89 0 23 5.65 0.84 4.03 8 6.75 2.33 6.58 0.87 7 20 6.65 0.89 3.98 7 6.86 2.27 6.01 0.63 14 13 6-54 1.03 3.73 7 5.86 2.05 5.43 0.54 21 6 6.67 1.18 2.88 6 7.5 2.55 6.25 0.96 28 3 8.67 4.17 7.23 3 9.33 4.84 8.39 1 35 2 6.5 1.5 2.12 2 11 8 11.31 1 42 0 - - - 1 1 - - - 100 20 6.5 0.86 3.86 6 5.57 2.61 6.9 0.27 Confusion -7 21 4.96 0.57 2.8 7 4.75 1.0 2.82 0.89 0 23 3.78 0.41 1.98 8 5.38 1.13 3.2 0.25 7 20 3.3 0.4 1.78 7 5 1.09 2.89 0.2 14 13 3.69 0.55 0.55 6 4.67 0.92 2.35 0.39 21 6 4.17 0.4 0.4 6 5.5 1.5 3.67 1 28 3 7.33 0.88 0.88 3 4 2 3.46 0.3 35 2 4.5 1.5 1.5 2 5 2 2.83 1 42 0 - - - 1 7 - - - 100 18 2.72 0.42 0.42 6 3.57 1.09 2.88 0.55 Abbreviations: POMS, Profile of Mood States-B, SEM, Standard Error of Means, STD, Standard Deviation, PIG, Parental Intervention Group, PPCG Prospective Parental control Group Mann-whitney test used to test the difference between the intervention and the control group.

8
Table 7: Mean CHIP scores from admission to day 100 for parents in the parental intervention group (PIG) and the prospective parental control group (PPCG) included in a FNN conducted, controlled supervised intervention study to parents of children treated with allogeneic HSCT, 2004-2009, Denmark CHIP PIG PPCG PIG v
PPCG day N Mean SEM SD N Mean SEM SD P Family integration
-7 4 33 4.93 8.54 3 40.33 1.45 2.52 0.4
0 3 36.33 5.55 9.61 2 40 2 3.46 1 7 3 33.33 4.91 8.5 1 40 - - 1 14 1 37 - - 3 33.33 5.24 9.07 1 21 2 29.5 0.5 3 32.33 6.36 11.02 0.8 28 0 - - 0.71 2 40 4 5.66 - 35 0 - - - 1 42 - - - 42 0 - - - 0 - - - - 100 4 28 3.63 - 2 40 5 7.07 0.27 Social support -7 3 35.25 3.86 7.72 2 39.67 23.67 4.62 0.34 0 3 43.67 4.63 7.26 2 41 2.5 4.24 1 7 3 34.67 3.29 8.92 2 26.5 3.85 3.54 0.8 14 1 34 - 5.69 3 33.67 6.5 6.66 1 21 1 35 - - 2 29.5 - 9.19 1 28 0 - - - 1 39 - - - 35 0 - - - 1 36 - - - 42 0 - 2 - 0 - - - - 100 2 31 2.64 2.83 1 44 - - 0.67 Communication -7 3 14 1.53 2.65 2 17 2 2.83 0.5 0 4 16 0.5 5.29 4 16.75 0.75 1.5 0.89 7 2 11.5 - 0.71 2 15.5 1.5 2.12 0.33 14 1 9 - - 3 15.33 2.19 3.79 0.5 21 1 15 - - 3 13 1.15 2 0.75 28 0 - - - 2 14.5 3.5 3.5 - 35 0 - - - 1 15 - - - 42 0 - - - 0 - - - - 100 3 11.67 1.45 2.52 3 16.67 1.2 1.2 0.1 Abbreviations: CHIP, Coping Health Index for Parents, SEM, Standard Error of Means, STD, Standard Deviation PIG, Parental Intervention group, PPCG Prospective Parental Control Group Mann-whitney test used to test the difference between the intervention and the control group.
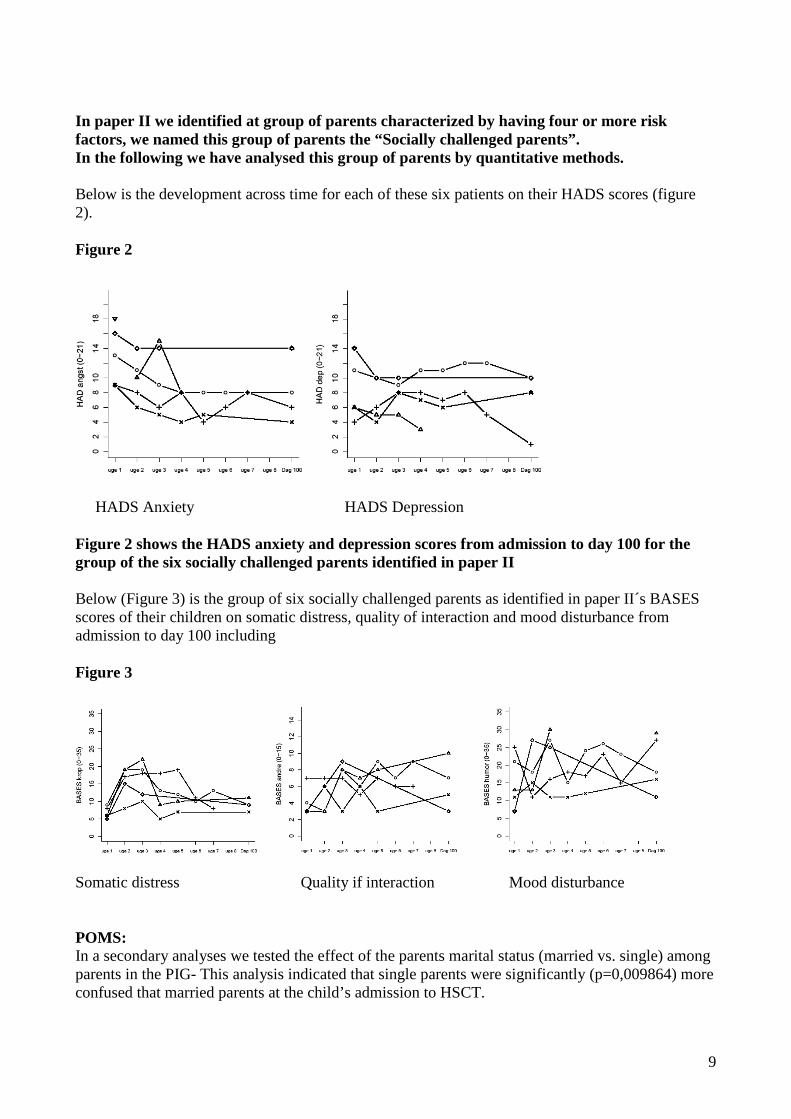
9
In paper II we identified at group of parents characterized by having four or more risk factors, we named this group of parents the “Socially challenged parents”. In the following we have analysed this group of parents by quantitative methods. Below is the development across time for each of these six patients on their HADS scores (figure 2). Figure 2
HADS Anxiety HADS Depression Figure 2 shows the HADS anxiety and depression scores from admission to day 100 for the group of the six socially challenged parents identified in paper II Below (Figure 3) is the group of six socially challenged parents as identified in paper II´s BASES scores of their children on somatic distress, quality of interaction and mood disturbance from admission to day 100 including Figure 3
Somatic distress Quality if interaction Mood disturbance POMS: In a secondary analyses we tested the effect of the parents marital status (married vs. single) among parents in the PIG- This analysis indicated that single parents were significantly (p=0,009864) more confused that married parents at the child’s admission to HSCT.

APPENDIX C
Approvals:
• Regional Ethical Scientific Comittee approval • National Data Protection Board approval
Participant information
Personaleafdelingen Enheden for Personale og Jura Blegdamsvej 9 2100 København Ø
Afsnit
5212
Direkte 3545 6496
Journal nr.: 30-0257 Ref.: UTK/bpv Dato: 12. maj 2011
Godkendelse af databehandling Din anmeldelse af databehandlingen med titlen ” SCT og Livskvalitet” er nu godkendt og anmeldt under Region Hovedstadens paraplyanmeldelse for Sundhedsvidenskabelig Forskning med j.nr. 2007-58-0015. Dit lokale journalnummer her i enheden er 30-0257 og skal anvendes ved forespørgsler, ændringer eller ansøgning om forlængelse af projektet. Du bedes være opmærksom på, at du selv har pligt til at tage initiativ til at slette oplysningerne senest på det i anmeldelsen angivne sletningstidspunkt eller søge om forlængelse af opbevaringstiden. De godkendte dokumenter er vedhæftet som fil i fremsendelsesmailen. Med venlig hilsen Ulla Terese Kræmer Juridisk Konsulent, cand.jur Enheden for Personale og Jura E-mail: [email protected] Telefon direkte: 3545 6496
Hanne Bækgaard Laursen Finsencentret afsnit 4042 Rigshospitalet Blegdamsvej 9 2100 Kbh. Ø

ID Nr:_____
Ph.d. studerende Hanne Bækgaard Laursen, tlf: 22284269
1
Deltagerinformation. Vi vil gerne gøre det bedre! Derfor vil vi undersøge om vi kan skabe et psykosocialt program, vi kan tilbyde forældre der har børn som skal igennem en stamcelletransplantation. Det er derfor vi henvender os til dig, da dit barn inden for den kommende tid vil gennemgå behandling med stamcelletransplantation. Hvad er det vi vil? Vi vil forsøge at reducere den belastning som er forbundet med behandlingen for såvel børn som forældre. Forældre til børn som gennemgår behandlingen har vigtige erfaringer og viden om hvordan behandlingsforløbet er. Den viden vil blive anvendt til at finde ud af om det nye psykosociale tilbud kan forbedre forholdene for såvel børn som forældre. Det er derfor vigtigt, at du vælger at deltage i undersøgelsen. Dine svar og deltagelse vil nemlig få betydning for hvilke psykosociale tilbud fremtidige børnefamilier tilbydes i forbindelse med et barns behandling med stamcelletransplantation. Det psykosociale program vi vil tilbyde dig er baseret på erfaringer fra forældre hvis børn tidligere er behandlet med stamcelletransplantation og de tiltag er i litteraturen er beskrevet at have effekt. Vi vil understrege at din deltagelse i denne undersøgelse er frivillig og at den på ingen måde vil have indflydelse på den behandling som dit barn modtager på Rigshospitalet. Du kan til enhver tid trække dig ud af undersøgelsen ved at kontakte Hanne Bækgaard. Hvordan gør vi? Såfremt du ønsker at deltage i denne undersøgelsen, vil vi bede dig om at udfylde et spørgeskema inden dit barn bliver transplanteret, et spørgeskema hver uge under indlæggelsen samt et spørgeskema ca. 100 dage efter transplantationen. I spørgeskemaet er der en del der skal udfyldes af forældrene og en del som vi vil bede dit barn om at udfylde, såfremt dit barn er ældre end 6 år og har lyst til at deltage i undersøgelsen. Vi vil også bede dig om at skrive dagbog under indlæggelsesforløbet, samt deltage i et interview af ca. 30 min varighed 100 dage efter dit barns stamcelletransplantation. Vi er meget interesseret i at modtage din besvarelse af spørgeskemaet også selv om dit barn ikke deltager i undersøgelsen. Da formålet med denne undersøgelse er undersøge hvorvidt vi kan forbedre den psykosociale støtte til forældre, hvis børn behandles med stamcelletransplantation, vil vi også tilbyde dig følgende:
1. At der på alle hverdage kommer en sygeplejerske med erfaring inden for stamcelletransplantation og taler med dig og dit barn om hvorledes det foregående døgn er gået ved projektsygeplejerske Hanne Bækgaard.
2. Deltagelse i et undervisningsprogram, der løber over fem uger under barnets
indlæggelse af en times varighed. Der vil blive undervist i følgende emner: - Ændringer i familien ved et barns sygdom ved projektsygeplejerske Hanne
Bækgaard - Børn og søskendes reaktioner på indlæggelse og behandling ved
sundhedsplejerske Helen Munck

ID Nr:_____
Ph.d. studerende Hanne Bækgaard Laursen, tlf: 22284269
2
- Håndtering af potentielle konflikter mellem børn og forældre under indlæggelse ved psykolog Bo Snedker Boman
- Hvordan kan du støtte dit barns udvikling ved pædagog Lise Auscher - Erfaringsudveksling med en forældre hvis barn tidligere er behandlet med
stamcelletransplantation ved Tine Banke Høgsberg Undervisningen finder sted i Ronald McDonald huset. I det omfang det er muligt vil vi arrangere at der er personale hos dit barn i mens du ikke er der.
3. Fysisk aktivitet i form at en gå tur en gange om ugen og cykeltræning to gang om
ugen af ca. en times varighed. Den fysiske aktivitet vil foregå i dit eget tempo og formålet med dette er ikke at forbedre din kondition, men i stedet at tilbyde dig mulighed for at forlade barnets stue, få lidt adspredelse og frisk luft. I det omfang det er muligt vil vi arrangere at der er personale hos dit barn i mens du ikke er der. Projektsygeplejerske Hanne Bækgaard vil deltage i den fysiske aktivitet sammen med dig.
Det samlede program ser således ud:
Mandag Tirsdag Onsdag Torsdag Fredag Besøg af sygeplejerske
Besøg af sygeplejerske
Besøg af sygeplejerske
Besøg af sygeplejerske
Besøg af sygeplejerske
Gåtur Cykeltræning Gåtur Undervisning Hvad indebærer det at være med? Det tager lidt tid at udfylde spørgeskemaet, men er du først i gang går det hurtigt. Når du udfylder spørgeskemaet vil vi bede dig om at tænke tilbage på den sidste uge og besvare spørgsmålene ud fra din oplevelse. Vi vil bede dig om at markere det svar som du først tænker på, såfremt du er i tvivl om hvorledes du vil besvare spørgsmålet. Spørgeskemaet indeholder spørgsmål om hvordan du oplever behandlingen og om hvordan du har det. Når du har udfyldt spørgeskemaet vil projektlederen, Hanne Bækgaard samle dette ind. Til deltagelse i den fysiske aktivitet vil det være en fordel hvis du medbringer et par gode sko til at gå tur i, samt træningstøj til cykeltræning. Fortrolighed: Dit spørgeskema vil blive forsynet med et nummer og vi vil kun anvende dine oplysninger i videnskabelige rapporter, hvor det ikke er muligt at identificere enkelt personer. Undersøgelsen er godkendt af den centrale videnskabs etiske komite´ (journal nummer 01 2006-7216) og af datatilsynet (journal nummer 30-0257). På Rigshospitalet er undersøgelsen godkendt af Klinikcheferne for børneafdelingen og hæmatologiskafdeling. Undersøgelsen bliver styret af professor Carsten Heilmann fra børneafdelingen, professor Lis Adamsen fra UCSF og overlæge Christoffer Johansen fra Kræftens Bekæmpelse. Oplysninger om økonomiske forhold: Projektet støttes økonomisk af fondsmidler fra Børne Cancer Fonden, Helsefonden, Lundbeck Fonden, Gangsted Fonden og Rigshospitalet.
ID Nr:_____
Ph.d. studerende Hanne Bækgaard Laursen, tlf: 22284269
3
Såfremt du har spørgsmål i forbindelse med din deltagelse i undersøgelsen er du meget velkommen til at kontakte mig – det er mig der står for den daglige drift. Mange tak for hjælpen Bedste hilsner Hanne Bækgaard Laursen Projektleder, sygeplejerske Rigshospitalet, KMT afsnit 4043/44 Blegdamsvej 9 2100 København Ø Tlf: 22284269 e-mail: [email protected]