the effects of assisted cycle therapy on executive and ... · the effects of assisted cycle therapy...
TRANSCRIPT

The Effects of Assisted Cycle Therapy on Executive and Motor Functioning
in Young Adult Females with Attention-Deficit Hyperactivity Disorder
by
Natasha Birchfield
A Thesis Presented in Partial Fulfillment of the Requirements for the Degree
Master of Science
Approved July 2014 by the Graduate Supervisory Committee:
Shannon Ringenbach, Chair
Chong Lee Jack Chisum
Kathryn Campbell
ARIZONA STATE UNIVERSITY
August 2014

i
ABSTRACT
Voluntary exercise has been shown to generate post exercise improvements in executive
function within the attention-deficit hyperactivity disorder (ADHD) population. Research
is limited on the link between exercise and motor function in this population. Whether or
not changes in executive and motor function are observed under assisted exercise
conditions is unknown. This study examined the effect of a six-week cycling
intervention on executive and motor-function responses in young adult females with
ADHD. Participants were randomized to either a voluntary exercise (VE) or an assisted
exercise (AE) group. Both groups performed 30 minute cycling sessions, three times per
week, at either a voluntary or assisted rate, on a modified Theracycle Model 200
motorized stationary cycle ergometer. The Mann-Whitney U tests were used to detect
median differences between groups, and the Wilcoxon signed-rank tests were used to test
median differences within groups. Executive function improvements were greater for AE
compared to VE in activation (MDNAE = 162 vs. MDNVE = 308, U = .00, p = .076, ES =
.79); planning (MDNAE = 51.0 vs. MDNAE = 40.5, U = .00, p = .083, ES = .77); attention
(MDNAE = 13.0 vs. MDNVE = 10.0, U = .00, p = .083, ES = .77); and working memory
(MDNAE = 10.0 vs. MDNVE = 6.5, U = .00, p = .076, ES = .79). Motor function
improvements were greater for AE compared to VE in manual dexterity (MDNAE = 18 vs.
MDNVE = 15.8, U = .00, p = .083, ES = .77); bimanual coordination (MDNAE = 28.0 vs.
MDNVE = 25.3, U = .00, p = .083, ES = .77); and gross motor movements of the fingers,
hands, and arms (MDNAE = 61.7 vs. MDNVE = 56.0, U = .00, p = .083, ES = .77). Deficits
in executive and motor functioning have been linked to lifelong social and psychological
impairments in individuals with ADHD. Finding ways to improve functioning in these

ii
areas is important for cognitive, emotional and social stability. Compared to VE, AE is a
more effective strategy for improving executive and motor functioning in young adult
females with ADHD.

iii
DEDICATION
I dedicate this thesis to my husband Justin and my daughter Paige. Without their
unwavering support this project would not have been possible. Thank you both for giving
me love, support and encouragement throughout this journey. I am truly blessed and
thankful to have you both in my life.

iv
ACKNOWLEDGMENTS
I would like to thank the Graduate and Professional Student Association at Arizona State
University for the funding they were able to provide me, making this research possible.
I would like to extend my sincerest gratitude to Dr. Shannon Ringenbach for providing
the inspiration and guidance I have needed throughout this project. I would also like to
thank Dr. Ringenbach’s undergraduate students who dedicated their time and effort in
bringing this project to fruition.
Many thanks to Dr. Jack Chisum and Dr. Kathy Campbell for the wisdom and advice you
have provided throughout the years. Your support helped nurture the strength and
confidence I needed to successfully complete this portion of my academic journey.

v
TABLE OF CONTENTS
Page
LIST OF TABLES ................................................................................................................. vii
LIST OF FIGURES .......................................................................................................... viii-ix
CHAPTER
1 INTRODUCTION ................. ................................................................................ 1-8
Study Purpose ............................................................................................. 6
Hypotheses ............................................................................................. 6-7
Definition of Terms ................................................................................ 7-8
Delimitations and Limitations ................................................................... 8
2 BACKGROUND LITERATURE ........................................................................ 9-27
Attention Deficit Hyperacitivity Disorder Defined............................. 9-10
Prevalence of Adult ADHD ............................................................... 10-11
Executive Function ............................................................................ 11-15
Motor Function ......................................................................................... 15
Neurobiology of ADHD ................................................................... 15-18
Treatment Recommendations for ADHD ......................................... 18-20
Exercise and Executive and Motor Functioning ............................... 20-24
Exercise and Nurological Changes .................................................... 22-24
Assisted Exercise ............................................................................... 24-27
3 METHODOLOGY .................. .......................................................................... 28-36
Particiapants and Study Design ......................................................... 28-29
Exercise Equipment and Evaluation .................................................. 29-30

vi
CHAPTER Page
Executive and Motor Function Measures .......................................... 30-35
Statistical Analysis ............................................................................ 35-36
4 RESULTS ...................... .................................................................................... 37-69
Quantitative Data .............................................................................. 37-69
Qualitative Data ...................................................................................... 69
5 DISCUSSION ................... ................................................................................. 70-78
Executive Function Findings ............................................................ 70-76
Motor Function Findings .................................................................. 76-77
Conclusion and Future Direction ...................................................... 77-78
REFERENCES....... ........................................................................................................ 79-87
APPENDIX
A RECRUITMENT FLYER ................................................................................ 88-89
B CONSENT FORM ............................................................................................ 90-94
C VOLUNTARY CYCLING GROUP EXERCISE DATA SHEET ................. 95-96
D ASSISTED CYCLING GROUP EXERCISE DATA SHEET ........................ 97-98
E TOWER OF LONDON DATA SHEET ........................................................ 99-100
F STROOP TEST DATA SHEET ................................................................... 101-102
G VERBAL FLUENCY DATA SHEET ........................................................ 103-105
H DIFFICULTIES IN EMOTION REGULATION SCALE ......................... 106-110
I AUDITORY NUMBER MEMORY DATA SHEET ................................... 111-112
J SELF-REGULATION QUESTIONNAIRE ................................................. 113-118
K PURDUE PEGBOARD DATA SHEET ..................................................... 119-121

vii
LIST OF TABLES
Table Page
1. Participant Demographics .................................................................................... 37
2. Pre-intervention Executive and Motor Function Assessments ........................... 37
3. Post-intervention Between Group Outcome Measures .................................. 40-41
4. Assisted Cycling Profile of Pre/Post Outcome Measures .............................. 51-52
5. Voluntary Cycling Profile of Pre/Post Outcome Measures ........................... 53-54

viii
LIST OF FIGURES
Figure Page
1. Brown’s Model of Executive Function ........................................................ 12
2. Albert’s Schematic of the Effects of Assisted Exercise ............................... 26
3. Tower of London Task Diagram .................................................................. 31
4. Stroop Task Testing Cards ....................................................................... 32-33
5. Purdue Pegboard ............................................................................................ 35
6. Between Group Effects: Cognitive Activation ............................................ 41
7. Between Group Effects: Cognitive Planning ............................................... 42
8. Between Group Effects: Working Memory .................................................. 43
9. Between Group Effects: Attention & Working Memory ............................. 44
10. Between Group Effects: Manual Dexterity ................................................... 45
11. Between Group Effects: Bimanual Coordiation ........................................... 46
12. Between Group Effects: Gross Motor Movement ........................................ 47
13. Within Group Effects: Cognitive Activation ................................................ 55
14. Within Group Effects: Cognitive Planning .................................................. 56
15. Within Group Effects: Cognitive Attention .................................................. 57
16. Within Group Effects: Set-Shifting .............................................................. 58
17. Within Group Effects: Sustaining Effort ....................................................... 59
18. Within Group Effects: Processing Speed ..................................................... 60
19. Within Group Effects: Cognitive Effort ....................................................... 61
20. Within Group Effects: Working Memory .................................................... 62
21. Within Group Effects: Attention and Working Memory .............................. 63

ix
Figure Page
22. Within Group Effects: Self-Regulation ......................................................... 64
23. Within Group Effects: Dominant Hand Manual Dexterity ......................... 65
24. Within Group Effects: Non-dominant Hand Manual Dexterity ................... 66
25. Within Group Effects: Bimanual Coordination ............................................ 67
26. Within Group Effects: Gross Motor Movement ........................................... 68
27. Within Group Effects: Fingertip Dexterity ................................................... 69

1
CHAPTER 1
INTRODUCTION
Disorganization, recklessness, distractibility, restlessness, and dysregulated
emotions are among some of the traits that disrupt the lives of many individuals with
attention deficit hyperactivity disorder (Smith & Segal, 2013). Attention deficit
hyperactivity disorder (ADHD) is recognized worldwide as one of the most prevalent
developmental disorders in the world (Polanczyk, de Lima, Horta, Biederman & Rhode,
2007). While commonly considered a childhood disorder, according to the National
Institutes for Mental Health, ADHD affects approximately four percent of adults in the
United States alone, with an estimated 41 percent of those individuals being classified as
severe. Kessler et al. (2006) has reported that among adult females aged 18-44, three
percent are affected by the disorder.
Although it was previously thought that most cases of ADHD resolved before
adulthood, it is now estimated that 50-60% of children diagnosed with ADHD in
childhood continue to suffer from the disorder into adulthood (Farone, Biederman &
Mick, 2006). ADHD is highly associated with behavioral dysfunction in children, but in
adults the disorder commonly disrupts cognitive, emotional, and social functioning.
Adults with ADHD are more likely to experience joblessness due to excessive errors,
lateness and absenteeism, interpersonal and relationship difficulties, and are at a
significantly higher risk for engaging in risky behaviors and substance abuse (Harpin,
2005). The symptoms of ADHD cause a great deal of distress and, according to the CDC
(2008), often lead to additional psychological dysfunction such as depression and
anxiety. ADHD has been known to lead to persistent, lifelong impairments and, coupled

2
with ineffective treatment, often becomes problematic and costly; associated costs are not
only those considered in terms of monetary expenses, rather are reflective of the social
and psychological impairments that often lead to a diminished quality of life (Halperin &
Healey, 2011; Matza, Paramore & Prasad, 2005)
The estimated annual costs associated with ADHD are approximately $42.5
billion, including health care, education, disciplinary costs, loss of work, and justice costs
(Pelham, Foster & Robb 2007). This is a tremendous financial burden that is not only
assumed by those directly affected by ADHD but also by government agencies. Health
care expenses for diagnosed individuals, including medications prescribed to treat the
illness, exceed $13 billion annually (Birnbaum, et al., 2000). Medications, such as Ritalin
(methylphenidate) and Adderall (amphetamine), Class II stimulant narcotics, are
commonly prescribed to treat the symptoms associated with ADHD, costing $1.3 billion
per year. These medications target the dopaminergic pathways in the brain, in order to
minimize the dysfunction caused by ADHD, by acting on the pathway to increase the
production and availability of dopamine in the prefrontal region of the brain (Frank-
Briggs, 2011; Hillman, Buck, Themanson, Pontifex, & Castelli, 2009).
Dopamine is an essential neurotransmitter that plays a role in executive and motor
functioning in the brain and has been found to be significantly less available in the
ADHD brain (del Campo, Chamberlain, Sahakian & Robbins, 2011). Executive
functioning is a collective term used to describe “high-level cognitive processes that
control and regulate other lower-level processes” (Chandler, 2010). Thus executive
function is imperative for inhibition, attending, and emotion regulation, as well as
organization, planning and execution (Brown, 2006). Individuals who experience the

3
symptoms associated with ADHD often have difficulty with each of these tasks. While
ADHD is most often associated with uncontrolled, disruptive behaviors, the deficits of
the disorder are primarily due to neuropsychological dysfunction. ADHD creates deficits
in neuropsychological functioning, most commonly identified as executive dysfunction
(Hummer et al., 2011; Halperin & Healey, 2011). Executive dysfunction often leads to
dysregulated processes and may be due to a reduction in the production and availability
of dopamine in the brain (Sagvolden, Johansen, Aase, & Russell, 2005).
In addition to impaired executive functioning, approximately 50% of the ADHD
population experiences the effects of dysfunctional motor control (Pitcher, Piek, & Hay,
2003). Impaired motor control, specifically motor inhibition, has been known to affect
fine motor movements such as eating and handwriting, and gross motor movements
typically observed as clumsiness, in ADHD populations (Stray, Stray, Iversen, Ruud,
Ellertsen, & Tonnessen, 2009). Clumsy behaviors associated with ADHD are often
attributed to inattention and distractibility but may be better understood as impairments in
motor control and movement coordination (Stray, et al., 2009).
Executive and motor functioning develops throughout childhood as the brain
develops and this process may follow an abnormal trajectory in children and adolescents
with ADHD (Halperin & Healey, 2011; Stray, et al., 2009). Castellanos (1997) has
suggested that the brain of an individual with ADHD has developmental lag of
approximately two years. However, more recent studies suggest, that the brain is actually
smaller in those with ADHD, with a total brain volume reduction of approximately 3-5%
(Halperin & Healey, 2011). Although a reduction in brain size may not adequately
4
explain the differences between an ADHD brain and an unaffected brain, it is the regions
of the brain that are smaller that deserve closer attention.
Subcortical regions of the brain, which include the nucleus accumbens, caudate
nucleus, the midbrain, and the prefrontal cortex are the regions that are most affected by
dopamine (del Campo et al., 2011). Molecular imaging studies have shown that within
the ADHD brain, these areas not only produce lower levels of dopamine, they actually
house fewer dopamine receptors (del Campo et al., 2011). The receptors are important for
accepting neurotransmitters released in the brain cells. Without the presence of the
receptors, the chemicals have no distinct pathway to follow. Lower production of
dopamine and less neural availability of the neurotransmitter may be one explanation for
many of the symptoms associated with ADHD. Distractibility, attention sustainability,
emotional regulation and behavioral regulation are all highly influenced by the
dopaminergic pathways (Arnsten, 2009). Although ADHD medications target these areas
of the brain and increase dopamine production, alternative methods of treatment should
be considered for those who wish to avoid the potential for complications associated with
amphetamine (Adderall and Vyvanse) and methylphenidate (Ritalin) use. Exercise may
be one potential alternative treatment that could improve executive and motor functioning
by increasing dopamine production as well as proteins specific to neurogenesis in ADHD
individuals.
Exercise has been shown to influence cognition, executive functioning and the
dopaminergic pathways in ADHD individuals, positively influencing their ability to plan,
execute and perform executive functioning tasks (Chang, Liu, Yu & Lee, 2012).
Treadmill exercise has been found to increase dopamine levels and dopaminergic

5
transmission in regions of the brain affecting cognition and motor function (Petzinger,
Fisher, McEwen, Beeler, Walsh, & Jakowec, 2007). Brain derived neurotrophic factor,
BDNF, is a protein responsible for neurogenesis, the growth of neurons in the brain.
Chemical specific receptors such as dopamine receptors are comprised of post-synaptic
neurons. Physical exercise has been shown to increase levels of BDNF by approximately
32 percent (Scehmolesky, Webb & Hansen, 2013).
Assisted or forced exercise is a mode of aerobic exercise that is enhanced by the
use of motorized equipment. The mechanical assistance enables a participant to achieve
and maintain an exercise speed that is greater than a preferred self-selected, voluntary
speed (Alberts, Argollo, Oliveira, Cardoso, Bueno, Xavier, 2011). Forced exercise has
been evaluated in persons with Parkinson’s disease, a progressive neurodegenerative
disorder resulting in the degeneration of the dopaminergic pathways, and found to
enhance motor function above and beyond that of (VE) (Alberts, et al., 2011). This may
be due to altered activation patterns that trigger the release of neurotrophic factors,
including dopamine and brain derived neurotrophic factor (Alberts, et al., 2011).
Ringenbach et al. (2014) have demonstrated similar patterns of improvement in persons
with Down syndrome, in addition to improvements in cognitive functioning. Changes at
the molecular level, i.e. altered dopaminergic pathways, are thought to be affecting the
function of the prefrontal and motor cortices through increases in afferent neurological
signaling (Ringenbach, Albert, Chen, & Alberts, 2014). Assisted Cycle Therapy is an
innovative approach to evaluating neuropsychological function in the ADHD brain.
Due to these recent findings, AE could be implicated as a non-medicinal approach
to treating ADHD and presents with an insignificant number of negative side effects.

6
Drug use in and of itself often carries an excess of negative side effects. Not only could
individuals receiving medical interventions benefit from an alternative approach to drug
therapy or further improved functioning, those not actively receiving treatment could also
be positively impacted.
Purpose of the Study
The primary objective of this between group pre-test/post-test study is to evaluate
the effects of AE on the ADHD brain. This study aims to look at whether or not a
prescribed assisted cycling therapy program can improve executive and motor
functioning above and beyond that of VE.
Questions to be Answered
1) Is there a significant pre-test/post-test difference in the cognitive clusters
(activation, focus, effort, emotion, memory, and action) associated with executive
functioning following a six-week assisted or voluntary exercise protocol?
2) Is there a significant pre-test/post-test difference in manual dexterity, bimanual
coordination, gross movement of the fingers, hands and arms, or fingertip dexterity
following a six-week assisted or voluntary exercise protocol?
Hypotheses
The primary hypothesis is that Assisted Cycle Therapy will elicit significantly
greater improvements in activation, focus, effort, emotion, memory and action, the
cognitive clusters associated with executive function, compared to VE in adult females
diagnosed with ADHD. The secondary hypothesis states Assisted Cycle Therapy will
elicit significantly greater improvements in manual dexterity, bimanual coordination,
gross finger, hand, arm movement, and fingertip dexterity, measures of functional motor

7
behaviors, compared to VE in adult females diagnosed with ADHD. It is also
hypothesized that within each group the observed changes in executive and motor
functions will be significantly different only within the AE group.
Definition of Terms
• Amphetamine: A synthetic psychostimulant drug
• Caudate nucleus: A brain structure found in the basil ganglia that is responsible for
regulating and organizing information that is being passed between the two lobes of
the brain. This structure is also involved in voluntary movement, learning and
memory.
• Dopamine: A chemical messenger found in the brain responsible for regulating
executive functioning, motor function and the reward centers in the brain.
• Dopamine receptor: A neurochemical receptor that can only transmit the
neurotransmitter dopamine.
• Dopaminergic pathway: Part of the brains neural transmission center, this pathway
transmits the neurotransmitter dopamine from one region of the brain to another.
• Executive functioning: The coordination of and regulation of mental and cognitive
processes.
• Methylphenidate: A synthetic psychostimulant drug
• Midbrain: This structure is primarily used to transmit sensory and motor input to the
cerebral cortex for processing.
• Molecular imaging: A method of imaging that not only captures the physical aspects
of the body but the biochemical aspects as well such as molecular functioning.

8
• Neurotransmitter: A chemical found in the brain that transmits electrical signals from
one nerve ending to another.
• Nucleus accumbens: An area of the brain responsible for processing reward and
motivation cues.
• Prefrontal cortex: This region of the brain is extremely important for maintaining
cognitive and emotional functioning. The PFC is responsible for processes like short-
term memory, learning, goal setting, and overall executive functioning.
• Subcortical region of the brain: The region of the brain located below the cerebral
cortex which is responsible for higher order functions like sensory perception,
voluntary movement, cognition and memory.
Delimitation and Limitations
• Participants will be delimited to ADHD diagnosed adult females aged 18-24 years.
• Behavioral measures will be used to indirectly measure changes in the brain via
changes in executive function and motor function assessments. Direct measurement
utilizing fMRI scans is expensive and exceeds the scope of this study.
• Medicated participants will be allowed in the study in order to evaluate any
differences between the non-medicated counterparts. Univariate statistical tests can be
run to control for this confounding factor.
• If a large enough population sample is not recruited, a small sample size may impact
the statistical power and findings of the study.
• Self-report measures give insight into individual perspective but may present issues
of under-reporting the severity of symptoms.

9
CHAPTER 2
BACKGROUND LITERATURE
Attention Deficit Hyperactivity Disorder Defined
Attention-deficit hyperactivity disorder (ADHD) is a developmental disorder that
typically manifests before age seven with continued presence into adolescence, often
extending into adulthood. Keen and Hadjikoumi (2007) report that 70% of hyperactive
children may struggle with ADHD into adolescence with 65% of those adolescents
continue to meet diagnostic criteria for ADHD in adulthood. The disorder is commonly
associated with disruptive behaviors but can also be present in individuals who do not
demonstrate overtly disruptive behaviors. Diagnosis is made by a qualified health care
professional, based on the presence of symptoms, not attributable to another disorder, for
a period of at least 6 months, causing behavioral disorder and cognitive impairment
(Keen & Hadjikoumi, 2007).
The American Psychiatric Association’s Diagnostic and Statistical Manual of
Mental Disorders (DSM) provides diagnostic criteria for mental health professionals.
Unlike all previous versions, the DSM-V allows for the assessment of adults with
ADHD. In order to identify the presence of ADHD in adulthood, the following
considerations must be evaluated; demonstrates a persistent pattern of inattention and/or
hyperactivity-impulsivity that hinders with functioning; symptoms must have presented
before age 12; symptoms must be present in at least two settings; symptoms must
interfere with the quality of functioning in social, school or work settings; and symptoms
cannot be attributed to another mental disorder (CDC, 2014). Based on the symptoms of
inattention and/or hyperactivity-impulsivity, one of three ADHD sub-types can occur; (I)

10
combined inattentive, hyperactive-impulsive presentation, (II) predominantly inattentive
presentation, or (III) predominantly hyperactive-impulsive determination (CDC, 2014).
According to the National Institute of Mental Health (2008), individuals
diagnosed as predominantly hyperactive-impulsive, often present as fidgety, overly
talkative, overly active, and impatient with unrestrained emotion, often times disrupting
others around them. Individuals diagnosed as predominantly inattentive, are often more
difficult to recognize due to the absence of the hyperactive component. Those who are
predominantly inattentive typically viewed as day dreamers, often seeming unfocused
and bored, with high distractibility, inattention to detail, and forgetfulness, and have
difficulty completing tasks, meeting deadlines and are generally disorganized. Those with
the third subtype present a combination of characteristics from both the inattentive and
hyperactive-impulsive subtypes and may have fewer issues with impulsivity.
Prevalence of Adult ADHD
Attention deficit hyperactivity disorder has long been considered a developmental
disability occurring only in childhood. However, current research and evaluation has
uncovered the pervasive nature of the disorder, which has been shown to persist well into
adulthood for a high-proportion of individuals (Simon, Czobor, Balint, Meszaros, Bitter,
2009). While it has been difficult to estimate the prevalence rate among adult
populations, based on a survey conducted by the National Institutes for Mental Health,
4.4 percent of adults age 18-44 report the occurrence of the symptoms and disability
associated with ADHD (NIMH, 2006). Simon et al. (2009), suggest a more conservative
value at 2.5 percent based on meta-analysis. The actual rate of prevalence is likely within

11
this range based on the current adolescent prevalence rates of 5-11 percent and estimates
that 50-60 percent of adolescents have the disorder into adulthood (CDC, 2013).
Executive Function
Executive functioning is a broad term that encompasses the top-down, higher-
order decisional process that helps individuals control their actions and behaviors.
Executive function is used for several important processes, including planning,
organizing, strategizing, focus and attention, working memory, and time and space
management (National Centers for Learning Disabilities, N.D.). Executive functioning
has also been described as a combination of processes in the brain that are the primary
regulators of behavior, planning and other cognitive processes, often associated with self-
control (Sagvoldent, et al., 2005). Deficits in executive functioning have been found to
play a major role in the dysregulated behaviors commonly associated with ADHD. In
individuals with ADHD, executive functioning deficiencies have been implicated in
diminished attention, working memory, verbal fluency, processing speed and motor
control (Biederman et al., 2006). Although the disorder has been primarily evaluated in
adolescents with ADHD, researchers have found similar patterns of neuropsychological
deficits in ADHD adults (Hervey, Epstein, & Curry, 2004; Seidman, Doyle, Fried,
Valera, Crum, & Matthews, 2004).
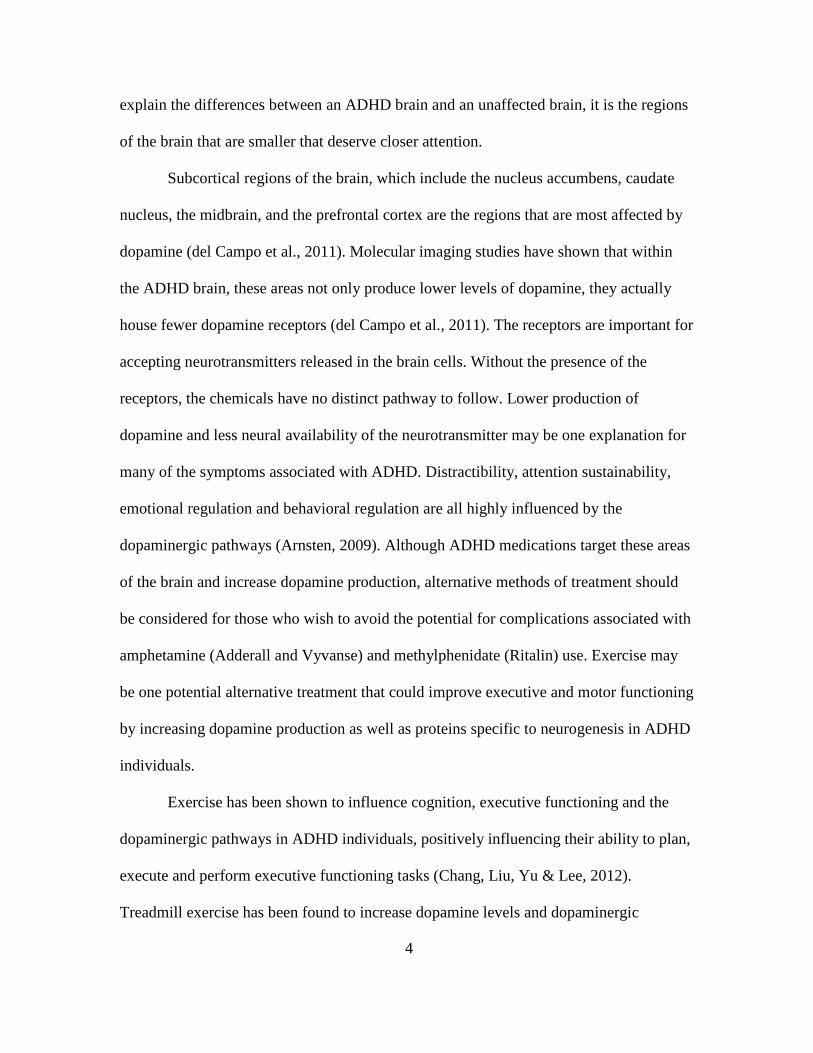
Brown (2006) has created a conceptual model of executive function which
includes six primary clusters of cognitive processes; (1) activation, (2) focus, (3) effort,
(4) emotion, (5) memory and (6) action (Figure 1). Each cluster consists of a variety of
behaviors related to the primary cognitive process; the activation cluster describes the
executive functions of organization, prioritization, and activation; the focus cluster is

primarily involved in focus, sustained attention, and the ability to shift attention; effort is
related to alertness, sustaining effort and processing speed; the emotion cluster helps with
managing frustration and modulating emotions; memory deals with utilizing working
memory and accessing recall; and the action cluster is involved with monitoring and self
regulation. Brown (2006, 2013
executive function as a result of impairments in the cognitive clusters.
Figure 1 – Brown’s model of impaired cognitive behaviors resulting in impaired executive function. The cognitive clusters represeelements and the accompanying impaired behaviors. While each cluster of executive functioning is distinct, there is a degree of
interaction between the domains as a re
example, disorganization (activation) is often attributed to an inability to sustain attention
(focus) but may also be a result of the inability to sustain effort (effort) or self
behaviors (action). While it is difficult to
these behavioral characteristics
individuals with ADHD. The inhibitory process
inability to disrupt an ongoing task, ignore stimuli,
12
primarily involved in focus, sustained attention, and the ability to shift attention; effort is
related to alertness, sustaining effort and processing speed; the emotion cluster helps with
d modulating emotions; memory deals with utilizing working
memory and accessing recall; and the action cluster is involved with monitoring and self
, 2013) has suggested individuals with ADHD have impaired
executive function as a result of impairments in the cognitive clusters.
Brown’s model of impaired cognitive behaviors resulting in impaired executive function. The cognitive clusters represent the primary cognitive elements and the accompanying impaired behaviors.
While each cluster of executive functioning is distinct, there is a degree of
between the domains as a result of deficits in executive inhibition.
nization (activation) is often attributed to an inability to sustain attention
(focus) but may also be a result of the inability to sustain effort (effort) or self
is difficult to differentiate which deficits specifica
behavioral characteristics, a deficit in the inhibitory process has been identified in
he inhibitory process deficit has been implicated in
inability to disrupt an ongoing task, ignore stimuli, and inhibit responses, all of which
primarily involved in focus, sustained attention, and the ability to shift attention; effort is
related to alertness, sustaining effort and processing speed; the emotion cluster helps with
d modulating emotions; memory deals with utilizing working
memory and accessing recall; and the action cluster is involved with monitoring and self-
) has suggested individuals with ADHD have impaired
Brown’s model of impaired cognitive behaviors resulting in impaired nt the primary cognitive
While each cluster of executive functioning is distinct, there is a degree of
sult of deficits in executive inhibition. For
nization (activation) is often attributed to an inability to sustain attention
(focus) but may also be a result of the inability to sustain effort (effort) or self-regulate
differentiate which deficits specifically cause
process has been identified in
implicated in one’s
all of which

13
lead to interference with focus, working memory, planning and organized behavior
(Seidman et al., 2004). Many individuals with ADHD also express dysregulated attention
behaviors, leading to compulsive characteristics. A hyperfocused state leads to an
inability to inhibit the extreme focus of attention in order to monitor other aspects of the
environment (Carver, 2009).
Deficits in the inhibitory process have also been linked to impulsivity and risk
taking, as well as deficits in emotion and self-regulation (Brown, Miller & Lawendowski,
1999; Barkley, 2010). While, hyperactivity may be the most commonly associated
symptom of ADHD and often conjures images of unruly children, in adults hyperactive
behaviors may be better identified as rapid speech, dysregulated emotion, incessant
fidgeting, and nail biting (Carver, 2009). Finally, impulsivity is often thought of as a
failure to self-regulate but when the inhibitory process becomes dysregulated, the brain is
reacting before ADHD individual can make a conscious plan for action (Brown, Miller &
Lawendowski, 1999).
Individuals may not experience deficiencies in all areas of functioning but if
weaknesses are present, the daily demands associated with these functions become
increasingly difficult with an overall increase in dysfunction. When individuals
experience weakness in the activation cluster, issues with procrastination, task initiation
and organization are areas that interfere with cognitive performance (Kelly & Ramundo,
2006). Often times individuals understand what they need to do they just have difficulty
with the initiation process. When weaknesses are observed in the focus cluster,
persistence is often times a major deficiency (Kelly & Ramundo, 2006). Even when
individuals recognize the importance of focusing on a task for an appropriate amount of
14
time needed to complete the task, executing this seems impossible. Distractibility is often
times heightened and it is common to become hyper-focused on background noises,
thoughts, or even the environment (Kelly & Ramundo, 2006).
Individuals that experience weaknesses in effort are those who have difficulty
staying alert when there is little cognitive feedback and may often times result in
sleepiness or drowsiness (Kelly & Ramundo, 2006). Weaknesses in emotion regulation
lead to hyper-active emotionality, high occurrence of reactive emotions, and an
intolerance for frustration (Kelly & Ramundo, 2006). Emotional outbursts are common
and these individuals often become overwhelmed with their overreactions and the
feelings of sadness or depression that occur when they realize their degree of intolerance
(Kelly & Ramundo, 2006). If weaknesses in memory are present, academic success is
often times challenging. Weaknesses in the action cluster often appear as impulsive and
hyperactive behaviors due to the fact that there is little forethought before acting and an
impaired ability to inhibit behaviors (Kelly & Ramundo, 2006)
Willcutt et al. (2005) have identified executive functioning as the most important
component for successful navigation of the ever-changing environment. The importance
of proper functioning is essential in order to continuously evaluate the barrage of stimuli
and choose an appropriate action or response from a seemingly endless list of
possibilities. Marx, et al. (2010), have evaluated deficiencies in memory tasks,
interference control, time perception, and delay aversion, cognitive functions that are
problematic for the ADHD individual. They suggest the ADHD brain often operates in a
hyper-speed mode leading to the observed deficiencies in these constructs of cognition.
There is also evidence that memory tasks may be more difficult for the ADHD individual

15
due to a limited storage mechanism within the memory circuit which inhibits active
processing of information. In order to fully understand dysregulated executive
functioning, impaired cognitive functioning and maladaptive behaviors, it is necessary to
understand the role of the neurobiological forces at work.
Motor Function
While ADHD is primarily associated with behavioral symptoms, there is evidence
of the presence of motor coordination dysfunction within this population, not attributed to
other neurological deficiencies (Piek, Pitcher & Hay, 1999). Motor dysfunction, observed
in manual dexterity tasks and handwriting skills, is reported to be present in 50 percent of
individuals with ADHD (Piek, Pitcher & Hay, 1999; Flapper, Houwen & Schoemaker,
2006). Deficiencies in attention and impulse are predominant predictors for motor deficits
within the ADHD population (Tseng, Henderson, Chow, & Yao, 2004). Motor
coordination dysfunction is not currently recognized as a component of the ADHD
diagnosis based on DSM-V criteria. However, many countries in Europe, the United
Kingdom, and Scandinavia, refer to ADHD as Hyperkinetic Disorder and include the
impairment of motor development in addition to the inattention, impulsivity and
hyperactivity components when diagnosing the disorder (Stray et al., 2009).
Neurobiology of ADHD
Neurobiological dysfunction provides one explanation of the etiology of ADHD
and may aid in understanding cognitive deficiency. Hummer et al. (2011) have defined
executive function as “a collective set of processes that encompasses planning, cognitive
flexibility, working memory, organization, inhibition and problem solving”. These are
often areas of functioning that are seemingly difficult for the ADHD individual.
16
Disorganization, inattention to detail, difficulty with focusing attention, and boredom
often lead to defective planning, forgetfulness and uninhibited behaviors.
Although many consider executive dysfunction a collective set of maladaptive
behaviors, some research has suggested there may be a neurobiological pathway
associated with executive function. Marx, et al. (2009) have suggested that there are two
separate neurobiological pathways, a cognitive pathway and a motivational pathway, that
are useful for explaining ADHD symptoms. The cognitive pathway is the pathway most
associated with deficits in executive functioning and may be the primarily associated with
cognitive and behavioral dysregulation (Marx, et al., 2009). However, the motivational
pathway is more associated with the reward system and may explain dysfunction in
inhibition and an inability to delay gratification which is also an indicator of behavioral
dysfunction (Marx, et al., 2009).
There is a neurobiological component that is seemingly the most likely
explanation and has led to the exploration of the genetic etiology of the disorder. Through
the evaluation heritability data researchers have been able to determine that 80 percent of
the etiology of ADHD can be attributed to genetic factors (Biederman & Farone, 2001).
Adoption and twin imaging studies have implicated catecholamine disruption, primarily a
deficiency in the dopaminergic systems within the subcortical regions of the brain, as a
leading genetic explanation for ADHD brain dysfunction (Biederman & Farone, 2001).
The dopaminergic pathways are neural pathways that transmit the
neurotransmitter dopamine throughout the sub-cortical regions of the brain. Dopamine is
synthesized in the brain and plays a fundamental role in attention, thinking, alertness,
focus, effort, and motivation (Hunt, 2006). Dopamine also helps to regulate mood and

17
emotional stability and is a key component in the brain’s reward and motor functioning
systems (Powers, 2004). Volkow, Wang, & Kollins (2009) have shown through brain
imaging studies that individuals with ADHD have disrupted dopamine transmission
patterns which may be the underlying cause of inattention, impulsivity, hyperactivity and
deficits in reward and motivation. It has also been suggested that individuals with ADHD
may have minimal neurotransmitter levels, in the range of ten to twenty-five percent
(Carver, 2009). Low levels of dopamine have been linked to deficits in the inhibitory
process, which has been identified as the core ADHD deficit (Carver, 2009; Seidman et
al., 2004).
The dopaminergic system consists of five dopamine receptors, essential for
central nervous system functioning (Wu, Xian, Sun, Zou, Zhu, 2012). It has been
suggested that some of the receptors not only pick up neurochemicals, they regulate
dopamine production, consequently making them responsible for the initiation of the
synthesis and release of the neurotransmitter throughout different areas of the brain (Wu
et al., 2012) Dysregulation of these particular systems is highly implicated in individuals
with ADHD. Some researchers have evaluated the D2 and D4 receptor genes in order to
gain a better understanding of brain functioning in ADHD populations.
The D2 receptor gene has been found to be the regulator of the catecholamine
system in the brain (Wu, et al., 2012). Catecholamines are a group of neurochemicals
involved in neural regulation and have been implicated in neural dysregulation.
Dopamine is considered to be one of the primary Catecholamines and attention to this
system is important for gaining a better understanding of the neural workings of the
ADHD brain. The D4 receptor, the primary dopamine receptor in the brain, has also been

18
evaluated and has been implicated in other neuropsychological disorders such as
Parkinson’s disease and schizophrenia, in addition to ADHD (Wu et al., 2012). The D4
receptor is responsible for the modulation of neuronal firing and has been found to be
impaired in those with neuropsychological disorders leading to dysregulated motor
activity (Wu, et al., 2012).
As previously discussed, dysregulated function in the dopamine motivational
pathway, plays a role in a dysregulated reward and motivation process. Some research
suggests this is a result of disrupted neurotransmission in the ADHD brain (Volkow, et
al., 2009). Reward and motivation deficits are commonly observed in ADHD populations
and may be the result of abnormal neural responses to reward and punishment. This
dysregulation may lead to the impulsive behaviors and the inability to delay gratification.
Understanding the role of these structures in the brain is important when considering how
to treat the symptoms associated with ADHD. Although it seems that little is known
about the exact nature of the pathophysiology of ADHD, the role dopamine plays is
undeniable. Researchers have been looking at dopaminergic systems for over three
decades and while it seems little progress has been made aside from
psychopharmacological development, there have been tremendous gains in understanding
how these systems work (Blum et al., 2008).
Treatment Recommendations
The use of psychostimulant medications is the most common treatment for
controlling the symptoms of hyperactivity, impulsivity and inattention in individuals
diagnosed with ADHD. The Center for Disease Control reports that 50% of diagnosed
ADHD children and adolescents are being treated with prescription medication (2008).

19
Methyphenidate (Ritalin) and l-amphetamine (Adderall), the two most commonly
prescribed ADHD medications, act on the subcortical regions of the brain to increase
dopamine production and concentration of the neurotransmitter in these regions (Tang,
Wanchoo, Swan, & Dafney, 2009). Psychostimulant medications have also been found
to modulate the expression of BDNF, elevating BDNF activity in the brain (Ribasés et
al., 2008; Tsai, 2007). In addition, BDNF has been found to modulate neuroadaptations
and locomotor activity through the dopaminergic pathways (Ribasés et al., 2008).
The primary goal of treating ADHD with stimulant drugs is to induce the
stimulating response of chemical production and preventing the reuptake process.
Dopamine is a chemical messenger responsible for message transmission to certain
regions of the brain. The synaptic cleft of a neuron is the location in which
neurotransmitters like dopamine are released in order to pass along the message they are
sending to other neurons. When that message is delivered to the receiving neuron, the
neurotransmitter is sent back into the cell of the initiating neuron; this is the reuptake
process. When reuptake occurs the chemical is not longer available for use by the
messengers. The more dopamine the messengers have to use the longer those messengers
have to send the messages and the more regulated the systems of the brain become. Both
methylphenidate and 1-amphetamine inhibit dopamine reuptake presynaptically
increasing the levels of dopamine available in the synaptic cleft (Kolar, Keller,
Golfinopoulos, Cumyn, Syer, Hechtman, 2008)
While stimulant use has proven to be efficacious, long-term stimulant use is not
without consequences. Some researchers have observed the effects of these drugs through
animal observation. Tang et al. (2009) have looked at the negative impacts of long-term

20
stimulant use in rats and have found that tolerance, withdrawal and behavioral
sensitization actually reduce natural dopamine production, facilitate the need for greater
amounts of the drug, and can lead to chemical dependence. Although there have been a
few studies looking at whether or not stimulant use causes structural changes within the
brain, there is no information on long-term use and dependency, or, disruption of the
developmental process.
Although stimulant medication is the most common method of treatment,
alternative treatment modalities have been suggested. Psychotherapy, utilizing a
combination of psychoeducation and psychosocial treatment, has been recommended as
an alternative to psychostimulant medication therapy. The combination of
psychoeducation, teaching individuals about their disorder, and psychosocial treatment
such as cognitive-behavioral therapy (CBT), is the most common approach used with
adult populations. Approaches involving CBT involve focusing on self-mediation and
control strategies, in order to promote self-controlled behaviors (Kolar et al., 2008).
Exercise and Executive and Motor Functioning
Sedentary behavior is often associated with a plethora of negative health
consequences including cognitive decline. This may be particularly concerning in
sedentary populations with a genetic predisposition for cognitive impairments, such as
individuals with ADHD. In recent years, the connection between brain health and
exercise has been highlighted as an important determinant of health. Research indicates
there is a positive relationship between adhering to a regular physical activity regimen
and improved cognitive function (Etnier, Nowell, Landers, Sibley, 2006). Verret, Guay,
Berthiaume, Gardiner, & Beliveau, (2010) have found that physical activity has a positive
21
impact on motor performance, behavioral scores which evaluated social skills, attention,
thought processes, and information processing.
Chaddock, Hillman, Pontifex, Johnson, Raine, & Kramer, (2012) have evaluated
aerobic fitness as a mediator for cognitive performance in adolescents, and have found
that achievement scores, cognitive performance and attentional processes are superior in
fit versus not-fit. They have also found that the un-fit group demonstrated deficiencies in
performance during conditions requiring greater inhibition control, suggesting that fit
individuals are better able to control their cognitive processes (Chaddock et al., 2012).
The facilitation of improved cognition through fitness is also evident in the later stages of
the life cycle and does not diminish across the lifespan. Researchers have observed this in
adult and elderly populations. Fitness is predictive of achievement in the adult life and
can delay cognitive impairment associated with neuropsychological disorders (Chaddock,
et al., 2021).
Physical activity is generally viewed as a way to maintain optimum physical
health and is recommended at some level for most populations. Current National
Institutes of Health recommendations for adults are at least 150 minutes of moderate-
intensity or 75 minutes of vigorous aerobic activity per week for optimum physical
health. Although, physical activity is often regarded as a physical health benefit, there is a
great deal of evidence supporting the idea that it is equally important for cognitive health.
Some researchers have specifically looked at the benefits of exercise as a means
of improving functioning within individuals with ADHD. Verret et al. (2012) have shown
that significant behavioral and cognitive function improvements were seen after a
physical activity program was implemented for a period of 10 weeks. Improvements were

22
observed in informational processing, motor performance, behavioral adaptability, and
attention within the ADHD population. Interestingly, there were no significant
differences in the improvements in fitness parameters between groups; the only
improvement was found in processes involving executive functioning. Dishman, et al.,
(2006) have looked at the effects of exercise on both emotional and cognitive processes
and have found that exercise is more positively associated with processes that require
higher-level executive control, such as scheduling, planning, and task coordination;
changes in the brain’s plasticity, down to the intercellular level, were also observed, and
are thought to be responsible for improvements in learning and memory.
Stroth, Hille, Spitzer, & Reinhardt, (2009) have also studied the effect of exercise
on cognition and report that aerobically fit individuals perform better on tasks involving
learning, attention, and memory. They evaluated speed tasks, visuospatial tasks, and
visual attention, processes of executive control, and found that individuals in the fit
category significantly outperformed their unfit counterparts (Stroth et al., 2009). They
also suggest that exercise is not only great for improving cognitive function in childhood
and adolescence, it is essential for preventing cognitive decline in adults.
Exercise and Neurological Changes
Neuroplasticity, the ongoing process involving neural pathway synthesis as well
as the development of new structures, is enhanced through exercise which improves the
synthesis and use of neural structures, neurochemicals, and neuroproteins (Alberts et al.,
2011). The synthesis of neural receptors is has been implicated in both cognitive change,
changes in the reward/motivation mechanisms as well as movement control (Simonen, et
al., 2003). Dopamine is the primary neurochemical deficit in the ADHD brain and has

23
been implicated in the feeling of reward and pleasure. Due to dysregulated dopamine
levels, the reward and pleasure pathways become dysregulated in those with
neuropsychological disorders, drug or alcohol addiction, and substance abuse. With
substance abuse, greater consumption of the substance leads to an increase in the
activation of dopamine, the pleasure chemical, as well as an increased desire for greater
amounts of the activation substance. Individuals with ADHD have demonstrated reduced
reward pathways as well as the inhibited production and release of dopamine. It has been
suggested that exercise may alter dopaminergic activation and the reward center response
through a positive feedback loop, leading to greater activation of neurochemical synthesis
and activation (Simonen, et al., 2003). Evaluating how exercise alters the dopaminergic
system is important to understand how this neurotransmitter can be altered.
In animals studies, increased levels of exercise, have led to increased production
and release of the neurotransmitter dopamine due to an increase in the plasticity of the
neurotransmitter systems (Foley & Fleschner, 2008). It has been discovered that not only
can dopamine production be improved by exercise an increase in dopamine receptor sites
also occurs. Foley and Fleshner (2008) have observed substantial changes in production
of dopamine and in the growth of receptors in mice that adhered to an activity regimen
when compared to sedentary mice. Lenz (2012) also identifies structures of the brain
impacted by exercise due to changes in neurochemical availability and suggests that
exercise based therapies may reduce the chance for negative outcomes associated with
stimulant medication use. One of the primary benefits identified is an immediate change
in neurochemical availability observed after a single bout of exercise; stimulant

24
medications can take anywhere from one to five hours to produce a therapeutic effect
(Lenz, 2012).
The effects of exercise on improvements in cognition are also thought to be
mediated by BDNF through an interactive process between the neuroprotein and energy
metabolism that modulates neuronal plasticity (Gomez-Pinilla, Vaynman & Ying, 2008).
Neuroplasticity involves changes in the neural pathways, through the formation of new
neural connections and synapses, in response to changes in the neural environment. Brain
derived neurotrophic factor (BDNF) is a neural protein that plays a key role in the
regulation of neurogenesis, the prevention of neuronal death, and may mediate synaptic
and morphological plasticity (Tsai, 2003). The growth of neuronal tissues, neurogenesis,
while occurring most rapidly during pre-natal development, is believed to continue
throughout the lifespan. Neurogenesis is directly related to an individual’s brain volume,
which has been found to be five percent less in individuals with ADHD compared to
those without the disorder, suggesting an impaired neurodevelopment process (Tsai,
2003). The BDNF protein is directly involved in synthesis of the dopaminergic structures,
dopamine transporters and receptors, as well as dopaminergic function (Tsai, 2007).
Deficiency in BDNF activity may be an underlying mechanism and play an integral role
in the pathogenesis of ADHD.
Assisted (Forced) Exercise
Assisted or Forced Exercise has been defined as aerobic exercise that is
mechanically augmented to assist the participant to maintain an exercise rate that is
greater than the preferred voluntary rate (Alberts et al., 2011). Forced exercise protocols
have been used in addition to VE in order to evaluate neurocognitive and motor control

25
changes. Although there is an established link between cognitive improvement and VE in
ADHD populations, AE has yet to be evaluated. AE has been found to elicit an even
greater improvement response in other populations demonstrating neurocognitive
impairments.
In order to better understand how exercise influences the dopaminergic systems,
animal models deficient in the neurotransmitter, as well as dopaminergic neurons, have
been evaluated under exercise conditions. Under AE conditions, neuroprotection, the
preservation of dopaminergic neurons and the restoration of dopaminergic terminals, has
been demonstrated (Petzinger et al., 2013). Exercise has been found to enhance
neurorestoration through modulating dopamine neurotransmission and synaptic
occupancy, altering dopamine receptor expression, leading to the restoration of
neuropsychological properties (Petzinger et al., 2013). While the exact mechanism is
unknown, AE has been show to increase levels of dopamine availability, leading
researcher to posit that assisted exercise also elevates levels of BDNF facilitating changes
in Neuroplasticity (Alberts et al., 2011).
In healthy adults acute bouts of VE have been shown to increase levels of BDNF
and have been associated with increased levels of neurotransmitters, both of with have
been implicated in improvements in cognition, learning and memory (Alberts et al.,
2011). The effects of AE has also been evaluated in individuals with Parkinson’s disease
(PD), a degenerative neurological disorder characterized by the loss of dopamine and the
degeneration of dopaminergic neurons, leading to impaired in motor and executive
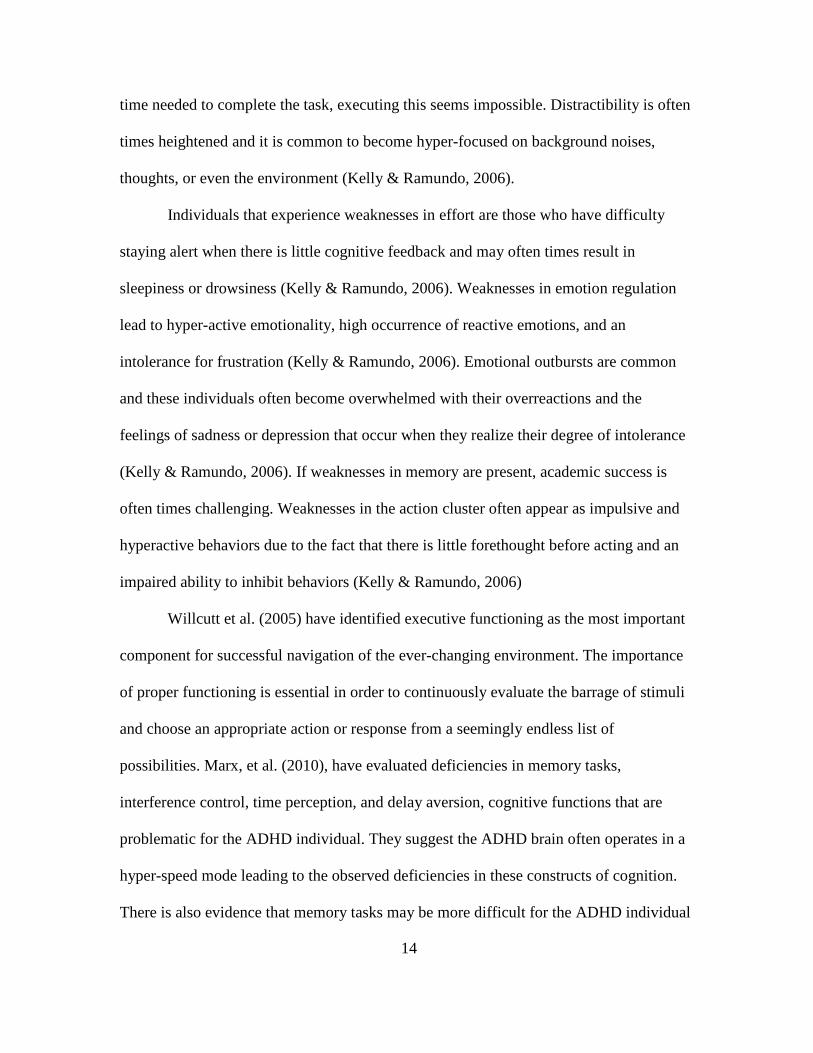
function (Alberts et al., 2011; Petzinger et al., 2013). Exercise facilitates changes within
the central nervous system through increased extrinsic and intrinsic feedback (Figure 2),

the latter of which is even greater during
feedback is thought to increase afferent input
factors and dopamine, aiding in
In individuals with PD, AE compared to
improvements in motor control and is likely able to influence cognition as well (Alberts
et al., 2011).
Figure 2 – Schematic of the pnervous system structuresintrinsic feedback, leading to increased production of neurotrophic factors and dopamine; resulting in increased cognitive and motor functions. Similar patterns of improvement have been demonstrated in Down syndrome
(DS) populations following acute bouts of
disability which causes intellectual
compromised CNS functioning,
working memory, inhibition, planning, set
26
the latter of which is even greater during AE (Alberts et al., 2011). The increased intrinsic
thought to increase afferent input, triggering the release of neurotrophic
factors and dopamine, aiding in Neuroplasticity and neurogenesis (Alberts et al., 2011).
compared to VE, has been associated with greater
control and is likely able to influence cognition as well (Alberts
chematic of the proposed effect of assisted exercise on the central nervous system structures, mediated by an increase in afferent signaling t
leading to increased production of neurotrophic factors and resulting in increased cognitive and motor functions.
Similar patterns of improvement have been demonstrated in Down syndrome
populations following acute bouts of AE. Down syndrome is a developmental
disability which causes intellectual and physical impairment, and is associated with
compromised CNS functioning, demonstrated through deficits in cognitive functioning
ry, inhibition, planning, set-shifting and motor functioning (Ringenbach,
(Alberts et al., 2011). The increased intrinsic
of neurotrophic
(Alberts et al., 2011).
, has been associated with greater
control and is likely able to influence cognition as well (Alberts
exercise on the central mediated by an increase in afferent signaling through
leading to increased production of neurotrophic factors and
Similar patterns of improvement have been demonstrated in Down syndrome
Down syndrome is a developmental
associated with
deficits in cognitive functioning,
shifting and motor functioning (Ringenbach,

27
Chen & Alberts, 2014). As with the PD population, AE has been shown to improve
functional movement, cognitive planning, and information processing (Ringenbach, Chen
& Alberts, 2014). Although ADHD is not directly associated with PD or DS, there are
similar structural and chemical impairments that explain many of the deficits associated
with each of the disorders. The primary focus of this research is to explore whether or not
similar patterns of improvement will be achieved in individuals with ADHD following
AE compared to VE.

28
CHAPTER 3
METHODOLOGY
Participants and Study Design
Eight female volunteers between the ages of 18 and 24 were screened for
attention deficit hyperactivity disorder. Selection was limited to individuals with a
diagnosis of ADHD by a qualified health care professional; met Physical Activity
Readiness Questionnaire (PAR-Q) criteria in order identify if the participant was positive
for risk factors associated with aerobic exercise; had no physical limitations for cycling;
had no history of trauma or injury to the brain; did not meet current physical activity
guidelines. Participants were recruited through flyers posted at the Arizona State
University Downtown and Tempe campuses as well as word of mouth (Appendix A). The
Arizona State University Institutional Review Board evaluated and approved all
procedures. Each participant was required to provide informed consent prior to
participation in the study (Appendix B).
Qualified professionals assess and indentify the presence of ADHD using the
diagnostic criteria of the DSM-IV. There are three types of ADHD; (1) ADHD
predominantly inattentive type; (2) ADHD predominantly hyperactive-impulsive type;
(3) ADHD combined hyperactive-impulsive and inattentive subtype; all of which were
accepted for the study. Pharmaceuticals are often prescribed to help with the symptoms of
ADHD and participants taking medications were accepted as well as those not receiving
prescribed medications. Participants were randomly assigned to either a treatment as
usual group or an experimental group.

29
A between group pre-test/post-test design with two treatment groups was
administered over a period of six weeks to inactive, female participants with ADHD. An
evaluation and pre-test was conducted on both groups to obtain demographic and baseline
executive and motor function assessment data. A final evaluation and post-test session
was conducted at the end of six weeks to assess any changes in executive and motor
function.
Treatment as Usual (Voluntary Exercise): This group consisted of participants
cycling on a stationary cycle ergometer at a voluntary speed for 30 minutes. The rate of
cycling (cadence, rpm’s) was voluntarily selected by the participant. Each cycling session
was preceded by a five minute warm-up followed by a five minute cool down. Heart rate
and cadence were monitored for the duration of the session, with an average being
recorded every minute (Appendix C).
Experimental Treatment (Assisted Exercise): This group consisted of participants
cycling on a stationary cycle ergometer at an assisted predetermined speed for 30
minutes. In order to determine the cadence at which each participant was to cycle, the
participant first cycled at a voluntary speed for five minutes during which an average
voluntary cadence was observed and recorded. The average cadence was then increased
by 35 percent to determine the assisted rate at which the motor was to be set. Each
cycling session was preceded by a five minute warm-up followed by a five minute cool
down. Heart rate and cadence were monitored for the duration of the session, with an
average being recorded every minute (Appendix D).

30
Exercise Equipment and Evaluation
Cycling Equipment: A modified Theracycle Model 200 motorized cycle,
developed for use in populations with limited mobility, was used for this study in
conjunction with the Power Control Monitor (PCM). The PCM stores HR, power
produced by the subject, power contribution of the motor, and cadence. There were also
safety measures in place to ensure participant safety such as an emergency stop tether and
an excessive load detector within the motor. The motorized component of the Theracycle
was only used in the AE group. Cadence (revolutions per minute) was manually recorded
every minute during the 30 minute exercise session.
Heart rate: The participants wore a Polar HR monitor (Mode S 610i; Polar
Electro, Finland) in order to measure heart rate during exercise. This model transmitted
data via a short-range radio to the PCM in order to collect data during the 30 minute
exercise session. Average heart rate data was manually recorded every minute of the
exercise bout.
Exercise Intensity: Predicted heart rate (HR) values were calculated to determine
the appropriate intensity of the exercise administered to the participants. There is no
evidence of variance in HR between ADHD adults and typical adults. Target heart rates
were calculated based on a percentage of maximal heart rate. Maximal heart rate was
calculated using the following formula for typical populations: Max HR = 207 – (0.7 X
age). The target heart rate was calculated using the following formula: Target HR =
(HRmax – HRrest) X % desired intensity (60-80%) + HR Rest. Participants were
encouraged to maintain an exercise intensity to keep their target heart rate close the
calculated value.

31
Executive and Motor Function Measures
Each participant was evaluated for deficiencies in executive function based on
Brown’s model of executive function. Each cluster of cognitive function was assessed pre
and post-intervention with the following tasks; (1) Activation and planning – Tower of
London; (2) Focus, attention, and set shifting – Stroop Test; (3) Sustaining effort and
processing speed – Verbal Fluency task; (4) Emotion regulation – Difficulty with
Emotion Regulation Scale; (5) Working memory – Auditory Number Memory task; (6)
Action – Self Regulation Questionnaire.
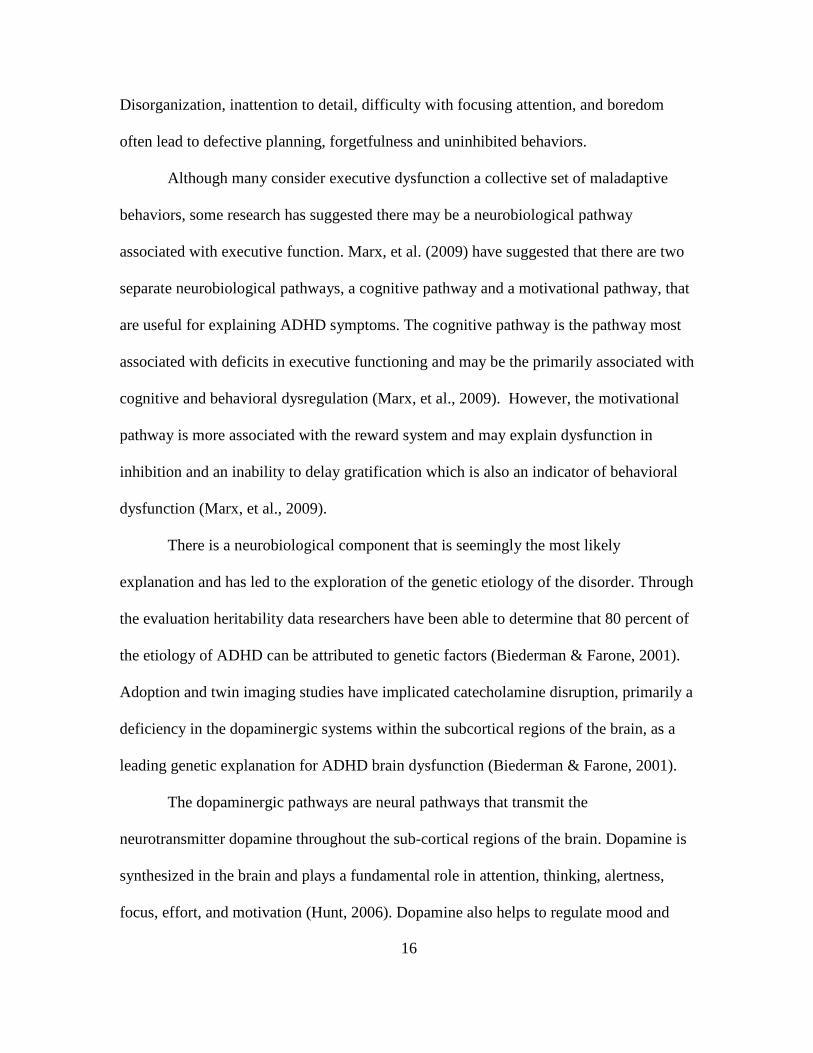
Tower of London: Cognitive planning represents the higher-order processes
necessary for problem solving and adaptation involving interaction between the
prefrontal lobe, cortical and sub-cortical regions of the brain (Culbertson& Zillmer,
1998). The Tower of London (r = .81) assesses cognitive planning and problem solving
skills through a series of tasks. The researcher placed three colored balls onto three pegs
always in the same starting position; the participant was shown a picture of which the
colored balls were to be positioned (goal pattern) and was given a total number of moves
in which they were to replicate the goal pattern. The time for completion, attempts, and
the number of moves the participant made were recorded (Appendix E).
Figure 3 – Tower of London diagram showing the initial position followed by

32
examples of the goal position (below) and the number of moves required to get to the goal position (above).
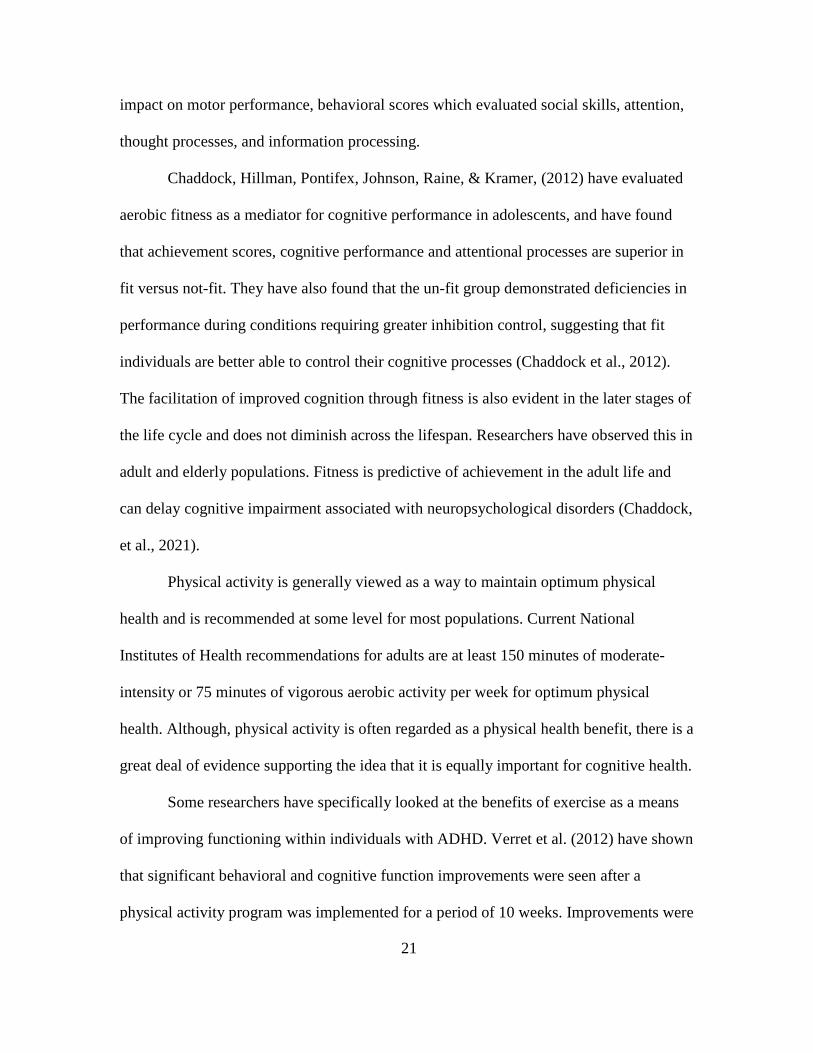
Stoop Test: Focus, attention, and set-shifting (the ability to shift cognitive
processes when responding to environmental change) are characteristics of the cognitive
process of activation. Cognitive activation involves being exposed to a stimulus and
determining an appropriate response, requiring a degree of interference control requiring
focus, attention and set-shifting (Lansbergen & Kenemans, 2007; Gualtieri & Johnson,
2006). The Stroop test (r = .87) has been widely used to assess and quantify response
inhibition and interference control deficiencies within the ADHD population. The
participant was given a set of cards and instructed to read a set of baseline words
displayed in black ink (Figure 3a), name a set of colored blocks (Figure 3b), and read a
set of incongruent ink color words (Figure 3c) as quickly as they could in 45 seconds.
The number of responses (maximum of 100) as well as the time of completion was
recorded for each task (Appendix F).
Figure 4a – Baseline word set

33
Figure 4b – Colored block set
Figure 4c – Incongruent color word set
Verbal Fluency: Cognitive processing requires effort, planning and self
monitoring as a means of sustaining cognitive behavior involving the frontal lobe regions
of the brain (Kozial & Stout, 1992). The Verbal Fluency task (r = .92) assesses cognitive
output and the process of response inhibition. The objective for the participant was to
produce as many words belonging to a given category, semantic or phonemic, within 60
second time periods which were recorded by the researcher (Appendix G).

34
Difficulties with Emotion Regulation Scale: The domains of emotion regulation
involve affect regulation and behavioral control. Individuals with ADHD have a greater
propensity for aggression and dysregulated emotional responses, characterized as high
intensity behaviors as well as high levels of both positive and negative behaviors
(Wheeler Maedgen & Carlson, 2000). The Difficulties with Emotion Regulation Scale (r
= .88) assess the degree to which individuals are able to regulate their emotional
behaviors (Neumann et al., 2009). The DERS questionnaire was administered by the
researcher and answered by the participant (Appendix H).
Auditory Digit Span: Working memory underlies several cognitive abilities,
involving the short-term ability to retain and manipulate information, and has been found
to be impaired in individuals with ADHD (Klingberg, Forssberg & Westerberg, 2002;
Gropper & Tannock, 2009). The Auditory Digit Span task (r = .80) required the
researcher reading aloud a sequence of digits, each of which became increasingly longer,
at a rate of one number per second. The task consisted of forward and backwards trials.
During the forward trials the participant is asked to repeat the sequence exactly as it was
given. During the backward trial the participant was instructed to repeat the sequence in
reverse order. Responses were recorded and scored by the researcher (Appendix I).
Self-Regulation Questionnaire: Self-regulation involves the ability to develop,
implement and maintain behavior and may be hindered due to one or more deficits in the
following processes; receiving relevant information, evaluating the information,
triggering change, searching for options, formulating a plan, implementing the plan, and
assessing the plan’s effectiveness (Miller & Brown, 1999; CAASA, 2006). The self-

35
regulation questionnaire (r = .94) was administered by the researcher and answered by
the participant (Appendix J).
Purdue Pegboard: Motor and movement coordination processes involving fine
and gross motor control will be assessed by evaluation of manual dexterity. The Purdue
Pegboard (r = .76) assess fundamental motor limitations through the evaluation of intra-
and interlimb movements and has been used to detect neuropsychological deficits
(Redden et al., 1988). The tests consisted of three trials and required the participant to
unimanually and bimanually place pins, or assemble units of pins, washers and collars, as
modeled by the researcher. The objective was to place or assemble as many units or sets
possible during a timed trial (Appendix K).
Figure 5 – Purdue Pegboard
Statistical Analysis
All outcome measures were tested for normality assumption using the Shapiro-
Wilk test. Descriptive statistics (M, SD) were used to estimate participants’ demographic

36
information and pre-intervention executive and motor functions at baseline. The Mann-
Whitney U tests were used to compare median differences for the executive and motor
function between VE and AE groups. The executive and motor function tests include
Tower of London (executive time and score), Stroop Test (colored block and incongruent
word tasks), Verbal Fluency (semantic, phonemic and total scores), DERS, Auditory
Digit Span (forward and backward), SRQ, and Purdue Pegboard (dominant hand, non-
dominant hand, both hands, a sum of the three, and an assembly task). The Wilcoxon
signed-rank tests were used to test median differences for the executive and motor
functions within AE and VE groups, respectively. Effect size was calculated to
determine practical significance of the experimental treatment effect using the following
threshold Cohen criteria; 1) small effect, ES = .10, 2) medium effect, ES = .30, and 3)
large effect, ES = .50. All p-values were two-tailed, and values of less than 0.05 were
considered to indicate statistical significance. Statistical analyses were conducted using
SPSS software, version 21 (SPSS 21.0 IBM Corporation, Armonk, New York, USA).

37
CHAPTER 4
RESULTS
Quantitative Data
Eight female participants were screened for this study of which six met the
ADHD and physical activity criteria. Five of the six selected participants completed the
study. One participant dropped out of the study due to scheduling difficulties. Participant
characteristics are presented in Table 1. Baseline (pre-intervention) executive and motor
function assessments are presented in Table 2.
Table 1: Participant demographic information (mean + SD; N=5) Sex (M/F) Age (Years) Height (Inches) Weight (Pounds) Physical Activity (Y/N) Medication Use (Y/N) Handedness (R/L)
0/5 21.4 + 2.3 65.0 + 1.9 151.8 + 50.1 0/5 5/0 5/0
Table 2: Pre-intervention executive and motor function assessments (mean + SD; N=5) Executive Function Tower of London – Executive Time Tower of London – Moves Stroop Test – Colored Block Task Stroop Test – Incongruent Color Word Test Verbal Fluency – Semantic Verbal Fluency – Phonemic Verbal Fluency – Combined DERS Auditory Digit Span – Forward Auditory Digit Span – Backward SRQ Motor Function Purdue Pegboard – Dominant Hand Purdue Pegboard – Non-Dominant Hand Purdue Pegboard – Both Hands Purdue Pegboard – Right, Left, Both Hands Sum Purdue Pegboard – Assembly
383.4 + 58.7 36.6 + 2.6 66.0 + 10.8 44.0 + 6.9 35.8 + 10.8 31.8 + 7.0 67.6 + 14.0 84.8 + 25.2 9.8 + 1.9 6.0 + 1.0 211 + 11.1 15.7 + 1.0 14.4 + 1.6 24.1 + 2.6 54.1 + 5.0 7.3 + 1.9

38
Executive Function Assessments: Between AE and VE Groups
The Mann-Whitney U tests detected borderline significance for several outcome
measures between VE and AE groups. For instance, Tower of London executive time
scores showed a favorable decreasing trend in total execution time for the AE group
(MDNAE = 162) when compared to the VE group (MDNVE = 308), indicating quicker
cognitive activation time, U = .00, p = .076, ES = .79 (Table 3, Figure 6). Participants in
the AE group also had a considerable increasing trend toward significance in the Tower
of London aggregate score (MDNAE = 51.0) compared to the VE group (MDNAE = 40.5),
pointing to improvements in cognitive planning, U = .00, p = .083, ES = .77, (Table 3,
Figure 7).
Participants in the AE group had a strong increasing trend for the forward
auditory digit span task (MDNAE = 13.0) when compared to the VE group (MDNVE = 10.0),
signifying improvements in working memory, U = .00, p = .083, ES = .77, (Table 3,
Figure 8). Participants in the AE group also documented a marked increasing trend for
the backward auditory digit span task (MDNAE = 10.0) when compared to the VE group
(MDNVE = 6.5), suggesting increased capacity for attention and working memory, U = .00,
p = .076, ES = .79, (Table 3, Figure 9). While each of the aforementioned measures is at
the edge of conventional levels of significance, the effect size (ES > .50) indicates AE has
a large effect on each suggesting a high level of practical significance.
Motor Function Assessments: Between Group Results
Participants in the AE group demonstrated a definite increasing trend for manual
dexterity of the dominant hand during the Purdue pegboard task (MDNAE = 18) when
compared to the VE group (MDNVE = 15.8), U = .00, p = .083, ES = .77, (Table 3, Figure

39
10), indicating increases in fine motor skill and coordination in the dominant hand. A
similar positive trend in bimanual coordination was also observed in the median scores
for bi-manual the Purdue Pegboard bimanual task in the AE group (MDNAE = 28.0) when
compared to the VE group (MDNVE = 25.3), U = .00, p = .083, ES = .77, (Table 3, Figure
11). An increasing tendency towards significance was also observed in the combined
dominant/non-dominant/both hands summed score in the AE group (MDNAE = 61.7)
when compared to the VE group (MDNVE = 56.0), suggesting improvements in gross
motor movements of fingers, hands, and arms, U = .00, p = .083, ES = .77, (Table 3,
Figure 12). Although the trends are close to meeting the conventional requirements for
statistical significance, the effect size (ES > .50) suggests AE has a large effect on manual
dexterity, bimanual coordination and overall gross motor control of the fingers, hands and
arms.

40
Table 3: Comparison profile of post-intervention executive function and motor function outcome measures between VE and AE groups, (N=5).
Profile of Outcome Measures
Measure VE AE Median Difference
Inter-quartile Range
p value
ES value
Activation Tower of London
– Executive Time
308 162 146.0 161 .076* .79**
Planning
Tower of London – Moves
40.5 51 10.5 12 .083* .77**
Focus/Attention
Stroop Test – Colored Block
71.5 78 6.5 17 .374 .39
Set Shifting Stroop Test – Incongruent Color Word
43.5 52 8.5 19 .564 .26
Effort Verbal Fluency – Semantic
42.5 52 9.5 17.5 1.00 .00
Processing Speed
Verbal Fluency – Phonemic
41 42 1.0 17 1.00 .00
Verbal Fluency – Combined
83.5 84 0.5 29.5 .564 .26
Emotion Regulation
DERS
98 69 29.0 43.5 .248 .52**
Working Memory
Auditory Digit Span – Forward
10 13 3.0 3.5 .083* .77**
Attention/ Working Memory
Auditory Digit Span – Backward
6.5 10 3.5 3.5 .076* .79**
Self Regulation SRQ
1.5 2.0 .5 1.0 .197 .56**
Motor Control Purdue Pegboard –
Dominant Hand
15.8 18 2.2 4.2 .083* .77**
Purdue Pegboard – Non-Dominant Hand
14.8 16.3 1.5 3.3 .139 .66**
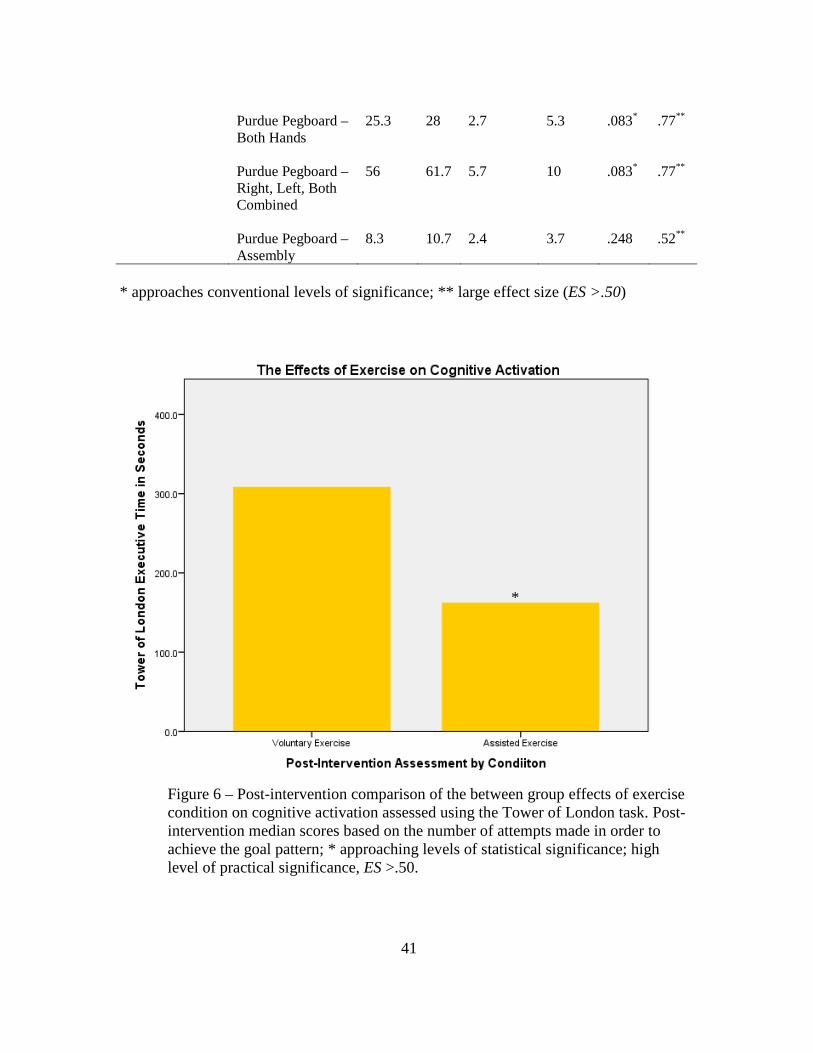
41
Purdue Pegboard –
Both Hands
25.3 28 2.7 5.3 .083* .77**
Purdue Pegboard – Right, Left, Both Combined
56 61.7 5.7 10 .083* .77**
Purdue Pegboard – Assembly
8.3 10.7 2.4 3.7 .248 .52**
* approaches conventional levels of significance; ** large effect size (ES >.50)
Figure 6 – Post-intervention comparison of the between group effects of exercise condition on cognitive activation assessed using the Tower of London task. Post-intervention median scores based on the number of attempts made in order to achieve the goal pattern; * approaching levels of statistical significance; high level of practical significance, ES >.50.
*

42
Figure 7 – Post-intervention comparison of the between group effects of exercise condition on cognitive planning assessed using the Tower of London task. Post-intervention median scores based on the number of attempts made in order to achieve the goal pattern without rule violation; * approaching levels of statistical significance; high level of practical significance, ES >.50.
*

43
Figure 8 – Post-intervention comparison of the between group effects of exercise condition on working memory assessed using the forward auditory digit span task. Post-intervention median scores based on the number of correctly repeated numerical sequences; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

44
Figure 9 – Post-intervention comparison of the between group effects of exercise condition on attention and working memory assessed using the backward auditory digit span task. Post-intervention median scores based on the number of correctly repeated numerical sequences; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

45
Figure 10 – Post-intervention comparison of the between group effects of exercise on manual dexterity assessed using the Purdue pegboard dominant hand task. Post-intervention median scores based on the number of correctly placed pegs using only the dominant hand; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

46
Figure 11 – Post-intervention comparison of the between group effects of exercise on bimanual coordination assessed using the Purdue pegboard bimanual task. Post-intervention median scores based on the number of correctly placed pegs using both hands; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

47
Figure 12 – Post-intervention comparison of the between group effects of exercise condition on gross movement of the fingers, hands and arms, using the sum of scores for dominant hand, non-dominant hand and both hand during the Purdue pegboard task. Post-intervention median scores based on the total number of correctly placed pegs; *approaching levels of statistical significance; high level of practical significance, ES >.50.
Executive Function Assessments: Within Group Results
Wilcoxon Signed-ranks tests indicated near significant differences between pre-
intervention scores and post-intervention scores on every measure but one within the AE
group (Table 4). Similar trends were not observed within the VE group (Table 5). The
median executive execution time for the Tower of London task, greatly decreased within
the AE group post-intervention (MDNAEPost = 162.0) compared to pre-intervention
(MDNAEPre = 403.0, SD = 62.1), suggesting a possible trend toward significant
improvement in cognitive activation, z = -1.60, p = .109, ES = .65 (Table 4, Figure 13).
*
48
The median scores for the Tower of London task, demonstrated an encouraging trend
within the AE group post-intervention (MDNAEPost = 51.0 compared to pre-intervention
scores (MDNAEPre = 35.0), pointing to improvements in cognitive planning, z = -1.60, p =
.109, ES = .65 (Table 4, Figure 14). There was an evident increasing trend in median
score for the Stroop test colored block task in post-intervention scores (MDNAEPost = 78.0)
compared to pre-intervention scores (MDNAEPre = 68.0), pointing to improvements in
focus and attention, z = -1.60, p = .109, ES = .65 (Table 4, Figure 15). There was also an
observed increase in the Stroop test incongruent word task score within the AE group
post-intervention (MDNAEPost = 52.0) compared to pre-intervention scores (MDNAEPre =
43,), suggesting a fairly significant improvement in set-shifting ability, z = -1.60, p =
.109, ES = .65 (Table 4, Figure 16).
The median score for the semantic verbal fluency task approached the margin of
significance within the AE group post-intervention (MDNAEPost = 52.0) when compared to
pre-intervention scores (MDNAEPre = 28.0), suggesting improvements in sustaining
cognitive effort, z = -1.604, p = .109, ES = .65 (Table 4, Figure 17). Phonemic verbal
fluency median scores are also marginally significant post-intervention (MDNAEPost =
84.0) compared to pre-intervention (MDNAEPre = 65.0, SD = 21.2), indicating improved
processing speed, z = -1.604, p = .109, ES = .65 (Table 4, Figure 18). The combined
verbal fluency median score, a sum of semantic and phonemic scores, also demonstrated
increasing trends at the brink of significance within the AE group post-intervention
(MDNAEPost = 84.0) compared to pre-intervention scores (MDNAEPre = 65.0, SD = 21.2), z
= -1.604, p = .109, ES = .65 (Table 4, Figure 19).

49
Also approaching significance, the median score for the forward auditory digit
span task increased post-intervention (MDNAEPost) = 13.0) compared to pre-intervention
scores (MDNAEPre = 9.0), signifying improvements in working memory, z = -1.604, p =
.109, ES = .65 (Table 4, Figure 20). The median scores for the backward auditory digit
span task also approached significant increases within the AE group post-intervention
(MDNAEPost = 10) compared to pre-intervention scores (MDNAEPre = 6.0), pointing to a
greater capacity for attention and working memory, z = -1.604, p = .109, ES = .65 (Table
4, Figure 21). The median rank score for the Self-Regulation Questionnaire indicated an
close to significant increase within the AE group when comparing post-intervention
scores (MDNAEPost = 2) to pre-intervention scores (MDNAEPre = 1.0), showing
improvements in self-regulating capacity, z = -1.732, p = .083, ES = .71 (Table 4, Figure
22). While all scores were at the margin of statistical significance, the effect size (ES >
.50) suggests the AE intervention had a large effect on measures of cognitive
performance following the intervention.
Motor Function Assessment: Within Group Results
Motor function assessments were also found to be approaching statistical
significance within the AE group. Near significant increases for the dominant hand
Purdue Pegboard task were observed within the AE group post-intervention (MDNAEPost =
18.0) compared to pre-intervention scores (MDNAEPre = 15.7), suggesting improvements
in fine motor skill and coordination in the dominant hand, z = -1.633, p = .102, ES = .66
(Table 4, Figure 23). A similar marginally significant trend was observed in median
scores for the non-dominant hand post-intervention (MDNAEPost = 16.3) compared to pre-
intervention scores (MDNAEPre = 13.3), suggesting improvements in fine motor skill and

50
coordination in the non-dominant hand, z = -1.604, p = .109, ES = .65 (Table 4, Figure
24). Purdue pegboard bimanual task median score also approached levels of significant
increases within the AE group post intervention (MDNAEPost) = 28.0) compared to pre-
intervention scores (MDNAEPre = 22.0), indicating improvements in bimanual
coordination z = -1.604, p = .109, ES = .65 (Table 4, Figure 25). The median score for the
combined sum of scores for dominant hand, non-dominant hand, and both hands, also
approached a significant increase within the AE group post-intervention (MDNAEPost) =
61.7) compared to pre-intervention scores (MDNAEPre = 50.7), pointing to improvements
in gross movements of the fingers hands and arms, z = -1.633, p = .102, ES = .66 (Table
4, Figure 26). The median score for the Purdue pegboard assembly task, also increased
near the limit of significance for the AE group post-intervention (MDNAEPost) = 10.7)
compared to pre-intervention scores (MDNAEPre = 6.3), representing improvements in
fingertip dexterity, z = -1.604, p = .109, ES = .65 (Table 4, Figure 27). All scores for
motor function demonstrated improvements just outside the conventional levels of
significance but the effect size (ES > .50) suggests the AE intervention has a large effect
on motor function task performance.

51
Table 4: Comparison profile of executive function and motor function outcome measures within the assisted cycling group, (n=3). Measure Assisted
Exercise Pre
Assisted Exercise Post
Median Difference
p value
ES value
Executive Function Activation Tower of
London – Executive Time
403.0 162.0 241.0 .109* .65**
Planning
Tower of London – Moves
35.0 51.0 16.0 .109* .65**
Focus/Attention Stroop Test – Colored Block
68.0 78.0 10.0 .109* .65**
Set Shifting Stroop Test – Incongruent Color Word
43.0 52.0 9.0 .109* .65**
Effort Verbal Fluency – Semantic
28.0 52.0 24.0 .109* .65**
Processing Speed Verbal Fluency – Phonemic
25.0 42.0 17.0 .109* .65**
Verbal Fluency – Combined
65.0 84.0 19.0 .109* .65**
Emotion Regulation
DERS
68.0 69.0 1.0 .414 .33
Working Memory/ Attention
Auditory Digit Span – Forward
9.0 13.0 4.0 .102* .67**
Working Memory Auditory Digit Span – Backward
6.0 10.0 4.0 .102* .67**
Self Regulation SRQ
1.0 2.0 1.0 .083* .71**
Motor Function

52
Manual Dexterity Purdue Pegboard – Right Hand
15.7 18.0 2.3 .102* .66**
Purdue Pegboard – Left Hand
13.3 16.3 3.0 .109* .65**
Purdue Pegboard – Both Hands
22.0 28.0 6.0 .109* .65**
Purdue Pegboard – Right, Left, Both Combined
50.7 61.7 11.0 .102* .66**
Purdue Pegboard – Assembly
6.3 10.7 4.4 .109* .65**
* approaches conventional levels of significance; ** large effect size (ES >.50)

53
Table 5: Comparison profile of executive function and motor function outcome measures within the voluntary cycling group, (n=2).
Measure Voluntary Exercise Pre
Voluntary Exercise Post
Median Difference
p value
Executive Function Activation Tower of
London – Executive Time
407.0 308.0 99.0 .180
Planning
Tower of London – Moves
38.0 40.5 2.5 .317
Focus/Attention Stroop Test – Colored Block
69.0 71.5 2.5 .655
Set Shifting Stroop Test – Incongruent Color Word
45.5 43.5 2.0 .655
Effort Verbal Fluency – Semantic
39.5 42.5 3.0 .180
Processing Speed Verbal Fluency – Phonemic
35.5 41.0 5.5 .180
Verbal Fluency – Combined
75.0 83.5 8.5 .180
Emotion Regulation
DERS
100.0 98.0 2.0 .180
Working Memory/ Attention
Auditory Digit Span – Forward
10.5 10.0 0.5 .655
Working Memory Auditory Digit Span – Backward
6.0 6.5 0.5 .655
Self Regulation SRQ
1.5 1.5 0 1.00
Motor Function

54
Manual Dexterity Purdue Pegboard – Right Hand
15.3 15.8 0.5 .180
Purdue Pegboard – Left Hand
14.3.0 14.8 0.5 .655
Purdue Pegboard – Both Hands
25.0 25.3 0.3 .655
Purdue Pegboard – Right, Left, Both Combined
54.7 56.0 1.3 .655
Purdue Pegboard – Assembly
6.8 8.3 1.5 .180

55
Figure 13 – Pre and post intervention comparison of the within group effects of exercise condition on cognitive activation. Median scores based on total execution time for completion of the Tower of London task; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

56
Figure 14 – Pre and post intervention comparison of the within group effects of exercise condition on cognitive planning assessed using the Tower of London task. Median scores based on the number of attempts made in order to achieve the goal pattern without rule violation; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

57
Figure 15 – Pre and post intervention comparison of the within group effects of exercise condition on cognitive attention assessed using the Stroop test colored block task. Median scores based on the number of blocks correctly named within 45 seconds; *approaching levels of statistical significance; high level of practical significance, ES >.50.
*

58
Figure 16 – Pre and post intervention comparison of the within group effects of exercise condition on set-shifting assessed using the Stroop test incongruent color word task. Median scores based on the number of incongruent words correctly read within 45 seconds; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

59
Figure 17 – Pre and post intervention comparison of the within group effects of exercise condition on sustaining effort assessed using the verbal fluency semantic task. Median scores based on the number of given responses in 60 seconds; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

60
Figure 18 – Pre and post intervention comparison of the within group effects of exercise condition on processing speed assessed using the verbal fluency phonemic task. Median scores based on the number of given responses in 60 seconds; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

61
Figure 19 – Pre and post intervention comparison of the within group effects of exercise condition on cognitive effort assessed using the verbal fluency combined semantic and phonemic scores. Median scores based on the combined number of given responses in 60 seconds; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

62
Figure 20 – Pre and post intervention comparison of the within group effects of exercise condition on working memory assessed using the forward auditory digit span task. Median scores based on the number correctly repeated numerical sequences; *approaching levels of statistical significance; high level of practical significance, ES >.50
*
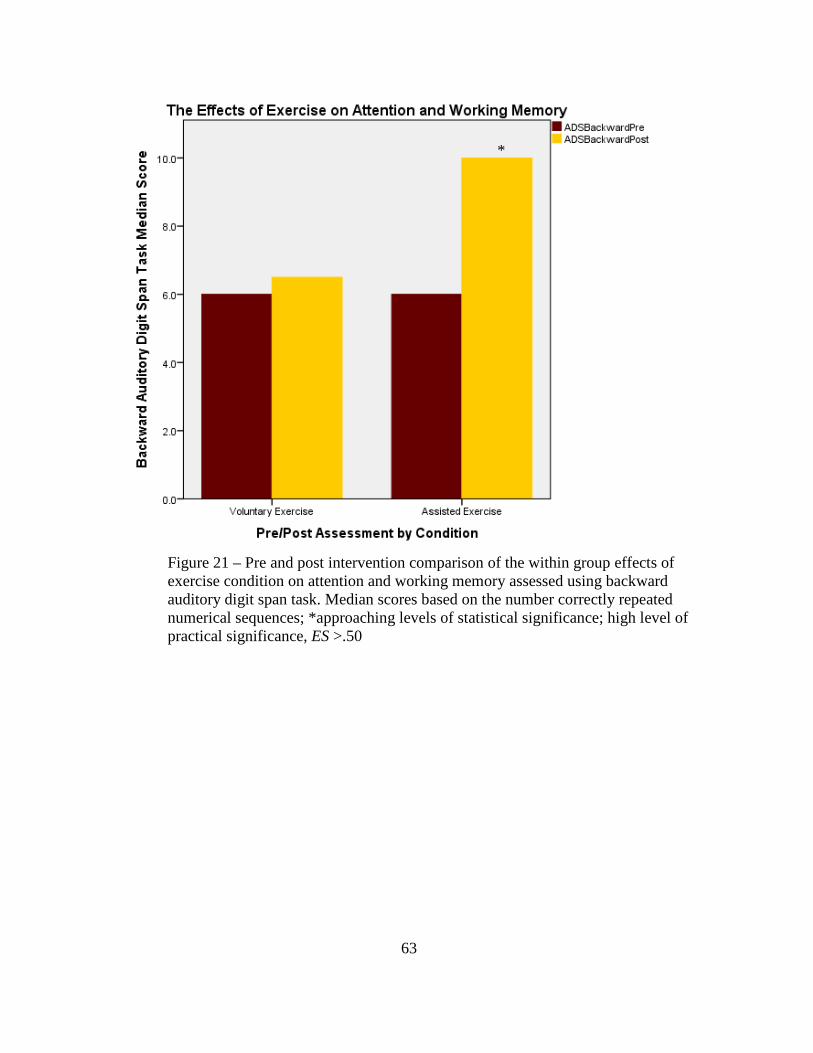
63
Figure 21 – Pre and post intervention comparison of the within group effects of exercise condition on attention and working memory assessed using backward auditory digit span task. Median scores based on the number correctly repeated numerical sequences; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

64
Figure 22 – Pre and post intervention comparison of the within group effects of exercise condition working memory assessed using Self-Regulation Questionnaire. Median scores based on the group classification value based on the scored questionnaire; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

65
Figure 23 – Pre and post intervention comparison of the within group effects of exercise condition on manual dexterity assessed using the Purdue Pegboard. Median scores calculated based on the group the number of pins placed in the pegboard in 30 seconds using the dominant hand; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

66
Figure 24 – Pre and post intervention comparison of the within group effects of exercise condition on manual dexterity assessed using the Purdue Pegboard. Median scores calculated based on the group the number of pins placed in the pegboard in 30 seconds using the non-dominant hand; *approaching levels of statistical significance; high level of practical significance, ES >.50
*
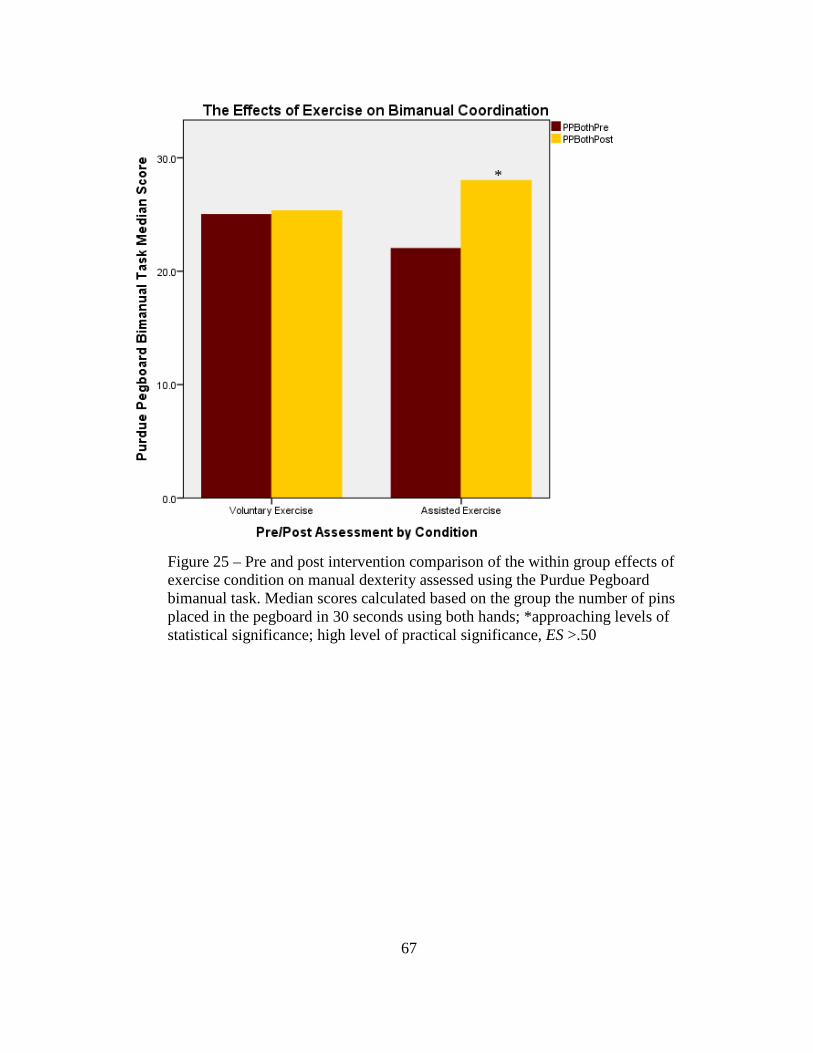
67
Figure 25 – Pre and post intervention comparison of the within group effects of exercise condition on manual dexterity assessed using the Purdue Pegboard bimanual task. Median scores calculated based on the group the number of pins placed in the pegboard in 30 seconds using both hands; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

68
Figure 26 – Pre and post intervention comparison of the within group effects of exercise condition gross movement of the fingers, hands and arms. Median scores calculated based on the summed Purdue Pegboard scores for dominant, non-dominant, and both hands tasks; *approaching levels of statistical significance; high level of practical significance, ES >.50
*

69
Figure 27 – Pre and post intervention comparison of the within group effects of exercise condition on fingertip dexterity. Median scores calculated based on the number of correctly assembled units during the Purdue Pegboard assembly task; *approaching levels of statistical significance; high level of practical significance, ES >.50
Qualitative Data
Medication recall was assessed prior to beginning each cycling session. All five
participants reported taking medication on a daily basis prior to the exercise intervention,
of which two AE participants and both VE participants discontinued medication use
within one week of beginning the cycling intervention; of those who reported
discontinuance, both of the AE participants and one of the VE participants also reported
fewer noticeable occurrences of inattention and distraction.
*

70
CHAPTER 5
DISCUSSION
The effects of acute bouts of VE on executive functioning have been well
recognized in ADHD adolescent populations but there is no known documented research
on the effects of exercise in adult populations. While it is clear that VE positively
influences cognitive and motor processes AE has been shown to facilitate significantly
greater responses in other populations with neuropsychological impairment. The results
of this study have identified similar trends within the young adult female ADHD
population.
Executive Function Findings: Between Group Effects
Consistent with my hypothesis, one of the main findings of this research indicates
that six weeks of assisted cycling three times per week improved functioning in
activation, one of the cognitive clusters associated with executive functioning. According
to Brown’s model of executive function, the activation cluster consists of the cognitive
abilities for planning and activating to work. Activation, organization and planning are
considered to be major impairments for individuals with ADHD (Riccio, Wolge, Romine,
Davis, & Sullivan, 2004; Mitchell, 2012). The activation cognitive cluster was assessed
using the Tower of London outcome measure. To evaluate the activation to work,
executive time in seconds was recorded for each Tower item, the sum of which was
analyzed. The Tower of London score, based on the number of attempts made to achieve
the goal pattern without rule violation assessed cognitive planning. The findings indicate
participants improved in the amount of time it took to organize, strategize, activate and
move the colored balls into the goal pattern positions. Post-intervention, both the AE and

71
VE group decreased the amount of time it took to complete all items as well as fewer
attempts for completion. However, the AE group demonstrated this trend to a greater
degree.
While the decrease in activation time and increase in score approached
conventional levels of significance differences between groups, the effect of AE appears
to be greater for cognitive activation compared to VE. Based on the calculated effect size,
AE accounts for a greater proportion of the variance between groups. There have been no
previous studies designed to evaluate the effects of AE on the specific cognitive
activation characteristic in ADHD but acute bouts of voluntary aerobic exercise have
been found to be a significant predictor of better performance as well as facilitate
significant change during tower tasks administered in typical populations (Berwid &
Halperin, 2012; Chang, Tsai, Hung, So, Chen, Etnier, 2011). In addition, AE has been
found to significantly improve cognitive outcomes in Parkinson’s and Down syndrome,
other special populations with neuropsychological impairment (Alberts et al., 2011;
Ringenbach et al., 2014). The findings of this study are consistent with the research in
that there were improvements in cognitive activation and planning.
Another main finding of this study is that it shows increased improvements in the
memory cluster for the AE group when compared to the voluntary group. Brown’s model
implicates working memory and recall as the primary cognitive characteristics for this
cluster. Working memory is another cognitive impairment frequently observed in
individuals with ADHD (Fassbender et al., 2011). To assess working memory, the
auditory digit span task was utilized. The number of correctly repeated sequences,
forward and backward, was scored and analyzed. While both the forward and backward

72
auditory digit span tasks assess working memory, the backward task also relies heavily
on auditory attention (Hale, Hoepppner & Fiorello, 2012). The median difference
between groups was at the brink of statistical significance for both the forward and
backwards tasks, consistent with other findings. Previous research indicates that working
memory is significantly improved after one 30 minute bout of aerobic exercise during
tasks requiring increased working memory capacity (Pontifex et al, 2009; Hillman,
Erickson & Kramer, 2009). While the research appears to be limited to acute bouts of
exercise and has not been evaluated specifically in ADHD, the findings of this study are
consistent with improvements in working memory found in typical populations.
Executive Function Findings: Within Group Effects
Within the AE group near significant effects were observed between pre and post
intervention assessments in all cognitive clusters except emotion and were greater than
the observed changes in the VE group. In addition none of the outcome measures
approached significance levels of change within VE group. As seen in the between group
comparisons, trends approaching significance in activation and working memory were
observed within AE group. Changes were also observed in the verbal fluency tasks,
which assess the effort required to quickly produce a cognitive output response
(semantic) as well as cognitive efficiency (phonemic). Based on Brown’s model,
cognitive effort requires the cognitive capacity to sustain effort and is highly influential
on processing speed, or cognitive efficiency; characteristics often reported as problematic
in individuals with ADHD (Brown, 2013; Abreu 2013).
Semantic activation requires the capacity and effort to cognitively organize and
filter words and concepts that are associated with the given category. If this process is

73
impaired this can lead to associated word responses that may be related but do not fit the
category. For example, if the category is animals, a correct response would be horse and
an associated but incorrect response would be stable. Effort also involves the cognitive
capacity to recognize and inhibit incorrect responses. Phonemic activation involves
processing speed, or cognitive efficiency, which is better assessed by the phonemic task
due to a greater capacity for related word-sound association that does not require
categorical filtering. While the VE group had only slight improvements in the semantic
and phonemic measures, the AE group approached significant improvement for both
tasks. The effect size also indicates the AE intervention had a tremendous effect on the
outcome. There were no research studies found that have specifically evaluated the effect
of exercise on cognitive effort in ADHD populations but there is evidence of significant
improvements in verbal fluency tasks following six months of aerobic exercise in
populations with mild cognitive impairments as well as typical populations (Baker et al.,
2010; Hillman, Erickson, & Kramer, 2008).
The AE group also demonstrated improvements on the tasks associated with the
cognitive clusters focus, while the VE group showed minimal improvement or no
appreciable change. Dysregulated attention capacity is one of the primary characteristics
associated with ADHD. While most struggle with the inability to focus or sustain
attention for long periods of time, there are often states of hyperfocus that also interfere
with the ability to appropriately shift attention. The Stroop test evaluated these cognitive
abilities with the use of the colored block and incongruent color word tasks. The number
of responses within 45 seconds was recorded and analyzed for each task. The colored
block task assesses focus and attention while the incongruent word task assesses set-

74
shifting. The AE group demonstrated a slight trend for significance in focus and attention
(p = 0.099) and a substantial trend toward significance in set-shifting (p = .060). The
literature in this area does not specifically address AE but the findings are consistent with
improvements in focus and set-shifting capacity following bouts of acute aerobic exercise
in typical young adults as well as older adults with middle cognitive impairment
(Yanagisawa, et al., 2009; Baker et al., 2010). Yanagisawa et al., (2009) also observed
through neuroimaging, post exercise improvements in neural activation, specifically in
the pre-frontal cortex. The increased activity in the prefrontal cortex, associated with
interference processing and response inhibition, is likely a mediating factor for improved
focus and set-shifting abilities.
Dysregulated emotion has been identified as one of the cognitive deficits
associated with ADHD (Baker, 1997). However, the findings of this study failed to
produce any appreciable changes within this cognitive domain for either group. This is
likely due to the small sample size, but may also be explained by the researcher’s failure
to control for the sub-types of ADHD and/or a family history of emotional disorders.
There is evidence suggesting dysregulated emotion is present more so in the combined
inattentive/hyperactive presentation in children but in adults it appears a combined family
history of ADHD and emotional impairment is more predictive of difficulties with
emotion regulation (Wheeler Maegden, 2000; Surman et al., 2011). Even though the
sample population used for this study presented many of the cognitive deficits associated
with ADHD it is unknown if other the other factors associated with dysregulated
emotions were present.

75
Self-regulation is another domain that has been reported to be deficient within the
ADHD population. The findings of this study showed statistical differences approaching
significance only within the AE groups for median classification score. What is most
interesting about this finding is when the scores were individually interpreted based on
the parameters of the scale, two of the AE participants produced categorical scores which
moved them into the moderate self-regulating capacity from a low self-regulating
capacity, while the third participant moved from a moderate capacity to an intact
capacity. Neither of the VE participant’s pre/post evaluation scores differed, one initially
scored and remained at a moderate capacity while the other scored and remained in the
low capacity. Differences approaching conventional levels of significance were observed
in only within the AE group for pre and post median classification scores. Within group
differences and the accompanied interpretation implicates the participants demonstrated
noticeable changes in self-regulating action capacity. There is extremely limited research
on the relationship between self-regulating behaviors and exercise. However, Oaten and
Cheng (2010) found self-regulatory capacity was significantly improved in typical adult
populations after two months of physical exercise.
Although the findings of this study are consistent with previous research, in that
exercise improves executive functioning, the implications for this population are greater
due to the known deficiencies associated with ADHD. If the deficit is greater to begin
with so is the potential for gains. While it is evident that exercise in general improves
executive functioning, the majority of the research evaluates acute bouts and the
immediate effects. Impairments in functioning within the ADHD population are
pervasive and many times life-long. While we know exercise is beneficial, the assisted

76
exercise component is a new area of research that has shown the potential for even
greater benefit in other special populations with neurocognitive disorders.
Motor Function Findings
In addition to executive function, motor function was evaluated through the
Purdue Pegboard tasks for manual dexterity. Fine motor ability and coordination has been
found to be significantly impaired in adolescent ADHD populations (Pitcher, Piek &
Hay, 2003). The Purdue Pegboard is a widely used assessment for the evaluation of fine
motor ability through manual dexterity tasks involving the use of the dominant hand,
non-dominant hand, and both hands combined. Each unimanual and bimanual task
assesses coordination as well as how quickly and accurately the participant works with
their fingers, hands and arms. The assembly task assesses coordination and fingertip
dexterity. Differences approaching significance between exercise groups were
demonstrated in the dominant hand task and the bimanual task. The AE group
demonstrated greater increases in dexterity and coordination compared to the VE group.
Within group comparisons also showed increases the AE group demonstrated greater
increases improved on all manual dexterity tasks while the VE group demonstrated
minimal improvements. Improvements in motor function have been evaluated in other
special populations and the findings of this study are consistent with the research in
Down syndrome and Parkinson’s, populations demonstrating neurocognitive motor
impairments, after bouts of AE (Chen, Ringenbach & Albert, 2014; Alberts et al., 2011).
What is most interesting about the findings is there were improvements in the fine
musculature of the finger, hands and arms, even though they were not exercised. This can
be interpreted as changes occurring at the cortical level of brain rather than a direct

77
physiological change. The AE is thought to increase afferent input via increased intrinsic
feedback mechanisms leading to amplified cortical excitability (Alberts et al., 2011).
Alberts et al., (2011) proposes that the increases in afferent signaling from the Golgi
tendon organs within the lower extremities triggers the release of neurotrophic factors
and dopamine, and may be the mechanism behind the observed improvements in both
executive and motor functioning in populations with cognitive and motor declines.
Conclusion and Future Direction
In conclusion, a six-week, three times per week AE intervention improved
cognitive capacities associated with executive function as well as manual dexterity.
Evaluating the effects of AE is an innovative approach to assessing changes in executive
and motor function among adult ADHD population and to the author’s knowledge is the
first of its kind. Most research has been conducted in typical populations and in children
with ADHD and commonly limited to acute bouts of voluntary aerobic exercise. While
there were clear observable changes in some of the executive and motor function
outcomes, studies with greater number of participants should be conducted in order to
further investigate these findings. The results of this study are also limited to young adult
females with ADHD and future studies involving other populations would be of great
contribution, especially in children and adolescents. Early intervention may have the
potential to greatly reduce the symptoms and deficits associated with the disorder. It
would also be of great benefit for future studies to include additional comparisons using a
control group with ADHD as well as comparing the intervention effects in non-ADHD
populations. Evaluating if there is a dose-response relationship would also aid in tailoring
effective interventions.

78
Gaining a better understanding of the mechanisms involved with the observed
changes is also of great importance. While it can by posited that neurocognitive changes
are related to increases in production and upregulation of dopamine and BDNF, being
able to measure these changes would provide greater insight into changing the
developmental trajectory. While it is possible to evaluate these changes utilizing fMRI
scans this component was beyond the scope of this study. It is evident that exercise
produces changes in executive and motor functioning but in order for researchers to
better observe and differentiate the changes observed between assisted and voluntary
interventions, fMRI scans could be a useful instrument. ADHD follows a lifelong
trajectory of impairment and AE may be one way to positively alter the course of
development leading to improved functioning and quality of life for many individuals.

79
REFERENCES
Abreu, N., Argollo, N., Oliveira, F., Cardoso, A. L., Bueno, J. L., & Xavier, G. F. (2013). Semantic and phonologic verbal fluency tests for adolescents with ADHD. Clinical Neuropsychiatry, 10(2).
Alberts, J. L., Linder, S. M., Penko, A. L., Lowe, M. J., & Phillips, M. (2011). It is not
about the bike, it is about the pedaling: forced exercise and Parkinson's disease. Exercise and Sport Sciences Reviews, 39(4), 177-186.
Arnsten, A. F. (2009). Toward a new understanding of attention-deficit hyperactivity
disorder pathophysiology. CNS Drugs, 23(1), 33-41. Baker, L. D., Frank, L. L., Foster-Schubert, K., Green, P. S., Wilkinson, C. W.,
McTiernan, A., ... & Craft, S. (2010). Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Archives of Neurology, 67(1), 71-79.
Barkley, R. A. (2010). Differential diagnosis of adults with ADHD: the role of executive
function and self-regulation. The Journal of Clinical Psychiatry, 71(7), e17-e17. Berwid, O. G., & Halperin, J. M. (2012). Emerging support for a role of exercise in
attention-deficit/hyperactivity disorder intervention planning. Current Psychiatry Reports, 14(5), 543-551.
Biederman, J., & Faraone, S. V. (2001). Current concepts on the neurobiology of
Attention-Deficit/Hyperactivity Disorder. Journal of Attention Disorders, 6, S7-16.
Biederman, J., Petty, C., Fried, R., Fontanella, J., Doyle, A., Seidman, L., & Faraone, S.
(2006). Impact of psychometrically defined deficits of executive functioning in adults with attention deficit hyperactivity disorder. American Journal of Psychiatry, 163(10), 1730-1738.
Birnbaum, H. G., Kessler, R. C., Lowe, S. W., Secnik, K., Greenberg, P. E., Leong, S. A.,
& Swensen, A. R. (2005). Costs of attention deficit-hyperactivity disorder (ADHD) in the US: excess costs of persons with ADHD and their family members in 2000. Current Medical Research and Opinion®, 21(2), 195-205.
Blum, K., Chen, A. L. C., Braverman, E. R., Comings, D. E., Chen, T. J., Arcuri, V., ... &
Oscar-Berman, M. (2008). Attention-deficit-hyperactivity disorder and reward deficiency syndrome. Neuropsychiatric Disease and Treatment, 4(5), 893.
Brown, J. M., Miller, W. R., & Lawendowski, L. A. (1999). The self-regulation
questionnaire.

80
Brown, T. E. (2013). A new understanding of ADHD in children and adults: Executive function impairments. Routledge.
Brown, T. E. (2006). Executive functions and attention deficit hyperactivity disorder:
Implications of two conflicting views. International Journal of Disability, Development and Education, 53(1), 35-46.
CAASA, (2006). Self-regulation questionnaire. Assessment Instruments. Retreived from
http://casaa.unm.edu/Instruments Carver, J. M. (2009). Attention-Deficit Hyperactivity Disorder (ADHD). Retrieved
March, 29(2009), 851-854. Castellanos, F. X. (1997). Toward a pathophysiology of attention-deficit/hyperactivint
disorder. Clinical Pediatrics, 36(7), 381-393. Castellanos, F. X., Sonuga-Barke, E. J., Milham, M. P., & Tannock, R. (2006).
Characterizing cognition in ADHD: beyond executive dysfunction. Trends in Cognitive Sciences, 10(3), 117-123.
Centers for Disease Control and Prevention (2014). Attention-deficit/hyperactivity
disorder: Symptoms and diagnosis. Retrieved from http://www.cdc.gov/ncbddd/adhd/diagnosis.html.
Centers for Disease Control and Prevention (2013). Attention-deficit/hyperactivity
disorder: Data and statistics. http://www.cdc.gov/ncbddd/adhd/data.html. Centers for Disease Control and Prevention (2008). Youth risk behavior surveillance
system: Selected 2008 national health risk behaviors and health outcomes by sex. Retrieved from http://www. cdc. gov/ healthyyouth /yrbs/pdf/us_disparitysex_yrbs.pdf.
Chaddock, L., Hillman, C. H., Pontifex, M. B., Johnson, C. R., Raine, L. B., & Kramer,
A. F. (2012). Childhood aerobic fitness predicts cognitive performance one year later. Journal of Sports Sciences, 30(5), 421-430.
Chandler, C. (2010). The science of ADHD: A guide for parents and professionals. John
Wiley & Sons. Chang, Y. K., Tsai, C. L., Hung, T. M., So, E. C., Chen, F. T., & Etnier, J. L. (2011).
Effects of acute exercise on executive function: a study with a tower of london task. Journal of Sport and Exercise Psychology, 33(6), 847.
81
Chang, Y. K., Liu, S., Yu, H. H., & Lee, Y. H. (2012). Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Archives of Clinical Neuropsychology : The Official Journal of the National Academy of Neuropsychologists, 27(2), 225-237. doi: 10.1093/arclin/acr094
Chen, C., Ringenbach, S. D. R., & Albert, A. R. (2014). Assisted cycling exercise
improves fine manual dexterity in persons with Down's syndrome. Journal of Applied Research in Intellectual Disabilities, 27(3), 264-272.
Culbertson, W. C., & Zillmer, E. A. (1998). The construct validity of the Tower of
London DX as a measure of the executive functioning of ADHD children. Assessment, 5(3), 215-226.
del Campo, N., Chamberlain, S. R., Sahakian, B. J., & Robbins, T. W. (2011). The roles
of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biological psychiatry, 69(12), e145-e157.
Dishman, R. K., Berthoud, H. R., Booth, F. W., Cotman, C. W., Edgerton, V. R., Fleshner, M. R., . . . Zigmond, M. J. (2006). Neurobiology of exercise. Scandinavian Journal of Medicine & Science in Sports, 16(6), 470-470. doi: 10.1111/j.1600-0838.2006.00610_1.x
DuPaul, G. J., & White, G. P. (2006). ADHD: Behavioral, Educational, and Medication
Interventions. Education Digest: Essential Readings Condensed for Quick Review, 71(7), 57-60.
Etnier, J. L., Nowell, P. M., Landers, D. M., & Sibley, B. A. (2006). A meta-regression to
examine the relationship between aerobic fitness and cognitive performance. Brain Research Reviews, 52(1), 119-130. doi: 10.1016/j.brainresrev.2006.01.002
Faraone, S. V., & Biederman, J. (1998). Neurobiology of attention-deficit hyperactivity
disorder. Biological Psychiatry, 44(10), 951-958. doi: 10.1016/S0006-3223(98)00240-6
Farone, S.V., Biederman, J., & Mick, E. (2006). The age dependent decline of attention
deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychological Medicine, 36(2), 159-165. doi: 10.17/S003329170500471X
Fassbender, C., Schweitzer, J. B., Cortes, C. R., Tagamets, M. A., Windsor, T. A.,
Reeves, G. M., & Gullapalli, R. (2011). Working memory in attention deficit/hyperactivity disorder is characterized by a lack of specialization of brain function. PloS One, 6(11), e27240.

82
Flapper, B. C., Houwen, S., & Schoemaker, M. M. (2006). Fine motor skills and effects of methylphenidate in children with attention-deficit–hyperactivity disorder and developmental coordination disorder. Developmental Medicine & Child Neurology, 48(03), 165-169.
Foley, T. E., & Fleshner, M. (2008). Neuroplasticity of dopamine circuits after exercise:
implications for central fatigue. Neuromolecular Medicine, 10(2), 67-80. Frank-Briggs, A. I., (2011). Attention deficit hyperactivity disorder (ADHD). Journal of
Pediatric Neurology 9(3), 291-298. Gualtieri, C. T., & Johnson, L. G. (2006). Reliability and validity of a computerized
neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology, 21(7), 623-643.
Hale, J. B., Hoeppner, J. A. B., & Fiorello, C. A. (2002). Analyzing digit span
components for assessment of attention processes. Journal of Psychoeducational Assessment, 20(2), 128-143.
Halperin, J. M., & Healey, D. M. (2011). The influences of environmental enrichment,
cognitive enhancement, and physical exercise on brain development: can we alter the developmental trajectory of ADHD?. Neuroscience & Biobehavioral Reviews, 35(3), 621-634.
Harpin, V. A. (2005). The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Archives of Disease in Childhood, 90(suppl 1), i2-i7.
Hervey, A. S., Epstein, J. N., & Curry, J. F. (2004). Neuropsychology of adults with
attention-deficit/hyperactivity disorder: a meta-analytic review. Neuropsychology, 18(3), 485.
Hillman, C. H., Buck, S. M., Themanson, J. R., Pontifex, M. B., & Castelli, D. M. (2009).
Aerobic fitness and cognitive development: Event-related brain potential and task performance indices of executive control in preadolescent children. Developmental Psychology, 45(1), 114-129. doi: http://dx.doi.org/10.1037/a0014437
Hillman, C. H., Erickson, K. I., & Kramer, A. F. (2008). Be smart, exercise your heart:
exercise effects on brain and cognition. Nature Reviews Neuroscience, 9(1), 58-65.
Hummer, T., Kronenberger, W., Wang, Y., Dunn, D., Mosier, K., Kalnin, A., &
Mathews, V. (2011). Executive functioning characteristics associated with ADHD comorbidity in adolescents with disruptive behavior disorders Springer Netherlands. doi: 10.1007/s10802-010-9449-3

83
Hunt, R.D. (2006). Functional roles of norepinephrine and dopamine in ADHD.
Medscape Psychiatry Mental Health, 11(1). Keen, D., & Hadijikoumi, I. (2008). ADHD in children and adolescents. Clinical
Evidence, 2008, 0312. Kelly, K., & Ramundo, P. (2006). You mean I'm not lazy, stupid or crazy?!: the classic
self-help book for adults with attention deficit disorder. Simon and Schuster. Kessler, R., Adler, L., Barkley, R., Biederman, J., Conners, C., Demler, O., ... &
Zaslavsky, A. (2006). The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. American Journal of Psychiatry, 163(4), 716-723.
Klingberg, T., Forssberg, H., & Westerberg, H. (2002). Training of working memory in
children with ADHD. Journal of Clinical and Experimental Neuropsychology, 24(6), 781-791.
Kolar, D., Keller, A., Golfinopoulos, M., Cumyn, L., Syer, C., & Hechtman, L. (2008).
Treatment of adults with attention-deficit/hyperactivity disorder. Neuropsychiatric Disease and Treatment, 4(1), 107.
Koziol, L. F., & Stout, C. E. (1992). Use of a verbal fluency measure in understanding
and evaluating ADHD as an executive function disorder. Perceptual and Motor Skills, 75(3f), 1187-1192.
Lansbergen, M. M., Kenemans, J. L., & van Engeland, H. (2007). Stroop interference and
attention-deficit/hyperactivity disorder: a review and meta-analysis. Neuropsychology, 21(2), 251.
Lenz, T. L. (2012). A Pharmacological/Physiological Comparison between ADHD
Medications and Exercise. American Journal of Lifestyle Medicine, 1559827612443346.
Madras, B. K., Miller, G. M., & Fischman, A. J. (2005). The dopamine transporter and
attention-deficit/hyperactivity disorder. Biological psychiatry,57(11), 1397-1409. Marx, I., Hübner, T., Herpertz, S., Berger, C., Reuter, E., Kircher, T., . . . Konrad, K.
(2010). Cross-sectional evaluation of cognitive functioning in children, adolescents and young adults with ADHD Springer Wien. doi: 10.1007/s00702-009-0345-3
Matza, L. S., Paramore, C., & Prasad, M. (2005). A review of the economic burden of
ADHD. Cost Effectiveness and Resource Allocation, 3(1), 1-9.

84
Miller, W. R., & Brown, J. M. (1991). Self-regulation as a conceptual basis for the
prevention and treatment of addictive behaviours. Self-control and the Addictive Behaviours, 3-79.
Mitchell, J. T. (2012). Cognitive-Behavioral Therapy for Adult ADHD: Targeting
Executive Dysfunction. Archives of Clinical Neuropsychology, 27(8), 934-935. National Centers for Learning disabilities (N.D.). What is Executive Function? Retrieved
from http://www.ncld.org/types-learning-disabilities/executive-function-disorders/what-is-executive-function
National Institutes of Mental Health (N.D.). Attention deficit hyperactivity disorder:
What is attention deficit hyperactivity disorder? Retrieved from http://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
National Institutes of Mental Health (2006). Harvard study suggests significant
prevalence of ADHD symptoms among adults. Retrieved from http://www.nimh.nih.gov/news/science-news/2006/harvard-study-suggests-significant-prevalence-of-adhd-symptoms-among-adults.shtml.
Neumann, A., van Lier, P. A., Gratz, K. L., & Koot, H. M. (2009). Multidimensional
assessment of emotion regulation difficulties in adolescents using the difficulties in emotion regulation scale. Assessment.
Oaten, M., & Cheng, K. (2006). Longitudinal gains in self‐regulation from regular
physical exercise. British Journal of Health Psychology, 11(4), 717-733. Pelham, W. E., Foster, M., & Robb, J. A. (2007). The economic impact of attention-
deficit/hyperactivity disorder in children and adolescents. Journal of Pediatric Psychology, 32(6), 711-727. doi:10.1093/jpepsy/jsm022
Petzinger, G. M., Fisher, B. E., McEwen, S., Beeler, J. A., Walsh, J. P., & Jakowec, M.
W. (2013). Exercise-enhanced neuroplasticity targeting motor and cognitive circuitry in Parkinson's disease. The Lancet Neurology, 12(7), 716-726.
Petzinger, G. M., Walsh, J. P., Akopian, G., Hogg, E., Abernathy, A., Arevalo, P., ... &
Jakowec, M. W. (2007). Effects of treadmill exercise on dopaminergic transmission in the 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine-lesioned mouse model of basal ganglia injury. The Journal of Neuroscience, 27(20), 5291-5300.

85
Piek, J. P., Pitcher, T. M., & Hay, D. A. (1999). Motor coordination and kinaesthesis in boys with attention deficit–hyperactivity disorder. Developmental Medicine & Child Neurology, 41(3), 159-165.
Pitcher, T. M., Piek, J. P., & Hay, D. A. (2003). Fine and gross motor ability in males
with ADHD. Developmental Medicine & Child Neurology, 45(8), 525-535. Polanczyk, G., de Lima, M., Horta, B., Biederman, J., & Rohde, L. (2007). The
worldwide prevalence of ADHD: a systematic review and metaregression analysis. American Journal of Psychiatry, 164(6), 942-948.
Pontifex, M., Hillman, C., Fernhall, B., Thompson, K., & Valentini, T. (2009). The effect
of acute aerobic and resistance exercise on working memory.Medicine+ Science in Sports & Exercise, 41(4), 927.
Powers, J. L. (2004). In J. J. Lagowski (Ed.), Chemistry: Foundations and applications
(pp. 22-23). New York: Macmillan Reference USA. Ribasés, M., Hervás, A., Ramos-Quiroga, J. A., Bosch, R., Bielsa, A., Gastaminza, X., ...
& Bayés, M. (2008). Association study of 10 genes encoding neurotrophic factors and their receptors in adult and child attention-deficit/hyperactivity disorder. Biological psychiatry, 63(10), 935-945.
Riccio, C. A., Wolfe, M. E., Romine, C., Davis, B., & Sullivan, J. R. (2004). The Tower
of London and neuropsychological assessment of ADHD in adults. Archives of Clinical Neuropsychology, 19(5), 661-671.
Ringenbach, S. D., Albert, A. R., Chen, C. C., & Alberts, J. L. (2014). Acute Bouts of
Assisted Cycling Improves Cognitive and Upper Extremity Movement Functions in Adolescents With Down Syndrome. Mental Retardation, 52(2), 124-135.
Sagvolden, T., Johansen, E. B., Aase, H., & Russell, V. A. (2005). A dynamic
developmental theory of attention-deficit/hyperactivity disorder (ADHD) predominantly hyperactive/impulsive and combined subtypes. Behavioral and Brain Sciences, 28(3), 397-418.
Schmolesky, M. T., Webb, D. L., & Hansen, R. A. (2013). The effects of aerobic exercise
intensity and duration on levels of brain-derived neurotrophic factor in healthy men. Journal of Sports Science & Medicine, 12(3), 502.
Seidman, L. J., Doyle, A., Fried, R., Valera, E., Crum, K., & Matthews, L. (2004).
Neuropsychological function in adults with attention-deficit/hyperactivity disorder. Psychiatric Clinics of North America, 27(2), 261-282.

86
Simon, V., Czobor, P., Bálint, S., Mészáros, Á., & Bitter, I. (2009). Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis.The British Journal of Psychiatry, 194(3), 204-211.
Simonen, R. L., Rankinen, T., Pérusse, L., Leon, A. S., Skinner, J. S., Wilmore, J. H., ...
& Bouchard, C. (2003). A dopamine D2 receptor gene polymorphism and physical activity in two family studies. Physiology & Behavior, 78(4), 751-757.
Smith, M., & Segal, R. (2013). Adult ADD/ADHD: Signs, symptoms, effects and
treatment. Retreived from http://www.helpguide.org/mental/adhd_add_adult_symptoms.htm
Stray, L. L., Stray, T., Iversen, S., Ruud, A., Ellertsen, B., & Tonnessen, F. E. (2009). The Motor Function Neurological Assessment (MFNU) as an indicator of motor function problems in boys with ADHD. Behav Brain Funct, 5(1), 22.
Stroth, S., Hille, K., Spitzer, M., & Reinhardt, R. (2009). Aerobic endurance exercise
benefits memory and affect in young adults. Neuropsychological Rehabilitation, 19(2), 223-243.
Surman, C. B., Biederman, J., Spencer, T., Yorks, D., Miller, C. A., Petty, C. R., &
Faraone, S. V. (2011). Deficient emotional self-regulation and adult attention deficit hyperactivity disorder: a family risk analysis. American Journal of Psychiatry, 168(6), 617-623.
Tang, A., Wanchoo, S. J., Swann, A. C., & Dafny, N. (2009). Psychostimulant treatment
for ADHD is modulated by prefrontal cortex manipulation. Brain Research Bulletin, 80(6), 353-358.
Tsai, S. J. (2003). Attention-deficit hyperactivity disorder and brain-derived neurotrophic
factor: a speculative hypothesis. Medical Hypotheses, 60(6), 849-851. Tsai, S. J. (2007). Attention-deficit hyperactivity disorder may be associated with
decreased central brain-derived neurotrophic factor activity: clinical and therapeutic implications. Medical Hypotheses, 68(4), 896-899.
Tseng, M. H., Henderson, A., Chow, S. M., & Yao, G. (2004). Relationship between
motor proficiency, attention, impulse, and activity in children with ADHD. Developmental Medicine & Child Neurology, 46(06), 381-388.
Verret, C., Guay, M. C., Berthiaume, C., Gardiner, P., & Beliveau, L. (2012). A Physical
Activity Program Improves Behavior and Cognitive Functions in Children with ADHD: An Exploratory Study. Journal of Attention Disorders, 16(1), 71-80.
87
Volkow ND, Wang G, Kollins SH, et al. (2009). Evaluating dopamine reward pathway in adhd: Clinical implications. JAMA: The Journal of the American Medical Association, 302(10), 1084-1091.
Wheeler Maedgen, J., & Carlson, C. L. (2000). Social functioning and emotional
regulation in the attention deficit hyperactivity disorder subtypes. Journal of Clinical Child Psychology, 29(1), 30-42.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005).
Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biological Psychiatry, 57(11), 1336-1346.
Wu, J., Xiao, H., Sun, H., Zou, L., & Zhu, L. (2012). Role of dopamine receptors in
ADHD: A systematic meta-analysis. Molecular Neurobiology, 45(3), 605-620. doi: 10.1007/s12035-012-8278-5
Yanagisawa, H., Dan, I., Tsuzuki, D., Kato, M., Okamoto, M., Kyutoku, Y., & Soya, H.
(2010). Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage, 50(4), 1702-1710.
88
APPENDIX A
RECRUITMENT FLYER

89
Are you a young adult (18-24) with ADHD?
Want to earn up to $150?
Researchers at ASU are looking for
volunteers for a 6 week exercise study. To request more information, please visit
our recruitment site or contact us by phone, text or e-mail.
www.surveymonkey.com/s/FFJFFJN
602-430-0525

90
APPENDIX B
CONSENT FORM

91
CONSENT FORM- Individuals with Developmental Disabilities Assisted Cycle Therapy (ACT)
in Persons with Attention-Deficit Hyperactivity Disorder Sensorimotor Development Research Laboratory, ABC1 270
PROGRAM OF KINESIOLOGY, ARIZONA STATE UNIVERSITY
Introduction The purposes of this form are to provide you with information about the nature of this research study and how you will participate in it, if you consent to do so. Signing this form indicates that you have been so informed and you give your consent for to participate. Federal regulations require written informed consent prior to participation in this research study so that you know the nature and risks of participation and can decide whether or not you consent to his participation in a free and informed manner. Researchers Natasha Birchfield, Master’s Degree student and Shannon D. R. Ringenbach, Ph.D., Associate Professor of Kinesiology, invite your voluntary participation in a research study being performed at Arizona State University. Purpose You are invited to participate in a research study to investigate the effects stationary cycling exercise on motor, cognitive and clinical functions in people with Attention-Deficit Hyperactivity Disorder (ADHD). Selection Criteria Any individual with ADHD, between 9 and 60 years old with no physical disabilities is invited to participate. If he/she has or has had an injury or condition that might affect his/her abilities to perform the cycling activities in this experiment, he/she will not be allowed to participate at this time. In addition all participants have been prescreened for cardiovascular fitness by answering ‘No’ to all seven questions of the Physical Activity Readiness Questionnaire or have received exercise clearance from their physician using the Physical Activity Readiness Medical Exam. Procedures Pre and Post Tests On the first visit, we will assess hearing, vision, handedness, receptive language, and perform initial cardiovascular testing which will be used to determine individualized target hart rates. At the beginning of the study, 3 weeks, and end of study we will conduct neuropsychological assessments to measure motor (e.g., manual coordination, grip force), cognitive (e.g., task switching, planning, inhibition, cognitive processing, and working memory), physical health (e.g., waist circumference, functional exercise capacity, Vineland Adaptive Behavior Scale) and mental health (e.g., self-efficacy, social support and emotion regulation). A behavior questionnaire will be completed by the parents/guardians of people under the age of 18 with ADHD. Testing of all of these tests will last approximately between 1 ½ - 2 hours. Intervention First, participants will be randomized into one of three groups: 1) Voluntary exercise 2) Assisted exercise 3) No exercise. Participants in the no exercise intervention will come to the laboratory

92
for pre and post testing and are asked to resume normal routines during the 8 week interval between testing. Participants in both exercise groups will participate in a supervised exercise protocol for eight weeks; three one-hour sessions per week. Each exercise session will be separated by at least one day. Exercise intensity, from an aerobic perspective, will be matched for both exercise groups. Intensity will be determined on an individual basis based on the results of initial cardiovascular testing. Maximum Heart Rate (MHR) intensity will be determined using a formula specialized for persons with developmental disabilities (Fernhall et al., 2001). During exercise, all participants will be kept within 60-80% of their MHR. The participants will be instructed to exercise during the 30 minute main exercise set. The main exercise set will occur between a 5 minute warm-up and a 5 minute cool-down phase. Some participants may be de-conditioned upon study enrollment. Therefore, if necessary, the 30 minute main exercise set will include ‘on the cycle’ rest breaks of 2 minutes, every 10 minutes. To monitor participant’s exercise intensity, the participant will be asked to visually point to and rate their perceived rate of exertion (RPE) on a scale from 1 (easy) to 10 (difficult) every ten minutes. If he/she exhibits signs of cardiac distress (e.g., pressure, tightness, aching, or burning in their upper back, neck, shoulders, and arms, or even in their jaw, or shortness of breath, fatigue, stomach pain, cold sweats, dizziness, indigestion, or nausea, etc.) 911 will be called immediately. The study coordinator will have completed a Cardiac Life Support training course. Risks It is possible that feelings of fatigue or muscle tension may be uncomfortable. There may be cardiovascular risks in participating in any exercise program, which is why we are requiring all participants to complete the Physical Activity Readiness Questionnaire or receive exercise clearance from their physician using the Physical Activity Readiness Medical Exam. An exercise cycle was used instead of a treadmill to eliminate balance and other safety risks. If a medical emergency were to occur during the study we will call 911 to bring emergency medical technicians to the study. For minor complications, you may be treated by a physician at the Campus Health Center. There are no other known risks to participants with this experiment. As with any research, there is some possibility that there are risks that have not yet been identified. There are no known alternatives available for this study. Benefits You will not personally benefit from participation. However, the possible benefit of participation is to develop rehabilitation strategies that will serve to reduce the impact of difficulties with motor, cognitive and health functions for people with ADHD. New Information If the researcher finds new information during the study that would reasonably change your decision about participating, they will provide this information to you. Confidentiality

93
All information obtained and recorded in this study is strictly confidential. The identity of participants will not be revealed in publications that may result from this study, nor will names be used in other research communications such as lectures to scientific meetings. Only summary statistics such as the participants’ age and gender will be included in published experimental results. After the experiment is completed, the principal investigator, Shannon D. R. Ringenbach, Ph.D., will store and lock the signed documents with personal information and data in a filing cabinet in the principal investigator’s lab (ABC 1 270, Program of Kinesiology). All data can be accessed only by the Principal Investigator and her authorized personnel (i.e., graduate research assistants, postdoctoral associates, and research associates) and will be stored indefinitely. Withdrawal Privilege It is okay to say that you do not want to participate. If you agree to participate now, you are free to withdraw without any penalty at any time. If you decide not to participate it will not affect you in any way or harm any relationship you have with Arizona State University. Costs and Payments The researcher wants your decision to be absolutely voluntary. Yet, the researcher recognizes that participation may pose some inconvenience. In order to compensate you, the participants in both exercise groups will be paid $40 at the pretest and mid-test and $70 at the posttest. Participants in the no exercise group will be paid $10 at pretest and $15 at posttest. Liability Side effects or harm are possible in any research program despite the use of high standards of care and could occur through no fault of yours, your participant’s, or the investigator involved, and may require care. You do not give up any of your legal rights by signing this form. In the event of medical emergency arising from this study neither Arizona State University nor the researcher are able to give you any money, insurance, free medical care or compensation. Voluntary Consent Any questions you have concerning the research study or your participation in it, before or after consent can be answered by the Principal Investigator, Dr. Shannon D. R. Ringenbach ([email protected]). If you have any questions about your rights as a participant in this research, or if you feel that you will be placed at risk, you may contact the Chair of Human Subjects Institutional Review Board, through the Office of Research Integrity and Assurance, at (480) 965-6788. Your signature below indicates that you consent to participation. Before giving your consent for participation by signing this form, the methods, inconveniences, risks, and benefits have been explained to you and your questions have been answered. You understand that you may ask questions at any time. You are free to withdraw from the project at any time with no penalty. Participation in this project may be ended by the investigator for reasons that would be explained. This consent form will be filed in a locked filing cabinet with access restricted to the

94
principal investigator, Shannon D. R. Ringenbach, Ph.D., or authorized representatives of the Program of Kinesiology. You understand that you do not give up any of your legal rights by signing this form. A copy of this consent form will be given to you. ____________________________________________________________________ Participant’s Printed Name ________________________________________ ____________________ Participant’s Signature Date Investigator’s Affidavit I have clearly explained to the participant the nature of the above research project. I hereby certify that to the best of my knowledge, the person who is signing this consent form clearly understands the nature, demands, benefits, and risks involved in his/her participation and his/her signature is legally valid. A medical problem or language or educational barrier has not precluded this understanding. _______________________________________ ____________________ Signature of Investigator Date

95
APPENDIX C
VOLUNTARY CYCLING GROUP EXERCISE SESSION DATA SHEET

96
1. Calibrate bike computer (see instructions) 2. Complete medication, diet and exercise recall log 3. Put on Heart rate monitor. -Wet strap with water prior to putting it on -The strap must sit flush on participant’s chest
-Sit participant on bicycle chair for approx 3-4 minutes or until HR stabilizes Take heart rate reading from SRM bike computer – this is RHR. Rest HR: ______ 4. Adjust bicycle seat. Seat Height: __________ Seat Distance: __________ 5. Have participant sit on the bike and strap their feet into the pedals. 6 .Orient the participant to the bicycle and allow them five minutes of practice on the bike at a self-selected rate. Then, RESET the computer by clicking ‘pro’ and ‘set’ simultaneously. 7. Thirty-minutes of cycling exercise intervention 9. Calculate average cadence and HR during 5 minute intervals. Record average cadence and HR from SRM monitor at the end of each minute and calculate averages for each 5 minute interval at the end of the session. Minutes Cadence Avg
Cadence RPE HR Avg
HR 05:00 Warm up 05:00 1 2 3 4 10:00 1 2 3 4 15:00 1 2 3 4 20:00 1 2 3 4 25:00 1 2 3 4 30:00 1 2 3 4 05:00
Cool Down
Notes Peak Cadence: ________
9. Remove HR monitor 10. Let the participant rest for 5 minutes before walking to their car 11. Remind them of their next appointment.
APPENDIX D

97
ASSISTED CYCLING GROUP EXERCISE SESSION DATA SHEET

98
1. Calibrate bike computer (see instructions) 2. Put on Heart rate monitor. -Wet strap with water prior to putting it on -The strap must sit flush on participant’s chest
-Sit participant on bicycle chair for approx 3-4 minutes or until HR stabilizes Take heart rate reading from SRM bike computer – this is RHR. Rest HR: ______ 3. Complete medication, diet and exercise recall log 4. Adjust bicycle seat. Seat Height: __________ Seat Distance: __________ 5. Have participant sit on the bike and strap their feet into the pedals. 6. For day 1, have participant ride the bike for five minutes at their self-selected rate. When five minutes are up hit ‘mode’ to scroll through and find the average heart rate on the bike computer; record Avg Cadence_____. Then RESET the computer by clicking ‘pro’ and ‘set’ simultaneously. 7. Multiple (Avg Cad x 1.35) to find Target Cadence_____. 8. Turn on the bicycle and set the cadence to Target Cad and 30 minutes duration 9. Calculate average cadence and HR during 5 minute intervals. Record average cadence and HR from SRM monitor at the end of each minute and calculate averages for each 5 minute interval at the end of the session. Minutes Cadence Avg
Cadence RPE HR Avg
HR 05:00 Warm up 05:00 1 2 3 4 10:00 1 2 3 4 15:00 1 2 3 4 20:00 1 2 3 4 25:00 1 2 3 4 30:00 1 2 3 4 05:00
Cool Down
Notes Peak Cadence: ________
10. Remove HR monitor 11. Let the participant rest for 5 minutes before walking to their car 12. Remind them of their next appointment.

99
APPENDIX E
TOWER OF LONDON DATA SHEET

100
Tower of London:
• The rules are as follows: 1) Only one ball can be moved at a time. 2) A ball may not be placed on the table or in the top or be held in one hand while
moving a ball with the other hand. 3) A move cannot be changed once the participant has taken his or her hand off the ball. 4) Self-corrections while the hand is still on the ball, are allowed. 5) When rule violation occurs, continue timing and move the ball(s) back to the original
location prior to the violation. • Remind participants of the rule but do not count this as failure. • Time limit: Item 3-4 30 seconds per item.
Item 5-20 45 seconds per item. • Discontinue testing when participants get 4 consecutive scores of 0. • Any rule violation needs to be recorded.
Item Executive time Time Limit Note 3 30s 4 30s 5 45s 6 45s 7 45s 8 45s 9 45s 10 45s 11 45s 12 45s 13 45s 14 45s 15 45s 16 45s 17 45s 18 45s 19 45s 20 45s
The participant earns three points if a solution is reached in only one attempt, two points if the solution is reached in two attempts, one point if the solution is reached in three attempts and zero points if the solution is not reached in three attempts. Therefore, the total score can range from 0 to 36 points.
APPENDIX F

101
STROOP TEST DATA SHEET
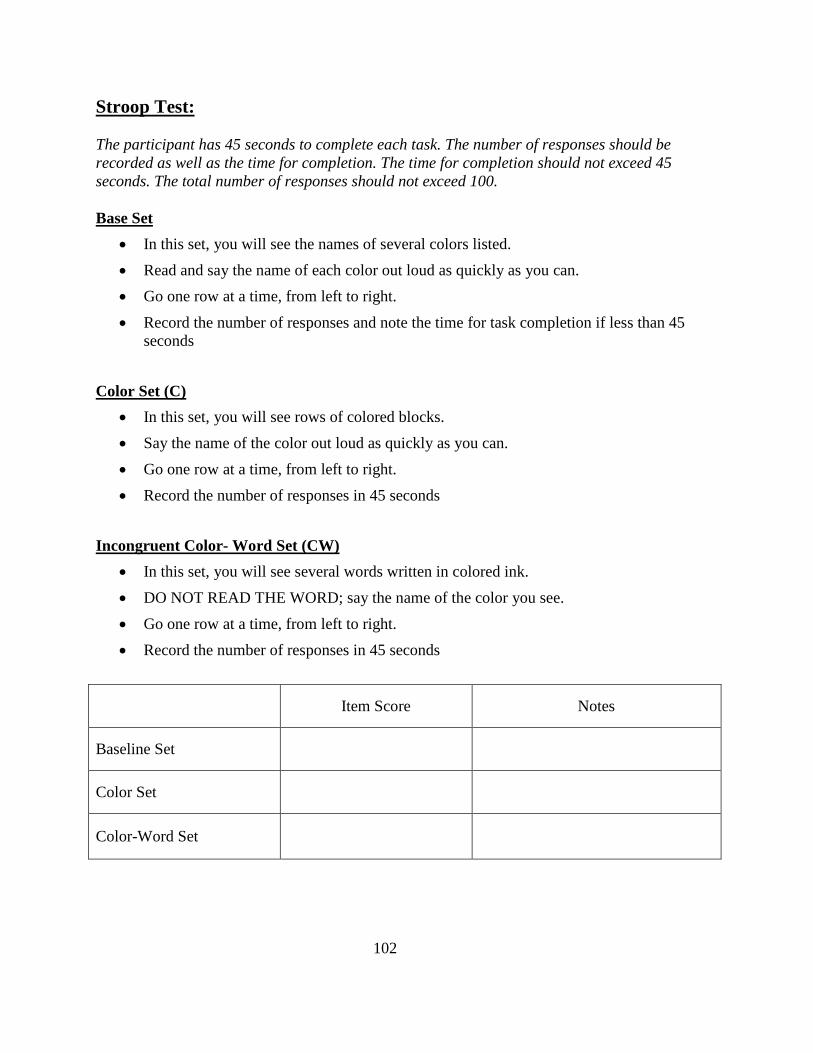
102
Stroop Test: The participant has 45 seconds to complete each task. The number of responses should be recorded as well as the time for completion. The time for completion should not exceed 45 seconds. The total number of responses should not exceed 100. Base Set
• In this set, you will see the names of several colors listed.
• Read and say the name of each color out loud as quickly as you can.
• Go one row at a time, from left to right.
• Record the number of responses and note the time for task completion if less than 45 seconds
Color Set (C)
• In this set, you will see rows of colored blocks.
• Say the name of the color out loud as quickly as you can.
• Go one row at a time, from left to right.
• Record the number of responses in 45 seconds
Incongruent Color- Word Set (CW)
• In this set, you will see several words written in colored ink.
• DO NOT READ THE WORD; say the name of the color you see.
• Go one row at a time, from left to right.
• Record the number of responses in 45 seconds
Item Score Notes
Baseline Set
Color Set
Color-Word Set

103
APPENDIX G
VERBAL FLUENCY DATA SHEET

104
Verbal Fluency:
• 60 seconds per category • Instruct the participant to say as many words as they can think of corresponding to each
given category
Total Interval Semantic
1. Animals 2. Food or Drinks
0”-15”
16”-30”
31”-45”
45”-60”
Total Words

105
Total Interval Phonemic
1. S words 2. F words
0”-15”
16”-30”
31”-45”
45”-60”
Total Words
Scores (Semantic items):_________________ Scores (Phonemic items):________________ Total scores (Semantic + Phonemic): __________________

106
APPENDIX H
DIFFICULTIES IN EMOTION REGULATION SCALE

107
Emotion Regulation
Please indicate how often the following statements apply to you by circling the appropriate
number that corresponds with the scale below:
1 Almost never
2 Sometimes
3
About half the time
4 Most of the time
5 Almost always
1. I am clear about my feelings
1 2 3 4 5
2. I pay attention to how I feel
1 2 3 4 5
3. I experience my emotions as overwhelming and out of control
1 2 3 4 5
4. I have no idea how I am feeling
1 2 3 4 5
5. I have difficult making sense out of my feelings
1 2 3 4 5
6. I am attentive to my feelings
1 2 3 4 5
7. I know exactly how I am feeling
1 2 3 4 5
108
1 Almost never
2 Sometimes
3
About half the time
4 Most of the time
5 Almost always
8. I care about what I am feeling
1 2 3 4 5
9. I am confused about how I feel
1 2 3 4 5
10. When I’m upset, I acknowledge my emotions
1 2 3 4 5
11. When I’m upset, I become angry with myself for feeling that way
1 2 3 4 5
12. When I’m upset, I become embarrassed for feeling that way
1 2 3 4 5
13. When I’m upset I have difficulty getting work done
1 2 3 4 5
14. When I’m upset, I become out of control
1 2 3 4 5
15. When I’m upset, I believe that I will remain that way for a long time
1 2 3 4 5
16. I believe that I’ll end up feeling very depressed
1 2 3 4 5
17. When I’m upset, I believe that my feelings are valid and important
1 2 3 4 5

109
1 Almost never
2 Sometimes
3
About half the time
4 Most of the time
5 Almost always
18. When I’m upset, I have difficulty focusing on other things
1 2 3 4 5
19. When I’m upset, I feel out of control
1 2 3 4 5
20. When I’m upset, I can still get things done
1 2 3 4 5
21. When I’m upset, I feel ashamed with myself for feeling that way
1 2 3 4 5
22. When I’m upset, I know that I can find a way to eventually feel better
1 2 3 4 5
23. When I’m upset, I feel like I am weak
1 2 3 4 5
24. When I’m upset, I feel like I can remain in control of my behaviors
1 2 3 4 5
25. When I’m upset, I feel guilty for feeling that way
1 2 3 4 5
26. When I’m upset, I have difficulty concentrating
1 2 3 4 5
27. When I’m upset, I have difficulty controlling my behaviors
1 2 3 4 5

110
1 Almost never
2 Sometimes
3
About half the time
4 Most of the time
5 Almost always
28. When I’m upset, I believe that there is nothing I can do to make myself feel better
1 2 3 4 5
29. When I’m upset, I become irritated with myself for feeling that way
1 2 3 4 5
30. When I’m upset, I start to feel very bad about myself
1 2 3 4 5
31. When I’m upset, I believe that wallowing in it is all I can do
1 2 3 4 5
32. When I’m upset, I lose control over my behaviors
1 2 3 4 5
33. When I’m upset, I have difficulty thinking about anything else
1 2 3 4 5
34. When I’m upset, I take time to figure out what I’m really feeling
1 2 3 4 5
35. When I’m upset, it takes me a long time to feel better
1 2 3 4 5
36. When I’m upset, my emotions feel overwhelming
1 2 3 4 5

111
APPENDIX I
AUDITORY NUMBER MEMORY DATA SHEET

112
Auditory Number Memory : • The experimenter reads loudly and at a slow pace by following the order. The participant
is request to repeat the numbers. Discontinue testing when participant has failed two consecutive sets of numbers in the same # of length sequence.
Forward Example: 3 – 1, 4 – 2
6 – 4 2 – 5 3 - 1 – 6 7 - 4 – 9 6 - 9 - 5 – 7 3 - 6 - 9 – 2 8 - 3 - 9 - 4 – 6 5 - 1 - 7 - 3 – 9 4 - 2 - 5 - 1 - 8 – 7 5 - 8 - 4 - 9 - 3 – 6 1 - 5 - 3 - 8 - 4 - 9 – 7 9 - 4 - 2 - 7 - 3 - 1 – 6 9 - 3 - 7 - 5 - 1 - 6 - 8 – 4 2 - 6 - 4 - 8 - 3 - 2 - 1 – 5
Total Forward ___________
• The experimenter reads loudly and at a slow pace by following the order. The participant is request to repeat the numbers in reverse sequence. Discontinue testing when participant has failed two consecutive sets of numbers in the same # of length sequence.
Backward Example: 2 – 3, 7 – 1
5 – 3 4 – 2 3 - 1 – 5 6 - 9 – 2 9 - 2 - 6 – 4 1 - 8 - 6 – 3 7 - 9 - 6 - 2 – 5 3 - 5 - 8 - 4 - 1 2 - 8 - 3 - 1 - 6 – 9 8 - 6 - 1 - 9 - 4 – 7 6 - 4 - 8 - 2 - 9 - 3 – 1 3 - 7 - 4 - 9 - 6 - 2 – 8
Total Backward ___________

113
APPENDIX J
SELF-REGULATION QUESTIONNAIRE

114
SRQ
Please answer the following questions by circling the response that best describes how you are. If you STRONGLY DISAGREE with a statement, circle 1; if you DISAGREE circle 2; if you are UNCERTAIN or UNSURE circle 3; if you AGREE circle 4; if you STRONGLY AGREE circle 5. There are no right or wrong answers. Work quickly and don't think too long about your answers. Strongly
Disagree Disagree Uncertain
or Unsure
Agree Strongly Agree
1. I usually keep track of my progress toward my goals.
1 2 3 4 5
2. My behavior is not that different from other people's.
1 2 3 4 5
3. Others tell me that I keep on with things too long.
1 2 3 4 5
4. I doubt I could change even if I wanted to.
1 2 3 4 5
5. I have trouble making up my mind about things.
1 2 3 4 5
6. I get easily distracted from my plans. 1 2 3 4 5
7. I reward myself for progress toward my goals.
1 2 3 4 5
8. I don't notice the effects of my actions until it's too late.
1 2 3 4 5
9. My behavior is similar to that of my friends.
1 2 3 4 5
10. It's hard for me to see anything helpful about changing my ways
1 2 3 4 5
11. I am able to accomplish goals I set for myself.
1 2 3 4 5
12. I put off making decisions. 1 2 3 4 5
13. I have so many plans that it's hard for me to focus on any one of them.
1 2 3 4 5

115
Strongly Disagree
Disagree Uncertain or Unsure
Agree Strongly Agree
14. I change the way I do things when I see a problem with how things are going.
1 2 3 4 5
15. It's hard for me to notice when I've “had enough” (alcohol, food, sweets).
1 2 3 4 5
16. I think a lot about what other people think of me.
1 2 3 4 5
17. I am willing to consider other ways of doing things.
1 2 3 4 5
18. If I wanted to change, I am confident that I could do it.
1 2 3 4 5
19. When it comes to deciding about a change, I feel overwhelmed by the choices.
1 2 3 4 5
20. I have trouble following through with things once I've made up my mind to do something.
1 2 3 4 5
Strongly Disagree Uncertain Agree Strongly
1 2 3 4 5
21. I don't seem to learn from my mistakes.
1 2 3 4 5
22. I'm usually careful not to overdo it when working, eating, drinking.
1 2 3 4 5
23. I tend to compare myself with other people.
1 2 3 4 5
24. I enjoy a routine, and like things to stay the same.
1 2 3 4 5
25. I have sought out advice or information about changing.
1 2 3 4 5
26. I can come up with lots of ways to change, but it's hard for me to decide which one to use.
1 2 3 4 5
27. I can stick to a plan that's working well.
1 2 3 4 5

116
Strongly Disagree
Disagree Uncertain or Unsure
Agree Strongly Agree
28. I usually only have to make a mistake one time in order to learn from it.
1 2 3 4 5
29. I don't learn well from punishment. 1 2 3 4 5
30. I have personal standards, and try to live up to them.
1 2 3 4 5
31. I am set in my ways. 1 2 3 4 5
32. As soon as I see a problem or challenge, I start looking for possible solutions.
1 2 3 4 5
33. I have a hard time setting goals for myself.
1 2 3 4 5
34. I have a lot of willpower. 1 2 3 4 5
35. When I'm trying to change something, I pay a lot of attention to how I'm doing.
1 2 3 4 5
36. I usually judge what I'm doing by the consequences of my actions.
1 2 3 4 5
37. I don't care if I'm different from most people.
1 2 3 4 5
38. As soon as I see things aren't going right I want to do something about it.
1 2 3 4 5
39. There is usually more than one way to accomplish something.
1 2 3 4 5
40. I have trouble making plans to help me reach my goals.
1 2 3 4 5
41. I am able to resist temptation. 1 2 3 4 5
42. I set goals for myself and keep track of my progress.
1 2 3 4 5
43. Most of the time I don't pay attention to what I'm doing.
1 2 3 4 5

117
Strongly Disagree
Disagree Uncertain or Unsure
Agree Strongly Agree
44. I try to be like people around me. 1 2 3 4 5
45. I tend to keep doing the same thing, even when it doesn't work.
1 2 3 4 5
46. I can usually find several different possibilities when I want to change something.
1 2 3 4 5
47. Once I have a goal, I can usually plan how to reach it.
1 2 3 4 5
48. I have rules that I stick by no matter what.
1 2 3 4 5
49. If I make a resolution to change something, I pay a lot of attention to how I'm doing.
1 2 3 4 5
50. Often I don't notice what I'm doing until someone calls it to my attention.
1 2 3 4 5
51. I think a lot about how I'm doing. 1 2 3 4 5
52. Usually I see the need to change before others do.
1 2 3 4 5
53. I'm good at finding different ways to get what I want.
1 2 3 4 5
54. I usually think before I act. 1 2 3 4 5
55. Little problems or distractions throw me off course.
1 2 3 4 5
56. I feel bad when I don't meet my goals. 1 2 3 4 5
57. I learn from my mistakes. 1 2 3 4 5
58. I know how I want to be. 1 2 3 4 5

118
Strongly Disagree
Disagree Uncertain or Unsure
Agree Strongly Agree
59. It bothers me when things aren't the way I want them.
1 2 3 4 5
60. I call in others for help when I need it. 1 2 3 4 5
61. Before making a decision, I consider what is likely to happen if I do one thing or another.
1 2 3 4 5
62. I give up quickly. 1 2 3 4 5
63. I usually decide to change and hope for the best.
1 2 3 4 5

119
APPENDIX K
PURDUE PEGBOARD DATA SHEET

120
Purdue Pegboard Score:
• “This is a task to see how quickly and accurately you can work with your hands.” Instruction to right/left hand (begin with dominant hand:
• “Pick up one pin at a time with your right (left) hand from the right (left) -handed cup. Starting with the top hole, place each pin in the right (left) -handed row, starting from the first hole and working down the line. Now, you can practice this by putting some pins into the holes.”
• “When I say ‘Begin’, place as many as pins possible in the right (left) -handed row, starting with the top hole and working down the line. Make sure to pick up one pin at a time and you use only your right (left) hand only. Work as fast as you possibly can until I say ‘Stop’”
• Have the participant do 2 practice trials and ensure they understand the instructions • Count the number of pins inserted and record it as right (left) hand score.
Instruction to both hands:
• “This time you will use both hands at the same time. Pick up a pin with your right hand from the right-handed cup and at the same time pick up a pin with your left hand from the left-handed cup. Starting with the top hole of both rows and working down. Make sure that you are placing both of the pins into the holes at the same time. Now, you can practice by putting some pins into the holes.”
• “When I say ‘Begin’, place as many pins as possible in both rows starting with the top holes and working down the line. Work as fast as you can until I say ‘Stop’”
• Have the participant do 2 practice trials and ensure they understand the instructions • Count the number of pins inserted and record it as both hands score.
Instruction to Right + Left + Both: • Add the scores for right hand, left hand and both hands. This is the score for R+L+B.
Instruction to Assembly:
• “Pick up one pin at a time with your right hand from the right-handed cup. While you are placing the pin in the hole in the right-handed row, pick up a washer with your left hand. As soon as the pin has been placed, drop the washer over the pin. While the washer is being placed over the pin with your left hand, pick up a collar with your right hand. While the collar is being dropped over the pin, pick up another washer with your left hand and drop it over the collar.”
• “Now, you can practice assemblies.” Have the participant do 2 practice trials and ensure they understand the instructions.
• Each assembly consists of a pin, a washer, a collar and a washer. • Count the number of completely assembled objects inserted and record the score.
Trial One Trial Two Trial Three Trial average

121
Right Hand (30s)
Left Hand (30s)
Both Hands (30s)
Right + Left + Both
Assembly (60s)